Page 1
’
Page 1 of 37
MED AUF
CRANIAL NERVES and NEUROLOGICAL EXAMINATION HOMEWORK AND SEATWORK | June 26, 2015 | NEUROLOGY
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
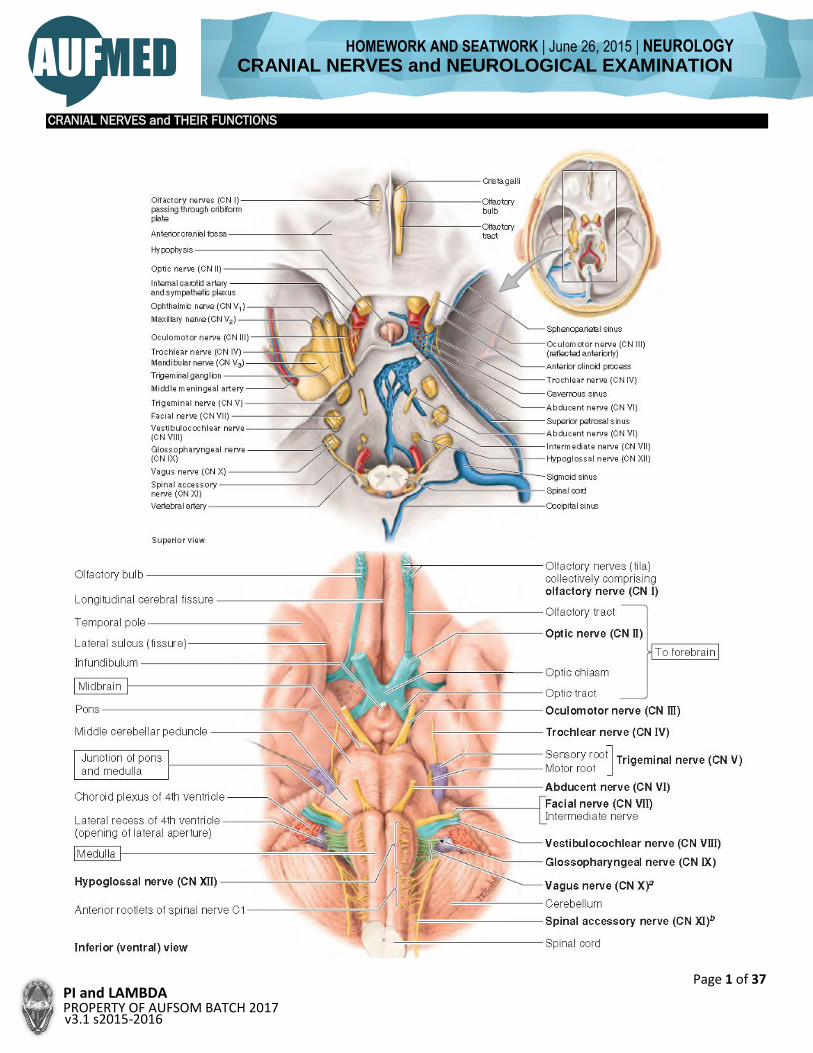
CRANIAL NERVES and THEIR FUNCTIONS
Page 2
Page 2 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
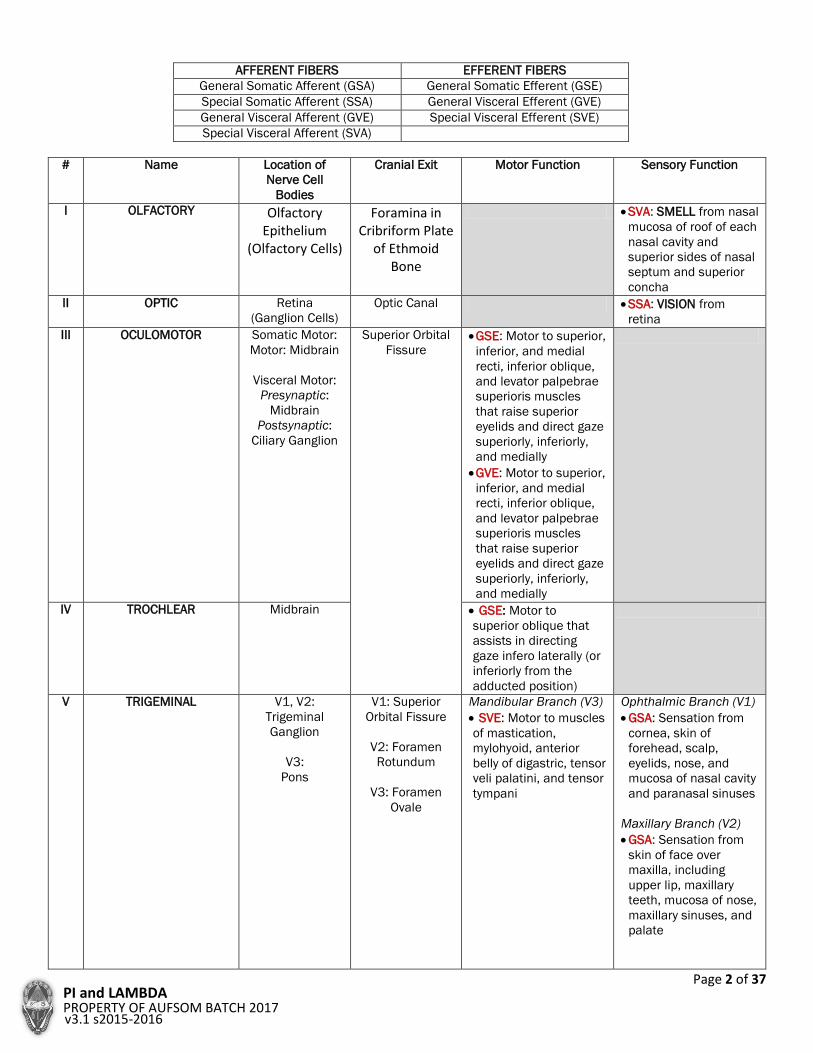
AFFERENT FIBERS EFFERENT FIBERS
General Somatic Afferent (GSA) General Somatic Efferent (GSE)
Special Somatic Afferent (SSA) General Visceral Efferent (GVE)
General Visceral Afferent (GVE) Special Visceral Efferent (SVE)
Special Visceral Afferent (SVA)
# Name Location of
Nerve Cell
Bodies
Cranial Exit Motor Function Sensory Function
I OLFACTORY Olfactory Epithelium
(Olfactory Cells)
Foramina in Cribriform Plate
of Ethmoid Bone
SVA: SMELL from nasal
mucosa of roof of each
nasal cavity and
superior sides of nasal
septum and superior
concha
II OPTIC Retina
(Ganglion Cells)
Optic Canal SSA: VISION from
retina
III OCULOMOTOR Somatic Motor:
Motor: Midbrain
Visceral Motor:
Presynaptic:
Midbrain
Postsynaptic:
Ciliary Ganglion
Superior Orbital
Fissure GSE: Motor to superior,
inferior, and medial
recti, inferior oblique,
and levator palpebrae
superioris muscles
that raise superior
eyelids and direct gaze
superiorly, inferiorly,
and medially
GVE: Motor to superior,
inferior, and medial
recti, inferior oblique,
and levator palpebrae
superioris muscles
that raise superior
eyelids and direct gaze
superiorly, inferiorly,
and medially
IV TROCHLEAR Midbrain GSE: Motor to
superior oblique that
assists in directing
gaze infero laterally (or
inferiorly from the
adducted position)
V TRIGEMINAL V1, V2:
Trigeminal
Ganglion
V3:
Pons
V1: Superior
Orbital Fissure
V2: Foramen
Rotundum
V3: Foramen
Ovale
Mandibular Branch (V3)
SVE: Motor to muscles
of mastication,
mylohyoid, anterior
belly of digastric, tensor
veli palatini, and tensor
tympani
Ophthalmic Branch (V1)
GSA: Sensation from
cornea, skin of
forehead, scalp,
eyelids, nose, and
mucosa of nasal cavity
and paranasal sinuses
Maxillary Branch (V2)
GSA: Sensation from
skin of face over
maxilla, including
upper lip, maxillary
teeth, mucosa of nose,
maxillary sinuses, and
palate
Page 3
Page 3 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
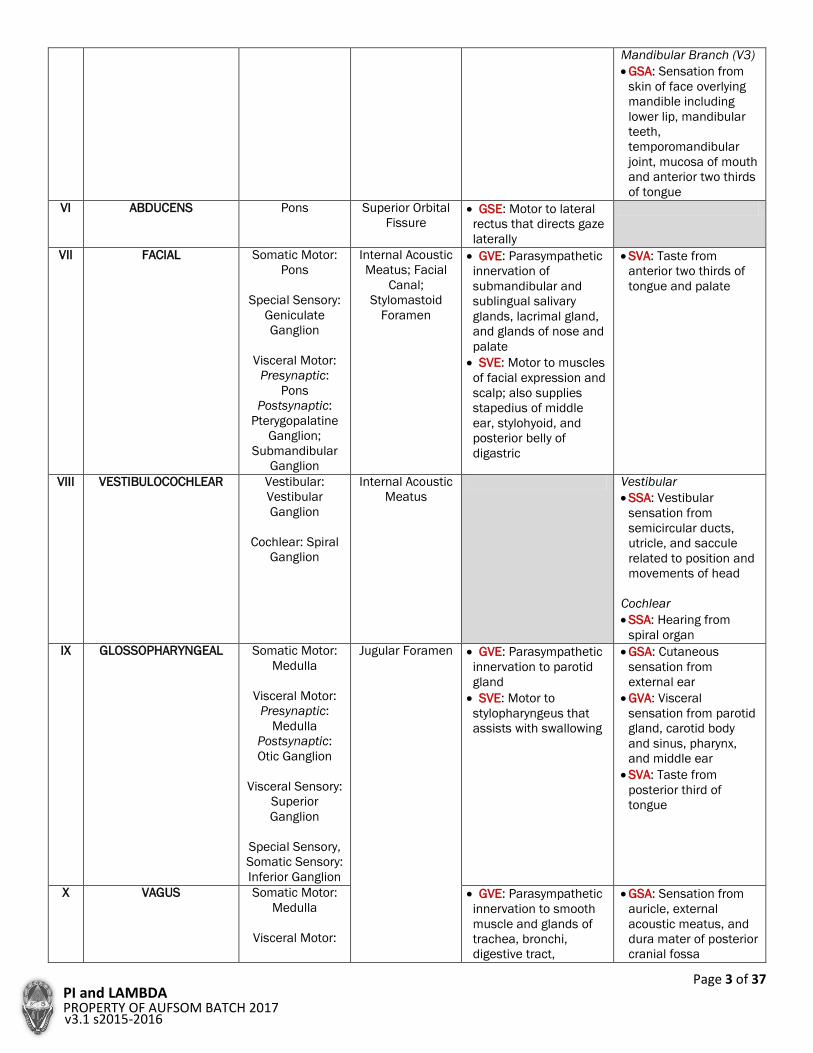
Mandibular Branch (V3)
GSA: Sensation from
skin of face overlying
mandible including
lower lip, mandibular
teeth,
temporomandibular
joint, mucosa of mouth
and anterior two thirds
of tongue
VI ABDUCENS Pons Superior Orbital
Fissure GSE: Motor to lateral
rectus that directs gaze
laterally
VII FACIAL Somatic Motor:
Pons
Special Sensory:
Geniculate
Ganglion
Visceral Motor:
Presynaptic:
Pons
Postsynaptic:
Pterygopalatine
Ganglion;
Submandibular
Ganglion
Internal Acoustic
Meatus; Facial
Canal;
Stylomastoid
Foramen
GVE: Parasympathetic
innervation of
submandibular and
sublingual salivary
glands, lacrimal gland,
and glands of nose and
palate
SVE: Motor to muscles
of facial expression and
scalp; also supplies
stapedius of middle
ear, stylohyoid, and
posterior belly of
digastric
SVA: Taste from
anterior two thirds of
tongue and palate
VIII VESTIBULOCOCHLEAR Vestibular:
Vestibular
Ganglion
Cochlear: Spiral
Ganglion
Internal Acoustic
Meatus
Vestibular
SSA: Vestibular
sensation from
semicircular ducts,
utricle, and saccule
related to position and
movements of head
Cochlear
SSA: Hearing from
spiral organ
IX GLOSSOPHARYNGEAL Somatic Motor:
Medulla
Visceral Motor:
Presynaptic:
Medulla
Postsynaptic:
Otic Ganglion
Visceral Sensory:
Superior
Ganglion
Special Sensory,
Somatic Sensory:
Inferior Ganglion
Jugular Foramen GVE: Parasympathetic
innervation to parotid
gland
SVE: Motor to
stylopharyngeus that
assists with swallowing
GSA: Cutaneous
sensation from
external ear
GVA: Visceral
sensation from parotid
gland, carotid body
and sinus, pharynx,
and middle ear
SVA: Taste from
posterior third of
tongue
X VAGUS Somatic Motor:
Medulla
Visceral Motor:
GVE: Parasympathetic
innervation to smooth
muscle and glands of
trachea, bronchi,
digestive tract,
GSA: Sensation from
auricle, external
acoustic meatus, and
dura mater of posterior
cranial fossa
Page 4
Page 4 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Presynaptic:
Medulla
Postsynaptic:
Viscera
Visceral Sensory:
Inferior Ganglion
Special Sensory:
Inferior Ganglion
Somatic Sensory:
Superior
Ganglion
coronary arteries, and
nodes of conduction
system of heart
SVE: Motor to muscles
of pharynx (except
stylopharyngeus).
intrinsic muscles of
larynx, muscles of
palate (except tensor
veli palatini), and
striated muscle in
superior two thirds of
esophagus
GVA: Visceral
sensation from base of
tongue, pharynx,
larynx, trachea,
bronchi, heart,
esophagus, stomach,
and intestine to left
colic flexure
SVA: Taste from
epiglottis and palate
XI SPINAL ACCESSORY Spinal Cord Cranial Root
SVE: Muscles of soft
palate (except tensor
veli palatine), pharynx
(except
stylopharyngeus), and
larynx (except
cricothyroid) in
branches of the vagus
Spinal Root
SVE: Motor to
sternocleidomastoid
and trapezius
XII HYPOGLOSSAL Medulla Hypoglossal
Canal GSE: Motor to intrinsic
and extrinsic muscles
of tongue (except
palatoglossus)
Reference: Moore, K.L., Dalley, A.F., & Agur, A.M.R. (2014). Moore’s clinically-oriented anatomy [7th ed.]. pp. 1058-1059.
