138
Neuropathic pain Dr. Rashiml Haque ( Rimon) MBBS, FCPS,MD Associate professor Department of neuro-medicine Uttara Adhunik Medical College
| Date post: | 13-Feb-2017 |
| Category: |
Health & Medicine |
| Upload: | rashimul-haque-rimon |
| View: | 37 times |
| Download: | 0 times |
Neuropathic pain
Dr. Rashiml Haque ( Rimon)MBBS, FCPS,MD
Associate professorDepartment of neuro-medicineUttara Adhunik Medical College
What is pain?
• “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
Type of pain
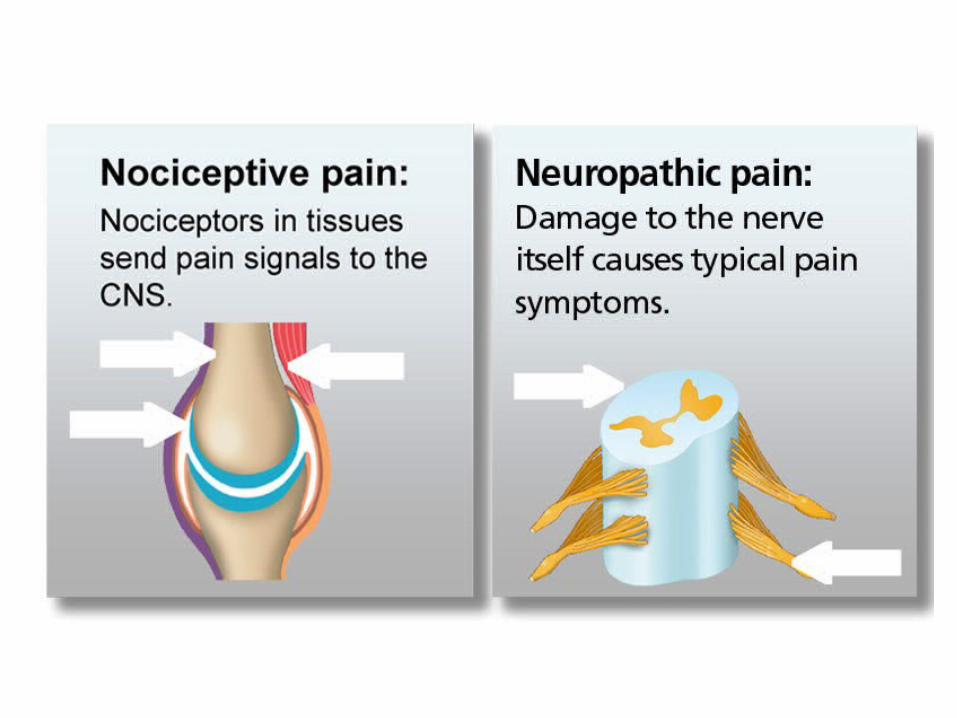
• Nociceptive pain
• Neuropathic pan


Nociceptive vs. Neuropathic Pain
Nociceptive
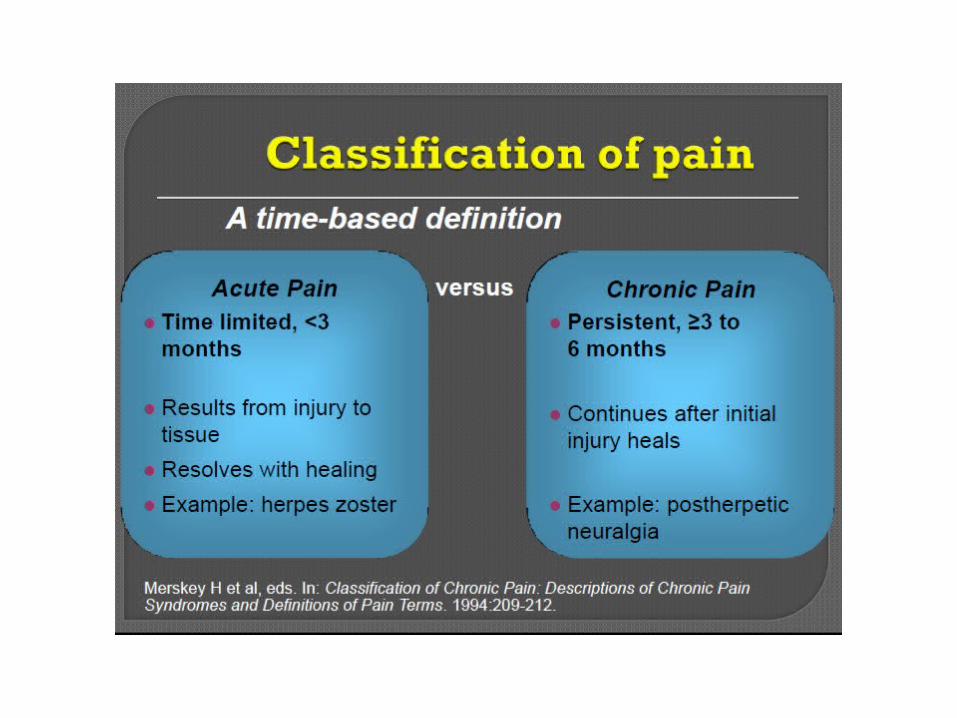
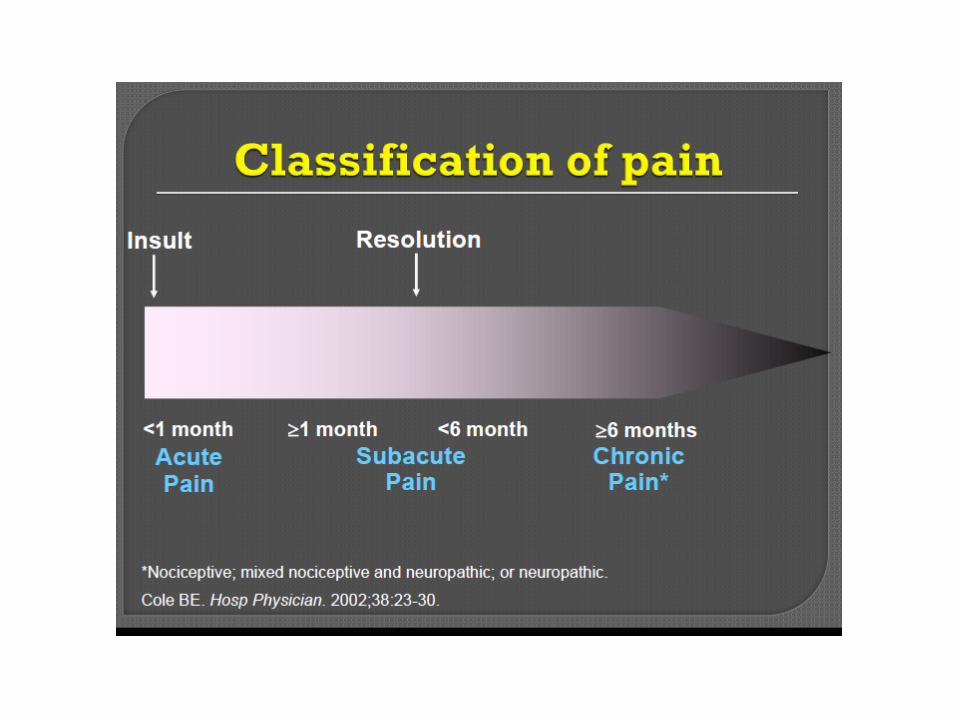
•Usually aching or throbbing and well-localized•Usually time-limited (resolves when damaged tissue heals), but can be chronic•Generally responds to conventional analgesics
Neuropathic
•Pain often described as tingling, shock-like, and burning – commonly associated with numbness•Almost always a chronic condition•Responds poorly to conventional analgesics
Dray A. Br J Anaesth 2008; 101(1):48-58; Felson DT. Arthritis Res Ther 2009; 11(1):203; International Association for the Study of Pain. IASP Taxonomy. Available at: http://www.iasp-pain.org/AM/Template.cfm?Section=Pain_Definitions. Accessed: July 15, 2013; McMahon SB, Koltzenburg M (eds). Wall and Melzack’s Textbook of Pain. 5th ed. Elsevier; London, UK: 2006; Woolf CJ. Pain 2011; 152(3 Suppl):S2-15.

Neuropathic pain
• Neuropathic pain arises from abnormal neural activity secondary to disease, injury, or dysfunction of the nervous system. It commonly persists without ongoing disease (eg, diabetic neuropathy, trigeminal neuralgia, or thalamic pain syndrome).


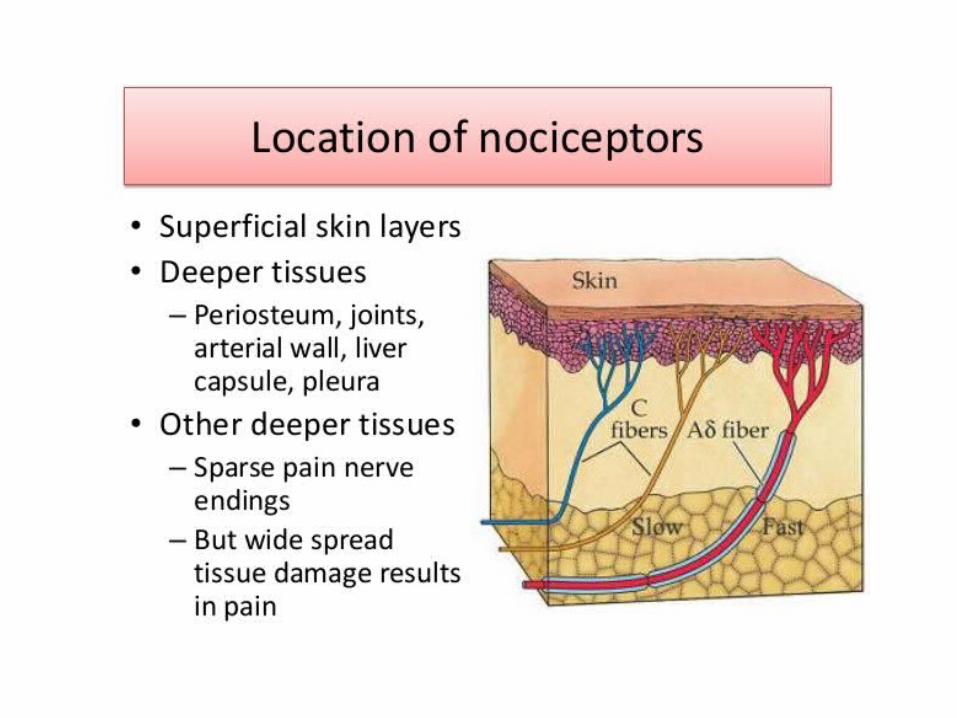
PATHOGENESIS OF PAIN —• Pain sensation begins in the periphery of the nervous system.• • Pain stimuli are sensed by specialized nociceptors that are the
nerve terminals of the primary afferent fibers.
• The pain signal is then transmitted to the dorsal horn of the spinal column and transmitted through the central nervous system (CNS) where it is processed and interpreted in the somatosensory cerebral cortex
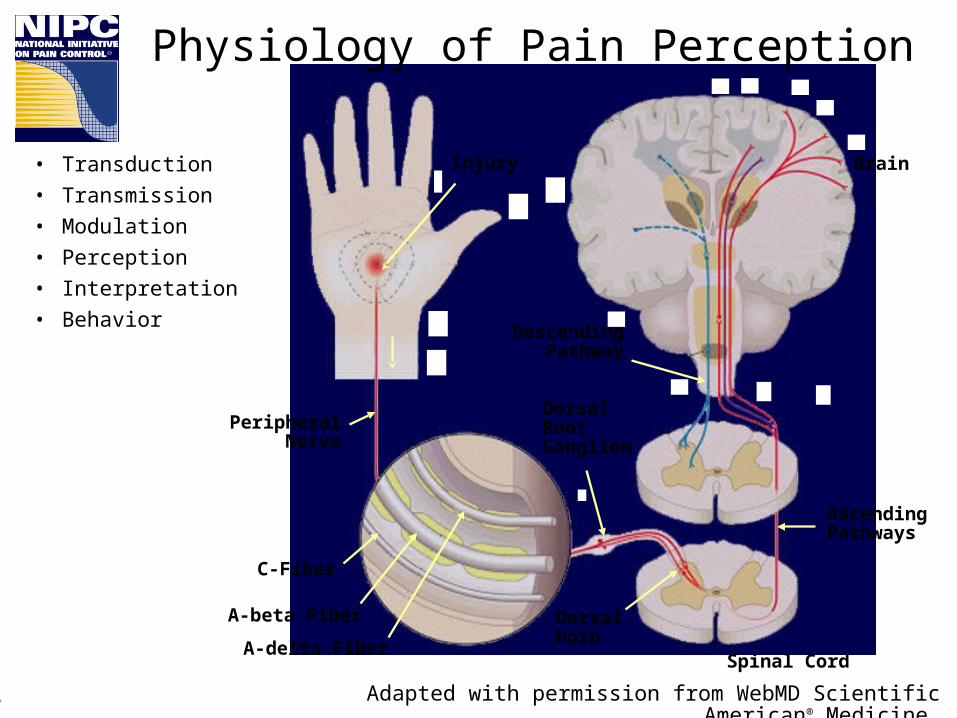
Physiology of Pain Perception
• Transduction• Transmission• Modulation• Perception• Interpretation• Behavior
Injury
Descending Pathway
PeripheralNerve
Dorsal RootGanglion
C-Fiber
A-beta Fiber
A-delta Fiber
AscendingPathways
Dorsal Horn
Brain
Spinal Cord
Adapted with permission from WebMD Scientific American® Medicine.18




