Neuropsychiatric Emergencies Neuropsychiatric Emergencies Andy Jagoda, MD, FACEP Andy Jagoda, MD, FACEP Professor of Emergency Medicine Professor of Emergency Medicine Mount Sinai School of Medicine Mount Sinai School of Medicine New York, New York New York, New York
Andy Jagoda, MD, FACEPAndy Jagoda, MD, FACEPProfessor of Emergency MedicineProfessor of Emergency MedicineMount Sinai School of MedicineMount Sinai School of Medicine
New York, New YorkNew York, New York
The CaseThe Case
26 year old female presents to the ED with a chief complaint 26 year old female presents to the ED with a chief complaint of “acting strange”of “acting strange”
According to her husband, for the past 24 hours she has been According to her husband, for the past 24 hours she has been having periods of fear and paranoia having periods of fear and paranoia
Psychiatrists should be able to Psychiatrists should be able to medically evaluate their own patients medically evaluate their own patients by performing a complete history by performing a complete history and physical examination?and physical examination?
True True FalseFalse
Emergency physicians should be able to Emergency physicians should be able to competently evaluate the psychiatric and competently evaluate the psychiatric and neurologic mental status of their patientsneurologic mental status of their patients
TrueTrue FalseFalse
BackgroundBackground
• 105 million ED visits a year in the USA105 million ED visits a year in the USA
• 2% to 12% of patients presenting to the ED have a 2% to 12% of patients presenting to the ED have a psychiatric complaintpsychiatric complaint
• 25% to 50% of patients with psychiatric illness also 25% to 50% of patients with psychiatric illness also have a medical disorder that can contribute to acute have a medical disorder that can contribute to acute disturbances in thought, behavior, mood, or social disturbances in thought, behavior, mood, or social relationshipsrelationships
• 4% to 12% of psych inpatients have a medical 4% to 12% of psych inpatients have a medical condition identified as precipitating the admission condition identified as precipitating the admission
Tintinalli et al. Ann Emerg Med 1994; 23:859Tintinalli et al. Ann Emerg Med 1994; 23:859Dolan et al. Arch Intern Med 1985; 145: 2085Dolan et al. Arch Intern Med 1985; 145: 2085
Challenges to overcome caring for the patient with a Challenges to overcome caring for the patient with a psychiatric complaintpsychiatric complaint
• Bias against patients with mental illnessBias against patients with mental illness
• Prioritization of “sicker” patientsPrioritization of “sicker” patients
• Patient unwilling or unable to cooperatePatient unwilling or unable to cooperate
• Time constraintsTime constraints
McIntyre JA, Romano J: Is there a stethoscope in the house (and McIntyre JA, Romano J: Is there a stethoscope in the house (and is it used?). Arch Gen Psych 1977; 34:1147is it used?). Arch Gen Psych 1977; 34:1147
87% of surveyed psychiatrists did not routinely perform a 87% of surveyed psychiatrists did not routinely perform a physical examination on their inpatientsphysical examination on their inpatients
Patterson C. Psychiatrists and physical examinations: A survey. Patterson C. Psychiatrists and physical examinations: A survey. Am J Psych 1978; 135:967Am J Psych 1978; 135:967
83% of psychiatrists did not routinely perform physical 83% of psychiatrists did not routinely perform physical examinations on their inpatients. Reasons: examinations on their inpatients. Reasons: -- uncomfortable performing an exam uncomfortable performing an exam-- already performed by someone else, already performed by someone else, -- desire to avoid transference / countertransference desire to avoid transference / countertransference-- dislike of performing medical examinations dislike of performing medical examinations