Philadelphia, PD: Wolters Kluwer Health, Lippincott Williams & Wilkins
NEUROLOGICAL ASSESSMENT
Text in BLUE are ABNORMAL FINDINGS in the videos found at
http://library.med.utah.edu/neurologicexam/html/home_exam.html
A. MENTAL STATUS EXAMINATION
The cerebral hemispheres represent the highest and most
complex level of neurological function. There is so much
integration of cortical function that whatever system is used
to clinically "examine" the cerebral hemispheres will be an
over simplification and somewhat artificial
compartmentalization. Although a lot of mental status reflects
integration of cortical function, it can still be divided into parts
that correspond to the divisions of the cerebral hemispheres.
This anatomy review will be a brief overview of areas of
cortical function that can be examined by components of the
mental status exam.
Frontal Lobes
The frontal lobes are important for attention, executive
function, motivation, and behavior. Tests for frontal lobe
function include working memory (digit span, spelling
backward), judgment, fund of knowledge, task organization
and set generation such as naming lists of things in a certain
category.
Temporal Lobes
The temporal lobes are important for emotional response
(amygdala and its connections to the hypothalamus and
frontal lobes) and memory (hippocampus and limbic
connections). Clinically the main tests for temporal lobe
function are those of memory, particularly declarative
memory.
Language- Temporal and Frontal Lobes
The principle area for receptive language is Wernicke's Area,
which is located in the posterior part of the superior temporal
gyrus of the dominant temporal lobe. The major region for
expressive language is Broca's Area located in posterior part
of the inferior frontal gyrus of the dominant hemisphere.
Homologous regions of the non-dominant hemisphere are
important for the non-verbal contextual and emotional
aspects as well as the prosody (rhythm) of language. Tests for
written and spoken receptive and expressive language are
used to "view" these language centers.
Page 5
Page 5 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Parietal Lobes
The parietal lobes are important for perception and
interpretation of sensory information especially
somatosensory information. The non-dominant parietal lobe
is particularly important for visual-spatial function. The
dominant parietal lobe is important for praxis, which is the
formation of the idea of a complex purposeful motor act while
the frontal lobes are important for the execution of the act.
The Gerstmann Syndrome, which consists of the constellation
of acalculia, finger agnosia, right-left confusion and agraphia,
occurs with damage to the dominant inferior parietal lobe.
Clinical tests for parietal lobe function include tests for
agnosia (such as inability to identify objects by tactile
exploration), apraxia (inability to perform purposeful motor
acts on command), constructional apraxia (inability to draw
objects which require use of visual spatial organization) and
testing for elements of Gerstmann's syndrome.
Occipital Lobes
The occipital lobes are important for perception of visual
information. Areas in the inferior temporal visual association
cortex are important for recognition of color and shape as well
as the recognition of faces. Projections from the occipital lobe
to the superior temporal-parietal area are important for
perceiving motion of objects. Tests that are used to examine
the occipital lobes and its connections include visual fields
(see Cranial Nerve 2), naming of objects, naming of colors and
recognition of faces.
1. ORIENTATION, MEMORY Asking questions about month, date,
day of week and place tests orientation,
which involves not only memory but
also attention and language. Three-
word recall tests recent memory for
which the temporal lobe is important.
Remote memory tasks such as naming
Presidents, tests not only the temporal
lobes but also heteromodal association
cortices.
This patient has difficulty with
orientation questions. The day of the
week is correct but he misses the
month and date. He is oriented to
place. Orientation mistakes are not
localizing but can be due to problems
with memory, language, judgement,
attention or concentration. The patient
has good recent memory (declarative
memory) as evidenced by the recall of
three objects but has difficulty with long
term memory as evidenced by the
difficulty recalling the current and past
presidents.
2. ATTENTION-WORKING
MEMORY
Digit span, spelling backwards and
naming months of the year backward
test attention and working memory
which are frontal lobe functions.
The patient has difficulty with digit span
backwards, spelling backwards and
giving the names of the months in
reverse order. This indicates a problem
with working memory and maintaining
attention, both of which are frontal lobe
functions.
3. JUDGEMENT-ABSTRACT
REASONING
These frontal lobe functions can be
tested by using problem solving, verbal
similarities and proverbs
The patient gives the correct answer for
a house on fire and his answers for
similarities are also good. He has
problems with proverb interpretation.
His answers are concrete and consist of
rephrasing the proverb or giving a
simple consequence of the action in the
proverb. Problems with judgement,
abstract reasoning, and executive
function can be seen in patients with
frontal lobe dysfunction.
4. SET GENERATION This is a test of verbal fluency and the
ability to generate a set of items which
are frontal lobe functions. Most
individuals can give 10 or more words
in a minute.
Set generation tests word fluency and
frontal lobe function. The patient starts
well but abruptly stops after only four
words. Most individuals can give more
then 10 words in one minute.
5. RECEPTIVE LANGUAGE Asking the patient to follow commands
demonstrates that they understand the
meaning of what they have heard or
read. It is important to test reception of
both spoken and written language.
Patients with a receptive aphasia
(Wernicke’s) cannot comprehend
language. Their speech output is fluent
but is devoid of meaning and contains
nonsense syllables or words
(neologisms). Their sentences are
usually lacking nouns and there are
paraphasias (one word substituted for
Page 6
Page 6 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
another). The patient is usually unaware
of their language deficit and prognosis
for recovery is poor.
This patient’s speech is fluent and
some of her sentences even make
sense but she also has nonsense
sentences, made up of words and parts
of words. She can’t name objects
(anomia). She doesn’t have a pure or
complete receptive aphasia but pure
receptive aphasias are rare.
6. EXPRESSIVE LANGUAGE In assessing expressive language it is
important to note fluency and
correctness of content and grammar.
This can be accomplished by tasks that
require spontaneous speech and
writing, naming objects, repetition of
sentences, and reading
comprehension.
This patient with expressive aphasia
has normal comprehension but her
expression of language is impaired. Her
speech output is nonfluent and often
limited to just a few words or phases.
Grammatical words such as
prepositions are left out and her speech
is telegraphic. She has trouble saying
“no ifs , ands or buts”. Her ability to
write is also affected.
Patients with expressive aphasia are
aware of their language deficit and are
often frustrated by it. Recovery can
occur but is often incomplete with their
speech consisting of short phrases or
sentences containing mainly nouns and
verbs.
7. PRAXIS The patient is asked to perform skilled
motor tasks without any nonverbal
prompting. Skills tested for should
involve the face then the limbs. In order
to test for praxis the patient must have
normal comprehension and intact
voluntary movement. Apraxia is typically
seen in lesions of the dominant inferior
parietal lobe.
The patient does well on most of the
tests of praxis. At the very end when he
is asked to show how to cut with
scissors he uses his fingers as the
blades of the scissors instead of acting
like he is holding onto the handles of
the scissors and cutting. This can be an
early finding of inferior parietal lobe
dysfunction.
8. GNOSIS Gnosis is the ability to recognize objects
perceived by the senses especially
somatosensory sensation. Having the
patient (with their eyes closed) identify
objects placed in their hand
(stereognosis) and numbers written on
their hand (graphesthesia) tests
parietal lobe sensory perception.
With his right hand the patient has
more difficulty identifying objects then
with his left hand. One must be careful
in interpreting the results of this test
because of the patient’s motor deficits
but there does seem to be
astereognosis on the right, which would
indicate left parietal lobe dysfunction.
This is confirmed with graphesthesia
where he definitely has more problems
identifying numbers written on the right
hand then the left (agraphesthesia of
the right hand).
9. DOMINANT PARIETAL LOBE
FUNCTION
Tests for dominant inferior parietal lobe
function includes right-left orientation,
naming fingers, and calculations.
This patient has right-left confusion and
difficulty with simple arithmetic. These
are elements of the Gertsmann
syndrome, which is seen in lesions of
the dominant parietal lobe. The full
syndrome consists of right-left
confusion, finger agnosia, agraphia and
acalculia.
Page 7
Page 7 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
10. NON-DOMINANT PARIETAL
LOBE FUNCTION
The non-dominant parietal lobe is
important for visual spatial sensory
tasks such as attending to the
contralateral side of the body and
space as well as constructional tasks
such as drawing a face, clock or
geometric figures.
The patient’s drawing of a clock
demonstrates a problem with
visuospatial construction tasks, which
reflects parietal lobe dysfunction. He
doesn’t neglect the left side of space
but he lists the numbers of the clock in
two columns and then draws a line
between the 8 and the 3 for 8:15.
11. VISUAL RECOGNITION Recognition of colors and faces tests
visual association cortex (inferior
occiptotemporal area). Achromatopsia
(inability to distinguish colors), visual
agnosia (inability to name or point to a
color) and prosopagnosia (inability to
identify a familiar faces) result from
lesions in this area.
Colors are correctly identified but the
patient has difficulty correctly
identifying the face of a president that
he is familiar with. Further testing would
be necessary to make sure this is
prosopagnosia rather then a problem
with attention or long term memory.
B. CRANIAL NERVES
Examination of the cranial nerves allows one to "view" the
brainstem all the way from its rostral to caudal extent. The
brainstem can be divided into three levels, the midbrain, the
pons and the medulla. The cranial nerves for each of these
are: 2 for the midbrain (CN 3 & 4), 4 for the pons (CN 5-8),
and 4 for the medulla (CN 9-12). It is important to remember
that cranial nerves never cross (except for one exception, the
4th CN) and clinical findings are always on the same side as
the cranial nerve involved. Cranial nerve findings when
combined with long tract findings (corticospinal and
somatosensory) are powerful for localizing lesions in the
brainstem.
Cranial Nerve 1
Olfaction is the only sensory modality with direct access to
cerebral cortex without going through the thalamus. The
olfactory tracts project mainly to the uncus of the temporal
lobes.
Cranial Nerve 2
This cranial nerve has important localizing value because of
its "x" axis course from the eye to the occipital cortex. The
pattern of a visual field deficit indicates whether an
anatomical lesion is pre- or postchiasmal, optic tract, optic
radiation or calcarine cortex.
Cranial Nerve 3 and 4
These cranial nerves give us a view of the midbrain. The 3rd
nerve in particular can give important anatomical localization
because it exits the midbrain just medial to the cerebral
peduncle. The 3rd nerve controls eye adduction (medial
rectus), elevation (superior rectus), depression (inferior
rectus), elevation of the eyelid (levator palpebrae superioris),
and parasympathetics for the pupil.
The 4th CN supplies the superior oblique muscle, which is
important to looking down and in (towards the midline).
Pontine Level
Cranial nerves 5, 6, 7, and 8 are located in the pons and give
us a view of this level of the brainstem.
Cranial Nerve 6
This cranial nerve innervates the lateral rectus for eye
abduction. Remember that cranial nerves 3, 4 and 6 must
work in concert for conjugate eye movements; if they don't
then diplopia (double vision) results. The medial longitudinal
fasciculus (MLF) connects the 6th nerve nucleus to the 3rd
nerve nucleus for conjugate movement.
Major Oculomotor Gaze Systems
Eye movements are controlled by 4 major oculomotor gaze
systems, which are tested for on the neurological exam.
They are briefly outlined here:
1. Saccadic (frontal gaze center to PPRF (paramedian
pontine reticular formation) for rapid eye movements
to bring new objects being viewed on to the fovea.
2. Smooth Pursuit (parietal-occipital gaze center via
cerebellar and vestibular pathways) for eye
movements to keep a moving image centered on the
fovea.
3. Vestibulo-ocular (vestibular input) keeps image
steady on fovea during head movements.
4. Vergence (optic pathways to oculomotor nuclei) to
keep image on fovea predominantly when the viewed
object is moved near (near triad- convergence,
accommodation and pupillary constriction).
Cranial Nerve 5
The entry zone for this cranial nerve is at the mid pons with
the motor and main sensory (discriminatory touch) nucleus
located at the same level. The axons for the descending tract
of the 5th nerve (pain and temperature) descend to the level
of the upper cervical spinal cord before they synapse with
neurons of the nucleus of the descending tract of the 5th
nerve. Second order neurons then cross over and ascend to
the VPM of the thalamus.
Cranial Nerve 7
This cranial nerve has a motor component for muscles of
facial expression (and, don't forget, the strapedius muscle
which is important for the acoustic reflex), parasympathetics
for tear and salivary glands, and sensory for taste (anterior
Page 8
Page 8 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
two-thirds of the tongue). Central (upper motor neuron-UMN)
versus Peripheral (lower motor neuron-LMN) 7th nerve
weakness- with a peripheral 7th nerve lesion all of the
muscles ipsilateral to the affected nerve will be weak whereas
with a "central 7th ", only the muscles of the lower half of the
face contralateral to the lesion will be weak because the
portion of the 7th nerve nucleus that supplies the upper face
receives bilateral corticobulbar (UMN) input.
Cranial Nerve 8
This nerve is a sensory nerve with two divisions- acoustic and
vestibular. The acoustic division is tested by checking auditory
acuity and with the Rinne and Weber tests. The vestibular
division of this nerve is important for balance. Clinically it be
tested with the oculocephalic reflex (Doll's eye maneuver) and
oculovestibular reflex (ice water calorics).
Medullary Level
Cranial nerves 9, 10, 11, and 12 are located in the medulla
and have localizing value for lesions in this most caudal part
of the brainstem.
Cranial Nerves 9 and 10
These two nerves are clinically lumped together. Motor wise,
they innervate pharyngeal and laryngeal muscles. Their
sensory component is sensation for the pharynx and taste for
the posterior one-third of the tongue.
Cranial Nerve 11
This nerve is a motor nerve for the sternocleidomastoid and
trapezius muscles. The UMN control for the
sternocleidomastoid (SCM) is an exception to the rule of the
ipsilateral cerebral hemisphere controls the movement of the
contralateral side of the body. Because of the crossing then
recrossing of the corticobulbar tracts at the high cervical level,
the ipsilateral cerebral hemisphere controls the ipsilateral
SCM muscle. This makes sense as far as coordinating head
movement with body movement if you think about it
(remember that the SCM turns the head to the opposite side).
So if I want to work with the left side of my body I would want
to turn my head to the left so the right SCM would be
activated.
Cranial Nerve 12
The last of the cranial nerves, CN 12 supplies motor
innervation for the tongue.
1. CRANIAL NERVE 1- OLFACTION This CN is tested one nostril at a time
by using a nonirritating smell such as
tobacco, orange, vanilla, coffee, etc.
Detection of the smell is more
important than the actual identification.
This patient has difficulty identifying the
smells presented. Loss of smell is
anosmia. The most common cause is a
cold (as in this patient) or nasal
allergies. Other causes include trauma
or a meningioma affecting the olfactory
tracts. Anosmia is also seen in Kallman
syndrome because of agenesis of the
olfactory bulbs.
2. CRANIAL NERVE 2- VISUAL
ACUITY
The first step in assessing the optic
nerve is testing visual acuity. This can
be done with a standard Snellen chart
or with a pocket chart (Rosenbaum).
Have the patient use their glasses if
needed to obtain best-corrected vision.
