397 NEUROVASCULAR SYNDROMES OF THE SHOULDER GIRDLE AND UPPER EXTREMITY: THE COMPRESSION DISORDERS AND THE SHOULDER-HAND SYNDROME By H. HAROLD FRIEDMAN, M.D., THOMAS G. ARGYROS, M.D., AND OTTO STEINBROCKER, M.D.* Introduction Some of the most perplexing and difficult musculoskeletal disorders are included among those affecting the shoulder girdle and upper extremity. Pain, paresthesias, hyperesthesia and vasomotor disturbances may occur in any of them, but these symptoms in combination are character- istic of few, chiefly the neurovascular syndromes. The interpretation and differentiation of the clinical features may embrace a large number of diseases and disorders (Table I). The purpose of this paper is to summarize present knowledge of two groups of these conditions-the reflex neuro- vascular disorders, as fully exemplified by the shoulder-hand syndrome, and the compression neurovascular syndromes (' thoracic outlet syn- dromes '). Since anatomic factors are of basic importance in the genesis of these disturbances, the pertinent anatomy must be visualized in these problems (Fig. i). Anatomy The anatomy is complex, so only its main features will be mentioned here. The normal components of this area include the first rib, the scalene muscles (anterior, medial, occasionally inferior), clavicle and subclavius, the coracoid process and pectoralis minor muscle. Added to these at times may be encountered bony de- formities of the first rib and the clavicle, cervical ribs, gross deformities due to kyphoscoliosis, thoracoplasty and injury, bizarre insertions of the scalene muscles and assorted congenital fibrous bands, vascular anomalies, lymph node enlarge- ments, tumours, etc.11 The key to the whole problem consists of the size and the adaptability of the thoroughfare, the thoracic outlet and its con- tiguous space, through which the neurovascular bundle must pass in close relationship to the *From General Rose Memorial Hospital and the University of Colorado Medical Center, Denver Colorado (Dr. Friedman) and the Rheumatology Department, Hospital for Joint Diseases and Lenox Hill Hospital, N.Y.C. (Drs. Argyros and Steinbrocker). anatomic constitutents already mentioned. In the vast majority of people this short distance is traversed without difficulty, even in the presence of anomalous structures. In some, however, the bundle is impinged upon, in one way or another, to produce the symptoms underlying the syn- dromes under discussion. Normally, the subclavian artery hooks up and over the first rib, lying between the insertions of the scalenus anterior and medius muscles, passes down under the coracoid process and then into the axilla. The subclavian vein runs a parallel route, except that it proceeds between the scalenus anterior and the clavicle. The brachial plexus in this region tends to course along the artery and is represented primarily by fibers from C8-Ti. The prominent points of compression have given their names to the syndromes they provoke. At present, these include the cervical rib, scalenus anticus, first rib and costoclavicular syndromes. The hyperabduction syndrome might be regarded, accordingly, as the ' coracoid pectoralis minor clavicle syndrome.' Contributory or Provocative Factors Contributing factors in the production of symptoms include the great mobility of the shoulder which, even in normal structures, permits compression of the neurovascular bundle in certain positions. Generally, these are responsible for symptoms only when there is prolonged main- tenance of bizarre positions, as in work, sleep, recreation, etc. As people age there is a tendency toward a reduction in muscle mass and a loss of tone with a drooping of the shoulders. Anomalies and trauma play an obvious role. Arteriosclerosis with loss of pliability is a frequent predisposing factor to vascular complication from compression in the older age groups. Symptomatology of the Compression Syndromes The clinical manifestations of these syndromes are dependent upon compression of the brachial copyright. on 23 June 2018 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.35.405.397 on 1 July 1959. Downloaded from
Transcript
397
NEUROVASCULAR SYNDROMES OF THESHOULDER GIRDLE AND UPPER EXTREMITY:THE COMPRESSION DISORDERS AND THE
SHOULDER-HAND SYNDROMEBy H. HAROLD FRIEDMAN, M.D., THOMAS G. ARGYROS, M.D., AND OTTO STEINBROCKER, M.D.*
IntroductionSome of the most perplexing and difficult
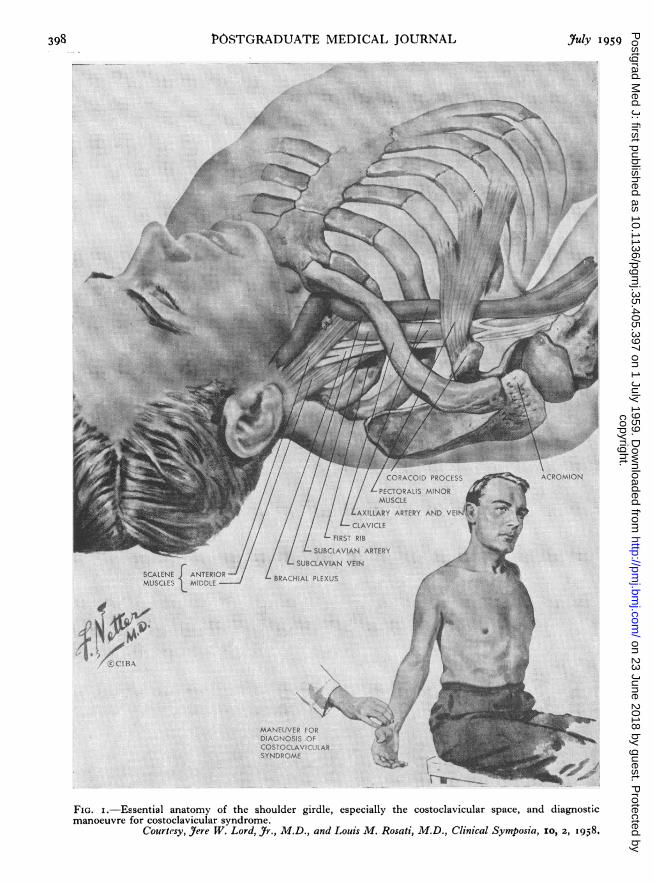
musculoskeletal disorders are included amongthose affecting the shoulder girdle and upperextremity. Pain, paresthesias, hyperesthesia andvasomotor disturbances may occur in any of them,but these symptoms in combination are character-istic of few, chiefly the neurovascular syndromes.The interpretation and differentiation of theclinical features may embrace a large number ofdiseases and disorders (Table I). The purpose ofthis paper is to summarize present knowledge oftwo groups of these conditions-the reflex neuro-vascular disorders, as fully exemplified by theshoulder-hand syndrome, and the compressionneurovascular syndromes (' thoracic outlet syn-dromes '). Since anatomic factors are of basicimportance in the genesis of these disturbances,the pertinent anatomy must be visualized in theseproblems (Fig. i).
