Page 1
© Copyright 2012 Oregon State University. All Rights Reserved
Drug Use Research & Management Program
Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079
Phone 503-947-5220 | Fax 503-947-1119
1
NewDrugEvaluation:Linaclotide
Month/YearofReview:November,2012 Enddateofliteraturesearch:November,2012GenericName:Linaclotide DrugClass:ProsecretoryGastrointestinalAgentBrandName(Manufacturer):Linzess®(ForestLaboratories,Inc.;IronwoodPharmaceuticals,Inc.) FDAApprovedIndication:Treatmentofirritablebowelsyndromewithconstipation(IBS‐C)andforthetreatmentofchronicidiopathicconstipation(CIC).1 ResearchQuestions:• Islinaclotidemoreeffectivethanlubiprostone,laxatives,orothernon‐pharmacologicalagentsforthereductionofconstipationsymptomsinIBS‐CandCIC?• Islinaclotidebettertoleratedthanlubiprostone,theonlyotheragentthatisFDAapprovedforbothnon‐emergencyIBS‐CandCIC?• Aretherespecificpopulationsforwhichlinaclotideisbettertoleratedormoreeffective?Conclusions:• ThereisamoderatelevelofevidencethatlinaclotidereducessymptomsofconstipationandpainassociatedwithCICandIBS‐C.Thereisinsufficient
evidencetodeterminewhetherlinaclotideimprovesclinicaloutcomesassociatedwithhealthrelatedqualityoflife.• TherearenocomparativeanalysespublishedtodatetodetermineiflinaclotideismoreeffectiveorbettertoleratedthanlubiprostoneforCICandIBS‐C.• Itisunknownatthistimewhetherlinaclotidehasthepotentialtocausethedevelopmentofanti‐linaclotideantibodiesandcross‐reactionwithendogenous
peptides.• Thereisinsufficientevidencetomakeconclusionsofanyimprovedefficacyorsafetyoflinaclotideinspecificsubpopulations.Recommendations:• IBSandconstipationarebelowtheOregonHealthPlanlineontheprioritizedlist.IncludepriorauthorizationtocoverforonlyOHPcovereddiagnoses.Background:Irritablebowelsyndrome(IBS)isagastrointestinaldisordercharacterizedbyabdominalpainanddiscomfortthatisaccompaniedbyalteredbowelhabits.2TheconditionisthemostfrequentlydiagnosedGIdisorderwithaprevalenceof10‐15%ofthepopulationinNorthAmerica.3Upto50%ofallvisitstothe
Page 2
2
gastroenterologistareforIBS,withfemalepopulationspredominatingataratioof2:1comparedtomales.WhileyoungerpatientsandwomenaremorelikelytobediagnosedwithIBS,thedisorderaffectsbothsexesandallagegroups.Patientsmaydescribeaconstellationofsymptomsrangingfromcrampingpain,diarrhea,alternatingdiarrheaandconstipation,andperiodsofnormalbowelhabitsinterspersedwitheitherconstipationordiarrhea.Bloodinthestool,nocturnaldiarrhea,greasystoolsorlargevolumediarrheaarenotassociatedwithIBSandindicatefurtherinvestigationiswarrantedtoisolateanorganiccause.2,3IrritablebowelsyndromewithconstipationisasubsetofIBSthataffectsapproximatelyonethirdofallIBSpatients.4SymptomsthataccompanyIBS‐Cincludeabdominalbloating,hardstools,straining,andasensationofincompleteevacuation.2,4HistoricalagentsforthetreatmentofIBS‐CincludedTegaserod,a5‐HT4partialagonistthatwasremovedfromthemarketin2007followingincreasedcardiovasculareventsrelatedtothemedication;itisnowonlyavailableasaprokineticagentonanemergencyINDbasis.TheonlyotherapprovedagentintheU.S.forthetreatmentofIBS‐Cislubiprostone,anE1prostaglandinanaloguechloridechannelactivatorthatincreaseschloridetransport,intestinalfluidsecretionandintestinalmotility.4However,lubiprostoneisonlyapprovedforadult,femalepatientswithIBS‐C.Themostcommonsideeffectfromlubiprostoneisnausea,withanoveralldose‐relatedincidencerangingfrom7to29%.5Lubiprostoneisalsoapprovedforthetreatmentofchronicidiopathicconstipation(CIC),aconditionthatisseparatefromIBS‐C.ThesymptomsofchronicidiopathicconstipationaresimilartoIBS‐C,i.e.bloating,strainingduringdefecation,hardstools,abdominaldiscomfort,andasenseofincompleteevacuation.2,6,7Chronicidiopathicconstipationismoreprevalentinfemales,olderindividuals,andindividualsoflowereconomicstatusorlowereducationallevel.7,8Theestimatedprevalenceofthedisorderrangesfrom4‐20%,basedoncross‐sectionalsurveysofU.S.andEuropeanpopulations.8CICbydefinitionhasnoknowncause,andisnotassociatedwithneurologicormetabolicdisorders,lesionsoftheGItract,ordisorderssuchasdiabetesoranorexianervosa.ConstipationisthehallmarksymptomthatissharedbetweenIBS‐CandCIC.InsightintotheplacementofpharmacologicaltherapyintothetreatmentalgorithmforconstipationmaybegleanedfromprucaloprideguidanceprovidedbyNICE.9AlthoughprucaloprideisnotavailableintheU.S.,theguidancesuggestsastepwiseapproachtothetreatmentofconstipationbeforepharmacologictherapyisconsidered.Firstlineoptionsfortreatingconstipationshouldfocusonlifestyleanddietarymodifications;shortcoursesoflaxativesmaybeadministeredifdietaryandlifestylemodificationsfail.A2005systematicreviewsupportstheuseofspecificlaxativesinastepwisefashionafterfirstlineoptions,citingadequatehydration,increasedfiberintake,andnonstrenuousexerciseasinitialrecommendationsfortreatingconstipation.10Reviewersanalyzeddatafromrandomizedtrialscomparingnon‐pharmacologicalagentstoplacebo.Theauthorsconcludedthatgoodevidenceexistedtosupportadditionaltherapywithpolyethyleneglycolforthetreatmentofchronicconstipation(GradeA).Moderateevidencesupportedtheuseofpsylliumandlactulose(GradeB).Therewasinsufficientevidencetosupporttheuseofbisacodyl,senna,milkofmagnesia,orstoolsoftenersforchronicconstipation.Patientswhodonotrespondtolifestylemodificationsornon‐pharmacologicaltreatmentofIBS‐CandCICmaywishtoaugmenttherapywithpharmacologicaloptions.Linaclotideisanewmedicationthatwillbecomeavailableinthe4thquarterof2012asanadditionaltreatmentoptionforbothIBS‐CandCIC.1Theagentisasynthetic,14‐aminoacidpeptidethatisstructurallyrelatedtoendogenousguanylinpeptides.ThedrugbindstoandactivatestheguanylatecyclaseCreceptorontheluminalsurfaceofintestinalepithelium.Oncebound,activationofthereceptorcausesanincreaseinbothintracellularandextracellularcGMPlevels.Withinintestinalepithelialcells,increasesincGMPinitiateasignal‐transductioncascadethatactivatesthecysticfibrosistransmembraneconductanceregulator.Ultimately,thiscausessecretionofchlorideandbicarbonateintotheintestinallumen,leadingtoincreasedluminalfluidsecretionandacceleratedintestinaltransit.FDAapproveddosingincludeslinaclotide290mcgforirritablebowelsyndromewithconstipation,whilethe145mcgdoseisindicatedfor
Page 3
3
chronicidiopathicconstipation.1ApproveddoseshavebeenmodifiedtoreflectpotenciesdeterminedthroughanalyticalanalysisduringproductdevelopmentanddifferslightlyfromthedosesreportedinphaseIItrials.12
ClinicalEfficacy:
Atotalof4PhaseIII,randomized,placebocontrolled,parallelgroup,multicentertrialshavebeenpublishedthatevaluatetheefficacyoflinaclotideinthetreatmentofchronicidiopathicconstipationandirritablebowelsyndromewithconstipation.4,6,11AllstudiesevaluatedtheclinicalefficacyandsafetyoflinaclotideinthetreatmentofCICorIBS‐C.BaselinedemographiccharacteristicsintheCICtrialsweresimilarandwell‐matched;baselinedemographicsintheIBS‐CtrialsweresimilarexceptforsexintrialMCP‐103‐302,whichhadahigherproportionofmalesintheplaceboarm(p=0.038).Baselineclinicalcharacteristicsweresimilarinalltrialswiththeexceptionofabdominalfullness(P=0.011),stoolconsistency(P=0.046)andstraining(P=0.020)inIBS‐CtrialLIN‐MD‐31.Patientsinalltrialswerepredominantlywhite,female,underage65,andwithameanagerangeof43to49years.Efficacydatawasevaluatedforallprimaryendpointsat12weeksbasedonintention‐to‐treatpopulationswhoreportedatleastonepost‐randomization,completespontaneousbowelmovement(CSBM).Forallstudies,patientswereallowedtocontinueastable,continuousregimenoffiber,bulklaxatives,orstoolsoftenersifconstantdosewasmaintained.Oralorsuppositorybisacodylupto15mgwasallowedasrescuemedicationforsevereconstipationat72hrsafterthelastbowelmovementorforintolerableconstipation.OfthephaseIIItrials,twowerefairqualitytrialsthatevaluatedlinaclotidevs.placeboinpatientswithCIC.TrialsLIN‐MD‐01andMCP‐103‐303wereidentical,exceptfortheinclusionofanadditional4‐weekrandomizedwithdrawalafterweek12intrial303.6Dataforbothtrialswerereportedinthesamepublication,withatotalof1276patientsstratifiedpost‐randomizationtoreceive145mcglinaclotide,290mcglinaclotide,oridenticalplacebooncedaily.Eligiblepatientsincludedmenandwomenages18yearsorolderwithlessthanthreespontaneousbowelmovements(SBMs)perweekplusoneormoresignsorsymptomsduringgreaterthan25%ofbowelmovementsforaminimumof12weeks:straining;lumpy/hardstools;orsensationofincompleteevacuation.PatientsmusthavealsohadlessthanorequaltosixSBMsperweekandlessthanthreeCSBMsduringthebaseline14weeks.Theprimaryefficacyendpointfortrials01and303wasthreeormoreCSBMsperweekandanincreaseofoneormoreCSBMsfrombaselineduringatleast9outof12weeksoftreatment.ThisendpointhasbeenestablishedastheFDAprimaryefficacyendpointforCIC.ItincludesCSBMasamoreclinicallymeaningfulendpointthanspontaneousbowelmovement,sinceconstipationsufferersoftencomplainaboutasenseofincompleteevacuationregardlessofstoolfrequency.6,12Theprimaryefficacyanalysiswasthedifferenceinresponderratebetweenlinaclotidetreatmentarmsandplacebo.Atotalof1272patientsreportedatleastonepost‐randomizationCSBMandwereincludedintheITTanalysis.Therewerestatisticallysignificantdifferencesforalllinaclotidedosescomparedtoplacebo,howevertheoverallresponseratesthatmettheprimaryendpointcriteriawerelowforbothstudies.Intrial01,16.0%ofthe145mcgarmand21.3%ofthe290mcgarmattainedtheprimaryendpoint,comparedto6.0%oftheplaceboarm(NNT=10&7,respectively;P≤0.01&≤0.001,respectively).Intrial303,21.2%ofthe145mcgarmand19.4%ofthe290mcgarmvs.3.3%oftheplaceboarmmetthecriteriafortheprimaryendpoint(NNT=6&6,respectively;P≤0.001forbothlinaclotidearms).Secondaryendpointanalysesfortrials01and303revealedstatisticallysignificantdifferencesforallendpoints,includingstoolfrequency,stoolconsistency,severityofstraining,abdominaldiscomfort,bloating,andconstipationseverity.TheFDAconsideredthefollowingsecondaryendpointstobeappropriateforinclusioninlabeling:weeklychangefrombaselineinnumberofCSBMsandSBMs,andchangefrombaselinestoolconsistencybasedonthevalidated7‐pointBristolStoolFormScale.12Ascoreof1ontheBSFSisindicativeofconstipation,whileascoreof7indicatesdiarrhea.Foralllinaclotidearms,CSBMsincreasedbyapproximatelytwoperweekcomparedtolessthanoneforplacebo,whileSBMsincreasedbyapproximatelythreeperweekcomparedtoanincreaseofoneforplacebo(allP‐values<0.001).Overall,meanbaselinestoolconsistencyscoresforallarmswereapproximatelya2(lumpy,indicativeofconstipation).At12weeks,
Page 4
4
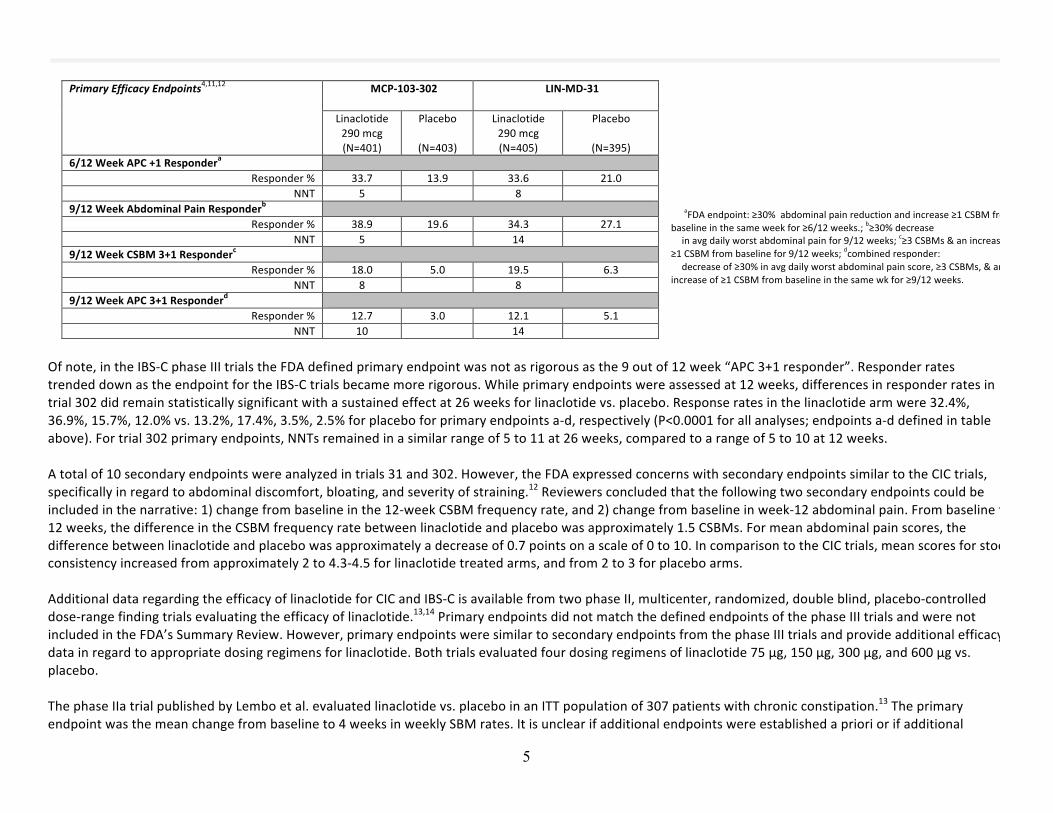
linaclotidearmmeanscoresincreasedto4(smooth,softstool)vs.3(cracks,suggestinghardness)forplacebo,allP‐values<0.001.Inregardtoothersecondaryendpoints,theFDAdeterminedinitssummaryreviewthatthescoringsystemsusedtoassessobservedtreatmentchangesforseverityofstraining,abdominaldiscomfort,bloating,andconstipationseveritywereproblematic.12Theordinalscalesutilizedforthesesecondaryendpointswerenotvalidated.Patientswerealsoaskedtorateconstipationsymptomscomparedtobaseline,i.e.overanextendedperiodoftime&introducingthepotentialforrecallbias.Forexample,weeklyquestionstoevaluatebloatingandabdominaldiscomfortwereconsideredproblematicbecausewordingdidnotspecify“severity”eventhoughresponseoptionsincluded“none,mild,moderate,severe,orverysevere”onanordinalscaleof1to5.Inaddition,meanandmedianbaselinescoreswereintherangeof3onallarms(moderate),butonlydroppedtoarangeconsideredtobemildconstipationforbothlinaclotideandplaceboarms.TwoadditionalphaseIIItrialshavebeenpublishedevaluatingtheefficacyoflinaclotide.TrialsLIN‐MD‐31andMCP‐103‐302werefairqualitytrialsevaluating290mcglinaclotidevs.placeboinpatientswithIBS‐C,withthesamedesignmethodsforprimaryendpointassessments.4,11Trial31includedanadditional4‐weekrandomizedwithdrawalperiod,whiletrial302gatheredadditionalefficacyandsafetydataastertiaryanalysesbeyondthe12‐weekprimaryendpointthrough26weeks.Eligiblepatientsincludedmenandwomenages18yearsorolderwhometmodifiedRomeIIcriteriaforIBS‐C,plusabdominalpainordiscomfortwithatleast2of3featuresreportedforaminimumof12weeksinthe12monthsbeforescreening:relievedw/defecation;onsetassociatedwithachangeinthefrequencyofstool;oronsetassociatedwithachangeintheformofstoolbeforetakingtegaserodorlubiprostone.PatientsmustalsohavehadlessthanthreeSBMsperweekandoneormoresignsorsymptomsduringgreaterthan25%ofbowelmovementsforaminimumof12weeks:straining;lumpy/hardstools;asensationofincompleteevacuationduringgreaterthan25%ofbowelmovements,plusanaveragescoreofatleast3fordailyabdominalpainandanaverageoflessthanthreeCSBMsperweekandlessthanorequaltofiveSBMsperweek.Bothtrialsincludedthesamefourprimaryefficacyendpointsassessedat12weeks.Atotalof804patientsintrial31and800patientsintrial302completedatleastonepost‐randomizationreportandwereevaluatedintheITTpopulations.Primaryefficacyendpointsincluded:a)responderswithatleasta30%reductioninabdominalpainandanincreaseofatleastoneCSBMfrombaselineinatleast6outof12weeks(theFDAprimaryendpointestablishedforIBS‐C),12b)atleasta30%reductionintheaveragedailyworstabdominalpainforatleast9outof12wks,c)atleastthreeCSBMsandanincreaseofatleastoneCSBMfrombaselineforatleast9outof12weeks,and4)acombinedresponder(a+b).SimilartotheCICtrials,theprimaryefficacyanalysiswasthedifferenceinresponderratebetweenlinaclotidetreatmentarmsandplacebo.Thepercentresponsetotreatmentbystudyistabulatedbelow.Allresultsfortrial302werestatisticallysignificantwithP‐values<0.0001;P‐valuesfortrial31were<0.0001,exceptforendpointb(P=0.0262)andendpointd(P=0.0004).SimilartotheCICtrials,overallresponseratestolinaclotidewereloweventhoughresultswerestatisticallysignificantwhencomparedtoplacebo.
Page 5
5
aFDAendpoint:≥30%abdominalpainreductionandincrease≥1CSBMfrombaselineinthesameweekfor≥6/12weeks.;b≥30%decrease inavgdailyworstabdominalpainfor9/12weeks;c≥3CSBMs&anincreaseof≥1CSBMfrombaselinefor9/12weeks;dcombinedresponder: decreaseof≥30%inavgdailyworstabdominalpainscore,≥3CSBMs,&anincreaseof≥1CSBMfrombaselineinthesamewkfor≥9/12weeks.
