si6 NEW AND DEVELOPING TECHNIQUES (ULTRASOUNDS, MR, ECT) I STANDARDIZATION AND QUALITY ASSURANCE 158; ULTRASOUND ATTENUATION AND VELOCITY IMAGING IN THE OS CALCIS: AN IMPROVED METHOD P Laugier, P Giat, P Droin, G Berger. Laboratoire lmagerie ParamBtriiue, URA CNRS 1458, Paris, FRANCE Among the considerable advances in bone densitometry techniques and their clinical applications, the quantitative ultrasonic method has come to be seen as a promising technique. One of the main problem encounteredwhen measuring attenuation coefticient (BUA) or speed of sound (SOS) is related to the heterogeneity of the os calcis and to the sensitivity of the attenuation to small changes in density and structure. So, a high variability of the measurements is related to the transducers positioning. The object of this study was to investigate the possibility of generating ultrasonic images of the attenuation and velocity by scanning the entire os calcis in vitro. A complete assessment of BUA and SOS distributions within the os cakis was made, using an ultrasonic mechanical scanning device with focused transducers. Measurementswere performedon 12 os cakes removed from fresh female cadavers. The bones were examined extensively by scanning both the x and y directions in 1 mm intewals. A value of BUA and SOS were obtained for each position of the transducers and images of the parameter of 70x70 pixels could be processed. To date, we present the first BUA and SOS images of the os calcis. The resolution provided by the focused transducers was approximately 4 or 5 mm in the focal zone. The assessment of the aualitv and Dotential interest of our ultrasonic imaaes was performed by comparison with X-ray computed tomography ( 6 ~ ) . Direct comparison of images obtained with unrasound and CT showed that ultrasonic parametric images of reasonable quality could be reached with focused transducers. As for dual enerov X-rav absomtiometw (DEXA) or quantitative computed tomography, ultr%sound~imagesof the os b k i s give the possibility of controllingthe placement, size and shape of the region of interest and to use multipk measurement sites. DEXA was systematically used to measure the bone mineral density (BMD) of the os cakes. A highly significant correlation between BMD and a local average BUA was found (r= 0.97 p<O.OOl). 1591 BROADBAND ULTRASOUND ATTENUATION (BUA): PRECISION, APPLICATIONS AND CORRELATION WITH PHOTON ABSORPTIOMETRIC METHODS G Economou, J E Adams. Department of Diagnostic Radiology, University of Manchester, UK. Introduction: Broadband Ultrasound Attenuation (BUA) -- is a relatively recent technique used to measure bone mass in the calcaneum. In comparison with the established photon absorptiometric methods BUA equipment is cheap and portable. Most BUA scanners require a waterbath and although compact are not easily carried. A new s c a n n e r (CUBA C l i n i c a l - McCue Ultrasonics) which does not require a waterbath has been assessed. Precision of the measurements and correlations with other bone mineral density techniques have been examined. Subjects and Methods: BUA meaurements were repeated with conventional positioning (n=35) and in 20 patients in the supine position. Precision was calculated as coefficient of variation (CVZ). Patients (n=30) with femoral neck fracture were measured on the ward. Correlation between BUA and other BMD measurements i n 165 women were calculated. Results: BUA scanning was easy, fast and could be performed on the ward with the patient in the supine position. Precision (CV%): a) phantom = 1.5%, b) conventional positioning = 3.9%, c) patients supine = 5 . 1 % . C o r r e l a t i o n s : a ) 3UA v s DXA s p i n e r = 0.554, b) BUA v s DXA f e m o r a l n e c k r = 0 . 5 5 9 , c ) BUA v s SEQCT r = 0.745, d) BUA vs Proximal SPA r = 0.570, e) BUA vs Distal SPA r = 0.526. Conclusions: The measured precision i s less good than that of other established techniques, but acceptable even in a novel position. BUA measures predominantly trabecular bone and the results correlated most closely with SEQCT. BUA shows potential but further studies are needed to establish its use in clinical practice. g SHOULD BUA BE NORMALISED FOR THE WIDTH OF THE CALCANEUS? RJM Herd, GM Blake, CG Miller, I Fogelman. Department of Nuclear Medicine, Guy's Hospital, London, UK. BUA ( u n i t s dB/MHz) representsanintegralmeasurementthrough the calcaneus that is dependent on bone thickness as well as the density of scattering centres. In this study we examined whether the normalisation of BUA for calcaneal width (nBUA: units dB/MHz/mm) improved the discrimination of clinical ultrasoundmeasurements. BUAandcalcanealwidth weremeasuredin200womenusing a contact ultrasound (CUBA) system. nBUA was evaluated by dividing BUA by bone width. There were 150 early postmenopausal subjects (Group1)and 50 osteoporotic women with vertebral fractures (Group 2). Shorttermprecisionwasstudiedusingduplicatemeasurements and evaluated using the root mean squarestandard deviation (RMS SD) and coefficient of variation (CV). The long term precision of the bone wi.dth measurement was studied by repeating the scans after 12months. Theability of BUAand nBUA t o differentiate between women i n Groups 1 and 2 was compared using ROCanalysis. Themean (and standard deviation) were for Group 1 : BUA: 70.2 (14.5) dB/MHz; nBUA: 3.72 (0.91) dB/MHz/mm, and f o r Group 2: BUA: 45.7 (14.6) dB/MHz; nBUA: 2.15 (0.77) dB/MHz/mm. Mean calcaneal width for all 200 women studied was 19.9 (3.6) mm. The short term precision study gave the following figures for RMSSD (CV): BUA:5.8 dB/MHz ( 9 . 1 % ) ; nBUA: 0.41 dB/MHz/mm (12.3%); bone width: 1.66mm (8.3%). Thelyear scans gave a long term precision for bone width of 1.95 mm (9.8%). The areas (and standard errors) under the ROC curves were 0.878 (0.033) for BUA and 0.910 (0.028) for nBUA. Normalisation for bone width increased ROC curve area by 0.033 (0.026). Although not statistikally si.gnificant, theincreaseinROCareaoccurred despitethesubstantialadditionalerrorsintroduced by t h e relatively poor precision of the bone width measurements. This suggests that nBUA should be reevaluated using an ultrasound system with better precision for the calcaneal width measurement than the present CUBA instrument. m THE IMPACT OF BONE SIZE ON BROADBAND ULTRASOUND ATTENUATION Wu CY, Glijer CC, Jergas M, Bendavid E, Genant HK, Quantitative Ultrasound (QUS) is a simple, inexpensive and radiation-free technique to assess skeletal properties that may not be reflected by other bone measurements. Many investigators have usually adopted Broadband Ultrasound Attenuation (BUA) as a parameter in the study of osteoporosis without normalizing to tissue thickness. Previously we have shown in-vitro that BUA increase with bone width in a nonlinear fashion. We carried out two in-vivo studies to investigate whether variations in bone thickness represent a source of accuracy errors of BUA. BUA measurement were obtained on the Walker Sonic UBA 575 (study I) and UBA 575+ (study II) system. For the first study, BUA and an axial radiograph of the calcaneus were obtained in 28 postmenopausal women. BUA and computed tomography (CT) of the heel was performed in another 17 women in the second study. Calcaneal bone width was measured on the radiographs for study I and was obtained from reformatted CT images in study II. BUA in both studies was not significantly associated with the calcaneus bone width although a consistent tend towards a positive correlation was observed ( r2= 0.13 and r 2 = 0.007, p >0.05). BUA increased by approximately 0.5 and 1.7 dB/MHz/mm in the two studies, respectively. Variability in heel width was about f 3 mm in study I and f2.8 mm in study II (1SD). Therefore, the accuracy error due to variability of bone width should be less than 2-5 dBIMHz (3-7%) and represents only a minor source of accuracy errors. Our studies demonstrate that although BUA results depend on the bone dimension, the impact of bone size on BUA in the clinical setting was relatively small. Unless marked variability of calcaneal bone width is encountered (e.g. in pediatric studies), bone thickness does not need to be included in the analysis of BUA values.
Transcript
si6 NEW AND DEVELOPING TECHNIQUES (ULTRASOUNDS, MR, ECT) I STANDARDIZATION AND QUALITY ASSURANCE
158; ULTRASOUND ATTENUATION AND VELOCITY IMAGING IN THE OS CALCIS: AN IMPROVED METHOD
P Laugier, P Giat, P Droin, G Berger. Laboratoire lmagerie ParamBtriiue, URA CNRS 1458, Paris, FRANCE
Among the considerable advances in bone densitometry techniques and their clinical applications, the quantitative ultrasonic method has come to be seen as a promising technique. One of the main problem encountered when measuring attenuation coefticient (BUA) or speed of sound (SOS) is related to the heterogeneity of the os calcis and to the sensitivity of the attenuation to small changes in density and structure. So, a high variability of the measurements is related to the transducers positioning. The object of this study was to investigate the possibility of generating ultrasonic images of the attenuation and velocity by scanning the entire os calcis in vitro. A complete assessment of BUA and SOS distributions within the os cakis was made, using an ultrasonic mechanical scanning device with focused transducers. Measurements were performed on 12 os cakes removed from fresh female cadavers. The bones were examined extensively by scanning both the x and y directions in 1 mm intewals. A value of BUA and SOS were obtained for each position of the transducers and images of the parameter of 70x70 pixels could be processed. To date, we present the first BUA and SOS images of the os calcis. The resolution provided by the focused transducers was approximately 4 or 5 mm in the focal zone. The assessment of the aualitv and Dotential interest of our ultrasonic imaaes was performed by comparison with X-ray computed tomography ( 6 ~ ) . Direct comparison of images obtained with unrasound and CT showed that ultrasonic parametric images of reasonable quality could be reached with focused transducers. As for dual enerov X-rav absomtiometw (DEXA) or quantitative computed tomography, ultr%sound~imagesof the os b k i s give the possibility of controlling the placement, size and shape of the region of interest and to use multipk measurement sites. DEXA was systematically used to measure the bone mineral density (BMD) of the os cakes. A highly significant correlation between BMD and a local average BUA was found (r= 0.97 p<O.OOl).
1591 BROADBAND ULTRASOUND ATTENUATION (BUA): PRECISION, APPLICATIONS AND CORRELATION WITH PHOTON ABSORPTIOMETRIC METHODS
G Economou, J E Adams. Department of Diagnos t i c Radiology, U n i v e r s i t y of Manchester , UK.
I n t r o d u c t i o n : Broadband Ultrasound A t t e n u a t i o n (BUA) -- is a r e l a t i v e l y r e c e n t t echn ique used t o measure bone mass i n t h e calcaneum. I n comparison w i t h t h e e s t a b l i s h e d pho ton a b s o r p t i o m e t r i c methods BUA equipment i s cheap and p o r t a b l e . Most BUA s c a n n e r s r e q u i r e a w a t e r b a t h and a l t h o u g h compact a r e n o t e a s i l y c a r r i e d . A new scanner (CUBA C l i n i c a l - McCue U l t r a s o n i c s ) which does no t r e q u i r e a w a t e r b a t h has been a s s e s s e d . P r e c i s i o n of t h e measurements and c o r r e l a t i o n s w i t h o t h e r bone m i n e r a l d e n s i t y t e c h n i q u e s have been examined.