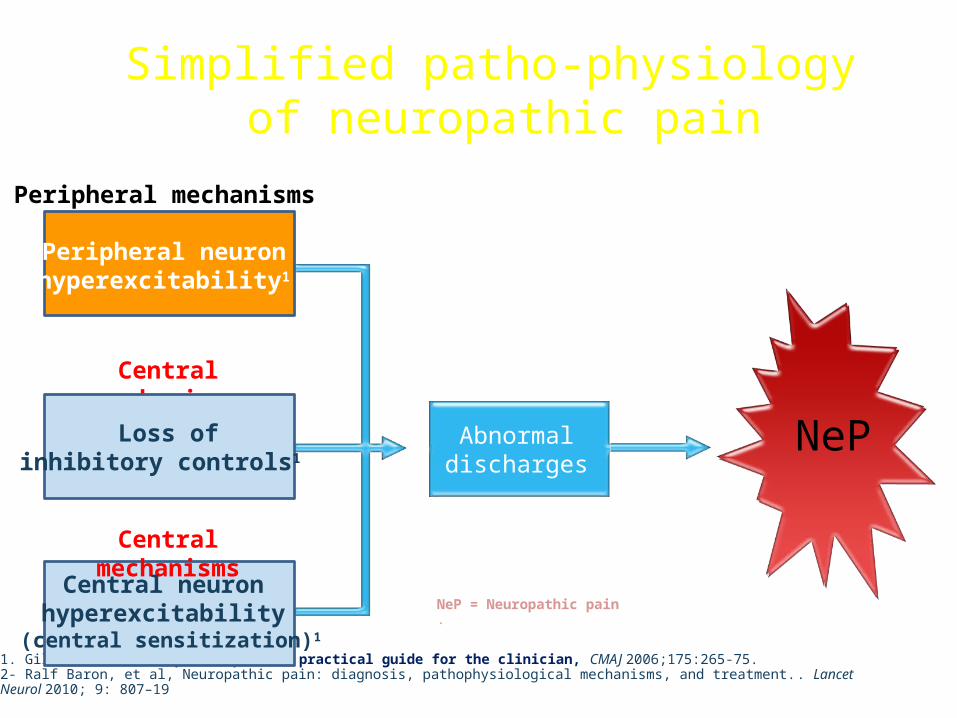
Simplified patho-physiology of neuropathic pain
NeP
Peripheral mechanisms
Abnormaldischarges
Central mechanisms
1. Gilron I et al. Neuropathic pain: a practical guide for the clinician, CMAJ 2006;175:265-75.2- Ralf Baron, et al, Neuropathic pain: diagnosis, pathophysiological mechanisms, and treatment.. Lancet Neurol 2010; 9: 807–19
Peripheral neuronhyperexcitability1
Loss ofinhibitory controls1,2
Central mechanisms
Central neuron hyperexcitability
(central sensitization)1
NeP = Neuropathic pain.

26
Your Patients may be suffering NeP if they have following characteristic
6/15/13

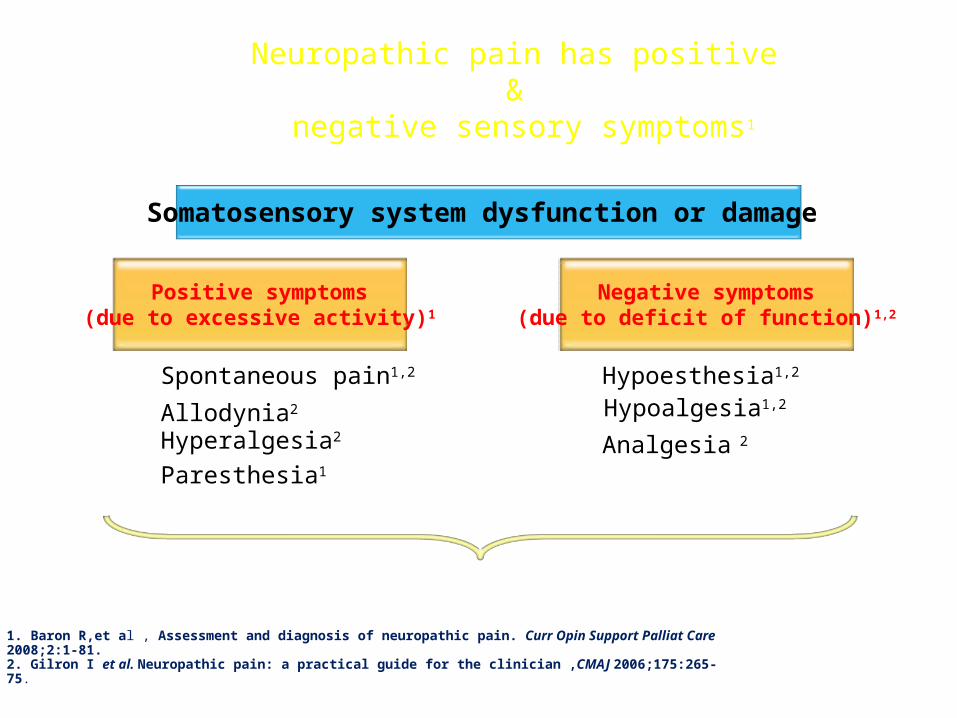
Neuropathic pain has positive &
negative sensory symptoms1
Somatosensory system dysfunction or damage
Positive symptoms(due to excessive activity)1
Paresthesia1
Spontaneous pain1,2
Hyperalgesia2Allodynia2
Negative symptoms(due to deficit of function)1,2
Hypoesthesia1,2
Hypoalgesia1,2
Analgesia 2
1. Baron R,et al , Assessment and diagnosis of neuropathic pain. Curr Opin Support Palliat Care 2008;2:1-81. 2. Gilron I et al. Neuropathic pain: a practical guide for the clinician ,CMAJ 2006;175:265-75.
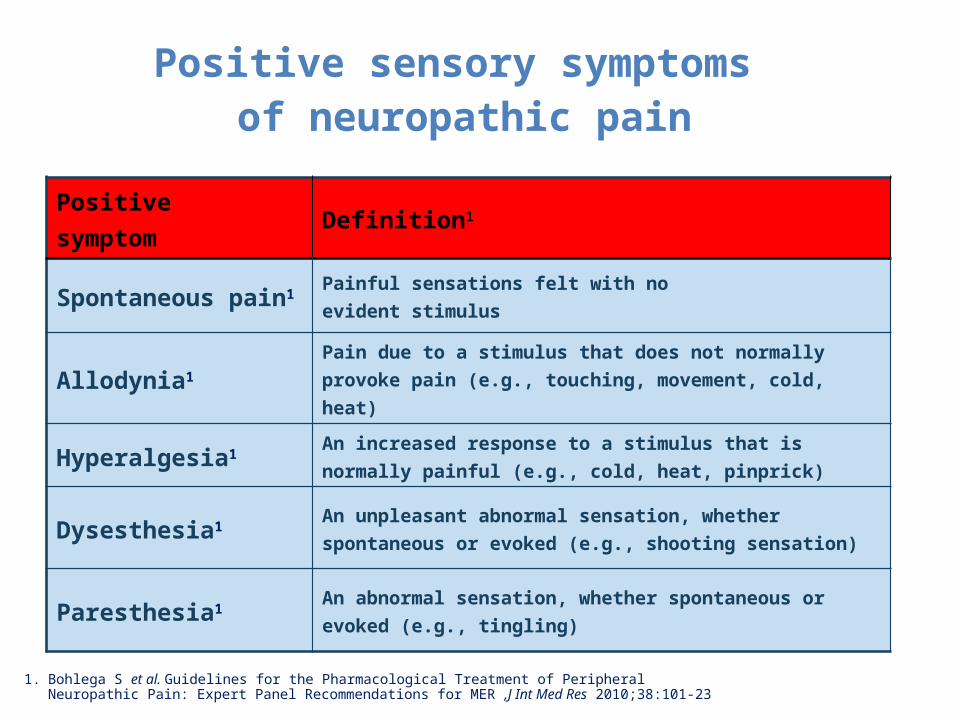
Positive symptom Definition1
Spontaneous pain1 Painful sensations felt with no evident stimulus
Allodynia1 Pain due to a stimulus that does not normally provoke pain (e.g., touching, movement, cold, heat)
Hyperalgesia1 An increased response to a stimulus that is normally painful (e.g., cold, heat, pinprick)
Dysesthesia1 An unpleasant abnormal sensation, whether spontaneous or evoked (e.g., shooting sensation)
Paresthesia1 An abnormal sensation, whether spontaneous or evoked (e.g., tingling)
Positive sensory symptoms of neuropathic pain
Adapted from:1. Bohlega S et al. Guidelines for the Pharmacological Treatment of Peripheral Neuropathic Pain: Expert Panel
Recommendations for MER ,J Int Med Res 2010;38:101-23