Have the patient hold the pocket chart
at the focal length that is best for them
which is usually 14 inches. Have them
recite the line with the smallest letters
that they can read and record the
acuity.
This patientâs visual acuity is being
tested with a Rosenbaum chart. First
the left eye is tested, then the right eye.
He is tested with his glasses on so this
represents corrected visual acuity. He
has 20/70 vision in the left eye and
20/40 in the right. His decreased visual
acuity is from optic nerve damage.
3. CRANIAL NERVE 2- VISUAL
FIELDS
There are several different screening
tests that can be used to assess visual
fields at the bedside. First hold up both
hands superiorly and inferiorly and ask
the patient if they can see both hands
and do they look symmetric. Then test
each eye individually using your fingers
in the four quadrants of the visual field
and ask the patient to count fingers
held up or point to the hand when a
finger wiggles using yourself as a
control. A second screening test is to
use a grid card. Have the patient focus
on the dot in the center of the grid then
The patient's visual fields are being
tested with gross confrontation. A right
sided visual field deficit for both eyes is
shown. This is a right hemianopia from
a lesion behind the optic chiasm
involving the left optic tract, radiation or
striate cortex.
Page 9
Page 9 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
ask if any part of the grid is missing or
looks different. A third method is to use
a cotton tip applicator. Testing one eye
at a time ask the patient to say "now" as
soon as they see the applicator come
into their side vision as they focus on
the examiner's nose. All of these tests
are screening tests. Formal perimetry is
the most accurate way of assessing
visual fields
4. CRANIAL NERVE 2-
FUNDOSCOPY
Direct visualization of the optic nerve
head is an important and valuable part
of assessing CN 2. Systematically look
at the optic disc, vessels, retinal
background and fovea.
The first photograph is of a fundus
showing papilledema. The findings of
papilledema include:
1. Loss of venous pulsations
2. Swelling of the optic nerve head so
there is loss of the disc margin
3. Venous engorgement
4. Disc hyperemia
5. Loss of the physiologic cup and
6. Flame shaped hemorrhages.
This photograph shows all the signs
except the hemorrhages and loss of
venous pulsations.
The second photograph shows optic
atrophy, which is pallor of the optic disc
resulting form damage to the optic
nerve from pressure, ischemia, or
demyelination.
5. CRANIAL NERVES 2 & 3-
PUPILLARY LIGHT REFLEX
The afferent or sensory limb of
the pupillary light reflex is CN2 while the
efferent or motor limb is the
parasympathetics of CN3. Shine a
flashlight into each eye noting the direct
as well as the consensual constriction
of the pupils.
The swinging flashlight test is used to
test for arelative afferent pupillary
defect or a Marcus Gunn pupil.
Swinging the flashlight back and forth
between the two eyes identifies if one
pupil has less light perception than the
other. Shine the flashlight at one eye
noting the size of both pupils. Then
swing the flashlight to the other eye. If
both pupils now dilate then that eye has
perceived less light stimulus (a defect
in the sensory or afferent pathway) than
the opposite eye.
The swinging flashlight test is used to
show a relative afferent pupillary defect
or a Marcus Gunn pupil of the left eye.
The left eye has perceived less light
stimulus (a defect in the sensory or
afferent pathway) then the opposite eye
so the pupil dilates with the same light
stimulus that caused constriction when
the normal eye was stimulated.
6. CRANIAL NERVES 3, 4 & 6-
INSPECTION AND OCULAR
ALIGNMENT
Before checking ocular movements it is
important to inspect the eyes. Look for
ptosis. Note the appearance of the eyes
and check for ocular alignment (the
reflection of your light source should fall
on the same location of each eyeball).
This patient with ocular myasthenia
gravis has bilateral ptosis, left greater
than right. There is also ocular
misalignment because of weakness of
the eye muscles especially of the left
eye. Note the reflection of the light
source doesn't fall on the same location
of each eyeball.
Page 10
Page 10 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
7. CRANIAL NERVES 3, 4 & 6-
VERSIONS
Testing extraocular range of motion
with both eyes open and following the
target (conjugate gaze) is
called versions. The patient is asked to
follow a target through the six principle
positions of gaze. Note any
misalignment of the eyes or complaint
of diplopia (double vision).
The first patient shown has incomplete
abduction of her left eye from a 6th
nerve palsy.
The second patient has a left 3rd nerve
palsy resulting in ptosis, dilated pupil,
limited adduction, elevation, and
depression of the left eye.
8. CRANIAL NERVES 3, 4 & 6-
DUCTIONS
If there is any misalignment of the eyes
or diplopia on versions it is important to
then examine each eye with the other
covered (this is called ductions). The
patient should follow an object through
the six principle positions of gaze so
each extraocular muscle's function is
tested.
Each eye is examined with the other
covered (this is called ductions). The
patient is unable to adduct either the
left or the right eye. If you watch closely
you can see nystagmus upon abduction
of each eye. When both eyes are tested
together (testing versions) you can see
the bilateral adduction defect with
nystagmus of the abducting eye. This
isbilateral internuclear
ophthalmoplegia often caused by a
demyelinating lesion effecting the MLF
bilaterally. The adduction defect occurs
because there is disruption of the MLF
(internuclear) connections between the
abducens nucleus and the lower motor
neurons in the oculomotor nucleus that
innervate the medial rectus muscle.
9. SUPRANUCLEAR GAZE
SYSTEMS
The purpose of supranuclear control of
gaze is to insure that the image that is
being looked at is centered or
maintained on the fovea of the retina.
The following maneuvers test the major
systems that control eye movements.
10. SACCADES Saccades are tested by holding up your
two hands about three feet apart and
instructing the patient to look at the
finger that is wiggling without moving
their head. The patient's eyes should be
able to quickly, smoothly and accurately
jump from target to target.
11. SMOOTH PURSUIT To test Smooth Pursuit ask the patient
to keep watching the target without
moving their head. Then move the
target slowly from side to side and up
and down. The eyes should be able to
follow the target smoothly without
lagging behind or jerking to catch up
with the target.
The patient shown has progressive
supranuclear palsy. As part of this
disease there is disruption of fixation by
square wave jerks and impairment of
smooth pursuit movements. Saccadic
eye movements are also impaired.
Although not shown in this video,
vertical saccadic eye movements are
usually the initial deficit in this disorder.
12. OPTOKINETIC NYSTAGMUS Optokinetic Nystagmus is a test of
smooth pursuit with quick resetting
saccades. Use a tape with repeating
shapes on it and ask the patient to look
at each new object as it appears as you
run the tape between your fingers to
the right, left, up, and down. The patient
will have brief pursuit eye movements
in the direction of the tape movement
with quick saccades or jerks in the
This patient has poor optokinetic
nystagmus when the tape is moved to
the right or left. The patient lacks the
input from the parietal-occipital gaze
centers to initiate smooth pursuit
movements therefore her visual
tracking of the objects on the
tape is inconsistent and erratic.
Patients who have a lesion of the
parietal-occipital gaze center will have
Page 11
Page 11 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
opposite direction. The resetting
saccades are easier to observe than the
brief pursuit movement.
absent optokinetic nystagmus when the
tape is moved toward the side of the
lesion.
13. VESTIBULO-OCULAR REFLEX The vestibulo-ocular reflex is obtained
by having the patient visually fixate on
an object straight ahead, then rapidly
turning the patient's head form side to
side and up and down. The eyes should
stay fixed on the object and turn in the
opposite direction of the head
movement.
The vestibulo-ocular reflex should be
present in a comatose patient with
intact brainstem function. This is called
intact "Doll’s eyes" because in the old
fashion dolls the eyes were weighted
with lead so when the head was turned
one way the eyes turned in the opposite
direction. Absent "Doll’s eyes" or
vestibulo-ocular reflex indicates
brainstem dysfunction at the midbrain-
pontine level.
14. VERGENCE Vergence eye movements occur when
the eyes move simultaneously inward
(convergence) or outward (divergence)
in order to maintain the image on the
fovea that is close up or far away. Most
often convergence is tested as part of
the near triad. When a patient is asked
to follow an object that is brought from
a distance to the tip of their nose the
eyes should converge, the pupil will
constrict and the lens will round up
(accommodation).
Light-near dissociation occurs when the
pupils don't react to light but constrict
with convergence as part of the near
reflex. This is what happens in the
Argyll-Robertson pupil (usually seen
with neurosyphilis) where there is a
pretectal lesion affecting the
retinomesencephalic afferents
controlling the light reflex but sparing
the occipitomesencephalic pathways for
the near reflex.
15. CRANIAL NERVE 5- SENSORY Test for both light touch (cotton tip
applicator) and pain (sharp object) in
the 3 sensory divisions (forehead,
cheek, and jaw) of CN 5.
There is a sensory deficit for both light
touch and pain on the left side of the
face for all divisions of the 5th nerve.
Note that the deficit is first recognized
just to the left of the midline and not
exactly at the midline. Patients with
psychogenic sensory loss often identify
the sensory change as beginning right
at the midline.
16. CRANIAL NERVES 5 & 7 -
CORNEAL REFLEX
The ophthalmic division (V1) of the 5th
nerve is the sensory or afferent limb
and a branch of the 7th nerve to the
orbicularis oculi muscle is the motor or
efferent limb of the corneal reflex. The
limbal junction of the cornea is lightly
touched with a strand of cotton. The
patient is asked if they feel the touch as
well as the examiner observing the
reflex blink.
A patient with an absent corneal reflex
either has a CN 5 sensory deficit or a
CN 7 motor deficit. The corneal reflex is
particularly helpful in assessing
brainstem function in the unconscious
patient. An absent corneal reflex in this
setting would indicate brainstem
dysfunction.
17. CRANIAL NERVE 5- MOTOR The motor division of CN 5 supplies the
muscles of mastication (temporalis,
masseters, and pterygoids). Palpate the
temporalis and masseter muscles as
the patient bites down hard. Then have
the patient open their mouth and resist
the examiner's attempt to close the
mouth. If there is weakness of the
pterygoids the jaw will deviate towards
the side of the weakness. The last test
for this nerve is testing for a jaw jerk,
which is a stretch reflex. Have the
patient slightly open their mouth then
place your finger on their chin and
strike your finger with a reflex hammer.
The first patient shown has weakness
of the pterygoids and the jaw deviates
towards the side of the weakness
(without sound).
The second patient shown has a
positive jaw jerk which indicates an
upper motor lesion affecting the 5th
cranial nerve (with sound).
Page 12
Page 12 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Normally there is no movement. If there
is a jaw jerk it is said to be positive and
this indicates an upper motor neuron
lesion.
18. CRANIAL NERVE 7- MOTOR The motor division of CN 7 supplies the
muscles of facial expression. Start from
the top and work down. Have the
patient wrinkle forehead (frontalis
muscle), close eyes tight (orbicularis
oculi) show their teeth (buccinator), and
purse lips or blow a kiss (orbicularis
oris). If there is weakness especially in
a bilateral upper motor neuron
distribution, get the patient to smile by
telling a joke or funny story. With a
pseudobulbar palsy automatic or
emotional facial expression will be more
complete than movements to
command.
The first patient has weakness of all the
muscles of facial expression on the
right side of the face indicating a lesion
of the facial nucleus or the peripheral
7th nerve.
The second patient has weakness of
the lower half of his left face including
the orbicularis oculi muscle but sparing
the forehead. This is consistent with a
central 7th or upper motor neuron
lesion.
19. CRANIAL NERVE 7- SENSORY,
TASTE
Taste is the sensory modality tested for
the sensory division of CN 7. The
examiner can use a cotton tip
applicator dipped in a solution that is
sweet, salty, sour, or bitter. Apply to one
side then the other side of the extended
tongue and have the patient decide on
the taste before they pull their tongue
back in to tell you their answer.
The patient has difficulty correctly
identifying taste on the right side of the
tongue indicating a lesion of the
sensory limb of the 7th nerve.
20. CRANIAL NERVE 8- AUDITORY
ACUITY, WEBER & RINNE TESTS
The cochlear division of CN 8 is tested
by screening for auditory acuity. This
can be done by the examiner lightly
rubbing their fingers by each ear or by
using a ticking watch. Compare right
versus left. Further screening for
conduction versus neurosensory
hearing loss can be accomplished by
using theWeber and Rinne tests. The
Weber test consists of placing a
vibrating tuning fork on the middle of
the head and asking if the patient feels
or hears it best on one side or the
other. The normal patient will say it is
the same in both ears. The patient with
unilateral neurosensory hearing loss
will hear it best in the normal ear while
the patient with a unilateral conductive
hearing loss will hear it best in the
abnormal ear. The Rinne test consists
of comparing bone conduction (placing
the tuning fork on the mastoid process)
versus air conduction (placing the
tuning fork in front of the pinna).
Normally, air conduction is greater than
bone conduction. For neurosensory
hearing loss air conduction is still
greater than bone conduction but for
conduction hearing loss bone
conduction will be greater than air
conduction.
This patient has decreased hearing
acuity of the right ear. The Weber test
lateralizes to the right ear and bone
conduction is greater than air
conduction on the right. He has a
conductive hearing loss.
Page 13
Page 13 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
21. CRANIAL NERVE 8- VESTIBULAR The vestibular division of CN 8 can be
tested for by using the vestibulo-ocular
reflex as already demonstrated or by
using ice water calorics to test
vestibular function. The later test is
usually reserved for patients who have
vertigo or balance problems or in the
comatose patient when one is testing
brainstem function.
Patients with vestibular disease
typically complain of vertigo – the
illusion of a spinning movement.
Nystagmus is the principle finding in
vestibular disease. It is horizontal and
torsional with the slow phase of the
nystagmus toward the abnormal side in
peripheral vestibular nerve disease.
Visual fixation can suppress the
nystagmus. In central causes of vertigo
(located in the brainstem) the
nystagmus can be horizontal, upbeat,
downbeat, or torsional and is not
suppressed by visual fixation.
22. CRANIAL NERVES 9 & 10-
MOTOR
The motor division of CN 9 & 10 is
tested by having the patient say "ah" or
"kah". The palate should rise
symmetrically and there should be little
nasal air escape. With unilateral
weakness the uvula will deviate toward
the normal side because that side of
the palate is pulled up higher. With
bilateral weakness neither side of the
palate will elevate and there will be
marked nasal air escape.
When the patient says "ah" there is
excessive nasal air escape. The palate
elevates more on the left side and the
uvula deviates toward the left side
because the right side is weak. This
patient has a deficit of the right 9th &
10th cranial nerves.
23. CRANIAL NERVES 9 & 10-
SENSORY AND MOTOR: GAG
REFLEX
The gag reflex tests both the sensory
and motor components of CN 9 & 10.
This involuntary reflex is obtained by
touching the back of the pharynx with
the tongue depressor and watching the
elevation of the palate.
Using a tongue blade, the left side of
the patient's palate is touched which
results in a gag reflex with the left side
of the palate elevating more then the
right and the uvula deviating to the left
consistent with a right CN 9 & 10
deficit.
