Network Psychiatry Investigating models of mental constructs and disorders with complex systems and Bayesian Artificial Intelligence Giovanni Briganti Th` ese d´ efendue pour l’obtention du grade de Docteur en Sciences M´ edicales Jury Prof. Samuel Leistedt, MD, PhD, Promoteur, Universit´ e de Mons Prof. Paul Linkowski, MD, PhD, Co-Promoteur, Universit´ e libre de Bruxelles Prof. Alexandre Legrand, MD, PhD, Pr´ esident du Jury, Universit´ e de Mons Dr. Quoc Lam Vuong, PhD, Secr´ etaire du Jury, Universit´ e de Mons Prof. Pierre Manneback, PhD, Universit´ e de Mons Prof. Christophe Lelubre, MD, PhD, Universit´ e de Mons Prof. Adelin Albert, PhD, Universit´ e de Li` ege Prof. Pierre Thomas, MD, PhD, Universit´ e de Lille
Transcript
Network Psychiatry
Investigating models of mental constructs and disorders
with complex systems and Bayesian Artificial Intelligence
Giovanni Briganti
These defendue pour l’obtention du grade de Docteur en Sciences Medicales
Jury
Prof. Samuel Leistedt, MD, PhD, Promoteur, Universite de Mons
Prof. Paul Linkowski, MD, PhD, Co-Promoteur, Universite libre de Bruxelles
Prof. Alexandre Legrand, MD, PhD, President du Jury, Universite de Mons
Dr. Quoc Lam Vuong, PhD, Secretaire du Jury, Universite de Mons
Prof. Pierre Manneback, PhD, Universite de Mons
Prof. Christophe Lelubre, MD, PhD, Universite de Mons
Prof. Adelin Albert, PhD, Universite de Liege
Prof. Pierre Thomas, MD, PhD, Universite de Lille
Network Psychiatry
Investigating models of mental constructs and disorders with complex
systems and Bayesian Artificial Intelligence
Giovanni Briganti
Abstract
Inspired by the network approach to psychopathology, this thesis aims to investigate several
mental constructs and disorders with complex systems and Bayesian Artificial Intelligence
in order to model interactions among construct features and symptoms, evaluate their re-
spective importance in the determination of the network structure, as well as offer new
methodological perspectives to be used in network studies.
This work is organized as follows: first, an introduction to the network approach in psy-
chiatric research and potentially in clinical practice will be introduced. Second, a statistical
introduction to the network techniques, both frequentist and Bayesian will be offered to the
reader. Third, I will investigate from a network perspective several important psychiatric
constructs found in the general population. Fourth, I will translate the network approach to
psychiatric disorders using both nonclinical and clinical samples. Finally, I will discuss the
implications of this work as well as set further challenges based on my analyses.
1
List of publications
The publications resulting from this dissertation are listed below.
Briganti, G., Kempenaers, C., Braun, S., Fried, E. I., and Linkowski, P. (2018). Network
analysis of empathy items from the interpersonal reactivity index in 1973 young adults.
Psychiatry Research, 265:87–92.
Briganti, G., Fried, E. I., and Linkowski, P. (2019). Network analysis of Contingencies
of Self-Worth Scale in 680 university students. Psychiatry Research, 272:252–257.
Briganti, G. and Linkowski, P. (2019). Exploring network structure and central items
of the narcissistic personality inventory. International Journal of Methods in Psychiatric
Research, e1810.
Briganti, G. and Linkowski, P. (2019). Item and domain network structures of the Re-
silience Scale for Adults in 675 university students. Epidemiology and Psychiatric Sciences,
pages 1–9.
Briganti, G. and Linkowski, P. (2019). Network approach to items and domains from
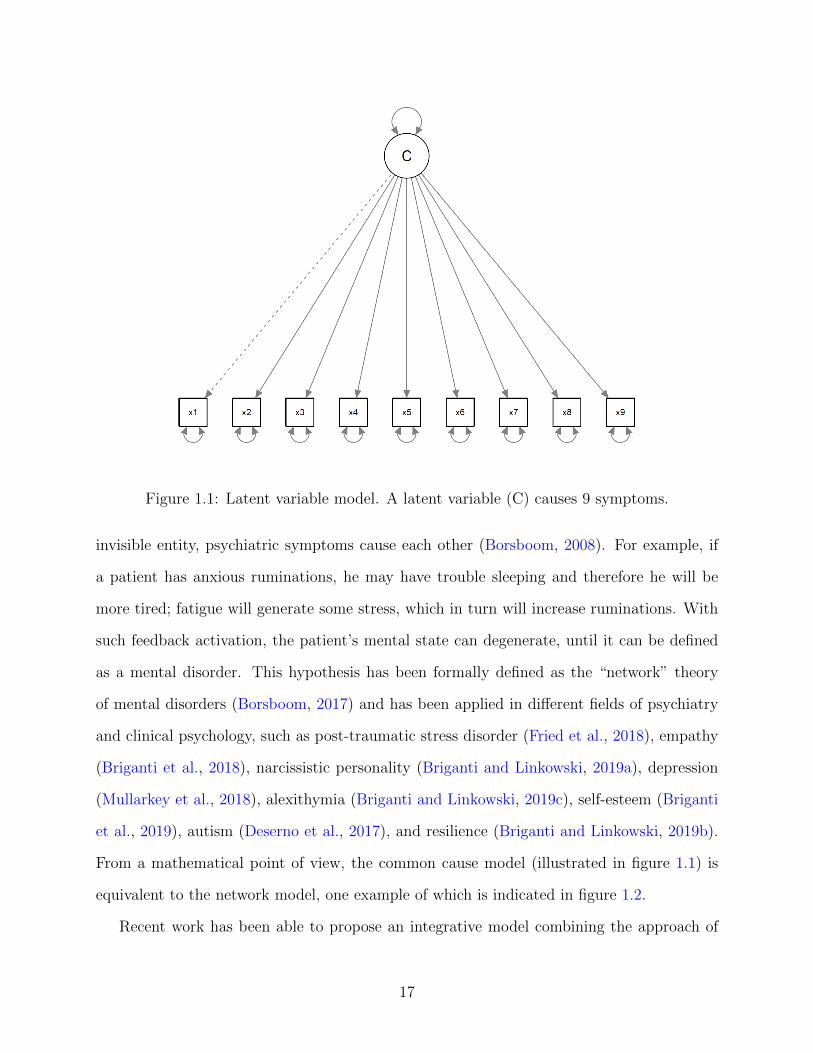
invisible entity, psychiatric symptoms cause each other (Borsboom, 2008). For example, if
a patient has anxious ruminations, he may have trouble sleeping and therefore he will be
more tired; fatigue will generate some stress, which in turn will increase ruminations. With
such feedback activation, the patient’s mental state can degenerate, until it can be defined
as a mental disorder. This hypothesis has been formally defined as the “network” theory
of mental disorders (Borsboom, 2017) and has been applied in different fields of psychiatry
and clinical psychology, such as post-traumatic stress disorder (Fried et al., 2018), empathy
(Briganti et al., 2018), narcissistic personality (Briganti and Linkowski, 2019a), depression
(Mullarkey et al., 2018), alexithymia (Briganti and Linkowski, 2019c), self-esteem (Briganti
et al., 2019), autism (Deserno et al., 2017), and resilience (Briganti and Linkowski, 2019b).
From a mathematical point of view, the common cause model (illustrated in figure 1.1) is
equivalent to the network model, one example of which is indicated in figure 1.2.
Recent work has been able to propose an integrative model combining the approach of
17
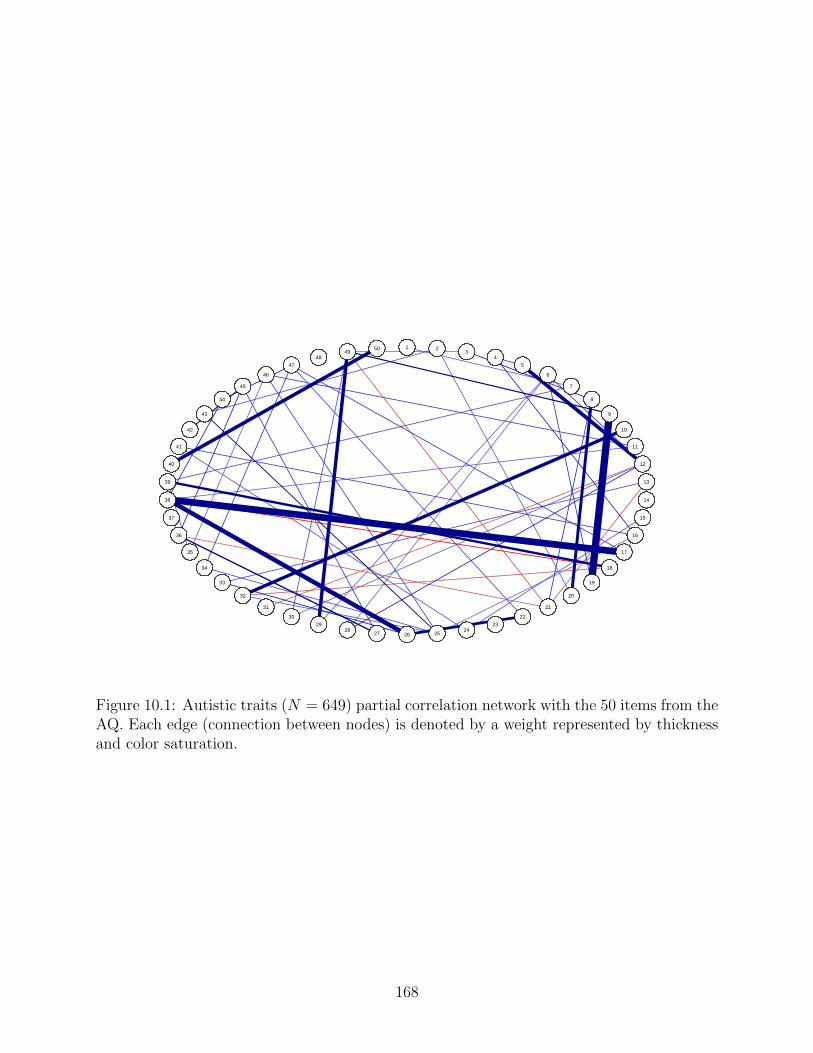
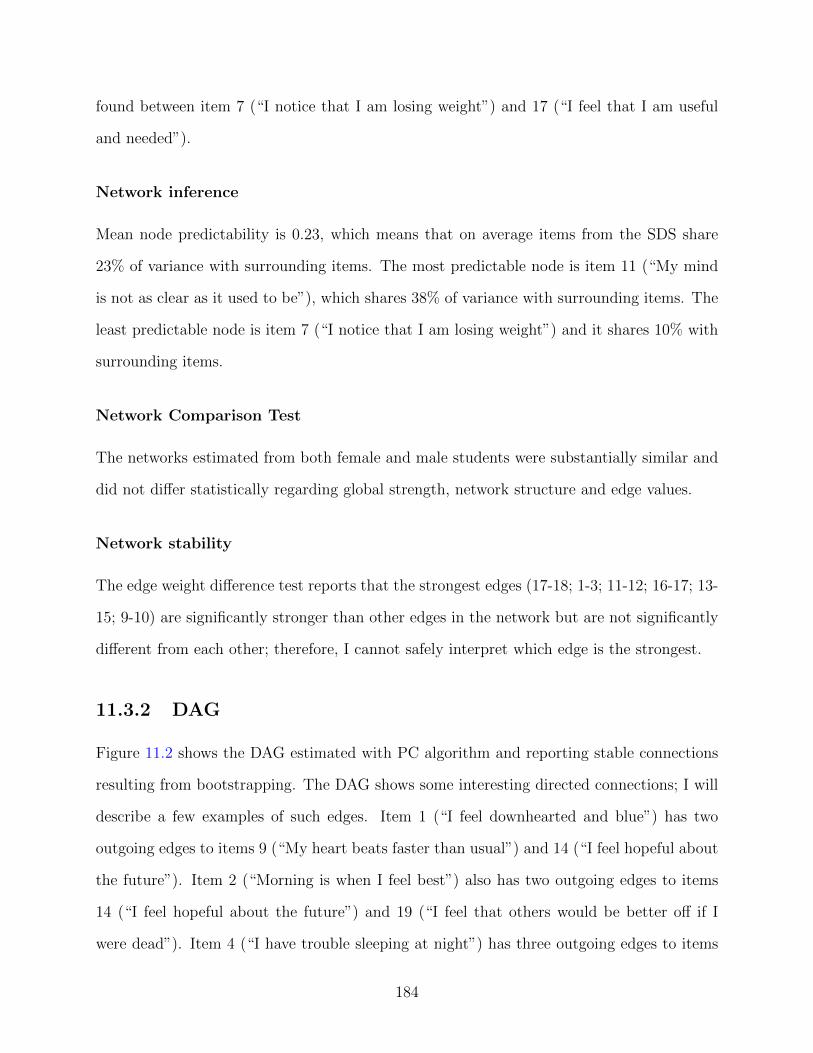
Figure 1.2: The network model. Variables (nodes) interact through connections (edges).Positive edges are colored in blue, negative edges are colored in red. The correspondingthickness of an edge denotes its intensity (weight).
18
latent variables with the network approach: in this approach, called generalized network
psychometrics (Epskamp et al., 2017b) the symptoms can be caused by different latent
variables and interact with each other. This approach has proven useful in simplifying the
analysis of networks based on psychometric scales, where different dimensions are represented
by several redundant items. Once the redundancy is limited by representing the symptoms by
the latent variables that it measures, for example a particular domain of a mental construct,
such as the contribution of self-opinion in the construct of self-esteem (Briganti et al., 2019),
an interaction between the different latent variables is observed. Some work has been able
to demonstrate that new tools, such as exploratory graphical analysis (Golino and Epskamp,
2017), specifically designed for the detection of domains in networks (translate “factors” in
the approach by latent variables) is capable of detecting the correct number of dimensions
in a sample; if the number detected is not the same, a new model is proposed which is better
suited to the sample data.
The aim of this work is to offer a general introduction to network psychiatry, paying
particular attention to the implications that the development of this approach can have on
the diagnosis and treatment of mental disorders. I detail the challenges, opportunities and
main criticisms that have been described in the literature in this area, which has evolved
rapidly in the last decade. I will first describe the structure and composition of a psychiatric
network. Next, I will detail the different processes for estimating a psychiatric network.
Third, I will detail the different measures used to interpret the results of a network, as well
as their stability and accuracy. Finally, I will discuss the main applications that this approach
could develop in current clinical practice. The main criticisms of the network approach will
be integrated as the different methodologies are introduced.
19
Figure 1.3: An undirected network with three nodes (A, B, and C). The three nodes areconnected by two edges, A-B, and A-C. A-B is thicker than A-C; it has a greater weight.
1.2 Structure and composition of a psychiatric network
1.2.1 Elements composing a network
A network is composed of a set of nodes, connected through a set of edges (Boccaletti et al.,
2006).
A node represents a measured entity. In other areas, nodes represent people (social
network), stations, or cities. Networks can also explore brain regions via neuroimaging
(neuroanatomical networks). In psychiatry, nodes represent either observed symptoms/signs
(in the context of mental disorders) or other parts of mental constructs (such as empathy,
narcissism, or resilience). In graphic visualization, nodes are usually represented by circles,
squares or even triangles.
An edge represents a connection (or absence of connection, depending on the network
model that is chosen) between two nodes. An edge is usually interpreted as the presence (or
absence) of interaction, or morbidity, or causality between two entities. The interpretation
of the edge depends on the network model that is estimated. For example, if I choose to
explore the rail network of a region, an edge will represent the railway that connects two
stations. Likewise, a social network will use the edges to indicate a mutual relationship
between two people. The edges can be observed (the observer knows a priori that two nodes
20
are connected) or else unobserved (the presence or absence of a relationship between two
nodes must therefore be tested, by defining a null hypothesis and an alternative hypothesis).
1.2.2 Types of networks
There are different types of networks. Below I will detail the types of networks most used
in psychiatry.
Undirected network, weighted or unweighted
An undirected network is a structure with nodes connected by edges whose direction is
unknown. An example of an undirected network is illustrated in figure 1.3. The edge A-B
connecting nodes A and B, could, in an undirected network, assume 3 possible directions:
A to B, B to A, or symmetrically from A to B and vice-versa. The edges of an undirected
network can have a weight, reflecting the relative importance of one edge compared to others.
The weight of the edge is most often represented by a thicker link. Networks containing
weights are called weighted networks; weightless networks are unweighted.
To understand the importance of weighting, let’s take the example of three known symp-
toms of depression (Zung, 1965) that could underlie the figure 1.3: insomnia (A), fatigue (B),
and suicidal ideation (C). Insomnia could be linked to suicidal ideation as well as fatigue, but
its connection to fatigue is much more clinically important than to suicidal ideation. The
edge weights are used precisely to express this difference between the connections within a
network.
In weighted networks, edge weights can be positive (denoting a positive association be-
tween two nodes) or negative (representing a negative association). Figure 1.4 shows a
network with a positive association (A-B) and a negative association (A-C).
Weighted undirected networks are the most used networks in clinical and methodological
research (Epskamp and Fried, 2018). Edges most often represent partial correlations.
21
Figure 1.4: An undirected weighted network with three nodes (A, B, and C). The threenodes are connected by two edges, A-B and A-C. A-B denotes a positive connection. A-Cdenotes a negative connection. A-B has a greater weight than A-C.
Directed network, cyclic or acyclic
Some works use advanced statistical methods to determine a causal relationship between
two nodes (Moffa et al., 2017), even in cross-sectional data, using machine learning methods
(Scutari, 2010). These methodologies use so-called “directed” networks since the direction
of the edges is determined (Briganti et al., 2020b). There are two types of directed net-
works: cyclic and acyclic. Although their use is less popular than undirected networks, it is
important to know the basic structures of directed networks since a directed structure could
be the “ground truth” which underlie certain symptoms of mental disorders. If underlying
during the analysis of an undirected network, directed networks can generate unexpected
results that can be difficult to interpret.
Two examples of acyclic directed networks are proposed in the figures 1.5 and 1.6.
In figure 1.5, two nodes B and C cause the node A. This structure is also known under the
name of “V-structure”, or “collider” and constitutes the basis for the automatic learning of
the algorithms which will discover the structure underlying the analyzed data (Scutari, 2010).
The collider structure is useful since it stores temporal information at a given instant. For
example, if nodes B and C represent two police officers pointing a weapon against a criminal
(node A), I can, by determining the status of A (0 = dead, 1 = alive), and one of the two
22
Figure 1.5: An acyclic directed network composed of three nodes A, B, and C. B and Ccause A. This is commonly defined as a collider situation.
Figure 1.6: An acyclic directed network composed of three nodes A, B, and C. A causes B,B causes C.
23
Figure 1.7: A cyclic directed network composed of three nodes A, B, and C. A causes B, Bcauses C, and C causes A.
police officers (0 = did not fire, 1 = fired), infer the status of the other police officer.
In figure 1.6, A cause B which in turn causes C. C does not cause A, which leaves the
loop open.
The loop is however closed in the figure 1.7, representing a cyclic directed network.
Cyclic networks are most often encountered in time series, where repeated measurements of
psychiatric parameters are made to control the mental state. Cyclical directed networks could
be useful in order to show the existence of a “critical slowing down” of symptoms: during the
deterioration of a mental state, the prediction between the symptoms in a network becomes
more concrete (Wichers and Groot, 2016).
1.3 An introduction to the estimation of a psychiatric
network
This constitutes a brief and clinical introduction to the estimation of network models used in
clinical research. A statistical introduction of the methods used in this thesis can be found
in Chapters 2 and 3.
24
1.3.1 Conditional dependence and independence
The presence of an edge in a network can mean the presence or absence of a connection
between two nodes. This depends on whether the estimation of a network aims to detect the
presence of a conditional dependence or a conditional independence (Williams et al., 2019).
A conditional dependence is understood as an association between two variables when a
third variable is set. Conditional independence is understood as the absence of association
between two variables when a third variable is fixed at given levels (Epskamp et al., 2017b).
1.3.2 Partial correlations
Most often, the edges between the nodes are estimated in the form of partial correlations,
one of the statistical translation of the theoretical concept of conditional dependence relation
(Epskamp and Fried, 2018). A network of partial correlations will look like the models
proposed in the figures 1.2 and 1.4: a weighted network not directed. The partial correlations
will be positive or negative, reflecting a corresponding association between the nodes.
How to interpret the presence of a positive partial correlation between two variables X
and Y found in a network of psychiatric symptoms such as collected with self-administered
scales? From a statistical point of view, I can affirm that, if a partial correlation is present
between X and Y, that implies that, by controlling all the other variables of the network, a
connection exists between the two nodes (Briganti et al., 2018).
To translate this mathematical explanation into clinical practice, a possible interpretation
is as follows: by controlling all the other symptoms, if X and Y share a connection, this means
that in the observed sample the average response of the observed group to question X will
be able to predict that of Y and vice-versa, since the network is undirected (Briganti et al.,
2019). In practice, if I observe a partial correlation between two symptoms insomnia and
fatigue, I can deduce that if the observed group has on average significant insomnia, it will
also present significant fatigue, controlling the levels of other network symptoms.
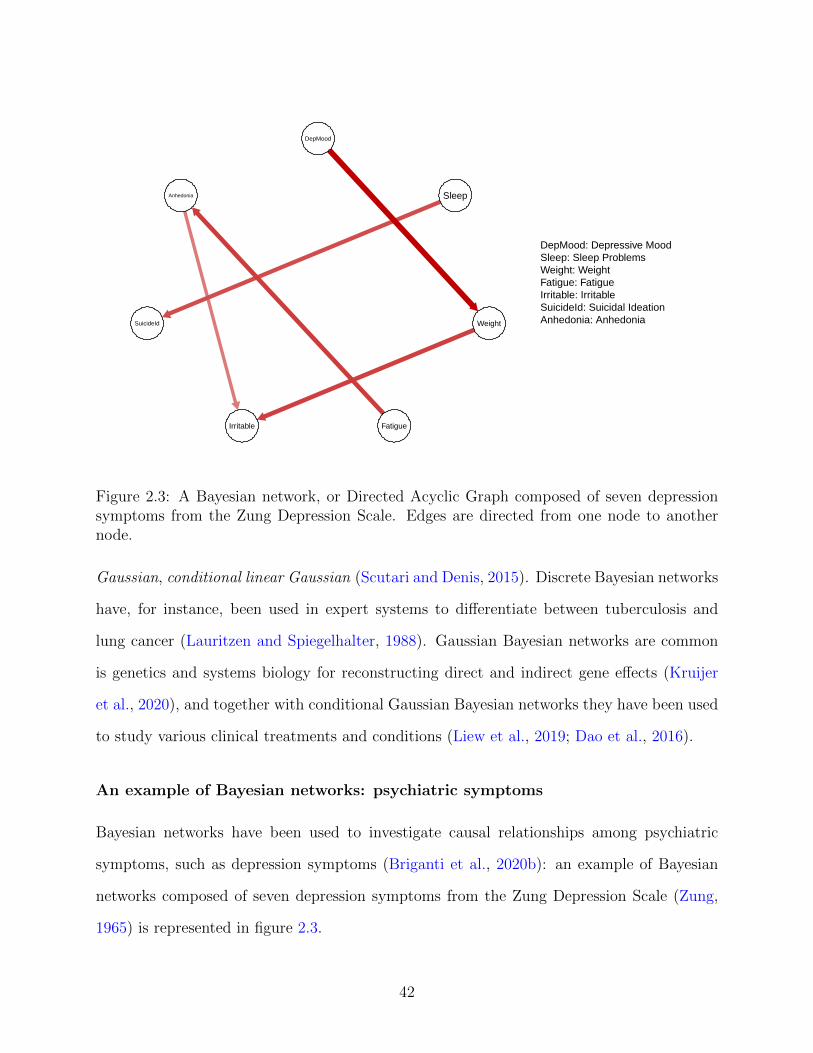
Figure 2.3: A Bayesian network, or Directed Acyclic Graph composed of seven depressionsymptoms from the Zung Depression Scale. Edges are directed from one node to anothernode.
Gaussian, conditional linear Gaussian (Scutari and Denis, 2015). Discrete Bayesian networks
have, for instance, been used in expert systems to differentiate between tuberculosis and
lung cancer (Lauritzen and Spiegelhalter, 1988). Gaussian Bayesian networks are common
is genetics and systems biology for reconstructing direct and indirect gene effects (Kruijer
et al., 2020), and together with conditional Gaussian Bayesian networks they have been used
to study various clinical treatments and conditions (Liew et al., 2019; Dao et al., 2016).
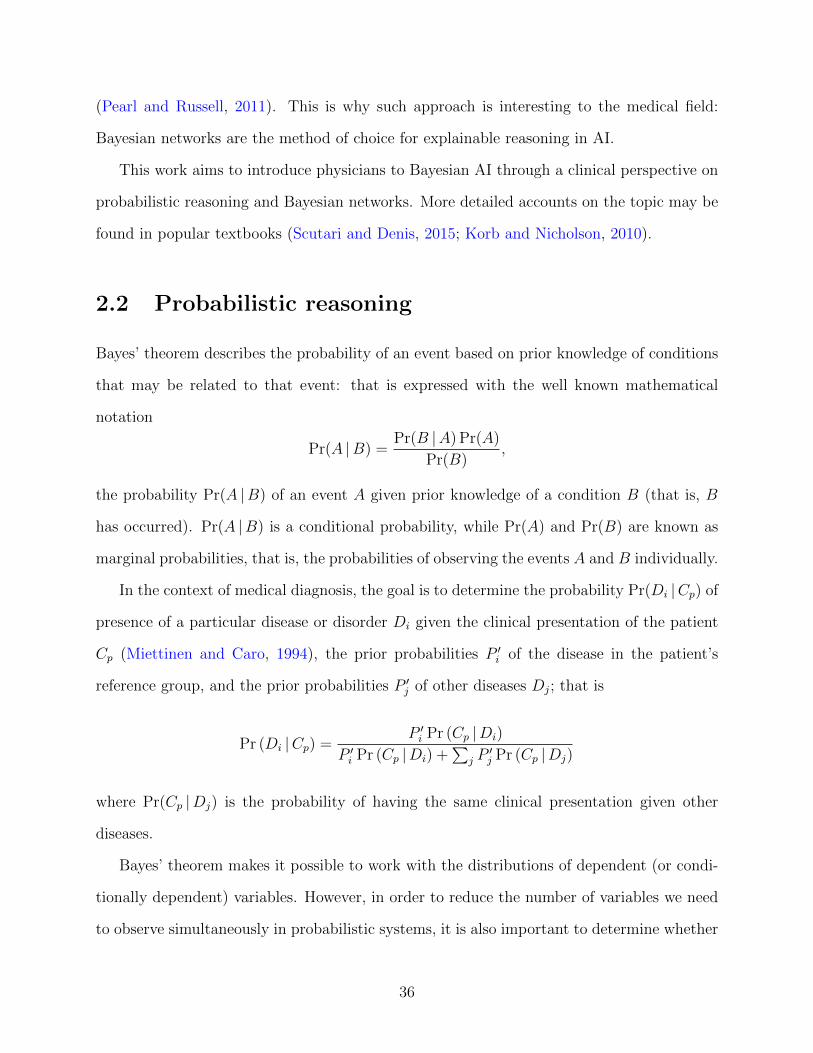
An example of Bayesian networks: psychiatric symptoms
Bayesian networks have been used to investigate causal relationships among psychiatric
symptoms, such as depression symptoms (Briganti et al., 2020b): an example of Bayesian
networks composed of seven depression symptoms from the Zung Depression Scale (Zung,
1965) is represented in figure 2.3.
42
Such Bayesian networks are computed from a data set of symptom scores: edges there-
fore represent admissible causal relationships among symptoms (Moffa et al., 2017). In the
example shown in figure 2.3, for instance, depressive mood has a causal relationship directed
towards weight loss, which in turn has a causal relationship directed towards irritability.
2.5 Difference between neural networks and Bayesian
networks
Neural networks, often called Artificial Neural Networks (ANNs), are in widespread use
in the AI field. They represent networks of interconnected artificial neurons that change
their state with the external or internal information that flows through the network during
a learning phase (Hecht-Nielsen, 1990). Neural networks are usually organised in several
layers: an input layer, several intermediate layers of latent variables, and an output layer.