S u b j e c t s and Methods: BUA meaurements were r e p e a t e d w i t h c o n v e n t i o n a l p o s i t i o n i n g (n=35) and i n 20 p a t i e n t s i n t h e s u p i n e p o s i t i o n . P r e c i s i o n was c a l c u l a t e d a s c o e f f i c i e n t of v a r i a t i o n (CVZ). P a t i e n t s (n=30) wi th femora l neck f r a c t u r e were measured on t h e ward. C o r r e l a t i o n between BUA and o t h e r BMD measurements i n 165 women were c a l c u l a t e d .
R e s u l t s : BUA scann ing was easy , f a s t and cou ld be performed on t h e ward w i t h t h e p a t i e n t i n t h e sup ine p o s i t i o n . P r e c i s i o n (CV%): a ) phantom = 1.5%, b) c o n v e n t i o n a l p o s i t i o n i n g = 3.9%, c ) p a t i e n t s sup ine = 5.1%. C o r r e l a t i o n s : a ) 3UA v s DXA s p i n e r = 0.554, b) BUA v s DXA femora l neck r = 0.559, c ) BUA v s SEQCT r = 0.745, d ) BUA v s Proximal SPA r = 0.570, e ) BUA v s D i s t a l SPA r = 0.526.
Conclusions: The measured p r e c i s i o n i s l e s s good than t h a t of o t h e r e s t a b l i s h e d t echn iques , b u t a c c e p t a b l e even i n a nove l p o s i t i o n . BUA measures predominantly t r a b e c u l a r bone and t h e r e s u l t s c o r r e l a t e d most c l o s e l y wi th SEQCT. BUA shows p o t e n t i a l b u t f u r t h e r s t u d i e s a r e needed t o e s t a b l i s h i t s u s e i n c l i n i c a l p r a c t i c e .
g SHOULD BUA BE NORMALISED FOR THE WIDTH OF THE CALCANEUS? R J M Herd, GM Blake, CG M i l l e r , I Fogelman. Department of Nuclear Medicine, Guy's H o s p i t a l , London, UK.
BUA ( u n i t s dB/MHz) r e p r e s e n t s a n i n t e g r a l m e a s u r e m e n t t h r o u g h t h e c a l c a n e u s t h a t is dependent on bone t h i c k n e s s a s we l l a s t h e d e n s i t y of s c a t t e r i n g c e n t r e s . I n t h i s s t u d y we examined whether t h e n o r m a l i s a t i o n of BUA f o r c a l c a n e a l width (nBUA: u n i t s dB/MHz/mm) improved t h e d i s c r i m i n a t i o n of c l i n i c a l ul t rasoundmeasurements . BUAandca lcanea lwid th weremeasured in200womenus ing a c o n t a c t u l t r asound (CUBA) system. nBUA was eva lua ted by d i v i d i n g BUA by bone width. There were 150 e a r l y postmenopausal s u b j e c t s (Group1)and 50 o s t e o p o r o t i c women wi th v e r t e b r a l f r a c t u r e s (Group 2 ) . S h o r t t e r m p r e c i s i o n w a s s t u d i e d u s i n g d u p l i c a t e m e a s u r e m e n t s and eva lua ted us ing t h e r o o t mean s q u a r e s t a n d a r d d e v i a t i o n (RMS SD) and c o e f f i c i e n t of v a r i a t i o n (CV). The long term p r e c i s i o n of t h e bone wi.dth measurement was s t u d i e d by r e p e a t i n g t h e s c a n s a f t e r 12months. T h e a b i l i t y of BUAand nBUA t o d i f f e r e n t i a t e between women i n Groups 1 and 2 was compared us ing ROCanalysis . Themean (and s t a n d a r d d e v i a t i o n ) were f o r Group 1 : BUA: 70.2 (14.5) dB/MHz; nBUA: 3.72 (0 .91) dB/MHz/mm, and f o r Group 2: BUA: 45.7 (14.6) dB/MHz; nBUA: 2.15 (0.77) dB/MHz/mm. Mean c a l c a n e a l width f o r a l l 200 women s t u d i e d was 19.9 (3.6) mm. The s h o r t term p r e c i s i o n s tudy gave t h e fo l lowing f i g u r e s f o r RMSSD (CV): BUA:5.8 dB/MHz (9 .1%) ; nBUA: 0.41 dB/MHz/mm (12.3%); bone width: 1.66mm (8.3%). T h e l y e a r s c a n s gave a long term p r e c i s i o n f o r bone width of 1.95 mm (9.8%). The a r e a s (and s tandard e r r o r s ) under t h e ROC c u r v e s were 0.878 (0.033) f o r BUA and 0.910 (0.028) f o r nBUA. Normalisat ion f o r bone width i n c r e a s e d ROC c u r v e a r e a by 0.033 (0.026). Although not s t a t i s t i k a l l y s i . g n i f i c a n t , theincreaseinROCareaoccurred d e s p i t e t h e s u b s t a n t i a l a d d i t i o n a l e r r o r s i n t r o d u c e d by t h e r e l a t i v e l y poor p r e c i s i o n of t h e bone width measurements. T h i s s u g g e s t s t h a t nBUA should be r e e v a l u a t e d us ing an u l t rasound system wi th b e t t e r p r e c i s i o n f o r t h e c a l c a n e a l width measurement than t h e p resen t CUBA i n s t r u m e n t .
m THE IMPACT OF BONE SIZE ON BROADBAND ULTRASOUND ATTENUATION Wu CY, Glijer CC, Jergas M, Bendavid E, Genant HK,
Quantitative Ultrasound (QUS) is a simple, inexpensive and radiation-free technique to assess skeletal properties that may not be reflected by other bone measurements. Many investigators have usually adopted Broadband Ultrasound Attenuation (BUA) as a parameter in the study of osteoporosis without normalizing to tissue thickness. Previously we have shown in-vitro that BUA increase with bone width in a nonlinear fashion. We carried out two in-vivo studies to investigate whether variations in bone thickness represent a source of accuracy errors of BUA. BUA measurement were obtained on the Walker Sonic UBA 575 (study I) and UBA 575+ (study II) system. For the first study, BUA and an axial radiograph of the calcaneus were obtained in 28 postmenopausal women. BUA and computed tomography (CT) of the heel was performed in another 17 women in the second study. Calcaneal bone width was measured on the radiographs for study I and was obtained from reformatted CT images in study II. BUA in both studies was not significantly associated with the calcaneus bone width although a consistent tend towards a positive correlation was observed ( r2= 0.13 and r2 = 0.007, p >0.05). BUA increased by approximately 0.5 and 1.7 dB/MHz/mm in the two studies, respectively. Variability in heel width was about f 3 mm in study I and f2.8 mm in study II (1SD). Therefore, the accuracy error due to variability of bone width should be less than 2-5 dBIMHz (3-7%) and represents only a minor source of accuracy errors. Our studies demonstrate that although BUA results depend on the bone dimension, the impact of bone size on BUA in the clinical setting was relatively small. Unless marked variability of calcaneal bone width is encountered (e.g. in pediatric studies), bone thickness does not need to be included in the analysis of BUA values.
New and Developing Techniques (Ultrasounds, MR, ect) /Standardization and Quality Assurance
/621 QUANTITATIVE ULTRASOUND - WHICH PARAMETER TO MEASURE FOR THE ASSESSMENT OF BONE MICROSTRUCTURE?
C.4 . Gluer, C. Y. Wu, M. Jergas, S. A. Goldstein, H. K. Genant Osteoporosis Research Group, Department of Radiology, University of California, San Francisco and Biomechanics, Trauma, and Sports Medicine Laboratory, Section of Orthopaedic Surgery University of Michigan, Ann Arbor
Quantitative Ultrasound (QUS) techniques including either velocity or attenuation measurements are increasingly being used for the assessment of osteoporosis status. We investigated which measurements were associated with parameters of bone structure independent of bone mineral density (BMD). QUS measurements including Ultrasound Velocity through bone (UVB, this velocity parameter solely reflects the "bone component" of the velocity, excluding all soft tissue components), Broadband Ultrasound Attenuation (BUA), and Ultrasound Attenuation in Bone (UAB, defined as mean attenuation at ultrasound frequencies of 200-600 kHz) were obtained on 20 cubes of trabecular bone using a Walker Sonix UBA 575+ scanner. Bone structural parameters including trabecular separation (Tb.Sp), mean intercept length (MIL), and connectivity were based on MicroCT images with appr. 80 pm spatial resolution. Correlations between the QUS parameters were: UVB vs. BUA r=0.33, UVB vs. UAB b0.17, UAB vs. BUA r=0.67. After adjustment for BMD we found associations between Tb.Sp and BUA (partial corr. coeff. pr=-0.32, p<0.05), TbSp and UVB (pr=-0.36, pc0.01), Tb.Sp and both UVB (pr=-0.44, p<0.001) and UAB (pk0.30, p<0.05), MIL and UVB (pk0.36, p<0.005), and connectivity and UAB (pr=-0.33, p<0.05). We found that UVB, BUA and (as a new additional ultrasound parameter) UAB were associated with bone structure independent of BMD. Because of the moderate associations among QUS parameters and their independent associations with bone structure a combined use of velocity and attenuation parameters along with BMD may provide better results for assessment of skeletal status and fracture risk.
1631 DETECTION OF OSTEOPOROSIS BY TIBIAL ULTRASOUND MEASUREMENT AND RESONANT FREQUENCY ANALYSIS. G. Lowet, G. Van &r Perre, P. Geusens, J. Dequeker. Division of Biomechanics and UZ Pellenber; K.U. Leuven, Belgium.
Eighteen osteoporotic female patients were compared to a group of 25 control fet,nales (all in the range of 50 to 8 1 years). For all patients and controls, the ultrasound velocity (UV) in the tibial cortex was determined using a newly developed method. The resonant frequency relating to the first smgle bending vibration of the tibia was measured using a dedicated protocol. The total mineral content (TBMC) in the tibia plus fibula was determined for all subjects from a total body DXA scan. From the resonant frequencies and the bone mineral content, estimations for bendmg stiflkess, bending rigidity and specific bending rigidity (defined as the ratio of bendmg rigidity and the amount of bone material in the cross section of the bone, responsible for that rigidity) were calculated. A small but highly signxficant difFerence was found for the ultrasound velocity (Table 1). This difference was only slightly less significant than that observed for TBMC. Also for the bending rigidity and the bendmg sti&ess a significant difference was observed. The difference for the speclfic bendmg rigidity is small and not sigdicant. This means that the bone material present in the cross section is redistributed over the cross section such that a maximum of bendq rigidity is preserved. It was concluded from a ROC analysis that ultrasound velocity is as efficient as TBMC for the discrimination between both groups, but bendmg rigidity is a much less efficient parameter. Furthermore, these results show that the tibia and the tibial mechanical characteristics are affected by osteoporosis.
