j ourna l homepage: www.e lsev ie r.com/ locate /schres
Neural markers of remission in first-episode schizophrenia: A volumetricneuroimaging study of the hippocampus and amygdala
Michael Bodnar a,b, Ashok K. Malla b, Yvonne Czechowska b, Audrey Benoit a,b, Ferid Fathalli a,Ridha Joober a,b, Marita Pruessner b, Jens Pruessner a, Martin Lepage a,b,⁎a Brain Imaging Group, Douglas Mental Health University Institute, Montreal, Canadab Prevention and Early Intervention Program for Psychoses (PEPP-Montreal), Douglas Mental Health University Institute, Montreal, Canada
a r t i c l e i n f o
Abbreviation: FES, first-episode schizophrenia.⁎ Corresponding author. Douglas Mental Health Uni
B Common Pavilion, F1143, 6875 LaSalle Blvd., Verdun1R3. Tel.: +1 514 761 6131x4393; fax: +1 514 888 4
Article history:Received 8 March 2010Received in revised form 11 June 2010Accepted 18 June 2010Available online 13 July 2010
Objective: The temporolimbic region has been implicated in the pathophysiology inschizophrenia. More specifically, significantly smaller hippocampal volumes but not amygdalavolumes have been identified at onset in first-episode schizophrenia (FES) patients. However,volumetric differences (namely, in the hippocampus) exhibit an ambiguous relationship withlong-term outcome. So, we examined the relationship between hippocampus and amygdalavolumes and early remission status.Methods: We compared hippocampus and amygdala volumes between 40 non-remitted and 17remitted FES patients and 57 healthy controls. Amygdala and hippocampusweremanually tracedwith the hippocampus additionally segmented into three parts: body, head, and tail. Remissionwas defined asmild or less on both positive and negative symptoms over a period of 6 consecutivemonths as per the 2005 Remission in Schizophrenia Working Group criteria.Results: A significant [group×structure×side] interaction revealed outcome groups differed inhippocampus tail volumes; significantly on the left (non-remitted=694±175 mm3;remitted=855±133 mm3; p=0.001) with a trend difference on the right (non-remitted=723±162 mm3; remitted=833±126 mm3; p=0.023). Groups did not differ in body, head, oramygdala volumes bi-laterally.Conclusions: A smaller hippocampal tail volume may represent a neural marker in FES patientswhodonot achieve early remission after thefirst 6 months of treatment. The early identificationofpatients with poor outcome with respect to the hippocampus tail may encourage the search fornew, more target-specific, medications in hope of improving outcome and moving us towards abetter understanding of the pathophysiology of schizophrenia.
Meta-analyses have confirmed that significantly smallerhippocampal volumes but not amygdala volumes are observedat the onset of illness in first-episode schizophrenia (FES)patients compared to controls (Steen et al., 2006; Vita and dePeri, 2007; Vita et al., 2006). As such, different patterns ofinvolvement for temporolimbic structures are apparent inschizophrenia (Vita and de Peri, 2007) that may be neurode-velopmental or neurodegenerative or both (Harrison, 2004). Infact, the hippocampus has been recognized as an importantbrain structure in thepathophysiologyof schizophrenia throughstructural and functional neuroimaging, neuropsychological,
73M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
and neurochemical studies (Harrison, 2004). With such a closerelationship to schizophrenia, it is equally important tounderstand how the hippocampus relates to such importantaspects of schizophrenia such as functional outcome, remission,and recovery.
Focusing on structural neuroimaging in FES, severalstudies, for example, have investigated the relationshipbetween neuroimaging volumes and outcome (Ho et al.,2003; Lieberman et al., 2001; Robinson et al., 2004; Wobrocket al., 2009). However, only two studies have directlycompared outcome groups in hippocampus volume. In onestudy, Lieberman et al., 2001 compared 34 poor outcome and64 good outcome FES patients. Poor outcome was defined ashaving persistent symptoms from the first-episode orsubsequent relapses that occurred during the follow-upperiod and scan interval that did not remit with treatment.Hippocampus and amygdala were manually delineated asone structure because no clear border could be visualizedbetween the structures on the 1.0 Tesla scans. At time 1(baseline) and time 2 (2.5 years later), poor and goodoutcome groups did not significantly differ in amygdala–hippocampus complex volume. In the other study, Wobrocket al., 2009 compared 11 poor outcome and 12 stable (good)outcome FES patients. Poor outcome was defined as anincrease of PANSS total score above 40% of baseline score(approximately 20 points). More importantly, they manuallydelineated the hippocampus separate from the amygdalausing 1.5 T scans. However, they also found that poor andgood outcome patients did not significantly differ in hippo-campus volumes bi-laterally. These results suggest thathippocampus volumes do not significantly differ betweengood and poor outcome FES patients.
However, the hippocampus is a complex structure thatcan be divided into two (posterior and anterior) or three(head, body, and tail) subregions (Konrad et al., 2009) thatare believed to be functionally different based on previousfindings. Briefly, the hippocampus head bi-laterally has beenrelated to verbal memory performance while the body andtail were not in healthy controls (Hackert et al., 2002).Moreover, the anterior subregion has been associated withmemory deficits in people with schizophrenia (Szeszko et al.,2002) and their first-degree relatives (O'Driscoll et al., 2001);the left posterior hippocampus has been related to negativesymptomology in schizophrenia (Rajarethinam et al., 2001)as well as to verbal memory in healthy controls and in peoplewith mild-cognitive impairment (Schmidt-Wilcke et al.,2009). Additionally, the Moser theory postulated the poste-rior hippocampus to be involved in memory functions whilethe anterior hippocampus more involved with emotionalmodulation and affective processes (Moser andMoser, 1998).Finally, regarding connectivity, the anterior hippocampus isprimarily connected with the medial entorhinal cortex andthe medial prefrontal cortex whereas the posterior region isprimarily connected with the lateral entorhinal cortex andthe dorsolateral aspects of the prefrontal cortex (Barbas andBlatt, 1995; Goldman-Rakic et al., 1984; Witter et al., 2000).With the abovementioned regions related to different brainfunctions, the differing connections to the hippocampalsubregions may represent distinct subregional functions.However, the exact functions of each subregion are not yetfully understood but do appear to be different.
At any rate, relative to controls, smaller volumes havebeen found in the posterior subregion in FES patients(Hirayasu et al., 1998; Narr et al., 2004; Witthaus et al.,2010) and younger aged people with schizophrenia (Beckeret al., 1996; Rametti et al., 2007) as well as in the anteriorsubregion in FES patients (Narr et al., 2004; Szeszko et al.,2003; Verma et al., 2009). Thus, subregional differences areapparent in FES patients but findings are not convergent.With no significant differences found in whole hippocampusvolumes between clinical outcome groups in FES patients,subregional differences may exist.