Ofnote,intheIBS‐CphaseIIItrialstheFDAdefinedprimaryendpointwasnotasrigorousasthe9outof12week“APC3+1responder”.ResponderratestrendeddownastheendpointfortheIBS‐Ctrialsbecamemorerigorous.Whileprimaryendpointswereassessedat12weeks,differencesinresponderratesintrial302didremainstatisticallysignificantwithasustainedeffectat26weeksforlinaclotidevs.placebo.Responseratesinthelinaclotidearmwere32.4%,36.9%,15.7%,12.0%vs.13.2%,17.4%,3.5%,2.5%forplaceboforprimaryendpointsa‐d,respectively(P<0.0001forallanalyses;endpointsa‐ddefinedintableabove).Fortrial302primaryendpoints,NNTsremainedinasimilarrangeof5to11at26weeks,comparedtoarangeof5to10at12weeks.Atotalof10secondaryendpointswereanalyzedintrials31and302.However,theFDAexpressedconcernswithsecondaryendpointssimilartotheCICtrials,specificallyinregardtoabdominaldiscomfort,bloating,andseverityofstraining.12Reviewersconcludedthatthefollowingtwosecondaryendpointscouldbeincludedinthenarrative:1)changefrombaselineinthe12‐weekCSBMfrequencyrate,and2)changefrombaselineinweek‐12abdominalpain.Frombaselineto12weeks,thedifferenceintheCSBMfrequencyratebetweenlinaclotideandplacebowasapproximately1.5CSBMs.Formeanabdominalpainscores,thedifferencebetweenlinaclotideandplacebowasapproximatelyadecreaseof0.7pointsonascaleof0to10.IncomparisontotheCICtrials,meanscoresforstoolconsistencyincreasedfromapproximately2to4.3‐4.5forlinaclotidetreatedarms,andfrom2to3forplaceboarms.AdditionaldataregardingtheefficacyoflinaclotideforCICandIBS‐CisavailablefromtwophaseII,multicenter,randomized,doubleblind,placebo‐controlleddose‐rangefindingtrialsevaluatingtheefficacyoflinaclotide.13,14PrimaryendpointsdidnotmatchthedefinedendpointsofthephaseIIItrialsandwerenotincludedintheFDA’sSummaryReview.However,primaryendpointsweresimilartosecondaryendpointsfromthephaseIIItrialsandprovideadditionalefficacydatainregardtoappropriatedosingregimensforlinaclotide.Bothtrialsevaluatedfourdosingregimensoflinaclotide75µg,150µg,300µg,and600µgvs.placebo.ThephaseIIatrialpublishedbyLemboetal.evaluatedlinaclotidevs.placeboinanITTpopulationof307patientswithchronicconstipation.13Theprimaryendpointwasthemeanchangefrombaselineto4weeksinweeklySBMrates.Itisunclearifadditionalendpointswereestablishedaprioriorifadditional
MCP‐103‐302
LIN‐MD‐31
PrimaryEfficacyEndpoints4,11,12 Linaclotide
290mcg(N=401)
Placebo
(N=403)
Linaclotide290mcg(N=405)
Placebo
(N=395)6/12WeekAPC+1Respondera
Responder% 33.7 13.9 33.6 21.0NNT 5 8
9/12WeekAbdominalPainResponderb Responder% 38.9 19.6 34.3 27.1
NNT 5 14 9/12WeekCSBM3+1Responderc
Responder% 18.0 5.0 19.5 6.3NNT 8 8
9/12WeekAPC3+1Responderd Responder% 12.7 3.0 12.1 5.1
NNT 10 14
Page 6
6
endpointswereconsideredsecondaryassessments.SimilartothephaseIIItrials,ordinalscalesusedforseverityassessmentsofadditionalendpointswerenotvalidated.However,fortheprimaryendpointtherewasalineardoseresponseinthemeanfrequencyofSBMsfrombaselineto4weeks,withincreasesof2.6,3.3,3.6and4.3SBMsfordosesof75,150,300,and600µgrespectively,comparedto1.5forplacebo(P<0.05).TherewasalsoatrendtowardimprovementinmeanweeklyCSBMfrequencyandstoolconsistencywithincreasingdose;however,resultsshouldbeinterpretedwithcautiongiventhatthedescriptionofadditionalendpointsisvagueinregardtohierarchyandwhethertheywereadhocanalyses.Whilebowelfunctiontrendedtowardgreatestimprovementatthe600µgdose,therewerealsomoresideeffectsreportedatthisdose,withdiarrheaasthemostcommonadverseevent.Authorsconcludedthatthe150µgand300µgdosesoflinaclotideprovidedthebestbalanceofefficacyandsafetyforpatientswithchronicconstipation.ThephaseIIbtrialpublishedbyJohnstonetal.evaluatedlinaclotidevs.placeboinanITTpopulationof419patientswithIBS‐C.14Theprimaryendpointwasthemeanchangefrombaselineto12weeksinweeklyCSBMrates.SimilartothephaseIIatrial,itisunclearifahierarchyofadditionalendpointswasestablishedandordinalscalesforseveritymeasureswerenotvalidated.Resultsfortheprimaryendpointacrossallarmswerestatisticallysignificant(allP<0.01).MeanincreasesforCSBMfrequencyrangedfrom2.5to3.6,withthelargestincreaseof3.6CSBMsoccurringinthe300µgarm(P<0.001).Diarrheawastheonlydose‐dependentsideeffect.Authorsconcludedthatthe300µgdoseprovidedcomparableefficacytothe600µgdosewithfewerGIsideeffects,andrecommendedthedosebeselectedforphaseIIIstudies.Todate,comparativeefficacydataoflinaclotidevs.commonlyusedlaxativesislacking.However,arecentsystematicreviewandmeta‐analysiswaspublishedthatprovidessomeinsightintohowlinaclotidecomparestoothertherapiesforchronicconstipation.8Twenty‐onerandomizedcontrolledtrialswereevaluatedfortheeffectivenessoflaxativesandpharmacologicaltherapiesinthetreatmentofCIC,includinglinaclotide.Authorsconcludedthefollowingagentsweremoreeffectivethanplacebo:linaclotide(RR0.84;95%CI0.80‐0.87);lubiprostone(RR0.67;95%CI0.56‐0.80);laxatives(RR0.52;95%CI0.46‐0.60;includedPEG,sodiumpicosulfateandbisacodyl).Prucalopridewasalsofoundtobemoreeffectivethanplacebo(RR0.82;95%CI0.76‐0.88),butitisnotavailableintheU.S.Numbersneededtotreattopreventonepatientfromfailingtorespondtotherapyrangedfrom3to6.Therearenopublishedcomparativeefficacytrialscomparinglinaclotidetolubiprostone.However,overallresponseratestolubiprostonevs.placeboinanadultfemale,IBS‐Cpopulationintwodouble‐blind,placebocontrolledtrialswas13.8/7.8%and12.1/5.7%.15TheprimaryendpointforthelubiprostoneIBS‐Ctrialswasbasedonthepatient’sresponsetoaglobalsymptomreliefscaleandwaslessrigorousthantheendpointsinthelinaclotideCIC/IBS‐Ctrials.Itisthereforedifficulttointerpretanydifferencesinresponseratestolinaclotidevs.lubiprostone.Head‐to‐headtrialsareneededtoevaluatetheefficacyoflinaclotidecomparedtootheravailableagentsforthetreatmentofchronicconstipation.Inconclusion,theoverallstrengthofevidenceismoderateinsupportoflinaclotide'sefficacyinthetreatmentofCICandIBS‐C.However,statisticallysignificantresultsmaynotbeclinicallymeaningfultopatients.Overallresponseratestolinaclotidearelow,andthemeasuresutilizedtoevaluateclinicallyrelevantsymptomreductionforabdominalpainandsymptomseverityweresuboptimalinphaseIIandphaseIIItrials.ForphaseIIItrialprimaryefficacyendpoints,aresponseto9outof12weeksinthecaseofCICandto6outof12weeksforIBS‐Cmeansupto50%ofthetimethepatientmayexperiencenorelieffromsymptoms.Inaddition,theimpactoflinaclotideonhealth‐relatedqualityoflifewasnotassessedasapre‐definedprimaryorsecondaryendpoint.Patientsinthegeneralpopulationwhohaveconstipationmaybeolder,sinceprevalenceincreaseswithage.Thedatamaynotaccuratelyreflectanydifferencesinresponseduetosexasthestudypopulationswerepredominantlyfemale.Finally,theFDAprimaryendpointsforIBS‐CandCICarerelativelynewandhavenotbeenfullyvettedinclinicaltrials.Therefore,itisdifficulttodeterminetheclinicalmeaningfulnessoftheendpoints,e.g.withanincreaseofoneCSBMperweekoverbaselinethepatientmaystillexperiencediscomfortand/orpainiftheirbaselinenumberofCSBMswaszero.PatientsshouldstillseektooptimizeallotheroptionsfortreatingIBS‐CandCICbeforetryinglinaclotide.
Page 7
7
ClinicalSafety:Thesafetyoflinaclotideinpatientsundertheageof18hasyettobedetermined.Thereisablackboxwarningforpatientsupto6yearsofageanduseisdiscouragedinpediatricpatients6through17yearsofage.TheFDAhasrequestedthatthemanufacturerperformadditionalsafetyanalysesinanimalandhumanmodelstodeterminethesafetyprofileforthispopulation.Thisrequestfollowsdatademonstratingtoxicityinneonatalandjuvenilemice.Inaddition,theFDAhasexpressedconcernthatthegreatestsafetyriskoflinaclotideisthetheoreticaldevelopmentofanti‐linaclotideantibodiesandcross‐reactionwithendogenouspeptides.Nodataisavailabletodatetoassessthisrisk;howeverthemanufacturerisrequiredtoperformadditionalanti‐drugantibodyassaysplusaclinicaltrialinadultstodeterminetheriskofdevelopingantibodyresponsesinresponsetotreatment.1,12ThemostcommonadversedrugeventinallfourphaseIIItrialswasdiarrhea,withanoverallincidenceof16%atthe145mcgdoseoflinaclotideand20%at290mcglinaclotide.12Likewise,datafromthephaseIItrialssuggestsatrendofincreasingincidenceofdiarrheawithincreaseddosesoflinaclotide.Twoopen‐label,long‐termsafetystudieshavesincebeenconductedonlinaclotide.Althoughpublisheddataisnotavailable,theoutcomeshavebeenincludedintheFDASummaryReview.12NearlyathirdofbothCICandIBS‐Cpatientsreporteddiarrheaasanadverseevent.Overall,inthelong‐termstudiesdiarrheawasreportedasseverein3%ofpatients.Theagentcarriesapregnancyratingof“C”.Sevenknowndeathsoccurredfromallstudypopulations,howevernonewereattributedtothedrug.Onepatientdiedduringscreeningpriortostudydrugexposure,twopatientsdiedfromcancer,onepatientfellfromaladder,andthreedeathswereattributedtonarcoticuse.Therewasnoevidencelinkinglinaclotidetorenalorhepatictoxicity,correlatingtolowsystemicexposuretothedrug.Noneofthedatafromtherandomizedcontrolledtrialsestablishedacausallinkbetweenlinaclotideanddiverticulitis,gallbladderdisease,ischemiccolitis,orhematologicaldisorders;however,therewasahigherpercentageofpatientswithlowRBClevelsinthe290microgramarmsoftheIBS‐CandCICtrialscomparedtoplaceboandthelowerdosearm(0.5%/0.2%/0.2%,respectively).Themeaningofthisfindingisunclear,astherewasnostatisticaldifferencebetweenHCTorHgbbetweenstudyarms.12COMPARATIVECLINICALEFFICACYRelevantEndpoints:1)Reducedsymptomseverityoreliminationofsymptoms‐Improvedbowelfunction‐Reducedpain/discomfortassociatedwithdiseasestate2)Improvedhealth‐relatedqualityoflife3)Tolerability
PrimaryStudyEndpoints(PhaseIIITrials):1) CICtrials:Patientswithatleast3CSBMsperweekandanincrease
ofatleastoneCSBMperwkfrombaselineforatleast9weeksduringthe12‐weektreatmentperiod(FDAdefined1°endpoint)
2) IBS‐Ctrials:Responderswith≥30%abdominalpainreductionandanincreaseofatleastoneCSBMfrombaselineinthesameweekforatleast6outof12weeks(FDAdefined1°endpoint)
3) IBS‐Ctrials:≥30%reductionofaveragedailyworstabdominalpainforatleast9outof12wks
4) IBS‐Ctrials:atleast3CSBMs&anincreaseofatleastoneCSBMfrombaselinefor9outof12weeks
5) IBS‐Ctrials:Combinedresponder:decreaseof≥30%inavgdailyworstabdominalpainscore,≥3CSBMs,&anincreaseof≥1CSBMfrombaselineinthesamewkfor≥9/12weeks
Page 8
8
1.LemboAJ,etal.