Table 1 : megsurement results on 18 osteooorotic oatients and 25 controls,
3c ULTRASOUND OF THE OS CALCIS FOR OSTEOPOROSIS RISK ASSESSMENT COMPARED TO DXA AT OTHER SITES Christian Wfister, Klaus Brandt, Christa Scheidt-Nave, Gudrun Leidig- Bruckner, Wolfgang Paetzold and Reinhwd Ziegler. Dep. lntemal Med. I, University of Heidelberg, Germany
The study objective was to assess reliability and validity of ultrasound (U) for estimation of bone mineral density (8MD) in comparison with dual-X- ray-absorptiometry (DXA) at different sites. As part of a screening for vertebral osteoporosis (OPO), we determined BMD in a randomly selected population sample from a South Westem G~inan community (289 women, 271 men, ages 50-82). BMD was measured with DXA (Hologic QDR 1000, Waltham, USA) at the lumbar spine (LS), the femur (F) and the os calcis (C). Using U of the os calcis (Achilles, Lunar, Madison, WI) BMD was estimated by speed of sound (SOS) and broadband ultrasound attenuation (BUA). Lateral X-rays of lumbar and thoracic spine were performed for radiological diagnosis of prevalent vertebral OPO (2 1 fracture(#)). Receiver operating curves (ROC) analyses were used to determine sensitivity (SE) and specificity (SP) of U in identification of persons at high risk for OPO (LS-z-scores-2 SD) and patients with #. The in vitro and in vivo coefficients of variation were 0.27% and 0.27% for SOS and 0.98% and 1.56% for BUA respectively. SOS and BUA significantly correlated with DXA measures in both sexes at all sites. Hawever the strength of the correlation varied ranging from r4.20 (BUA with LS in men) to r4.64 (SOS with C in women). Due to the size of standard errors of the estimate (SEE) U measures did not permit sufficiently accurate prediction of BMD by DXA. The SE at 90% SP of U regarding identificat'in of persons at hfgh risk for OPO was low at 20%. the diagnostic validity of U was consistently lower in comparison with DXA except C (ROC area 0.7%~ 0.9/0.&410.73 for LSIFIC). We conclude that DXA still seems to be the method of choice in risk assessment for OPO. Prospective shldies will be needed to clarify the role of U in screening.
1651 CORRELATION BETWEEN DXA AND CALCANEUS ULTRA-SOUND DENSITOMETRY. Devoeelaer JP, Van Sante N, Nagant de Deuxchaisnes C. Department of Rheumatology, St-Luc University Hospital, Brussels, Belgium. Ultra-sound (US) broadband attenuation (BUA), and the speed of sound (SOS) in bone have been proposed as an alternative to BMD measurements. We have correlated the BMD of the spine (LS), of the hip and subregions, and of total body BMC measured by DXA (Hologic, Inc) with the results obtained with the Achilles ultra-sound densitometer of the calcaneus (Lunar Corp.) in 34 patients with a large range of lumbar BMD from osteopenia to normal (0.582 to 1.182 g/crn2). The results are summarized in the table. QDR-1000 W BUA P SOS P
(clB/MHZ) (dsec) Lumbar spine BMD 0.78 < 0.001 0.76 < 0.001 Total hip BMD 0.68 < 0.001 0.67 < 0.001 Troch BMD 0.70 < 0.001 0.63 < 0.001 Inter BMD 0.66 < 0.001 0.65 < 0.001 Neck BMD 0.67 < 0.001 0.73 < 0.001 Ward's BMD 0.51 < 0.01 0.66 < 0.001 Total body BMC 0.68 < 0.001 0.51 < 0.01 There is an excellent correlation in the whole group of patients between US of the calcaneus (a purely trabecular bone) and BMD of distant sites of the body with various trabecular contents like LS and the hip or with predominantly cortical bone like total body BMC. When limiting the correlation to patients with a L-BMD (< 0.800 glcmz), the correlation between L-BMD, SOS and BUA was less good (r=0.44 and r=0.20, respectively). For mass screening, U.S. could be used as an alternative to other techniques of bone mass measurements like DXA. A weaker correlation between BUA and L-BMD in osteopenics could suggest that BUA does not represent simply a BMD measurement.
10th Internutionul Bone Densitometiy Workshop
(66 T2' relaxation times of trabecular bone specimens and their relation to bone density and elastic moduli: preliminary results using gradient echo and asymmetric spin echo sequences. Michael Jergas, Sharmila Majumdar, Stephan D Grampp, Joyce H Keyak, David Newitt, Irving Lee, Harry B Skinner, Harry K Genant Department of Radiology and Orthopedic Surgery, University of California San Francisco Relationships between the transverse relaxation rate 1/T2* and bone mineral density have been reported by several authors. The purpose of this study was to determine the relationship between transverse relaxation time T2' within trabecular bone specimens and their ash density or elastic moduli. Methods: T2' times in 2 sets of specimens of trabecular bone from the human tibia were calculated from images in an axial plane (series 1) and in three orthogonal planes (series 2), respectively. The images were obtained on a GE Signa MR scanner using a gradient echo sequence (TR=70 msec) for series 1 (12 specimens, defatted) with TE times of 5, 10, 15, 20 and 25 msec, and an asymmetric spin-echo sequence (TR=300 msec) for series 2 (18 specimens, not defatted) with TE times of 4,8,12,16,20 and 24 msec. Ash weight and elastic moduli E in three planes were determined for all specimens. Results: Series I: The correlation coefficient between l/T2* and ash density was 0.57. A good correlation was found between T2' and the reciprocal ash density ( ~ 0 . 8 8 , pc0.01). The correlation coefficients between ash density and E in three planes ranged from 0.79 to 0.92. A moderate correlation was found between 1F2' and E. A good correlation existed between T2* and E in all planes (r=0.87 to 0.95, p<0.01). Series 7. Correlation coefficients for T2' between the three different planes ranged from 0.52 to 0.7, and were comparable for 1/T2'. Correlation coefficients between 11T2' and ash density of the specimens in ail three planes ranged from 0.57 to 0.83 (pe0.05). Similar relationships were found between T2' and reciprocal ash density. An only moderate correlation was found between 1/T2* and E, and a moderate to good correlation between T2* and 1lE in the different planes. Conclusion: Our results indicate that a relationship between structural and density parameters and T2" exist. It seems possible to obtain information in addition to bone density using MR techniques. The results also indicate that MR sequence, plane of data acquisition and specimen preparation play an important role for assessing bone properties with MR. Further investigations are required to implement proper MR techniques for an assessment of the skeletal status.
COMPARISON OF SPIN-ECHO AND GRADIENT ECHO MAGNETIC RESONANCE IMAGING OF TRABECULAR STRUCTURE
S.Majumdar,D.N.Newitt,M.D.Jergas,A.A.Gies,s.Grampp, J.Keltner.H.K.Genant, Univ. of Calif.,San Francisco, USA.
High resolution magnetic resonance (MR) techniques combined with standard techniques of stereology and texture analysis have recently been proposed as a modality to quantify trabecular structure and assess osteoporosis. In this study we evaluate the relative merits of quantifying trabecular structure using volumetric gradient echo (GE) and spin-echo (SE) MR imaging. Phantom studies were conducted using polyethelene strings with diameters ranging from 312.5 - 825.5 pm and in trabecular bone specimens from human tibiae (-1 cm3). In-plane image resolution ranged from 128 - 150 pm; slice thickness ranged from 128-1000 pm. The images were transfered to a SUN Workstation and image thresholding and boundary detection techniques were used to identify the bone, marrow, and the interface between the two phases. Stereological measures such as the mean intercept length, trabecular width, fractional area of trabecular bone, as well as texture-related parameters such as the fractal dimension were derived. The phantom studies were used to assess the accuracy of measuring absolute dimensions of trabecular structure by these sequences. From phantom studies we found that errors in determing absolute stereological measures such as width and fractional area were -12.5% and 75% respectively in gradient echo images; and -17% and 0.3% respectively in spin-echo images, for a structure with a diameter of 312.5 pm. The magnitude of the errors depended on the size of the structure relative to pixel resolution. From in vitro studies, trabecular wldth, fractional area and fractal dimension as measured from gradient echo images was 27%. 13.5% and 0.6% greater, respectively, than those calculated from spin-echo images.Based on the results of this evaluation, for in vivo quantification of trabecular structure, a fast gradient echo technique combined with texture analysls of the trabecular network is proposed as a feasible technique for assessing trabecular structure.
168 QUANTITATIVE MAGNETIC RESONANCE (QMR) TO ASSESS THE REGIONAL VARIATION IN TRABECULAR BONE OF THE CALCANEUS G ~ugl ielmi l s2, S ~ajumdar l , M ~ergasl, BA ~ i u n t l , HK ~ e n a n t l . Department of ~ a d i o l o ~ ~ l , Universit of California. San Francisco, CA,
Giovanni Rotondo, FG, ITALY. I USA. Department of Radiology , Scientific Institute "CSS", San
The calcaneus is composed primarily of trabecular bone (95%) and has evolved as an impoltant site for assessment of osteoporotic changes and orediction of fracture risk. In order to determine variation of trabecular r - - - - - - bone density we evaluated six normal young volunteers (mean age 33.5 f 6.8 vrsl for in vivo variation of T2* MR relaxation time of different kcations in the calcaneus. Using a 1 . 5 ~ GE Signa, we obtained Quantitative Magnetic Resonance (QMR) sagittal and axial plane images of the calcaneus from which three diierent circular regions of interest (ROI) were defined, and signal intensly (SI) measured. The relaxation rate of 1K2' was measured from the decay of the natural logarithm of the signal intensly [In(SI)] with increasing echo time. Calcaneal bone density was measured using Dual X-ray Absorptiometry (DXA). The mean T2' of bone marrow in the sagittal and axial planes of the calcaneus was 10.26 mlsec f 1.89 (range 7.69-13.30) and 8.08 mlsec f 1 .O1 (range 6.84-9.70) respetiwely. Since the volumes of interest in the sagittal and axial planes were not identical, given the regional variation of T2', the mean difference (-2.18 mlsec) was not unexpected. The measurements of individual short-term precision ranged from 2.20 to 4.37 %CV in the sagittal plane and from 12.11 to 15.70 %CV in the axial plane, depending on the placement of the ROI. There were no significant intra or inter-reader analysis differences for Tp* measurements. For DXA measurements the precision ranges from 0.3 to 2 %CV. The DXA values were all within the normal range with a mean of 0.66 QIC+ f 0.04 and thus the T2' values represent the extent of variation seen within this small range of normal denslies. QMR may be a promising tool for studying trabecular bone in the calcaneus, however, given the regional variation of bone mineral densly and structure at this site, the choice of the ROI is likely to play a major role in establishing the accuracy, precision and overall e f f ' icy of T2' measurements.