Negative symptom Definition
Hypoesthesia1 Diminished sensitivity to stimulation to non Painful stimulus.
Anesthesia1 Total loss of sensation (especially tactile sensitivity)
Hypoalgesia1 Diminished pain in response to a normally painful stimulus
Analgesia1 Absence of pain in response to stimulation that would normally be painful
Negative sensory symptoms of neuropathic pain
Adapted from:1. Bohlega S et al. Guidelines for the Pharmacological Treatment of Peripheral Neuropathic Pain: Expert Panel
Recommendations for MER ,J Int Med Res 2010;38:101-23
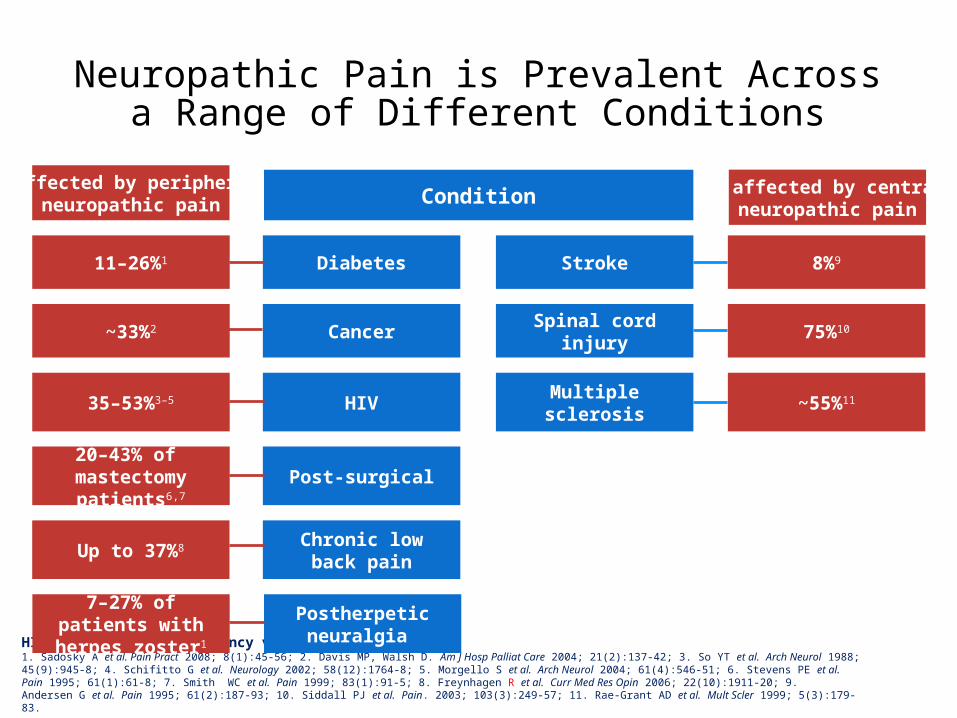
Neuropathic Pain is Prevalent Across a Range of Different Conditions
HIV = human immunodeficiency virus1. Sadosky A et al. Pain Pract 2008; 8(1):45-56; 2. Davis MP, Walsh D. Am J Hosp Palliat Care 2004; 21(2):137-42; 3. So YT et al. Arch Neurol 1988; 45(9):945-8; 4. Schifitto G et al. Neurology 2002; 58(12):1764-8; 5. Morgello S et al. Arch Neurol 2004; 61(4):546-51; 6. Stevens PE et al. Pain 1995; 61(1):61-8; 7. Smith WC et al. Pain 1999; 83(1):91-5; 8. Freynhagen R et al. Curr Med Res Opin 2006; 22(10):1911-20; 9. Andersen G et al. Pain 1995; 61(2):187-93; 10. Siddall PJ et al. Pain. 2003; 103(3):249-57; 11. Rae-Grant AD et al. Mult Scler 1999; 5(3):179-83.
11–26%1
~33%2
35–53%3–5
20–43% of mastectomy patients6,7
Up to 37%8
Diabetes
Cancer
HIV
Post-surgical
Postherpeticneuralgia
Chronic low back pain
8%9
75%10
~55%11
Stroke
Spinal cord injury
Multiple sclerosis
7–27% of patients with herpes zoster1
Condition% affected by peripheral
neuropathic pain% affected by central
neuropathic pain
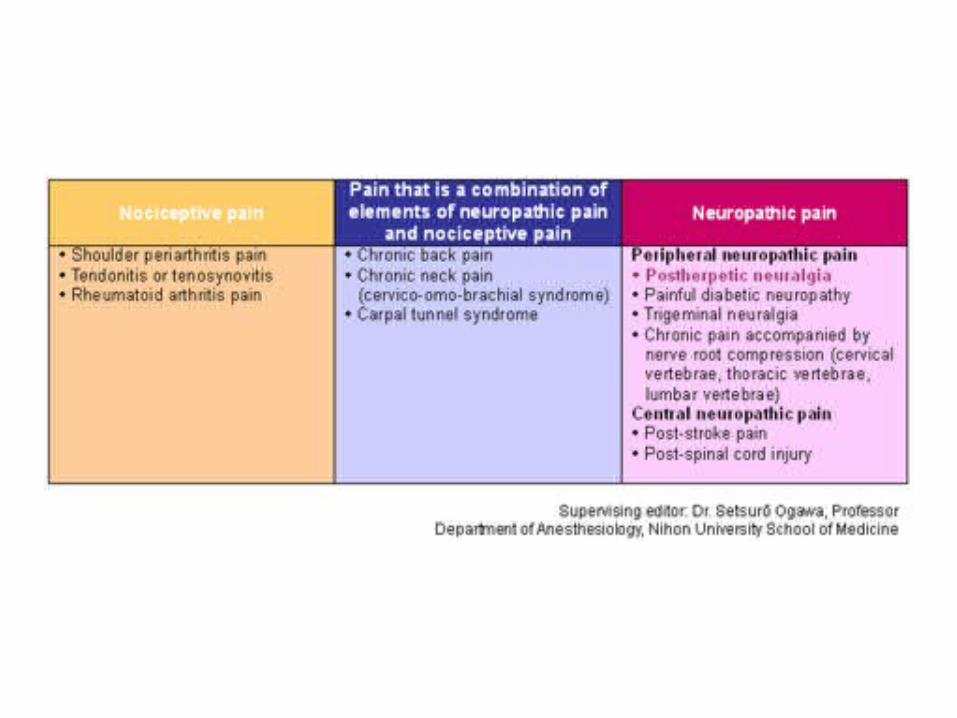
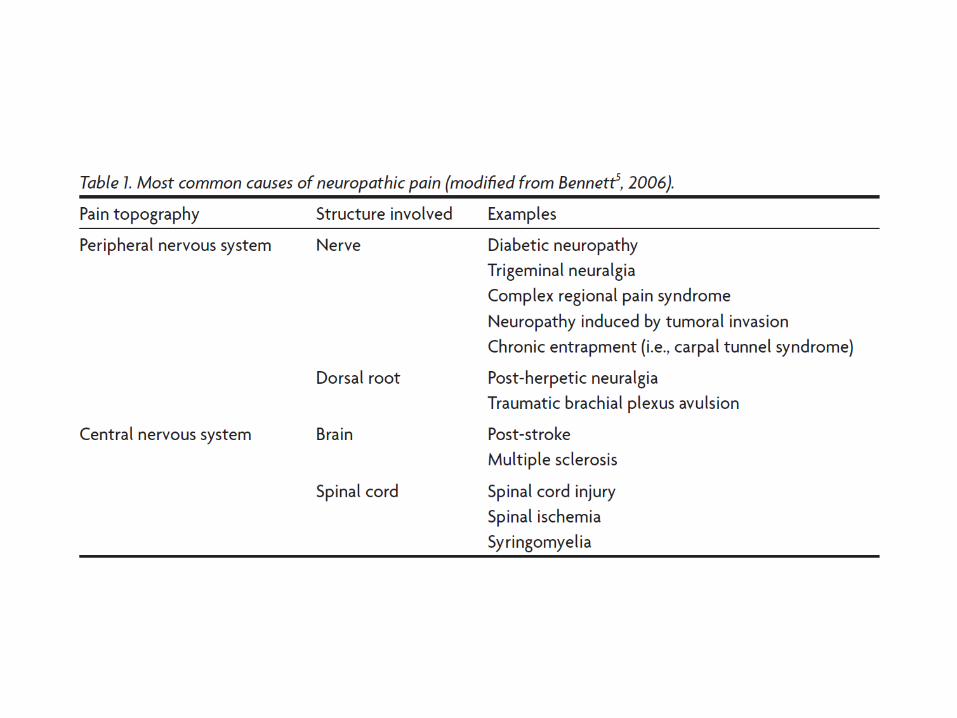
CAUSES OF NEUROPATHIC PAIN
Central Neuropathic Pain• Stroke,• Multiple sclerosis,• Spinal cord injury.

PERIPHERAL NEUROPATHIC PAIN
• Diabetic peripheral neuropathy,• Post herpetic neuralgia,• Trigeminal neuralgia,• Nutritional deficiency,• Vasculitis and immune-mediated• Chemotherapy or drug induced• Cancer-related• Toxin-induced





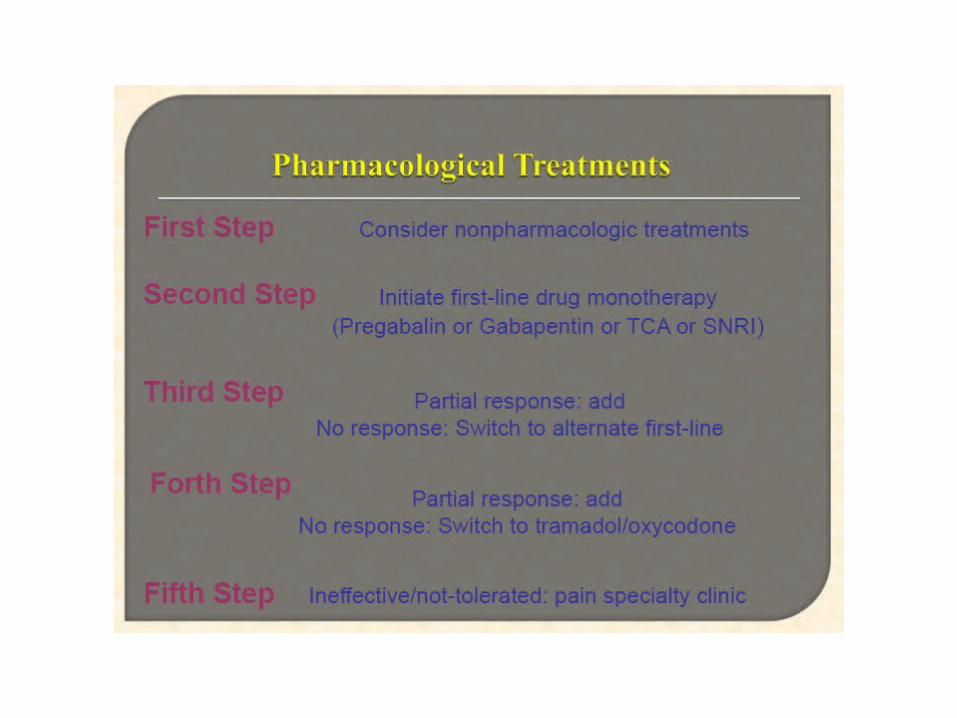
Treatment options for chronic pain
• pharmacologic, • physical medicine,• behavioral medicine, • neuromodulation, • interventional, and • surgical approaches
Optimal patient outcomes often result from multiple approaches utilized in concert, coordinated via a multidisciplinary team




Capsaicin • Capsaicin depletes
substance P and relieves neuropathic pain,
• 0.075% cream and 0.8% transdermal patch have been tested,
• Effective in treating post herpetic neuralgia,
• Commonest side effect is local skin irritation (burning, itching, rash, etc)

TOPICAL LIDOCAINE
• Lidocaine 5% transdermal patch is approved for PHN, and is effective for other painful neuropathies too.
• Gel formulations are also available,• No dose titration is necessary• Well tolerated, as so significant systemic
absorption occurs

Lidocaine • Lidocaine 5% transdermal
patch is approved for PHN, and is effective for other painful neuropathies too.
• Gel formulations are also available,
• No dose titration is necessary

