Intern. J. Neuroscience, 116:1271–1293, 2006 Copyright C 2006 Informa Healthcare ISSN: 0020-7454 / 1543-5245 online DOI: 10.1080/00207450600920928 NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTING DISEASES: ALZHEIMER’S DEMENTIA, VASCULAR DEMENTIA, FRONTOTEMPORAL DEMENTIA, AND MAJOR DEPRESSIVE DISORDER ALYSSA J. BRAATEN Nova Southeastern University Center for Psychological Studies Fort Lauderdale, Florida, USA THOMAS D. PARSONS Department of Neurology, School of Medicine University of North Carolina at Chapel Hill Chapel Hill, North Carolina, USA. ROBERT McCUE South Florida Neurology Associates, P.A. Delray Beach, Florida, USA ALFRED SELLERS WILLIAM J. BURNS Nova Southeastern University Center for Psychological Studies Fort Lauderdale, Florida, USA Received 19 July 2005. Address correspondence to Thomas D. Parsons, Ph.D., Department of Neurology, CB # 7025, University of North Carolina School of Medicine, 3114 Bioinformatics Building, Chapel Hill, NC 27599-7025, USA. E-mail: [email protected]1271
Nova Southeastern UniversityCenter for Psychological StudiesFort Lauderdale, Florida, USA
THOMAS D. PARSONS
Department of Neurology, School of MedicineUniversity of North Carolina at Chapel HillChapel Hill, North Carolina, USA.
ROBERT McCUE
South Florida Neurology Associates, P.A.Delray Beach, Florida, USA
ALFRED SELLERSWILLIAM J. BURNS
Nova Southeastern UniversityCenter for Psychological StudiesFort Lauderdale, Florida, USA
Received 19 July 2005.Address correspondence to Thomas D. Parsons, Ph.D., Department of Neurology, CB # 7025,
University of North Carolina School of Medicine, 3114 Bioinformatics Building, Chapel Hill, NC27599-7025, USA. E-mail: [email protected]
1271
1272 A. J. BRAATEN ET AL.
Similarities in presentation of Dementia of Alzheimer’s Type, Vascular Dementia,Frontotemporal Dementia, and Major Depressive Disorder, pose differentialdiagnosis challenges. The current study identifies specific neuropsychologicalpatterns of scores for Dementia of Alzheimer’s Type, Vascular Dementia,Frontotemporal Dementia, and Major Depressive Disorder. Neuropsychologicaldomains directly assessed in the study included: immediate memory, delayedmemory, confrontational naming, verbal fluency, attention, concentration, andexecutive functioning. The results reveal specific neuropsychological comparativeprofiles for Dementia of Alzheimer’s Type, Vascular Dementia, FrontotemporalDementia, and Major Depressive Disorder. The identification of these profiles willassist in the differential diagnosis of these disorders and aid in patient treatment.
Clinical overlap in the presentation of Dementia of the Alzheimer’s Type,Vascular Dementia, Fronto-Temporal Dementia, and Major Depressive Disor-der, poses significant challenges in differential diagnosis. Although numerousstudies have compared the neuropsychological profile of patients with Dementiaof the Alzheimer’s Type, Vascular Dementia, and depression, findings have beeninconsistent. Due to these inconsistencies, unique neuropsychological profilesfor each disorder, when present, are not firmly established. As such, it hasbeen difficult for clinicians confidently to discern which neuropsychologicalvariables provide relevant information for differential diagnoses. Althoughless research has been done comparing Fronto-Temporal Dementia to that ofDementia of the Alzheimer’s Type, Vascular Dementia, and depression, similarinconsistencies exist in the few studies currently available. Inconsistenciesacross studies may be attributable to several factors, primarily related tomethodological considerations. These include: (1) differences in selection ofparticipants for study inclusion, (2) failure to control for dementia severity, and(3) over-reliance on tests of statistical significance.
The neuropathological process behind Dementia of the Alzheimer’s Typeinvolves a preferential destruction of the parieto-temporal regions, includingthe hippocampus and surrounding cortical structures, thus deficits in memoryand learning are thought to be hallmark features of the disease (Bondiet al., 1996; Storey et al., 2002). Previous studies have shown that themost prominent feature of Dementia of the Alzheimer’s Type, and mostfrequently noticed distinguishing feature of the disorder, is a disproportionatedecline in memory function relative to other cognitive domains. Patients withDementia of the Alzheimer’s Type may also display a clearly progressiveanomic aphasia, or difficulty in naming in the context of relatively intact
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1273
speech fluency, auditory comprehension, articulation, prosody, and repetition(e.g., Cummings & Benson, 1992). Studies have shown that the firstlanguage abnormality to become apparent in Dementia of the Alzheimer’sType is impaired word finding; this anomia leads to circumlocution thatis evidenced in poor word-list generation, particularly for words in agiven semantic category (Mendez & Cummings, 2003). Literature has alsoshown that patients with Dementia of the Alzheimer’s Type have difficultyaccessing semantic information intentionally which manifests itself in amanner that appears to reflect a general semantic deterioration (Bondi et al.,1996).
Fronto-Temporal Dementia is a degenerative condition of the frontaland anterior temporal lobes, which control reasoning, personality, movement,speech, social graces, language and some aspects of memory. Fronto-TemporalDementia is characterized by rigid and inflexible thinking and impairedjudgment. Because the neuropathological process involved in Fronto-TemporalDementia differs from that of Dementia of the Alzheimer’s Type, and affectsprimarily the frontal lobes, deficits in memory are not a prominent feature ofFronto-Temporal Dementia (Neary et al., 1998; Brun et al., 1994; Rosen et al.,2002).
Major Depressive Disorder most commonly affects attention, concentra-tion, and memory abilities. The extent of cognitive deficits has been shown tocorrelate with depression severity. Memory failure in these patients may reflectimpairment in retrieval processes, which in turn depend on ability to attend tostimuli. These results may be useful in the differential diagnosis between MajorDepressive Disorder and early Dementia of the Alzheimer’s Type (Baudicet al., 2004; Lezak, 1995; Levy et al., 1998).
The nature of the neuropsychological profile associated with VascularDementia is highly variable and dependent on the distribution of cerebrovascu-lar disease and related factors (Cummings & Benson, 1992). Consequently,Vascular Dementia can be primarily cortical, primarily subcortical, or acombination of cortical and subcortical. The location and nature of the lesionsubstantially determines the nature of deficits observed. In general, deficitswill conform to known neuroanatomical correlates of behavior (Roman et al.,2004).