24. CRANIAL NERVE 11- MOTOR CN 11 is tested by asking the patient to
shrug their shoulders (trapezius
muscles) and turn their head
(sternocleidomastoid muscles) against
resistance.
When the patient contracts the muscles
of the neck the left sternocleidomastoid
muscle is easily seen but the right is
absent. Looking at the back of the
patient, the left trapezius muscle is
outlined and present but the right is
atrophic and hard to identify. These
findings indicate a lesion of the right
11th cranial nerve.
25. CRANIAL NERVE 12- MOTOR The 12th CN is tested by having the
patient stick out their tongue and move
it side to side. Further strength testing
can be done by having the patient push
the tongue against a tongue blade.
Inspect the tongue for atrophy and
fasciculations. If there is unilateral
weakness, the protruded tongue will
deviate towards the weak side.
By having the patient say lah-pah-kah,
the examiner is testing the motor
components of CN 12, 7, and 9 & 10.
Notice the atrophy and fasciculation of
the right side of this patient's tongue.
The tongue deviates to the right as well
because of weakness of the right
intrinsic tongue muscles. These findings
are present because of a lesion of the
right 12th cranial nerve.
C. COORDINATION
The principle area of the brain that is examined by the
coordination exam is the cerebellum. The cerebellum is
important for motor learning and timing of motor activity. It
fine-tunes the force of agonist and antagonist muscle activity
simultaneously and sequentially across multiple joints to
produce smooth flowing, goal directed movements.
Cerebellar dysfunction results in decomposition of
movements and under and over shooting of goal directed
Page 14
Page 14 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
movements (dysmetria). Decomposition of movement and
dysmetria are the main elements of ataxia.
Subdivisions
The cerebellum has 3 functional subdivisions, which function
as feedback and feed forward systems.
Vestibulocerebellum
The first is the vestibulocerebellum. This consists of the
connections between the vestibular system and the
flocculonodular lobe. Dysfunction of this system results in
nystagmus, truncal instability (titubation), and truncal ataxia.
Spinocerebellum
The 2nd subdivision is the spinocerebellum. This system
consists of the connections between the cutaneous and
proprioceptive information coming from the spinal cord to the
vermis and paravermis regions with corrective feedback
predominantly to the muscles of truncal stability and gait.
Dysfunction of this system results in gait and truncal ataxia.
Midline Ataxia
Clinically, the ataxic syndromes caused by vestibulocerebellar
and spinocerebellar disease are lumped together and are
called midline or equilibratory (gait) ataxias. The hallmarks of
these midline ataxic syndromes are truncal instability
manifested by titubation (tremor of the trunk in an anterior-
posterior plane at 3-4 Hz) and gait ataxia (wide based,
irregular steps with lateral veering).
Cerebrocerebellum
The 3rd subdivision of the cerebellum is the
cerebrocerebellum. This system consists of connections from
the cerebral cortex (predominantly motor) to the cerebellar
hemispheres then back to the cerebral cortex. This system is
important in motor planning. Dysfunction of the cerebellar
hemispheres results in ataxia of speech (scanning dysarthria)
and ataxia of the extremities (appendicular ataxia). It is
important to remember that ataxia caused by disease of the
cerebellar hemispheres will be ipsilateral to the dysfunctional
hemisphere. The findings of appendicular ataxia are
hypotonia, decomposition of movement, dysmetria, and
difficulty with rapid alternating movements
(dysdiadochokinesia).
EXAM TESTS
The following tests of the neuro exam can be divided
according to which system of the cerebellum is being
examined:
Vestibulocerebellum and Spinocerebellum (Midline):
Station
Walking
Tandem Gait
Cerebrocerebellum (Appendicular):
Rapid Alternating Movements
Finger-to-Nose
Toe-to-Finger
Heel-to-Shin
Rebound and Check Reflex
Speech
1. SPEECH RAPID ALTERNATING
MOVEMENTS
Having the patient say lah-pah-kah can
test rapid alternating movements of the
tongue, lips, and palate.
Impaired speech articulation of
cerebellar origin is characterized by
being slow, indistinct, and scanning
(scanning refers to decomposition of
words into monosyllabic parts and loss
of normal phrasing and intonation).
2. TREMOR Patient's arms are held outstretched
and fingers extended. Watch for
postural or essential tremor.
A cerebellar intention tremor (1st scene
in this movie) arises mainly from limb
girdle muscles and is maximal at the
most demanding phase of the active
movement. This must be distinguished
from a postural tremor (fine distal 8-13
Hz)(2nd scene) or resting tremor
(coarse distal 5-6 Hz pill-rolling type of
tremor)(3rd scene).
3. REBOUND Tap outstretched arms. Patient's arms
should recoil to original position.
Increased range of movement with lack
of normal recoil to original position is
seen in cerebellar disease.
4. CHECK REFLEX Examiner pulls on actively flexed arm
then suddenly releases. The patient
should be able to check or stop the
arm's movement when released.
The patient is unable to stop flexion of
the arm on sudden release so the arm
may strike the chest and doesn't recoil
to the initial position. This is most likely
due to failure of timely triceps
contraction.
5. HAND RAPID ALTERNATING
MOVEMENTS
Finger tapping, wrist rotation and front-
to-back hand patting. Watch for the
rapidity and rhythmical performance of
Movements are slow and irregular with
imprecise timing. Inability to perform
repetitive movements in a rapid
Page 15
Page 15 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
the movements noting any right-left
disparity.
rhythmic fashion is
called dysdiadochokinesia.
6. FINGER-TO-NOSE The patient moves her pointer finger
from her nose to the examiner's finger
as the examiner moves his finger to
new positions and tests accuracy at the
furtherest outreach of the arm.
Under (hypometria) and over
(hypermetria) shooting of a target
(dysmetria) and the decomposition of
movement (the breakdown of the
movement into its parts with impaired
timing and integration of muscle
activity) are seen with appendicular
ataxia.
7. FOOT RAPID ALTERNATING
MOVEMENTS
Patient taps her foot on the examiner's
hand or on the floor.
Movements are slow and irregular with
imprecise timing of agonist and
antagonist muscle action.
8. TOE-TO-FINGER The patient touches her toe to the
examiner's finger repetitively as the
examiner moves his finger to new
positions.
Same as finger-to-nose except for the
lower extremities. For both the upper
and lower extremities, it is important to
always compare right versus left.
9. HEEL-TO-SHIN The patient places her heel on the
opposite knee then runs the heel down
the shin to the ankle and back to the
knee in a smooth coordinated fashion.
The patient with ataxia of the lower
extremity will have difficulty placing the
heel on the knee with a side-to-side
irregular over- and undershooting as
the heel is advanced down the shin.
Dysmetria on heel-to-shin can be seen
in midline ataxia syndromes as well as
cerebellar hemisphere disease so there
is overlap between the two types of
ataxias for this finding.
10. STATION Have the patient stand still. Note the
position of the feet and how steady the
patient is with eyes open. In the
demonstrated exam, the patient is
asked to hop and pat at the same time.
This is a good way to test upper and
lower extremity coordination and
balance simultaneously.
Patient's feet will be placed wider apart
then usual in order to maintain balance
(broad or wide-based station). Midline
ataxias cause instability of station with
eyes opened or closed.
11. NATURAL GAIT The patient should be observed walking
as she normally would.
Wide-based, unsteady, irregular steps
with lateral veering; ataxia is most
prominent when sudden changes are
needed such as turning, standing up or
stopping.
12. TANDEM GAIT The patient is asked to walk heel-to-toe.
Note steadiness. Tandem gait requires
the patient to narrow the station and
maintain balance over a 4-5 inch width.
Patients with midline ataxias have
difficulty with tandem gait.
Patients with ataxia have difficulty
narrowing the station in order to walk
heel to toe. Tandem gait is helpful in
identifying subtle or mild gait ataxia.
D. MOTOR FUNCTION
When one thinks of the motor system it is usually reduced to
the direct corticospinal tract and the lower motor neuron
(LMN). Although these 2 components are main stage players,
it is important to add a few more components to our
oversimplified scheme of the motor system.
Control Circuits
First, we need to add two "control circuits" that influence the
corticospinal tract- the basal ganglia and the cerebellum.
Brainstem Motor Control Centers
There are also the indirect brainstem motor control centers
and their pathways (rubrospinal, vestibulospinal, and
reticulospinal) that tonically activate lower motor neurons,
especially those that innervate axial and antigravity muscles
(those motor neurons that are in the medial part of the ventral
horn).
Upper Motor Neuron Lesion
The corticospinal tract has its main influence on the motor
neurons that innervate the muscles of the distal extremities-
Page 16
Page 16 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
the hand and the foot (motor neurons in the lateral part of the
ventral horn). The corticospinal tract also (and this a key
point) has collaterals that modulate and control the indirect
brainstem motor centers so that we are not a stiff statue
opposing gravity but rather we can move at will and have just
the right amount of supporting tone. So when there is a lesion
of the upper motor neuron (the UMN is the corticospinal tract
and it's collaterals to the brainstem motor nuclei) the clinical
findings are a combination of the loss of direct effect of the
corticospinal tract on the LMN plus the loss of control and
modulation of the indirect brainstem motor control centers.
UMN Lesion Clinical Findings
The clinical findings from a UMN lesion will include loss of
distal extremity strength, dexterity and a Babinski sign (loss
of direct corticospinal effect) plus increased tone,
hyperreflexia, and the clasp-knife phenomenon (from loss of
control of the indirect brainstem centers).
LMN Lesion Clinical Findings
Lesions of the LMN, "the final common pathway", result in loss
of strength, tone and reflexes with the denervated muscle
showing wasting and denervation hypersensitivity-
fasciculations.
UMN Syndrome
The UMN syndrome is a combination of loss of the direct
corticospinal tract effect on the LMN and the loss of
regulation of the indirect brainstem motor control centers.
Decorticate vs. Decerebrate
A UMN lesion above the level of the red nucleus will result in
decorticate posture (thumb tucked under flexed fingers in
fisted position, pronation of forearm, flexion at elbow with the
lower extremity in extension with foot inversion) while a lesion
below the level of the red nucleus but above the level of the
vestibulospinal and reticulospinal nuclei will result in
decerebrate posture (upper extremity in pronation and
extension and the lower extremity in extension). The reason
for this is that the red nucleus output reinforces antigravity
flexion of the upper extremity. When its output is eliminated
then the unregulated reticulospinal and vestibulospinal tracts
reinforce extension tone of both upper and lower extremities.
If there is a lesion in the medulla then all the brainstem motor
nuclei as well as the direct corticospinal tract would be out
and the patient would be flaccid acutely. If the patient were to
survive, tone would return because of interneuronal activity at
the spinal cord level.
Localizing a UMN Lesion
An UMN lesion is on the opposite side of the clinical findings
for a lesion above the decussation of the pyramids (where the
corticospinal tracts cross) whereas it is on the same side as
clinical findings if the lesion is in the spinal cord.
Spinal Cord Lesions
Spinal cord lesions often give UMN signs below the level of
the lesion (from effect on the corticospinal tract) and LMN
signs at the level of the lesion (from effect on the ventral horn
or ventral nerve root). LMN signs are good for locating the
level of a spinal cord lesion.
EXAM TESTS
Clinical testing of the motor system:
Muscle Strength
Tone
Reflexes
Pathological Reflexes
1. UPPER EXTREMITIES –
INSPECTION AND PALPATION
The muscles are inspected for bulk and
fasciculations and, when indicated,
palpated for tenderness, consistency
and contractures.
In this patient there are fasciculations
(spontaneous contraction of a motor
unit) noted in the deltoid muscle as well
as atrophy. There is also atrophy of the
interosseous muscles of the hands.
These findings can be seen in motor
neuron disease such as amyotrophic
lateral sclerosis.
2. TONE – UPPER EXTREMITY Muscle tone is assessed by putting
selected muscle groups through
passive range of motion. The most
commonly used maneuvers for the
upper extremities are flexion and
extension at the elbow and wrist.
There is increased tone in the right
upper extremity that is rate dependent
with the clasp-knife phenomena noted
when the arm is flexed. This is spasticity
from an upper motor neuron lesion.
3. STRENGTH TESTING Muscle strength is tested from the
proximal to the distal part of the
extremity so that all segmental levels
for the extremity are tested (for the
upper extremity that is C5 to T1 – see
table). Muscle power is graded on a
scale of 0-5 (see table).
With an UMN lesion the fine,
fractionated movements of the fingers
and hand are lost. Distal extremity
weakness is greater than proximal
weakness. With greater effort to move
the paretic hand, there is overflow
activation of proximal muscles and
even of the contralateral hand, which
produces mirror or synkinetic
movements.
Page 17
Page 17 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
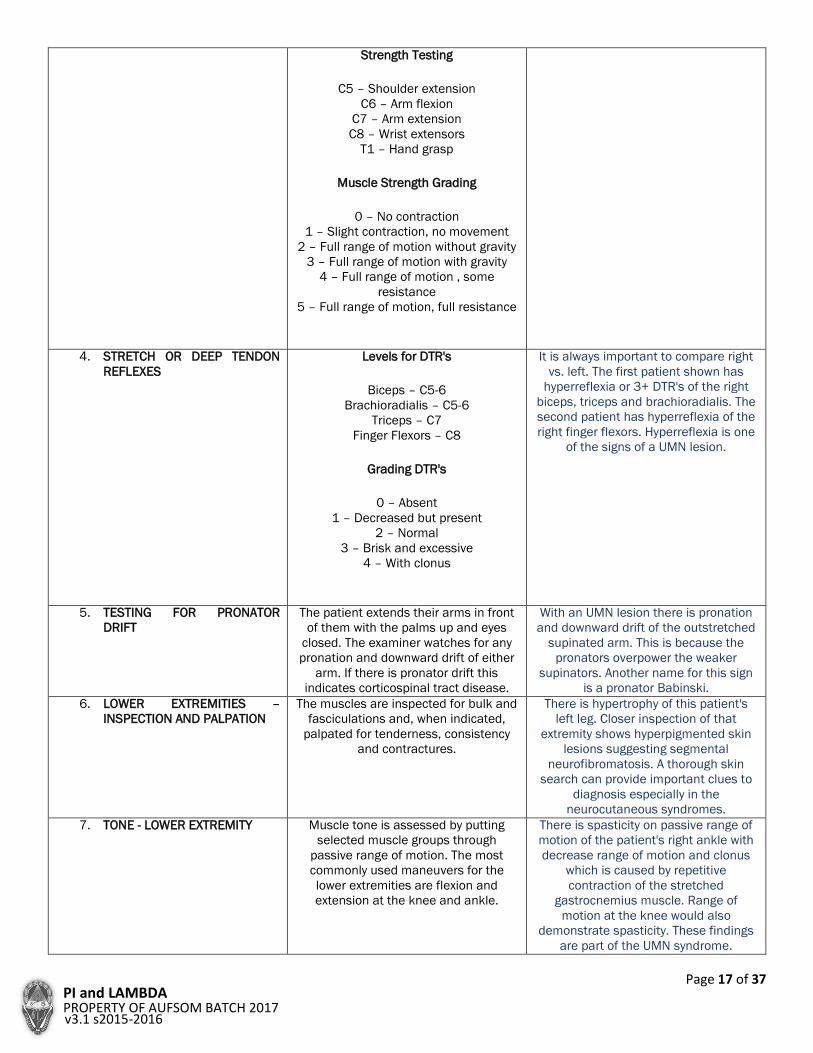
Strength Testing
C5 – Shoulder extension
C6 – Arm flexion
C7 – Arm extension
C8 – Wrist extensors
T1 – Hand grasp
Muscle Strength Grading
0 – No contraction
1 – Slight contraction, no movement
2 – Full range of motion without gravity
3 – Full range of motion with gravity
4 – Full range of motion , some
resistance
5 – Full range of motion, full resistance
4. STRETCH OR DEEP TENDON
REFLEXES
Levels for DTR's
Biceps – C5-6
Brachioradialis – C5-6
Triceps – C7
Finger Flexors – C8
Grading DTR's
0 – Absent
1 – Decreased but present
2 – Normal
3 – Brisk and excessive
4 – With clonus
It is always important to compare right
vs. left. The first patient shown has
hyperreflexia or 3+ DTR's of the right
biceps, triceps and brachioradialis. The
second patient has hyperreflexia of the
right finger flexors. Hyperreflexia is one
of the signs of a UMN lesion.
