60
Neuromuscular injuries and pharyngeal dysfunction in snorers and sleep apnea patients Farhan Shah

UMEÅ UNIVERSITY
Neuromuscular injuries and pharyngeal dysfunction in
snorers and sleep apnea patients
Farhan Shah

Neuromuscular injuries and pharyngeal dysfunction in snorers and sleep apnea
patients
A study on pathological changes in the human soft palate and its relationship with swallowing dysfunction
Farhan Shah
Department of Integrative Medical Biology, Laboratory of Muscle Biology, and Department of Clinical Sciences, Otorhinolaryngology
Umeå University, Sweden 2018

Copyright © 2018 Farhan Shah Responsible publisher under Swedish law: The Dean of the Faculty of Medicine This work is protected by the Swedish Copyright Legislation (Act 1960:729) Dissertation for PhD New Series Number 1948 ISBN: 978-91-7601-844-6 ISSN: 0346-6612
Electronic version available at: http://umu.diva-portal.org/ Printed by: UmU Print Service, Umeå University Umeå, Sweden, 2018 Cover: Muscle cross-section from uvula of a sleep apnea patient showing abnormalities in cytoskeletal protein desmin (green color) and the C-terminus of dystrophin (red color). The original article 1 is reproduced with permission from the publisher Figures 1 and 5. Illustrated by Per Stål Figure 2. Illustration by Mona Lindström Figure 3. Based on illustration in article by Goldfarb and Dalakas (2009). Figure 4. Illustrated by Farhan Shah

"The outcome of any serious research can only be to make two questions grow where only one grew
before." ---Thorstein Veblen
Dedicated to my family


i
Table of Contents
Abstract ....................................................................................... …iv Abbreviations ................................................................................... v List of original papers ..................................................................... vi Introduction ..................................................................................... 1Background ............................................................................................................. 1 OSA - signs, symptoms, and consequences on health ............................................ 1 Risk factors determining upper airway collapsibility ............................................ 2 Upper airway .......................................................................................................... 2
Reflexogenic mechanism ............................................................................... 2 The site of collapse in OSA ............................................................................ 3 Factors behind the upper airway collapse ................................................... 3
Snoring ................................................................................................................... 3 Swallowing ............................................................................................................. 4
Pharyngeal phase of swallowing .............................................................. 4 Swallowing dysfunction among snorers and OSA patients ........................ 5
Muscles of the soft palate ....................................................................................... 5 Muscle fiber phenotypes in the soft palate muscles……………………..............6
Muscle morphology ................................................................................................ 6 Myosin composition and fiber phenotypes .................................................. 6 Muscle cell cytoskeletal proteins ................................................................... 7 The cytoskeletal proteins desmin and dystrophin ....................................... 7
Nerve morphology .................................................................................................. 8 Neurotrophins ........................................................................................................ 9 Neuromuscular changes in OSA .......................................................................... 10
Upper airway muscle changes in OSA ....................................................... 10 Nerve changes in OSA ................................................................................. 10 The theory behind neuromuscular changes………………………………………….11 Is there a link between neuromuscular changes and pharyngeal dysfunction? ................................................................................................ 11
Aims of the study ............................................................................. 12
Materials and Methods .................................................................... 14Patients ................................................................................................................. 14 Controls ................................................................................................................ 14
Biopsies ........................................................................................................ 14 Autopsies ...................................................................................................... 14
Sleep registration .................................................................................................. 15 Swallowing examination ....................................................................................... 15 Muscle samples ..................................................................................................... 16 Staining for basic histology ................................................................................... 16 Immunohistochemistry ......................................................................................... 16 Antibodies and ligands .......................................................................................... 17

ii
Control staining and pre-absorption for neurotrophins (paper III) ................... 17 Analysis of muscles (paper I-IV) .......................................................................... 19 Muscle fiber type classification (paper I and II) .................................................. 19 Analysis of nerve fascicles (paper IV) ................................................................... 19 Statistical analysis ................................................................................................ 20 Ethical approval ................................................................................................... 20 Results ............................................................................................ 21 Clinical results (paper I-IV) ................................................................................. 21 Soft palate muscles in controls (paper I) ............................................................. 21
Immunoreactive patterns of muscle cytoskeleton and membrane proteins……………………………………………………………………………………………21
The uvula muscle of soft palate in patients (paper II-IV) .................................. 22 Morphology ................................................................................................. 22 Immunoreactive patterns of muscle cytoskeleton and membrane proteins .............................................................................. 23 Immunoreactive patterns of neurotrophins in muscle fibers ................... 24 Immunoreactive patterns of neurotrophin BDNF in relation to desmin .......................................................................................................... 25 BDNF expression in muscle fibers of patients with and without swallowing dysfunction .............................................................................. 25
Soft palate nerves (paper IV) .............................................................................. 25 Nerve fascicle morphology ......................................................................... 25
Neuromuscular changes in patients with vs. without swallowing dysfunction (paper II and IV) .......................................................... 26
Immunoreactive patterns of muscle cytoskeleton in patients with and without a swallowing dysfunction ............................................. 26 Nerve fascicle morphology in patients with and without a swallowing dysfunction ............................................................. 26
Cross-reference with control autopsies (paper II and IV) .................................. 26 Comparison between neuromuscular abnormalities and AHI in patients (paper II and IV) ................................................................................................. 27
Discussion ...................................................................................... 28Main findings ....................................................................................................... 28 Novel cytoarchitecture of soft palate muscles in humans (Paper I) .................. 28 Cytoskeletal abnormalities in the uvula muscle of the soft palate in patients (paper II) ............................................................................................................. 28 Upregulation of BDNF in muscle fibers (Paper III) ........................................... 30 Changes in preterminal nerve fascicles (Paper IV) ............................................. 31 Neuromuscular changes correlate with pharyngeal swallowing dysfunction in snorers and sleep apnea patients (paper II and IV) ................... 32 Neuromuscular changes and AHI ........................................................................ 32 Muscle changes reflecting neuropathy and myopathy in the upper airway ....... 33 The possible cause of neuromuscular changes and pharyngeal dysfunction in snorers and sleep apnea patients ............................. 33 Conclusions .......................................................................................................... 34

iii
Summary ........................................................................................ 35
Funding ........................................................................................... 37 Acknowledgement .......................................................................... 38 References ..................................................................................... 40

iv
Abstract Obstructive sleep apnea (OSA) is a prevalent progressive sleep disorder with serious negative health consequences. Although several risk factors such as obesity can make an individual vulnerable to develop OSA, the pathophysiological mechanism for the collapse of the upper airway is unclear. Moreover, the etiology of the commonly occurring swallowing dysfunction in snorers and sleep apnea patients is not understood. In the light of this, we aimed to investigate whether muscle and nerve changes in upper airway contributes to pharyngeal dysfunction in snorers and sleep apnea patients. Twenty-two patients (1 female, 21 males, mean age 45 years) undergoing soft palate surgery because of snoring and sleep apnea were included in the study. Ten healthy non-snoring males, mean age 38 years, were recruited as controls. Biopsies from the uvula were obtained from both patients and voluntary controls. Control autopsies from both uvula and palatopharyngeus muscles were taken post mortem from 6 previously healthy adult subjects (3 males, 3 females, mean age 52 years) and two male infants (age 4 months and 1.4 years). Overnight sleep registration and videoradiographic examinations of pharyngeal swallowing function were performed in both patients and voluntary controls. Enzyme and immunohistochemistry and morphometric techniques were used to investigate cytoskeletal and membrane proteins desmin and dystrophin and two neurotrophins, brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF). The nerve fascicles in the soft palate were explored for changes in axon and Schwann cell density and for signs of axon regeneration. All patients were snores, and 14 patients had OSA with a mean apnea-hypopnea index 24, range 5-84. Sixteen of the 22 patients had swallowing dysfunction. None of the 10 voluntary controls had sleep apnea or swallowing dysfunction. In both controls and patients, a subgroup of muscle fibers in the soft palate lacked immunoreaction for desmin and the C-terminus of dystrophin, and these fibers were more common in patients than in controls (p<0.001). Moreover, muscle fibers with disorganized desmin were commonly observed in patients, but not in controls (p<0.001). Thus, overall, desmin abnormalities were significantly more frequent in patients (46 vs. 15%, p<0.001), and some of these fibers showed upregulation of BDNF. In addition, nerve fascicles from the soft palate of patients displayed lower density of axons (p<0.02) and a smaller area occupied by Schwann cells (p=0.001) compared to controls. The axon density within nerve fascicles as well as the cytoskeletal abnormalities in muscles correlated significantly with swallowing dysfunction (rs=0.50 and 0.76, respectively, p≤0.03). To conclude, human soft palate muscles seem to be of a unique allotype. In the soft palate of snorers and sleep apnea patients, cytoskeletal myopathy and neuropathy were frequently observed, and these changes correlate significantly with pharyngeal swallowing dysfunction. The upregulation of BDNF in muscle fibers of patients may relate to a regenerative attempt after injury. Consequently, a disturbed sensorimotor function and muscle weakness may contribute to development and progression of swallowing dysfunction and OSA. Traumatic snoring vibrations and muscle overload are plausible causes of the neuromuscular injuries.
v
Abbreviations
AHI Apnea-hypopnea index
BDNF Brain derived neurotrophic factor
BMI Body mass index
CCD Charged couple device
CPAP Continuous positive airway pressure
CSA Cross-sectional area
CV Coefficient of variation
DAPC Dystrophin associated protein complex
DAPI 4',6-diamidino-2-phenylindole
ECM Extracellular matrix
FITC Fluorescein isothiocyanate
H&E Hemotoxylin and eosin
IHC Immunohistochemistry
mAb Monoclonal antibody
MyHC Myosin heavy chain
NGF Nerve growth factor
OCT Optimal cutting temperature
OSA Obstructive sleep apnea
pAb Polyclonal antibody
PBS Phosphate-buffered saline
SC Schwann cell
SD Standard deviation
SDB Sleep disordered breathing
TRITC Tetramethylrhodamine-isothiocyanate
UA Upper airway

vi
List of original papers
1. Unique expression of cytoskeletal proteins in human soft palate muscles
Shah F, Berggren D, Holmlund T, Levring Jäghagen E, Stål P. J Anat. 2016;228(3):487–94. doi: 10 1111/joa.12 417.
2. Desmin and dystrophin myopathy in the upper airway of snoring and obstructive sleep apnea patients
Shah F, Franklin KA, Holmlund T, Levring Jäghagen E, Berggren D, Forsgren S, Stål P. Manuscript submitted.
3. Upregulated expression of brain-derived neurotrophic factor in soft palate muscles of snorers and obstructive sleep apnea patients
Shah F, Forsgren S, Holmlund T, Levring Jäghagen E, Berggren D, Franklin KA, Stål P. Manuscript submitted.
4. Axon and Schwann cell degeneration in nerves of upper airway relates to pharyngeal dysfunction in snorers and sleep apnea patients
Shah F, Holmlund T, Levring Jäghagen E, Berggren D, Franklin KA, Forsgren S, Stål P. Manuscript submitted.

1
Introduction
Background
Obstructive sleep apnea (OSA) is a serious disease characterized by repetitive episodes of complete or partial obstructions of the upper airway during sleep. The airway obstruction leads to decreased (hypopnea), or pauses (apnea) of airflow followed by decreased oxygenation (hypoxia), central nervous system arousal and sleep fragmentation. It is well known that pharyngeal collapse forms the basis of OSA pathogenesis (Pham and Schwartz, 2015), although the reason behind the failure of the upper airway dilator muscles to keep the airway tract patent during sleep remains unclear.
Over the years the prevalence of OSA has been reported to increase steadily in the general population. One of the reasons attributed to this is a rise in obesity and perhaps different diagnostic criteria. It is estimated from eleven published articles between 1992 to 2013, that OSA is present in 22% of men (range, 9-37%) and 17% of women (range, 4-50%) (Franklin and Lindberg, 2015). The variation in prevalence in different studies to some extent reflects differences in age span of the cohorts and different diagnostic criteria of OSA. Snoring is the most common symptom of OSA, occurring in 70% to 95% of patients (Whyte et al., 1989, Hoffstein et al., 1993). Studies have reported that in the general population, up to 25% of women and 45% of men are habitual snorers (Young et al., 1993, Ohayon et al., 1997).
Despite the high prevalence of OSA, the mechanism behind its development and progression are still not entirely understood, and treatment strategies have therefore mostly targeted symptoms.
OSA - signs, symptoms, and consequences on health
Daytime sleepiness and snoring are common symptoms of OSA (Gottlieb et al., 2000, Engleman and Douglas, 2004). Other signs and symptoms are fatigue, tiredness, nocturia, anxiety, depression, and cognitive decline (Chervin, 2000, Guilleminault et al., 2004, Saunamaki and Jehkonen, 2007, Lal et al., 2012). OSA has been associated with several morbid conditions such as an increased risk of cardiovascular disorders including myocardial infarction, stroke and premature death (Punjabi, 2008, Lurie, 2011). Patients having OSA and coronary artery disease have been reported to have 3 times increased risk for stroke (Valham et al., 2008). Sleep-disordered breathing is also suggested as a risk factor for hypertension and consequent cardiovascular morbidity in the general population (Peppard et al., 2000). The episodes of oxygen deprivation

2
during respiratory pauses have significant effects on heart rate, blood pressure, and stress hormones. Both hypoxia and hypercapnia result in increased sympathetic response causing vasoconstriction and subsequent increase in blood pressure during sleep and during daytime as well (Narkiewicz and Somers, 1997). Apart from being a risk for cardiac disease, intermittent hypoxia has been shown to increase the risk of developing insulin resistance and diabetes, cognitive impairment, and cancer (Dewan et al., 2015).
Risk factors determining upper airway collapsibility
There are several factors that may predispose an individual for developing OSA, such as obesity, large tonsils and anatomical abnormalities, certain medications, high alcohol intake, smoking, hypothyroidism, and neurological disorders (Young et al., 2004, Garvey et al., 2015). Among these factors obesity is one of the strongest risk factors associated with developing OSA (Punjabi, 2008). However, these risk factors do not explain the progressive course of the disease in most of the cases, and individuals without these recognized traits and conditions also develop OSA (Gray et al., 2017).
Upper airway
The upper airway of human is involved in vital functions such as respiration, swallowing, and speech. There are more than 20 muscles in the upper airway that by a complex neural feedback system determines its patency during inspiration and expiration.
An important determinant for development of OSA is the size of the upper airway space. A decreased caliber of the upper airway due to factors such as retruded mandible, increased adipose content in pharyngeal walls and tongue, inflammation and edema, hypertrophied tonsils and enlargement of other lymphoid tissue makes it more vulnerable to collapse. Although the caliber of the upper airway is influenced by risk factors, the efficiency of the dilator muscles will determine the patency of the upper airway during sleep. Therefore, obstruction could only develop when neuromuscular responses are inadequate to keep the upper airway patent against the collapsing forces during breathing.
Reflexogenic mechanism
The patency of the upper airway depends on an efficient feedback mechanism reacting to the negative intra-pharyngeal pressure at inspiration. The sensory receptors in the upper airway respond to changes in airway pressure, airflow, temperature and to the upper airway muscle tone itself. Signals from these receptors, in turn, activate motor neurons that influence the upper airway