Riba M: Medical clearance: Fact or fiction in the hospital Riba M: Medical clearance: Fact or fiction in the hospital emergency room. Psychosomatics 1990: 31; 400-404emergency room. Psychosomatics 1990: 31; 400-404
• Retrospective chart review of 137 ED Retrospective chart review of 137 ED patients with psychiatric diagnosespatients with psychiatric diagnoses
• 32% no vital signs32% no vital signs• 64% no documentation of general 64% no documentation of general
appearanceappearance• 67% no documentation of present illness67% no documentation of present illness• 92% no neurologic examination92% no neurologic examination• 92% no laboratory testing92% no laboratory testing
Tintinalli J et al. Emergency medical evaluation of Tintinalli J et al. Emergency medical evaluation of psych patients. Ann Emerg Med 1994 23;4: 859-862psych patients. Ann Emerg Med 1994 23;4: 859-862
• Retrospective review, 298 charts of patients Retrospective review, 298 charts of patients with psychiatric chief complaintwith psychiatric chief complaint
• 12 (4%) required acute medical tx within 24 12 (4%) required acute medical tx within 24 hours of admission: 10 (3%) were hours of admission: 10 (3%) were transferred to a medical servicetransferred to a medical service
• Neuro exam, including mental status, was Neuro exam, including mental status, was most frequent deficiencymost frequent deficiency
• Younger patients had a four fold greater risk Younger patients had a four fold greater risk of having a missed medical diagnosisof having a missed medical diagnosis
General Approach to Medical ClearanceGeneral Approach to Medical Clearance
• Triage based on chief Triage based on chief
complaint and vital signscomplaint and vital signs
• HistoryHistory
• PhysicalPhysical
• Laboratory testingLaboratory testing
Findings Suggestive of an Underlying Medical Findings Suggestive of an Underlying Medical Disorder for Psychiatric SymptomsDisorder for Psychiatric Symptoms
• Onset after age 40 / No past history of psychiatric illnessOnset after age 40 / No past history of psychiatric illness
• Sudden onsetSudden onset
• Presence of a “toxidrome”Presence of a “toxidrome”
• Baseline mental and physical status prior to Baseline mental and physical status prior to psychiatric historypsychiatric history
• Good listeners and patient advocates have the best Good listeners and patient advocates have the best chance of getting an appropriate historychance of getting an appropriate history
• Involve family, friends, othersInvolve family, friends, others• Time and rapidity of onsetTime and rapidity of onset• Medications and / or changes in dosingMedications and / or changes in dosing• Alcohol and / or illicit drug useAlcohol and / or illicit drug use• ““Why now”: conceptual framework to understand Why now”: conceptual framework to understand
what overwhelmed usual coping mechanismswhat overwhelmed usual coping mechanisms
The PhysicalThe Physical• Vital signs: accurate temp, pulse oximetryVital signs: accurate temp, pulse oximetry
• AppearanceAppearance
• Head exam: signs of traumaHead exam: signs of trauma
(memory) (memory) • Language (repetition / Language (repetition /
naming)naming)• Visual SpatialVisual Spatial
• O x 3O x 3• Could not give monthsCould not give months• Could repeat but could not Could repeat but could not
recall 3 objectsrecall 3 objects• IntactIntact
• IntactIntact
The Psychiatric Mental Status ExamThe Psychiatric Mental Status Exam
• AppearanceAppearance
