354
New Hospitals Programme Barts and the London NHS Trust July 2006

New Hospitals Programme Barts and the London NHS Trust July 2006
New Hospitals Programme
Version 11
Document Control Sheet Organisation Barts and the London NHS Trust
Document Title New Hospitals Programme Full Business Case
Version 11
Status Version 11 of the FBC
Author New Hospitals Programme Team, Barts and The London NHS Trust
Date February 2009
Further copies from Email: [email protected] Quality Assurance By: Barts and The London NHS Trust
Document History
Version Date Author Comments
01 19 May 2005 Tim Keenan Trevor Doherty
Reformatted and re-presented Trust text. NOT COMPLETE. Awaiting update to activity modelling and Trust QA.
02 20 May 2005 Tim Keenan Trevor Doherty
Inclusive of first text and Q&A. Addition of missing finance and activity data.
03 2 June 2005 Graham Scott xxxxx xxxxxx
Appendix reconciliation. Partial QA by Trust
04 27 June 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite
Revised to incorporate responses to queries raised by the Capital Investment Unit and the North East London Strategic Health Authority
05 23 August 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite xxxxx xxxxxx
Revised to incorporate queries raised by the first integrated review of the CIU, NELSHA and DH.
06 07 September 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite
Revised to incorporate responses to further queries raised by the CIU and NELSHA
07 16 September 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite
Revised to incorporate responses to further queries raised by the CIU and NELSHA
08 23 September 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite
Revised to incorporate responses to further queries raised by the CIU and NELSHA
09 18 November 05
Graham Scott Vince Chalmers John Goulston Lee Outhwaite
Revised to incorporate responses to queries raised by the Department of Health
New Hospitals Programme
Version 11
9.5 31 March 06 Graham Scott Vince Chalmers John Goulston
Incorporating DH and CIU comments to receive approval in conjunction with the Addendum to the FBC 31 March 06.
10 26 May 2006 Graham Scott John Goulston Morag Jackson
Revised in line with the Addendum to the FBC to reflect the approved scheme.
10.1 20 July 2006 John Goulston Graham Scott
Revised to incorporate CIU, SHA and DH comments on version 10.
11 January 2009 John Goulston Matthew Tulley Graham Scott
Revised to incorporate Descoping
New Hospitals Programme
Version 11
Contents EXECUTIVE SUMMARY............................................................................................................ i
1 STRATEGIC CONTEXT............................................................................................... 1 1.1 Introduction ................................................................................................................... 1 1.2 Overview of Barts and The London NHS Trust ............................................................ 1 1.3 The North East London Strategic Health Authority (NELSHA) .................................... 1 1.4 Population Projections.................................................................................................. 1 1.5 The North East London Health Economy..................................................................... 1 1.6 From Tomlinson to Turnberg: Strategic Reviews......................................................... 1 1.7 Chapter Conclusion ...................................................................................................... 1 1.8 Chapter Appendices ..................................................................................................... 1 2 THE CASE FOR CHANGE .......................................................................................... 1 2.1 Strategic Pressures for Change ................................................................................... 1 2.2 Trust–Specific Factors for Change............................................................................... 1 2.3 Chapter Conclusion ...................................................................................................... 1 2.4 Chapter Appendices ..................................................................................................... 1 3 NEW MODELS OF CARE............................................................................................ 1 3.1 Introduction ................................................................................................................... 1 3.2 Clinical Development Plan............................................................................................ 1 3.3 Outcome of the CDP .................................................................................................... 1 3.4 New Models of Care ..................................................................................................... 1 3.5 Emergency Care Model................................................................................................ 1 3.6 New Elective Care Model ............................................................................................. 1 3.7 New Planned Acute Care Model .................................................................................. 1 3.8 The Clinical Facilities for the Models of Care ............................................................... 1 3.9 Implication of New Models of Care for RLH ................................................................. 1 3.10 Implication of New Models of Care for SBH ................................................................. 1 3.11 Chapter Conclusion ...................................................................................................... 1 3.12 Chapter Appendices ..................................................................................................... 1 4 REVIEW OF THE OUTLINE BUSINESS CASE.......................................................... 1 4.1 Introduction ................................................................................................................... 1 4.2 Summary of the Outline Business Case....................................................................... 1 4.3 Review of OBC ............................................................................................................. 1 4.4 Changes Since OBC Approval: Beds........................................................................... 1 4.5 Changes Since OBC Approval: Capital Costs.............................................................. 1 4.6 Benchmarking............................................................................................................... 1 4.7 Revenue Costs Changes Since OBC Approval ........................................................... 1 4.8 Advance Schemes........................................................................................................ 1 4.9 Chapter Conclusion ...................................................................................................... 1 4.10 Chapter Appendices ..................................................................................................... 1 5 THE PUBLIC SECTOR COMPARATOR..................................................................... 1 5.1 Introduction ................................................................................................................... 1 5.2 Description of the PSC ................................................................................................. 1 5.3 Phasing for the PSC ..................................................................................................... 1 5.4 Calculation of the PSC – Capital Costs Methodology .................................................. 1 5.5 Changes Following OBC .............................................................................................. 1 5.6 PSC Approach – Non-Clinical Service ......................................................................... 1 5.7 PSC Capital Costs........................................................................................................ 1 5.8 Land Sales.................................................................................................................... 1 5.9 Lifecycle Costs.............................................................................................................. 1
New Hospitals Programme
Version 11
5.10 Revenue Costing Principles ......................................................................................... 1 5.11 Capital Charges............................................................................................................ 1 5.12 Clinical Costs ................................................................................................................ 1 5.13 Non-Clinical Costs ........................................................................................................ 1 5.14 Summary of Revenue Costs......................................................................................... 1 5.15 Audit Trail of Beds, Space and Capital Costs .............................................................. 1 5.16 Chapter Conclusion ...................................................................................................... 1 5.17 Chapter Appendices ..................................................................................................... 1 6 THE PFI PROCUREMENT PROCESS........................................................................ 1 6.1 Introduction ................................................................................................................... 1 6.2 Outline of the Scheme .................................................................................................. 1 6.3 Structure of the Project................................................................................................. 1 6.4 Stakeholder Engagement ............................................................................................. 1 6.5 The Procurement Strategy ........................................................................................... 1 6.6 Procurement Process ................................................................................................... 1 6.7 Project Agreement........................................................................................................ 1 6.8 Funding Support ........................................................................................................... 1 6.9 CABE ............................................................................................................................ 1 6.10 GLA Involvement in the Planning Application .............................................................. 1 6.11 Audit of PFI Procurement Process ............................................................................... 1 6.12 Gateway Review........................................................................................................... 1 6.13 Chapter Conclusion ...................................................................................................... 1 6.14 Chapter Appendices ..................................................................................................... 1 7 THE PREFERRED SOLUTION.................................................................................... 1 7.1 Introduction ................................................................................................................... 1 7.2 The Consortium Members ............................................................................................ 1 7.3 How the Consortium will Work with the Trust............................................................... 1 7.4 The Funding Structure.................................................................................................. 1 7.5 Description of the New Hospitals Design Solution ....................................................... 1 7.6 Communicating the design solution.............................................................................. 1 7.7 Decanting, Construction and Commissioning Programme........................................... 1 7.8 Fire Strategy ................................................................................................................. 1 7.9 Transport and Access Arrangements........................................................................... 1 7.10 FM Services – The Approach Adopted ........................................................................ 1 7.11 Equipment – The Approach Adopted ........................................................................... 1 7.12 Approach to IT/Telecommunications............................................................................ 1 7.13 The Sustainability of the Preferred Solution ................................................................. 1 7.14 Benefits to the Hospital Community ............................................................................. 1 7.15 Chapter Conclusion ...................................................................................................... 1 7.16 Chapter Appendices ..................................................................................................... 1 8 FINANCING THE SCHEME ......................................................................................... 1 8.1 Introduction ................................................................................................................... 1 8.2 Overview of the PFI Deal.............................................................................................. 1 8.3 Approach and Solution to Funding ............................................................................... 1 8.4 Funding Competition .................................................................................................... 1 8.5 Cost Assumptions Underlying the Level of Service Payment ...................................... 1 8.6 The Consortium’s Financing Proposal.......................................................................... 1 8.7 Method of Funding........................................................................................................ 1 8.8 Description of the Financial Model and Auditing Undertaken ...................................... 1 8.9 Financial Adviser’s Commentary on the Funding Structure ......................................... 1 8.10 Conclusion .................................................................................................................... 1 8.11 Chapter Appendices ..................................................................................................... 1 9 ECONOMIC APPRAISAL ............................................................................................ 1 9.1 Introduction ................................................................................................................... 1
New Hospitals Programme
Version 11
9.2 Green Book Methodology............................................................................................. 1 9.3 Description of the Assumptions used for the Economic Appraisal............................... 1 9.4 Details of how the PSC was calculated........................................................................ 1 9.5 Net Present Costs......................................................................................................... 1 9.6 Impact of Extending the Concession............................................................................ 1 9.7 Sensitivity Analysis: Switching Points........................................................................... 1 9.8 Chapter Conclusion ...................................................................................................... 1 9.9 Chapter Appendices ..................................................................................................... 1 10 ACCOUNTING TREATMENT...................................................................................... 1 10.1 Accounting for Land and Buildings............................................................................... 1 10.2 Summary of Projected Key Asset Values..................................................................... 1 10.3 Equipment..................................................................................................................... 1 10.4 Impact on accounting treatment of changes to the FBC from December 2005 ........... 1 10.5 Accounting Treatment of the Annual Service Charge .................................................. 1 10.6 Impairments .................................................................................................................. 1 10.7 VAT Treatment ............................................................................................................. 1 10.8 Conclusion .................................................................................................................... 1 10.9 Chapter Appendices ..................................................................................................... 1 11 AFFORDABILITY ANALYSIS ..................................................................................... 1 11.1 Overview....................................................................................................................... 1 11.2 Financial Performance.................................................................................................. 1 11.3 Affordability at Preferred Bidder Letter Stage............................................................... 1 11.4 Efficiency ...................................................................................................................... 1 11.5 Affordability at FBC/Financial Close............................................................................. 1 11.6 Affordability and Payment by Results........................................................................... 1 11.7 Market Forces Factor ................................................................................................... 1 11.8 Activity Modelling for PCTs........................................................................................... 1 11.9 Productivity Assumptions in the FBC and Activity Reconciliation to OBC Stage......... 1 11.10 Response of PCTs to the Activity Modelling ................................................................ 1 11.11 Other Income................................................................................................................ 1 11.12 Expenditure................................................................................................................... 1 11.13 NHS Bank Transitional Relief for PFI Schemes ........................................................... 1 11.14 Summary of Affordability of Scheme ............................................................................ 1 11.15 Affordability ................................................................................................................... 1 11.16 Sensitivity Analysis ....................................................................................................... 1 11.17 Handling Strategy for Changes to the Base Case Income & Expenditure Model ........ 1 11.18 Balance Sheet .............................................................................................................. 1 11.19 Chapter Conclusion ...................................................................................................... 1 11.20 Chapter Appendices ..................................................................................................... 1 12 RISK ANALYSIS.......................................................................................................... 1 12.1 Introduction ................................................................................................................... 1 12.2 Risk Methodology ......................................................................................................... 1 12.3 Risk Identification.......................................................................................................... 1 12.4 Risk Assessment and Quantification............................................................................ 1 12.5 Risk Management......................................................................................................... 1 12.6 Risks Transferred to the PFI Partner............................................................................ 1 12.7 Retained Risks.............................................................................................................. 1 12.8 Maximum Financial Risk Exposure .............................................................................. 1 12.9 Chapter Conclusion ...................................................................................................... 1 12.10 Chapter Appendices ..................................................................................................... 1 13 EQUIPMENT ................................................................................................................ 1 13.1 Introduction ................................................................................................................... 1 13.2 Trust Approach to Equipment....................................................................................... 1 13.3 Assessment of Equipment Requirements .................................................................... 1
New Hospitals Programme
Version 11
13.4 Procurement Options.................................................................................................... 1 13.5 Project Co.’s Equipment Responsibilities..................................................................... 1 13.6 The Managed Equipment Service ................................................................................ 1 13.7 Transfer of equipment .................................................................................................. 1 13.8 Equipment Costs .......................................................................................................... 1 13.9 IT Costs ........................................................................................................................ 1 13.10 Chapter Conclusion ...................................................................................................... 1 13.11 Chapter Appendices ..................................................................................................... 1 14 PROGRAMME MANAGEMENT ARRANGEMENTS .................................................. 1 14.1 Introduction ................................................................................................................... 1 14.2 Objectives for the Implementation Phase..................................................................... 1 14.3 Project Management Milestones -Timetable to Completion......................................... 1 14.4 Programme Management Structure ............................................................................. 1 14.5 Programme Support Office........................................................................................... 1 14.6 Programme Implementation (Team) Structure............................................................. 1 14.7 Project Management Costs .......................................................................................... 1 14.8 The Descoping Project Team....................................................................................... 1 14.9 Programme Management – Business Continuity ......................................................... 1 14.10 Control Arrangements .................................................................................................. 1 14.11 Interface with Capital Hospitals Limited (CHL)............................................................. 1 14.12 Post-Project Evaluation ................................................................................................ 1 14.13 Chapter Conclusion ...................................................................................................... 1 14.14 Appendices ................................................................................................................... 1 15 PROJECT AGREEMENT SUMMARY......................................................................... 1 15.1 Introduction ................................................................................................................... 1 15.2 Change in Law.............................................................................................................. 1 15.3 Construction Cost Inflation ........................................................................................... 1 15.4 Look Forward Test........................................................................................................ 1 15.5 Delay Events/Excusing Causes.................................................................................... 1 15.6 Interim Services............................................................................................................ 1 15.7 Insurance and Indemnities of Existing Buildings .......................................................... 1 15.8 Insurance Price Adjustments........................................................................................ 1 15.9 Advance Works............................................................................................................. 1 15.10 Site and Ground Risk Allocation................................................................................... 1 15.11 Managed Equipment Service ....................................................................................... 1 15.12 Sterile Services............................................................................................................. 1 15.13 Benchmarking and Market Testing............................................................................... 1 15.14 Compensation on Termination ..................................................................................... 1 15.15 Payment Mechanism .................................................................................................... 1 15.16 Payment in Advance..................................................................................................... 1 15.17 Descoping Variations.................................................................................................... 1 15.18 Chapter Conclusion ...................................................................................................... 1 15.19 Chapter Appendices ..................................................................................................... 1 16 WORKFORCE, HUMAN RESOURCES AND CHANGE MANAGEMENT ................. 1 16.1 Introduction ................................................................................................................... 1 16.2 Future Workforce – Planning Assumptions .................................................................. 1 16.3 Reduction to the Scope of the Scheme........................................................................ 1 16.4 Workforce Planning Strategy........................................................................................ 1 16.5 New Models of Care ..................................................................................................... 1 16.6 Thames Gateway.......................................................................................................... 1 16.7 Technology and Design................................................................................................ 1 16.8 Efficiency Gains............................................................................................................ 1 16.9 The HR Strategy........................................................................................................... 1 16.10 Delivering HR in the NHS Plan..................................................................................... 1 16.11 Change Management to Support Models of Care........................................................ 1
New Hospitals Programme
Version 11
16.12 Working in Partnership ................................................................................................. 1 16.13 Implementing the HR Strategy ..................................................................................... 1 16.14 Change Management ................................................................................................... 1 16.15 Staffside Involvement ................................................................................................... 1 16.16 TUPE and ROE Provisions........................................................................................... 1 16.17 Chapter Conclusions .................................................................................................... 1 16.18 Chapter Appendices ..................................................................................................... 1 17 INFORMATION COMMUNICATION & TECHNOLOGY.............................................. 1 17.1 The Trust’s Information Communication and Technology Strategy ............................. 1 17.2 Strategic context for ICT............................................................................................... 1 17.3 National Context ........................................................................................................... 1 17.4 London Context ............................................................................................................ 1 17.5 The Trust’s ICT Culture ................................................................................................ 1 17.6 Scope and Timing of the CRS Implementation ............................................................ 1 17.7 ICT’s Contribution to the Objectives of the PFI Scheme.............................................. 1 17.8 ICT Training .................................................................................................................. 1 17.9 Management of Risks................................................................................................... 1 17.10 Approach to ICT in the PFI Scheme............................................................................. 1 17.11 Future Expansion and Technologies............................................................................ 1 17.12 Managing the IT Infrastructure ..................................................................................... 1 17.13 Decanting Programme.................................................................................................. 1 17.14 Chapter Conclusion ...................................................................................................... 1 17.15 Chapter Appendices ..................................................................................................... 1 18 BENEFITS REALISATION .......................................................................................... 1 18.1 Introduction ................................................................................................................... 1 18.2 The Overall Investment Objectives............................................................................... 1 18.3 Benefits Identified in the Outline Business Case.......................................................... 1 18.4 The Benefits to be Realised ......................................................................................... 1 18.5 Chapter Conclusion ...................................................................................................... 1 18.6 Chapter Appendices ..................................................................................................... 1 19 POST-PROJECT EVALUATION ................................................................................. 1 19.1 Introduction ................................................................................................................... 1 19.2 Post-Project Evaluation Objectives .............................................................................. 1 19.3 Key Deliverables........................................................................................................... 1 19.4 The Process.................................................................................................................. 1 19.5 Organisation ................................................................................................................. 1 19.6 Chapter Conclusion ...................................................................................................... 1 19.7 Chapter Appendices ..................................................................................................... 1
i
New Hospitals Programme
Version 10.1 i
EXECUTIVE SUMMARY
Introduction
1. This Full Business Case (FBC) sets out a detailed and robust case in respect of the development of a new acute teaching hospital at The Royal London Hospital in Whitechapel and the redevelopment of St Bartholomew’s Hospital (Barts) as a Cancer and Cardiac Centre of Excellence in West Smithfield, London. The London Chest Hospital, which currently forms part of the Trust, will close on completion of the scheme, its services being reprovided at Barts.
2. The Scheme will provide, for the benefit of the people of Tower Hamlets, The City of London and the wider health economy, new hospitals with the space to provide 1,248 beds (although 250 will initially be mothballed) in a modern purpose-built environment that is suitable for the provision of healthcare in the 21st century.
3. The FBC demonstrates that the preferred private finance initiative (PFI) solution, developed in partnership with the Skanska Innisfree consortium (SI), provides the best solution for the delivery of services and value for money for the National Health Service (NHS).
4. Throughout the business case references are made to documents as abbreviations, and acronyms are used. A full bibliography is provided at Appendix 0A and a list of abbreviations at Appendix 0B.
Requirement to reduce costs
5. Changes to this business case have been made in response to the concerns expressed by DH in December 2005 about affordability, and the consequent review of capital schemes announced in the NHS Operating Framework 2006/07. The financial environment in which the NHS operates has changed significantly since the Trust assessed affordability in September 2005, in particular further developments in:
■ Lower levels of funding growth to the NHS from 2008 onwards; ■ Current financial overspend of the NHS ■ The recent White Paper on care outside of hospitals; and ■ Regime (Payment by Results 2006/07) and policy (Best Research for Best Health, SIFT
revision to unit costs, etc.) changes.
6. Although Barts and The London NHS Trust has attempted to address some of these issues through a further £15 million workforce cost reduction programme (equivalent to 0.3% p.a. of turnover, over the 10 years to steady state), there are further potential downside risks over the next 10 years and these are best addressed by achieving a reduction in the unitary payment and having greater flexibility in the final scale of buildings and physical capacity.
Descoping proposals
7. As detailed below, the Trust has examined four types of adjustments to the FBC to achieve this reduction in the UC:
■ Type 1 adjustments have involved the Trust modifying the PFI scheme in an innovative way. The Trust’s output requirements and Project Co’s proposals remain as set out in the December 2005 Project Agreement (PA), but the funding provided under the contract is varied to allow flexibility in the extent to which these proposals are fully implemented within secured planning approvals. The two elements of Project Co’s proposals described below, mothballing and refurbishment in Phases 2 and 3, have been included within an
ii
New Hospitals Programme
Version 10.1 ii
amended variation schedule (Schedule 22, part 7), the effect of which is that there is no contractual obligation on them to carry out the works, unless instructed to do so by the Trust. The works will only be implemented on the basis that they are required to meet planning approvals and health need, and that they are affordable to the Trust, which is subject to Departmental approval. The schedule includes a capital figure to : carry out the works and the price to go back on the UC for the services (Appendix 1 to Schedule 22, part 7).
Under this arrangement the Trust can keep its requirements under review during the long construction period. If activity and associated income arise as projected, then additional funds will be raised.
The two elements subject to specific review in this context are:
• Mothballing two floors at The Royal London (192 beds out of 905 bed complement) and one floor at St Bartholomew’s (58 beds out of 343 bed complement) of newly built space.
• Not proceeding with certain refurbishments projected to get under way in Phase 2 and Phase 3.
• Type 2 adjustments are relatively straightforward in commercial terms and involved reducing the Interest Rate buffer. The Trust had preserved a 25bps interest rate buffer (spread on the long term index links gifts) throughout the procurement. Given the closeness to financial close and following discussions with the Department of Health and Project Co, the buffer was reduced to 5bps.
In addition, the updated position on the European Investment Bank funding was 9 bps lower.
Together this achieved savings of about £2.5 million.
Type 3 adjustments reflect capital contributions to the costs of the scheme. They fall into
two categories, namely medical equipment and enabling works:
• Medical equipment – The St Bartholomew and The Royal London Charitable Foundation has agreed in principle that it will donate equipment covering the capital cost consequences of the initial tranche of medical equipment (i.e. up to the point when the first equipment refresh requirements arises). This reduces the UC by more than £3 million per annum.
• Enabling works – Project Co had undertaken a series of enabling works with a gross capital value of approximately £8 million (construction costs). The ODPM Thames Gateway office contributed £4 million towards certain of these enabling works1.
• Type 4 adjustments represent are minor modifications to the Project Agreement and
included:
• The removal from the UC of the 0.7% construction cost inflation buffer for post-Phase 1 works. At the £100.8 million level, the UC will now fund construction cost inflation at an annual rate of 3.5% per annum. i.e. 3.5% is the agreed estimate for construction costs in phases 2 and 3.
1 See Appendix 0K for the funding agreement letter from the Office of the Deputy Prime Minister.
iii
New Hospitals Programme
Version 10.1 iii
• A potential reduction in the interim service costs which, perhaps, assumed an over-prudent level of double-running costs in the period prior to steady state.
Background
8. For many years it has been widely accepted and acknowledged that there is a need to redevelop the facilities provided at The Royal London Hospital (RLH) and Barts for the benefit of the people in East London, The City and the wider community.
9. Much of the estate is old and generally in a poor condition. It was never designed to support 21st century healthcare and is in desperate need of modernisation. Departments are not co-located for efficiency and the buildings do not lend themselves to the implementation of modern models of care. This can be seen from the North East London Strategic Health Authority’s (NELSHA) ERIC returns2 which show the Trust as the worst in its peer group for suitability of purpose.
10. The present scheme has been heavily influenced from the outset by Government-led strategic policies for healthcare in London, most notably, The London Review (Turnberg 1997)3 to pursue a two-site solution to the redevelopment of Barts and The London NHS Trust reversed the strategic direction of the original project, which had been guided by the Tomlinson report (1992)4 which recommended a single site solution based at the Royal London Hospital.
11. The original outline business case (OBC) which had been based on Tomlinson’s one-site recommendation was therefore withdrawn, and the present scheme was developed in line with the new Government’s recommendations. These recommendations are as relevant today as they were then. The SHA’s independent management consultants’ (Matrix) review of activity and affordability (See Appendix OJ) has also since endorsed the cardiac and cancer provision at Barts. The scheme involves:
• Developing and refurbishing St Bartholomew’s Hospital (SBH) for use as a specialist cancer and cardiac hospital;
• Developing and refurbishing the Royal London Hospital (RLH) to provide all other services on the Whitechapel site; and
• Closing The London Chest Hospital (LCH).
(See Chapter 1 (section 1.6) for more detail of the Government’s strategic reviews.)
12. Over the course of time, the scheme has embraced evolving strategic plans for healthcare in England. The New Hospitals Programme has been developed to deliver services in line with national policies outlined in papers such as the NHS Plan, National Service Frameworks (NSFs) and the National Cancer Plan. The affordability position reflects the developing financial implications arising from Patient Choice and Payment by Results (PbR). The Trust originally valued income and expenditure at 2005/06 pay and price levels, which includes the implications of Agenda for Change (AfC). However, this has been updated to reflect 2006/07 pay and price levels in Version 10.
13. The Trust serves a population drawn from the full economic and social spectrum and operates within areas of diverse social and economic realities, ranging from the affluence of The City of London to the acute deprivation of some parts of the East End. Details relating to the nature of the population that the Trust serves can be found in Chapter 15. Analysis has been undertaken to ensure that the scheme will be able to deliver the necessary healthcare requirements to these varied communities and will be of a suitable size to cope with the expected population growth in the Thames Gateway development area (a predicted 100,000
2 NHS Estates ERIC returns for North East London, 2004-2005. 3 The Health Service in London: A Strategic View – Sir Leslie Turnberg, 1997 [See Section 1.6]. 4 Report of the inquiry into London’s health service, medical education and research – Tomlinson, 1992 [See Section 1.6]. 5 Section 1.5 details the North East London health economy.
iv
New Hospitals Programme
Version 10.1 iv
increased population in Tower Hamlets and 310,000 increased population in other North East London Primary Care Trust (PCT) areas over the next 10 years). Although the development will have the necessary floor space to accommodate this growth, decisions on fitting out the facilities will be made when the actual growth materialises.
14. With this aim in mind, at a regional and local level the project team has worked closely with commissioning PCTs and partner organisations to ensure that the scheme will deliver added value and real benefits to the community, to patients and to the local and wider health economy. See Chapter 11 (section 11.8) and Chapter 18.
Objectives of the Scheme
15. The scheme has been developed to realise the following key objectives:
• To provide 21st century healthcare in an environment of which staff, patients and our local communities can be proud;
• To have facilities for our patients that truly reflect the Trust’s long tradition of clinical excellence;
• To provide purpose built facilities which will enable the Trust to meet the needs of patients through the implementation of Department of Health (DH) policy and guidance such as consumerism, new models of care and waiting time targets;
• To replace many of the existing buildings with a coherent structure, purpose-built to support the delivery of 21st century clinical care, while sympathetic to the historic buildings which form part of the Trust;
• To reduce the backlog maintenance of today’s ageing building stock and introduce output-based standards that will ensure a “nearly new” quality for at least 30 years;
• To design and provide buildings that will be able to respond flexibly to the Trust’s evolving clinical strategy and advances in modern healthcare provision;
• To ensure that services and activities performed by the Trust will continue safely during the construction period, 24 hours a day, 365 days a year, with the minimum of disruption and inconvenience;
• To ensure that the scheme can support the delivery of the Trust’s long-term Pathfinder Clinical Strategy, that our services are flexible and meet the changing needs of patients, with particular emphasis on clinical excellence, patient experience, access and clinical efficiency;
• To ensure that the scheme takes into account the impact of key national NHS policies and initiatives, including Patient Choice, Payment by Results, Agenda for Change and the new Consultant Contract, as well as dovetailing with local developments such as the Thames Gateway expansion, NELSHA assumptions and GLA population forecasts, by working closely with Tower Hamlets PCT and other partner organisations;
• To protect the terms and conditions of staff being seconded or transferred to the private sector partner under the terms of Transfer of Undertakings Protection of Employment (TUPE) legislation and Retention of Employment (RoE) policy;
• To put patients at the heart of the new hospitals and transform the hospital experience for millions of patients from London and beyond.
