VOL 22, NO. 4, 1996 Neuroimaging and the Cognitive Neuroscience of Schizophrenia NIMH Activities by Robert W. McCarley, John K. Hsiao, Robert Freedman, Adolf Pfefferbaum, and Emanuel Donchin Abstract The Carmel Workshop on Cognitive Psychophysiology began in 1980, and the focus of the 1996 workshop was on schizophrenia. Research into schizophrenia is in the midst of a period of unparalleled advance, dri- ven in large part, by improvements in neuroimaging technology that make detailed examination of in vivo brain structure and function possible. Neuroimaging studies may help provide a bridge between investigations demonstrating molec- ular and cellular abnormalities in schizophrenia and those demon- strating cognitive dysfunction. The workshop brought together experts in different neuroimaging modali- ties to present the strengths and advantages of each, as well as the insights each modality might bring into normal and schizophrenic cog- nition. It began with a series of tuto- rials to inform participants of the state of the art in various disci- plines. It then broke into four pan- els, each given a very specific topic assignment related to neuroimaging and/or the cognitive neuroscience of. schizophrenia. After VA days of dis- cussion, each panel reported its con- clusions to the workshop. Croup I presented cellular models of the pathophysiology of schizophrenia. Group II examined experimental paradigms for studying cognitive function and schizophrenia. Croup III examined technical issues in image processing and combining data across different modalities. Group IV sought to survey the cur- rent state of knowledge about the pathophysiology of schizophrenia. The conclusions of each of the groups are presented in this report. Schizophrenia Bulletin, 22(4): 703-725,1996. The field of schizophrenia is now in the midst of unparalleled advances, largely because of new technologies that have made it possible to examine the in vivo brain with functional and structural resolution possible only in animals a decade ago. Furthermore, basic neuroscientists have become interested in the possibility of bridg- ing work at the cellular level with cognitive work, and this trend is now becoming evident in the basic re- search relevant to schizophrenia. The Carmel Conference was designed to bring together experts in the various neuroimaging modalities and in basic neuroscience for sustained interac- tion in focused discussion groups. The following reports of the four dis- cussion groups, compiled and edited by each chairperson, furnish a snap- shot of current activity in the field and offer suggestions for promising future lines of work. Group I. Elementary Neuronal Dysfunction in Schizophrenia Charge and Introduction. The charge to Discussion Group I was to develop a cellular model of the This article represents the proceedings of a workshop held at the Highland Inn in Carmel Valley, California, January 3-7, 1996, sponsored by the Schizophrenia Research Branch, Division of Clinical and Treatment Research, and the Neuroscience Branch of the National Institute of Mental Health. Additional support was received from Janssen Pharmaceuticals, Bristol- Myers Squibb, Eli Lilly Laboratories, Ab- bott Pharmaceuticals, and the Schizo- phrenia Center at Brockton Veterans Affairs Medical Center. Reprint requests should be sent to Dr. R.W. McCarley, Psychiatry 116A, Harvard Medical School/Brockton VA Medical Center, 940 Belmont St., Brockton, MA 02401. Downloaded from https://academic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 December 2021
Transcript
VOL 22, NO. 4, 1996 Neuroimaging and theCognitive Neuroscience ofSchizophrenia
NIMHActivities
by Robert W. McCarley,John K. Hsiao, RobertFreedman, Adolf Pfefferbaum,and Emanuel Donchin
Abstract
The Carmel Workshop on CognitivePsychophysiology began in 1980,and the focus of the 1996 workshopwas on schizophrenia. Research intoschizophrenia is in the midst of aperiod of unparalleled advance, dri-ven in large part, by improvementsin neuroimaging technology thatmake detailed examination of invivo brain structure and functionpossible. Neuroimaging studiesmay help provide a bridge betweeninvestigations demonstrating molec-ular and cellular abnormalities inschizophrenia and those demon-strating cognitive dysfunction. Theworkshop brought together expertsin different neuroimaging modali-ties to present the strengths andadvantages of each, as well as theinsights each modality might bringinto normal and schizophrenic cog-nition. It began with a series of tuto-rials to inform participants of thestate of the art in various disci-plines. It then broke into four pan-els, each given a very specific topicassignment related to neuroimagingand/or the cognitive neuroscience of.schizophrenia. After VA days of dis-cussion, each panel reported its con-clusions to the workshop. Croup Ipresented cellular models of thepathophysiology of schizophrenia.Group II examined experimentalparadigms for studying cognitivefunction and schizophrenia. CroupIII examined technical issues inimage processing and combiningdata across different modalities.Group IV sought to survey the cur-rent state of knowledge about thepathophysiology of schizophrenia.The conclusions of each of thegroups are presented in this report.
Schizophrenia Bulletin, 22(4):703-725,1996.
The field of schizophrenia is now inthe midst of unparalleled advances,largely because of new technologiesthat have made it possible to examinethe in vivo brain with functional andstructural resolution possible only inanimals a decade ago. Furthermore,basic neuroscientists have becomeinterested in the possibility of bridg-ing work at the cellular level withcognitive work, and this trend is nowbecoming evident in the basic re-search relevant to schizophrenia. TheCarmel Conference was designed tobring together experts in the variousneuroimaging modalities and in basicneuroscience for sustained interac-tion in focused discussion groups.The following reports of the four dis-cussion groups, compiled and editedby each chairperson, furnish a snap-shot of current activity in the fieldand offer suggestions for promisingfuture lines of work.
Group I. Elementary NeuronalDysfunction in Schizophrenia
Charge and Introduction. Thecharge to Discussion Group I was todevelop a cellular model of the
This article represents the proceedingsof a workshop held at the Highland Inn inCarmel Valley, California, January 3-7,1996, sponsored by the SchizophreniaResearch Branch, Division of Clinical andTreatment Research, and the NeuroscienceBranch of the National Institute of MentalHealth. Additional support was receivedfrom Janssen Pharmaceuticals, Bristol-Myers Squibb, Eli Lilly Laboratories, Ab-bott Pharmaceuticals, and the Schizo-phrenia Center at Brockton VeteransAffairs Medical Center.
Reprint requests should be sent to Dr.R.W. McCarley, Psychiatry 116A, HarvardMedical School/Brockton VA MedicalCenter, 940 Belmont St., Brockton, MA02401.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
704 SCHIZOPHRENIA BULLETIN
pathophysiology of schizophrenia.The members of the group wereRobert Freedman (chair), ClaudeAlain, Robert Greene, Daniel Javitt,Ann Olincey, John Olney, and LynnSelemon.
Schizophrenia is a disease that im-mediately brings to mind the floridpsychotic symptoms of hallucina-tions and delusions; however, pa-tients with this disease also exhibitan array of more subtle cognitive andperceptual abnormalities, includingmemory disturbances, attentionaldeficits, sensory-gating defects, andeye-movement disorders. Indeed,neuropsychological impairmentforms the core deficit of the diseaseand is largely resistant to treatmentwith standard neuroleptic drugs.Until recently, research on the brainsof schizophrenia patients tended tofocus on one or the other of the neuro-psychological deficits and a singlecortical area that likely mediates thedisturbed function (e.g., frontal cor-tex and memory disturbance). Anewer approach, and one that mayhelp bridge many seemingly un-related areas of research in schizo-phrenia, is to define the basic corticalcircuitry that underlies all these dis-parate functions and look for a com-mon defect at the neuronal level.
The search for specific dysfunc-tions at the cellular level is an at-tempt to find elementary neuronaldeficits that might underlie morecomplex symptoms, such as atten-tional difficulties, or even psychosisitself. Some elementary neuronaldeficits might reflect biological alter-ations in specific synaptic or othermolecules, caused by single geneticmutations. Although there are limita-tions in the study of simple neuronalmechanisms, such as difficulties inrelating them directly to higher brainfunctions, this strategy has signifi-cant advantages as well. For exam-
ple, elementary deficits can be mod-eled at the neuronal and molecularlevels in laboratory animals morereadily than schizophrenia, whichappears to be a uniquely human ill-ness. Clinical validation of the result-ing model of schizophrenia maycome from pharmacological trials,brain-imaging studies, or molecularand genetic investigations. A con-verging theme is the importance ofdefects in the activation of both exci-tatory and inhibitory mechanisms inschizophrenia. While simple inhibi-tion and excitation appear to beintact, modulatory mechanisms thatnormally intensify the activity ofthese basic mechanisms appear defi-cient (figure 1).
Cortical Morphometry. Lynn Sele-mon presented the findings of her
recent morphometric study (Selemonet al. 1995) in which cell-packing den-sity is increased in both prefrontaland occipital cortices. This elevationin neuronal density, found in con-junction with a small decrease in cor-tical thickness, suggests that there isless interneuronal neuropil in thebrain of schizophrenia patients thanin normal controls. Therefore, schizo-phrenia patients may lack the redun-dancy of connections between neu-rons that normal individuals possess.Increase in both nonpyramidal andpyramidal cell density in the pre-frontal cortex indicate that cell loss ingeneral, or of any specific cell class, isnot a pathophysiological correlate ofthe disease. A number of cerebralblood-flow studies have indicatedthat schizophrenia patients are un-able to activate the prefrontal cortex
Figure 1. A model for neuromodulation of cortical pyramidal cells
(from brainstem) DA(-)
alpha 7 nlcotonic
(from thalamus,other cortex)
GABAA / \ Pyramidal cell
GABA (-)
(from basal forebrain)(to other cortex, striatum)Glut (+)
DA = dopamine, D1 = dopamine receptor, Glut = glutamate, NMDA = W-methyl-o-aspartate, GABA =gamma-amino-butyric acid, Ach = acetylcholine.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 705
to perform tasks that are normallymediated by the prefrontal areas(e.g., Weinberger et al. 1986; Buchs-baum et al. 1990; Andreasen et al.1992). At the cellular level, this fail-ure of activation may translate into areduction of synaptic inputs onto thespines of large pyramidal cells. More-over, the fact that abnormally highcell density is not only confined toregions of the brain that mediateworking memory function (i.e., theprefrontal cortex) but is also found ina primary sensory area indicates thatthis relative lack of connectivity maycompromise cortical function globally,leading to the multitude of symptomsassociated with schizophrenia.
Auditory Cortex and Short-TermMemory. Claude Alain pointed outthat patients with schizophreniashow a decrement in the amplitudeof the mismatch negativity (MMN),an event-related potential (ERP) com-ponent that measures early corticalprocessing associated with detectionof deviations in the auditory environ-ment (Javitt et al. 1993; Catts et al.1995). Generation of the MMN de-pends on the ability of the primaryauditory cortex to maintain a mem-ory of the types of stimuli that arepresented and is thought to reflect aneural mismatch between an incom-ing stimulus and the representationof those presented over the previous5 to 10 seconds (Naatanen 1992). Theabnormalities of MMN generation inpatients with schizophrenia raise thepossibility that there might be a fun-damental deficit in auditory short-term memory.
Failure of Pyramidal Neuronal Dis-inhibition. Daniel Javitt, on thebasis of work in a primate model,proposed that failure to activateN-methyl-D-aspartate (NMDA)receptors on cortical pyramidal neu-
rons might be responsible fordecreased activation of corticalcolumns by specific stimuli, so thatsubsequent different or mismatchedstimuli would elicit smaller evokedresponses in schizophrenia subjectsthan in normal subjects. NMDAreceptors are normally maintainedunder tonic inhibition of gamma-amino-butyric acid (GABA)-ergicinterneurons. In order for NMDAreceptors to be activated, theGABAergic interneurons must them-selves be inhibited, leading to disin-hibition of pyramidal neurons.Decreased MMN generation in schiz-ophrenia may reflect a failure of thisdisinhibitory process (Javitt et al.1994).
Alpha-7 Nicotinic Receptor andSensory-Gating Defects. AnnOlincey reported that nicotine nor-malizes two psychophysiologicaldysfunctions in schizophrenia—smooth-pursuit eye-movement gainand a deficit in the inhibition of theP50-evoked response to repeatedauditory stimuli. This pharmacologi-cal effect is consonant with heavysmoking by schizophrenia patientsand points to a possible similarity inthe underlying neurobiological def-icit responsible for these two dys-functions. Using an animal model,Robert Freedman showed howblockade of the alpha-7 nicotinicreceptor, localized to hippocampalinterneurons, causes loss of the in-hibitory gating of response to audi-tory stimuli (Freedman et al. 1994).Support for this nicotinic receptormechanism as a pathophysiologicalelement in sensory-gating deficits inschizophrenia stems from findinglinks from the deficit to polymor-phism at the site of the alpha-7 recep-tor on chromosome 15.
Neuronal Disinhibition and Excito-
toxicity. John Olney proposed thatpsychotomimetic drugs can provideuseful animal models for studyingboth psychopathological and neu-ropathological aspects of schizophre-nia. He showed that NMDA antago-nists, such as phencyclidine (PCP),that trigger psychotic reactions inhumans cause damage to neurons inseveral cortical and limbic areas ofthe rat brain. Using pharmacologicalstrategies to block the neurotoxicreaction has provided insight into thecircuitry and complex receptor mech-anisms that mediate this brain-dam-age syndrome. Blockade of NMDAreceptors inactivates GABA neurons,thereby disinhibiting cholinergic andglutamatergic pathways throughwhich excitotoxic activity is ex-pressed, with consequent damage todendritic spines and cell bodies ofcerebrocortical neurons. The evi-dence suggests that disinhibition ofspecific corticolimbic neural net-works is the basic mechanism under-lying this type of brain damage.Olney and Farber (1995) postulatethat disinhibition of these networksmay also be the basic mechanismresponsible for the psychotomimeticeffects of NMDA antagonists andthat a similar disinhibition processtriggered by a defective function ofthe NMDA transmitter system mightbe viewed as a disease mechanismthat, if operative in schizophrenia,could help explain the cardinal mani-festations of this illness—psychosisand corticolimbic brain changes.Thus, deciphering the circuitry andreceptor mechanisms underlying theneurotoxic action of NMDA antago-nists may lead to a better under-standing of neural networks andtransmitter systems responsible forpsychotic symptoms formation andstructural brain changes in schizo-phrenia.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
706 SCHIZOPHRENIA BULLETIN
Failure of Recurrent Inhibition.Robert Greene, like Dr. Javitt, foundthat NMDA activation was critical.However, in his model, the hippo-campal in vitro slice, the critical func-tion is the NMDA-dependent modu-lation of inhibitory interneurons, justas the modulation of inhibition ap-pears to be the critical target forcholinergic activation in the studiesby Drs. Olincey and Freedman. Witha biophysically realistic model of thehippocampal cornu ammonis (CA)1region, Dr. Greene showed how lessexcitatory modulation of interneu-rons can result in aberrant spread ofexcitation that interferes with learnedpattern recognition, consistent withthe errors of cognition associatedwith schizophrenia.