Issues of differences in selection of participants for study inclusion andfailure to control for dementia severity have led to considerable inconsistenciesin currently published studies. Standardized criteria are not commonly usedin the selection of participants for investigation. This leniency in participantinclusion creates confounds in between group comparisons, as patient groups
1274 A. J. BRAATEN ET AL.
may not be correctly defined and varying stages of illness severity may beincluded. This issue is particularly noteworthy in light of the fact that certaincharacteristics of a given disorder are absent at some stages and quite evident atothers. Fortunately, the development of consensus statements for the diagnosisof Dementia of the Alzheimer’s Type, Vascular Dementia, and Fronto-TemporalDementia (NINCDS-ADRDA, NINDS-AIREN, Hackinski Ischemia Scale,DSM-IV-TR, Neary Consensus Criteria), and making use of instruments suchas the Folstein Mini-Mental Status Exam (MMSE; Folstein et al., 1975) makedefining dementia type and severity possible.
A further issue is that null hypothesis significance testing does not quantifythe size of effects. Null hypothesis tests yield binary results that offer limitedclinical utility. Furthermore, null hypothesis significance testing is greatlyinfluenced by sample size (Cohen, 1990). A remedy for this over relianceon null hypothesis statistical significance is the use of the Cohen’s d statistic tocalculate an effect size. It is calculated by computing the difference betweenmeans and dividing this difference by their pooled standard deviations (i.e.,[u1-u2 ]/SDp). It provides a standard unit of measure that allows compilation offindings across studies as well as comparison of variables otherwise calibratedon dissimilar scales. Further, it offers an index of the degree to which groupsoverlap on a given variable (Zakzanis, 2001). Cohen (1988) suggested that d =0.2 represents a small effect size, d = 0.5 reflects a medium effect size, andd = 0.8 is considered a large effect size. A more conservative view, however,proposes an effect size of d = 1.0, which corresponds to a 45% overlap, andoffers improved possibility of discriminating. An ideal effect size is one of d =3.0 or greater which suggests a degree of overlap of 5% or less allowingoptimum separation of groups on a given variable (Zakzanis, 1998a). Overall,the use of effect sizes in addition to tests of null hypothesis offers importantinformation regarding which variables are most appropriate for use in thedifferential diagnosis of dementia.
Ambiguity regarding the nature of neuropsychological differences amongdementia groups and those with depression has served to obscure the ability tomake a distinction among these diagnoses. The neuropsychological differentialdiagnosis of dementia is further complicated by the fact that little research hasbeen conducted comparing the performance of patient’s with Fronto-TemporalDementia to patients with Vascular Dementia. This presents a significantproblem due to the fact that patients with Vascular Dementia tend to display“frontal” deficits upon neuropsychological evaluation (e.g., Cummings, 1990;Perez et al., 1975; Villardita, 1993). Hence, identifying a neuropsychologicalprofile of patients with Fronto-Temporal Dementia in comparison to those
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1275
with Dementia of the Alzheimer’s Type and Vascular Dementia would beadvantageous.
In summary, there is a growing need for research that will aid the clinicianin early and accurate differential diagnosis of the dementias. Although decadesof research have provided a wealth of data concerning the neuropsychologicalcharacteristics of Dementia of the Alzheimer’s Type, Vascular Dementia,Fronto-Temporal Dementia, and Major Depressive Disorder, inconsistenciesin findings raise concerns, and very little research has been done to assist in theease of differential diagnosis. The problem addressed by the current researchstudy was to identify specific neuropsychological comparative profiles, or atypical pattern of scores, for Dementia of the Alzheimer’s Type, VascularDementia, Fronto-Temporal Dementia, and Major Depressive Disorder. Theidentification of these profiles will assist in the differential diagnosis of thesedisorders and aid in patient treatment. Based upon the current literature(drawing heavily from Zakzanis et al., 1999), the following hypothesesare made:1. Dementia of the Alzheimer’s Type patients perform significantly lower than
patients with Vascular Dementia, Fronto-Temporal Dementia, or MajorDepressive Disorder on measures of delayed memory, confrontationalnaming, and semantic fluency.
2. Vascular Dementia patients perform significantly lower than patientsdiagnosed with Dementia of the Alzheimer’s Type, Fronto-TemporalDementia, or Major Depressive Disorder on measures of phonemic fluency,immediate recall.
3. Fronto-Temporal Dementia patients perform significantly lower than pa-tients diagnosed with Dementia of the Alzheimer’s Type, Vascular Dementia,or Major Depressive Disorder on the color/word portion of the Stroop test. Inaddition to the Stroop, it is hypothesized that patients with Fronto-TemporalDementia perform significantly lower on Trail Making Test Part B.
4. Major Depressive Disorder patients perform significantly lower than patientsdiagnosed with Dementia of the Alzheimer’s Type, Vascular Dementia, orFronto-Temporal Dementia on measures of attention and concentration, aswell as delayed recall portion.
METHOD
Design
Archival data of 120 community-dwelling individuals examined in a neurologyclinic were analyzed in this study. Each participant was administered a
1276 A. J. BRAATEN ET AL.
neuropsychological battery including tests of verbal fluency, expressivelanguage, memory, and executive functioning. Participants were divided intofour groups according to diagnosis. The four groups are described in detail inwhat follows, and include patients diagnosed with Dementia of the Alzheimer’sType, Vascular Dementia, Fronto-Temporal Dementia, and Major DepressiveDisorder. Patients included in dementia categories were also divided intosubgroups according to disease severity. Mild and moderate subgroups wereincluded in the study, whereas those within the severe range were eliminated.
Participants
Participants were referred by a neurologist for neuropsychological assessmentto assist in clarifying the absence or presence of, extent, and nature of cognitiveimpairment. The sample consisted of 111 participants, 56 male and 55 female,with a mean age of 76.55 years (SD = 5.54; range = 47 to 88). All participantsin the study were Caucasian (Table 1). Premorbid intelligence estimates werecalculated using the Wechsler Test of Adult Reading (WTAR; PsychologicalCorporation, 2001) and the regression equation of Barona and colleagues (1984)for the prediction of premorbid intellectual functioning. The mean premorbidintelligence estimate for the group was 109.62 (SD = 9.53; range = 89 to130).
