Neuropathy I POS-002-165 DECREASING VARIABILITY IN ASSESSMENT OF DIABETIC PERIPHERAL NEUROPATHY CA LAUDADI0, RD AITCHISON ICI Pharmaceuticals, Wilmington, DE, USA Assessment of the onset and progress of diabetic neuropathy presents difficulties in both clinical practice and epidemiological research. Measurements available for the longitudinal assessment of neuropathy are often noisy and unreliable. Reducing the variability inherent in the measurement of neuropathy will provide both a more meaningful estimate of the true state of a study population and will increase the statistical power to detect a treatment effect in a clinical trial. The noise inherent in these measurements can be substantially reduced by repeated assessments at critical time points. Thus a good study design should utilize multiple assessments. This abstact provides data to support these recommendations and gives examples of these approaches. In a trial of diabetic neuropathy triplicate assessments of thermal and vibratory thresholds were obtained during baseline and at critical time points in double blind therapy. Triplicate assessment decreased the analytical variance by 31% and 37% for thermal and vibratory thresholds, respectively. The power of the trial to detect a 20% treatment effect (n/group=200,alpha =.05) was increased from .6 to .8 for the thermal assessments and was maintained (>.95) for the vibratory data. The effect of repeated assessments can also be expressed as a reduction in the number of patients needed for a trial. That actual savings realized depends upon the ratio of the between-patient to the within-patient variability. For this study recruitment was reduced by 50% by triplicate assessment. In conclusion we recommend that repeated assessments be considered as a part of trial design whenever measurements are subject to repeat variability. POS-002-166 VESICOURETHRAL DYSFUNCTION OF DIABETIC PATIENTS. AN URODYNAMIC EVALUATION. K Kitamil), K Miyai 2) and T Takahashi 3) Department of Urology Yamato City Hospital I) , Yokohama City Kouwan Hospital 2) , and Hadano Red Cross Hospital 3) Yokohama, Japan In order to evaluate vesicourethral dysfunction of diabetic patients, urodynamic studies were performed on 163 diabetic patients and 20 control cases. In addition to the classical findings as impaired bladder sensation, decreased detrusor function and poor flow rate with residual urine, diabetic patients showed varieties of vesicourethral dysfunction such as hyperactive bladder, low compliance bladder and loss of detrusor-sphincter coordination. The main factors related with poor vesicourethral function were early onset, longer duration, poor control of the disease, cases on insulin treatment and presence of diabetic neuropathy. Cases with associated cerebrovascular diseases, benign prostatic hyper plasia had influence on voiding condition. In cases with long standing chronic urinary tract infection, fibrosis of the bladder wall resulted in low compliance bladder urodynamically. Fibrotic obstruction of ureterovesical junction can cause hydroureteronephrosis and lead to renal function impairment of diabetic patients. As vesical damage was irreversible at this late stage, proper management of early stage is crucial for management of diabetic patients. Our method of treatment and result on diabetic vesicourethral dysfunction will be presented and discussed. $309
Transcript
Neuropathy I
POS-002-165 DECREASING VARIABILITY IN ASSESSMENT OF DIABETIC PERIPHERAL NEUROPATHY
CA LAUDADI0, RD AITCHISON ICI Pharmaceuticals, Wilmington, DE, USA
Assessment of the onset and progress of diabetic neuropathy presents difficulties in both clinical practice and epidemiological research. Measurements available for the longitudinal assessment of neuropathy are often noisy and unreliable. Reducing the variability inherent in the measurement of neuropathy will provide both a more meaningful estimate of the true state of a study population and will increase the statistical power to detect a treatment effect in a clinical trial. The noise inherent in these measurements can be substantially reduced by repeated assessments at critical time points. Thus a good study design should utilize multiple assessments. This abstact provides data to support these recommendations and gives examples of these approaches.
In a trial of diabetic neuropathy triplicate assessments of thermal and vibratory thresholds were obtained during baseline and at critical time points in double blind therapy. Triplicate assessment decreased the analytical variance by 31% and 37% for thermal and vibratory thresholds, respectively. The power of the trial to detect a 20% treatment effect (n/group=200,alpha =.05) was increased from .6 to .8 for the thermal assessments and was maintained (>.95) for the vibratory data.
The effect of repeated assessments can also be expressed as a reduction in the number of patients needed for a trial. That actual savings realized depends upon the ratio of the between-patient to the within-patient variability. For this study recruitment was reduced by 50% by triplicate assessment.
In conclusion we recommend that repeated assessments be considered as a part of trial design whenever measurements are subject to repeat variability.
POS-002-166 VESICOURETHRAL DYSFUNCTION OF DIABETIC PATIENTS. AN URODYNAMIC EVALUATION.
K Kitamil), K Miyai 2) and T Takahashi 3) Department of Urology Yamato City Hospital I) , Yokohama City Kouwan Hospital 2) , and Hadano Red Cross Hospital 3) Yokohama, Japan
In order to evaluate vesicourethral dysfunction of diabetic patients, urodynamic studies were performed on 163 diabetic patients and 20 control cases.