We set out to investigate volumetric differences insubregions of the hippocampus between remitted and non-remitted FES patients. We included the amygdala in ouranalysis because a previous FES outcome study included it aspart of an anterior hippocampus structure investigated(Lieberman et al., 2001). Remission was defined followingthe proposed Remission in Schizophrenia Working Group(RSWG) criteria (mild or less on 8 key symptoms maintainedfor 6 consecutive months) (Andreasen et al., 2005). As thefirst study, to the best of our knowledge, to investigatevolumetric differences in hippocampus subregions andamygdala between remitted and non-remitted FES patients,we could not speculate if or which structure or subregionwould show a significant difference between outcomegroups.
2. Materials and methods
2.1. Participants and treatment setting
All patients were recruited and treated through thePrevention and Early Intervention Program for Psychoses(PEPP-Montreal), a specialized early intervention service withintegrated clinical, research, and teaching modules, at theDouglasMental Health University Institute inMontreal, Canada.People aged 15 to 30 years from the local catchment areasuffering from either affective or non-affective psychosis whohad not taken antipsychotic medication for more than onemonthwith aminimum IQof 70were consecutively admitted tothe program as either in- or out-patients. For complete programdetails seeMalla et al., 2003or http://www.douglas.qc.ca/pages/view?section_id=165. Of those treated at PEPP, only patientsaged 18 to 30with no previous history of neurological disease orhead trauma causing loss of consciousness were eligible for theneuroimaging study; only those suffering from schizophreniaspectrum disorders were considered for this analysis.
In all, 57 FES patients were subsequently separated intotwo groups: remitted (n=17, 29.8%) and non-remitted(n=40, 70.2%). Remission was defined as mild or less on8 key symptoms [delusions, unusual thought content,hallucinatory behavior, conceptual disorganization, manner-isms and posturing, blunted affect, passive or apathetic socialwithdrawal, and lack of spontaneity and flow of conversation]maintained for 6 consecutive months (month 6 to month 12,in our case) as per the RSWG consensus definition (Andrea-sen et al., 2005). All patients met DSM-IV criteria forschizophrenia (remitted=13; non-remitted=31), schizoaf-fective (remitted=3; non-remitted=9), or schizophreni-form (remitted=1) diagnoses according to the StructuredClinical Interview for DSM-IV (First et al., 1998). Diagnoses
74 M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
were confirmed between two senior research psychiatrists(A.M. and R.J.).
Fifty-seven healthy controls were recruited throughadvertisements in local newspapers. Controls were includedonly if they had no current or past history of 1) any Axis Idisorders, 2) any neurological diseases, 3) head traumacausing loss of consciousness, and 4) a first-degree familymember suffering from schizophrenia or related schizophre-nia spectrum psychosis.
After a comprehensive description of the study, writteninformed consent was obtained from all participants. Re-search protocols were approved by the McGill UniversityFaculty of Medicine review board.
2.2. Data collection
2.2.1. Symptom, medication, and socio-demographic dataAs per PEPP protocol, the following data were obtained at
each interview session conducted at baseline, months 1, 2, 3,6, 9, and 12. Positive and negative symptoms were assessedusing the Positive and Negative Syndrome Scale (PANSS)(Kay et al., 1987); raters have established an ICC of 0.75 onthis scale. The type and dosage of antipsychotic taken wererecorded and subsequently converted into chlorpromazineequivalents (Jensen and Regier, 2010; Woods, 2003). Medi-cation adherence, based on a 5-point scale ranging from 0(never) to 4 (fully), was obtained from patients or, whenpossible, from family members. At baseline, parental SES wasmeasured with the Hollingshead two-factor index (Hollings-head, 1965) and handedness with the Edinburgh HandednessInventory (Oldfield, 1971).
2.2.2. Scanning procedure and MRI data acquisitionScanning was carried out at the Montreal Neurological
Institute (MNI) on a 1.5 TSiemens whole body MRI system.Structural T1 volumeswere acquired for each participant usinga three-dimensional (3D) gradient echo pulse sequence withsagittal volume excitation (repetition time=22 ms, echotime=9.2 ms, flip angle=30°, 180 1 mm contiguous sagittalslices). The rectangular field-of-view for the images was256 mm (SI)×204 mm (AP). Patient groups did not differ asto when sessions took place past entry (non-remittedmean=17.9±7.6 weeks; remitted mean=20.4±8.2 weeks;and t=−1.11, df=55, p=0.27).
2.3. MR image analysis
2.3.1. Automated MR image preprocessingAll images were transferred to a Macintosh workstation
(Apple Computer, Cupertino, Ca, USA). A combination ofdifferent algorithms was used to prepare the rawMRI volumesfor manual segmentation. This process corrected for imageintensity non-uniformities (Sled et al., 1998), linear stereotaxictransformation (Collins et al., 1994) intoMNI coordinates basedon the Talairach atlas (Talairach and Tournoux, 1988) andresampling onto a 1 mm voxel grid prior to image segmenta-tion using a linear interpolation kernel. It has been shown thatthe automatic stereotaxic transformation is as accurate as themanual procedure, but shows higher stability (Collins et al.,1994). Also, the correction for image intensity has been provento recovermost of the artifacts present in rawMRI data (Sled et
al., 1998). Finally, signal-intensity normalization was per-formed across all subjects in the study to adjust individualsignal range and render the contrast between subjectscomparable.
2.3.2. Manual tracing of hippocampus and amygdalaThe amygdala and hippocampus were traced following a
validated protocol developed by Dr Jens Pruessner (Pruessneret al., 2000). A recent update to this protocol by Dr J Pruessnerin 2006 allows to accurately and consistently subdivide thehippocampus into three different subregions: head, body, andtail.