AnatomyThe anatomy is complex, so only its main
features will be mentioned here. The normalcomponents of this area include the first rib, thescalene muscles (anterior, medial, occasionallyinferior), clavicle and subclavius, the coracoidprocess and pectoralis minor muscle. Added tothese at times may be encountered bony de-formities of the first rib and the clavicle, cervicalribs, gross deformities due to kyphoscoliosis,thoracoplasty and injury, bizarre insertions of thescalene muscles and assorted congenital fibrousbands, vascular anomalies, lymph node enlarge-ments, tumours, etc.11 The key to the wholeproblem consists of the size and the adaptability ofthe thoroughfare, the thoracic outlet and its con-tiguous space, through which the neurovascularbundle must pass in close relationship to the
*From General Rose Memorial Hospital and theUniversity of Colorado Medical Center, DenverColorado (Dr. Friedman) and the RheumatologyDepartment, Hospital for Joint Diseases and LenoxHill Hospital, N.Y.C. (Drs. Argyros and Steinbrocker).
anatomic constitutents already mentioned. Inthe vast majority of people this short distance istraversed without difficulty, even in the presenceof anomalous structures. In some, however, thebundle is impinged upon, in one way or another,to produce the symptoms underlying the syn-dromes under discussion.
Normally, the subclavian artery hooks up andover the first rib, lying between the insertions ofthe scalenus anterior and medius muscles, passesdown under the coracoid process and then into theaxilla. The subclavian vein runs a parallel route,except that it proceeds between the scalenusanterior and the clavicle. The brachial plexusin this region tends to course along the arteryand is represented primarily by fibers from C8-Ti.The prominent points of compression have giventheir names to the syndromes they provoke. Atpresent, these include the cervical rib, scalenusanticus, first rib and costoclavicular syndromes.The hyperabduction syndrome might be regarded,accordingly, as the ' coracoid pectoralis minorclavicle syndrome.'
Contributory or Provocative FactorsContributing factors in the production of
symptoms include the great mobility of theshoulder which, even in normal structures, permitscompression of the neurovascular bundle in certainpositions. Generally, these are responsible forsymptoms only when there is prolonged main-tenance of bizarre positions, as in work, sleep,recreation, etc. As people age there is a tendencytoward a reduction in muscle mass and a loss oftone with a drooping of the shoulders. Anomaliesand trauma play an obvious role. Arteriosclerosiswith loss of pliability is a frequent predisposingfactor to vascular complication from compressionin the older age groups.
Symptomatology of the CompressionSyndromesThe clinical manifestations of these syndromes
July 1959 FRIEDMAN, ARGYROS and STEINBROCKER: Neurovascular Syndromes 399
1TABLE I
DisoRDRms WITH NEURAL, VASCULAR AND NEUROVASCULAR FEATURES AT THE SHOULDER AND UPPER ExmRziTYNeurovascular Disorders Neurological Disorders, Predominantly
Compression Syndromes Spinal cord traumaCervical rib, scalenus or first rib syndrome SyringomyeliaCostoclavicular syndrome Protruded intervertebral diskHyperabduction syndrome Neuropathy or tumours of the brachial plexus or
Vascular Disorders, Predominantly Systemic Diseases with Local FeaturesArterial Diffuse vasculitisAcute arterial occlusion Relapsing nodular panniculitisChronic occlusive arterial disease Rheumatoid arthritisAneurism Osteoarthritis of the cervical spine and shoulderErythromelalgia DermatomyositisRaynaud's disease SclerodermaArteriovenous fistula Other Disorders
Venous Fibromyalgias of the neck and shoulderAcute thrombophlebitis Intrinsic lesions of the shoulderChronic venous insufficiency Bicipital tendovaginitis
Lymphatic Calcific tendinitisAcute lymphangitis Periarthritis of the shoulderChronic lymphedema Psychalgias
plexus and/or vascular structures and the radiationor referral of pain from the structures compressed.Vascular symptoms are frequently absent, some-times prevail, and occasionally are the only onespresent. Neurologic symptoms and signs arepresented more often than those of vascular origin.They may be either sensory or motor, or both.Pain at the shoulder or along the extremity may bedescribed. Local tenderness may be elicited bypalpation at the sites of complaint. Symptoms,therefore, may be essentially musculoskeletal,neurologic, vascular or any combination of them.
Pain and paresthesias are the predominantsymptoms in most cases, but they are variable.Pain in the shoulder and deltoid regions withradiation to the elbow is a not uncommon com-plaint. Frequent, also, is pain felt in the ulnaraspect of the forearm and hand in the fourth andfifth fingers. Sometimes the pain spreads to theradial aspect of the forearm, hand and fingers;to the head, neck and face; and to the scapulararea or chest. The pain is generally describedas being of an aching or shooting nature.While the pain in these syndromes may occur
during the course of the day's activities it has adecided tendency to become worse at night,particularly when the patient is lying down.There often is difficulty in falling asleep and, ifasleep, the patient is apt to be awakened by thediscomfort. Whenever pain occurs, the patientattempts to find relief by adopting differentpositions. Sometimes the symptoms are allevi-ated by lying prone and permitting the arms to
swing over the side of the bed. At other times,relief is obtained by elevating the shoulders, as inleaning forward on the elbows, or by bending theneck toward the affected side, a position whichreduces the drag on the brachial plexus. Somepatients are more comfortable with the arms ad-ducted and with the forearm and hands placedacross the chest.The pain is generally aggravated by activities
which involve the use of the arms and shoulderssuch as lifting, reaching or pushing. Activitieswhich depress the shoulder, such as carryingsuitcases or heavy objects, also are likely to in-tensify symptoms. Deep inspiration and hyper-extension of the neck often increase the dis-comfort.There is usually a paucity of objective neuro-
logical signs. Sensory changes, such as hyper-esthesiae, are infrequent. When present, theytend to occur in the distribution of the median orulnar nerves. Such motor abnormalities asweakness, atrophy and muscle twitchings, arelikewise found in similar distribution.26 In rareinstances, in the presence of a cervical rib, aHomer's syndrome provides evidence of involve-ment of the cervical sympathetic fibers.The vascular changes which occur in these
syndromes include: (i) coldness, pallor andcyanosis of the hand; (2) swelling of the hand(s);(3) dependent rubor; (4) gangrene and ulcera-tions of the finger tips; (5) classical Raynaud'sphenomenon2; and (6) complications such asaxillary vein or subclavian artery thrombosis and
aneurysm of the subclavian artery with or withoutocclusion of the vessel.1'
In an affected extremity, the pulse is more easilyobliterated than in the normal person, by variousmanoeuvres to be discussed. An arterial bruit maybe heard in the supraclavicular space.4 Cervicalribs, if present, can often be palpated in this region.Sometimes the blood pressure will be found to belower on the affected side.