Their aim is to identify a relationship between the input and the output. Hence they are
discriminative models, and do not provide any insight into the interplay of the variables nor
a semantic representation of causes and effects. They are known to be difficult to interpret
(Correa et al., 2009), to the point that post hoc methods to improve their interpretability
and explainability are now a challenging new avenue for research(Holzinger et al., 2019). The
key advantage of Bayesian networks is that they model of the real world: the phenomenon
under investigation is understood by the machine, dissected, and clearly represented as a
set of causal relationships. This allows for a predictive reasoning much needed in medicine:
Bayesian networks can answer diagnostic and prognostic questions of the form “how will
symptom/sign/disease A change if we act upon symptom/sign/disease B?” in a way that is
understandable by both patients and clinicians. This is possible because of the reversibility
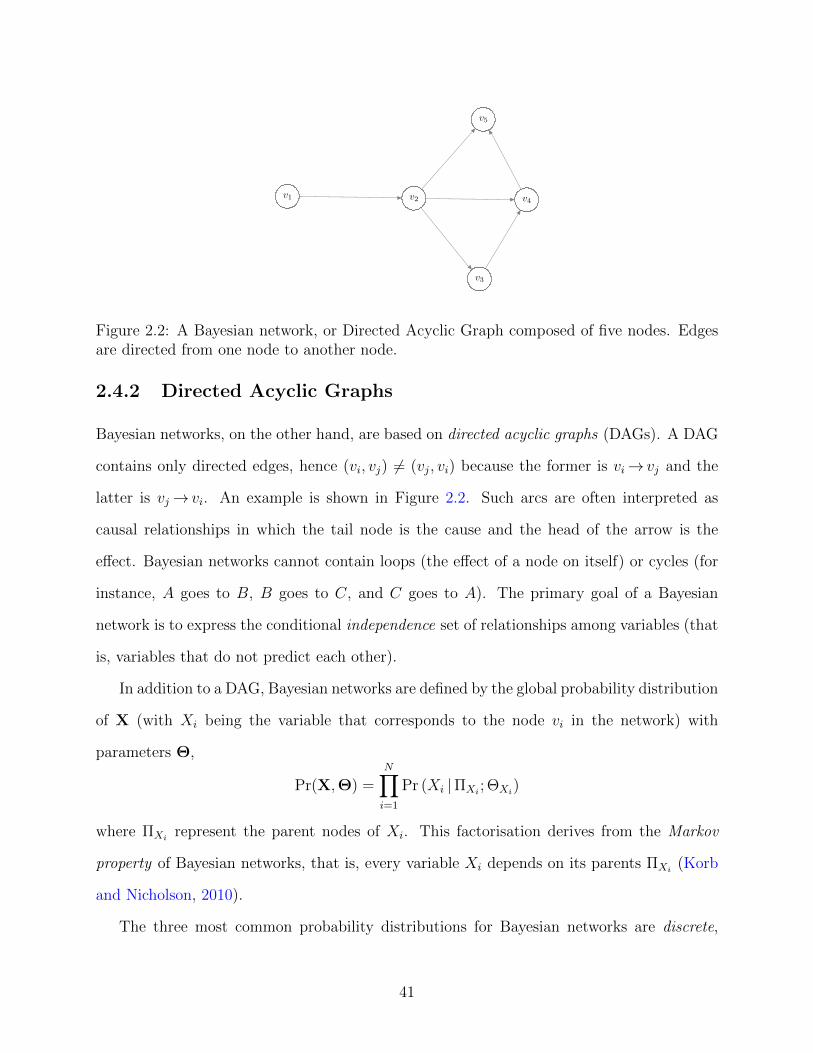
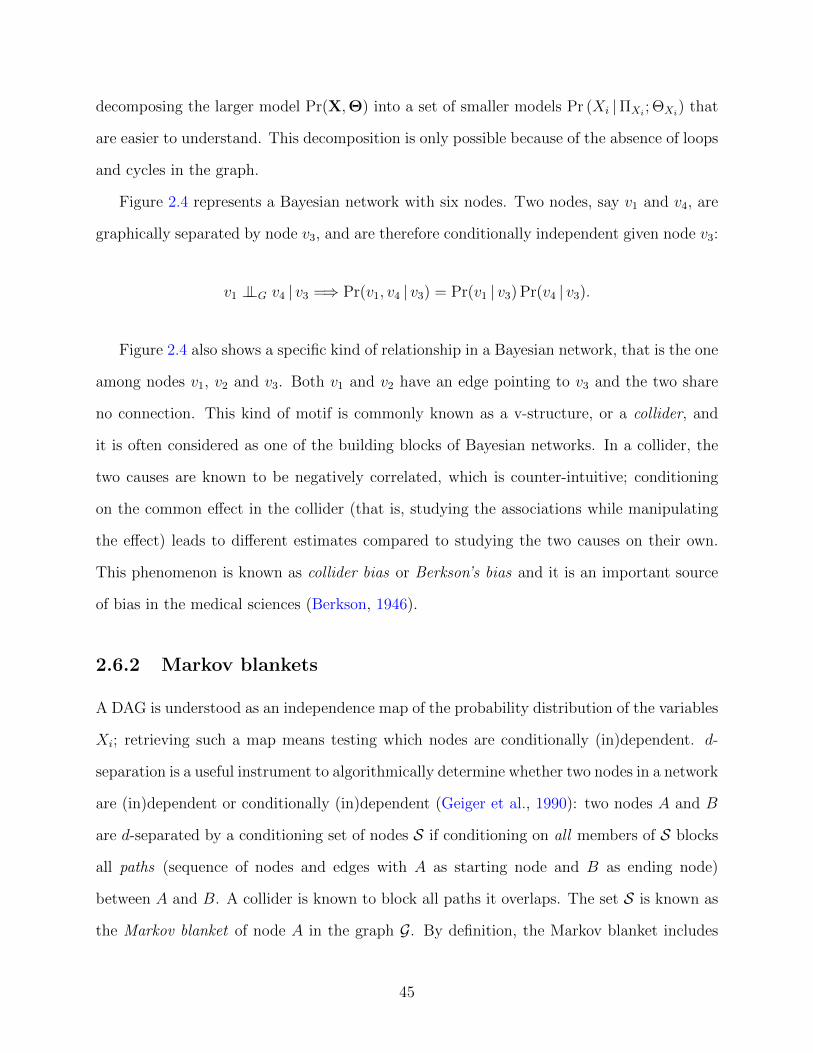
Figure 2.4: A Bayesian network of six nodes to illustrate graphical separation (meaning twonodes are not connected in the network). For instance, 1 is separated from 4 and 5 through3; 2 is separated from 4 and 5 through 3, and 3 is separated from 6 through 5.
2.6 Structure learning of Bayesian networks
In this section we will introduce the concepts of graphical separation and probabilistic inde-
pendence.
2.6.1 The Markov property
In Bayesian networks, if two nodes are unconnected (that is, they do not share an edge),
that means that they are also conditionally independent: this is called the Markov property
(Korb and Nicholson, 2010). Graphical separation implies probabilistic independence,
A ⊥⊥G B |C =⇒ A ⊥⊥P B |C.
making the network itself is a clear representation of the conditional independence rela-
tionships between nodes. For this reason, the DAG is called an independence map of the
variables. The Markov property makes it possible to write
Pr(X,Θ) =N∏i=1
Pr (Xi |ΠXi ; ΘXi) ,
44
decomposing the larger model Pr(X,Θ) into a set of smaller models Pr (Xi |ΠXi ; ΘXi) that
are easier to understand. This decomposition is only possible because of the absence of loops
and cycles in the graph.
Figure 2.4 represents a Bayesian network with six nodes. Two nodes, say v1 and v4, are
graphically separated by node v3, and are therefore conditionally independent given node v3:
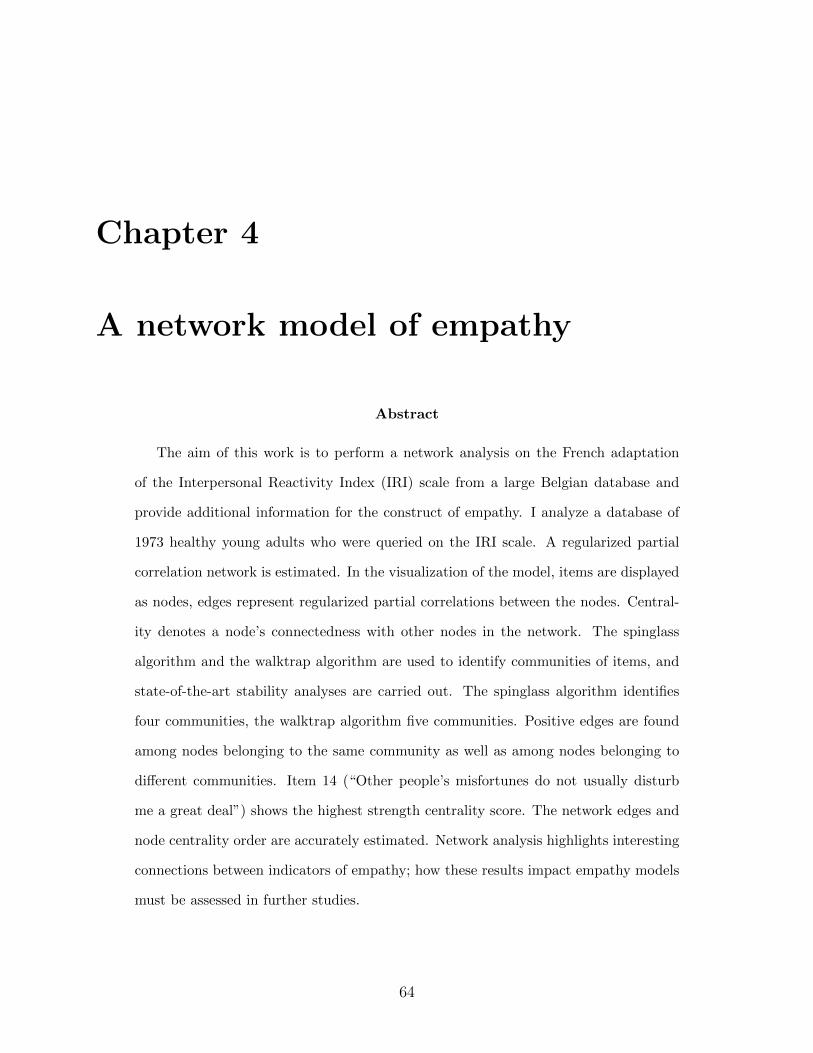
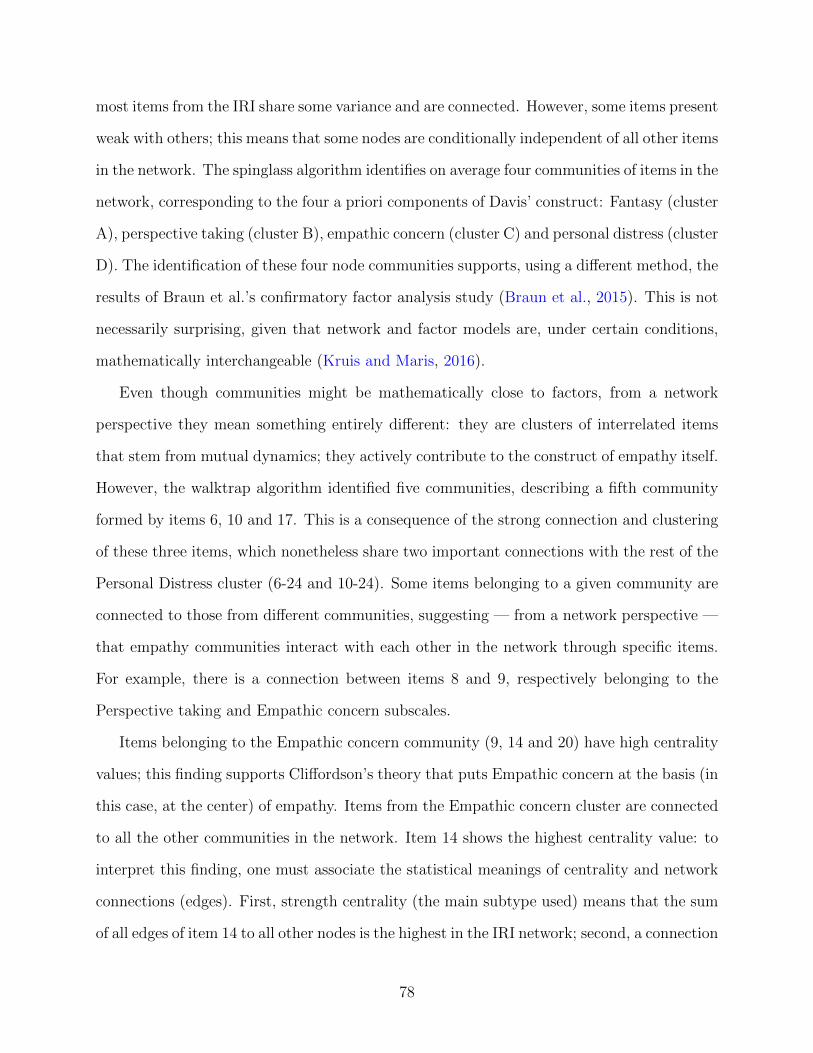
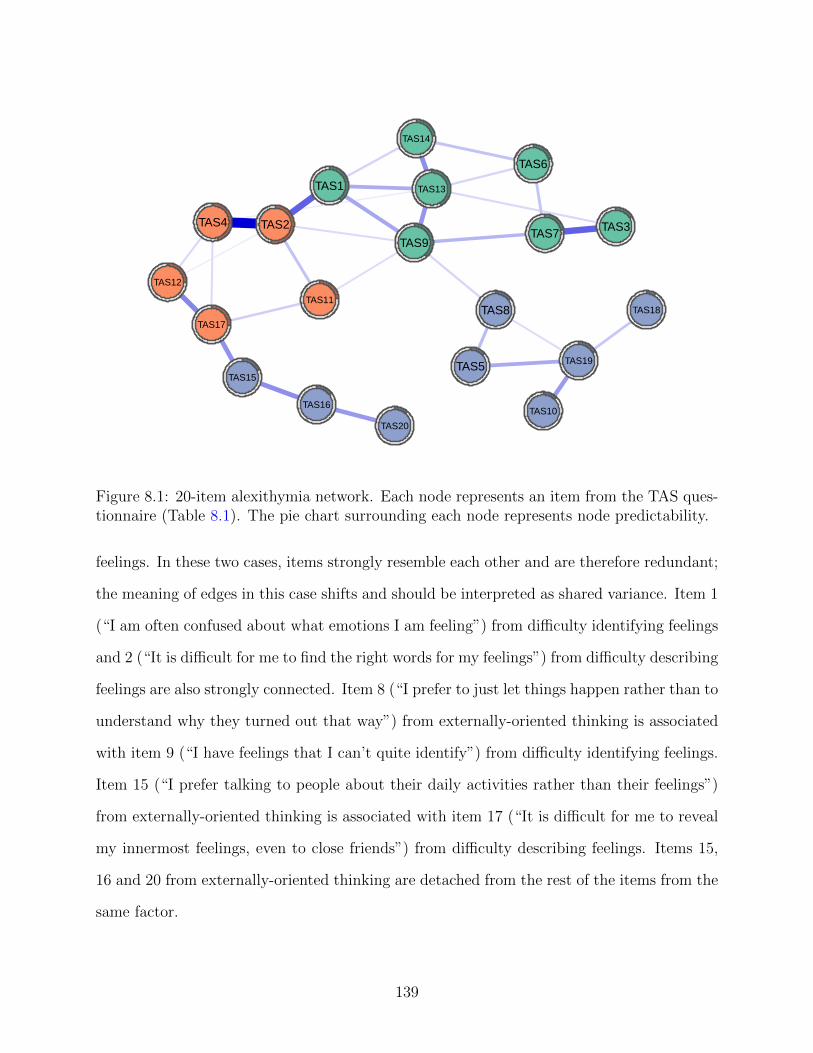
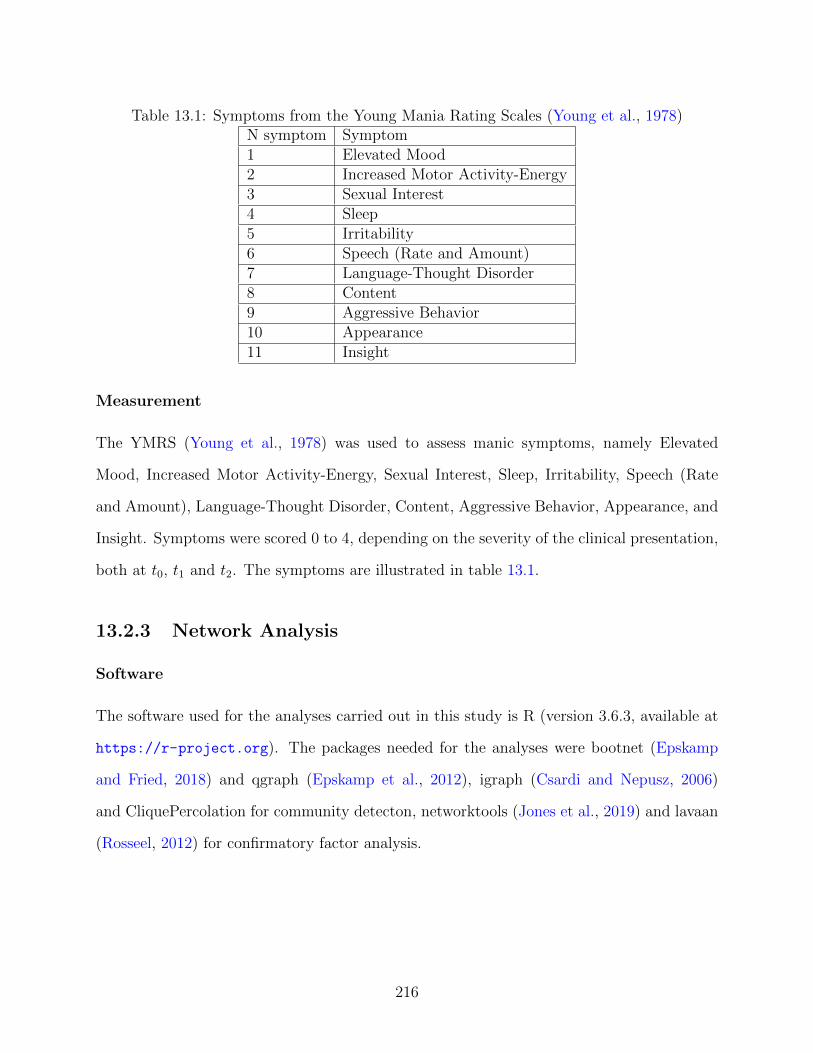
Figure 4.1: Network composed of the 28-item IRI. Each item is represented by a node(1 to 28) and belongs to a different community of empathy, indicated by a code in thecolumn on the right: Fantasy Scale (FS), Perspective Taking (PT), Empathic Concern (EC)and Personal Distress (PD). Reversed items are marked with an R (e.g. 7FS R indicatesa reversed item). Blue lines are positive connections, red lines are negative connections.The thickness of the line represents the connection strength. Colored areas in the ringssurrounding the nodes represent the node predictability (percentage of variance of a givennode explained by surrounding nodes).
74
et al., 2015). Cluster A is composed of items 1, 16, 23, 26, 5, 12, 7, forming the Fantasy
component (FS). Cluster B is formed by items 25, 28, 21, 8, 11, 15, 3, all of which constitute
the Perspective-taking component (PT). Cluster C is formed by items 22, 20, 2, 14, 18, 4, 9
and reflects the Empathic concern component (EC). Cluster D is formed by items 10, 17, 6,
24, 27, 13, 19 and represents the Personal distress component (PD).
The walktrap algorithm identifies 5 communities of items. Most items belong to the same
communities in the spinglass solution above, whereas items 6 (“In emergency situations, I
feel apprehensive and ill-at-ease”), 10 (“I sometimes feel helpless when I am in the middle
of a very emotional situation”) and 17 (“Being in a tense emotional situation scares me”)
form a new community of items (community 5).
Furthermore, in some cases, two items from different communities (as identified by the
spinglass algorithm) have a positive connection: for example, this is the case of item 1 (“I
daydream and fantasize, with some regularity, about things that might happen to me”) and
item 10 (“I sometimes feel helpless when I am in the middle of a very emotional situation”),
item 23 (“When I watch a good movie, I can very easily put myself in the place of a leading
character”) and item 22 (“I would describe myself as a pretty soft-hearted person”), item 8
(“I try to look at everybody’s side of a disagreement before I make a decision”) and item 9
(“When I see someone being taken advantage of, I feel kind of protective towards them”).
Mean node predictability is 0.27, which means that on average, 27% of the variance of each
node is explained by its neighbors: assuming that all edges go to the node under investigation
from its neighbors, I can see how well the given node can be predicted by the other nodes
surrounding it (Haslbeck and Fried, 2017).
4.3.2 Network inference
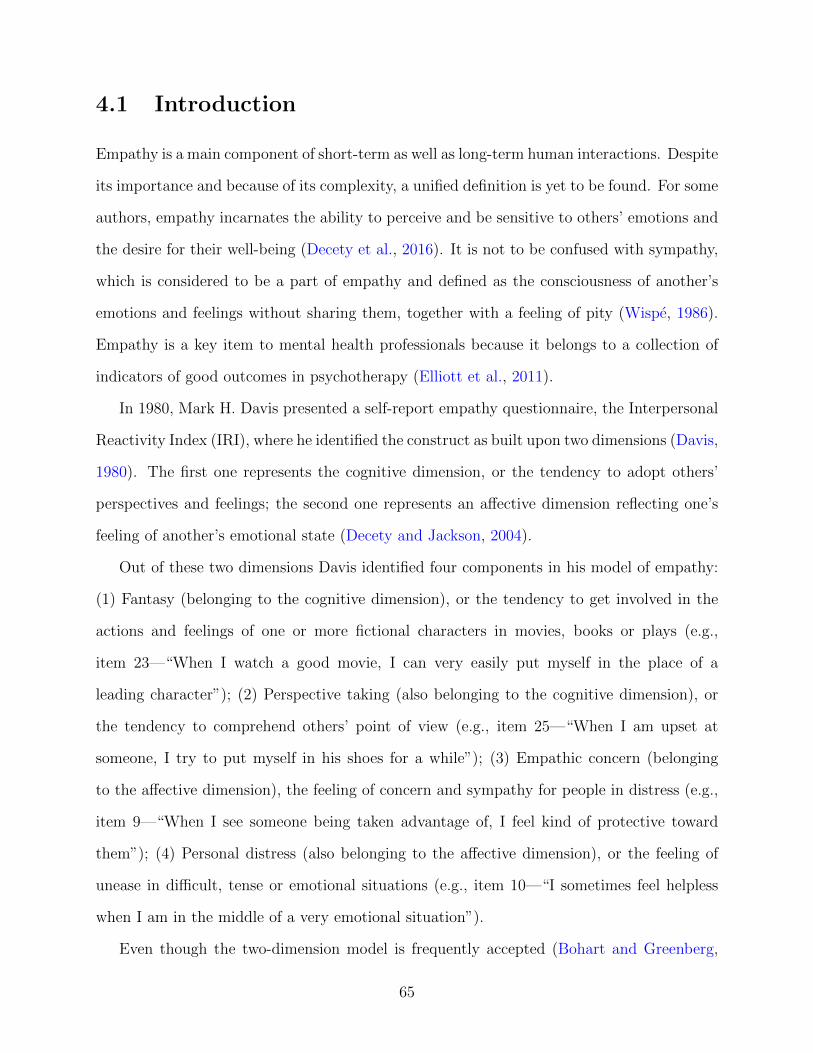
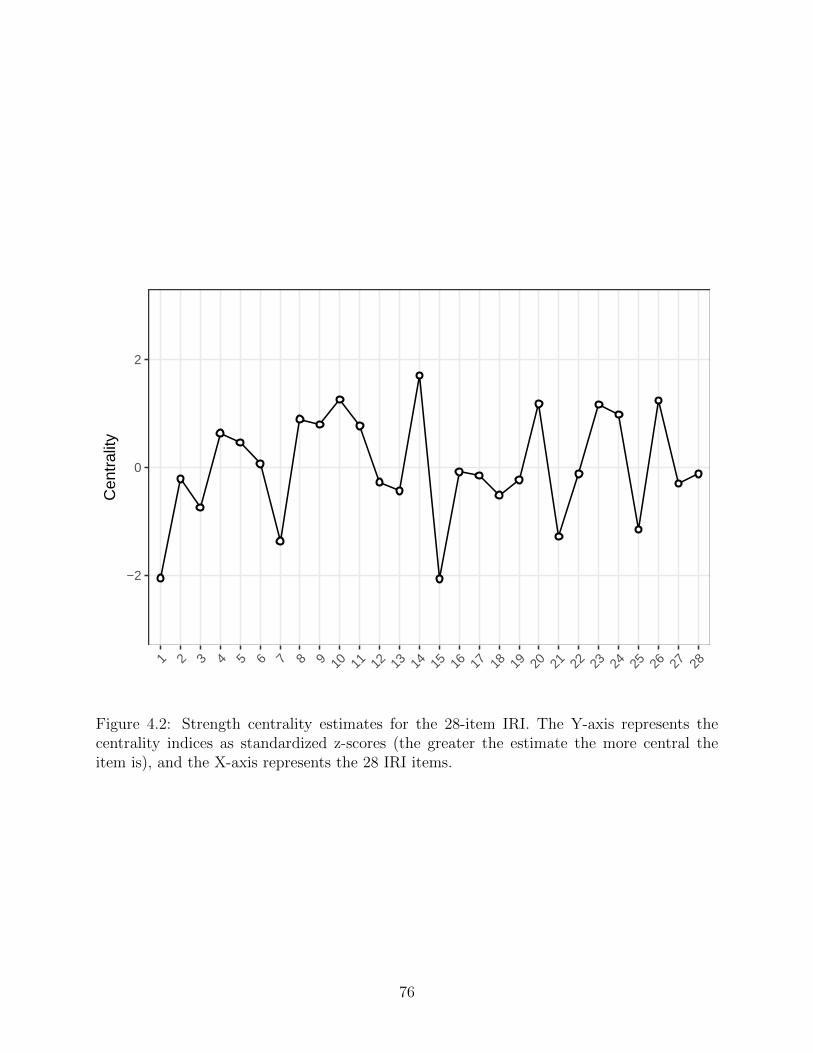
In Figure 4.2, I illustrate the strength centrality estimates for the 28 questionnaire items.
Item 14 (“Other people’s misfortunes do not usually disturb me a great deal”) has the
highest standardized strength centrality in the network. Other central items include node
Figure 4.2: Strength centrality estimates for the 28-item IRI. The Y-axis represents thecentrality indices as standardized z-scores (the greater the estimate the more central theitem is), and the X-axis represents the 28 IRI items.
76
10 (“I sometimes feel helpless when I am in the middle of a very emotional situation “), and
node 26 (“When I am reading an interesting story or novel, I imagine how I would feel if the
events in the story were happening to me”). Items 1 (“I daydream and fantasize, with some
regularity, about things that might happen to me”) and 15 (“If I’m sure I’m right about
something, I don’t waste much time listening to other people’s arguments”) show the lowest
strength centrality values.
4.3.3 Network accuracy and stability
The edge weight bootstrap revealed relatively small CIs, which indicates a more precise
estimation. The edge weight difference test reveals that the empathy network is accurately
estimated and that the strongest edges are significantly stronger than other edges. The
subset bootstrap shows that the order of item strength centrality is more stable than the
other kinds of centrality values, which is consistent with numerous prior papers (Armour
et al., 2017; Epskamp and Fried, 2018). CS-values obtained are 0.44 for node betweenness,
0.67 for node closeness and 0.75 for node strength. CS-values should preferably be above 0.5
and should not in any case be lower than 0.25: my results are above 0.5 and are therefore very
stable. The centrality difference test shows that highest centrality estimates are statistically
different from lowest centrality estimates, even though a statistical difference is not shown
among nodes with the highest strength centrality estimates.
4.4 Discussion
The network analysis I presented is, to my knowledge, the first one applied to empathy
research. This study highlights connections between empathy components and provides new
insights on how they might interact: some items are more interconnected than others, items
differ in centrality, and interactions exist between items from different empathy components.
Positive connections are found throughout the network, confirming that, in my sample,
77
most items from the IRI share some variance and are connected. However, some items present
weak with others; this means that some nodes are conditionally independent of all other items
in the network. The spinglass algorithm identifies on average four communities of items in the
network, corresponding to the four a priori components of Davis’ construct: Fantasy (cluster
A), perspective taking (cluster B), empathic concern (cluster C) and personal distress (cluster
D). The identification of these four node communities supports, using a different method, the
results of Braun et al.’s confirmatory factor analysis study (Braun et al., 2015). This is not
necessarily surprising, given that network and factor models are, under certain conditions,
mathematically interchangeable (Kruis and Maris, 2016).
Even though communities might be mathematically close to factors, from a network
perspective they mean something entirely different: they are clusters of interrelated items
that stem from mutual dynamics; they actively contribute to the construct of empathy itself.
However, the walktrap algorithm identified five communities, describing a fifth community
formed by items 6, 10 and 17. This is a consequence of the strong connection and clustering
of these three items, which nonetheless share two important connections with the rest of the
Personal Distress cluster (6-24 and 10-24). Some items belonging to a given community are
connected to those from different communities, suggesting — from a network perspective —
that empathy communities interact with each other in the network through specific items.
For example, there is a connection between items 8 and 9, respectively belonging to the
Perspective taking and Empathic concern subscales.
Items belonging to the Empathic concern community (9, 14 and 20) have high centrality
values; this finding supports Cliffordson’s theory that puts Empathic concern at the basis (in
this case, at the center) of empathy. Items from the Empathic concern cluster are connected
to all the other communities in the network. Item 14 shows the highest centrality value: to
interpret this finding, one must associate the statistical meanings of centrality and network
connections (edges). First, strength centrality (the main subtype used) means that the sum
of all edges of item 14 to all other nodes is the highest in the IRI network; second, a connection
78
between item 14 and another item means for instance that a high-score answer to item 14
(which is reversed) lets us guess a high-score answer to all the items item 14 is connected
to, controlling all other nodes. I can then interpret the high centrality of item 14 as the one
that might influence and/or might be influenced by most answers of the IRI. However, when
I look at the centrality difference test, I understand that the strength centrality of node 14
is not statistically different than strength centralities of nodes 10, 26, 20, 23 and 24, but is
statistically different from that of all other nodes: this means that these nodes are roughly
equivalent in their centrality. Node predictability, especially when focusing on the average,
is somewhat more straightforward to interpret: on average, if I influence a group of nodes
surrounding a given node, and assume that all edges go towards this node, I can influence
27% of its variance (Haslbeck and Waldorp, 2016).
Stability analysis shows that both centrality and edge weight estimates were reasonably
stable. My results must be interpreted in the light of a number of limitations. First, my
empathy network is estimated from a sample of young adults, which likely limits the general-
izability of my results; further studies should investigate networks structures across different
samples. Second, because I used cross-sectional data to carry out the analyses, I cannot
determine the direction of edges. For instance, I cannot interpret whether the most central
item activates other items, is activated by other items, or both. Third, similar to many other
statistical models such as factor models, the network model used here estimates between-
subjects effects on a group level. This means that network properties such as structure or
centrality may not replicate in the same way in single individuals. Fourth, Marshall et al.
provided evidence that the order in which items are presented in a questionnaire may influ-
ence their relationships (Marshall et al., 2013). Again, this is a limitation for any statistical
model based on the correlation matrix among items, such as factor models, and not a spe-
cific shortcoming over network models, but important enough to warrant mentioning. Fifth,
network analysis, in which I interpret edges as putative causal connections, is based on the
premise that nodes differ from each other meaningfully: if two nodes represent the same
79
aspect of a construct, an edge is not a putative causal connection, but simply represents
shared variance (Fried and Cramer, 2017). IRI might in some cases have this problem, for
instance item 7 (“I am usually objective when I watch a movie or play, and I don’t often get
completely caught up in it”) and item 12 (“Becoming extremely involved in a good book or
movie is somewhat rare for me”) seem to measure the same concept.
Future research may also endeavor to apply empathy networks in people with psy-
chopathology.
80
Chapter 5
A network model of self-worth
Abstract
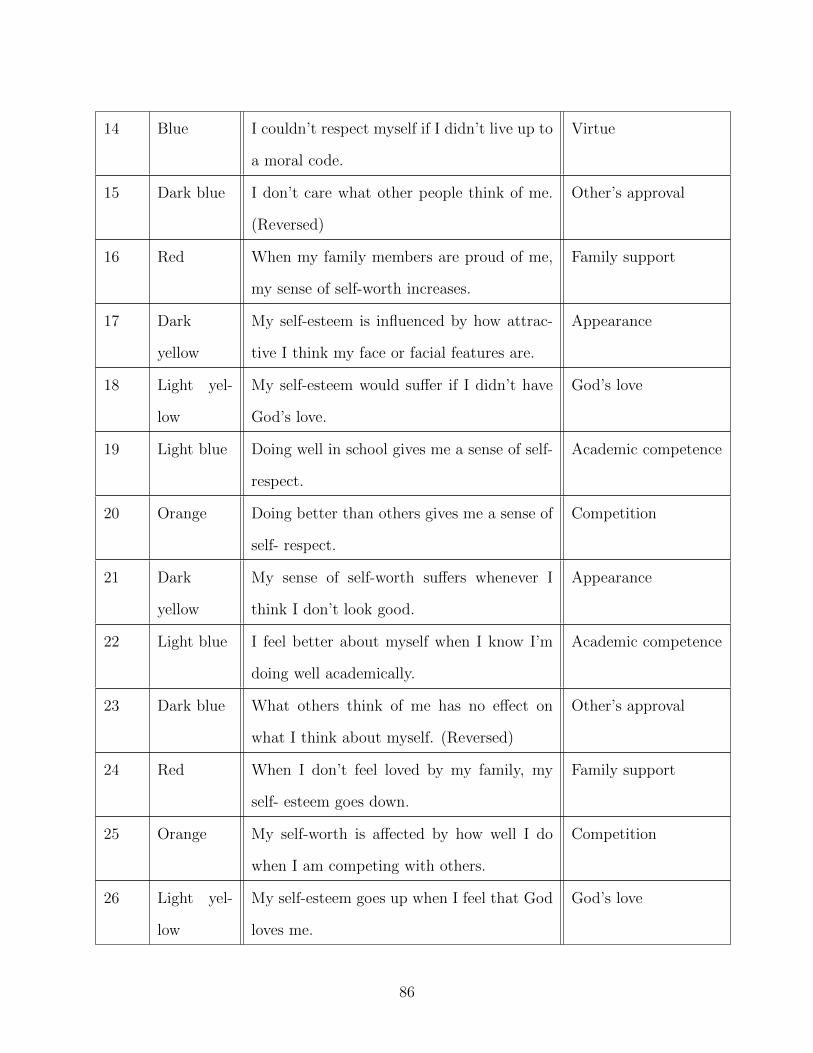
This study investigates the Contingencies of Self-Worth Scale (CSWS) in a sample
of 680 university students from a network perspective. I estimated regularized partial
correlations among seven CSWS domains: family support, competition, appearance,
Figure 5.1: 7-domain CSWS network. Each node represents a domain: FS is “Familysupport”, C is “Competition”, A is “Appearance”, GL is “God’s love”, AC is “Academiccompetence”, V is “Virtue” and OA is “Other’s approval” cluster. Blue edges representpositive connections and red edges represent negative connections; the thicker the connec-tion the stronger it is. The pie chart surrounding the node represents node predictability(percentage of shared variance with all connected nodes).
