Page 1
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 1/23
THE CONDITIONAL CASH TRANSFER, INITIATIVE OF THE MDG OFFICE
The Concept Paper
1.0 Introduction
Conditional Cash Transfer (CCT) programmes in general use money as an incentive for
parents to invest in their children’s human capital development, which will enable them to have
capabilities to escape poverty when they reach adulthood. The incentive is conditional upon the
recipient's actions, which may include enrolling children into public schools, getting regular
check-ups at the doctor's office, receiving vaccinations e.t.c.
Although conditional cash transfers (CCTs) are traditionally evaluated in relation to child
schooling and nutrition outcomes, however, there is a growing interest in specifically examining
maternal and reproductive health impacts. Large-scale government CCT programmes are
considered to be a mainstay in social protection and poverty reduction strategies throughout
Central and South America and are increasingly being implemented in Sub-Saharan Africa and
the Middle East (Fiszbein et al. 2009; Handa and Davis 2006; Lagarde, Haines, and Palmer
2007).
In 2010/2011, an operation research project on Cash Transfers (CT) for Safe Motherhood (SM)
led by Interact Worldwide and supported by ODI was set-up with the aim being to provide cashtransfers to vulnerable women to increase their access to, and use of, maternal health services.
The rationale was that such services, i.e. ante-natal care, skilled delivery at birth and post-natal
care, reduce maternal and neonatal mortality and morbidity (Jones et al., 2011).
Ogun State ante-natal CCT-Gbomoro typically conditions the transfer to the poor pregnant
women (recipients) on obtaining ante-natal care, delivery at the health facility, post-natal clinic
attendance and receiving child immunization from birth to nine months.
1.1 Rationale for the Programme
Ogun State in the South-Western Nigeria is one of the 10 states selected to pilot the 2011 CCT
programme. According to the 2006 Core Welfare Indicator Questionnaire (CWIQ) survey
conducted by the National Bureau of Statistics, some indicators as shown in table (1) were
Page 2
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 2/23
identified placing Ogun State in a relatively disadvantaged position in the socio-economic status
of states in the South-West zone.
Table 1: Some Indicators of Ogun State in the South-West Nigeria
S/NO INDICATOR OGUN
STATE
AVERAGE
SOUTH-WEST
ZONE
1. Higher than average dependency ratio 0.8 0.7
2.Higher proportion of households with difficulty satisfying
household food need
28.8 13.1
3. Lower than average Primary School completion rate 13.1 18.7
4. Lower than average access to Secondary School 58.0 69.4
5. Lower than average Secondary School Net Enrollment 53.8 64.9
6. Lower than average Secondary School Completion rate 25.1 39.6
7. Lower than average health access to Medical Services 67.7 73.1
8. Higher than average proportion of household self
classified as poor
70.9 61.4
9. Lower than average birth registration of children under 5 44.5 56.4
Adapted from: South-West Zone Core Welfare Indicators (2006)
The ‘Ogun state MDG status at a glance’ also gives an overview of the performance of the State
in achieving the MDGs from 2006 – 2010 and identified the likelihood of attaining the 2015
targets. The key problem areas identified and challenges highlighted are shown in table 2.
Table 2: Key Problems and Challenges Identified
Page 3
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 3/23
Key problem areas identified Challenges highlighted
• The increasing proportion of people
living below $1 a day and proportionof population in extreme poverty
• Increased maternal mortality ratio
• The prevalence of HIV among
pregnant women
• The prevalence of tuberculosis and
malaria diseases
• The problem of access to basic
sanitation
• Low utilization rate of Health
Facilities for post-natal care (NDHS,2008)
• Increased maternal mortality ratio
• Increasing proportion of the population living
in extreme poverty 29.22 percent as at 2008• Consistent decrease in primary school
completion rate since 2006
• Declining child immunization rate at 62.2
percent as at 2010
• Increasing infant mortality rate from 13 in 2007
to 65 in 2010
• Increasing maternal mortality rate at 245 per
100,000 live birth as at 2009
Adapted from: Ogun MDG Status at a Glance 2006 - 2010
The indicators shown in table (1) support the case for a Food security, Health and Education
oriented CCT programme for Ogun State. While the challenges highlighted in table (2) identify
the focus of the core components of CCT programme in Ogun State. Additional data collected
from the Ministry of Health stated that in Ogun State, as at 2012, the maternal mortality stands at
245/100,000 live births, which is about half of the national average, while infant mortality stands
at 21/1,000 live births. One of the contributory factors to high maternal mortality has been
identified as the level of poverty, which stands at 27% among pregnant women in Ogun State.