16. In addition to achieving these objectives, there are a number of key benefits that the scheme will deliver. These include the following (all of which are described in more detail in Chapter 18):
• Better access to services through the provision of better clinical adjacencies;
• Improved clinical quality of services by enabling new models of care to be introduced;
v
New Hospitals Programme
Version 10.1 v
• Improved environmental quality;
• Improved strategic fit of services with others in acute and primary care settings;
• Ability to meet national, regional and local policy imperatives;
• Improved recruitment and retention and better training and development of staff; and
• Improved cost efficiency.
The Outline Business Case (OBC)
17. In approving the OBC in February 2000, the NHS Executive recommended that a number of significant changes be made to the scheme. The main alteration being to undertake a review of the basis for the activity assumptions and to include additional beds for cardiac and acute elderly services6.
18. In response, the Trust undertook a full-scale review of clinical requirements in conjunction with the health authority at that time, East London and The City Health Authority (ELCHA), general practitioners and the Trust’s clinical staff. This review, which took into account the outcome of the National Beds Enquiry, resulted in agreement for the provision of 85 additional beds. The provision of cardiac services for Essex has subsequently been reworked for the FBC, to reflect the bed reduction associated with the transfer of cardiac activity to the new Essex Cardiac Centre, which has been calculated to be 37 beds. A full reconciliation of beds from OBC to the FBC position is set out in Chapter 4 (Figure 32). Costs of the scheme have increased as a result of this change. Other cost pressures have been introduced and accommodated as a result of building cost inflation, the implementation of the NHS Plan (particularly the modernisation agenda and consumerism) and the implementation of the National Service Frameworks. The impacts of these changes are shown in Chapter 4 (Figure 33).
The Procurement Process
19. Chapter 6 sets out in detail the procurement process followed to the appointment of a preferred bidder and demonstrates that the Trust has complied throughout the procurement process with:
• European Community (EC) public procurement rules;
• United Kingdom public procurement rules;
• Adopted guidance on PFI procurement (as set out in Public Private Partnerships in the NHS: The Private Finance Initiative Good Practice)7; and
• Subsequent publications issued by the Department of Health (DH), including The Public Private Partnership in the NHS: The Private Finance Initiative Good Practice.
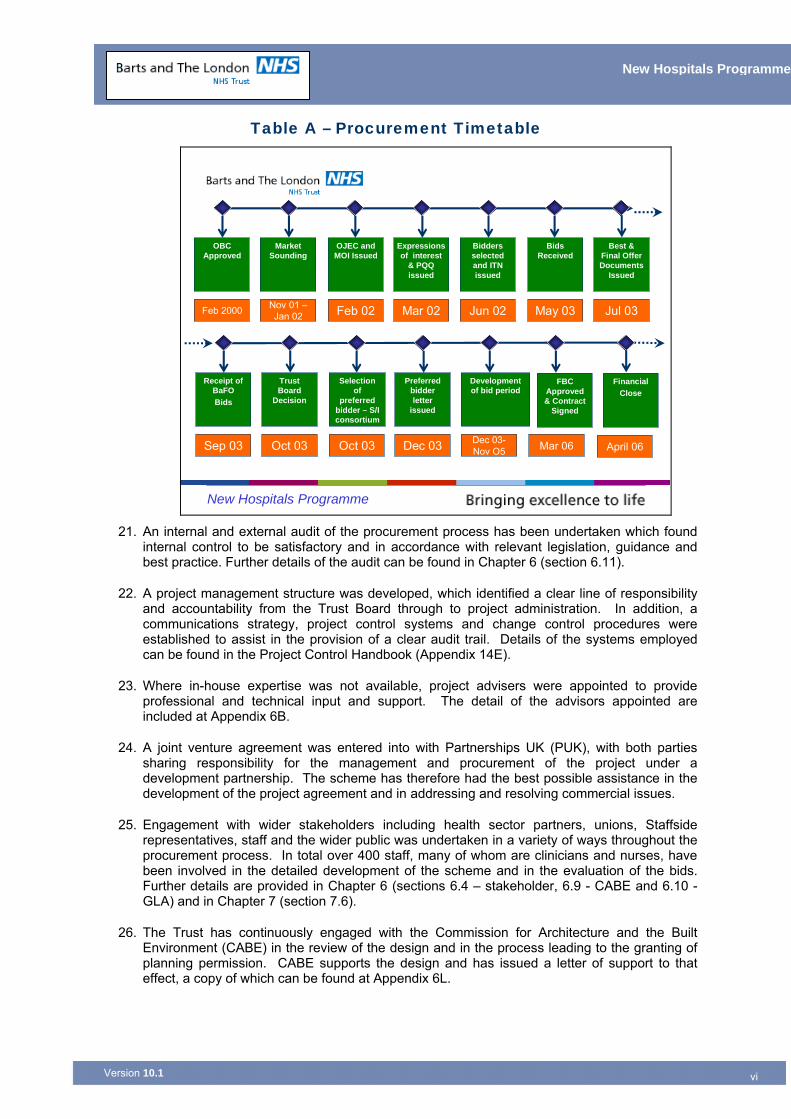
20. Key milestones in the procurement process are set out below in Table A.
6 Appendix 4F for copies of OBC approval letters containing proposed changes to the scheme. 7 See Section 6.11 for further details of the audit of the procurement process, which confirms compliance.
vi
New Hospitals Programme
Version 10.1 vi
Table A – Procurement Timetable
New Hospitals Programme
Feb 2000 Feb 02 Mar 02 Jun 02 May 03 Jul 03Nov 01 –Jan 02
OBC Approved
OJEC and MOI Issued
Expressions of interest
& PQQ issued
Bidders selected and ITN issued
Bids Received
Best & Final Offer Documents
Issued
Market Sounding
Sep 03 Oct 03 Dec 03 Dec 03-Nov O5 Mar 06Oct 03
Receipt of BaFOBids
Selection of
preferred bidder – S/I consortium
Preferred bidder letter
issued
Development of bid period
FBC Approved & Contract
Signed
Trust Board
Decision
FinancialClose
April 06
21. An internal and external audit of the procurement process has been undertaken which found
internal control to be satisfactory and in accordance with relevant legislation, guidance and best practice. Further details of the audit can be found in Chapter 6 (section 6.11).
22. A project management structure was developed, which identified a clear line of responsibility and accountability from the Trust Board through to project administration. In addition, a communications strategy, project control systems and change control procedures were established to assist in the provision of a clear audit trail. Details of the systems employed can be found in the Project Control Handbook (Appendix 14E).
23. Where in-house expertise was not available, project advisers were appointed to provide professional and technical input and support. The detail of the advisors appointed are included at Appendix 6B.
24. A joint venture agreement was entered into with Partnerships UK (PUK), with both parties sharing responsibility for the management and procurement of the project under a development partnership. The scheme has therefore had the best possible assistance in the development of the project agreement and in addressing and resolving commercial issues.
25. Engagement with wider stakeholders including health sector partners, unions, Staffside representatives, staff and the wider public was undertaken in a variety of ways throughout the procurement process. In total over 400 staff, many of whom are clinicians and nurses, have been involved in the detailed development of the scheme and in the evaluation of the bids. Further details are provided in Chapter 6 (sections 6.4 – stakeholder, 6.9 - CABE and 6.10 - GLA) and in Chapter 7 (section 7.6).
26. The Trust has continuously engaged with the Commission for Architecture and the Built Environment (CABE) in the review of the design and in the process leading to the granting of planning permission. CABE supports the design and has issued a letter of support to that effect, a copy of which can be found at Appendix 6L.
vii
New Hospitals Programme
Version 10.1 vii
27. In summary, the procurement process has followed a defined path and has been robust. PUK were involved from the outset and the Department of Health’s Private Finance Unit (PFU) were fully involved in the process of developing and agreeing the project agreement.
The Preferred Partner
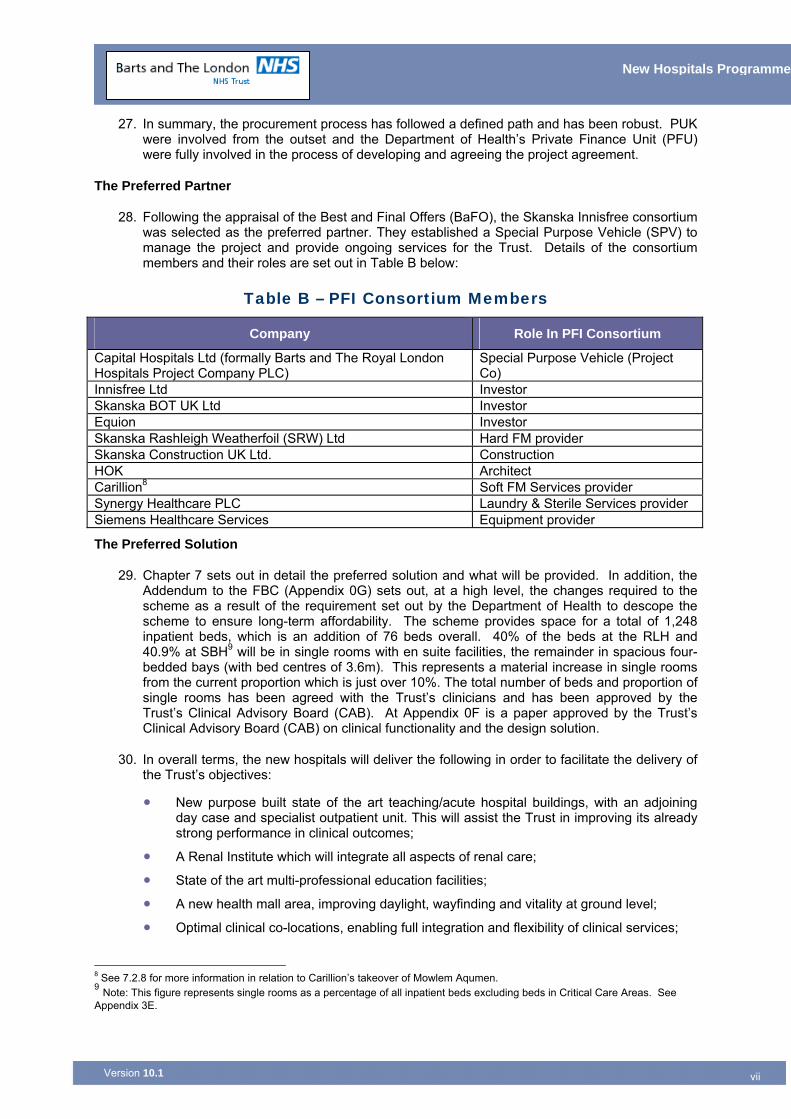
28. Following the appraisal of the Best and Final Offers (BaFO), the Skanska Innisfree consortium was selected as the preferred partner. They established a Special Purpose Vehicle (SPV) to manage the project and provide ongoing services for the Trust. Details of the consortium members and their roles are set out in Table B below:
Table B – PFI Consortium Members
Company Role In PFI Consortium
Capital Hospitals Ltd (formally Barts and The Royal London Hospitals Project Company PLC)
Special Purpose Vehicle (Project Co)
Innisfree Ltd Investor Skanska BOT UK Ltd Investor Equion Investor Skanska Rashleigh Weatherfoil (SRW) Ltd Hard FM provider Skanska Construction UK Ltd. Construction HOK Architect Carillion8 Soft FM Services provider Synergy Healthcare PLC Laundry & Sterile Services provider Siemens Healthcare Services Equipment provider
The Preferred Solution
29. Chapter 7 sets out in detail the preferred solution and what will be provided. In addition, the Addendum to the FBC (Appendix 0G) sets out, at a high level, the changes required to the scheme as a result of the requirement set out by the Department of Health to descope the scheme to ensure long-term affordability. The scheme provides space for a total of 1,248 inpatient beds, which is an addition of 76 beds overall. 40% of the beds at the RLH and 40.9% at SBH9 will be in single rooms with en suite facilities, the remainder in spacious four-bedded bays (with bed centres of 3.6m). This represents a material increase in single rooms from the current proportion which is just over 10%. The total number of beds and proportion of single rooms has been agreed with the Trust’s clinicians and has been approved by the Trust’s Clinical Advisory Board (CAB). At Appendix 0F is a paper approved by the Trust’s Clinical Advisory Board (CAB) on clinical functionality and the design solution.
30. In overall terms, the new hospitals will deliver the following in order to facilitate the delivery of the Trust’s objectives:
• New purpose built state of the art teaching/acute hospital buildings, with an adjoining day case and specialist outpatient unit. This will assist the Trust in improving its already strong performance in clinical outcomes;
• A Renal Institute which will integrate all aspects of renal care;
• State of the art multi-professional education facilities;
• A new health mall area, improving daylight, wayfinding and vitality at ground level;
• Optimal clinical co-locations, enabling full integration and flexibility of clinical services;
8 See 7.2.8 for more information in relation to Carillion’s takeover of Mowlem Aqumen. 9 Note: This figure represents single rooms as a percentage of all inpatient beds excluding beds in Critical Care Areas. See Appendix 3E.
viii
New Hospitals Programme
Version 10.1 viii
• A modern therapeutic environment, through the provision of artwork, open spaces, light and gardens;
• Future-proofing in: the flexibility of design of internal space; universally high floor loadings on the lower floors capable of supporting the heaviest equipment; generous space provision for service areas and risers, facilitating re-routing if necessary; and provision of built-in expansion space;
• A range of facilities management (FM) services; and
• An efficient operating cost base.
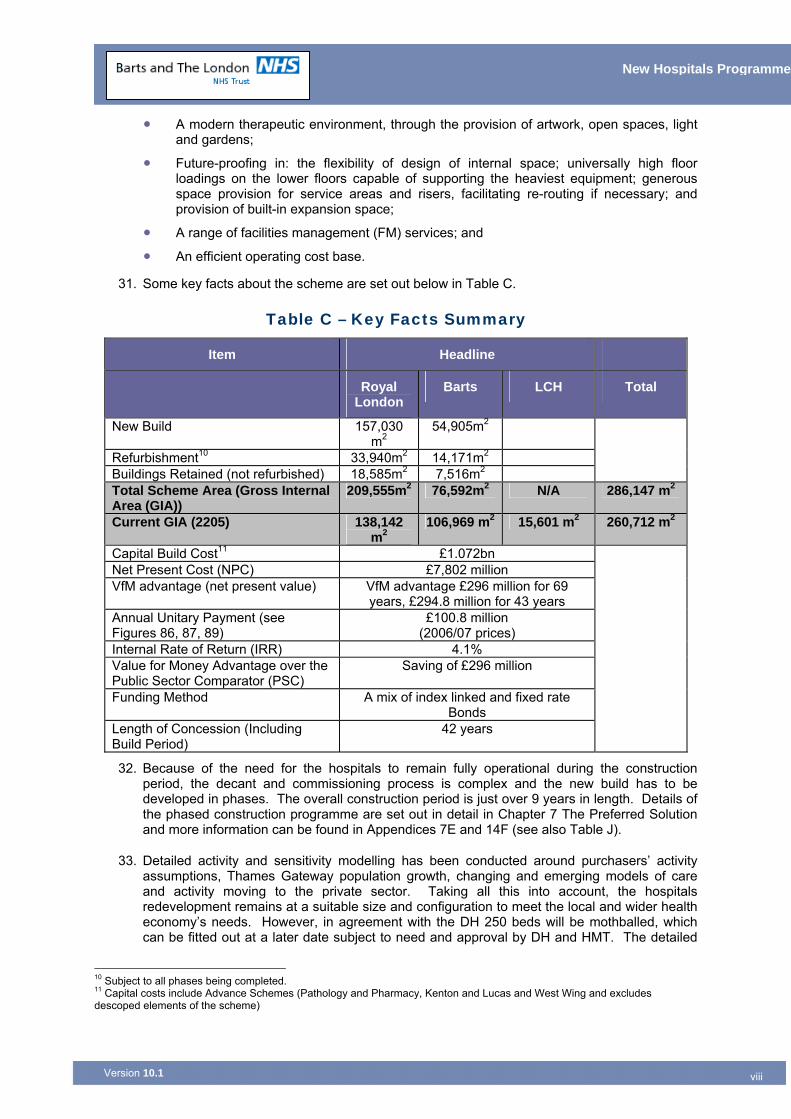
31. Some key facts about the scheme are set out below in Table C.
Table C – Key Facts Summary
Item Headline
Royal London
Barts LCH Total
New Build 157,030 m2
54,905m2
Refurbishment10 33,940m2 14,171m2 Buildings Retained (not refurbished) 18,585m2 7,516m2
Total Scheme Area (Gross Internal Area (GIA))
209,555m2 76,592m2 N/A 286,147 m2
Current GIA (2205) 138,142 m2
106,969 m2 15,601 m2 260,712 m2
Capital Build Cost11 £1.072bn Net Present Cost (NPC) £7,802 million VfM advantage (net present value) VfM advantage £296 million for 69
years, £294.8 million for 43 years Annual Unitary Payment (see Figures 86, 87, 89)
£100.8 million (2006/07 prices)
Internal Rate of Return (IRR) 4.1% Value for Money Advantage over the Public Sector Comparator (PSC)
Saving of £296 million
Funding Method A mix of index linked and fixed rate Bonds
Length of Concession (Including Build Period)
42 years
32. Because of the need for the hospitals to remain fully operational during the construction period, the decant and commissioning process is complex and the new build has to be developed in phases. The overall construction period is just over 9 years in length. Details of the phased construction programme are set out in detail in Chapter 7 The Preferred Solution and more information can be found in Appendices 7E and 14F (see also Table J).
33. Detailed activity and sensitivity modelling has been conducted around purchasers’ activity assumptions, Thames Gateway population growth, changing and emerging models of care and activity moving to the private sector. Taking all this into account, the hospitals redevelopment remains at a suitable size and configuration to meet the local and wider health economy’s needs. However, in agreement with the DH 250 beds will be mothballed, which can be fitted out at a later date subject to need and approval by DH and HMT. The detailed
10 Subject to all phases being completed. 11 Capital costs include Advance Schemes (Pathology and Pharmacy, Kenton and Lucas and West Wing and excludes descoped elements of the scheme)

ix
New Hospitals Programme
Version 10.1 ix
activity assumptions are considered in Chapter 11 (section 11.8) and take account of the Thames Gateway population expansion, based on the Health Authority’s assumptions (paragraph 1.4 provides more detail as to the population projections). In terms of the Thames Gateway development, the July 2005 Housing Capacity Study states that capacity for housing development in London has increased to an annual total of 31,500 new homes per year from the aspirational London Plan figure of 30,000 new homes per year, with 46% of this capacity in East London. This is a big increase from the original London Plan figure of 32% in East London. This indicates that the East London sub-region is now expected to contribute a much larger proportion of London's new homes than before, with a consequential greater increase in population than previously anticipated. Revised population projections are in the process of being produced.
34. This indicates that the 12-year activity model, agreed with North East London PCTs, provides a prudent estimate of likely patient care activity levels, since the increase in population is based on the lower levels of the original London Plan.
35. This is confirmed in the letters of support received from local and geographically more distant PCTs, in respect of the scheme and the ongoing activity they will support12.
36. Current average occupancy is 97% at RLH and c88% at SBH with 250 beds mothballed averages 88% across both hospitals. Key activity assumptions are set out in Table D below.
Table D – Key Activity and Performance Assumptions
37. As will be noted, the projected length of stay is anticipated to remain broadly static between 2004/05 and 2016. This is due to the increased severity and complexity of case mix expected as a result of expansion of day case surgery, improvements to primary care services and the transfer of activity to the independent sector (within Independent Sector Treatment Centres (ITSCs)).
12 See Appendix 0C for copies of commissioner support letters
Spells (elective and non elective)
Percentage Change over Base Activity
Starting Activity 2004/05 Base Activity 93,254 Cardiac Plan Adjustment (due to changes in Cardiac provision in NEL and Essex)
-1,266
Reduction in Activity due to LTC Management (net effect after reduction in growth in 2004/05)
-3,750 (7.4%) of Non Elective
Independent Sector provision of Elective Work (reduction inn Basket of 25 day case procedures)
-3,175 (7.6%) of all Elective
Thames Gateway Activity Growth (factored in)
21,349 21.8%of all activity
Resultant FCE Activity by 2016/17 106,412
x
New Hospitals Programme
Version 10.1 x
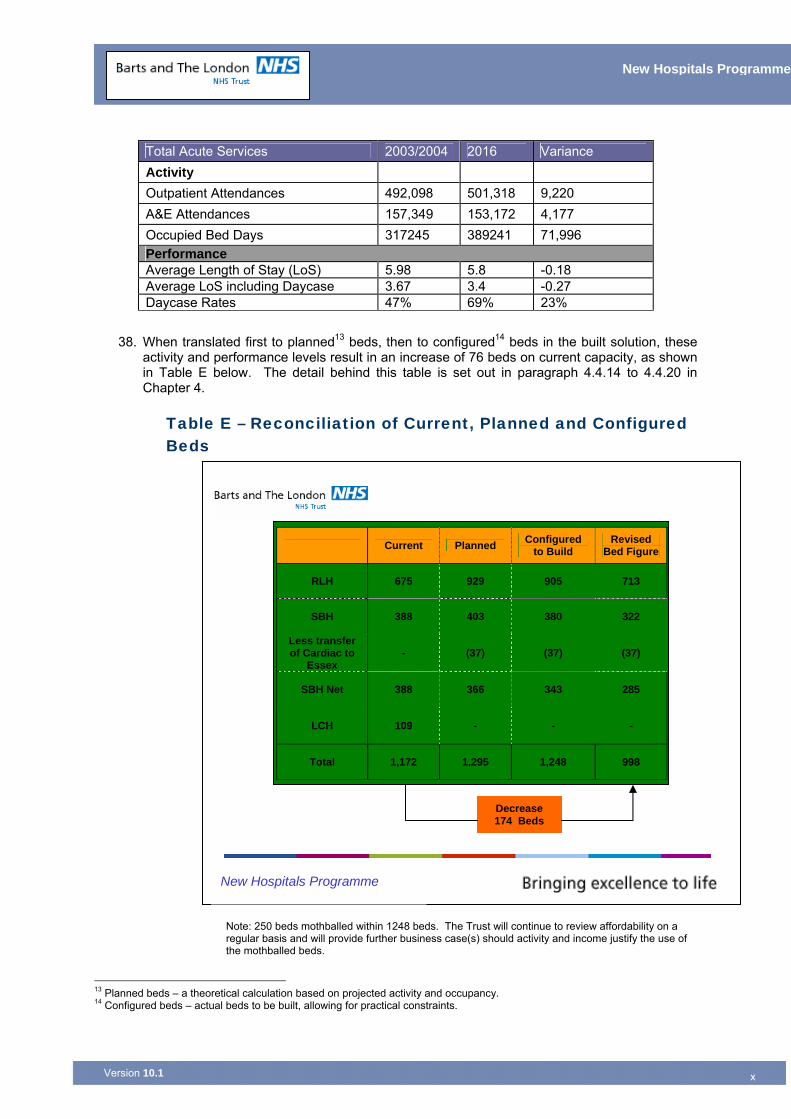
38. When translated first to planned13 beds, then to configured14 beds in the built solution, these activity and performance levels result in an increase of 76 beds on current capacity, as shown in Table E below. The detail behind this table is set out in paragraph 4.4.14 to 4.4.20 in Chapter 4.
Table E – Reconciliation of Current, Planned and Configured Beds
Note: 250 beds mothballed within 1248 beds. The Trust will continue to review affordability on a regular basis and will provide further business case(s) should activity and income justify the use of the mothballed beds.
13 Planned beds – a theoretical calculation based on projected activity and occupancy. 14 Configured beds – actual beds to be built, allowing for practical constraints.
Total Acute Services 2003/2004 2016 Variance Activity Outpatient Attendances 492,098 501,318 9,220 A&E Attendances 157,349 153,172 4,177 Occupied Bed Days 317245 389241 71,996 Performance Average Length of Stay (LoS) 5.98 5.8 -0.18 Average LoS including Daycase 3.67 3.4 -0.27 Daycase Rates 47% 69% 23%
Current Planned Configured to Build
Revised Bed Figure
RLH 675 929 905 713
SBH 388 403 380 322
Less transfer of Cardiac to
Essex - (37) (37) (37)
SBH Net 388 366 343 285
LCH 109 - - -
Total 1,172 1,295 1,248 998
Decrease 174 Beds
New Hospitals Programme
xi
New Hospitals Programme
Version 10.1 xi
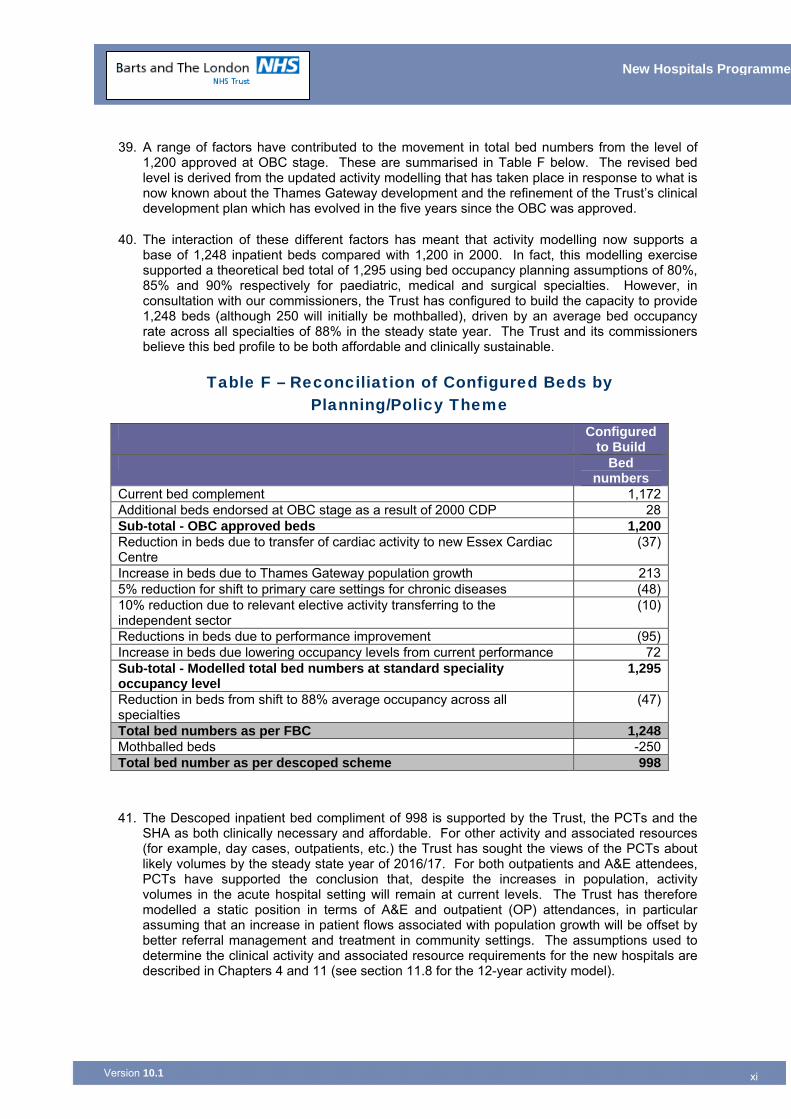
39. A range of factors have contributed to the movement in total bed numbers from the level of 1,200 approved at OBC stage. These are summarised in Table F below. The revised bed level is derived from the updated activity modelling that has taken place in response to what is now known about the Thames Gateway development and the refinement of the Trust’s clinical development plan which has evolved in the five years since the OBC was approved.