91
−2
0
2
A AC C FS GL OA V
CSWS_Domain
Exp
ecte
d In
fluen
ce
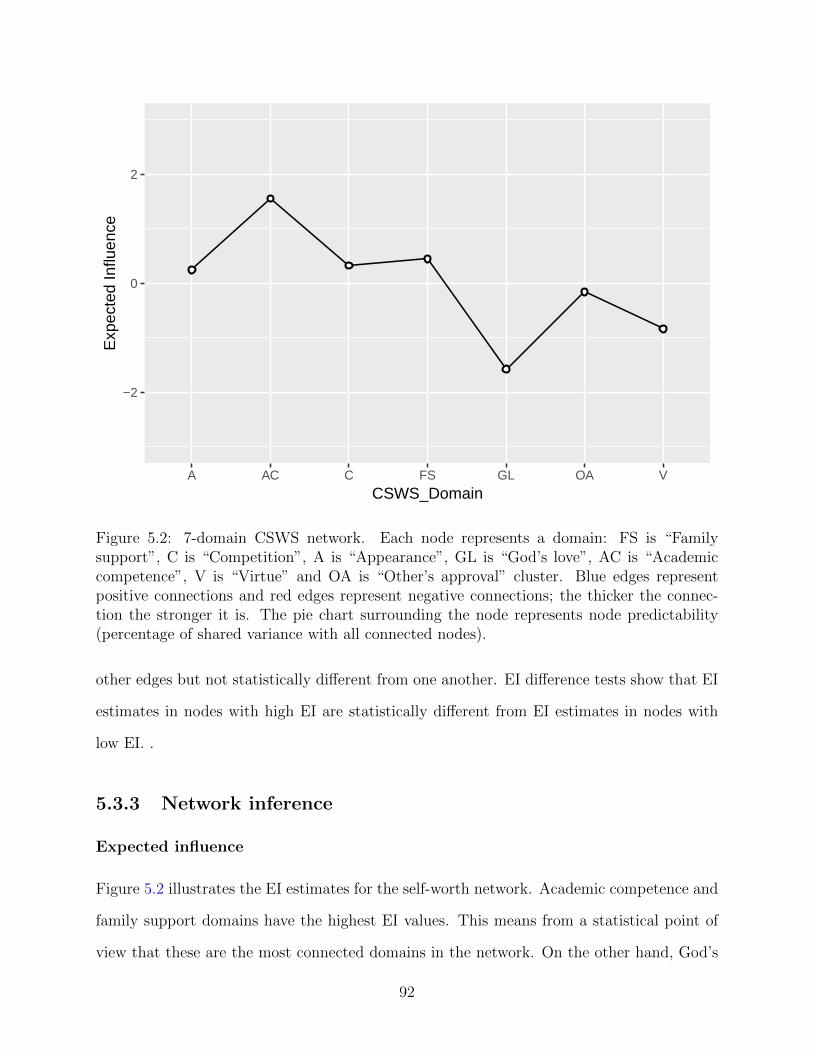
Figure 5.2: 7-domain CSWS network. Each node represents a domain: FS is “Familysupport”, C is “Competition”, A is “Appearance”, GL is “God’s love”, AC is “Academiccompetence”, V is “Virtue” and OA is “Other’s approval” cluster. Blue edges representpositive connections and red edges represent negative connections; the thicker the connec-tion the stronger it is. The pie chart surrounding the node represents node predictability(percentage of shared variance with all connected nodes).
other edges but not statistically different from one another. EI difference tests show that EI
estimates in nodes with high EI are statistically different from EI estimates in nodes with
low EI. .
5.3.3 Network inference
Expected influence
Figure 5.2 illustrates the EI estimates for the self-worth network. Academic competence and
family support domains have the highest EI values. This means from a statistical point of
view that these are the most connected domains in the network. On the other hand, God’s
92
love has the lowest EI value. This means that it is the domain that least influences the rest
of domains in the network. Correlation between EI and predictability is 0.96.
Node predictability
Mean node predictability ranges from 0.06 to 0.40, with an average of 0.25. This means that
on average, 25% of the variance of the node in the network can be explained by its neighbors.
God’s love is the domain with the lowest node predictability: it shares 6% of variance with
its surrounding nodes. Academic competence has the highest node predictability: it shares
40% of its variance with its surrounding nodes. Competition has the second highest node
predictability (0.35).
5.4 Discussion
To my knowledge, I have conducted the first network analysis of the psychological construct
self-worth contingencies. Overall, the seven domains of self-worth form a heterogeneous
system in which domains are not uniformly positively connected with each other. This is
interesting, because a homogeneous network with uniformly positive connections would be
expected if all domains are passive and interchangeable measures of one latent variable:
self-worth. Below, I discuss the findings in more detail.
Academic competence and competition share the strongest connection in the network:
it is reasonable to consider that the impact on self-esteem of competing with others and
obtaining good grades are connected while following a university curriculum. The same
kind of connection is found between appearance and other’s approval; this means that, while
considering self-worth, if physical appearance is important to an individual, so is the approval
of others, and vice versa. Competition also shares a strong connection with appearance,
which means that physical appearance might be important for individuals competing with
others (and vice-versa). Family support and other’s approval share connections with most
93
domains in the network. Appearance showed a negative connection to virtue: that means
that people that base their self-worth upon acting and living by a moral code might not draw
self-worth from physical appearance (and vice-versa), controlling for all other associations in
the network. While there is no prior work on partial correlations, previous work on zero-order
correlations found a positive association between the two domains (Crocker et al., 2003).
Negative edges have not been observed commonly in the psychopathology network lit-
erature, which calls for an explanation. In this case, the negative association between ap-
pearance and virtue might be plausible from a theoretical perspective. Since both subscales
are positively associated with academic competence and family support, the finding implies
that in individuals whose self-worth is simultaneously contingent on academic competence
and family support, knowing that self-esteem is more contingent on virtue allows predicting
that their self-esteem is less likely to be also contingent on physical appearance (and vice
versa). Two other possibilities also come to mind. First, negative connections in Gaussian
Graphical Models can arise when dealing with small samples and/or when estimating poly-
choric correlations (Epskamp and Fried, 2018), which I can rule out as explanation here.
Second, collider structures in conditional dependence networks can induce spurious negative
relations between two nodes in case they both cause a third node (Greenland et al., 1999).
God’s love is a relatively disconnected node: it shares only one positive connections
with virtue: this is not surprising, since in the original work (Crocker et al., 2003) God’s
love showed its strongest correlation with virtue. From a network perspective, this means
that God’s love is largely conditionally independent from other domains in the network.
From a network perspective, one plausible interpretation of the conditional independence
of God’s Love in the self-esteem network is that people may derive a sense of self-worth
from their religious belief (in this case, feeling that they have the love of God) regardless
of the other contingencies; this may highlight religious belief as an independent source of
self-esteem in people. Another possible interpretation of this finding is statistical, i.e. a floor
effect or a ceiling effect: because of a low or high parameter, the domain might share few
94
connections with other domains. This may be applicable to my findings, since God’s love
has the highest standard deviation among all domains in the network, as well as the lowest
mean. I identified strong differences in predictability, ranging from 6% (God’s love) to 40%
(academic competence). Average node predictability is 0.25, which means that on average,
25% of the variance of the nodes is explained by other nodes in the network. From a network
perspective, I can infer that some domains such as academic competence are well explained
by its surrounding domains. Academic competence and God’s love are respectively the most
and least predictable nodes in the network.
The analysis of EI shows that academic competence, and family support have the highest
values in the network: this means that these two domains share the strongest connections
in the network and therefore may influence or be influenced by other domains of contingent
self-worth the most. Node predictability is therefore simpler to interpret than EI and gives
us a clear information about how a node is influenced by surrounding nodes, assuming all
edges are directed towards this node.
This study should be interpreted in the light of some limitations. First, my network is
estimated from a sample of university students. While the CSWS was originally developed
based on a similar sample (Crocker et al., 2003), it is worth noting that results of my study
may not generalize to other samples. Second, the current cross-sectional data set does not
allow for causal or even Granger-causal inference. For instance, I cannot interpret whether
a given domain causes or is caused by domains sharing a connection with it. This requires
temporal follow-up studies, which would be most interesting across important developmental
periods such as adolescents and early adulthood. Third, the network model I estimated is
a between-subjects models. This also means that inferences from the study should only be
drawn for a group of people, and it is unclear if and how well the present between-subjects
network structure describes individuals’ networks of self-worth contingency.
Future research may endeavor to apply self-worth contingency networks in other kinds
of samples, both healthy and with different kinds of psychopathology, as to analyze possible
95
differences in network structure, node predictability and centrality.
96
Chapter 6
A network model of resilience
Abstract
The Resilience Scale for Adults (RSA) is a questionnaire that measures protective
factors of mental health. The aim of this paper is to perform a network analysis of the
Resilience Scale for Adults (RSA) in a dataset composed of 675 French-speaking Belgian
university students, to identify potential targets for intervention to improve protective
factors in individuals. I estimated a network structure for the 33-item questionnaire
and for the six domains of resilience: perception of self, planned future, social com-
petence, structured style, family cohesion and social competence. Node predictability
(shared variance with surrounding nodes in the network) was used to assess the con-
nectivity of items. An Exploratory Graph Analysis (EGA) was performed to detect
communities in the network: the number of communities detected being different than
the original number of factors proposed in the scale, I estimated a new network with
the resulting structure and verified the validity of the new construct which was pro-
posed. The network composed of items from the RSA is overall positively connected
with strongest connections arising among items from the same domain. The domain
network reports several connections, both positive and negative. The EGA reported
the existence of four communities that I propose as an additional network structure.
Node predictability estimates show that connectedness varies among the items and
domains of the RSA. Network analysis is a useful tool to explore resilience and identify
97
targets for clinical intervention. In this study, the four domains acting as components
of the additional four-domain network structure may be potential targets to improve
an individual’s resilience. Further studies may endeavor to replicate my findings in
different samples.
6.1 Introduction
Resilience is understood as a positive adaptation despite significant adversities or trauma
(Luthar, 2006). Resilience is a psychological construct which has been proven to be related
to psychiatric disorders, such as anxiety, depression, substance abuse obsessive-compulsive
disorder (Hjemdal et al., 2011a; Bonfiglio et al., 2016).
In recent years, the construct of resilience has been conceived as an outcome rather than a
trait, which highlights the ability to improve an individual’s protective factors against mental
illness (Chmitorz et al., 2018). In this framework, protective factors composing resilience
compete with risk factors, for instance, adverse events (such as traumatic experiences, loss
or neglect) which have been shown to be present in up to 50% of individuals under the age
of 18 (Fritz et al., 2018). Other important factors influencing the framework of resilience
involve age, social status and education (Aburn et al., 2016).
The Resilience Scale for Adults (RSA) is a psychometric questionnaire that assesses
protective factors of mental health (Friborg et al., 2003). The RSA has been defined as one of
the best resilience questionnaires with regard to psychometric ratings (Windle et al., 2011).
Largely validated in Norwegian samples, the construct has undergone in the last decade
cross-cultural validation in different countries, such as Belgium (Hjemdal et al., 2011b), Iran
(Jowkar et al., 2010), Italy (Bonfiglio et al., 2016) and Peru (Morote et al., 2017). The
RSA measures six domains of resilience: (1) perception of self represents the confidence in
oneself, one’s own capabilities, judgment and decision-making (e.g. item 17 “My judgment
and decisions I trust completely”); (2) planned future identifies goal-oriented individuals (e.g.
item 32 “My goals for the future are well thought through”); (3) social competence represents
98
the ability to adapt in social environments (e.g. item 21 “Meeting new people is something I
am good at”); (4) structured style identifies with organized individuals who follow routines
(e.g item 23 “When I start on new things/projects, I prefer to have a plan”); (5) family
cohesion measures the loyalty, support, optimism, mutual understanding and appreciation
among family members (e.g. item 3 “My family understanding of what is important in life
is very similar”); (6) social resources identifies the availability of social support from friends
and family (e.g. item 6 “I can discuss personal issues with friends/family members”). These
six domains are commonly understood as being effects of the construct of resilience itself,
since they are measurable indicators of the construct.
However, in recent years, network theory has emerged as a way of studying psychological
constructs as interacting entities (Borsboom, 2017). Such entities are uncovered in real-world
data using network models, usually composed of pairwise interactions of its elements, and
the constructs emerge from these connections (Borsboom and Cramer, 2013). Interactions
between elements composing a network are often statistically represented as regularized
partial correlations (Epskamp and Fried, 2018). Several mental disorders have been analyzed
using a network perspective, such as posttraumatic stress disorder (Fried et al., 2018; Phillips
et al., 2018), depression (Mullarkey et al., 2018), schizophrenia (Galderisi et al., 2018) and
obsessive-compulsive disorder (Ruzzano et al., 2015). Network analysis has also been applied
to several psychological constructs, such as personality (Costantini et al., 2015), empathy
(Briganti et al., 2018), attitudes (Dalege et al., 2017), intelligence (van der Maas et al., 2006)
and self-worth (Briganti et al., 2019). Other studies used innovative methods, including
networks to harmonize rating scales (Gross et al., 2018; Purgato et al., 2018; Haroz et al.,
2016).
Learning the network structure of a given construct (such as resilience) or mental disor-
der (such as PTSD) is particularly relevant in clinical practice since it highlights potential
clinical target that may affect multiple symptoms or elements composing the network (Fried
et al., 2018); for instance, intervening on the connection between two components of the
99
network is likely to modify the clinical presentations of said components (such as symp-
toms). In the specific case of resilience, which is considered a protection against mental
disorders, learning the network structure of resilience components may highlight potential
targets to strengthen the overall mental health of a given individual. In recent years, several
intervention methods to foster resilience have been studied worldwide, but their efficiency is
variable because of limited comprehension of this relevant psychological construct (Chmitorz
et al., 2018). A network analysis of resilience factors has also been proposed in two sample
of adolescent subjects with and without childhood adversities (Fritz et al., 2018) and showed
that childhood adversities impact the degree of connectivity of resilience factors.
Network components are usually answers of an observed group to items of a questionnaire,
such as the RSA. A current challenge in network models when dealing with self-report
scales is the redundancy of several items of a given questionnaire in measuring the same
aspect of a construct (Fonseca-Pedrero et al., 2018); while addressing the meaning of a
given connection between two items, their interaction will represent shared variance (and
not a pairwise relationship) if they tend to measure the same thing (Fried and Cramer,
2017). In the case of the RSA, this challenge goes beyond the notion of a single items of the
questionnaire and may apply to entire domains of the RSA: for instance, questions from both
perception of self and planned future refer to one’s own dispositional attributes and internal
source of resilience and were original part of the same factor, which was called personal
competence (Friborg et al., 2003). The same line of reasoning applies to family cohesion
and social resources, even though originally distinct factors, since they represent an external
source of resilience – that is, the support that the individual feels both within and without
the family nucleus: furthermore, several items from social resources include the concept of
family support (e.g. item 6 “I can discuss personal issues with friends/family). Exploratory
graph analysis (EGA) has emerged as a highly effective and reliable tool in network analysis
when addressing the issue of recovering the number of factors (CFA) in datasets (Golino and
Epskamp, 2017). An optimum solution proposed in the literature is to first explore the basic
100
dimensionality of an instrument with an EGA then authenticate the suggested structure by
performing a confirmatory factor analysis (Golino and Demetriou, 2017).
I aim to extend the conceptual framework of network analysis to the construct of re-
silience such as represented by the RSA and address the challenge of domain redundancy
using both network models and structural equation models. First, I want to explore the con-
nectivity of the RSA as a network composed of its items, then study the connections arising
among resilience domains, such as performed in recent network papers (Briganti et al., 2019).
Second, I want to apply community detection algorithms and the EGA to the item network,
explore then verify the suggested structure with CFA and network analysis. Third, I want
to measure node predictability which an absolute measure of interconnectedness (Haslbeck
and Fried, 2017) of a node in a network.
Statistically speaking, node predictability represents the shared variance of a network
component with surrounding components. Although performed on university students, ex-
ploring a network structure that shows how domains of resilience interact may have mean-
ingful clinical implications as it highlights potential target to improve the overall protective
factors of a given individual; also, it may serve as basis for future replication studies designed
to identify the network structure of RSA in other samples.
6.2 Method
6.2.1 Participants
The analyses in this paper are performed on a dataset composed of 675 university students
from the French-speaking region of Belgium. 59% of the students were women and 41% were
men; subjects were 17 to 25 years old (M=19 years, SD=1.5 years).
101
6.2.2 Measurement
The RSA is composed of 33 items that measure resilience in 6 domains: perception of self,
planned future, social competence, structured style, family cohesion and social competence.
The items are shuffled in the questionnaire. Item scoring is semantic and differential-based
(Friborg et al., 2006a): for instance, when scoring item 13 “My family is characterized by”,
a minimum score of 1 is represented by the answer “Disconnection” and a score of 7 is
represented by the answer “Healthy cohesion”. Reversed-score items are included in the
scale.
This study was approved by the Ethical Committee of the Erasme university hospital.
6.2.3 Network analysis
I used the software R (open source, available at https://www.r-project.org/). Pack-
ages and functions to carry out the analysis include qgraph (Epskamp et al., 2012), glasso
(Friedman et al., 2014b) for network estimation and visualization, mgm (Haslbeck and Wal-
dorp, 2016) for node predictability, EGA (Golino and Epskamp, 2017) and igraph (Csardi
and Nepusz, 2006) for community detection, and bootnet (Epskamp and Fried, 2018) for
stability.
Item network
I calculated correlations for the 33 RSA items and used the resulting correlation matrix as
an input to estimate a Gaussian Graphical Model (GGM), a regularized partial correlation
network (Epskamp and Fried, 2018). Graphical lasso (least absolute shrinkage and selection
operator) was used to regularize the parameters resulting from the GGM, therefore avoiding
the estimation of spurious connections (non-existing connections that may be present due
to noisy information). In the item network, nodes represent resilience items from the RSA
questionnaire. Each node is surrounded by a pie chart representing node predictability.
Connections between nodes are called edges. An edge in a network is interpreted as the
existence of an association between two nodes, controlling for all other nodes in the network.
An edge between two items of the RSA may be statistically interpreted as following: if
two given nodes X and Y share an edge XY in the network, and the observed group of
subjects scores high on X, then the observed group is also more likely to score high on Y
(Briganti et al., 2018). Each edge in the network represents either positive regularized partial
correlations (visualized as blue edges) or negative regularized partial correlations (visualized
as red edges). The thickness and color saturation of an edge denotes its weight (the strength
of the association between two nodes). The Fruchterman-Reingold algorithm places the
items in the network based on the sum of connections of a given node with other nodes
(Fruchterman and Reingold, 1991).
Six-domain network
To assess the overall connectedness of the domains of resilience as described in the RSA
(Hjemdal et al., 2011a) I used the methodology described in recent papers (Briganti et al.,
2019) and estimated a factor model using CFA for each of the six RSA domains. I then used
the factor scores obtained to estimate an additional GGM.
Network stability
Network stability is composed of several state-of-the-art analyses which are necessary to
safely interpret results from a network analysis. I estimated 95% confidence intervals (CI)
of the edge weight through bootstrapping (Epskamp and Fried, 2018), 2000 bootstraps were
used and performed an edge weight difference test to answer the question “is edge A signifi-
cantly stronger than edge B?”.
Network inference
I estimated node predictability for the 33 RSA items and for the six domains. Node pre-
dictability (Haslbeck and Fried, 2017) represents shared variance of a given node with sur-
103
rounding nodes in a network. Node predictability is an absolute measure of the interconnect-
edness of network nodes (Fried et al., 2018). Other measures of inference frequently used in
network literature such as strength centrality (Boccaletti et al., 2006) or expected influence
(Robinaugh et al., 2016) can only address the relative importance of nodes (Briganti et al.,
2019) and are therefore less informative when it comes to address the issue of interconnect-
edness; that is why I decided not to use these measures in this paper. One interpretation
of node predictability that has been previously described in the literature (Briganti et al.,
2019) is that of the upper bound of controllability: this measure can provide an estimate
of how much a node X can be influenced by all other nodes if I assume that all edges that
node X shares with other nodes are directed towards X. To explore the dimensionality of
the RSA in my sample I performed an EGA on the item network. EGA uses the walktrap
algorithm to detect communities. This algorithm is based on the principle that adjacent
nodes tend to belong to the same community (Yang et al., 2016), was shown to have high
accuracy in simulation studies (Golino and Epskamp, 2017) and used in empirical network
papers (Briganti et al., 2018).
Four-domain network
Because I detected a different structure – composed of four domains instead of six as the
one originally proposed (Hjemdal et al., 2011a), I used CFA to estimate a four-factor model
and used the resulting factor scores to estimate a four-domain network; because the network
estimation procedure selected the network (out of a 100 networks) with the lowest tuning
parameter (called lambda value), I lowered the lambda value to follow standard recommen-
dations. I also calculated node predictability for the four nodes of the resulting network.
104
F1 F2
F3
F4
F5
F6
F7
F8
F9
F10
F11
F12
F13
F14 F15
F16
F17
F18
F19
F20
F21
F22
F23
F24
F25F26
F27
F28
F29
F30F31
F32 F33
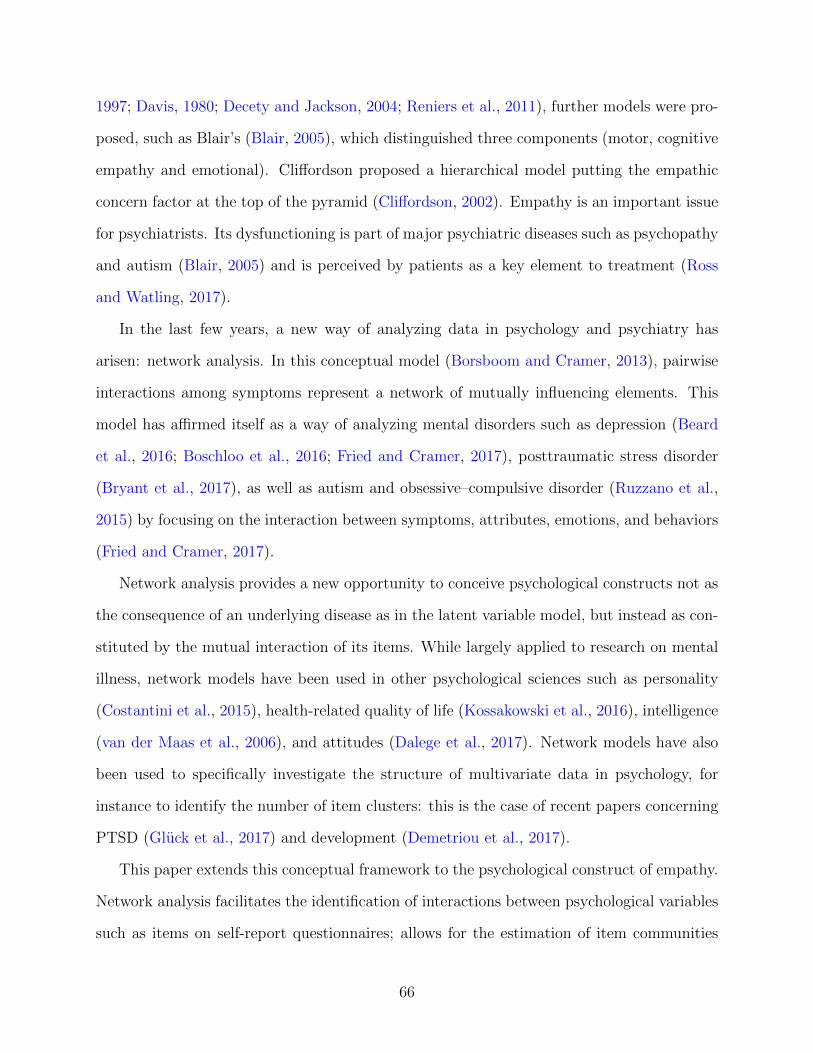
Figure 6.1: 33-item RSA network. Each node represents an item from the questionnaire.Blue edges represent positive connections and red edges represent negative connections; thethicker the connection the stronger it is. The pie chart surrounding the node represents nodepredictability (percentage of shared variance with all connected nodes).
105
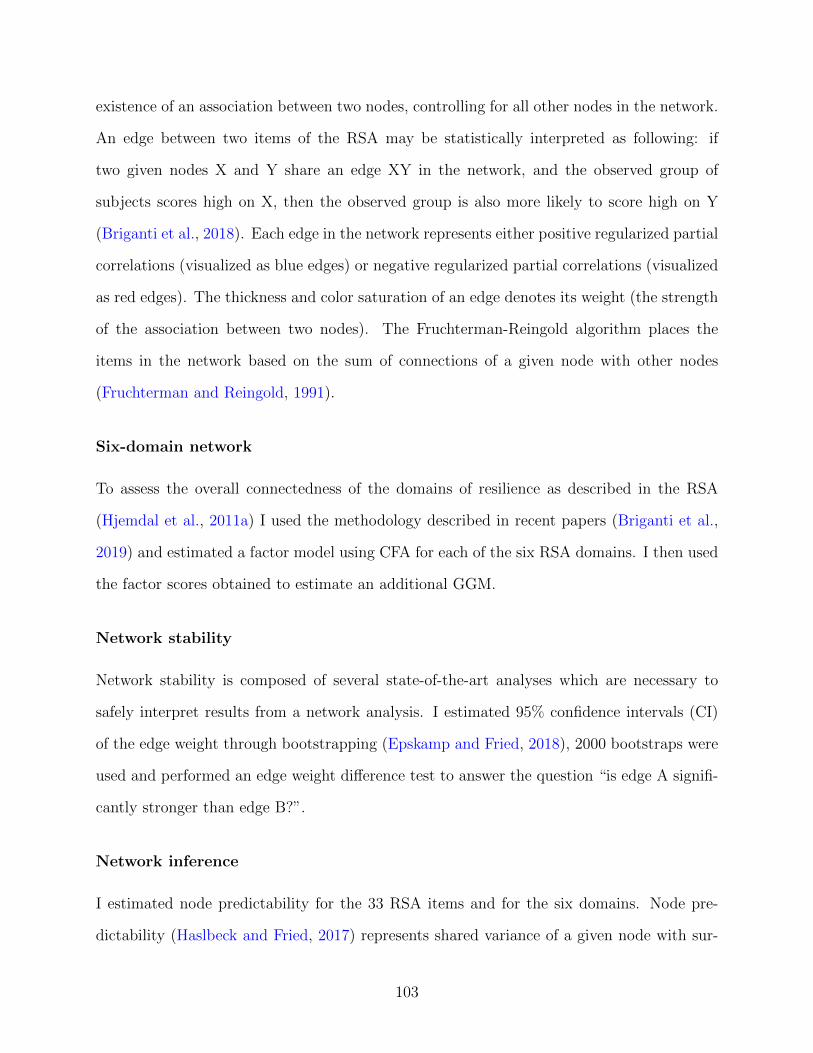
6.3 Results
6.3.1 Item network
Figure 6.1 represents the item network: to render the visualization more readable, I hid
all edges smaller than 0.05 (one tenth of the value of the maximum edge weight). Overall,
the 33 items from the RSA form a network of positively connected nodes. The strongest
connection (0.5) is the edge between node 18 (“New friendships are something I make easily”)
and node 21 (“Meeting new people is something I am good at”), both belonging to social
competence. Two other examples of strong connections are edge 9-15 belonging to social
resources (“Those who are good at encouraging me are some close friends/family; “I get
support from friends/family members”) and edge 4-32 belonging to planned future (“I feel
that my future looks very promising”; “My goals for the future are very thought through”).
These examples of highly connected nodes reflect the challenge of items representing the same
aspect of a construct and are discussed in section 4. However, several edges connect different
domains of resilience. For instance, edge 11-19 connects perception of self and social resources
(“My personal problems I know how to solve”; “When needed, I have always someone who
can help me”), and edge 17-26 connects perception of self and social competence (“My
judgment and decisions I trust completely”; “For me, thinking of good topics of conversation
is easy”).