A Final Common Pathway. Dr.Selemon concluded, in her discus-sion, that cortical circuitry could becompromised at different sites andresult in a similar spectrum of symp-tomatology. For example, deficits ineither the NMDA receptor or alpha-7nicotinic receptor sites on theGABAergic interneuron would resultin impairment in the function of theinhibitory neuron. It is interesting inthis regard that the PCP-mediateddamage to pyramidal dendriticspines in rats, described by Dr. Olney,mimics the neuropathology observedin the brains of schizophrenia pa-tients. Hyperstimulation of theNMDA receptor on the pyramidalcell might damage this cell and inter-fere with the major outflow pathwayof the cerebral cortex. While thecausal factors (genetic, pre- or perina-tal trauma, or overpruning in adoles-cence) leading to a reduction in neu-ropil in the cortex of a schizophreniapatient have not been determined,any mechanism that results in eitheratrophy of dendritic arborization orreduction in excitatory inputs onto
the pyramidal cell would have thesame effect as an excitotoxic lesion atthe NMDA site.
Group II. ExperimentalParadigms for NeuroimagingStudies of Schizophrenia
Charge. Discussion Group II wasinstructed to design the ideal para-digm for functional imaging experi-ments for schizophrenia and includea discussion of possible artifacts andissues of data analysis. The membersof the group were Emanuel Donchin(chair), Jonathan Cohen, Ruben Gur,Brian O'Donnell, Cindy Wible, andDeborah Yurgelin-Todd.
Introduction. In designing an ex-periment one makes predictions, orinspired guesses, as to which of aplethora of choices would yield themost effective design, given the issueone is trying to resolve. The processof designing an experiment is neces-sarily a chaotic give and take: Op-tions are explored and rejected; seem-ingly wonderful ideas fall flat whenexamined closely; gambles are pro-posed and sometimes taken. In theend one has a prospectus for actionthat, until tested in the crucible of thelaboratory, is nothing more than apromissory note. Hence, this groupcannot present the orderly systematicreport generated by the other threegroups. What we can do is describebriefly the process by which thegroup arrived at the experiment itchose to describe in its report, sketchthe paradigm we selected to exam-ine, and briefly list some of the con-clusions that emerged from the dis-cussion.
The exercise was of interest be-cause the group was forced to con-sider the factors that would increasethe probability that the experimentdesigned would in fact be doable,
and that it would address issues thatwould be of either theoretical orpractical significance. As a conse-quence, the group had to translatethe knowledge base and the method-ological issues that were discussedby the other three groups into a set ofdiscrete action messages.
We began with an examination ofthe major assumption underlying ourcharge—namely, that there are issueswithin the schizophrenia domain thatcan be addressed by the methods ofscience and, moreover, that neuro-imaging data could be usefully de-ployed in resolving at least some ofthese theoretical issues. As we re-flected on the nature of the experi-ments that could be designed toaddress these issues, it became evi-dent that a common paradigm wasshared by most of the experimentswe could imagine. The theoreticalissues generate specific predictionsabout the manner in which the pa-tient with schizophrenia processesinformation. With such predictionson hand, two experimental paths areopened.
In a purely exploratory phase, theexperimenters can undertake to con-trol the subject's information proc-essing so that the hypothesized proc-esses are brought under experimentalcontrol. Brain function is then moni-tored and changes in brain functioncorrelated with changes in the con-trolled variables are used as clues tothe spatio-temporal locus of theprocessing. Changes in such activityin the patients show the degree towhich the cognitive deficits can beattributed to specific changes in brainfunction.
A more proactive paradigm be-comes possible if the exploratoryphase can be augmented by informa-tion or models of brain function thatallow predictions about the way thatbrain functions will change as a con-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL 22, NO. 4, 1996 707
sequence of the behavioral manipula-tions. Consider, for example, the re-search strategy that can be employedto elucidate hypotheses about func-tional differences between the twohemispheres of the brain. One canhypothesize, for example, that thereis a processing distinction between,say, holistic and detailed processingtasks. One can present subjects withtasks that are presumed to activateone or another processing mode, thenmeasure any number of electrophysi-ological, or hemodynamic, depend-ent variables, hunting for any mani-festations of the difference betweenthe way the brain handles the tasks.Such explorations are sometimes theonly available strategy. The experi-mental program, however, can mate-rially change and become more fruit-ful if, when designing the studies,one takes into account the structureof the visual pathways and the rela-tionship between the visual fieldstimulated and the hemisphere thatfirst receives (or, in the case of splitbrain subjects, uniquely receives) theinput. By structuring experiments totake advantage of the selective inputpathways, the research program isenormously enriched.
It is very important, however, toemphasize that neuroanatomicalsophistication is not sufficient toensure the success of the researchprogram. No amount of neuro-anatomical sophistication will helpthe study if there is inadequate con-trol over the cognitive aspects of theexperiment. If the theoretical issue isfocused on the relationship betweenthe processing mode and the hemi-spheric loci, the experimenter mustcontrol the processing modes as care-fully as the neuroanatomical vari-ables. This requires close attention tothe "cognitive" aspects of the experi-mental design.
The group noted, as it considered
various experiments, that the con-crete translation of this caveat callsfor the subject to be assigned taskswhose nature can be articulated inthe form of detailed process models.Such models should specify the theo-retical significance of manipulationsand should also generate detailedpredictions about the behavior ofdependent variables such as reactiontime (RT) and error data when thetasks are manipulated.
The group concurred that beforean experiment can be designed,agreement on the issue to be resolvedby the study must be reached. Wespent considerable time examiningvarious assertions, both theoreticaland practical, about schizophrenia,considering in each case the degree towhich the proposition can be trans-lated into empirically testable propo-sitions. It is not difficult to translatealmost all such propositions to adichotomy that asserts that one spe-cific group of individuals differs fromanother group. One can then com-pare the two groups on any numberof measures, be it position emissiontomography (PET), functional mag-netic resonance imaging (fMRI), orERPs, and cataloging the observeddifferences. The group was not per-suaded that such an enterprise is par-ticularly productive, because it leadsto accumulation and cataloging ofdifferences whose significance canrarely be placed in a useful theoreti-cal context. Yet, such empirical ex-plorations do sometimes yieldserendipitous, interesting observa-tions and discoveries. Nonetheless,the group proceeded on the assump-tion that research should be based ontheory.
An Experimental Design. In an at-tempt to design a specific study, wenarrowed our interest to the proposi-tion that one of the deficits in schizo-
phrenia is the failure of a self-moni-toring system. A number of theoristshave attributed the inability of a pa-tient to maintain contact with realityand the display of bizarre mentationand behavior to a failure in the pa-tient's capacity for self-monitoring,which appears to be an importantcomponent of properly functioningcognitive systems. (For referencesregarding models of schizophrenia,see the reports of the other groups.)
This proposition became the foun-dation of our research because datareported in the ERP domain sug-gested that a neural system is acti-vated uniquely when an individualhas committed an error (Falkensteinet al. 1990; Gehring et al. 1993,1995).This error-related negativity (ERN) isillustrated by a negative ERP compo-nent that is time locked to the re-sponse, rather than to the stimulus,and is evoked whenever the subjectchooses to respond with the "wrong"hand in a choice RT study. The ERNseems to vary monotonically with theimportance that the subject assigns toaccuracy. These and other data cur-rently available on the ERN (e.g.,Bernstein et al. 1995; Coles et al. 1995;Scheffers et al. 1996) suggest that theERN is indeed a manifestation of asystem that monitors for errors andtakes action to adjust the subject'soperating characteristics in order toreduce further errors. Dehaene et al.(1994) replicated Gehring et al. (1993)and, using dense array mapping andcomputational localization ap-proaches, concluded that a likelygenerating source for the ERN is theanterior cingulate. Miltner et al. (inpress) reached similar conclusions.
The group decided to design anexperiment that will (1) use fMRI todetermine if systems whose activityis consequent on the execution of anerror can be detected; (2) determinethe extent to which the systems are
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
708 SCHIZOPHRENIA BULLETIN
likely sources for generation of theERN, if such systems are found, and(3) assess both the ERN and the fMRIactivations in patients with schizo-phrenia. This strategy was viewed bythe group as an approach that mightilluminate the degree to which atleast one established self-monitoringneural system varies across diagnos-tic categories of schizophrenia sub-jects.
With this general strategy in mind,the group had to define an experi-mental paradigm that would allowsuch a study and to consider propermethods for selecting subjects. A rareluxury for the group provided by thenature of the exercise was that moneywas no object. Within this frame-work, we proposed a paradigm forselecting subjects that may have beenunrealistic but sketched what weconsidered an ideal process for struc-turing schizophrenia research.
The primary observation drivingthis method of subject selection isthat about half the individuals whofirst present at a clinic with a likelydiagnosis of schizophrenia do not, infact, develop the disease. Our notionis that those "first presenters" whoescape the disease might be an excel-lent control group. Furthermore, webelieve that there is value in longitu-dinal monitoring of the subjects asthe disease process progresses.
Thus, we propose to begin thestudy by identifying a fairly largenumber of first presenters. Ideally,the project should be a multisiteenterprise to recruit a large enoughsample. This entire sample will bestudied 1, 6, and 12 months after ini-tial presentation. Within a year, weassume, about half the sample will bediagnosed with schizophrenia. Asample of the schizophrenia patientswill be identified as the group to befollowed up over an extended pe-riod. This group will probably be
smaller than the total number of firstpresenters who were diagnosed withschizophrenia. A subset of the controlgroup who best match individuals inthe schizophrenia group will be iden-tified. The study will continue andacquire data on a semiannual basis.This general strategy of repeated test-ing was well received by the partici-pants in the Carmel workshop andhas in part been incorporated into thegeneral recommendation of the con-ference in favor of a multisite studythat will apply neuroimaging tech-niques to the study of schizophrenia.
With respect to the paradigm, itseemed clear that we needed a taskthat has been well studied so thatthere would be a solid base of re-ported observations to compare withour current results. The task had togive the subjects a choice betweentwo responses to each of a long seriesof stimuli. The responses were to bethe consequence of a relatively deeplevel of processing, yet such thatschizophrenia subjects could under-take and be willing to perform themover a session lasting at least 2 hours.It was also important that therewould be a substantial percentage ofincorrect responses so that the database for the assessment of the ERNand hemodynamic imaging would beof sufficient size.
The "two-back" paradigm used byCohen and his colleagues seemed tofit the requirements nicely (Cohen etal. 1994; Braver et al. 1995; Casey etal. 1995). In this paradigm the subjectis presented with a list of letters andthe task is to determine if the itemwas presented as the second mostrecent item. Thus, one would re-spond "yes" to the A at the end of thesequence "... C,A,G,A," but "no" tothe A at the end of"... C,G,A,A," or"... A,C,G,A." The subject, obviously,must retain a sequence of at least twoitems in memory and compare each
new item with the first item in thistwo-item buffer. This is not an easytask but, as Jonathan Cohen reportedto the panel, it has been used success-fully in neuroimaging work. Notethat the difficulty of the task can bemodulated by increasing the lengthof the sequence the subject needs toretain (i.e., by running a "three-back"or "four-back" version).
We proposed to first conduct a two-back study in an ERP version to ascer-tain that an ERN is indeed elicited byerrors in this task. If that worked, wewould run a pilot study in patientswith schizophrenia to determine (1) ifthe version of the task that is requiredfor ERP data acquisition is tolerable tothe subjects and (2) if they generate aneven rudimentary ERN. At the sametime, or perhaps as the next stage, wewould begin to study the neuroimag-ing consequences of the commissionof an error in the fMRI setting. This isnot a trivial task: The ERN initializa-tion follows with almost no latencythe appearance of error-related activ-ity in the electromyogram (EMG) ofthe erring hand. It peaks within 100ms of the response, and its total dura-tion is no more than 200 ms. Thegroup discussed various strategies forincreasing fMRI temporal resolution,such as taking a series of closelyspaced echo-planar readings. Thedetails are beyond the scope of thisreport.
Conclusion. The most positiveaspect of our discussion was therecognition that such a multidiscipli-nary discussion that brings togetherpsychiatry, cognitive psychology, andthe study of the electrical activity ofthe brain, as well as the study ofhemodynamic imaging, is feasible. Itis in fact such a combination of ap-proaches that is needed for success inthe enterprise of clinical /cognitiveneuroscience.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL. 22, NO. 4, 1996 709
Group III. CombiningNeuroimaging InformationAcross Modalities and AcrossSubjects
Charge. The charge to DiscussionGroup III was to design the idealmethodology for combining informa-tion across methods (coregistration),across subjects, and for statisticalanalysis. Members of the group wereAdolf Pfefferbaum (chair), RobertBilder, Fred Bookstein, Henry Hol-comb, John Hsiao, Robert Innis,Bruce Turetsky, and Chris Wood.David Silbersweig and Mark Cohenalso contributed.