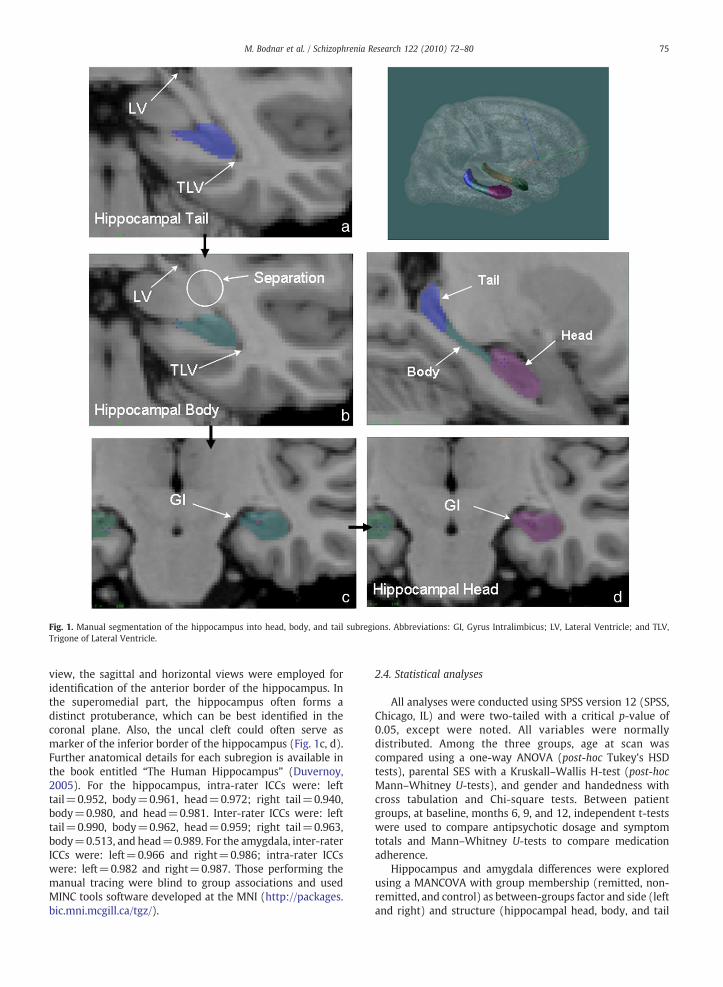
The following guidelines for hippocampal segmentationwere used: themost posterior part of the hippocampus tail wasdefined as the first appearance of ovoid mass of gray matterinferiomedial to the trigone of the lateral ventricle (TLV). Thelateral border of the hippocampus tail at this pointwas the TLV,whereas medially, the border of the hippocampus wasidentified bywhitematter. Further anterior, an arbitrary borderwas defined for the superior and medial border of thehippocampus, in order to differentiate hippocampus graymatter from the gray matter of the Andreas Retzius gyrus, theFasciolar gyrus, and the crus of the fornix (cfx). This border wasemployed by drawing a vertical line from themedial end of theTLV inferiorly to the parahippocampal gyrus, and a horizontalline from the superior border of the quadrogeminal cistern tothe TLV. The inferior border of the hippocampus at this point isagain identified by white matter. Moving further anterior fromthe hippocampus tail, the slice where the TLV separatescompletely from the lateral ventricle (LV) is the first slice ofthe hippocampus body (Fig. 1a, b). While the landmark forseparating hippocampus tail from hippocampus body isexternal to the structure itself, it has been found to be a veryconsistent approach across subjects and groups as it seemsrobust in the presence of neurodegeneration. That is, even if thehippocampus is reduced in volume, or the ventricles areenlarged, the separation of the TLV from the LV is occurring atthe same anterior–posterior extent.
For the hippocampus body, the most visible inferiolaterallayer of gray matter was excluded, assuming that it actuallyrepresents entorhinal cortex. Next, the white matter band atthe superomedial level of the hippocampus body, the fimbria,was included. If gray matter was found superior to the fimbria,the first row of gray matter was also included. The dentategyrus, located in between the four CA regions in thehippocampal formation, together with the CA regions them-selves and the subiculum were included. The subiculum wasdivided by drawing a straight line with an angle of approxi-mately 45° from the most inferior part of the hippocampusmedially to the cistern if no white matter delineation wasvisible between these two structures. The lateral border at thispointwas identified by the inferior horn of the LV. If the inferiorhorn was invisible, the caudally adjacent white matter wasemployed. The quadrogeminal cistern defined the super-omedial border of the hippocampus.
The appearance of the hippocampus head was defined bythe emergence of the gyrus intralimbicus in the superomedialregion of the hippocampus. Themost important structures foridentification of lateral, anterior and superior borders of thehippocampus head were the uncal recess of the inferior hornof the lateral ventricle and the alveus. Besides the coronal
Fig. 1. Manual segmentation of the hippocampus into head, body, and tail subregions. Abbreviations: GI, Gyrus Intralimbicus; LV, Lateral Ventricle; and TLV,Trigone of Lateral Ventricle.
75M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
view, the sagittal and horizontal views were employed foridentification of the anterior border of the hippocampus. Inthe superomedial part, the hippocampus often forms adistinct protuberance, which can be best identified in thecoronal plane. Also, the uncal cleft could often serve asmarker of the inferior border of the hippocampus (Fig. 1c, d).Further anatomical details for each subregion is available inthe book entitled “The Human Hippocampus” (Duvernoy,2005). For the hippocampus, intra-rater ICCs were: lefttail=0.952, body=0.961, head=0.972; right tail=0.940,body=0.980, and head=0.981. Inter-rater ICCs were: lefttail=0.990, body=0.962, head=0.959; right tail=0.963,body=0.513, and head=0.989. For the amygdala, inter-raterICCs were: left=0.966 and right=0.986; intra-rater ICCswere: left=0.982 and right=0.987. Those performing themanual tracing were blind to group associations and usedMINC tools software developed at the MNI (http://packages.bic.mni.mcgill.ca/tgz/).
2.4. Statistical analyses
All analyses were conducted using SPSS version 12 (SPSS,Chicago, IL) and were two-tailed with a critical p-value of0.05, except were noted. All variables were normallydistributed. Among the three groups, age at scan wascompared using a one-way ANOVA (post-hoc Tukey's HSDtests), parental SES with a Kruskall–Wallis H-test (post-hocMann–Whitney U-tests), and gender and handedness withcross tabulation and Chi-square tests. Between patientgroups, at baseline, months 6, 9, and 12, independent t-testswere used to compare antipsychotic dosage and symptomtotals and Mann–Whitney U-tests to compare medicationadherence.
Hippocampus and amygdala differences were exploredusing a MANCOVA with group membership (remitted, non-remitted, and control) as between-groups factor and side (leftand right) and structure (hippocampal head, body, and tail
Table 1Socio-demographic data for non-remitted patients, remitted patients, and healthy controls. Data presented as Mean±SD or as ratio.
Characteristic Non-remitted (n=40)
Remitted(n=17)
Controls(n=57)
Analysis
Statistic df p
Age at scan (years) 23.6±3.9 24.5±3.3 24.7±3.4 F=1.2 2, 111 0.31Parental SES status a 3.5±1.2 3.2±1.3 3.2±1.1 χ2=2.3 2 0.32Handed (R/L/A) 34/0/6 14/3/0 52/3/2 χ2=13.1 4 0.01Sex (M/F) 30/10 11/6 37/20 χ2=1.2 2 0.54
Abbreviations: A, ambidextrous; F, female; L, left; M, male; and R, right.a Hollingshead parental socio-economic status, in which 1=highest and 5=lowest.