6
TrialMCP‐103‐303(CIC)DB,PC,PG,MC,RCTPhaseIII
R1:Linaclotide145µgR2:Linaclotide290µgP:PlaceboDuration:12weeksTrials303and01wereidentical,exceptTrial303hadanadditional4‐wkrandomizedwithdrawalafter12weeks.
Meanage:47/48/49yearsMale:13/12/12.9%White:72.7/75.6/76.6%Age≥65yrs:12.4/12.5/13.4%InclusionCriteria:Men&women≥18yrswith<3SBMs/wk+oneormores/sxduring>25%BMsforminof12weeks:straining;lumpy/hardstools;sensationofincompleteevacuation.Plus:≤6SBMs/wk&<3CSBMsduringbaseline14wks.ExclusionCriteria:looseorwaterystoolinabsenceoflaxativefor>25%BMsinpreceding12wks;mushystoolfor>1SBMduringbaseline,RomeIIcriteriaforIBS;hxpelvicfloordysfunction;alarmsxconfirmedbycolonoscopy.Patientsonastable,continuousregimenoffiber,bulklaxatives,orstoolsoftenersallowedtocontinueifconstantdosewasmaintained.POorsuppositorybisacodylupto15mg/dayallowedasrescuemedicationforsevereconstipationat72hrsafterlastBMorforintolerableconstipation.
N=643ITT=642R1:217R2:216P:209
FDA1°endpoints:Patientswith≥3CSBMs/weekandan↑ofatleastoneCSBM/wkfrombaselinefor≥9weeksduringthe12‐wktreatmentperiod[n(%)]:R1:46(21.2);P≤0.001R2:42(19.4);P≤0.001P:7(3.3)OR(linaclotide:Placebo):R1:7.72,95%CI(3.41,17.47)P≤0.0001R2:7.21,95%CI(3.14,16.59)P≤0.00012°endpoints:CSBMschangefrombaseline(no./wk):R1:1.9R2:2.0P:0.5P<0.001SBMschangefrombaseline(no./wk):R1:3.0R2:3.0P:1.1P<0.001Stoolconsistency,changefrombaselinescore:R1:1.9R2:1.8P:0.6P<0.001
NNTR1:6R2:6
Pooleddata303/01(R1/R2/P;CI&P‐valuesnotreported):Anyevents:60.5%/55.7%/52.1%Themostcommondose‐relatedADE(%):Diarrhea:16/14.2/4.7OtherADEsin≥3%ofpatients:flatulence,abpain,URI,abdistention,nasopharyngitis,sinusitis,upperabpainMortality:0%(oneptdiedfromfentanylOD)SeriousADEs(%):1.4/2.6/2.1DiscontinuationduetoADEs(%):7.9/7.3/4.21stoccurrenceofdiarrheaADEreportedin1st2weeks:61.7%DiarrheagradedassevereADE(R/P;%):1.5/0.2
NNHR1:9R2:10
QualityRating:FairAnalysis:ITT;totalof1272patients(trials01&303);4patientsoutof1276didnotreportanypost‐randomizationCSBMs.Sensitivityanalysesincludingthe4non‐reportingpatientsrevealedsimilarresults.Observed‐casesapproachtomissingpost‐baselinedatawithlast‐observation‐carried‐forwardapplied.OverallAttrition:R1/R2/P(%)14.3/18.4/15.3RiskofBiasInternalValidity:Selection:Lowbias;randomizationandallocationconcealmentclear;viaoffsiteIVRSPerformance:Lowbias,blindingofpatientsandstudymonitors;unclearhowPKsamplesatwk7wereblindedbutlinaclotidelevelswerenotdetectableAttrition:Lowbias;Lessthan20%overall,with<10%differencebetweentreatmentgroups.AdherencetoIVRS:88.3%Levelofadherencetostudymedication,crossovers,andcontaminationnotdiscussed.ExternalValidity:PatientCharacteristics:similarbetweengroups;maynotreflectgeneralpopulationSetting:geographicregionusedasafixedeffecttermforanalysisinsteadoftrialcenterassomesiteshadsmallnumbersofpatientsOutcomes:200patientsprovided90%powertodetecttreatmentdifferencesintheprimaryendpoint.2°outcomesthatrequiredptstorecallcurrentsymptomscomparedtobaselinesubjecttobias(e.g.,severity,straining).
Ref./StudyDesign
DrugRegimens/Duration
PatientPopulation(R1/R2/P)
N Outcomes/EfficacyResults(CI,p‐values)
NNT SafetyResults(CI,p‐values)
NNH QualityRating;InternalValidityRiskofBias/ExternalValidityConcerns
Page 9
9
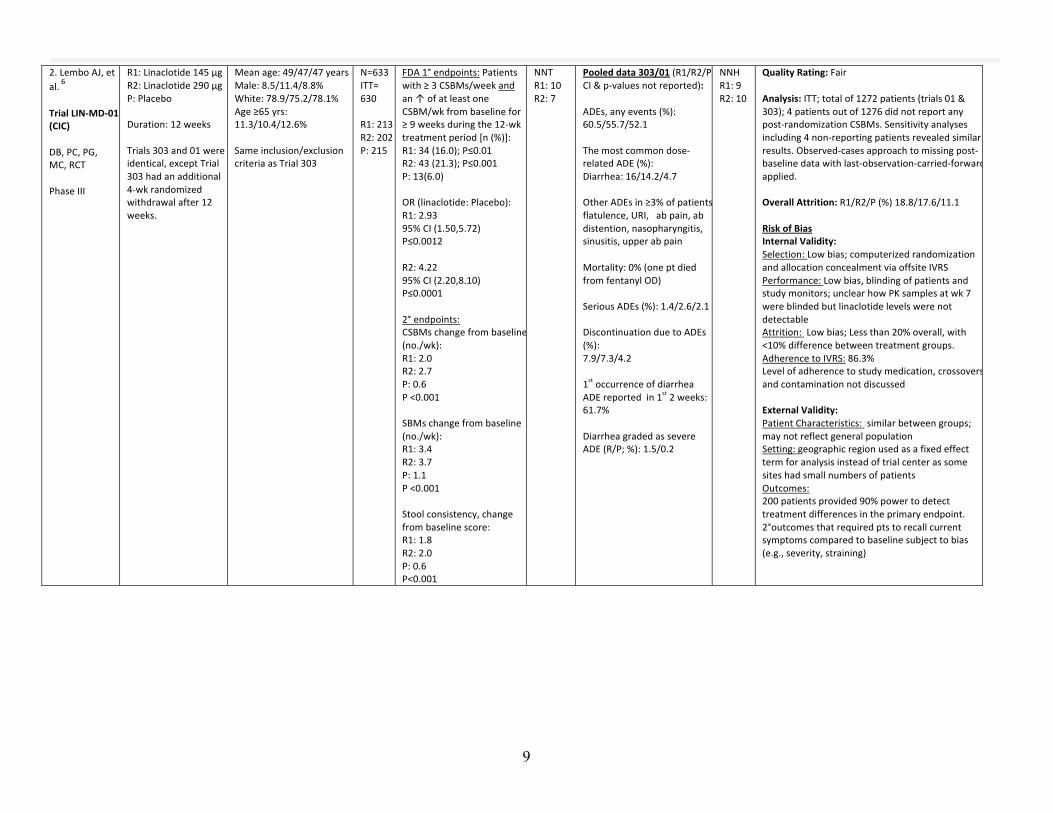
2.LemboAJ,etal.
6
TrialLIN‐MD‐01(CIC)DB,PC,PG,MC,RCTPhaseIII
R1:Linaclotide145µgR2:Linaclotide290µgP:PlaceboDuration:12weeksTrials303and01wereidentical,exceptTrial303hadanadditional4‐wkrandomizedwithdrawalafter12weeks.