3
muscle tone, thereby promoting airway patency. Moreover, the dilator muscles are influenced by inputs from respiratory centers in the brainstem, changes in lung volume and sleep/wake state of the brain (Ryan and Bradley, 2005). During sleep when tonic and phasic activity of dilator muscles decreases, and gravity negatively influences the width of the pharyngeal lumen, an ineffective response of the dilator muscles may result in upper airway collapse during inspiration, especially when the patients are sleeping on their back. Effective responses in pharyngeal dilators are crucial for keeping the respiratory tract open, and this depends both on intact feedback from sensory receptors and a functional motor-output, as well as on healthy functional muscles.
The site of collapse in OSA
The most frequent site of collapse in the upper airway is oropharynx (Trudo et al., 1998). The retropalatal area is reported to be the first site of collapse in 56-75% of OSA patients during sleep. The second most common site is the base of the tongue, observed in 25–44% of patients. A collapse of the hypopharyngeal region is reported to be less common (Shepard and Thawley, 1989, Katsantonis et al., 1993, Bhattacharyya et al., 2000).
Factors behind the upper airway collapse
There are several individual factors acting synergistically to trigger the upper airway collapse. All anatomical factors constricting the upper airway lumen are critical for the development of OSA. Other factors such as impairment of upper airway mechanoreceptor sensitivity and reflexes that maintain pharyngeal patency and respiratory control have also been identified as possible causes facilitating instability and pharyngeal collapse. During sleep, when the tonic activity of muscles is decreased and upper airway narrows, airflow can become turbulent during breathing resulting in snoring vibrations and stretch of the pharyngeal tissue as the air passes through. Repeated snoring vibrations and tissue stretch can cause mechanical trauma of the pharyngeal structures, which may lead to a vicious circle by disrupting both their structure and function. Moreover, in an attempt to keep the upper airway patent and prevent it from collapsing, the muscle can get overloaded. These various factors suggest that OSA is a heterogeneous disorder, rather than a single disease entity. Hence, the mechanism of airway instability and collapse during sleep is multifactorial, including both anatomical and neurophysiological factors (Ryan and Bradley, 2005, Dempsey et al., 2010).
Snoring
The narrow passage in the collapsible parts of the airway causes the air to vibrate the tissue structures resulting in noisy snoring sounds during breathing.

4
Snoring has been associated with adverse effects such as cardiovascular disease (Lee et al., 2008), metabolic syndromes i.e., hyperglycemia, central adiposity, hypertension, and low high-density lipoprotein cholesterol (Troxel et al., 2010) as well as carotid artery intima-media thickness (Deeb et al., 2014). Snoring vibrations and stretch may cause pathological changes in the endothelium of carotid vessels in the pharyngeal region leading to inflammation, which might explain the intima media thickness in snorers.
Although a relationship between the intensity of snoring and severity of OSA has been reported (Maimon, 2010, Acar et al., 2016), there seems to be no relationship between severity of OSA and duration of snoring (Hong et al., 2017). In fact, Hong et al. (2017) reported that snoring is more common in moderate OSA compared to in mild and severe forms. This highlights that there is a complex interplay of several etiological factors in the development and progression of OSA. Considering this, the present criteria for diagnosing the severity of OSA have been proposed to be re-evaluated, especially in relation to the degree of oxygen desaturation and other associated comorbid conditions (Hudgel, 2016).
Swallowing
Swallowing is a complex process regulated by an intricate neuromuscular system requiring both voluntary and autonomic activity. Broadly, the swallowing process can be divided into 3 phases, i.e., oral phase, pharyngeal phase and esophageal phase (Lang, 2009). The voluntary, or the oral phase, is followed by an involuntary pharyngeal phase when food reaches the palatoglossal arch. Receptors that initiate the pharyngeal phase are scattered over the base of the tongue, the palatoglossal and palatopharyngeal arches, the tonsillar fossa, uvula, valleculae, and posterior pharyngeal wall (Steele and Miller, 2010).
Pharyngeal phase of swallowing
After the oral phase, when pharyngeal swallowing is initiated, respiration is inhibited to prevent bolus from entering the airway. The propagation wave starts propelling the bolus through pharynx, the velopharyngeal sphincter closes to prevent bolus from entering the nasal cavity, the epiglottic folds and the vocal cords close to protect the airway. Finally, the upper esophageal sphincter opens for the bolus to proceed into esophagus and the pharyngeal phase of swallowing is finalized.

5
Swallowing dysfunction among snorers and OSA patients
Several investigators have reported the presence of swallowing dysfunction among snorers and sleep apnea patients (Levring Jäghagen et al., 2003, Jobin et al., 2007). The etiology of swallowing dysfunction in snorers and sleep apnea patients is unclear. In the absence of any systemic or local pathological factors, the most likely cause is traumatic snoring vibrations and tissue stretch causing nerve or muscle injuries (Levring Jäghagen et al., 2003, Jobin et al., 2007). Neuromuscular changes might also contribute to nocturnal obstruction in these patients.
Muscles of the soft palate
Soft palate has a complicated anatomy with muscles working against each other in different directions. Five pairs of muscles contribute to the formation and the various movements of the soft palate. Three of these, the uvula, tensor veli palatini, and levator veli palatini muscles descend from bony attachment in the skull and insert into the soft palate, while two, the palatopharyngeus and palatoglossus muscles, ascend from the pharyngeal walls and the tongue, respectively (Fig. 1). This complex anatomy with an absence of a firm muscle attachment at one or both ends, suggests a low capacity for generation of static
contraction and high tension. Moreover, it is reported that some of the palate muscles lack muscle spindles, a receptor in the muscle that senses muscle length during movement and load (Stål and Lindman, 2000). Lack of muscle spindles would imply that sensory nerves/receptors in the palatal mucosa must play a crucial role in the proprioceptive control of the pharynx. In consideration of this, nerve lesions in the upper airway mucosa might have critical consequences for the reflex feedback system. Furthermore, since the purpose of stretch reflexes
triggered by muscle spindles is to help in maintaining muscle tone and to resist muscle stretch, a muscle without muscle spindles might be more vulnerable to receive stretch-induced damages. Hence, the soft palate forms an intricate entity that might require a special cytoarchitecture of the muscle cells and a sensory feedback system relying on other receptors than muscle spindles.
Fig. 1. Illustration of the uvula, tensor veli palatini, levator veli palatini, palatopharyngeus and palatglossus muscles of the human soft palate viewed from the side.

6
Muscle fiber phenotypes in the soft palate muscles
The uvula and palatopharyngeus muscles are predominantly built up of fast contracting type II fibers, whereas muscles elevating the soft palate, levator and tensor veli palatini, are predominated by slow contracting fatigue resistant type I fibers (Stål and Lindman, 2000). Based on the fiber type composition, the uvula and palatopharyngeus muscles seem to be suited for quick shaping of the soft palate and to act as intrinsic support to quickly control stiffness in the nasal and lateral aspect of the soft palate, preventing distortion. The levator veli palatini and the tensor veli palatini muscles, on the other hand, have a fiber type profile more designed for slower and more long-standing contractions in elevating and stretching the soft palate.
Muscle morphology
Skeletal muscles are made up of several multinucleated closely packed muscle fibers that are surrounded by a thin layer of connective tissue, sarcolemma. Two major components of the muscle fibers are the myofibrils, the contractile element of fibers, and the mitochondria, the energy supplier of the fibers. The myofibrils are composed of series of sarcomeres, the functional unit of the myofibril. These sarcomeres are built up of thick and thin filaments, mainly composed of myosin, actin, troponin, and tropomyosin (Fig. 2). The interaction between these two filaments is the basic mechanism for muscle contraction.
Myosin composition and fiber phenotypes
Myosin is the protein determining contraction of the muscle cells. The myosin converts free energy derived from the hydrolysis of ATP to mechanical work. The myosin molecule consists of two myosin heavy chains (MyHC) and four light chains that exist in multiple isoforms determined by variations in their amino acid composition (Stål et al., 1994). Myosin heavy chain is the molecular motor protein of the thick filaments, and the type of myosin isoform that determines
Fig. 2. Muscle structure. Schematic illustration of skeletal muscle structures. Muscle, muscle fibers with capillaries, myofibrils, myofilaments and contractile molecules are shown.
7
the velocity of contraction. The MyHC composition of a muscle is regarded as the best marker of the functional heterogeneity among muscle fibers. Four different major MyHC isoforms have been identified in humans and these form the basis for phenotypic classification of muscle fibers. MyHC-I predominates in muscle fibers with slow and fatigue resistant contracting properties, i.e type I fibers, while MyHC-II predominates in muscle fibers with fast contracting properties i.e. type II fibers. In humans, fibers containing MyHC-II can be subdivided into type IIa and type IIx. Type IIa is more fatigue resistant compared to type IIx. Fibers expressing two or more isoforms are classified as hybrid fibers i.e., type I+II or type IIa+IIx fibers.
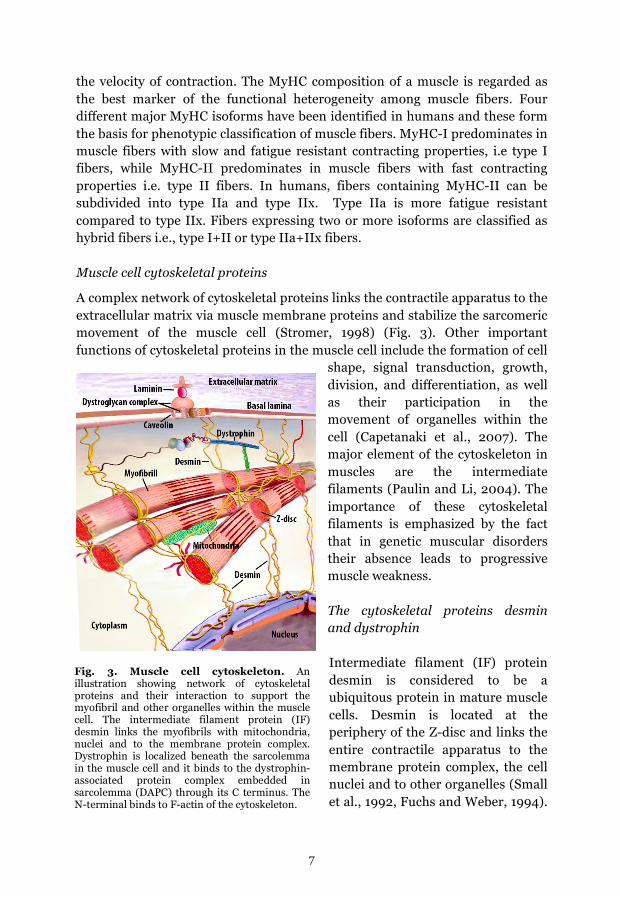
Muscle cell cytoskeletal proteins
A complex network of cytoskeletal proteins links the contractile apparatus to the extracellular matrix via muscle membrane proteins and stabilize the sarcomeric movement of the muscle cell (Stromer, 1998) (Fig. 3). Other important functions of cytoskeletal proteins in the muscle cell include the formation of cell
shape, signal transduction, growth, division, and differentiation, as well as their participation in the movement of organelles within the cell (Capetanaki et al., 2007). The major element of the cytoskeleton in muscles are the intermediate filaments (Paulin and Li, 2004). The importance of these cytoskeletal filaments is emphasized by the fact that in genetic muscular disorders their absence leads to progressive muscle weakness.
The cytoskeletal proteins desmin and dystrophin Intermediate filament (IF) protein desmin is considered to be a ubiquitous protein in mature muscle cells. Desmin is located at the periphery of the Z-disc and links the entire contractile apparatus to the membrane protein complex, the cell nuclei and to other organelles (Small et al., 1992, Fuchs and Weber, 1994).
Fig. 3. Muscle cell cytoskeleton. An illustration showing network of cytoskeletal proteins and their interaction to support the myofibril and other organelles within the muscle cell. The intermediate filament protein (IF) desmin links the myofibrils with mitochondria, nuclei and to the membrane protein complex. Dystrophin is localized beneath the sarcolemma in the muscle cell and it binds to the dystrophin-associated protein complex embedded in sarcolemma (DAPC) through its C terminus. The N-terminal binds to F-actin of the cytoskeleton.

8
When the contractile apparatus generates force or contractions, desmin filaments help in maintaining the structural and mechanical integrity by transmitting the force and longitudinal load bearing (Paulin and Li, 2004, Shah et al., 2004) (Fig. 3).
Dystrophin is another vital cytoskeletal protein connecting to other cytoskeletal proteins in the cytoplasm and to the surrounding extracellular matrix (ECM) through the cell membrane (Campbell, 1995, Srivastava and Yu, 2006). The dystrophin-associated proteins can be divided into three groups based on their cellular localization in the muscle cell, i.e., extracellular, transmembrane and cytoplasmic proteins. Dystrophin binds to the membrane-spanning dystrophin-associated protein complex (DAPC) through its C-terminus domain, whereas its N-terminus interacts with actin filaments. The DAPC has important roles in stabilizing sarcolemma and transmitting force generated in the muscle sarcomere to the ECM (Petrof et al., 1993). Mutations of desmin and dystrophin lead to genetic muscular dystrophy, which results in progressive muscle weakness (Fuchs and Weber, 1994, Campbell, 1995) (Fig. 3).
Nerve morphology
Peripheral nerves are the communicative channel between the brain and rest of the body. The basic component of peripheral nerves is axons bundled into nerve fascicles that are wrapped in a sheath, the perineurium. Many fascicles are enclosed together in a layer called the epineurium to form the whole nerve.
Fig 4. Peripheral nerve transverse section. A nerve fascicle with myelinating Schwann cells (green) wrapped around the axons (red) and non-myelinating Schwann cells (green) embedding bundles of small sized axons.