76 M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
and amygdala) as within-group factors with handedness as acovariate. Univariate ANCOVAs with post-hoc Fisher LSD testswere used to analyze group differences where necessary. Thecritical p-value was set to 0.006 (0.05/8) for this analysis.
3. Results
3.1. Socio-demographic and clinical data
The three groups did not significantly differ in age,parental SES, or sex but did in handedness (Table 1). Forpositive and negative symptoms, patient groups did notsignificantly differ at baseline but remitted patients showedsignificantly lower totals at months 6, 9, and 12 (Table 2).Patient groups received equal amounts of antipsychoticdosage (in chlorpromazine equivalents) at baseline; howev-er, at months 6, 9, and 12, non-remitted patients receivedhigher total dosages that significantly differed at month 6.Groups did not differ on medication adherence at any timepoint investigated (Table 2).
Table 2Clinical symptomology, antipsychotic dosage, and medication adherence fornon-remitted and remitted patients. Data presented as Mean±SD.
Abbreviations: PANSS, Positive and Negative Syndrome Scale.a Degrees of freedom=54.b Antipsychotic totals presented in chlorpromazine equivalents.c Medication adherence: 0 (never adherent) to 4 (fully adherent).
3.2. Hippocampus and amygdala
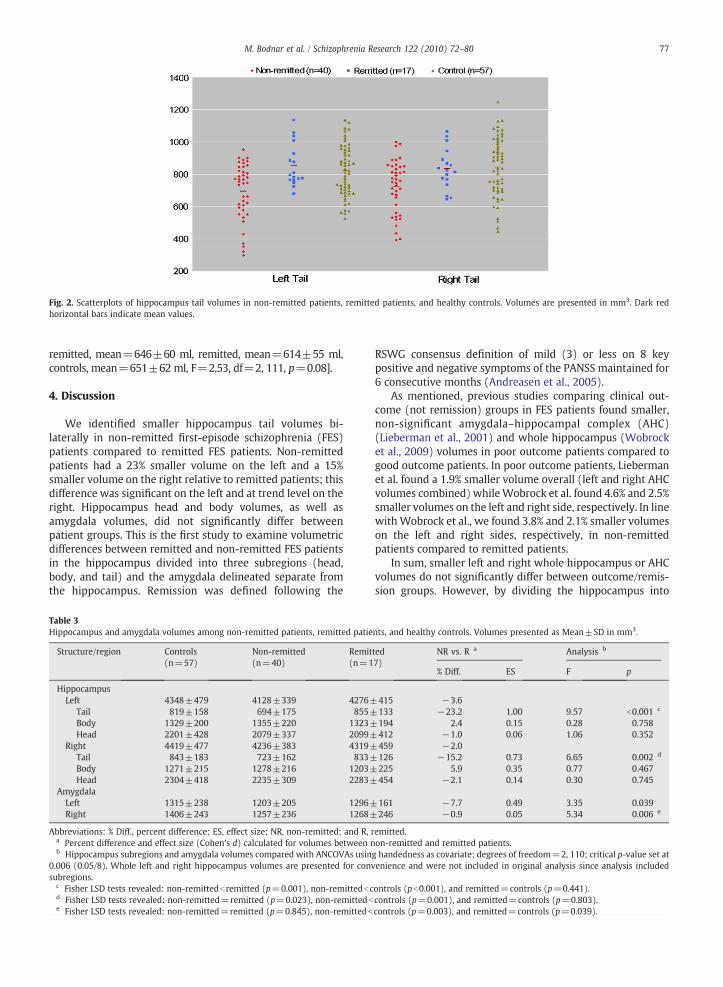
The MANCOVA revealed a significant group×structure×side interaction (F=5.46, df=3,109, p=0.002). Furtheranalyses revealed significant group differences in the rightand left hippocampus tail and right amygdala. For thehippocampus tail, non-remitted patients had smaller volumesbi-laterally compared to remitted patients (significant on theleft and trend level on the right); compared to controls, non-remitted patients had significantly smaller volumes bi-laterallywhile remitted patients did not significantly differ bi-laterally(Fig. 2). For the right amygdala, remitted and non-remittedpatients did not significantly differ. Compared to controls, non-remitted patients had a significantly smaller volume whileremitted patients did not significantly differ. See Table 3 forvolumes and statistical values.
3.2.1. Supplementary imaging analysesAlthough we were investigating a first-episode sample to
reduce the effect of antipsychotic exposure on brain morphol-ogy, patients were scanned, on average, 18 weeks past entrywhere all but 2 remitted patients had taken various medica-tions. As such we calculated a cumulative antipsychoticdosage (in chlorpromazine equivalents) from PEPP entry untilscan weighted on medication adherence (non-remittedmean=614±561; remitted mean=600±444; t=0.09,df=55, p=0.93) and re-analyzed the MANCOVA includingthis as another covariate. The triple interaction remainedsignificant (F=5.29, df=3,108, p=0.002) with further anal-yses still showing a significant group difference in the lefthippocampus tail (F=8.34, df=2,109, pb0.001) but only atrend level difference in the right hippocampus tail (F=4.34,df=2,109, p=0.015); right amygdala volume no longersignificantly differed among the groups (F=3.21, df=2,109,p=0.044). Regarding the hippocampus tail, non-remittedpatients still showed a significantly smaller volume on the left(p=0.001) with the trend level difference on the right (p=0.024) compared to remitted patients. Next, we used partialcorrelations controlling for remission status to explore therelationship between hippocampus tail volumes and symptomtotals at baseline and months 6, 9, and 12. No significant cor-relationswere identifiedoneither the left (allp-valuesN0.11)orright (all p-valuesN0.12) side. Finally, gray matter volumeswere estimated for each participant using the VBM8 toolboxcreated by C. Gaser (http://dbm.neuro.uni-jena.de/vbm/download/). A one-way ANOVA revealed total gray mattervolume did not significantly differ among the 3 groups [non-
Fig. 2. Scatterplots of hippocampus tail volumes in non-remitted patients, remitted patients, and healthy controls. Volumes are presented in mm3. Dark redhorizontal bars indicate mean values.
77M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
We identified smaller hippocampus tail volumes bi-laterally in non-remitted first-episode schizophrenia (FES)patients compared to remitted FES patients. Non-remittedpatients had a 23% smaller volume on the left and a 15%smaller volume on the right relative to remitted patients; thisdifference was significant on the left and at trend level on theright. Hippocampus head and body volumes, as well asamygdala volumes, did not significantly differ betweenpatient groups. This is the first study to examine volumetricdifferences between remitted and non-remitted FES patientsin the hippocampus divided into three subregions (head,body, and tail) and the amygdala delineated separate fromthe hippocampus. Remission was defined following the
Table 3Hippocampus and amygdala volumes among non-remitted patients, remitted patie
Abbreviations: % Diff., percent difference; ES, effect size; NR, non-remitted; and R, ra Percent difference and effect size (Cohen's d) calculated for volumes between nb Hippocampus subregions and amygdala volumes compared with ANCOVAs usin
0.006 (0.05/8). Whole left and right hippocampus volumes are presented for convsubregions.