The Compression Syndromes of the ShoulderCervical Rib, Scalenus Anticus and First RibSyndrome
Historically, the first of these to be describedwas the cervical rib syndrome. Cervical ribsoccur as anomalous appendages in approximatelyo to o.o5 per cent. of individuals, with more thanhalf being bilateral. They are two to three timesmore common in women. Usually they are in-cidental findings, with only some io per cent. ofthem causing any difficulty. The size, shapeand insertion of the rib will frequently be thedetermining factors in the production of symptoms.Often there is arterial compression, with post-stenotic dilatation and incipient thrombosis. Thescalenus muscles may or may not be important inthe activation of symptoms. Their participation,however, frequently cannot be determined withcertainty preoperatively. The approach to theseproblems, in the more severe cases, has been surgi-cal removal of the rib, initiated by Coste in i861.25This procedure, although surgically sound, toooften was attended by va'rious complications whichresulted in equally severe symptoms, sometimesworse. Law25 in I920, and Adson and Coffey' inI927, suggested resection of the scalenus anticusmuscle as an easier method of decompression.They found in an impressive series that simpletenotomy was quite effective. Today, scaleno-tomy is performed, with partial resection of therib, if necessary. The precipitating factors in theproduction of symptoms probably are those men-tioned among the contributory factors, since mostpatients do not present symptoms until theyreach the 2o- to 40-year age group.Numerous workers during the past 50 years have
been impressed by the presence of the ' cervicalrib syndrome in the absence of cervical rib.'Observers during the I9O3-I9I7l3 period attributedthese cases to stretching of the brachial plexus overthe first rib due to dropping of the shouldergirdle from an increased lateral diameter of thechest with age. In 1933 Adson suggested thepossible responsibility of the scalenus anticusmuscle and in 1935 the 'scalenus anticus syn-drome' was given its present formulation byNaffziger and Grant,'4 as well as Ochsner, Gageand DeBakey.'5 The basic concept is the de-
duction that, in the presence of a normal shouldergirdle, the scalenus anticus muscle compressesthe neurovascular bundle against the first rib and anormal scalenus medius through a process ofspastic irritability and hypertrophy. Their theoryholds that the scalenus anticus is irritated in somefashion, so bringing about its spasticity, wherebyit compresses the brachial plexus. This compres-sion reflexly increases the spasm of the scalenusanticus. These reactions are believed to producea vicious circle. The corollary, in the thesis of theoriginators, is breaking the circle by sectioning thescalenus anticus muscle.
Diagnosis of a scalenus anticus syndrome wasbased on evidence of a tender scalenus anterior,the dampening of the pulse of the affected extre-mity by certain manoeuvres, especially the Adsonroutine* and the partial relief of symptoms byprocaine injection of the scalenus anticus muscle.'0This clinical formulation was followed by a cycle offavourable reports on the resection of the anteriorscalene muscle. In time, however, subsequentobservers indicated frequent failures. These ledto further critical evaluation, with the elucidationof other mechanisms of the compression. Theinitial concept has been challenged on severalgrounds by many clinicians. Walshe26 feels thatmost of these disorders really are instances of firstrib syndrome. Others hold that the size of thescalenus is variable, that infiltration with procainefrequently spills over and produces a sympatheticblock of the stellate ganglion with a Horner'ssyndrome, or that the solution may even flow overto the brachial plexus with relief of pain. Dampen-ing of the pulse is not regarded as specific. Theabsence of any spasm or change in the similarlyinnervated scalenus medius is thought to remainunexplained by this theory. Finally, the pos-sibility has been suggested that the tenderness isnot definitely indicative of scalenus origin, butmay arise from underlying structures. Thegeneral view of observers today is that the scalenusanticus syndrome, as postulated in the 1930S,remains unproved and that relief of symptoms bysurgical tenotomy is secondary to simple de-compression of the neurovascular bundle. Thisrelief, according to present views, arises from theremoval of one arm of a passive vise, or to thesimpler fact that the patient receives, together withthe surgery, a period of bed rest and change inusual habits. The more severe symptomaticfailures, when restudied, often were found to haveother mechanisms or sources of compression.
*The Adson manoeuvre is carried out with the patientupright and the examiner's fingers on the radial pulse ofthe tested extremity, which is held at the side of thesubject who takes a deep breath and holds it, then turnsthe head to the side tested.