El QUANTITATIVE MR IMAGING OF VEWTEBRAL BONE IN THE DIAGNOSIS OF OSTEOPOROSIS
M. Funke. H. Bruhn. R. Vosshenrich, E. Grabbe. Dept. Radiolo@ I. University Goettingen. Germany
Rupolle: The current methodology for diagnosing osteoporosh is mainly based on bone densitometry. This technique allows the estimation of bone mass precisely but does not yield information about bone structure. Quantitative MR Imaging offers a new approach to structural properties of bone non-invaaively. Candous bone has been shown to induce a characteristic reduction of the transverse relaxation time (T2*) due to local magnetic inhomogeneities. The objectives of this work were to explore an appropriate pulse sequence for the reproducible measurement of T2* and to assess its applicability in a clinical setting.
116- MR measurements of the lumbar spine were obtained in 42 healthy subjects (2 1-76 years) and 16 patients with osteoporosis (38-79 years) using a surface coil at 1.5 Tesla (Magnetom SP 63. Fa. Siemens, Erlangen). A specially designed gradient echo pulse sequence (TRs300 ma. TEs9-81 ma, FA=4Oo1 was ueed whlch enables to read out up to sixteen echoes following the excitation pulse. The echo times were fixed according to the phase coherence of fat and water protons. T2* was calculated by fitting the decay curve to the measured signal intensities in the center of L4 assumlng a mo~z~exponential decay.
Radt.: Excellent reproducibility (coefllcient of variation 2.5%) was obtalned when echo times were chosen to account for phase coherence. T2* was related positively to the age of the subjects. Patients with osteoporosis showed a signillcant increase of T2' (19.723.8 ma) compared tothe healthy subjects (13.421.9 ma). These flndings correspond to the rarefication of vertebral trabecular structure. Thus quantitative MR Imaging is able to providing another diagnostic parameter in addition to bone densitometry.
New and Developing Techniques (Ultrasounds, MR, ect) /Standardization and Qualih Assurance
701 STANDARDIZATION OF BONE MINERAL MEASUREMENTS: REVIEW OF THE PRESENT STATE OF THE ART. WA ~alenderl, D ~elsenber~~, P ~ i i e ~ s e ~ ~ e r ~ . l~iemens Medical Systems, Erlangen, Germany. 2~linikum Steglitz, FU Berlin, Germany. 3~iomed. Technik, ETH, Zurich, Switzerland.
Efforts at standardizing bone mineral measurements for different skeletal sites have been started by a number of organizations internationally. We will review the results obtained up to now, with a particular focus on the efforts initiated within the European Community. A key issue has been standardization of spinal bone mineral measurements. The European Spine Phantom (ESP) has undergone several revisions; it is now established as a worldwide standard and has just recently been accepted as an industry standard. This geometrically defined, quasi-anthropomorphic spine phantom will be presented in detail. The ESP is equally suited for DXA and QCT; examples for its use in cross-calibration and quality control will be given. Continuing efforts aim at standardizing bone mineral measurements of the forearm and the hip. The European Forearm Phantom (EFP) and two types of femur phantoms, which are all based on the same technology and tissue- equivalent plastics as the ESP, will be presented. While several tasks have been successfully completed, a lot remains to be done. In particular, cooperation of the manufacturers is requested furtheron as, for example, with respect to evaluation protocols.
171) USE OF THE EUROPEAN SPINE PHANTOM (ESP) FOR CROSS- CALIBRATION OF DXA DENSITOMETRY MEASUREMENTS ON THE PROXIMAL FEMUR: RESULTS IN NORMAL EUROPEAN POPULATIONS. J Reeve, J Pearson, J Dequeker, W Kalender, D Felsenberg, J Adams, DM Reid, P Lips, H Pols, H Kroger, R Perez Cano, F Galan, P Jaeger, C Ribot, P Schneider, M Henley, J Bright Institute of Public Health, U.Forvie Site, CAMBRIDGE CB2 2SR
Thirteen centres obtained 855 valid bone densitometry records in women and 517 in men selected from their normal local populations. Criteria used to exclude subjects included bone disease & risk factors for secondary osteoporosis. Data for Hologic, Lunar & Norland densitometers were expressed as standardized densities (g/cm2) after cross-calibration with the ESP. Reference ranges for these combined populations were derived using linear and quadratic regressions against age for femoral neck (FN) and trochanter (TR). Where necessary, the data were first log transformed. In men FN density decreased at an average rate of 4.5%/decade, whereas in pre-menopausal women it declined at 3.0% and in post-menopausal women at 8.7%/decade (8.0% per 10 years after menopause). TR was better modelled using untransformed data. Pre-menopausal women showed no decline with age whereas men declined at a mean rate which was less then 1/3 that seen in post-menopausal women. For both sites, the reference ranges fitted the data well and when the data for the 3 brands were superimposed on the reference ranges, there was good agreement between the observed and expected numbers of outliers. In women, cross-calibration reduced Hologic/Lunar differences from 15.3 to 1.0% (FN) and from 15.6 to 0.5% (TR). There were however, in both sexes, significant differences between centres in rates of decline in bone density with age and in mean age-adjusted bone density levels.
Hagiwara,S.. van Kuijk,C. University of Caliiomia, San Fransico, Department of Radiibgy, Osteoporosis Research Group
Introduction: Currently the comparison of patient data amng different DXA scanners is complicated, because no universally accepted cross calibration procedure or standard exists. This study was performed under the auspices of the International DXA Standardization Committee to establish appropriate cross calibration parameters. Methods: P.A. - lumbar spine measurements of 100 women,. ages 20-80 years (mean 52.6f 15.98), (range of BMD = 0.4-1.6 g/cm2) were obtained on a Noriand XR26 Mark II, a Lunar DPX-L, and a Hokgii QDR 2000 (in pencil beam mode) densitometer. Area, BMC, and BMD results from the different scanners were compared for all patients. Spine phantoms from all three manufacturers and the European Spine Phantom (ESP) were also scanned on all systems. To achieve universal scanner calibration we used the intercept and sbpe of the patient's correlations and the value of the mMdle vertebra of the ESP as a 'pegging point" in a series standardization formulae, and have expressed the results as sBMD in mgbn2. Results: The correlation of the patients' BMD values was hiihly linear for each of the three scanner pairs (r>0.98). The mean differences of absolute BMD values (L2-L4) were between Hologic and Norland -1.3%, between Hologic and Lunar +I 1.7%, and between Lunar and Norland -12.2%. Mean BMD values of the patient population were 0.972 g/cm2 on the Hologic, 1.100 g/cm2 on the Lunar, and 0.969 gcm2 on the Norland scanner. Most phantom data lay cbse to the patient regressions for all systems. After applying the standardization formulae the mean differences of absolute BMD values were between Hologic and Norland +2.2%, between Holopic and Lunar -2.2%, and between Lunar and Noriand +2.1%. Mean values of the patient population after correction were 1011 mglcm2 on the Hologic, 1009 mglcm2 on the Lunar. and 1011 ~ c m 2 on the Norland scanner. Conclusions: Quantification of diflerences in scanners as determined in this study, and application of appropriate standardization provide the basis for universal DXA calibration.
173) DEVELOPMENT OF A QUALITY ASSURANCE PHANTOM FOR THE ULTRASONIC ASSESSMENT OF BONE M A Whitehead and C M Langton Health Research Centre, Sheffield Hallam University, UK
Three commercial systems are currently available for the ultrasonic assessment of bone. Comparative studies have indicated that these systems do not provide exactly the same broadband ultrasonic attenuation (BUA) results for a given patient. Clinical trials and the collection of normative data are often multicentre and multi-system. The manufacturers supply simple phantoms with their systems but they are essentially qualitative.
There is an ugent need therefore for reference and calibration phantoms to be available for clinical users. The European Community Biomedical and Health Research (Biiomedl) programme is cunently funding the development of a variable, stable and repeatable phantom.
The phantom should have a BUA dynamic range of 20 to 120 dB MHZ-~, be stable with respect to time and water immersion and be able to be manufactured to high performance tolerances.
Previous attempts to manufacture single and two component phantoms have been unsuccessful. Usins comwter aided design (CAD) and stereo-lithography, an openceiporo"s solid with defined struhural parameters representing both type I and type II osteoporosis in cancellous bone has been developed.
10th International Bone Densitometry Workshop
El COMPARISONS BETWEEN BOLOGIC, LUNAR AND NORLAND DUAL- ENERGY X-RAY ABSORPTIMTERS USED FOR WHOLE-BODY BONE MINERAL MEASUREMENTS P To th i l l ' , A Avenel12, D Reid2. Department of Medical Physics , Western General Hosp i t a l , Edinburgh, U . K . ' and C i ty Hosp i t a l , Aberdeen, U . K V 2
DXA has brought high p r e c i s i o n t o t h e measurement o f whole-bone minera l , bu t i t s accuracy i s l e s s we l l de f ined . I t i s necessary t o make assumptions about f a t d i s t r i b u t i o n and t h e s e cannot be v a l i d f o r a l l s u b j e c t s . For some purposes, comparabi l i ty of r e s u l t s from d i f f e r e n t dens i tometers i s a s impor tant a s accuracy. We compared a Hologic QDR-1000W, a Lunar DPX and a Norland XR36. During t h e course o f t h e i n v e s t i g a t i o n , sof tware changes were in t roduced by each manufacturer . A phantom devised by Nord, i n which th i ckness and f a t p ropor t ion can be a l t e r e d , was used. Small dependences of t o t a l BMC on th i ckness and 8 f a t were c o r r e c t e d by new so f tware . BMC was h ighe r than nominal w i th Lunar, lower w i th Hologic. Anomalies o f r e g i o n a l BMC were removed by new sof tware . 11 vo lun tee r s were measured on each machine. The so f tware changes d i d no t a l t e r t h e mean BMC f o r Hologic and Norland, bu t changed i t s f a t dependence. There were h igh c o r r e l a t i o n s of r e s u l t s between ins t ruments , bu t s i g n i f i c a n t d i f f e r e n c e s . To ta l BMC was h i g h e s t f o r Morland, lowest f o r Hologic. There were anomalies of r eg iona l BMC measurements; f o r t runk , Norland>Lunar>Hologic; f o r l e g s , Hologic> Lunar>Norland. P a r t of t h e d i f f e r e n c e may be due t o t h e t h re sho ld used by Hologic, which excludes bones of low BMD, such a s t h e r i b s . For t o t a l BMD, Lunar>Hologic>Norland; t h e bone a rea de f ined by Norland was much h ighe r . S o f t t i s s u e measurements were a l s o d i f f e r e n t . For t o t a l body % f a t , Norland>Lunar>Hologic. The c a l i b r a t i o n s and f a t d i s t r i b u t i o n models used by t h e d i f f e r e n t manufacturers a r e probably too d i s s i m i l a r t o a l low comparabi l i ty .