Participants included in the study were selected on the basis of meetingcriteria for dementia or depression according to published standards. Partici-pants with dementia were then classified into three levels of disease severity(mild, moderate, and severe) according to scores on the Folstein Mini-MentalStatus Exam (MMSE; Folstein et al., 2001). Participants with MMSE scores
Table 1. Demographic data: Means (Standard deviations)
Gender Age (years) Barona/WTAR IQ MMSEGroup n M/F M(SD) M(SD) M(SD)
DAT = Dementia of the Alzheimer’s Type; VaD = Vascular Dementia; FTD = Fronto-Temporal Dementia; MDD = Major Depressive Disorder; MMSE = Folstein Mini-Mental StatusExam; WTAR = Wechsler Test of Adult Reading.
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1277
of 27–30 were classified as within the mild range, participants with scores of21–26 were defined as moderately impaired, and patients with scores of 20 andbelow were classified as severe. Patients with severe dementia classificationwere not included in the study.
Group 1, identified as the Dementia of the Alzheimer’s Type Group,consisted of 30 patients diagnosed with probable Alzheimer’s Diseaseaccording to the criteria developed by the National Institute of Neurologicaland Communicative Disorders and Stroke-Alzheimer’s Disease and RelatedDisorders Association Work Group criteria (NINCDS-ADRDA; McKhannet al., 1984). Dementia of the Alzheimer’s Type group participants had a meanage of 77.67 years (SD = 3.67; range = 70 to 88). There were 17 males and13 females in Group 1. The mean premorbid intelligence estimate for theDementia of the Alzheimer’s Type group was 110.47 (SD = 7.76; range = 99to 130).
Group 2 consisted of 31 patients diagnosed with Vascular Dementia accord-ing to the National Institutes of Neurological Disorders and Stroke-AssociationInternationale pour la Recherche et l’Enseignement en Neurosciences (NINDS-AIREN) criteria for Vascular Dementia (Roman et al., 1993) and the HachinskiIschemia Scale (Hachinski et al., 1975). Vascular Dementia group participantshad a mean age of 78.26 years (SD = 4.48; range = 69 to 89). There were17 males and 14 females in the Vascular Dementia group. The mean premorbidintelligence estimate for the Vascular Dementia group was 107.65 (SD = 5.40;range = 98 to 123).
Group 3 consisted of 20 patients diagnosed with Fronto-TemporalDementia according to the consensus criteria postulated by Neary et al. (1998).As listed previously, these criteria include the presence of five core diagnosticfeatures including insidious onset, early decline in social interpersonal conduct,and early impairment in the regulation of personal conduct, early emotionalblunting, and early loss of insight. The criteria also require the presenceof behavioral disorder, speech and language deficits, physical signs, andneuropsychological, brain imaging, or EEG verification for diagnosis.
Those participants included in the Fronto-Temporal Dementia group hada mean age of 74.00 years (SD = 5.63; range = 47 to 83). There were 8 malesand 12 females in the Fronto-Temporal Dementia group. The mean premorbidintelligence estimate for the Fronto-Temporal Dementia group was 109.95(SD = 14.15; range = 95 to 124).
Group 4 consisted of 30 patients diagnosed with Major Depressive Disor-der according to Beck Depression Inventory-Second Edition (BDI-II) score andcriteria as listed in the Diagnostic and Statistical Manual-Fourth Edition, Text
1278 A. J. BRAATEN ET AL.
Revision (DSM-IV-TR; American Psychiatric Association, 2000). Depressiongroup participants had a mean age of 76.27 years (SD = 8.39; range = 60 to80). There were 14 males and 16 females in the Depression group. The meanpremorbid intelligence estimate for the Depression group was 110.4 (SD =10.81; range = 83 to 127).
Group Classification
The independent variable in this study was the diagnostic group (Dementiaof the Alzheimer’s Type, Vascular Dementia, Fronto-Temporal Dementia,and Major Depressive Disorder). In each case, the diagnostic categorizationwas made according to relevant criteria as described earlier (e.g., NINCDS-ADRDA, NINDS-AIREN, Hackinski Ischemia Scale, DSM-IV-TR, NearyConsensus Criteria). In diagnosing the clinical groups (i.e., groups 1 through4), emphasis was placed on non-neuropsychological variables, to the degreepossible, which included emphasis on such variables as clinical history,neurological factors, and neuroimaging data. Specifically, clinical historiesand neurological factors were used for the diagnosis of each of the 111 studyparticipants. However, of the 111 participants, only 104 were classified intodiagnostic category with the assistance of neuroimaging data (e.g., ComputedTomography (CT) Scan/Magnetic Resonance Imaging (MRI) data). Twenty-nine of the 30 Dementia of the Alzheimer’s Type group participants, 31/31Vascular Dementia patients, 20/20 Fronto-Temporal Dementia patients, and24/30 Major Depressive Disorder patients were classified with the assistanceof neuroimaging data. This was done in order to avoid problems of circularitywhen subsequently comparing the groups on neuropsychological variables.Premorbid intelligence levels were estimated with the use of the Wechsler Testof Adult Reading.
Instrumentation
The dependent variables in the present study consisted of measures thatreflect the neuropsychological domains identified for analysis: verbal fluency(phonemic and semantic), confrontational naming, immediate recall, delayedrecall, working memory (attention and concentration), and executive func-tioning. These measures include the Controlled Oral Word Association Test(COWAT-FAS), Category Naming (Animals), Boston Naming Test (BNT),selected subtests from the Wechsler Memory Scale-Third Edition (WMS-III),the Stroop Test, and the Trail Making Test-Parts A and B. Additional
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1279
measures utilized in the study include the Folstein Mini-Mental Status Exam(MMSE; Folstein et al., 1975), the Beck Depression Inventory-Second Edition(BDI-II; Beck, 1987), and the Wechsler Test of Adult Reading (WTAR; ThePsychological Corporation, 2001).
Analyses
Multiple planned comparisons were performed to test the hypotheses detailedpreviously. The critical level for tests of statistical significance was set at! " .01 to provide protection against Type I error while attempting toavoid the susceptibility to Type II error that may occur with the introductionof a more stringent procedure. The magnitude of effect size (d statistic;Cohen, 1998) for each planned comparison was also examined. Twenty-sevenplanned comparisons were performed and effect sizes were calculated foreach. Specifically, planned comparisons were conducted for each of the 11neuropsychological variables in order to compare performances between thegroups. Effect sizes were calculated between each of the four groups. Statisticalfindings are presented later in the article for each hypothesis in turn. Bonferronicorrections were applied to adjust the critical alphas for these effect sizes, usingan alpha of .05 divided by 12 neuropsychological test variables, compared toyield a critical alpha of .0042.