TRICYCLIC ANTIDEPRESSANTS
• Amitriptyline, nortriptyline and imipramine
• Effective in diabetic neuropathy, PHN, traumatic nerve injury and post-stroke pain,
• Starting dose 10-25 mg at bed time, can be gradually increased to a maximum of 150 mg at bedtime.
• Helps in improving sleep and depression
• Inexpensive and once daily dosing are plus points
• Common side effects- dry mouth, urinary retention, sedation, constipation, decreased seizure threshold and cardiac toxicity.
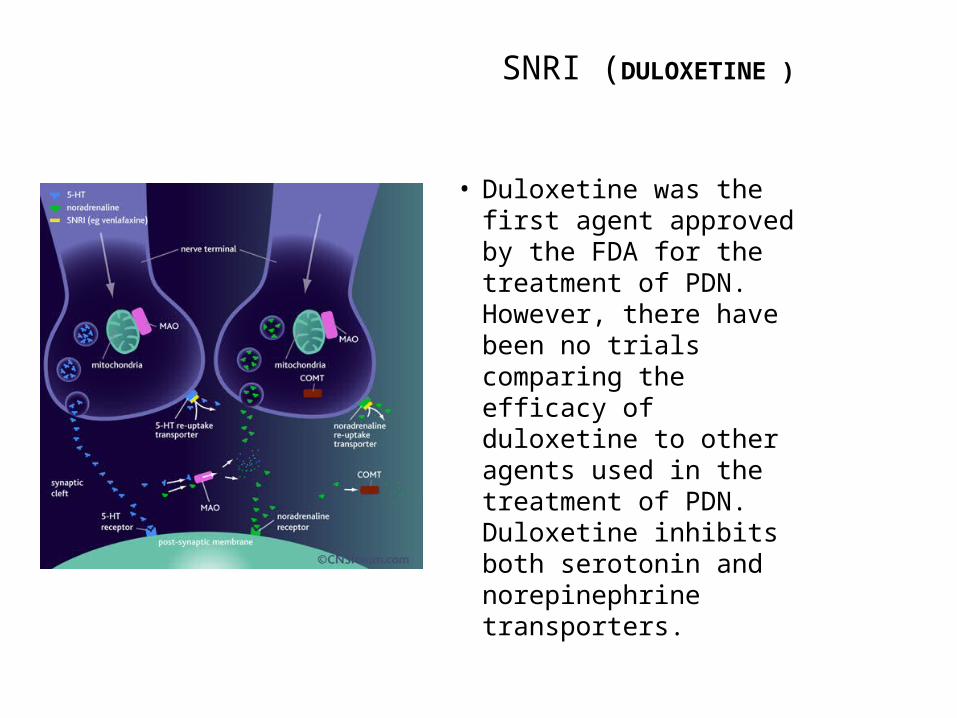
SNRI (DULOXETINE )
• Duloxetine was the first agent approved by the FDA for the treatment of PDN. However, there have been no trials comparing the efficacy of duloxetine to other agents used in the treatment of PDN. Duloxetine inhibits both serotonin and norepinephrine transporters.
SNRI-DULOXETINE
• DULOXETINE- approved for painful diabetic neuropathy
• It is also approved for generalized anxiety disorder, depression and fibromyalgia.
• Starting dose 20-30 mg , can be titrated to a maximum dose of 60 mg daily at night
• Nausea is a common side effect

Caution of duloxetine
• Duloxetine must be avoided in patients with any degree of hepatic insufficiency or substantial alcohol use.
• Patients on duloxetine therapy should have their blood pressure, heart rate, and liver enzymes monitored.
• Sexual adverse effect
SNRI-VENLAFAXINE
• VENLAFAXINE- is approved for generalized anxiety, panic disorder, depression and social anxiety
• Effective in treating diabetic and other painful neuropathies
• Starting dose is 37.5 mg at bed time, can be titrated to a maximum dose of 225 mg per day
• Immediate release formulation can be used BD, extended release formulation once daily

Carbamazepine/ Oxcarbazepine
• Carbamazepine was the first agent studied in the treatment of PDN.
• Although carbamazepine has good efficacy in the treatment of PDN, it also is associated with serious adverse events, including aplastic anemia, SJS
CARBAMAZEPINE/OXCARBAZEPINE
• Carbamazepine has been approved for use in trigeminal neuralgia (TN)
• Initial dose is 200 mg twice daily, can be given upto a maximum dose of 1200 mg per day in 3 divided doses
• Oxcarbazepine is also used for TN. • Side effects include drowsiness, dizziness, skin
rash and hyponatremia (more common with oxcarbazepine)
Gabapentine/ Pregabaline

GABAPENTIN
• Effective for most types of neuropathic pain,• Starting dose 100-300 mg HSOD to TID,• Can be gradually titrated to a maximum dose of
3600 mg per day• Common side effects- sedation, dizziness, edema,
weight gain; increased risk of falls and worsening of cognition (in elderly)
• Gabapentin-Nortriptyline combination is more effective than gabapentin or nortriptyline alone.
PREGABALIN
• Useful for most types of neuropathic pain,• Also reduces anxiety, improves sleep and
controls epilepsy,• Dose ranges from 75 mg to 600 mg per day,• Start low, and gradually escalate the dose,• Common side effects are drowsiness,
dizziness, weight gain, peripheral edema and worsening of depression.

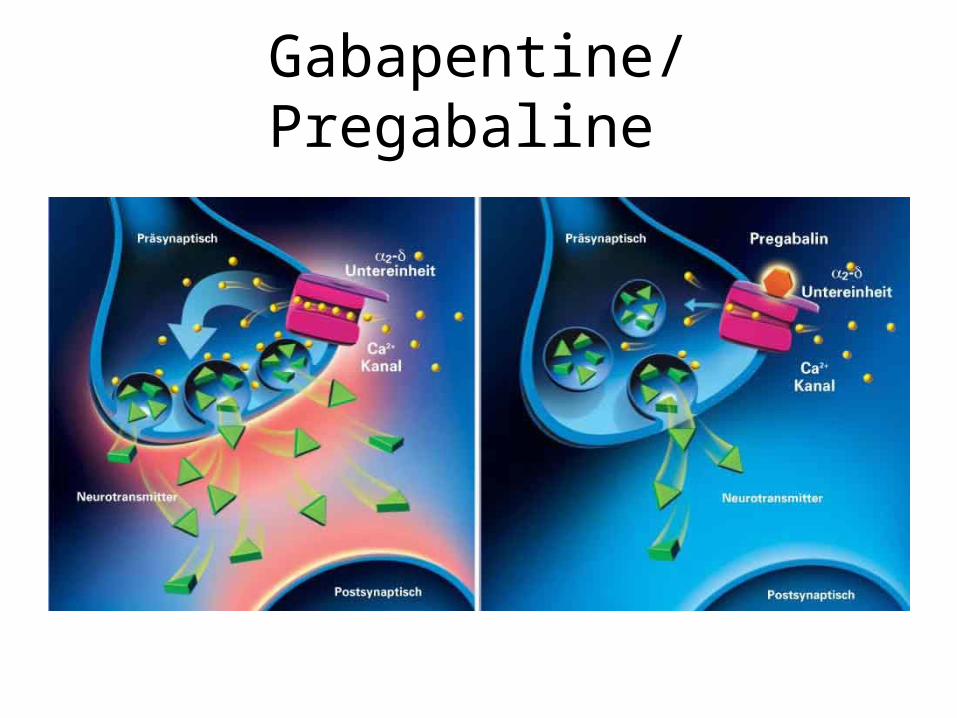
Mechanism of Action
Pregabalin
Binds with α2-δ site of Calcium channel in CNS
Reduces Ca+ influx and thus reduces the release of
calcium dependent neurotransmitters
Reduces pain
Ref.: www.lyrica.com
• PREGABALINE inhibit the release the excitatory neurotransmitter including glutamate, noradrelanine,serotonin, dopamine, substance P.

PREGABALIN
• Useful for most types of neuropathic pain,• Also reduces anxiety, improves sleep and
controls epilepsy,• Dose ranges from 75 mg to 600 mg per day,• Start low, and gradually escalate the dose,• Common side effects are drowsiness,
dizziness, weight gain, peripheral edema and worsening of depression.

73
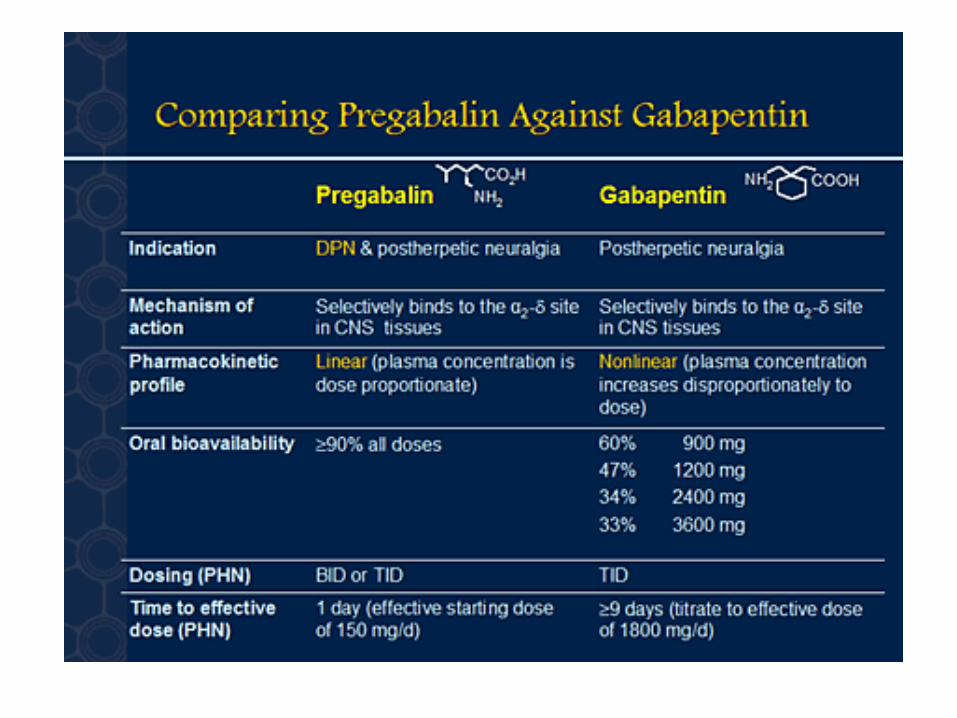
The Difference
Pregabalin is different molecule from gabapentin1
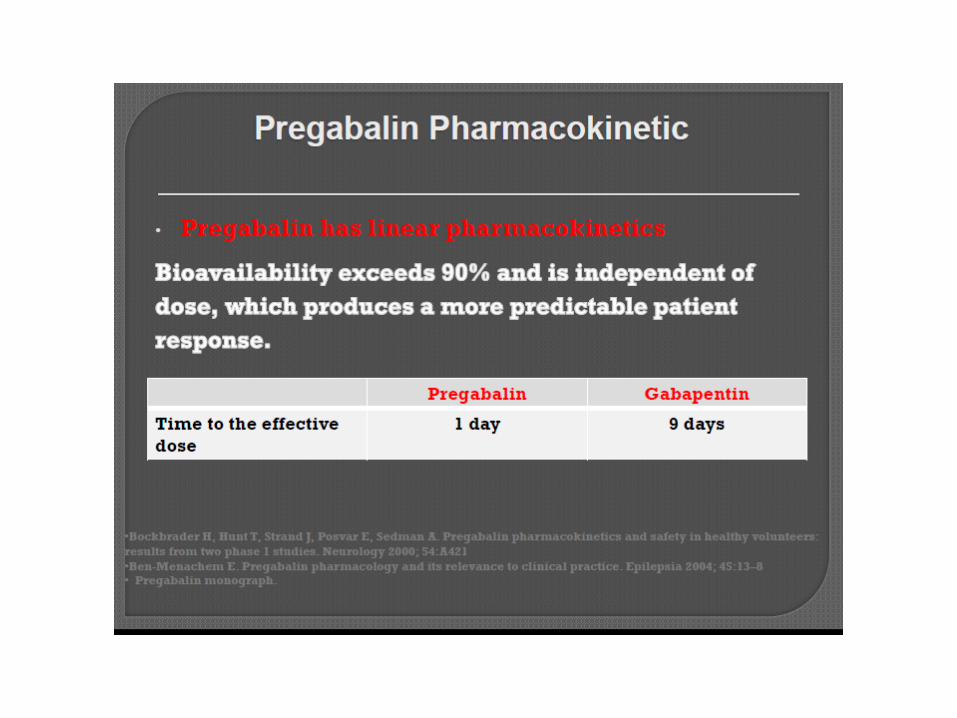
Pregabalin is rapidly absorbed 1 fast pain relief 4,5
Pregabalin plasma concentration is proportional to dose (high bioavailability)1more predictable pharmacokinetics 6ease to use in clinical practice6
6/15/13
References: 1. Bockbrader HN et al. A comparison of the pharmacokinetics and pharmacodynamics of pregabalin and gabapentin. Clin Pharmacokinet 2010; 49: 661–69. 2. Provelyn Product Information. 3. Nepatic Product Information. 4. Lesser H et al. Pregabalin relieves symptoms of painful diabetic neuropathy: a randomized controlled trial. Neurology 2004; 63: 2105. 5. Dworkin RH et al. Pregabalin in the treatment of postherpetic neuralgia: A randomized, placebo-controlled trial. Neurology 2003; 60: 1274–83. 6. Ben-Menachem E. Pregabalin pharmacology and its relevance to clinical practice. Epilepsia 2004; 45 Suppl 6: 13–18.
Pregabalin Gabapentin
Pharmacokinetics of Pregabalin
• Absorption: Rapid absorption in empty stomach Peak plasma conc. In 1 Hour.• Bioavailability: > 90%
• Distribution: Crosses the BBB and Placenta
• Pregnancy Category: C
• Metabolism: 98% unchanged
• Excretion: Unchanged in renal excretion.
• Drug Interaction: Dose not show any Interaction when administered with Ant diabetic, Antiepileptic, Benzodiazepine or Diuretics.
Ref.: www.lyrica.com
Warning /precaution of pregabaline
• CNS effect- dizziness, somnolence• Peripheral edema• Angioedema• Hypersensitivity• Rhabdomyolysis• Weight gain• Suicidal thought• Visual disturbance

NAME OF PRESENTATION | 76

The Right choice for Neuropathic Pain….