Introduction. Tremendous ad-vances in digital image processinghave been made over the past dec-ade. Improved spatial and temporalresolution with each generation ofscanners, coupled with exponentialgrowth in computer processor, mem-ory, and storage capacity, now makeit possible to call forth and analyze,at the desktop, images of brain struc-ture and function that even the mostsophisticated neuroimaging centercould not have produced just 10years ago. The pace of change hasbeen such that investigators are asoften paralyzed by the anticipation ofimminent improvements in softwareas they are by the limitations of avail-able image analysis programs.
The traditional focus of clinicalradiology and nuclear medicine hasbeen detecting the presence or ab-sence of "lesions" that separate nor-mal from abnormal. The radiologist'stask is to qualitatively identify over-all patterns of form or function ratherthan quantifying structure or metab-olism in specific regions. As a multi-tude of investigations demonstrate,however, there is no gross anatomic"lesion" that separates patients withschizophrenia from controls, and the
neuroanatomy of the disorder mustbe studied by comparing groups ofsubjects rather than by examiningindividual patients.
Combining Data: General Consider-ations. The need to combine imagesacross modalities derives from therequirement that functional data beinterpreted in the context of struc-tural integrity. In order to betterunderstand brain function, especiallyin disease states, it is important toobtain information about both (1) theabsolute activity in a region of inter-est (ROI) (e.g., the total metabolicactivity in the dorsal lateral pre-frontal cortex) and (2) the functionalactivity per unit volume of brain tis-sue (e.g., the regional metabolic rateper cubic centimeter of gray matter inthe dorsal lateral prefrontal cortex).
The need to combine data acrossindividuals derives from the need totest hypotheses using more than onesubject. This can be accomplished atthe ROI level whenever group statis-tics are used. However, the ability tocombine data across individuals, atthe level of pixel-by-pixel image data,holds forth the potential to apply sig-nal averaging to enhance signal-to-noise ratio. This in turn could lead toexploratory investigations and newdirections for hypothesis testing. Tocreate an average, one must not onlymeasure a brain region, but alsomake sure that the region measuredis the same in all subjects. Fortu-nately, human brains are more or lessalike in structure and functions.Unfortunately, no two brains areexactly alike. Resolution of this ten-sion between the neuroanatomicallysimilar and dissimilar is one of theprimary tasks in analyzing any neu-roimaging data set.
Discussion Group III noted a num-ber of methodological factors thatmust be considered in addressing the
"data-combining task" either acrosssubjects or across modalities.
1. The brain is a large place. Thedata from a high resolution, three-dimensional (3-D), structural mag-netic resonance (MR) scan, with a1 mm voxel resolution, typically isrepresented by 8 million individualnumbers (i.e., 8 megabytes of data).This necessitates large data storageand computer analysis capabilities.There is a real need to consider thewhole brain, because few mentaloperations occur in isolation andeven simple neural circuits mayinvolve many widely distributedregions of the brain. Similarly, thediseases of interest to psychiatryprobably involve multiple brainregions.
2. The resolution of the variousfunctional imaging techniques variesgreatly and presents varying chal-lenges and opportunities for registra-tion. (See table 1.) Many sites rou-tinely obtain better resolution thanpresented in table 1—less than1.0 mm3isotropic voxels with MRIand fMRI voxels of 9 or 10 mm3 cannow be achieved. Table 1 is meant todemonstrate the relative resolution ofthe various techniques as there isimproved resolution with each newgeneration of scanners.
3. Inconsistent findings across lab-oratories for functional imaging stud-ies arise from a number of sources—subject populations, protocol andtask demands, imaging modality,technical acquisition, and analysisdetails. Within an imaging modality,techniques often differ in detail fromlaboratory to laboratory, but they areall based on the same principles, andwith care and a priori agreement,comparable across-laboratory datacan be obtained. However, the under-lying physical/biological mechanism(blood volume, blood flow, glucose
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
710 SCHIZOPHRENIA BULLETIN
Table 1. Spatial resolution of various imaging modalities
Note.—MRI = magnetic resonance imaging, fMRI = functional magnetic resonance imaging, 'H =hydrogen, MRS = magnetic resonance spectroscopy, 3-D = three dimensional, SPECT = singlephoton emission computed tomography, PET = positron emission tomography.
turnover, blood oxygen content) doesdiffer across techniques. There isremarkable agreement in the resultsacross modalities, but this may beserendipitous. Until further compari-son studies are undertaken, across-laboratory collaborative studies willbe strongest when they all employthe same functional imaging tech-nique.
4. Some functional imaging meth-ods lend themselves readily to across-individual comparison (e.g., quanti-tative PET, wherein the absolutemetabolic rate of glucose metabolismis determined). Others are more qual-itative, such as "nonquantitative" or"semiquantitative" PET, where eachpixel as acquired does represent thenumber of counts per unit of time,but the final result is usually ex-pressed relative to the global activityof the brain. The quantitative ap-proach is desirable but requires thedetermination of the arterial inputfunction (usually via insertion of anarterial catheter), and the qualitativeapproach is widely and successfullyused for across-individual compar-isons. Functional MRI data are simi-lar to nonquantitative PET data.
Analytic Approaches.ROI analysis. At their simplest,
flurodeoxyglucose (FDG) and15oxygen-water images can be directlysegmented and metabolism can bemeasured in various ROIs using anadjustable template (e.g., boxes or cir-cles) or by outlining selected areaswithin a scan. Virtually every com-puter platform and operating systemhas software that can be adapted tothis level of analysis. A noncom-mercial program for Macintosh com-puters, NIH Image, was developedand continues to be supported at theNational Institute of Mental Health(available via the World Wide Web-site, at http://rsb. info.nih.gov/ nih-image/). For UNIX platforms, arapidly emerging and widely avail-able standard for display and analysisof neuroimaging data is Analyze,developed at the Mayo Clinic (infor-mation available via the Website athttp://www. mayo.edu/ bir/).
The chief shortcoming of directsegmentation of PET data is the rela-tive lack of anatomical detail in FDGand 15oxygen-water images. Whileone has a rough idea of where an ROIis, the relationship to individual gyriand sulci is not known, as the sameROI from different scans may or maynot be measuring activity in the samebrain regions. A better approach tosegmentation is to use an anatomi-
cally detailed image, such as an MRI,from the same subject to defineregions that are then applied to thePET data. This requires cross-modal-ity alignment of PET and MRI data,and a number of algorithms havebeen developed for reregisteringimaging data from different modali-ties. Early attempts at cross-modalitycoregistration used surface matching(the "hat and head" approach ofChen and Pelizzari [1989]), and a ver-sion of this has been implemented inAnalyze. More recently, cross-correla-tional approaches (minimizing inten-sity differences between data sets)have been developed, and the AIRsuite of image registration programs,developed at the University of Cali-fornia-Los Angeles (UCLA) is com-ing into wide use (available via theWebsite at http://128.97.134.164/AIR/).
Atlas-base analysis. With MRI-guided ROI segmentation, it is possi-ble to accurately and reproduciblymeasure metabolism in small regionsof the brain. ROI segmentation gen-erally requires a good deal of userintervention, however; and observerbias and interrater reliability areimportant issues. Another problemwith any kind of ROI-based imagesegmentation is the loss of spatialresolution that occurs when multiplepixels are collapsed into one ROI.Alternate, atlas-based approaches tosegmentation may avoid some ofthese problems. Atlas-based segmen-tation is predicated on the fact thathuman brains are generally morealike then they are different, and in-volves deformation (warping) ofindividual imaging data into a com-mon, "averaged," coordinate systemor atlas.
Statistical Parametric Mapping(SPM) is a software package for theprocessing and statistical analysis of
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 711
functional neuroimaging data. It wasdiscussed in detail by the group as anexample of atlas-based analysis thatcurrently enjoys considerable (but byno mean unanimous, see below) pop-ularity. SPM includes programs forcoregistration of images acrossmodalities (functional to structural)and for registration across individu-als. It has a number of important pos-itive attributes. It is an evolvingpackage, developed by Karl Fristonand associates at Hammersmith(available via the Website at http://www.fil.ion.bpmf.ac.uk/spm/), andis used internationally by many re-search groups. SPM is a form of"mapping" because it assesseschange at each point in the wholebrain. This is a particularly helpfulway to obtain new information aboutdistributed brain functions and dif-fers from ROI approaches that look inpredefined areas for change. Onceimages are transformed into stan-dardized, coordinate space (Talairachand Tournoux 1988), a wide varietyof statistical operations can be per-formed. These range from t tests tocorrelational analyses or principalcomponent analyses, within or acrossgroups or in single subjects. SPMtakes into account the peak signifi-cance and spatial extent of activa-tions (Friston et al. 1994) that are con-sidered in calculations of p valuesand image resolution and smooth-ness (Worsley et al. 1992) to reducethe Type I error rate.
The analysis of individual subjectscan be useful in assessing the impactof group morphological mappingroutines. Once one has ascertainedthat some change has occurred insome particular place in multiple sin-gle cases, it is then possible to sys-tematically create progressivelylarger groups and monitor the effectof spatial normalization on the groupdata. To the extent that the group has
an activation in the same "place,"and to the extent that the geographyof this "place" is retained in thewarping procedure that creates acommon group anatomical substrate,this activation focus will appear inthe data derived from the groupanalysis (Grabowski et al. 1995).
To the extent that the anatomicalnormalization algorithms provide theinvestigator with a common space,applicable to all subjects, the re-searcher is able to take advantage ofthe data base in building models ofbehavior and pharmacology, forinstance by using regional cerebralblood flow as one of the general out-come measures of various interven-tions. This is extremely helpful inas-much as it aids substantially inhypothesis testing (Horwitz 1994).
Pros and cons of the analyticmethods. Two major concerns tem-per enthusiasm for atlas-based imagesegmentation and analysis methods.The assumption that human brainsare more alike then they are different,while reasonable on the large scale(lobar architecture), is questionable atsmaller scales (e.g., individual gyriand sulci). This may be less of anissue when the spatial resolution of ascan is limited, as with PET or singleproton emission computed tomogra-phy, but application of an atlas ap-proach to MRI data will likely provemore problematic, although not in-tractable. Producing a statisticalimage is attractive on many counts,particularly when the goal of analysisis primarily descriptive. However,the sheer number of elements in anyneuroimage (tens of thousands ofpixels in a single PET scan, millionsin a structural MRI scan) make theusual approaches to hypothesis test-ing and Type I and II error untenable.
Further, function does not alwaysfollow structure. Especially in thecerebral cortex, isomorphic corre-
spondence may not exist across indi-viduals. That is, the surface foldingsof the cortex (i.e., its gyri and sulci)are quite varied from individual toindividual and a "morphing strat-egy" may not be applicable. Corticalsurfaces are as different as faces.
SPM was discussed as an exampleof atlas-based analysis. Members ofthe group disagreed about the seri-ousness of these limitations. How-ever, they did agree that for experi-ments involving more than one sub-ject at a time, the "classic" SPMapproach (pixel-by-pixel or voxel-by-voxel consideration of z-scored dif-ferences, perhaps using the Worsley[Worsley et al. 1992] adjustment forlarger regions) is worthwhile. Thecomputation will often yield a partialdescription of true task effects: a sub-set of the list of pixels at which thereare "true" differences. This is the casewhen (1) there is optimal structuralregistration and (2) either there is nocorrelation between structure andfunction or the correlation betweenstructure and function is accountedfor.
For this purpose, structural regis-tration is by one or another of thecomplete deformation models (Book-stein, in press a, in press b) aligningin principle on every scrap of ana-tomical information that arises ineither a structural or a functionalimage. This registration is geometric,not statistical. Registration by any adhoc method, whether deriving fromthe Talairach tradition (Talairach andTournoux 1988), the Woods tradition(Woods et al. 1992,1993), or anyother approach, is not satisfactory.Optimal registration is particularlyproblematic for the cortex. In addi-tion, even for subcortical structures,if parameters are inadequate, spatialwarping can do more harm thangood. Further, some factors known toinfluence brain structure and func-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
712 SCHIZOPHRENIA BULLETIN
tion, such as age and gender, caneither obscure or interact with dis-ease and need to be "controlled for."
To deal with the correlationbetween structure and function, thedeformation can be simplified (usingone or another a priori basis, thepyramid of displacements of Evans,the partial warps of Bookstein (inpress a, in press b), and the relationbetween structure and function as-sessed (via singular-value decompo-sition of the full cross-covariancematrix of deformation parameters bystandardized voxel contents). Thefunctional image is not "adjusted."Rather, structure can be used as apredictor—as one aspect of any sci-entific report, along with predictionsby task parameters, clinical grouping,or the like.
Conclusion. Regardless of the limi-tations of the present methodologies,the currently available techniques areadequate for many applications, andthey continue to improve. It is impor-tant to the field to proceed with thetools now at hand. In a field that isevolving as rapidly as neuroimaging,one expects today's state of the art tobe tomorrow's commonplace. Asrecently as the early 1980s, it was stillcommon for cranial computed tomo-graphy and even MRI data to bequantified using planimeter measure-ments on x-ray film images. Whilethis methodology would not be ac-ceptable in any modern study, it isworth remembering that most of theconclusions from published reportsusing planimetry remain valid. It willbe surprising if many (or any) of theimage analysis software programsused now will be acceptable 10 yearsfrom now. Nevertheless, what welearn about brain structure and func-tion in schizophrenia using thesemethods will remain valid and willgenerate the hypotheses that will be
tested by the next generation ofimage analysis methods.