July 1959 FRIEDMAN, ARGYROS and STEINBROCKER: Neurovascular Syndromes 401
Costoclavicular SyndromeIn 1943, Weddel and Falconer5 described the
costoclavicular syndrome. In restudying threecases of scalenotomy failure, they found theprincipal site of compression located between theclavicle and the first rib. They were able todemonstrate that backward and downward bracingof the shoulders, as in the exaggerated militaryposture, would approximate the two bonystructures and compress the neurovascular ele-ments. That this mechanism could occur in anormal shoulder had been appreciated by earlierworkers. It has been reaffirmed by Wright andLordl8 and by Walshe.26
This syndrome was common during the lastWorld War, when heavy packs could not be wornby many men owing to the severe pain, pares-thesias, venous congestion and edemawhichwoulddevelop, due to direct costoclavicular com-pression.5 19 Interestingly, many of these youngsoldiers were able to sustain the packs followingsix to eight weeks of army life and training.'9 Inthe absence of deformities or exogenous factorsthis is not a common syndrome. Walshe, how-ever, cites repetitive costoclavicular compressionas a frequent contributor to symptoms.26 Telfordand Mottershead were unable to demonstratecompression by simple depression of the shoulder,but in their work they do not comment on whetherthey retracted the shoulder as well.23 (The pulsecan be dampened in some 6o per cent. of peopleby an exaggerated military posture.)'9
Hyperabduction SyndromeWright described the mechanism of the hyper-
abduction syndrome in 1945.28 2 In this group ofpatients with clear-cut neurovascular symptoms,mostly of a vascular nature, the principal points ofcompression were found to be under the coracoidprocess and between the clavicle and first rib.The symptoms were demonstrated to occur bylaterally circumducting the arms and claspingthe hands over the head. The neurovascularbundle becomes taut as it crosses the coracoidprocess and the head of the humerus. It is furthercompressed by the clavicle and the muscular actionof the pectoralis minor. Some reduction of thepulse by this manoeuvre has been observed in 6oto 8o per cent. of normal individuals. Theoriginal paper reported on eight patients in whomthe principal factor was this persistent posture insleep.28 Symptoms were relieved by a change inthe habit. Most individuals affected have beenfound to maintain a hyperabducted position of theextremity in sleep, recreational activities or incertain occupations-ballet dancers, painters,grease pit mechanics and others. Subsequentobservations also have shown the presence of
Raynaud's phenomenon in about 50 per cent. ofthe patients. In some cases symptoms includedsuperficial gangrene of the finger tips which healedreadily, when the provocation was eliminated.28'2
Management of Compression SyndromesThe management depends upon the cause and
the severity of symptoms, as well as the majorpoint of compression. Where postural or exo-genous factors play a role, such as pushing, pulling,lifting, carrying heavy objects, etc., simple cor-rections may relieve the symptoms. Whenshoulder drooping is due to poor posture, age andrelated factors, muscle development may beindicated. Physical therapy in the form of heatand the use of analgesics may help resolve residualsoreness of muscles. Structural deformities ofthe bony, muscular or other tissues may requiresurgical decompression. When surgery is per-formed, the current trend is to do a thoroughexploration in order to adequately decompress theneurovascular canal by combined procedures,where necessary-scalenotomy with clavicularremoval; possibly resection of the first rib or ofthe cervical rib; or section of the pectoralis minormuscle in some cases.
The Shoulder-Hand SyndromeNature of the SyndromeThe shoulder-hand syndrome is a reflex neuro-
vascular disorder, often termed ' reflex neuro-vascular dystrophy,' characterized by painfuldisability of the shoulder preceding, accompanyingor following painful disability, vasomotor changes,with swelling, or dystrophic alterations in the laterphases, at the hand and fingers. This conditionis seen largely in the older age groups, in medicaldisorders, arising often from etiologic factors en-countered in the later decades of life. Thesymptom-complex develops in most patients soclosely after external trauma or internal lesions,such as myocardial infarction, that the etiologicrelationship seems obvious. A multiplicity ofdesignations (Table 2), according to the observers'viewpoints, have obscured the clinical similarity ofthe physiologic disturbance and symptoms,whether they originate in external trauma orinternal violence to tissue.
Symptomatology of the Shoulder-Hand SyndromeThe clinical picture has been divided roughly
into three stages (Table 3). In the first phase theessential features consist of pain and disability ofthe shoulder, of insidious or sudden onset, whichfrequently is thought to be a bursitis or peri-arthritis. Usually, a short time after (sometimessimultaneously or before) the appearance of theshoulder symptoms, a sudden or gradual onset of
Post-traumatic trophoneurosisInternal Lesions Post-traumatic vasomotor syndromeChangesinpareticlimbsofhemiplegics Reflex dystrophyNeurotrophic rheumatism Reflex hyperemic deossificationPainful disability of the shoulder (and Reflex sympathetic dystrophy
hand) after coronary occlusion Sudeck's atrophyPost-infarction sclerodactylia Sympathetic trophoneurosisSwollen atrophic hand with cervical Shoulder-hand syndrome
osteoarthritisShoulder-hand syndrome
From the Shoulder-Hand Syndrome: Present Status as a Diagnostic andTherapeutic Entity Medical Ci. N.A., November, 1958.
TABLE 3*CLINICAL EVOLUrION OF THE SHOULDER-HAND SYNDROME
Stage I Stage 2 Stage 3
ShoulderPain Pain and disability resolving or Residual pain infrequentlyDisability in all ranges persistingTenderness, diffuse (localized Possible atrophy of muscles Disability sometimes
early)Osteoporosis, patchy at humeral Osteoporosis, patchy then ground- Ground-glass, diffuse osteoporosishead sometimes glass
Hand and FingersPain Symptoms resolving or continuing Persistent pain, rarely
with earlv dystrophic changesTenderness, diffuse Residual dystrophy and contracturesCutaneous hyperesthesiaDisabilityMassive dorsal swelling Often induration of cutis and
subcutis
Digital ChangesDermal swelling, diffuse Firm induration with obliteration Rarely increased
of dorsal skin creasesSometimes early, shiny cutis and Shiny, trophic skin surface Dull, diffuse atrophy of skin and
trophic changes as in next stage Trophic nail changes initiated subcutissometimes Marked occasionally
Dorsal hypertrichosis sometimes Increased sometimesIncomplete, painful digital flexion Resolving or impending digital Residual contractures and dis-
atrophy and contractures tortions
Vasomotor ChangesVasodilatation or vasospasm Vasospasm often with hyper- Vasomotor imbalance occasionally
hidrosisColour changes Usually absent with dystrophicHyperhidrosis at palms changes
RoentgenographicSpotty osteoporosis of humeral More marked Ground-glass diffuse osteoporosis of
head, wrist humeral head, wrist and fingers
*From the Shoulder-Hand Syndrome: Present Status as a Diagnostic and Therapeutic Entity. Medical Cl. N.A.,November, I958.