In addition to the classical findings as impaired bladder sensation, decreased detrusor function and poor flow rate with residual urine, diabetic patients showed varieties of vesicourethral dysfunction such as hyperactive bladder, low compliance bladder and loss of detrusor-sphincter coordination.
The main factors related with poor vesicourethral function were early onset, longer duration, poor control of the disease, cases on insulin treatment and presence of diabetic neuropathy.
Cases with associated cerebrovascular diseases, benign prostatic hyper plasia had influence on voiding condition. In cases with long standing chronic urinary tract infection, fibrosis of the bladder wall resulted in low compliance bladder urodynamically. Fibrotic obstruction of ureterovesical junction can cause hydroureteronephrosis and lead to renal function impairment of diabetic patients. As vesical damage was irreversible at this late stage, proper management of early stage is crucial for management of diabetic patients.
Our method of treatment and result on diabetic vesicourethral dysfunction will be presented and discussed.
$309
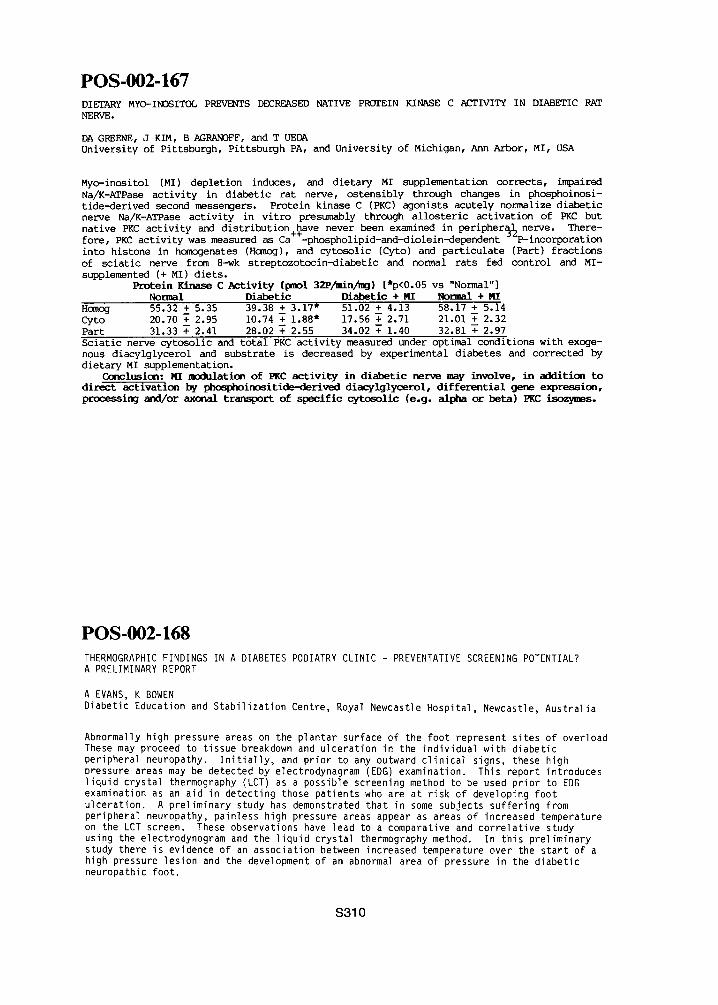
POS-002-167 DIETARY MYO-INOSITOL PREVENTS DECREASED NATIVE PROTEIN KINASE C ACTIVITY IN DIABETIC RAT NERVE.
DA GREENE, J KIM, B AGRANOFF, and T UEDA University of Pittsburgh, Pittsburgh PA, and University of Michigan, Ann Arbor, MI, USA
Myo-inositol (MI) depletion induces, and dietary MI supplementation corrects, impaired Na/K-ATPase activity in diabetic rat nerve, ostensibly through changes in phosphoinosi- tide-derived second messengers. Protein kinase C (PKC) agonists acutely normalize diabetic nerve Na/K-ATPase activity in vitro presumably through allosteric activation of PKC but native PKC activity and distribution+~ave never been examined in peripher~h nerve. There- fore, PKC activity was measured as Ca -phospholipid-and-diolein-dependent - P-incorporation into histone in homogenates (Homog), and cytosolic (Cyto) and particulate (Part) fractions of sciatic nerve from 8-wk streptozotocin-diabetic and normal rats fed control and MI- supplemented (+ MI) diets.
Protein Kinase C Activity (pmol 32P/rain/rag) [*p<0.05 vs "Normal"] Normal Diabetic Diabetic + MI Normal + MI
Homog 55.32 + 5.35 39.38 + 3.17" 51.02 + 4.13 58.17 + 5.14 Cyto 20.70 • 2.95 10.74 T 1.88" 17.56 ~ 2.71 21.01 ~ 2.32 Part 31.33 ~ 2.41 28.02 ~ 2.55 34.02 ~ 1.40 32.81 ~ 2.97 Sciatic nerve cytosolic and total PKC activity measured under optimal conditions with exoge- nous diacylglycerol and substrate is decreased by experimental diabetes and corrected by dietary MI supplementation.