40. The interaction of these different factors has meant that activity modelling now supports a base of 1,248 inpatient beds compared with 1,200 in 2000. In fact, this modelling exercise supported a theoretical bed total of 1,295 using bed occupancy planning assumptions of 80%, 85% and 90% respectively for paediatric, medical and surgical specialties. However, in consultation with our commissioners, the Trust has configured to build the capacity to provide 1,248 beds (although 250 will initially be mothballed), driven by an average bed occupancy rate across all specialties of 88% in the steady state year. The Trust and its commissioners believe this bed profile to be both affordable and clinically sustainable.
Table F – Reconciliation of Configured Beds by Planning/Policy Theme
Configured to Build
Bed numbers
Current bed complement 1,172Additional beds endorsed at OBC stage as a result of 2000 CDP 28Sub-total - OBC approved beds 1,200Reduction in beds due to transfer of cardiac activity to new Essex Cardiac Centre
(37)
Increase in beds due to Thames Gateway population growth 2135% reduction for shift to primary care settings for chronic diseases (48)10% reduction due to relevant elective activity transferring to the independent sector
(10)
Reductions in beds due to performance improvement (95)Increase in beds due lowering occupancy levels from current performance 72Sub-total - Modelled total bed numbers at standard speciality occupancy level
1,295
Reduction in beds from shift to 88% average occupancy across all specialties
(47)
Total bed numbers as per FBC 1,248Mothballed beds -250Total bed number as per descoped scheme 998
41. The Descoped inpatient bed compliment of 998 is supported by the Trust, the PCTs and the SHA as both clinically necessary and affordable. For other activity and associated resources (for example, day cases, outpatients, etc.) the Trust has sought the views of the PCTs about likely volumes by the steady state year of 2016/17. For both outpatients and A&E attendees, PCTs have supported the conclusion that, despite the increases in population, activity volumes in the acute hospital setting will remain at current levels. The Trust has therefore modelled a static position in terms of A&E and outpatient (OP) attendances, in particular assuming that an increase in patient flows associated with population growth will be offset by better referral management and treatment in community settings. The assumptions used to determine the clinical activity and associated resource requirements for the new hospitals are described in Chapters 4 and 11 (see section 11.8 for the 12-year activity model).
xii
New Hospitals Programme
Version 10.1 xii
The Economic and Financial Case
Value for Money
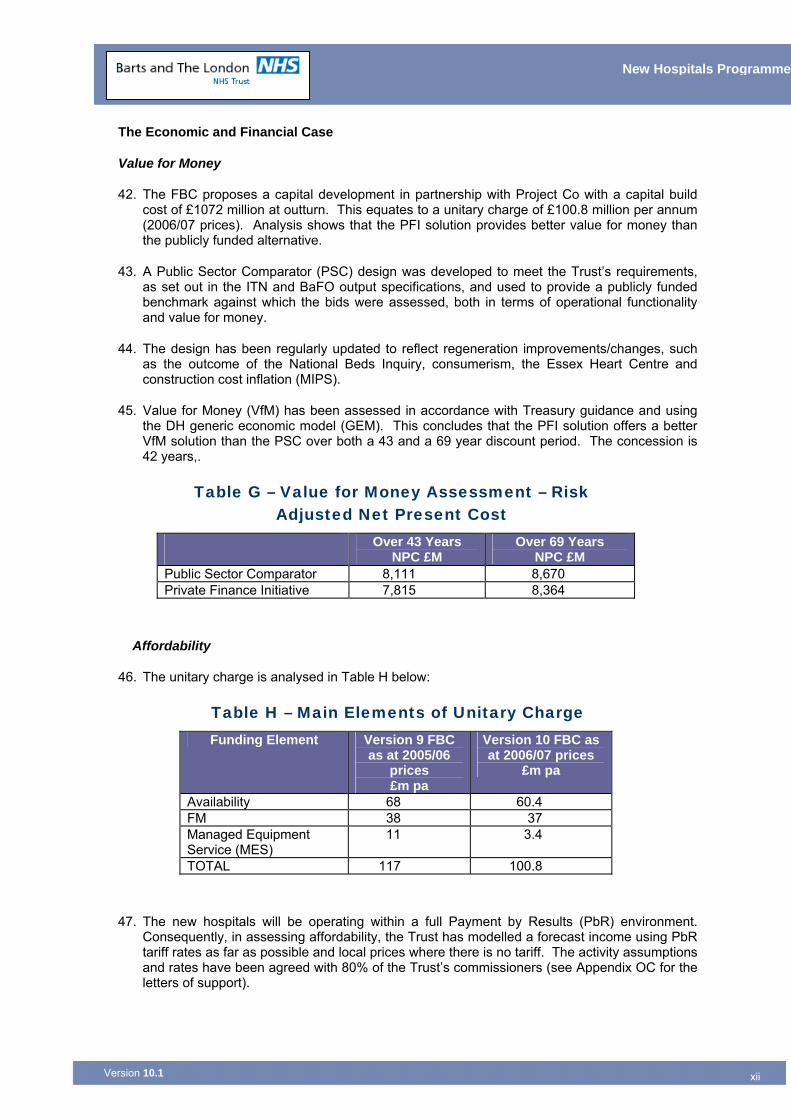
42. The FBC proposes a capital development in partnership with Project Co with a capital build cost of £1072 million at outturn. This equates to a unitary charge of £100.8 million per annum (2006/07 prices). Analysis shows that the PFI solution provides better value for money than the publicly funded alternative.
43. A Public Sector Comparator (PSC) design was developed to meet the Trust’s requirements, as set out in the ITN and BaFO output specifications, and used to provide a publicly funded benchmark against which the bids were assessed, both in terms of operational functionality and value for money.
44. The design has been regularly updated to reflect regeneration improvements/changes, such as the outcome of the National Beds Inquiry, consumerism, the Essex Heart Centre and construction cost inflation (MIPS).
45. Value for Money (VfM) has been assessed in accordance with Treasury guidance and using the DH generic economic model (GEM). This concludes that the PFI solution offers a better VfM solution than the PSC over both a 43 and a 69 year discount period. The concession is 42 years,.
Table G – Value for Money Assessment – Risk Adjusted Net Present Cost
Over 43 Years NPC £M
Over 69 Years NPC £M
Public Sector Comparator 8,111 8,670 Private Finance Initiative 7,815 8,364
Affordability
46. The unitary charge is analysed in Table H below:
Table H – Main Elements of Unitary Charge Funding Element Version 9 FBC
as at 2005/06 prices £m pa
Version 10 FBC as at 2006/07 prices
£m pa
Availability 68 60.4 FM 38 37 Managed Equipment Service (MES)
11 3.4
TOTAL 117 100.8
47. The new hospitals will be operating within a full Payment by Results (PbR) environment. Consequently, in assessing affordability, the Trust has modelled a forecast income using PbR tariff rates as far as possible and local prices where there is no tariff. The activity assumptions and rates have been agreed with 80% of the Trust’s commissioners (see Appendix OC for the letters of support).
xiii
New Hospitals Programme
Version 10.1 xiii
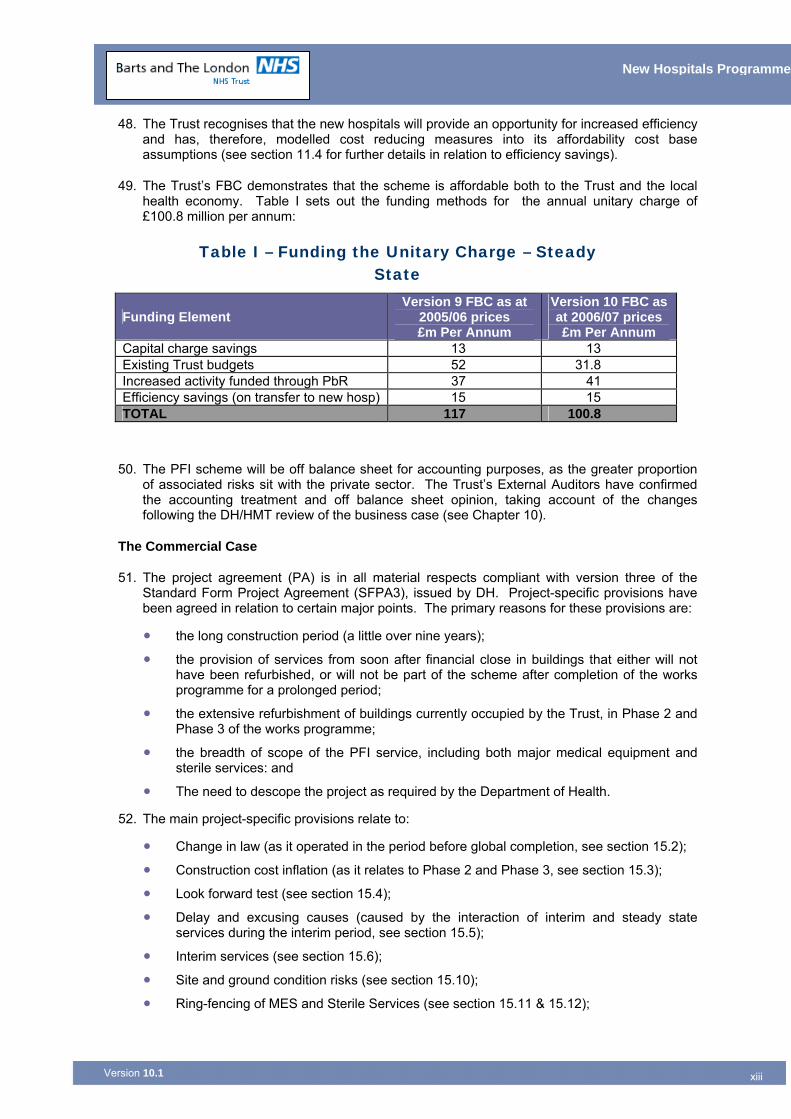
48. The Trust recognises that the new hospitals will provide an opportunity for increased efficiency and has, therefore, modelled cost reducing measures into its affordability cost base assumptions (see section 11.4 for further details in relation to efficiency savings).
49. The Trust’s FBC demonstrates that the scheme is affordable both to the Trust and the local health economy. Table I sets out the funding methods for the annual unitary charge of £100.8 million per annum:
Table I – Funding the Unitary Charge – Steady State
Funding Element Version 9 FBC as at
2005/06 prices £m Per Annum
Version 10 FBC as at 2006/07 prices £m Per Annum
Capital charge savings 13 13 Existing Trust budgets 52 31.8 Increased activity funded through PbR 37 41 Efficiency savings (on transfer to new hosp) 15 15 TOTAL 117 100.8
50. The PFI scheme will be off balance sheet for accounting purposes, as the greater proportion of associated risks sit with the private sector. The Trust’s External Auditors have confirmed the accounting treatment and off balance sheet opinion, taking account of the changes following the DH/HMT review of the business case (see Chapter 10).
The Commercial Case
51. The project agreement (PA) is in all material respects compliant with version three of the Standard Form Project Agreement (SFPA3), issued by DH. Project-specific provisions have been agreed in relation to certain major points. The primary reasons for these provisions are:
• the long construction period (a little over nine years);
• the provision of services from soon after financial close in buildings that either will not have been refurbished, or will not be part of the scheme after completion of the works programme for a prolonged period;
• the extensive refurbishment of buildings currently occupied by the Trust, in Phase 2 and Phase 3 of the works programme;
• the breadth of scope of the PFI service, including both major medical equipment and sterile services: and
• The need to descope the project as required by the Department of Health.
52. The main project-specific provisions relate to:
• Change in law (as it operated in the period before global completion, see section 15.2);
• Construction cost inflation (as it relates to Phase 2 and Phase 3, see section 15.3);
• Look forward test (see section 15.4);
• Delay and excusing causes (caused by the interaction of interim and steady state services during the interim period, see section 15.5);
• Interim services (see section 15.6);
• Site and ground condition risks (see section 15.10);
• Ring-fencing of MES and Sterile Services (see section 15.11 & 15.12);
xiv
New Hospitals Programme
Version 10.1 xiv
• Service commencement given the phased nature of the development, benchmarking and market testing (see section 15.13);
• Compensation on termination (as it relates to a bond financial scheme which includes partially ring-fenced services, see section 15.14);
• Payment in advance (see section 15.16): and
• An amended variation procedure to deal with the “descoping” variations (see section 15.17).
53. Regular contact has been maintained with the PFU as the PA developed, particularly in relation to project-specific matters. There are no material issues of concern with the position now reached.15.
54. Appropriate steps have been put in place to identify and mitigate the impact of risks retained by the Trust and which may crystallise following contract signature (See Chapter 12 and Appendix 12C).
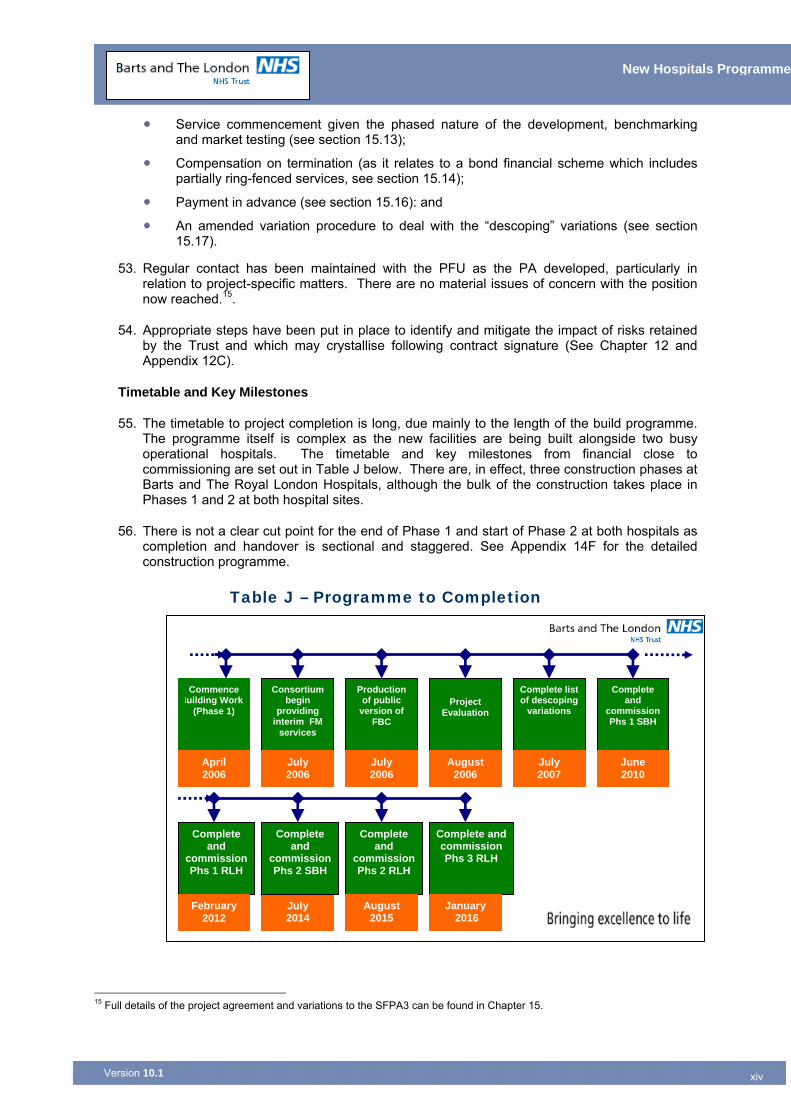
Timetable and Key Milestones
55. The timetable to project completion is long, due mainly to the length of the build programme. The programme itself is complex as the new facilities are being built alongside two busy operational hospitals. The timetable and key milestones from financial close to commissioning are set out in Table J below. There are, in effect, three construction phases at Barts and The Royal London Hospitals, although the bulk of the construction takes place in Phases 1 and 2 at both hospital sites.
56. There is not a clear cut point for the end of Phase 1 and start of Phase 2 at both hospitals as completion and handover is sectional and staggered. See Appendix 14F for the detailed construction programme.
Table J – Programme to Completion 15 Full details of the project agreement and variations to the SFPA3 can be found in Chapter 15.
Commence Building Work
(Phase 1)
Consortium begin
providing interim FM
services
Production of public
version of FBC
Project
Evaluation
Complete listof descoping
variations
Complete and
commission Phs 1 SBH
Complete and
commission Phs 1 RLH
Complete and
commission Phs 2 RLH
Complete andcommission Phs 3 RLH
April 2006
February 2012
July 2006
July 2006
August 2006
July 2007
June 2010
July 2014
August 2015
January 2016
Complete and
commission Phs 2 SBH
xv
New Hospitals Programme
Version 10.1 xv
57. As a result of the need to reduce costs of the scheme, elements of phases 2 and 3 may not be commissioned unless activity demands it and approvals are granted by DH.
58. Prior to the commencement of Phase 1, the Trust entered into a number of small publicly funded projects to enable those buildings which were in the footprint of the new build to be vacated, and thus facilitate the build programme and ensure the smooth commencement of Phase 1. These projects were grouped together as the Pre-Phase One Decant Project, the business case for which was approved by the North East London Strategic Health Authority.16
59. The Trust also procured three advanced schemes17 separately from the PFI project, all of which are complete. The principal aim of carrying out the advanced schemes ahead of the PFI development was to reduce the complexity of the staff decanting programme and thus reduce the overall development timetable.
60. Robust project management arrangements have been put in place to ensure that the construction programme proceeds to time; to monitor the administration of the contract; to address post-project evaluation; and to develop and monitor achievement of the benefits realisation programme.
61. Post-project evaluation will be carried out after each phase of the project to ensure that lessons learned will be subsumed into each subsequent phase of the scheme.
62. In summary, the project has been phased so that the Trust can continue to provide its services with the least disruption to its operations and achieve its long-term goals of “delivering excellence in healthcare’. Phasing also ensures that maximum clinical space is delivered early in the scheme at RLH (i.e. in Phase 1), with the second phase focusing principally on non-clinical space18.
Support and Approval
63. The original FBC was supported by the Trust Board and approved at a meeting on 4 May 2005. The Addendum to the FBC, which detailed the descoping required by the DH was approved by the Trust Board 29 March 2006.
64. The original FBC dated October 2005 also had the full support of Tower Hamlets PCT and the support of the North East London Strategic Health Authority, who considered the business case in June 2005 and gave approval in principle, with a number of issues to be further considered by a sub-committee of the SHA Board. This sub-committee met in September 2005 and endorsed version 8 of the FBC, with some comments which have been addressed. The Addendum was approved by the SHA.
65. Letters of support have been received from 80% of the Trust’s commissioners19.
Gateway Audit of the Scheme
66. The Project has been subject to the Gateway Project Profile model (risk score 64) and appropriate Gateway Reviews. Gateway 3 was conducted in May 2005 and the project received an amber status. An action plan addressing the recommendations from that review has been approved by the Trust Board and is being implemented. A copy of the action plan is attached at Appendix 0D.
16 See Appendix 0E for budget details in relation to Pre-Phase One Decant Schemes. 17 See section 4.8 for further details in relation to advance schemes. 18 Phase 1 of the RLH delivers 70% of all clinical space, ensuring that over 80% of clinical accommodation is delivered within five years. 19 See Letters of Support from PCTs (Appendix 0C).
xvi
New Hospitals Programme
Version 10.1 xvi
Conclusion and Recommendation
67. In conclusion, the FBC demonstrates that:
• The preferred solution gives the flexibility to meet the requirements of the modernisation agenda, The NHS Plan20, National Service Frameworks, the National Beds Inquiry21 and other national, regional and local strategies and policies and is a key element in the local health economy’s strategy for healthcare delivery in North East London, taking into account the estimated 310,000 population growth in the Thames Gateway development area;
• The preferred solution provides better value for money than the public sector comparator and also provides a superior clinical solution;
• The proposals are affordable and provide the most sound economic, commercial and financial solution for the benefit of the NHS; and
• The project management arrangements are comprehensive and appropriate for the successful delivery of the project’s objectives and associated benefits.
68. There is overwhelming support for the proposals from the Trust’s clinicians and Barts and the London Queen Mary School of Medicine and Dentistry (who have been involved with the design and evaluation process), the Trust Board (who have approved the Full Business Case) and the PCTs in North East London and Essex who have approved the activity assumptions in relation to the scheme.
69. The Trust’s lead commissioner for acute services, Tower Hamlets PCT and the North East London Strategic Health Authority have been involved throughout the development of the project and are fully supportive. In particular, the Trust’s commissioners support the activity and income assumptions associated with the development. The Department of Health and HM Treasury are therefore asked to approve the proposals set out in this Full Business Case.
Chapter Appendices
0A Bibliography 0B Abbreviations 0C Letters of Commissioner Support 0D Gateway Review Action Plan 0E Pre-Phase One Decant Schemes - Budgets 0F Clinical Ownership of the Design Solution 0G Addendum to the Full Business Case 0H Department of Health Approval of Scheme Letter 0I BLT Response to the Department of Health at Financial Close 0J Independent Management Report on Affordability 0K Funding Agreement Office of the Deputy Prime Minister
20 The NHS Plan – a Plan for Investment, a Plan for Reform, 2000. 21 “Shaping the Future NHS: Long term Planning for Hospitals & Related Services”, Department of Health, 2001.
Version 10.1
1
New Hospitals Programme
1 STRATEGIC CONTEXT Chapter Synopsis – Strategic Context
This Chapter sets out:
The two major reviews of health services in London which addressed the future of Barts and The London:
■ The first was led by Sir Bernard Tomlinson22 in 1992 and was endorsed in the Government’s response, Making London Better23 (1993). This recommended a single site solution based at The Royal London Hospital.
■ The second was undertaken by an independent advisory panel headed by Sir Leslie Turnberg in 199724 and was endorsed by the Government’s response, The Future of London’s Health Services (1998)25. This effectively reversed the recommendation of Making London Better by recommending a two site development, with Barts to become a Centre of Excellence for Cancer and Cardiac Services.
The Government’s endorsement in 1998 which provided the starting point for the development of this project by clearly stating that a twin site solution, as recommended by Turnberg, was the preferred option, with healthcare services situated at both Barts and The Royal London Hospital sites.
A summary of the distinctive and changing health needs of the local population, dominant features of which are:
■ The diversity of the health needs of the local population
■ The foreseeable population bulge with the Thames Gateway development alone set to increase the local population by over 310,000 in the next 10 years. This represents 17% of the anticipated total population of the area covered by NELSHA in 2016 which is approx 1.8 million (see Figure 7).
■ The outcome of the DH/HM Treasury review of activity projections and affordability in the light of the Government’s White Paper “Our Health, Our Care, Our Say: A New Direction for Community Services.”
1.1 Introduction 1.1.1 This chapter provides a brief overview of Barts and The London NHS Trust, the
services it delivers and the environment within which it operates.
1.1.2 This chapter also sets out the historical development of the scheme and the central policy changes that have directed the shape of the project.
1.2 Overview of Barts and The London NHS Trust 1.2.1 Barts and The London NHS Trust is one of the largest, busiest and most respected
teaching hospital trusts in the country, with some of the best clinical results in the UK. For the fourth year running, Barts and The London has maintained one of the
22 Tomlinson report: A report of the inquiry into London’s Health Service, medical education and research, HMSO 1992 23Making London Better: The Governments response to the Tomlinson Inquiry, 1993 24 The Health Service in London: A Strategic Review – Sir Leslie Turnberg, DOH 1998 25 The Future of London’s Health Services – The Government’s response to the Turnberg Review, 1998
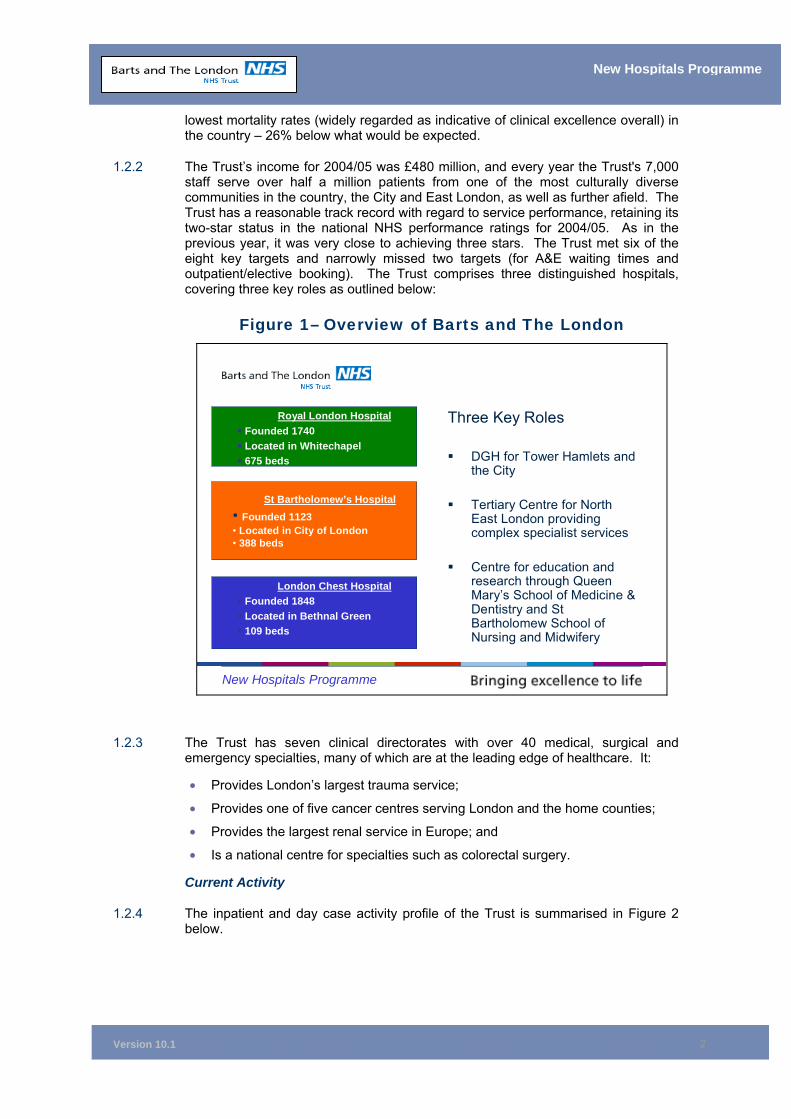
Version 10.1
2
New Hospitals Programme
lowest mortality rates (widely regarded as indicative of clinical excellence overall) in the country – 26% below what would be expected.
1.2.2 The Trust’s income for 2004/05 was £480 million, and every year the Trust's 7,000 staff serve over half a million patients from one of the most culturally diverse communities in the country, the City and East London, as well as further afield. The Trust has a reasonable track record with regard to service performance, retaining its two-star status in the national NHS performance ratings for 2004/05. As in the previous year, it was very close to achieving three stars. The Trust met six of the eight key targets and narrowly missed two targets (for A&E waiting times and outpatient/elective booking). The Trust comprises three distinguished hospitals, covering three key roles as outlined below:
Figure 1– Overview of Barts and The London
New Hospitals Programme
Royal London HospitalFounded 1740Located in Whitechapel675 beds
St Bartholomew’s Hospital• Founded 1123• Located in City of London• 388 beds
London Chest HospitalFounded 1848Located in Bethnal Green109 beds
Three Key Roles
DGH for Tower Hamlets and the City
Tertiary Centre for North East London providing complex specialist services
Centre for education and research through Queen Mary’s School of Medicine & Dentistry and St Bartholomew School of Nursing and Midwifery
1.2.3 The Trust has seven clinical directorates with over 40 medical, surgical and emergency specialties, many of which are at the leading edge of healthcare. It:
• Provides London’s largest trauma service;
• Provides one of five cancer centres serving London and the home counties;
• Provides the largest renal service in Europe; and
• Is a national centre for specialties such as colorectal surgery.