RESULTS
Group Demographic Data
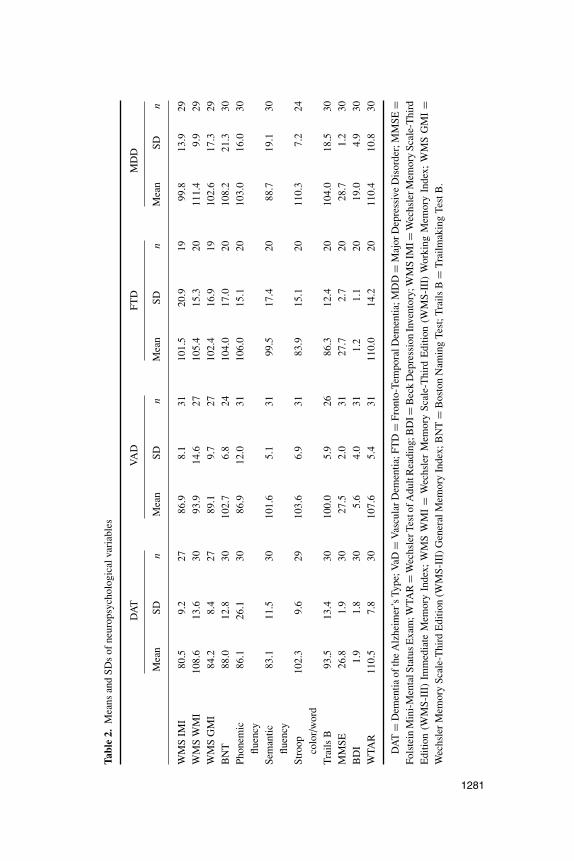
Demographic data, including means and standard deviations, are included inTable 1. Means and standard deviations of all neuropsychological variables arein Table 2. There were no significant differences among the participant groupson sex (F (3,107) = .484, p = .694), or estimated premorbid intelligence level (F(3, 107) = .591, p = .622). However, there was a significant difference amongthe participant groups for age (F (3, 107) = 6.010, p = .001) and MMSE scores(F (3, 107) = 4.933, p = .003). Post-hoc Tukey indicated that patients in theVascular Dementia participant group were slightly older overall as comparedto patients belonging to the Major Depressive Disorder and Fronto-TemporalDementia groups. This age difference likely had little effect on subsequentanalyses, as patient performance has been found to be independent of age. TheTukey also indicated that patients within the Dementia of the Alzheimer’s Typegroup performed significantly lower overall as compared to patients within
1280 A. J. BRAATEN ET AL.
the Major Depressive Disorder group. These significant differences occurreddespite attempts to limit differences by including only participants with MMSEscores of 21 and greater.
Dementia of the Alzheimer’s Type
Of the planned comparisons between groups with regard to delayed memory,two were significant. Specifically, the Dementia of the Alzheimer’s Type groupperformed significantly below the Major Depressive Disorder ( p < .001) andFronto-Temporal Dementia ( p < .001) groups. Calculated effect sizes revealeda small to moderate difference in performance between patients diagnosed withDementia of the Alzheimer’s Type and those diagnosed with Vascular Dementia(i.e., d = #.32). However, large differences in performance were identifiedbetween patients with Dementia of the Alzheimer’s Type and Fronto-TemporalDementia (i.e., d = #1.21), and Dementia of the Alzheimer’s Type and MajorDepressive Disorder (i.e., d = #.90). Effect sizes for delayed memory arelisted in Table 3. Of the planned comparisons between groups with regard todelayed memory, all three were significant. Specifically, the Dementia of theAlzheimer’s Type group performed significantly below the Vascular Dementiagroup (p = .007), the Fronto-Temporal Dementia group (p = .005), and MajorDepressive Disorder group ( p < .001). Effect sizes for confrontational namingin the Dementia of the Alzheimer’s Type group are listed in Table 3. Of theplanned comparisons between groups with regard to category fluency, twowere significant. Specifically, the Dementia of the Alzheimer’s Type groupperformed significantly below the Vascular Dementia group ( p < .001), andFronto-Temporal Dementia group ( p < .001). Effect sizes for category fluencyfor the Dementia of the Alzheimer’s Type group are listed in Table 3.
Vascular Dementia
Of the planned comparisons between groups with regard to phonemic fluency,two were significant. Specifically, the Vascular Dementia group performedsignificantly below the Major Depressive Disorder ( p < .001) and Fronto-Temporal Dementia ( p < .001) groups. Effect sizes for phonemic fluency arelisted in Table 3. Of the planned comparisons between groups with regardto immediate recall, two were significant. Specifically, the Vascular Dementiagroup performed significantly below the Major Depressive Disorder ( p < .001)and Fronto-Temporal Dementia ( p < .001) groups. Immediate recall effect sizesare listed in Table 3.
3 FTD<DAT Stroop Test 43.72 <.001 1.23FTD<VAD Stroop Test 51.29 <.001 1.32FTD<MDD Stroop Test 82.40 <.001 1.76FTD<DAT TrailMaking Test B 3.44 .066 .49FTD<VAD TrailMaking Test B 11.50 <.001 .91FTD<MDD TrailMaking Test B 19.55 <.001 1.16
DAT = Dementia of the Alzheimer’s Type; VaD = Vascular Dementia; FTD = Fronto-TemporalDementia; MDD = Major Depressive Disorder; MMSE = Folstein Mini-Mental Status Exam;WTAR = Wechsler Test of Adult Reading; WMS = Wechsler Memory Scale—Third Edition(WMS—III); COWAT = Controlled Oral Word Association Test.
Fronto-Temporal Dementia
Of the planned comparisons between groups with regard to executive function-ing as measured by the Stroop Test (color/word), all three were significant.Specifically, the Fronto-Temporal Dementia group performed significantlybelow the Dementia of the Alzheimer’s Type ( p < .001), Vascular Dementia( p < .001), and Major Depressive Disorder ( p < .001) groups. Effect sizes fordelayed memory are listed in Table 3. Of the planned comparisons between
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1283
groups with regard to executive functioning, as measured by the Trail-MakingTest Part B, two were significant. Specifically, the Fronto-Temporal Dementiagroup performed significantly below the Vascular Dementia ( p < .001) andMajor Depressive Disorder ( p < .001) groups. Effect sizes for delayed memoryare listed in Table 3.