Group IV. The Pathophysi-ology of Schizophrenia
Charge. The charge to DiscussionGroup IV was to survey the currentstate of knowledge about the patho-physiology of schizophrenia. Mem-bers of the group were RobertMcCarley (chair), Mark Cohen,Judith Ford, Jeffrey Lieberman, JayPettegrew, Martin Reite, and DavidSilbersweig.
The group reached a strong con-sensus on the following conclusions.In the last decade, considerable prog-ress has been made by neuroimagingstudies in developing evidence forstructural, functional, and molecularchanges in schizophrenia that arerelated to symptomatology. Most ofthe progress has come in cross-sectional assessments, that is, assess-ments at one point in time. Thegroup noted that developing evi-dence concerning the longitudinaltime course of the disorder and itspathophysiology was the mostimportant next step in forming andtesting models of the pathophysiol-ogy of this disorder. Current neu-roimaging tools, with structural MRIcombined with functional measures,offer the possibility of developingsuch a pathophysiology through apremorbid and postmorbid assess-ment of individuals at high risk fordeveloping schizophrenia. A multi-center study appears to offer the bestapproach to implementation of thisplan.
Cross-Sectional PathophysiologicalAssessment. A considerableamount of data links brain abnormal-ities to aspects of the schizophreniasyndrome. The following examples,
not intended to be a complete list,will illustrate some of these relation-ships. One of the clear trends evidentin neuroimaging-based schizophre-nia research is for laboratories toemploy several neuroimaging tech-niques to take advantage of the bestfeatures of each.
Structural MRI. Several impor-tant structural-functional relation-ships have emerged. In general, mor-phologic abnormalities of the medialand superior temporal lobes havebeen associated with the positivesymptoms of schizophrenia psycho-pathology, while negative symptomshave tended to be associated morewith frontal cortical and ventricularsystem abnormalities. The most con-sistently found parenchymal alter-ation has been volume reductionswithin the medial temporal lobe inthe hippocampus and amygdala(Bogerts et al. 1990,1993; Suddath etal. 1990; Shenton et al. 1992). Thesefindings have been more prominentin males and in the left hemisphere inright-handed subjects. Also withinthe temporal lobe, volume reductionsin the anterior portion of the superiortemporal gyrus have been found tobe associated with hallucinations(Barta et al. 1990), while reductions inthe posterior portion, especially onthe left in right-handed subjects, havebeen associated with thought disor-der (Shenton et al. 1992), delusions(O'Donnell et al. 1993), and a left-lat-eralized reduction in amplitude ofthe P300 ERP (McCarley et al. 1993).Since reduction in superior temporalgyrus volume is associated with vol-ume reductions in the neurally linkedmedial temporal zones of hippocam-pus/amygdala and parahippocampalgyrus, these zones may also play arole in the pathophysiology (al-though not having a direct correla-tional relationship); indeed, neu-ropsychological studies have found
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL 22, NO. 4, 1996 713
significant associations between poorscores on tests of verbal memory,abstraction, and categorization andreduced volume in both medial tem-poral lobe and superior temporalgyrus (Nestor et al. 1993). The vol-ume reductions of soft tissue struc-tures are predominantly due todecreased gray matter. In the contextof longitudinal studies, poor treat-ment response and long-term out-come tend to be associated with ven-tricular system abnormalities.
One of the major limitations onstructural MRI is the intensive laborthat is required for manual delin-eation of ROI. Developing automatedprocedures for mapping structuralidentification from an atlas brainonto subject brains is consequentlyone of the highest priority items ofthe field. Robert McCarley presentedpreliminary data showing that anautomated warping procedure hadachieved high congruence with vol-umes derived from manual ROI trac-ing for 10 schizophrenia and 10 con-trol subjects for the thalamus, withmean absolute percentage agreementon volume of 97 percent. Agreementwas also good for overall gray matterand white matter volumes. However,agreement was less on gray/whitematter in individual cortical gyri,where frequent anomalous patternsmade matches much more difficult(see further discussion in the reportby Discussion Group III). Othergroups have developed tools that canwarp the geometry of an individualbrain to a standardized and labeledatlas space, providing a differentalternative to brain segmentation andregion quantification; these includethe Montreal Neurological Institute,the UCLA Brain Mapping Division,and the Research Imaging Center atthe University of Texas Health Sci-ences Center.
Magnetic resonance spectroscopy
(MRS). Over the past 5 years, sev-eral MRS studies in schizophreniahave appeared in the literature,mainly involving phosphorus (31P)MRS and proton ('H) MRS studies.The strength of MRS is its ability tononinvasively obtain molecular andmetabolic information from thebrain. The limitation of MRS is itsspatial resolution, which is approxi-mately a voxel volume of 1 cc for 'HMRS and approximately 8 cc for 31PMRS.
31P MRS studies. A study using31P MRS of brain high-energy phos-phate and membrane phospholipidmetabolism in the dorsal prefrontalcortex of neuroleptic-naive, first-episode schizophrenia patients (Pet-tegrew et al. 1991) showed decreasedlevels of the membrane precursors,phosphomonoesters (PMEs), andincreased levels of membrane break-down products, phosphodiesters(PDEs). These findings have beenreplicated in part by three othergroups examining the frontal lobe(Deicken et al. 1995; Kato et al. 1995;Stanley et al. 1995). These findingsmay reflect a neurodevelopmentallymediated exaggeration of the processof peripubertal synaptic pruning(Feinberg 1982; Pettegrew et al. 1991;Keshavan et al. 1994). Increases inadenosine 5'-triphosphate and reduc-tions in inorganic phosphate, indicat-ing decreased energy utilization,were also found by Pettegrew et al.(1991). There are now several other invivo 31P MRS studies of schizophre-nia patients (Williamson et al. 1991;Fukuzako et al. 1994; Deicken et al.1995; Kato et al. 1995; Stanley et al.1995).
Proton MRS studies. Proton MRSstudies have revealed a fairly consis-tent body of evidence suggestingmetabolic abnormalities in the tem-poral cortex of schizophrenia pa-tients. Most of these studies have
focused on quantification of N-acetylaspartate (NAA), a metabolite essen-tially confined to neurons and henceconsidered to be a neuronal marker(Urenjak et al. 1991). Nasrallah et al.(1994) reported a significant reduc-tion in NAA in the right hippocam-pus/amygdala complex of schizo-phrenia patients. Fukuzako et al.(1994), Maier et al. (1995), and Ren-shaw et al. (1995), have now repli-cated a reduction in NAA in both theright and left temporal lobes of schiz-ophrenia patients. These findings areconsistent with observations of re-ductions in the volume of temporalcortex in schizophrenia patients(McCarley et al. 1993). This metabolicabnormality could be related to re-ductions in the number, density, orvolume of neurons in this brainregion. The NAA reductions couldalso result from loss of neuropil com-posed largely of synapses (whichalso contain NAA) due to an exag-gerated synaptic pruning process dis-cussed above. In general, the meta-bolic alterations in the temporal andfrontal cortex are consistent with asynaptic pruning abnormality andother models (see "LongitudinalPathophysiology" section) of schizo-phrenia pathology.
fMRI. While PET is the currentstandard for high-sensitivity imagingof neural systems throughout theentire brain, the field of fMRI isextremely promising and is advanc-ing rapidly. fMRI is based on ad-vances in MR biophysics and ultra-fast echo-planar imaging techniques.Intrinsic signal changes associatedwith localized neuronal activity aredetected with specialized pulsesequences using T2-weighted blood-oxygen-level-dependent (BOLD) con-trast (Ogawa et al. 1990,1992; Kwonget al. 1992) and, more recently, withTl-weighted time-of-flight tech-niques (Edelman et al. 1994). Regions
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
714 SCHIZOPHRENIA BULLETIN
of increased activity become evidentin time series of such images, appear-ing as areas of MR signal change thatare readily discriminated from back-ground signal variations. The higherresolution and lack of radiation areadvantages of fMRI compared withPET. At present, the chief limitationsof fMRI include difficulties in imag-ing certain regions of the brain, dueto problems of magnetic field homo-geneity; the lack of a resting statemeasure of brain activity; a still-spec-ulative understanding of underlyingphysiology, particularly couplingbetween neuronal activity and MRsignal change through changes inlocal blood flow; and lack of a stan-dardized approach to quantificationof signal changes. Compared withestablished functional imagingmodalities such as PET, fMRI is in itsinfancy, although the results obtainedthus far are in broad agreement withother techniques. The confining andnoisy scanning environment is apotential limitation for some studies.
Preliminary work addressingfrontal lobe function (Callicott et al.1995) and auditory hallucinations inschizophrenia has been reported.Mark Cohen presented data showingfocal areas of increased MR signal inthe superior temporal lobe and infe-rior frontal gyrus during sponta-neously occurring auditory halluci-nations in schizophrenia subjects(Cohen and Green 1995). The mostparsimonious interpretation of theseresults is that they indicate the pres-ence of increased neural activity inreceptive speech areas that may giverise to the perception of auditory hal-lucinations (Cohen and Green 1995).Other fMRI studies are discussed inthe report of Discussion Group II.
PET. PET has been efficacious inexploring the functional neuro-anatomy of schizophrenia. PET tech-niques employ positron-emitting
radiotracers to measure localizedchanges in cerebral blood flow orglucose metabolism associated withfocal neuronal activity, or to measurethe distribution and binding charac-teristics of specific neurochemicalsystems (Phelps 1992). Cross-sec-tional studies of schizophreniapatients have identified neural corre-lates of the three clinical subsyn-dromes of psychomotor poverty, dis-organization, and reality distortion(Liddle et al. 1992). There has beenmuch work concerning the roles ofthe prefrontal cortex and mesolimbicregions in negative symptoms andcognitive deficits (Weinberger et al.1986; Friston et al. 1992; Tamminga etal. 1992; Frith et al. 1995; Gur et al.1995). Twin studies (Berman et al.1992), work on the central effects ofneuroleptic medication (Buchsbaumet al. 1992), and pharmacologic chal-lenges (Dolan et al. 1995) and radioli-gand studies (Andreasen et al. 1988)of neurochemistry have also beenperformed. Recently, the neural cor-relates of specific positive symptomssuch as hallucinations have beenidentified (Silbersweig et al. 1995).This work employed new methods(Silbersweig et al. 1994) that detectbrain areas in which measured activ-ity (reflecting regional cerebral bloodflow, an index of neuronal activity)over many repeated scans correlateshighly with a calculation of radio-tracer input during the target symp-tom.
The results of these schizophreniaPET studies implicate functional ab-normalities of prefrontal and supe-rior temporal association cortices,parahippocampal and anterior cingu-late paralimbic cortices, limbic struc-tures such as the hippocampus, andsubcortical regions such as the thala-mus and ventral striatum. These dis-tributed systems are responsible forthe integration of higher-order per-
ception, cognition, emotion, and be-havior. The demonstration of func-tional abnormalities in these systemsis consistent with and extends anato-mical and cytoarchitectonic studies ofschizophrenia to date. The chief limi-tations of PET are its use of ionizingradiation, which limits repeat stud-ies, and a spatial resolution less thanthat of MRI techniques.
Electrophysiology, ERPs. ERPs, alow-cost functional brain-imagingtechnique having a millisecond tem-poral resolution, outperforms otherfMRI and PET functional imagingtechniques in temporal resolution.The major limitation of ERPs is poorspatial resolution; current work onstructural MRI-derived realistic mod-els of head geometry and conduc-tance is thus extremely important,since this will allow much better spa-tial resolution. ERPs can be elicitedby the presence or absence of a stim-ulus; they can be elicited by a stimu-lus that is attended or ignored; andthey can be recorded preceding, dur-ing, or following an overt movement.The different components of the ERPreflect a range of sensory, cognitive,and motor brain activities. The P300component of the ERP is primarily acognitive component. Its amplitudereflects the amount of resources allo-cated to a task, and its latency reflectshow long it takes to allocate them.P300 has been extensively studied inschizophrenia, and its reduction inamplitude is one of the most replica-ble biological observations of the dis-order. Its amplitude is limited by cor-tical gray matter volumes (McCarleyet al. 1993; Ford et al., in press) and issensitive to the trait and state of thedisorder Puncan et al. 1987; Ford etal. 1995). Judith Ford presented pre-liminary data suggesting that P300amplitude further decreases with dis-ease duration. Its latency is delayedwith age more in patients with schiz-
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 715
ophrenia than in normal controls(O'Donnell et al. 1995).
Magnetoencephalography (MEG).Magnetic fields produced by neu-ronal activity are less influenced byintervening tissues of varying con-ductivity (brain tissue, cerebrospinalfluid, bone, skin) than are electricalfields, permitting a greater degree ofspatial resolution for selected sourcesthan is possible with conventionalsurface electroencephalogram (EEG)recordings. Certain source geome-tries are selectively emphasized inMEG recordings, particularly thoseneuronal arrays whose currents aretangential to the surface of the head,whereas EEG is selectively more sen-sitive to radially oriented sources.During the last several years, MEGrecording technology has improvedconsiderably with the availability ofmultichannel instruments, includingwhole-head arrays. The increasingcomplexity of the instrumentationleads to concerns about how varyingsensor geometry (ranging from mag-netometers, through first-, second-,and third-order gradiometers, tomultichannel planar array systems)may influence the nature of therecorded brain activity. It is hopedthat answers to such questions willsoon be forthcoming. Currently themajor limitations of MEG-based con-tributions to our understanding ofschizophrenia are the very high costof new MEG instrumentation and theconsequent severely limited avail-ability of MEG recording sites. Theselimitations compromise the ability toreplicate and extend findings.