Current Activity
1.2.4 The inpatient and day case activity profile of the Trust is summarised in Figure 2 below.
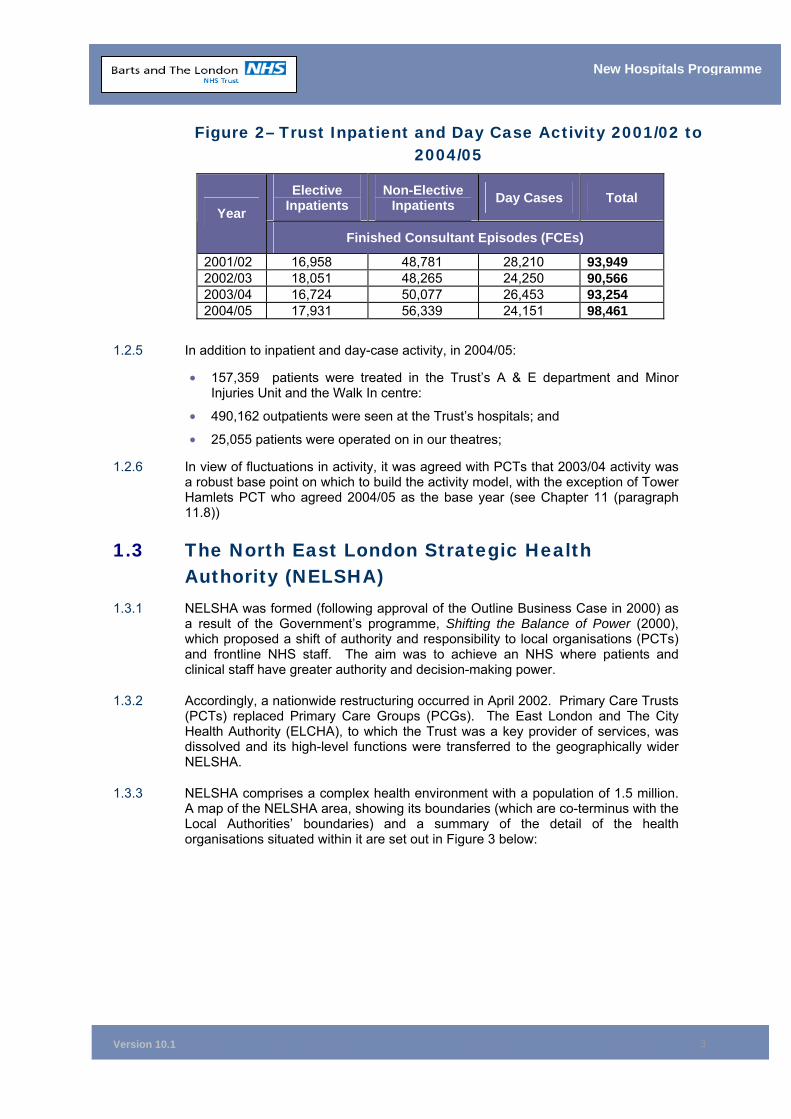
Version 10.1
3
New Hospitals Programme
Figure 2– Trust Inpatient and Day Case Activity 2001/02 to 2004/05
Elective Inpatients
Non-Elective Inpatients Day Cases Total
Year
Finished Consultant Episodes (FCEs)
2001/02 16,958 48,781 28,210 93,949 2002/03 18,051 48,265 24,250 90,566 2003/04 16,724 50,077 26,453 93,254 2004/05 17,931 56,339 24,151 98,461
1.2.5 In addition to inpatient and day-case activity, in 2004/05:
• 157,359 patients were treated in the Trust’s A & E department and Minor Injuries Unit and the Walk In centre:
• 490,162 outpatients were seen at the Trust’s hospitals; and
• 25,055 patients were operated on in our theatres;
1.2.6 In view of fluctuations in activity, it was agreed with PCTs that 2003/04 activity was a robust base point on which to build the activity model, with the exception of Tower Hamlets PCT who agreed 2004/05 as the base year (see Chapter 11 (paragraph 11.8))
1.3 The North East London Strategic Health Authority (NELSHA)
1.3.1 NELSHA was formed (following approval of the Outline Business Case in 2000) as a result of the Government’s programme, Shifting the Balance of Power (2000), which proposed a shift of authority and responsibility to local organisations (PCTs) and frontline NHS staff. The aim was to achieve an NHS where patients and clinical staff have greater authority and decision-making power.
1.3.2 Accordingly, a nationwide restructuring occurred in April 2002. Primary Care Trusts (PCTs) replaced Primary Care Groups (PCGs). The East London and The City Health Authority (ELCHA), to which the Trust was a key provider of services, was dissolved and its high-level functions were transferred to the geographically wider NELSHA.
1.3.3 NELSHA comprises a complex health environment with a population of 1.5 million. A map of the NELSHA area, showing its boundaries (which are co-terminus with the Local Authorities’ boundaries) and a summary of the detail of the health organisations situated within it are set out in Figure 3 below:
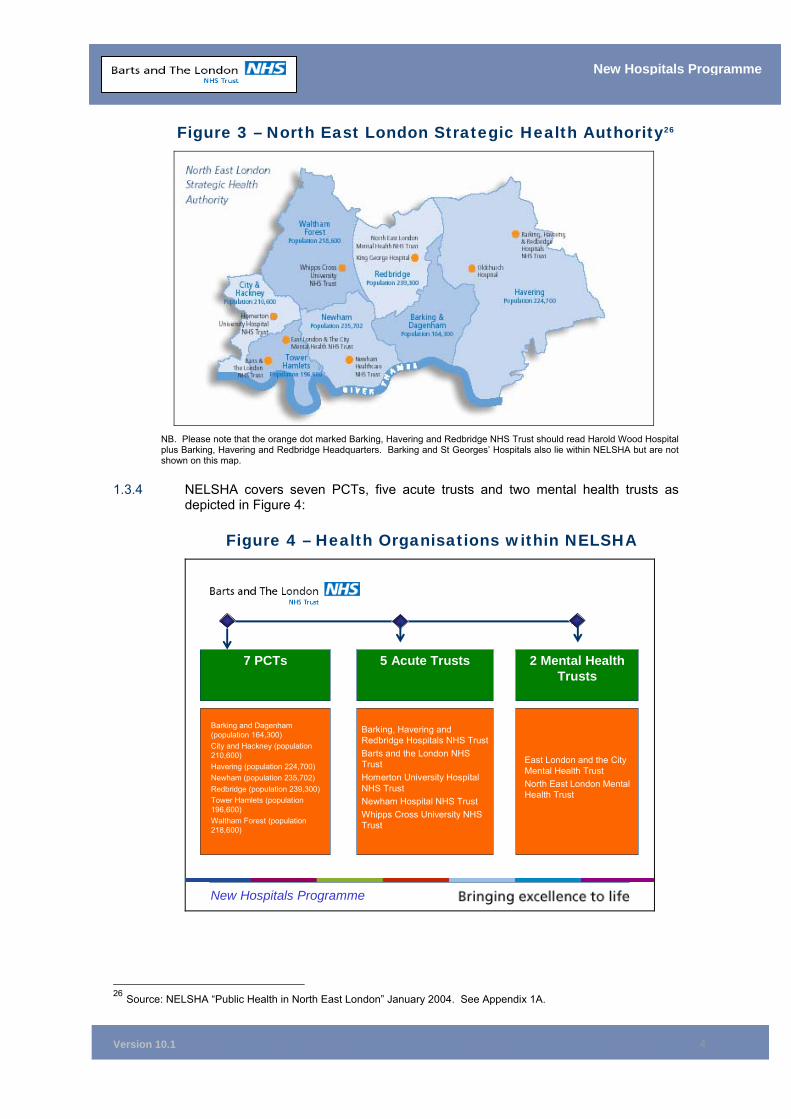
Version 10.1
4
New Hospitals Programme
Figure 3 – North East London Strategic Health Authority26
NB. Please note that the orange dot marked Barking, Havering and Redbridge NHS Trust should read Harold Wood Hospital plus Barking, Havering and Redbridge Headquarters. Barking and St Georges’ Hospitals also lie within NELSHA but are not shown on this map.
1.3.4 NELSHA covers seven PCTs, five acute trusts and two mental health trusts as depicted in Figure 4:
Figure 4 – Health Organisations within NELSHA
New Hospitals Programme
East London and the City Mental Health TrustNorth East London Mental Health Trust
7 PCTs 2 Mental Health Trusts
5 Acute Trusts
Barking, Havering and Redbridge Hospitals NHS TrustBarts and the London NHS TrustHomerton University Hospital NHS TrustNewham Hospital NHS TrustWhipps Cross University NHS Trust
Barking and Dagenham (population 164,300)City and Hackney (population 210,600)Havering (population 224,700)Newham (population 235,702)Redbridge (population 239,300)Tower Hamlets (population 196,600)Waltham Forest (population 218,600)
26 Source: NELSHA “Public Health in North East London” January 2004. See Appendix 1A.
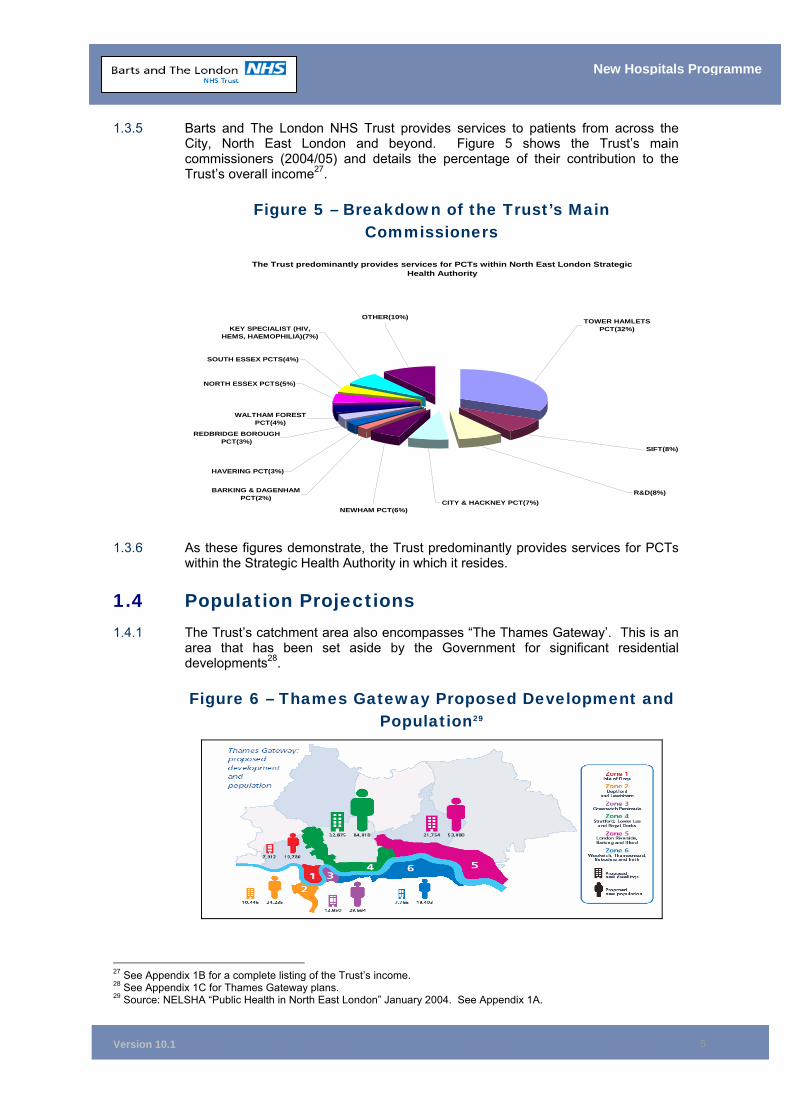
Version 10.1
5
New Hospitals Programme
1.3.5 Barts and The London NHS Trust provides services to patients from across the City, North East London and beyond. Figure 5 shows the Trust’s main commissioners (2004/05) and details the percentage of their contribution to the Trust’s overall income27.
Figure 5 – Breakdown of the Trust’s Main Commissioners
The Trust predominantly provides services for PCTs within North East London Strategic Health Authority
NORTH ESSEX PCTS(5%)
SOUTH ESSEX PCTS(4%)
OTHER(10%)
KEY SPECIALIST (HIV, HEMS, HAEMOPHILIA)(7%)
WALTHAM FOREST PCT(4%)
HAVERING PCT(3%)
REDBRIDGE BOROUGH PCT(3%)
NEWHAM PCT(6%)
BARKING & DAGENHAM PCT(2%)
CITY & HACKNEY PCT(7%)R&D(8%)
SIFT(8%)
TOWER HAMLETS PCT(32%)
1.3.6 As these figures demonstrate, the Trust predominantly provides services for PCTs
within the Strategic Health Authority in which it resides.
1.4 Population Projections 1.4.1 The Trust’s catchment area also encompasses “The Thames Gateway’. This is an
area that has been set aside by the Government for significant residential developments28.
Figure 6 – Thames Gateway Proposed Development and Population29
27 See Appendix 1B for a complete listing of the Trust’s income. 28 See Appendix 1C for Thames Gateway plans. 29 Source: NELSHA “Public Health in North East London” January 2004. See Appendix 1A.
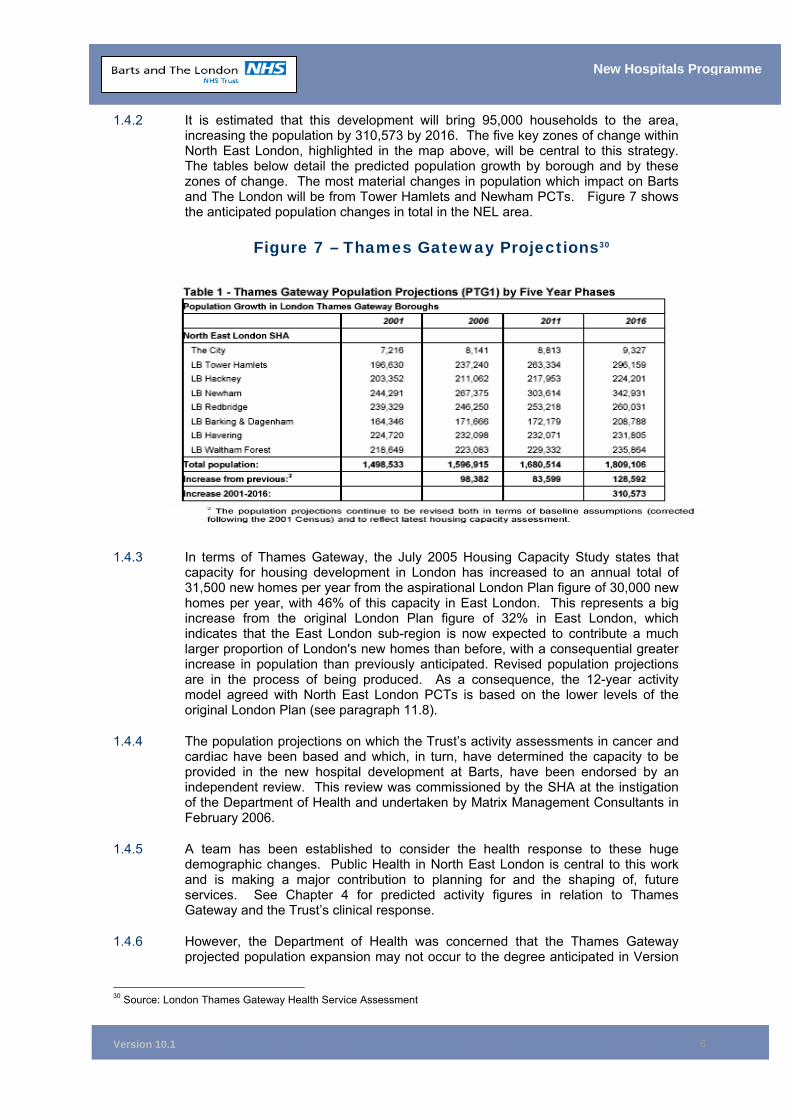
Version 10.1
6
New Hospitals Programme
1.4.2 It is estimated that this development will bring 95,000 households to the area, increasing the population by 310,573 by 2016. The five key zones of change within North East London, highlighted in the map above, will be central to this strategy. The tables below detail the predicted population growth by borough and by these zones of change. The most material changes in population which impact on Barts and The London will be from Tower Hamlets and Newham PCTs. Figure 7 shows the anticipated population changes in total in the NEL area.
Figure 7 – Thames Gateway Projections30
1.4.3 In terms of Thames Gateway, the July 2005 Housing Capacity Study states that capacity for housing development in London has increased to an annual total of 31,500 new homes per year from the aspirational London Plan figure of 30,000 new homes per year, with 46% of this capacity in East London. This represents a big increase from the original London Plan figure of 32% in East London, which indicates that the East London sub-region is now expected to contribute a much larger proportion of London's new homes than before, with a consequential greater increase in population than previously anticipated. Revised population projections are in the process of being produced. As a consequence, the 12-year activity model agreed with North East London PCTs is based on the lower levels of the original London Plan (see paragraph 11.8).
1.4.4 The population projections on which the Trust’s activity assessments in cancer and cardiac have been based and which, in turn, have determined the capacity to be provided in the new hospital development at Barts, have been endorsed by an independent review. This review was commissioned by the SHA at the instigation of the Department of Health and undertaken by Matrix Management Consultants in February 2006.
1.4.5 A team has been established to consider the health response to these huge demographic changes. Public Health in North East London is central to this work and is making a major contribution to planning for and the shaping of, future services. See Chapter 4 for predicted activity figures in relation to Thames Gateway and the Trust’s clinical response.
1.4.6 However, the Department of Health was concerned that the Thames Gateway projected population expansion may not occur to the degree anticipated in Version
30 Source: London Thames Gateway Health Service Assessment
Version 10.1
7
New Hospitals Programme
9 of the FBC. Combined with the shift of healthcare activity to smaller hospitals and the primary care sector, as outlined in the Government’s White Paper entitled Our Health, Our Care, Our Say: A New Direction for Community Services, there was concern that the activity demands forecast in the business case would therefore not occur in full, making the planned development unaffordable. As a result, the DH decided to cut back the size of the development which, in effect, means that elements of phases at both Barts and The London will not be implemented unless and until, activity demands the additional capacity and necessary DH approvals are obtained.
1.5 The North East London Health Economy 1.5.1 In addition to the challenges of meeting the needs of the predicted population
growth, the existing demographics present a number of health issues for the Trust. North East London is an area of stark contrast. Stretching from The City to the outer London boundary with Essex, the region contains both extreme affluence and extreme hardship. Although the “Square Mile” of The City houses some of the richest concentrations of economic business in the world, its neighbours include some of the UK's most deprived communities.
1.5.2 Barts hospital is located within a prosperous neighbourhood with a small residential population, though as a tertiary centre it treats many patients from lower socio-economic groups. As the health requirements of the local population are less onerous, the decision was taken to make this a centre for tertiary care, concentrating emergency and walk-in treatments at Whitechapel, which is surrounded by a much denser population from a poorer socio-economic background.
1.5.3 While there are some health advantages to the North East London region, e.g. a youthful population31, overall the boroughs continue to be more deprived than London as a whole. Tower Hamlets, Hackney and Newham rank in the worst 10 local authorities in England in respect of deprivation (London Health Commission). Figure 8 below demonstrates key demographics of the NEL boroughs (please note that a number of source documents have been employed, as not all health case comparators are available in one publication).
Figure 8 – Demographics of North East London32
Housing Classified Unfit to Inhabit
Newham has the highest number of dwellings classified as unfit, with over 12% in this category. Islington, Hackney and Tower Hamlets are also above the London average (GLA).
Overcrowding
29% of Tower Hamlets households are overcrowded – twice the London average (THPCT2). The NELSHA population is projected to grow from 1.5 million in 2001 to 1.65 million in 2016 – a growth of 11%.
In addition to this general growth, spurred on by exceptionally high birth rates in the area (Tower Hamlets is 25% higher than
31 Tower Hamlets has a notably younger population, with 57% of the population being aged 15-44, compared with 41.5% for England and Wales and a lower proportion of people aged 65+ compared to England and Wales and North East London. 32 Sources for data within this figure: THPCT1: Tower Hamlets Primary Care Trust Annual Public Health Report 2004, THPCT2: Clinical Governance Report and Development Plan 2003 – 04, NELSHA: North East London Strategic Health Authority Public Health in North East London Jan 04, GLA: London Health Commission Health in London April 2004
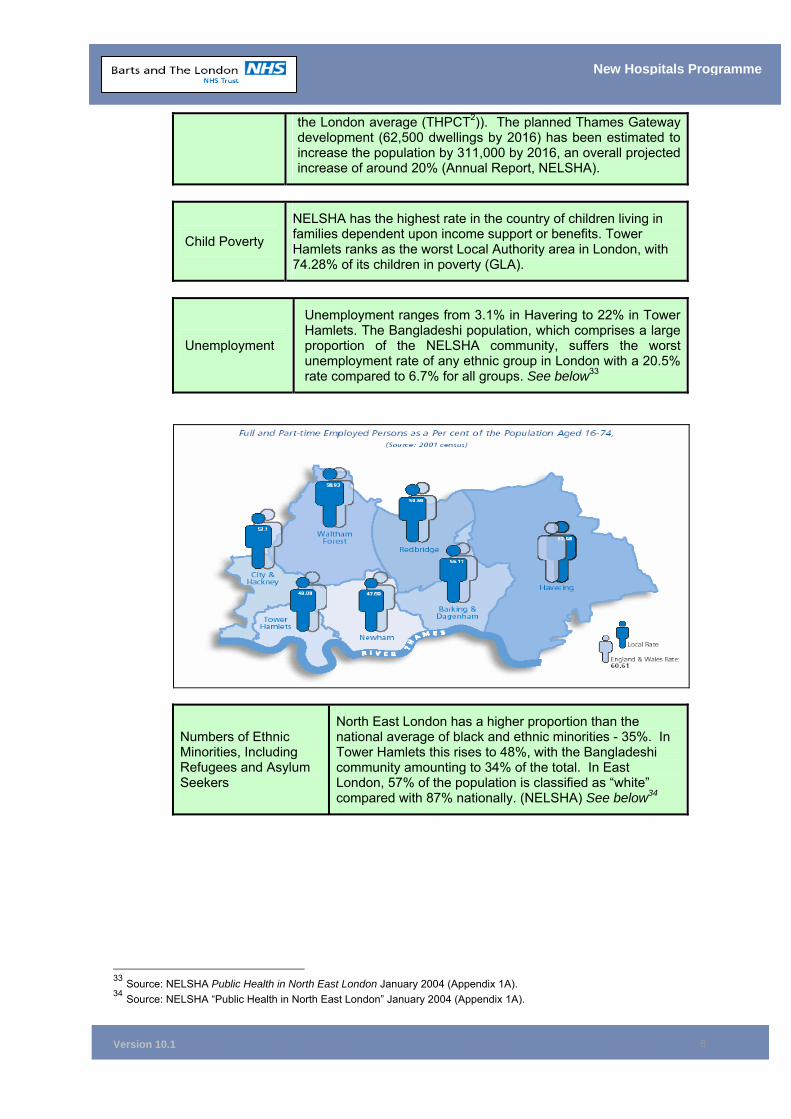
Version 10.1
8
New Hospitals Programme
the London average (THPCT2)). The planned Thames Gateway development (62,500 dwellings by 2016) has been estimated to increase the population by 311,000 by 2016, an overall projected increase of around 20% (Annual Report, NELSHA).
Child Poverty
NELSHA has the highest rate in the country of children living in families dependent upon income support or benefits. Tower Hamlets ranks as the worst Local Authority area in London, with 74.28% of its children in poverty (GLA).
Unemployment
Unemployment ranges from 3.1% in Havering to 22% in Tower Hamlets. The Bangladeshi population, which comprises a large proportion of the NELSHA community, suffers the worst unemployment rate of any ethnic group in London with a 20.5% rate compared to 6.7% for all groups. See below33
Numbers of Ethnic Minorities, Including Refugees and Asylum Seekers
North East London has a higher proportion than the national average of black and ethnic minorities - 35%. In Tower Hamlets this rises to 48%, with the Bangladeshi community amounting to 34% of the total. In East London, 57% of the population is classified as “white” compared with 87% nationally. (NELSHA) See below34
33 Source: NELSHA Public Health in North East London January 2004 (Appendix 1A). 34 Source: NELSHA “Public Health in North East London” January 2004 (Appendix 1A).
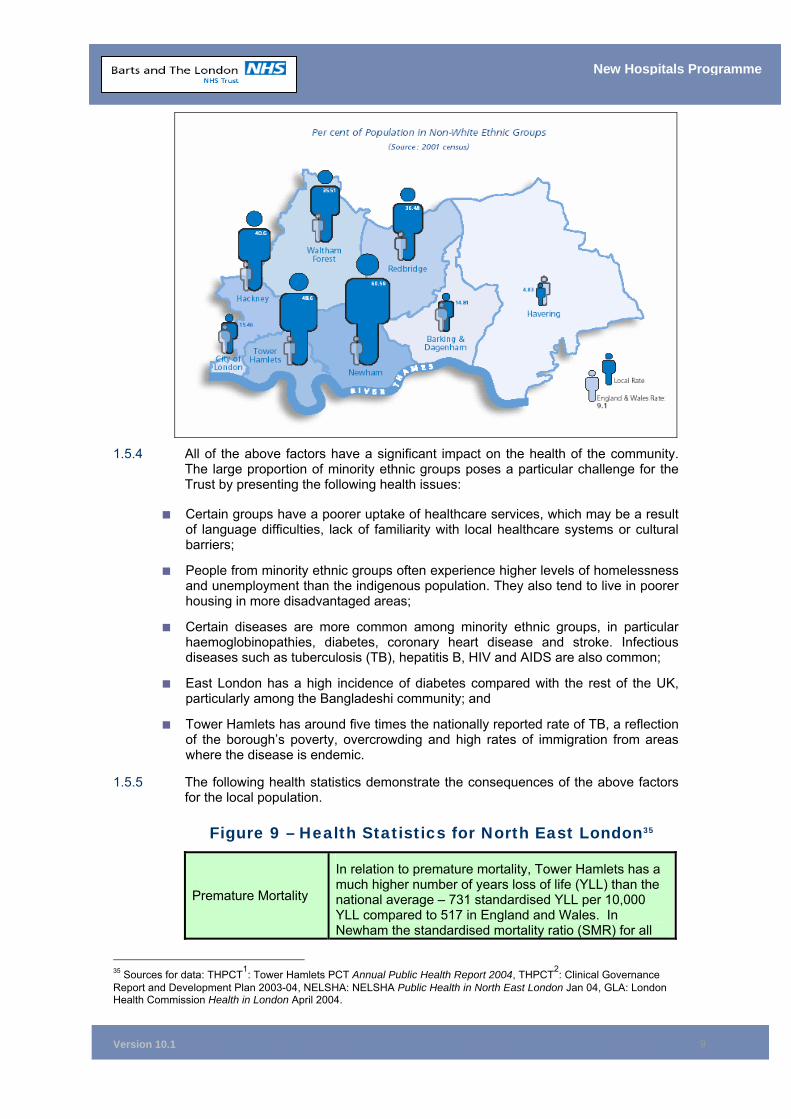
Version 10.1
9
New Hospitals Programme
1.5.4 All of the above factors have a significant impact on the health of the community.
The large proportion of minority ethnic groups poses a particular challenge for the Trust by presenting the following health issues:
■ Certain groups have a poorer uptake of healthcare services, which may be a result of language difficulties, lack of familiarity with local healthcare systems or cultural barriers;
■ People from minority ethnic groups often experience higher levels of homelessness and unemployment than the indigenous population. They also tend to live in poorer housing in more disadvantaged areas;
■ Certain diseases are more common among minority ethnic groups, in particular haemoglobinopathies, diabetes, coronary heart disease and stroke. Infectious diseases such as tuberculosis (TB), hepatitis B, HIV and AIDS are also common;
■ East London has a high incidence of diabetes compared with the rest of the UK, particularly among the Bangladeshi community; and
■ Tower Hamlets has around five times the nationally reported rate of TB, a reflection of the borough’s poverty, overcrowding and high rates of immigration from areas where the disease is endemic.