5. TESTING FOR PRONATOR
DRIFT
The patient extends their arms in front
of them with the palms up and eyes
closed. The examiner watches for any
pronation and downward drift of either
arm. If there is pronator drift this
indicates corticospinal tract disease.
With an UMN lesion there is pronation
and downward drift of the outstretched
supinated arm. This is because the
pronators overpower the weaker
supinators. Another name for this sign
is a pronator Babinski.
6. LOWER EXTREMITIES –
INSPECTION AND PALPATION
The muscles are inspected for bulk and
fasciculations and, when indicated,
palpated for tenderness, consistency
and contractures.
There is hypertrophy of this patient's
left leg. Closer inspection of that
extremity shows hyperpigmented skin
lesions suggesting segmental
neurofibromatosis. A thorough skin
search can provide important clues to
diagnosis especially in the
neurocutaneous syndromes.
7. TONE - LOWER EXTREMITY Muscle tone is assessed by putting
selected muscle groups through
passive range of motion. The most
commonly used maneuvers for the
lower extremities are flexion and
extension at the knee and ankle.
There is spasticity on passive range of
motion of the patient's right ankle with
decrease range of motion and clonus
which is caused by repetitive
contraction of the stretched
gastrocnemius muscle. Range of
motion at the knee would also
demonstrate spasticity. These findings
are part of the UMN syndrome.
Page 18
Page 18 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
8. STRENGTH TESTING Muscle strength is tested from the
proximal to the distal part of the
extremity so that all segmental levels
for the extremity are tested (for the
lower extremity that is L2 to S1 – see
table). Muscle power is graded on a
scale of 0-5 (see table).
Strength Testing
L2 – Hip flexion
L3 – Knee extension
L4 – Knee flexion
L5 – Ankle dorsiflexon
S1 – Ankle plantar flexion
Muscle Strength Grading
0 – No contraction
1 – Slight contraction, no movement
2 – Full range of motion without gravity
3 – Full range of motion with gravity
4 – Full range of motion, some
resistance
5 – Full range of motion, full resistance
Testing of the muscle strength in this
patient shows 1/5 weakness of
dorsiflexion, plantar flexion, inversion
and eversion of the right ankle with
normal proximal strength.
9. STRETCH OR DEEP TENDON
REFLEXES
A brisk tap to the muscle tendon using
a reflex hammer produces a stretch to
the muscle that results in a reflex
contraction of the muscle. The muscles
tested, segmental level, and grading of
DTR's is listed below.
Levels for DTR's
Patellar or Knee – L2-4
Ankle – S1-2
Grading DTR's
0 – Absent
1 – Decreased but present
2 – Normal
3 – Brisk and excessive
4 – With clonus
There is hyperreflexia of the right knee
jerk (3+) with a rightsided crossed
adductor response (the crossed
adductor contraction occurred because
of the increased right leg tone which
resulted in reflex contraction of the
adductor magnus with the very slight
stretch of this muscle caused by
tapping the opposite knee). There is
also hyperreflexia with clonus (4+ DTR)
of the right ankle. The second patient
demonstrates a 4+ ankle jerk on the
left with sustained clonus.
Hyperreflexia is one of the signs of the
UMN syndrome.
10. PLANTAR REFLEX The plantar reflex is a superficial reflex
obtained by stroking the skin on the
lateral edge of the sole of the foot,
starting at the heel advancing to the
ball of the foot then continuing medially
to the base of the great toe. The normal
response is flexion of all the toes. The
abnormal response is called a Babinski
signand consists of extension of the
great toe and fanning of the rest of the
toes.
The patient has a Babinski sign on the
right with an up going great toe and
dorsiflexion and fanning of the other
toes. This is an important indication of
UMN disease.
Page 19
Page 19 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
11. PATHOLOGICAL REFLEXES-
FRONTAL RELEASE SIGNS-
SNOUT, ROOT, PALMOMENTAL
These patterned behavior reflexes
appear when there is damage to the
frontal lobes, which inhibits these
primitive reflexes. In the normal person
these reflexes are absent.
Pressing a tongue blade on the lips
tests for thesnout reflex. The abnormal
response is a pouting of the lips.
The root reflex is tested for by gently
stroking the lateral upper lip. The
abnormal response is movement of the
mouth towards the stimuli.
Stroking the palm of the hand while
watching for contraction of the
ipsilateral mentalis muscle of the lower
lip tests for the palmomental reflex.
These patterned behavior reflexes
appear when there is damage to the
frontal lobes, which normally inhibits
these primitive reflexes.
A snout reflex occurs when a tongue
blade is pressed on the lips and there is
pouting of the lips.
A root reflex occurs when gently
stroking the lateral upper lip causes the
mouth to moves toward the stimuli.
A palmomental reflex occurs when
stroking the palm of the hand causes
the ipsilateral mentalis muscle of the
lower lip to contract.
12. STRENGTH TESTING USING
SQUAT & RISE, HEEL & TOE
The strength of the powerful muscles of
the lower extremities is often best
assessed by using the patient's own
weight. Having the patient squat and
rise tests the pelvic girdle and upper leg
muscles while heel and toe walking
tests the muscles of the foreleg.
This patient has proximal pelvic girdle
weakness which is demonstrated by his
using his hands to climb the wall and
then pushing on his thighs to get his
trunk upright. When a patient uses his
hands to climb up his legs to get to a
standing position is this called a
Gowers' sign.
E. SENSORY FUNCTION
Clinically, there are 2 major somatosensory pathways that are
examined. The first is the spinothalamic (ST) part of the
anterolateral system and the second is the dorsal column-
medial lemniscus (DCML) system. The principle sensory
modalities for the ST system are pain and temperature. The
principle sensory modalities for DCML system are vibratory,
position sense and discriminatory or integrative sensation.
Spinothalamic
The anatomical pathways for the 2 major sensory systems is
as follows:
ST- the axons from the 1st order neuron located in the dorsal
root ganglion enter the dorsal root entry zone and within
several segments synapse with 2nd order neurons in the
dorsal horn. Axons from the 2nd order neuron cross
immediately via the ventral white commissure to the
anterolateral quadrant of the spinal cord then ascend as the
spinothalamic tract to the ventral posterior lateral nucleus
(VPL) of the thalamus. The axons of the 3rd order neurons
project to the postcentral gyrus or somatosensory cortex
(there are also projections to the insular and anterior
cingulate cortex but we are mainly focusing on the primary
somatosensory cortex).
Dorsal Column-Medial Lemniscus
The axons from the 1st order neurons located in the dorsal
root ganglion enter the dorsal root entry zone and then
ascend in the dorsal columns on the same side of the cord
until they reach the 2nd order neurons in the medulla. Axons
from the 2nd order neurons cross at the level of the medulla
and then travel near the midline in the medial lemniscus. By
the time the medial lemniscus reaches the rostral pons it has
moved laterally and at this point it is in close proximity to the
spinothalamic tract as it ascends to the VPL of the thalamus.
The 3rd order neuron projects to the primary somatosensory
cortex in the postcentral gyrus.
Trigeminal System
The trigeminal system is the somatosensory system for the
face, which is clinically tested in the cranial nerve exam. For
the trigeminal system it is important to remember that the
descending tract of the trigeminal nerve, which serves pain
and temperature, descends to the level of the upper cervical
spinal cord and then axons from the 2nd order neurons cross
over to the opposite side and ascend to the ventral posterior
medial (VPM) nucleus of the thalamus.
LEVEL OF CROSSING
The level of crossing of the axons of the 2nd order neurons is
immediate for the ST system and not until the medulla for the
DCML system.
Location of Tracts
The ST tract is lateral in the cord and lower brainstem while
the DCML system is dorsal and medial in the cord and medial
in the lower brainstem. It is not until the rostral pons that the
2 tracts are anatomically close to each other.
Page 20
Page 20 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Trigeminal Crossing
The descending trigeminal tract is ipsilateral to its origin and
axons from the 2nd order neurons cross at the lower medulla-
upper cervical spinal cord level.
FINDINGS
Sensory Dissociation
Spinal cord and lower brainstem lesions can result in sensory
dissociation, which means one sensory system is affected
without the other one.
Crossed Findings
Crossed or alternating findings. For example one side of the
face is affected and the opposite side of the body for
brainstem lesions. In the spinal cord, lesions can cause DCML
system findings on one side of the body and ST findings on
the opposite side.
EXAM TESTS
The ST is examined by testing:
Pain
Temperature
The DCML is examined by testing:
Vibratory sensation
Position sense
Discriminative sensation (must have intact DCML
plus intact parietal cortex):
o Tactile direction
o 2-point discrimination
o Graphesthesia
o Stereognosis
o Double simultaneous Stimulation
1. LIGHT TOUCH Light touch (thigmesthesia) is used as a
screening test for touch. Both the
spinothalamic and DCML systems serve
this sensation so it is not specific for
either one. A cotton tip applicator or
fine hair brush is used. Select areas
from different dermatomes and
peripheral nerves and compare right
versus left.
With light touch the patient indicates
that the perception of the stimulus is
different over the left side of the face.
The feeling has an abnormal quality to
it described as different, uncomfortable
or burning. This would be called
paresthesia or dysesthesia. Light touch
causing pain would be allodynia.
2. PAIN – UPPER EXTREMITIES Pain is one of the principle sensory
modalities of the spinothalamic system.
The sharp end of a broken wooden
cotton tip applicator can be used then
discarded. It is important for the patient
to be able to identify the sensation as
sharp and then compare between
dermatomes, distal versus proximal and
right versus left for the upper
extremities.
A sharp wooden stick is used to
delineate the area of decreased sharp
sensation. There is loss over the ulnar
side of the right hand as well as the
ulnar aspect of the forearm but the arm
is normal. This loss is constant with a
C8-T1 dermatome distribution.
3. PAIN – LOWER EXTREMITIES Pain is one of the principle sensory
modalities of the spinothalamic system.
The sharp end of a broken wooden
cotton tip applicator can be used then
discarded. It is important for the patient
to be able to identify the sensation as
sharp and then compare between
dermatomes, distal versus proximal and
right versus left for the lower
extremities.
This patient has a sensory level at T3
with decreased pain sensation below
the level including the leg. The sensory
level is one to two spinal cord segment
levels below the actual anatomical cord
lesion because the spinothalamic axons
ascend several spinal cord levels prior
to crossing. The left sided T3 sensory
level combined with this patient's upper
extremity sensory finding indicates a
lesion of the right side of the spinal
cord at the C8-T1 level.
4. TEMPERATURE Temperature is the other sensory
modality that is used to test the
spinothalamic system. Tubes or vials of
hot and cold water can be used but this
is usually impractical. Using a tuning
fork, which is normally perceived as
cool or cold to the touch, compare
between dermatomes and right versus
left.
The patient is unable to distinguish the
difference between a hot and cold test
tube simultaneously applied to the
ulnar side of the right hand and arm
and the left leg. This deficit is in the
same distribution as the pain deficit
noted when testing sharp sensation.
Pain and temperature sensation are
tests for spinothalamic tract function.
Page 21
Page 21 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
5. VIBRATORY Vibratory sensation (pallesthesia) is one
of the sensory modalities of the DCML
system. It is tested by using a 128 Hz
tuning fork and placing the vibrating
instrument over a bone or boney
prominence. By varying the force of
vibration and comparing the patient to
yourself you can detect any deficits.
Compare distal versus proximal and
right versus left.
Vibratory sensation is decreased on the
right great toe compared to the left.
This could be due to a peripheral
neuropathy but it also could be
secondary to DCML deficit, which is
actually the case for this patient.
6. POSITION SENSE Position sense (proprioception), another
DCML sensory modality, is tested by
holding the most distal joint of a digit by
its sides and moving it slightly up or
down. First, demonstrate the test with
the patient watching so they
understand what is wanted then
perform the test with their eyes closed.
The patient should be able to detect 1
degree of movement of a finger and 2-3
degrees of movement of a toe. If the
patient can't accurately detect the
distal movement then progressively test
a more proximal joint until they can
identify the movement correctly.
The patient makes more mistakes
identifying the correct direction of toe
movement on the right then left
indicating a proprioceptive loss. For this
patient this is secondary to a lesion
effecting the dorsal column on the right
side of the spinal cord.
7. TACTILE MOVEMENT Tactile movement as well as the
remaining sensory tests are
discriminatory sensory tests that
examine cortical somatosensory
(parietal lobe) function and require an
intact DCML system. Tactile movement
tests the patient's ability to detect the
direction of a 2-3 cm cutaneous
stimulus.
When comparing left vs. right, the
patient has more difficulty on the right
side again indicating dorsal column
dysfunction. If the dorsal column
pathways are intact, then tactile
movement is a sensitive test of parietal
cortical function.
8. TWO-POINT DISCRIMINATION Two-point discrimination is tested by
using calipers or a fashioned paper clip.
The smallest and most dense sensory
units are located in those areas that
have the greatest somatosensory
cortical representation. The patient
should be able to recognize two-point
separation of 2-4 mm on the lips and
finger pads, 8-15 mm on the palms and
3-4 cm on the shins.
Patients with a lesion of the primary
somatosensory cortex will have
difficulty with two-point discrimination
on the opposite side of the body. The
peripheral nerve and DCML pathway
must be intact for this test to be a test
of parietal cortical function.