• CAP PRETOR -50mg, 75mg,150mg

TRAMADOL
• Tramadol is a weak mu opioid receptor agonist and weakly inhibits serotonin and noradrenalin reuptake,
• Tramadol is effective in DPN, PHN, radiculopathy and phantom limb pain,
• Starting dose 50 mg BD, can be gradually increased to 100 mg QID
• Common side effects include sedation, constipation, postural drop in BP and lowering of seizure threshold.

FDA-Approved Treatments for Neuropathic Pain
• Carbamazepine• –trigeminal neuralgia• •Duloxetine• –peripheral diabetic neuropathy• •Gabapentin• –postherpetic neuralgia• •Lidocaine Patch 5%• –postherpetic neuralgia• •Pregabalin• –peripheral diabetic neuropathy• –postherpetic neuralgia

THANK YOU
MEDICAL TREATMENT
• Pregabalin• Gabapentin• Dothiepin• Amitriptyline• Carbamazepine/oxcarbazepine• Duloxetine• Venlafaxine• Botox• Topical agents
DOSULEPIN (DOTHIEPIN)
• Prothiaden has been used for long and is effective in several conditions causing neuropathic pain,
• Safer than amitriptyline, lesser cardiac toxicity, and can be safely used in geriatric population,
• Effective in patients with comorbid depression• Initiate a dose of 25 mg at bed time; can be
increased to 75 mg per day at bedtime.
BOTULINUM TOXIN
• Intradermal Botox injection has been tested in DPN, PHN and TN
• Moderate success in small case series, further research is needed
• Reasonably safe.
CONCLUSIONS
• Several drugs are available to treat neuropathic pain,
• Choice of drug depends on age, comorbid conditions (insomnia, depression, anxiety, etc) and the cause of neuropathic pain,
• Start low, and gradually escalate the dose, until the desired effect is reached,
• Side effects are mild and uncommon, mainly sedation and dizziness.
Neuropathic Pain - TreatmentNeuropathic pain can be very difficult to treat with only some 40-60% of patients
achieving partial relief.
1.Antidepressants
2.Anticonvulsants
3.Opioids
4.Topical agents
5.Cannabinoids
6.Botulinum toxins
7.NMDA antagonism
8.Dietary Supplimentary
9.Others Ref.: www.wikipedia.org/wiki/Neuropathic_pain
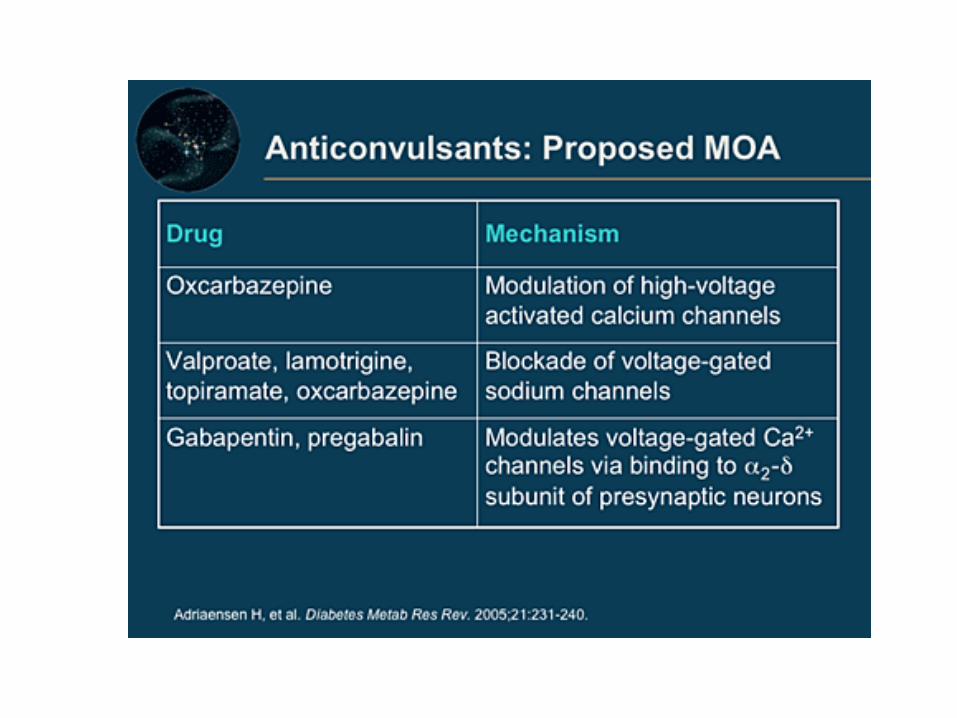
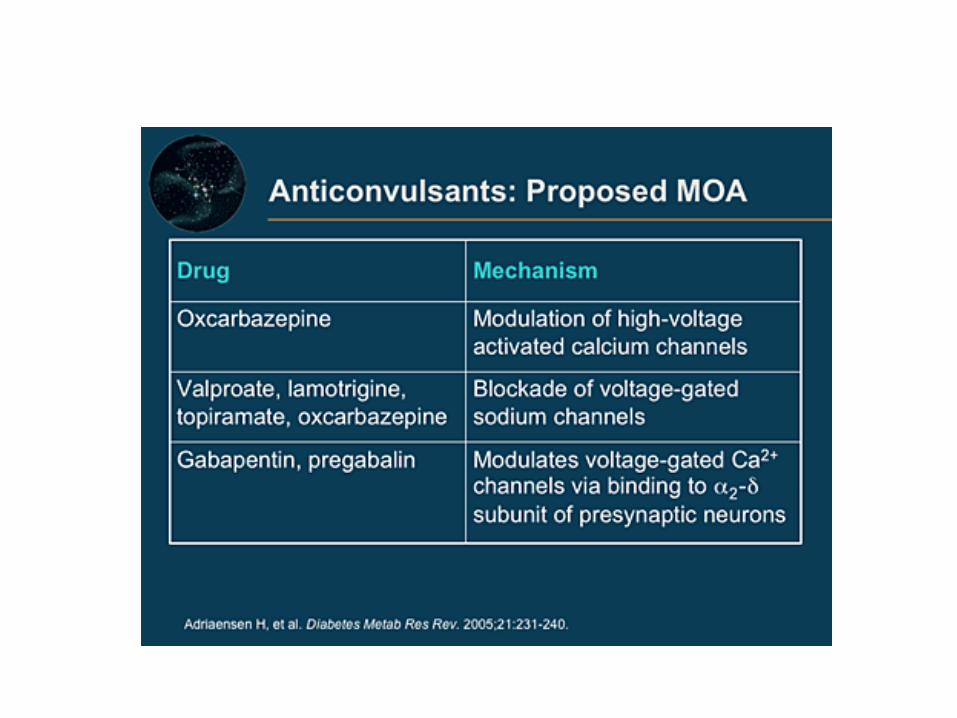
Mechanisms of Action: Analgesic Agents
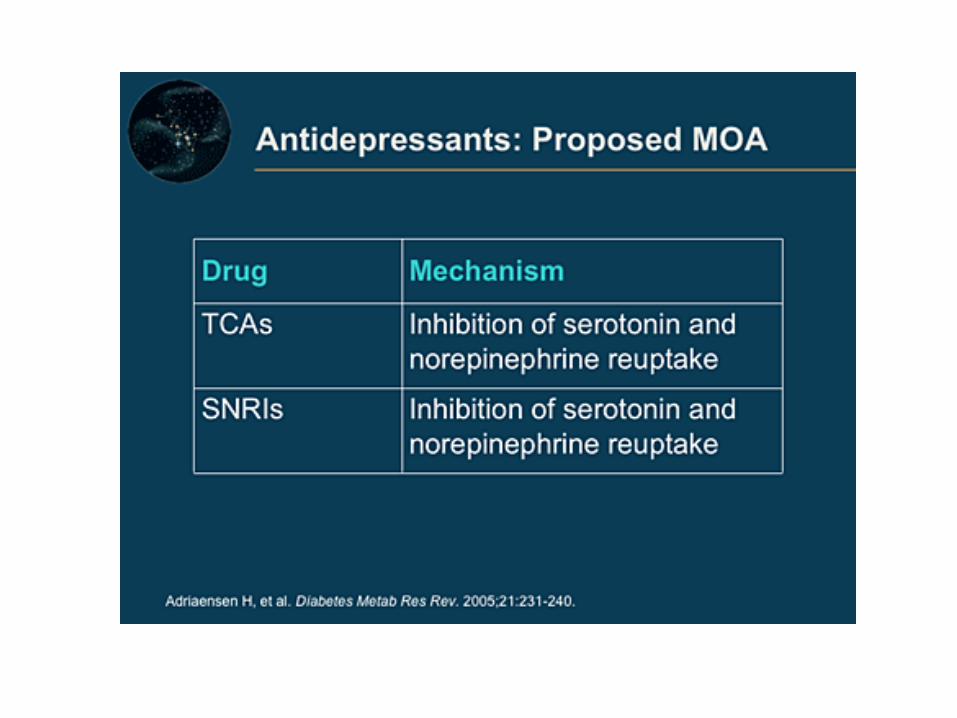
• Anticonvulsants• –sodium-channel blockade (oxcarbazepine [Trileptal])• –calcium-channel blockade (gabapentin)• •Antidepressants• –inhibit reuptake of norepinephrine and serotonin into presynaptic neurons
(duloxetine)• –sodium-channel blockade (tricyclics)• •Opioids• –block neurotransmitter-release by nociceptive fibers, thus decreasing
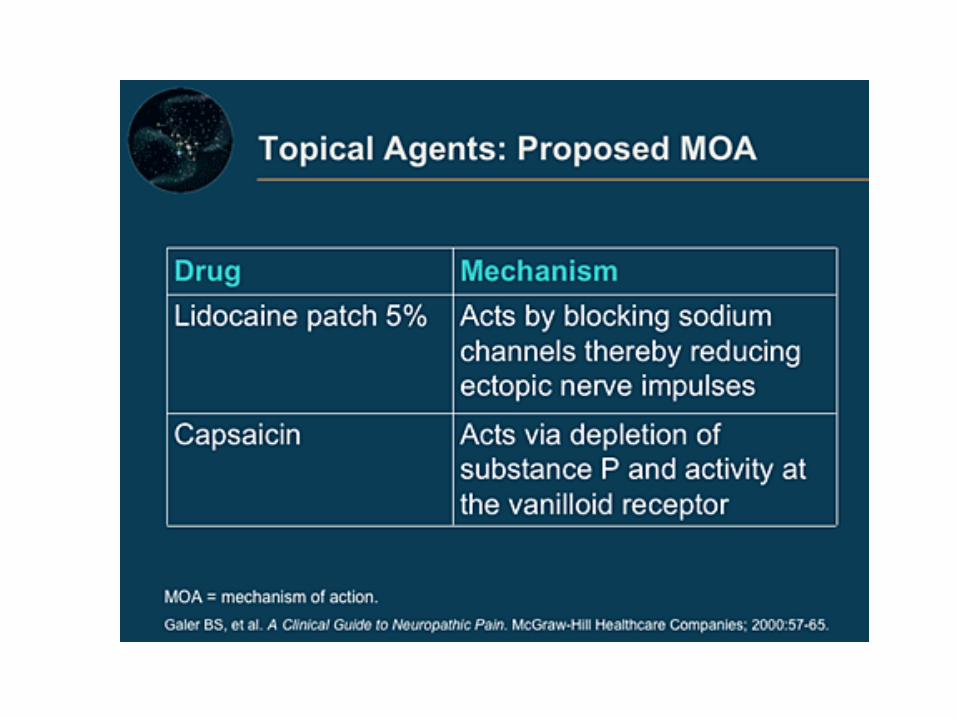
transmission of pain-producing signals (oxycodone)• •Topical Analgesics• –sodium-channel blockade (lidocaine patch 5%)• –vanilloid receptor (capsaicin)
• Currently available treatment modalities on average result in only about a 30 percent decrease in pain . But even a partial response of 30 percent can be clinically significant and improve the patient’s quality of life
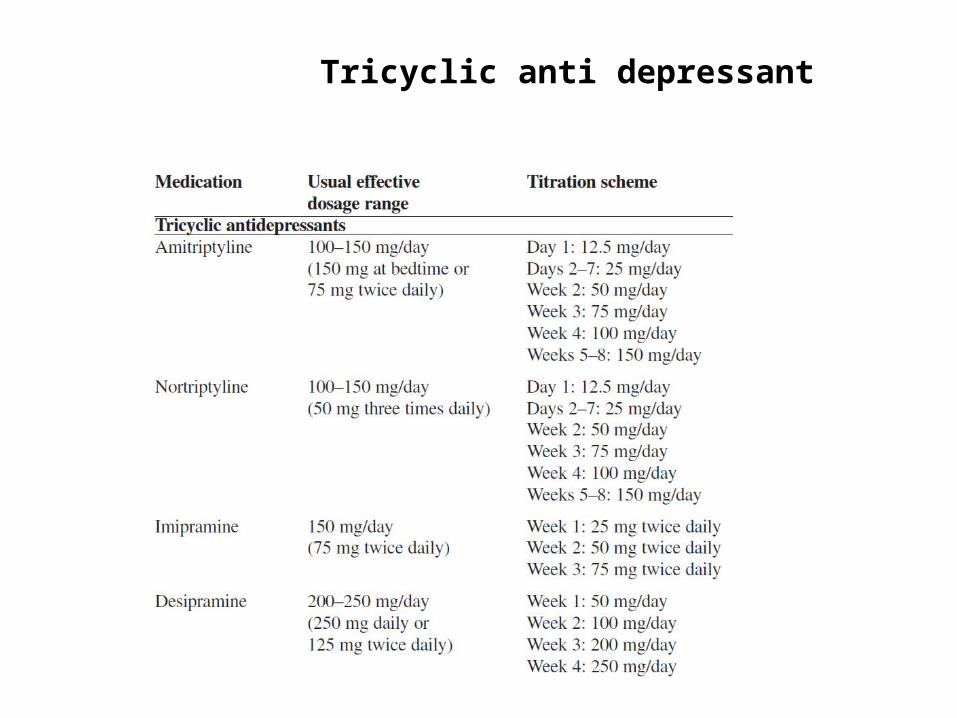
Tricyclic anti depressant
tricyclic anti depressant
• In summarizing the trials performed for treatment of PDN with TCAs, ~ 30% of patients obtain 50% pain relief.