Meanage:49/47/47yearsMale:8.5/11.4/8.8%White:78.9/75.2/78.1%Age≥65yrs:11.3/10.4/12.6%Sameinclusion/exclusioncriteriaasTrial303
N=633ITT=630R1:213R2:202P:215
FDA1°endpoints:Patientswith≥3CSBMs/weekandan↑ofatleastoneCSBM/wkfrombaselinefor≥9weeksduringthe12‐wktreatmentperiod[n(%)]:R1:34(16.0);P≤0.01R2:43(21.3);P≤0.001P:13(6.0)OR(linaclotide:Placebo):R1:2.9395%CI(1.50,5.72)P≤0.0012R2:4.2295%CI(2.20,8.10)P≤0.00012°endpoints:CSBMschangefrombaseline(no./wk):R1:2.0R2:2.7P:0.6P<0.001SBMschangefrombaseline(no./wk):R1:3.4R2:3.7P:1.1P<0.001Stoolconsistency,changefrombaselinescore:R1:1.8R2:2.0P:0.6P<0.001
NNTR1:10R2:7
Pooleddata303/01(R1/R2/P;CI&p‐valuesnotreported):ADEs,anyevents(%):60.5/55.7/52.1Themostcommondose‐relatedADE(%):Diarrhea:16/14.2/4.7OtherADEsin≥3%ofpatients:flatulence,URI,abpain,abdistention,nasopharyngitis,sinusitis,upperabpainMortality:0%(oneptdiedfromfentanylOD)SeriousADEs(%):1.4/2.6/2.1DiscontinuationduetoADEs(%):7.9/7.3/4.21stoccurrenceofdiarrheaADEreportedin1st2weeks:61.7%DiarrheagradedassevereADE(R/P;%):1.5/0.2
NNHR1:9R2:10
QualityRating:FairAnalysis:ITT;totalof1272patients(trials01&303);4patientsoutof1276didnotreportanypost‐randomizationCSBMs.Sensitivityanalysesincluding4non‐reportingpatientsrevealedsimilarresults.Observed‐casesapproachtomissingpost‐baselinedatawithlast‐observation‐carried‐forwardapplied.OverallAttrition:R1/R2/P(%)18.8/17.6/11.1RiskofBiasInternalValidity:Selection:Lowbias;computerizedrandomizationandallocationconcealmentviaoffsiteIVRSPerformance:Lowbias,blindingofpatientsandstudymonitors;unclearhowPKsamplesatwk7wereblindedbutlinaclotidelevelswerenotdetectableAttrition:Lowbias;Lessthan20%overall,with<10%differencebetweentreatmentgroups.AdherencetoIVRS:86.3%Levelofadherencetostudymedication,crossovers,andcontaminationnotdiscussedExternalValidity:PatientCharacteristics:similarbetweengroups;maynotreflectgeneralpopulationSetting:geographicregionusedasafixedeffecttermforanalysisinsteadoftrialcenterassomesiteshadsmallnumbersofpatientsOutcomes:200patientsprovided90%powertodetecttreatmentdifferencesintheprimaryendpoint.2°outcomesthatrequiredptstorecallcurrentsymptomscomparedtobaselinesubjecttobias(e.g.,severity,straining)
Page 10
10
3.RaoS,etal.4
TrialLIN‐MD‐31(IBS‐C)DB,PC,PG,MC,RCTPhaseIII
R:Linaclotide290µgP:PlaceboDuration:12weeks+4weeksRWperiod
Meanage:43.3/43.7yearsMale:9.4/9.6%White:77.5/76.2%Age≥65yrs:4.7/6.6%InclusionCriteria:Menandwomen≥18yrswhometmodifiedRomeIIcriteriaforIBS‐C;abdominalpainordiscomfortwith≥2of3featuresreportedforminof12wksinthe12mobeforescreening:i)relievedw/defecation,ii)onsetassocw/Δfreqofstool,oriii)onsetassocw/Δinformofstoolbeforetakingtegaserodorlubiprostone;<3SBMs/wk+oneormores/sxduring>25%BMsforminof12weeks:straining;lumpy/hardstools;sensationofincompleteevacuation;avgscoreof≥3fordailyabpain;avg<3CSBMs/wkand≤5SBMs/wk.ExclusionCriteria:looseorwaterystoolfor>25%BMsinpreceeding12wks;duringbaseline,aBSFSscoreof7foranySBM,or6for>1SBM;hxcatharticcolon,laxativeabuse,ischemiccolitis,GIsurgery,diverticulitis,familyhxcolorectalca.Constipatingdrugslikenarcoticsexcluded;however,patientsonstabledosesofdrugsforIBSfor30dayspriortotrialthatmaycauseconstipationallowedtocontinue(e.g.TCAs).Rescuemedallowed~CICtrials
N=803ITT:800R:405P:395
1°endpoints(n(%))a)Responderswith≥30%↓abpainand↑≥1CSBMfrombaselinein≥6/12wks(FDA1°):R:136(33.6)P:83(21.0)OR(95%CI):1.9(1.4,2.7)P<0.0001b)≥30%↓avgdailyworstabpain(9/12wks)R:139(34.3)P:107(27.1)OR(95%CI):1.4(1.0,1.9)P=0.0262c)≥3CSBMs&≥1CSBMfrombaseline(≥9/12weeks):R:79(19.5)P:25(6.3)OR(95%CI):3.7(2.3,5.9)P<0.0001d)Combinedresponder(a+b):R:49(12.1)P:20(5.1)OR(95%CI):2.6(1.5,4.5)P=0.00042°endpointsa)CSBMΔfrombaseline(mean):R:2.3P:0.7P<0.0001b)Worstabpain,Δfrombaseline(mean):R:‐1.9P:‐1.1P<0.0001
NNT(1°)a)8b)14c)8d)14NNT(2°)N/A
ADEs,anyevents(%):56.2/53.0ADEswith≥2%incidence(%):Diarrhea:19.5/3.5P<0.0001Abdominalpain:5.4/2.5;P=0.0462Flatulence:4.9/1.5;P=0.0084Headache:4.9/3.5;P=0.3825Abdominaldistension:2.2/0.8;P=0.1434Mortality:NodeathsduringtreatmentSAEs:2patientseacharm(0.5%botharms)DiscontinuationduetoADEs(%):7.9/2.8Discontinuationduetodiarrhea(%):5.7/0.3>50%ofpatientsw/diarrheaexperiencedinthe1st2weeksNodiarrheagradedassevereADE
NNHR:6
QualityRating:FairAnalysis:ITT;800patientsmetcriteriaforefficacyanalysis&802metcriteriaforsafetyanalysisOverallAttrition:(R/P):23.2%/15.6%RiskofBiasInternalValidity:Selection:Lowbias;computerizedrandomizationandallocationconcealmentviaoffsiteIVRSPerformance:Lowbias,blindingofpatientsandstudymonitors;unclearhowPKsamplesatbaselineandwk4wereblindedbutlinaclotidelevelswerenotdetectableAttrition(R/P):Potentialbias;overallattritionoflinaclotidearm>20%duetogreaterlosstofollow‐up(4.2/2.5%)&incidenceofadverseevents(7.9/2.5%).Betweengroupdifference<10%.AdherencetoIVRS:(R:P;%):71/73Levelofadherencetostudymedication,crossovers,andcontaminationnotdiscussed.ExternalValidity:PatientCharacteristics:significantdifferencesexistedatbaselineforsymptomsofabdominalfullness,stoolconsistency&straining;maynotreflectgeneralpopulation.Setting:geographicregionusedasafixedeffecttermforanalysisinsteadoftrialcenterassomesiteshadsmallnumbersofpatientsOutcomes:400patientsperarmprovided>85%powertodetecttreatmentdifferences.Comorbidconditionssuchasdiverticulitismaybepresentinthegeneralpopulation;PatientscouldmeetsomecriteriaforprimaryendpointsbutstillhavedxofconstipationaccordingtoRomeIIIguidelines(if<3BMs/wk).
Page 11
11
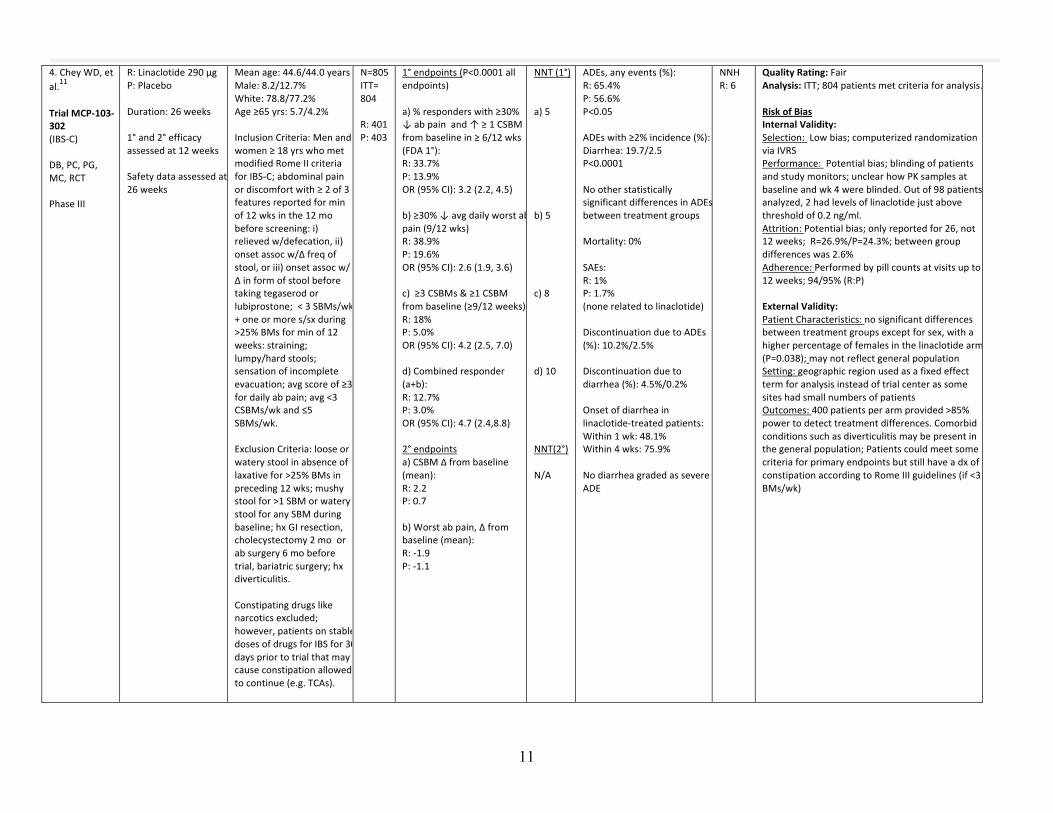
4.CheyWD,etal.
11
TrialMCP‐103‐302(IBS‐C)DB,PC,PG,MC,RCTPhaseIII
R:Linaclotide290µgP:PlaceboDuration:26weeks1°and2°efficacyassessedat12weeksSafetydataassessedat26weeks
Meanage:44.6/44.0yearsMale:8.2/12.7%White:78.8/77.2%Age≥65yrs:5.7/4.2%InclusionCriteria:Menandwomen≥18yrswhometmodifiedRomeIIcriteriaforIBS‐C;abdominalpainordiscomfortwith≥2of3featuresreportedforminof12wksinthe12mobeforescreening:i)relievedw/defecation,ii)onsetassocw/Δfreqofstool,oriii)onsetassocw/Δinformofstoolbeforetakingtegaserodorlubiprostone;<3SBMs/wk+oneormores/sxduring>25%BMsforminof12weeks:straining;lumpy/hardstools;sensationofincompleteevacuation;avgscoreof≥3fordailyabpain;avg<3CSBMs/wkand≤5SBMs/wk.ExclusionCriteria:looseorwaterystoolinabsenceoflaxativefor>25%BMsinpreceding12wks;mushystoolfor>1SBMorwaterystoolforanySBMduringbaseline;hxGIresection,cholecystectomy2moorabsurgery6mobeforetrial,bariatricsurgery;hxdiverticulitis.Constipatingdrugslikenarcoticsexcluded;however,patientsonstabledosesofdrugsforIBSfor30dayspriortotrialthatmaycauseconstipationallowedtocontinue(e.g.TCAs).