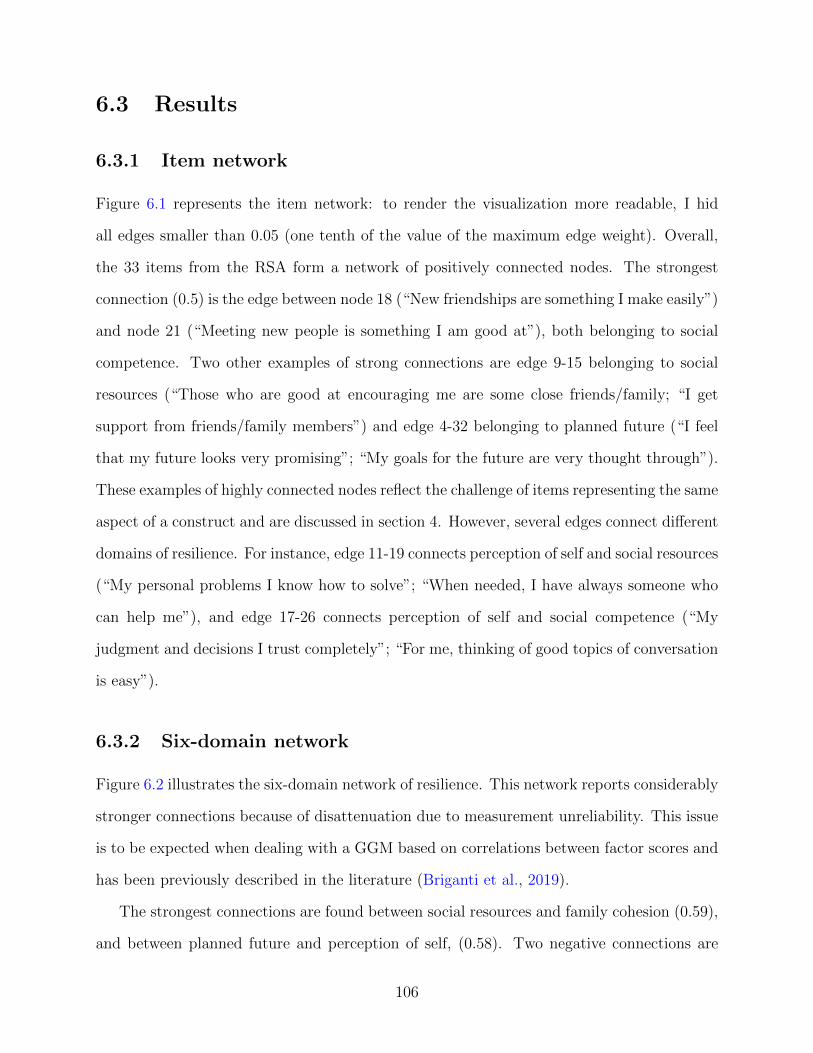
6.3.2 Six-domain network
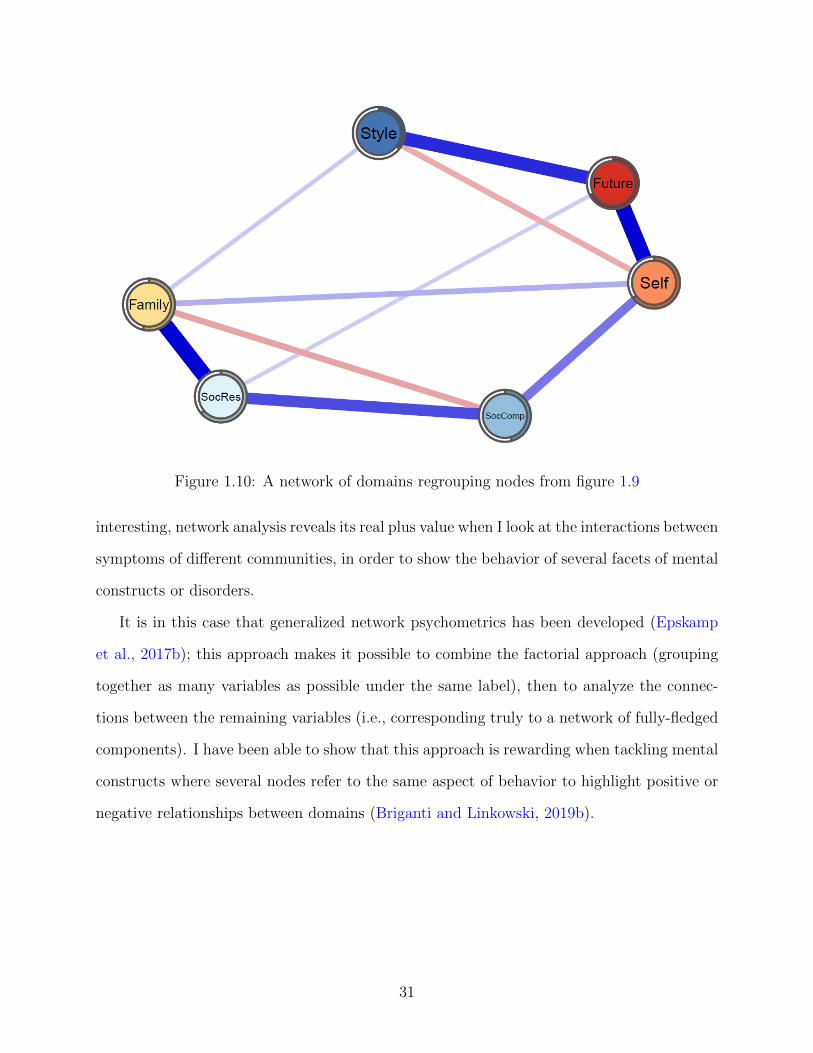
Figure 6.2 illustrates the six-domain network of resilience. This network reports considerably
stronger connections because of disattenuation due to measurement unreliability. This issue
is to be expected when dealing with a GGM based on correlations between factor scores and
has been previously described in the literature (Briganti et al., 2019).
The strongest connections are found between social resources and family cohesion (0.59),
and between planned future and perception of self, (0.58). Two negative connections are
106
Future
SelfFamily
SocRes
SocComp
Style
Future: Planned FutureSelf: Perception of SelfFamily: Family CoherenceSocRes: Social ResourcesSocComp: Social CompetenceStyle: Structured Style
Figure 6.2: Six-domain RSA network. Each node represents a domain from the RSA.
found between structured style and perception of self (0.19) and between family cohesion
and social competence (0.21). Several domains present no direct connection with each other,
such as structured style and social competence or social resources and perception of self;
from a network perspective, that means that the two domains are conditionally independent
from each other.
I performed a CFA to assess the validity of the six-domain structure. Root Mean Square
Error of Approximation (RMSEA) is 0.047 (cut-off for good fit < 0.06) and the Standardized
Root Mean Square Residual (SRMSR) is 0.058 (cut-off for good fit <0.08); Cronbach’s alpha
is 0.64 (>0.8 for good fit); Comparative Fit Index (CFI) is 0.87 (>0.9 for good fit) and the
p-value for the chi-square fit test is 0 (> 0.05 for good fit; Schreiber, 2017).
6.3.3 Network stability
Bootstrapped 95% edge weight CI show that the edge weights are accurately estimated, and
the edge weight difference tests report that stronger edges can be safely interpreted as to
be stronger that other edges in both the item network and the six-domain network, but do
not statistically differ from each other in the six-domain network. For instance, one cannot
safely interpret the edge between social resources and family cohesion to be stronger than
107
the edge between perception of self and planned future.
6.3.4 Network inference
Node predictability
Node predictability was estimated in both the item network and the six-domain network.
In the item network, the two nodes with the highest node predictability are node 18 (“New
friendships are something I make easily”; 0.54) and 21 (“Meeting new people is something
I am good at”; 0.53), which both belong to social competence and also share the strongest
edge in the network. The node with the lowest node predictability is node 33 which belongs
to perception of self (“Events in my life that I cannot influence I manage to come to terms
with”; 0.13). Mean node predictability is 0.32, which means that on average, items from
the RSA share 32% of their variance with surrounding nodes. In the six-domain network,
planned future shows the highest node predictability (0.67) and structured style is the least
predictable node (0.36). The mean node predictability is 0.55, which means that on average,
domains present 55% of shared variance.
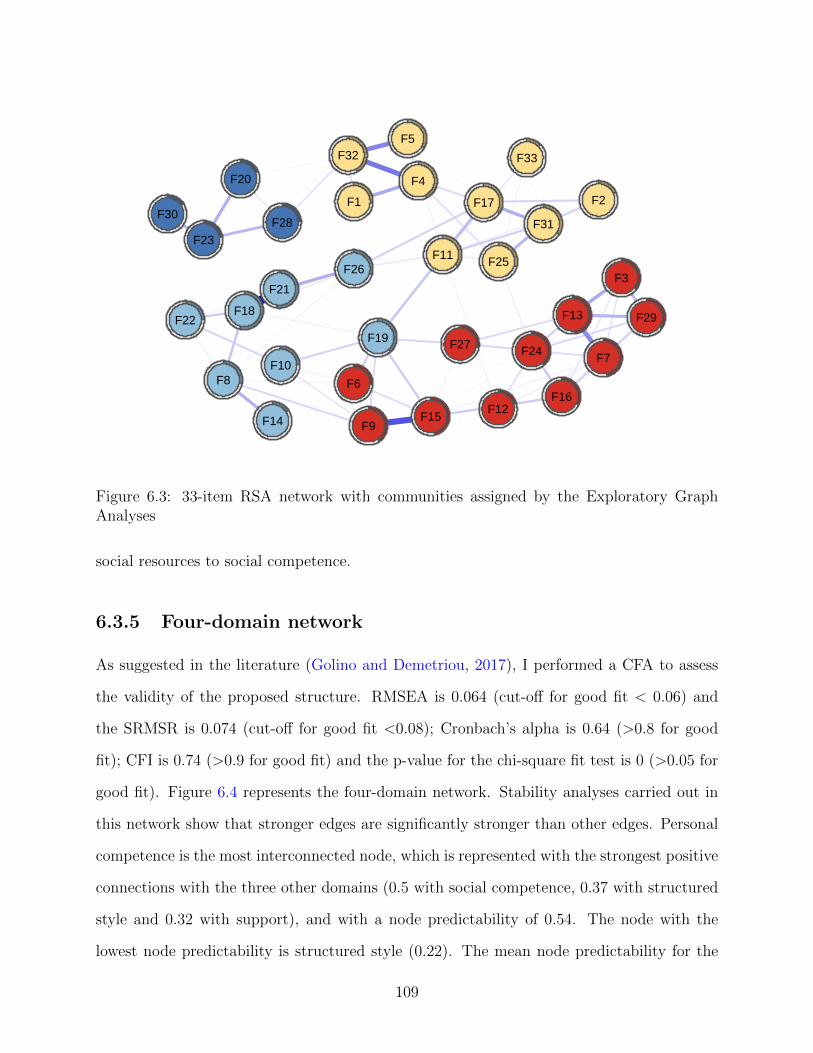
Community detection
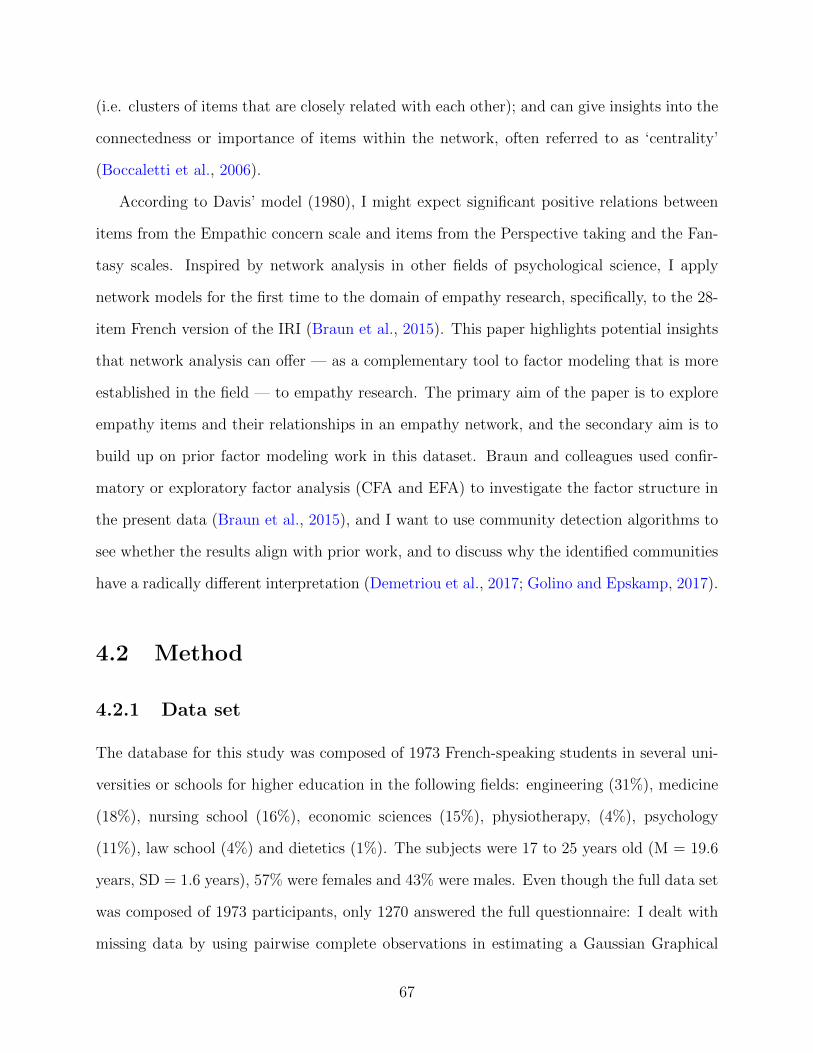
The EGA and walktrap algorithm applied to the item network report four communities of
items instead of six as proposed in the original scale. To visualize the differences between
communities, I first reestimate the network with a different color palette, each color indicating
a community of items as detected by the algorithm as shown in Figure 6.3.
Overall, items from perception of self and planned future form a new community, that
I identify as personal competence, referring to one of the first versions of the RSA (Friborg
et al., 2006b); the same process applies to items from social resources and family cohesion,
forming a new community that I identify as support since it is an aspect of resilience that
the two domains represent. Items 10 (“The bonds among my friends are strong”) and 19
(“When needed, I have always someone who can help me”) switch communities, going from
108
F1 F2
F3
F4
F5
F6
F7
F8
F9
F10
F11
F12
F13
F14 F15
F16
F17
F18
F19
F20
F21
F22
F23
F24
F25F26
F27
F28
F29
F30F31
F32 F33
Figure 6.3: 33-item RSA network with communities assigned by the Exploratory GraphAnalyses
social resources to social competence.
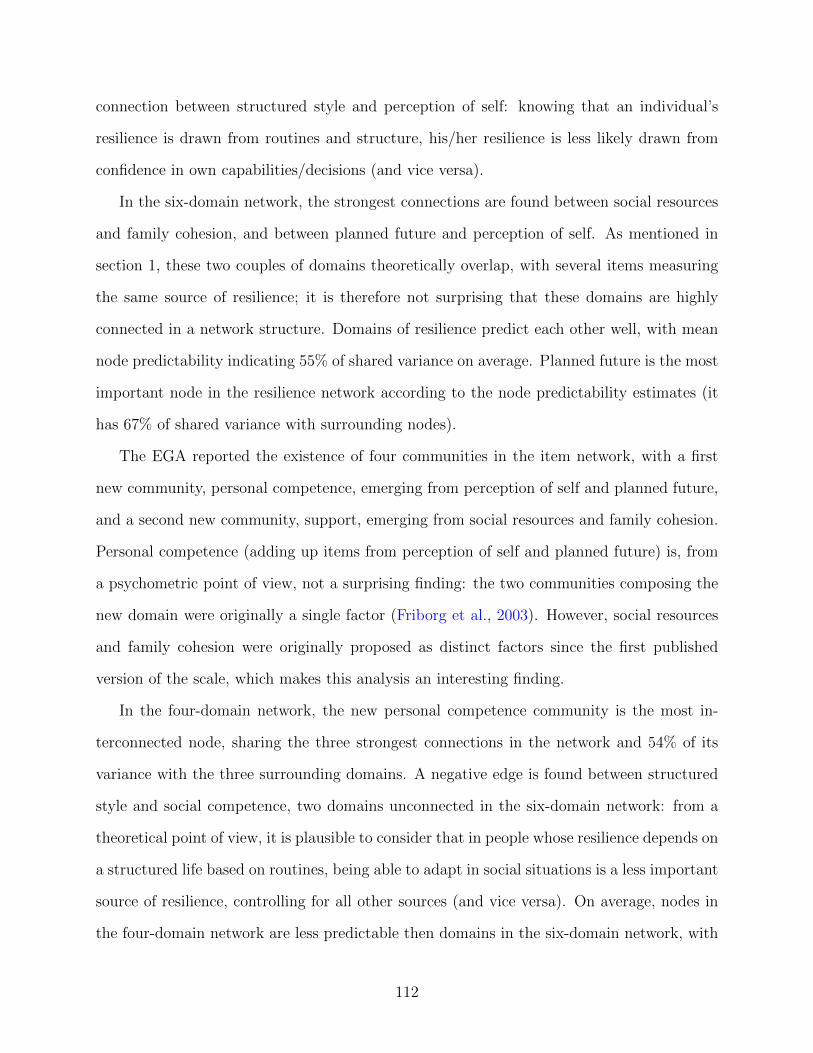
6.3.5 Four-domain network
As suggested in the literature (Golino and Demetriou, 2017), I performed a CFA to assess
the validity of the proposed structure. RMSEA is 0.064 (cut-off for good fit < 0.06) and
the SRMSR is 0.074 (cut-off for good fit <0.08); Cronbach’s alpha is 0.64 (>0.8 for good
fit); CFI is 0.74 (>0.9 for good fit) and the p-value for the chi-square fit test is 0 (>0.05 for
good fit). Figure 6.4 represents the four-domain network. Stability analyses carried out in
this network show that stronger edges are significantly stronger than other edges. Personal
competence is the most interconnected node, which is represented with the strongest positive
connections with the three other domains (0.5 with social competence, 0.37 with structured
style and 0.32 with support), and with a node predictability of 0.54. The node with the
lowest node predictability is structured style (0.22). The mean node predictability for the
109
PersComp
Support
SocComp
Style
PersComp: Personal CompetenceSupport: SupportSocComp: Social CompetenceStyle: Structured Style
Figure 6.4: Four-domain network of resilience. Each node represents a domain as detectedby the Exploratory Graph Analysis.
four-domain network is 0.37. A negative edge is found between structured style and social
competence.
6.4 Discussion
This paper is to my knowledge the first work to report a network analysis of the psychological
construct of resilience as conceived in RSA. The different analyses carried out bring new
and interesting information on the construct, reporting overall that resilience is formed of
interacting components which are not mere consequences of a latent variable. If the network
structures presented in this work were to replicate in different samples, interventions to
improve protective factors in individuals may become more efficient by acting on meaningful
targets, such as two highly connected nodes in the resilience network.
The item network shows that the strongest edges are shared between items representing
overall the same aspect of a domain: such connections must therefore be interpreted as shared
variance between items, such as reported in recent papers that further address the issue (Fried
and Cramer, 2017) and propose solutions such as estimating a network of domains instead of
a network of items (Briganti et al., 2019). However, in the case of the RSA, the item network
110
sheds light on the connectivity between items from different subscales: items from the RSA
in my sample therefore form a complex system of mutual interactions that actively contribute
to the construct of resilience itself. From a network perspective, this means the observed
group is likely to similarly answer items that present a connection in the resilience network,
after controlling for all other items in the network (Briganti et al., 2018). Items from the RSA
also have different levels of importance in the network; this information is provided by node
predictability, which is an absolute measure of the interconnectedness of a node (Haslbeck
and Fried, 2017). In the item network, two nodes from the social competence domain (18
and 21) show the highest predictability, sharing over 50% of variance with surrounding nodes
in the network structure: however, as addressed in the section 3, the two nodes with the
highest node predictability are also the nodes sharing the strongest edge in the network; the
high predictability is therefore largely influenced by the presence of one very strong edge,
which is also a known feature influencing centrality criteria.
The six-domain network further helps us explore the connectivity and importance of the
protective factors as described in the most recent version of the RSA. Domains of the RSA
form a heterogenous system with positive and negative connection: this further supports the
theory that domains of resilience are not interchangeable measures of resilience; the construct
arises from the connections among domains. For instance, two negative connection exists, the
first between structured style and perception of self, and the second between family cohesion
and social competence. Negative edges are a rare finding when dealing with a network
approach of psychological constructs; a recent paper (Briganti et al., 2019) addressed the
issue of interpreting negative edges in the case of a domain network such as the six-domain
network of RSA estimated in this paper. From a theoretical point of view, I may interpret
the negative edge between social competence and family cohesion as follows: knowing that
an individual’s resilience is strongly drawn from the ability to rapidly adapt in different social
context, that individual’s resilience is less likely to be drawn from the support originating
from a cohesive family (and vice versa). The same line of reasoning applies to the negative
111
connection between structured style and perception of self: knowing that an individual’s
resilience is drawn from routines and structure, his/her resilience is less likely drawn from
confidence in own capabilities/decisions (and vice versa).
In the six-domain network, the strongest connections are found between social resources
and family cohesion, and between planned future and perception of self. As mentioned in
section 1, these two couples of domains theoretically overlap, with several items measuring
the same source of resilience; it is therefore not surprising that these domains are highly
connected in a network structure. Domains of resilience predict each other well, with mean
node predictability indicating 55% of shared variance on average. Planned future is the most
important node in the resilience network according to the node predictability estimates (it
has 67% of shared variance with surrounding nodes).
The EGA reported the existence of four communities in the item network, with a first
new community, personal competence, emerging from perception of self and planned future,
and a second new community, support, emerging from social resources and family cohesion.
Personal competence (adding up items from perception of self and planned future) is, from
a psychometric point of view, not a surprising finding: the two communities composing the
new domain were originally a single factor (Friborg et al., 2003). However, social resources
and family cohesion were originally proposed as distinct factors since the first published
version of the scale, which makes this analysis an interesting finding.
In the four-domain network, the new personal competence community is the most in-
terconnected node, sharing the three strongest connections in the network and 54% of its
variance with the three surrounding domains. A negative edge is found between structured
style and social competence, two domains unconnected in the six-domain network: from a
theoretical point of view, it is plausible to consider that in people whose resilience depends on
a structured life based on routines, being able to adapt in social situations is a less important
source of resilience, controlling for all other sources (and vice versa). On average, nodes in
the four-domain network are less predictable then domains in the six-domain network, with
112
37% of shared variance.
However, when comparing results from the CFA of both the six-factor model and the
four-factor model such as suggested in the literature (Golino and Demetriou, 2017), the
six-factor model presents with better indicators than the four-factor model. This being the
first network approach to this particular scale of resilience, future papers may endeavor to
replicate these findings in other samples while comparing the original six-factor structure
with structures proposed from EGA.
My analyses should be interpreted in the light of several limitations. First, my dataset
is composed of university students, which may likely limit the generalization of my findings
to different samples. Second, because this is a cross-sectional study, I cannot infer whether
a given node (item or domain) causes or is caused by another node to which it is connected;
determination of causality requires time-series which may be interesting in follow-up studies
of, for instance, young individuals with and without childhood adversities (Fritz et al., 2018).
113
Chapter 7
A network model of narcissism
Abstract
The aim of this work is to explore the Narcissistic Personality Inventory (NPI) using
network analysis in a dataset of 942 university students from the French-speaking part
of Belgium. I estimated an Ising Model for the forty items in the questionnaire and
explored item interconnectedness with strength centrality. The NPI is presented as
an overall positively connected network with items from entitlement, authority and
superiority reporting the highest centrality estimates. Network analysis highlights new
properties of items from the NPI. Future studies should endeavor to replicate my
findings in other samples, both clinical and non-clinical.
7.1 Introduction
Narcissism has been defined as the ability to maintain a positive self-image despite various
internal and external processes. Narcissistic subjects have a need for self-enhancing experi-
ences from their social environment (Pincus et al., 2009). Narcissism has been theorized to
possess both normal and pathological aspects, which have been considered by some authors
as two different personality constructs (Von Kanel et al., 2017) and as a continuum by oth-
ers (Paulhus, 1998). Grandiosity and vulnerability are considered as the two expressions of
114
narcissism (Cain et al., 2008): grandiose narcissism is associated with the predisposition to
exploit others, a lack of empathy and one’s feelings of entitlement and superiority, whether
vulnerable narcissism is associated with a depleted self-image, social withdrawal and suici-
dality (Miller et al., 2013). The current gold-standard models of narcissism, the trifurcated
model (Miller et al., 2016) and the narcissism spectrum model (Krizan and Herlache, 2018)
postulate that grandiosity and vulnerability are two largely independent factors that are tied
together by a core of entitlement.
The main tool used to study the construct of narcissism is the Narcissistic Personality
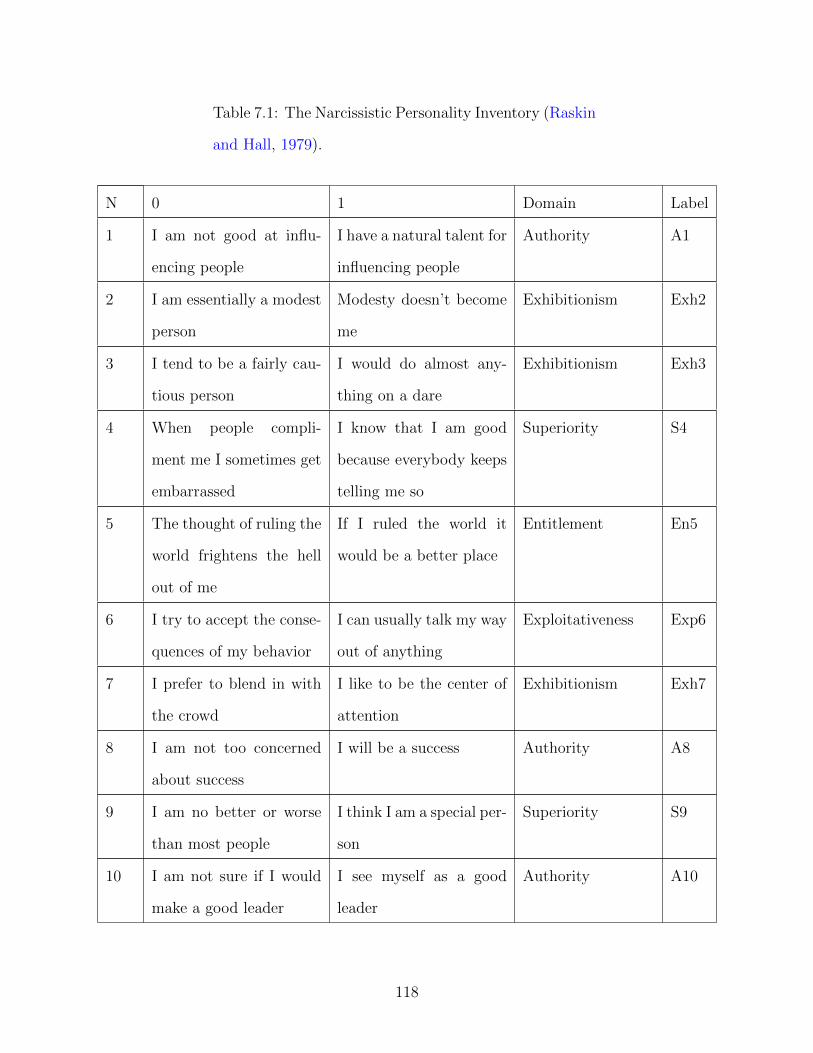
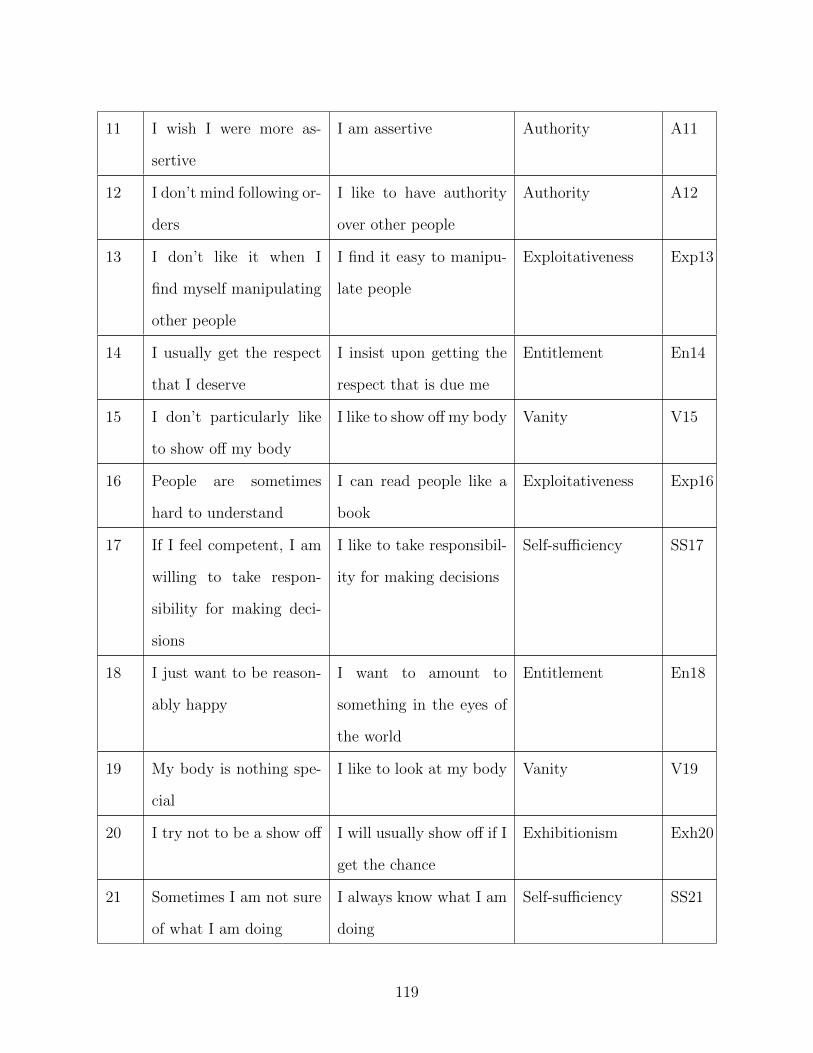
Inventory or NPI (Raskin and Hall, 1979), which represents grandiose narcissism (Krizan
and Herlache, 2018). The NPI consists of forty dichotomous items composed of both a
narcissistic and a non-narcissistic statement. The authors of the questionnaire propose seven
domains of narcissism: authority reflects one’s need for authority and success (e.g., item 33
“I would prefer to be a leader”); exhibitionism represents one’s need to be the center of
attention in a social context (e.g., item 30 “I like to be the center of attention”); superiority
measures one’s belief of being better than other people (e.g., item 40 “I am an extraordinary
person”); entitlement reflects one’s desire to receive respect and wield power (e.g., items 14
“I insist upon getting the respect that is due me” and 27 “I have a strong will to power”);
exploitativeness represents one’s capacity to manipulate other people (e.g., item 13 “I find it
easy to manipulate people”); self-sufficiency measures one’s autonomy and belief in oneself
(e.g., items 22 “I rarely depend on anyone else to get things done” and 34 “I am going to
be a great person”); vanity measures one’s admiration of one’s own physical appearance
(e.g., item 19 “I like to look at my body”). However, this seven-domain structure of the
NPI is controversial; several studies report different structures of the questionnaire, such as
a four-factor model (Emmons, 1987) and a three-factor model (Boldero et al., 2015).
Despite inconsistent results in the exploration of dimensionality (Ackerman et al., 2011;
Corry et al., 2008; Kubarych et al., 2004), narcissism is commonly understood as composed
of domains that are interchangeable measures of the construct proposed. In the last decade,
115
a new way of analyzing psychological constructs as complex systems has been proposed:
the network approach (Borsboom, 2017). Such complex systems are uncovered in empirical
studies with network models, that represent a given construct as emerging from mutual
interactions of its components (Borsboom and Cramer, 2013).
The network approach has been used to analyze a number of mental disorders, such as
depression (Mullarkey et al., 2018), posttraumatic stress disorder (Fried et al., 2018; Phillips
et al., 2018). Psychological constructs such as personality (Costantini et al., 2015), empathy
(Briganti et al., 2018) and self-worth (Briganti et al., 2019) have also been proposed as
network structures. The Pathological Narcissism Inventory has been recently investigated
through the lens of network analysis (Di Pierro et al., 2019), which identified Contingent self-
esteem, Grandiose Fantasies and Entitlement Rage to be important traits of the constructs.
A network can be composed of items of a questionnaire such as the NPI. In the case of a
network of self-reported questions, several items tend to be redundant and represent the
same aspect of a construct; this has been described in the network literature as a delicate
challenge, since the meaning of a connection between two redundant elements changes and
simply represent shared variance between the two corresponding questions that measure the
same thing (Fried and Cramer, 2017).