Disadvantage of TCA
• Often contraindicated
• Risk of arrythmia
• Caution after > 65 yrs
• Sedation• Dry mouth• Weight gain

Recommendations about ANTI DEPRESSANT
• 1. Amitriptyline, venlafaxine, and duloxetine should be considered for the treatment of PDN (Level B). Data are insufficient to recommend one of these agents over the others.
• 2. Venlafaxine may be added to gabapentin for a better response (Level C).
• 3. There is insufficient evidence to support or refute the use of desipramine, imipramine, fluoxetine, or the combination of nortriptyline and fluphenazine in the treatment of PDN (Level U).

• Antiepileptic medications have been used for pain management since the 1960s. Three antiepileptic drugs (gabapentin, pregabalin, and carbamazepine) are among the five drugs approved by the US Food and Drug Administration (FDA) for the treatment of neuropathic pain
• Gabapentin and pregabalin — Gabapentin and pregabalin bind to the voltage-gated calcium channels at the alpha 2-delta subunit and inhibit neurotransmitter release. They have proven efficacy versus placebo in several neuropathic pain conditions .

• Gabapentin has primarily been studied and found effective for the treatment of postherpetic neuralgia and painful diabetic neuropathy .
• Treatment with gabapentin should be initiated at a low dose with gradual increases until pain relief, dose limiting adverse affects, or 3600 mg per day in three divided doses is achieved. An adequate trial of treatment with gabapentin can require two months or more.

Pregabaline
• Pregabalin is the second agent approved by the FDA for the indication of PDN.
• It acts peripherally at the GABA receptor to block the perception of pain.
• Pregabalin is relatively well tolerated and causes less sedation than gabapentin.

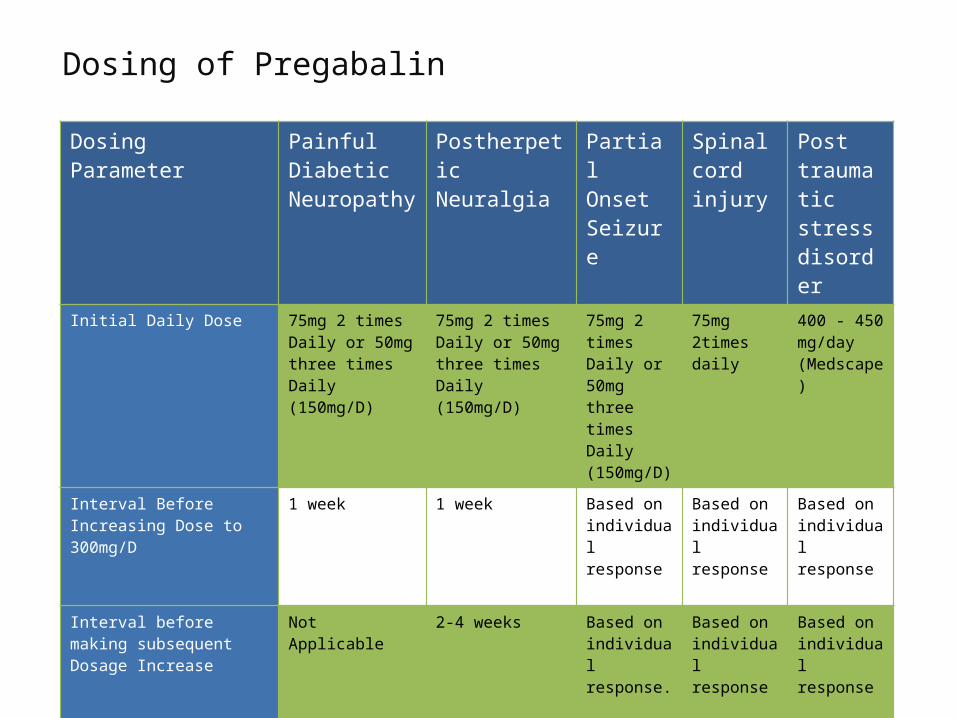
Dosing of Pregabalin
Dosing Parameter Painful Diabetic Neuropathy
Postherpetic Neuralgia
Partial Onset Seizure
Spinal cord injury
Post traumatic stress disorder
Initial Daily Dose 75mg 2 times Daily or 50mg three times Daily (150mg/D)
75mg 2 times Daily or 50mg three times Daily (150mg/D)
75mg 2 times Daily or 50mg three times Daily (150mg/D)
75mg 2times daily
400 - 450 mg/day (Medscape)
Interval Before Increasing Dose to 300mg/D
1 week 1 week Based on individual response
Based on individual response
Based on individual response
Interval before making subsequent Dosage Increase
Not Applicable 2-4 weeks Based on individual response.
Based on individual response
Based on individual response
Maximum Daily Dose 300mg/day 600mg/day 600mg/day 300 mg/day 600 mg/day(Medscape)
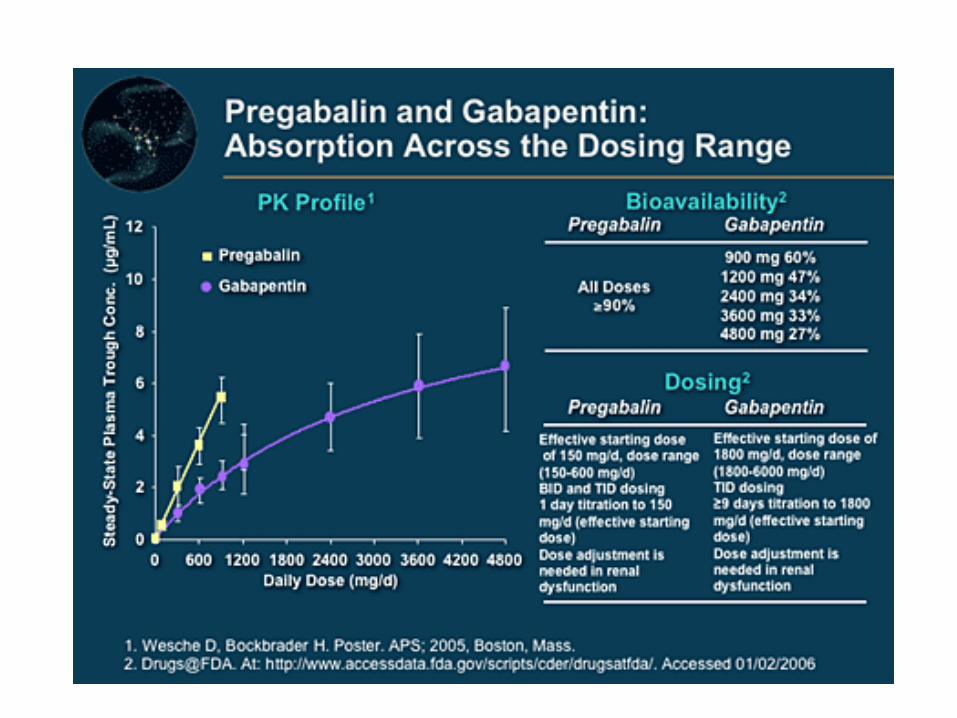
GABAPENTIN/PREGABALINE• Pregabalin was designed as a lipophilic gamma aminobutyric acid (GABA)
analog to facilitate diffusion across the blood-brain barrier.
• Pregabalin may provide analgesia more quickly than gabapentin, both because a lower initial dose (150 mg/day) was efficacious in some trials and because of a shorter time required to titrate to a full dose .
• Although gabapentin and pregabalin have few drug interactions, both can produce dose-dependent dizziness and sedation that can be reduced by starting with lower doses and titrating cautiously. Pregabalin has been reported to cause euphoria, and is classified as a Schedule V controlled substance in the United States.
Introduction of Pretor:
• Molecule: Pregabalin
• Class of drug: Anti-convulsant
• Therapeutic Class: Gamma amino Butyric acid.
• Presentation: 50 & 75 mg Capsule
Indication: • Management of neuropathic pain associated with diabetic
peripheral neuropathy.• Management of Postherpetic neuralgia.• Adjunctive therapy for adult patients with partial-onset of
Seizures.• Post traumatic stress disorder• Fibromyalgia • Neuropathic pain due to spinal cord injury
Ref.: www.lyrica.com
Mode of Action:
Binds to the alpha2-delta (A2D) receptors of an auxiliary subunit associated with voltage-gated calcium channels in central nervous system and thereby inhibits influx of calcium and release of glutamate, norepinephrine, substance P, and other neurotransmitters.
• >10%: Dizziness, drowsiness.
• 1 – 10%: Blurred vision, diplopia, increased appetite, euphoria confusion, changes
in libido (increase or decrease), irritability, ataxia, attention changes, abnormal
coordination, memory impairment, tremors, dysarthria.
• <1%: Neutropenia, first degree heart block, hypotension, hypertension,
pancreatitis, oliguria.
Side effects:
Ref.: www.lyrica.com