N=805ITT=804R:401P:403
1°endpoints(P<0.0001allendpoints)a)%responderswith≥30%↓abpainand↑≥1CSBMfrombaselinein≥6/12wks(FDA1°):R:33.7%P:13.9%OR(95%CI):3.2(2.2,4.5)b)≥30%↓avgdailyworstabpain(9/12wks)R:38.9%P:19.6%OR(95%CI):2.6(1.9,3.6)c)≥3CSBMs&≥1CSBMfrombaseline(≥9/12weeks):R:18%P:5.0%OR(95%CI):4.2(2.5,7.0)d)Combinedresponder(a+b):R:12.7%P:3.0%OR(95%CI):4.7(2.4,8.8)2°endpointsa)CSBMΔfrombaseline(mean):R:2.2P:0.7b)Worstabpain,Δfrombaseline(mean):R:‐1.9P:‐1.1
NNT(1°)a)5b)5c)8d)10NNT(2°)N/A
ADEs,anyevents(%):R:65.4%P:56.6%P<0.05ADEswith≥2%incidence(%):Diarrhea:19.7/2.5P<0.0001NootherstatisticallysignificantdifferencesinADEsbetweentreatmentgroupsMortality:0%SAEs:R:1%P:1.7%(nonerelatedtolinaclotide)DiscontinuationduetoADEs(%):10.2%/2.5%Discontinuationduetodiarrhea(%):4.5%/0.2%Onsetofdiarrheainlinaclotide‐treatedpatients:Within1wk:48.1%Within4wks:75.9%NodiarrheagradedassevereADE
NNHR:6
QualityRating:FairAnalysis:ITT;804patientsmetcriteriaforanalysis.RiskofBiasInternalValidity:Selection:Lowbias;computerizedrandomizationviaIVRSPerformance:Potentialbias;blindingofpatientsandstudymonitors;unclearhowPKsamplesatbaselineandwk4wereblinded.Outof98patientsanalyzed,2hadlevelsoflinaclotidejustabovethresholdof0.2ng/ml.Attrition:Potentialbias;onlyreportedfor26,not12weeks;R=26.9%/P=24.3%;betweengroupdifferenceswas2.6%Adherence:Performedbypillcountsatvisitsupto12weeks;94/95%(R:P)ExternalValidity:PatientCharacteristics:nosignificantdifferencesbetweentreatmentgroupsexceptforsex,withahigherpercentageoffemalesinthelinaclotidearm(P=0.038);maynotreflectgeneralpopulationSetting:geographicregionusedasafixedeffecttermforanalysisinsteadoftrialcenterassomesiteshadsmallnumbersofpatientsOutcomes:400patientsperarmprovided>85%powertodetecttreatmentdifferences.Comorbidconditionssuchasdiverticulitismaybepresentinthegeneralpopulation;PatientscouldmeetsomecriteriaforprimaryendpointsbutstillhaveadxofconstipationaccordingtoRomeIIIguidelines(if<3BMs/wk)
Page 12
12
5.JohnstonJM,etal.
14
LinaclotideImprovesAbdominalPain&BowelHabitsinaPhaseIIbStudyofPatientswithIBS‐CDB,PC,MC,RCTPhaseIIbdose‐rangefindingstudy
R1:Linaclotide75µgR2:Linaclotide150µgR3:Linaclotide300µgR4:Linaclotide600µgP:Placebo
MeanAge(range):44.4(18‐72)yrsMale:8%White:80%InclusionCriteria:menandwomen≥18yrswhometmodifiedRomeIIcriteriaforIBSreporting<3SBMsperweek&1ormoreofthefollowingSxfor≥12weeksinthe12monthsprecedingstudyentry:1)strainingduring≥25%ofBMs;2)lumpy/hardstoolsduring≥25%ofBMs;3)sensationofincompleteevacuationduring>25%ofBMs.During2‐wkbaseline,requiredtoreportameanscoreof≥2.0fordailyassessmentofabpainorabdiscomfort,plusmeanof<3CSBMsand≤6SBMs/week.Exclusioncriteria:pregnantorbreast‐feedingpatients,presenceofloose,mushy,waterystoolsfor>25%BMsORscoreof6or7onBSFSw/olaxativeuseforprevious24hrsduring2‐wkbaseline,Hxofpelvicfloordysfunction,colonsurgery,absurgeryinprevious60days,needformanualmaneuversforBM,orlaxativeabuse.POorsuppositorybisacodylupto15mg/dayallowedasrescuemedicationforsevereconstipationat72hrsafterlastBM,providedno>2dosesandnoneused3daysbeforefirstdosestudymed.Stable,continuousfiberregimen&antidepressantsallowedifstable30dayspriortoenrollment.
N=420ITT=419R1:79R2:82R3:84R4:89P:85
1°endpoint:Meanchangefrombaselineto12weeksinweeklyCSBMrate:R1:2.90(P<0.001)R2:2.49(P<0.01)R3:3.61(P<0.001)R4:2.68(P<0.001)P:1.01Additionalendpoints:CSBM75%responder(≥3CSBMs/weekandan↑of≥1CSBM/wkfor≥9outof12weeks).forallvaluesexceptlinaclotide150µg:R1:25.3%(P<0.05)R2:19.5%R3:32.1%(P<0.01)R4:23.6%(P<0.05)P:11.8%Meanchangefrombaselineto12weeksinweeklySBMrate:R1:4.62(P<0.001)R2:4.36(P<0.001)R3:4.97(P<0.001)R4:5.64(P<0.001)P:1.68SBM75%responder(≥3SBMs/weekandan↑of≥1SBM/wkfor≥9outof12weeks)(%):R1:54.4%(P<0.01)R2:39.0%R3:65.5%(P<0.001)R4:52.8%(P<0.01)P:29.4%StoolConsistency(BSFSmeanchangefrombaseline):R1:1.91(P<0.001)R2:1.80(P<0.001)R3:2.28(P<0.001)R4:2.20(P<0.001)P:0.56
NNT(1°)N/ANNT(2°)R1:7R2:13R3:5R4:8N/AR1:4R2:10R3:3R4:4N/A
ADEswith≥3%incidence(%):Diarrhea:14.6%Abdominalpain:5.4%UTI:4.2%Nausea:3.9%Nasopharyngitis:3.3%Headache:3.3%URTI:3.3%Diarrheawastheonlydose‐dependentAE:R1:11.4%R2:12.2%R3:16.5%R4:18.0%P:1.2%Diarrheagradedassevere:R1:2.3%R2:2.5%R3:1.2%R4:4.5%DiscontinuationduetoAE(%):R1:5%R2:7.3%R3:3.5%R4:11.2%P:2.3%Discontinuationduetodiarrhea:R1:2.5%R2:4.9%R3:1.1%R4:6.7%P:0%Medianno.ofdaystoinitialonsetofdiarrhea:4Mortality:nonereported
NNHR1:10R2:9R3:7R4:6
QualityRating:FairAnalysis:ITT,419metcriteriaforanalysis;missingdatanotimputed;analysisdidnotincludealastobservationcarriedforwardapproach(patientswereconsiderednon‐respondersforweekswithmissingdata)OverallAttrition(R1/R2/R3/R4/P):20.2/18.3/16.5/20.2/23.5%Endpointswerenotidentifiedasapriori;itisunclearwhenadditionalendpointswereassessedP‐valuesandconfidenceintervalsnotprovidedforsafetydataRiskofBiasInternalValidity:Selection:Lowbias;computerizedrandomizationviaastatisticiannotassociatedwiththetrialPerformance:Likelylowbias;allstudypersonnelblindedbutaformaldescriptionofdummyplacebodesignwasnotprovidedAttrition:Potentialbias;over20%in75µgand600µgarms(R1&R4)andplaceboarms,howeverbetweengroupdifferencesare<10%Adherence:Patientsreportedtimestudymedication(andanyrescuemedication)wastakendailyviaIVRS.Adherenceratesnotreported.ExternalValidity:PatientCharacteristics:NobaselineP‐valuesareprovided;characteristicsappearsimilarbetweentreatmentgroups.Resultsmaynotreflectresponseingeneralpopulationw/respecttorace.Setting:U.S.geographicregionusedasafixedeffecttermforanalysisinsteadoftrialcenterassomesiteshadsmallnumbersofpatientsOutcomes:80patientsperarmprovided95%powertodetecttreatmentdifferences.AbdominalpainisasignificantcomponentofIBS,howevertheordinalscaleusedtomeasurepatientresponsetotreatmentwasnotvalidated.Itisunclearwhichadditionaloutcomeswereidentifiedapriori,thereforeresponsestonon‐validatedinstruments(meanchangesinabpain,bloating,straining)mustbeinterpretedwithcautionwhenconsideringthegeneralpopulation.
Page 13
13
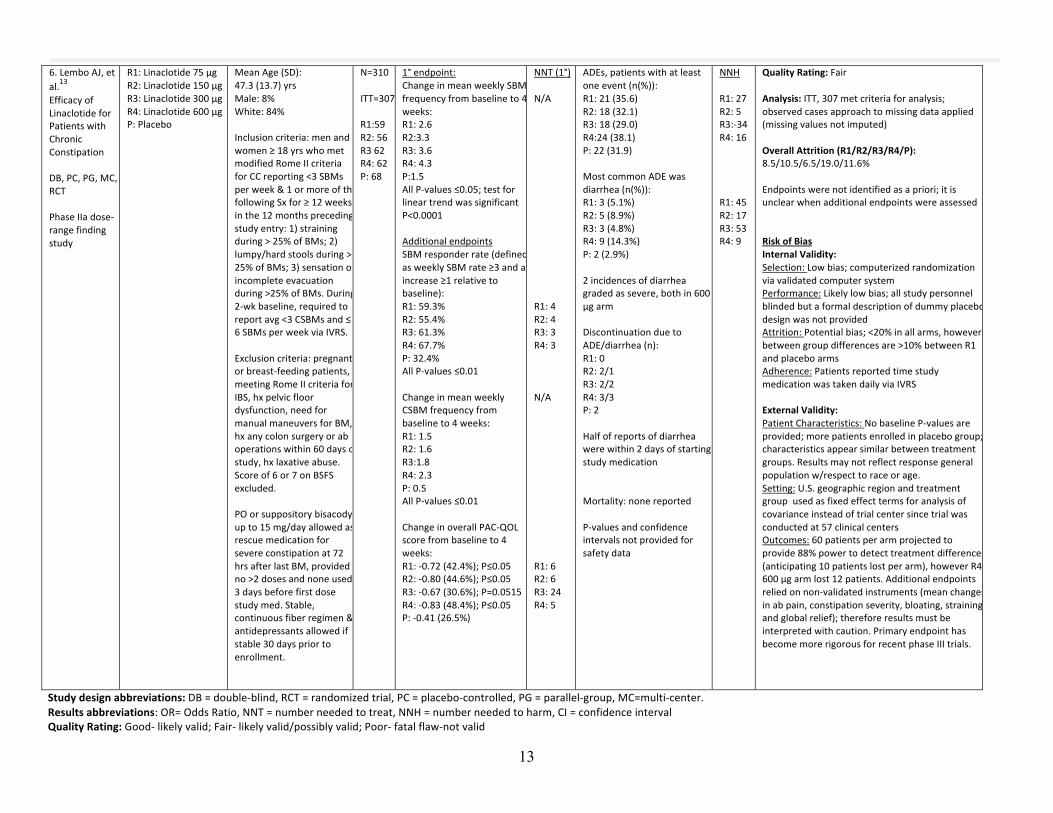
6.LemboAJ,etal.