Conclusion: MI modulation of PKC activity in diabetic nerve may involve, in addition to direct activation by phos~inc~itide-derived diacylglycerol, differential gene expression, processing and/or axonal transport of specific cytosolic (e.g. alpha orb eta) ~ i~s.
POS-002-168 THERMOGRAPHIC FINDINGS IN A DIABETES PODIATRY CLINIC - PREVENTATIVE SCREENING POTENTIAL? A PRELIMINARY REPORT
A EVANS, K BOWEN Diabetic Education and Stabilization Centre, Royal Newcastle Hospital, Newcastle, Australia
Abnormally high pressure areas on the plantar surface of the foot represent s i tes of overload These may proceed to t issue breakdown and ulcerat ion in the ind iv idual with d iabet ic peripheral neuropathy. I n i t i a l l y , and p r io r to any outward c l i n i ca l signs, these high pressure areas may be detected by electrodynagram (EDG) examination. This report introduces l i qu id crystal thermography (LCT) as a possible screening method to be used pr io r to EDG examination as an aid in detect ing those pat ients who are at r isk of developing foot u lcerat ion. A prel iminary study has demonstrated that in some subjects suffer ing from peripheral neuropathy, painless high pressure areas appear as areas of increased temperature on the LCT screen. These observations have lead to a comparative and cor re la t i ve study using the electrodynogram and the l i qu id crystal thermography method. In th is prel iminary study there is evidence of an association between increased temperature over the s ta r t of a high pressure lesion and the development of an abnormal area of pressure in the d iabet ic neuropathic foot.
$310
POS-002-169 VARIABILITY OF VIBRATION THRESHOLD IN DIABETIC PATIENTS
CD WILLIAMS, S TILL, AF MacLEOD, and PH SONKSEN. Department of Medicine. UMDS, St Thomas" Hospital, London SEI 7EH, UK.
Biothesiometry provides an objective measure ot vlbration threshold. We have routinely recorded blothesiometry readings taken at the thumbs, medial malleoli and great toes of all diabetic patients newly attending our department. 1052 records, complete for biothesiometry and 25 other items of clinical data have been examined statistically. 511 patients had diabetes for 1-58 years and 541 patients were newly diagnosed. Readings differed by 30 % between left and right in 16 % of patients, and abnormally high readings at one site in the lower limbs were observed in 8 % of patients. Of these only 25 % had abnormally high readings at all four sites. Univariate analyses showed an association between biothesiometry readings and age (p<0.O01) and significant associations (p<O.001) between higher age-adjusted scores and proteinuria, retinopathy, diabetic foot problems and Dupuytrens contracture. Age-adjusted scores increased with increasing duration of diabetes (p<0.001) and those taken at the medial malleoli and great toe increased with patients" height (p<O.O01), alcohol (p<0.Ol) and cigarette (p<0.025) consumption. Lower scores were observed in women (p<0.O01) and Afro-Carlbbean patients (p<O.O01). Multiple linear regression demonstrated higher readings to be associated independently to a significant level (p<0.025) with age, duration of diabetes and ambient blood glucose. In the lower limb, scores were associated independently to a significant level with height and race, but not with alcohol consumption, smoking or gender. We conclude biotheslometry readings are associated with several microvascular complications and increase with duration of diabetes independently of age. Readings vary according to the site of measurement. Tall patients have higher readings in the lower limbs, lower readings are obtained in Afro-Caribbean patients.
POS-002-170 INVERSTIGATION THE MECHANISM OF DIABETIC GANGRENE.
*T SHIMADA, H ITO, S TANAKA, Y ISOGAI, *~Y MORI, K KAWAKAMI *The 3rd Dept. of the Internal Med., ~Dept. of Radiology of Jikei University School of Medicine, Tokyo, Japan.
The shunt blood flow(Fshunt) in the leg of the diabetics was evaluated by radionuclide method. Shunt rate in lower extremities was calculated from pulmonary activity after injection of Tc-99m-MAA into femoral arteries. In 48% of 82 diabetics, the shunt rate was exceed the average+2SD of shunt rate(l.86%) in i0 normal All of cases with gangrene were included in this group. Shunt rate in the sym- pathetectomized legs in 6 cases with TAO was high (13.2%). To evaluate regulation of Fshunt, total, skin and muscle flow(Ft,Fs,Fm) were measured by admittance plethysmography and Xe-133 clearance method. Fshunt was calculated from the equation Fshunt=Ft-(0.1Fs+0.7Fm). (0.1 and 0.7 was vol% of skin and muscle respectively). Fshunt in the normal subjects was 0.51ml/min/100g at rest and was markedly increased upon warming of the lower leg. In diabetics with high shunt rate, Fshunt was i.i at rest and 1.0ml/min/ 100g upon warming. In 6 dogs, phentolamine and noradrenalin were administered. Fm was increased by phentolamine and decreased by noradrenalin. While Fs responded inversely to Fm, indicating steal phenomenon. These results suggest that in normal subjects Fshunt is small and is increased upon warming by opening of dermal arterio-venous anastomoses, but in the diabetics, Fshunt is large even at rest due the diabetic autonomic neuropathy. This was supported by the results of sympathetectomized cases and animal
experiments. These results suggest in creased shunt flow due to diabetic auto-
nomic nerve disturbance may be a prodromal symptom of diabetic gangrenes.