In view of the foregoing, Ogun MDG selected ante-natal for pregnant women under health
component for the CCT programme, being the first State in the Country to pioneer the ante-natal
CCT programme.
The following were also highlighted as part of contributory factors for the selection of ante-natal
CCT under health component:
• Since pregnancy and immunization are time bound to 18 – 24 months, it would be possible
to show impact within 21/2 years of commencing the CCT programme.
Page 4
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 4/23
• Ante-natal CCT would involve working closely with health facilities, who keep good
records, which is expected to facilitate effective monitoring and evaluation of the
programme
• No other State in the Country has conducted ante-natal CCT programme - Gbomoro, in
view of this, it is expected that the successful implementation of this component would
bring the State much acclaim.
1.3 Goal of Ogun State Ante-Natal CCT Programme - Gbomoro
The programme aims to achieve MDG goals 5: to improve maternal health and 4: to reduce child
mortality by addressing the problems of poor pregnant and lactating women and child & infant
malnutrition & mortality rates, by way of instigating and increasing regular visits to health
facilities in their areas.
1.4 Objectives of Ogun State Pre-Natal CCT Programme - Gbomoro
1. To increase ANC conducted by skilled attendant at birth from 89.9% in 2008 (NDHS) to
100% in 2014 among pregnant women in the State.
2. To Increase the number of skilled birth deliveries at the health facilities from 71.8% in
2008 (NDHS) to 100% in 2014.
3. To increase the State immunization coverage from 72.28% in 2010 (NICS 2010) to 85%
(recommended national target for routine immunization coverage) in 2014.
4. To increase the infant welfare clinic attendance from 44.2% in 2011 (State routine data)
to 60% in 2014.
Page 5
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 5/23
NDHS: National Demographic Health Survey
NICS: National Immunisation Coverage Survey
2.0 Components of Ante-Natal Conditional Cash Transfer - Gbomoro
In Ogun State, the ante-natal CCT - Gbomoro is based on five (5) main components which are:
• Antenatal care
• Nutritional assessment and care
• Postnatal care/Infant Welfare
• Education
• Women empowerment
The successful implementation of ante-natal CCT-Gbomoro will require that all essential
components of the programme are well captured and clearly articulated. In general, ante-natal
CCT-Gbomoro will share a common basic structure of the following three areas:
i. A cash transfer
ii. A targeting mechanism, and
iii. Conditionality
By targeting the transfers to poor pregnant women, the program will alleviate maternal and
infant mortality and morbidity in Ogun State.