9
Within each nerve fascicle, axons are embedded in endoneurial connective tissue. Nerves can be divided into motor (efferent), sensory (afferent), autonomic or mixed nerves.
In the nerve fascicle, Schwann cells wrap around the axons. Schwann cells are the main glial cells of the peripheral nervous system. They provide trophic support by releasing neurotrophins such as nerve growth factor (NGF) and forming myelin for faster conduction. The most heavily myelinated fibers are the large motor neurons (type Aα), followed by the afferent fibers from muscle spindles (type Aβ). These neurons have the fastest conduction velocity. Non-myelinating Schwann cells surround several small diameter axons, ensheathing each axon in a pocket of its cytoplasm, forming a Remak bundle. They provide support and nutrition to axons, ensuring their survival. Unmyelinated neurons (type C), such as the sensory neurons involved in transmitting pain and temperature and postganglionic sympathetic neurons have the slowest conduction velocity (Menorca, 2013) (Fig. 4).
Neurotrophins
Neurotrophins are a family of proteins that promote survival, development, and differentiation of neural cells. Nerve growth factor (NGF) was the first recognized prototypic neurotrophic factor. Other structurally and functionally related growth factors are the brain-derived neurotrophic factor (BDNF), neurotrophin-3 (NT3), and neurotrophin-4/5 (NT4/5), together forming the neurotrophin protein family (Huang and Reichardt, 2001). Initially, neurotrophins were believed to primarily have a neuroprotective role and to be involved in development and function of the central and peripheral nervous systems only. Subsequently, their presence in non-neuronal cells (Sariola, 2001) has generated interest regarding their role and function both in health and disease.
Nerve growth factor NGF was originally thought to promote the survival and differentiation of sensory and sympathetic neurons. Its role in neural development has been studied extensively, and recent findings point to a diverse role of NGF (Sofroniew et al., 2001). Similarly, BDNF was believed to only play a role in regulating survival, growth, and maintenance of neurons (Huang and Reichardt, 2001). Since then, it´s presence has also been shown in other tissues, e.g. muscle fibers (Matthews et al., 2009).
Although several non-neuronal cells have been reported to express neurotrophins, their role in non-neuronal cells remains unclear. Skeletal muscles for example have been reported to express neurotrophins and their receptors not only throughout the developmental stages (Griesbeck et al., 1995,

10
Chevrel et al., 2006, Pitts et al., 2006), but also during muscle transformation as well as in various physiological and pathological conditions (Sakuma and Yamaguchi, 2011). It has also been shown that BDNF is upregulated in denervated muscle fibers possibly to attract motor-nerves for reinnervation (Koliatsos et al., 1993, Zhang et al., 2000). The expression of BDNF and NGF was found to be upregulated in allergic rhinitis, also highlighting a role in the upper airway (Raap et al., 2008). However, their expression and role in the muscles of the upper airway have not been reported before, and investigations of their expression in these muscles can shed more light on the pathophysiological processes involved in the development of OSA.
Neuromuscular changes in OSA
Upper airway muscle changes in OSA
Skeletal muscles have an adaptive potential to modify their composition of muscle fiber phenotypes and the fiber size in response to altered patterns of activity (Pette and Staron, 1997, Scott et al., 2001). Moreover, denervation of muscle fibers may also affect the size of the fibers and the fiber type composition. In snoring and OSA patients, studies of the soft palate muscles have reported either a higher or a lower proportion of type I and type IIA fibers, respectively, compared to controls (Woodson et al., 1991, Series et al., 1995, Friberg et al., 1998, Lindman and Stål, 2002, Boyd et al., 2004). Moreover, findings showing a presence of both atrophic and hypertrophic fibers as well as fascicular atrophy in patients indicate muscle fiber denervation (Edström et al., 1992, Series et al., 2000, Boyd et al., 2004). The findings of disorganized and low number of mitochondria in muscle fibers of snorer and OSA patients also suggest the presence of myopathy (Stål and Johansson, 2012). Inflammation in the soft palate has been reported in both muscle and mucosae of OSA patients (Woodson et al., 1991, Boyd et al., 2004). However, changes in muscle cytoskeletal proteins remain unknown.
Nerve changes in OSA
Sensory and to some extent motor neuropathy have been proposed by several investigators as a cause for the inability of the muscles to maintain the airway patency during sleep (Kimoff et al., 2001, Guilleminault et al., 2002, Eckert et al., 2011, Sunnergren et al., 2011). Broadly, findings indicating sensory neuropathy include impaired ability to detect temperature changes, vibratory sensation, and two-point discrimination, as well as abnormal vascular responses (Series et al., 2009, Saboisky et al., 2012). Sunnergren et al. (2011) reported a correlation between sensory disturbances in the upper airway and the severity of sleep apnea. The important role of an intact sensory feedback system for upper airway stability was shown by application of topical anesthesia on the

11
upper airway mucosa. This resulted in an increased pharyngeal airflow resistance compromising the upper airway patency (Horner et al., 1991). Furthermore, histological studies have revealed an increase in peripheral nerve fibers stained for protein gene product 9.5 (PGP 9.5), which was considered to be nerve sprouting secondary to traumatic nerve damage (Friberg et al., 1997, Boyd et al., 2004). The preterminal part of innervation was not examined. Moreover, electron microscopy studies reported signs of changes in nerves in the soft palate of snorers and sleep apnea patients, although the changes were not quantified and compared to controls (Woodson et al., 1991, Bassiouny et al., 2009). Therefore, there is a need to quantify changes in preterminal nerves in patients and to relate the findings to the degree of pharyngeal dysfunction.
The theory behind neuromuscular changes
Several investigators have proposed that OSA is a progressive heavy snorer’s disease. Snoring vibratory trauma might injure upper airway tissue, triggering a vicious cycle in OSA (Svanborg and Larsson, 1993, Petrof et al., 1996, Lugaresi and Plazzi, 1997, Friberg et al., 1997). However, despite the fact that there are many signs of neuropathy in snoring and sleep apnea patients, it remains to be established whether the nerves in the upper airway of snorers and OSA patients show loss of axons and Schwann cells and if these changes have an impact on pharyngeal function. Moreover, limb muscles exposed to vibration and contraction against lengthening are reported to have cytoskeletal changes (Lieber et al., 1996, Barash et al., 2002, Necking et al., 2004, Murfee et al., 2005), Therefore, changes in the muscle cytoarchitecture from snorers and sleep apnea patients needs to be investigated.
Is there a link between neuromuscular changes and pharyngeal dysfunction?
Based on the present knowledge, the theories on OSA progression require further elucidation by investigating muscle and nerve changes at the structural and molecular level and to correlate these findings against pharyngeal function. In a review on neuromuscular function of the soft palate in snorers and sleep apnea patients, Patel et al. (2018) concluded that although there are clinical and histological studies showing changes typical of nerve damage, yet a causal relationship cannot be supported.
The present project is an attempt to investigate whether there is a link between neuromuscular changes in the soft palate and the commonly occurring pharyngeal swallowing dysfunction among snorers and sleep apnea patients.

12
Aims of the study
It has been proposed by many investigators that years of snoring vibration and tissue stretch in snorers and sleep apnea patients have the potential to cause neuromuscular damage, thereby triggering a vicious cycle leading to progression and gradual worsening of sleep apnea (Fig. 5).
The present project is developed around the hypothesis that ‘neuromuscular changes in the upper airway are associated with pharyngeal dysfunction among adult snorers and sleep apnea patients. Based on this hypothesis the specific aims of this project were to:
1. Compare the cytoarchitecture of soft palate muscles with limb muscles in healthy humans
Fig 5. A plausible mechanism behind the proposed hypothesis. During sleep, when the muscles relax, and the upper airway becomes restricted, airflow gets turbulent and the oropharyngeal tissue vibrates and stretches as the air passes through. Predisposing factors may render individuals more susceptible. Over a period of time, traumatic vibrations and tissue stretches result in neuromuscular injuries that deteriorates function by disturbing the reflexogenic mechanism and causing muscle wasting and weakness. A vicious circle is formed that contributes to pharyngeal dysfunction and OSA.

13
2. Investigate cytoskeletal changes in soft palate muscles of snorers and sleep apnea patients and compare the result with healthy controls
3. Study expression of neurotrophins in the soft palate muscles of snorers and sleep apnea patients and compare the findings with healthy controls
4. Analyze for axon and Schwann cells loss in preterminal nerve fascicles
5. Analyze the muscle morphology for signs of denervation in snorers and sleep apnea patients
6. Compare and correlate the changes in muscles and nerves with pharyngeal swallowing dysfunction and apnea-hypopnea index (AHI) in snoring and sleep apnea patients

14
Materials and Methods
Patients
Twenty-two patients (21 males and 1 female) undergoing soft palate surgery because of snoring and sleep apnea were included. Criteria for exclusion were smoking, previous palatal surgery, systemic disease, medications and drug abuse. The mean age was 45 (range 29-60 years), and the mean body mass index (BMI) was 28 (range 21-34 kg/m2). A biopsy was taken from the entire base of the uvula in connection with the soft-palate surgery.
Controls
Biopsies
Ten volunteering healthy controls were recruited through advertisements. All subjects were males, mean age 38 (range 30-51 years), mean BMI 24 (range 22-30 kg/m2). The exclusion criteria were similar as in patients and also included habitual snoring and sleep apnea. The clinical examination of voluntary controls was done similarly as in patients. Using punch biopsy technique, a sample was acquired from the corresponding site as in patients, except in one case where complete surgical resection of the uvula was performed. Moreover, for comparison, samples from a thigh muscle, musculus vastus lateralis, and an arm muscle, musculus biceps brachii were acquired from 6 healthy voluntary adult subjects (Table 1).
Autopsies
Due to the fact that a punch biopsy represents only a part of the whole muscle cross-section, the punch biopsies were compared with autopsies of the entire cross-section of uvula for cross-reference to validate the findings (paper II and IV) (Table 1). Samples from the uvula and palatopharyngeus muscles were
Table 1. The number of muscle fibers and nerve fascicles analyzed in biopsies and autopsies of the soft palate in each study
Control biopsies
Control autopsies
Patient biopsies
No.muscle fibers analyzed
No. nerve fascicles analyzed
Paper I 5 12 6373 Paper II 10 5 22 12732 Paper III 10 22 3208 Paper IV 6 6 22 11713 178

15
obtained from six subjects who died accidentally, 3 males and 3 females, mean age 52 (range 42-75 years), mean BMI 25 (range 21-31, kg/m2), and two male infants (age 4 months and 1.4 years). The exclusion criteria were similar to those in voluntary controls. There was no medical history of snoring and sleep apnea and any systemic diseases. All subjects had a normal craniofacial and oro-pharyngeal anatomy and no signs showing elongation or hypertrophy of uvula were observed. All samples were taken within 24 hours post-mortem.
Sleep registration
Ambulatory overnight sleep apnea recordings (Embletta, Embla systems, Kanata, Canada) was done for all patients and volunteering controls. Sleep apnea recordings included continuous recordings of airflow using nasal cannula pressure, thoracic and abdominal respiratory effort (Xact Trace Belts, Embla Systems, Kanata, Canada), finger puls oximetry (Nonin Oximeter XPOD, Nonin Medical, Inc., Plymouth, USA) and a body position sensor. All the recordings were scored manually, and the duration of sleep was estimated from the recordings. The scorer was blinded to treatment, and the scoring was not performed by any of the authors. An apnea was defined as a ≥90% cessation of airflow lasting 10 seconds or more, while a hypopnea was defined as a 50% reduction in airflow compared with baseline, in combination with oxygen desaturation of ≥3% (Berry et al., 2012).
Swallowing examination
Swallowing function was examined videoradiographically (C-arm, Philips BV 29, field width 23 cm) i n lateral and frontal projections, with the subject in an upright position comfortable for swallowing. The subjects chewed and swallowed a solid bolus consisting of crisp bread and barium sulfate (Mixobar Esophagus; Astra) followed by swallowing of a liquid barium sulfate contrast bolus (Mixobar High Density; Astra). All standard boluses were repeated twice in each projection. Two investigators evaluated the recordings. Swallowing function was graded as 1. normal function, 2. mild dysfunction in the presence of one of the following deviant features: premature leakage, velar dysfunction, residual or laryngeal penetration, 3. moderate dysfunction when two of the deviant features in grade 2 or dysfunction of the upper esophageal sphincter, the epiglottis or the propagation wave was present and 4. severe dysfunction with aspiration below the vocal cords (Jäghagen et al., 2008).

16
Muscle samples
The muscle samples were either fixed or immediately frozen directly after the acquisition. Fixation was done using 4% formaldehyde in 0.1 M phosphate buffer, pH 7.0, for 24 hours at 4 °C. The samples were then washed overnight at 4° C in Tyrodes solution containing 10% sucrose. All samples were oriented and mounted for transverse or longitudinal sectioning in OCT compound (Tissue Tek, Miles, Elkhart, IN, USA) and rapidly frozen in liquid propane chilled with liquid nitrogen and stored at -80 °C until further processing.
Staining for basic histology
Tissue cross-sections, 7-8 µm thick, were cut in a cryostat (Leica CM3050) at -20°C. The sections were mounted on glass slides and stained with routine hematoxylin and eosin (H&E) for the demonstration of basic morphology. Briefly, air dried sections were put onto slides and placed in Harris’ haematoxylin for 2.5 min. Subsequently, the sections were rinsed in distilled water followed by dipping in 0.1% acetic acid for 15 seconds and rinsing in tap water (around 37°C) for 4 min. Lastly, staining with 1% eosin for 1 min followed by dehydration in ethanol 3 x 2 min, clearing, and mounting.
Immunohistochemistry
Serial muscle cross-sections, 5 µm thick, were immunohistochemically stained using modified standard techniques and well-characterized monoclonal (mAb) and polyclonal (pAb) antibodies (Abs). When required, post-fixation of unfixed tissue sections was performed using 2% paraformaldehyde. In brief, the sections were immersed in 5% normal non-immune donkey serum (Jackson ImmunoResearch Laboratories, West Grove, PA, USA) for 15 min and rinsed in 0.01 M phosphate-buffered saline (PBS) for 3 x 5 min. The sections were then incubated with the primary antibody diluted to appropriate concentrations in PBS with bovine serum albumin in a humid environment. Double- or triple-staining procedures were performed in different combinations with different Abs. Incubation was carried out overnight at 4 °C. After additional washes in PBS, sections were immersed in 5% normal non-immune donkey serum and then incubated with the secondary Ab (37 °C for 30 min) and washed in PBS for 3 x 5min. Bound primary Abs were visualized by indirect immunofluorescence using affinity-purified Abs prepared for multiple labeling and conjugated with fluorochrome with different emission spectra; Fluorescein isothiocyanate (FITC), Rhodamine Red-X (RRX; Jackson ImmunoResearch Laboratories,West Grove, PA, USA), Alexa fluor 488 and Alexa fluor 647 (Invitrogen, CA, USA). The sections were thereafter washed in PBS for 3 x 5 min and then mounted in

17
Vectashield Mounting Medium (H-1000) or Mounting Medium with 4ʹ́ ,6-diamidino-2-phenylindole (DAPI) for staining of nuclei (Vector Laboratories, Burlingame, CA, USA). Control sections were treated as above, except that the primary Abs were exchanged with non-immune serum. For details, see (Lindström and Thornell, 2009).
Antibodies and ligands
A panel of Abs was used for detection of cytoskeletal and membrane-associated proteins (Table 2). For visualization of dystrophin, one anti-dystrophin mAb directed against the rod, two against the C-terminus and one against the N-terminus were used. Three different Abs were used for identification of desmin. The basement membrane of the muscle cell was identified with an anti-laminin antibody. Muscle cell membrane proteins were investigated with mAbs against spectrin and vinculin, and members of DAPC were detected with mAbs against β-dystroglycan, nNOS and caveolin-3. Cytoskeletal proteins expressed during development and regeneration were identified by mAbs against vimentin, H-nestin and utrophin (Blake et al., 1996, Herrmann and Aebi, 2000). A cytoskeletal protein linking actin to the Z disc of the sarcomere was detected with an antibody directed against α-actinin 2. Rhodamine-Phalloidin, a ligand (R-415; Molecular Probes, Leiden, the Netherlands) conjugated to the red-orange fluorescent dye, Tetramethylrhodamine (TRITC), was used to identify filamentous actin (F-actin). In preterminal nerve fascicles the axons and Schwann cells were identified by antibodies directed against Beta III-tubulin and S-100B, respectively. Additionally, a pAb pan-neuronal marker, PGP 9.5, was also used to identify the nerves. Neurotrophins were identified with Abs against NGF and BDNF.
For fiber phenotype classification, muscle cross-sections were stained with three mAbs against the major contractile MyHC isoforms. Monoclonal Ab A4.840 having strong affinity for MyHC-I, mAb A4.74 strong affinity for MyHC-IIa, and mAb N2.261 showing strong affinity to MyHC-IIa, weak affinity to MyHC-I, and no affinity to MyHC-IIx. Slow tonic MyHC was identified with mAb MYH14.
Control staining and pre-absorption for neurotrophins (paper III)
For control purposes, sections were treated as above except that the primary antibodies were excluded. Furthermore, to confirm the specificity of the antibodies against BDNF and NGF, the antibodies were pre-absorbed with BDNF (50 µg/mL antiserum: sc-546P, Santa Cruz) and NGF (50 µg /mL antiserum; sc-548P, Santa Cruz) peptides. The pre-absorption was done overnight at 4 °C (Bagge et al., 2009).