In male paranoid schizophreniapatients, the expected interhemi-spheric asymmetry of M100 superiortemporal gyrus sources (right hemi-sphere more anterior than left hemi-sphere) was not present (Reite et al.1995), a finding replicated in males,but not in females. Martin Reite pre-
sented unpublished data indicatingthat normal subjects demonstratedsignificant magnetic alpha suppres-sion over both left and right hemi-sphere recording points following aprobe tone while memory scanningwas taking place (Sternberg task).However, males with paranoid schiz-ophrenia failed to demonstrate alphasuppression over the left hemisphere,but did suppress over the right hemi-sphere. Since their performance (i.e.,their ability to judge the probe toneas included or not) was not signifi-cantly different from normals, thepresumptive left hemisphere deficitmight have been compensated for byright hemisphere or other mecha-nisms. Other paradigms, such asinvestigating the echoic trace, areunder active current investigation.Thus, while relatively little has yetbeen published on MEG-based tech-niques applied to schizophrenia dis-orders, the existing studies suggestthat MEG is a useful technology,especially when combined withstructural MRI for source localiza-tion.
Longitudinal Pathophysiology.The major models for the longitudi-nal time course of schizophrenia arepurely neurodevelopmental events(genetically programmed, infections,etc.) and the "two-hit" model, withprogression of pathology after theonset of symptoms. Although recog-nizing that the issue remains unset-tled, a strong consensus of the dis-cussion was that the two-hit modelwas more likely. This consensus wasechoed by the full conference mem-bership during Discussion GroupIV's plenary presentation. All atten-dees recognized that this controver-sial and very important issue couldbe definitively addressed only bylongitudinal data on individuals pre-onset and postonset of the disorder.
Findings in first-episode patients,while of great value, do not resolvethe issue of whether the changesobserved have been present andfixed since early development or arepartially or completely the productof additional changes antecedent tofirst-episode data collection. Severalmonths or even years may haveelapsed between first-episode datacollection and the onset of symp-toms. The following data, not meantto be a comprehensive list, supportthe two-hit model.
First hit—neurodevelopmental.Evidence includes temporal lobesulco-gyral patterns that are formedin the third trimester of gestation andpattern abnormalities in schizophre-nia patients that have been reportedboth by postmortem studies (Jacoband Beckmann 1986) and by in vivoMRI studies (e.g., Kikinis et al. 1994).Some schizophrenia patients exhibita cavum septum pellucidum, repre-senting a failure to fuse two laminarmembranes, an event usually occur-ring in the third trimester of gesta-tion. This neurodevelopmentalanomaly has been associated withpoorer treatment response and out-come (Degreef et al. 1992). The rarecase reports of preonset ventricularenlargement may represent a usuallyundetected but generalized finding,or they may be quite atypical in thatnegative findings have not beenreported. MRS alterations in phos-pholipid metabolites similar to thoseobserved in schizophrenia (decreasedPME, increased PDE) were seen in acontrol subject who was studied 2years before her first psychoticepisode (Keshavan et al. 1991).
While preonset data are sparse,there are now an increasing numberof reports of changes detectable atthe onset of the first psychoticepisode, and if one includes abstractreports, these include almost the full
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
716 SCHIZOPHRENIA BULLETIN
spectrum of MRI-volume abnormali-ties reported in chronic schizophreniapatients including MRI-volume in-creases and asymmetry alterations ofthe ventricular system, volume re-ductions in hippocampus/amygdala(perhaps the most constant finding)and the superior temporal gyrus, andasymmetry alterations in prefrontalcortex.
Second hit—Ongoing changesafter onset of symptoms. The ini-tial data from longitudinal structuralMRI studies suggest that neuro-pathology progresses over the earlyphases of the illness. Preliminarydata presented by Raquel Gur indi-cate progressive reductions in tempo-ral and frontal lobe volumes in fol-lowup MRI scans done 32 monthsafter the initial scan of first-episodepatients. Jeffrey Lieberman reportedsimilar changes in those first-episodepatients who experienced a poor out-come and extended periods of psy-chosis. This is consistent with differ-ences in the prevalence and severityof ventricular enlargement andmesiotemporal volume reductionsobserved cross-sectionally betweenfirst-episode and chronic schizophre-nia patients (Bogerts et al. 1990,1993;Lieberman et al. 1992). O'Donnell etal. (1995) found, in a cross-sectionalsample, trend-level differences be-tween the greater rate of age-relateddecline in volume of superior tempo-ral gyrus in schizophrenia patientsthan in controls. Similarly, there is apreliminary report, in a first-episodepopulation, of volume reduction ofsuperior temporal gyrus correlatingwith duration of illness (Haas et al.1995). Attempts to determine themechanisms underlying the structuraland molecular changes in schizophre-nia should take into consideration thequestion of which changes are relatedto the proposed second hit and whichare secondary to medications. Longi-
tudinal studies have demonstratedthat enlargement of the basal ganglianuclei found in chronic schizophreniapatients are most likely the result ofthe effects of conventional antipsy-chotic drug treatment and not due toinnate disease pathophysiology(Chakos et al. 1994).
Cross-sectional P300 data indicatethat P300 latency is more delayedwith age in schizophrenia patientsthan is expected with normal aging(O'Donnell et al. 1995); this finding iscompatible with a neurodegenerativehypothesis. Judith Ford presenteddata confirming this finding and alsosuggesting, in a cross-sectional sam-ple, that P300 amplitude may be sen-sitive to how long a patient has beensick. Stanley et al. (1995) showed thatPMEs were reduced in both newlydiagnosed and chronic patients, butthe PDE elevations were seen only inthe first-episode cases, suggestingthat the PME reductions may be traitmarkers, while the PDE changes mayreflect state-related phenomena. JayPettegrew reported that, in an ongo-ing study using a prospective longi-tudinal followup design, PME reduc-tions appear to persist, even withneuroleptic treatment. However, thequestion remains unclear whetherthe membrane phospholipid abnor-malities in schizophrenia progress.
Spectrum disorder abnormalitiesin schizophrenia. The preliminaryevidence for neurobehavioral, P300(Salisbury et al. 1996), PET (Siegel etal. 1994), and structural MRI ab-normalities in schizotypal personal-ity disorder may represent the effectsof the first hit without the second hit.
Possible causative agents andmechanisms for postonset changes.There are now a number of models ofneurotoxic mechanisms that couldaccount for the postonset alterations.Most involve NMDA receptor-medi-ated mechanisms, with many of the
possible cellular mechanisms ad-dressed in the report of DiscussionGroup I. The models include freeradical or secondary metabolite toxic-ity (Wyatt 1991) and endogenousneurochemical sensitization (Grace1993). A set of mechanistically similarmodels involves failure of neuronalinhibition with resulting overactivityin excitatory amino acid neurotrans-mission, leading to processing abnor-malities and, in some cases, to excito-toxicity The Discussion Group Ireport discusses the NMDA receptorhypofunction model of John Olneyand a related model postulating fail-ure of recurrent inhibition, secondaryto GABAergic neuronal loss and/orNMDA blockade by endogenoussubstances, such as N-acetyl-L-aspartyl-glutamate (Grunze et al.1996). Finally, Dr. Pettegrew pointedout that altered PMEs might affectNMDA neurotransmission. L-phos-phoserine, one of the PMEs, has aclose structural similarity to L-gluta-mate and is a competitive antagonistat NMDA and kainate receptor sites(Klunk et al. 1991). This PME couldserve as a physiologically relevantantagonist at the NMDA receptorsites. A disease-related reduction inthis metabolite, therefore, could con-tribute to increased glutamatergicneurotransmission, perhaps con-tributing to postschizophrenia onsetneurotoxicity. L-phosphoserine alsoinitially reduces and then enhancesthe population of excitatory post-synaptic potentials in rat hippo-campal CA1 pyramidal cells (Bradleret al. 1991).
Current status of longitudinaldata. While a plausible case can bemade for postonset alterations, themajor problem for developing amodel of longitudinal pathophysiol-ogy is that there is no clear evidenceon when the structural and func-tional alterations occur in the course
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 717
of schizophrenia. There was a strongconsensus that obtaining such data isthe major current priority in develop-ing a data-based pathophysiology ofschizophrenia. The therapeutic andpublic health implications of whetherthere is an ongoing process of neuro-degeneration following symptom on-set are clear: If such a process existsand can be arrested or amelioratedby medication, then it becomes ex-tremely important to have early in-tervention following the onset ofsymptoms.
In order to investigate the patho-genic factors and the pathophysio-logical course of schizophrenia, it ap-pears essential to have a prospectivestudy of subjects before and follow-ing the onset of illness. This ap-proach, although scientifically opti-mal, is unfortunately logisticallycomplex. First, it requires identifyingan appropriate target population andfollowing subjects for extended peri-ods of time. The most informativecandidate groups would be high-risksubjects still within the age of risk.One candidate group would includefirst-degree relatives of schizophreniapatients, and another would bemonozygotic twins discordant forschizophrenia with the well twin stillwithin the age of risk.
Although limitations of space pre-vent discussion of all the complexissues related to selection of individ-uals likely to become ill with schizo-phrenia, a brief sketch of the consid-erations can be presented. In theRoscommon study, Kendler et al.(1993) estimated a 6.5 percent lifetimerisk for first-degree relatives of pro-bands to develop schizophrenia. It ispossible to increase the probabilityby selecting for certain, easily deter-minable traits. For example, eye-tracking disorder is about twice asfrequent in schizophrenia probandsas in first-degree relatives (see review
by Levy et al. 1994; recent data arefrom a personal communication fromthese authors to Dr. McCarley), and itis thus likely that, by choosing onlyeye-tracking disorder-positive sub-jects, one could double the probabil-ity of studying a subject who laterlikely would become ill with schizo-phrenia. Thus, to obtain 20 subjectswho would become ill with schizo-phrenia, it would be necessary tostudy 150 high-risk subjects. Withmonozygotic twins, the probability ofthe cotwin of the proband becomingill with schizophrenia is about one-half, but identification of the twinproband may be difficult and thenumber of potential subjects rela-tively small. In both subject groups,duration of the study relative to theduration of a maximal risk period forthe subjects is also considered.
Expense and cost-benefit consider-ations of recruiting many subjectswho would not later become ill withschizophrenia should also take intoaccount the opportunity to surveythe previously largely unknownbrain "endophenotype" of relativesof patients with schizophrenia, a use-ful feature in understanding the gen-tics of the disorder. Also to be con-sidered is the possibility of a jointproject with a genetic component,collecting blood from the families ofthe probands for linkage analysis.
Given the paucity of such high-risksubjects, a multicenter study wouldbe necessary to ascertain an adequatesample. Since neuroimaging wouldbe an important assessment modality,the issue of feasibility of a multicen-ter imaging study is raised. Althoughthe problems in establishing uni-formity and standardization of meth-ods across sites are considerable, thecurrent state of the technology andthe research methodology are suchthat a multisite imaging study doesappear feasible. To give one neu-
roimaging example, a multicenterstudy could achieve uniformity instructural MRI, the neuroanatomicaltechnique of choice, by using identi-cal scanner versions and softwarethroughout the study. Scanner per-formance would be validated andcalibrated on phantoms and volun-teers on a regular basis throughoutthe study, as systematic alterations inperformance may bias the data. Thestructural data would be obtained atthe highest spatial and contrast reso-lution consistent with realistic single-subject imaging times of about 45minutes and include images thatspan a range of MR contrast mecha-nisms (Tl, T2, proton density, diffu-sion, etc.) to augment the value ofthis data set for retrospective analy-sis. These MRI data would be anextremely valuable research resourceand, after taking suitable steps toprotect anonymity, should be madeavailable to the research communitythrough electronic network inter-faces.
The study design for either or bothhigh-risk target populations wouldinvolve finding subjects and charac-terizing them by multiple measuresof assessment, including psycho-pathology as well as brain morphol-ogy and functional assessment atstudy entry and at regular time inter-vals (clinical followup annually andneuroimaging followup at 2-3 years).A critical outcome event would bethe onset of illness in previously wellsubjects, at which time they would beextensively characterized with theassessment measures and followedthereafter. The issue of which func-tional measures to use is a complexone with cost-benefit tradeoffs. ERPs,fMRI, and MRS have the advantageof not using ionizing radiation andare thus desirable for young subjects(< 18 years). One possible way to fol-low up on the consensus suggestion
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
718 SCHIZOPHRENIA BULLETIN
of a prospective study of high-riskindividuals would be to convene aworking group to explore the feasi-bility and cost-benefit desirability inmore detail.
References
Andreasen, N.C.; Carson, R.; Diksic,M.; Evans, A.; Farde, L.; Gjedde, A.;Hakim, A.; Lai, S.; Nair, N.; Sedvall,G.; Tune, L.E.; and Wong, D. Work-shop on schizophrenia, PET, anddopamine D2 receptors in the humanneostriatum. Schizophrenia Bulletin,14(3):471- 484,1988.
Andreasen, N.C.; Rezai, K.; Alliger,R.; Swayze, V.W. II; Flaum, M; Kirch-ner, P.; Cohen G.; and O'Leary, D.S.Hypofrontality in neuroleptic-naivepatients and in patients with chronicschizophrenia: Assessment withXenon 133 single-photon emissioncomputer tomography and the Towerof London. Archives of General Psychi-atry, 49(12):943-958,1992.Barta, P.E.; Pearlson, G.D.; Powers,R.E.; Richards, S.S.; and Tune, L.E.Auditory hallucinations and smallersuperior temporal gyral volume inschizophrenia. American Journal ofPsychiatry, 147:1457-1462,1990.