1.5.5 The following health statistics demonstrate the consequences of the above factors for the local population.
Figure 9 – Health Statistics for North East London35
Premature Mortality
In relation to premature mortality, Tower Hamlets has a much higher number of years loss of life (YLL) than the national average – 731 standardised YLL per 10,000 YLL compared to 517 in England and Wales. In Newham the standardised mortality ratio (SMR) for all
35 Sources for data: THPCT1: Tower Hamlets PCT Annual Public Health Report 2004, THPCT2: Clinical Governance Report and Development Plan 2003-04, NELSHA: NELSHA Public Health in North East London Jan 04, GLA: London Health Commission Health in London April 2004.
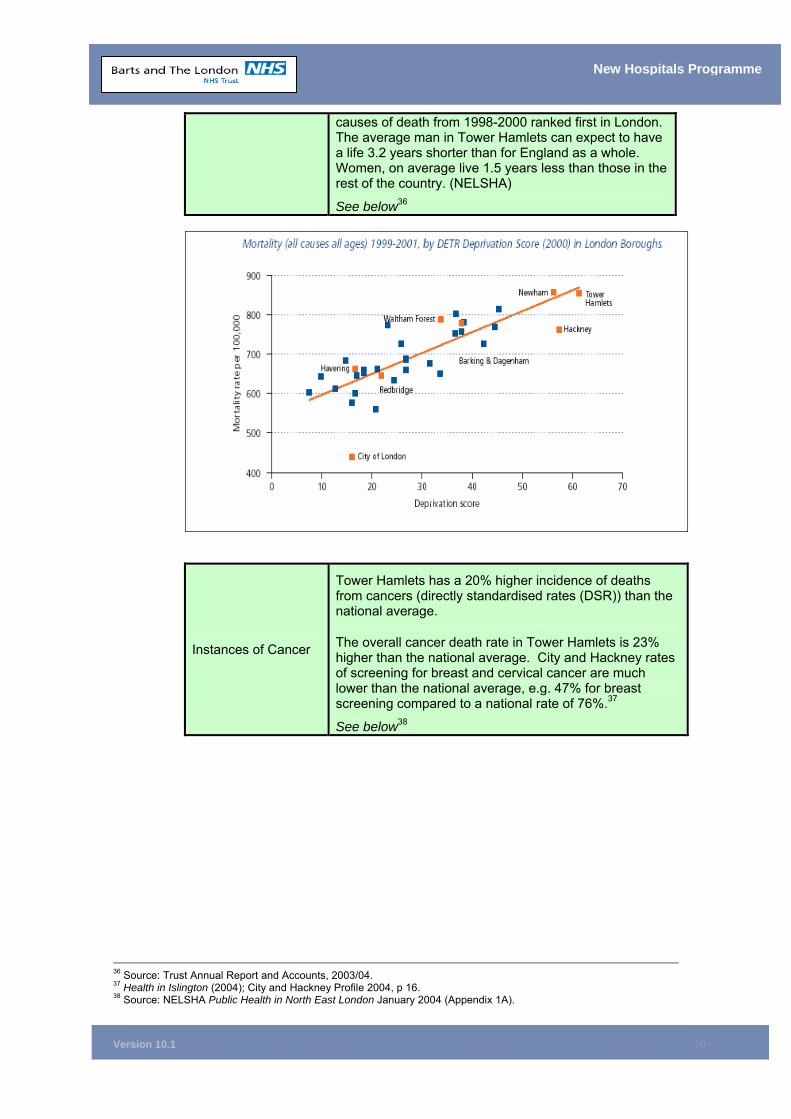
Version 10.1
10
New Hospitals Programme
causes of death from 1998-2000 ranked first in London. The average man in Tower Hamlets can expect to have a life 3.2 years shorter than for England as a whole. Women, on average live 1.5 years less than those in the rest of the country. (NELSHA)
See below36
Instances of Cancer
Tower Hamlets has a 20% higher incidence of deaths from cancers (directly standardised rates (DSR)) than the national average.
The overall cancer death rate in Tower Hamlets is 23% higher than the national average. City and Hackney rates of screening for breast and cervical cancer are much lower than the national average, e.g. 47% for breast screening compared to a national rate of 76%.37
See below38
36 Source: Trust Annual Report and Accounts, 2003/04. 37 Health in Islington (2004); City and Hackney Profile 2004, p 16. 38 Source: NELSHA Public Health in North East London January 2004 (Appendix 1A).
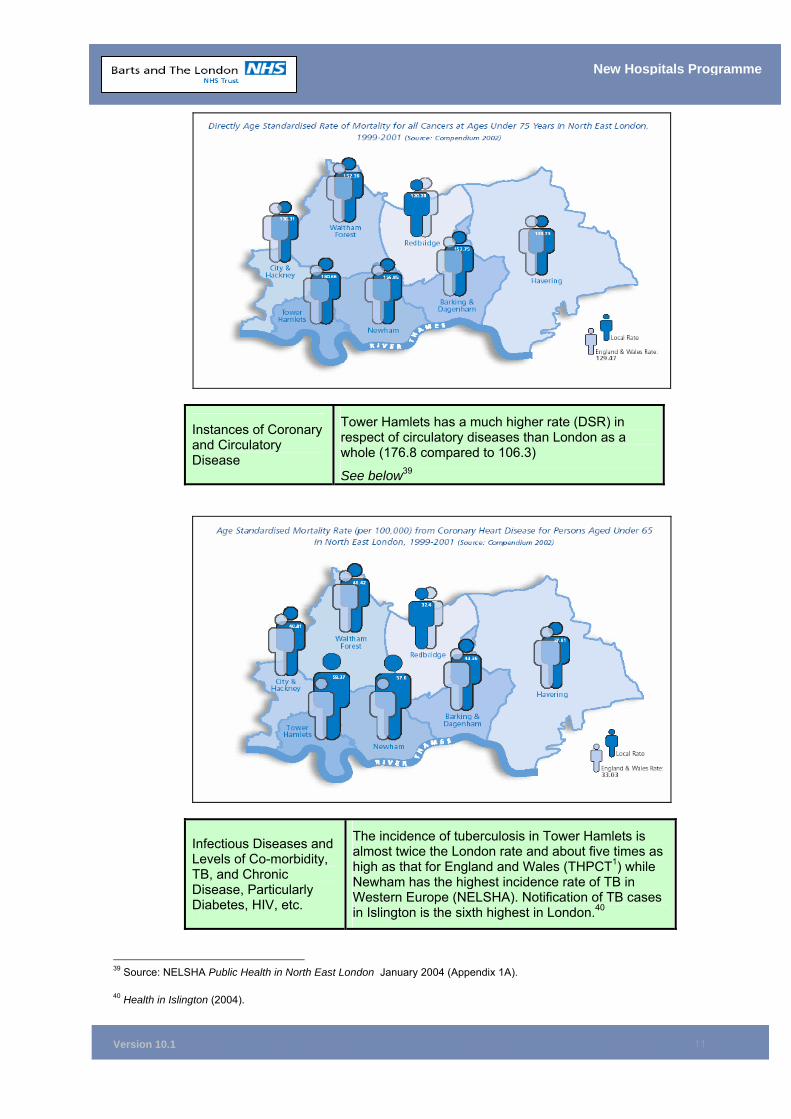
Version 10.1
11
New Hospitals Programme
Instances of Coronary and Circulatory Disease
Tower Hamlets has a much higher rate (DSR) in respect of circulatory diseases than London as a whole (176.8 compared to 106.3)
See below39
Infectious Diseases and Levels of Co-morbidity, TB, and Chronic Disease, Particularly Diabetes, HIV, etc.
The incidence of tuberculosis in Tower Hamlets is almost twice the London rate and about five times as high as that for England and Wales (THPCT1) while Newham has the highest incidence rate of TB in Western Europe (NELSHA). Notification of TB cases in Islington is the sixth highest in London.40
39 Source: NELSHA Public Health in North East London January 2004 (Appendix 1A). 40 Health in Islington (2004).
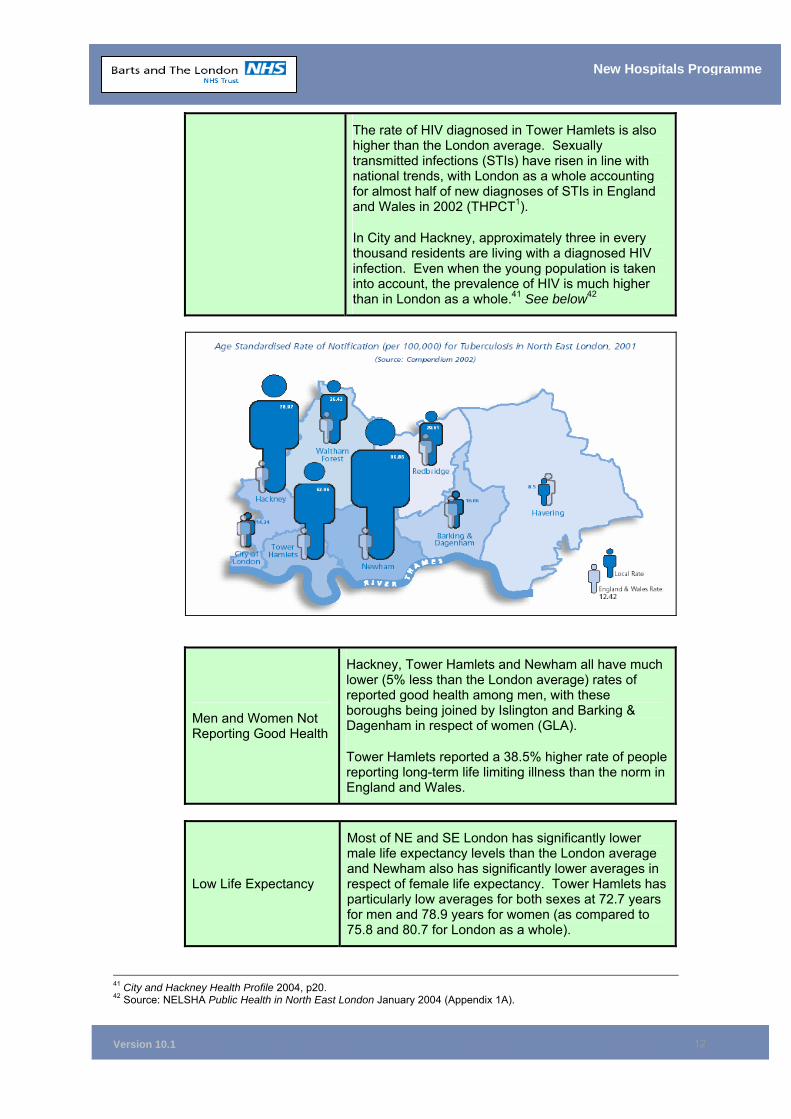
Version 10.1
12
New Hospitals Programme
The rate of HIV diagnosed in Tower Hamlets is also higher than the London average. Sexually transmitted infections (STIs) have risen in line with national trends, with London as a whole accounting for almost half of new diagnoses of STIs in England and Wales in 2002 (THPCT1).
In City and Hackney, approximately three in every thousand residents are living with a diagnosed HIV infection. Even when the young population is taken into account, the prevalence of HIV is much higher than in London as a whole.41 See below42
Men and Women Not Reporting Good Health
Hackney, Tower Hamlets and Newham all have much lower (5% less than the London average) rates of reported good health among men, with these boroughs being joined by Islington and Barking & Dagenham in respect of women (GLA).
Tower Hamlets reported a 38.5% higher rate of people reporting long-term life limiting illness than the norm in England and Wales.
Low Life Expectancy
Most of NE and SE London has significantly lower male life expectancy levels than the London average and Newham also has significantly lower averages in respect of female life expectancy. Tower Hamlets has particularly low averages for both sexes at 72.7 years for men and 78.9 years for women (as compared to 75.8 and 80.7 for London as a whole).
41 City and Hackney Health Profile 2004, p20. 42 Source: NELSHA Public Health in North East London January 2004 (Appendix 1A).
Version 10.1
13
New Hospitals Programme
Numbers of People Suffering Mental Health Problems
Tower Hamlets PCT reports that the borough suffers from a much higher incidence of mental illness than the average rate for England and Wales. Hospital admissions for schizophrenia are 163.5 (age standardised rate per 100,000 population) compared to a 72.6 England and Wales average (THPCT1).
City and Hackney PCT report “unusually high levels of mental illness”. Admissions for schizophrenia are three times as high as in England as a whole, for both men and women (NELSHA).
1.5.6 Chapter 3 provides detailed analysis of how Barts and The London NHS Trust proposes to provide clinical services to meet the needs outlined above and describes models of care for service delivery.
1.6 From Tomlinson to Turnberg: Strategic Reviews 1.6.1 The Government has long recognised the difficulty of providing a healthcare service
for a community with such diverse and extreme needs. Successive reviews in the 1990s shaped the way in which future health services in London could be aligned to meet these needs. These reviews have directed the nature of the redevelopment at Barts and The London NHS Trust.
1.6.2 The first was led by Sir Bernard Tomlinson in 1992 and was endorsed in the Government’s response Making London Better (1993). The second was undertaken by an independent advisory panel headed by Sir Leslie Turnberg in 1997 and was endorsed by the Government’s response The Future of London’s Health Services (1998).
1.6.3 Both acknowledged the need for new and improved health facilities in East London and both supported the Trust’s overwhelming case for change:
Figure 10 – Extracts from the Turnberg Report, 199743
New Hospitals Programme
Quotes from Turnberg…
“The population of east London is amongst the most deprived in the UK -deprivation indicators place Tower Hamlets at the top of the league;….The services currently provided in primary care, in the community, and in hospitals, are failing to meet needs;The Royal London Hospital buildings are in a poor state; old stock inefficiently arranged and poorly maintained. A new hospital on this site is desperately needed;Against the background that Londoners as a whole can ill afford to lose more beds, loss in this particularly deprived part of London would require special justification;As well as a requirement to remedy the gaps in the services for the local population, the Trust has a wider responsibility for education and training, for research and for specialised tertiary services to the rest of the region and outside it. There is a tension between funding for these responsibilities and for those to the local community; and‘The health needs of the people of east London have…represented the starkest mismatch between needs and services available’.
43 Source: The Health Service in London: A Strategic Review – Sir Leslie Turnberg 1997
Version 10.1
14
New Hospitals Programme
1.6.4 However, the two reviews differed significantly in their recommended approach to redevelopment at Barts and The London.
1.6.5 Making London Better (1993) recommended that the Trust should concentrate all facilities on the Whitechapel site and close both St Bartholomew’s Hospital and The London Chest Hospital. This has become known as “the single site solution” and involved the construction of a 1,200 bed acute teaching hospital on the Whitechapel site which would encompass the services of the entire Trust. The Trust accordingly developed an initial scheme on this basis, achieving OBC approval from the NHS Executive – North Thames in 1995.
1.6.6 However, the potential closure of the St Bartholomew’s site sparked significant debate both locally and within Parliament. While negotiations with potential PFI partners were underway, the new Labour Government announced the second review in 1997. The scheme was halted awaiting its advice.
1.6.7 In February 1998, the recommendations of the London Review (Turnberg 1997) were announced. The single-site solution was criticised on a number of fronts. It was found to be inflexible for future developments and unable to deliver the efficiencies predicted. The report also argued that both the increased health needs of the area and the potential costs of delivering the scheme had been underestimated.
1.6.8 Fuelled by the desire for the “preservation of a hospital currently providing high quality care, especially tertiary care” and the aspiration to make use of refurbished facilities at St Bartholomew’s, the report recommended the establishment of a “dual site solution’.
1.6.9 While it acknowledged that “the dual site would be more expensive”, the review specifically proposed the establishment of a “rather smaller development…on the Whitechapel site, probably of the order of 900 beds, combining local secondary care and some tertiary facilities and the development of St. Bartholomew’s” to “focus on a small number of tertiary services” of which “currently the most favourable options are for cardiac and oncology services”.
1.6.10 Turnberg and his review team concluded that “We could not envisage as viable, a dual site option which simply left two hospitals each providing similar services…The only possibility for a dual site proposal would have to incorporate a rational distribution of services between the hospitals, so that the two sites were run as one with complementarily and not duplication.”
1.6.11 The Government’s response, The Future of London’s Health Services (February 1998) fully endorsed Turnberg’s vision.
1.6.12 The Trust therefore withdrew the original OBC and undertook to re-determine a configuration of services in compliance with the Government’s recommendations and directive. The new scheme contained within this full business case reflects this history, by proposing a 905 bed new hospital at Whitechapel, a 343 bed Centre of Excellence for Cardiac and Cancer at the West Smithfield site and the closure of The London Chest Hospital.
1.6.13 Although the Turnberg Report is now 8 years old, the recommendations are as appropriate now as they were then and were further confirmed by the independent review of cancer and cardiac services at Barts. This review commissioned by NELSHA, at the instigation of the Department of Health, strongly endorsed the Trust’s current plans for the service provision at Barts.
Version 10.1
15
New Hospitals Programme
Figure 11 – Extracts from the Government’s Response to the Turnberg Report, 1998
New Hospitals Programme
Quotes from Governments Response to Turnberg…
““The government recognises the special needs of the East End, and the current inadequacy of many primary, community and hospital services in that part of London. That is why the Government is committed to the major and urgent re-development of the Royal London Hospital at Whitechapel”…and…”now wishes to build on the tradition of medical excellence at St. Bartholomew’s Hospital. To this end the Health Authority and the Trust will now develop plans for a specialist hospital providing cardiac and cancer services at St. Bartholomew’s Hospital’.
1.6.14 There is an urgent need to provide purpose built facilities for the benefit of the population of The City and North East London, as confirmed by the SHA in their full endorsement of this business case.
1.7 Chapter Conclusion 1.7.1 The strategic need for the provision of new purpose built hospitals for the people of
North East London, the City and beyond is in no doubt.
1.7.2 The investment proposed in this FBC has been driven from two important directions simultaneously:
• Top down – by the outcome of the Turnberg Report favouring a twin site solution; and
• Bottom up – by the diverse and complex needs of the local population of North East London.
1.7.3 The population growth projections used in this business case are those published by the Office of the Deputy Prime Minister and are therefore robust. The redevelopment is necessary to meet the expected growth in demand for health services.
1.8 Chapter Appendices
1A Public Health in North East London, North East London Strategic Health Authority, January 2004
1B Commissioner Breakdown 1C Thames Gateway Plans
Version 10.1
16
New Hospitals Programme
2 THE CASE FOR CHANGE Chapter Synopsis – Case For Change
This chapter clearly sets out the case for change, which is driven by a combination of strategic and local factors to modernise the physical environment and the provision of clinical services.
The strategic factors include the: ■ Implementation of Payment by Results ■ Patient Choice agenda ■ Implementation of National Service Frameworks ■ Need to improve the quality of service provision ■ Need to improve primary care ■ Challenges set by significant demographic change forecast for North East
London ■ Provision of new technologies ■ Implementation of changes in medical and dental training Additional local factors driving change include the: ■ Need to improve the poor physical environment of the hospitals ■ Need to continue improving clinical quality ■ Desire to improve access to services ■ Lack of flexibility in facilities to respond to policy initiatives ■ Need to improve training and teaching ■ Need to make better use of resources ■ Necessity to improve partnership working ■ Need for the Trust to play an important role in redeveloping the local
economy All of these factors combine to produce a compelling case for change – one endorsed by Sir Leslie Turnberg in 1997 and accepted by the Government in full in 1998.
2.1 Strategic Pressures for Change 2.1.1 The overall context of the change taking place throughout the NHS is that of
modernising Britain, as developed in the White Papers: Modernising Government (March 1999), and Modern Local Government: In Touch with the People (July 1998). This modernisation agenda has been supported by a range of initiatives designed to deliver improved and user-focused public services.
2.1.2 The Saving Lives: Our Healthier Nation White Paper (July 1999) presented a health strategy centred on the priority areas of cancer, coronary heart disease and stroke, accidents and mental health. It sets a wider public health agenda that focuses on “health” rather than simply the “health service” and emphasises a new partnership between the individual, local organisations and the Government.
2.1.3 Publication of the NHS Plan: A Plan for Investment, A Plan for Reform (July 2000) and the more recent NHS Improvement Plan: Putting People at the Heart of Public Services sets the NHS a number of further challenges. In particular, the plan focuses on delivery of 4 key objectives: Improvement of Health of the Population, Chronic Care Management, patient user/carer experience and access to services.
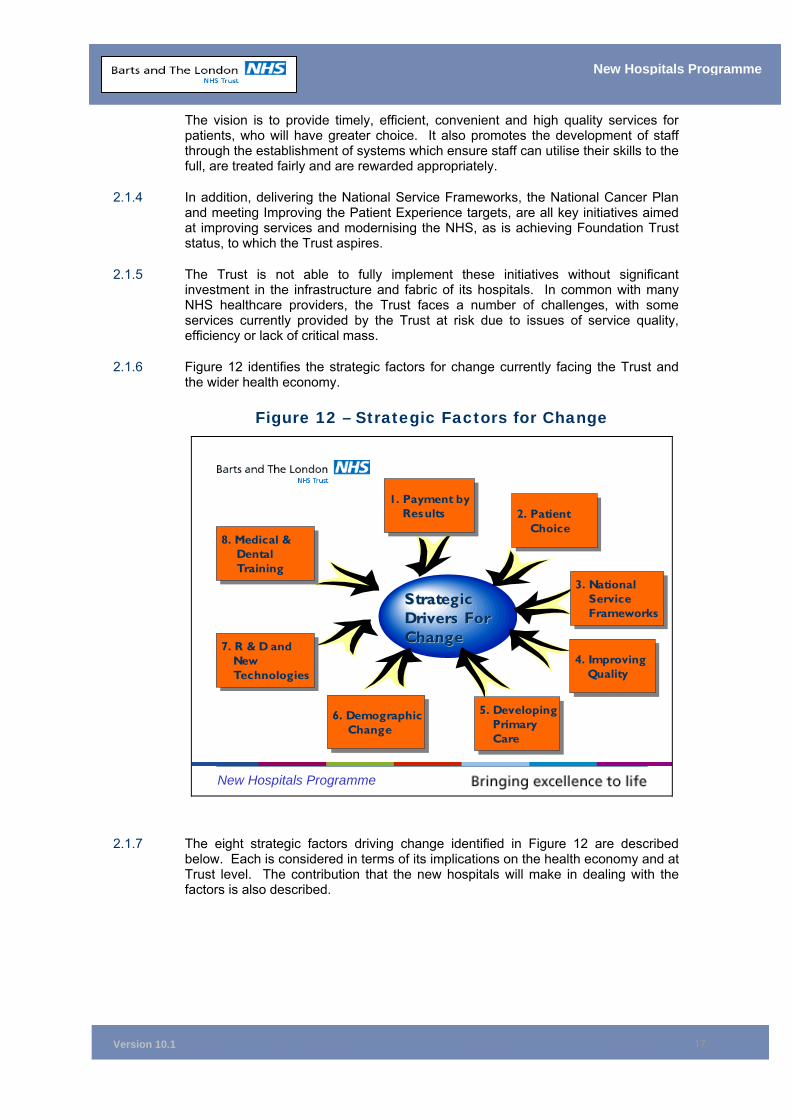
Version 10.1
17
New Hospitals Programme
The vision is to provide timely, efficient, convenient and high quality services for patients, who will have greater choice. It also promotes the development of staff through the establishment of systems which ensure staff can utilise their skills to the full, are treated fairly and are rewarded appropriately.
2.1.4 In addition, delivering the National Service Frameworks, the National Cancer Plan and meeting Improving the Patient Experience targets, are all key initiatives aimed at improving services and modernising the NHS, as is achieving Foundation Trust status, to which the Trust aspires.
2.1.5 The Trust is not able to fully implement these initiatives without significant investment in the infrastructure and fabric of its hospitals. In common with many NHS healthcare providers, the Trust faces a number of challenges, with some services currently provided by the Trust at risk due to issues of service quality, efficiency or lack of critical mass.
2.1.6 Figure 12 identifies the strategic factors for change currently facing the Trust and the wider health economy.
Figure 12 – Strategic Factors for Change
New Hospitals Programme
1. Payment byResults
1. Payment byResults 2. Patient
Choice2. Patient
Choice
3. National Service Frameworks
3. National Service Frameworks
4. Improving Quality
4. Improving Quality
5. DevelopingPrimary Care
5. DevelopingPrimary Care
6. DemographicChange
6. DemographicChange
7. R & D and New Technologies
7. R & D and New Technologies
8. Medical & Dental Training
8. Medical & Dental Training
Strategic Strategic Drivers For Drivers For ChangeChange
2.1.7 The eight strategic factors driving change identified in Figure 12 are described below. Each is considered in terms of its implications on the health economy and at Trust level. The contribution that the new hospitals will make in dealing with the factors is also described.
Version 10.1
18
New Hospitals Programme
(1) Payment By Results - The Drive For Cost Efficiency And Effectiveness
Strategic Implications for Acute Services in NEL
The need to: ■ Rationalise clinical, clinical support and non-
clinical services, to reduce unit costs; ■ Maintain and improve income levels from
teaching and research Implications for the Trust The need to:
■ Improve efficiency of the use of capital, equipment and buildings;
■ Reduce unit costs; ■ Reduce operational costs generally through
improved procedures; ■ Maintain and improve levels of fixed income
from teaching and research; ■ Maintain and improve income streams from
tertiary referrals for specialist work; How the New Hospitals Will Assist
■ Services that are custom-designed to modern healthcare allow for greater cost efficiency;
■ Operational efficiency can be improved by reorganised, co-located and flexible services;
■ New buildings result in lower maintenance costs and remove the burden of backlog maintenance issues thus impacting positively on unit costs and price.
(2) Patient Choice - Changing Patient Expectations; “Improving The Patient Experience’
Strategic Implications for Acute Services in NEL
The need to: ■ Improve the quality of service provision; ■ Maintain patient flows within the Strategic
Health Authority area; ■ Increase the availability of information for
patients; Implications for the Trust The need to:
■ Provide better access to services (particularly one stop clinic and shorter waiting times);
■ Improve the quality of patient care and general patient support services (eg catering);
■ Improve the fabric of buildings and patient amenities;
■ Implement and expand “Booked Admissions’; ■ Lower current staff tolerance of poor
customer service; ■ Improve patient-staff communications; ■ Address consumerism targets.