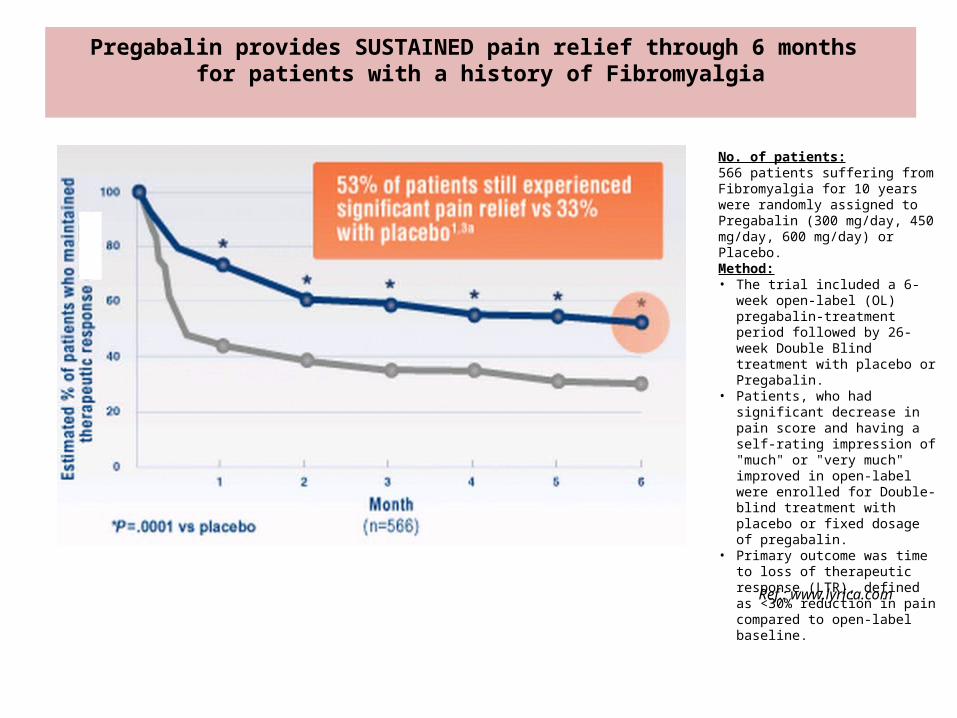
Pregabalin provides SUSTAINED pain relief through 6 months for patients with a history of Fibromyalgia
No. of patients:566 patients suffering from Fibromyalgia for 10 years were randomly assigned to Pregabalin (300 mg/day, 450 mg/day, 600 mg/day) or Placebo.Method:• The trial included a 6-week open-
label (OL) pregabalin-treatment period followed by 26-week Double Blind treatment with placebo or Pregabalin.
• Patients, who had significant decrease in pain score and having a self-rating impression of "much" or "very much" improved in open-label were enrolled for Double-blind treatment with placebo or fixed dosage of pregabalin.
• Primary outcome was time to loss of therapeutic response (LTR), defined as <30% reduction in pain compared to open-label baseline.
Ref.: www.lyrica.com



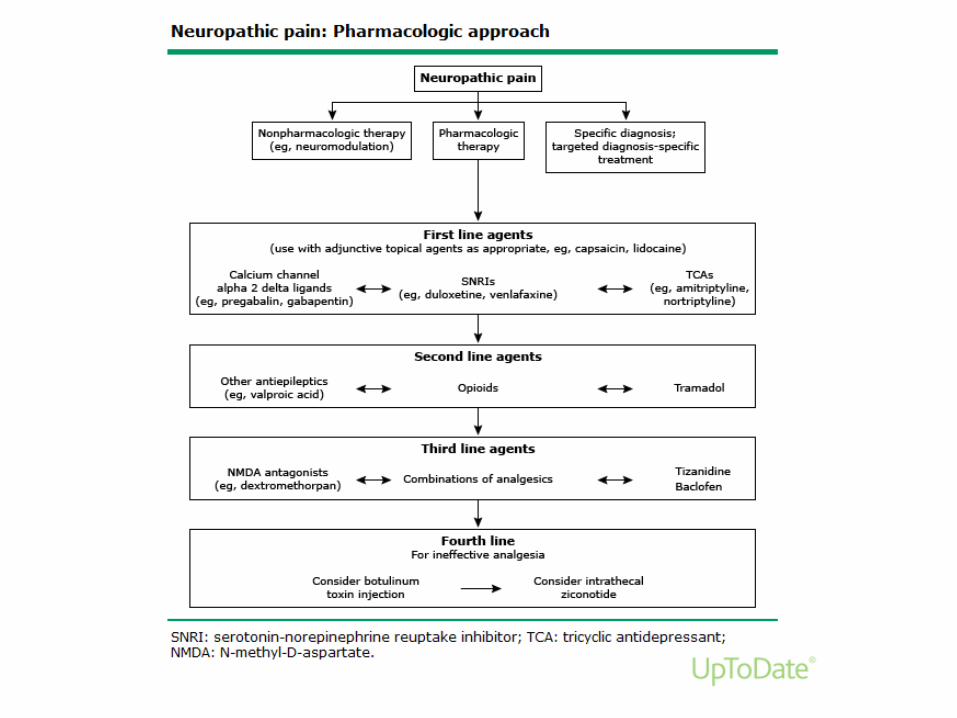
• When pharmacologic management of chronic neuropathic pain is required, the choice of an initial agent will be guided by individual patient factors including the pathophysiology of the pain syndrome, other symptoms and comorbidities, other medications being taken, organ reserves, pharmacokinetics/pharmacodynamics, and the likelihood of adverse effects.
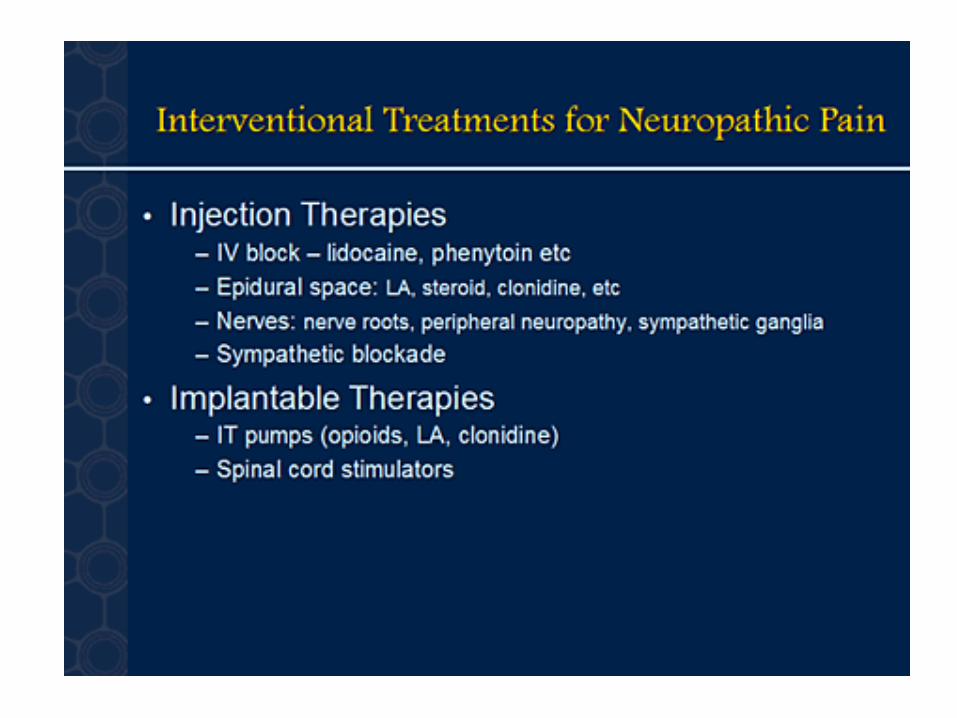
Interventional Treatments for Neuropathic Pain
• Neural blockade– sympathetic blocks for CRPS-I and II
(reflex sympathetic dystrophy and causalgia)• Neurolytic techniques
– alcohol or phenol neurolysis– pulse radio frequency
• Stimulatory techniques– spinal cord stimulation– peripheral nerve stimulation
• Medication pumps
CRPS = complex regional pain syndrome.
Thank you
• Pain is one of the most common and debilitating patient complaints, affecting individual patients, their friends and families, the work force, and society in general
• Over 100 million Americans suffer chronic pain and roughly 63 percent of pain sufferers seek help from their primary care clinicians.
• Pain accounts for 20 percent of outpatient visits and 12 percent of all prescriptions .
• Patients with symptoms of chronic pain are seen by clinicians in multiple clinical settings.
• Persistent pain often causes functional impairment and disability, psychological distress (anxiety, depression), and sleep deprivation .
• Almost 80 percent of chronic pain patients report that pain disrupts their activities of daily living, and two-thirds indicate that pain has negatively impacted personal relationships

• Nociceptive pain — Nociceptors are a highly-specialized subset of primary sensory neurons that respond only to pain stimuli.
• Nociceptive pain is the perception of nociceptive input, usually due to tissue damage (eg, postoperative pain).
Type of nociceptive pain
• Somatic pain arises from injury to body tissues. It is well localized but variable in description and experience.
• Visceral pain is pain arising from the viscera mediated by stretch receptors. It is poorly localized, deep, dull, and cramping (eg, pain associated with appendicitis, cholecystitis, or pleurisy).
Neuropathic pain is further subdivided as follows:
• ●Sympathetically mediated pain (SMP) is pain arising from a peripheral nerve lesion and associated with autonomic changes (eg, complex regional pain syndrome I and II, formerly known as reflex sympathetic dystrophy and causalgia)
• ●Peripheral neuropathic pain is due to damage to a peripheral nerve without autonomic change (eg, postherpetic neuralgia, neuroma formation).
• ●Central pain arises from abnormal central nervous system (CNS) activity (eg, phantom limb pain, pain from spinal cord injuries, and post-stroke pain).