Berman, K.F.; Torrey, E.F.; Daniel,D.G.; and Weinberger, D.R. Regionalcerebral blood flow in monozygotictwins discordant and concordant forschizophrenia. Archives of GeneralPsychiatry, 49(12):927-934,1992.Bernstein, P.S.; Scheffers, M.K.; andColes, M.G.H. "Where did I gowrong?" A psychophysiologicalanalysis of error detection. Journal ofExperimental Psychology: Human Per-ception and Performance, 21:1312-1322,1995.
Bogerts, B.; Ashtari, M.; Degreef, G.;Alvir, J.M.; Bilder, R.M.; and Lieber-man, J.A. Reduced temporal limbic
structure volumes on magnetic reso-nance images in first episode schizo-phrenia. Psychiatry Research, 35:1-13,1990.
Bogerts, B.; Lieberman, J.A.; Ashtari,M.; Bilder, R.; Degreef, G.; Lerner, G.;Johns, C; and Masiar, S. Hippo-campus-amygdala volumes andpsychopathology in chronic schizo-phrenia. Biological Psychiatry,33:236-246,1993.
Bookstein, F.L. Biometrics and brainmaps: The promise of the morpho-metric synthesis. In: Koslow, S., andHuerta, M., eds. Neuroinformatics: AnOverview of the Human Brain Project.Progress in Neuroinformatics. Vol. I.Hillsdale, NJ: Lawrence ErlbaumAssociates, in press a.
Bookstein, F.L. Biometrics, biomathe-matics, and the morphometric syn-thesis. Bulletin of Mathematical Biology,in press b.
Bradler, J.E.; Barrionuevo, G.; Pan-chalingam, K.; McKeag, D.; andPettegrew, J. W. Actions of phospho-monoesters on CA1 hippocampalneurons as revealed by a combinedelectrophysiological and nuclearmagnetic resonance study. Synapse,9:7-13,1991.
Braver, T.S.; Cohen, J.D.; Jonides, J.;Smith, E.E.; Awh, E.; Schumacher, E.;Lauber, E.; and Noll, D.C. A paramet-ric study of prefrontal cortex involve-ment in human working memory us-ing functional MRI. [Abstract] Societyof Neuroscience Abstracts, 21:274,1995.
Buchsbaum, M.S.; Nuechterlein,K.H.; Haier, R.J.; Wu, J.; Sicotte, N.;Hazlett, E.; Asarnow, R.; Potkin, S.;and Guich, S. Glucose metabolic ratein normals and schizophrenics duringthe Continuous Performance Test as-sessed by positron emission tomogra-phy. British Journal of Psychiatry,156:216-227,1990.
Buchsbaum, M.S.; Potkin, S.G.; Mar-
shall, J.F.; Lottenberg, S.; Teng, C;Heh, C.W.; Tafalla, R.; Reynolds, C;Abel, L.; Plon, L.; and Bunney, W.E.Effects of clozapine and thiothixeneon glucose metabolic rate in schizo-phrenia. Neuropsychopharmacology,6(3):155-163,1992.
Callicott, J.; Ramsey, N.; Tallent, K.;Bertolino, A.; Coppola, R.; Goldberg,T; Knable, M.; Mattay, V.; vanGelderen, P.; Moonen, C; and Wein-berger, D. "3-D fMRI of a WorkingMemory Task in Schizophrenia." Pre-sented at the 34th Annual Meeting ofthe American College of Neuro-psychopharmacology, San Juan, PR,December 1995.
Casey, B.J.; Cohen, J.D.; Jezzard, P.;Turner, R.; Noll, D.C; Trainor, R.;Giedd, J.; Pannier, L.; Kaysen, D.; andRapoport, J.L. Activation of the pre-frontal cortex in children during anon-spatial working memory taskwith functional MRI. Neuroimaging,2:221-229,1995.
Catts, S.V.; Shelley, A.M.; Ward, P.B.;Leibert, B.; McConaghy, N.; Andrews,S.; and Mitchie, P.T. Brain potentialevidence for an auditory sensorymemory deficit in schizophrenia.American Journal of Psychiatry,152:213-219,1995.
Chakos, M.H.; Lieberman, J. A.;Bilder, R.M.; Borenstein, M.; Lerner,G.; Bogerts, B.; Wu, H.; Kinon, B.; andAshtari, M. Increase in caudate nucleivolumes of first-episode schizo-phrenic patients taking antipsychoticdrugs. American Journal of Psychiatry,151:1430-1436,1994.
Chen, G.T., and Pelizzari, C.A. Imagecorrelation techniques in radiationtherapy treatment planning. Comput-erized Medical Imaging and Graphics,13(3):235-240,1989.
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 719
frontal cortex in a non-spatial work-ing memory task with functftmalMRI. Human Brain Mapping, 1:293—304,1994.
Cohen, M.S., and Green, M. "Wherethe Voices Come From: Imaging theSchizophrenic Auditory Hallucina-tions." Presented at the 25th AnnualMeeting of the Society for Neuro-science Abstracts, San Diego, CA,October 1995.Coles, M.G.H.; Scheffers, M.K.; andFournier, L. Where did you gowrong? Errors, partial errors, and thenature of human information proc-essing. Ada Psychologica, 90:129-144,1995.
Degreef, G.; Lantos, G.; Bogerts, B.;Ashtari, M.; and Lieberman, J.A. Ab-normalities of the septum pelluci-dum on MRI scans in first episodeschizophrenic patients. Americanjournal of' Neuroradiology, 13:835-840,1992.
Dehaene, S.; Posner, M.I.; and Tucker,D.M. Commentary: Localization of aneural system for error detectionand compensation. Psychological Sci-ence, 5:303-305,1994.Deicken, R.F.; Errin, E.L.; Floyd, T.C.;and Weiner, M.C. Correlation be-tween left frontal phospholipids andWisconsin Card Sort Test perfor-mance in schizophrenia. SchizophreniaResearch, 14:177-181,1995.Dolan, R.J.; Fletcher, P.; Frith, CD.;Friston, K.J.; Frackowiak, R.S.J.; andGrasby, P.M. Dopaminergic modula-tion of impaired cognitive activationin the anterior cingulate cortex inschizophrenia. Nature, 378:180-182,1995.
Duncan, C.C.; Morihisa, J.M.; Faw-cett, R.W.; and Kirch, D.G. P300 inschizophrenia: State or trait marker?Psychopharmacology Bulletin, 23(3):497-501,1987.
Edelman, R.R.; Sievert, B.; Wielopolski,
P.; Pearlman, J.; and Warach, F. "Non-Invasive Mapping of Cerebral Perfu-sion by Using EPISTAR MR Angiog-raphy." [Abstract] Presented at theMeeting of the Society of MagneticResonance, February 1994.
Falkenstein, M.; Hohnsbein, J.; Hoor-mann, J.; and Blanke, L. Effects oferrors in choice reaction tasks on theERP under focused and divided at-tention. In: Brunia, C.H.M.; Gaillard,A.W.K.; and Kok, A., eds. Psychophys-iological Brain Research. Tilburg, TheNetherlands: Tilburg UniversityPress, 1990. pp. 192-195.Feinberg, I. Schizophrenia: Causedby a fault in programmed synapticelimination during adolescence? jour-nal of Psychiatric Research, 17(4):319-334,1982.Ford, J.M.; Mathalon, D.H.; and Pfef-ferbaum, A. P300 amplitude tracksclinical status in schizophrenic pa-tients. Biological Psychiatry, 37:671-672,1995.
Ford, J.M.; Mathalon, D.H.; Sullivan,E.V.; Lim, K.O.; and Pfefferbaum, A.Effects of cortical gray matter, atten-tion, and schizophrenia on P300amplitude. Recent advances in event-related brain potential research. Pro-ceedings of the Xlth International Con-ference on Event-Related Potentials ofthe Brain (EPIC XI). Okinawa, Japan,in press.
Friston, K.J.; Liddle, P.F.; Frith, CD.;Hirsch, S.R.; and Frackowiak, R.S.J.The left medial temporal region andschizophrenia. A PET study. Brain,115(Part 2):367-382,1992.
Friston, K.J.; Worsley, K.J.; Frack-owiak, R.S.J.; and Evans, A.C Assess-ing the significance of focal activationsusing their spatial extent. HumanBrain Mapping, 1:210-220,1994.
Frith, CD.; Friston, K.J.; Herold, S.;Silbersweig, D.; Fletcher, P.; Cahill,C; Dolan, R.J.; Frackowiak, R.S.J.;and Liddle, P.F. Regional brain activ-ity in chronic schizophrenic patientsduring the performance of a verbalfluency task. British journal of Psychia-try, 167:343-349,1995.
Fukuzako, H.; Takeuchi, K.; Ueyama,K.; Fukuzako, T.; Hokazono, Y;Hirakawa, K.; Yamada, K.;Hashiguchi, T; Takigawa, M.; andFujimoto, T. 31P magnetic resonancespectroscopy of the medial temporallobe of schizophrenic patients withneuroleptic-resistant marked positivesymptoms. European Archives of Psy-chiatry and Clinical Neuroscience,244:236-240,1994.
Gehring, W.J.; Coles, M.G.H.; Don-chin, E.; and Meyer, D.E. A brainpotential manifestation of error-related processing. In: Karmos, G.;Molnar, M.; Csepe, V; Czigler, I.; andDesmedt, J.E., eds. Perspectives ofEvent-Related Potentials Research-Amsterdam, The Netherlands:Elsevier Science Publishers, 1995.pp. 287-296.
Gehring, W.J.; Goss, B.; Coles, M.G.H.;Meyer, D.E.; and Donchin, E. A neuralsystem for error-detection and com-pensation. Psychological Science, 4:385-390,1993.
Grabowski, T.J.; Damasio, H.; Frank,R.J.; Brown, C.K.; Boles Ponto, L.L.;Watkins, G.L.; and Hichwa, R.D.Neuroanatomical analysis of func-tional brain images: Validation andretinotopic mapping. Human BrainMapping, 2:134-148,1995.
Grace, A.A. Cortical regulation ofsubcortical dopamine systems and its
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
720 SCHIZOPHRENIA BULLETIN
possible relevance to schizophrenia.Journal of Neural Transmission, 91:111—134,1993.Grunze, H.C.R.; Rainnie, D.G.; Has-selmo, M.E.; Barkal, E.; Hearn, E.F.;McCarley, R.W.; and Greene, R.W.NMDA-dependent modulation ofCAl local circuit inhibition. Journal ofNeuroscience, 16:2034-2043,1996.
Gur, R.E.; Mozley, P.D.; Resnick, S.M.;Mozley, L.H.; Shtasel, D.L.; Gallacher,R; Arnold, S.E.; Karp, J.S.; Alavi, A.;Reivich, M.; and Gur, R.C. Restingcerebral glucose metabolism in first-episode and previously treated pa-tients with schizophrenia relates toclinical features. Archives of GeneralPsychiatry, 52(8):657-667,1995.Haas, G.L.; Keshaven, M.S.; Schooler,N.R.; Bagwell, W.W.; and Pettegrew,J.W. "Temporal Cortical Volume Cor-relates With Illness Duration in First-Episode Schizophrenia." Presented atthe 34th Annual Meeting of theAmerican College of Neuropsycho-pharmacology, San Juan, PR, Decem-ber 1995.Horwitz, B. Data analysis paradigmsfor metabolic-flow data, combiningneural modeling and functional neu-roimaging. Human Brain Mapping,2:112-122,1994.
Jacob, H., and Beckmann, H. Prenataldevelopmental disturbances in thelimbic allocortex in schizophrenia.Journal of Neural Transmission, 65:303-326,1986.
Javitt, D.C.; Doneshka, P.; Nussen-zweig, I.Z.; Ritter, W.; and Vaughan,H.G., Jr. Impairment of early corticalprocessing in schizophrenia: Anevent-related potential confirmationstudy. Biological Psychiatry, 33:513-519,1993.
Javitt, D.C.; Schroeder, C.E.; Sten-schneider, M.; Zrezzo, J.C.; Ritter, W.;and Vaughan, H.G., Jr. Cognitiveevent-related potentials in human
and non-human primates: Implica-tions for the PCP/NMDA model ofschizophrenia. Electroencephalographyand Clinical Neurophysiology,44(Suppl.):161-175,1994.
Kato, T; Shioiri, T; Murashita, J.;Hamakawa, H.; Inubushi, T.; andTakahashi, S. Lateralized abnormalityof high-energy phosphate and bilat-eral reduction of phosphomonoestermeasured by phosphorus-31 mag-netic resonance spectroscopy of thefrontal lobes in schizophrenia. Psychi-atry Research, 61:151-160,1995.
Kendler, K.S.; McGuire, M; Gruen-berg, A.M.; O'Hare, A.; Spellman, M.;and Walsh, D. The Roscommon Fam-ily Study: I. Methods, diagnosis ofprobands, and risk of schizophreniain relatives. Archives of General Psychi-atry, 50:527-540,1993.
Keshavan M.S.; Anderson, S.; andPettegrew, J.W. Is schizophrenia dueto excessive synaptic pruning in theprefrontal cortex? Journal of Psychi-atric Research, 28:239-265,1994.Keshavan, M.S.; Pettegrew, J.W.; Pan-chalingam, K.; Kaplan D.B.; andBozik, E. Phosphorus 31 magneticresonance spectroscopy detectsaltered brain metabolism beforeonset of schizophrenia. Archives ofGeneral Psychiatry, 48:1112-1113,1991.
Kikinis, R.; Shenton, M.E.; Gerig, G.;Hokama, H.; Haimson, J.; O'Donnell,B.F.; Wible, C.G.; McCarley, R.W.; andJolesz, F. A. Temporal lobe sulcal-gyralpattern anomalies in schizophrenia:An in vivo MRI three-dimensionalsurface rendering study. [Letter]Neuroscience Letters, 182:7,1994.