S311
POS-002-171 SKIN PERFUSION PRESSURE IN THE LEG OF DIABETIC PATIENTS.
"H ITO, T SHIMADA, "S TANAKA, " Y ISOGAI, "'Y MORI, "'K KAWAKAMI "The 3rd Dept. of Internal Med., "'Dept. Radiology of Jikei University School of Medicine, Tokyo, Japan.
We developed a new technique for measuring the skin perfusion pressure (SPP) by Xe-133 clearance method and studied the SPP in diabetics to investigate the mechanism of diabetic gangrene. Our method has two features compared with the conventional method. 1) A small cuff was used not to disturb venous drainage. 2) Decreasing pressure method was applied instead of increasing pressure method. The SPP was measured in 20 nolmal volunteers and 66 diabetics, 6 of whom had diabetic gangrene. Xe-133 dissolved saline (0.01 ml, 100~Ci) was injected into the skin of the pretibial region. The depot was covered with a small cuff. The cuff was inflated quickly to stop the peripheral blood flow, then deflated gradually while monitoring its pressure with a electric pressure controlling equipment. When the cuff pressure falls to a certain point, clearing of the Xe-133 by the blood flow starts. This point of the pressure was considered the SPP. The skin blood flow was calculated from the clearance curve of this Xe-133. The SPP was 33.5~7.2 cm H20 in normal subjects, 25.4~8.7 cm H20 in the diabetics without gangrene, and 19.1 ±4.9 cm H20 in the diabetics with gangrene. The skin blood flow was also significantly decreased in diabetic patients. The low SPP in the diabetics may be due to the steal phenomenon of the blood flow through the arteriovenous shunt vessels that dilate abnormally due to diabetic neuropathy. The blood flow in the capillary bed is, therefore, decreased in the diabetics. The simultaneous measurement of the SPP and the skin blood flow by Xe-133 clearance method is useful to assess the impairment of peripheral circulation by diabetic neuropathy.
POS-002-172 ELECTRODYNOGRAM (EDG) IN OBJECTIVE ASSESSMENT OF BEARING PRESSURES IN THE FEET OF DIABETIC PATIENTS.
L. SMITH, W. PLEHWE, D.K. YUE, J.R. TURTLE. Diabetes Centre, Royal Prince Alfred Hospital, Sydney, N.S.W., Australia.
The exact role of foot bearing pressures (FBP) in the pathogenesis of foot ulcers (FU) is net clear. The EDG 1184 system was used to compare maximum and mean FBP in both feet of ii diabetic patients (Gp I) who had recently healed unilateral FU, with FBP in ii patients with no history of FU (Gp 2). To assess methods of reduction of FBP, mean and maximum FBP were also measured in 12 patients without active FU (Gp 5) for l:barefoot, 2:wearing shoes, 3:shoes with PPT shock-absorbing inlay (Langer Biemechanics Group). Measurements were taken from electrodes at 7 standard positions including ulcer site if applicable, during a 5s period after walking for at least 20m. Stance phase duration (contact, midstance, propulsion) was measured bilaterally. No difference in maximum FBP, duration of weightbearing, and percentage of stance at which peak FBP occurred was found in Gp 1 patients between previously FU and control feet. Mea_~tetal maximum FBP in Gp 1 was greater than in Gp 2 (10.64+--5.91 vs 4.19~ 1.29kg.cm , mean+SD, P<0.01) and duration of propulsion phase was slightly shorter in Gp 1 than in Gp 2 (232~37 vs 195~47ms P=0.054). Mean FBP during a step was altered inconsistently by wearing shoes with or without PPT (Gp 3), but total maximum FBP (sum of maximum FBP of the 7 electrodes) was reduced bilaterally by wearing shoes and was further reduced to 17Z below barefoot by inserting PPT (R: 6.68± 2.23 [i], 6.13+--1.82 [2], 5.55+-1.73 [3]: P<0.02 vs [I]; L: 7.41+-1.53 [i], 6.54+_1.28 [2], 6.13+--1.34 [3]: P<0.01 vs [i]). Maximum FBP was reduced significantly at 5 of the 14 individual pressure points. However maximum FBP reduction by PPT was small. These data indicate that while maximum FBP may be important in the pathogenesis of FU, the roles of other factors (eg duration of stance phases, biomechanical dysfunction) also require definition.
S312
POS-002-173 EFFECTS OF 5 YEARS CONTINUOUS SUBCUTANEOUS INSULIN INFUSION (CSII) ON PERIPHERAL NERVE
Diabetes-Research I n s t i t u t e at the Un ivers i ty of D~sseldorf, DDsseIdorf, F.R.G.