18
Table 2. Data on antibodies used for immunohistochemistry
Antibody Code Specificity Gene* Host/Clone Dilution Source
Dystrophin GTX15277 Human dystrophin (C terminus)
DMD pAb-rabbit 1:7500 1
Dystrophin NCL-DYS1 Human dystrophin (Rod domain)
DMD mAb-mouse/ Dy4/6D3
1:5 2
Dystrophin NCL-DYS2 Human dystrophin (C terminus)
DMD mAb-mouse/ Dy8/6C5
1:10 2
Dystrophin NCL-DYS3 Human dystrophin (N terminus)
DMD mAb-mouse/ DY10/12B2
1:10 2
Desmin M0760 Human and animal desmin
DES mAb-mouse/ D33 1:100 3
Desmin 18-0016 Human desmin DES mAb-mouse/ ZC18
1:1000 4
Desmin ab15200 Human and animal desmin
DES pAb-rabbit 1:2000 5
Laminin PC 128 Human laminin LAM pAb-sheep 1:15000 6
Laminin Z0097 Human and animal LAM pAb-rabbit 1:3000 3
βeta-Dystroglycan
NCL-b-DG Human beta-dystroglycan
DAG1 mAb-Mouse/ 43DAG1/8D5
1:500 2
Caveolin 3 610421 Animal caveolin3 CAV3 mAb-mouse/ 26/Caveolin3
1:500 7
Neuronal nitric oxide
AB5380 Human and animal nNOS, NOS-I, bNOS
NOS1 pAb-Rabbit 1:5000 8
Vinculin V9131 Human vinculin VCL mAb-Mouse/ hVIN-1
1:5000 9
H-Nestin MAB1259 Human Nestin NES mAb-mouse/ 196908
1:250 10
Utrophin sc-33700 Human utrophin UTRN mAb-mouse/ 8A4 1:200 11
α-Actinin ab9465 Human and animal α-actinin (sarcomeric)
ACTN3 mAb-mouse/EA-53
1:5000 9
Spectrin NCL-SPEC2 Human and animal spectrin
SPBT mAb-Mouse/ RBC1/5B1
1:1000 12
Vimentin sc-6260 Human vimentin VIM mAb-Mouse/ V9 1:250 11
MyHC A4.840 Human and animal MyHC-I
MYH7 mAb-mouse 1:400 13
MyHC A4.74 Human and animal MyHC-II
MYH2 mAb-mouse 1:500 13
MyHC
N2.261 Human and animal MyHC-I and IIA,
MYH2, 6, 7, 13,
mAb-mouse 1:400 14
PGP 9.5 7863-0504 Human and animal PGP pAb-rabbit 1:2500 15
Beta III-tubulin
T8660 Human and animal TUBB3 mAb-mouse 1:5000 9
S-100B S2532 Human and animal S100B mAb-mouse 1:500 9 GAP-43 AB5220 Human and animal GAP43 pAb-rabbit 1:500 8
NGF sc 548 Human and animal NGF pAb-rabbit 1:2000 11
BDNF sc 546 Human and animal BDNF pAb-rabbit 1:1000 11
* Official gene nomenclature according to OMIM. (http://www.ncbi.nlm.nih.gov/omim/) 1. GeneTex Inc., Taiwan; 2. Novocastra Laboratories Ltd., UK; 3. Dako, Sweden/Denmark, 4. Invitrogen Corporation, CA, USA; 5. Abcam, UK; 6. Binding site Group, UK; 7. BD Biosciences, USA; 8 Chemicon, CA, USA; 9. Sigma-Aldrich Co, UK/NY USA; 10. R&D Systems, UK; 11. Santa Cruz Biotechnology Inc; UK; 12. Leica Biosystems, UK; 13. Developmental Studies Hybridoma Bank, developed under the auspices of the NICHD and maintained by the University of Biological Sciences, Iowa City, Iowa, USA; 14. gift from Stefano Schiaffino, CNR Inst of Neuroscience, Padova, Italy; 15. Biogenesis, UK

19
Analysis of muscles (paper I-IV)
Random areas, and in paper 1 also selected areas, from each muscle cross-section were scanned at 20x or 40x magnification with a fluorescence microscope (Leica DM6000B, Leica Microsystems CMS GmbH, Wetzlar, Germany) equipped with a digital high-speed fluorescence charge-coupled device (CCD) camera (Leica DFC360 FX). The total number of unstained, weakly stained, or disorderly stained fibers for the Abs directed against desmin, dystrophin, and BDNF were quantified manually on each photo (Photoshop CS5, version 12.0.4).
Randomly chosen muscle cross-sectional areas were analyzed for fiber size variability, area occupied by muscle fibers and amount of connective tissue. The cross-sectional area of each muscle fibers was calculated by tracing the circumference of the muscle fiber basement membrane stained for laminin using customized morphometric software (Leica QWin Standard V3.5.1 software, Leica Microsystems Ltd. Heerbrugg, Switzerland). Variability in muscle fiber size was expressed as the coefficient of variation (CV). The percentage of area occupied by muscle fibers was calculated according to the formula: total muscle cross-sectional area/total scanned tissue area x 100 (%). The amount of extracellular tissue, i.e. connective tissue including glands, vessels, and nerves, was calculated by subtracting the total muscle cross-sectional area from the total tissue area of each scanned photo. Muscle fiber type classification (paper I and II)
Based on the immunostaining pattern for the different MyHC mAbs, the muscle fibers were classified as slow MyHC-I (type I) or fast MyHC-II (type II) fibers.
Analysis of nerve fascicles (paper IV)
In sections of the uvula, nerve fascicles were randomly identified in both muscle and mucosal areas stained for laminin. The nerve fascicles were scanned at 40x magnification from 6 volunteering controls, 6 autopsies, and 22 patients.
The area of each nerve fascicle and each Schwann cell within the fascicles was measured by tracing the circumference of the nerve fascicle membrane stained for the pAb Z0097 against laminin and tracing the periphery of Schwann cells stained for mAb S-100B, respectively. The number of axons stained for Beta III-tubulin was counted in each nerve fascicle, and the density was calculated by dividing the number of axons in the nerve fascicle by the cross-sectional area of the fascicle (axons x 10-3 per µm2). The cluster of small-sized axons embedded in

20
Schwann cells was not quantified due to practical reason regarding discriminating individual axons.
The percentage of area occupied by Schwann cells in the nerve fascicle was calculated as the total Schwann cell area divided by the fascicle area x 100 (%). Schwann cells lacking immunostaining for central axons were also counted, and the value was presented as the percentage of Schwann cells lacking axons within the nerve fascicle. All calculations were made blinded to the origin of the samples.
Statistical analysis
Normality in distribution of data showing muscle and nerve findings was tested by the Shapiro-Wilk test. Comparisons between the control and patient groups were made using an independent sample t-test for variables with normal distribution and the Mann-Whitney U test for non-normal distribution. Correlation analysis was done with Spearman’s rank-order correlation test. Values are presented as the mean proportion ± standard deviation (SD). Results were considered significant at a p-value of ≤0.05. All the tests were performed with SPSS software (IBM SPSS 23, statistical software).
Ethical approval
Approval of the study was obtained from the regional Ethical Review Committee in Umeå (Dnr 05-130M). Patients and voluntary controls were informed orally and in writing about the purpose of the study and risks. All subjects gave their written consent to participate. Autopsy collection was in agreement with Swedish law and regulations on autopsy and transplantation. The tissue samples were encoded and were untraceable without a code-key. All samples were collected in agreement with the Declaration of Helsinki.

21
Results
Clinical results (paper I-IV)
All 22 patients snored. Fourteen out of the 22 patients had obstructive sleep apnea with an apnea-hypopnea index of ≥5 (mean AHI 24, range 5-84). In supine sleep position, seventeen of the patients had AHI of ≥5. Ten patients demonstrated a moderate swallowing dysfunction, 6 patients had a mild dysfunction, and 6 had a normal function (Fig. 6). None of the 10 voluntary controls had sleep apnea or swallowing dysfunction.
Soft palate muscles in controls (paper I)
Immunoreactive patterns of muscle cytoskeleton and membrane proteins
In the control samples, a subpopulation of muscle fibers in uvula and palatopharyngeus lacked or had a faint immunoreaction for desmin (desmin-negative fibers, 11.7% and 9.8%, respectively) and the C-terminal of the dystrophin molecule (4.2% and 6.4%, respectively). These fibers mostly expressed slow contractile protein myosin heavy chain I. The majority of muscle fibers lacking immunoreaction for the dystrophin C-terminus also lacked immunoreaction for desmin. The proportion of fibers negative for both the
Fig. 6. Lateral videoradiographic view. Residual of liquid bolus in the piriform sinus (R) from a previous swallow indicating reduced sensibility. A patient with normal sensibility would make a second swallow to clear the pharynx before swallowing the next bolus. Now a chewed solid bolus (B) is passing passively into pharynx without eliciting the swallowing reflex, i.e. premature bolus leakage. When bolus enters the pharynx, swallowing is normally initiated, and respiration is inhibited. Here the airway is open, implying a risk of aspiration if the patient inhales rapidly or talks.

22
dystrophin C-terminus and desmin was 2.7% in uvula and 5.0% in palatopharyngeus (Fig. 8, A-C). In limb muscles, all fibers showed immunoreaction for desmin and dystrophin, including the C-terminal of dystrophin. Furthermore, an unusual staining pattern was also observed in soft palate muscle fibers for β-dystroglycan, caveolin-3, and neuronal nitric oxide synthase nNOS, which are all membrane-linking proteins associated with the dystrophin C-terminus. The immunoreaction for nNOS was generally weak or absent, while β-dystroglycan and caveolin-3 showed a moderate to strong immunoreactivity. Basement membrane protein laminin was intact, and utrophin was not upregulated in any fibers.
The uvula muscle of soft palate in patients (paper II-IV)
Morphology
In the soft palate of patients, the uvula muscles displayed loosely packed fibers with a more round than polygonal shape. The muscle samples differed significantly from those of controls by having 9% greater fiber size variability (CV, coefficient of variation, p=0.02), i.e., a larger number of hypo- and hypertrophied fibers, as well as the presence of fascicular and group atrophy. In the scanned sections, the area occupied by muscle fibers was 10% lower in patients than in controls. Conversely, there was 10% larger amount of connective tissue compared to controls (p=0.04, respectively) (Fig. 7).
Fig 7. Uvula muscle cross-sections stained with hemotoxylin and eosin (H&E) in a control (A) and a patient (B). Notice the loosely packed muscle fibres, pronounced fibre size variability and increase in connective tissue in patients (B) compared to controls (A). Scale bar=200µm.

23
Immunoreactive patterns of muscle cytoskeleton and membrane proteins
Desmin and dystrophin C-terminus negative fibers. In snoring and sleep apnea patients, the desmin-negative fibers were significantly higher in number compared to in voluntary controls (25±12 vs. 14±7 %, p=0.009). Muscle fibers lacking expression for dystrophin C-terminus were also significantly more frequent in patients than in controls (19±18 vs. 7±2 %, p=0.04). Muscle fibers negative for both the desmin and dystrophin C-terminus were significantly more frequent in patients than in controls (15±12% vs. 3±1%, p=0.002) (Fig. 8). The desmin-negative fibers in patients were predominantly found in slow-contracting type I fibers (64±22%), and they often showed subsarcolemmal aggregations of desmin (Fig 8 D).
Desmin-disorganized fibers. A subgroup of muscle fibers in uvula from snoring and sleep apnea patients expressed abnormally distributed desmin, referred to as desmin-disorganized fibers. The disorganized immunoreaction of desmin ranged from fibers expressing small punctate or large aggregates to lobulated or trabecular patterns with areas lacking desmin (Fig. 9). Desmin-disorganized fibers were observed in 21±13% of the fiber population in patients, while they
Fig. 8. Muscle cross-sections stained for desmin (A, D), dystrophin (B, E) and merged for desmin and dystrophin (C, F) in the uvular muscle of a control (A-C) and a patient (D-F). Note a subgroup of muscle fibers lacking or almost lacking expression for desmin and dystrophin C terminus (*) in both controls and patients. Scale bar=50 µm.