How the New Hospitals Will Assist
■ Modern, attractive buildings will provide a more conducive healing environment;
■ Facilities will be tailored to both the clinical and cultural needs of the community;
■ An improved ICT infrastructure will improve
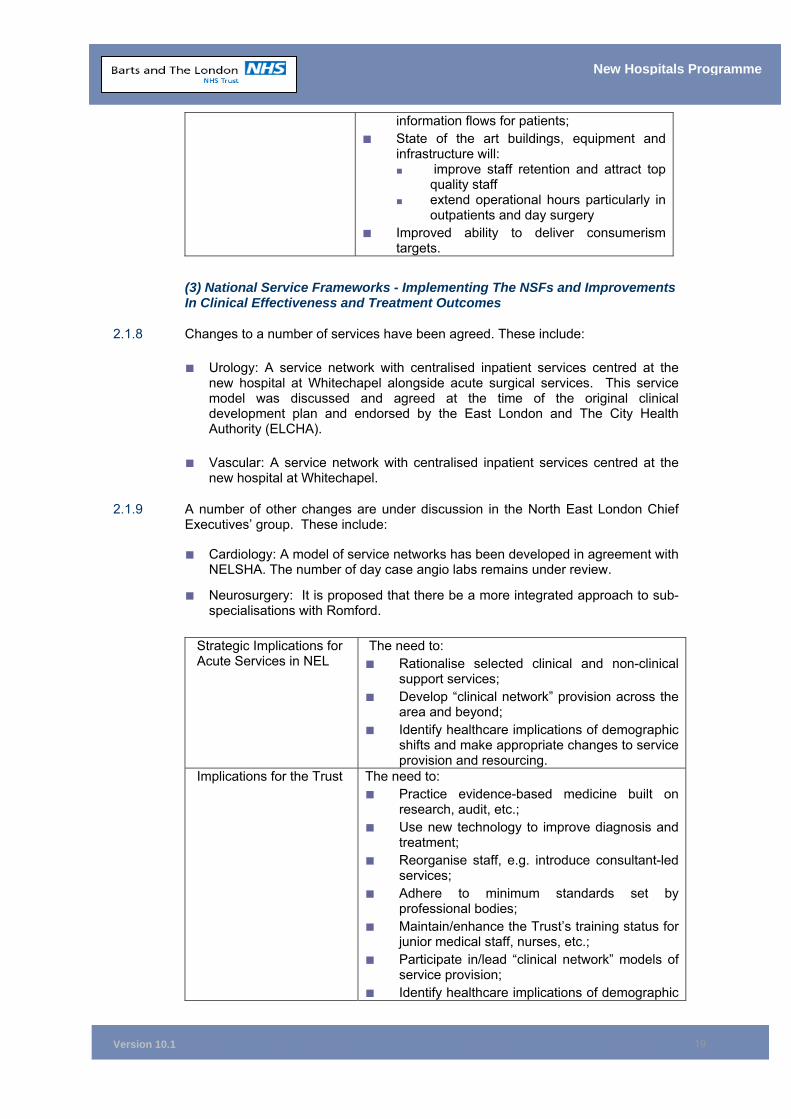
Version 10.1
19
New Hospitals Programme
information flows for patients; ■ State of the art buildings, equipment and
infrastructure will: ■ improve staff retention and attract top
quality staff ■ extend operational hours particularly in
outpatients and day surgery ■ Improved ability to deliver consumerism
targets.
(3) National Service Frameworks - Implementing The NSFs and Improvements In Clinical Effectiveness and Treatment Outcomes
2.1.8 Changes to a number of services have been agreed. These include:
■ Urology: A service network with centralised inpatient services centred at the new hospital at Whitechapel alongside acute surgical services. This service model was discussed and agreed at the time of the original clinical development plan and endorsed by the East London and The City Health Authority (ELCHA).
■ Vascular: A service network with centralised inpatient services centred at the new hospital at Whitechapel.
2.1.9 A number of other changes are under discussion in the North East London Chief Executives’ group. These include:
■ Cardiology: A model of service networks has been developed in agreement with NELSHA. The number of day case angio labs remains under review.
■ Neurosurgery: It is proposed that there be a more integrated approach to sub-specialisations with Romford.
Strategic Implications for Acute Services in NEL
The need to: ■ Rationalise selected clinical and non-clinical
support services; ■ Develop “clinical network” provision across the
area and beyond; ■ Identify healthcare implications of demographic
shifts and make appropriate changes to service provision and resourcing.
Implications for the Trust The need to: ■ Practice evidence-based medicine built on
research, audit, etc.; ■ Use new technology to improve diagnosis and
treatment; ■ Reorganise staff, e.g. introduce consultant-led
services; ■ Adhere to minimum standards set by
professional bodies; ■ Maintain/enhance the Trust’s training status for
junior medical staff, nurses, etc.; ■ Participate in/lead “clinical network” models of
service provision; ■ Identify healthcare implications of demographic
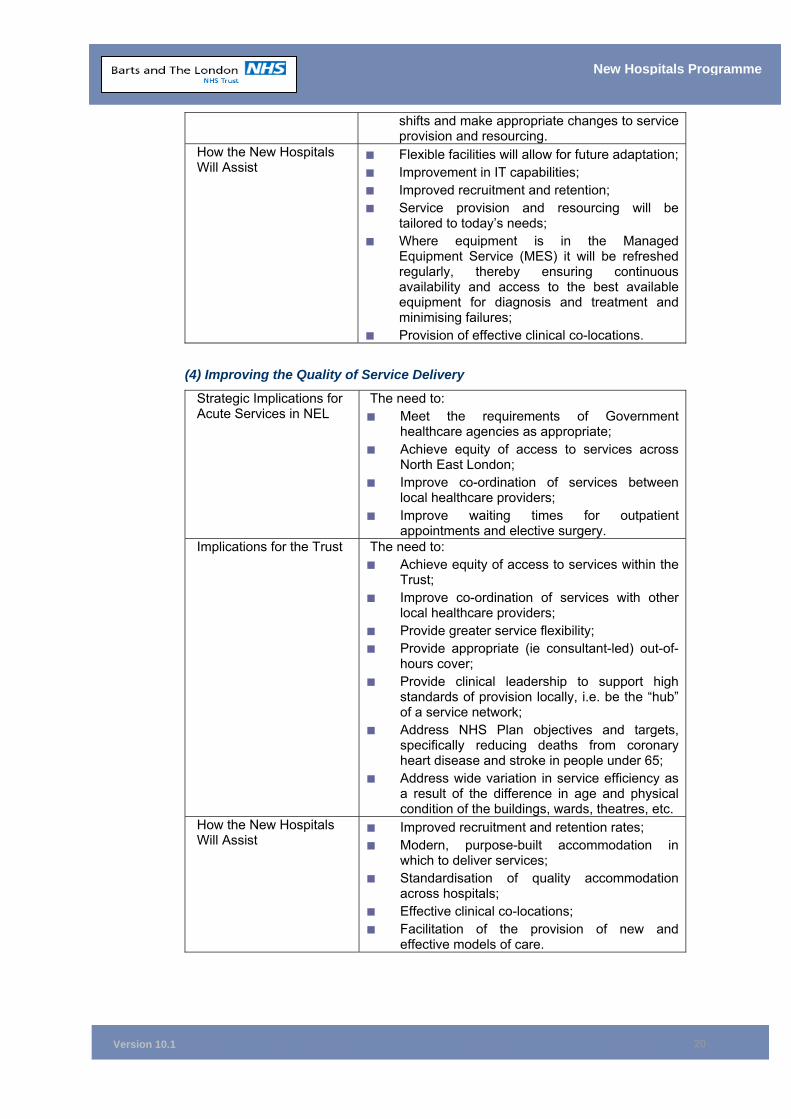
Version 10.1
20
New Hospitals Programme
shifts and make appropriate changes to service provision and resourcing.
How the New Hospitals Will Assist
■ Flexible facilities will allow for future adaptation;■ Improvement in IT capabilities; ■ Improved recruitment and retention; ■ Service provision and resourcing will be
tailored to today’s needs; ■ Where equipment is in the Managed
Equipment Service (MES) it will be refreshed regularly, thereby ensuring continuous availability and access to the best available equipment for diagnosis and treatment and minimising failures;
■ Provision of effective clinical co-locations.
(4) Improving the Quality of Service Delivery
Strategic Implications for Acute Services in NEL
The need to: ■ Meet the requirements of Government
healthcare agencies as appropriate; ■ Achieve equity of access to services across
North East London; ■ Improve co-ordination of services between
local healthcare providers; ■ Improve waiting times for outpatient
appointments and elective surgery. Implications for the Trust The need to:
■ Achieve equity of access to services within the Trust;
■ Improve co-ordination of services with other local healthcare providers;
■ Provide greater service flexibility; ■ Provide appropriate (ie consultant-led) out-of-
hours cover; ■ Provide clinical leadership to support high
standards of provision locally, i.e. be the “hub” of a service network;
■ Address NHS Plan objectives and targets, specifically reducing deaths from coronary heart disease and stroke in people under 65;
■ Address wide variation in service efficiency as a result of the difference in age and physical condition of the buildings, wards, theatres, etc.
How the New Hospitals Will Assist
■ Improved recruitment and retention rates; ■ Modern, purpose-built accommodation in
which to deliver services; ■ Standardisation of quality accommodation
across hospitals; ■ Effective clinical co-locations; ■ Facilitation of the provision of new and
effective models of care.
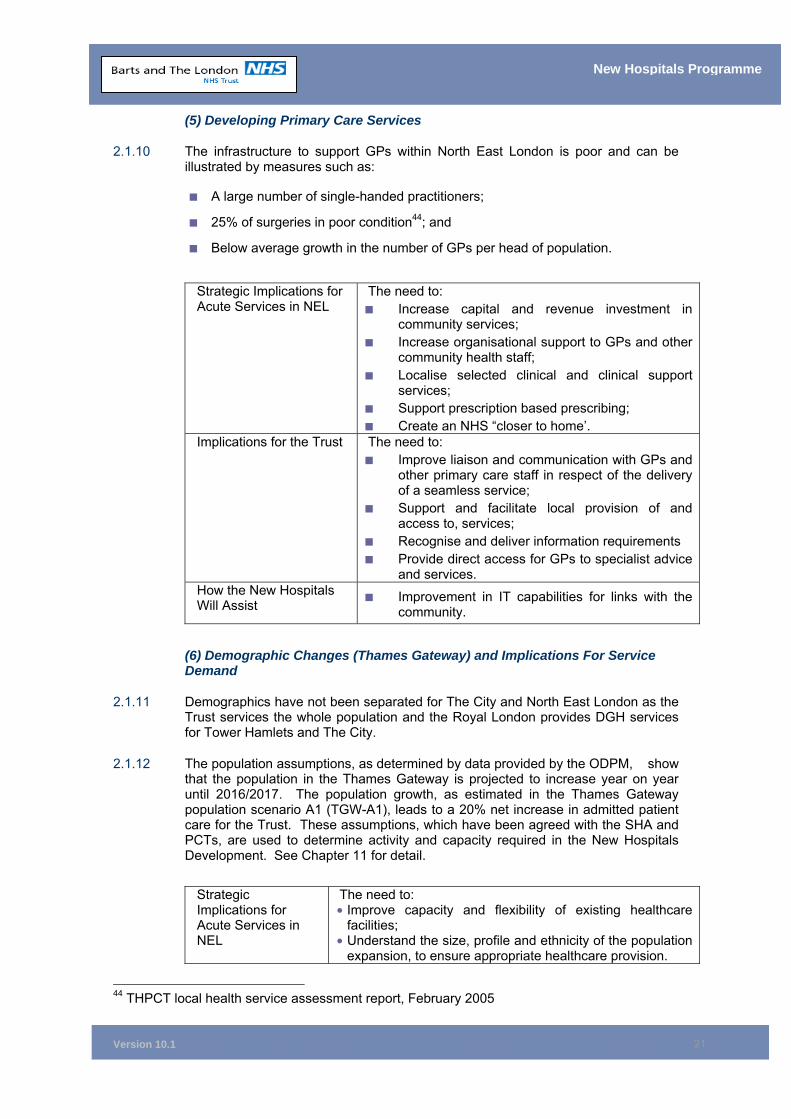
Version 10.1
21
New Hospitals Programme
(5) Developing Primary Care Services
2.1.10 The infrastructure to support GPs within North East London is poor and can be illustrated by measures such as:
■ A large number of single-handed practitioners;
■ 25% of surgeries in poor condition44; and
■ Below average growth in the number of GPs per head of population.
Strategic Implications for Acute Services in NEL
The need to: ■ Increase capital and revenue investment in
community services; ■ Increase organisational support to GPs and other
community health staff; ■ Localise selected clinical and clinical support
services; ■ Support prescription based prescribing; ■ Create an NHS “closer to home’.
Implications for the Trust The need to: ■ Improve liaison and communication with GPs and
other primary care staff in respect of the delivery of a seamless service;
■ Support and facilitate local provision of and access to, services;
■ Recognise and deliver information requirements ■ Provide direct access for GPs to specialist advice
and services. How the New Hospitals Will Assist ■ Improvement in IT capabilities for links with the
community.
(6) Demographic Changes (Thames Gateway) and Implications For Service Demand
2.1.11 Demographics have not been separated for The City and North East London as the Trust services the whole population and the Royal London provides DGH services for Tower Hamlets and The City.
2.1.12 The population assumptions, as determined by data provided by the ODPM, show that the population in the Thames Gateway is projected to increase year on year until 2016/2017. The population growth, as estimated in the Thames Gateway population scenario A1 (TGW-A1), leads to a 20% net increase in admitted patient care for the Trust. These assumptions, which have been agreed with the SHA and PCTs, are used to determine activity and capacity required in the New Hospitals Development. See Chapter 11 for detail.
Strategic Implications for Acute Services in NEL
The need to: • Improve capacity and flexibility of existing healthcare
facilities; • Understand the size, profile and ethnicity of the population
expansion, to ensure appropriate healthcare provision.
44 THPCT local health service assessment report, February 2005
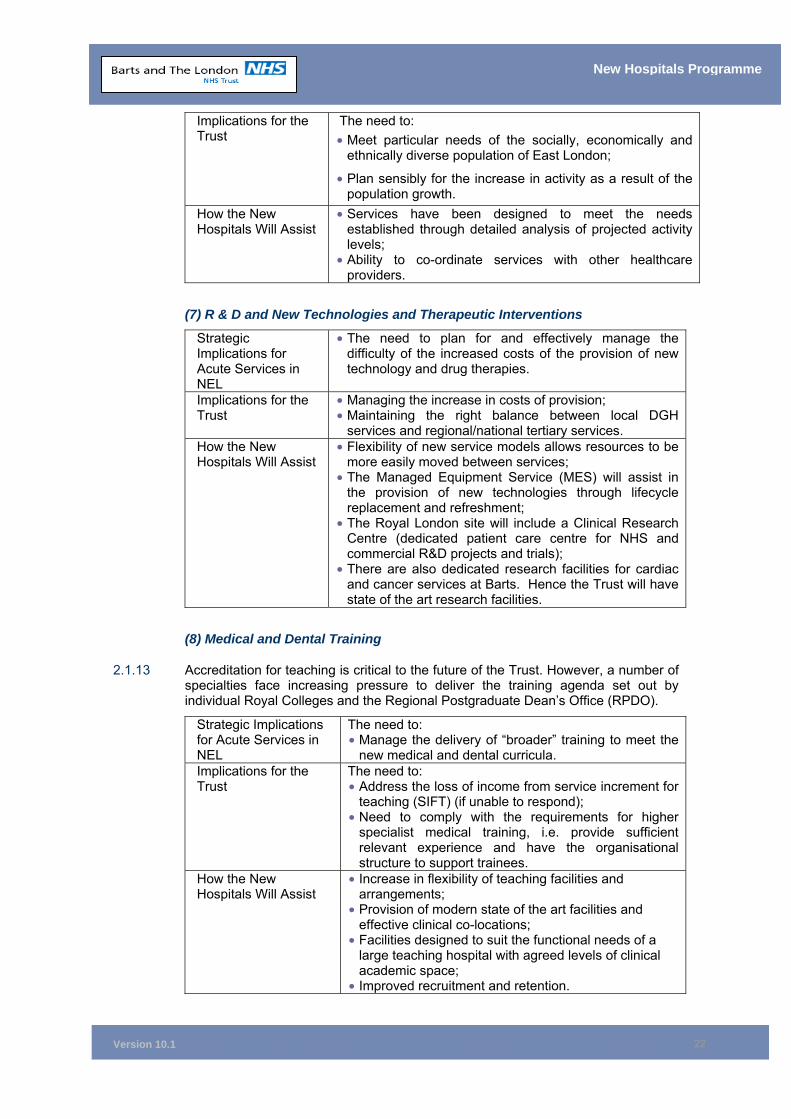
Version 10.1
22
New Hospitals Programme
Implications for the Trust
The need to: • Meet particular needs of the socially, economically and
ethnically diverse population of East London;
• Plan sensibly for the increase in activity as a result of the population growth.
How the New Hospitals Will Assist
• Services have been designed to meet the needs established through detailed analysis of projected activity levels;
• Ability to co-ordinate services with other healthcare providers.
(7) R & D and New Technologies and Therapeutic Interventions
Strategic Implications for Acute Services in NEL
• The need to plan for and effectively manage the difficulty of the increased costs of the provision of new technology and drug therapies.
Implications for the Trust
• Managing the increase in costs of provision; • Maintaining the right balance between local DGH
services and regional/national tertiary services. How the New Hospitals Will Assist
• Flexibility of new service models allows resources to be more easily moved between services;
• The Managed Equipment Service (MES) will assist in the provision of new technologies through lifecycle replacement and refreshment;
• The Royal London site will include a Clinical Research Centre (dedicated patient care centre for NHS and commercial R&D projects and trials);
• There are also dedicated research facilities for cardiac and cancer services at Barts. Hence the Trust will have state of the art research facilities.
(8) Medical and Dental Training
2.1.13 Accreditation for teaching is critical to the future of the Trust. However, a number of specialties face increasing pressure to deliver the training agenda set out by individual Royal Colleges and the Regional Postgraduate Dean’s Office (RPDO).
Strategic Implications for Acute Services in NEL
The need to: • Manage the delivery of “broader” training to meet the
new medical and dental curricula. Implications for the Trust
The need to: • Address the loss of income from service increment for
teaching (SIFT) (if unable to respond); • Need to comply with the requirements for higher
specialist medical training, i.e. provide sufficient relevant experience and have the organisational structure to support trainees.
How the New Hospitals Will Assist
• Increase in flexibility of teaching facilities and arrangements;
• Provision of modern state of the art facilities and effective clinical co-locations;
• Facilities designed to suit the functional needs of a large teaching hospital with agreed levels of clinical academic space;
• Improved recruitment and retention.
Version 10.1
23
New Hospitals Programme
2.1.14 In developing its proposals for the future delivery of service, the Trust is looking at how to overcome many of the barriers identified previously. This would include:
■ Securing commissioners’ acknowledgement of the duplication of some services caused by working on two sites and seeking to secure the necessary ongoing funding to address this as part of the long-term financial strategy;
■ Promoting more flexible, user-focused services and models of care;
■ Using information technology imaginatively to reduce bureaucracy and deliver more effective services;
■ Developing an empowered management structure, designed to ensure decision making takes place as close to the service user as possible, but within a clear framework of corporate accountability;
■ Maintaining rigorous performance management arrangements with a key focus on quality and outcomes as well as finance and manpower;
■ Developing a human resources and pay and reward strategy, aimed at overcoming the current recruitment and retention problems and building for the future; and
■ Investing in high quality, flexible clinical and support accommodation, replacing and renewing the existing building stock.
2.2 Trust–Specific Factors for Change 2.2.1 The Trust also faces significant local factors for change, borne largely out of a poor
physical environment. Such pressures are depicted and discussed below:
Figure 13 Local Factors for Change
New Hospitals Programme
9. Improvedenvironment
9. Improvedenvironment
10. Improved clinical quality
10. Improved clinical quality
12. Respons iveness to policy initiatives
12. Respons iveness to policy initiatives13. Training &
Teaching13. Training &Teaching
14. Improved use of Resources
14. Improved use of Resources
Local Drivers Local Drivers For ChangeFor Change 11. Improved
Access11. Improved Access
15. Improved PartnershipWorking
15. Improved PartnershipWorking
16. Economic Regeneration
16. Economic Regeneration
Version 10.1
24
New Hospitals Programme
(9) The Need for Improved Physical Environment
2.2.2 In 2002 the Trust estimated that the total cost of bringing its building stock to compliance was £92 million (including fees and VAT). The Trust’s 2004/05 estates returns (ERIC returns) are based on the Department of Health’s revised methodology for calculating backlog maintenance. These returns show a cost of £46 million (excluding fees and VAT) for backlog maintenance. However, just addressing backlog maintenance problems does not address the inherent problem of multi-site working within the Trust’s ageing building stock, which is not suited to the provision of 21st century healthcare or the delivery of new models of care. Paragraphs 2.2.4 and 2.2.5 demonstrate the inadequacies of the current estate in relation to the provision of modern healthcare.
2.2.3 Although significant investment has been made in the last few years, the overall condition of the estate is deteriorating as resources available for annual maintenance do not meet all emerging requirements. Investments made have generally only allowed the Trust to mark time and have not reduced the size of problems inherited from a period when the hospital estate enjoyed Crown Immunity and emerging from further changes in legislation. The Trust has highlighted its non-compliance plan and assessed the issues. The final part of the mitigation plan being the building of the new hospitals through the PFI scheme.
2.2.4 In summary, the estate is in a poor condition both at Barts and The Royal London (see Figure 14), although the condition of the estate at The Royal London is generally poorer than that at Barts. For example, at The Royal London, backlog maintenance costs by risk category are:
■ £1.9 million – high
■ £4.3 million – significant
■ £14.3 million – moderate
■ £10.0 million - low
2.2.5 The following is an assessment of the ability of the current estate to meet its functional requirements:
Figure 14 – Condition of the Estate
Estate Function Assessment
Suitability For Purpose
■ The Trust has inappropriate accommodation for the delivery of modern clinical services, teaching, training and research;
■ The wards at The Royal London are not conducive to modern patient care and expectations in that they offer very limited sanitary facilities with inadequate privacy, with communal facilities being shared by large numbers of patients;
■ There is limited scope for reorganisation to improve efficiency;
■ Major refurbishment is prohibitively expensive; ■ The estate fails to meet the needs of the ethnic
population as departments are disparate and wayfinding is poor;
Version 10.1
25
New Hospitals Programme
Estate Function Assessment
■ There is limited ability to improve the quality of teaching and research ;
■ Opportunities to reorganise in order to maintain training accreditation and improve clinical standards are compromised by inflexible accommodation;
■ There is limited ability to introduce new technology cost-effectively;
■ The estates have poor accessibility issues, particularly for the blind and wheelchair users.
Physical Condition
■ Trust accommodation and central services are poor, with £46 million of backlog maintenance45 using the new methodology of reporting;
■ The current estate reduces the Trust’s ability to recruit and retain key medical, nursing and other support staff;
■ The current estate is costly to maintain and keep clean, making it difficult to maintain PEAT compliance;
■ There are a number of health and safety issues which compromise a safe working environment, an essential requirement of clinical governance.
Space Utilisation
■ Usage has developed piecemeal, resulting in ineffective utilisation and there is dispersed, rather than centralised or co-located, accommodation.
Fire Safety ■ The estate does not meet the minimum standards of statutory codes in all areas.
Energy Conservation
■ The majority of the estate is made up of old buildings with poor insulation and energy conservation.
Equipment
■ The Trust possesses some state of the art medical equipment but is generally unable to invest sufficient funds to meet lifecycle requirements and, consequently, much equipment is beyond its standard working life.
2.2.6 A comparison of the Trust’s estate and fitness for purpose with other similar providers in North East London shows that the Trust is the:
■ Worst in its peer group for suitability for purpose;
■ Second worst in its peer group in respect of physical condition; and
■ Highest in its peer group for inadequate space utilisation46.
2.2.7 Specific instances where the poor condition of the estate has a detrimental impact on the delivery of Trust services include:
■ There are inadequate day surgery facilities at The Royal London, where most surgical specialties are based;
■ Access to radiotherapy facilities is currently very poor. At present there is a lack of integration with the rest of cancer services. Radiotherapy is currently isolated in a basement at Barts. The new hospitals will enable radiotherapy to
45 See Appendix 2A for Backlog Maintenance Survey. 46 Figures taken from NHS Estates ERIC returns for NELSHA – 2004/05.
Version 10.1
26
New Hospitals Programme
integrate with the rest of cancer services, co-located with the cancer wards, outpatients, daycare and nuclear medicine;
■ Urology, Ear Nose and Throat and Neurophysiology, currently located at Barts, should ideally be located at The Royal London alongside the Neurosciences service. In the new build, this has the major benefit of co-locating Head and Neck clinical teams and associated staff and facilities, with access to specialist rehabilitation and interventional services;
■ Diagnostic Imaging services are scattered across sites. A similar problem was previously faced by Pathology services, which has been rectified by the construction of the new Pathology and Pharmacy building (part of the separately funded advance schemes, approved by the London Regional Office in November 2001 (see Chapter 4, paragraph 4.7));
■ Outpatient departments at both The Royal London and Barts are a considerable distance from the main clinical areas. Outpatient access to support departments for diagnostic tests, etc. is poor. The distance between these departments is approx 1/4 of a mile. Outpatient clinics are not centralised in one location and are scattered across the sites in a variety of buildings, causing wayfinding problems for patients and decreased throughput leading to delays in investigation;
■ Space for teaching and research is very limited. There is a severe shortage of teaching and conference rooms required for audit meetings and post-graduate medical education. Facilities are also very poor for clinical support staff, resulting in problems with meeting professional body requirements. Co-location of education space with clinical services, where appropriate, allows for greater integration of academic and clinical staff;
■ Expansion of critical care facilities is limited by space constraints and inflexible accommodation. There is a requirement for doubling the size of the current facility to meet a range of critical care requirements from levels 1 to 3. Current space is critical and a publicly-funded scheme has been proposed to expand capacity in the light of the immediate need; and
■ Due to inflexible accommodation at Barts there would be a need for major investment in co-locations of services before it could operate as a cancer and cardiac centre.
2.2.8 In addition, the cost of refurbishing existing ward space to modern standards is very high, both in capital and operational terms. Refurbishment has been successfully carried out in a number of areas. However, the need to meet current standards (eg single sex requirements) has necessitated, in some cases, in a reduction in available facilities. An example of this is the refurbishment of Treves Ward at The Royal London, which was improved to provide eight single rooms, four four-bedded bays and one six-bedded bay, a total of 30 beds. This now takes up one floor of the Link Block, the space previously occupied by two old-style wards which used to provide 54 beds in total.
2.2.9 In conclusion, although backlog maintenance costs may appear relatively low, adoption of a “do minimum” approach (tackling backlog maintenance) will not enable the Trust to: implement Government policy; meet cost targets; achieve efficiency savings or meet the needs of its catchment population, without significant and ongoing further investment.
(10) The Need for Improved Clinical Quality of Services
2.2.10 The high standard of clinical services provided at the Trust’s three main hospitals is fully acknowledged by patients and commissioners alike and is reflected in the Dr
Version 10.1
27
New Hospitals Programme
Foster Guide, where, for the fourth year running, the Trust has been reported as maintaining one of the lowest mortality rates in the country, 26% below what would be expected. However, the poor fabric of the buildings which were not designed for 21st century healthcare continues to impact on overall Trust performance.
2.2.11 In May 2004, Barts and The London launched Pathfinder, one of the most ambitious clinical strategies in the modern NHS. This sets the Trust on course to deliver excellence in everything we do - service efficiency, patient experience and clinical quality – with the support systems, culture and partnerships to support our ambitions (see Chapter 3). However, to enable the Trust to deliver this level of quality the following improvements, which are secured by the PFI scheme, are vital:
■ Ensuring services are more closely aligned and co-located than at present;
■ Improving co-ordination between services;
■ Adopting new technology and treatments not possible within the current building stock; and
■ Addressing “critical mass” and teaching issues.
(11) The Need for Better Access to Services
2.2.12 The nature of the local population presents access issues for the Trust:
■ Current services offered do not adequately address the different healthcare needs of the various ethnic and social groups within the wider population; and
■ Characteristics of the local population, described in Chapter 1, result in inequalities of access to healthcare which the Tower Hamlets PCT is seeking to reduce (see Chapter 3).