RSWG consensus definition of mild (3) or less on 8 keypositive and negative symptoms of the PANSS maintained for6 consecutive months (Andreasen et al., 2005).
As mentioned, previous studies comparing clinical out-come (not remission) groups in FES patients found smaller,non-significant amygdala–hippocampal complex (AHC)(Lieberman et al., 2001) and whole hippocampus (Wobrocket al., 2009) volumes in poor outcome patients compared togood outcome patients. In poor outcome patients, Liebermanet al. found a 1.9% smaller volume overall (left and right AHCvolumes combined) whileWobrock et al. found 4.6% and 2.5%smaller volumes on the left and right side, respectively. In linewith Wobrock et al., we found 3.8% and 2.1% smaller volumeson the left and right sides, respectively, in non-remittedpatients compared to remitted patients.
In sum, smaller left and right whole hippocampus or AHCvolumes do not significantly differ between outcome/remis-sion groups. However, by dividing the hippocampus into
nts, and healthy controls. Volumes presented as Mean±SD in mm3.
161 −7.7 0.49 3.35 0.039246 −0.9 0.05 5.34 0.006 e
emitted.on-remitted and remitted patients.g handedness as covariate; degrees of freedom=2, 110; critical p-value set atenience and were not included in original analysis since analysis included
ontrols (pb0.001), and remitted=controls (p=0.441).controls (p=0.001), and remitted=controls (p=0.803).controls (p=0.003), and remitted=controls (p=0.039).
78 M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
subregions, non-remitted FES patients compared to remittedFES patients have smaller tail volumes bi-laterally (significanton the left and trend level on the right) and no significant ortrend level differences in body or head volumes bi-laterally.These findings, of course, need to be verified in other FESstudies.
4.1. The hippocampus in schizophrenia: a target for treatment
The hippocampus appears central to the pathology ofschizophrenia (Gothelf et al., 2000; Harrison, 2004). As alreadymentioned, reduced hippocampal volumes have been associ-ated with schizophrenia (Steen et al., 2006; Vita and de Peri,2007; Vita et al., 2006). We extended this relationship bydemonstrating the left tail (most posterior) subregion of thehippocampus was significantly smaller in non-remitted FESpatients compared to remitted FES patients; however, wewereunable to relate either positive or negative symptoms to thesesubregions. Yet, a previous study identified a significantrelationship between negative symptomology and the leftposterior hippocampus (Rajarethinam et al., 2001). Discrepan-cies between our findings may extend from the fact that theirstudy examined the posterior region and employed peoplewith chronic schizophrenia whereas we investigated thehippocampus tail explicitly and employed people in theirfirst-episode of schizophrenia. Nevertheless, the hippocampusappears to be a potential target for future studies in relation tosymptomology and outcome.
In fact, a recent study demonstrated that physical exerciseactually increased the relative volume of the hippocampus inboth healthy controls and those affected by schizophrenia.Moreover, the positive change in volume was significantlycorrelated with improved verbal memory in the schizophre-nia group and a non-significant improvement (decrease) intotal symptoms (Pajonk et al., 2010). Although not investi-gated, it would be interesting to see which subregion of thehippocampus, if any, displayed the most change and relatedto the symptom changes observed. More studies are neededto investigate the exact relationship the subregions of thehippocampus may have in the pathophysiology of schizo-phrenia to encourage more target-specific research.
In schizophrenia, altered protein expressions of cytoarchi-tecture has been observed in the posterior hippocampus(Nesvaderani et al., 2009)whichmay lead to a reducednumberof oligodendrocytes (Schmitt et al., 2009) and the poorconnectivity within the posterior hippocampus (Kalus et al.,2004) or the surrounding area, like the fornix (Fitzsimmons etal., 2009; Rametti et al., 2009; Takei et al., 2008; Zhou et al.,2008), for example. Poor connectivity in schizophrenia mayalso stem from dysfunctions in GABAergic or dopaminergicneurotransmission systems (Harrison and Weinberger, 2005).Again, in the posterior hippocampus, reduced expression ofguanine nucleotide-binding protein G(o) alpha subunit 1(GNAO1) was identified (Nesvaderani et al., 2009) that isbelieved to play an important role in the aforementionedneurotransmission systems (Hubbard and Hepler, 2006;Vawter et al., 2004). With strong links to schizophrenia andreduced cell and protein expressions isolated to the posteriorhippocampus, it would be interesting to see if a differentialexpressionof oligodendrocytes or related genes likeGNAO1, forexample, exists in the hippocampus tail in relation to remission.
This may help narrow the range in developing target-specificmedications in hope of a better outcome for those with a poorprognosis. Moreover, by using pharmaco-fMRI techniques(Honey and Bullmore, 2004; Stein, 2001), for example, newcompounds can be detected that may increase regional brainfunction in or near the hippocampus in relation to memory(Binder et al., 2009). These new medications could lead to abetter outcome by treating patients identified early on in thetreatment process that display a reliable marker of pooroutcome such as very poor verbal memory (Toulopoulou andMurray, 2004).
Of course, future studies should not be restricted tostudying the hippocampus only but the medial temporal lobe(MTL) appears to be a strong starting point. To beginwith, theMTL is accepted to be central to various memory processesand, in schizophrenia, poor verbal memory has beenidentified as a marker of both functional outcome (Green,1996) and remission (Bodnar et al., in press; Helldin et al.,2006). Moreover, using voxel-based morphometry, werecently identified smaller parahippocampal gray matterconcentration bi-laterally in non-remitted FES patientscompared to remitted FES patients with no significantdifferences in any other region, specifically the prefrontalcortex (Bodnar et al., in press). Of course, investigationsshould also not be limited to the gray matter only. Inschizophrenia, both neuropathological and neuropsycholog-ical results have associated reduced connectivity from thehippocampus to the prefrontal cortex and parahippocampalgyrus to the disorder rather than within the hippocampusitself (Harrison, 2004; Talamini et al., 2005; Zhou et al., 2008).So, the gray matter reductions in the MTL we have observedin non-remitted patients could ultimately be related todisrupted white matter. Although no study has investigatedconnectivity with respect to remission, one DTI study didinvestigate people at ultra-high risk for developing psychosisand found reduced white matter integrity (lower FA values)in the MTL at baseline predicted poor social functioning15 months later (Karlsgodt et al., 2009). With remissionstatus strongly related to functional outcome (Cassidy et al.,2010), the idea of white matter integrity in relation toremission needs to be investigated with a focus on connec-tions juxtaposed to the hippocampus tail (posterior region)based on our current results.