• MotorMotor
• SpeechSpeech
• Affect and moodAffect and mood
• Thought contentThought content
• Thought processThought process
• PerceptionPerception
• Insight / JudgementInsight / Judgement
• Impulse control / safetyImpulse control / safety
• DisheveledDisheveled
• NormalNormal
• NormalNormal
• FlatFlat
• Paranoid, No suicidal ideationParanoid, No suicidal ideation
• ConcreteConcrete
• No hallucinationsNo hallucinations
• No insight into her illnessNo insight into her illness
• Did not feel out of controlDid not feel out of control
Laboratory TestingLaboratory Testing
• Hall et al. Unrecognized physical illness prompting Hall et al. Unrecognized physical illness prompting psychiatric admission: A prospective study. Am J psychiatric admission: A prospective study. Am J Psych 1981; 138:629Psych 1981; 138:629
• 100 state hospital psych patients with no known 100 state hospital psych patients with no known medical disease or substance abusemedical disease or substance abuse
• SMA-34, urine tox, EEGSMA-34, urine tox, EEG
• 60/100 had an abnormality on the SMA-3460/100 had an abnormality on the SMA-34
• Did not address how many of the abnormalities were Did not address how many of the abnormalities were clinically significantclinically significant
Laboratory TestingLaboratory Testing
• Henneman et al. Prospective evaluation of ED Henneman et al. Prospective evaluation of ED medical clearance. Ann Emerg Med 1994; 24: 672medical clearance. Ann Emerg Med 1994; 24: 672
• 100 ED patients with new psychiatric complaints100 ED patients with new psychiatric complaints• H&P, ETOH, urine tox, CBC, SMA 7; CT H&P, ETOH, urine tox, CBC, SMA 7; CT
optional, LP if febrileoptional, LP if febrile• Excluded known patients with psych disorders, Excluded known patients with psych disorders,
psych patients with medical complaints, known psych patients with medical complaints, known drug use or suicide attemptdrug use or suicide attempt
• 63/100 had medical cause identified: 30/63 tox, 63/100 had medical cause identified: 30/63 tox, 25/63 neurologic, 5/63 infectious (3 CNS)25/63 neurologic, 5/63 infectious (3 CNS)
Laboratory TestingLaboratory Testing
• Olshaker et al. Medical clearance and screening of Olshaker et al. Medical clearance and screening of psychiatric patients in the ED. 1997:2:124psychiatric patients in the ED. 1997:2:124
• 345 patients for medical clearance345 patients for medical clearance
• 65 (19%) found to have a medical condition65 (19%) found to have a medical condition
• History 94% sensitivity; laboratory testing 20% History 94% sensitivity; laboratory testing 20% sensitivesensitive
• Conclude that H&P is the most important part Conclude that H&P is the most important part medical clearance and laboratory testing is “low medical clearance and laboratory testing is “low yield”yield”
Summary on Medical ClearanceSummary on Medical Clearance
• A complete history and physical is key to A complete history and physical is key to “medical clearance”“medical clearance”
• Laboratory testing is driven by the H&PLaboratory testing is driven by the H&P• Consider laboratory testing:Consider laboratory testing:
• Underlying medical conditionUnderlying medical condition• Abnormal vital signsAbnormal vital signs• ElderlyElderly• New onset psychiatric complaintNew onset psychiatric complaint
Medical Screen vs Medical EvaluationMedical Screen vs Medical Evaluation
• ““Medical screen” establishes that the patient is currently Medical screen” establishes that the patient is currently stable vs “Medical evaluation” establishes patients stable vs “Medical evaluation” establishes patients baseline state of healthbaseline state of health