Page 6
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 6/23
2.1 Programme Components
The table below provides a summary of the major components of Ogun State Government (OGSG) ante-natal CCT programme -
Gbomoro
Table 3: Components of Gbomoro
PROGRAMME COMPONENT INITIATIVESEligibility:
- Geographic,
community, and
specific targeting
- Eligibilityassessment
Geographic Geographic
• LGAs that are recognized as having high
population of poor pregnant women in thecommunities
• To be implemented in the 3
senatorial districts of Ogun state
• 3 Local Government Areas per
Senatorial district
Community Community
- Selection based on baseline survey • Sensitisation campaign on CCT
• Use existing Ward DevelopmentCommittees (WDC)
• ToR for WDC
Specific Specific
-Use categorical indicators to selectrecipients (Vulnerability Test)
• Eligibility/VulnerabilityAssessment Questionnaire(E/VAQ)
Score of 5 or more pointsacceptable as vulnerable andeligible for inclusion
Demand Side:
- Recipientsselection
• Use the eligibility criteria • Enrollment screening
Information about the processfor appeal and settlement of
Page 7
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 7/23
- Benefits
• Cash & in-kind
transfers
grievances
• Cash transfer
• In-kind transfer
• Ante-natal heath care
• Free delivery
• Post-natal health care
• Cash transfer of ₦1,000:00 foreach ANC visit (max 6 visits),₦1,000:00 for each PNC visit(max 4 visits), ₦3,000:00 atdelivery and ₦1,000:00 forreferral services in case of
emergency(non-transferable)• Mama kits at on-set of labour
• Purpose-specific handsets
For continuous contact withMedicare agents all throughperiod of participation in theprogramme
Supply Side:
- Selection
• Services provided
• Facility selection criteria
4 PHC/ LGA
Each PHC to serve a group of Communities
• Health talk every month
• Child growth and monitoring
• Free medication
• Family Planning workshops
• Weekly/monthly
• Provision of de-worming tablets
• Vitamins & iron supplements
• Vaccinations
Conditionality• Attend a minimum of 4 ante-natal clinic
(depending on the gestational age)
• Recipients must have institutional delivery (orat least attended to by a skilled birthattendant)
• Attend at least one post-natal appointment 6
weeks after
• Recipients receive incentive of
cash for each attendance
• Mama-kits will be provided at theon-set of labour
• Nutritional items and few items
of clothing for the baby
• Family planning precautions are
Page 8
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 8/23
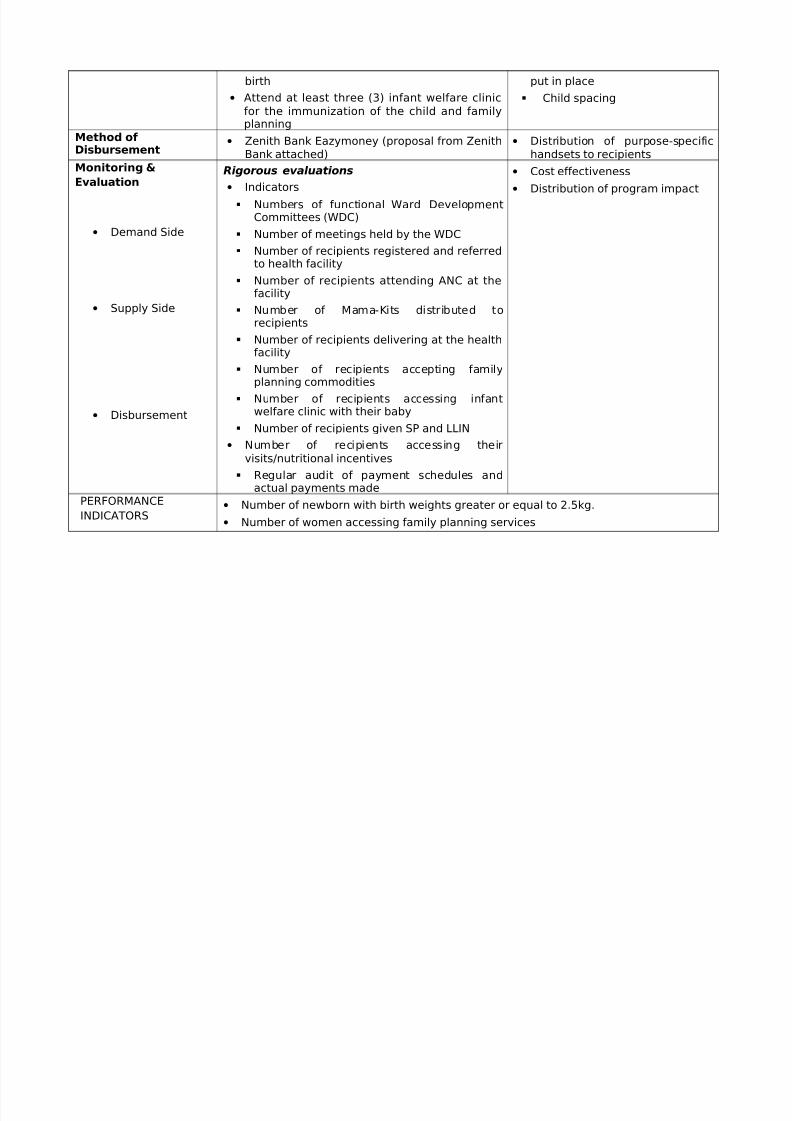
birth
• Attend at least three (3) infant welfare clinic
for the immunization of the child and familyplanning
put in place
Child spacing
Method of Disbursement
• Zenith Bank Eazymoney (proposal from ZenithBank attached)
• Distribution of purpose-specifichandsets to recipients
Monitoring &
Evaluation
• Demand Side
• Supply Side
• Disbursement
Rigorous evaluations
• Indicators
Numbers of functional Ward DevelopmentCommittees (WDC)
Number of meetings held by the WDC
Number of recipients registered and referredto health facility
Number of recipients attending ANC at thefacility