24
were rare or absent in voluntary controls (1.0±0.9, p<0.001). No specific fiber type predilection was observed for fibers with disorganized desmin.
In longitudinal muscle sections from patients, some of the fibers showed disruptions in the normal striations of desmin in the Z-band region of the sarcomere, while others displayed complete disorganization or absence of desmin. Most fibers lacking desmin often showed aggregates of desmin subsarcolemmally and along the myofibrils (Fig. 9).
Desmin-deficient fibers. The pooled fraction of desmin-negative and desmin-disorganized fibers, referred to as desmin-deficient fibers, was significantly higher in patients (46±18%) than in voluntary controls (15±6%, <0.001).
Membrane proteins laminin and utrophin. Basement membrane laminin was intact in all muscle fibers. Utrophin was not present in the membrane of any muscle fibers.
Immunoreactive patterns of neurotrophins in muscle fibers
A subpopulation of muscle fibers showed immunoreaction for BDNF in the uvula muscle of both patients and voluntary controls. Two types of immunoreaction patterns were observed, one in both patients and voluntary controls and the other mainly in patients. The first reaction patterns displayed an even distribution of a fine grainy point like staining reaction (41±23 vs. 25±17%, respectively, p=0.06), while the other pattern, mainly observed in muscle fibers of patients, was expressed as a dotted to disorganized intense
Fig. 9. Muscle cross-sections (A-C) stained for desmin in the uvular muscle of patients. Note the presence of desmin-disorganized muscle fibers expressing small punctate immunoreaction (arrowheads, A) or large aggregates in a trabecular pattern (small arrows in B). Note also the disruptions of desmin in the longitudinal section (arrows). Scale bar=25 µm.

25
reaction (8±8 vs. 2±2%, p=0.02). No immunoreaction for nerve growth factor (NGF) was observed in muscle fibers of uvula in both controls and patients.
Immunoreactive patterns of neurotrophin BDNF in relation to desmin
Muscle fibers with upregulated immunoreaction for BDNF also often showed disorganized desmin immunoreaction. The muscle fibers showing none or a grainy point like distribution of BDNF had a normal immunoreaction for desmin.
BDNF expression in muscle fibers of patients with and without swallowing dysfunction
Patients with swallowing dysfunction showed a significantly higher proportion of muscle fibers with upregulated BDNF expression compared to patients without swallowing dysfunction (10±8% vs. 3±3% p=0.05)
Soft palate nerves (paper IV)
Nerve fascicle morphology
The density of axons in nerve fascicles was significantly lower in patients than in controls (5.4±2.0 vs. 17.9±10.6 x 10-3 axons/µm2, p<0.02). Clusters of fine-sized axons embedded in Schwann cells were more common in nerve fascicles of patients, but due to technical reason, they were not included in the quantification of axon density.
Compared with controls, Schwann cells occupied a significantly smaller area within the nerve fascicles of patients (45.2±7.1% vs. 17.5±6.5%, p=0.001). The number of circular shaped Schwann cells lacking central axons within nerve fascicles was significantly higher in patients than in controls (43.0±16.6 vs. 12.7±7.6% respectively, p<0.001). In the nerve fascicles, the area occupied by connective tissue was 36% larger in patients (p<0.001) (Fig. 10). Immunoreaction for mAb GAP43, known to stain growth cones in regenerating axons, was commonly observed in nerve fascicles of patients but was rare in controls.

26
Neuromuscular changes in patients with vs. without swallowing dysfunction (paper II and IV)
Immunoreactive patterns of muscle cytoskeleton in patients with and without a swallowing dysfunction
Desmin-negative fibers were significantly more prevalent in patients with a swallowing dysfunction (29±10%) compared with patients without a swallowing dysfunction (13±5%), p<0.001. There was a significant relationship between the proportion of desmin-negative fibers and the degree of swallowing dysfunction (rs =0.72, p< 0.001).
Desmin-disorganized fibers corresponded to 25±12% of muscle fibers in patients with a swallowing dysfunction vs. 9±4% in patients without a swallowing dysfunction, p<0.001. A significant correlation was found between desmin-disorganized fibers and the degree of swallowing dysfunction (rs=0.53, p=0.01).
Desmin-deficient fibers, i.e. the pooled proportion of desmin-negative and desmin-disorganized fibers, were 55±10% in patients with a swallowing dysfunction vs. 22±6% in patients with a normal swallowing function, p<0.001. The proportion of desmin-deficient fibers correlated with the degree of swallowing dysfunction (rs = 0.76, p<0.001).
Dystrophin C-terminus-negative fibers were more frequent in patients with swallowing dysfunction versus patients with normal function, but no significant difference was observed (9±8% vs. 22±19%, respectively, p=0.09). The frequency of fibers lacking both dystrophin C-terminus and desmin was also higher in patients with a swallowing dysfunction than in patients with a normal function (18±13% vs. 7±5%, p=0.007).
Nerve fascicle morphology in patients with and without a swallowing dysfunction
There was a significant correlation between the low density of axons in nerve fascicles and the degree of pharyngeal swallowing dysfunction in snorers and sleep apnea patients (rs=0.5, p=0.03). The percentage of circular shaped Schwann cells lacking central axons was significantly higher in patients with a pharyngeal swallowing dysfunction compared with patients with a normal function (47.7±14.1 vs. 28.0±15.3%, p=0.001)
Cross-reference with control autopsies (paper II and IV)
No significant differences in the proportion of cytoskeletal abnormalities in

27
muscle fibers and axon density and Schwann cell area within nerve fascicles were observed between control autopsies and control biopsies. There was a statistical difference between patients and voluntary controls as well as between patients and control autopsies in neuromuscular changes.
Comparison between neuromuscular abnormalities and AHI in patients (paper II and IV)
All samples from snoring and sleep apnea patients had neuromuscular abnormalities in the soft palate. However, there was no significant correlation between the degree of AHI and neuromuscular abnormalities.

28
Discussion
Main findings
The major findings of this thesis are the presence of both myopathy and neuropathy in the soft palate of snorers and sleep apnea patients and these neuromuscular changes related to the degree of pharyngeal swallowing dysfunction. Moreover, the soft plate muscles in both healthy subjects and patients revealed unique fibers indicating that these muscles might be of a separate allotype.
Novel cytoarchitecture of soft palate muscles in humans (Paper I)
A sub-group of muscle fibers in the uvula and palatopharyngeus muscles of healthy humans lacked expression for the vital cytoskeletal intermediate protein desmin and had a trunked form of dystrophin, i.e. lacking expression for the C-terminus of the dystrophin molecule. In human limb muscles, abnormal expression or substitute isoforms of these ubiquitous cytoskeletal muscle proteins has only been reported in genetic muscular disorders (Fuchs and Weber, 1994, Campbell, 1995, Clemen et al., 2013).
Most of the fibers lacking immunoreaction for the C-terminus of dystrophin were also unreactive for desmin. Interestingly, desmin is indirectly connected to the C-terminus domain of the dystrophin molecule, which reflects a unique molecular linkage between desmin and dystrophin. Accordingly, this subgroup of atypical muscle fibers may have special biomechanical properties influencing fiber stiffness, sarcolemma deformability, stability of costameres, contraction velocity and transmission of forces to the extracellular matrix.
Considering the complex anatomy of the soft palate with muscles interacting against each other from different directions and lacking skeletal attachment either at one or both ends, the presence of a unique cytoarchitecture could be an evolutionary specialization to meet complex demands in various oro-pharyngeal functions.
Cytoskeletal abnormalities in the uvula muscle of the soft palate in patients (paper II)
The muscle samples from the patients revealed substantial cytoskeletal abnormalities compared to controls. A significantly higher number of muscle fibers in patients than in controls revealed an absence, disorganization, molecular disruption or modification of cytoskeletal proteins desmin and

29
dystrophin. These abnormalities resembled changes found in some genetic myopathies (Campbell, 1995, Clemen et al., 2013, Ng et al., 2012).
Muscle fibers lacking desmin, i.e., desmin-negative fibers, were 44% more frequent in patients than in controls. The presence of these fibers in both controls and patients further indicates a new muscle fiber allotype in the soft palate of humans. Since knock-out or mutation of the desmin gene leads to muscle weakness (Milner et al., 1996, Milner et al., 2000, Sam et al., 2000), an individual inheriting a large proportion of desmin-negative fibers might have weaker upper airway muscles (Sam et al., 2000). Alternatively, the over-representation of desmin-negative fibers in patients might be due to a harmful load on the palatal muscles in an attempt to keep the airway patent during sleep. Transient loss of desmin in skeletal muscles has been shown following acute or eccentric activity in animal studies (Lieber et al., 1996, Barash et al., 2002).
The high frequency of desmin-disorganized fibers in patients, which were rare or absent in controls, suggests that the disruption of desmin probably is a locally acquired phenomenon. Since it has been reported that denervation of muscle fibers does not disrupt desmin (Thornell, 1983), the presence of cytoskeletal disorganization is most likely due to myofibrillar trauma rather than a consequence of nerve damage. Interestingly, the disorganization of desmin largely resembles the mitochondrial disorganization previously reported in muscular dystrophies and in the soft-palate muscles of snoring and sleep apnea patients (Calore et al., 1994, Stål and Johansson, 2012). Since desmin have links to mitochondria (Small et al., 1992, Fuchs and Weber, 1994, Milner et al., 2000), and mutant desmin substantially disturbs mitochondrial organization and function in skeletal muscle tissue (Winter et al., 2016), desmin disruptions may be the cause for maldistribution of mitochondria in muscle fibers of snorers and sleep apnea patients (Stål et al., 2009). Accordingly, disruption of desmin might result in mitochondria disturbances leading to lowered energy production and muscle weakness. These changes may have the potential to affect pharyngeal muscle function.
Approximately 20% of the muscle fibers in patients had truncated dystrophin. While the N-terminus and rod domain of the dystrophin molecule were present, the C-terminus was missing. The C-terminus of dystrophin is important for normal muscle function, as it binds to the glycoprotein complex in the sarcolemma and transfers forces from the contractile apparatus to the extracellular matrix and adjoining muscle fibers (Campbell, 1995, Rahimov and Kunkel, 2013). Studies have demonstrated that force production is significantly reduced in dystrophin-deficient muscle fibers (Deconinck et al., 1998). Furthermore, dystrophin-deficient sarcolemma is reported to be fragile, and

30
muscle activity results in the increased permeability of membrane-impermeable molecules. In Duchenne muscular dystrophy, loss or truncated forms of dystrophin leave the membrane highly susceptible to contraction-induced injury and hypoxic stress (Greenberg et al., 1994, Banks et al., 2014), resulting in detrimental consequences for the intra-myofibrillar environment. Consequently, the high number of dystrophin C-terminus-deficient fibers in snorers and sleep apnea patients might render the muscle weaker and more vulnerable to high contraction stress. No upregulation of utrophin, a paralog of dystrophin, was found in the muscle fibers missing dystrophin C-terminus. Utrophin is expressed on the sarcolemma of developing and regenerating fibers, but it is ultimately replaced by dystrophin in maturing fibers (Love et al., 1989). In Duchenne muscular dystrophy, where dystrophin is lacking, utrophin is strikingly upregulated.
Upregulation of BDNF in muscle fibers (Paper III)
Two main expression patterns of BDNF were observed in a subgroup of muscle fibers in the soft palate of both snoring and sleep apnea patients and controls. One of the reaction patterns displayed an even distribution of a fine grainy point like staining reaction, while the other pattern, which was mainly observed in muscle fibers of patients, was expressed as a dotted to a disorganized intense reaction. The muscle fibers expressing an even point-like grainy pattern of BDNF, which were present in both controls and patients, seems to be a normal biological state (Liem et al., 2001). However, there was a tendency to be more of these fibers in patients. The observation of BDNF in muscle cells support previous postulations that muscles have autocrine, paracrine and trophic effects (Koliatsos et al., 1993, Matthews et al., 2009, Pedersen and Febbraio, 2012).
The muscle fibers displaying an upregulated BDNF expression in a dotted to disorganized pattern were mainly observed in patients. These fibers often showed disruption of intermediate filament protein desmin indicating muscle fiber injury. An increase in BDNF mRNA within skeletal muscle has previously been shown in both humans and animals in response to various physical exercises, electrical muscle stimulation, and muscle overload (Dupont-Versteegden et al., 2004, Cuppini et al., 2007, Matthews et al., 2009, Ogborn and Gardiner, 2010). It has also been shown that BDNF is upregulated in denervated muscle fibers possibly to attract motor-nerves for reinnervation (Koliatsos et al., 1993, Zhang et al., 2000). However, since fibers showing upregulation of BDNF often had desmin disruption, which normally is not a consequence of denervation (Thornell, 1983), muscle injury is a more likely cause. Thus, the higher proportion of fibers expressing BDNF in patients may be related to a higher load on upper airway muscles to uphold the patency during sleep or due to local trauma. The higher proportion of fibers expressing BDNF

31
could be related to an attempt for repair and regeneration.
Changes in preterminal nerve fascicles (Paper IV)
The preterminal nerves in the upper airway of snorers and sleep apnea patients revealed significant polymorphic changes indicating injury. A significantly lower density of axons within the nerve fascicle and a higher proportion of Schwann cells lacking central axons were present in the soft palate of patients compared to controls. Moreover, the area occupied by Schwann cells in the nerve fascicles of patients was also significantly lower.
Schwann cells are known to maintain homeostasis and provide support, nutrition, and protection for axons in the peripheral nervous system. Myelination for axons is provided by the Schwann cells wrapping around them to form a fatty layered sheath, making the conduction velocity of the nerve faster, while non-myelinating Schwann cells surround small-sized sensory and to some extent autonomic sympathetic axons. The significantly smaller area occupied by Schwann cell in the nerve fascicles together with a large number of Schwann cells lacking large central axons reflect both demyelination and loss of motor axons in sleep apnea patients.
The nerve fascicles from patients also contained a relatively large number of fine-sized axons. Most of these axons were gathered in clusters separated by Schwann cells, but some were randomly scattered throughout the nerve fascicles. Interestingly, a large number of fine sized axons in the patients, but not in controls, were immunostained for neuromodulin, or GAP-43, an intracellular growth-associated protein involved in axon regeneration during development. Following nerve damage, an increase in the expression of GAP-43 can be observed in the growth cones of axons (Chen et al., 2013). The extensive expression of GAP-43 in axons in snorers and sleep apnea patients highlights a regenerative process in the nerves, most likely subsequent to nerve injuries in the upper airway of snorers and sleep apnea patients.
It is known that Schwann cells play a role in axon regeneration by producing neurite-promoting factors which help axon growth cones adhere to endoneurial tubes (Guenard et al., 1991). Hence, the reduced Schwann cell number in nerves might adversely affect the regenerative capacity of axons in snorers and sleep apnea patients.