RATES OF VERTEBRAL BONE LOSS MEASURED USING TWO DIFFERENT MANUFACTURER'S DENSITOMETERS. NFA Peel, R Eastell. Department of Human Metabolism & Clinical Biochemistry, University of Sheffield, Clinical Sciences Centre, Northern General Hospital, Sheffield, UK.
It is unknown whether rates of bone loss measured using different manufacturer's densitometers are comparable. Our aim was to determine whether the rate of bone loss from the lumbar spine (LS) was the same measured using a Lunar DPX and a Hologic QDR 10001'. We measured bone mineral density (BMD) in 17 postmenopausal women at 0 and 2 years. The mean rate of loss of LS-BMD was the same using both densitometers (Lunar. -0.0039 i 0.023 glcm2/year; Hologic, -0.0039 + 0.012 gIcmYyear). The variance of the rate of loss of LS-BMD was greater for Lunar than Hologic (F = 4.1, 95% CI 1.5 to 11.3). We used the approach described by Bland and Altman (Lancet 1986:307) to relate the difference in the rate of loss estimate between the two densitometers to the mean rate of loss ( r = 0.64, P = 0.005). This significant correlation could be explained if the precision error of LS-BMD measurements by Lunar DPX was twice that by Hologic QDR 1000MI. This finding raises concerns about combining results for the rate of bone loss measured using different manufacturer's densitometers in multi-centre studies.
1761 LOCAL DOSE AND EQUIVALENCE DOSE OF 3D-pQCT
W Kaissl, H Keller, B Schaffner, P Ruegsegger. Institute for Biomedical Engineering, University and ETH, Zurich, Switzer- land
Patient exposure is one of the key factors limiting the use of CT equipment, especially in children, in volunteers and for screen- ing purposes. It Is, therefore, mandatory to evaluate the dose distribution if a new CT modality is introduced, such as that of our 35-pQCT-system.
We used TLDs to determine the radiation dose. They were first calibrated with an X-ray source matching the energy spectrum of the CT-system to be evaluated. The TLDs were positioned in a plexiglas-aluminum phantom simulating the soft tissues and bones of a limb. 2D and 3 0 measurements were performed with the same CT settings as for patient examinations. In addi- tion to the measurements we performed Monte-Carlo calcula- tions too. Using the code GEANT we were able to simulate the complete measuring process by following each photon on its way from the X-ray source through ths various collimators, through the patient and into the detectors.
In the 2D case the measurements showed a radiation dose of 0.2 mSv in the hot spot of the scans, the results of the 3D case are dependent on the measuring mode used and range from 0.2 rnSv to 1 rnSv. MC calculations and TLD measurements were well in accordance. Whole body equivalence dose was in the 3D case below 1 ~ S V . Hence, also the 3D-pQCT applica- tion is really low-dose.
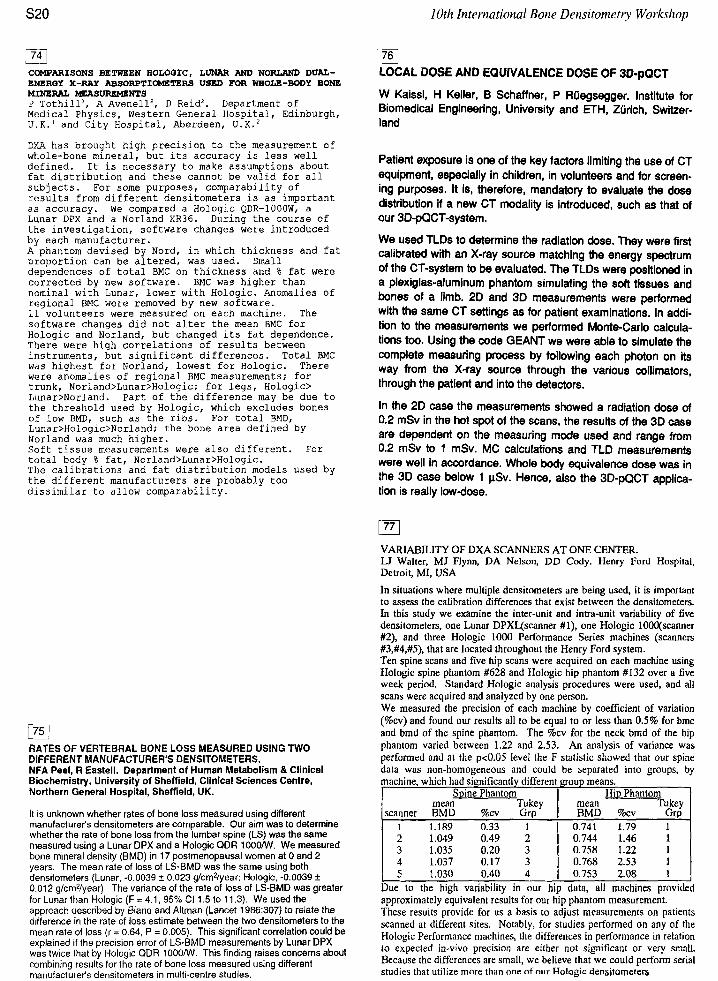
VARIABILITY OF DXA SCANNERS AT ONE CENTER. U Walter, MJ Flynn, DA Nelson, DD Cody. Henry Ford Hospital, Detroit, MI, USA In situations where multiple densitometers are being used, it is important to assess the calibration differences that exist between the densitometers. In this study we examine the inter-unit and intra-unit variability of five densitometers, one Lunar DPXYscanner #I), one Hologic 1000(scanner #2), and three Hologic 1000 Performance Series machines (scanners #3,#4,#5), that are located throughout the Henry Ford system. Ten spine scans and five hip scans were acquired on each machine using Hologic spine phantom #628 and Hologic hip phantom #I32 over a five week period. Standard Hologic analysis procedures were used, and all scans were acquired and analyzed by one person. We measured the precision of each machine by coefficient of variation (%cv) and found our results all to be equal to or less than 0.5% for bmc and bmd of the spine phantom. The %cv for the neck bmd of the hip phantom varied between 1.22 and 2.53. An analysis of variance was performed and at the p<0.05 level the F statistic showed that our spine data was non-homogeneous and could be separated into groups, by
1.049 1 0.744 1.035 0.20 ( 0.758 1.22
4 1.037 0.17 1 0.768 2.53 I 5 1.030 0.40 4 j 0.753 2.08 1 I Due to the high variability in our hip data, all machines provided approximately equivalent results for our hip phantom measurement. These results provide for us a basis to adjust measurements on patients scanned at different sites. Notably, for studies performed on any of the Hologic Performance machines, the differences in performance in relation to expected in-vivo precision are either not significant or very small. Because the differences are small, we believe that we could perform serial studies that utilize more than one of n w Hologic densitometers
New and Developing Techniques (Ultrasounds, MR, ect) /Standardization and Qualio Assurunce
1781 CROSS CALIBRATION OF DXA SYSTEMS WITH AN ANTHROPOMORPHIC SPINE PHANTOM CR Wilson, Medical College of Wisconsin, Milwaukee, WI; M Mahesh, Johns Hopkins, Baltimore, MD. USA.
An anthropomorphic spine phantom has been designed and constructed which closely simulates the in vivo absorptiometric property of the human lumbar spine. The purpose of the phantom(s) is to provide a means of cross calibration of DXA scanners of different manufacturers or DXA scanners of the same manufacturer with different analysis and acquisition software without the necessity of conducting in vivo studies involving large number of subjects. The phantom consists of dried human lumbar vertebrae in which the marrow spaces have been filled with a lipid and collagen mixture which simulates the composition of 50% red and 50% yellow human marrow. The vertebrae are encased in tissue-equivalent epoxy which simulates the radiographic and densitometric properties of soft tissue with a compositioh of 30% adipose and 70% muscle. One lumbar phantom with an areal density of approximately 0.85 g/cm2 has been fabricated. This phantom has been scanned using three DXA systems; a Norland XR26, a Lunar DPX-L and a Hologic QDR 1000/W. Measured BMD values obtained with these three systems were 0.81, 0.95 and 0.82 g/cm2, respectively. The differences in BMD among the scanners are consistent with differences seen in vivo with these three scanners. Two other phantoms of areal density of approx- imately 1.0 and 1.2 g/cm2 are being fabricated. The three phantoms will thus span a range of normal BMD values for 0.8 to 1.2 g/cm2. At the time of the workshop, regression relationships of the phantoms for different DXA scanners will be discussed.
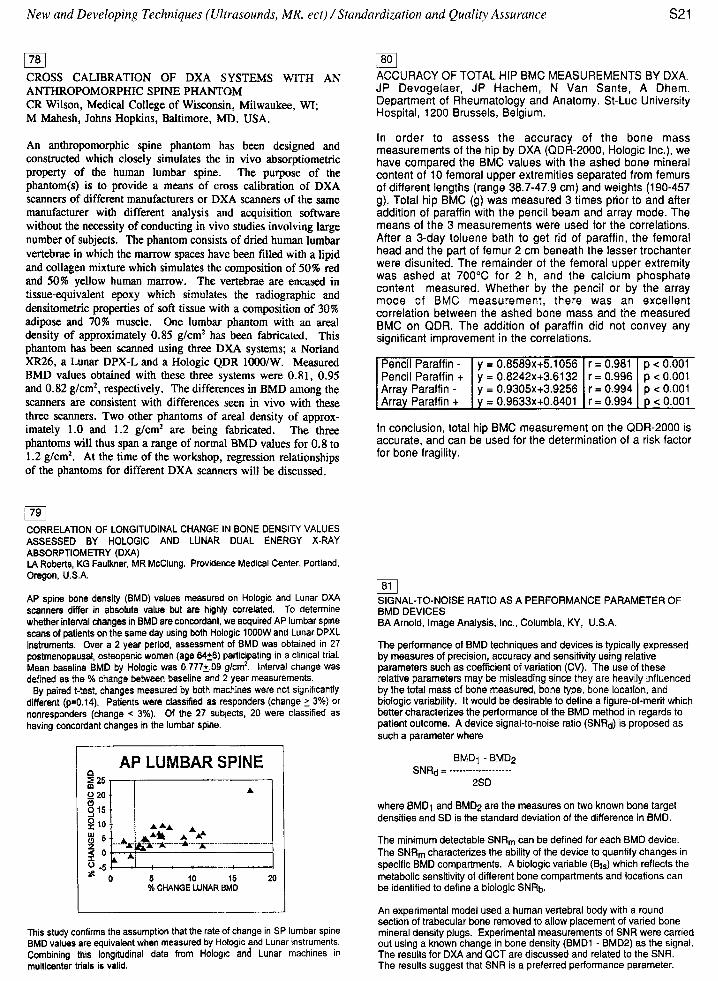
1791 CORRELATION OF LONGITUDINAL CHANGE IN BONE DENSITY VALUES ASSESSED BY HOLOGlC AND LUNAR DUAL ENERGY X-RAY ABSORPTIOMETRY (DXA) LA Roberts, KG Faulkner, MR McClung. Providence Medical Center, Portland, Oregon, USA.