This challenge applies to the NPI: for instance, items 19 (“I like to look at my body”)
and 29 (“I like to look at myself in the mirror”) are two very similar measurements from
vanity. This is the case for several other items in the questionnaire, including items from
different domains, such as items 12 (“I like to have authority over other people”) and 27
(“I have a strong will to power”) that respectively belong to authority and entitlement. In
a network structure, I would expect these items to be strongly associated. It is plausible
to consider narcissism as a network of components (in this case, items from a self-reported
questionnaire indicating an individual’s perspective on narcissistic traits) that mutually in-
fluence each other instead of being passive consequences of the same construct. The network
approach to narcissism is relevant because it might allow in clinical samples the identification
116
of meaningful targets for intervention, even more so if considered that normal and patholog-
ical narcissism form a continuum. The aim of this work is to explore for the first time NPI
items and their relationship in a network of narcissism, therefore applying network analysis
to the items of the questionnaire. Network analysis has been shown to offer substantial in-
sight as a complementary tool to factor analysis, which is a more established technique in the
field of personality assessment (Briganti et al., 2018): as mentioned, modeling a construct or
mental disorder as a network can highlight connections between items or symptoms which
can therefore be used for intervention (Blanken et al., 2019). First, I want to explore the
connectivity of the NPI network. Second, I want to explore the importance of each item in
the questionnaire using strength centrality, which is the absolute sum of connections of a
given node in the network (Boccaletti et al., 2006).
7.2 Method
7.2.1 Participants
The data set used for this study is composed of 942 university students from the French-
speaking region of Belgium. The participants were first-year students in several Belgian
universities and in different undergraduate courses and they volunteered to fill a set of
questionnaires which included a French version of the NPI.
7.2.2 Measurement
The NPI (Table 7.1) contains 40 items that are meant to assess seven domains of narcis-
sism: authority, exhibitionism, superiority, entitlement, exploitativeness, self-sufficiency and
vanity. Items from different domains are shuffled in the questionnaire, and their scoring is
dichotomous: each item possesses both a narcissistic and a non-narcissistic statement. The
protocol of this study was approved by the Ethical Committee of the Erasme university
hospital.
117
Table 7.1: The Narcissistic Personality Inventory (Raskin
and Hall, 1979).
N 0 1 Domain Label
1 I am not good at influ-
encing people
I have a natural talent for
influencing people
Authority A1
2 I am essentially a modest
person
Modesty doesn’t become
me
Exhibitionism Exh2
3 I tend to be a fairly cau-
tious person
I would do almost any-
thing on a dare
Exhibitionism Exh3
4 When people compli-
ment me I sometimes get
embarrassed
I know that I am good
because everybody keeps
telling me so
Superiority S4
5 The thought of ruling the
world frightens the hell
out of me
If I ruled the world it
would be a better place
Entitlement En5
6 I try to accept the conse-
quences of my behavior
I can usually talk my way
out of anything
Exploitativeness Exp6
7 I prefer to blend in with
the crowd
I like to be the center of
attention
Exhibitionism Exh7
8 I am not too concerned
about success
I will be a success Authority A8
9 I am no better or worse
than most people
I think I am a special per-
son
Superiority S9
10 I am not sure if I would
make a good leader
I see myself as a good
leader
Authority A10
118
11 I wish I were more as-
sertive
I am assertive Authority A11
12 I don’t mind following or-
ders
I like to have authority
over other people
Authority A12
13 I don’t like it when I
find myself manipulating
other people
I find it easy to manipu-
late people
Exploitativeness Exp13
14 I usually get the respect
that I deserve
I insist upon getting the
respect that is due me
Entitlement En14
15 I don’t particularly like
to show off my body
I like to show off my body Vanity V15
16 People are sometimes
hard to understand
I can read people like a
book
Exploitativeness Exp16
17 If I feel competent, I am
willing to take respon-
sibility for making deci-
sions
I like to take responsibil-
ity for making decisions
Self-sufficiency SS17
18 I just want to be reason-
ably happy
I want to amount to
something in the eyes of
the world
Entitlement En18
19 My body is nothing spe-
cial
I like to look at my body Vanity V19
20 I try not to be a show off I will usually show off if I
get the chance
Exhibitionism Exh20
21 Sometimes I am not sure
of what I am doing
I always know what I am
doing
Self-sufficiency SS21
119
22 I sometimes depend on
people to get things done
I rarely depend on any-
one else to get things
done
Self-sufficiency SS22
23 Sometimes I tell good
stories
Everybody likes to hear
my stories
Exploitativeness Exp23
24 I like to do things for
other people
I expect a great deal from
other people
Entitlement En24
25 I take my satisfactions as
they come
I will never be satisfied
until I get all that I de-
serve
Entitlement En25
26 Compliments embarrass
me
I like to be complimented Superiority S26
27 Power for its own sake
doesn’t interest me
I have a strong will to
power
Entitlement En27
28 I don’t care about new
fads and fashions
I like to start new fads
and fashion
Exhibitionism Exh28
29 I am not particularly in-
terested in looking at my-
self
I like to look myself in the
mirror
Vanity V29
30 It makes me uncomfort-
able to be the center of
attention
I really like to be the cen-
ter of attention
Exhibitionism Exh30
31 People can’t always live
their lives in term of
what they want.
I can live my life in any
way I want to
Self-sufficiency SS31
120
32 Being an authority
doesn’t mean that much
to me
People always seem to
recognize my authority
Authority A32
33 It makes little difference
to me whether I am a
leader or not
I would prefer to be a
leader
Authority A33
34 I hope I am going to be
successful
I am going to be a great
person
Self-sufficiency SS34
35 People sometimes believe
what I tell them
I can make anybody be-
lieve anything I want
them to
Exploitativeness Exp35
36 Leadership is a quality
that takes a long time to
develop
I am a born leader Authority A36
37 I don’t like people to pry
into my life for any rea-
son
I wish somebody would
someday write my biog-
raphy
Superiority S37
38 I don’t mind blending
into the crowd when I go
out in public
I get upset when people
don’t notice how I look
when I go out in public
Exhibitionism Exh38
39 There is a lot that I can
learn from other people
I am more capable than
other people
Self-sufficiency SS39
40 I am much like every-
body else
I am an extraordinary
person
Superiority S40
121
7.3 Network analysis
The software R (open source, available at https://www.r-project.org/) was used to carry
out the analyses. I used the R-packages “qgraph” (Epskamp et al., 2012) and “glasso”
(Friedman et al., 2014b) and IsingFit (van Borkulo et al., 2014) for network estimation and
visualization, and “bootnet” (Epskamp and Fried, 2018) for stability analyses.
7.3.1 Network estimation
An Ising Model (IM) was estimated from my dataset. An IM (van Borkulo et al., 2014;
Marsman et al., 2018) is the binary equivalent of the Gaussian Graphical Model used for
continuous datasets (Epskamp and Fried, 2018). A lasso (least absolute shrinkage and se-
lection operator) was used to provide a conservative network structure (Epskamp and Fried,
2018). I used the default eLasso procedure which combines an l1-regularized logistic re-
gression with an Extended Bayesian Information Criterion or EBIC (Chen and Chen, 2008)
which reports relevant connections between variables. The lasso procedure provides a neigh-
borhood (set of nodes that interact) and decides the best set of regression coefficients given
the data, based on EBIC (which is in turn based on log likelihood); the set of regression
coefficients with the lowest EBIC is the best fit. To construct the final network, a connec-
tion is drawn between two nodes A and B if node A has node B in its set of neighbors and
vice-versa.
The default eLasso procedure was used in bootnet and IsingFit (van Borkulo et al.,
2014). The hyperparameter gamma (to select how many edges the model recovers) was set
by default at 0.25; the optimal tuning parameter lambda (used to select the model with
the best fit) was automatically chosen by the eLasso procedure. The network structure
resulting from this estimation contains items from the NPI represented as nodes. An edge
is a connection between two nodes in the network, which is interpreted as the existence of a
connection between two nodes controlling for all other nodes in the network.
122
While estimating a network structure from items of a questionnaire, a connection between
two nodes means that the observed group answers on average in a similar way to both items
of the questionnaire (Briganti et al., 2018). Each edge in the network represents either a
positive (visualized as blue edges) or a negative connection (visualized as red edges). The
thickness and color saturation of an edge denotes its weight (the strength of the connection
between two nodes). The Fruchterman-Reingold algorithm places the items in the network
based on the inverse of the sum of connections of a given node with other nodes (Fruchterman
and Reingold, 1991): this means that strongly connected nodes are put closer in the network
visualization.
7.3.2 Network inference
I estimated strength centrality (Boccaletti et al., 2006) for the 40 items in the questionnaire.
Strength centrality represents the absolute sum of the edges of a given node and therefore
informs us of the connectedness of items in the network (Briganti et al., 2018).
7.3.3 Network stability
Stability analyses (Epskamp and Fried, 2018) were carried out through bootstrapping, which
is a repeated estimation of a model under sampled data: I used 2000 bootstraps in this pa-
per. An edge weight difference test was performed to compare all edges against all other
edges and to answer the question “is edge A significantly stronger than edge B?”. Centrality
stability analyses for strength centrality were also carried out to answer the question “is the
centrality order stable?”. Centrality difference test was performed to answer the question
“is the centrality estimate of node A statistically different from that of node B?”. I used the
subsetting bootstrap procedure that re-estimates the network with a dropping percentage of
participants to determine the stability of centrality estimation, and results in a centrality-
stability coefficient (CS-coefficient) that should not be lower than 0.25 and preferably above
0.5. Both difference tests (edge weight and centrality) are carried out by estimating con-
123
fidence intervals around the difference of two elements A and B (which are bootstrapped
edge weights or bootstrapped centrality estimates, depending on the test): if 0 belongs in
the confidence interval then there is no difference between A and B.
7.4 Results
7.4.1 Participants
Participants were 17 to 25 years old (M=20 years, SD=1.7 years), 55% of them were female
and 45% were male. 25.4% of students studied engineering, 20% medicine, 17.7% economics,
11.3% sciences, 4.7% psychology and 2% law. The average NPI score of the participants of
this study was 13 (out of 40), and the standard deviation was 6.4.
7.4.2 Network of narcissism
Figure 7.1 illustrates the estimated network of the 40-item NPI. Overall, items from the
NPI form a positively connected network. The strongest connections in the network are
found between nodes belonging to the same domain of narcissism: for instance, item 10
(“I see myself as a good leader”) is strongly associated to item 33 (“I would prefer to be
a leader”) and both belong to the authority domain; item 7 (“I like to be the center of
attention”) presents the second strongest connection in the network to item 30 (“I really
like to be the center of attention”) and both belong to exhibitionism; item 9 (“I think
I am a special person”) shares the strongest edge of the network with item 40 (“I think
I am an extraordinary person”) and both belong to the superiority cluster. In the case
of these three connections, the items involved in an edge measure the same aspect of the
construct. Several connections are found between items belonging to different domains, and
I want to illustrate some of these connections. Domains superiority and self-sufficiency are
connected through items 9 (“I think I am a special person”) and 39 (“I am more capable than
other people”); domains authority and entitlement connect through items 12 (“I like to have
124
A1
Exh2
Exh3
S4
En5
Exp6
Exh7
A8
S9
A10
A11
A12
Exp13
En14
V15
Exp16
SS17
En18
V19Exh20
SS21SS22
Exp23
En24
En25
S26
En27
Exh28
V29
Exh30
SS31
A32
A33
SS34
Exp35
A36
S37
Exh38
SS39
S40
Figure 7.1: Network composed of the 40 items from the NPI (Table 7.1). Each item isrepresented by a node (1 to 40) and belongs to a different domain of the NPI (indicatedby a color code). The name of each node is composed as following: an abbreviation of thedomain to which the item belongs to followed by the item number.
125
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●●
●
●
●
●
● ●
●
●
●
●
●
●
●
●
●
●
●
●●
●
●●
●
0 10 20 30 40
01
23
45
67
Index
grap
h1.c
$InD
egre
e
Figure 7.2: Strength centrality estimates for the 40 items of the NPI. The Y-axis repre-sents centrality indices (the higher the estimate the more central the item), and the X-axisrepresents the 40 NPI items.
authority over other people”) and 27 (“I have a strong will to power”); domains authority and
exploitativeness connect through items 1 (“I have a natural talent for influencing people”)
and 35 (“I can make anybody believe anything I want them to”). These domains also tend to
measure the same thing, even though belonging to different domains. Some small, negative
edge are also found in the network, such as the one between items 11 (“I am assertive”) and
24 (“I expect a great deal from other people”).
7.4.3 Network inference
Figure 7.2 shows strength centrality estimates for the 40-item NPI. Item 27 from entitlement
(“I have a strong will to power”) presents the highest strength estimate, which means that
it is the most interconnected node in the network. Other strong items include item 33
from authority (“I would prefer to be a leader”) and item 40 from superiority (“I am an
extraordinary person”). Several items present with a strength centrality of 0, which means
that they are not connected with any item in the network.
126
7.4.4 Network stability
The edge weight bootstrap shows relatively narrow CIs, which indicates a precise estimation
of the edge weights in the network. The edge-weight difference test performed shows that
stronger edges are significantly stronger than other edges in the network; however, edges
9-40 and 7-30 are not statistically different from each other, which means that, even though
edge 9-40 reports a stronger connection in the network, I cannot safely interpret it to be
statistically stronger than edge 7-30. Strength centrality stability analyses report that the
centrality order is relatively stable, with a centrality stability coefficient (CS-coefficient)
of 0.67. Strength centrality difference test reports that stronger centrality estimates are
significantly stronger than other estimates but are not significantly different from each other;
for instance, I cannot infer whether the centrality of item 27 is really stronger than that of
item 33. I obtained a CS-coefficient of 0.67, which indicates stable results.
7.5 Discussion
This study is to my knowledge the first application of network analysis to the NPI. Con-
nections are shown between narcissistic domains and shed light on how they interact. Items
from the NPI are overall positively connected and some items are more connected than
others. Most items from the NPI share some variance and are connected. However, some
items present weak connections with others; this means that some nodes are conditionally
independent of all other items in the network. Connections exist both between items from
the same domain and between items from domain, and stability analyses show that I can
safely interpret connections in this study.
Several strong connections between items from the NPI are found in the network. In
the case of the three connections between items 10-33, 7-30 and 9-40 belonging to the same
domains (respectively authority, exhibitionism and superiority) as described in the Results
section, the interpretation of an edge changes (Fried and Cramer, 2017), and the resulting
127
connection simply represents shared variance between the two questions (since they measure
the same thing). In some cases, items from different domains also tend to represent the same
construct, such as items 12 and 27 that connect authority and entitlement in the network.
These items can be considered as “bridge items”, since they can transfer information from
one domain to another and vice-versa; however, bridge items as the examples described in
the Results section also tend to represent the same aspect of narcissism.
Centrality analysis shows that items from entitlement, authority, and superiority present
the highest strength centrality estimates: that means that items from these domains connect
well to a greater number of nodes in the network, therefore identifying these 3 domains as
containing specific items that are important in this NPI network. From a network point
of view, it is also not surprising to find entitlement to contain central items, as this find-
ing supports my current gold standard models of narcissism, the trifucated model (Miller
et al., 2016) and the narcissism spectrum model (Krizan and Herlache, 2018) that describe
entitlement as a connection between grandiosity and vulnerability. My finding also supports
the recent network study of pathological narcissism (Di Pierro et al., 2019), which reported
high centrality values for Entitlement Rage. In the network approach, if the observed group
scores high on a highly central node, then the observed group is also more likely to score high
on a relevant number of nodes in the network. The identification of central items may help
in identifying potential targets for clinical intervention in people suffering from narcissism.
My findings should be interpreted in the light of several limitations. First, my dataset is
composed of university students, which limits the potential generalization of my findings to
different samples. Second, because this is a cross-sectional study, I cannot infer whether a
given node (item or domain) causes or is caused by another node to which it is connected.
Third, redundancy among items that measure the same thing is an important issue that
has yet to be solved in psychological networks of self-reported questionnaires; in the case
of the NPI network, several items can be considered as redundant, which would alter the
connectivity with other items (such as reported with strength centrality values).
128
Further studies may endeavor to replicate my findings in different samples, both non-
clinical and clinical, to identify central features of narcissism.
129
Chapter 8
A network model of alexithymia
without fantasizing
Abstract
The aim of this paper is to explore network structures of the Toronto Alexithymia
Scale (TAS) in a large sample of 1925 French-speaking Belgian university students
and compare results with previous studies from different samples and tools to identify
potential targets for clinical intervention. I estimated network models for the twenty
items of the TAS and for its three domains difficulty identifying feelings, difficulty de-
scribing feelings and externally-oriented thinking. I explored item connectivity through
node predictability (shared variance with other network components). I performed an
Exploratory Graph Analysis (EGA) to explore the dimensionality of my dataset and
compare results with the original three-factor model; because a different model was pro-
posed, I estimated an additional network structure on the new structure. Items from
the TAS connect both within and between domains. The three-domain network iden-
tifies difficulty describing feelings as the most connected domain. The EGA reported
that three items from externally-oriented thinking form a new domain, distraction. In
the new four-domain network, difficulty describing feelings remains the most intercon-
nected domain; however, two negative connections are found. My findings support the
130
relative importance of identifying and describing feelings as a meaningful target for
intervention.
8.1 Introduction
The construct of alexithymia has been around for more than half a century: it was named
from Greek meaning “lack of word for emotion” (Sifneos, 1972). Alexithymia is understood
as a personality construct with four main features: 1) difficulty identifying and distinguishing
emotions from bodily sensations; 2) difficulty describing and verbalizing emotions; 3) poverty
of fantasy life; and 4) externally-oriented thinking (Loas et al., 2017).
It is a subject of interest in psychiatric research so as to better understand the physi-
ological basis of mental disorders associated with emotions, such as mania, addiction and
depression. Extensive neuroimaging research has been conducted on alexithymia, report-
ing alterations in affective arousal to external stimuli, voluntary cognitive functioning; an
impaired activation of the insula during cognitive processes has indicated a potential over-
lap between alexithymia and other psychiatric disorders presenting with impaired empathy
such as psychopathy and autism (Moriguchi and Komaki, 2013). Because of such clinical
implications, some researchers recommend totranspose the concept of alexithymia to that of
“affective agnosia” (Lane et al., 2015). The Toronto Alexithymia Scale (TAS) is the most
commonly used measure of alexithymia in empirical research (Bagby et al., 1994) and is
composed of twenty items designed to assess three domains: difficulty identifying feelings
(e.g. item 1 “I am often confused about what emotion I am feeling”); difficulty describing
feelings (e.g. item 4 “It is difficult for me to find the right words for my feelings”), and
externally-oriented thinking (e.g. item 8 “I prefer to just let things happen rather than to
understand why they turned out that way”). These three domains as originally described
are to be interpreted as passive and interchangeable consequences of the construct itself, and
therefore are not active contributors to alexithymia (Van Bork et al., 2017).
131
In the last decade, network analysis has affirmed itself as new way of analyzing data
in psychiatry and psychology, which allows to conceive constructs or mental disorders as a
complex system of mutually influencing elements (Borsboom and Cramer, 2013). In this
framework, the unobserved interactions between psychological components (for instance
symptoms, or items from a questionnaire) are often computed as regularized partial cor-
relations (Epskamp and Fried, 2018). Network analysis has been used to explore several
mental disorders, such as posttraumatic stress disorder (Fried et al., 2018; Phillips et al.,
2018), depression (Mullarkey et al., 2018), and autism (Ruzzano et al., 2015), but also psy-
chological constructs such as empathy (Briganti et al., 2018), self-worth (Briganti et al.,
2019) and resilience (Fritz et al., 2018; Briganti and Linkowski, 2019b).
When considering a network model of a psychological construct (such as represented by
a given questionnaire), a known challenge is that of redundancy of items in addressing the
measure of the same aspect of a given construct. This may result in the case of an empirical
study in a network where redundant items share very strong connections whose meaning
is different (it represents shared variance rather than a true interaction between the two
components). A solution to address this problem is the estimation of a network model of
the domains of the construct instead of a network model of items (Briganti et al., 2019)
to facilitate the process of inference (e.g. identifying relevant interactions between network
components).
Network analysis is also useful to recover the true number of item communities (or fac-
tors) in a dataset; this can be achieved to the highly effective and reliable Exploratory Graph
Analysis or EGA (Golino and Demetriou, 2017); in this case, a confirmatory factor analysis
(CFA) is useful to authenticate the structure suggested by EGA, as suggested in a simula-
tion study (Golino and Epskamp, 2017). A recent empirical study (Briganti and Linkowski,
2019b) which applied the recommended EGA procedure showed that the problem of redun-
dancy in psychological networks is not exclusive to questionnaire items but can extend to
construct domains as well; community detections in psychological networks may therefore
132
also be useful to re-evaluate the construct themselves.
Network models of a construct such as alexithymia are particularly interesting to inte-
grate in clinical practice since relevant components may serve as targets for intervention
(Fried et al., 2018); in the case of alexithymia, finding and acting upon potentials tar-
gets is particularly interesting since it may attenuate the neurocognitive alterations that
have been described in the literature. The construct of alexithymia as represented by the
Bermond-Vorst Alexithymia Questionnaire (BVAQ) and the Toronto Structured Interview
for Alexithymia (TSIA) has already been explored through the lenses of network analysis
(Watters et al., 2016a,b); in the case of the TSIA whose factors closely resemble those of the
TAS, the domains difficulty identifying feelings and difficulty describing feelings formed one
community and provided the most connected items.
I therefore aim to extend the conceptual framework of psychological networks to the
construct of alexithymia as represented by the TAS. In this study, I want first to explore
alexithymia as both a network of items (as reported in the questionnaire) and domains.
Second, I want to apply EGA to recover the number of communities in the network, compare
the outcome with previous studies (Watters et al., 2016a,b), and authenticate the suggested
structure with CFA; if the result differs from the original three-domain structure, I want
to estimate the network of the structure proposed by the community detection. Third, I
want to explore the connectedness of items and domains with node predictability, which
statistically represent the shared variance of a given network component with surrounding
components (Haslbeck and Fried, 2017). These exploratory analyses may have meaningful
clinical implications and serve as basis for future replication studies to identify and act upon
potential clinical targets in people with alexithymia.
133
8.2 Method
8.3 Data set
My dataset is composed of 1925 university students from the French-speaking region of
Belgium. Subjects were 17 to 25 years old (M = 19 years; SD = 1.6 years); 58% of them
were women and 42% were men.
8.4 Measurement
The TAS (Table 8.1) is composed of 20 shuffled items that measure alexithymia in three
domains: difficulty identifying feelings, difficulty describing feelings and externally-oriented
thinking. The minimum score for each item is 1 (“I completely disagree”) and the maximum
score is 5 (“I completely agree”). The questionnaire contains reverse-scored items whose
score is reversed before data analysis (Table 8.1). The protocol for this study was approved
by the ethical committee of the Erasme teaching hospital.
Table 8.1: The Toronto Alexithymia Scale (Bagby et al.,
1994)
N Item Domain WC
1 I am often confused about what emotion I
am feeling
Difficulty identifying
feelings
1
2 It is difficult for me to find the right words
for my feelings
Difficulty describing
feelings
4
3 I have physical sensations that even doctors
don’t understand
Difficulty identifying
feelings
1
4 I am able to describe my feelings easily (re-
versed)
Difficulty describing
feelings
4
134
5 I prefer to analyse problems rather than just
describe them (reversed)
Externally-oriented
thinking
3
6 When I am upset, I don’t know if I am sad,
frightened, or angry
Difficulty identifying
feelings
1
7 I am often puzzled by sensations in my body Difficulty identifying
feelings
1
8 I prefer to just let things happen rather than
to understand why they turned out that way
Externally-oriented
thinking
3
9 I have feelings that I can’t quite identify Difficulty identifying
feelings
1
10 Being in touch with emotions is essential (re-
versed)
Externally-oriented
thinking
3
11 I find it hard to describe my feelings more Difficulty describing
feelings
4
12 People tell me to describe my feelings more Difficulty describing
feelings
4
13 I don’t know what’s going on inside me Difficulty identifying
feelings
1
14 I often don’t know why I am angry Difficulty identifying
feelings
1
15 I prefer talking to people about their daily
activities rather than their feelings
Externally-oriented
thinking
2
16 1 prefer to watch “light” entertainment
shows rather psychological dramas
Externally-oriented
thinking
2
17 It is difficult for me to reveal my innermost
feelings, even to close friends
Difficulty describing
feelings
4
135
18 I can feel close to someone, even in moments
of silence (reversed)
Externally-oriented
thinking
3
19 I find examination of my feelings useful in
solving personal problems (reversed)
Externally-oriented
thinking
3
20 Looking for hidden meanings in movies or
plays distracts from their enjoyment.
Externally-oriented
thinking
2
8.4.1 Network analysis
Software
I used the software R (open source, available at https://www.r-project.org/). Packages
and functions to carry out the analysis include qgraph (Epskamp et al., 2012), glasso (Fried-
man et al., 2014b) for network estimation and visualization, mgm (Haslbeck and Waldorp,
2016) for node predictability, EGA (Golino and Epskamp, 2017) and igraph (Csardi and Ne-
pusz, 2006) for community detection, lavaan (Rosseel, 2012) for CFA and bootnet (Epskamp
and Fried, 2018) for stability.
Item network
A correlation matrix was calculated for the 20 TAS items and used as input to estimate a
Gaussian Graphical Model (GGM) which is a regularized partial correlation network (Ep-
skamp and Fried, 2018). I regularized the parameters of the GGM with a graphical lasso
(least absolute shrinkage and selection operator). Although recent relevant discoveries in
the network field (Williams et al., 2019) showed that regularized partial correlation network
estimation may provide an anti-conservative network model, my regularized TAS network
model reports fewer edges (and is therefore easier to interpret) than the nonregularized
partial correlation network.
The item network is composed of nodes representing alexithymia questions from the
TAS, and each node is surrounded by a pie chart representing its predictability (shared
variance with surrounding nodes). The position of nodes in the network is determined by
the Fruchterman-Reingold algorithm (Fruchterman and Reingold, 1991), which runs on the
sum of connections that a given node has with other nodes. Nodes are connected through
edges, which are interpreted as an association between two components, controlling for all
other nodes in the network. In the alexithymia item network, if two nodes A and B are
connected, it means for instance that if the observed group scored high on A, then the
observed group is also more likely to score high on B and vice versa (Briganti et al., 2018).
Each edge in the network has a weight which is defined as the importance of association
between two nodes and is denoted by thickness and color saturation; edges can therefore
be positive (blue edges, denoting a positive association) or negative (red edges, denoting a
negative association). For this work, I lowered the lambda parameter (tuning parameter).
Three-domain network
To better explore the interactions between alexithymia domains from the TAS, I estimated
a factor model for the three domains and obtained factor scores to estimate a GGM and
therefore a domain network as described in recent empirical papers (Briganti et al., 2019;
Briganti and Linkowski, 2019b).
Network stability
To safely interpret results from network analysis several stability tests were performed as
recommended in the literature (Briganti et al., 2018; Epskamp and Fried, 2018). To answer
the question “are edge weights accurately estimated”, 95% confidence intervals (CI) were
estimated through bootstrapping (2000 bootstraps were used). To answer the question “is
edge A significantly stronger than edge B” I performed an edge weight difference test.
137
Network inference
Node predictability (Haslbeck and Fried, 2017) represents shared variance that a given node
has with surrounding nodes; it has been defined as the upper bound of controllability: if
one assumes that all edges for a given node are directed toward that node, then node pre-
dictability provides an estimate of how much influence one can have on that node via all
other nodes (Briganti et al., 2019). Node predictability was estimated for all nodes in the
item and domain network and is represented as a pie chart surrounding each node.
To detect the number of communities in my TAS dataset, an EGA was performed (Golino
and Epskamp, 2017), which uses the walktrap algorithm. The algorithm is based on the
principle that adjacent nodes tend to belong to the same community (Yang et al., 2016).
Following the methodology of a recent study (Briganti and Linkowski, 2019b) and because
I found a different number of dimensions than the original model, I estimated an additional
network structure based on the results from EGA.
Four-domain network
I used CFA to estimate a four-factor model in the data and used the scores to estimate an
additional GGM. Node predictability and stability analyses were also carried out.
8.5 Results
8.5.1 Item network
Figure 8.1 shows the 20-item alexithymia network. Nodes connect both within and between
communities. I will hereby detail some of the connections. Item 2 (“It is difficult for me to
find the right words for my feelings”) is highly connected to item 4 (“I am able to describe
my feelings easily”, reversed) and both belong to difficulty describing feelings. Item 3 (“I
have physical sensations that even doctors don’t understand”) shares a connection with item
7 (“I am often puzzled by sensations in my body”) and both belong to difficulty identifying
138
TAS1
TAS2 TAS3TAS4
TAS5
TAS6
TAS7
TAS8
TAS9
TAS10
TAS11
TAS12
TAS13
TAS14
TAS15
TAS16
TAS17
TAS18
TAS19
TAS20
Figure 8.1: 20-item alexithymia network. Each node represents an item from the TAS ques-tionnaire (Table 8.1). The pie chart surrounding each node represents node predictability.
feelings. In these two cases, items strongly resemble each other and are therefore redundant;
the meaning of edges in this case shifts and should be interpreted as shared variance. Item 1
(“I am often confused about what emotions I am feeling”) from difficulty identifying feelings
and 2 (“It is difficult for me to find the right words for my feelings”) from difficulty describing
feelings are also strongly connected. Item 8 (“I prefer to just let things happen rather than to
understand why they turned out that way”) from externally-oriented thinking is associated
with item 9 (“I have feelings that I can’t quite identify”) from difficulty identifying feelings.
Item 15 (“I prefer talking to people about their daily activities rather than their feelings”)
from externally-oriented thinking is associated with item 17 (“It is difficult for me to reveal
my innermost feelings, even to close friends”) from difficulty describing feelings. Items 15,
16 and 20 from externally-oriented thinking are detached from the rest of the items from the
(Epskamp and Fried, 2018) for stability analyses and bnlearn (Scutari, 2010) for DAG esti-
mation.
Partial correlation network
Estimation of the partial correlation network I estimated a Gaussian Graphical
Model (GGM), that is, a partial correlation network for the items in the AQ. The GGM is
calculated as the inverse-covariance matrix: it is a network that includes a set of nodes that
correspond to the alexithymia items in the AQ and a set of edges that connect the nodes in
the network. If two nodes are connected, that means they are conditionally dependent given
all other nodes in the network (i.e their partial correlation is nonzero).
In the network of alexithymia components, if two nodes A and B are connected, it means
for instance that if the observed group scored high on component A, then the observed group
is also more likely to score high on component B, and vice versa, controlling for other nodes
in the network (Briganti et al., 2018). Each edge in the network has a weight representing
the strength of association between two alexithymia components; edges can be positive (and
therefore represent a positive association) or negative (denoting a negative association). In
the network the edge weight is represented as a combined thickness and saturation of the
edge; positive edges are shown in blue, and negative edges in red. Nodes are placed in the
network by the Fruchterman-Reingold algorithm, based on the sum of the connections a
given node has with other nodes (Fruchterman and Reingold, 1991).
Network inference To find comparatively important items in the partial correlation net-
work, I used strength centrality, which represents the absolute sum of the edges that nodes
in the network share with other nodes (Boccaletti et al., 2006).
Network accuracy and stability Accuracy and stability analyses were carried out fol-
lowing state-of-the-art methods (Epskamp and Fried, 2018) that were applied in previous
empirical papers (Briganti et al., 2018).