I t is possib]e to achieve t i gh metabol ic cont ro l by CSII even in unstable d iabe t i c pa t ien ts . The bene f i c ia l e f f ec t of near-normoglycemia on per iphera l nerve funct ion is also wel l documented over a period of one or two years, longer studies have not yet been performed . Therefore in a prospect ive study 15 c-pept ide negat iv pat ients (7 male, 8 female, age 35,8 yrs , range 22-50, dura t ion of diabetes 16,2 yrs , range 3-29) were a l loca ted to CSII t reatment and fo l lowed up over 5 years. Metabol ic cont ro l was done monthly by HbA1-measurement (normal range 5.5-8.5%). Mean HbAI values were ca lcu la ted over one year and compared to the HbAI value at the beginning of the study (mean + SD). Assessement of per iphera l nerve funct ion was done once a year by motor and sensory n@rve conduction v e l o c i t y (MNCV,SNCV) of the median, peroneal and sural nerve.MNCV and SNCV values of each year were compared to the values at basel ine (mean + SD). Paired t - t e s t was appl ied to d i f ferences over t ime. HbAI decreased s i g n i f i c a n t l y from 11.8 + 3 .1% to 8.9 , 9.3 % over 5 years. MNCV of the peronea! nerve increased s i g n i f i c a n t l y from basel ine to the f i r s t , second and t h i r d year of CSII therapy (38.5 m/s to 42.6 m/s, t h i r d year, p<O.05) and decreased in the las t two years to 40.3 m/s (N.S.) . MNCV of the median nerve increased s i g n i f i c a n t l y only in the f i r s t year of therapy (48.5 m/s to 50.7 m/s, p<O.05). No fu r the r improvement of MNCV was ob- served u n t i l the end of the study. No s i g n i f i c a n t changes in SNCV (median and sural nerve) were observed over 5 years. We conclude tha t t i gh metabol ic contro l by t reatment with CSII over 5 years leads to s i g n i f i c a n t improvement of MNCV of the peroneal nerve over 3 years and MNCV of the median nerve over one year . SNCV remains unchanged.
POS-002-174 NO ENHANCEMENT OF VAGAL TONE BY CAPTOPRIL ON INFRA-RED PUPILLOMETRY OF DIABETIC PATIENTS WITH AUTONOMIC NEUROPATHY
A. DE VOS*, S. COPPACK, T.D.R. HOCKADAY Dep. of Endocrin.*, Free Univ. Hosp., Amsterdam, The Netherlands, Sheikh Rashid Diabetes Unit, Radcliffe Infirmary, Oxford, U.K.
The hypotensive drug Captopril has been claimed to increase vagal activity, even in diabetics with autonomic neuropathy. We have studied its effect in 8 diabetic patients (6 M, 2 F; age range:40-72 years, mean 57), who had given informed consent. All had clinical signs or symptoms of autonomic neuropathy. In a double blind, randomised, cross over study, the patients were given a single dose of either 25 mg Captopril or placebo, with a washout of one week. 3 Tests of autonomic function were applied: i) Heart rate responses to deep breathing (~I-E), 2) to standing up (~HR) and 3) pupi i lome try (latency of the constriction of the pupil in the response to a light stimulus measured by an infra-red light reflection technique). Systolic supine blood pressure, measured at 2 h, showed a significant fall (125.2 + 19.9 vs 137.0 + 15.0 mmHg, Mean + ISD, p<0.05) while dias to~ic dropped also (71.8 + 5.4 vs 76.3 ~ 6. I) but not significantly. Captopril didn't change either ~I-E (7.0 + 5.0 vs 6.5 + 4.0, beats per minute) or ~HR (19.1 + 4.9 vs 19.1--+ 9.6). Pupi~lometry, a proven more accurate and sensitive t~st of autonomic function, didn't show improvement in the constriction latency either (319 + 56 vs 313 + 57 ms). We conclude that Captopril doesn't enhance vagal activity in diabetic patients with autonomic dysfunction.
$ 3 1 3
POS-002-175 GARETH J. PARRY, M.D., JOHN SCHAEFFER D.O., HAHNEMANN UNIVERSITY PHILADELPHIA, PA
Resistance to ischemic nerve conduction failure (RINCF) occurs in diabetes, even in the absence of overt neuropathy. The cause is unknown but hyperglycemia may increase stores of energy substrate in nerve. We therefore examined the effect of acute hyperglycemia (>300 mg/dl), produced by intraperitoneal glucose injection, on RINCF in normal rats. In the first experiment RINCF was measured hourly for five hours in normoglyeemic rats. Baseline time to block was 19.0±1.7 minutes, falling to 13.3±1.0 minutes at one hour and then remaining constant. In the second experiment baseline RINCF was measured immediately before hyperglycemia and repeated hourly for four hours. After one hour of hyperglycemia the time to block had fallen from baseline of 18.7±2.4 to 17.3±2.1 minutes which is significantly different from controls (p<O.01). At two hours, RINCF had returned to baseline where it remained to four hours. In the third experiment baseline RINCF was measured 24 hours prior to hyperglycemia and then repeated 24 hours later, after one to four hours of hyperglycemia. Baseline time to block was 18.7_+0.8. After one hours of hyperglycemia it increased to 21.3_+0.8 minutes and after two hours to 23.3--+0.9 minutes. There was no further increase between two and four hours. We postulate that with normal blood glucose the initial fall in RINCF in successive hourly studies represents depletion of energy substrate during ischemia. With hyperglycemia the depletion of substrate caused by each period of ischemia is rapidly replenished and RINCF is unchanged. When no preceding period of ischemia has occurred, hyperglycemia increases substrate with a parallel increase in RINCF.