32
Neuromuscular changes correlate with pharyngeal swallowing dysfunction in snorers and sleep apnea patients (paper II and IV)
In humans swallowing and respiratory function are complex neuromuscular activities, and the central reflex control system is dependent on an efficient feedback mechanism. Any deficit either in the neural circuits or in oro-pharyngeal musculature has the potential to adversely affect the efficiency of swallowing and upper airway function.
The most common finding of swallowing dysfunction in patients was premature leakage with bolus passing into pharynx without eliciting a swallow, pointing at a loss of sensibility for initiation of the swallow when bolus passed the pharyngeal pillars. This implies an increased risk of aspiration if the patient rapidly inhales while the bolus passively passes into pharynx and an open airway. Another common finding was residual remnants of the bolus in pharynx after the swallow was finalized, also pointing at a loss of sensibility in the region, or a second swallow would otherwise have been initiated, pointing at ineffective muscle function, not efficient to empty the pharynx (unpublished observations).
In this study, we found that changes in both nerves and muscles of the soft palate correlated significantly with pharyngeal swallowing dysfunction in patients. There was a significant correlation between the low density of axons in nerve fascicles and swallowing dysfunction. Moreover, the proportion of Schwann cells lacking central axons was significantly higher in patients with a pharyngeal swallowing dysfunction compared with patients with a normal function, reflecting axon loss. Interestingly, the presence of desmin-deficient fibers also correlated significantly with findings of pharyngeal swallowing dysfunction. These findings highlight a neuromuscular deficit in the pharyngeal region of snores and sleep apnea patients. The presence of both neuropathy and myopathy may have a synergetic effect on pharyngeal function.
Neuromuscular changes and AHI
The lack of a significant correlation between the degree of AHI and severity of neuromuscular abnormalities reflects the complex interaction of several central and peripheral etiological risk factors in development and progression of sleep apnea. Hence, neuromuscular injuries alone will not determine the degree of AHI (Hudgel, 2016). However, swallowing dysfunction in sleep apnea patients seems to be an indicator for the presence of neuromuscular injuries in the upper airway.

33
Muscle changes reflecting neuropathy and myopathy in the upper airway
Several pathological features in the soft palate muscles can be discussed concerning both neuropathic and myopathic changes. Our findings revealed both fiber atrophy and hypertrophy, as well as group and fascicular atrophy and loss of muscle mass. The high number of small atrophied fibers might be due to muscle fiber denervation and degeneration, while the large number of hypertrophic fibers can be related to a compensatory process in which remaining innervated muscle fibers are more frequently used to uphold function. Myopathic changes are highlighted by our observation of muscle fibers with cytoskeletal abnormalities and disorganized mitochondria in soft palate muscle of snores and sleep apnea patients (Stal and Johansson, 2012). These changes probably decrease the capability of the muscle cell to generate energy and force.
Our research group has previously reported that a subgroup of fibers in the soft palate muscles of snorers and sleep apnea patients express a developmental protein isoform (fetal MyHC) (Lindman and Stål, 2002), Fetal MyHC is normally only expressed in the early stages of muscle fiber development, but is upregulated in muscle fibers in regeneration after injury (Schiaffino et al., 1986). The presence of muscle fibers containing developmental MyHC in the upper airway, suggests a parallel process of muscle injury, denervation, degeneration, and regeneration.
Together, the muscle abnormalities in the soft palate strongly indicate that both myopathy and motor neuropathy have a role in the pathophysiology of pharyngeal swallowing dysfunction and OSA.
The possible cause of neuromuscular changes and pharyngeal dysfunction in snorers and sleep apnea patients
The patency of the upper airway depends on an efficient feedback mechanism reacting to the negative intra-pharyngeal pressure at inspiration. Breathing through a narrowed airway generates a greater intraluminal negative pressure, which increases the collapsing forces so that pharyngeal muscles have to contract more forcefully (Deegan and McNicholas, 1995). Risk factors such as obesity and enlarged tonsils will aggravate narrowing of the upper airway. During sleep, when the tonic activity of dilator muscles decreases, and gravity negatively influences the width of the pharyngeal lumen, an ineffective response in the dilator muscles may result in upper airway collapse during inspiration. Effective responses of pharyngeal dilators are therefore crucial for keeping the respiratory tract open and this, in turn, depends on both intact sensory-motor

34
reflexes and healthy functional muscles. Our findings of both nerve and muscle injuries in the soft palate that correlates to pharyngeal swallowing dysfunction in snoring and sleep apnea patients highlight that the pathophysiological mechanism of airway instability during sleep is multifactorial, including anatomical, neurophysiological and neuromuscular factors (Dempsey et al., 2010).
The mechanism behind the neuromuscular abnormalities is unclear, although snoring vibratory trauma, muscle overload, tissue stretch, inflammation, and hypoxia all have been discussed as potential causes of nerve injuries in the upper airway (Petrof et al., 1996, Friberg et al., 1997, Mayer et al., 1999, Svanborg, 2001, Boyd et al., 2004, Kimoff, 2007). Since sleep apnea frequently is preceded by years of snoring, traumatic vibrations and tissue stretch appear to be major initiating factors for neuromuscular injuries in the upper airway (Svanborg and Larsson, 1993, Petrof et al., 1996, Lugaresi and Plazzi, 1997, Friberg et al., 1997, Rodrigues HP, 2005). It is well known that long-standing exposure to mechanical vibrations in limbs cause nerve lesions, disturbed cytoarchitecture in muscle cells, vasospasm, reduced blood flow, loss of capillaries and mitochondria and reduced muscle strength (Curry et al., 2002, Necking et al., 2004, Murfee et al., 2005). Animal models have also shown that prolonged vibration causes structural damage to the nerve myelin sheath (Davis et al., 2014). Moreover, disorganized mitochondria, together with our previous findings of reduced capillarization in the palatal muscles of long-term snorers (Stal et al., 2009), underpins lowering of energy production, resulting in muscle weakness. The lowered capillarization also suggests a potential for developing local hypoxia followed by neuropathy. Moreover, stretch trauma as well as eccentric exercise have also been reported to cause histopathological changes and transient loss of desmin in skeletal muscles (Lieber et al., 1996, Barash et al., 2002), a finding indicating muscle overload in snorers and sleep apnea patients.
Therefore, the present findings point towards traumatic snoring vibrations, muscle overload and tissue stretch as causes for injuries in nerves and muscles disturbing the reflex circuits responsible for normal swallowing function and patency of the upper airway. Any changes that render the upper-airway muscles less capable of generating force have the potential to affect pharyngeal function.
Conclusions
In the present project, we found that the human soft palate muscles of healthy individuals differ from limb muscles in their expression of cytoskeletal proteins. A subgroup of muscle fibers lacked expression for desmin and had a truncated

35
isoform of dystrophin. This cytoarchitecture may reflect muscle specialization to meet complex requirements in various oropharyngeal functions. The findings also challenge the present concept of desmin and other cytoskeletal proteins as ubiquitous components in skeletal muscles. Interestingly, fibers expressing abnormal immunoreaction for desmin and dystrophin were overrepresented in the soft-palate muscles of snoring and sleep apnea patients. Since it has been shown that absence of desmin and dystrophin results in muscle weakness, this raises important questions whether these cytoskeletal abnormalities in snoring and OSA patients are inherited or a consequence of muscle overload or trauma. Nevertheless, the significant proportion of muscle fibers with disorganized or disrupted expression of desmin in patients, but not in controls, highlights the presence of myopathic changes, possibly acquired by traumatic snoring and tissue stretch. Muscle fiber injury is further strengthened by the upregulation of BDNF in desmin-disorganized fibers. Since BDNF is known to have trophic and autocrine/paracrine functions, this upregulation could be an attempt for tissue repair after injury.
Importantly, polymorphic changes in nerve fascicles were significantly more frequent in patients than in controls and correlated to swallowing dysfunction, highlighting nerve injury in the pharyngeal region. The correlation of swallowing dysfunction to both nerve and muscle changes indicates a synergistic effect of these changes on pharyngeal function, although the nerve injuries most likely have an important role in the pathophysiology of pharyngeal dysfunction. The lack of a significant correlation between neuromuscular abnormalities and AHI emphasize that there are several factors interacting to cause obstruction of the upper airway in OSA patients.
Taken together, acquired neuromuscular changes seem to contribute to disturbed reflexogenic feedback mechanism and muscle weakness in the upper airway in snoring and sleep apnea patients. Therefore, acquired neuropathy and myopathy can be considered as risk factors for pharyngeal swallowing dysfunction and OSA.
Summary
• Healthy human soft palate muscles contain unique muscle fibers lacking expression of intermediate filament protein desmin and having a truncated dystrophin
• Muscle fibers lacking desmin and having truncated dystrophin were significantly more frequent in the soft palate of snorers and sleep apnea patients compared to controls

36
• A significant proportion of muscle fibers with a disorganized expression
of desmin were present in the soft palate of patients, but not in controls
• Muscle fibers with abnormal desmin immunoreaction often showed upregulation of the neurotrophin BDNF
• The preterminal nerve fascicles in the soft palate showed significantly lower axon density and Schwann cell area in snorers and sleep apnea patients.
• The neuromuscular changes observed in the soft palate of patients correlated significantly with pharyngeal swallowing dysfunction

37
Funding
Financial support was obtained from Swedish Heart and Lung Foundation (Dnr 20110210, 20140339), the JC Kempe Memorial Scholarship Foundation, the Swedish Dental Society and Insamlingsstiftelsen Umeå University (Dnr 223-1881-13).
Funding agencies had no role in the study design, data collection, analysis and preparation of the manuscripts.

38
Acknowledgments
Gratitude is the finest form of human expression. It has been a pleasure and a rich learning experience to be a part of Integrative Medical Biology. I would gladly take this opportunity to thank all the wonderful people whom I associated with on my journey of knowledge. I am extremely thankful to Docent Per Stål, my supervisor and friend, who with his wisdom and enthusiasm have helped me steer through research. Your guidance and help are the foundation for this achievement. My co-supervisor Professor Sture Forsgren, who helped me keep my nerves while studying the nerves. Your patience and understanding are deeply admired. I am also thankful to my co-supervisor Professor Diana Berggren for your interest, wisdom, generosity, and involvement in the project. Special thanks to Anna-Karin Olofsson for your splendid laboratory skills, administrative capacity, and always ready to help. I extend warm thanks to my co-authors: Eva Levring Jäghagen for your amazing support, smart advice, and positivity, Thorbjörn Holmlund for being an encouraging co-author, your timely help and being a wonderful friend, Karl Franklin, for your valuable insight and helpful comments, now I know how to cut short an article. Professor Lars-Eric Thornell for your interest, keen eye and meaningful advice for my research and your good humor. To Göran Dahlgren for your persistent help in keeping my data safe and interesting discussions about market investments. Peyman Kelk for being so inspiring, intelligent, always ready to help, and being a family friend. Paul Kingham for all the help with Schwann cells findings. Gustav Andersson for the illustration in the first article and always being nice and helpful. My gratitude is due to Fatima Pedrosa Domellöf, for your energy and encouragement at every step of the way. I am thankful to Anton Tjust for all the help in academics, encouragement and wonderful socializing. Karl Gunner Westberg, for your concern and thoughtfulness, which adds to your excellent leadership qualities, IMB is fortunate to have you as the head. Completing this work would have been all the more difficult were it not for the support and friendship provided by Anita Dreyer-Perkiömäki, Selam Kefalawit and Kathrine Nylund for their constant willingness to help. I am also thankful to Anna-Lena Tallander, Frida Olofsson and Ulrika Rosenbrand for managing the complex finances. To my good friend Fred-Ole Laberg who was always there with his funny comments to cheer me up, you are a generous person. I like to thank faculty and all my dear colleagues during my time in the department: Mona Lindström, Jing-Xia Liu, Andre Vicente, Gunnel Folkesson, M. Angel Rodriguez Garcia, Cecilia E Fernandez-Echevarria, Lev Novikov, Ludmila Novikova, Patrik Danielson, Roine El-Habta, Juha Prittinen, Fahad Sultan, Nils Dennhag, Hanna Nord. A special thank to my friend Arvin Behzadi

39
for your company and encouragement. I am also thankful to Prof. G. Abdullah Khallaf Albadran, for his positive inspiration for pursuing Ph.D. To my wife, Nausheen, the love of my life, without you this or any journey is unimaginable. To our dearest son Adam - You are the spark of bliss and joy that adds meaning to my endeavors. To my parents for instilling in me a love for learning and my siblings for their emotional support.

40
References
ACAR, M., YAZICI, D., BAYAR MULUK, N., HANCI, D., SEREN, E. & CINGI, C. 2016. Is There a Relationship Between Snoring Sound Intensity and Frequency and OSAS Severity? Ann Otol Rhinol Laryngol., 125, 31-6. doi: 10.1177/0003489415595640. Epub 2015 Jul 14.
BAGGE, J., LORENTZON, R., ALFREDSON, H. & FORSGREN, S. 2009. Unexpected presence of the neurotrophins NGF and BDNF and the neurotrophin receptor p75 in the tendon cells of the human Achilles tendon. Histol Histopathol., 24, 839-48. doi: 10.14670/HH-24.839.
BANKS, G. B., COMBS, A. C., ODOM, G. L., BLOCH, R. J. & CHAMBERLAIN, J. S. 2014. Muscle structure influences utrophin expression in mdx mice. PLoS Genet, 10, e1004431.
BARASH, I. A., PETERS, D., FRIDEN, J., LUTZ, G. J. & LIEBER, R. L. 2002. Desmin cytoskeletal modifications after a bout of eccentric exercise in the rat. Am J Physiol Regul Integr Comp Physiol., 283, R958-63.
BASSIOUNY, A., NASR, S., MASHALY, M., AYAD, E., QOTB, M. & ATEF, A. 2009. Electron microscopy study of peripheral nerves in the uvulae of snorers and obstructive sleep apnoea patients. J Laryngol Otol., 123, 203-7. doi: 10.1017/S0022215108002971. Epub 2008 Jun 13.
BERRY, R. B., BUDHIRAJA, R., GOTTLIEB, D. J., GOZAL, D., IBER, C., KAPUR, V. K., MARCUS, C. L., MEHRA, R., PARTHASARATHY, S., QUAN, S. F., REDLINE, S., STROHL, K. P., DAVIDSON WARD, S. L. & TANGREDI, M. M. 2012. Rules for scoring respiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med., 8, 597-619. doi: 10.5664/jcsm.2172.
BHATTACHARYYA, N., BLAKE, S. P. & FRIED, M. P. 2000. Assessment of the airway in obstructive sleep apnea syndrome with 3-dimensional airway computed tomography. Otolaryngol Head Neck Surg., 123, 444-9. doi: 10.1067/mhn.2000.109367.
BLAKE, D. J., TINSLEY, J. M. & DAVIES, K. E. 1996. Utrophin: a structural and functional comparison to dystrophin. Brain Pathol, 6, 37-47.
BOYD, J. H., PETROF, B. J., HAMID, Q., FRASER, R. & KIMOFF, R. J. 2004. Upper airway muscle inflammation and denervation changes in obstructive sleep apnea. Am J Respir Crit Care Med., 170, 541-6. Epub 2004 May 19.
CALORE, E. E., CAVALIERE, M. J., WAKAMATSU, A., PEREZ, N. M., MAEDA, M. Y. & RUSSO, D. H. 1994. An unusual case of muscular limb-girdle dystrophy and mitochondrial myopathy. Pathologica., 86, 649-51.
CAMPBELL, K. P. 1995. Three muscular dystrophies: loss of cytoskeleton-extracellular matrix linkage. Cell., 80, 675-9.
CAPETANAKI, Y., BLOCH, R. J., KOULOUMENTA, A., MAVROIDIS, M. & PSARRAS, S. 2007. Muscle intermediate filaments and their links to membranes and membranous organelles. Exp Cell Res., 313, 2063-76. Epub 2007 Apr 3.