AP spine bone density (BMD) values measured on Hologic and Lunar DXA scanners differ in absolute value but are highly correlated. To determine whether in te~a l changes in BMD are concordant, we acquired AP lumbar spine scans of patients on the same day using both Hologic lOOOW and Lunar DPXL instruments. Over a 2 year period, assessment of BMD was obtained in 27 postmenopausal, osteopenic women (age 6426) participating in a clinical trial. Mean baseline BMD by Hologic was 0.7712.09 glcm2, Interval change was defined as the % change between baseline and 2 year measurements. By paired t-test, changes measured by both machines were not significantly
different (p=0.14). Patients were classified as responders (change 2 3%) or nonresponders (change < 3%). Of the 27 subjects, 20 were classified as having concordant changes in the lumbar spine.
AP LUMBAR SPINE 1
* - 0 5 10 15 20 % CHANGE LUNAR BMD
This study confirms the assumption that the rate of change in SP lumbar spine BMD values are equivalent when measured by Hologic and Lunar instruments. Combining this longitudinal data from Hologic and Lunar machines in multicenter trials is valid.
/801 ACCURACY OF TOTAL HIP BMC MEASUREMENTS BY DXA. JP Devogetaer, JP Hachem, N Van Sante, A Dhem. Department of Rheumatology and Anatomy. St-Luc University Hospital, 1200 Brussels, Belgium.
In order to assess the accuracy of the bone mass measurements of the hip by DXA (QDR-2000, Hologic Inc.), we have compared the BMC values with the ashed bone mineral content of 10 femoral upper extremities separated from femurs of different lengths (range 38.7-47.9 cm) and weights (190-457 g). Total hip BMC (g) was measured 3 times prior to and after addition of paraffin with the pencil beam and array mode. The means of the 3 measurements were used for the correlations. After a 3-day toluene bath to get rid of paraffin, the femoral head and the part of femur 2 cm beneath the lesser trochanter were disunited. The remainder of the femoral upper extremity was ashed at 700•‹C for 2 h, and the calcium phosphate content measured. Whether by the pencil or by the array mode of BMC measurement, there was an excellent correlation between the ashed bone mass and the measured BMC on QDR. The addition of paraffin did not convey any significant improvement in the correlations.
[ ~ r r a i Paraffin + I i = 0.9633x+0.8401 1 r = 0.994 1 < 0.001
In conclusion, total hip BMC measurement on the QDR-2000 is accurate, and can be used for the determination of a risk factor for bone fragility.
1811 SIGNAL-TO-NOISE RATIO AS A PERFORMANCE PARAMETER OF BMD DEVICES BA Arnold, Image Analysis, Inc., Columbia, KY, U.S.A.
y = 0.8589x+5.1056 y = 0.8242x+3.6132 v = 0.9305x+3.9256
r = 0.981 r = 0.996 r = 0.994
The performance of BMD techniques and devices is typically expressed by measures of precision, accuracy and sensitivity using relative parameters such as coefficient of variation (CV). The use of these relative parameters may be misleading since they are heavily influenced by the total mass of bone measured, bone type, bone location, and biologic variability. It would be desirable to define a figure-of-merit which better characterizes the performance of the BMD method in regards to patient outcome. A device signal-to-noise ratio (SNRd) is proposed as such a parameter where
p < 0.001 p < 0.001 D < 0.001
where BMDl and BMD:, are the measures on two known bone target densities and SD is the standard deviation of the difference in BMD.
The minimum detectable SNRm can be defined for each BMD device. The SNR, characterizes the ability of the device to quantify changes in specific BMD compartments. A biologic variable (Bt,) which reflects the metabolic sensitivity of different bone compartments and locations can be identified to define a biologic SNRb.
An experimental model used a human vertebral body with a round section of trabecular bone removed to allow placement of varied bone mineral density plugs. Experimental measurements of SNR were carried out using a known change in bone density (BMD1 - BMD2) as the signal. The results for DXA and QCT are discussed and related to the SNR. The results suggest that SNR is a preferred performance parameter.
10th International Bone Densitomety Workshop
182j ULTRASONIC AND MECHANICAL CHARACTERISATION OF HUMAN VERTEBRAL BONE. P.H.F.Nicholson, ~.~.Haddawa~: M.W.J.Davie. Charles Salt Research Centre and '~e~artment of Diagnostic imaging, Robert Jones and Agnes Hunt Orthopaedic Hospital, Oswestry, Shropshire, UK.
Cubes were prepared from lumbar vertebrae obtained at post-mortem from subjects aged over 50 years. Speed of Sound (SOS) and Broadband Ultrasonic Attenuation (BUA) were measured in the three orthogonal axes (Cranio-Caudal CC, Dorso-Ventral DV, Lateral LT) using a pulse -transmission ultrasoundsystem developed at this centre. Young's modulus (E) was determined in non-destructive mechanical tests in three axes. Apparent density (p) was determined using direct physical methods. Both SOS and BUAvaried significantly between axes (p<0.001), confirming that ultrasound was measuring aspects of bone structure in addition to density. SOS and BUA were greatest in the CC axis (2249tl-124 m.s.', 34.0t1-22.4 d B . ~ ~ i ~ . c m " r e s ~ e c t i v e l ~ ) and least in the LT axis (1 709+/-Il4 m.s-I, 1 OW-6.9 ~B.MHZ-' .cm.'). In individual axes, both SOS and BUA correlated with p (r=0.69-0.97). The data suggested that differences in structure between axes account for 40-50% of the variation in BUA. Anomalous behaviour, suggestive of two distinct transmission paths, was observed in the CC axis. Measurements on the same cubes in air supported this hypothesis. E was greatest in the CC axis (150t1-72 MPa) and least in the LT axis (43tl-40 MPa) (p<O.OOl). Effective moduli (calculated as pS0s2) derived from the ultrasonic data correlated strongly with E in the individual axes (r=0.95-0.98) but were substantially greater in magnitude. E was proportionat approximately to p'.2 in the CC axis, and to p2.0 in AP and LT axes. Thus at low densities, there was a proportionally greater decrease in E in DV and LT axes than in the CC axis. This suggests that structural changes occur with reducing bone density that tend to maintam mechanical competence in the principal load-bearing direction, at the expense of that in other directions.
/831 A BONE-MIMICKING MATERIAL FOR USE IN ULTRASOUND INVESTIGATIONS J.A. Evans, J. Clarke , J. T r u s c o t t and R. M i l n e r . Department o f M e d i c a l Phys ics, U n i v e r s i t y o f Leeds, Leeds, U.K.
The n a t u r e o f u l t r a s o n i c wave p r o p a g a t i o n i n bone con t inues t o b e t h e s u b j e c t o f c o n s i d e r a b l e 'debate. Var ious t h e o r i e s p u r p o r t t o d e s c r i b e t h e u l t r a s o n i c a t t e n t i o n , v e l o c i t y and s c a t t e r and t h e i r f requency dependence i n te rms o f a r c h i t e c t u r a l and mechanica l f e a t u r e s o f bone. Research i n t h i s area has been hampered b y t h e l a c k o f p r a c t i c a l p h y s i c a l models and t h e consequent i n a b i l i t y t o c o n t r o l v a r i a b l e s . I n t h i s paper we d e s c r i b e t h e r e c e n t developments i n t h e p r o d u c t i o n o f a bone-mimicking m a t e r i a l which w i l l f a c i l i t a t e f u t u r e s t u d i e s i n t h i s area. The m a t e r i a l based on a s tandard epoxy r e s i n i s f a b r i c a t e d t o a pre-determined p o r o s i t y v a l u e b y t h e i n c l u s i o n o f a marrow-mimicking substance thereby i n t r o d u c i n g a known and c o n t r o l l e d mean p o r e s i z e . Producing the m a t e r i a l i n t h i s way a l l o w s t h e o p t i o n o f g e n e r a t i n g an i s o t r o p i c o b j e c t o r one w i t h a n i s o t r o p y s i m i l a r t o r e a l c a n c e l l o u s bone.
(841 COMPARISON OF ULTPASOUHD VELOCITY 9rND ATTENUATION WITR BONE MINERAL
DENSITY
J . L . Cunn;nghame, J.N. Fordham and C. Speed.
Department of Rheumatoloqy, Sourh Cleveland Hospital, Mlddlesbraugh and
-School o : Englneerinq and Computer Science, U n l v e ~ s ~ t y of Durham, U.K.
Current methods of detecting lndivlduals wlth Increased rlsk of
sustalnlng an osteoporosis related fracture rely on measurements of bone
mineral denslty IBMDI. It has been shown that there 1 s a 'threshold
valu?' of bone mlneral density below whlch there is an increased risk of
fracture"'. Although bone density 1s an Important determinant of
fracture risk, the archltectuce of bone may also influence fractuce
susceptrblllty. Transmrssion and sttenuatron of ultrasound I" bane have
been proposed as alternatives to radiation based methods for the
quantitative assessment of oste~poros~s'~' and may provide qualltatlve
information about bone structure. In thls study both ultrasound
velocity and attenuation ir bone were enarnlned as alternative
measurements of bone quallty by comparlng ultrasound velocity and
attenuatlon wlth BMU In a group or pre- and post-menopausal female
subjects.
Measurements of ultrasound velocity were performed in the tlbla in a
group of 89 female sublects lage range 2 5 - 7 4 ) . Dual energy X-ray
absorptlometry (DEXAI scans were also performed on all of these sub]ects
enabllng measurements of lumbar spine and femoral neck BMD to be
obtalned. In a small sub-group of 20 sublects, measurenients of tlbial
BMD were also performed. Measurements of broad band ultrasound
attenuation IBUAl of the os-calcis were performed in a separate group of
40 female sublects In which BMD measurements oi the lumbar s p l n e ,
femoral neck and ns-calcls were also obtalned.
Tiblal 8MD and ultrasound velocity were found to be reasonably
correlated lr = 0.711 although both splne and femoral neck BMD were
poorly correlated wlth ultrasound veloclry. For the ultrasound
attenuation measurements, the best corcelatlon was found between lumbar
spine BMD and BUA of the os-calcls. In both studies, lumbar spine and
femoral neck BMD were found to be q u ~ t e closely correlated, wlth a
correlation coefficient, r, of aro~nd 0 . 7 .
/85/ ASSESSING THE VERTEBRAL TRABECULAR NETWORK: CT, MRI AND MECHANICAL STRENGTH TESTS. S.Allein, RLuypaert, E. De Bisschop. 0. Louis, H.Eisendrath. Biomedical MR Unlt, Vrve Universitelt Brussel, BELGIUM
In osteoporosis the biomechanical strength of trabecular bone is intluenced by bone density as well as structure effects. The former can be obtalned using quantitative CT. The latter can be assessed in MRI by measuring T2*, the apparent transverse relaxation time which depends on field Inhomogeneities caused by the difference in susceptibility of bone and surrounding marrow. In this study both measurements are compared with each other and will be compared with the mechanical strength test.