Major Depressive Disorder
Of the planned comparisons between groups with regard to Major DepressiveDisorder and attention and concentration, one was significant. Specifically, theMajor Depressive Disorder group performed significantly below the VascularDementia group ( p < .001). Effect sizes for delayed memory are listed inTable 3. Of the planned comparisons between groups with regard to delayedmemory, two were significant. Specifically, the Major Depressive Disordergroup performed significantly above the Dementia of the Alzheimer’s Typegroup ( p < .001) and significantly below the Fronto-Temporal Dementia group( p < .001). There was no significant difference in delayed memory abilitiesbetween the Major Depressive Disorder and Vascular Dementia groups. Effectsizes for delayed memory are listed in Table 3.
DISCUSSION
The primary goals of the present study were to: (1) evaluate the neuropsy-chological differences between dementia types and (2) to assess directly thepresence, if any, of differences in neuropsychological performance betweenpatients with Dementia of the Alzheimer’s Type, Vascular Dementia, Fronto-Temporal Dementia, and Major Depressive Disorder. Neuropsychologicaldomains directly assessed in the study included: immediate memory, delayedmemory, confrontational naming, verbal fluency, attention, concentration, andexecutive functioning. Four hypotheses were generated based on a review ofthe literature comparing the patient groups across various neuropsychologicaldomains.
Dementia of the Alzheimer’s Type
With regard to delayed memory abilities, patients with Dementia of theAlzheimer’s Type performed significantly worse than patients diagnosedwith Fronto-Temporal Dementia or Major Depressive Disorder, according todemographically corrected standard scores. However, there was no significant
1284 A. J. BRAATEN ET AL.
difference in performance between patients diagnosed with Dementia ofthe Alzheimer’s Type and those diagnosed with Vascular Dementia. Theneuropathological process behind Dementia of the Alzheimer’s Type involvesa preferential destruction of the parieto-temporal regions, including thehippocampus and surrounding cortical structures, thus deficits in memoryand learning are thought to be hallmark features of the disease (Bondi et al.,1996). More specifically, previous literature has shown that the most prominentfeature of Dementia of the Alzheimer’s Type, and most frequently noticeddistinguishing feature of the disorder, is a disproportionate decline in memoryfunction relative to other cognitive domains. Thus, the significant deficitsexhibited by Dementia of the Alzheimer’s Type patients on a measure ofdelayed memory substantiate prior research. Because the neuropathologicalprocess involved in Fronto-Temporal Dementia differs from that of Dementiaof the Alzheimer’s Type, and affects primarily the frontal lobes, deficits inmemory are not a prominent feature of Fronto-Temporal Dementia. Similarly,although patients suffering from Major Depressive Disorder exhibit decreasedmotivation and some delayed memory deficits, the deficits were not significantas compared to those of Dementia of the Alzheimer’s Type (Lezak, 1995;Levy et al., 1998). However, because, as discussed previously, the nature ofthe neuropsychological profile associated with Vascular Dementia is highlyvariable and dependent on the distribution of cerebrovascular disease andrelated factors (Cummings & Benson, 1992), Vascular Dementia can beprimarily cortical, primarily subcortical, or a combination of cortical andsubcortical. The location and nature of the lesion substantially determinesthe nature of deficits observed. In general, deficits will conform to knownneuroanatomical correlates of behavior. This variability in deficits likelyexplains the lack of significant difference between the performance of patientsdiagnosed with Dementia of the Alzheimer’s Type and those diagnosed withVascular Dementia.
Effect sizes revealed large differences in performance between patientswith Dementia of the Alzheimer’s Type when compared to those with Fronto-Temporal Dementia and Major Depressive Disorder. However, only a smallto moderate effect size was found when comparing patients with Dementiaof the Alzheimer’s Type and those with Vascular Dementia. Clinically, theseeffect sizes indicate that patients with Dementia of the Alzheimer’s Type canbe expected to perform significantly worse on measures of delayed memorythan patients diagnosed with Fronto-Temporal Dementia or Major DepressiveDisorder. Thus, the use of measures of delayed memory can contributeconsiderably to the differential diagnosis of Dementia of the Alzheimer’s
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1285
Type from that of Fronto-Temporal Dementia or Major Depressive Disorder.In contrast, only a small to moderate difference in performance on delayedmemory measures between Dementia of the Alzheimer’s Type and VascularDementia groups indicates minimal benefit in contributing to the differentialdiagnosis between these disorders.
With regard to the BNT, patients with Dementia of the Alzheimer’s Typeperformed significantly worse than patients diagnosed with Vascular Dementia,Fronto-Temporal Dementia, or Major Depressive Disorder, according todemographically corrected standard scores.
Clinically, these findings suggest that confrontational naming is of limitedbenefit in contributing to the differentiation of Dementia of the Alzheimer’sType from Vascular Dementia. In contrast, Dementia of the Alzheimer’sType patients can be expected to perform significantly worse than patientswith Fronto-Temporal Dementia, and Major Depressive Disorder. Therefore,consideration of this domain may offer great benefit in the differentialdiagnosis of Dementia of the Alzheimer’s Type from that of Fronto-TemporalDementia and Major Depressive Disorder. This finding is consistent withprevious literature, which states that patients with Dementia of the Alzheimer’sType display a clearly progressive anomic aphasia, or difficulty in namingin the context of relatively intact speech fluency, auditory comprehension,articulation, prosody, and repetition (e.g., Cummings & Benson, 1992).Language changes are sensitive indicators of cortical dysfunction, and thedifficulty with confrontational naming found in patients with Dementia ofthe Alzheimer’s Type is indicative of the cortical destruction associated withthe disease. Once again, the lack of significant difference in confrontationalnaming deficits between patients with Dementia of the Alzheimer’s Type andthose diagnosed with Vascular Dementia is likely due to the variability in lesionlocation and the associated unpredictability in deficits common to VascularDementia.
With regard to semantic word fluency as measured by the patients’ abilityto name as many animals as possible within a one minute period, patientsdiagnosed with Dementia of the Alzheimer’s Type performed significantlyworse than patients diagnosed with Vascular Dementia and those diagnosedwith Fronto-Temporal Dementia. However, there was no significant differencebetween the performance of patients diagnosed with Dementia of theAlzheimer’s Type and those diagnosed with Major Depressive Disorder.