2.2.13 The inner North East London health economy has lower intervention rates than other health economies and the Department of Health (DH), when reviewing the sector capacity planning work, noted that these lower than national rates needed to be addressed. The inner NEL PCTs all have strategies to help ensure that intervention rates are appropriate by ensuring suitable infrastructure is available in primary and secondary care. These strategies are mindful of the nature of the inner NEL population and their social, economic and ethnic differences.
2.2.14 To overcome these issues and keep the Trust at the forefront of specialised provision, the services provided by the Trust must adapt to meet the changing healthcare needs of local people. In addition, local services must be organised in conjunction with other local providers to ensure appropriate range and coverage to serve the wider population with a range of specialist services. Current facilities lack the flexibility to ensure this, as they do not allow services and departments to be co-located in such a way as to maximise the opportunities for a higher quality of patient care. In the past, the Trust has been forced to compromise on the care it is able to deliver, to maximise the use of existing accommodation.
2.2.15 For example, maternity services are currently spread across The Royal London site in a variety of different locations. This results in a convoluted patient journey, with the lack of an integrated care pathway, which may sometimes mean that a mother is separated from her baby in neonatal intensive care as this is located in another building and necessitates a journey through the hospital garden. The proposed scheme will allow mothers to be admitted to a Labour Delivery Recovery and Post-partum (LDRP) room where they will remain for the entire duration of their stay, facilitating antenatal delivery and post-partum care in the same homely environment. These rooms are co-located with ultrasound, obstetric theatres and the neonatal unit, facilitating provision of all obstetric services in one location.
Version 10.1
28
New Hospitals Programme
2.2.16 The physical solution that has been developed by the Trust and its PFI partner, will address similar issues in other services by providing facilities to accommodate efficient and modern care pathways across the appropriate range of services, to meet the activity levels projected (see Chapter 3).
2.2.17 The solution will also improve the physical access difficulties which visitors and patients of the Trust currently encounter (see Chapter 7 for further information and Estates Annex Ref E27 and E28 for design solutions). At present:
■ Trust sites have inadequate designated disabled parking facilities; and
■ Access to The Royal London Hospital from the Whitechapel underground station needs improving, as it is difficult for those with difficulties walking.
(12) The Need to Change to Meet National and Local Policy Imperatives
2.2.18 Existing accommodation limits the Trust’s ability to respond fully to new initiatives or to take a proactive lead in tackling service pressures. While the Trust has successfully responded to a number of major initiatives, provision of modern, flexible accommodation would allow it to respond more effectively and to meet such policy imperatives as:
■ Improving clinical performance and reducing waiting lists and waiting times;
■ Responding to winter pressures;
■ Improving relationships with PCTs;
■ Eliminating mixed sex wards;
■ Integrating services with other local providers;
■ Improving services to patients with long-term conditions; and
■ Enhancing dignity for patients.;
(13) The Need to Change to Meet Training, Teaching and Research Needs
2.2.19 As a teaching hospital Trust, Barts and The London provides a large number of placements for student doctors, dentists, nurses and other healthcare professionals in training at the Medical and Dental School at Queen Mary and Westfield (QMW). These students benefit from the expertise and experience of some of the most skilled clinicians in the country.
2.2.20 The constituent colleges of QMW led the way in developing the work that informed Tomorrow's Doctors (the report produced by the General Medical Council). QMW was the first medical school in the UK to implement a new curriculum following its recommendations.
2.2.21 In Tomorrow's Doctors, the General Medical Council (GMC) emphasised the importance of an integrated approach to the medical curriculum, stressing links between students, health service users and practitioners, from the initial training stages. This breaks the historic pattern of medical education in which teaching has been organised by clinical specialty and the traditional separation of pre-clinical (basic medical sciences) and clinical (hospital-based) elements.
2.2.22 The Curriculum Management Committee of the Medical and Dental School emphasised the need for enhanced facilities to support the developing curriculum, including:
Version 10.1
29
New Hospitals Programme
• A major communications skills facility with adjacent seminar/interview rooms and a substantial clinical skills laboratory;
• Adequate space for an education unit;
• Adequate provision to expand computer-assisted learning and medical informatics; and
• Provision for a rapid turnaround multi-use teaching laboratory.
2.2.23 A key factor in the success of such a curriculum is that it can be offered within a more diverse clinical environment. The curriculum itself demands that students have access to an enhanced range of specialities and a substantially broader patient base than is possible without reconfiguration. However, following re-development of the Trust, the major services on which the curriculum is based will be located at The Royal London, adjacent to the Medical School’s (approximately) £50 million redevelopment, which has recently been completed on this site.
2.2.24 Fundamental to the planning of future teaching and research is strong support for the view that teaching and research follows clinical services, and not vice versa.
2.2.25 Co-location of teaching and research facilities with the clinical specialties is a fundamental requirement to teach and develop research of international repute. This will produce better trained doctors, many of whom will be committed to East London, while benefiting the local health economy and the NHS as a whole.
2.2.26 The new buildings would also enable the creation of a “centre of excellence’. There is strong evidence to suggest that this would enable the Trust to recruit the highest quality staff, something that the Trust would hope to achieve within a very short period of time.
(14) The Need to Change to Make More Effective Use of Resources
2.2.27 To make better use of resources, both human and capital, the Trust must provide the following, all of which are significantly enabled by the redevelopment:
• The most effective integration and linking of clinical services to teaching, research and development, thereby facilitating maximisation of closer working relationships to achieve teaching capabilities and development opportunities;
• The best possible fit between teaching and research and the facilities in which they are to be provided;
• A compact “campus” style facility, which minimises travel and movement times between departments for staff and patients; and
• The efficient deployment of capital assets to secure an optimal cost base related to estate and facilities management, in order to maximise the proportion of expenditure directed towards clinical services. At present, resources have to be spent on maintaining old and unsuitable buildings which would be better spent on direct patient care.
(15) The Need to improve Partnership Working
2.2.28 The Trust has undertaken extensive liaison with NELSHA, Tower Hamlets PCT (as PCT lead) and clinicians, in order to ensure the clinical suitability of the proposed scheme (Chapter 3 outlines how the preferred solution will meet local requirements). A partnership approach has also been essential in planning and accommodating the affordability pressures that arise as a consequence of the project. (See Chapter 11)
Version 10.1
30
New Hospitals Programme
2.2.29 Both the Trust and the PCTs, particularly those in Tower Hamlets, Newham and City and Hackney, who together provide a large proportion of the Trust’s annual income and who have committed significant amounts of growth to meet the extra cost of the planned development (see Chapter 11), are convinced that the New Hospitals Project delivers a solution which supports and delivers commissioners’ future ongoing activity requirements, while remaining affordable. Close working between the Trust and its healthcare and local authority partners to coordinate, plan and organise the delivery of local services, is essential for the delivery of seamless patient care.
2.2.30 PCT involvement has included regular reports to the North East London Chief Executive’s Group, which has representation from all PCTs and trusts within NELSHA. At an operational/management level, representatives from NELSHA and Tower Hamlets PCT have been members of the Project Board. This has enabled them to have a contributory voice on the overarching, decision-making body of the project, responsible for taking high-level decisions regarding both the direction and the detail of the scheme as required (see Chapter 14 for details).
2.2.31 The project is a key element in NELSHA’s plans to meet the growing needs of the population, the Cancer Plan and the implementation of the National Service Frameworks. NELSHA’s strategy47 describes the external developments both within primary and secondary care facilities across the region, with which the Barts and The London development will dovetail. These include hospital redevelopments at Whipps Cross and Barking, Havering and Redbridge (Romford) NHS Trusts, the new ITSC at King George’s in Ilford, further development phases at Newham General, re-provision of Tower Hamlets mental health services and the establishment of LIFT in all PCTs (See Chapter 3 for the project’s fit with all local healthcare providers).
2.2.32 There are developments underway in the region to improve the significant access problems to the 42 GP practices. This number is insufficient for the population size, but there are difficulties in recruiting to vacancies. In addition, many premises are significantly below standard and too small for modern primary care services. Tower Hamlets PCT is actively working on increasing capacity in this aspect of primary care. It was successful in establishing two PMS Practices in 2002 and is continuing with its scheme for salaried GPs. In addition, extra GP sessions are being made available in the Whitechapel Walk-in-Centre.
2.2.33 The new hospitals will therefore support, and be supported by, a primary healthcare system expanding in volume, quality and choice. Developments such as the increase in treatment centres for elective surgery, occurring across the sector, will enable healthcare providers to work together to meet waiting list targets (see Chapter 3 for further details).
2.2.34 The Trust is not, however, dependent on planned external developments for the delivery of its objectives.
2.2.35 The support and contribution of our local partners has been invaluable in taking the project forward. It will be vital to continue to work in tandem to ensure that activity targets and commissioners’ requirements are met through the development of this scheme and that the very best possible healthcare is delivered to the community that we serve.
47 See Appendix 1A for the NELSHA strategy.
Version 10.1
31
New Hospitals Programme
(16) The Need to Play a Proactive Role in Regenerating the Local Economy
2.2.36 Community partnerships have developed since the project’s inception. The scale of the redevelopment has encouraged the Trust to instigate a regeneration process that complements its business priorities and reflects the impact of the development on the local community and economy which, as noted above, is characterised by high deprivation and social exclusion.
2.2.37 Following a feasibility study supported by NELSHA and the London Development Agency (LDA), the Trust appointed a Regeneration Manager in March 2004 to develop a regeneration strategy and implementation plan.
2.2.38 This strategy was completed and approved by the Trust in May 2004.48 It has been developed in line with NHS policy objectives to reflect:
• The new hospitals development;
• NHS policy (see Tackling Health Inequalities: a Programme for Action 2003); and
• The Strategic Health Authority’s Regeneration Strategy (2003).
2.2.39 The Trust’s regeneration strategy and implementation plan sets out the following objectives:
Employment: To achieve a staff complement that is progressively more representative of the Trust’s diverse locality and that has the opportunity to attain career progression.
Development To develop sustainable hospitals that meet the triple bottom line (financial, environmental and social).
Procurement: To source goods and services locally where possible and practicable.
Community: To ensure effective community use and ownership of Trust facilities and services.
2.2.40 The strategy recognised that the Trust can do more to respond to the regeneration need of its local communities, especially in the area of employment, where local people are currently under-represented within the workforce, particularly those from the Bangladeshi community. In addressing this, the Trust will also make progress in addressing the following important business needs (see Chapter 16 for further details):
• Reduced recruitment costs;
• Reduced turnover rates;
• Opportunity to generate job-ready staff;
• A reduction in staff accommodation needs; and
• Better service delivery through culturally/linguistically sensitive staff.
2.2.41 It will also result in the following longer-term benefits;
• Local ownership of facilities by the local community;
• Improved staff retention through local renewal; 48 See Appendix 2.B, Improving Health; Growing and Sustaining Prosperity, 2004
Version 10.1
32
New Hospitals Programme
• Generating secondary employment through local procurement; and
• Improving public health through increased local employment.
2.2.42 The Regeneration Strategy centrally involves partnership with Skanska Innisfree (SI), who will play the lead role in achieving the development objective and play a critical role in achieving the employment, procurement and community objectives in their facilities management role. As developer, SI will be responsible for meeting the Local Authority’s aspirations in relation to use of local labour in the construction contracts for the new hospitals. SI has employed a Community Relations Manager to manage their input into the regeneration programme and to establish community contacts.
2.2.43 Both the Trust and SI are involved in wider discussions that relate to the regeneration implications of the development. In Tower Hamlets, plans for The Royal London hospital will involve the creation of a health and education campus that will play a key role in the regeneration of Whitechapel. The additional public space and concentration of staffing and facilities will complement the development of the new Medical School building south of the development and a range of initiatives on Whitechapel Road. These range from the Council’s new IDEAs Store (library, advice and training centre) to the new East London Muslim Centre and expanded Whitechapel Gallery.
2.2.44 The regeneration programme has developed a close partnership with the Ocean New Deal for Communities Programme which lies adjacent to the east of the site and is the largest social housing scheme in Tower Hamlets. This area is being targeted for training, employment and business opportunities.
2.2.45 There are opportunities being generated by the PFI for complementary developments on The Royal London site that will add value to the main development. These include the scope for developing key worker housing, extended childcare provision and additional retail and leisure facilities.
2.2.46 In relation to Barts, the focus has been to form a partnership with The City Fringe Partnership (CFP) which, since 1996, has brought together the Corporation of The City of London and the London Boroughs of Hackney, Islington, Tower Hamlets and Camden in the regeneration of the areas to the immediate north and east of The City. The CFP is supported mainly through the LDA and has targeted health and social care as a key sector for encouraging local unemployed people.
2.2.47 Barts sits at the heart of The City Fringe area and, although the opportunities for physical regeneration are less evident than for the Royal London, the development of Barts will contribute to the improvement of the area and secure the provision of hospital services in the City. The development will play a full role in extending the opportunities to residents in the City fringe, including local labour opportunities in construction, FM and health.
2.2.48 SI and the Trust are working with partners in implementing the aims of the FRESA (Framework for Regional Employment Skills Assessment). The Framework was set up by the London Skills Commission and established a set of actions relating to employment and skills on a regional basis. This set out the overall strategy for London and provides key themes. The FRESA highlights a number of employment sectors where it expects an improvement in skills and employment. These include both health and social care and construction. The Trust and SI have had the opportunity to input into the sub-groups established to guide the work in these areas.
Version 10.1
33
New Hospitals Programme
2.2.49 To ensure stakeholder involvement in the regeneration programme, a Sustainable Regeneration Stakeholder Group (SRSG) has been set up that includes NELSHA, Tower Hamlets PCT, the LDA, the London Health Commission, City Fringe Partnership, Job Centre Plus, REMPLOY and the Ocean New Deal for Communities programme. Both the Trust and SI are involved in local regeneration structures such as the Tower Hamlets Partnership, Local Area Partnerships, NELSHA FRESA, Tower Hamlets Business Forum and the CFP.
2.2.50 In order to demonstrate the interconnections of the programme and to ensure a comprehensive approach, an overarching Sustainable Development Plan has been developed. This forms the basis for further engagement with the local authorities and the wider community. A key element of the plan is to ensure that the development of the new hospitals meets sustainability criteria, including socio-economic needs, energy use, carbon efficiency, waste minimisation and green transport. The links with the Thames Gateway Sustainable Communities Programme will be made during this process so that the scheme takes into account the new communities envisaged in this plan and the need for sustainable development in this context.
2.2.51 The Trust is developing three action plans to generate programmes to deliver its objectives:
• Actions for Community Employment (ACE);
• Healthy Local Economy (HLE); and
• Sustainable Friendly Environment (SFE).
2.2.52 Further detail of the ACE programme, which is well underway, is given below. The other two programmes are being developed under the Sustainable Development Index, which sets out the range of sustainable outcomes and opportunities created by the development and operations of the Trust. The most developed of these will consist of a sustainable procurement programme, including support for local businesses. This is under discussion with Business Link and other partners.
2.2.53 The ACE programme began in January 2005 and will create a three-part process to encourage community applications for entry-level jobs with the Trust. Entry-level jobs are defined as those requiring an NVQ 2 or lower qualification and account for 1,800 posts within the Trust. They include A & C Grades 3 and 4, ancillaries, healthcare support workers (HCSWs) and junior technical staff. High turnover rates in these staff groups mean that there are over 300 vacancies annually that could be filled through the ACE strategy.
2.2.54 The threefold approach entails:
• Employment of a Community Employment Manager to ensure ring-fenced posts are available for community candidates and to work with general managers and human resource managers to remove blockages to this approach;
• Creation of a shop front access point for community candidates, staffed by a multi-agency team including the Trust, Job Centre Plus and Employment Solutions (an employment brokerage agency run by the Local Authority and Tower Hamlets College). This will include advice and guidance for candidates for construction jobs in the new build schemes as well as health related employment; and
• Intensifying the use of a range of training and employment schemes including apprenticeships and transitional employment measures, including the Trust’s work placement programme “Work Wise’.
Version 10.1
34
New Hospitals Programme
2.2.55 It is planned that these approaches will be funded from external sources, including funding from the LDA, Job Centre Plus, Local Authority, and Neighbourhood Renewal Funding.
2.2.56 The ACE strategy will link to the new hospitals programme by:
• Linking local economic inactivity with the workforce needs of the Trust;
• Creating a single point of access for members of the community looking at careers within the Trust and the local health economy;
• Generating more effective services through having a staff that is more representative of the local community and which will be able to provide a more culturally and linguistically sensitive service. Currently the Trust's staff are not representative of the local population, especially in regard to the Bangladeshi population. The new development will support more local recruitment by emphasising local regeneration and providing a focal point for recruitment campaigns. It will also parallel local recruitment campaigns in construction;
• Linking with SI to provide signposting to vacancies in health, facilities management and construction. Candidates for vacancies in these areas will be assessed at nearby locations in Stepney and Poplar; and
• Using the opportunity of major investment and greatly enhanced new health facilities, to generate a positive relationship between the Trust and the local community by offering direct employment benefits.
2.2.57 ACE will be the first major project within the regeneration strategy and will be designed as a three-year initiative to change the way the Trust approaches community employment in advance of the new hospitals being available.
Achieving Foundation Status
2.2.58 Achieving Foundation Trust status is a priority for the Trust. Addressing the strategic and Trust-specific factors for change will clearly place the Trust in a much stronger position to achieve such status. However Foundation Trust status will be achieved at a time when the new hospitals are under construction and a huge change agenda is underway. The Trust considers it will be able to operate under the Foundation Trust regime post-FBC (see section 11.18).
2.2.59 The Trust has established a comprehensive post-FBC project management structure and is in the process of recruiting the associated delivery team, to ensure that the project is managed effectively and in such a way that supports the Trust’s endeavours in pursuing Foundation Trust status. This, coupled with a clear accountability framework and escalation procedure, will ensure that only relevant and important issues or decisions take up the Trust Board and senior management time.
2.3 Chapter Conclusion 2.3.1 There are weaknesses in the Trust's current service provision due to the poor
condition of the Trust’s facilities. When allied to the social, demographic and environmental factors of East London, the Trust’s future strategy for service delivery, the outcome of the London (Turnberg) Review and the range of pressures the services will face in the coming years, makes the case for the redevelopment of the hospitals in the Trust overwhelming.
2.3.2 Without change, the existing weaknesses would be accentuated and pressures on the current service model would increase. If the Government’s initiatives, set out in
Version 10.1
35
New Hospitals Programme
the NHS Plan for modernising the health service are to be achieved and the 10 High Impact Changes are to be delivered for the people of North East London and beyond, a modern, purpose-built facility is required. The Trust will struggle to sustain performance and deliver against these initiatives without the new hospitals (see section 2.2 above).
2.3.3 The Trust has therefore endeavoured to prepare and commission, in partnership with local organisations and healthcare providers, the best (most economic efficient and innovative) solution. The following chapters in the FBC set out how this process has been undertaken and the resulting PFI scheme.
2.4 Chapter Appendices
2A Backlog Maintenance Survey 2B Improving Health; Growing and Sustaining Prosperity, May 2004
Version 10.1
36
New Hospitals Programme
3 NEW MODELS OF CARE Synopsis – New Models of Care
This chapter sets out: ■ The process undertaken to develop the Trust’s service models.
■ The proposed new models of care in the wider health economy.
■ The proposed new service models as they apply to the Trust.
■ An overview of the design and clinical adjacencies of the new hospitals.
■ The planning assumptions used to inform the bed requirements, activity and performance.
3.1 Introduction 3.1.1 This chapter describes the Trust’s models of care, activity and facilities in relation to
beds and theatres. It also describes the clinical strategy to implement the new models of care, design services around the needs of the patients and improve access to services through the coming years.
3.1.2 The Trust’s clinical strategy49 sets out a framework for future development. Its objectives are to achieve excellence in clinical quality, service efficiency and patient experience, supported by effective and appropriate cultures, systems and partnership working.
3.2 Clinical Development Plan 3.2.1 When the NHS Executive approved the Outline Business Case (OBC) in February
2000, it recommended that the Trust increase the number of planned beds by 26 and elderly patient beds by 25 providing, in total, an additional 51 beds. In response, the Trust undertook an extensive exercise in liaison with clinicians across all specialties in the Trust, to establish activity and forecast case mix requirements and, in turn, bed numbers. As part of this detailed exercise, clinical performance targets were reviewed, i.e. individual specialty length of stay, inpatient and day-case/short stay rates and a review of the models of care assumed in the OBC. This exercise resulted in the production of the Clinical Development Plan (CDP), a joint exercise undertaken with the local health authority. The outputs of the CDP are described in section 3.3 below. See also Chapter 4, Figure 31 for a detailed reconciliation of bed numbers from the OBC.
Pathfinder Clinical Strategy
3.2.2 Following the establishment of the CDP, during 2003 and 2004 the Trust developed its Pathfinder Clinical Strategy. Developed by 300 Trust clinicians and managers in conjunction with key partner organisations, Pathfinder sets out the challenges ahead over the next five years, the opportunities opening up to the Trust and how it intends to seize them. This strategic framework recognises (in line with the Clinical Development Plan) that some services will be better provided in community settings, with some complex sub-specialist services benefiting from greater centralisation. The development of Pathfinder has been driven by the strong
49 Pathfinder Clinical Strategy 2004-09: Barts and The London NHS Trust, 2004. See Appendix 3A.
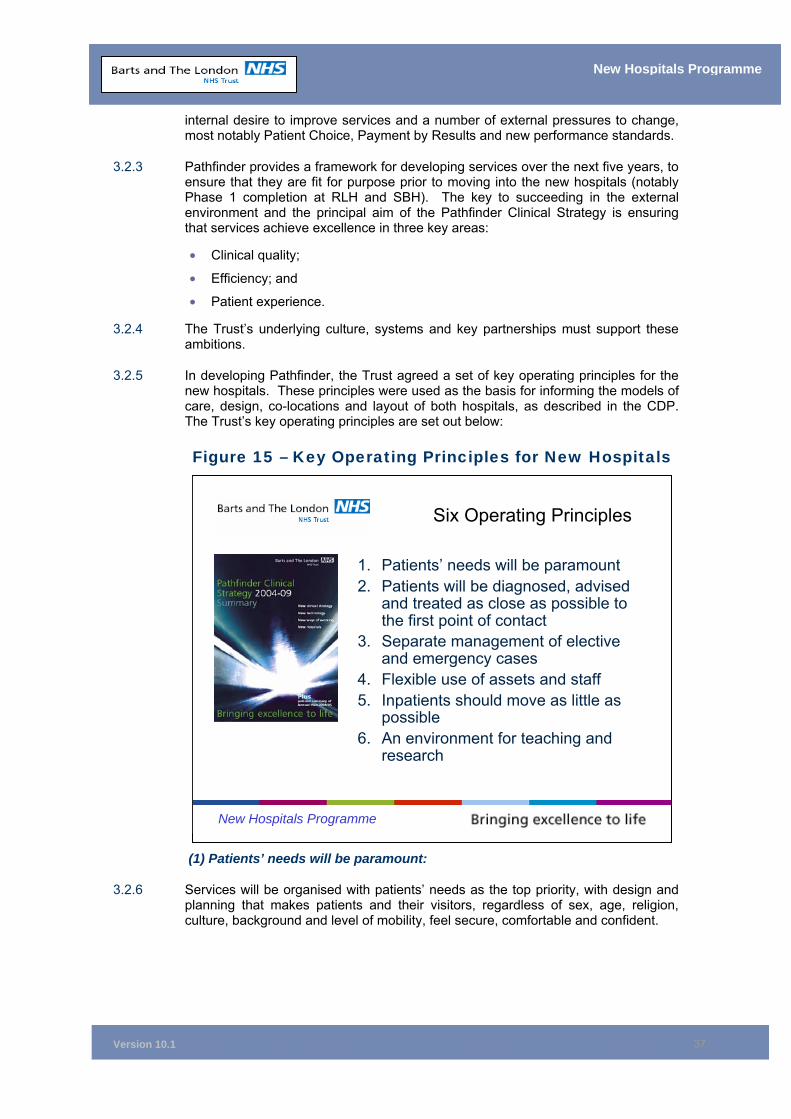
Version 10.1
37
New Hospitals Programme
internal desire to improve services and a number of external pressures to change, most notably Patient Choice, Payment by Results and new performance standards.
3.2.3 Pathfinder provides a framework for developing services over the next five years, to ensure that they are fit for purpose prior to moving into the new hospitals (notably Phase 1 completion at RLH and SBH). The key to succeeding in the external environment and the principal aim of the Pathfinder Clinical Strategy is ensuring that services achieve excellence in three key areas:
• Clinical quality;
• Efficiency; and
• Patient experience.
3.2.4 The Trust’s underlying culture, systems and key partnerships must support these ambitions.
3.2.5 In developing Pathfinder, the Trust agreed a set of key operating principles for the new hospitals. These principles were used as the basis for informing the models of care, design, co-locations and layout of both hospitals, as described in the CDP. The Trust’s key operating principles are set out below:
Figure 15 – Key Operating Principles for New Hospitals
(1) Patients’ needs will be paramount:
3.2.6 Services will be organised with patients’ needs as the top priority, with design and planning that makes patients and their visitors, regardless of sex, age, religion, culture, background and level of mobility, feel secure, comfortable and confident.
New Hospitals Programme
Six Operating Principles
1. Patients’ needs will be paramount 2. Patients will be diagnosed, advised
and treated as close as possible to the first point of contact
3. Separate management of elective and emergency cases
4. Flexible use of assets and staff 5. Inpatients should move as little as
possible6. An environment for teaching and
research
Version 10.1
38
New Hospitals Programme
(2) Patients will be diagnosed, advised and treated as close as possible to the first point of contact
3.2.7 Diagnostic and treatment services will reflect differing patient flows, with clinical information and expertise available to make a diagnosis during the first contact. There will be particular focus on rapid diagnosis and immediate treatment to patients attending A&E, to prevent unnecessary admission. The Trust will work in partnership with local GPs to avoid inappropriate hospital referrals.
(3) Separate management of elective and emergency cases
3.2.8 A number of factors will be implemented to achieve the separate management of elective and emergency cases. A&E attendances will be curtailed through the implementation of a number of primary care initiatives (see paragraph 3.5.3). Both emergency and elective patients will be admitted according to clinical need. A significant proportion of short stay elective surgery and scheduled medical treatment will be carried out within an ambulatory/short stay setting. There will be more formal separation of unscheduled/emergency and scheduled/elective facilities, with resources allocated on a flexible basis to reflect changing patterns of care and needs. (See section 3.3.5 below for further information)
(4) Flexible use of assets and staff
3.2.9 Through more effective use of integrated information systems and capital equipment, the Trust will offer a more comprehensive 24-hours a day, seven days a week capability. For example the Outpatients Department will offer extended flexible opening and short stay surgery will be open from 8am Monday to 6pm Saturday (inclusive). Flexible design and agreed performance standards will support this operation.
(5) Inpatients should move as little as possible
3.2.10 The overall design of the hospitals will ensure that patient movement is minimised, with diagnostic and treatment facilities being co-located wherever practicable.
(6) An environment for teaching and research
3.2.11 The overall design will take full account of the needs of teaching and research, while operational policies of both clinical and non-clinical services will ensure that issues such as teaching accreditation are properly addressed. As far as possible, teaching and research will be integrated with clinical services.
3.3 Outcome of the CDP 3.3.1 The outcome of the CDP review resulted in revised bed numbers and changes to
associated short stay and diagnostic/interventional facilities, based on the new models of care as described in the CDP. The CDP identified the need for an additional 85 beds, giving a total complement of 1,285 beds.