9. GRAPHESTHESIA Graphesthesia is the ability of the
patient to identify characters that are
written on the skin using a dull pointed
object. The examiner demonstrates the
test by writing single numbers on the
palm of the hand while the patient is
watching. The patient then closes their
eyes and identifies numbers that are
written by the examiner.
This patient has more difficulty
identifying numbers written in the right
hand than in the left hand. This is called
agraphesthesia and is from a lesion of
the somatosensory cortex in the left
parietal lobe.
10. STEREOGNOSIS Stereognosis is the ability to identify
objects that are placed in the hand
when the eyes are closed. The patient is
given common objects and asked to
identify them without looking at them.
The inability to do this
The patient is asked to identify objects
placed in both the right and left hand
with his eyes closed. He knows that
something is in his right hand but he is
unable to identify it while he readily
identifies the same object placed in the
left hand. This is called astereognosis.
Page 22
Page 22 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
calledastereognosis and indicates
parietal lobe dysfunction.
The patient has a lesion involving the
left parietal lobe.
11. DOUBLE SIMULTANEOUS
STIMULATION
The patient should be able to attend to
and identify a tactile stimulus that is
applied to both sides of the body at the
same time. Double simultaneous
stimulation (DSS) is tested by touching
homologous parts of the body on one
side, the other side or both sides at
once with the patient identifying which
side or if both sides are touched with
their eyes closed. If the patient neglects
one side on DSS
(extinction or simultanagnosia) this
indicates dysfunction of the
contralateral posterior parietal lobe.
When the patient is touched on the
right or left he correctly identifies the
side touched but when both sides are
touched simultaneously he neglects the
stimulus on the right. This is extinction
or simultanagnosia and indicates a
lesion in his left parietal cortex.
12. ROMBERG TEST The Romberg test is a test of
proprioception. This test is performed
by asking the patient to stand, feet
together with eyes open, then with eyes
closed. The patient with significant
proprioceptive loss will be able to stand
still with eyes open because vision will
compensate for the loss of position
sense but will sway or fall with their
eyes closed because they are unable to
keep their balance.
With his eyes open, the patient is able
to hold still but when his eyes are
closed he sways and loses his balance.
He has a significant loss of
proprioception.
F. GAIT EXAM
All levels of the neuroaxis contribute to gait although most gait
abnormalities are motor in nature. In assessing gait it is
important to not only watch the lower extremities but also the
upper extremities for normal associated movements.
Localizing Value
There are 7 basic pathological gaits that should be recognized
by their characteristic pattern. These pathological gaits are:
Hemiplegic
Spastic diplegic
Neuropathic
Myopathic
Parkinsonian
Chorea
Ataxic
These gaits have localizing value because they can indicate
levels (an "y" axis as well as an "x" axis) of neurological
disease or systems abnormalities (such as cerebellar or basal
ganglia).
Normal gait is demonstrated in the normal neuro exam
section of this tutorial.
1. STATION The patient should be able to stand still with her feet less then shoulder width apart.
2. NATURAL GAIT The patient should be able to walk with a smooth, coordinated gait. There should be
normal associated movement of the upper extremities.
3. HEEL AND TOE WALKING A good way to test balance as well as strength of the distal lower extremities is to
have the patient heel and toe walk.
4. TANDEM GAIT Have the patient walk heel-to-toe. The patient should be able to balance without
falling or stepping to the side.
ABNORMAL GAITS
HEMIPLEGIC GAIT The patient has unilateral weakness
and spasticity with the upper extremity
held in flexion and the lower extremity
in extension. The foot is in extension so
the leg is "too long" therefore, the
patient will have to circumduct or swing
the leg around to step forward. This
type of gait is seen with a UMN lesion.
This girl has a right hemiparesis. Note
how she holds her right upper extremity
flexed at the elbow and the hand with
the thumb tucked under the closed
fingers (this is "cortical fisting"). There is
circumduction of the right lower
extremity.
DIPLEGIC GAIT The patient has spasticity in the lower
extremities greater than the upper
This man has an UMN lesion affecting
both lower extremities. He has
Page 23
Page 23 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
extremities. The hips and knees are
flexed and adducted with the ankles
extended and internally rotated. When
the patient walks both lower extremities
are circumducted and the upper
extremities are held in a mid or low
guard position. This type of gait is
usually seen with bilateral
periventricular lesions. The legs are
more affected than the arms because
the corticospinal tract axons that are
going to the legs are closest to the
ventricles.
spasticity and weakness of the legs and
uses a walker to steady himself. There
is bilateral circumduction of the lower
extremities.
NEUROPATHIC GAIT This type of gait is most often seen in
peripheral nerve disease where the
distal lower extremity is most affected.
Because the foot dorsiflexors are weak,
the patient has a high stepping gait in
an attempt to avoid dragging the toe on
the ground.
This girl has weakness of the distal right
lower extremity so she can't dorsiflex
her foot. In order to walk she has to lift
her right leg higher then the left to clear
the foot and avoid dragging her toes on
the ground.
MYOPATHIC GAIT With muscular diseases, the proximal
pelvic girdle muscles are usually the
most weak. Because of this the patient
will not be able to stabilize the pelvis as
they lift their leg to step forward, so the
pelvis will tilt toward the non-weight
bearing leg which results in a waddle
type of gait.
This young boy has pelvic girdle
weakness, which produces a waddling
type of gait. Note the lumbar
hyperlordosis with the shoulders thrust
backwards and the abdomen being
protuberant. This posture places the
center of gravity behind the hips so the
patient doesn't fall forward because of
weak back and hip extensors.
PARKINSONIAN GAIT This type of gait is seen with rigidity and
hypokinesia from basal ganglia disease.
The patient's posture is stooped
forward. Gait initiation is slow and steps
are small and shuffling; turning is en
bloc like a statue.
This man's gait is bradykinetic and his
steps are smaller then usual. There is
also the pill-rolling tremor in his hands.
He turns en bloc and there is decreased
facial expression.
CHOREIFORM GAIT This is a hyperkinetic gait seen with
certain types of basal ganglia disorders.
There is intrusion of irregular, jerky,
involuntary movements in both the
upper and lower extremities.
Note the involuntary, irregular, jerky
movements of this woman's body and
extremities, especially on the right side.
There are also choreiform movements
of the face. A lot of her movements
have a writhing, snake-like quality to
them, which could be called
choreoathetoisis.
ATAXIC GAIT The patient's gait is wide-based with
truncal instability and irregular lurching
steps which results in lateral veering
and if severe, falling. This type of gait is
seen in midline cerebellar disease. It
can also be seen with severe lose of
proprioception (sensory ataxia).
This woman's gait is wide-based and
unsteady. She has to use a walker or
hold on to someone in order to
maintain her balance (note how hard
she has to work with the hand that
she's holding on with in order to
maintain her balance). Her ataxia is
even more apparent when she tries to
turn.
Reference: University of Utah. (2015). Neurologic Examination
http://library.med.utah.edu/neurologicexam/html/home_exam.html
Page 24
Page 24 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
PEDIATRIC NEUROLOGIC EXAMINATION
DEVELOPMENTAL ANATOMY
Major Events in Brain Development
Brain and spinal cord development begins with formation of
the neural tube closure, which is completed by 28 days of
gestation. Prosencephalization then occurs to form the
cerebral hemispheres and diencephalon. At 2 to 4 months
gestation, there is neuronal proliferation followed by
migration at 3 to 5 months. Formation of the gyri begins with
the major fissures being formed in the 5th month, the
secondary sulci by 7 months, and the tertiary sulci by 9
months gestation. Finally, neuronal organization and
myelination starts in the 3rd trimester and continues on well
after birth. Organization and myelination are the major
processes that account for brain growth and maturation.
Brain Growth
The newborn brain weighs 400 grams. At one year of age the
brain weighs 1,000 grams. By 2 years of age the brain has
reached 80 percent of its adult size. By 18 years of age the
brain has reached its adult weight of 1400 grams.
Neuronal Growth and Organization
By 36 weeks gestation, the process of neuronal proliferation
is nearly complete. Although there is some limited
proliferation of neurons throughout life, their contribution to
brain growth is negligible. Growth of the individual neurons
plus the elaboration and proliferation of dendritic and axonal
processes and connections is responsible for most of the
brain’s growth.
The diameter of a neuroblast is 5 microns while a mature
neuron can measure 50 microns, a 1,000-fold increase in cell
volume. Increase in the size of glial cells also occurs. During
the organization process of brain development there is
increasing dendritic arborization, synaptogenesis, and axonal
connections, which make a significant contribution to brain
growth as well as the maturation and development of brain
function.
Myelination and Development
The next developmental process that greatly contributes to
brain growth and maturation is myelination. Myelination
begins early in the 3rd trimester with the most rapid period of
myelination occurring in the first two years of life. The
myelination process follows a specific time course and
pattern. The acquisition of neurodevelopmental milestones
parallels and reflects this pattern. Myelination occurs early for
motor-sensory roots, special senses and the brainstem; those
structures necessary for reflex behavior and survival.
The corticospinal tract starts to myelinate at 36 weeks
gestation and myelination is completed by the end of the 2nd
year of life. Myelination of the corticospinal tract begins at the
proximal portion of the axon and the shortest axons are the
first to myelinate. The axons for the upper extremities and the
trunk myelinate next. The axons for the lower extremities,
which are the longest axons, are the last to myelinate with the
process being completed by 24 months of age. This
myelination pattern correlates with the progressive head-to-
toe acquisition of developmental milestones.
The motor patterns of the immature brain are predominately
under brainstem control and lack cortical modulation until
there is the necessary maturation of these higher brain center
connections.
Cerebral Hemisphere Myelination
The areas of the cerebral hemispheres that are first to
myelinate are the posterior portion of the frontal lobes, the
parietal lobes and areas of the occipital lobes. The frontal
and temporal lobes then myelinate and by the end of the
second year, myelination of the cerebrum is largely
completed, although there are interconnections of the
association cortex that are still being myelinated into the
2nd and 3rd decades of life.
NEWBORN
Behavior
This 5-day-old infant is in the alert, quiet state. He has spontaneous movements, which have a
smooth flowing quality to them and are not excessive, jerky or asymmetric. He seems to be
attentive to the environment. He makes attempts to organize and comfort himself by sucking on
his fists, which is a favorable behavioral response. When a bright light is directed towards his
eyes he has a definite response, which consists of blinking and avoiding the light. With repeated
stimulus there is habituation, a diminished response to the stimulus. He responds to sound by
quieting and even turning is head and eyes toward the sound. The above observations are the
baby equivalent to the adult mental status exam.
Cranial Nerves
Examination of the baby’s cranial nerve function is often accomplished by observing
spontaneous activity. During crying, facial movement (Cranial Nerve 7) is observed for fullness or
asymmetry. The quality and strength of the cry is a way of looking at Cranial Nerves 9 and 10
function. Sucking and swallowing assesses Cranial Nerves 5, 7, 9, 10, and 12 because all of
these cranial nerves are involved in this complex act. Eye movements (Cranial Nerves 3, 4 and 6)
can be assessed by using the vestibulo-ocular reflex (doll’s eyes maneuver). When the head is
turned, there is conjugate eye movement in the opposite direction. Testing a baby’s behavior
response to light (Cranial Nerve 2) and sound (Cranial Nerve 8) also adds to the cranial nerve
Page 25
Page 25 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
exam. Pupillary light reflex, corneal reflex, gag reflex and funduscopic exam are done in the same
manner as the adult exam.
Tone - Resting Posture
For a term newborn the resting posture is flexion of the extremities with the extremities closely
adducted to the trunk. After the first few days of life, the extremities are still predominantly in the
flexed position but they are not as tightly adducted as they are in the first 48 hours of life.
Tone - Upper Extremity Tone
Assessing motor function of the upper extremities begins with passive range of motion. This is
done by rotating each extremity at the shoulder, elbow and wrist and feeling the resistance and
the range of movement. Too little or too much resistance reflects hypotonia or hypertonia.
Further testing helps to better define tone and any tone abnormalities.
Tone - Arm Traction
Arm traction is done with the baby in the supine position. The wrist is grasped and the arm is
pulled until the shoulder is slightly off the mat. There should be some flexion maintained at the
elbow. Full extension at the elbow is seen in hypotonia.
Tone - Arm Recoil
Arm recoil tests tone and action of the biceps. The arms are held in flexion against the chest for
a few seconds, then are quickly extended and released. The arms should spring back to the
flexed position. The hyotonic infant will have slow incomplete recoil. Asymmetry to this response
with lack of recoil would be seen with Erb’s or brachial plexus palsy.
Tone - Scarf Sign
The tone of the shoulder girdle is assessed by taking the baby’s hand and pulling the hand to the
opposite shoulder like a scarf. The hand should not go past the shoulder and the elbow should
not cross the midline of the chest.
Tone - Hand Position
A newborn baby’s hand is held in a fisted position with the fingers flexed over the thumb. The
hand should open intermittently and should not always be held in a tight fisted position. Rubbing
the ulnar aspect of the hand or touching the dorsum of the hand will often cause extension of
the fingers. Over the first 1 to 2 months of life, the baby’s hand becomes more open. Persistence
of a fisted hand is a sign of an upper motor neuron lesion in an infant.
Tone - Lower Extremity Tone
Assessing motor function of the lower extremities begins with passive range of motion. This is
done by flexing the hips, then abducting and adducting the hips. Next, flex and extend the hips,
the knees and ankles. Further testing helps to better define the tone and any tone abnormalities.
Tone - Leg Traction
Leg traction is done by holding the leg by the ankle. The leg is pulled upward until the buttock
starts to be lifted off the mat. The knee should maintain a flexed angle. Full extension of the
knee with little resistance to pulling on the leg is a sign of hypotonia.
Tone - Leg Recoil
To test leg recoil, the legs are fully flexed on the abdomen for a few seconds, then the legs are
quickly extended and released. The legs should spring back to the flexed position. Legs that
remain extended could be due to either hypotonia or abnormal extensor tone.
Page 26
Page 26 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Tone - Popliteal Angle
The popliteal angle is an assessment of the tone of the hamstring muscles. It is done one leg at
a time. The thigh is flexed on the abdomen with one hand and then the other hand straightens
the leg by pushing on the back of the ankle until there is firm resistance to the movement. The
angle between the thigh and the leg is typically about 90 degrees. Extension of the leg beyond
90 to 120 degrees would be seen in hypotonia.
Tone - Heel to Ear
Holding the baby’s foot in one hand, draw the leg towards the ear to see how much resistance
there is to the maneuver. The foot should go to about the level of the chest or shoulder, but not
all the way to the ear. If the foot can be drawn to the ear then there is hypotonia.
Tone - Neck Tone
The tone of the neck can be assessed by passively rotating the head towards the shoulder. The
chin should be able to rotate to the shoulder but not beyond the shoulder. If the chin goes
beyond the shoulder then there is hypotonia of the neck muscles, which is associated with poor
head control.