41
CHEN Z, LEE H, HENLE SJ, CHEEVER TR, EKKER SC, HENLEY JR. Primary neuron culture for nerve growth and axon guidance studies in zebrafish (Danio rerio). PLoS One. 2013;8(3):e57539.
CHERVIN, R. D. 2000. Sleepiness, fatigue, tiredness, and lack of energy in obstructive sleep apnea. Chest., 118, 372-9.
CHEVREL, G., HOHLFELD, R. & SENDTNER, M. 2006. The role of neurotrophins in muscle under physiological and pathological conditions. Muscle Nerve., 33, 462-76. doi: 10.1002/mus.20444.
CLEMEN, C. S., HERRMANN, H., STRELKOV, S. V. & SCHRODER, R. 2013. Desminopathies: pathology and mechanisms. Acta Neuropathol., 125, 47-75. doi: 10.1007/s00401-012-1057-6. Epub 2012 Nov 11.
CUPPINI, R., SARTINI, S., AGOSTINI, D., GUESCINI, M., AMBROGINI, P., BETTI, M., BERTINI, L., VALLASCIANI, M. & STOCCHI, V. 2007. Bdnf expression in rat skeletal muscle after acute or repeated exercise. Arch Ital Biol., 145, 99-110.
CURRY, B. D., BAIN, J. L., YAN, J. G., ZHANG, L. L., YAMAGUCHI, M., MATLOUB, H. S. & RILEY, D. A. 2002. Vibration injury damages arterial endothelial cells. Muscle Nerve, 25, 527-34.
DAVIS, J., WANG, Z., ZHANG, L. L., AGRESTI, M., MATLOUB, H. S. & YAN, J. G. 2014. A quantitative study of vibration injury to peripheral nerves-introducing a new longitudinal section analysis. Hand (N Y). 9, 413-8. doi: 10.1007/s11552-014-9668-0.
DECONINCK, N., RAFAEL, J. A., BECKERS-BLEUKX, G., KAHN, D., DECONINCK, A. E., DAVIES, K. E. & GILLIS, J. M. 1998. Consequences of the combined deficiency in dystrophin and utrophin on the mechanical properties and myosin composition of some limb and respiratory muscles of the mouse. Neuromuscul Disord., 8, 362-70.
DEEB, R., JUDGE, P., PETERSON, E., LIN, J. C. & YAREMCHUK, K. 2014. Snoring and carotid artery intima-media thickness. Laryngoscope., 124, 1486-91. doi: 10.1002/lary.24527. Epub 2014 Jan 28.
DEEGAN, P. C. & MCNICHOLAS, W. T. 1995. Pathophysiology of obstructive sleep apnoea. Eur Respir J., 8, 1161-78.
DEMPSEY, J. A., VEASEY, S. C., MORGAN, B. J. & O'DONNELL, C. P. 2010. Pathophysiology of sleep apnea. Physiol Rev., 90, 47-112. doi: 10.1152/physrev.00043.2008.
DEWAN, N. A., NIETO, F. J. & SOMERS, V. K. 2015. Intermittent hypoxemia and OSA: implications for comorbidities. Chest, 147, 266-274.
DUPONT-VERSTEEGDEN, E. E., HOULE, J. D., DENNIS, R. A., ZHANG, J., KNOX, M., WAGONER, G. & PETERSON, C. A. 2004. Exercise-induced gene expression in soleus muscle is dependent on time after spinal cord injury in rats. Muscle Nerve., 29, 73-81. doi: 10.1002/mus.10511.
ECKERT, D. J., LO, Y. L., SABOISKY, J. P., JORDAN, A. S., WHITE, D. P. & MALHOTRA, A. 2011. Sensorimotor function of the upper-airway muscles and respiratory sensory processing in untreated obstructive sleep apnea. J Appl Physiol (1985). 111, 1644-53. doi: 10.1152/japplphysiol.00653.2011. Epub 2011 Sep 1.
EDSTRÖM, L., LARSSON, H. & LARSSON, L. 1992. Neurogenic effects on the palatopharyngeal muscle in patients with obstructive sleep apnoea: a muscle biopsy study. J Neurol Neurosurg Psychiatry., 55, 916-20.

42
ENGLEMAN, H. M. & DOUGLAS, N. J. 2004. Sleep. 4: Sleepiness, cognitive function, and quality of life in obstructive sleep apnoea/hypopnoea syndrome. Thorax., 59, 618-22.
FRANKLIN, K. A. & LINDBERG, E. 2015. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis., 7, 1311-22. doi: 10.3978/j.issn.2072-1439.2015.06.11.
FRIBERG, D., ANSVED, T., BORG, K., CARLSSON-NORDLANDER, B., LARSSON, H. & SVANBORG, E. 1998. Histological indications of a progressive snorers disease in an upper airway muscle. Am J Respir Crit Care Med., 157, 586-93.
FRIBERG, D., GAZELIUS, B., HOKFELT, T. & NORDLANDER, B. 1997. Abnormal afferent nerve endings in the soft palatal mucosa of sleep apnoics and habitual snorers. Regul Pept., 71, 29-36.
FUCHS, E. & WEBER, K. 1994. Intermediate filaments: structure, dynamics, function, and disease. Annu Rev Biochem, 63, 345-82.
GARVEY, J. F., PENGO, M. F., DRAKATOS, P. & KENT, B. D. 2015. Epidemiological aspects of obstructive sleep apnea. J Thorac Dis, 7, 920-9.
GOTTLIEB, D. J., YAO, Q., REDLINE, S., ALI, T. & MAHOWALD, M. W. 2000. Does snoring predict sleepiness independently of apnea and hypopnea frequency? Am J Respir Crit Care Med., 162, 1512-7. doi: 10.1164/ajrccm.162.4.9911073.
GRAY, E. L., MCKENZIE, D. K. & ECKERT, D. J. 2017. Obstructive Sleep Apnea without Obesity Is Common and Difficult to Treat: Evidence for a Distinct Pathophysiological Phenotype. J Clin Sleep Med., 13, 81-88. doi: 10.5664/jcsm.6394.
GREENBERG, D. S., SUNADA, Y., CAMPBELL, K. P., YAFFE, D. & NUDEL, U. 1994. Exogenous Dp71 restores the levels of dystrophin associated proteins but does not alleviate muscle damage in mdx mice. Nat Genet., 8, 340-4.
GRIESBECK, O., PARSADANIAN, A. S., SENDTNER, M. & THOENEN, H. 1995. Expression of neurotrophins in skeletal muscle: quantitative comparison and significance for motoneuron survival and maintenance of function. J Neurosci Res., 42, 21-33. doi: 10.1002/jnr.490420104.
GUENARD, V., VALENTINI, R. F. & AEBISCHER, P. 1991. Influence of surface texture of polymeric sheets on peripheral nerve regeneration in a two-compartment guidance system. Biomaterials., 12, 259-63.
GUILLEMINAULT, C., LI, K., CHEN, N. H. & POYARES, D. 2002. Two-point palatal discrimination in patients with upper airway resistance syndrome, obstructive sleep apnea syndrome, and normal control subjects. Chest., 122, 866-70.
GUILLEMINAULT, C., LIN, C. M., GONCALVES, M. A. & RAMOS, E. 2004. A prospective study of nocturia and the quality of life of elderly patients with obstructive sleep apnea or sleep onset insomnia. J Psychosom Res., 56, 511-5. doi: 10.1016/S0022-3999(04)00021-2.
HERRMANN, H. & AEBI, U. 2000. Intermediate filaments and their associates: multi-talented structural elements specifying cytoarchitecture and cytodynamics. Curr Opin Cell Biol, 12, 79-90.

43
HOFFSTEIN, V., MATEIKA, S. & METES, A. 1993. Effect of nasal dilation on snoring and apneas during different stages of sleep. Sleep., 16, 360-5.
HONG, S. N., YOO, J., SONG, I. S., JOO, J. W., YOO, J. H., KIM, T. H., LEE, H. M., LEE, S. H. & LEE, S. H. 2017. Does Snoring Time Always Reflect the Severity of Obstructive Sleep Apnea? Ann Otol Rhinol Laryngol., 126, 693-696. doi: 10.1177/0003489417727014. Epub 2017 Aug 23.
HORNER, R. L., INNES, J. A., HOLDEN, H. B. & GUZ, A. 1991. Afferent pathway(s) for pharyngeal dilator reflex to negative pressure in man: a study using upper airway anaesthesia. J Physiol., 436, 31-44.
HUANG, E. J. & REICHARDT, L. F. 2001. Neurotrophins: roles in neuronal development and function. Annu Rev Neurosci, 24, 677-736.
HUDGEL, D. W. 2016. Sleep Apnea Severity Classification - Revisited. Sleep, 39, 1165-6.
JAGHAGEN, E. L., BODIN, I. & ISBERG, A. 2008. Pharyngeal swallowing dysfunction following treatment for oral and pharyngeal cancer--association with diminished intraoral sensation and discrimination ability. Head Neck., 30, 1344-51. doi: 10.1002/hed.20881.
JOBIN, V., CHAMPAGNE, V., BEAUREGARD, J., CHARBONNEAU, I., MCFARLAND, D. H. & KIMOFF, R. J. 2007. Swallowing function and upper airway sensation in obstructive sleep apnea. J Appl Physiol (1985). 102, 1587-94. Epub 2006 Dec 21.
KATSANTONIS, G. P., MOSS, K., MIYAZAKI, S. & WALSH, J. 1993. Determining the site of airway collapse in obstructive sleep apnea with airway pressure monitoring. Laryngoscope., 103, 1126-31. doi: 10.1288/00005537-199310000-00009.
KIMOFF, R. J. 2007. Upperairway myopathy is important in the pathophysiology of obstructive sleep apnea. J Clin Sleep Med., 3, 567-9.
KIMOFF, R. J., SFORZA, E., CHAMPAGNE, V., OFIARA, L. & GENDRON, D. 2001. Upper airway sensation in snoring and obstructive sleep apnea. Am J Respir Crit Care Med., 164, 250-5. doi: 10.1164/ajrccm.164.2.2010012.
KOLIATSOS, V. E., CLATTERBUCK, R. E., WINSLOW, J. W., CAYOUETTE, M. H. & PRICE, D. L. 1993. Evidence that brain-derived neurotrophic factor is a trophic factor for motor neurons in vivo. Neuron., 10, 359-67.
LAL, C., STRANGE, C. & BACHMAN, D. 2012. Neurocognitive impairment in obstructive sleep apnea. Chest., 141, 1601-1610. doi: 10.1378/chest.11-2214.
LANG, I. M. 2009. Brain stem control of the phases of swallowing. Dysphagia., 24, 333-48. doi: 10.1007/s00455-009-9211-6. Epub 2009 Apr 28.
LEE, S. A., AMIS, T. C., BYTH, K., LARCOS, G., KAIRAITIS, K., ROBINSON, T. D. & WHEATLEY, J. R. 2008. Heavy snoring as a cause of carotid artery atherosclerosis. Sleep., 31, 1207-13.
LEVRING JÄGHAGEN, E., FRANKLIN, K. A. & ISBERG, A. 2003. Snoring, sleep apnoea and swallowing dysfunction: a videoradiographic study. Dentomaxillofac Radiol., 32, 311-6.
LIEBER, R. L., THORNELL, L. E. & FRIDEN, J. 1996. Muscle cytoskeletal disruption occurs within the first 15 min of cyclic eccentric contraction. J Appl Physiol (1985). 80, 278-84.
44
LIEM, R. S., BROUWER, N. & COPRAY, J. C. 2001. Ultrastructural localisation of intramuscular expression of BDNF mRNA by silver-gold intensified non-radioactive in situ hybridisation. Histochem Cell Biol., 116, 545-51. doi: 10.1007/s00418-001-0349-z. Epub 2001 Nov 27.
LINDMAN, R. & STÅL, P. S. 2002. Abnormal palatopharyngeal muscle morphology in sleep-disordered breathing. J Neurol Sci, 195, 11-23.
LINDSTRÖM, M. & THORNELL, L. E. 2009. New multiple labelling method for improved satellite cell identification in human muscle: application to a cohort of power-lifters and sedentary men. Histochem Cell Biol., 132, 141-57. doi: 10.1007/s00418-009-0606-0. Epub 2009 May 31.
LOVE, D. R., HILL, D. F., DICKSON, G., SPURR, N. K., BYTH, B. C., MARSDEN, R. F., WALSH, F. S., EDWARDS, Y. H. & DAVIES, K. E. 1989. An autosomal transcript in skeletal muscle with homology to dystrophin. Nature., 339, 55-8.
LUGARESI, E. & PLAZZI, G. 1997. Heavy snorer disease: from snoring to the sleep apnea syndrome--an overview. Respiration, 64, 11-4. doi: 10.1159/000196730.
LURIE, A. 2011. Obstructive sleep apnea in adults: epidemiology, clinical presentation, and treatment options. Adv Cardiol, 46:1-42., 10.1159/000327660. Epub 2011 Oct 13.
MAIMON, N. H. P. 2010. Does Snoring Intensity Correlate with the Severity of Obstructive Sleep Apnea? J Clin Sleep Med., 6, 475-478.
MATTHEWS, V. B., ASTROM, M. B., CHAN, M. H., BRUCE, C. R., KRABBE, K. S., PRELOVSEK, O., AKERSTROM, T., YFANTI, C., BROHOLM, C., MORTENSEN, O. H., PENKOWA, M., HOJMAN, P., ZANKARI, A., WATT, M. J., BRUUNSGAARD, H., PEDERSEN, B. K. & FEBBRAIO, M. A. 2009. Brain-derived neurotrophic factor is produced by skeletal muscle cells in response to contraction and enhances fat oxidation via activation of AMP-activated protein kinase. Diabetologia., 52, 1409-18. doi: 10.1007/s00125-009-1364-1. Epub 2009 Apr 22.
MAYER, P., DEMATTEIS, M., PEPIN, J. L., WUYAM, B., VEALE, D., VILA, A. & LEVY, P. 1999. Peripheral neuropathy in sleep apnea. A tissue marker of the severity of nocturnal desaturation. Am J Respir Crit Care Med., 159, 213-9. doi: 10.1164/ajrccm.159.1.9709051.
MENORCA, R. M., FUSSEL, T.S., ELFAR, J. C. 2013. Peripheral Nerve Trauma: Mechanisms of Injury and Recovery. Hand Clin, 29, 317-330.
MILNER, D. J., MAVROIDIS, M., WEISLEDER, N. & CAPETANAKI, Y. 2000. Desmin cytoskeleton linked to muscle mitochondrial distribution and respiratory function. J Cell Biol., 150, 1283-98.
MILNER, D. J., WEITZER, G., TRAN, D., BRADLEY, A. & CAPETANAKI, Y. 1996. Disruption of muscle architecture and myocardial degeneration in mice lacking desmin. J Cell Biol., 134, 1255-70.
MURFEE, W. L., HAMMETT, L. A., EVANS, C., XIE, L., SQUIRE, M., RUBIN, C., JUDEX, S. & SKALAK, T. C. 2005. High-frequency, low-magnitude vibrations suppress the number of blood vessels per muscle fiber in mouse soleus muscle. J Appl Physiol (1985). 98, 2376-80. Epub 2005 Jan 27.