Number of Mama-Kits distributed torecipients
Number of recipients delivering at the healthfacility
Number of recipients accepting familyplanning commodities
Number of recipients accessing infantwelfare clinic with their baby
Number of recipients given SP and LLIN
• Number of recipients accessing their
visits/nutritional incentives
Regular audit of payment schedules andactual payments made
• Cost effectiveness
• Distribution of program impact
PERFORMANCE
INDICATORS• Number of newborn with birth weights greater or equal to 2.5kg.
• Number of women accessing family planning services
Page 9
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 9/23
• Number of women attending ANC services in selected facilities
• Number of infants immunized at 6 weeks of delivery
• Post-partum Vitamin A coverage
• Number of infants with appropriate weight at 6 weeks
KEY STRATEGIC
INITIATIVES• Engagement of traditional/mission/community birth attendants in the selected
community
• Involvement of community-based organizations in the selected localities
• Referrals of complicated cases to secondary facilities
• Enhanced developmental relations between health workers and the recipients
Page 10
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 10/23
Page 11
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 11/23
2.2 Targeting Method and Mechanism
• Method: this refers to the set of rules, criteria, and other elements of programme design
that define recipient eligibility
• Mechanism: refers to the larger elements of program design, including the very
important question of the choice of intermediary agents and organizational design.
2.3 Recipient Selection/ Method of Implementation:
In the implementation process of the ante-natal CCT-Gbomoro, it is imperative that all the
essential components are well captured and clearly articulated to guarantee a holistic approach
and overall success of the project.
2.4 Targeting / Selection
2.4.1 Geographical-based targeting:
Ogun State is divided into three Senatorial districts with 20 LGAs. Three LGAs will be selected
per Senatorial district based on the poverty index and population from the Central Department of
Statistics in the State. The wards will be selected from each LGA, while the State Social Assistance
Committee on CCT (SSAC-CCT) as established by the state shall work hand-in-hand with the selection
committee in each LGA. The LGAs are outlined in table 4 below:
Table 4: Selected LGAs from the three (3) Senatorial Districts
S/N Senatorial Districts LGA
1Ogun Central
Abeokuta South
2 Obafemi Owode
3 Odeda
4Ogun East
Ijebu Ode
5 Ogun Waterside
6 Sagamu
7Ogun West
Ado Odo Ota
8 Ipokia
9 Yewa North
2.4.2 Ward-based targeting:
Page 12
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 12/23
A total of four wards per LGA will be selected for the programme using the following criteria:
• Population of pregnant women
• Poverty index
• Availability of health facilities running 24 hrs service
• Availability of skilled attendants at birth
In view of the foregoing, a total of 36 wards (4 per LGA) will be selected from 9 LGAs
participating in the programme.