Tone - Head Lag
Starting in the supine position, the baby is pulled by the arms to the sitting position. The head
and the arms are observed during the maneuver. The arms should remain partially flexed at the
elbow and the head may lag behind the trunk, but should not be fully flexed backwards. When
the baby is in the sitting position, the head should be able to come to the upright position for at
least a few seconds before dropping forward or backward.
Tone - Head Control
The strength and tone of the neck extensors can be tested by having the baby in sitting position
and neck flexed so the baby’s chin is on the chest. The baby should be able to bring the head to
the upright position. The neck flexors can be tested by having the head in extension while in the
sitting position. The baby should be able to bring the head to the upright position. These tests are
an extension of the test for head lag and are done at the same time.
Positions - Prone
In the prone position, the baby should be able to extend the neck to the point where the head
can be turned side to side. When the arms are extended by the side of the trunk, the baby should
be able to bring them forward into a flexed position. The buttock should be somewhat elevated
because the hips are flexed and adducted. A baby that is flat on the mat and can’t turn the head
back and forth has low tone and weakness.
Positions - Ventral Suspension
The baby is placed in the prone position, suspended in the air by the hand placed under the
chest. The baby’s head position, back and extremities are observed. The head should stay in the
same plane as the back. The back should show some resistance to gravity and not be simply
draped over the hand on the chest. The extremities should maintain some flexion tone and not
dangle in extension. Ventral suspension is a very good way to assess a baby’s neck and trunk
tone.
Positions - Vertical Suspension
The examiner holds the baby in the upright position with feet off the ground by placing the hands
under the arms and around the chest. The baby should be suspended in this position without
slipping through the hands of the examiner. If there is shoulder girdle weakness the arms will
extend upwards and the examiner will have to reposition their grasp of the baby to avoid the
baby slipping through their hands. It feels like trying to hold on to a slippery fish.
Reflexes - Deep Tendon Reflexes
Testing deep tendon reflexes is an important part of the newborn neurological exam. They can be
technically difficult to do. The first thing is to use a reflex hammer, not a finger or a stethoscope.
Ideally, the baby is in a quiet alert state with the head in the midline. The head turned to one side
can reinforce the tone and reflexes on that side. I usually start with the knee jerk because is the
easiest to obtain. Take control of the leg with the hand under the knee and the leg at about a 90
Page 27
Page 27 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
degree angle at the knee. Then strike the patellar tendon with the reflex hammer using a
pendular action rather a chopping action.
Reposition the leg and try several times if you have trouble getting a knee jerk. Next, I go to the
ankle jerk. If I can’t get an ankle jerk in the conventional fashion, I place my fingertips on the
plantar aspect of the foot, flex the foot slightly, then strike the back of my fingers. For the bicep
jerk, have the arm flexed at the elbow, thumb over the bicep tendon, then strike the thumb with
a pendular action. Because of the predominantly flexor tone of the newborn, it is rare to obtain a
triceps jerk.
Absence of deep tendon reflexes is a much more important finding than hyperreflexia in the
newborn. A normal newborn can have hyperreflexia and still be normal, if the tone is normal, but
absent reflexes associated with low tone and weakness is consistent with a lower motor neuron
disorder. Preserved or exaggerated reflexes associated with low tone is the hallmark of what is
called central or cerebral hypotonia and the cause is an upper motor neuron lesion.
Reflexes - Plantar Reflex
The normal response to stroking the lateral aspect of the plantar surface of the foot is extension
of the great toe and fanning of the other toes. If the stimulus is brought across the ball of the
foot then a grasp reflex will be elicited and the toes will plantar flex. The up going toes or
“Babinski sign” is normal in the infant and may be present for the first year of life because of the
incomplete myelination of the corticospinal tracts.
Primitive Reflexes - Suck, Root
The baby should have a strong coordinated suck reflex with good stripping action of the tongue.
There should be resistance to pulling out the pacifier. A root reflex is obtained by gently stroking
the cheek towards the lips. The baby should open the mouth towards the stimulus and turn the
head to latch on to the object.
Primitive Reflexes - Moro
The Moro reflex is obtained by holding the baby’s head and shoulders off of the mat with the
arms held in flexion on the chest. The examiner suddenly lets the head and shoulders drop back
a few inches while releasing the arms. The arms should fully abduct and extend, then return
towards the midline with the hand open and the thumb and the index finger forming a “C” shape.
An absent or incomplete Moro is seen in upper motor neuron lesions. An asymmetric Moro is
most often seen with a brachial plexus lesion. The brachial plexus palsy is on the side of the
poorly abducted arm.
Primitive Reflexes - Galant
The Galant reflex (trunk incurvation) is obtained by placing the baby in ventral suspension, then
stroking the skin on one side of the back. The baby’s trunk and hips should swing towards the
side of the stimulus.
Primitive Reflexes - Stepping
The stepping or walking reflex is obtained by holding the baby upright over the mat with the sole
of the foot touching the mat. This initiates a reciprocal flexion and extension of the legs and it
looks like the baby is walking.
Primitive Reflexes - Grasp
Placement of the examiner’s finger in the palm of the hand or on the sole of the foot will cause
flexion and grasping of the fingers or toes. One should avoid touching the dorsum of the hand
while eliciting the grasp reflex because stimulating the back of the hand causes a hand opening
reflex to occur. With the two competing reflexes, the grasp response will be incomplete or
inconsistent. You can actually see this happen with the baby that is being examined. The grasp
reflex can be reinforced by applying traction on the arm.
Page 28
Page 28 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Head Shape and Sutures
The head should be closely inspected as part of the neurological examination. There can be
molding of the head, which is an expected finding in a newborn. Palpate the sutures and outline
the anterior and posterior fontanelles.
Head Circumference
It is very important to measure the head circumference, which sometimes is referred to as the
OFC (occipital-frontal circumference) because the measurement is obtained by placing the
measuring tape around the most prominent aspect of the frontal and occipital bones. The most
accurate measurements are obtained with a plastic tape measure rather than a paper tape
measure because the paper can stretch. The head circumference measurement should be
plotted on a standardized head growth chart for the appropriate sex.
3 MONTH OLD
Behavior
This baby is almost 3 months old. He is alert and attentive to the environment and the examiner.
He visually tracks. He has a social smile and is able to frown. There is definite social awareness
and interaction.
Cranial Nerves
The vestibulo-ocular reflex evokes a full range of conjugate eye movements. The baby should
also be able to visually track 180 degrees in the horizontal plane. Facial expression is full and
symmetric.
Motor - Upper Extremity Tone
In the newborn, flexor tone is predominate. After the first few weeks, the flexor tone is less.
Passive range of motion is still met with resistance but with the appropriate amount. The hand
pulled across the body to the opposite shoulder still does not extend beyond the shoulder.
Motor - Hand Movements
The hand is now held in a more open position. The infant will hold on to an object when placed in
his hand but will not yet reach for the object. At this age, the infant may start to bat at objects.
He also watches his hands.
Motor - Lower Extremity Tone
Tone in the lower extremities is present with the appropriate resistance to passive range of
motion. The tight flexor tone of the newborn is no longer present.
Motor - Head and Trunk Control
When pulled to a sitting position, a baby this age should be able to have only slight head lag and,
when sitting, the head should be upright but there may still be some wobbling of the head. The
back is still rounded, so the baby slumps forward.
Positions - Supine
In the supine position, the baby’s extremities are held off the mat and there is spontaneous
movement of all extremities. During the first 3 months of life, babies will often lie with their head
turned to one side or the other. This may be associated with extension of the arm that the head
is turned towards. This is part of the asymmetric tonic neck reflex, which is most prominent
during this time but diminishes by 3 to 4 months of age and is gone by 6 months of age.
Page 29
Page 29 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Positions - Prone
In the prone position, the baby is now able to bring his head up and look forward with the head
being 45 to 90 degrees off the mat. Weight is borne on the forearms. When the head and chest
are well off the mat, the baby is ready to start to roll from the prone to the supine position.
Rolling front to back usually occurs at 3 to 5 months of age. Rolling over too early can be due to
excessive extensor tone.
Positions - Ventral Suspension
In ventral suspension, the baby’s posture is very similar to the prone position. The trunk and legs
are in the same plane and the back is kept straight. The head is above the body looking forward.
The baby is able to maintain a forward-looking position.
Positions - Vertical Suspension
In vertical suspension with the feet touching the mat, the baby should start to support some
weight with his legs. Bearing weight on the legs is the earliest postural reflex to appear and
usually is present at 3 to 4 months of age. The baby’s shoulder girdle is strong and there is no
slipping through the examiner’s hands.
Reflexes - Deep Tendon Reflexes
One of the main obstacles to obtaining deep tendon reflexes at this age is catching the extremity
at rest. Positioning the extremity is also important. As demonstrated in this baby, a crossed
adductor can be seen at this age and still be normal but should not persist beyond 7 months of
age. A few beats of ankle clonus can be normal in the first few weeks of life but sustained ankle
clonus at any age is abnormal.
Reflexes - Plantar Reflex
Stroking the lateral aspect of the plantar surface of the foot still elicits a strong “Babinski sign”
which is an up-going great toe and fanning of the other toes.
Primitive Reflexes - Root
The baby still has a root reflex and turns the mouth towards the stimulus. The rooting reflex
disappears at about 4 months of age.
Primitive Reflexes - Moro
The baby no longer has a Moro reflex. Usually the Moro reflex is absent by 4 to 5 months of age.
Persistence of the Moro reflex beyond this time can be seen with upper motor neuron disorders.
Primitive Reflexes - Galant
The Galant reflex is still present but should diminish and be gone by 4 months of age.
Primitive Reflexes - Grasp
The palmer grasp reflex is still present for this baby. The grasp reflex is usually gone by 4 to 6
months of age for the hands and 6 to 12 months for the toes. The reflex palmer grasp is
gradually replaced by the voluntary activity of reaching and grasping with the hand.
Page 30
Page 30 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Primitive Reflexes - Asymmetric Tonic Neck
The asymmetric tonic neck reflex is present in the first 3 to 4 months of life. When the head is
turned to one side, the ipsilateral arm and leg will extend while the contralateral extremities will
be in flexion. The baby should be able to overcome this reflex and move out of this posture. If the
asymmetric reflex is obligate (the infant can not move out of or overcome the reflex) or if the
reflex persists beyond 6 months of age, then it is abnormal and can be seen in upper motor
neuron disorders.
6 MONTH OLD
Behavior
The baby is sitting comfortably in his mother’s lap. He is socially aware, inquisitive and readily
responds to visual objects and sounds. He smiles, laughs, and jabbers. At this age a baby will
start to make repetitive speech sounds that are nonspecific such as da, ma, or ba.
Cranial Nerves
The baby is able to visually track an object throughout the horizontal and vertical planes. An
interesting or colorful object is most helpful. To test visual fields, have the baby focus on an
object in front of him and then bring a second object from behind him until he sees the object in
his peripheral vision. He should turn toward the new object. Saccadic eye movements are tested
by using interesting toys and sounds and watching the eyes jump from object to object. To test
hearing, produce a sound out of the baby’s sight and then watch the baby turn and localize the
sound. Facial movements are noted as the baby smiles or cries.
Motor - Sitting
Independent sitting is accomplished by 6 to 8 months. This baby has good sitting posture (head
erect and spine straight) and has enough stability to reach for objects with both hands. He even
stretches to obtain an object without loosing his balance.
Motor - Hand
The baby is able to reach out and pick up an object and bring it to the midline, usually to his
mouth. He reaches equally well with either hand. Hand preference before one year of age is
always abnormal and indicates a motor deficit in the non-preferred hand.
At this age, the baby is able to transfer an object from hand to hand. By 5 to 6 months, a baby
grasps objects that are the size of a cube. An ulnar or palmer grasp is a raking motion with the
fingers trapping the object against the palm.
The next stage of hand development is to use the thumb in concert with the fingers to grasp an
object. This is called a whole hand grasp. The baby is starting to use the thumb so has developed
a whole hand grasp. A thumb-finger pincer grasp develops at 7 to 9 months.
Motor - Tone
Tone is assessed for the upper and lower extremities by passive range of motion when the baby
is cooperative. Distraction is a great way to get that cooperation. Babies at this age have found
their feet and can suck on their toes. On passive range of motion, the lower extremity should be
flexible enough to bring the foot to the baby’s mouth. There shouldn’t be any ankle clonus.
Motor - Traction
On traction, which is pulling to a sitting position, the baby has good head and trunk control. The
head and shoulders are flexed forward and the arms are flexed. The baby actively helps himself
to get to the sitting position by pulling with the arms. Also notice that the legs are flexed at the
hips and are off the mat as the baby pulls himself to sitting. On being laid back down to the
supine position, the baby doesn’t flop back, but is able to control the lowering of his head and
trunk to the mat.
Page 31
Page 31 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Position - Prone
In the prone position, the baby brings his chest all the way off the mat and supports his weight
on his hands, not his forearms. He works for toys out of his reach. He is close to crawling. He can
roll over from front to back and back to front.
Reflexes - Deep Tendon Reflexes
It is hard to get the baby relaxed and cooperative enough to get the limb in the optimal position
for obtaining deep tendon reflexes. At this age, all the deep tendon reflexes tested in an adult
exam should be obtainable.
Reflexes - Plantar Reflex
There is still a lot of plantar grasp at this age as well as withdrawal, which makes testing for the
plantar response difficult at this age. The toes are still up going until one year of age. The most
useful finding at this age is if there is asymmetry in the toe findings.
Primitive Reflexes
At six months of age this baby has lost the Moro reflex and the asymmetric tonic neck reflex.
Persistence of either one of these primitive reflexes would be abnormal.
Postural Reflexes - Positive Support Reflex
Some consider the positive support reflex as a primitive reflex, but others consider it a postural
reflex. I think it is a postural reflex because it is necessary for erect posture and blends into
volitional standing. Infants with prenatal or perinatal corticospinal tract disease will often refuse
to support their weight on their feet.
The positive support reflex is the first postural reflex to develop and is present by 3 to 4 months
of age. When the baby is placed in vertical suspension with the feet touching the mat, the baby
will extend the legs and attempts to support his weight while being balanced by the examiner. By
5 to 6 months of age the baby fully supports his weight while standing and by 7 months enjoys
bouncing.
Postural Reflexes - Landau
The Landau is an important postural reflex and should develop by 4 to 5 months of age. When
the infant is suspended by the examiner’s hand in the prone position, the head will extend above
the plane of the trunk. The trunk is straight and the legs are extended so the baby is opposing
gravity. When the examiner pushes the head into flexion, the legs drop into flexion. When the
head is released, the head and legs will return to the extended position. The development of
postural reflexes is essential for independent sitting and walking.
Postural Reflexes - Lateral Propping
Lateral propping or protective extension is essential for the baby to be able to sit independently.