13
EfficacyofLinaclotideforPatientswithChronicConstipationDB,PC,PG,MC,RCTPhaseIIadose‐rangefindingstudy
R1:Linaclotide75µgR2:Linaclotide150µgR3:Linaclotide300µgR4:Linaclotide600µgP:Placebo
MeanAge(SD):47.3(13.7)yrsMale:8%White:84%Inclusioncriteria:menandwomen≥18yrswhometmodifiedRomeIIcriteriaforCCreporting<3SBMsperweek&1ormoreofthefollowingSxfor≥12weeksinthe12monthsprecedingstudyentry:1)strainingduring>25%ofBMs;2)lumpy/hardstoolsduring>25%ofBMs;3)sensationofincompleteevacuationduring>25%ofBMs.During2‐wkbaseline,requiredtoreportavg<3CSBMsand≤6SBMsperweekviaIVRS.Exclusioncriteria:pregnantorbreast‐feedingpatients,meetingRomeIIcriteriaforIBS,hxpelvicfloordysfunction,needformanualmaneuversforBM,hxanycolonsurgeryoraboperationswithin60daysofstudy,hxlaxativeabuse.Scoreof6or7onBSFSexcluded.POorsuppositorybisacodylupto15mg/dayallowedasrescuemedicationforsevereconstipationat72hrsafterlastBM,providedno>2dosesandnoneused3daysbeforefirstdosestudymed.Stable,continuousfiberregimen&antidepressantsallowedifstable30dayspriortoenrollment.
N=310ITT=307R1:59R2:56R362R4:62P:68
1°endpoint:ChangeinmeanweeklySBMfrequencyfrombaselineto4weeks:R1:2.6R2:3.3R3:3.6R4:4.3P:1.5AllP‐values≤0.05;testforlineartrendwassignificantP<0.0001AdditionalendpointsSBMresponderrate(definedasweeklySBMrate≥3andanincrease≥1relativetobaseline):R1:59.3%R2:55.4%R3:61.3%R4:67.7%P:32.4%AllP‐values≤0.01ChangeinmeanweeklyCSBMfrequencyfrombaselineto4weeks:R1:1.5R2:1.6R3:1.8R4:2.3P:0.5AllP‐values≤0.01ChangeinoverallPAC‐QOLscorefrombaselineto4weeks:R1:‐0.72(42.4%);P≤0.05R2:‐0.80(44.6%);P≤0.05R3:‐0.67(30.6%);P=0.0515R4:‐0.83(48.4%);P≤0.05P:‐0.41(26.5%)
NNT(1°)N/AR1:4R2:4R3:3R4:3N/AR1:6R2:6R3:24R4:5
ADEs,patientswithatleastoneevent(n(%)):R1:21(35.6)R2:18(32.1)R3:18(29.0)R4:24(38.1)P:22(31.9)MostcommonADEwasdiarrhea(n(%)):R1:3(5.1%)R2:5(8.9%)R3:3(4.8%)R4:9(14.3%)P:2(2.9%)2incidencesofdiarrheagradedassevere,bothin600µgarmDiscontinuationduetoADE/diarrhea(n):R1:0R2:2/1R3:2/2R4:3/3P:2Halfofreportsofdiarrheawerewithin2daysofstartingstudymedicationMortality:nonereportedP‐valuesandconfidenceintervalsnotprovidedforsafetydata
NNHR1:27R2:5R3:‐34R4:16R1:45R2:17R3:53R4:9
QualityRating:FairAnalysis:ITT,307metcriteriaforanalysis;observedcasesapproachtomissingdataapplied(missingvaluesnotimputed)OverallAttrition(R1/R2/R3/R4/P):8.5/10.5/6.5/19.0/11.6%Endpointswerenotidentifiedasapriori;itisunclearwhenadditionalendpointswereassessedRiskofBiasInternalValidity:Selection:Lowbias;computerizedrandomizationviavalidatedcomputersystemPerformance:Likelylowbias;allstudypersonnelblindedbutaformaldescriptionofdummyplacebodesignwasnotprovidedAttrition:Potentialbias;<20%inallarms,howeverbetweengroupdifferencesare>10%betweenR1andplaceboarmsAdherence:PatientsreportedtimestudymedicationwastakendailyviaIVRSExternalValidity:PatientCharacteristics:NobaselineP‐valuesareprovided;morepatientsenrolledinplacebogroup;characteristicsappearsimilarbetweentreatmentgroups.Resultsmaynotreflectresponsegeneralpopulationw/respecttoraceorage.Setting:U.S.geographicregionandtreatmentgroupusedasfixedeffecttermsforanalysisofcovarianceinsteadoftrialcentersincetrialwasconductedat57clinicalcentersOutcomes:60patientsperarmprojectedtoprovide88%powertodetecttreatmentdifferences(anticipating10patientslostperarm),howeverR4600µgarmlost12patients.Additionalendpointsreliedonnon‐validatedinstruments(meanchangesinabpain,constipationseverity,bloating,straining,andglobalrelief);thereforeresultsmustbeinterpretedwithcaution.PrimaryendpointhasbecomemorerigorousforrecentphaseIIItrials.
Studydesignabbreviations:DB=double‐blind,RCT=randomizedtrial,PC=placebo‐controlled,PG=parallel‐group,MC=multi‐center.Resultsabbreviations:OR=OddsRatio,NNT=numberneededtotreat,NNH=numberneededtoharm,CI=confidenceintervalQualityRating:Good‐likelyvalid;Fair‐likelyvalid/possiblyvalid;Poor‐fatalflaw‐notvalid
Page 14
14
Appendix1:SpecificDrugInformationCLINICALPHARMACOLOGY1Linaclotideisstructurallyrelatedtoendogenousguanylinpeptidesandactsasaguanylatecyclase‐C(GC‐C)agonist.Guanylatecyclase‐Cispresentontheluminalsurfaceofintestinalepithelium.LinaclotideanditsactivemetabolitebindtoGC‐Candstimulateincreasesinintracellularandextracellularcyclicguanosinemonophosphate(cGMP).Withinintestinalepithelialcells,increasesincGMPinitiateasignal‐transductioncascadethatactivatesthecysticfibrosistransmembraneconductanceregulator(CFTR)ionchannel.Thisresultsinsecretionofchlorideandbicarbonateionsintotheintestinallumen,whichultimatelyresultsinincreasedintestinalfluidandacceleratedintestinaltransit.LinaclotidemediatedincreaseincGMPisthoughttobethemechanismthatleadstoareductioninintestinalpainsymptoms,sinceincreasedcGMPhasbeenshowntodecreasetheactivityofpain‐sensingnervesinanimalmodels.PHARMACOKINETICS1Parameter Result
OralBioavailability
Lowsystemicbioavailability;belowthelimitofquantitationwith145mcgand290mcgdoses
ProteinBinding
PlasmaconcentrationsfollowingPOdosesarenotmeasurable,thereforedegreeofbindingcannotbecalculated
Elimination
Eliminatedinfeces.Recoveryinstoolaverages5%(fasted)and3%(fed),virtuallyallasactivemetabolite.
Half‐LifeStandardPKparameterscannotbecalculated
Metabolism
MetabolizedbytheGItracttoactivemetaboliteMM419447thatlacksthetyrosinemoiety.Drugandmetaboliteareproteolyticallydegradedinthelumentosmallerpeptidesandaminoacids.
Page 15
15
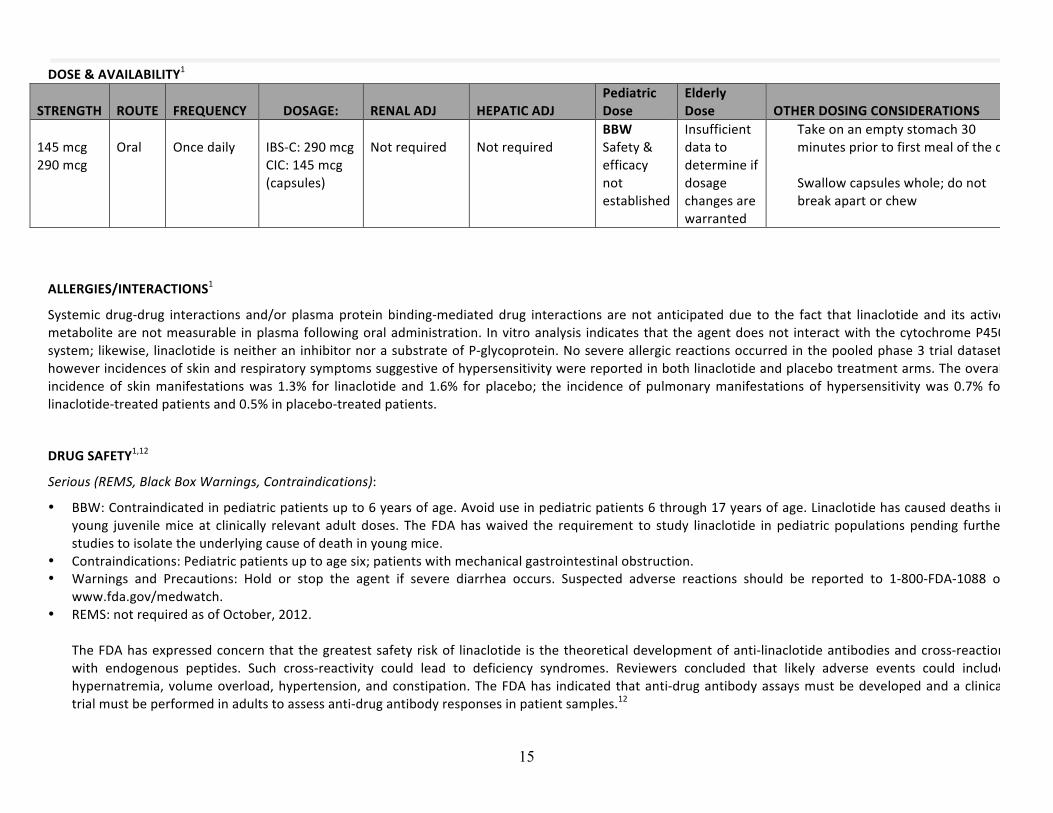
DOSE&AVAILABILITY1
STRENGTH ROUTE FREQUENCY DOSAGE: RENALADJ HEPATICADJPediatricDose
ElderlyDose OTHERDOSINGCONSIDERATIONS
145mcg290mcg
Oral
Oncedaily
IBS‐C:290mcgCIC:145mcg(capsules)
Notrequired
Notrequired
BBWSafety&efficacynotestablished
Insufficientdatatodetermineifdosagechangesarewarranted
Takeonanemptystomach30minutespriortofirstmealofthedaySwallowcapsuleswhole;donotbreakapartorchew
ALLERGIES/INTERACTIONS1
Systemicdrug‐drug interactions and/or plasmaproteinbinding‐mediateddrug interactions arenot anticipateddue to the fact that linaclotide and its activemetabolitearenotmeasurable inplasmafollowingoraladministration. Invitroanalysis indicatesthattheagentdoesnot interactwiththecytochromeP450system;likewise, linaclotideisneitheraninhibitornorasubstrateofP‐glycoprotein.Nosevereallergicreactionsoccurredinthepooledphase3trialdataset,howeverincidencesofskinandrespiratorysymptomssuggestiveofhypersensitivitywerereportedinbothlinaclotideandplacebotreatmentarms.Theoverallincidence of skinmanifestationswas 1.3% for linaclotide and 1.6% for placebo; the incidence of pulmonarymanifestations of hypersensitivitywas 0.7% forlinaclotide‐treatedpatientsand0.5%inplacebo‐treatedpatients.