Klunk, W.E.; McClure, R.J.; and Pette-grew, J.W. Possible roles of L-phos-phoserine in the pathogenesis ofAlzheimer's disease. Molecular Chem-ical Neuropathology, 15:51-73,1991.
Poncelet, B.P.; Kennedy, D.N.; Hop-pel, B.E.; Cohen, M.S.; Turner, R.;Cheng, H.M.; Brady, T.J.; and Rosen,B.R. Dynamic magnetic resonanceimaging of human brain activity dur-ing primary sensory stimulation. Pro-ceedings of the National Academy of Sci-ences of the United States of America,89(12)5675-5679,1992.
Levy, D.L.; Holzman, P.S.; Matthysse,S.; and Mendell, N.R. Eye trackingand schizophrenia: A selective re-view. Schizophrenia Bulletin, 20(l):47-62,1994.
Liddle, P.F.; Friston, K.J.; Frith, CD.;Hirsch, S.R.; Jones, T; and Frack-owiak, R.S.J. Patterns of cerebralblood flow in schizophrenia. BritishJournal of Psychiatry, 160:179-186,1992.Lieberman, J.A.; Bogerts, B.; Degreef,G.; Ashtari, M.; and Alvir, J. Qualita-tive assessment of brain morphologyin acute and chronic schizophrenia.American Journal of Psychiatry, 149(6):784-794,1992.
Maier, M.; Ron, M.A.; Barker, G.J.;and Tofts, P.S. Proton magnetic reso-nance spectroscopy: An in vivomethod of estimating hippocampalneuronal depletion in schizophrenia.Psychological Medicine, 25:1201-1209,1995.
McCarley, R.W.; Shenton, M.E.;O'Donnell, B.F.; Faux, S.F.; Kikinis, R.;Nestor, P.G.; and Jolesz, F.A. AuditoryP300 abnormalities and left posteriorsuperior temporal gyrus volume re-duction in schizophrenia. Archives ofGeneral Psychiatry, 50:190-197,1993.
Miltner, W.H.R.; Braun, C.H.; andColes, M.G.H. Event-related poten-tials following incorrect feedback in atime-estimation task: Evidence for a"generic" neural system for errordetection. Journal of Cognitive Neuro-science, in press.
Naatanen, R. Attentio>i and BrainFunction. Hillsdale, NJ: Lawrence
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL. 22, NO. 4, 1996 721
Erlbaum Associates, 1992.Nasrallah, H.A.; Skinner, T.E.;Schmalbrock, P.; and Robitaille, P.M.Proton magnetic resonance spec-troscopy (1H MRS) of the hippo-campal formation in schizophrenia:A pilot study. British Journal of Psychi-atry, 165:481^185,1994.
Nestor, P.G.; Shenton, M.E.; McCarley,R.W.; Haimson, J.; Smith, R.S.;O'Donnell, B.F.; Kimble, M.O.;Kikinis, R.; and Jolesz, F. A. Neuro-psychological correlates of MRItemporal lobe abnormalities in schiz-ophrenia. American Journal of Psychia-try, 150(12):1849-1855,1993.,
O'Donnell, B.F.; Faux, S.F.; McCarley,R.W.; Kimble, M.O.; Salisbury, D.F.;Nestor, P.G.; Kikinis, R.; Jolesz, F.A.;and Shenton, M.E. Increased rate ofP300 latency prolongation with age inschizophrenia: Electrophysiologicalevidence for a neurodegenerativeprocess. Archives of General Psychiatry,52:544-549,1995.
O'Donnell, B.F.; Shenton, M.E.;McCarley, R.W.; Faux, S.F.; Smith,R.S.; Salisbury, D.F.; Nestor, P.G.; Pol-lak, S.D.; Kikinis, R.; and Jolesz, F.A.The auditory N2 component in schiz-ophrenia: Relationship to MRI tempo-ral lobe gray matter and to other ERPabnormalities. Biological Psychiatry,34:26-40,1993.
Ogawa, S.; Lee, T.M.; Kay, A.R.; andTank, D.W. Brain magnetic resonanceimaging with contrast dependent onblood oxygenation. Proceedings of theNational Academy of Sciences of theUnited States of America, 87:9868-9872,1990.
Ogawa, S.; Tank, D.W.; Menon, R.;Ellermann, J.M.; Kim, S.G.; Merkle,H.; and Ugurbil, K. Intrinsic signalchanges accompanying sensory stim-ulation: Functional brain mappingwith magnetic resonance imaging.Proceedings of the National Academy ofSciences of the United States of America,
89(13):5951-5955,1992. .Olney, J.W., and Farber, N.B. Gluta-mate receptor dysfunction and schiz-ophrenia. Archives of General Psychia-try, 52:998-1007,1995.
Pettegrew, J.W.; Keshavan, M.S.; Pan-chalingam, K.; Strychor, S.; Kaplan,D.B.; Tretta, M.G.; and Allen, M. Al-terations in brain high-energy phos-phate and phospholipid metabolismin first episode, drug-naive schizo-phrenia: A pilot study of the dorsalprefrontal cortex by in vivo 31P NMRspectroscopy. Archives of General Psy-chiatry, 48:563-568,1991.
Phelps, M.E. Positron emissiontomography (PET). In: Mazziotta,J.C., and Gilman, S., eds. Cliitical BrainImaging: Principles and Applications.Philadelphia, PA: F.A. Davis Com-pany, 1992. pp. 71-107.
Reite, M.; Sheeder, J.; Teale, P.;Richardson, D.; Adams, M.; andSimon, J. MEG-based brain laterality:Sex differences in normal adults. Neu-ropsychologia, 33:1607-1616,1995.
Renshaw, PR; Yurgelin-Todd, D.A.;Tohen, M.; Gruber, S.; and Cohen,B.M. Temporal lobe proton magneticresonance spectroscopy of patientswith first-episode psychosis. AmericanJournal of Psychiatry, 152:444-446,1995.
Salisbury, D.F.; Voglmaier, M.V.; Seid-man, L.J.; and McCarley, R.W. Topo-graphic abnormalities of P3 in schizo-typal personality disorder. BiologicalPsychiatry, 40:165-172,1996.
Scheffers, M.K.; Coles, M.G.H.; Bern-stein, P.; Gehring, W.J.; and Donchin,E. Event-related brain potentials anderror-related processing: An analysisof incorrect response to Go and No-Go stimuli. Psychophysiology, 33:42-53,1996.
Selemon, L.D.; Rajkowsak, G.; andGoldman-Rakic, P.S. Abnormally highneuronal density in the schizophreniccortex: A morphometric study of pre-frontal area 9 and occipital area 17.
Archives of General Psychiatry, 52:805—818,1995.Shenton, M.E.; Kikinis, R.; Jolesz, F.A.;Pollak, S.D.; LeMay, M.; Wible, C.G.;Hokama, H.; Martin, J.; Metcalf, D.;Coleman, M.; and McCarley, R.W.Abnormalities of the left temporallobe and thought disorder in schizo-phrenia: A quantitative magnetic res-onance imaging study. New EnglandJournal of Medicine, 327:604-612,1992.
Siegel, B.V.; Siever, L.; Trestman, R.L.;and Buchsbaum, M.S. "RegionalBrain Glucose Metabolism in Schizo-typal Personality Disorder." Pre-sented at the 33rd Annual Meeting ofthe American College of Neuropsy-chopharmacology, San Juan, PR,December 1994.
Silbersweig, D.A.; Stern, E.; Frith, C;Cahill, C; Holmes, A.; Grootoonk, S.;Seaward, J.; McKenna, P.; Chua, S.E.;Schnorr, L.; Jones, T; and Frackowiak,R.S.J. A functional neuroanatomy ofhallucinations in schizophrenia.Nature, 378:176-179,1995.
Silbersweig, D.A.; Stern, E.; Schnorr,L; Frith, CD.; Ashburner, J.; Cahill,C; Frackowiak, R.S.J.; and Jones, T.Imaging transient randomly occur-ring neuropsychological events in sin-gle subjects with positron emissiontomography: An event-related countrate correlational analysis. Journal ofCerebral Blood Flow and Metabolism,14:771-782,1994.
Stanley, J.A.; Williamson, PC; Drost,D.J.; Carr, T.J.; Rylett, J.; Malla, A.; andThompson, R.T. An in vivo study ofthe prefrontal cortex of schizophrenicpatients at different stages of illnessvia phosphorus magnetic resonancespectroscopy. Archives of General Psy-chiatry, 52:399^106,1995.
Suddath, R.L.; Christison, G.W.; Tor-rey, E.F.; Casanova, M.F.; and Wein-berger, D.R. Anatomical abnormali-ties in the brains of monozygotictwins discordant for schizophrenia.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
722 SCHIZOPHRENIA BULLETIN
New England journal of Medicine,322:789-794,1990.Talairach, J., and Tournoux, P., eds.Co-planar Stereotaxic Atlas of theHuman Brain: 3-Dimensiondl Propor-tional System: An Approach to CerebralImaging. Stuttgart, Germany: ThiemeMedical Publishers, 1988.
Tamminga, C.A.; Thaker, G.K.;Buchanan, R.; Kirkpatrick, B.; Alphs,L.D.; Chase, T.N.; and Carpenter,W.T., Jr. Limbic system abnormalitiesidentified in schizophrenia usingpositron emission tomography withfluorodeoxyglucose and neocorticalalterations with deficit syndrome.Archives of General Psychiatry,49(7):522-530,1992.
Urenjak, ].; Noble, M.; Williams, S.R.;and Gadian, D.G. N-acetyl aspartate:Re-evaluation of its specificity as aneuronal marker in 1H NMR spec-troscopy. [Abstract] Society for Mag-netic Resonance in Medicine, 1:420,1991.
Williamson, P.; Drost, D.; Stanley, J.;Carr, T; Morrison, S.; and Merskey,H. Localized phosphorus31 magneticresonance spectroscopy in chronicschizophrenic patients and normalcontrols. [Letter] Archives of GeneralPsychiatry, 48:578,1991.
Woods, R.P.; Cherry, S.R.; and Maz-ziotta, J.C. Rapid automated algo-rithm for aligning and reslicing PETimages. Journal of Computer AssistedTomography, 16(4):620-633,1992.
Worsley, K.J.; Evans, A.C.; Marrett, S.;and Neelan, P. A three-dimensionalstatistical analysis for CBF activationstudies in human brain, journal ofCerebral Blood Flow and Metabolism,12:900-918,1992.
Wyatt, R.J. Neuroleptics and the nat-ural course of schizophrenia. Schizo-phrenia Bulletin, 17(2):325-351,1991.
Additional Readings
Andreasen, N.C.; Arndt, S.; Swayze,V.; Cizadlo, T; Flaum, M.; O'Leary,D.; Ehrhardt, J.C; and Yuh, W.T.Thalamic abnormalities in schizo-phrenia visualized through magneticresonance image averaging. Science,266(5183):294-298,1994.
Cannon, T.D.; Mednick, S.A.; Parnas,J.; Schulsinger, F.; Praestholm, J.; andVestergard, A. Developmental brainabnormalities in the offspring ofschizophrenic mothers: II. Structuralbrain characteristics of schizophreniaand schizotypal personality disorder.Archives of General Psychiatry, 51:955-962,1994.Chen, E.Y.H.; Wilkins, A.J.; andMcKenna, P.J. Semantic memory isboth impaired and anomalous inschizophrenia. Psychological Medicine,24:193-202,1994.
Clare, L.; McKenna, P.J.; Mortimer,A.M.; and Baddeley, A.D. Memory inschizophrenia: What is impaired andwhat is preserved? Neuropsychologia,31:1225-1241,1993.
Clementz, B.A.; Sweeney, J.A.; Hirt,M.; and Haas, G. Pursuit gain andsaccadic intrusions in first-degree rel-atives of probands with schizophre-nia, journal of Abnormal Psychology,99:327-335,1990.Cornblatt, B.A., and Keilp, J.G.Impaired attention, genetics, and thepathophysiology of schizophrenia.
Schizophrenia Bulletin, 20(l):31^3,1994.
Davis, K.L.; Kahn, R.S.; Ko, G.; andDavidson, M. Dopamine in schizo-phrenia: A review and reconceptual-ization. American Journal of Psychiatry,148(11):1474-1486,1991.
Degreef, G.; Ashtari, M.; Wu, H.;Borenstien, M.; Geisler, S.; andLieberman, J.A. Follow-up MRIstudy in first episode schizophrenia.Schizophrenia Research, 5:204—206,1991.
Degreef, G.; Bogerts, B.; Falkai, P.;Greve, B.; Lantos, G.; Ashtari, M.;and Lieberman, J.A. Increased prev-alence of the cavum septum pellu-cidum in MRI scans and post mortembrains of schizophrenic patients. Psy-chiatry Research: Neuroimaging, 45:1-13,1992.
Degreef, G.; Lantos, G.; Bogerts, B.;Ashtari, M.; and Lieberman, J.A.Abnormalities of the septum pellu-cidum on MR scans in first-episodeschizophrenic patients. AmericanJournal of Neuroradiology, 13(3):835-840,1992.
Eidelberg, D.; Moeller, J.R.; Dhawan,V.; Spetsieris, P.; Takikawa, S.;Ishikawa, T.; Chaly, T.; Robeson, W.;Margouleff, D.; and Przedborski, S.The metabolic topography of parkin-sonism. journal of Cerebral Blood Flowand Metabolism, 14(5):783-801,1994.