Pain pathway• Multiple ascending pathways may be involved in relaying
nociceptive information to the
• The majority of the wide dynamic range and nociceptive specific neurons project contralaterally within the spinal cord and ascend within the anterolateral quadrant, forming the spinothalamic tract which synapses in the thalamus
• Neurons from the thalamus project to multiple brain areas in the primary and secondary somatosensory cortex, cingulate cortex, prefrontal cortex, insular cortex, amygdala, and the cerebellum
Neuropathic Pain - Mechanism Mechanism:
Peripheral:After a peripheral nerve lesion, aberrant regeneration may occur. Neurons become
unusually sensitive and develop spontaneous pathological activity, abnormal
excitability, and heightened sensitivity to chemical, thermal and mechanical stimuli.
This phenomenon is called "peripheral sensitization".
Ref.: www.wikipedia.org/wiki/Neuropathic_pain
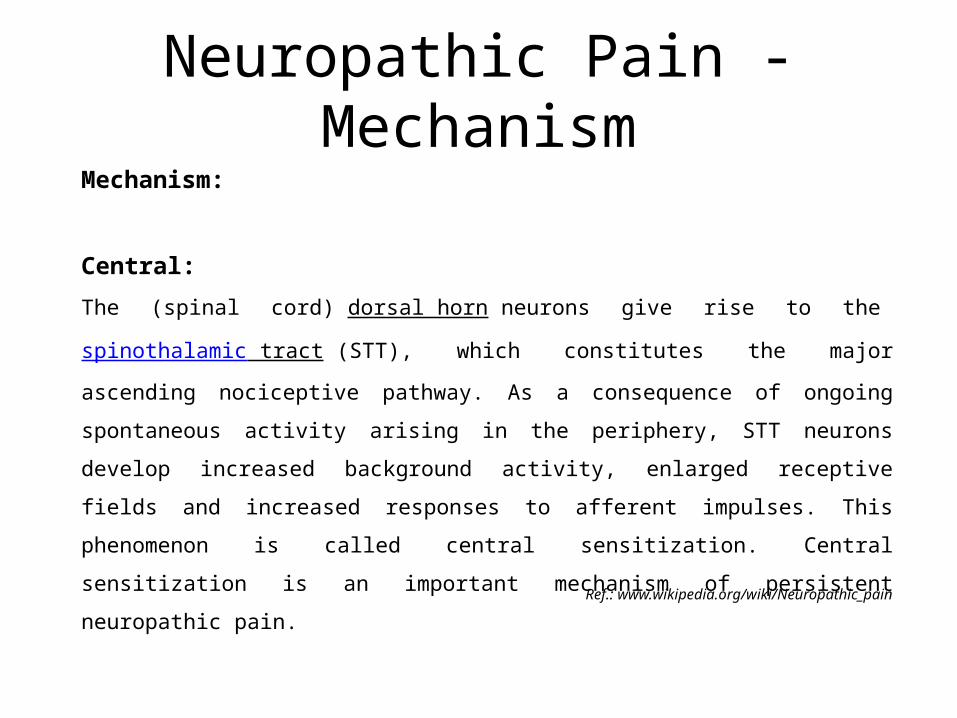
Neuropathic Pain - MechanismMechanism:
Central:The (spinal cord) dorsal horn neurons give rise to the spinothalamic tract (STT), which
constitutes the major ascending nociceptive pathway. As a consequence of ongoing
spontaneous activity arising in the periphery, STT neurons develop increased
background activity, enlarged receptive fields and increased responses to afferent
impulses. This phenomenon is called central sensitization. Central sensitization is an
important mechanism of persistent neuropathic pain.
Ref.: www.wikipedia.org/wiki/Neuropathic_pain

• Nociceptors — Nociceptors are a highly-specialized subset of primary sensory neurons that respond only to pain stimuli. They are categorized by the kind of stimulation they respond to and the nature of their response [28]. Most noxious stimuli activate a variety of nociceptor types in the affected area. Their signals sum to produce the nociceptive input, leading to the subjective sense of pain.
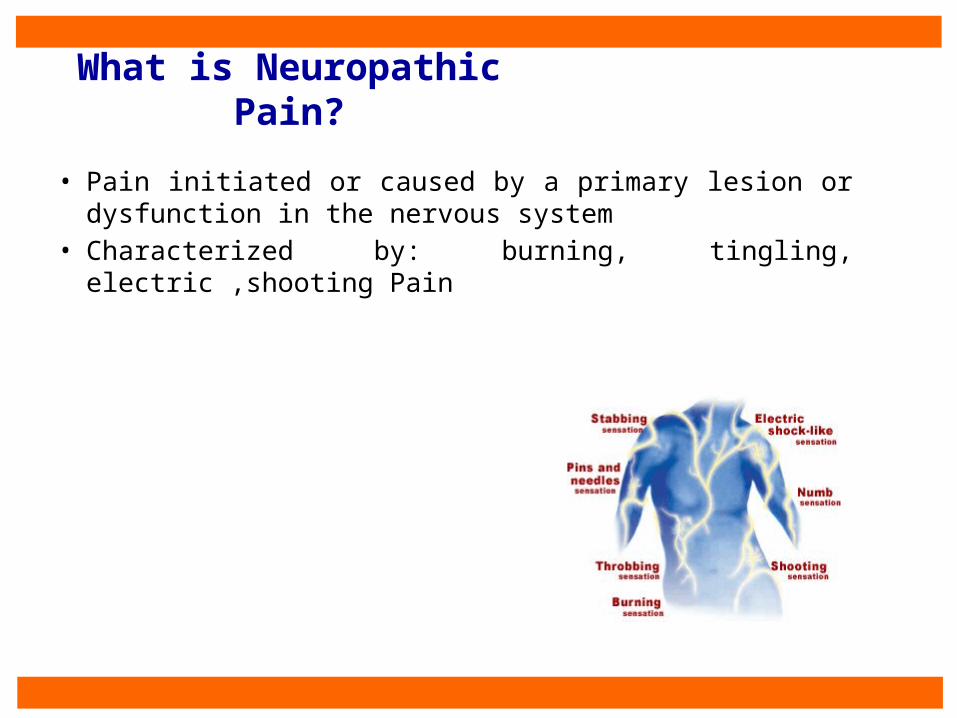
What is Neuropathic Pain?
• Pain initiated or caused by a primary lesion or dysfunction in the nervous system
• Characterized by: burning, tingling, electric ,shooting Pain
138
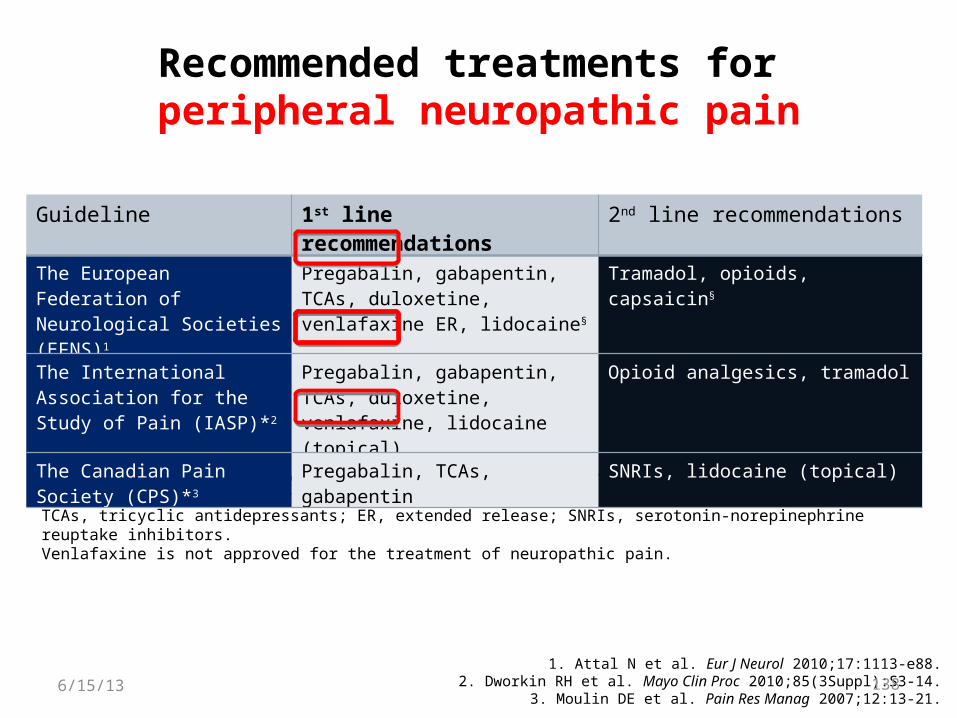
Recommended treatments for peripheral neuropathic pain
1. Attal N et al. Eur J Neurol 2010;17:1113-e88.2. Dworkin RH et al. Mayo Clin Proc 2010;85(3Suppl):S3-14.
3. Moulin DE et al. Pain Res Manag 2007;12:13-21.
*Guidelines did not distinguish between peripheral and central neuropathic pain.§For focal neuropathy, such as postherpetic neuralgia.TCAs, tricyclic antidepressants; ER, extended release; SNRIs, serotonin-norepinephrine reuptake inhibitors.Venlafaxine is not approved for the treatment of neuropathic pain.
Guideline 1st line recommendations 2nd line recommendations
The European Federation of Neurological Societies (EFNS)1
Pregabalin, gabapentin, TCAs, duloxetine, venlafaxine ER, lidocaine§
Tramadol, opioids, capsaicin§
The International Association for the Study of Pain (IASP)*2
Pregabalin, gabapentin, TCAs, duloxetine, venlafaxine, lidocaine
(topical)
Opioid analgesics, tramadol
The Canadian Pain Society (CPS)*3
Pregabalin, TCAs, gabapentin SNRIs, lidocaine (topical)
6/15/13
139
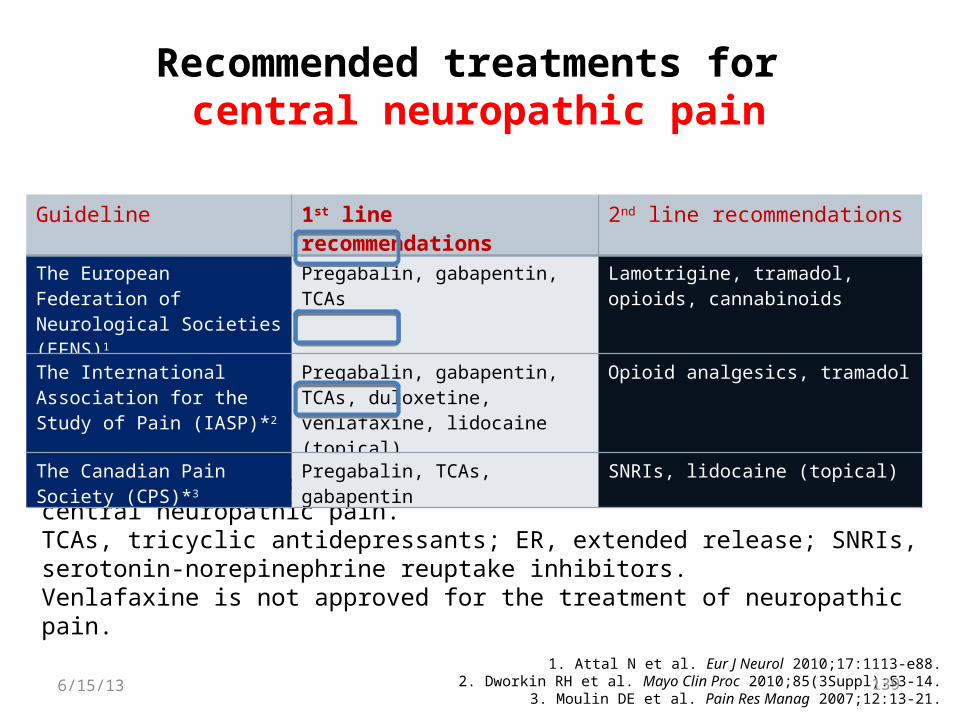
Recommended treatments for central neuropathic pain
1. Attal N et al. Eur J Neurol 2010;17:1113-e88.2. Dworkin RH et al. Mayo Clin Proc 2010;85(3Suppl):S3-14.
3. Moulin DE et al. Pain Res Manag 2007;12:13-21.
*Guidelines did not distinguish between peripheral and central neuropathic pain.TCAs, tricyclic antidepressants; ER, extended release; SNRIs, serotonin-norepinephrine reuptake inhibitors. Venlafaxine is not approved for the treatment of neuropathic pain.
Guideline 1st line recommendations 2nd line recommendations
The European Federation of Neurological Societies (EFNS)1
Pregabalin, gabapentin, TCAs Lamotrigine, tramadol, opioids, cannabinoids
The International Association for the Study of Pain (IASP)*2
Pregabalin, gabapentin, TCAs, duloxetine, venlafaxine, lidocaine
(topical)
Opioid analgesics, tramadol
The Canadian Pain Society (CPS)*3
Pregabalin, TCAs, gabapentin SNRIs, lidocaine (topical)
6/15/13

