July 1959 FRIEDMAN, ARGYROS and STEINBROCKER: Neurovascular Syndromes 403
painful disability of the hand and fingers develops,marked by swelling of the latter, pain on passivemotion of hand joints, loss of skin wrinkles, in-ability to flex the fingers, and often spotty osteo-porosis of the carpus in films. The first stage maylast up to three to six months. It may graduallyresolve, spontaneously, but may progress to thesecond stage. The pain in the shoulder graduallysubsides, the swelling of the hand decreases,possibly with increasingly painful and limitedmobility; sometimes with a Dupuytren-likethickening at the palm, often with coldness of thehand and some degree of dystrophic skin changes.This phase may gradually merge into the finalstage with the production of a ' fibrosed,' distortedhand with contracted fingers, a ' frozen shoulder 'and an impaired extremity. The process maystop anywhere along this line of progression,spontaneously or as a result of treatment.
Etiology and Mechanism of the Shoulder-HandSyndromeThe etiology remains obscure in some 30 per
cent. of our carefully studied cases in which it mustbe classified as ' idiopathic.' Severe or minortrauma to limbs, myocardial infarction, peri-carditis, hemiplegia, cervical osteoarthritis anddisc changes, brain tumours and many internallesions, with neural or segmental connections tothe upper extremity, have been implicated.However, the sequence of events in the manyconditions with which there is a frequent associa-tion suggests a common pathway of production ofsymptoms. The concept most widely held todayis that of a traumatic focus, internal or external,with a channelling of stimulating impulses to thecervico-thoracic spinal cord.
According to this widely regarded theory, thenormal physiology of the ' internuncial pool ' ofneurons at the level of local injury is disturbed.From the site of the lesion through the inter-nuncial communications, along the pathways ofthe autonomic and motor systems, the symptom-producing neurovascular impulses reach the peri-phery of the upper extremity. Once the syn-drome has been produced by the injury or lesion,a self-perpetuating mechanism or ' feedback ' isset up via the afferent, sensory fibers to the inter-nuncial pool with short and long reverberating'closed loop ' relays of neurological impulses inthe 'pool,' which are thought to keep the processgoing until it runs its course. This is one ofseveral, different, helpful working concepts.There are, nevertheless, many unknown facets ofthis group of disorders leaving great room forfurther clarifying observations. Why only a smallgroup of subjects should develop these reflex
symptoms in the presence of injury has not beenexplained.
Both varieties of these neurovascular complexes,the compressive and reflex, may be disabling.The shoulder-hand syndrome tends to become amore serious disorder, because its progressionto a disabled or even a useless extremnity may berapid, and the time for successful interventionshort. The average case of any of the com-pression disorders is apt to be symptomatic overthe course of many years and, in the absence ofsevere injury to vessels leading to thrombosis orembolism, generally does not lead to seriousconsequencies.
Management of the Shoulder-Hand SyndromeMost of the treatment employed until recently
was ineffectual. X-ray therapy to the cervico-thoracic ganglia or to the shoulder and hand,physical modalities, ganglionic blocking agentsand local infiltration of trigger points have beenreported to be helpful in early cases. Gradedexercises within the limits of tolerance un-doubtedly should be initiated at all stages as anadjunct to any form of therapy. Effective earlytreatment is provided by serial stellate ganglionblocks, especially in the first and second stagesoften with complete or satisfactory remissons (andoccasional relapses). With the advent of thecorticosteroids, comparable results have beenobtained with these compounds. A completelyreliable form of treatment still is needed.
PreventionAn important consideration is the prevention of
reflex phenomena, when possible. In conditionsknown to provoke reflex symptoms, such as ex-ternal trauma, myocardial infarction, osteo-arthritic neuropathy, hemiplegia, and others, itmay be useful to introduce mobilizing exercises atthe extremity as soon as practical, also analgesicinfiltration of trigger points. Violent proceduresto extremities presenting any suggestive symptomsare to be avoided. Alertness to early reflexneurovascular symptoms in underlying conditionspredisposing to them should lead to early treat-ment which appears to prevent more severedevelopments.
Differential Diagnosis of NeurovascularDisorders of the Shoulder
Diagnostic evaluation requires a careful historyand physical examination to investigate thecharacteristic pressure points and their features,given under the various headings. Apart fromstandard physical examination, these include in-spection, palpation and postural tests for local
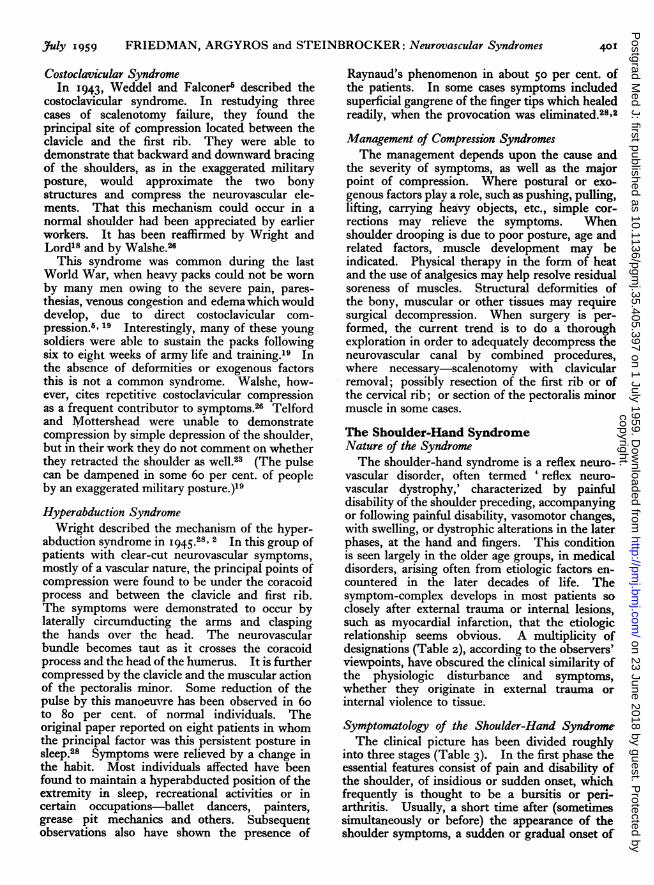
TABLE 4DIAGNOSTIC FEATUREs OF COMPRESSION AND REFLEs NEuRovAscuLAR SYNDROMES OF TH SHOULDER GIRDLE
History Pulse Neurologic Signs Diagnostic Test Therapeutic Response
Costoclavicular Symptoms associated Reduced in abnormal Usually except with Forced abnormal po- Elimination of postu-Syndrome with shoulders forc- shoulder position deformities sition of shoulder ral defects giving re-
ed downward and reproduces signs liefbackward for long and symptomsperiods
Hyperabduction Hyperabduction in Reducedinhyperabd. Often Hyperabduction re- Correction of sleepingSyndrome (Costo- sleep or at work for (also B.P. and oscil- production of signs or working positionclavicular Syndrome) long periods lometry) and symptoms giving relief