POS-002-176 EVALUATION OF THERMAL, PAIN, AND VIBRATION SENSATION THRESHOLDS IN NEWLY DIAGNOSED
TYPE I (INSULIN-DEPENDENT) DIABETIC PATIENTS.
D. ZIEGLER, P.MAYER, F.A.GRIES Diabetes Research I n s t i t d t e at the Un ivers i t y of DOsse]dorf, DOsseldorf, F.R.G.
I t is not known whether cutaneous detect ion thresholds may a l ready be impaired at diagnosis of d iabetes. Therefore, we studied small and large f i b e r funct ion by 12 (6 in the hand and the foo t , respec t i ve ly ) q u a n t i t a t i v e tes ts fo r assessment of cutaneous sensation in 40 newly diagnosed Type I d iabe t i c pat ients (mean + SD:age: 26 + 7 y r , dura t ion of i nsu l i n t reatment : 10 + 5 days, HbA1c: 11.0 + 2.6%, mean blood glucose: 128 + 29 mg/dl) and in 48 age-matched cont ro l subjects. Thermal d i sc r im ina t ion ( f o o t ) , warm and cold percept ion ( thenar and f o o t ) , and heat and cold percept ion thresholds ( thenar) were s i g n i f i - cant ly e levated in the pat ien ts as compared to the cont ro ls (p<O.05 to p<O.O01). There were no s i g n i f i c a n t d i f fe rences between the groups with regard to thermal d i sc r im ina t ion ( thenar) , heat and cold pain percept ion ( f oo t ) , and metacarpal as wel l as ma l leo la r v i b ra t i on per- cept ion thresholds. The rates of abnormal i t ies in the i nd i v idua l tests ranged from 0% to 27,5 %, being lowest f o r v i b ra t i on percept ion and highest f o r thermal percept ion thresholds a f t e r cold s t imu l i . Nine of 12 tests cor re la ted s i g n i f i c a n t l y with age but only 2 were re la ted to HbA1c. Results of one tes t were s i g n i f i c a n t l y associated with those of another tes t in 32 of 66 regression analyses. Each of the small f i b e r parameters was re la ted to another on the foot but not on the thenar.
We conclude tha t only cutaneous sensation thresholds t ransmi t ted by small f i be rs are impaired at diagnosis of Type I diabetes despi te of the cor rec t ion of i n i t i a l ketosis and hypergIy- caemia. Cold percept ion tests were most sens i t i ve in detec t ing abnormal i ty . A d i f fuse a f fec t ion of d i f f e r e n t small f i b e r funct ions which is re la ted to age is present in newly diagnosed Type I d iabe t i c pa t ien ts .
$ 3 1 4
POS-002-177 DOES THE SYMPATHETIC DYSFUNCTION ~RECEDE THE PARASYMPATHETIC DYSFUNCTION IN DIABETIC AUTONOMIC NEUROPATHY?
T HASUNUMA, S MOCHIO, H OKA, A KURITA, T NOHARA, Y ISOGAI 3rd Department of Medicine, Jikei University School of Medicine, Tokyo, Japan.
Autonomic dysfunction is often found in diabetics. We investigated the relationship between the sympathetic and parasympathetic function in diabetics. The subjects were 15 diabetics and 6 healthy controls.We used the following two methods.: The coefficient of R-R interval variations of ECG (CVR-R) was used as indicator of the parasympathetic function. The coefficient of variation of amplitudes in digital plethysmography (CVamp) was used as indicator of the sympathetic function (Toshima's method). Plethysmography of the second finger of the hand was recorded, of which thirty waves were analyzed. It has been already reported that administration of the sympathetic alpha-blocker decreases the variation of the amplitudes in digital plethysmography. Therefore, it can be assumed that the CVamp represents the sympathetic function. The follow- ing results were obtained; i) The CVR-R in diabetics was lower than that of the controls(2.1% vs 3.9%). 2) The CVamp in diabetics was lower than that of the controls (7.1% vs 9.8%). 3) When the diabetics were divided into severe and mild groups by the severity of the parasympathetic function, there was no significant difference in the values of CVamp between the two groups. From the above results, it ~;as suggested that sympathetic dysfunction precedes parasympathetic dysfunction in diabetic autonomic neuropathy.
POS-002-178 CENTRAL NEUROPATHY IN DIABETES MELLITUS
A KURITA, S MOCHIO The Third Dept. of Intern. Med., The Jikei Univ. School of Medicine, Tokyo, Japan.