2.4.3 Community-based targeting:
Upon selection of the LGAs, the communities will be selected based on the report of the prior-to-
conducted baseline survey in which the following factors will be considered:
• Selection of poor communities with high population of pregnant women, and
• Proximity to health facilities running 24hrs services
Following the selection of communities and in order to provide basic understanding of ante-natal
CCT-Gbomoro at the community level, a sensitization campaign on ante-natal CCT- Gbomoro
will be conducted with the various interest groups in the community. Participants at the
community sensitization are expected to include pregnant women (0-9months), representatives
of organizations and associations in the community. The sensitization will be facilitated by the
health educator from each LGA, the ward focal person and a technical representative from the
State CCT committee. The highlights of the sensitization meeting will include:
• Definition of CCT
• Reasons for CCT
• Who should benefit from CCT?
• The selection criteria for recipients of CCT
• What they will benefit from CCT
Page 13
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 13/23
• What to expect from the facility if qualified for CCT
• Registration modalities for qualified candidates
The existing structure at the community level is such that there are WDC. The WDC will be
given Terms of Reference (ToR) as it applies to the CCT such that there is community ownership
of the programme. The WDC will play a critical role in the validation of the selection of the poor
in their communities and the ToR is given to avoid errors of inclusion or exclusion. The ToR is
to be strictly adhered to and its adherence will be closely monitored by the SSAC-CCT.
The ToR to be given to the committee is outlined as follows:
a. Validation of the selection of recipients (poor pregnant women) in the community
b. Presentation of validated recipients for biometric registration with issuance of ID card
c. Refer registered recipients to the health facility
d. Liaise with the bank vendors and the recipients to confirm the payment of stipends
e. Distribute information packages for the recipients and potential recipients at all times.
f. Hold meeting with health facility officials to review the weakness and areas of adjustment of the scheme.
g. The committee will also play a role in conflict resolution on the scheme
h. The committees will also serve as a watch-dog to prevent affluent pregnant women in the
community from encroaching on the programme.
In the event that there are no existing WDCs in the selected communities, new committee will be
inaugurated to serve the ToR.
Community based targeting is expected to generate better information, better enforcement, and
more positive spillovers. Efforts are geared towards mitigating against the possibility of this
methodology to create costly rent-seeking activities. Emphasis on the need for transparency and
integrity in the recipient selection process will be communicated to the community committees
Page 14
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 14/23
to ensure the enrolment of pregnant women that are truly poor and not a biased selection of
family and friends or selection by political party affiliations.
2.4.4 Household targeting / Eligible pregnant women selection:
Recipients (poor pregnant women) for the programme were firstly selected by the community
leaders and these were then taken through the vulnerability tests (Proxy Means Tests) to finally
validate the women and select the final beneficiaries at the health facilities. The vulnerability
checklist to finalise the selection of recipients is outlined in Table 5 below.
Table 5: Vulnerability Checklist
QUESTIONS Yes = 1 No = 0Does the woman live in a single room, or house with earth/dirt/straw floor or mud/straw/corrugated sheet roofing?
Does she have less than 0.5 hectare of land?
Does she have less than two livestock (cows, sheep or goats)?
Is she illiterate or with education only up to primary school?
Is she often or occasionally having fewer than three meals a day?
Is she or anyone in her household suffering from chronic or regular illness?
Does she have disabled children/husband/household member living withher?
Is she widowed/single/separated/divorced?Does the household have over four dependants? (five or more)
Does each household member have less than two complete sets of clothing?