4.2. Limitations
By examining FES patients only our results cannot begeneralized to other first-episode populations. However,hippocampus reductions have been shown to be specific toschizophrenia and not other forms of psychosis (Hirayasu et al.,1998; Velakoulis et al., 2006). Another limitation involves theeffect of antipsychotic exposure on brain morphology (Mon-crieff and Leo, 2010), namely in the hippocampus (DeLisi et al.,1997). To control for this, we 1) employed first-episodepatients reducing the effect of long-term exposure, and 2) re-analyzed the data including a cumulative antipsychoticcovariate (since patients had psychotropic exposure, albeit fora limitedperiod of time) and found the same results. Our resultsappear unaffected by antipsychotic exposure but should beverified in antipsychotic naïve samples. Lastly, we examinedremission early on in treatment (from month 6 to month 12)
79M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
understanding that more patients may remit after longertreatment.However, ourgoalwas to investigate neuralmarkersof early remission. And besides, early treatment response hasbeen shown to be predictive of long-term outcome (Harrisonet al., 2001; Emsley et al., 2008).
4.3. Summary
Our study identified smaller hippocampus tail volumes innon-remitted FES patients compared to remitted FES patients;body and head volumes as well as amygdala volumes did notdiffer between patient groups. Together with previous results,it would appear that hippocampal pathology is not only part ofthe biological signature of schizophrenia but may varysignificantly as a function of future clinical status; however,more studies are needed to verify if one subregion in particular(namely the tail) is more related to remission or clinicaloutcomethan theothers. Furthermore, thequestionofoutcomeheterogeneity in relation to neural integrity is clinicallyrelevant. Understanding the neural basis of remission helpsmove us towards a better understanding of the pathophysiol-ogy of schizophrenia and may encourage the search for new,more target-specific, medications via pharmaco-fMRI techni-ques, for example, to help improve outcome for those with apoorer prognosis.
Role of funding sourceThis work was funded by operating grants from the Canadian Institutes
of Health Research (CIHR; #68961) and the Sackler Foundation to Drs LepageandMalla and a doctoral research award from CIHR (#9446) toM. Bodnar. M.Lepage is supported by a salary award from the Fonds de la recherche ensanté du Québec (FRSQ). A.K. Malla is supported by the Canada ResearchChairs program. The abovementioned funding agencies had no role in thestudy design; in the collection, analysis and interpretation of data; in thewriting of the report; and in the decision to submit the paper for publication.
ContributorsAuthor Martin Lepage designed the study. Author Michael Bodnar and
Martin Lepage managed the literature searches and analyses. Author MichaelBodnar undertook all statistical analyses and wrote the first draft of themanuscript. Authors Yvonne Czechowska, Audrey Benoit, and Ferid Fathallimanually traced the amygdala while author Yvonne Czechowska manuallytraced all hippocampi and oversaw all manual tracing protocols. Authors JensPruessner and Marita Pruessner developed the protocol for the triplesegmentation of the hippocampus. Authors Ashok Malla and Ridha Joobermanaged all patient recruitment and clinical assessments. All authorscontributed to and have approved the final manuscript.
Conflict of interestM. Lepage reports having received honorariums for educational events
from Janssen-Ortho & Lilly. A.K. Malla reports having received financialassistance/compensation for research and educational activities from Pfizer,Janssen-Ortho, AstraZeneca, and Bristol-Myers-Squibb. R. Joober reportshaving received consultancy honorarium from Pfizer and Janssen-Ortho. Allother authors declare that they have no conflicts of interest.
AcknowledgementsWe thank the PEPP-Montreal research staff for their help with
recruitment and clinical assessments of all patients involved. We wouldalso like to thank Caroline Chochol of the Brain Imaging Group forcontributing to the inter-reliability of the hippocampus.
References
Andreasen, N.C., Carpenter Jr., W.T., Kane, J.M., Lasser, R.A., Marder, S.R.,Weinberger, D.R., 2005. Remission in schizophrenia: proposed criteriaand rationale for consensus. Am. J. Psychiatry 162, 441–449.
Barbas, H., Blatt, G.J., 1995. Topographically specific hippocampal projectionstarget functionally distinct prefrontal areas in the rhesus monkey.Hippocampus 5, 511–533.
Becker, T., Elmer, K., Schneider, F., Schneider, M., Grodd, W., Bartels, M.,Heckers, S., Beckmann, H., 1996. Confirmation of reduced temporallimbic structure volume onmagnetic resonance imaging inmale patientswith schizophrenia. Psychiatry Res. 67, 135–143.
Binder, J.R., Desai, R.H., Graves, W.W., Conant, L.L., 2009. Where is thesemantic system? A critical review and meta-analysis of 120 functionalneuroimaging studies. Cereb Cortex. 19, 2767–2796.
Bodnar, M., Harvey, P.-O., Malla, A., Joober, R., Lepage, M., in press. Theparahippocampal gyrus as a neural marker of early remission in firstepisode psychosis: a voxel-based morphometry study. Clin SchizophrRelated Psychosis.
Cassidy, C.M., Norman, R., Manchanda, R., Schmitz, N., Malla, A., 2010. TestingDefinitions of Symptom Remission in First-Episode Psychosisfor Prediction of Functional Outcome at 2 Years. Schizophr Bull. 36,1001–1008.
Collins, D.L., Neelin, P., Peters, T.M., Evans, A.C., 1994. Automatic 3Dintersubject registration of MR volumetric data in standardized Talairachspace. J. Comput. Assist. Tomogr. 18, 192–205.
DeLisi, L.E., Sakuma, M., Tew, W., Kushner, M., Hoff, A.L., Grimson, R., 1997.Schizophrenia as a chronic active brain process: a study of progressivebrain structural change subsequent to the onset of schizophrenia.Psychiatry Res. 74, 129–140.
Duvernoy, H.M., 2005. The Human Hippocampus: Functional Anatomy,Vascularization, and Serial Sections with MRI., Ed. Springer Verlag,Berlin.
Emsley, R., Chiliza, B., Schoeman, R., 2008. Predictors of long-term outcome inschizophrenia. Curr. Opin. Psychiatry 21, 173–177.
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1998. Structured ClinicalInterview for DSM-IV Axis I Disorders, Patient Edition (SCID-I/P & SCID-I/NP), Version 2, Ed. New York Psychiatric Institute, Biometrics Research,New York.