Scalenus Anticus No special postural Reduced in resting Reflexes occasionally Adsonmanoeuvremay Correct injection ofSyndrome and Cer- features position or brought reduced on affected reproduce musculo- procaine into ant.vical Rib on by Adson man- side; noted weak- skeletal, neuritic and scalenus may give re-
oeuvre ness in same vascular signs. Ten- lief scalenotomyderpoint at scalenus often effectivearea
Shoulder-Hand Trauma, intrathor- Sometimes reduced Increased or de- Stellate ganglion Repeated blocks orSyndrome (Reflex acic disease or idio- creased reflexes of block produces tran- corticosteroids sym-Dystrophy) pathic, no special part sometimes sient or prolonged pathectomy e#tective
postural features relief in earlier stages
Symptoms common to some or all in each disorder: pain of shoulder, arm and/or hand; numbness, paresthesias of fingers; swelling ofhand(s), fingers; discoloration of hand(s); Raynaud's phenomenon; weakness of hand(s); supraclavicular bruit possible in compression disorders.
compression, cervical ribs, thoracic deformities,bulges or distortions in the supraclavicular area,evidence of vascular disturbance or disease;X-ray films of the cervical spine (with obliqueviews), and of the shoulder and hand, if necessary,as well as special tests where bizarre compressionmay arise from tumour, enlarged lymph nodes,etc. The main differential points are summarizedin Table 4.The compression neurovascular disorders are
the most easily understood from the mechanicalstandpoint. In all of them the production ofsymptoms is secondary to direct mechanicalcompression, of one anatomical variety or another,of the neurovascular bundle somewhere along thecourse of the cervico-axillary canal at the thoracicoutlet, leading to distinctive forms of ' thoracicoutlet syndromes.' The symptoms may arisefrom neural compression (usually the lower cordsof the brachial plexus containing fibers from rootsof C8-Ti) with the production of pain, pares-thesias, hypalgesia or hyperesthesia and atrophyof muscles. Involvement of the vascular com-ponents may cause vasospastic phenomena withclassical Raynaud's manifestations, ulceration,blanching of the skin, boring pain; in arterialcompression, diminution of the pulse, difference inblood pressure, swelling, discoloration, evengangrene; with venous impingement, venous dis-tention and edema. Thrombosis may occur atany time. In most instances removal of thecompression results in eliminating the neuro-vascular symptoms, except where obviously per-manent changes have occurred, as in thrombosis or
embolism. Occasionally, severe vascular or neuralcompression may provoke superimposed reflexsymptoms at the hand or possibly a shoulder-handsyndrome, creating a complex situation for anobserver who has not followed the evolution of theclinical picture. When musculoskeletal or neuro-muscular symptoms predominate, intrinsic dis-orders of the shoulder or neuropathy must bedifferentiated, most frequently cervical disco-genetic or osteoarthritic pathology.The reflex neurovascular disorders, as ex-
emplified by the shoulder-hand syndrome,generally differ characteristically from the com-pression syndromes in causation, manifestationsand therapy. The reflex clinical picture usually issecondary to initial injury, by either internal orexternal trauma, with a reflex neurovascularreaction mediated by a complicated spinal cordreflex. The tissue disturbance tends to be localizedat the shoulder and hand. It is reflected in variousdegrees and combinations of pain, disability,vasomotor fluctuations, swelling, edema, spottyosteoporosis and deforming trophic changes.The shoulder-hand syndrome is more likely tosimulate some form of rheumatic disorder, such asrheumatoid arthritis, bursitis, gout or scleroderma.When it is in mild form, or when neuritic symp-toms are impressive, and especially when thereare localized reflex neurovascular symptoms, as incircumscribed hand involvement, the question ofexcluding compressive neurovascular disorders ismore apt to arise.For references see page 412
The Shoulder-Hand SyndromeThe shoulder-hand syndrome consists of pain,
stiffness and limitation of movement of theshoulder, hand and fingers, and trophic changes inthe skin and other tissues of the hand, followingacute cardiac infarction. The complete picture isuncommon, occurring in less than 5 per cent. ofinfarctions. Some degree of stiffness of one orboth shoulders develops in about io per cent. ofpatients within a month or six weeks of anacute infarction.
In the mildest form of the syndrome, the patientcomplains of slight pain or stiffness on moving thearm. Severe limitation of movement with painshooting down the arm, upwards to the neck anddown the side of the thorax on abduction andlateral rotation is known as a ' frozen shoulder.'In some cases the hand is warm and the fingerspulsate, reflecting vaso-dilation. These changesmay be the forerunners of severe, if uncommontrophic changes, namely swelling of the fingersand hand, stretching of the skin with red-purplediscoloration, trophic ulceration of the fingers orhand, and thickening and contracture of the palmaraponeurosis. The condition in any degree ofseverity except the slightest, may be very resistantto treatment and sometimes the results of monthsof painstaking physiotherapy may be disappoint-ing. Occasionally, all stiffness and pain maydisappear spontaneously within a few weeks.The shoulder-hand syndrome has not been
satisfactorily explained. The changes show atendency to appear in joints which have been theseat of arthritis or peri-arthritis. The left arm isthe more often affected but the right arm is in-volved when the ischaemic pain was right-sided.Protective disuse of the limb is responsible tosome extent, but other factors are involved, too.One of these is a neurovascular reflex mechanism.Pain impulses arising from the heart, reflexly pro-duce muscular spasm and neuro-vascular reac-tions in the ligaments, muscles and skin, innervated
by the eighth cervical to the fourth thoracic spinalsegments.