DRUGSAFETY1,12
Serious(REMS,BlackBoxWarnings,Contraindications):
• BBW:Contraindicatedinpediatricpatientsupto6yearsofage.Avoiduseinpediatricpatients6through17yearsofage.Linaclotidehascauseddeathsinyoung juvenilemice at clinically relevant adult doses. The FDAhaswaived the requirement to study linaclotide inpediatric populationspending furtherstudiestoisolatetheunderlyingcauseofdeathinyoungmice.
• Contraindications:Pediatricpatientsuptoagesix;patientswithmechanicalgastrointestinalobstruction.• Warnings and Precautions: Hold or stop the agent if severe diarrhea occurs. Suspected adverse reactions should be reported to 1‐800‐FDA‐1088 or
www.fda.gov/medwatch.• REMS:notrequiredasofOctober,2012.
TheFDAhasexpressedconcernthatthegreatestsafetyriskof linaclotide isthetheoreticaldevelopmentofanti‐linaclotideantibodiesandcross‐reactionwith endogenous peptides. Such cross‐reactivity could lead to deficiency syndromes. Reviewers concluded that likely adverse events could includehypernatremia,volumeoverload,hypertension,andconstipation.TheFDAhas indicatedthatanti‐drugantibodyassaysmustbedevelopedandaclinicaltrialmustbeperformedinadultstoassessanti‐drugantibodyresponsesinpatientsamples.12
Page 16
16
Look‐alike/Sound‐alike(LA/SA)ErrorRiskPotential:noneidentified.Pregnancy/Lactationrating:Pregnancyratingof“C”.Noadequate,well‐controlledstudiesoflinaclotidehavebeenperformedinpregnantwomen.Fetalaffectshavebeenobservedinanimalstudiesatdosesmuchhigherthanthe290mcgceilingdose,butonlywithmaternaltoxicity.Therefore,linaclotideshouldbeusedinpregnancyonlywhenthebenefitoutweighstherisk.Itisunknownwhetherlinaclotideisexcretedinhumanbreastmilk,howeverplasmalevelsoflinaclotideanditsmetabolitearenotmeasurableatapproveddoses.Cautioniswarrantedwhentheagentisadministeredtonursingwomen.Tolerability:DiarrheawasthemostcommonadversereactionreportedinIBS‐CandCICpatients.Severediarrheaoccurredatarateof2%forpatientstreatedwithboththe145mcgand290mcgdosesoflinaclotide,vs.lessthan1%ofplacebo‐treatedpatients.Overall,5%oflinaclotide‐treatedpatientsdiscontinuedduetodiarrheavs.lessthan1%ofplacebo‐treatedpatients.Diarrheaoccurredinthefirsttwoweeksoftreatmentforthemajorityofpatientstreatedwithlinaclotide.8%ofCICpatientstreatedwithlinaclotideand4%ofplacebo‐treatedpatientsdiscontinuedtreatmentprematurelyduetoadversereactions.
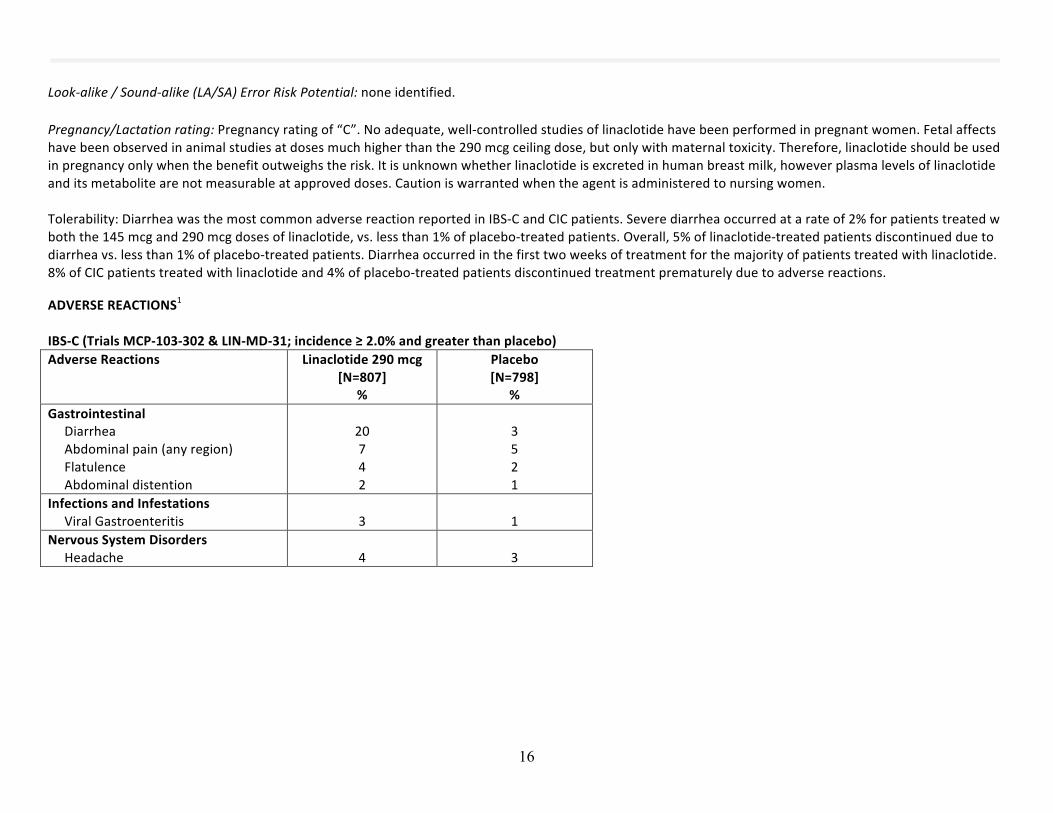
ADVERSEREACTIONS1IBS‐C(TrialsMCP‐103‐302&LIN‐MD‐31;incidence≥2.0%andgreaterthanplacebo)AdverseReactions Linaclotide290mcg
[N=807]%
Placebo[N=798]
%GastrointestinalDiarrheaAbdominalpain(anyregion)FlatulenceAbdominaldistention
20742
3521
InfectionsandInfestationsViralGastroenteritis
3
1
NervousSystemDisordersHeadache
4
3
Page 17
17
CIC(TrialsLIN‐MD‐31andMCP‐103‐302;incidence≥2.0%andgreaterthanplacebo)AdverseReactions Linaclotide145mcg
[N=430]%
Placebo[N=423]
%GastrointestinalDiarrheaAbdominalpain(anyregion)FlatulenceAbdominaldistention
16763
5652
InfectionsandInfestationsUpperrespiratorytractinfectionSinusitis
53
42
Page 18
18
References1.Linzess.PrescribingInformation.ForestPharmaceuticals.St.Louis,MO,August2012.Availableonlineat:http://www.frx.com/pi/linzess_pi.pdf.AccessedOctober16,2012.2.RomeFoundation,Inc.AppendixA:RomeIIIdiagnosticcriteriaforfunctionalgastrointestinaldisorders.LastmodifiedJune2,2006.PDFavailableonlineatwww.romecriteria.org/criteria.AccessedOctober16,2012.3.WaldA.Clinicalmanifestationsanddiagnosisofirritablebowelsyndrome.In:UpToDate,Basow,DS(Ed),UpToDate,Waltham,MA,2012.TopiclastupdatedJuly23,2012.AccessedOctober18,2012.4.RaoS,etal.A12‐week,randomized,controlledtrialwitha4‐weekrandomizedwithdrawalperiodtoevaluatetheefficacyandsafetyoflinaclotideinirritablebowelsyndromewithconstipation.AmJGastroenterol.2012;September:1‐11.[epubaheadofprint]5.Lexi‐Comp,Inc.(Lexi‐DrugsTM).Lubiprostone:druginformation.Lexi‐Comp,Inc.;Copyright2012forhandheld.LastupdatedOctober19,2012.AccessedOctober19,2012.6.LemboAJ,etal.Tworandomizedtrialsoflinaclotideforchronicconstipation.NEJM.2011;365;527‐36.7.WaldA.Etiologyandevaluationofchronicconstipationinadults.In:UpToDate,Basow,DS(Ed),UpToDate,Waltham,MA,2012.TopiclastupdatedAugust22,2012.AccessedOctober18,2012.8.FordAC,SuaresNC.Effectoflaxativesandpharmacologicaltherapiesinchronicidiopathicconstipation:systematicreviewandmeta‐analysis.Gut.2011;60:209‐218.9.NICETechnologyAppraisalGuidance.Prucaloprideforthetreatmentofchronicconstipationinwomen.Reviewavailableonlineathttp://publications.nice.org.uk/prucalopride‐for‐the‐treatment‐of‐chronic‐constipation‐in‐women‐ta211/guidance.IssuedDecember,2010.AccessedNovember6,2012.10.RamkumarD,RaoS.Efficacyandsafetyoftraditionalmedicaltherapiesforchronicconstipation:systematicreview.AmJGastroenterol.2005;100:936‐971.11.CheyWD,etal.Linaclotideforirritablebowelsyndromewithconstipation:a26‐week,randomized,double‐blind,placebo‐controlledtrialtoevaluateefficacyandsafety.AmJGastroenterol.2012;July:1‐11.[epubaheadofprint]12.Linzess,FDACenterforDrugEvaluationandResearch.SummaryReview.PublishedAugust29,2012.PDFavailableonlineathttp://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/202811Orig1s000SumR.pdf.AccessedOctober16,2012.13.LemboAJ,etal.Efficacyoflinaclotideforpatientswithchronicconstipation.Gastroenterology.2010;138:886‐895.14.JohnstonJM,KurtzCB,MacDougallJE,etal.LinaclotideimprovesabdominalpainandbowelhabitsinaphaseIIbstudyofpatientswithirritablebowelsyndromewithconstipation.Gastroenterology.2010;139:1877‐1886.15.Amitiza.PrescribingInformation.SucampoPharmaceuticals,Inc.Bethesda,MD,February2011.Availableonlineathttp://www.amitiza.com/default.aspx.AccessedNovember2,2012.