Erlenmeyer-Kimling, L., and Corn-blatt, B. High-risk research in schizo-phrenia: A summary of what hasbeen learned. Psychiatry Research,21(4):401^11,1987.Friston, K.J. The dorsolateral pre-frontal cortex, schizophrenia andPET. journal of Neural Transmission,37(Suppl.):79-93,1992.Friston, K.J.; Dolan, R.J.; and Frack-owiak, R.S.J. Statistical ParametricMapping. London, England: MRC
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL. 22, NO. 4, 1996 723
Cyclotron Unit, Hammersmith Hos-pital, 1991.Friston, K.J.; Holmes, A.P.; Worsley,K.J.; Poline, J.P.; Frith, CD.; andFrackowiak, R.S.J. Statistical para-metric maps in functional imaging: Ageneral linear approach. Human BrainMapping, 2:189-210,1995.Goldberg, T.E.; Torrey, E.F.; Gold,J.M.; Ragland, J.D.; Bigelow, L.B.; andWeinberger, D.R. Learning and mem-ory in monozygotic twins discordantfor schizophrenia, Psychological Medi-cine, 23:71-85, 1993.
Gur, R. "Temporal Lobe VolumetricChanges in a Longitudinal Study ofPatients With Schizophrenia." Pre-sented at the 34th Annual Meeting ofthe American College of Neuropsy-chopharmacology, San Juan, PR,December 1995.
Kalivas, P.W. Neurotransmitter regu-lation of dopamine neurons in theventral tegmental area. Brain ResearchReviews, 18(1):75-113,1993.
Kaufman, L.; Curtis, S.; Wang, J.Z.;and Williamson, S.J. Changes in corti-cal activity when subjects scan mem-ory for tones. Electroencephalographyand Clinical Neurophysiology, 82:266-284,1992.
Kennedy, A.M.; Frackowiak, R.S.J.;Newman, S.K.; Bloomfield, P.M.; Sea-ward, J.; Roques, P.; Lewington, G.;Cunningham, V.J.; and Rossor, M.N.Deficits in cerebral glucose metabo-lism demonstrated by positron emis-sion tomography in individuals at riskof familial Alzheimer's disease. Neuro-science Letters, 186(l):17-20,1995.
571:91-100,1995.Keshavan, M.S.; Pettegrew, J.W.; andWard, R. Are membrane changes inschizophrenia familial? [Abstract]Biological Psychiatry, 33:45,1993.
Lieberman, J. A.; Alvir, J.M.; Koreen,A.; Geisler, S.; Chakos, M.; Sheitman,B.; and Woerner, M. Psychobiologiccorrelates of treatment response inschizophrenia. Neuropsychopharmacol-ogy, in press.
Linnville, S.; Teale, P.T.; Scheuneman,D.L.; Goldstein, L.; and Reite, M.A.Preliminary report on selective atten-tion differences in the Ml 00 in schiz-ophrenic and normal adult males.Neuropsychiatry and Clinical Neuro-sciences, 7:92-95,1995.
Lu, Z.L.; Williamson, S.J.; and Kauf-man, L. Behavioral lifetime of humanauditory sensory memory predictedby physiological measures. Science,258:1668-1670,1992.
Poline, J.P.; Worsley, K.J.; Holmes,A.P.; Frackowiak, R.S.J.; and Friston,K.J. Estimating smoothness in statis-tical parametric maps: Variability ofp values. Journal of Computer AssistedTomography, 19(5):788-796,1995.
Reite, M.; Teale, P.; Goldstein, L.;Whalen, J.; and Linnville, S. Lateauditory magnetic sources may differin the left hemisphere of schizo-phrenic patients: A preliminary re-port. Archives of General Psychiatry,46:565-572,1989.
Reite, M.; Teale, P.; Sheeder, J.; Rojas,D.; and Schneider, E.E. MEG evi-dence of abnormal early auditorymemory function in schizophrenia.Biological Psychiatry, in press.
Rosen, B.; Belliveau, J.W.; and Chien,D. Perfusion imaging by nuclearmagnetic resonance. Magnetic Reso-nance Quarterly, 5(4):263-281, 1989.
Saykin, A.J.; Shtasel, D.L.; Gur, R.E.;Kester, D.B.; Mozley, L.H.; Stafiniak,P.; and Gur, R.C. Neuropsychologicaldeficits in neuroleptic naive patientswith first-episode schizophrenia.Archives of General Psychiatry, 51:124-131,1994.
Talairach, J.; Szikla, G.; Tournoux, P.;Prosalentis, A.; Bordas-Ferrier, M.;Covello, L.; Iacob, M.; and Mempel, E.Atlas d'Anatomie Stereotaxique du Telen-cephale. Paris, France: Masson, 1967.
Waddington, J.L., and Lieberman,J.A. New insights into clinical issuesin schizophrenia. Journal of Psycho-pharmacology, 8:65-66,1994.
Weinberger, D.R. Implications of nor-mal brain development for the patho-genesis of schizophrenia. Archives ofGeneral Psychiatry, 44:660-669,1987.
The Authors
Robert W McCarley, M.D., is Profes-sor of Psychiatry, Harvard MedicalSchool/Brockton Veterans AffairsMedical Center, Brockton, MA. JohnK. Hsiao, M.D., is Chief, Neuroimag-ing Program and Acting Chief, Schiz-ophrenia Research Branch, Divisionof Clinical and Treatment Research,National Institute of Mental Health,Rockville, MD. Robert Freedman,M.D., is Professor of Psychiatry, Uni-versity of Colorado Health SciencesCenter, Denver, CO. Adolf Pfeffer-baum, M.D., is Professor, Psychiatryand Behavioral Sciences, StanfordUniversity School of Medicine andChief, Psychiatry Research, Palo AltoVeterans Affairs Medical Center, PaloAlto, CA. Emanuel Donchin, Ph.D., isProfessor of Psychology, Universityof Illinois, Champaign, IL.
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
724 SCHIZOPHRENIA BULLETIN
List ofParticipants
The Carmel Workshops on CognitivePsychophysiology were launched in1980 with the support of the SloanFoundation, within the framework ofthe Foundation's interest in fosteringthe development of the field of cogni-tive neuroscience. The meetings wereconceived as a framework for bring-ing together leading investigatorswhose primary research tool was theevent-related potential (ERP) andleading researchers in a domain ofresearch to which the study of ERPscould contribute or in a domain ofresearch that could provide informa-tion that would shape the study ofERPs. The workshops were designedfor a small number of participants, 20or so from each of the two disci-plines, and always begin with aseries of tutorials intended to informeach group of the state of the art inthe other discipline. The workshopthen breaks into four panels, eachgiven a very specific set of queriesrelated to the main topic of the work-shop. After a day and a half of dis-cussion in the breakout groups, theworkshop reassembles for discussionof the panel reports, with each panelassigned a 4-hour reporting session.
The format has proven very suc-cessful. The first meeting focused ona general review of the relationshipbetween cognitive psychology andpsychophysiology (see Donchin, E.,ed. Cognitive Psychophysiology: Event-Related Potentials and the Study of Cog-nition, The Carmel Conferences, Vol. 1.Hillsdale, NJ: Lawrence ErlbaumAssociates, 1984). Subsequent meet-ings reviewed language processes,human factors, aging, and so on. Themeetings were held until 1990 at theLa Playa Hotel in Carmel, California,and since then at the Highland Inn inCarmel Valley, the site of the meetingthat is the subject of this report. Onemeeting, supported by the Rocke-
feller Foundation and devoted to thephilosophical implications of ERPresearch, was held in Bellagio, Italy.When the initial Sloan grant periodcame to an end, the meetings contin-ued with support from the NationalInstitute of Mental Health, NationalAeronautics and Space Administra-tion, the Office of Navy Research,and Air Force Office of ScientificResearch.
Invited speakers, listed in order oftheir talks, included Drs. Nancy C.Andreasen (Keynote Address), LynnSelemon, Emanuel Donchin, BruceRosen, Chris Wood, Robert W.McCarley, Jay Pettegrew, Fred Book-stein, Raquel Gur, Robert Innis, andRuben Gur.
Claude Alain, Ph.D.University of CaliforniaDavis Martinez Veterans Affairs
Medical CenterNancy C. Andreasen, M.D., Ph.D.University of Iowa.Robert M. Bilder, Ph.D.Albert Einstein College of MedicineHillside HospitalFred Bookstein, Ph.D.University of MichiganJonathan D. Cohen, M.D., Ph.D.University of PittsburghWestern Psychiatric Institute and
Clinic
Mark S. Cohen, Ph.D.University of California, Los AngelesEmanuel Donchin, Ph.D.University of IllinoisJudith M. Ford, Ph.D.Stanford UniversityPalo Alto Veterans Affairs Medical
Center
Robert Freedman, M.D.University of Colorado School of
MedicineDenver Veterans Affairs Medical
Center
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
ecember 2021
VOL22.NO. 4, 1996 725
Robert Greene, M.D., Ph.D.Harvard UniversityBrockton/West Roxbury Veterans
Affairs Medical Center
Raquel Gur, M.D., Ph.D.University of Pennsylvania
Ruben Gur, Ph.D.University of PennsylvaniaHenry Holcomb, M.D.University of MarylandJohn K. Hsiao, M.D.National Institute of Mental HealthRobert Innis, M.D., Ph.D.Yale UniversityConnecticut Veterans Affairs Medical
Center
Daniel C. Javitt, M.D., Ph.D.Albert Einstein College of Medicine
Jeffrey A. Lieberman, M.D.Albert Einstein College of MedicineHillside Hospital
Robert W. McCarley, M.D.Harvard University
Brockton/West Roxbury VeteransAffairs Medical Center
Brian F. O'Donnell, Ph.D.Harvard UniversityBrockton/West Roxbury Veterans
Affairs Medical Center
Ann Olincey, M.D.University of ColoradoDenver Veterans Affairs Medical
Center
John W. Olney, M.D.Washington University School of
Medicine
Jay Pettegrew, M.D.University of Pittsburgh
Adolf Pfefferbaum, M.D.Stanford UniversityPalo Alto Veterans Affairs Medical
Center
Martin L. Reite, M.D.University of ColoradoDenver Veterans Affairs Medical
Center
Bruce Rosen, M.D., Ph.D.Harvard UniversityMassachusetts General HospitalWalton T. Roth, M.D.Stanford UniversityPalo Alto Veterans Affairs Medical
CenterLynn Selemon, Ph.D.Yale University School of MedicineDavid A. Silbersweig, M.D.Cornell UniversityNew York Hospital Cornell Medical
CenterBruce Turetsky, M.D.University of PennsylvaniaCindy Wible, Ph.D.Harvard UniversityBrockton/West Roxbury Veterans
Affairs Medical CenterChris Wood, Ph.D.Los Alamos National LaboratoryDeborah Yurgelin-Todd, Ph.D.Harvard UniversityMcLean Hospital
Dow
nloaded from https://academ
ic.oup.com/schizophreniabulletin/article/22/4/703/1939066 by guest on 27 D
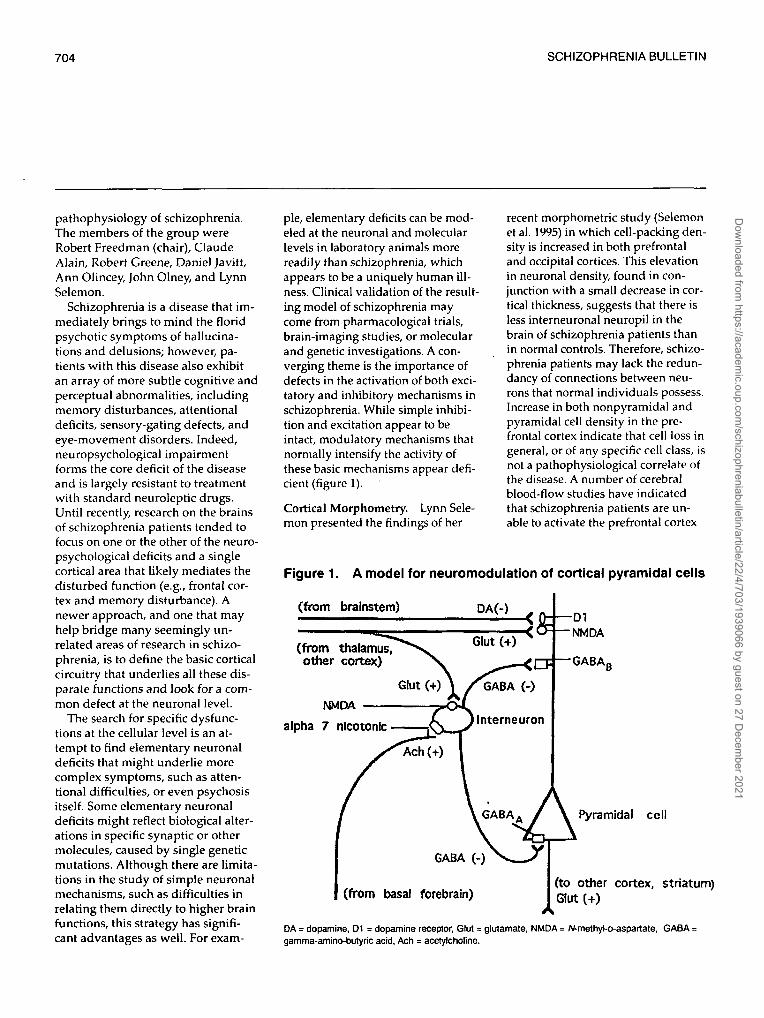


































![UNDER THE RADAR: NEUROIMAGING EVIDENCE IN THE CRIMINAL ... · PDF file29.01.2016 · 2016] Neuroimaging Evidence in the Criminal Courtroom 579 neuroscience. This emerging science a](https://static.documents.pub/doc/80x56/5a9e1a547f8b9a420a8da6b1/under-the-radar-neuroimaging-evidence-in-the-criminal-neuroimaging-evidence.jpg)