In order to examine the presence of central nervous involvement in diabetes, auditory brainstem evoked responses(ABER) and somatosensory evoked potentials (SEP) were observed in 27 diabetic subjects (mean~SD, 50.5 ~I0.3 years) and in 12 age-matched normal controls. The diabetics were divided into two groups, mild group(n=12) and severe group(n=15), based on the severity of peripheral neuropathy evaluated by the neurological findings and by the reduction in motor nerve conduction velocity(MCV) of the posterior tibial nerve. Central portion of the evoked potentials were assessed by the central transmission time(CTT) by measuring the intervals of waves I-V in ABER and those of N13-N20 in SEP from the median nerves. The diabetic subjects showed significantly longer CTT by both methods than controls(p<0.01), and CTT in the severe group were longer than those in the mild group(p<0.05). Moreover, among the diabetics, the reductions in MCV correlated significantly with the prolongations of CTT by both methods(ABER;r=0.63, p<0.01, SEP;r=0.72, p<0.01). The impairment of evoked potentials were not related to plasma glucose level, to the duration of illness and to the diabetic nephropathy. Only diabetic retinopathy, however, was related to ABER impairment. Our data suggest the presence of diabetic central neuropathy and its occurrence coincided with the peripheral neuropathy.
$315
POS-002-179 AUDITORY BRAINSTEM RESPONCE IN DIABETICS
Y ONO, S TSUSHIMA, M KUDOH, S NAKAGAWA* Department of Internal Medicine, Tonan Hospital, Sapporo, Japan. The Second Dep~rtment of Internal Medicine, Hokkaido University School of Medicine, Sapporo, Japan
To assess the changes of the central nervous system function in diabetics, the auditory brainstem response (ABR) was recorded in 53 diabetics and followed in 20 of them for 2 years. Interpeak latency (IPL) as well as a new analysis to measure the changes of the wave latencies under high power s t imu l i and low power s t imu l i was determined to evaluate the co r re la t i on between ABR and other complications of diabetes. The ABR was recorded by DISA system 1500 with I0 msec analysis time set from 60 dB to 120 dB.
In diabetics, the latency of wave I, l l I , V and IPL was prolonged especially in low power s t imu l i . The d i f ference of the latency of wave V between 120 dB and 60 dB s t imu l i was also prolonged in diabetics and i t was prolonged s ign i f icant ly in the patients with peripheral neuropathy, autonomic neuropathy, and long h is to ry of diabetes compared wi th the pat ients without them. But in the patients without diabetic complications and the patients with short h i s to ry of diabetes and good blood sugar contro ls , the d i f ference of the latency of wave V between 120 dB and 60 dB stimuli was s ign i f icant ly prolonged compared with normal controls. So th is new form of analysis for measuring the changes in the wave latencies under high power s t imu l i and low power s t imu l i in ABR was considered to be very useful fo r evaluat ing neurological abnormalities of the central nervous system in diabetic patients.
After 2 years, ABR became prolonged especially in patients whose renal function became worse and those whose blood sugar control were not good . I t 's prolongation was mainly wave I, and wave I-V IPL, I - I l l IPL and I I I -V IPL didn't prolong s ign i f icant ly for 2 years.
POS-002-180 TWO OPTIMIZED TESTS TO ASSESS DIABETIC AUTONOMIC NEUROPATHY
G SEGALINI, E BORSOTTI, F CALASSO, C GALLI, N MUSACCHIO, M PALADINI, A ROCCA, P RUHI
Divisione di Medicina Generale, Ospedale Bassini - Cinisello Balsamo, Milano
We evaluated the usefulness of two autonomic function tests, that is cold pressor (CP20) test for 20" and the handgrip test at maximal strength (HGm) for 5". We studied 93 diabetic patients (D) without autonomic neuropathy symptoms (aged 20-60 mean 40.5), 12 diabetics with autonomic neuropathy (aged 43-69, mean 55.2), and 70 normal control subjects (N) (aged 20-60, mean 39.7). The R-R variation and ratio between the maximum R-R interval of reco- very phase and the minimum R-R under stimulation, for CP20 and HGm, were calculated. The two tests showed a good reproducibility. The mean values (~DS)In the three groups resulted as follows:
N D NAD * p < 0.000 vs N C P 2 0 1 - 3 4 " 0 . 1 8 1 . 2 5 + 0 . 1 4 * 1 . 1 1 ÷ 0 . 0 3 - * # p < 0 . 0 0 5 v s N HGm 1 - 4 7 " 0 . 2 6 1 . 3 6 + 0 . 1 9 # 1 . 1 1 - 0 . 0 5 ~ * ~ * p < 0 . 0 0 0 MS D
In the whole population the following 5 tests were also performed: deep breathing, Valsalva ratio, standin~ ratio, blood pressure response to standing, sustained handgrip. We compared two different scoring systems for evaluating cardiovascular autonomic response. The scores obtained from 5 current tests was compared to the new scoring system, including the 2 new tests we adopted. We report a significant reduction of false positive and false negative cases. Both tests are easy to perform, not disturbing the patient and were proven to be very sensitive for the screening of autonomic neuropathy in diabetics.