This postural reflex develops at 5 to 7 months of age. Anterior propping actually develops first,
then lateral propping. For anterior propping the baby will extend the arms forward to catch
himself and prevent falling forward. Lateral propping occurs when the baby is falling to one side
or the other and he extends the arm laterally to catch himself. Asymmetric lateral propping can
be an early sign of hemiparesis. The baby will prop on one side but on the paretic side he will not
extend the arm to catch himself.
Postural Reflexes - Parachute
The parachute reflex is the last of the postural reflexes to develop. It usually appears at 8 to 9
months of age. When the baby is turned face down towards the mat, the arms will extend as if
the baby is trying to catch himself. Prior to developing this reflex, the baby will actually bring the
arms back to the plane of the body and away from the mat.
Page 32
Page 32 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Head Examination
The head circumference should be measured and plotted. This is usually done at the end of the
exam because babies usually resent the restriction of head movement necessary to obtain an
accurate measurement. Head shape should be noted and the sutures palpated.
Craniosynostosis (premature closure of the suture) can cause a misshaped head. Bone growth
occurs perpendicular to the suture. If one suture is closed, compensatory growth will occur in the
remaining open sutures. Synostosis of the sagittal suture (the most common type of synostosis)
results in scaphocephaly (a thin elongated head). Synostosis of the coronal sutures results in
brachycephaly (a wide flat head). Synostosis of the metopic suture results in trigonocephaly (a
triangular shaped head).
The most common cause of a misshapen head is flattening of the occipit on one side and is not
from lambdoid synostosis but is positional in nature (caused from the baby lying supine with the
head turned to one side as a preferred position).
It is important not only to palpate the sutures but also the fontanelles. The posterior fontanelle
cannot be palpated after six weeks. The anterior fontanelle is often small by six months. Closure
of the anterior fontanelle occurs between 10 and 20 months. The anterior fontanelle should be
palpated while the child is sitting and quiet and it should be flat or slightly concave. A full, slightly
bulging fontanelle can be seen with a child that is supine or crying.
12 MONTH OLD
Behavior - Shy
Infants at 12 months of age are often shy and have stranger anxiety. Most of the neurological
exam can be performed with the child on his parent’s lap. The parent helps reassure the child
and facilitates the exam. This infant is shy and frequently looks to his father for reassurance. The
examiner uses toys to try to engage the child in play and overcome the shyness.
Behavior - Social and Language
Infants this age imitate activities, wave bye-bye, and play pat-a-cake. They can follow simple
instructions especially if the desired action is demonstrated. They feed themselves finger foods.
They usually have one or two meaningful words, usually mama and dada.
Cranial Nerves
A colorful finger puppet is used to attract the infant’s attention and test extra ocular range of
movement. For testing visual fields, a finger puppet is again used to get the infant to visually
fixate, and then a dangling measuring tape is used to test peripheral vision.
Motor - Tone
Passive range of motion for both the upper and lower extremities is tested. Transforming the
movements into a game makes the exam less threatening to the infant.
Motor/Reflexes - Deep Tendon Reflexes
A reflex hammer can be a threatening object to the infant. By turning the reflex hammer into an
imaginary horse and adding sound effects, the infant is not threatened and cooperates for the
exam. Because using a reflex hammer can be a threat to the child, deep tendon reflexes are
usually done late in the exam and when the child is on the parent’s lap.
Page 33
Page 33 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Motor/Reflexes - Plantar Reflex
At 12 months of age the toes can go up or down. Generally, they are down going. In this age
group it’s hard not to get withdrawal of the foot. An abnormality of the plantar reflex is most
diagnostic if there is reproducible asymmetry.
Motor/Postural Reflexes - Parachute
The parachute is the last of the postural reflexes to develop. It usually appears at 8 to 9 months
and certainly is present by 12 months of age. The reflex is elicited by turning the child up side
down. The arms should come forward and the hands spread out to catch the fall. Asymmetry of
the reflex is abnormal and may indicate paresis in the non-extended extremity.
Motor/Coordination - Pincer Grasp
Fine motor coordination of the hand progresses in a definite pattern. At 6-7 months the hand is
used as a rake and objects are raked into the palm with the fingers. At 8-9 months the thumb
and the radial fingers are used to grasp an object and smaller objects are picked up. At 10-12
months, the fine pincer grasp is developed. This enables an infant to pick up a small object
between the distal thumb and index finger.
Both infants in this exam have developed a pincer grasp. The first infant uses the pincer grasp to
feed himself a cheerio. The second infant demonstrates a pincer grasp by grabbing the tip of a
measuring tape and pulling the tape out. The pincer grasp should be equal in either hand.
Handedness does not develop until after 12 months of age. Early handedness and asymmetric
fine motor skills are seen with a hemiparesis.
Motor/Coordination - Beads in the Cup
This test is a combination of understanding instructions, as demonstrated, and using a pincer
grasp to place the small bead in a container.
Motor/Coordination - Play Ball
The infant plays the simple game of throw the ball. His throw is not an overhand throw which is
seen in an 18 month old but rather a pushing away and dropping type of throw that is typical for
this age.
Motor - Transition in and out of Sitting
As far as gross motor skills, the infant is able to get in and out of the sitting position with ease
and creeps well.
Motor - Creeping
Crawling is a commando type of crawl which is an arm over arm propulsion forward with the
trunk on the ground and legs dragging. Crawling is usually seen at 7 to 9 months. Creeping is
crawling on hands and knees with the trunk off of the ground. Creeping is usually seen at 8 to 12
months.
Motor - Stoop and Recover
At one year, this infant has developed the ability to walk without support. Although still wobbly,
he can stoop down to pick up an object and stand back up without falling. He can maintain his
balance as he inspects and manipulates the toy. An infant usually develops the ability to stoop
and recover at 11 to 14 months of age.
Page 34
Page 34 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Motor/Gait - Stand, Walks with Support
The first infant demonstrates the ability to pull himself to a stand while holding on.
The second infant can stand, pull to a stand and cruise (not demonstrated because the baby is
upset). Cruising is walking along a piece of furniture while holding on. It usually develops
between 10 to 12 months. Along with cruising, the infant can take steps while holding on but
he’s not ready to walk unsupported.
Motor/Gait - Toddler’s Gait
Independent walking is achieved between 11 and 15 months of age. An infant is delayed if they
aren’t walking by 16 months. This 12 month old infant has a typical gait of an infant that has just
learned to walk. He has a wide base, is unsteady, and toddles. His arms are held at near
shoulder level in a high guard position. This is a protective position and probably aids in his
balance. As he matures, his arms will come down to a low guard position, then into the usual
associated arm movements seen with mature walking.
Head Circumference
The first attempt to measure the head circumference is easy but the examiner reads the
measurement as 50.6 cm, which is above the 98th percentile. Second attempt is much more
difficult because the infant doesn’t want the tape measure around his head. The measurement
however is read as 47.7 cm, which is at the 50th percentile. A third attempt verifies that the
47.7 cm measurement is correct. Always take at least two measurements and save the head
circumference to the last.
18 MONTH OLD
Behavior/Mental Status - Wants
At this age, the child indicates his wants by pointing, gesturing and using vocalizations other than
crying. At 18 months, he should have a vocabulary of 10 or more words and will use single words
to indicate wants. Social interaction at this age is rich and increasing in complexity as seen in
this child.
Behavior/Mental Status - Understanding
The toddler understands the use of objects and knows how things work. He’s trying to get the
pen to work. He will follow simple commands, but still needs reinforcement and at times
demonstration.
Behavior/Mental Status - Points to Pictures
The toddler is asked to point to pictures of a cat, horse, bird and dog. These pictures are part of
the Denver II assessment tool. An 18 month old should be able to point to at least 2 of the
pictures. This toddler identifies 4 pictures and repeats the name of 3.
Behavior/Mental Status - Points to Body Parts
When asked to point to body parts on the finger puppet, the toddler identifies eyes and mouth
correctly. The naming of 2 body parts is normal for an 18 month old. Between 18 and 30 months
the toddler should learn to identify 6 out of 8 body parts.
Cranial Nerves
Conjugate eye movements and the near reflex can be tested with an interesting object like a
finger puppet. Facial movement is noted as the toddler smiles.
Page 35
Page 35 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Fine Motor/Coordination - Blocks in Cup
The toddler shows good coordination as he takes blocks and puts them in the cup. He is able to
control the cup as well as reaching for the blocks.
Fine Motor/Coordination - Beads in Cup
He is able to pick up small beads and place them in a small container with good fine motor
control. By using both blocks and beads, one is testing increasing levels of difficulty of fine motor
control and coordination.
Fine Motor/Coordination - Stacking Blocks
Even more demanding than placing blocks or beads in a container is the task of stacking blocks.
The number of blocks that a child can stack is correlated with their level of motor development. A
15 month old can stack 2 blocks while an 18 month old should be able to stack at least 4
blocks. This toddler is able to stack 5 blocks.
Fine Motor/Coordination - Pincer Grasp and Handedness
The toddler has a good pincer grasp as he grasps the end of a tape measure and pulls on it. He
uses both hands well, but now the parents identify that he is starting to use the right hand more
than the left hand. Handedness develops in the 2nd year of life.
Fine Motor/Coordination - Drawing/Scribbling
An 18 month old child can hold a pen and imitates scribbling or can scribble spontaneously. At
this age he is holding the pen between the thumb and first 3 fingers and is developing a tripod
position of the hand for drawing.
Motor - Tone
Passive range of motion is tested for both the upper and lower extremities. Toddlers can be
apprehensive about having the examiner move his arms and legs, but reassurance and
distraction usually work to get an adequate exam.
Motor/Reflexes - Deep Tendon Reflexes/ Plantar Reflex
By making the reflex hammer into a play object and adding sound effects, the child usually
cooperates enough to adequately obtain deep tendon reflexes. Testing for the plantar reflex
shows that the toes are definitely down going.
Motor - Throwing Ball
The toddler is able to throw the ball overhand and shows pleasure in playing the game of
throwing and chasing after the ball.
Motor/Gait - Walking
The 18 month old has a much more steady and secure gait than the infant that is just learning to
walk. He still has a wide-based gait but no wobbling. His arms are held in a low guard position- at
the level of his waist. He squats without falling and is able to get up in the middle of the floor
without pulling himself up. Notice how he gets up from the supine position. He first rolls to his
stomach, then steadies himself with his hands on the floor to get up. As he gets older he’ll do a
sit up rather than rolling over and he will be able to get up without using his hands. Importantly,
there is no evidence for proximal pelvic girdle weakness as he gets up from the ground or walks.
Page 36
Page 36 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
2 ½ YEAR OLD
Behavior/Mental Status - Establishing Relationship
This 2.5 year old is apprehensive about being examined and isn’t quite sure she wants to be
there. The finger puppets are used in attempt to establish rapport and involve the child in play.
The child’s social interactions and motor skills are observed during this time. The child is also
examined on the mother’s lap.
Behavior/Mental Status - Follows Commands
At this age verbal instructions without demonstration are understood. The child can follow two-
step commands.
Behavior/Mental Status - Points to Pictures
The girl is first asked to name the pictures but doesn’t cooperate enough to determine if she
knows their names. So the examiner switches strategy and asks her to point to the picture he
names. She is able to do this for all five pictures. She asserts her autonomy by using her foot
instead of her finger. These pictures are from the Denver II.
Behavior/Mental Status - Names Pictures
Later on in the exam she cooperates enough to demonstrate that she is able to name all five
pictures that are shown to her, which is the next developmental level above pointing to them.
The next level after naming would be identification by the action of the picture, such as asking
which one flies. Pointing to 4 pictures should be accomplished by 2.5 years, naming by 3 years
and identification by action by 4 years.
Behavior/Mental Status - Response to Questions
The girl is shown a picture in an attempt to get her to talk. She is shy and doesn’t talk much but
responds to questions with yes and no. She is putting two words together in a simple sentence.
A child’s earliest sentences usually contain important content words and lack grammatical
words. A 3 year old forms a 3 to 4 word sentence and uses pronouns and plurals.
Behavior/Mental Status - Pointing to and Naming Body Parts
The girl is able to point to 8 out of 9 body parts. She can identify them on herself as well as
others. A 2.5 year old should be able to point to 6 out of 8 body parts.
Fine Motor/Coordination - Using Puppets
Using finger puppets facilitates coordination testing. First the girl is asked to place the puppets
on her finger, which shows that she accurately reaches a target without ataxia. The girl is then
taught how to do finger to nose by having her touch the puppet’s nose then her nose.
Fine Motor/Coordination - Using Measuring Tape
A measuring tape can also be used to test coordination. As the girl reaches for the tip of the
tape to pull it out and has to extend the arm to reach the target, she is being tested for
dysmetria. Having her manipulate the tape measure and work the control button is testing hand
coordination. The examiner tries to get her to click the button but she doesn’t do it. This was an
attempt to test repetitive movements.
Page 37
Page 37 of 37
PROPERTY OF AUFSOM BATCH 2017 v3.1 s2015-2016
PI and LAMBDA
Fine Motor/Coordination - Block Tower
The girl is able to build a 5 block tower and almost gets to 6 blocks. She’s not sitting in the best
position nor does she have the most stable platform to build a tower. A 2.5 year old should be
able to build a 6-8 block high tower. At 3 years, the child is able to build a 3-block bridge.
Assessing if a child is developmentally age appropriate is not based on one particular test but
rather how they do on several different tests as well as their overall performance.
Fine Motor/Coordination - Drawing
The girl imitates drawing a horizontal line as well as making circular shapes. At 3 years of age a
child should be able to draw a circle and at 4 years old can copy a cross.
Motor - Tone
Upper and lower extremity tone is tested using passive range of motion. The girl is apprehensive
about this but using the finger puppet as part of the exam helps.
Motor/Reflexes - Deep Tendon Reflexes
This segment of the exam illustrates the problems associated with obtaining deep tendon
reflexes. The reflex hammer is turned into a horse and initially she allows the examiner to test
the right upper extremity. Notice that after testing for the brachioradialis reflex she becomes
uncooperative. One of the ways to reduce apprehension in the child is to place your thumb or
index finger over the tendon to be examined and tap on it rather than directly tapping on the
child’s tendon. It’s less threatening.
Motor - Kicking and Throwing a Ball
At this age, the child is able to kick the ball and throws the ball overhand to the examiner. A ball
is a good tool to use during the neurological examination because the child enjoys playing with it
and it allows the examiner to see both fine and gross motor skills that the child has developed.
Motor/ Gait - Walking, Running
At this age, the gait is steady, well coordinated and no longer wide-based. The arms are down to
the side and there are normal associated movements. The hands are no longer used when
getting up off the floor or sitting down on the floor. The child is able to run.
Reference: University of Utah. (2015). Neurologic Examination
http://library.med.utah.edu/neurologicexam/html/home_exam.html