The reduced performance of patients with Dementia of the Alzheimer’sType on measures of semantic word fluency is analogous to the languagedifficulties discussed previously. Specifically, studies have shown that the
1286 A. J. BRAATEN ET AL.
first language abnormality to become apparent is the impaired word finding,this anomia leads to circumlocution, which is evidenced in poor word-listgeneration, particularly for words in a given semantic category (Mendez &Cummings, 2003). Literature has also shown that patients with Dementiaof the Alzheimer’s Type have a difficulty accessing semantic informationintentionally, which manifests itself in a manner that appears to reflect a generalsemantic deterioration (Bondi et al., 1996). On the other hand, the decreasedperformance by patients diagnosed with Major Depressive Disorder is likelydue to a lack of volition as presented in the recent literature (i.e., Mendez &Cummings, 2003).
Effect sizes revealed large differences in performance between patientswith Dementia of the Alzheimer’s Type when compared to those withVascular Dementia and Fronto-Temporal Dementia. However, only a smallto moderate effect size was found when comparing patients with Dementia ofthe Alzheimer’s Type and those with Major Depressive Disorder. Clinically,these effect sizes indicate that patients with Dementia of the Alzheimer’s Typecan be expected to perform significantly worse on measures of semantic fluencythan patients diagnosed with Vascular Dementia or Fronto-Temporal Dementia.Thus, the use of measures of semantic fluency can contribute considerably tothe differential diagnosis of Dementia of the Alzheimer’s Type from that ofVascular Dementia and Fronto-Temporal Dementia. In contrast, only a smalldifference in performance on semantic fluency measures between Dementiaof the Alzheimer’s Type and Major Depressive Disorder groups indicatesminimal benefit in contributing to differential diagnosis between Dementiaof the Alzheimer’s Type and Major Depressive Disorder patients, owing to avery substantial overlap in their performances.
Vascular Dementia
With regard to phonemic fluency, patients diagnosed with Vascular Dementiaperformed significantly worse than patients diagnosed with Major DepressiveDisorder and Fronto-Temporal Dementia. However, there was no significantdifference between the performance of patients diagnosed with VascularDementia and those diagnosed with Dementia of the Alzheimer’s Type.These findings are consistent with literature that suggests that patients witha vascular component to their dementia are prone to slowed mental processingand disturbances in executive functioning (Lezak, 1995). Dementia of theAlzheimer’s Type patient’s significantly poorer performance on measures ofphonemic fluency are likely explicated by the previously discussed language
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1287
difficulties associated with the disease, which include word-list generation.Effect sizes comparing Vascular Dementia to Dementia of the Alzheimer’sType revealed a small difference between groups. In contrast, a large effect sizewas found when comparing Vascular Dementia patient’s performance withthat of Fronto-Temporal Dementia patients. Similarly, a large effect size wasdiscovered when comparing Vascular Dementia patients to Major DepressiveDisorder patients. Clinically, this indicates that Vascular Dementia patientscan be expected to perform significantly worse on measures of phonemicfluency when compared to patients with Vascular Dementia or Fronto-TemporalDementia. In addition, this suggests that measures of phonemic fluency suchas the Controlled Oral Word Association Test (COWAT) offer a great benefitin the differential diagnosis between these groups. In contrast, this domainis of minimal benefit in contributing to the differential diagnosis betweenVascular Dementia and Dementia of the Alzheimer’s Type patients, due to avery substantial overlap in their performances.
With regard to immediate memory, patients diagnosed with VascularDementia performed significantly worse than patients diagnosed with MajorDepressive Disorder and Fronto-Temporal Dementia. However, there was nosignificant difference between the performance of patients diagnosed withVascular Dementia and those diagnosed with Dementia of the Alzheimer’sType. According to current literature, patients diagnosed with VascularDementia display deficits in short-term, or immediate, memory abilities due toa dysfunction in memory retrieval in the context of relatively intact memoryrecognition (Lezak, 1995). This deficit has been attributed to impairmentin the initiation of a systematic retrieval strategy when attempting to recallinformation, despite intact memory consolidation in subcortical dementias (e.g.,Bondi et al., 1996). In contrast, patients diagnosed with a cortical dementia suchas Dementia of the Alzheimer’s Type experience difficulty in both the retrievaland recognition of information due to an inability to consolidate informationfor recall (Lezak, 1995).
Effect sizes comparing Vascular Dementia to Dementia of the Alzheimer’sType revealed a moderate difference between groups. Large effect sizes werefound when comparing Vascular Dementia patients’ performance with that ofFronto-Temporal Dementia patients and Major Depressive Disorder patients.Clinically, this indicates that Vascular Dementia patients can be expected toperform significantly worse on measures of immediate memory when comparedto patients with Dementia of the Alzheimer’s Type or Major DepressiveDisorder. In addition, this suggests that measures of immediate memory suchas those within the Wechsler Memory Scale—Third Edition are an asset to
1288 A. J. BRAATEN ET AL.
the differential diagnosis between these groups. In contrast, this domain is ofminimal benefit in contributing to the differential diagnosis between VascularDementia and Dementia of the Alzheimer’s Type patients, due to substantialoverlap in performance.
Fronto-Temporal Dementia
In regard to executive functioning as measured by the Trail-Making Test PartB, patients diagnosed with Fronto-Temporal Dementia received significantlylower scores than patients diagnosed with Vascular Dementia or Major Depres-sive Disorder. However, there was no statistically significant difference betweenpatients diagnosed with Fronto-Temporal Dementia and those diagnosed withDementia of the Alzheimer’s Type. According to previous research, theneuropathological process involved in Fronto-Temporal Dementia affects, asthe name implies, the frontal and temporal lobes. This degeneration of thefrontal and temporal areas is the basis for deficits exhibited on the Trail-MakingTest, including difficulty with shifting set and deficits in attention. Similarly,the disease process indicative of Dementia of the Alzheimer’s Type, discussedearlier, also results in deficits of executive functioning, specifically in the earlystages of the disease course. These deficits include lack of insight, difficultieswith planning and goal-oriented behavior, and poor judgment and reasoning.Other abilities mediated by the frontal lobes and shown to be impaired inpatients diagnosed with Dementia of the Alzheimer’s Type including workingmemory, sustained and divided attention, set changing, response inhibition, andmotor programming (Mendez & Cummings, 2003).