S316
POS-002-181 MORTALITY IN DIABETIC AUTONOMIC NEUROPATHY
G. MENZINGER,V. SPALLONE*,M.R. MAIELLO,M.G. FELICI,S. GAMBARDELLA
CATT. MALATTIE DEL RICAMBIO,II UNIVERSITA' ROMA;*ENDOCRINOLOGIA I,l UNIVER$ITA' ROWA, ITALY
To assess whether autonomic neuropathy(AN)is associated with a higher mortality risk in diabetes,we
evaluated percentage(%)mortality rate in 122 diabetics,67 with abnormal beat to beat variation of
~artrate on deep breathing(DB)(41M and 26 F,mean age 48.7+10.5 yrs,mean duration of diabetes 16.1
~7.9 yrs),35 with normal DB(18 M and 17 F,mean age 44.5~9.4,mean duration of diabetes ll.9~7.3)and
20 with borderline score of DB(13M and 7F,mean age 50.2~9.3,mean duration of diabetes 12.7~i0). %
mortality rate was calculated at 1,2,3,4,5 and 6 yrs.The duration of retrospective study varied
from i to 6 yrs with 55 patients followed for 6 yrs.Statistical analysis was by Student's 't' and
×2 test.lO out of the diabetics with abnormal DB(15%)died during the observation period,1 after 6
yrs,5after 5 yrs,1 after 4 yrs,2 after 3 yrs and 1 after i yrs.% mortality rate was 25.7 at 5 yrs
and 33.3 at 6 yrs. In the group with borderline DB there was just i death(5%) with % mortality rate
of ll.1 at 5 yrs and of 12.5 at 6 yrs.None of diabetics with normal DB died.% mortality rate at 6
yrs was significantly higher in diabetics with abnormal DB than in diabetics with borderline and n 2 ormal DB(X =9.32,p<O.Ol).The causes of death were neoplasm(3 patients),cardiac failure,cirrhosis, m1~cavdial infarction(2 patients),renal failure,unknowu (3 pat.).In the AN group analysis of age,
duration of diabetes,% of IDD,the presence of retinopathy and nephropathy did not show significant differences between those who survived and those who died.DB test was significantly lower in those who died(1.8~l.4 BPM)than in those who survived (4.9~2.9 BPM)(p~O.OO25).Furthermore % mortality
rate was higher in AN diabetics with postural hypotension,reaching 46% at 6 yrs. In conclusion this study shows a significant higher mortality rate in diabetics with AN than in diabetics without AN. Postural hypotension in addition to abnormal autonomic tests increases the risk of death.
POS-002-182 GUSTAIDRY S~'LATING: A CLINICAL MARKER OF ADVANCED MICROANGIOPATHY.
G.CORIGLIANO, D.VITALL, L.h~IELLO, A .E . IDZZI , M.DISABATO, M.E.DE FEO, A.W. D'AGOSTINO. ASSOCIAZIONE ITALIANA DIABETE - NAPOLI - ITALY The aim of the study was to assess whether gustatory sweating(G.S.}could be consi-
dered a clinical marker of microangiopathy. PATIENTS:8 IDDM(6M,2F}who complained wi
th G.S.{~ZSD,age:48ZI3 ys,duration of disease 21.5Z6.2ys,BMI23±3,11BAI 8.6ZI},8 IDD
M comparable (p 0.5)for the precedings variables,without G.S.,were the controls(C).
~THODS:G.S.was evaluated after a standard meal by leaning on the foreheas a pre-
viously alkalised dabber,sprinkled w~th quinizarin,a red powder that turns to Blue
when in contact with water if pH is 8.HBA 1 was measured By microcolumn cromatogra-
ed,deep breathing~BD)and handgrip sustained{HS)tests were performed in all patien-
ts. Student t test was used to investigate differences of the variables Between the
two groups of patients,except for R(Mann and ~%%itney test u}.RESULTS:R in 7 cases
(proliferative in 3,blindness in 3)wile it was present in 4 cases among C(never p[
oliferative){pO.Ol},M 265~282mg/ l (C :21 .2~24 .7 ,pO.O44) , t IS13 .7±6 .4mmIIg(C:18 .1~3 .7n . s . } ~ F u r t h e r m o r e t h e r e were 5 c a s e s o f impo tence o u t o f 6 m a l e , 1 case o f d i a b e t i c d i a r r h e a and 2 o f a symptoma t i c h y p o g l i e e m i a s (none o f t h e s e c o m p l i c a t i o n s i n C).CON: CLUSIONS:G.S. is p o s i t i v e l y r e l a t e d to advanced m i c r o a n g i o p a t h i c f e a t u r e s ; i t s h o u l d be searched in all diabetic patients with more than 5 ys of disease:diabetic pati~
nts with G%S.arb to Be considered at elevated risk: a more sensitive test for G.S. could detect presTmptoma£ic cases and be an early marker of microangiopathy. *DB 5.7±9.1{C:14.2i7.2, p O.05),OH -24.3±12.6mmIIg(C: -6.2±8.3, p 0.005).