151
Accuracy analyses were carried out to answer the question: “is edge X accurately esti-
mated?”; 95% confidence intervals (CI) were estimated through bootstrapping (i.e., repeated
re-sampling from the original dataset to re-estimate network parameters; 2000 bootstraps
were used). Edge weight difference tests were carried out to answer the question: “is edge
X significantly stronger than edge Y?”.
Stability analyses were carried out to answer the question “is the centrality order stable?”
with the same bootstrapping method. Centrality difference tests were carried out to answer
the question “is the centrality of node A significantly stronger than the centrality of node
B?”.
Topological overlap To address the important topic of redundancy (i.e., items in the
questionnaire measuring the same aspect of the construct of alexithymia), the approach
proposed by Fried and Cramer (Fried and Cramer, 2017) of topological overlap was used.
Because items from the same domain strongly resemble each other, the most central item
from each domain (i.e items reporting the highest strength centrality score) was selected to
represent the corresponding facet of the construct in a five-item network.
Five-item network structure A five-item network structure was constructed with the
same methods described in the section “Estimation of the partial correlation network”, and
it was studied with inference analysis (that is, strength centrality computation) as well as
stability and accuracy analyses.
Directed Acyclic Graphs
In Bayesian networks an edge may represent a causal pathway between two nodes. The
structure of a Bayesian network can be estimated using constraint-based algorithms, which
analyze conditional independence relations among the nodes in the network. Constraint-
based algorithms produce a network model that can be interpreted as a causal model even
from observational data, under assumptions that in clinical terms exclude confounding and
152
sampling bias. In this paper the PC-algorithm is used, which is a constraint-based algorithm
(Spirtes et al., 1993).
To estimate a network model, the PC-algorithm first estimates an undirected network
model in which all pairs of nodes are connected, then deletes edges between conditional
independent pairs of variables, and directs edges starting with v-structures (two disconnected
nodes causing a third node). The estimated network was investigated using stability analysis
through bootstrapping.
Afterwards, a network is reported with a minimum connection strength (% of fitted
networks in which a given connection appears) of 85 and a minimum connection direction
(% of fitted networks in which a given connection has a given direction) of 50. This resulting
network therefore reports connections that are presents in more than 85% of the fitted
networks. Moreover, these connections present a direction (for instance, from node A to node
B) which is found in more than half of the fitted networks resulting from the bootstrapping
procedure. By default, with the software I used all edges are represented as red, and their
strength are represented as a combination of thickness and color saturation in the edges.
9.3 Results
9.3.1 Partial correlation network
Central items in the AQ
The five items showing the highest strength centrality values in each of the five domains are
reported in table 9.1.
“Difficulty identifying emotions” is represented by item 22, “I rarely let myself go to
my imagination”; “difficulty analyzing emotions” is represented by item 30, “I think one
should stay in touch with one’s feelings” (reversed item); “difficulty verbalizing emotions”
is represented by item 26, “When I am upset by something, I tell others about how I feel”
153
Table 9.1: Central items from the Bermond Vorst Alexithymia QuestionnaireN Item Domain22 I rarely let myself go to my imagination. Difficulty Identifying Emotions26 When I am upset by something, I tell others
about how I feel.Difficulty Verbalizing Emotions
29 I often get upset by unexpected events. Poor Emotional Insight30 I think one should stay in touch with one’s
feelings.Difficulty Analyzing Emotions
33 When I’m tired of myself, I can’t know if I’msad, afraid, or unhappy.
Poor Fantasy
(reversed item); “lack of emotional insight” is represented by item 29, “I often get upset by
unexpected events” (reversed item), and “poverty of fantasy life” is represented by item 33,
“When I’m tired of myself, I can’t know if I’m sad, afraid, or unhappy”. Three of the five
items with the highest centrality in the AQ twenty-item network have reversed scores.
Partial correlation network structure
The five-item network is represented in figure 9.1. As opposite as most construct networks
reported in the literature (Briganti et al., 2018, 2019; Briganti and Linkowski, 2019b,a,c),
the AQ network is not overall positively connected, as it includes several positive as well as
negative edges. Some of the connections in the network are described in the following. The
domains “difficulty identifying emotions” and “poor fantasy” show a positive connection, as
well as the domains “difficulty verbalizing emotions” and “emotional insight”, “poor emo-
tional insight” and “difficulty analyzing emotions”, and “difficulty verbalizing emotions” and
“difficulty analyzing emotions”. The domains “poor emotional insight” and “poor fantasy”,
are negatively connected in the network.
Network inference
The centrality estimates for the five-item network are reported in figure 9.2. Item 33 from
the domain “poor fantasy” and item 29 from the domain “poor emotional insight” report
Figure 9.1: Partial correlation network. Each item represents one of the five domains in theAQ. Blue connections represent positive edges, red connections represent negative edges.
155
●
●
●
●
●
Strength
−1.0 −0.5 0.0 0.5 1.0
A22
A26
A29
A30
A33
Figure 9.2: Strength centrality estimates for the five-item network. The x-axis reports thestandardized z-scores and the y-axis reports the corresponding item.
Figure 9.3: Directed Acyclic Graph of alexithymia components obtained with the constraint-based PC-algorithm. Relationships between nodes (arrows) can be understood as causalpathways under certain assumptions.
Network accuracy and stability
Edges are overall accurately estimated in both the five-item and twenty-item network. I can
safely interpret stronger edges to be significantly stronger than weaker edges in the network.
Centrality estimates of nodes 29 and 33 in the five-item network are not significantly different,
which means I cannot say which of the two items is the most central.
9.3.2 Directed Acyclic Graph
The DAG of alexithymia components is reported in figure 9.3. Item 29 from the domain
“poor emotional insight” has three incoming edges from “poor fantasy” (item 33), “difficulty
verbalizing emotions” (item 26) and “difficulty analyzing emotions” (item 30). Item 22 from
157
the domain “difficulty identifying emotions” has an outgoing edge to item 33 from the domain
“poor fantasy”.
9.4 Discussion
This is to my knowledge the first network analysis of alexithymia components that com-
bines the classic partial correlation network approach with the Bayesian network approach.
Several of the resulting analyses bring new and interesting information on the construct of
alexithymia.
The partial correlation network for the twenty-item AQ reports a structure with an
overall mixture of positive and negative connections among items. Because items from the
same domain tend to measure the same aspect of the construct of alexithymia (that is, the
domain they belong to), the solution of topological overlap is applied: the original twenty-
item network is translated to a network of the five items in the AQ that have the highest
centrality values in their respective domains and that are reported in table 9.1. In this work,
the exploratory analyses on the twenty-item network (representing the full questionnaire) was
important to highlight with network inference methods relevant alexithymia components so
as to analyze a more simple and non-redundant network structure.
The five-item network reports, similarly to the twenty-item network, a set of positive
and negative edges: alexithymia components therefore present a heterogeneous connectivity.
Items from domains “poor emotional insight”, “difficulty verbalizing emotions”, “difficulty
analyzing emotions” share a set of positive connections: this means that the average score
of the observed group on one of these three questions can be predicted based on the score
on the other two questions. The same phenomenon is observed with items representing
the domains “difficulty identifying emotions” and “poor fantasy”. However, “poor fantasy”
and “poor emotional insight” are negatively connected, which from an undirected network
perspective, can be interpreted as follows: given all other alexithymia components in the
158
network, if the average score on one component is high, I may expect that the average score
of the observed group on the other component is low, and vice versa. My findings differ
slightly in that respect from the recent work of Watters et al (Watters et al., 2016b), in
which the two domains sharing a negative connection are “difficulty identifying emotions”
and “poor fantasy”.
The inference analyses show that items 29 and 33 share a negative connection in the
five-item network and are also the two items with the highest centrality estimates. However,
stability analyses show how the two centrality indices are not statistically different from each
other, hence I cannot say whether item 29 (that reports the highest centrality estimate) is
really the most central item.
In this work, the study of the undirected interplay among relevant alexithymia compo-
nents was an important preliminary step before entering the realm of causal inference through
the lenses of Bayesian networks. The DAG structure derives from the constraint-based PC-
algorithm. Directed connections between alexithymia components can be interpreted as
causal pathways under assumptions that in clinical terms exclude confounding and sampling
bias. The DAG reports that “poor emotional insight”, the lack of ability to fantasize, is
essentially a consequence of a poor ability to fantasize, a difficulty in verbalizing emotions
and a difficulty in analyzing emotions.
The information from the undirected five-item network inference analyses and the Bayesian
network analyses can be combined to obtain some interesting insights. First, in the partial
correlation network, “poor emotional insight” has a high estimated centrality, and the overall
item connectivity to other items in the network can be interpreted as predictability. Second,
the DAG shows that all edges that item 29 shares with other nodes point towards “poor
emotional insight”, which means that not only is “poor emotional insight” is a highly “pre-
dictable” domain of alexithymia, but that it is also a highly “controllable” domain of the
construct. This notion can be interpreted as that the aspect of alexithymia that deals with
the lack of insight regarding emotional arousal can be controlled through other aspects of
159
the construct.
The two network models proposed in this paper present similarities as well as differences:
for instance, both the partial correlation network and the DAG share several edges between
the same nodes; however, some nodes that are connect in the partial correlation network
are not connected in the DAG. The reason is the different definitions of the two models: in
a DAG two nodes are not automatically connected when they share a common child node
(such as item 29), but they will be connected in the corresponding partial correlation network
because of the indirect dependence conditional on that child node.
My results must be interpreted in light of several limitations. First, my data set is com-
posed of university students, which may limit the generalization of my findings to different
samples. Second, DAG structures do not involve loops: if in a three-node network a com-
ponent A causes component B and a component C, component C cannot cause component
A (the structure is therefore acyclic). However, it is plausible to consider that in the case
of alexithymia components, certain items may activate each other in a loop. Third, causa-
tion may be inferred from a connection between two nodes in a DAG assuming there are
no confounding or sampling bias. Further studies may endeavor to replicate my findings of
network structures (both Bayesian and non-Bayesian) of alexithymia components in different
samples, both non-clinical and clinical.
160
Chapter 10
A network model of autistic traits
Abstract
The aim of this work is to explore the construct of autistic traits through the
lens of network analysis with recently introduced Bayesian methods. A conditional
dependence network structure was estimated from a data set composed of 649 university
students that completed an autistic traits questionnaire. The connectedness of the
network is also explored, as well as sex differences among female and male subjects
in regard to network connectivity.The strongest connections in the network are found
between items that measure similar autistic traits. Traits related to social skills are the
most interconnected items in the network. Sex differences are found between female and
male subjects. The Bayesian network analysis offers new insight on the connectivity
of autistic traits as well as confirms several findings in the autism literature.
10.1 Introduction
For the past two decades, there has been a growing interest in psychiatric research for the
classification and measurement of autistic traits (Volkmar et al., 2009). The Diagnostic and
Statistical Manual of Mental Disorders (DSM-V) has defined a framework for autistic traits:
the Autism Spectrum Disorder (ASD), that includes child autism, Kanner’s infantile autism,
161
high-functioning autism, and Asperger Syndrome.
To diagnose a patient with ASD as defined in the classification, the clinician must use
diagnostic criteria that associate persisting deficits in communication and social interactions
with narrow and repetitive behaviors, interests or activities. These two features manifest in
childhood, affect social, academic or professional functioning, and are not better explained by
an intellect developmental disorder or a global developmental delay (American Psychiatric
Association, 2013). Although initially considered as an abnormal condition, several works
have showed how the distribution of autistic traits across the population is continuous (Wing,
1988; Constantino and Todd, 2003), and people diagnosed with autism score at the extreme
end of the distribution when autistic traits are measured (Baron-Cohen, 2010).
The Autism-Spectrum Quotient (AQ) is a widely used self-administered questionnaire
that provides a quantified evaluation of the degree to which an adult with a normal intelli-
gence quotient presents with signs of ASD. This measurement tool assesses the respondent’s
behaviors, preferences and cognition based on five domains of autistic functioning: social
skill, attention switching, attention to detail, communication, and imagination; autistic traits
are considered when the respondent shows poor social skill, strong attention focus, excep-
tional attention to detail, poor communication and poor imagination (Baron-Cohen et al.,
2001). The AQ was translated in several languages, such as Italian (Ruta et al., 2012),
Dutch (Hoekstra et al., 2008), Chinese (Lau et al., 2013), Japanese (Wakabayashi et al.,
2006), Turkish (Kose et al., 2013), Polish (Pisula et al., 2013), and Persian (Mohammadi
et al., 2012), and French (Kempenaers et al., 2017), and its structural validity was studied
using exploratory and confirmatory factor analysis (EFA and CFA) in the different trans-
lations. Although initial evidence supporting the structural validity of AQ, several studies
reported doubts regarding the factorial aspects of the tool (Hoekstra et al., 2011; Hurst et al.,
2007), with multiple works not obtaining the five-factor original model to fit in student data
(Hoekstra et al., 2011; Kloosterman et al., 2011; Lau et al., 2013); most of which argued for
shorter versions of the questionnaire. An abridged ten-item version of the AQ was therefore
162
created including “red flag” items for autism screening in general practice (Allison et al.,
2012). Despite criticism, the AQ is the most commonly used measurement tool for autistic
traits detection and is widely cited in scientific research (Ruzich et al., 2015).
The AQ was conceived based on the assumption that autistic traits are measurable con-
sequences of an underlying cause – that is, ASD. There is growing evidence pointing towards
defects in neuronal migration and the consequent malformation and malfunction of various
brain circuits as etiology of several brain disorders such as ASD (Pan et al., 2019), which
then presents itself through several autistic traits; as understood in the latent variable model
of mental illness, however, autistic traits do not actively participate to the clinical manifesta-
tion in subjects, as they are effects of the construct they stem from. Recent works, however,
have shown how behaviors in the autism spectrum reinforce each other (i.e. present a mutual
influence): learning strategies can therefore be adopted as to correct the social behavior of
people with autistic traits, and brain responses to social stimuli can be altered, especially
if an early intervention is conducted (Schuetze et al., 2017). From an ontological point of
view, this changes the attribute of autistic traits, that evolve from measurable consequences
of ASD to participate in its clinical presentation.
In the last decade, network analysis has affirmed itself as a new way of analyzing data in
psychiatry and psychology, which allows the conception of of mental disorders or constructs
as emerging from a complex system of mutually influencing components (Borsboom and
Cramer, 2013). This novel theoretical and methodological approach has been widely used
to explore a variety of constructs including depression (Mullarkey et al., 2018), obsessive
compulsive disorder (McNally et al., 2017), empathy (Briganti et al., 2018), personality
(Costantini et al., 2015), alexithymia (Briganti and Linkowski, 2019c), self-worth (Briganti
et al., 2019), posttraumatic stress disorder (Fried et al., 2018; Phillips et al., 2018), resilience
(Fritz et al., 2018; Briganti and Linkowski, 2019b), and narcissism (Di Pierro et al., 2019;
Briganti and Linkowski, 2019a).
Researchers usually analyze mental disorders and constructs as network composed of
163
items – answers of the observed group to a given questionnaire, such as the AQ. Conceiving
mental disorders as networks is interesting in clinical practice, since relevant components
in the proposed model could serve as a target for intervention (Fried et al., 2018). Most
of the recent empirical works using network analysis compute the unobserved interactions
between psychological components as regularized partial correlations (Epskamp and Fried,
2018): this is commonly achieved with `1-regularization (Friedman et al., 2014b), which
is also known as the “least absolute shrinkage and selection operator” or “lasso”, which
pushes the smaller estimates in the network structure to zero and therefore renders a sparse
(or conservative) network. The dominant lasso procedure used in network papers is the
graphical lasso that associates the `1-regularization with an Extended Bayesian Information
Criterion to determine a tuning parameter for the Gaussian Graphical Model (i.e. the
network) λ (Chen and Chen, 2008). However, recent work (see for example Williams et al.,
2019) reported how the regularization of network estimates can be inconsistent for model
selection, and does not provide evidence for the null hypothesis (i.e. evidence for no effect);
the latter consequence is of great importance because one of the core ideas of estimating
network structure is to uncover the conditional independence structure of a construct, and
therefore zero partial correlations among the variables composing the network.
Recently, Bayesian methodology has been introduced for the estimation of network struc-
tures. This new methodological framework allows for the estimation of Gaussian Graphical
Models with posterior probabilities that can assess the conditional dependent and indepen-
dent relations among components of a network with a decision rule that can be calibrated to
a desired level of specificity (Williams, 2018a). The Bayesian approach to the estimation of
network structures shows advantages when determining conditional independence relations
based on a network estimation where the threshold for selection depends on Bayes factors
(Williams and Mulder, 2019): this technique allows for studying the amount of evidence for
no effect in a given structure, which is useful to assess the uncertainty of estimates. Despite
offering such advantages, Bayesian methodology for the estimation of Gaussian Graphical
164
Models has never been used in empirical works concerning network analysis in psychological
or psychiatric research.
Inspired by these new advances in network analysis that has been applied in many fields
of psychiatry and psychology, I apply the network methodology to autistic traits. The aim of
the present work is therefore to perform a network analysis of the autistic traits as presented
in the 50-item version of the AQ with the Bayesian inference methods that have been recently
introduced (Williams, 2018a), in a sample of 649 university students.
Autism has recently been analyzed through the lens of network analysis in relationship
with depression (van Heijst et al., 2019); however, to my knowledge, this is the first time
that the AQ in its full 50-item version is explored with the network methodology, therefore
expanding this conceptual and methodological framework to the construct of autistic traits.
In this work, I will first estimate the conditional dependence structure of the autistic traits
network. Second, I will estimate node predictability, i.e. point-estimate and confidence
intervals for variance explained in all items, to measure their overall connectedness to other
items in the questionnaire. Third, I will explore sex differences among female and male
subjects from this study. The protocol for this study was approved by the ethical committee
of Hopital Erasme (Erasme Teaching Hospital) in Brussels, Belgium.
10.2 Method
10.2.1 Data set
My data set is composed of 649 university students from the French-speaking region of
Belgium. Subjects were 17 to 25 years old (M = 19.3, SD= ± 1.49); 58% were female and
42% were male.
165
10.2.2 Measurement
The AQ is composed of 50 items that assess autistic traits based on five domains: social skill,
attention switching, attention to detail, communication, and imagination. The minimum
score for each item is 1 (“Definitely disagree”) and the maximum score is 4 (“Definitely
agree”); approximately half of the items in the questionnaire are to be reverse-scored (Baron-
Cohen et al., 2001).
10.2.3 Network analysis
Software and packages
I used the software R for statistical computing (open source, available at https://www.
r-project.org/). The package used to carry out the analysis is BGGM (Williams and
Mulder, 2019).
Network estimation
I estimated a Gaussian Graphical Model (GGM) with Bayesian methods (Williams, 2018a),
that is, a partial correlation network for the 50 items in the AQ. The GGM is calculated as
the inverse-covariance matrix: it is a network that includes a set of nodes that correspond
to the autistic traits in the AQ and a set of edges that connect the nodes in the network. If
two nodes are connected, that means they are conditionally dependent given all other nodes
in the network (i.e their partial correlation is nonzero). In the network of autistic traits, if
two nodes A and B are connected, it means for instance that if the observed group scored
high on trait A, then the observed group is also more likely to score high on trait B, and
vice versa, controlling for other nodes in the network (Briganti et al., 2018). Each edge
in the network has a weight representing the strength of association between two autistic
traits; edges can be positive (and therefore represent a positive association) or negative
(denoting a negative association). The estimation of network with Bayesian methods allows
for providing evidence for the hypothesis that best predicts the observed data. For instance,
when testing for conditional dependence relationships among nodes, providing a Bayes Factor
(BF) between 3 and 20 as a cut-off value is associated with positive evidence, while a BF >
20 is associated with strong evidence (Kass and Raftery, 1995). For the network estimation
in this paper, a BF of 20 was used.
Node predictability and sex differences
I computed Bayesian R2 for the fifty autistic traits in the network, which represents the
percentage of variance explained of a given autistic trait with all other autistic traits in the
network (Williams and Mulder, 2019): this measure is commonly defined “node predictabil-
ity” in the network literature (Haslbeck and Fried, 2017) as it can be interpreted as how
well a node connects to other nodes in the network, or the self-determination of the network.
Node predictability can be understood as the upper bound of controllability: if one assumes
that all edges for a given node are directed toward that node, predictability provides an
estimate of how much influence I can have on the given node via all other nodes (Briganti
et al., 2019). Because the estimation of node predictability results in a distribution, I com-
pared the predictability estimates of females and male subjects in my data set to detect sex
differences in the network structures.
10.3 Results
10.3.1 Partial correlation network
The autistic traits partial correlation network is reported in figure 10.1. The strongest
connections are found between items that measure the same (or similar) autistic traits: for
example item 38 (“I am good at social chit-chat”, reversed) is strongly connected to item 17
(“I enjoy social chit-chat”, reversed) and item 26 (“I frequently find that I don’t know how
to keep a conversation going“). Two other examples of this phenomenon can be found in
167
1 23
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
2324
25262728
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
4849
50
Figure 10.1: Autistic traits (N = 649) partial correlation network with the 50 items from theAQ. Each edge (connection between nodes) is denoted by a weight represented by thicknessand color saturation.
168
the connections between item 8 (“When I’m reading a story, I can easily imagine what the
characters might look like”, reversed) and 20 (“When I’m reading a story, I find it difficult to
work out the characters’ intentions”) as well as between item 9 (“I am fascinated by dates”)
and 19 (“I am fascinated by numbers”).
However, connections between items that measure different autistic traits can also be
found in the network: for instance, 27 (“I find it easy to read between the lines when
someone is talking to me”, reversed) and 36 (“I find it easy to work out what someone
is thinking or feeling just by looking at their face”, reversed), 11 (“I find social situations
easy”, reversed) and 38 (“I am good at social chit-chat”, reversed), 35 (“I am often the last
to understand the point of a joke”) and 46 (“New situations make me anxious“).
Several negative connections can also be found in the network, such as the ones between
items 18 (“When I talk, it isn’t always easy for others to get a word in edgeways”) and
32 (“I find it easy to do more than one thing at once”, reversed), 21 (“I don’t particularly
enjoy reading fiction”, reversed) and 49 (“I am not very good at remembering people’s date
of birth”, reversed), 12 (“I tend to notice details that others do not”, reversed) and 31 (“I
know how to tell if someone listening to me is getting bored”).
10.3.2 Node predictability
The computed values for node predictability in the network are reported in figure 10.2. Item
38 (“I am good at social chit-chat”, reversed) has the highest R2 score (54%) in the network,
while item 41 (“I like to collect information about categories of things”) has the lowest R2
score (9%) in the network. The average R2 score is 20%.
10.3.3 Sex differences
Figure 10.3 represents sex differences in node predictability. The autistic trait network struc-
tures are statistically different in female and male subjects, with a Kullback-Leibler diver-
gence value (that translates the difference between the two node predictability distributions)
169
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
●
4124484
154237133
1623311
33352843467
50342040212
1130271429106
39228
442532185
453649129
1947261738
0.2 0.4 0.6bayes_R2
Nod
epost.pred
Figure 10.2: Node predictability (Bayesian R2) for the 50 nodes in the partial correlationnetwork.
●Yg1 vs Yg2
4.0 4.5 5.0 5.5Predictive Check
Con
tras
t
Figure 10.3: Sex differences in the network of autistic traits.
Figure 10.4: Heat map reporting the edges that are statistically different in regard to thesex of participants. The darker the color, the higher the evidence.
of 5.8, and a p-value of 0.
A heat map is reproduced in figure 10.4 that represents which specific edges are different
in the female and male network structure (and the respective amount of evidence supporting
the difference, represented by a variation in BF). For instance, there is a moderate amount
of evidence supporting sex differences for the specific edges between items 14 (“I find making
up stories easy”) and 22 (“I find it hard to make new friends“), with a Bayes Factor of 115,
item 17 (“I enjoy social chit-chat”) and 34 (“I enjoy doing things spontaneously”), with a
Bayes Factor of 90.
The number of edges that are statistically different in regard to the sex of participants
variates among the items in the AQ and are reported in figure 10.5. Item 17 (“I enjoy social
chit-chat”) presents the highest number of edges in that regard.
Network estimation A network is composed of nodes (representing items from the SDS)
and edges (connections between items). A correlation matrix is used as input to estimate a
Gaussian Graphical Model (GGM), which is a regularized partial correlation network. Each
edge has a weight (parameter resulting from the GGM) which is regularized using a graphical
lasso (least absolute shrinkage and selection operator) to avoid the estimation of spurious
edges and therefore provides a conservative model (Epskamp and Fried, 2018). An edge
therefore represents a regularized partial correlation between two symptoms, controlling for
all other symptoms in the network. The thickness and color saturation of an edge represent
its weight (the strength of the association between two nodes); edges can therefore be positive
(blue) or negative (red). In the case of the SDS, a self-report scale which measures depression
symptoms, a positive edge can be statistically interpreted as following: if two given nodes
X and Y share an edge XY in the network, and the observed group of subjects scores high
on X, then the observed group is also more likely to score high on Y (Briganti et al., 2018).
On the other hand, a negative edge implies that if an observed group of subjects scores
high on X, then the observed group is less likely to score high on Y. Two nodes will be
disconnected if they are conditionally independent. Nodes are placed in the network by the
Fruchterman-Reingold algorithm, based on the sum of connections a given node has with
other nodes (Fruchterman and Reingold, 1991).
Network inference Node predictability is an absolute measure of the interconnectedness
of a node (Haslbeck and Waldorp, 2016) and is the percentage of variance of a given node
explained by surrounding nodes. Node predictability has been described as the upper bound
of controllability: “if one assumes that all edges for node A are directed towards that node,
predictability provides an estimate of how much influence I can have on A via all other
nodes” (Briganti et al., 2019). Node predictability is represented in the network as a pie
chart surrounding the node.
181
Network Comparison Test I performed a Network Comparison Test (NCT) to compare
networks from female and male subjects in my dataset (van Borkulo et al., 2016). The NCT
rearranges the samples to test whether two networks are invariant with respect to global
strength (sum of all edge weights), network structure and edge values.
Network stability State-of-the-art stability analyses (Epskamp and Fried, 2018) were
carried out using the same methodology used in my previous studies (Briganti et al., 2018).
An edge weight difference test was performed to answer the question “is edge A significantly
stronger than edge B?”.
Directed Acyclic Graph
In Bayesian networks an edge may represent a causal pathway between two nodes. The
structure of a Bayesian network can be estimated using constraint-based algorithms, that
analyze conditional independence relations among the nodes in the network. Constraint-
based algorithms generate a network model that can be interpreted as a causal model even
in observational data, under assumptions that in clinical terms exclude confounding and
sampling bias.
In this paper I used the PC algorithm, a constraint-based algorithm (Spirtes et al.,
1993). To estimate a network model, the PC algorithm first estimates an undirected network
model in which all pairs of nodes are connected, then deletes edges between conditional
independent pairs of variables, and directs edges starting with v-structures (two disconnected
nodes causing a third node).
The estimated network was investigated using stability analysis through bootstrapping.
Afterwards, a network is reported with a minimum connection strength (% of fitted networks
in which a given connection appears) of 85 and a minimum connection direction (% of
fitted networks in which a given connection has a given direction) of 50. This resulting
network therefore reports connections that are presents in more than 85% of fitted networks;
182
Blue
Morning
Crying
SleepP
Eat
Sex
Weight
Constipated
HeartR
Tired
Mind
Things
Restless
Hope
Irritable
Decision
Useful
LifeFull
Dead
Enjoy
Blue: I feel down hearted and blueMorning: Morning is when I feel the bestCrying: I have crying spells or feel like itSleepP: I have trouble sleeping at nightEat: I eat as much as I used toSex: I still enjoy sexWeight: I notice that I am losing weightConstipated: I have trouble with constipationHeartR: My heart beats faster than usualTired: I get tired for no reasonMind: My mind is as clear as it used to beThings: I find it easy to do the things I used toRestless: I am restless and cannot keep stillHope: I feel hopeful about the futureIrritable: I am more irritable than usualDecision: I find it easy to make decisionsUseful: I feel that I am useful and neededLifeFull: My life is pretty fullDead: I feel that others would be better off if I were deadEnjoy: I still enjoy the things I used to do
Figure 11.1: Regularized partial correlation network of items from the SDS. Each noderepresents an item from the SDS; positive connections are blue, negative connections arered. The pie chart surrounding each node represents node predictability.
moreover, these connections present a direction (for instance, from node A to node B) which
is found in more than half of the fitted networks resulting from the bootstrapping procedure.
11.3 Results
11.3.1 Regularized partial correlation network
Figure 11.1 represents the glasso network of items from the SDS. The network is overall
positively connected. The strongest connection in the network (0.26) is found between items
17 (“I feel that I am useful and needed”) and 18 (“My life is pretty full”). Other strong
connections include edge 1-3 (“I feel downhearted and blue”; “I have crying spells or feel
like it”), edge 11-12 (“My mind is as clear as it used to be”; “I find it easy to do the things
I used to”) and edge 16-17 (“I find it easy to make decisions”; “I feel that I am useful and
needed”). Items 2 (“Morning is when I feel best”) and 8 (“I have trouble with constipation”)
are poorly connected with the rest of the nodes in the network. One negative connection is
183
found between item 7 (“I notice that I am losing weight”) and 17 (“I feel that I am useful
and needed”).
Network inference
Mean node predictability is 0.23, which means that on average items from the SDS share
23% of variance with surrounding items. The most predictable node is item 11 (“My mind
is not as clear as it used to be”), which shares 38% of variance with surrounding items. The
least predictable node is item 7 (“I notice that I am losing weight”) and it shares 10% with
surrounding items.
Network Comparison Test
The networks estimated from both female and male students were substantially similar and
did not differ statistically regarding global strength, network structure and edge values.
Network stability
The edge weight difference test reports that the strongest edges (17-18; 1-3; 11-12; 16-17; 13-
15; 9-10) are significantly stronger than other edges in the network but are not significantly
different from each other; therefore, I cannot safely interpret which edge is the strongest.
11.3.2 DAG
Figure 11.2 shows the DAG estimated with PC algorithm and reporting stable connections
resulting from bootstrapping. The DAG shows some interesting directed connections; I will
describe a few examples of such edges. Item 1 (“I feel downhearted and blue”) has two
outgoing edges to items 9 (“My heart beats faster than usual”) and 14 (“I feel hopeful about
the future”). Item 2 (“Morning is when I feel best”) also has two outgoing edges to items
14 (“I feel hopeful about the future”) and 19 (“I feel that others would be better off if I
were dead”). Item 4 (“I have trouble sleeping at night”) has three outgoing edges to items
184
Blue
Morning
Crying
SleepP
Eat
Sex
Weight
Constipated
HeartR
Tired
Mind
Things
Restless
HopeIrritable
Decision
Useful
LifeFull
Dead
Enjoy
Blue: I feel down hearted and blueMorning: Morning is when I feel the bestCrying: I have crying spells or feel like itSleepP: I have trouble sleeping at nightEat: I eat as much as I used toSex: I still enjoy sexWeight: I notice that I am losing weightConstipated: I have trouble with constipationHeartR: My heart beats faster than usualTired: I get tired for no reasonMind: My mind is as clear as it used to beThings: I find it easy to do the things I used toRestless: I am restless and cannot keep stillHope: I feel hopeful about the futureIrritable: I am more irritable than usualDecision: I find it easy to make decisionsUseful: I feel that I am useful and neededLifeFull: My life is pretty fullDead: I feel that others would be better off if I were deadEnjoy: I still enjoy the things I used to do
Figure 11.2: Directed Acyclic Graph.