Effect sizes comparing Fronto-Temporal Dementia to Dementia of theAlzheimer’s Type revealed a moderate difference between groups. Largeeffect sizes were found when comparing Fronto-Temporal Dementia patientperformance with that of Vascular Dementia and Major Depressive Disorderpatients. Clinically, this indicates that Fronto-Temporal Dementia patientscan be expected to perform significantly worse on measures of executivefunctioning when compared to patients with Vascular Dementia or MajorDepressive Disorder. In addition, this suggests that measures of executivefunctioning such as the Trail-Making Test Part B can offer a substantial benefitin the differential diagnosis between these groups. In contrast, the Trail-MakingTest is of minimal benefit in contributing to the differential diagnosis betweenFronto-Temporal Dementia and Dementia of the Alzheimer’s Type patients,due to a sizeable overlap in performance.
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1289
In regard to executive functioning as measured by the Stroop Test (specif-ically the color/word segment), patients diagnosed with Fronto-TemporalDementia received significantly lower scores than patients diagnosed withDementia of the Alzheimer’s Type, Vascular Dementia, or Major DepressiveDisorder. Previous research has suggested that performance on the Stroop Test,unlike the Trail-Making Test, is less often reduced by variables other than frontaldeficits, and is less commonly found to be reduced in forms of dementia otherthan Fronto-Temporal Dementia. This clarifies the difference in significancebetween performances on the two, seemingly similar, tests.
Additionally, effect sizes revealed clinically important differences betweengroups. Specifically, large effect sizes were found when comparing theperformance of patients diagnosed with Fronto-Temporal Dementia to thosediagnosed with Dementia of the Alzheimer’s Type, patients with Fronto-Temporal Dementia to those with Vascular Dementia, and patients withFronto-Temporal Dementia compared to those with Major Depressive Disorder.These differences indicate that Fronto-Temporal Dementia patients can beexpected to perform significantly worse on measures of executive functioningwhen compared to patients with Dementia of the Alzheimer’s Type, VascularDementia, or Major Depressive Disorder. In addition, this suggests thatmeasures of executive functioning such as the Stroop Test can offer an importantadvantage in the differential diagnosis among these groups.
Major Depressive Disorder
In regard to attention and concentration skills, as measured by the WechslerMemory Scale—Third Edition, patients diagnosed with Major DepressiveDisorder performed significantly lower than patients diagnosed with VascularDementia. However, there was no significant difference in attention andconcentration skills among Major Depressive Disorder, Dementia of theAlzheimer’s Type, and Fronto-Temporal Dementia patients. These findings arepartially consistent with previous literature, which suggests that abnormalitiesin attention are a common finding in dementia with a subcortical component(Lezak, 1995; Paulsen et al., 1995). Additionally, although it was hypothesizedthat patients diagnosed with Major Depressive Disorder would performsignificantly below patients diagnosed with Dementia of the Alzheimer’sType on tasks measuring attention and concentration, previous literature hasshown that attention and concentration abilities are often impaired in Dementiaof the Alzheimer’s Type, specifically in the early stages of the disease.However, the finding that Major Depressive Disorder patients do not differ
1290 A. J. BRAATEN ET AL.
in attention/concentration performance from patients with Fronto-TemporalDementia is less consistent with previous literature.
Effect sizes indicate a small clinical difference between Major DepressiveDisorder and Dementia of the Alzheimer’s Type patient performance. Addition-ally, a small effect size was found when comparing the performance of MajorDepressive Disorder patients and that of Fronto-Temporal Dementia patients.In contrast, a large effect size was found when comparing Major DepressiveDisorder patient performance to that of Vascular Dementia patient performance.These differences indicate that Major Depressive Disorder patients can beexpected to perform significantly better on measures of immediate memorywhen compared to patients with Vascular Dementia. In addition, this suggeststhat measures of immediate memory such as that the Wechsler MemoryScale—Third Edition, can offer slight assistance in the differential diagnosisbetween patients with Major Depressive Disorder and Vascular Dementia.However, the absence of significant differences between performance ofpatients with Major Depressive Disorder, Dementia of the Alzheimer’s Type,and Fronto-Temporal Dementia indicate minimal contribution to the differentialdiagnosis of these disorders.
Regarding delayed recall, patients diagnosed with Major DepressiveDisorder performed significantly better than patients with Dementia ofthe Alzheimer’s Type. However, patients with Major Depressive Disorderperformed worse on a measure of delayed recall than those diagnosed withFronto-Temporal Dementia. Major Depressive Disorder patients’ performancedid not differ significantly from that of those diagnosed with Vascular Dementia.When considering effect sizes, a large effect size was found when comparingMajor Depressive Disorder to Dementia of the Alzheimer’s Type patientperformance. Similarly, a large effect size was found when comparing patientsdiagnosed with Major Depressive Disorder to those diagnosed with Fronto-Temporal Dementia. However, a small effect size was found between MajorDepressive Disorder and Vascular Dementia patient performance. These effectsizes suggest that when attempting to distinguish Major Depressive Disorderfrom Dementia of the Alzheimer’s Type or Fronto-Temporal Dementia, ameasure of delayed memory, such as that found within the Wechsler MemoryScale—Third Edition is of considerable assistance. However, when attemptingto differentiate Major Depressive Disorder from Vascular Dementia, a measureof delayed memory is of little benefit.
The sample sizes for each diagnostic group consisted of approximately20–30 patients each. This relatively small sample size warrants caution whenan attempt is made to generalize study results to other patients with memory
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1291
complaints or objective neuropsychological impairment. The repetition of thisstudy with the use of larger group sample sizes would strengthen and furtherdefine proposed diagnostic utility. Additionally, the current study does notinclude a control group. Future studies may benefit from utilizing a groupof patients without complaints of memory disturbance. This may facilitateanalyses of confounding factors and the identification and clarification ofsymptoms specific to each dementia type.
It should be noted that participants included in the present study were notadministered measures of symptom validity or effort, as it was not consideredlikely that elderly, nonlitigating, patients with reported memory deficits wereputting forth less than maximum effort. Nevertheless, although there was noclear evidence of insufficient effort in the cases included in the present studyand it is unlikely that insufficient effort was operant, it cannot be stated withabsolute certainty that insufficient effort was not a factor.
A suggested neuropsychological battery for use in the evaluation of de-mentia based on the results of the current study includes measures of executivefunctioning, memory, attention, concentration, intelligence, confrontationalnaming, phonemic fluency, and semantic fluency. Specific tests suggested foruse include the Stroop Test, Wechsler Memory Scale—Third Edition, WechslerAdult Intelligence Scale—Third Edition, Boston Naming Test, Controlled OralWord Association Test, and Category Fluency (i.e., Animal Naming).