TOTAL
If the total score for a pregnant woman was five or over, she would be considered eligible to
participate, particularly vulnerable or ‘ultra poor
Page 15
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 15/23
This final screening is done at the weekly recipient enrolment meeting done at the community
level before the pregnant woman can access the facility. At this enrolment the recipient is again
educated on the conditions to benefit fully from the CCT and the various entitlements with every
pre-scheduled visit to the facility as well as the patient flow matrix upon arrival at the facility.
Recipients will in addition be well-informed on their rights and the process of appeal. In this
case, the appeal process will be made quickly in all instances.
3.0 The Conditionalities:
The eligibility criteria to access this incentive will be dependent on a number of factors being
satisfied by the recipient which will be assessed at different milestones in the ante-natal and post
natal periods. These conditionalities include:
a. The recipient must attend a minimum of four ante-natal visits from the end of the third
month to delivery depending on gestational age at enrolment. At each visit, each recipient
will be given a pre-determined amount of money in cash (see table 3 above).
b. They have an institutional delivery, or are at least attended to by a skilled birth attendant:
At the on-set of labour, Mama-kits will be provided free to the recipients as well as post-
delivery package with nutritional items.
c. They attend at least one post-natal appointment six weeks after birth: This is a critical
part of the incentive provision as it ensures all necessary family planning precautions are
put in place for child spacing as multiple deliveries without adequate spacing also puts
the mothers at risk.
Page 16
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 16/23
d. They attend at least three infant welfare appointment for immunization, health talk, food
demonstration and growth monitoring
3.1 Access to Facility/Supply-Side Incentives
The facility selection process in each LGA and community will be carried out based on the
following:
a. Located in or relatively close to a highly populated rural area
b. A facility that has an existing institutional arrangement such as an ongoing Midwives Service
Scheme operating
c. Recently refurbished by the State/ LGA
The two major areas that require policy focus at the facility level are:
i. Service delivery, and
ii. Incentives for service providers.
3.2 Service delivery:
In the area of service delivery it is essential to ensure ease of navigation of recipients and that the
service providers are well-trained in the various areas that compliment service delivery. The flow
of service delivery relevant to the components of the ante-natal CCT-Gbomoro is as follows:
3.2.1 Ante-natal care:
The recipients upon arrival at the health facility will undergo the following:
a. Validation at entry to the facility by health workers (Nurse/Midwife).
b. Registration on each visit (ANC, Delivery and Post natal care) to the health facility.
c. The recipient is then allowed to see a health worker for the following:
i. Blood pressure
ii. Temperature
iii. Weight
iv. Height
v. Pulse rate
d. She then proceeds to have the health education talk on the following:
i. Nutrition
Page 17
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 17/23
ii. Hygiene
iii. Malaria prevention,
iv. Identification of danger signs in pregnancy
v. Signs of on-set of labor
vi. Exclusive breastfeeding
vii. Immunization
viii. Cord Care
ix. Family planning
e. She will then go to have her physical examination. This includes examination for
i. Anaemia
ii. Oedema
iii. Breast lumps or swellings
iv. Fundal height
v. Position of the foetus
vi. Presentation of the foetus
vii. Fetal heart beat
f. Her next booking could be for delivery Prescription of routine drugs
g. She then presents the prescription to the pharmacy where she obtains her free drugs.
h. She receives IPT and TT injection when necessary
i. She is booked for her next appointment and given a clearance for payment with the bank’s
agents.
j. She is referred to payment point by the attending midwife / nurse
Page 18
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 18/23
k. She then gets paid by the bank’s agent and drops a copy of her next appointment date with
the agent.
3.2.2 Nutritional care:
Nutritional care consists of:
a. Nutritional assessment
b. Provision of nutritional supplements (Folic acid and Iron folate)
c. Nutritional advice
d. Food Demonstration
3.2.3 Delivery:
a. Validation at entry to the facility by health workers (Midwife)
b. Examination and admission of the pregnant woman
c. Collection of mama kits on admission for labour d. Monitoring of the progression of labour till child birth
e. Delivery taken by a skilled attendant at birth
f. Initiation of breastfeeding
g. Administration of vaccines (BCG, HBV0 and OPV0)
h. Notification of the bank’s agent for payment by health worker
i. Appointment for post natal visit for the mother and first immunization visit for the child
j. In the event of complications e.g. bleeding, anti shock garment is worn to stabilize the patient
prior to referral to the secondary health facility.