Fitzsimmons, J., Kubicki, M., Smith, K., Bushell, G., Estepar, R.S., Westin, C.F.,Nestor, P.G., Niznikiewicz, M.A., Kikinis, R., McCarley, R.W., Shenton, M.E.,2009. Diffusion tractography of the fornix in schizophrenia. Schizophr. Res.107, 39–46.
Goldman-Rakic, P.S., Selemon, L.D., Schwartz, M.L., 1984. Dual pathwaysconnecting the dorsolateral prefrontal cortex with the hippocampalformation andparahippocampal cortex in the rhesusmonkey.Neuroscience12, 719–743.
Gothelf, D., Soreni, N., Nachman, R.P., Tyano, S., Hiss, Y., Reiner, O., Weizman,A., 2000. Evidence for the involvement of the hippocampus in thepathophysiology of schizophrenia. Eur. Neuropsychopharmacol. 10,389–395.
Green, M.F., 1996. What are the functional consequences of neurocognitivedeficits in schizophrenia? Am. J. Psychiatry 153, 321–330.
Hackert, V.H., den Heijer, T., Oudkerk, M., Koudstaal, P.J., Hofman, A., Breteler,M.M., 2002. Hippocampal head size associated with verbal memoryperformance in nondemented elderly. Neuroimage 17, 1365–1372.
Harrison, G., Hopper, K., Craig, T., Laska, E., Siegel, C.,Wanderling, J., Dube, K.C.,Ganev, K., Giel, R., an der Heiden, W., Holmberg, S.K., Janca, A., Lee, P.W.,Leon, C.A., Malhotra, S., Marsella, A.J., Nakane, Y., Sartorius, N., Shen, Y.,Skoda, C., Thara, R., Tsirkin, S.J., Varma, V.K., Walsh, D., Wiersma, D., 2001.Recovery from psychotic illness: a 15- and 25-year international follow-up study. Br. J. Psychiatry 178, 506–517.
Harrison, P.J., 2004. The hippocampus in schizophrenia: a review of theneuropathological evidence and its pathophysiological implications.Psychopharmacology (Berl) 174, 151–162.
Harrison, P.J., Weinberger, D.R., 2005. Schizophrenia genes, gene expression,and neuropathology: on the matter of their convergence. Mol. Psychiatry10, 40–68.
Helldin, L., Kane, J.M., Karilampi, U., Norlander, T., Archer, T., 2006. Remissionand cognitive ability in a cohort of patients with schizophrenia. J. Psychiatr.Res. 40, 738–745.
Hirayasu, Y., Shenton, M.E., Salisbury, D.F., Dickey, C.C., Fischer, I.A., Mazzoni,P., Kisler, T., Arakaki, H., Kwon, J.S., Anderson, J.E., Yurgelun-Todd, D.,Tohen, M., McCarley, R.W., 1998. Lower left temporal lobe MRI volumesin patients with first-episode schizophrenia compared with psychoticpatients with first-episode affective disorder and normal subjects. Am. J.Psychiatry 155, 1384–1391.
Ho, B.C., Andreasen, N.C., Nopoulos, P., Arndt, S., Magnotta, V., Flaum, M.,2003. Progressive structural brain abnormalities and their relationship toclinical outcome: a longitudinal magnetic resonance imaging study earlyin schizophrenia. Arch. Gen. Psychiatry 60, 585–594.
Hollingshead, A., 1965. Two-Factor Index of Social Position, Ed. Yale UniversityPress, New Haven, CN.
Honey, G., Bullmore, E., 2004. Human pharmacological MRI. TrendsPharmacol. Sci. 25, 366–374.
80 M. Bodnar et al. / Schizophrenia Research 122 (2010) 72–80
Hubbard, K.B., Hepler, J.R., 2006. Cell signalling diversity of the Gqalphafamily of heterotrimeric G proteins. Cell. Signal. 18, 135–150.
Karlsgodt, K.H., Niendam, T.A., Bearden, C.E., Cannon, T.D., 2009. Whitematter integrity and prediction of social and role functioning in subjectsat ultra-high risk for psychosis. Biol. Psychiatry 66, 562–569.
Kay, S., Fiszbein, A., Opler, L., 1987. The positive and negative synfrome scale(PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276.
Konrad, C., Ukas, T., Nebel, C., Arolt, V., Toga, A.W., Narr, K.L., 2009. Definingthe human hippocampus in cerebral magnetic resonance images—anoverview of current segmentation protocols. Neuroimage 47,1185–1195.
Lieberman, J., Chakos, M., Wu, H., Alvir, J., Hoffman, E., Robinson, D., Bilder, R.,2001. Longitudinal study of brainmorphology infirst episode schizophrenia.Biol. Psychiatry 49, 487–499.
Malla, A., Norman, R., McLean, T., Scholten, D., Townsend, L., 2003. ACanadian programme for early intervention in non-affective psychoticdisorders. Aust. N. Z. J. Psychiatry 37, 407–413.
Moncrieff, J., Leo, J., 2010. A systematic review of the effects of antipsychoticdrugs on brain volume. Psychol. Med. 1–14.
Moser, M.B., Moser, E.I., 1998. Functional differentiation in the hippocampus.Hippocampus 8, 608–619.
Narr, K.L., Thompson, P.M., Szeszko, P., Robinson, D., Jang, S., Woods, R.P.,Kim, S., Hayashi, K.M., Asunction, D., Toga, A.W., Bilder, R.M., 2004.Regional specificity of hippocampal volume reductions in first-episodeschizophrenia. Neuroimage 21, 1563–1575.
Nesvaderani, M., Matsumoto, I., Sivagnanasundaram, S., 2009. Anteriorhippocampus in schizophrenia pathogenesis: molecular evidence from aproteome study. Aust. N. Z. J. Psychiatry 43, 310–322.
O'Driscoll, G.A., Florencio, P.S., Gagnon, D., Wolff, A.V., Benkelfat, C., Mikula, L.,Lal, S., Evans, A.C., 2001. Amygdala–hippocampal volume and verbalmemory in first-degree relatives of schizophrenic patients. PsychiatryRes. 107, 75–85.
Oldfield, R.C., 1971. The assessment and analysis of handedness: theEdinburgh inventory. Neuropsychologia 9, 97–113.
Pajonk, F.G., Wobrock, T., Gruber, O., Scherk, H., Berner, D., Kaizl, I., Kierer, A.,Muller, S., Oest, M., Meyer, T., Backens, M., Schneider-Axmann, T.,Thornton, A.E., Honer, W.G., Falkai, P., 2010. Hippocampal plasticity inresponse to exercise in schizophrenia. Arch. Gen. Psychiatry 67,133–143.