12 (“I find it easy to do the things I used to”), 16 (“I find it easy to make decisions”) and
17 (“I feel that I am useful and needed”). Item 15 (“I am more irritable than usual”) has
three incoming connections from items 2 (“Morning is when I feel the best”), 11 (“My mind
is as clear as it used to be”), and 17 (“I feel that I am useful and needed”). Item 19 (“I feel
that others would be better off if I were dead”) has two incoming connections from items
2 (“Morning is when I feel best”) and 16 (“I find it easy to make decisions”). Regression
coefficients for nodes in the DAG are positive, which means that nodes from the DAG are
overall positively connected.
11.4 Discussion
This is to my knowledge the first application of network analysis to the SDS. This study,
conducted in a non-clinical large sample of French-speaking university students, sheds light
on the network structure of depression items, which may replicate in clinical samples. The
regularized partial correlation network shows that items from the SDS are overall positively
connected, but the degree of connectivity of a given node from the SDS to other nodes (also
185
defined as node degree in network science) varies; for instance, I identified two items from
the SDS (2 and 8) which are overall poorly connected to the rest of the network.
From a network point of view, disconnected items may be considered to be independent
controlling for other nodes in the network. Some connections are stronger than others as
reported in the stability analyses. Some strong edges however are shared between two items
that might measure the same symptom, such as edge 1-3 (“I feel downhearted and blue”;
“I have crying spells or feel like it”); in this case, this connection should be interpreted as
shared variance between the two items (Fried and Cramer, 2017). In most cases in this
network, however, connections offer novel insight as to how symptoms interact; I will detail
one example to show such insight offered by my study. For instance, the strongest connection
in the network between items 17 (“I feel that I am useful and needed”) and 18 (“My life is
pretty full”) may be interpreted as such: at the level of the observed group and controlling
for other nodes in the network, it is more likely not to feel useful and needed if one’s life
is empty, and vice-versa; if this same edge were to replicate at the individual network of a
person diagnosed with depression, intervening on one’s feeling of having a “full life” may
alleviate the feeling of being useless, and vice-versa.
Node predictability was used to assess the connectivity of items from the SDS. Item 11
(“My mind is not as clear as it used to be”) shows the highest node predictability value, which
means it shares the most variance with surrounding nodes. As reported in the DAG structure,
this item receives many incoming edges from different surrounding items; I may therefore
consider item 11 as the most controllable item in the network. Item 11 may therefore not
be a viable target for clinical intervention if a similar network structure were to replicate in
a clinical sample, since it may be considered as the consequence of surrounding symptoms.
Future studies may also endeavor to translate the causal meaning of node predictability in
other psychometric tools. The DAG offers additional insight as to how symptoms from the
SDS may cause each other. I described several symptoms that are mainly causing other
symptoms in the network, such as item 1 (“I feel downhearted and blue”), item 2 (“Morning
186
is when I feel best”) and item 4 (“I have trouble sleeping at night”). These symptoms might
be considered as viable targets for clinical intervention if the same network structure were
to replicate in clinical samples.
The two network models proposed in this paper present similarities as well as differences:
for instance, both the regularized partial correlation network and the DAG contain positive
edges; however, nodes that connect well in the regularized partial correlation network do not
connect in the DAG such as the redundant items discussed in the results. The reason the
different definitions of the two models: in a DAG two nodes are not automatically connected
when they share a common child node, but they will be connected in the corresponding
partial correlation network because of the indirect dependence conditional on that child
node.
My results must be interpreted in light of several limitations. First, my dataset is com-
posed of university students, which may limit the generalization of my findings to different
samples. Second, DAG structures do not involve loops: if in a three-node network a symptom
A causes symptom B and a symptom C, symptom C cannot cause symptom A (the struc-
ture is therefore acyclic); however, it is plausible to consider that in the case of depression
symptoms, certain symptoms may activate each other in a loop. Third, causation may be
inferred from a connection between two nodes in a DAG assuming there are no confounding
or sampling bias.
Further studies may endeavor to replicate my findings in different samples, both non-
clinical and clinical, to replicate network structure (both Bayesian and non-Bayesian) of
symptoms described in the SDS, and look for similarities as well as differences between
different models of depression components.
187
Chapter 12
A network model of mania
Abstract
The aim of this study is to explore mania as a network of its symptoms, inspired by
the network approach to mental disorders. Network structures of both cross-sectional
and temporal effects were measured at three time points (admittance, middle of hos-
pital stay, discharge) in a sample of 100 involuntarily committed patients diagnosed
with bipolar I disorder with severe manic features and hospitalised in a specialised
psychiatric ward. Elevated mood is the most interconnected symptom in the network
at admittance, while aggressive behavior and irritability are highly predictive of each
other, as well as language-thought disorder and delusions. Elevated mood influences
many symptoms in the temporal network. Network analysis is a useful tool to model
and explore the interconnectedness and relative importance of manic symptoms, as
well as monitor their evolution over time in patients under treatment.
12.1 Introduction
The word “mania” directly derives from two Greek words: “mania”, which can be translated
as “madness”, “enthusiasm”, or “passion”, and “mainomai”, which is the verb for “mania”
and translates the concepts “to be mad”, “to be furious”, and “to rage”. The notion of
188
mania can be traced back to Sophocles and his tragedy “Aias” first played almost 2500
years ago, based on the Homeric character Ajax from the Iliad and Odyssey. Ajax became
“mainomenos” (De Jong and Rijksbaron, 2006), meaning “berserk”, because he was cast a
spell from Athena, and killed a flock of sheep believing it was a group of enemy soldiers. 500
years later, Aretaeus of Cappadocia, a physician from Alexandria, first described mania as a
“worsening of melancholia”, therefore connecting the two states in the very first description
of bipolar disorder (Angst and Marneros, 2001).
Mania has come a long way since its first descriptions. In the fifth version of the Di-
agnostic and Statistical Manual of Mental Disorders (DSM V), a manic episode is defined
as a “distinct period of abnormally and persistently elevated, expansive or irritable mood
and abnormally and persistently increased goal-directed activity or energy, lasting at least
1 week and present most of the day, nearly every day (or any duration if hospitalization is
necessary)”, which may include a subset of three or more of symptoms including grandiosity,
decreased need for sleep, speech abnormalities, flight of ideas, distractibility, psychomotor
agitation, and involvement in activities with a high potential for painful consequences (e.g.,
engaging in unrestrained buying sprees, sexual indiscretions, or foolish business investments).
A manic episode causes marked impairment in social functioning and is not attributable to
the effects of a substance or another medical condition. (American Psychiatric Association,
2013). At least one manic episode is required to diagnose a bipolar I disorder. Correctly
diagnosing mania therefore has a meaningful impact on the treatment plan and follow-up for
the patient with bipolar I disorder: however, because of all the possible 5040 combinations
of the seven manic symptoms (and 35 different subsets of three symptoms out of seven) such
as described in the DSM V, diagnosis can be challenging for the psychiatrist.
The Young Mania Rating Scale (YMRS) is clinical tool for diagnosing mania and its
severity. It is composed of eleven features meant to assess different symptoms of mania
(Young et al., 1978), namely “Elevated Mood”, “Increased Motor Activity-Energy”, “Sexual
Interest”, “Sleep”, “Irritability”, “Speech (Rate and Amount)”, “Language-Thought Disor-
189
der”, “Content”, “Aggressive Behavior”, “Appearance”, and “Insight”. The items are used
to calculate a sum score, which is supposed to indicate the severity of the manic episode. The
YMRS is largely known and it has been validated in several languages, because it showed
good reliability and validity (Young et al., 1978).
Apart from reporting similar symptoms, the YMRS and the DSM V approach to mania
have another thing in common: they consider the symptoms of mania to be interchangeable
measures of the manic episode; in other words, they do not actively contribute to it, but
are rather consequences of it. From this categorical perspective of mental illness, manic
symptoms have no contributing role in the disease itself.
The categorical approach to mental disorders (such as the one used in the DSM V) has
been heavily criticized in recent years: for instance, it has been pointed out that it is unlikely
for one to be able to pinpoint a cause for a mental disorder that, when corrected, makes
the disorder disappear completely (as it would in a somatic disease); instead, psychiatric
symptoms are likely to influence each other (Kendler et al., 2011), and the mental disorder
arises from the set of interactions among the symptoms that are related to it (Borsboom,
2017). This approach is known as the network theory of mental disorders (Borsboom and
Cramer, 2013). Many fields in psychiatric research have translated network theory into em-
pirical studies for both behavioral constructs and mental disorders: for instance schizophrenia
(Galderisi et al., 2018), depression, (Mullarkey et al., 2018), posttraumatic stress disorder
(Fried et al., 2018; Phillips et al., 2018), autism (Ruzzano et al., 2015), empathy (Briganti
et al., 2018), self-worth (Briganti et al., 2019), resilience (Fritz et al., 2018; Briganti and
Linkowski, 2019b), alexithymia (Briganti and Linkowski, 2019c) and narcissism (Briganti
and Linkowski, 2019a). Predictors of lithium response (Scott et al., 2020) and relationships
between positive and negative affects (Curtiss et al., 2019) in bipolar disorder have been
studied with the network approach. The network approach comes with a set of statistical
methods called network analysis (Epskamp and Fried, 2018): mental disorders are usually
represented as partial correlation networks in which the network components (nodes) are
190
symptoms, and the connections (edges) are the partial correlations among symptoms. When
two nodes are connected in the network, the state of one node can be used to predict the
state of the other node, and vice-versa (Epskamp et al., 2017b).
It is reasonable to consider mania as a network of mutually influencing features, that
is, symptoms reinforce each other and determine the clinical presentation of the patient
(Borsboom, 2017). For instance, it is plausible to think that, when mood is elevated, the
patient is unable to sleep: insomnia could make the patient irritable, and the irritability
may in turn cause the patient to become aggressive. Although symptoms can influence each
other, it is also plausible to imagine that a given symptom can influence itself over time:
this may be the case for insomnia.
In network analysis, important nodes can be identified based on their quality to predict
(or be predicted by) other nodes in the network, and therefore their connectivity (Haslbeck
and Fried, 2017): such important nodes, which are customarily defined as “predictive” or
“predictable”, and could be considered as good targets for clinical intervention (Fried and
Cramer, 2017). Because these parameters can be determined, modeling mania as a network
of manic features can have considerable impacts on treatment decision: one could for instance
pharmacologically act upon one highly connected node to change the state of other nodes
that are connected to it.
In the case of a network approach to mania, it is reasonable to hypothesize that elevated
mood would be a highly connected node, because of the nature of bipolar I disorder itself:
however, it is also important to study what features of mania (besides the mood alteration)
are relatively important compared to others. Another research question that is important
to address is how network connectivity evolves in patients when they get pharmacological
treatment: in other words, “do symptoms show stronger connections before treatment or
after treatment?”.
While treating a severe manic episode and targeting specific features of mania (e.g. mood
stabilizers, neuroleptics) it is also important to know how the patient will respond: in other
191
terms, how do the states of given variables at time t0 predict the state of other variables at
time t1 (with the help of treatment). This principle is driven by Granger causality in panel
data (Wild et al., 2010): one variable in t0 predicts another in t1. The study of temporal
networks constitutes an important field in network analysis (Epskamp, 2019), along with
contemporaneous or cross-sectional networks, and can be applied in the case of mania. For
instance, it is interesting from a clinical perspective to investigate how stabilizing mood
has an effect on other features, or whether there are some symptoms that stay unaffected
after treatment (e.g. they reinforce each other or themselves). Inspired by what the network
approach can offer to the construct of mania, this study aims to explore mania as a network of
its symptoms as described in the YMRS (Young et al., 1978) in a sample of 100 involuntarily
committed patients hospitalized with severe bipolar I disorder. This work is organized as
follows: first, the cross-sectional network structures of mania at the start, middle and end
of the involuntary commitment are estimated. Second, node predictability (shared variance
of a given node with surrounding nodes) is studied as a measure of absolute connectivity
and therefore importance of symptoms in the network structure (Haslbeck and Waldorp,
2016). Third, the differences between the cross-sectional networks (start, middle and end of
commitment) are estimated regarding the strength of connections (van Borkulo et al., 2014).
Fourth, a temporal network is estimated between the time points to investigate temporal
effects.
12.2 Method
12.2.1 Ethical approval
This study was approved from the Ethical Committee of the Brugmann Teaching Hospital
in Brussels (CHU Bruxelles Brugmann).
192
12.2.2 Data sets
Participants
My data set is composed of 100 patients, hospitalized in the context of an involuntary
commitment in a secure psychiatric unit. To be included in this study, patients needed to
be diagnosed with bipolar I disorder and to present with a manic episode at admission.
An abnormal blood or urine analysis in regards to toxicology as well as a concomitant
personality or somatic disorder that could account for the presence of manic symptoms were
considered as exclusion criteria. All patients were involuntarily committed for a period which
lasted for 40 days on average (following the Belgian law for involuntary commitment).
All manic patients were treated with a standard set of drugs following the local protocol
for manic patients: in the first stage of treatment (when the clinical presentation is severe),
an association of a typical and atypical antipsychotic drugs is administered, with a mood
stabilizer as well as soporific and anxiolytic drugs when necessary and depending on the
symptoms presented. In the second stage of treatment (when the clinical presentation is
stable), the patient is left with an atypical antipsychotic, a mood stabilizer, as well as a
soporific and/or anxiolytic when necessary.
Three time points were collected for each patient: on admission (t0), halfway through the
commitment period t1, and on discharge (t2). The data sets were anonymized by default.
Patients were 20 to 72 years old (M = 44.5, SD = 14.5); 47 of them were female, and 53 of
them were male.
Measurement
The YMRS (Young et al., 1978) was used to assess manic symptoms, namely “Elevated
Mood”, “Increased Motor Activity-Energy”, “Sexual Interest”, “Sleep”, “Irritability”, “Speech
(Rate and Amount)”, “Language-Thought Disorder”, “Content”, “Aggressive Behavior”,
“Appearance”, and “Insight”. Symptoms were scored 0 to 4, depending on the severity of
193
Table 12.1: Symptoms from the Young Mania Rating Scales (Young et al., 1978)N symptom Symptom1 Elevated Mood2 Increased Motor Activity-Energy3 Sexual Interest4 Sleep5 Irritability6 Speech (Rate and Amount)7 Language-Thought Disorder8 Content9 Aggressive Behavior10 Appearance11 Insight
the clinical presentation, both at t0, t1 and t2. The symptoms are illustrated in table 12.1.
12.2.3 Network Analysis
Software
The software used for the analyses carried out in this study is R (version 3.6.3, available at
https://r-project.org). The packages needed for the analyses were bootnet (Epskamp
and Fried, 2018) and qgraph (Epskamp et al., 2012) for network estimation, visualization and
stability, psychonetrics (Epskamp, 2019) for temporal network estimation, mgm (Haslbeck
and Waldorp, 2016) for network inference, and NetworkComparisonTest (van Borkulo et al.,
2016) for comparing network structures at different measurement occasions.
Network estimation
Cross-sectional networks Let y be a a normal multivariate vector y = (y1, ..., yp) with
mean vector µ and a variance-covariance matrix Σ. For all subjects,
that is known as the precision matrix or a Gaussian Graphical Model (GGM). The
elements of of the GGM encode the partial correlation coefficients θij of two variables yi and
yj given all other variables in y, that is, y−(i,j):
Cor(yi, yj|y−(i,j)
)= − θij√
θii√θjj, (12.3)
therefore, the GGM represents the network itself.
The partial correlation θij between yi and yj is used as the edge weight, that is, the
strength of the connections between nodes Vi and Vj in the network. Edge weights can be
positive (usually represented as blue connections) or negative (usually represented as red
connections) depending on the sign of θij. The presence of an edge between two nodes Vi
and Vj in the network can be interpreted as a conditional dependence relationship: node
Vi predicts (or is predicted by) node Vj, after controlling for all other nodes in the network
V−(ij).
Three separate GGMs were estimated for t0, t1 and t2 data sets to study cross-sectional
effects among manic symptoms. For the estimation of the network structures, Spearman ρ
correlation was used as an input parameter because of the structure of the data (high scores
at t0, low scores at t2).
Further details about the GGM can be found in recent state of the art methodological
works (Epskamp et al., 2018).
Temporal network To model the dynamics of manic symptoms with a pharmacological
intervention in three time points t0, t1 and t2, a panel Graphical Vector Autoregressive
Model (GVAR). This model was first introduced in recent works with its own package for
computation (Epskamp, 2019) to translate time-series methods to panel data. GVAR can
195
be seen as a multivariate multiple regression on the previous measurement occasion.
For a set of symptoms y = (y1, ..., yp) measured in a given individual, GVAR is expressed
as
yt1 |yt0 ∼ N(µ+B(yt0 − µ),Σζ), (12.4)
where B represents a p × p matrix of temporal effects, µ the vector of means, Σt0 the
variance-covariance matrix on measurement occasion t0, and ζ a vector of normally dis-
tributed innovations. Because B encodes temporal prediction, a nonzero matrix element bij
means that yt1 is predicted by yt0 : this prediction is known as Granger causality (Granger,
1969) because the condition of “cause preceding the effect” is fulfilled. Non significant tem-
poral edges in the network are recursively removed by pruning (Pearl, 1984). More details
about GVAR can be found in the recent work that first introduces it in the psychonetrics
package (Epskamp, 2019).
Network inference
Node predictability was estimated for the 11 symptoms in the three data sets. Node pre-
dictability (Haslbeck and Fried, 2017) represents shared variance of a given node with sur-
rounding nodes in a network, that is, what percentage of variance of a given node can be
explained by other nodes. It can be interpreted as an absolute measure of how well a node
is connected in the network (Fried et al., 2018).
The Network Comparison Test (NCT) was performed to compare global strength in
the three networks (van Borkulo et al., 2016). Three tests were performed, respectively to
compare t0 and t1, t1 and t2, and t0 and t2. Because the samples were not independent, the
paired version of the NCT was used.
196
Network accuracy and stability
Accuracy analyses for the cross-sectional network structures were carried out following guide-
lines in network methodology (Epskamp and Fried, 2018). For the cross-sectional networks,
the accuracy of edge weights through bootstrapping (Epskamp et al., 2017a, I used 2000
bootstraps). I bootstrapped 95% confidence intervals of all edge weights (to answer the
question “is edge A accurately estimated?“), followed by an edge weight difference test to
see which edges differ from each other in size significantly (to answer the question “is edge
A significantly larger than edge B?”).
Similar stability analyses were carried out for the temporal network: a random subset
constituted of 10% of the data were dropped and the model was re-estimated.
12.3 Results
12.3.1 Cross-sectional networks
Table 12.2: Descriptive statistics for the eleven symptoms in the three time points.Mood0 Motor0 Sexual0 Sleep0 Irritable0 Speech0 LgTtAbn0 Content0 Aggressive0 Appearance0 Insight0
The three network structures of manic symptoms at t0, t1 and t2 are illustrated in figures
12.1, 12.2 and 12.3. For easier comparison, the three network structures are combined in
figure 12.4 (while only reporting edges with a weight greater than 0.1).
Overall, the networks present both positive and negative connections, however, the rel-
ative strength of connections (compared to other connections in the same network) in the
197
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Figure 12.1: Network structure of manic symptoms at t0. Each node represents one ofthe eleven items from the YMRS. Blue connections represent positive edges, red connectionsrepresent negative edges. The pie chart surrounding each node represents node predictability.
198
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Figure 12.2: Network structure of manic symptoms at t1. Each node represents one ofthe eleven items from the YMRS. Blue connections represent positive edges, red connectionsrepresent negative edges. The pie chart surrounding each node represents node predictability.
199
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Figure 12.3: Network structure of manic symptoms at t2. Each node represents one ofthe eleven items from the YMRS. Blue connections represent positive edges, red connectionsrepresent negative edges. The pie chart surrounding each node represents node predictability.
200
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Figure 12.4: Network structure of manic symptoms at t0, t1 and t2. Each node representsone of the eleven items from the YMRS. Blue connections represent positive edges, redconnections represent negative edges. The pie chart surrounding each node represents nodepredictability. Only edges with a weight greater than 0.1 are reported.
201
−2
0
2M
ood
Mot
or
Sexu
al
Slee
p
Irrit
Spee
ch
LgTA
b
Con
t
Aggr
App
Insg
Pre
dict
abili
ty Datasets
1
2
3
Figure 12.5: Network predictability values for the t0 (red line), t1 (green line) and t2 (blueline) networks a standardized z values.
respective networks varies over time. Hereby, some of the connections are described.
Aggressive behavior shares a strong connection to irritability at t0 and t1: however, at t2,
it shares a connection with Insight instead. Language-thought disorder is highly connected to
content at all time points; content is also connected with speech at all time points. Elevated
mood shares connections with motor activity and insight.
Network accuracy
On average, stronger connections in the network are significantly stronger than weaker con-
nections, but weaker connections are not on significantly different from each other.
202
Table 12.3: Node predictability estimates for the eleven symptoms at the three time points.R2t0 R2t1 R2t2
Network predictability estimates for the three time points are reported in 12.3 and repre-
sented in figure 12.5. Elevated mood is the most interconnected node at t0, and language-
thought disorder is the most interconnected node at t1 and t2.
The NCT reported a statistically significant difference between the global strength of
t0 and t2 (p = 0.0018); however, t0 and t1, as well as t1 and t2 do not present significant
differences in global strength (p = 0.49 and p = 0.98, respectively).
12.3.3 Temporal network
The temporal network, estimated through the GVAR adapted for panel data is represented
in figure 12.6. All variables have an effect on themselves over time. However, there are
several variables in the network that are Granger-caused by other variables: for instance,
mood Granger-causes aggressive behavior (which in turn also has a temporal effect on mood),
appearance, increased motor activity, irritability and speech disorder. Other variables, such
as sleep, receive few or no temporal effects.
203
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Figure 12.6: Temporal network.
204
Stability of the temporal effects
The correlation between the temporal effects before and after dropping 10% of subjects was
0.94 and points toward a certain stability of the network structure.
12.4 Discussion
This work tackled the important issue of the study of mania as a network of symptoms.
Several measures were used to study the network structure of manic symptoms.
The strong connection between aggressive behavior and irritability t0 and t1 means that,
when mania is untreated, the two symptoms are highly predictive of one another: if patients
are irritable, then there will be a high chance for them to be aggressive as well, and vice
versa. However, when mania is treated at t1, aggressive behavior becomes predictive of
insight instead: this can be interpreted as a hint that treated manic patients that tend to
have no insight, also tend to show greater signs of aggressive behavior (even though the
mean value for aggressive behavior at t2 is close to 0 in my sample), controlling for all other
symptoms in the network.
Language-thought disorder and content are highly connected at all time points: from
a network point of view, this means that the presence of a an abnormal communication
with the patient (due to, for instance, flight of ideas or echolalia) may suggest that there
is an ongoing delusional or hallucinatory process (and vice versa), controlling for all other
symptoms. The association of language-thought disorder and delusions or hallucinations is
recurrent in the literature: recent works on psychosis also suggest that the less patients are
in control of their thought process, the more likely they suffer from hallucinations (Hartley
et al., 2015). Language-thought disorder may therefore serve as a “proxy” for psychiatrists
to better investigate hallucinatory or delusional patterns. Another possible red flag linked to
delusions or hallucinatory processes may be found in speech alterations, such as logorrhea,
because of the association between speech and content at all time points.
205
Elevated mood is connected with an increased motor activity and insight: although this
is not very informative during severe manic episode which is the case at t0 (because an
elevated mood is the core feature of mania), it informs the clinician that, when the patient
is stable (t2) a loss of insight (if not present before) or an increased energy may be the sign
of a rising mood: this finding is supported by recent literature (Silva et al., 2018).
It is not surprising that at t0 elevated mood is the most interconnected symptom in the
manic network. Because edges are not directed in the partial correlation networks, elevated
mood can be interpreted as the symptom that best predicts (or is predicted by) all other
symptoms in the network at t0. However, when patients becomes more stable, language-
thought disorder becomes the most predictable node in the network: this is likely due to
the strong connection that it shares with content, which also presents high estimates at t1
and t2. This phenomenon is described as “centrality corruption” (Briganti and Linkowski,
2019d): that is, because two nodes share one strong network connection, they rapidly become
important in the self-determination of the network. For this reason and because it shows a
high estimate when patients have a severe mental state, the connectivity of elevated mood at
t0 is more straightforward to interpret, as it shares connections with several nodes: elevated
mood can be considered as the core feature of mania in my sample of manic patients.
The NCT reported a statistically significant difference between the global strength of
networks at t0 and t2. This means that the network present a different connectivity at the
two time points: it is worthy of note that the networks compared by NCT are slightly different
than the ones estimated, because they have regularised partial correlation estimated with a
Pearson’s rho input. Although other comparisons between network structures are described
in this work, the results from NCT offer supplementary arguments in favor of a difference in
network structures on admittance and discharge.
Granger causal effects were explored in the temporal network. From a network point of
view, it is not surprising to see how elevated mood (which is supposed to be the direct reflec-
tion of the manic episode) has a temporal effect on many other manic symptoms; however,
206
in the temporal network, several other symptoms influence each other over time, therefore
supporting a complex system view of the concept of mania. However, temporal effects be-
tween variables seem to be much weaker than the temporal effects that each variables has
on itself.
The results of this work should be interpreted in light of three limitations. First, the
assumption of stationarity (the variables have the same mean and the same standard devi-
ation over time) is likely violated in my sample, because patients present high scores at t0
and low scores at t2: this leads to a less good model fit. Second, and for the same reason
regarding patients scores, Spearman’s ρ correlation was used instead of Pearson’s as an input
for the GGM because the distribution of the data is skewed. Third, although GVAR can be
estimated from three measurement occasions, it would be optimal to obtain a sample with
many more time points, and with more subjects to obtain more accurate estimates.
This study expanded the network theory of mental disorders to mania. Manic symptoms
were interconnected in a network structure, and specific associations between symptoms,
both static (cross-sectional) and dynamic (temporal) nature were explored, as well as the
importance of symptoms in the self-determination of the network. Future work may endeavor
to replicate my results in other population, as well as in patient with a less severe condition.
207
Part IV
Overcoming challenges in network
psychiatry
208
Chapter 13
Investigating the heterogeneity of
psychiatric symptomatology using
community detection algorithms
Abstract
This work aims to challenge current state-of-the-art practices to retrieve and in-
terpret the number of domains of psychiatric symptoms while modeling disorders as
networks by comparing the performances of different community detection algorithms
in a sample of 100 severe manic patients diagnosed with bipolar disorder type I at
three time points (at the start, middle and end of hospital stay). The performance
of three known algorithms (walktrap algorithm, spinglass algorithm and clique perco-
lation) are compared to retrieve different domains of mania in the sample, while the
bridge centrality measure is used to interpret the membership of symptoms to a given
community. The spinglass algorithm is the only algorithm able to retrieve the same
number of communities at all time points. The clique percolation algorithm is useful
to retrieve symptoms that connect multiple communities. I formulate the recommen-
dation to use the spinglass algorithm in addition to the more established walktrap
algorithm to study the number of communities.
209
13.1 Introduction
Uncovering the way symptoms and signs of mental illness co-occur in a given patient or
group of patients has always been a domain of interest in psychiatric research. In the past
decades, the fields of clinical psychiatry and psychiatric epidemiology have tried through
statistical tools to formalize theories around such interactions. This has allowed theoretical
and empirical works to move away from a categorical approach to mental disorder which
dominates currently used diagnostic manuals like the Diagnostic and Statistical Manual of
Mental Disorders (DSM) (American Psychiatric Association, 2013), and to embrace a more
dimensional approach. Such approach has been driven in the last decades by the widely
known common cause framework, which considers that psychiatric symptoms are caused by
a common cause, that is, the mental disorder itself.
Some psychiatric disorders, however, are known to be heterogeneous, that is, symptoms
may occur in specific subsets, and therefore, two patients with the same disorder may present
with different combinations of symptoms: this is for instance the case of depression (Fried and
Nesse, 2015). The subsets of co-occurring symptoms in data sets have been named factors
in the common cause literature using structural equation modeling as a statistical approach
(Kempenaers et al., 2017): the common cause (the disorder itself) causes factors, which in
turn cause the symptoms, which can therefore be understood as passive and interchangeable
consequences of the disorder, and does not actively contribute to it.
A decade ago, some put forward the hypothesis that one cannot identify a single cause
that, if eliminated, can make the clinical presentation of a psychiatric disorder entirely dis-
appear because there is no such cause; instead, psychiatric symptoms mutually cause each
other, and the psychiatric disorder arises from the set of interactions among such symp-
toms. This hypothesis, which translates the science of complex systems to medicine, has
been formally introduced as the network theory of mental disorders (Borsboom, 2017), and
has enjoyed an increasing popularity in the past years. Network theory is accompanied by
a set of statistical tools, called network analysis, which allows researchers to compute disor-
210
ders as a network of nodes (symptoms) that interact with each other through edges (which
represent conditional dependence relationships), often computed as partial correlations. A
series of psychiatric constructs and disorders have been studied using network analysis, such
as empathy (Briganti et al., 2018), self-worth (Briganti et al., 2019), resilience (Briganti and
Linkowski, 2019b), narcissism (Briganti and Linkowski, 2019a), alexithymia (Briganti and
Linkowski, 2019c), post-traumatic stress disorder (Fried et al., 2018), depression (Fried et al.,
2016) and autism (Deserno et al., 2017).
The network framework is interesting because it allows for the study of individual con-
nections among symptoms: network inference methods can put forward symptoms that are
more important than others in the self-determination of the network: in other terms, such
symptoms can better predict (or be predicted by) other symptoms in the network than oth-
ers, and can therefore be considered as prime candidates for clinical intervention (Fried et al.,
2017). Studying network structures is also interesting because they tend to replicate across
populations (Fried et al., 2018): it is therefore probable that a connection discovered between
two symptoms in a given data set may replicate in other data sets, and the more network
structures replicate, the more intervention studies can effectively tackle relevant symptoms.
The measure of network centrality (Boccaletti et al., 2006) disposes of several measures
to capture the relative or absolute importance of symptoms in the network. Widely used
centrality measures are strength, which is the absolute sum of connections of a given node (a
measure of relative importance because there will always be a more central node even though
the network is poorly connected), and node predictability, which is the shared variance (R2)
of a given node with surrounding nodes (an absolute measure of connectivity). One reported
problem with centrality measures is that if two symptoms present a very strong connection
to one another, although poorly connected to the rest of the network, they tend to receive
very high centrality estimates: this phenomenon, which has been referred to as centrality
corruption (Briganti and Linkowski, 2019d), occurs with symptoms that are redundant, that
is they tend to represent the same thing. However, redundancy should not be exclusively
211
understood as a negative property, because it is a way of showing how two or more symptoms
connect more closely to each other than to other symptoms in the network, and therefore
highly influence each other.
However, although the way a given symptom connects to the rest of symptoms in the
network is very important, it should be considered in parallel with the way that a given
symptoms connects to neighboring symptoms; that is, how symptoms cluster together in
communities, or domains (understood as factors from a common cause point of view). This
is particularly important in the case of redundant symptoms, because they tend to form
communities.