• Drug of abuse screen screen may help in the psychiatric Drug of abuse screen screen may help in the psychiatric evaluation and disposition planningevaluation and disposition planning
• Liver function and renal function may help in the long Liver function and renal function may help in the long term treatment planningterm treatment planning• Many inpatient facilities do not have ready access to Many inpatient facilities do not have ready access to
these teststhese tests• Atypical antipsychotics may increase serum glucose and Atypical antipsychotics may increase serum glucose and
lipid levels; baseline required before initiating therapylipid levels; baseline required before initiating therapy• ECG necessary to evaluate the QT intervalECG necessary to evaluate the QT interval
The Case ContinuedThe Case Continued
ROS (by husband): 10 lb weight loss over past 6 months, ROS (by husband): 10 lb weight loss over past 6 months, occasional palpitations, periods of agitation / fear, occasional palpitations, periods of agitation / fear, withdrawn behavior, lack of initiative, poor hygienewithdrawn behavior, lack of initiative, poor hygiene
General Appearance: 30 yo female, disheveled, agitatedGeneral Appearance: 30 yo female, disheveled, agitated
Hypervigilant with paranoid ideation that her husband was Hypervigilant with paranoid ideation that her husband was trying to poison hertrying to poison her
Rest of exam was normal including normal thyroid, no heart Rest of exam was normal including normal thyroid, no heart murmur, normal GYN exam, normal skin and hairmurmur, normal GYN exam, normal skin and hair
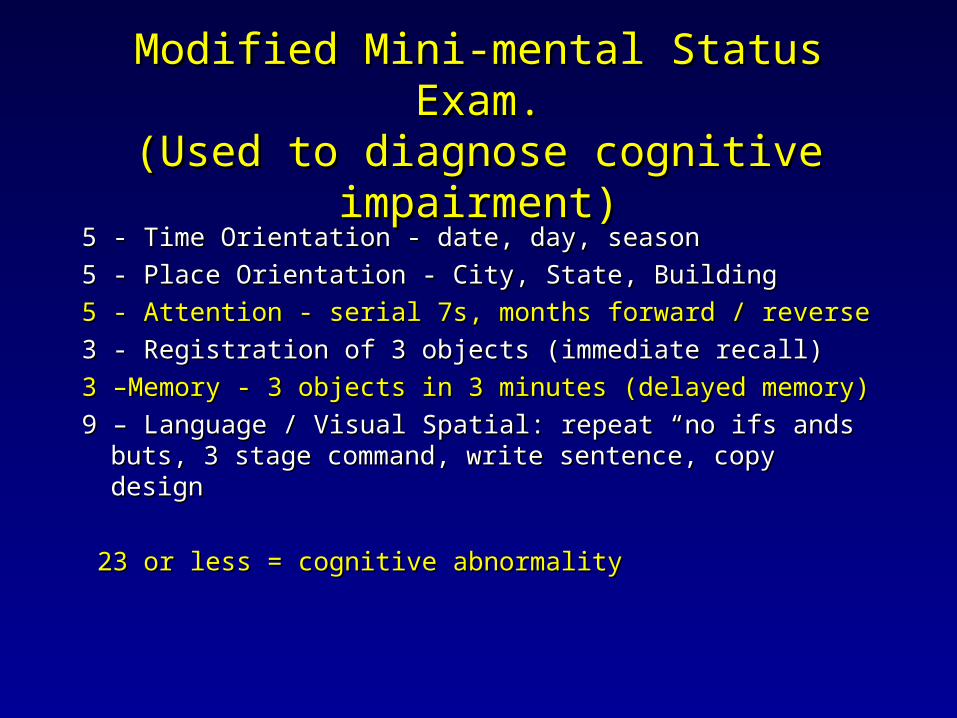
Delirium: DefinitionDelirium: Definition
• Acute, reversible, diffuse neuronal dysfunction Acute, reversible, diffuse neuronal dysfunction usually due to a toxic-metabolic derangementusually due to a toxic-metabolic derangement
Must have feature 1 and 2; and 3 or 4Must have feature 1 and 2; and 3 or 4
• Feature 1Feature 1: Acute onset and fluctuating course: Acute onset and fluctuating course• History by familyHistory by family• Change from the baselineChange from the baseline
• Structural CNS lesionStructural CNS lesion• Toxic: Overdose vs drug effectToxic: Overdose vs drug effect• Withdrawal syndromeWithdrawal syndrome• MetabolicMetabolic• Infection: Central vs systemicInfection: Central vs systemic• SeizureSeizure• Acute psychiatric disorderAcute psychiatric disorder
23 or less = cognitive abnormality23 or less = cognitive abnormality
Hustey. ED Prevalence and Documentation of Impaired Hustey. ED Prevalence and Documentation of Impaired Mental Status in Elderly. Ann Emerg Med 2002; 39Mental Status in Elderly. Ann Emerg Med 2002; 39
• 26% (78/297) of patients had altered ms26% (78/297) of patients had altered ms• 10% (30/297) had delirium10% (30/297) had delirium• 17/30 (57%) had documentation of abnormal 17/30 (57%) had documentation of abnormal
mental status by ED providermental status by ED provider• 70% of pts discharged home with cognitive 70% of pts discharged home with cognitive
impairment had no evidence available that the impairment had no evidence available that the mental status abnormality was chronic mental status abnormality was chronic
• Calm and DirectCalm and Direct• EmpathicEmpathic• Verbalize limits / expectationsVerbalize limits / expectations• Consistency among staffConsistency among staff
Interview TechniquesInterview Techniques
• Eye ContactEye Contact• Personal SpacePersonal Space• Door PositionDoor Position• Body LanguageBody Language
• Antispychotic plus BenzodiazepineAntispychotic plus Benzodiazepine• Atypical antipsychotic Atypical antipsychotic
BenzodiazapinesBenzodiazapines