In vitro measurements were made on a set of 9 deaned human vertebrae immersed in physiologic saline and placed in cranlo-caudal position. Bone mineral density (BMD) in mg CaHA/ml was measured by quantitative computed tomography. T2* measurements were made by fitting a single exponential to the signals in 8 gradient echo sagittal images with TE between 12 and 96 ms. Young's modulus of elasticity will be obtalned from compression tests in the verterbrae.
1/T2* was found not to be related to bone mass density on our set of samples, In contrast with previous st~dles[~l. A posslMe explanation of this discrepancy is that, when the vertebrae are placed in cranio-caudal position (the in vivo situation), QCT gives information on the trabeculae that Is not direction-related, while MR gives information on the trabeculae oriented in the transverse direction. A comparison between each technique and the mechanical strength test will also be presented.
[ I ] Majumdar et al, Magn Resin Med 22, 11 1-127 (1991).
New and Developing Techniques (Ultrasounds, MR, ect) /Standardization and Quality Assurance
186/ CORRECTIONS FOR MULTIPLE SCATTER IN COMPTON SCATTER DENSITOMETRY BONE DENSITY MEASUREMENTS M. J. MooneyA, S. S. D. NagaA, R. D. SpellerA, C Kang* and G. J. RoyleA. "Department of Medical Physics, University College London, London. UK.'AEA Technology, Hawel l Laboratory,Oxfordshire, UK.
Compton Scatter Densitometry (CSD) utilises the proportional relationship of Compton scatter intensity to physical density which provides a density measurement (g/cm3) of the required bone tissue unlike absorption techniques which provide an areal density (g/cm2). CSD measurements of bone density can specifically select the trabecular region which has been shown to be a better indicator of osteoporosis. However, the presence of multiple scatter in these measurements imposes a bias which must be corrected. CSD systems have used basic signal processing and multiple scatter
correction factors ( m d ) to remove the bias (Mooney, 1993). The correction factors are calculated for specific measurements us in^ Monte Carlo based computer simulations (Speller & Horrocks. 1988: Moonev. 19931 which are inconvenient for routine use and mav not be , ~ - -
directly appli&ble to the measurement subject. The implementation and optimisation of an supplementary detector
for the monitoring of multiple scatter in real-time during a CSD bone density measurement is presented. Monte Carla based computer simulations have been used to assess the distribution of multiple scatter within a femoral neck measurement site. This information was used to position a collimated detector around the site to monitor the multiple scatter produced during a CSD measurement. Results show a good correlation of the detector readings with
previously calculated mdvalues indicating that these supplementary detector readings could be used as a means of quantifying and hence removing multiple scatter bias.
Mooney M. J. 1993 Ph.0. Thesis, University of London, London, UK. Speller R. D. and Horrocks J. A. 1988 Med. Phys. (15) 707-712
- MEASUREMENT OF CALCANEAL BONE DENSITY BY COMPTON SCATTER DENSITOMETRY. C Kang'. MJ Mooney", RD Speller", GJ RoyleA. 'AEA Technology, Harwell Laboratory, Oxfordshire, UK. " Department of Medical Physics, University College London, UK.
Dual Energy X-ray Absorptiometry (DXA) has become an established technique for the clinical evaluation of bone mineral density, but can only provide an areal density measurement (glcmq. The probability of Compton scatter is determined by the number of scattering sites in the material irradiated which is related to its physical density. Compton Scatter Densitometry (CSD) is able to provide a true volumetric density measurement (glcms) and also to select trabecular or cortical regions of bone.
Our present CSD system consists of two collimated polychromatic x-ray sources diametrically opposed to two collimated Nal(TI) detectors. The finely collimated beams intersect to form a scattering volume of 0.57 cm3, which can be positioned within the trabecular region. The density of the bone within this volume is assessed. The patient couch is motorised and a ten second scout scan is made in two directions to locate the bone position. Measurements on phantoms and bone samples have indicated a measurement precision of 1 % (Mooney. 1993).
The calcaneus is a load-bearing site of predominately trabecular bone and is therefore suitable for studying Osteoporosis. Prospective studies have shown that women with low bone density in the calcaneus are at increased risk of hip fracture (Cummings et al. 1993). The calcaneus also provides ease of access and fast measurement time due to its position and size.
Initial investigations have concentrated on measurements of bone samples and also phantoms consisting of real or simulated bone encased in soft tissue substitute material. The next phase of the study will be to make CSD measurements on volunteers that will be compared to bone mineral density results for the calcaneum obtained by DXA.
References Mooney MJ. Ph.D thesis (University of London, London. UK) 1993 Cummings et al. The Lancet. Vol. 341: 72-89.1993
SOME PRELIMINARY MEAS-TS OF NEONATAL aONE MINERAL USING A RADIATION SENSITIVE CCD CAMERA. JG Truscott, R Milner, MA Smith. Centre for Bone and Body Composition Research, University of Leeds, Leeds, UK.
Babies born prematurely are under mineralised at birth compared to babies born at 40 weeks gestation (term) as most of the mineralisation of the fetal skeleton takes place in the final trimester of pregnancy. Within the group of preterm babies there is a large subgroup of very low birthweight (VLBW) preterm babies who suffer greater risk of compromise due to nutritional insufficiency in utero which is manifested in their more demineralised state. Up to now the available technology has dictated that measurement of bone mineral status immediately after birth could only be carried out on the well infant who could be easily transported. This excludes many premature infants requiring neonatal intensive care until such time as they are stable, by which time ante- and post- natal nutritional influences on mineral status are inextricably linked. Following a successful feasibility study1 we have constructed a prototype instrument capable of measuring bonk mineral in the incubator. Here we report on the calibration of this system and also on some preliminary in vivo measurements made in incubators on the Neonatal Intensive Care Unit at Leeds General Infirmary.
References
1. The use of a radiation sensitive CCD camera system to measure bone mineral content in the neonatal forearm: a feasibility study. JG Truscott, R Milner, S Metcalfe, MA Smith. Phys Med Biol 1992; 37: 1391-1397.
)89) DETERMINATION OF THE BONE MINERAL CONTENT IN THE HEEL BONE USING A GAMMA CAMERA R Jonson, Radiation Physics section, Dept. of
Clinical Physiology, N:a hlvsborgs LInssjukhus, Trollhattan, Sweden
An easy to use and low cost technique for the
determination of the bone mineral content in
the heel bone is described. The technique is
applicable to any gamma camera provided it can be run in the dual window mode. Two small flood
sources with aqueous solutions of Iodine-125
and Technetium-99m is used. The flood sources
are mounted on the outer side of a water-trough
which in turn is placed in close contact with
the collimator of a standard gamma camera. The
patient measurements are carried out with the
foot placed on a perspex rest in the water-
bath. The introduction of the water-bath
extends the common theory behind dual-photon
absorptiometry with the correction for fat. The
measurement time is 15 minutes and the
effective dose less than 10 pSv. Repeated
measurements on 12 healthy volunteers on a period of two months showed a reproducibility
in YiYn of 2.1%.
10th International Bone Densitometry Workshop
/90j IMPROVING MICRODENSITOMETRY OF THE PHALANX. Jan L Grashuis, L de Baat, AW Zwamborn, WTh Trouerbach, Depts. of Exp. Radiology and Med. Informatics, Erasmus University Rotterdam, The Netherlands
In 1984 we published (1) the set-up of a quantitative microdensitometric method to measure the bone mass and the bone mass density of the phalanx. The main constituents of the method were: - 2 (AP and lateral) radiographs were made of the index finger; - an aluminium wedge was photographed as well for calibration
purposes; - optical density was measured at a number of scans with a single
spot densitometer; - a special algorithm was used to measure bone volume in the scans. Since that time a number of changes and improvements were made in the measurement and processing of the optical densities: - the optical densities are measured with a CCD-camera and are fed
directly into a computer (PC); - the measurement of the density of the calibration-wedge is
automated and improved; - the scans of the phalanx are better positioned by means of
determining the mid-line of the phalanx with a contour-detection procedure;
- a number of scans are averaged to diminish noise; - a new procedure was developed to correct for the soft tissue in the
determination of the bone mass; - measured quantities are now expressed in more appropriate units
(bone mass in gram, bone mass density in gramkm3). By this improvements we were able to diminish inter- and intra-individual variation, as well as the systematic errors (accuracy).
m A NEW METHOD FOR THE SCREENING AND THE STUDY OF OSTEOPOROSIS R. Mele, I1 Department of Orthopaedics e Traumathology, Ospedale Civile of Pordenone, Italy.
Early diagnosis of osteoporosis has assumed increasing importance. The author presents a new method for the study of bone density through the use of ultrasounds. The innovation of the system results from absorption dependent measure of ultrasound speed in the metaphysis of the long fingers of the hand. This measure is indicative of the variations of the density and of the structure of the bone tissue, it is also more sensible than speed alone. The anatomical area chosen has revealed to be relevant to the general bone conditions, in particular for spine. The anatomical site allows measurements and good repeatability in absence of artifacts. Once established the reference curve of the absorption dependent measure of US speed values in relation with the age, 160 women aged between 45 and 80 are examined. The correlation with vertebral BMD and bone density measured is satisfactory. The method presented can be utilized both for the screening and for the study of osteoporosis. US define density and bone structure simultaneously; this second element is not taken in to consideration from the densitometry of different methods. Bone structural variations are constant and determining element of osteoporosis, besides they give information about the risk of fracture. In all the cases where, independently from age, the US speed value measured was lower than 1850 m/sec, vertebral fractures were found over the time.
1921 ULTRASOUND VELOCITY IN THE BONE OF THE PATELLA H Franck, M Munz, M Scherrer. Clinic Mayenbad, Bad Waldsee, Germany
Recently, ultrasound has been proposed as a new technique for non-invasively assessing bone. The purpose of this study was to compare the speed of sound (SOS) and its precision in the right and left patella and BMD of the lumbar spine and hip in normals. Furthermore, we looked at the relationship with BMD of the lumbar spine and hip. Methods: The SOS (Osteoson K4, MTO) and BMD (DEXA: Hologic 2000) of 90 healthy subjects between 26 and 76 years were measured. Results: Mean ( * SD) SOS were 2.0669k0.1845 kmls on the right and 2.0699*0.2018 kmls on the left patella. There was no significant (p=0.929) difference between both legs. Consequently, we found a highly significant (r=0.85, pc0.0001) correlation between SOS of right and left patella. Mean BMD of the lumbar spine and hip were 0.9039*0.1380 glcm2 and 0.7362k0.7237 glcm'. There was a highly significant correlation (r=0.682, p<0.0001) between BMD of lumbar spine and hip. No correlation between SOS and BMD of lumbar spine or hip could be found. Conclusion: SOS of the patella is a reproducable technique measuring ultrasound in this region with highly significant bilateral correlations but it seems to reflect different properties of bone densities than BMD of lumbar spine or hip.