3.2.4 Post Natal care:
a. Validation at entry to the facility by health workers (Nurse/Midwife)
b. Registration on Post natal care (PNC) visit to the health facility
c. The recipient is allowed to see a health worker for:
i. Blood pressure
ii. Temperature
iii. Weight
iv. Pulse rate
d. Recipient proceeds to have the health education talks on the following:i. Nutrition
ii. Hygiene
iii. Malaria prevention,
iv. Exclusive breastfeeding
Page 19
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 19/23
v. Immunization
vi. Family planning
vii. Management of diarrhea
e. During post-natal clinic, food demonstration sessions on preparation of locally madefoods for weaning of the child
f. Recipient goes to have the following physical examination:
i. Anaemia
ii. Oedema
iii. Vaginal discharge / lochia
iv. Breast lumps
v. Uterus retraction
vi. Any abnormalities (head circumference) in the baby
vii. Any nutritional deficiencies (weight and length) in the baby
viii. Prescription of necessary drugs
ix. Administration of Vitamin A for the recipient
g. Recipient takes the child for first dose of vaccination (OPV1 and Penta1)
h. Recipient is referred to family planning unit for family planning counseling and possible
uptake.
i. Recipient is booked for her next appointment and given a clearance for payment with the
bank’s agents.
j. Recipient is referred to payment point by the attending midwife / nurse
k. Recipient gets paid by the bank’s agent and drops a copy of her next appointment date
with the agent
l. Recipient will attend three more infant welfare clinics to enable the child complete his/
her immunization schedule as stated in the national immunization guidelines.
m. Recipient will be paid upon fulfillment of the conditions stated in (l) above.
3.3 Payment Disbursement Method
Page 20
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 20/23
Upon selection by the community, the recipient is referred to the health facility where validation
of eligibility will be done. The recipient is then registered at the facility and will be clustered to
be serviced by a particular bank vendor. There will be about 20 recipients clustered around a
bank vendor and about five bank vendors in a health facility. Upon registration at the facility the
schedule of visits of each pregnant woman i.e. number of ante-natal visits, tentative delivery date
and post natal visit dates will be compiled and sent to the operating bank. A PIN will be sent to
the recipients by the bank a day to the visit or early in the morning of the visit which will be
confirmed by the bank vendor before payment. This is to make disbursement evidenced- based
and fraud-proof.
Table 6: Benefits Package for CCT-Gbomoro Recipients
S/N Interventions
Cost per poor
pregnant woman
(₦)
1 Cash Transfer during ANC visit (at least 6 visits) @ 500/visit 3,000.00
2 Cash Transfer at Delivery 2,000.00
3 Nutritional supplements during ANC visits (at least 6 visits) @500/visit
3,000.00
4 Nutritional supplements at Delivery 1,000.005 Nutritional supplements during PNC (at 4 visits) @ 2,000/visit 4,000.00
6 Cost of Food demonstration at ANC visits (at least 6 visits) @250/visit
1,500.00
7 Cost of Mama Kits given at delivery 5,000.008 Cost of Oxytocin and other ANC drugs (Folic acid, heamatics
etc)1,000
9 Cost of De-worming at 2nd and/or 3rd trimester @ N250/trimester 50010. Referral Services @ N1,000/pregnant woman 1,000.0011. Provision of mobile phone for emergency services and cash
transfer alert3,000.00
TOTAL 25,000.00*** Find attached the proposal from Zenith Bank on disbursement of funds
4.0 Monitoring and Evaluation
Monitoring and Evaluation of the ante-natal Conditional Cash Transfer will be co-ordinated by
MDGs’ Office in Ogun State. Monitoring will be carried out by the non-governmental
Page 21
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 21/23
organizations (NGOs) in the SSAC-CCT set up by the State with assistance from MDGs’ Office.