• Lorazepam, diazepam, midazolamLorazepam, diazepam, midazolam• Anxiolitics not antipsychoticsAnxiolitics not antipsychotics• Less predictable effectLess predictable effect
• Paradoxical disinhibitionParadoxical disinhibition• Less titratabilityLess titratability• Risk of cardiorespiratory depressionRisk of cardiorespiratory depression
• Butyrophenone antipsychoticButyrophenone antipsychotic• 2.5- 5 mg IM or IV2.5- 5 mg IM or IV• Onset minutesOnset minutes• t 1/2 2-4 hourst 1/2 2-4 hours• Side effectsSide effects
• Lancet 2000: Droperidol reported to cause QT Lancet 2000: Droperidol reported to cause QT prolongation and possibly sudden death: Janssen withdrew prolongation and possibly sudden death: Janssen withdrew drug from the European marketdrug from the European market
• Patients self administered large dosesPatients self administered large doses
• Often used with other antipsychoticsOften used with other antipsychotics
• FDA 2001: Black box warning “Dear Health Care FDA 2001: Black box warning “Dear Health Care Professional . . . “Professional . . . “
• Recommended that it not be given to males with a QTc Recommended that it not be given to males with a QTc >440 and females with a QTc >450>440 and females with a QTc >450
The Droperidol DilemmaThe Droperidol Dilemma
• Acad Emerg Med 2002. “Behind the black box warning”Acad Emerg Med 2002. “Behind the black box warning”• The FDA data analyzed: 93 cases of death identifiedThe FDA data analyzed: 93 cases of death identified
• 52 cases at doses > 10 mg (most 50-100 mg IM)52 cases at doses > 10 mg (most 50-100 mg IM)• 22 cases, no dose given22 cases, no dose given
• 11 cases of torsades; 9 cases of prolonged QTc11 cases of torsades; 9 cases of prolonged QTc• 13 cases of death at doses below 10 mg13 cases of death at doses below 10 mg
• 3 involved multiple doses3 involved multiple doses• 3 were anesthetic related3 were anesthetic related• 1 case the dose was .635 mg1 case the dose was .635 mg• 1 case the dose was .25 mg1 case the dose was .25 mg• 5 potential cases out of the original 935 potential cases out of the original 93
Atypical AntipsychoticsAtypical Antipsychotics
• e.g. Respiridonee.g. Respiridone• Orally administered with or without a Orally administered with or without a
benzodiazepinebenzodiazepine• May prolong the QTcMay prolong the QTc• Role still undefinedRole still undefined
AAP. Practice guideline for the treatment of patients AAP. Practice guideline for the treatment of patients with delirium. Am J Psychiatry 1999; 156 (suppl):1-20with delirium. Am J Psychiatry 1999; 156 (suppl):1-20
• Monotherapy with a typical antipsychotic: haloperidol or Monotherapy with a typical antipsychotic: haloperidol or droperidoldroperidol• Droperidol has a faster onset and less frequent need for a Droperidol has a faster onset and less frequent need for a
second dosesecond dose• Need to monitor ECG and serum Mg levels Need to monitor ECG and serum Mg levels
• Benzodiazepines as a monotherapy is reserved for delirium Benzodiazepines as a monotherapy is reserved for delirium from drug withdrawalfrom drug withdrawal• Generally avoided as monotherapy in the elderlyGenerally avoided as monotherapy in the elderly• Lorazepam possibly preferred in patients with liver diseaseLorazepam possibly preferred in patients with liver disease
• Combined therapy of a antipsychotic plus a benzodiazepine Combined therapy of a antipsychotic plus a benzodiazepine may have faster onset of action with fewer side effectsmay have faster onset of action with fewer side effects
Physical RestraintsPhysical Restraints
• For imminent threat of harmFor imminent threat of harm• PreparationsPreparations