REFERENCES
American Psychiatric Association. (2000). Diagnostic and statistical manual of mentaldisorders (4th edn., text revision). Washington, DC: Author.
Barona, A., Reynolds, C. R., & Chastain, R. (1984). A demographically based indexof premorbid intelligence for the WAIS-R. Journal of Consulting and ClinicalPsychology, 52, 885–887.
Baudic, S., Tzortzis, C., Barba, G. D., & Traykov, L. (2004). Executive deficits inelderly patients with major unipolar depression. J. Geriatr. Psychiatry. Neurol., 4,195–201.
Beck, A. (1987). Beck depression inventory. San Antonio, TX: the psychologicalCorporation.
Bondi, M. W., Salmon, D. P., & Kaszniak, A. W. (1996). The neuropsychology ofdementia. In I. Grant. & K. M. Adams (Eds.), Neuropsychological assessmentof neuropsychiatric disorders. (2nd edn.). New York: Oxford, 164–199.
Brun, A., Englund, B., Gustafson, L., Passant, U., Mann, D. M. A., Neary, D., &Snowden, J. S. (1994). Consensus statement. Clinical and neuropathologicalcriteria for frontotemporal dementia. The Lund and Manchester Groups. Journalof Neurology, Neurosurgery, & Psychiatry, 57, 416–418.
1292 A. J. BRAATEN ET AL.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd edn.).Hillsdale, NJ: Lawrence Earlbaum Associates.
Cohen, J. (1990). Things I have learned (so far). American Psychologist, 45, 1304–1312.Cummings, J. L. (Ed). (1990). Subcortical dementia. New York: Oxford University
Press.Cummings, J. L., & Benson, D. F. (1992). Dementia: A clinical approach. (2nd edn.).
Boston, MA: Butterworth-Heinmann.Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). “Mini-mental state”: A
practical method for grading the cognitive sate of patients for the clinician. Journalof Psychiatric Research, 12, 189–198.
Folstein, M. F., Folstein, S. E., McHugh, P. R., & Fanjiang, G. (2001). Mini-mental stateexamination: User’s guide. Odessa, FL: Psychological Assessment Resources, Inc.
Hachinski, V. C., Iliff, L. D., & Zilhka, E. (1975). Cerebral blood flow in dementia.Archives of Neurology, 32, 632–637.
Levy, M. L., Miller, B. L., & Cummings, J. L. (1998). Frontal and frontotemporaldementia. In J. H. Growdon & M. N. Rosser (Eds.), The dementias. Boston, MA:Butterworth-Heinmann, 45–65.
Lezak, M. D. (1995). Neuropsychological assessment. (3rd edn.). New York: Oxford.McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M.
(1984). Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDAWork Group under the auspices of Department of Health and Human Services TaskForce on Alzheimer’s Disease. Neurology, 34, 939–944.
Mendez, M. F., & Cummings, J. L. (2003). Dementia: A clinical approach. (3rd edn.).Boston, MA: Butterworth-Heinemann.
Neary, D., Mann, D., & Snowden, J. (1998). Controversies in the classification of focallobar atrophies. In J. H. Growdon & M. N. Rossor (Eds.), The dementias. Boston,MA: Butterworth-Heinmann.
Neary, D., Snowden, J. S., Gustafson, L., Passant, U., Stuss, D., Black, S., Freedman,M., Kertesz, A., Robert, P. H., Albert, M., Boone, K., Miller, B. L., Cummings,J., & Benson, B. F. (1998). Frontotemporal lobar degeneration: A consensus onclinical diagnostic criteria. Neurology, 51, 1546–1554.
Paulsen, J. S., Butters, N., Sadek, J. R., Johnson, S. A., Salmon, D. P., Swerdlow, N. R.,& Swenson, M. R. (1995). Distinct cognitive profiles of cortical and subcorticaldementia in advanced illness. Neurology, 45, 951–956.
Perez, F. I., Rivera, V. M., Meyer, J. S., Gay, J. R. A., Taylor, R. L., & Mathew, N. T.(1975). Analysis of intellectual and cognitive performance in patients with multi-infarct dementia, vertebrobasilar insufficiency with dementia, and Alzheimer’sdisease. Journal of Neurology, Neurosurgery, & Psychiatry, 38, 533–540.
Roman, G. C., Tatemichi, T. K., Erkinjuntii, T., Cummings, J. L., Masdeu, J. C., Garcia,J. H., Amadocci, L., Orgogozo, J. M., Brun, A., & Hofman, A. (1993). Vasculardementia: Diagnostic criteria for research studies. Report of the NINDS-ADRDAinternational workshop. Neurology, 43, 250–260.
NEUROCOGNITIVE DIFFERENTIAL DIAGNOSIS OF DEMENTIA 1293
Roman, G. C., Sachdev, P., Royall, D. R., Bullock, R. A., Orgogozo, J. M., Lopez-Pousa,S., Arizaga, R., & Wallin, A. (2004). Vascular cognitive disorder: A new diagnosticcategory updating vascular cognitive impairment and vascular dementia. J. Neurol.Sci., 226, 1–2, 81–87.
Rosen, H. J., Hartikainen, K., & Jagust, W. (2002). Utility of clinical criteria indifferentiating frontotemporal degeneration (FTLD) from AD. Neurology, 58,1622–1628.
Storey, E., Slavin, M. J., & Kinsella, G. J. (2002). Patterns of cognitive impairmentin Alzheimer’s disease: Assessment and differential diagnosis. Front Biosci., 7,155–184.
The Psychological Corporation. (2001). Wechsler test of adult reading manual. SanAntonio, TX: Author.
Villardita, C. (1993). Alzheimer’s disease compared with cerebrovascular dementia:Neuropsychological similarities and differences. Acta Neurologica Scandinavica,87, 299–308.
Zakzanis, K. K. (2001). Statistics to tell the truth, the whole truth, and nothing butthe truth: Formulae, illustrative numerical examples, and heuristic interpretationof effect size analyses for neuropsychological researchers. Archives of ClinicalNeuropsychology, 16, 653–667.
Zakzanis, K. K., Leach, L., & Kaplan, E. (1999). Neuropsychological differentialdiagnosis. Netherlands: Swets & Zeitlinger.