The ante-natal CCT-Gbomoro will be monitored in three areas as follows:
a. Demand
b. Supply, and
c. Disbursement
Evaluation will be conducted by MDGs’ Office twice in the course of the programme (mid-term
and end-process).
Below are indicators to be used for monitoring selected LGAs
4.1 Demand level monitoring indicators
i. Numbers of functional ward development committees
ii. Number of meetings held by the ward development committees
iii. Number of recipients registered and referred to the health facility
4.2 Supply level monitoring indicators
i. Number of recipients attending ANC at the facility
ii. Number of mama kits distributed to recipients
iii. Number of recipients delivering at the health facility
iv. Number of recipients accepting family planning commodities
v. Number of recipients accessing infant welfare clinic with their baby
vi. Number of recipients given SP and LLIN
4.3 Disbursement level monitoring
Number of recipients accessing their visits/nutritional stipends
4.4 Overall programme indicators (Key Performance Indicators (KPI))
i. Number of newborn with birth weights greater or equal to 2.5kg
ii. Number of women accessing family planning services
iii. Number of women attending ANC services in selected facilities.iv. Number of infants immunized at 6 weeks of delivery
v. Post –partum vitamin A coverage
vi. Number of infants with appropriate weight at 6 weeks
4.5 Collection of Data
Page 22
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 22/23
M & E data will be collected from the following three sources;
i. The community
ii. The health facility, and
iii. The bank
M & E data collection tool will be designed and applied to the three sources while the analysis of
data collected will be done manually using the designed tool. There will be monthly rendition of
data collected at the three sources while there will be quarterly review of the data collected from
the MDGs’ Office.
5.0 Coordination of the Programme
The programme shall be coordinated at the three levels:
i. State level
ii. LGA level, and
iii. Community/Facility level
5.1 State level coordination:
At the State level, the programme is coordinated by MDGs’ Office through the SSAC-CCT and
the Technical working committee.
i. The SSAC-CCT shall give directions as to how the programme will be run. They shall give
advice on the best way the programme will be more beneficial to the people based on their
monitoring and reports from the programme implementation agency.
ii. The implementing agency shall be Ogun State Primary Healthcare Development Board
(OGPHECADEB), an agency in the Ministry of Health
iii. The programme technical working committee shall see to the day-to-day running of the
programme. They shall en-list most suitable recipients to the programme and ensure thatthe total programme packages are delivered to the recipients.
5.2 LGA level coordination:
The LGA coordination shall consist mainly of:
i. Supervision of the health workers at the facilities on the programme implementation
Page 23
8/22/2019 New CCT 2 2 new
http://slidepdf.com/reader/full/new-cct-2-2-new 23/23
ii. Serve as guide to the state monitoring team
iii. Responsible for data collation for the state MDGs’ office
5.3 Community/Facility level:
The health workers at the various facilities where the programme is being implemented shall:
i. Keep records of ANC attendance and deliveries of the recipients. They also ensure that the
in-kind benefits of the recipients are delivered to them when due.
ii. They shall also notify the LGA and the State of any emergency or special intervention e.g.
referral as it may deem fit for any recipient.
5.4 Key Strategic Initiatives
a. Engagement of traditional/mission/community birth attendants in the selected community
b. Involvement of community-based organizations in the selected communities
c. Enhance interpersonal communication between health workers and recipients
d. Referrals of complicated cases to a secondary facility
i. Who is eligible? This will be determined by the attending midwife based on laid
down guidelines and standard operating procedures for management of obstetrics
emergency
ii. Mode of referral: Arrangement will be made with the Ward development committees
on prompt transportation of eligible recipients to the accredited referral/secondaryfacility.