• Overwhelming show of forceOverwhelming show of force• Initiate only when preparedInitiate only when prepared• Preparation / de-escalationPreparation / de-escalation
Physical RestraintPhysical Restraint
• Once initiated, swift and definitiveOnce initiated, swift and definitive• Suspend negotiationsSuspend negotiations• Team leaderTeam leader• Secure large jointsSecure large joints• Constant reassuranceConstant reassurance
• Plan for reassessment and removal Plan for reassessment and removal
Case ContinuedCase Continued
The patient was sedated with droperidol, 5 mg / lorazepam 2 The patient was sedated with droperidol, 5 mg / lorazepam 2 mg IVmg IV
CT was negativeCT was negative
She was admitted to the Medicine ServiceShe was admitted to the Medicine Service
Blood and urine cultures:Blood and urine cultures: negativenegativeThyroid Function Tests:Thyroid Function Tests: negativenegativeEEG:EEG: normalnormal
Final Diagnosis: _________________________________Final Diagnosis: _________________________________
SchizophreniaSchizophrenia
• Psychotic disorder manifested by one or more active phase Psychotic disorder manifested by one or more active phase symptoms, marked social and or occupational dysfunction, symptoms, marked social and or occupational dysfunction, and a course lasting at least 6 months. and a course lasting at least 6 months.
• It is a diagnosis of exclusion.It is a diagnosis of exclusion.
• Positive symptoms include delusions, hallucinations, Positive symptoms include delusions, hallucinations, disorganization, and catatonia.disorganization, and catatonia.
• Negative symptoms include: affective flattening, Negative symptoms include: affective flattening, inappropriate affect, alogia, avolition, asocialtiy, inappropriate affect, alogia, avolition, asocialtiy, anhedonia, lack of insight, lack of initiative, poor hygieneanhedonia, lack of insight, lack of initiative, poor hygiene
SchizophreniaSchizophrenia
• Average age of onset for women is 27Average age of onset for women is 27• Three phases:Three phases:
• Active: emergence of active phase Active: emergence of active phase symptoms. May follow an acute symptoms. May follow an acute stressorstressor
• Residual phase: Attenuated positive / Residual phase: Attenuated positive / negative symptoms. Relapse may negative symptoms. Relapse may occuroccur
SchizophreniaSchizophrenia
• Patient was transferred to the inpatient Patient was transferred to the inpatient psychiatry servicepsychiatry service• Respiridone, 1 mg bid started and Respiridone, 1 mg bid started and
increased to 2 mg bid increased to 2 mg bid • Discharged after 3 weeks, stable with Discharged after 3 weeks, stable with
control of symptomscontrol of symptoms• Stopped taking medication after 3 Stopped taking medication after 3
months secondary to weight gain and months secondary to weight gain and sexual dysfunctionsexual dysfunction
• Represented to the ED six months after Represented to the ED six months after discharge with same symptomsdischarge with same symptoms
ConclusionsConclusions
• Patients with an acute change in behavior require Patients with an acute change in behavior require a careful medical evaluation a careful medical evaluation
• Historical and physical findings provide the Historical and physical findings provide the baseline necessary to determine diagnostic testing baseline necessary to determine diagnostic testing
• Delirium is a medical emergencyDelirium is a medical emergency
• In general, antipsychotics are still the In general, antipsychotics are still the pharmacologic intervention of choice in the pharmacologic intervention of choice in the acutely agitated patientacutely agitated patient