TreatmentNo special treatment is needed for the pain of
acute infarction referred to the arm. The mildvarieties of the shoulder-hand syndrome usuallyyield to passive and active shoulder and armexercises. The more severe degrees are oftenlong-lasting and resistant to treatment. If theinfarction heals satisfactorily and pain does notrecur, the shoulder stiffness may subside spon-taneously in a few months. Sometimes it maystill cause trouble after a year. In addition tophysiotherapy the various measures used i-ncludeprocaine infiltration around the shoulder joint,steroid therapy, upper thoracic sympathetic blockwith procaine and stellate ganglionectomy. Thesepoints are considered fully in other parts of thissymposium.
SummaryThe typical chest pain of ischaemic heart
disease (angina pectoris and cardiac infarction) isoften transmitted to one or both shoulders andarms. Occasionally, it is felt first in the forearmor arm and spreads upwards to the shoulder andacross the chest. Rarely, it may be confined to thearms. The correct diagnosis may be missed whenthe pain is dominantly in the arms or shoulders.The shoulder-hand syndrome is an uncommon
sequela of acute cardiac infarction. It consists ofstiffness of the shoulder, and in its severe form, ofgreat pain on moving the arm and trophic changesin the hand. The condition may respond onlyslowly to treatment, and may be troublesome formany months after an acute infarction.
BIBLIOGRAPHYHEBERDEN, W. (1772), Med. Trans. Roy. CoU. Phys., 2, 59.HERRICK, J. B. (I9I2), Y. Amer. med. Ass., 59, 2015.
References from page 404- H. Harold Friedman, M.D., Thomas G. Argyros, M.D., and Otto Steinbrocker. M.D.REFERENCES
I. ADSON, A. W., and COFFEY, J. R. (1927): 'Cervical rib,method of anterior approach for relief of symptoms bydivision of scalenus anticus,' Ann. Surg., 85, 839.
2. BEYER, J. A., and WRIGHT, I. S. (I95I): 'The hyper-abduction syndrome with special reference to its relationshipto Raynaud's syndrome,' Circulation (N. Y.), 4, No. 2.
3. EDEN, K. C. (1939): 'The vascular complications of cervicalribs and first thoracic rib abnormalities,' Bnt. _. Surg.,27, III.
4. EDWARDS, E. A., and LEVINE, H. D. (1942): 'Auscultationin the diagnosis of compression of the subclavian artery,'New Eng. J. Med., 247, 79.
5. FALCONER, M. A., and WEDDELL, G. (1943): 'C08to-clavicular compression of the subclavian artery and vein,'Lancet, 245, 539.
6. FALCONER, M. A. (1947): 'The costoclavicular syndrome,'correspondence, Brit. med. J7., July I2.
7. FISKE, L. G. (I952): ' Brachial plexus irritation due to hyper-trophied omohyoid muscle,' J.A.M.A., I49, 758.
8. GAMBLE, S. G. (1gsi): 'Costoclavicular syndrome,' Arch.phys. Med., August, 5x6-522.
9. HAGGERT, G. E. (Igg8): 'Value of conservative managementin cervicobrachial pain,' J.A.M.A., 137, So8-513.
so. JUDOVICH, B., BATES, W., and DRAYTON, W., Jr.(1944): 'Pain in the shoulder and upper extremity due toscalenus anticus syndrome,' Amer. J. Surg., 63, No. 3,March.
i I. LORD, J. W., Jr., and ROSATI, L. M. (5958): ' Neurovascularcompression syndromes of the upper extremity,' Clin. Symp.,10, NO. 2, March-April.
12. MURPHY, J. B. (igos): 'Cervical rib symptoms resemblingsubclavian aneurysm,' Ann. Surg., 4x, 399.
13. MURPHY, T. (I9I0): 'Brachial neuritis from pressure of thefirst rib,' Aust. med. Y., zI, 582-585.
July 1959 JANTET: Staphylococcal Infection in Hospitals 425
associated with a relaxation in aseptic techniques,is responsible for the emergence of and infectionswith, the 'Hospital Staphylococcus': an anti-biotic-resistant strain, apparently more virulentthan its predecessors, liable to cause large-scaleepidemics, extremely well adapted for cross-infec-tion by its ability to survive the most adverseconditions and particularly liable to produce acarrier-state. Its exact mode of spread is stillobscure but direct contact plays an important part.A hospital staphylococcal infection carries thetwofold danger of virulence and antibioticresistance. For this reason the problem is nowas serious as it was in the pre-antibiotic era, withother virulent organisms now replaced by thehospital staphylococcus. The problem is largelypreventable by strict control measures aimed atlimiting the use of antibiotics, and a return tostrict aseptic and cross-infection precautions. Theinfected 'case must be considered as a real sourceof danger to himself and to others.
AcknowledgmentI should like to thank Professor J. B. Kinmonth
for kindly reading this paper and making helpfulcriticisms.
BIBLIOGRAPHYAnnotation (I958), Lancet, if, 1i10.Annotation (1959), Ibid., i, 34.BARBER, M. (i957), in 'Drug Resistance in Micro-organisms,
edited by G. W. Wolstenholme and C. M. O'Connor, London.BRODIE, J., KERR, M. R., and SOMMERVILLE, T. (I956),
Lancet, i, I9.BURNETT, W., McDONALD, S., and TIMBURY, M. C.
(Ig98), Scot. med. 7., 3, 392.
BURNETT, W. E., CASWELL H T, SCHREK, K. M., CAR-RINGTON, E. R., LEARNiR, N., STEEL, H. H., TYSON,R. R., and WRIGHT, W. C. (x958), J. Amer. med. Ass.,566, Ix83.