45
NARKIEWICZ, K. & SOMERS, V. K. 1997. The sympathetic nervous system and obstructive sleep apnea: implications for hypertension. J Hypertens., 15, 1613-9.
NECKING, L. E., LUNDBORG, G., LUNDSTROM, R., THORNELL, L. E. & FRIDEN, J. 2004. Hand muscle pathology after long-term vibration exposure. J Hand Surg Br., 29, 431-7.
NG, R., BANKS, G. B., HALL, J. K.,MUIR, L. A, RAMOS,., WICKI, J. N., ODOM J., KONIECZNY, G. L., SETO, P., CHAMBERLAIN, J., & CHAMBERLAIN, J. S. 2012. Animal models of muscular dystrophy. Prog Mol Biol Transl Sci, 105, 83-111.
OGBORN, D. I. & GARDINER, P. F. 2010. Effects of exercise and muscle type on BDNF, NT-4/5, and TrKB expression in skeletal muscle. Muscle Nerve., 41, 385-91. doi: 10.1002/mus.21503.
OHAYON, M. M., GUILLEMINAULT, C., PRIEST, R. G. & CAULET, M. 1997. Snoring and breathing pauses during sleep: telephone interview survey of a United Kingdom population sample. BMJ., 314, 860-3.
PATEL, J. A., RAY, B. J., FERNANDEZ-SALVADOR, C., GOUVEIA, C., ZAGHI, S. & CAMACHO, M. 2018. Neuromuscular function of the soft palate and uvula in snoring and obstructive sleep apnea: A systematic review. Am J Otolaryngol, 5, 30011-5.
PAULIN, D. & LI, Z. 2004. Desmin: a major intermediate filament protein essential for the structural integrity and function of muscle. Exp Cell Res., 301, 1-7.
PEDERSEN, B. K. & FEBBRAIO, M. A. 2012. Muscles, exercise and obesity: skeletal muscle as a secretory organ. Nat Rev Endocrinol., 8, 457-65. doi: 10.1038/nrendo.2012.49.
PEPPARD, P. E., YOUNG, T., PALTA, M. & SKATRUD, J. 2000. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med., 342, 1378-84. doi: 10.1056/NEJM200005113421901.
PETROF, B. J., HENDRICKS, J. C. & PACK, A. I. 1996. Does upper airway muscle injury trigger a vicious cycle in obstructive sleep apnea? A hypothesis. Sleep., 19, 465-71.
PETROF, B. J., SHRAGER, J. B., STEDMAN, H. H., KELLY, A. M. & SWEENEY, H. L. 1993. Dystrophin protects the sarcolemma from stresses developed during muscle contraction. Proc Natl Acad Sci U S A., 90, 3710-4.
PETTE, D. & STARON, R. S. 1997. Mammalian skeletal muscle fiber type transitions. Int Rev Cytol, 170, 143-223.
PHAM, L. V. & SCHWARTZ, A. R. 2015. The pathogenesis of obstructive sleep apnea. J Thorac Dis., 7, 1358-72. doi: 10.3978/j.issn.2072-1439.2015.07.28.
PITTS, E. V., POTLURI, S., HESS, D. M. & BALICE-GORDON, R. J. 2006. Neurotrophin and Trk-mediated signaling in the neuromuscular system. Int Anesthesiol Clin., 44, 21-76.
PUNJABI, N. M. 2008. The epidemiology of adult obstructive sleep apnea. Proc Am Thorac Soc, 5, 136-43.
RAAP, U., FOKKENS, W., BRUDER, M., HOOGSTEDEN, H., KAPP, A. & BRAUNSTAHL, G. J. 2008. Modulation of neurotrophin and

46
neurotrophin receptor expression in nasal mucosa after nasal allergen provocation in allergic rhinitis. Allergy., 63, 468-75. doi: 10.1111/j.1398-9995.2008.01626.x. Epub 2008 Feb 11.
RAHIMOV, F. & KUNKEL, L. M. 2013. The cell biology of disease: cellular and molecular mechanisms underlying muscular dystrophy. J Cell Biol., 201, 499-510. doi: 10.1083/jcb.201212142.
RODRIGUES HP, B. D. 2005. Biology and treatment of sleep apnea, Thieme New Your, Stuttgart
RYAN, C. M. & BRADLEY, T. D. 2005. Pathogenesis of obstructive sleep apnea. J Appl Physiol (1985). 99, 2440-50. doi: 10.1152/japplphysiol.00772.2005.
SABOISKY, J. P., STASHUK, D. W., HAMILTON-WRIGHT, A., CARUSONA, A. L., CAMPANA, L. M., TRINDER, J., ECKERT, D. J., JORDAN, A. S., MCSHARRY, D. G., WHITE, D. P., NANDEDKAR, S., DAVID, W. S. & MALHOTRA, A. 2012. Neurogenic changes in the upper airway of patients with obstructive sleep apnea. Am J Respir Crit Care Med., 185, 322-9. doi: 10.1164/rccm.201106-1058OC. Epub 2011 Oct 20.
SAKUMA, K. & YAMAGUCHI, A. 2011. The recent understanding of the neurotrophin's role in skeletal muscle adaptation. J Biomed Biotechnol, 2011:201696., 10.1155/2011/201696. Epub 2011 Sep 25.
SAM, M., SHAH, S., FRIDEN, J., MILNER, D. J., CAPETANAKI, Y. & LIEBER, R. L. 2000. Desmin knockout muscles generate lower stress and are less vulnerable to injury compared with wild-type muscles. Am J Physiol Cell Physiol., 279, C1116-22.
SARIOLA, H. 2001. The neurotrophic factors in non-neuronal tissues. Cell Mol Life Sci., 58, 1061-6. doi: 10.1007/PL00000921.
SAUNAMAKI, T. & JEHKONEN, M. 2007. Depression and anxiety in obstructive sleep apnea syndrome: a review. Acta Neurol Scand., 116, 277-88. doi: 10.1111/j.1600-0404.2007.00901.x. Epub 2007 Sep 14.
SCHIAFFINO, S., GORZA, L., DONES, I., CORNELIO, F. & SARTORE, S. 1986. Fetal myosin immunoreactivity in human dystrophic muscle. Muscle Nerve., 9, 51-8. doi: 10.1002/mus.880090108.
SCOTT, W., STEVENS, J. & BINDER-MACLEOD, S. A. 2001. Human skeletal muscle fiber type classifications. Phys Ther., 81, 1810-6.
SERIES, F., COTE, C., SIMONEAU, J. A., GELINAS, Y., ST PIERRE, S., LECLERC, J., FERLAND, R. & MARC, I. 1995. Physiologic, metabolic, and muscle fiber type characteristics of musculus uvulae in sleep apnea hypopnea syndrome and in snorers. J Clin Invest., 95, 20-5. doi: 10.1172/JCI117640.
SERIES, F., SIMONEAU, J. A. & ST PIERRE, S. 2000. Muscle fiber area distribution of musculus uvulae in obstructive sleep apnea and non-apneic snorers. Int J Obes Relat Metab Disord., 24, 410-5.
SERIES, F., WANG, W. & SIMILOWSKI, T. 2009. Corticomotor control of the genioglossus in awake OSAS patients: a transcranial magnetic stimulation study. Respir Res., 10:74., 10.1186/1465-9921-10-74.
SHAH, S. B., DAVIS, J., WEISLEDER, N., KOSTAVASSILI, I., MCCULLOCH, A. D., RALSTON, E., CAPETANAKI, Y. & LIEBER, R. L. 2004. Structural and functional roles of desmin in mouse skeletal muscle during passive deformation. Biophys J, 86, 2993-3008.

47
SHEPARD, J. W., JR. & THAWLEY, S. E. 1989. Evaluation of the upper airway by computerized tomography in patients undergoing uvulopalatopharyngoplasty for obstructive sleep apnea. Am Rev Respir Dis., 140, 711-6. doi: 10.1164/ajrccm/140.3.711.
SMALL, J. V., FURST, D. O. & THORNELL, L. E. 1992. The cytoskeletal lattice of muscle cells. Eur J Biochem., 208, 559-72.
SOFRONIEW, M. V., HOWE, C. L. & MOBLEY, W. C. 2001. Nerve growth factor signaling, neuroprotection, and neural repair. Annu Rev Neurosci, 24:1217-81., 10.1146/annurev.neuro.24.1.1217.
SRIVASTAVA, D. & YU, S. 2006. Stretching to meet needs: integrin-linked kinase and the cardiac pump. Genes Dev, 20, 2327-31.
STÅL, P., ERIKSSON, P. O., SCHIAFFINO, S., BUTLER-BROWNE, G. S. & THORNELL, L. E. 1994. Differences in myosin composition between human oro-facial, masticatory and limb muscles: enzyme-, immunohisto- and biochemical studies. J Muscle Res Cell Motil., 15, 517-34.
STÅL, P. S. & JOHANSSON, B. 2012. Abnormal mitochondria organization and oxidative activity in the palate muscles of long-term snorers with obstructive sleep apnea. Respiration, 83, 407-17. doi: 10.1159/000336040. Epub 2012 Mar 1.
STÅL, P. S. & LINDMAN, R. 2000. Characterisation of human soft palate muscles with respect to fibre types, myosins and capillary supply. J Anat., 197, 275-90.
STÅL, P. S., LINDMAN, R. & JOHANSSON, B. 2009. Capillary supply of the soft palate muscles is reduced in long-term habitual snorers. Respiration, 77, 303-10. doi: 10.1159/000197975. Epub 2009 Jan 29.
STEELE, C. M. & MILLER, A. J. 2010. Sensory input pathways and mechanisms in swallowing: a review. Dysphagia, 25, 323-33.
STROMER, M. H. 1998. The cytoskeleton in skeletal, cardiac and smooth muscle cells. Histol Histopathol., 13, 283-91.
SUNNERGREN, O., BROSTROM, A. & SVANBORG, E. 2011. Soft palate sensory neuropathy in the pathogenesis of obstructive sleep apnea. Laryngoscope., 121, 451-6. doi: 10.1002/lary.21371.
SVANBORG, E. 2001. Upper airway nerve lesions in obstructive sleep apnea. Am J Respir Crit Care Med., 164, 187-9. doi: 10.1164/ajrccm.164.2.2105010c.
SVANBORG, E. & LARSSON, H. 1993. Natural evolution of obstructive sleep apnea syndrome. Sleep., 16, S124-5.
THORNELL, L. E., ERIKSSON, A., ERDSTOM, L. 1983. Intermediate filament in human myopathies. Cell and Muscle Motility. R.B. Dowben and J.W. Shay, eds. Plenum Press, New York.
TROXEL, W. M., BUYSSE, D. J., MATTHEWS, K. A., KIP, K. E., STROLLO, P. J., HALL, M., DRUMHELLER, O. & REIS, S. E. 2010. Sleep symptoms predict the development of the metabolic syndrome. Sleep., 33, 1633-40.
TRUDO, F. J., GEFTER, W. B., WELCH, K. C., GUPTA, K. B., MAISLIN, G. & SCHWAB, R. J. 1998. State-related changes in upper airway caliber and surrounding soft-tissue structures in normal subjects. Am J Respir Crit Care Med., 158, 1259-70. doi: 10.1164/ajrccm.158.4.9712063.

48
VALHAM, F., MOOE, T., RABBEN, T., STENLUND, H., WIKLUND, U. & FRANKLIN, K. A. 2008. Increased risk of stroke in patients with coronary artery disease and sleep apnea: a 10-year follow-up. Circulation., 118, 955-60. doi: 10.1161/CIRCULATIONAHA.108.783290. Epub 2008 Aug 12.
WHYTE, K. F., ALLEN, M. B., JEFFREY, A. A., GOULD, G. A. & DOUGLAS, N. J. 1989. Clinical features of the sleep apnoea/hypopnoea syndrome. Q J Med., 72, 659-66.
WINTER, L., WITTIG, I., PEEVA, V., EGGERS, B., HEIDLER, J., CHEVESSIER, F., KLEY, R. A., BARKOVITS, K., STRECKER, V., BERWANGER, C., HERRMANN, H., MARCUS, K., KORNBLUM, C., KUNZ, W. S., SCHRODER, R. & CLEMEN, C. S. 2016. Mutant desmin substantially perturbs mitochondrial morphology, function and maintenance in skeletal muscle tissue. Acta Neuropathol, 132, 453-73.
WOODSON, B. T., GARANCIS, J. C. & TOOHILL, R. J. 1991. Histopathologic changes in snoring and obstructive sleep apnea syndrome. Laryngoscope., 101, 1318-22.
YOUNG, T., PALTA, M., DEMPSEY, J., SKATRUD, J., WEBER, S. & BADR, S. 1993. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med., 328, 1230-5. doi: 10.1056/NEJM199304293281704.
YOUNG, T., SKATRUD, J. & PEPPARD, P. E. 2004. Risk factors for obstructive sleep apnea in adults. JAMA., 291, 2013-6. doi: 10.1001/jama.291.16.2013.
ZHANG, J. Y., LUO, X. G., XIAN, C. J., LIU, Z. H. & ZHOU, X. F. 2000. Endogenous BDNF is required for myelination and regeneration of injured sciatic nerve in rodents. Eur J Neurosci., 12, 4171-80.

ISBN 978-91-7601-844-6ISSN 0346-6612
UMEÅ UNIVERSITY
Department of Integrative Medical Biology, Laboratory of Muscle Biology Department of Clinical Science, Otorhinolaryngology Umeå University, SE-901 87 Umeå www.umu.se
ISBN 978-917601-844-6 ISSN 0346-6612




![Research Article Nerve Dysfunction in Hallux Valgus is Correlated … · Coughlin [3]. While a neuromuscular misbalance is obviously responsible for the deformity in most instances,](https://static.documents.pub/doc/80x56/60229ba9dac6560dbd0a2bd5/research-article-nerve-dysfunction-in-hallux-valgus-is-correlated-coughlin-3.jpg)