Pruessner, J.C., Li, L.M., Serles, W., Pruessner, M., Collins, D.L., Kabani, N.,Lupien, S., Evans, A.C., 2000. Volumetry of hippocampus and amygdalawith high-resolution MRI and three-dimensional analysis software:minimizing the discrepancies between laboratories. Cereb. Cortex 10,433–442.
Rajarethinam, R., DeQuardo, J.R., Miedler, J., Arndt, S., Kirbat, R., Brunberg, J.A.,Tandon, R., 2001. Hippocampus and amygdala in schizophrenia: assess-ment of the relationship of neuroanatomy to psychopathology. PsychiatryRes. 108, 79–87.
Rametti, G., Segarra, N., Junque, C., Bargallo, N., Caldu, X., Ibarretxe, N.,Bernardo, M., 2007. Left posterior hippocampal density reduction usingVBM and stereological MRI procedures in schizophrenia. Schizophr. Res.96, 62–71.
Rametti, G., Junque, C., Falcon, C., Bargallo, N., Catalan, R., Penades, R., Garzon,B., Bernardo, M., 2009. A voxel-based diffusion tensor imaging study oftemporal white matter in patients with schizophrenia. Psychiatry Res.171, 166–176.
Robinson, D.G.,Woerner,M.G.,McMeniman,M.,Mendelowitz, A., Bilder, R.M.,2004. Symptomatic and functional recovery from a first episode ofschizophrenia or schizoaffective disorder. Am. J. Psychiatry 161,473–479.
Schmidt-Wilcke, T., Poljansky, S., Hierlmeier, S., Hausner, J., Ibach, B., 2009.Memory performance correlates with gray matter density in the ento-/perirhinal cortexandposterior hippocampus in patientswithmild cognitiveimpairment and healthy controls—a voxel based morphometry study.Neuroimage 47, 1914–1920.
Stereologic investigation of the posterior part of the hippocampus inschizophrenia. Acta Neuropathol. 117, 395–407.
Sled, J.G., Zijdenbos, A.P., Evans, A.C., 1998. A nonparametric method forautomatic correction of intensity nonuniformity in MRI data. IEEE Trans.Med. Imaging 17, 87–97.
Steen, R.G., Mull, C., McClure, R., Hamer, R.M., Lieberman, J.A., 2006. Brainvolume in first-episode schizophrenia: systematic review and meta-analysis of magnetic resonance imaging studies. Br. J. Psychiatry 188,510–518.
Stein, E.A., 2001. fMRI: a new tool for the in vivo localization of drug actionsin the brain. J. Anal. Toxicol. 25, 419–424.
Szeszko, P.R., Strous, R.D., Goldman, R.S., Ashtari, M., Knuth, K.H., Lieberman,J.A., Bilder, R.M., 2002. Neuropsychological correlates of hippocampalvolumes in patients experiencing a first episode of schizophrenia. Am. J.Psychiatry 159, 217–226.
Szeszko, P.R., Goldberg, E., Gunduz-Bruce, H., Ashtari, M., Robinson, D.,Malhotra, A.K., Lencz, T., Bates, J., Crandall, D.T., Kane, J.M., Bilder, R.M.,2003. Smaller anterior hippocampal formation volume in antipsychotic-naive patients with first-episode schizophrenia. Am. J. Psychiatry 160,2190–2197.
Takei, K., Yamasue, H., Abe, O., Yamada, H., Inoue, H., Suga, M., Sekita, K., Sasaki,H., Rogers, M., Aoki, S., Kasai, K., 2008. Disrupted integrity of the fornix isassociatedwith impairedmemoryorganization in schizophrenia. Schizophr.Res. 103, 52–61.
Talairach, J., Tournoux, P., 1988. Co-Planar Stereotaxic Atlas of the HumanBrain, Ed. Thieme, New York.
Talamini, L.M.,Meeter,M., Elvevag, B.,Murre, J.M., Goldberg, T.E., 2005. Reducedparahippocampal connectivity produces schizophrenia-like memorydeficits in simulated neural circuits with reduced parahippocampalconnectivity. Arch. Gen. Psychiatry 62, 485–493.
Toulopoulou, T., Murray, R.M., 2004. Verbal memory deficit in patients withschizophrenia: an important future target for treatment. Expert Rev.Neurother. 4, 43–52.
Vawter, M.P., Ferran, E., Galke, B., Cooper, K., Bunney, W.E., Byerley, W., 2004.Microarray screening of lymphocyte gene expression differences in amultiplex schizophrenia pedigree. Schizophr. Res. 67, 41–52.
Velakoulis, D., Wood, S.J., Wong, M.T., McGorry, P.D., Yung, A., Phillips, L.,Smith, D., Brewer, W., Proffitt, T., Desmond, P., Pantelis, C., 2006.Hippocampal and amygdala volumes according to psychosis stage anddiagnosis: a magnetic resonance imaging study of chronic schizophrenia,first-episode psychosis, and ultra-high-risk individuals. Arch. Gen.Psychiatry 63, 139–149.
Vita, A., de Peri, L., 2007. Hippocampal and amygdala volume reductions infirst-episode schizophrenia. Br. J. Psychiatry 190, 271.
Vita, A., De Peri, L., Silenzi, C., Dieci, M., 2006. Brain morphology in first-episode schizophrenia: a meta-analysis of quantitative magneticresonance imaging studies. Schizophr. Res. 82, 75–88.
Witter, M.P., Wouterlood, F.G., Naber, P.A., Van Haeften, T., 2000.Anatomical organization of the parahippocampal–hippocampal network.In: W. Scharfman, H.E., M.P., Schwarcz, R. (Eds.), The ParahippocampalRegion, Implications for Neurological and Psychiatric Diseases. Annals ofthe New York Academy of Sciences, New York, pp. 1–24.
Witthaus, H., Mendes, U., Brune, M., Ozgurdal, S., Bohner, G., Gudlowski, Y.,Kalus, P., Andreasen, N., Heinz, A., Klingebiel, R., Juckel, G., 2010.Hippocampal subdivision and amygdalar volumes in patients in an at-risk mental state for schizophrenia. J. Psychiatry Neurosci. 35, 33–40.
Wobrock, T., Gruber, O., Schneider-Axmann, T., Wolwer, W., Gaebel, W.,Riesbeck, M., Maier, W., Klosterkotter, J., Schneider, F., Buchkremer, G.,Moller, H.J., Schmitt, A., Bender, S., Schlosser, R., Falkai, P., 2009. Internalcapsule size associated with outcome in first-episode schizophrenia. Eur.Arch. Psychiatry Clin. Neurosci. 259, 278–283.
Woods, S.W., 2003. Chlorpromazine equivalent doses for the newer atypicalantipsychotics. J. Clin. Psychiatry 64, 663–667.