Community detection algorithms are a popular way to retrieve the number of communities
in networks (Briganti et al., 2018): for instance, exploratory graph analysis is an increasingly
used tool that has been shown to have high accuracy (Golino and Epskamp, 2017) and
applied in empirical papers (Briganti et al., 2018, 2019; Briganti and Linkowski, 2019b).
The exploratory graph analysis (EGA) relies on the walktrap algorithm, which is based
on the principle that adjacent nodes tend to belong to the same community (Yang et al.,
2016). For an optimal use of EGA, it is recommended that, once the number of communities
retrieved empirically, fitness of the model should be checked with a traditional confirmatory
factor analysis (CFA) (Golino and Demetriou, 2017), even more so if the model proposed by
the algorithm is somewhat different from the one that was expected. These guidelines were
followed and supported by some recent empirical works (Briganti et al., 2019; Briganti and
Linkowski, 2019b). However, two other community detection algorithms are optimized for
use in symptom network: the spinglass algorithm and clique percolation.
The spinglass algorithm is based on the principle that edges should connect nodes of the
same community, whereas nodes belonging to different communities should not be connected
(Yang et al., 2016).
Clique percolation is an algorithm recently adopted in the psychiatric network framework:
it considers the network as a set of k-cliques (communities), that are understood subsets
212
of k nodes that are fully connected (Palla et al., 2005). Clique percolation accepts two
communities as adjacent if they share k−1 nodes, which means nodes can belong to multiple
communities, therefore establishing a meaningful bridge between them.
The notion of bridge has mainly been analyzed in network settings when studying comor-
bidity (Jones et al., 2019). A set of statistics, grouped under the name bridge centrality have
therefore been developed to assess which network nodes better connect different communities
within the network; it is currently used in networks composed of symptoms from different
disorders to detect which symptoms connect different disorders.
Except from the guidelines proposed within the framework of EGA (Golino and Epskamp,
2017), there is to this date no standardized way to explore communities in network structures.
This is an important issue to address, since retrieving how symptoms closely cluster together
is crucial when choosing a target for therapeutic intervention in the framework of mental
disorders as complex systems. It is also important to correctly interpret the membership of
a given symptom to a given community (or multiple communities), and how it impacts the
way the symptom connects to other items in the network. If a network of symptoms from
the same mental disorder is divided into multiple communities, than it is plausible to assume
that if a patient presents a given symptoms, the patient will more likely present symptoms
that belong to the same community than symptoms that belong to other communities. This
is likely to greatly impact how the patient is treated, even more so in severe situations, such
a psychotic or manic episode.
Bridge centrality can be helpful as a measure to interpret the connectivity of a given
symptom while taking into account the presence of community: it is a much needed measure
that circumvents the problem of centrality corruption and can therefore provide an estimate
of how a symptom connects two different communities, that is, how the symptom brings
different parts of the network together: in clinical terms, how the symptom, if activated,
may cause many other symptoms in the network to co-occur. This phenomenon has been
described as hysteresis in the network approach (Borsboom and Cramer, 2013).
213
An additional point of interest which has not been studied in the network field is how
communities of symptoms evolve over time when treatment has been administered. This
is a research question that can be difficult to answer in disorders such as depression or
PTSD, but may be easier to tackle in disorders such as bipolar disorder: for instance, the
administration of neuroleptic, anxiolytic and soporific treatment in acute and severe mania
can have a radical and rapid effect on behavior, and may change how symptoms co-occur.
The aim of this work is to delve into the complicate issue of community detection in psy-
chiatric network and its interpretation. In this work, I will first compare the performances of
the walktrap algorithm, clique percolation and spinglass algorithm in detecting communities
in a sample of 100 severe manic inpatients in three time points – start, middle and end of
hospital stay; I will also estimate bridge centrality parameters and interpret the results in
light of symptom membership.
It is interesting to choose a sample of severe manic inpatients, because there has been
interest in the past years into the hypothesis that there exists several types of mania. Three
types of mania were for instance described by Hanwella et al. (Hanwella and de Silva,
2011): elated mania (with elements of elevated mood and sexual interest), irritable mania
(mainly driven by irritability and aggressive behavior), and psychotic mania (with psychotic
symptoms). It is therefore expected that manic symptoms in my sample will also cluster
into different communities, and it is plausible to expect that one of several symptoms may
switch communities over time.
This work is organized as follows: first, I will introduce the reader to the statistical
methods associated with community detection and bridge centrality in network structures.
Second, I will compare the performance of the three algorithms chosen in the case of my
sample of manic inpatients and estimate bridge centrality parameters; third, I will test the
fitness of the average model proposed by the different algorithms through confirmatory factor
analysis; fourth, I will discuss my results and their implication in clinical practice.
214
13.2 Method
13.2.1 Ethical approval
This study was approved from the Ethical Committee of the Brugmann Teaching Hospital
in Brussels (CHU Bruxelles Brugmann).
13.2.2 Data sets
Participants
My data set is composed of 100 patients, hospitalized in the context of an involuntary
commitment in a secure psychiatric unit. To be included in this study, patients needed to
be diagnosed with bipolar I disorder and to present with a manic episode at admission.
An abnormal blood or urine analysis in regards to toxicology as well as a concomitant
personality or somatic disorder that could account for the presence of manic symptoms were
considered as exclusion criteria. All patients were involuntarily committed for a period which
lasted for 40 days on average (following the Belgian law for involuntary commitment).
All manic patients were treated with a standard set of drugs following the local protocol
for manic patients: in the first stage of treatment (when the clinical presentation is severe),
an association of a typical and atypical antipsychotic drugs is administered, with a mood
stabilizer as well as soporific and anxiolytic drugs when necessary and depending on the
symptoms presented. In the second stage of treatment (when the clinical presentation is
stable), the patient is left with an atypical antipsychotic, a mood stabilizer, as well as a
soporific and/or anxiolytic when necessary.
Three time points were collected for each patient: on admission (t0), halfway through the
commitment period t1, and on discharge (t2). The data sets were anonymized by default.
Patients were 20 to 72 years old (M = 44.5, SD = 14.5); 47 of them were female, and 53 of
them were male.
215
Table 13.1: Symptoms from the Young Mania Rating Scales (Young et al., 1978)N symptom Symptom1 Elevated Mood2 Increased Motor Activity-Energy3 Sexual Interest4 Sleep5 Irritability6 Speech (Rate and Amount)7 Language-Thought Disorder8 Content9 Aggressive Behavior10 Appearance11 Insight
Measurement
The YMRS (Young et al., 1978) was used to assess manic symptoms, namely Elevated
Mood, Increased Motor Activity-Energy, Sexual Interest, Sleep, Irritability, Speech (Rate
and Amount), Language-Thought Disorder, Content, Aggressive Behavior, Appearance, and
Insight. Symptoms were scored 0 to 4, depending on the severity of the clinical presentation,
both at t0, t1 and t2. The symptoms are illustrated in table 13.1.
13.2.3 Network Analysis
Software
The software used for the analyses carried out in this study is R (version 3.6.3, available at
https://r-project.org). The packages needed for the analyses were bootnet (Epskamp
and Fried, 2018) and qgraph (Epskamp et al., 2012), igraph (Csardi and Nepusz, 2006)
and CliquePercolation for community detecton, networktools (Jones et al., 2019) and lavaan
Figure 13.1: Communities detected by the walktrap algorithm at t0 (left), t1 (middle) andt2 (right). Eleven communities of one symptom each were detected at t1. Each communityis denoted by a different color.
Clique Percolation
Figure 13.2 shows the networks at t0, t1, and t2 with the communities retrieved by Clique
Percolation. The first of the two biggest communities at t0 involve Language-Thought disor-
der, Content and Speech: this could be customarily defined as Psychotic mania; the second
includes Elevated Mood, Increased Motor Activity, Irritability and Aggressive Behavior,
which could be customarily called Exalted Mania. The third, smaller community involves
Appearance and Insight: this could be customarily called Careless Mania. Sleep belongs to
all three communities. At t1 only two communities emerge: although Psychotic Mania stays
mostly unchanged as a community, Careless Mania disappears and its symptoms join the
Exalted Mania cluster. At t2, one giant community emerges regrouping Exalted and Psy-
chotic Mania, while Sleep, Irritability and Increased Motor Activity and Sleep form however
a different community.
224
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Mood
Motor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
Mood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual InterestSleep: SleepIrrit: IrritabilitySpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentAggr: Aggressive BehaviorApp: AppearanceInsg: Insight
Figure 13.2: Communities detected by Clique Percolation at t0 (left), t1 (middle) and t2(right). Each community is denoted by a different color. Symptoms can belong to differentcommunities: they will therefore be denoted by multiple colors. If a node is white, then itconstitutes its own community.
225
Mood
Motor
Sexual
Sleep
Irrit
SpeechLgTAb
Cont
Aggr
App
Insg
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−Energy
BSexual: Sexual InterestIrrit: IrritabilityAggr: Aggressive Behavior
CSleep: SleepApp: AppearanceInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: Content
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−Energy
BSexual: Sexual InterestIrrit: IrritabilityAggr: Aggressive Behavior
CSleep: SleepApp: AppearanceInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: Content
MoodMotor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual Interest
BIrrit: IrritabilityAggr: Aggressive Behavior
CSleep: SleepApp: AppearanceInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: Content
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual Interest
BIrrit: IrritabilityAggr: Aggressive Behavior
CSleep: SleepApp: AppearanceInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: Content
MoodMotor
Sexual
Sleep
Irrit
Speech
LgTAb
Cont
Aggr
App
Insg
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual Interest
BSleep: SleepIrrit: Irritability
CAggr: Aggressive BehaviorInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentApp: Appearance
●
●
●
●
●
●
●
●
●
●
●
AMood: Elevated MoodMotor: Increased Motor Activity−EnergySexual: Sexual Interest
BSleep: SleepIrrit: Irritability
CAggr: Aggressive BehaviorInsg: Insight
DSpeech: Speech (Rate and Amount)LgTAb: Language−Thought DisorderCont: ContentApp: Appearance
At t0 At t1 At t2
Figure 13.3: Communities detected by the spinglass algorithm at t0 (left), t1 (middle) and t2(right). Each community is denoted by a different color. Symptoms can belong to differentcommunities: they will therefore be denoted by multiple colors.
The spinglass algorithm
Figure 13.3 shows the networks at t0, t1, and t2 with the communities retrieved by the
spinglass algorithm.
The results of community detection are fairly stable across the three time points. Four
communities are detected. The first relates to Exalted Mania and contains Elevated Mood,
Increased Motor Activity and Sexual Interest, except for t0 where the latter is included in the
second community, customarily defined as Irritable Mania with the symptoms Aggressive Be-
havior and Irritability. The third community relates to Careless Mania and includes Sleep,
Appearance and Insight The fourth community is Psychotic Mania and includes Speech,
Language-Thought Disorder and Content. Psychotic Mania contains the symptom Appear-
ance at t2.
226
Table 13.2: Symptom membership retrieved by the three algorithms at each time point.Symptom WalktrapT0 CliqueT0 SpinglassT0Mood 3 1 & 2 1Motor 3 1 1Sexual 1 NA 3Sleep 2 1 & 2 & 3 2Irritable 2 1 3Speech 4 3 4LgTtAbn 2 3 4Content 5 3 4Aggressive 1 1 3Appearance 3 2 2Insight 3 2 2
Table 13.3: Fit indices reported by CFA for the three time points: the Comparative FitIndex (CFI; should be higher than 0.95), the Root Mean Square Error of Approximation(RMSEA; should be lower than 0.06) and Standardized Root Mean Square Residual (SRMR;should be lower than 0.08).
Time Point CFI RMSEA SRMRt0 0.990 0.021 0.067t1 0.993 0.014 0.065t2 0.814 0.087 0.089
Table 13.4: Bridge centrality of manic symptoms at the three time points.Symptom T0 T1 T2Mood 0.536553547572247 0.71117320254293 1.39122331371955Motor 0.557759501813567 0.554662780688992 0.969490158197589Sexual 0.585202022768328 0.671285105896003 0.848914759652126Sleep 1.02399980413521 0.717178621701378 0.64818785130062Irritable 0.919669074419216 0.428980471315663 0.76748772793819Speech 0.454110034973616 0.699339618436966 0.707135221780921LgTtAbn 0.642989557041043 0.526637276371529 0.907471762302611Content 0.642647813143483 0.528031950690735 1.02242089051355Aggressive 0.371135439017514 0.167709813268731 0.782824607734004Appearance 0.594002911110612 0.747660398297268 0.569317636625077Insight 0.44246399256873 0.518188886854173 1.27973007896221
Confirmatory Factor Analysis for the overall mean model
I estimated fit indices for the following model, which is strongly inspired by the one re-
trieved by the spinglass algorithm and to which overall converged the models retrieved by
the walktrap algorithm and Clique Percolation: Exalted Mania, composed by Mood, In-
creased Motor Activity, and Sexual Interest; Irritable Mania, composed by Irritability and
Aggressive Behavior; Careless Mania composed of Sleep, Appearance and Insight; Psychotic
Mania composed of Speech, Language-Thought Disorder and Content. The fit indices are
reported in table 13.3.
Fit indices indicate that a model is a good fit at t0 and t1 but not at t2.
228
●
●
●
●
●
●
●
●
●
●
●
Bridge Strength
−1 0 1 2
Agg
Ins
Spc
Mod
Mtr
Sxl
App
Cnt
LTA
Irr
Slp
●
●
●
●
●
●
●
●
●
●
●
Bridge Strength
−2 −1 0 1
Agg
Irr
Ins
LTA
Cnt
Mtr
Sxl
Spc
Mod
Slp
App
●
●
●
●
●
●
●
●
●
●
●
Bridge Strength
−1 0 1 2
App
Slp
Spc
Irr
Agg
Sxl
LTA
Mtr
Cnt
Ins
Mod
At t0 At t1
At t2
Figure 13.4: Bridge centrality estimates for the eleven manic symptoms at t0 (top left), t1(top right), and t2 (bottom).
13.3.2 Bridge centrality
Table 13.4 and figure 13.4 report the bridge centrality estimates for the eleven manic symp-
toms at t0, t1, and t2. At t0, Sleep is the most interconnected symptom, and it stays inter-
connected at t1, before becoming one of the poorly connected symptoms at t2. Appearance
is the most interconnected symptom at t1, and Mood at t2.
13.4 Discussion
This work tackled the important topic related to the study of the heterogeneity of psychi-
atric symptomatology using community detection algorithms within the network analysis
framework for mental disorders. I aimed to compare the performances of well-known com-
munity detection algorithms, as well as provide a possible solution to the phenomenon of
redundancy and centrality corruption among network symptoms. The conceptual framework
229
of community detection under examination in this work has important clinical implications
that I will also discuss in this section.
It is worth commenting on the choice of my study settings to contextualize the discussion
of the performance of the community detection algorithms itself. First, I deliberately chose
to compare the performance of community detection algorithms in a setting characterized
by a clinical sample of 100 patients and with a relatively small network of eleven symptoms,
because it is one of the most common settings in clinical research: this is important because
most of the network methodology was initially conceived for relatively big networks and for
relatively big samples. Second, the chosen data set is composed of severe manic patients
diagnosed with bipolar I disorder at three relatively relevant time points: on admission
(t0) and on discharge (t2), the data set likely presents a ceiling and floor effect –that is,
symptoms score very high on average at t0 (because patients are affected with severe mania)
and very low on average at t2 (because patients are treated and have present on average with
an improved mental examination); the low variability in the data set that comes with the
ceiling or floor effect is the reason why Spearman ρ was used instead of Pearson’s correlation
coefficient (Briganti et al., 2019). These are important parameters to take into account when
both developing or validating methods for network psychiatry and applying them in empirical
studies, because they are likely present in many data sets that deal with patients in clinical
settings: when admitted, symptoms are usually high, and are therefore likely to reinforce
each other: in network terms, their connection is stronger and they better predict each
other. The same happens when discharging patients, since their symptoms are either mild
or absent, but there is no reinforcement on a clinical basis, because although the connection
is strong, it is justified by a conditional dependence between variables that are lowly scored:
it is therefore crucial to take the data into account when interpreting connections among
symptoms in a network. Between admission and discharge (t1), however, there is a time
frame where certain symptoms are on the way to recovery because a psychiatric treatment
is effectively acting on those specific symptoms, and others are still unchanged because they
230
are either poorly connected, or because there has not been enough time for the effect to
disseminate to such entities; from a network point of view, this translates to an overall
desynchronized network at t1 (because symptoms present with very different scores)1.
The latter point greatly influences how community detection algorithms work, and in par-
ticular the performance of the walktrap algorithm and Clique Percolation, since the strength
of connections greatly impacts the determination of symptom membership in both of them.
It is likely to partially explain why the walktrap algorithm detects eleven communities of one
symptom each (and therefore no community at all) at t1. The same does not however happen
with Clique Percolation, although the low connectivity may influence the appearance of two
bigger communities instead of the three detected at the first time point where connectivity
is higher.
One of the main interest in using Clique Percolation lies in an exploratory approach to
detect symptoms that connect multiples communities, as a basis for an inference using bridge
centrality. However, its use and outcomes heavily rely on the choice of the two parameters
k and I which can vary. For instance, an optimal I was not retrieved for t1 and t2, and
therefore suboptimal thresholds had to be chosen.
The spinglass algorithm is the only algorithm able to retrieve the same number of com-
munities, with an overall stable symptom membership at all time points. Although running
the spinglass algorithm a limited number of times can lead to obtaining different community
memberships, it has been reported that retrieving the communities with highest frequency
over several runs leads to a certain stability of the results (Briganti et al., 2018). Such sta-
bility is likely influenced by the straightforwardness of the spinglass function that rewards
or penalizes the presence of edges within and between communities and focuses less on the
strength of edges: this is important because, when considering the principle of hysteresis
(Borsboom and Cramer, 2013) in the network theory of mental disorders 2, although the
1The difference in the overall connectivity of the network at the three time points was explored in aseparate paper (Briganti et al., 2020a). The overall connectivity is statistically different at t0 and t2.
2Hysteresis: symptoms stay connected over time but the strength of connection can vary if the patient iswell, (poorly connected in the case of this work), or unwell (strongly connected in the case of this work).
231
connectedness may vary, the network structure (and its partition into communities) is sup-
posed to remain unchanged, since symptoms are likely to be related by their nature (Kendler
et al., 2011). Therefore, although initially poorly introduced in the psychiatric network field,
I recommend the use of the spinglass algorithm as a complementary tool to the more es-
tablished walktrap algorithm to detect communities in network structures because of its
reliability and ease of use (since the algorithm does not depend like Clique Percolation on
the determination of optimal parameters).
It is also crucial to check for model fitness with CFA. Although CFA conceptually implies
a model where symptoms do not form a complex system but are instead a consequence of
a latent variable, it is plausible to interpret symptoms that are highly associated within the
same community as highly predictive of each other, because they convey a similar clinical
meaning. For instance, it is not surprising that Aggressive Behavior and Irritability are con-
nected at all three time points and form a community, since they can easily be interpreted
to clinically represent similar aspects of mania: this reason justifies the act of validating the
model found through exploratory community detection with CFA (Golino and Epskamp,
2017). However, validating through CFA the model retrieved does not necessarily mean
applying a reductionist view onto the model itself: the complex systems approach to mental
disorder implies that, if a network is more than the sum of its communities, than the com-
munity is more than the sum of its symptoms: within the community, there are symptoms
that interact with the neighboring network in different ways, and therefore contribute in
different ways to the emergence of the network and the heterogeneous nature of the clinical
presentation in psychiatric disorder; this means that one cannot reduce a network to a set
of communities either. From a probabilistic view, for instance, it is plausible to assume that
there exist sub-clinical entities within the manic presentation, such as the four communities
belonging to the overall recurring model retrieved in the present analysis (Exalted, Irritable,
Careless and Psychotic) that lead to different clinical presentation in patients, but all com-
munities within a network interact together through specific symptoms, and this is likely to
232
further increase the clinical heterogeneity.
From this perspective, bridge centrality is a good way forward to measure how commu-
nities interact together and which symptoms are the main responsible for such interactions.
Although initially introduced to tackle comorbidity in networks composed of symptoms from
different disorders (Jones et al., 2019), I showed how bridge centrality can be a very inter-
esting approach in networks of symptoms from one mental disorder that is susceptible of
be heterogeneous (that is most if not all mental disorders). My findings further show how
Clique Percolation and bridge centrality work well together and are complementary: Clique
Percolation reports which communities the interconnected item belongs to, and bridge cen-
trality quantifies the interaction itself among the different communities. For instance, Sleep
is identified to be the most interconnected network with both analyses: the former shows how
sleep disorders are symptoms that belong to multiple communities, and the latter reports
how they connect the multiple communities they belong to.
From a clinical point of view, symptoms that belong to different communities can be
considered as prime candidates when choosing a target for an intervention: because bridge
symptoms are predictive of symptoms in different communities, the effect of clinical interven-
tion on bridge symptoms is likely to greatly affect the overall clinical presentation by affecting
multiples communities. This is the case of Sleep, and its connectedness in my study justifies
further studies that explore it as a risk factor in bipolar disorder the (la Cour Karottki et al.,
2020).
The results of this work should be interpreted in light of a number of limitation. I hereby
describe three. First, my data set is composed of 100 patients over three time points: this
is likely to limit the replication of my results in other samples. Second, although symptoms
that are connected in a GGM can be interpreted to be highly predictive of one another,
I do not know whether there is a directed causal effect among symptoms: for instance, a
symptom with high bridge centrality score and belonging to different communities (such as
Sleep) could in fact be the common effect of different variables. Third the methodological
233
world of network analysis is based on software that is rapidly evolving: the computation
could be further optimised in the future, and this may slightly change the results retrieved.
Community detection is an important tool when addressing the heterogeneity of mental
disorders: the study of how symptoms co-occur and cluster together can lead to a better
theoretical and clinical framework for the definition and treatment of psychiatric illness.
234
Chapter 14
Discussion
In each chapter of this dissertation, I introduced improvements on the way psychiatric en-
tities are analyzed as networks. This work heavily relied on the use of Bayesian Artificial
Intelligence to uncover the underlying causal structure in the symptom data sets, which is
a new and interesting advance in the medical sciences that will help clinicians better pre-
vent, diagnose and treat mental disorders. The works in this dissertation therefore have
two scopes: first, to have a meaningful clinical impact through expanding the knowledge
of psychiatric entities while studying them as complex systems; second, to introduce and
discuss improvements of existing methods to reach such meaningful clinical impact.In this
discussion, I will detail how those aims were reached.
The first part of works constituting this dissertation is composed of the analyses of
psychiatric constructs of high clinical importance.
First, I analyzed empathy, which is a crucial construct in psychiatry, since its absence is
associated with several disorders, and I used the network approach to explore the connec-
tivity of empathy components such as they are represented in the Interpersonal Reactivity
Index (Briganti et al., 2018). I wanted to recover if some components of empathy are more
important than others, since several models put the affective components of empathy on top
of the others. This hypothesis was supported in my findings, since the affective component
235
of empathy was more important in the self-determination of the empathy network than other
components. In this paper, I showed how network methods for recovering the underlying
clustering structure of a data set are as effective as more established methods such as factor
analysis, while keeping a complex system view to the construct at hand. I also proposed
a way to interpret the connections among components of a psychiatric construct (that is,
two traits predict each other in the observed group and could therefore predict each other
in the individual), which could be interpreted to be fundamentally different from symptoms.
The most important caveat I observed in analyzing a full psychometric scale of a psychiatric
construct as a network is that traits from the same community tend to resemble each other
and are therefore redundant: it is therefore more difficult to infer from the network structure
with many redundant variables.
Second, I analyzed the construct of self-worth: I proposed a way forward for analyzing
constructs from psychometric scales such as analyzing domains instead of items (Briganti
et al., 2019). A domain is understood a community or cluster of items (and therefore is
defined with a data-driven method such a community detection algorithm). I found that
several domains of self-worth, including the self-worth drawn from religious beliefs, can be
unconnected, and therefore self-worth itself can be a very heterogeneous construct. This is
an important added value of analyzing domains, since the complex view allows for demon-
strating how theoretically uniform psychiatric entities can in fact be heterogenous: on an
interpersonal level, this can be interpreted as the possibility for different individuals to ex-
hibit different parts of a same psychiatric entity (a construct or a mental disorder).
Third, I analyzed resilience, an important psychiatric construct at the heart of therapy
outcomes (Briganti and Linkowski, 2019b): the psychometric tool at hand having had mul-
tiple revisions regarding the domain structure of the scale, it was an interesting opportunity
to test whether domains themselves can be redundant : that is why I adopted a data-driven
method to compare to choose a more parsimonious domain subdivision and test whether
using conventional factor analysis method such subdivision is a better fit for the data.
236
Fourth, I studied narcissistic personality, a topic of ever-growing interest in psychiatric
research. I performed a network analysis to detect which components of narcissistic person-
ality were the most important: entitlement, authority and superiority were found to be the
most contributing components to narcissistic personality. In this work I heavily relied on the
use of centrality measures (Briganti and Linkowski, 2019a) to infer the relative importance
of components and discussed their use.
Fifth, I tackled the important construct of alexithymia as represented in the two most
widely used measures, the Toronto Alexithymia Scale (which does not include the component
of fantasizing) and the Bermond-Vorst Alexithymia Questionnaire (which includes fantasiz-
ing) using both frequentist and Bayesian approaches (Briganti and Linkowski, 2019c). In
both constructs, the difficulty describing feelings was found to be the most important com-
ponent of the construct. These findings greatly contribute to support the fact that inference
from network structures is highly replicable across samples and different psychometric tools
(Fried et al., 2018). In the latter of the two alexithymia papers, I used centrality measures
to tackle the issue of redundancy and choose the most important item in each domain before
constructing a network structure: this is an additional method that can be used in large
scales to avoid having to interpret too many nodes.
Sixth, I used the Bayesian approach to Gaussian Graphical Models to investigate autistic
traits. Traits related to social skills are the most interconnected items in the network.
Sex differences were found between female and male subjects: using Bayesian methods to
estimate network structures lead to an easier interpretation of results, mainly because of
tools such as Bayesian factors that allow the researcher to dispose of supporting evidence for
a given parameter.
The second part of works composing this dissertation tackles the domain of affective
disorders in both a healthy sample and a sample of severe inpatients.
The construct of depressive symptoms such as represented in the Zung Depression Scale
was analyzed through the lenses of both undirected and directed network using both fre-
237
quentist and Bayesian approaches (Briganti et al., 2020b). Lack of focus was identified to
be the most interconnected symptom in the depression network in a healthy sample. In this
work I introduced the comparison between frequentist and Bayesian methods in the case of
network structures. Although stemming from different concepts, the two methods can be
combined in order to study different aspects of a mental disorder: the frequentist approach
is better suited to study the connectivity among symptoms, while the Bayesian approach is
better suited for (causal) inference.
In a sample of severe manic patients, I analyzed the connectivity of manic symptoms in
three time points (start, middle and end of hospital stay) during a psychiatric commitment.
Elevated mood was identified to be the most interconnected symptoms at the three time
points. I also estimated the network of temporal effects (Granger-causal effects), where
Elevated Mood emerged as an item causing many other symptoms over time. I used the
optimised Graphical Vector Autoregressive Model for panel data to infer the temporal effects
among manic symptoms.
In the last part, I proposed a methodological way forward for the important problem
of community detection in networks –a crucial way of addressing the heterogeneity of psy-
chiatric symptomatology. This methodological work stems from the previous works of the
dissertation and answers the relevant clinical question of identifying sub-types of disorders
(e.g. a manic patient may present with only a subset of symptoms and still be considered
a manic patients), and this particular complex view of the mental disorder challenges cur-
rent psychiatric diagnosis, which is based on summing the presence of several categories of
symptoms.
14.1 Future directions
I formulate the following recommendation for the future studies of psychiatric entities as
networks. Although sometimes too technical (Fried, 2020), cross-sectional reports of net-
238
work structures are useful to expand the current knowledge of psychiatric entities which
is necessary to build better models (Robinaugh et al., 2019). Cross-sectional networks of
observed groups are therefore the preferable way of studying the connection in a population
before trying to address the individual. To support the study of temporal data (to answer
the question which symptom influences which symptom over time), however, we need more
established models that stem from existing and widely used psychometric tools for clinical
practice.
It is however in the individual patient that lie the most promising advances of network
psychiatry: with temporal data (obtained either at the bedside or in between consultations)
psychiatrists will be able to monitor the evolution of individual symptoms and how they
affect others over time. The efficacy of identifying targets for clinical intervention will in the
future have to be tested with clinical trials. This will serve as a fundamental basis to achieve
what is called precision psychiatry –that is, optimize the right treatment for the right patient
based on a series of parameters, including its dynamic symptomatology.
14.2 Conclusion
Inspired by the ever-growing development of network psychometrics in the scientific liter-
ature, this dissertation aimed to translate and optimize the use of a selected number of
methods in complex systems and Bayesian Artificial Intelligence proposed by the network
approach to a number of mental constructs and disorders relevant to psychiatric practice.
It is worthy of note that my reports of network structures of the constructs and disorders
were realised using validated tools that are widely used in clinical practice, and were the first
to be studied as network structures in the literature. First, I introduced the methods that
the reader needs to understand this dissertation; second, I studied psychiatric constructs
(psychiatric entities that are not defined as mental disorders) as networks; third, I studied
unipolar depression and mania as network structures; fourth, I introduced a way forward for
239
the study of communities in networks by comparing the rationale and the performance of
several community-detection algorithm on a clinical sample.
Network psychiatry is a promising field that will be able to translate fundamental re-
search that aims to better understand mental disorders to clinical practice: its complex
view on mental disorders will in the future be able to integrate the study of symptoms with
other important variables, such as genes, neuroanatomy and environmental factors to achieve
precision psychiatry.
240
Bibliography
Aburn, G., Gott, M., and Hoare, K. (2016). What is resilience? An Integrative Review of
the empirical literature. Journal of Advanced Nursing, 72(5):980–1000.
Ackerman, R. A., Witt, E. A., Donnellan, M. B., Trzesniewski, K. H., Robins, R. W., and
Kashy, D. A. (2011). What does the narcissistic personality inventory really measure?
Assessment, 18(1):67–87.
Allison, C., Auyeung, B., and Baron-Cohen, S. (2012). Toward brief “red flags” for autism
screening: the short autism spectrum quotient and the short quantitative checklist in
1,000 cases and 3,000 controls. Journal of the American Academy of Child & Adolescent
Psychiatry, 51(2):202–212.
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Dis-
orders. American Psychiatric Association, fifth edition.
Angst, J. and Marneros, A. (2001). Bipolarity from ancient to modern times:: conception,
birth and rebirth. Journal of affective disorders, 67(1-3):3–19.
Armour, C., Fried, E. I., Deserno, M. K., Tsai, J., and Pietrzak, R. H. (2017). A network
analysis of DSM-5 posttraumatic stress disorder symptoms and correlates in U.S. military
veterans. Journal of Anxiety Disorders, 45:49–59.
Bagby, R. M., Parker, J. D. A., and Taylor, G. J. (1994). The twenty-item Toronto Alex-
241
ithymia scale—I. Item selection and cross-validation of the factor structure. Journal of
Psychosomatic Research, 38(1):23–32.
Baron-Cohen, S. (2010). Progress in brain research: Sex differences in the human brain,
their underpinnings and implications. Progress in Brain Research, 186:167–175.