CASWELL, H. T., SCHREK, K. M., BURNETT, W. E. CAR-RINGTON, E R. LEARNER, N., STEEL, H. H., TYSON,R. R., and WRIGHT, W. C. (I958), Surg. Gynec. Obstet.,I06, I.
CLARKE, S., DALGLEISH, P. G., and GILLEPSIE, W. A.(1952), Lancet, i, 1132.
CLARKE, S. K. R. (I957), Brit. J7. Surg., 44, 592.DINEEN, P., and PEARCE, C. (I958), Surg. Gynec. Obstet.
X06, 453.Editorial (I958), Brit. med. 7., i, 207.Editorial (1958), Lancet, i, SiSGILLEPSIE, W. A., SIMPSON, K., and TOZER, R. (x9S8),
Ibid., ii, I07S.GODFREY, M. E., and SMITH, I. M. (x958), 7. Amer. med. Ass.,
I66, 1197.GOULD, J. C. (I958), Lancet, i, 489.HlARE, R., and RIDLEY, M. (xg58), Brit. med. 7., i, 69.JEFFREY, J. S., and SKLAROFF, S. A. (I958), Lancet, i, 365.KINMONTH, J. B., HARE, R., TRACY, G. D., THOMAS,
C. G. A., MARSH, J. D., andJANTET, G. H. (I958), Brit. med.3'., 2, 407.
LANGMUIR, A. D. (I958), 7. Amer. med. Ass., I66, 1202.Leading Article (I958), Lancet, 1, 250.Leading Article (1958), Ibid., ii, I o6.LOH, W. P., and STREET, R. B. (I957), New Engl. 7. Med.,
256, 177.PETERSDORF, R. G., CURTIN, J. A., HOEPRICK, P. D.,
PEELER, R. N., and BENNETT, I. L. (I957), Ibid., 257, 1001.RAVENHOLT, R. T., and LA VECK, G. D. (1956), Amer. -7.Publ. Hlth, 46, 1287.RAVENHOLT, R. T., WRIGHT, P., and MULHERN, M.
(I957), New Engl. Y. Med., 257, 789.ROBERTSON, H. R. (19S8), Ann. Roy. CoU. Surg., 23, 141.ROWNTREE, P. M., and FREEMAN, B. M. (I95S), Medj.JAust., 2, 157.SHOOTER, R. A. (1958), Ann. Roy. CoU. Surg., 23, 312.SHOOTER, R. A., SMITH, M. A., GRIFFITHS, J. D., BROWN,
M. E. A., WILLIAMS, R. E. O., RIPPON, J. E., andJEVANS, M. P. (I958), Brit. med. ., i, 607.
SHOOTER, R. A., TAYLOR, G. W., ELLIS, G., and ROSS,J. P. (I956), Surg. Gynec. Obstet., 503, 257.
TIMBURY, M. C., WILSON, T. S., HUTCHISON, J. G. P.,and GOVAN, A. D. T. (I958), Lancet, ii, xo8i.
WISE, R. I. (I958), J. Amer. med. Ass., x66, 1178.VWYSHAM, D. N., and KIRBY, W. M. (I9S7), Ibid., I64, 1733.
References continued from page 412-H. Harold Friedman, M.D. Thomas G. Argyros, M.D., and Otto Stienbrocker, M.D.14. NAFFZIGER, H. C., and GRANT, W. T. (1938): 'Neuritis
of the brachial plexus, mechanical in origin: the scalenussyndrome,' Surg. Gynec. Obstet., 67, 722.
J5. OCHSNER, A., GAGE, M., and DEBAKEY, M. (1935):'Scalenus anticus (Naffziger) syndrome,' Amer. Y. Surg.,28, 669.
x6. PAULL, R. (1946): 'The neurovascular syndrome as mani-fested in the upper extremities, Amer. Heart Y., 32, 32.
17. PEET, R., HENRIKSEN, J. D., and ANDERSON, M. G. M.(x956): 'Thoracic outlet syndrome: evaluation of a thera-peutic exercise programme,' Staff Meet. Mayo Clin., May 2.
x8. RAAF, J. (Ig5s): 'Surgery for cervical rib and scalenusanticus syndrome,' Y.A.M.A., 157, 219-223.ig. STAMMERS, F. A. R. (ig5o): 'Pain in the upper limb from
mechanisms in the costoclavicular space,' Lancet, April I.20. STEINBROCKER, O., SPITZER, N., and FRIEDMAN,H. H. (x948): 'The shoulder-hand syndrome in reflex
dystrophy of the upper extremity,' Ann. intern. Med., 29, 22.21. STEINBROCKER, O., and ARGYROS, T. G. (I9S8): 'The
shoulder-hand syndrome: Present status as a diagnostic andtherapeutic entity,' Med. Clin. N. Amer., November.
22. STEINBROCKER, O., NEUSTADT, D., and BOSCH, S. J.(I955): 'Painful shoulder syndromes; their diagnosis andtreatment,' Ibid., 39, No. 2, I.23. TELFORD, E. D., and MOTTERSHEAD, S. (1947): 'The" costoclavicular syndrome,"' Brit. med. J., i, 325-328,March I5.24. THEIS, F. V. (1939): 'Scalenus anticus syndrome and cervicalribs,' Surgery, 6, No. I, I I2-125.25. COOTE and LAW, cited in UPMALIS, I. H. (I958): 'Thescalenus anticus and related syndromes,' Surg. Gynec. Obstet.,with Int. Abstr. Surg., 307, No. 6, December.26. WALSHE, F. M. R. (I95I): 'Nervous and vascular pressuresyndromes of the thoracic inlet and cervico-axillary canal.''Modem Trends in Neurology,' p. 542. Edited by A. Feiling.Butterworth, London.27. WILLSHIRE (I86o): Referred to in clinical records, 'Super-numerary first rib,' Lancet, il, 633.28. WRIGHT, I. S. (I945): 'The neurovascular syndrome pro-duced by hyperabduction of the arms,' Amer. Heart J.,






















![Imaging in Neurovascular conflicts [Neurovascular compression syndrome ]](https://static.documents.pub/doc/80x56/559b6a361a28ab2c188b4611/imaging-in-neurovascular-conflicts-neurovascular-compression-syndrome-.jpg)