1931 ULTRASONIC PREDICTION OF STRUCTURE AND MATERIAL PROPERTIES OF CANCELLOUS BONE C M Langton, C F Njeh, R Hodgskinson', R X Boutinaud, M A Whiiehead, G J Holden, Health Research Centre, Sheffield Hallam University, UK * Department of Biology, University of York, UK
There is an increasing interest in assessing the role of ultrasound in the i d e n t i r i i n and management of osteoporosis. Using ultrasound, we may measure the velocity of sound through bone, or the increase in attenuation with frequency, generally referred as Broadband Ultrasonic Attenuation (BUA). Although velocity measurements have previously been reported in the patella, current interest is concentrated on the calcaneum.
We are currently undertaking theoretical and experimental investigations to determine the exact nature of the relationships between ultrasonic with material and stnrctural parameters of cancellous bone. We have confirmed that velocity vis determined by the expression:
v = E l p where E is the elasticity of the bone and p is the density.
BUA is related to the density and stnrcture of bone, although the exact dependence has not been determined to date. The structure of cancellous bone may be represented in terms of porosity, connectivity and anisotropy, a combination of porosity and connectivity will detekine the permeability. Experimental studies have been undertaken on in-vim bovine and human cancellous bone samples, and on a physical mimic of cancellous bone. This work has ~rovided a valuable insiaht into the dependence of BUA on the material properties of cancelkus bone including stlucture and ultimately the compressive strength.
New and Developing Techniques ( Ultrasounds, MR, ect) /Standardization and Quality Assurance
1941 SKIN MEASUREMENT WITH ULTRASOUND SYSTEM : COMPARISON BETWEEN SKIN THICKNESS AND BONE DENSITY AS A DIAGNOSTIC CRITERIA OF OSTEOPORO- SIS. M.Valente, A.Mancuso, R.DIAngelo, A.L.Araneo, K.Santi, L.Zichella.
Since there is a significant relationship between the skin and bone con- tents of collagen and skin thickness, a specific measurement of OST (skin thickness) offers a methodic of prevention of osteoporosis. The skin thickness measurement by ultrasounds, associated with the patients anamnesis, makes possible to foresee the development of osteoporosis and moreover allows an indirect precox revelation in case of decrease of bone mass. The study aim is the development of a methodic of screening for the di- agnosis of osteoporosis. The working hypothesis belongs from the common onthogenetic origin of bone tissue and skin. Since both the or- ganic systems react to the nearclimateric fall of estrogens with a re- ducted regeneration, the determination of skin thickness should be considered as a parameter for diagnosis and for the therapy to reduction of bone mass. The method of measurement of skin thickness with ul- trasound~, for the rivelation of changes in bone mass, is based on some theories of Loch (1989): skin and bone are organs belonging to meso- derma, the main costituent of connettive tissue is collagen (35% in the corion, 70% in the bone), and their metabolism so as their isthologic structure is essentially influenced by estrogens. Numerous references on literature were done on this theme. We had done pilot studies (5 for patient) on different therapies (CT-Ipriflavon-Fluoride-Eliotherapy- etc.), to value the diagnostic impact on measurements carried out with the new methods.
(951 WHAT IS MEASURED IN WHAT UNITS IN BONE DENSITOMETRY? Jan L. Grashuis, Depts. of Exp. Radiology and Med. Informatics, Erasmus University Rotterdam, The Netherlands
In bone-densitometry various different methods are used, such as (SE- or DE-)QCT. DXA, micmdensitometry on radiographs (QMD), SPA, DPA, etc. Reading through literature on all these methods, it is striking that almost every method uses its own terminology, quantities and units. Terminology: BMD, BMC, BMME, BMMC Units: gram, mm Al, ggg/cm, g/cm2, mm Allmm3, m@ml CaHyAp, etc. Although great parts of this confusing situation can be explained from historical reasons, we will try to propose a more unified terminology with the appropriate units. In fact in an anatomical object (vertebrae, femur, phalanx) we only want to measure the following quantities - the dimensions of the bone in the object of interest; - the mass of the bone; - the mass density of the bone; - some structure parameters of the bone. Of these quantities the dimensions never give rise to confusions, while structure is still an underdevelopped item. In the terminology and units of the other two quantities a large variety is observed which is totally unnecessary. Mass should be expressed in gram and mass density in grarnlcm3. Terms like BMC an others should be avoided because for example: - BMC=Bone Mineral Content; but what do we mean by Content?
And we are not measuring the Mineral part of the bone (that can be done only by chemical analysis), but the bone as it is composed from its constituents;
- BMD=Bone Mineral Density. Confusion arises between the mass density to be measured and the optical density of the X-ray under observation. In Dxa BMD is called an areal density (g/cm2);
- gramlml CaHyAp is not a proper unit but a contamination of the units in which a mass density is expressed and the material used for calibration of the measuring process;
When we are able to agree on a unified terminology in the different measuring methods, it will be easier to compare results of the different methods and discuss the differences between them.
/96/ MASS ATTENUATION COEFFICIENTSr QUANTITIES AND UNITS FOR USE IN BONE MINERAL DETERMINATIONS R Jonson , R a d i a t i o n P h y s i c s s e c t i o n , Dept. o f C l i n i c a l Phys io logy , N:a ~ l v s b o r g s Lanss jukhus , T r o l l h a t t a n , Sweden
The need f o r agreement between d i f f e r e n t methods f o r bone m i n e r a l d e t e r m i n a t i o n becomes more and more a p p a r e n t a s t h e s e d e v i c e s a r e i n c r e a s i n g l y used . The aim o f t h e p r e s e n t paper is t o f a c i l i t a t e agreement on t h e b a s i c c o n s t a n t s and u n i t s used i n bone m i n e r a l d e t e r m i n a t i o n s .
T h e o r e t i c a l l y d e t e r m i n e d mass a t t e n u a t i o n coef - f i c i e n t s f o r d i f f e r e n t bone m i n e r a l s u b s t i t u t e m a t e r i a l s t o g e t h e r w i t h v a l u e s f o r wate r and f a t a r e t a b u l a t e d . The u s e o f h y d r o x y a p a t i t e a s a synonyme f o r bone m i n e r a l is proposed . The a b b r e v i a t i o n BMA (bone m i n e r a l a r e a l mass) is s u g g e s t e d f o r u s e i n c o n j u n c t i o n w i t h t h e u n i t g/cm2. S u g g e s t i o n s a r e a l s o made f o r o t h e r q u a n t i t i e s and u n i t s f o r u s e i n r e p o r t s o f bone m i n e r a l measurements.
1971 ANTHROPOMORPHIC SPINE PHANTOMS FOR DUAL ENERGY X-RAY ABSORPTIOMETRY SYSTEMS M. Mahesh, Johns Hopkins Hospital, Baltimore, MD; CR Wilson, Medical College of Wisconsin, Milwaukee, WI. USA
The dual energy x-ray absorptiometry (DXA) has become the most popular technique in bone densitometry in terms of its increased level of precision, shorteried scan times, low radiation dose, etc. However, a major hindrance to the widespread use of the DXA technique is the non-availability of uniform calibration methodology. Each of the major manufacturers of DXA systems calibrates its system differently. This affects the mobility of patients from site-to-site since the BMD's from one system cannot be readily compared with that of another system. Anthropomorphic spine phantoms are needed because of the nature of the software of the densitometers and the way each handles the region of interest scanned. Anthropomorphic spine phantoms were made out of human cadaveric vertebral bodies. Each of the vertebral bodies was filled with a formulated marrow mix to simulate a healthy adult in the fifth decade. Each of the marrow- filled vertebral bodies was reassembled to form a spine which was then embedded in a known composition of muscle/adipose surroundings. The design and fabrication of anthropomorphic spine phantoms will be discussed in detail in the workshop.
10th International Bone Densitometry Workshop
1981 QtAl.l ' l ' t ' A S S U R A N C E A N D BONE AHSORPTIOMETRY
I\ i l ;~rcl~i~rtdise X, Sabatier .I[', t iotzhi 1'0, Basse B - G R I O
(Croupc de Recherche et d' lnformation sur les Osteoporoses)
\llhcn rnedicirl imaging inis is towards iii I Y I Y ) measurement,
ilssur:lnce ol' quality gains a particular interest : actually, the
wncep ls o f :ICCLI~:IC~. o f precision or of' reproducibi l i ty o f
measurement are fa r f rom the concepts o f contrast, o f f ield
homogeneity or o f sharpness o f the image. Bone absorptiometry
on picture but gives a measuremen(. \Ye describe here how, i n
France. G R I O set-up :I n;~tion:~l quality assurance i n this field.
Assurance quality has been bui l t u p from three projects :
- i11)sorptiornety workshops : they use both theoretical and
pr:~ctic:rl i~ppro;~ches, in order to make physicians aware o f the
dil l icult ies ol'the rneasurenients they perform o r of the l imi ts o f
their c1inic;ll interpretation. 'Through 10 such workshops. more
than 180 physici:rns have been concerned at this time.
- elementary fantoms have been designed i n order to appraise
each fe;~ture ol'al)sorptio~ncters i ~ n d to characterize their limits.
Short i ~ n d long term reproducibil i ty, ;Iccuracy, linearity,
homogeneity, soii tissue elrects are so studied. Such phantoms
;Ire currently circulating through :~l)sorptiometric centers (more
than 20 centers reached at this time). Hydroxyapatite samples
ol'v;~rious quite definite densities are then used i n bl ind studies
to check the quality o f t he measurements.
- relying upon the confidence o f n1e;rsurements within involved
:~hsorp t i i~~net r ic centers, multicentric studies ;ire running.
1991 MONITORING QUALITY ASSURANCE OF DXA
QUALITY ASSURANCE CENTERS
D. Jones, G. H. Besselaar Associates, Princeton, New Jersey, USA
Contract Research Organizations performing clinical studies for pharmaceutical companies utilizing dual energy x-ray absorptiometry (DXA) to measure bone mineral density as a primary efficacy endpoint require the highest standards of excellence from the DXA Quality Assurance Centers. Each Quality Assurance Center must have appropriately trained and certified personnel and established quality control systems in place. Onsite visits by the Contract Research Organization staff must be performed concurrently at established intervals throughout the study period. Additionally, audits of random samplings of DXA study data by the DXA manufacturers, the experts in the field, can compliment audits of the Quality Assurance Center and the Contract Research Organization. Hence, it is necessary to include them in the evaluation process. This expert evaluation would include a review of each Quality Assurance Centers' standard operating procedures (SOPs) and testing the data analysis against the Quality Assurance Centers' SOPs and the manufacturers standards. Quality assurance of DXA bone mineral density study data requires continuous monitoring by the Quality Assurance Centers and Contract Research Organization personnel with results reported promptly to individual study centers, the Contract Research Organization project team, and the pharmaceutical study sponsor.