Changes to the CDP
3.3.2 The recent repatriation of routine cardiology and cardiothoracic services to Essex reduced the number of beds identified in the CDP by 37 to an overall total of 1,248 (905 at The Royal London and 343 at Barts). Following this change, the data and assumptions used in the CDP have been re-based on the 2003/04 performance and activity data projected forward to 2011. The bed requirement and outpatient
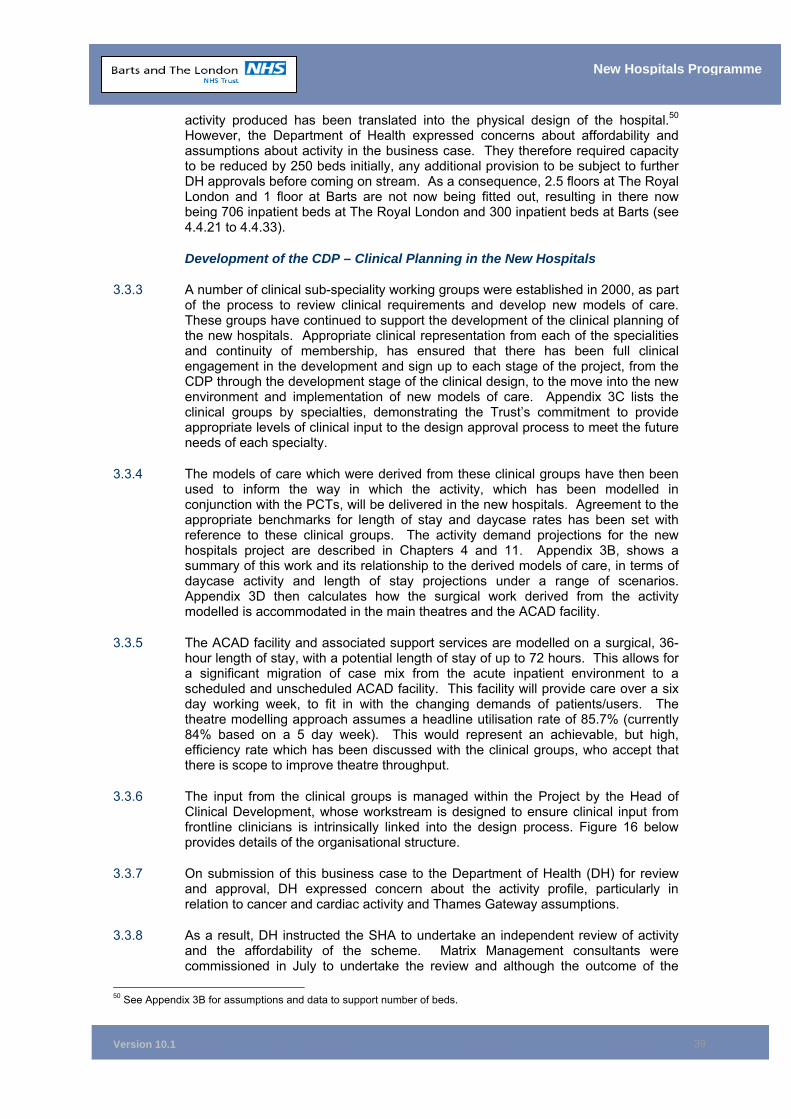
Version 10.1
39
New Hospitals Programme
activity produced has been translated into the physical design of the hospital.50 However, the Department of Health expressed concerns about affordability and assumptions about activity in the business case. They therefore required capacity to be reduced by 250 beds initially, any additional provision to be subject to further DH approvals before coming on stream. As a consequence, 2.5 floors at The Royal London and 1 floor at Barts are not now being fitted out, resulting in there now being 706 inpatient beds at The Royal London and 300 inpatient beds at Barts (see 4.4.21 to 4.4.33).
Development of the CDP – Clinical Planning in the New Hospitals
3.3.3 A number of clinical sub-speciality working groups were established in 2000, as part of the process to review clinical requirements and develop new models of care. These groups have continued to support the development of the clinical planning of the new hospitals. Appropriate clinical representation from each of the specialities and continuity of membership, has ensured that there has been full clinical engagement in the development and sign up to each stage of the project, from the CDP through the development stage of the clinical design, to the move into the new environment and implementation of new models of care. Appendix 3C lists the clinical groups by specialties, demonstrating the Trust’s commitment to provide appropriate levels of clinical input to the design approval process to meet the future needs of each specialty.
3.3.4 The models of care which were derived from these clinical groups have then been used to inform the way in which the activity, which has been modelled in conjunction with the PCTs, will be delivered in the new hospitals. Agreement to the appropriate benchmarks for length of stay and daycase rates has been set with reference to these clinical groups. The activity demand projections for the new hospitals project are described in Chapters 4 and 11. Appendix 3B, shows a summary of this work and its relationship to the derived models of care, in terms of daycase activity and length of stay projections under a range of scenarios. Appendix 3D then calculates how the surgical work derived from the activity modelled is accommodated in the main theatres and the ACAD facility.
3.3.5 The ACAD facility and associated support services are modelled on a surgical, 36-hour length of stay, with a potential length of stay of up to 72 hours. This allows for a significant migration of case mix from the acute inpatient environment to a scheduled and unscheduled ACAD facility. This facility will provide care over a six day working week, to fit in with the changing demands of patients/users. The theatre modelling approach assumes a headline utilisation rate of 85.7% (currently 84% based on a 5 day week). This would represent an achievable, but high, efficiency rate which has been discussed with the clinical groups, who accept that there is scope to improve theatre throughput.
3.3.6 The input from the clinical groups is managed within the Project by the Head of Clinical Development, whose workstream is designed to ensure clinical input from frontline clinicians is intrinsically linked into the design process. Figure 16 below provides details of the organisational structure.
3.3.7 On submission of this business case to the Department of Health (DH) for review and approval, DH expressed concern about the activity profile, particularly in relation to cancer and cardiac activity and Thames Gateway assumptions.
3.3.8 As a result, DH instructed the SHA to undertake an independent review of activity and the affordability of the scheme. Matrix Management consultants were commissioned in July to undertake the review and although the outcome of the
50 See Appendix 3B for assumptions and data to support number of beds.
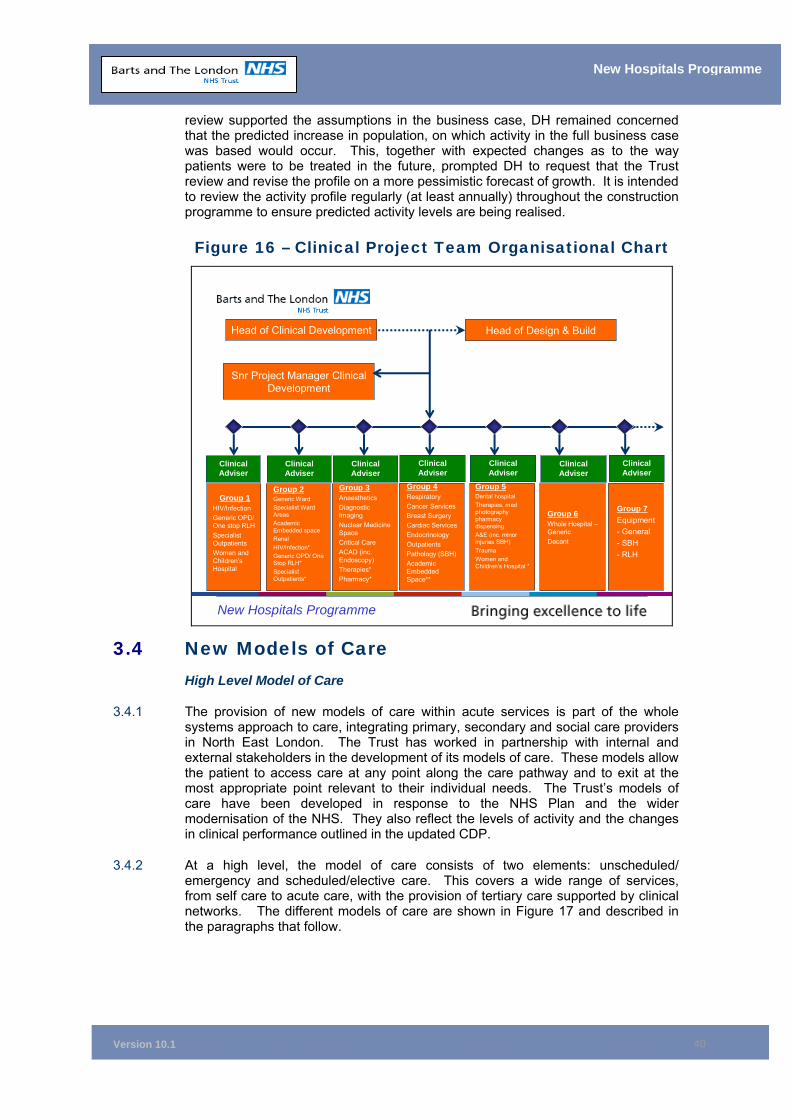
Version 10.1
40
New Hospitals Programme
review supported the assumptions in the business case, DH remained concerned that the predicted increase in population, on which activity in the full business case was based would occur. This, together with expected changes as to the way patients were to be treated in the future, prompted DH to request that the Trust review and revise the profile on a more pessimistic forecast of growth. It is intended to review the activity profile regularly (at least annually) throughout the construction programme to ensure predicted activity levels are being realised.
Figure 16 – Clinical Project Team Organisational Chart
New Hospitals Programme
Group 1HIV/InfectionGeneric OPD/ One stop RLHSpecialist OutpatientsWomen and Children’s Hospital
Clinical Adviser
Head of Clinical Development Head of Design & Build
Snr Project Manager Clinical Development
Group 2Generic WardSpecialist Ward AreasAcademic Embedded spaceRenalHIV/Infection*Generic OPD/ One Stop RLH*Specialist Outpatients*
Clinical Adviser
Group 3AnaestheticsDiagnostic ImagingNuclear Medicine SpaceCritical CareACAD (inc. Endoscopy)Therapies*Pharmacy*
Clinical Adviser
Group 4RespiratoryCancer ServicesBreast SurgeryCardiac ServicesEndocrinologyOutpatientsPathology (SBH)Academic Embedded Space**
Clinical Adviser
Group 5Dental hospitalTherapies, med photography pharmacy dispensingA&E (inc. minor injuries SBH)TraumaWomen and Children’s Hospital *
Clinical Adviser
Group 6Whole Hospital –GenericDecant
Clinical Adviser
Group 7Equipment- General- SBH- RLH
Clinical Adviser
3.4 New Models of Care High Level Model of Care
3.4.1 The provision of new models of care within acute services is part of the whole systems approach to care, integrating primary, secondary and social care providers in North East London. The Trust has worked in partnership with internal and external stakeholders in the development of its models of care. These models allow the patient to access care at any point along the care pathway and to exit at the most appropriate point relevant to their individual needs. The Trust’s models of care have been developed in response to the NHS Plan and the wider modernisation of the NHS. They also reflect the levels of activity and the changes in clinical performance outlined in the updated CDP.
3.4.2 At a high level, the model of care consists of two elements: unscheduled/ emergency and scheduled/elective care. This covers a wide range of services, from self care to acute care, with the provision of tertiary care supported by clinical networks. The different models of care are shown in Figure 17 and described in the paragraphs that follow.
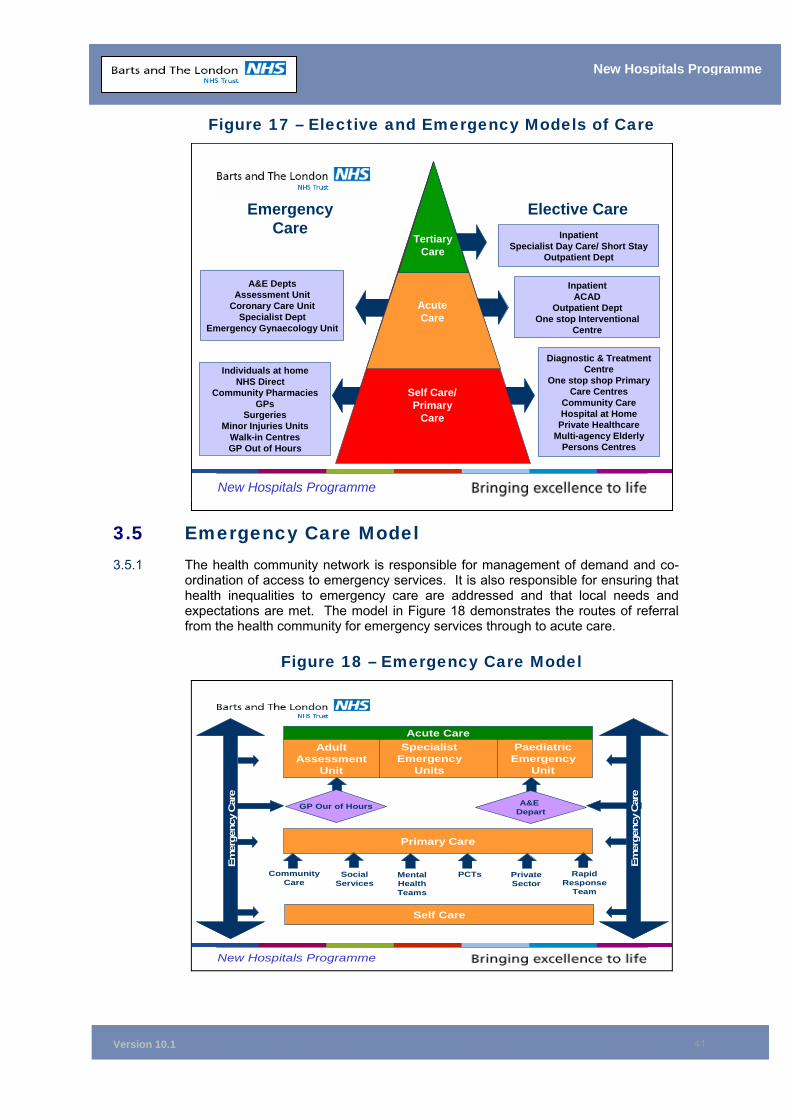
Version 10.1
41
New Hospitals Programme
Figure 17 – Elective and Emergency Models of Care
3.5 Emergency Care Model 3.5.1 The health community network is responsible for management of demand and co-
ordination of access to emergency services. It is also responsible for ensuring that health inequalities to emergency care are addressed and that local needs and expectations are met. The model in Figure 18 demonstrates the routes of referral from the health community for emergency services through to acute care.
Figure 18 – Emergency Care Model
New Hospitals Programme
Acute CareAdult
Assessment Unit
Specialist Emergency
Units
Paediatric Emergency
Unit
GP Our of Hours A&E Depart
Primary Care
Community Care
Social Services
Mental Health Teams
PCTs Private Sector
Rapid Response
Team
Self Care
Emer
genc
y C
are
Emer
genc
y C
are
New Hospitals Programme
Tertiary Care
Acute Care
Self Care/ Primary
Care
A&E Depts Assessment Unit
Coronary Care Unit Specialist Dept
Emergency Gynaecology Unit
Individuals at home NHS Direct
Community Pharmacies GPs
Surgeries Minor Injuries Units
Walk - in Centres GP Out of Hours
Inpatient Specialist Day Care/ Short Stay
Outpatient Dept
Inpatient ACAD
Outpatient Dept One stop Interventional
Centre
Diagnostic & Treatment Centre
One stop shop Primary Care Centres
Community Care Hospital at Home
Private Healthcare Multi - agency Elderly
Persons Centres
Emergency Care
Elective Care
Version 10.1
42
New Hospitals Programme
Emergency Self/Primary Care
3.5.2 The aim is to provide high quality, focused care to patients close to their homes, in line with Keeping the NHS Local – A New Direction of Travel. A proactive approach within primary care will allow this to happen. Patients with minor injuries or illnesses will be seen by senior nurses and GPs, which will result in early assessment, diagnosis, treatment and shorter waiting times.
3.5.3 Emergency care for minor illnesses and injuries will be provided within the primary care setting either by:
• Self treatment at home by the individual;
• Minor Injury Units that are nurse practitioner led using agreed clinical protocols;
• GP surgeries/clinics: with services provided by a range of health professionals such as health visitors, specialist nurses and GPs, including provision of phlebotomy and podiatry services;
• Emergency Nurse Practitioners within the Emergency Department: providing diagnosis and treatment;
• NHS Direct: providing protocol-driven advice and alternative solutions to avoid inappropriate visits to acute hospitals and GP surgeries;
• GP out-of-hours service: using rapid response teams to avoid admission to acute hospitals; and
• Community pharmacies: providing advice for minor ailments and injuries.
3.5.4 There will be direct primary care via “telemedicine” to diagnostics and specialist opinion 24 hours a day.
3.5.5 The Minor Injuries Unit at Barts will have direct referral access to the on-site Cardiac Unit, access to specialist opinion or diagnostics/reports linked to the A&E department at The Royal London.
3.5.6 The GP out-of-hours service is co-located with A&E at The Royal London providing rapid access to diagnostics and direct admission to acute services.
3.5.7 The development of the Care Record Service (CRS) and the Picture Archiving and Communication Systems (PACS) accessible also to primary care will improve the quality of care to the patient. The Trust is currently evaluating the option of taking an early release of the Care Cast package in Spring 2006. The CRS business case is being amended in line with the changes in the deployment programme (the Trust is about to receive details of proposed changes from Connecting for Health London and Capital Care Alliance (CCA)). Full CRS is due to be implemented by 2007/08 (subject to receipt of the latest deployment plan proposal). The Trust should therefore have CCA's CRS in place well in advance of completion of Phase 1 at Barts and the Royal London.
3.5.8 A whole system bed management service, available to all sectors of the local health economy, will improve management of care and use of resources.
Emergency Acute Care
3.5.9 Patients will be immediately assessed by a health professional and streamed according to the severity of the illness/trauma, diagnosis or age. Rapid assessment will ensure that the patient is directed to the most appropriate service. Patients will be seen and treated more quickly by consultant-led teams to achieve rapid
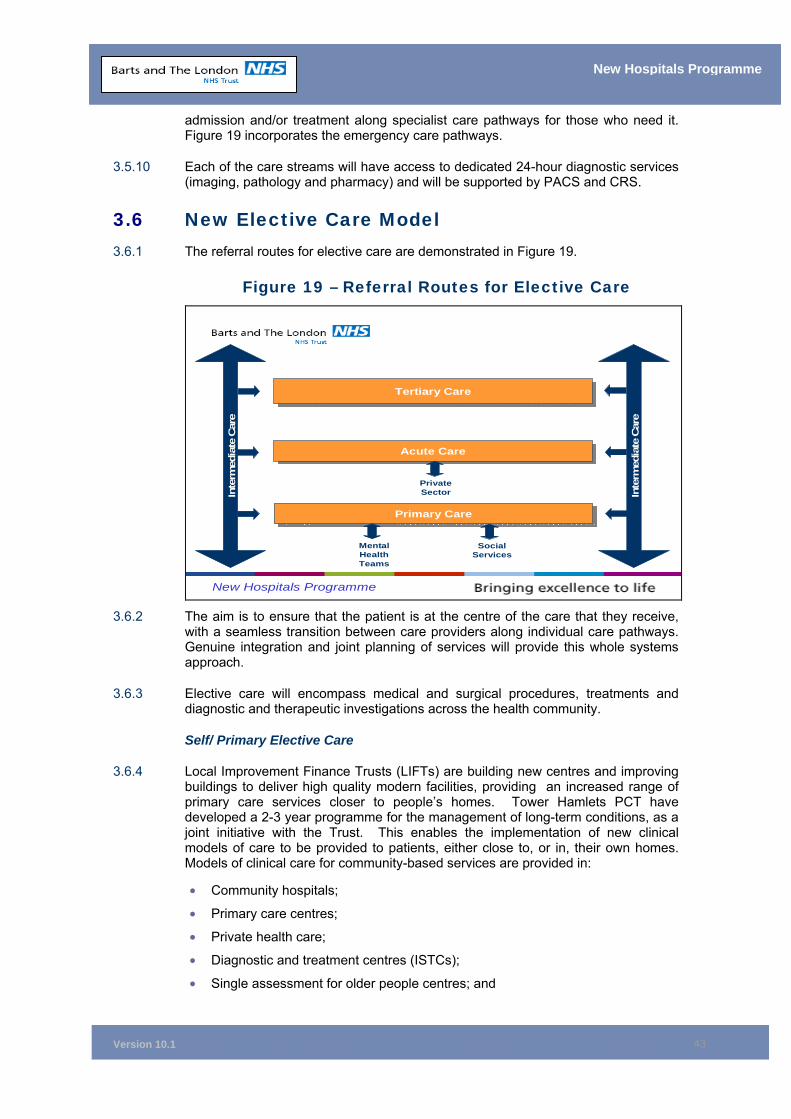
Version 10.1
43
New Hospitals Programme
admission and/or treatment along specialist care pathways for those who need it. Figure 19 incorporates the emergency care pathways.
3.5.10 Each of the care streams will have access to dedicated 24-hour diagnostic services (imaging, pathology and pharmacy) and will be supported by PACS and CRS.
3.6 New Elective Care Model 3.6.1 The referral routes for elective care are demonstrated in Figure 19.
Figure 19 – Referral Routes for Elective Care
New Hospitals Programme
Tertiary CareTertiary Care
Social Services
Mental Health Teams
Acute CareAcute Care
Inte
rmed
iate
Car
e
Inte
rmed
iate
Car
e
Primary CarePrimary Care
Private Sector
3.6.2 The aim is to ensure that the patient is at the centre of the care that they receive,
with a seamless transition between care providers along individual care pathways. Genuine integration and joint planning of services will provide this whole systems approach.
3.6.3 Elective care will encompass medical and surgical procedures, treatments and diagnostic and therapeutic investigations across the health community.
Self/ Primary Elective Care
3.6.4 Local Improvement Finance Trusts (LIFTs) are building new centres and improving buildings to deliver high quality modern facilities, providing an increased range of primary care services closer to people’s homes. Tower Hamlets PCT have developed a 2-3 year programme for the management of long-term conditions, as a joint initiative with the Trust. This enables the implementation of new clinical models of care to be provided to patients, either close to, or in, their own homes. Models of clinical care for community-based services are provided in:
• Community hospitals;
• Primary care centres;
• Private health care;
• Diagnostic and treatment centres (ISTCs);
• Single assessment for older people centres; and
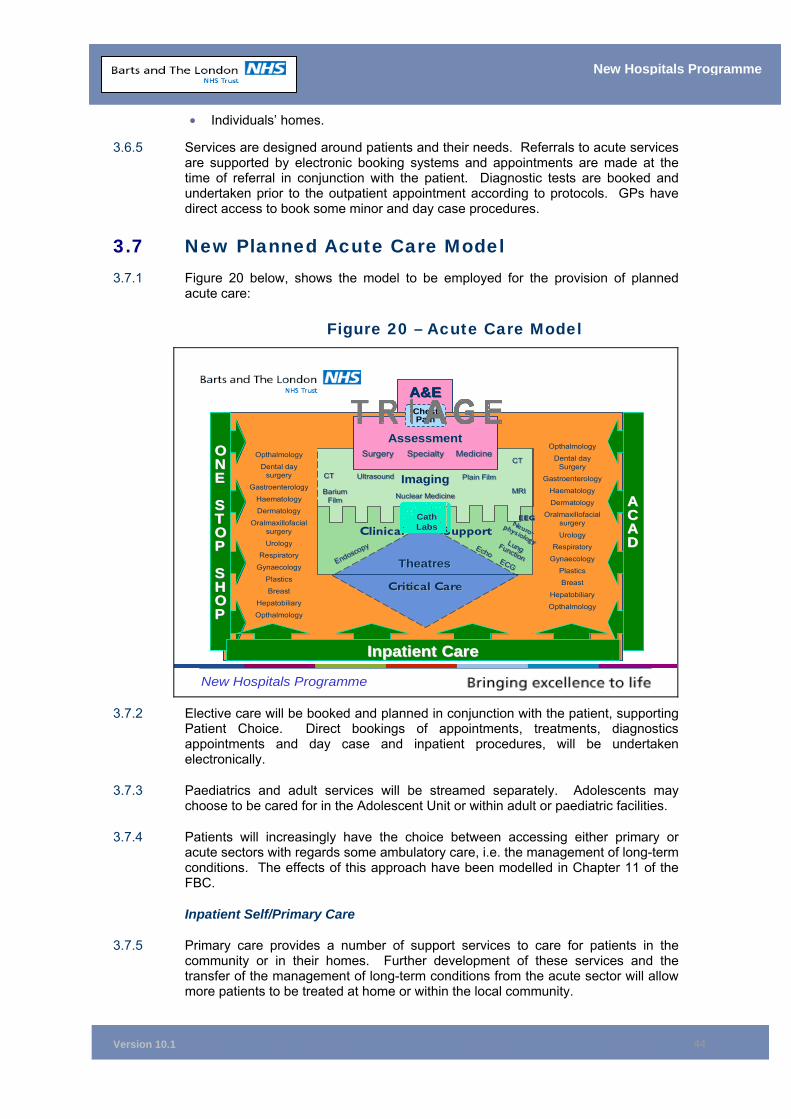
Version 10.1
44
New Hospitals Programme
• Individuals’ homes.
3.6.5 Services are designed around patients and their needs. Referrals to acute services are supported by electronic booking systems and appointments are made at the time of referral in conjunction with the patient. Diagnostic tests are booked and undertaken prior to the outpatient appointment according to protocols. GPs have direct access to book some minor and day case procedures.
3.7 New Planned Acute Care Model 3.7.1 Figure 20 below, shows the model to be employed for the provision of planned
acute care:
Figure 20 – Acute Care Model
New Hospitals Programme
A&EA&E
AssessmentAssessment
ImagingImaging
MedicineMedicineSpecialtySpecialtySurgerySurgery
Clinical SupportClinical Support
TheatresTheatres
Critical CareCritical Care
Opthalmology
Dental day Surgery
Gastroenterology
Haematology
DermatologyOralmaxillofacial
surgery
UrologyRespiratory
Gynaecology
PlasticsBreast
Hepatobiliary
Opthalmology
CTCT
MRIMRI
CTCT
EEGEEG
Lung Function
Lung FunctionEndoscopy
Endoscopy
Plain FilmPlain FilmUltrasoundUltrasound
Barium Film
Barium Film
Neuro-phys iology
Neuro-phys iology
EchoEcho
ECGECG
ONE
STOP
SHOP
OONNEE
SSTTOOPP
SSHHOOPP
CathCathLabsLabs
AACCAADD
Nuclear MedicineNuclear Medicine
Chest Pain
Opthalmology
Dental day surgery
Gastroenterology
HaematologyDermatology
Oralmaxillofacialsurgery
UrologyRespiratory
Gynaecology
PlasticsBreast
Hepatobiliary
Opthalmology
Inpatient CareInpatient Care
3.7.2 Elective care will be booked and planned in conjunction with the patient, supporting
Patient Choice. Direct bookings of appointments, treatments, diagnostics appointments and day case and inpatient procedures, will be undertaken electronically.
3.7.3 Paediatrics and adult services will be streamed separately. Adolescents may choose to be cared for in the Adolescent Unit or within adult or paediatric facilities.
3.7.4 Patients will increasingly have the choice between accessing either primary or acute sectors with regards some ambulatory care, i.e. the management of long-term conditions. The effects of this approach have been modelled in Chapter 11 of the FBC.
Inpatient Self/Primary Care
3.7.5 Primary care provides a number of support services to care for patients in the community or in their homes. Further development of these services and the transfer of the management of long-term conditions from the acute sector will allow more patients to be treated at home or within the local community.
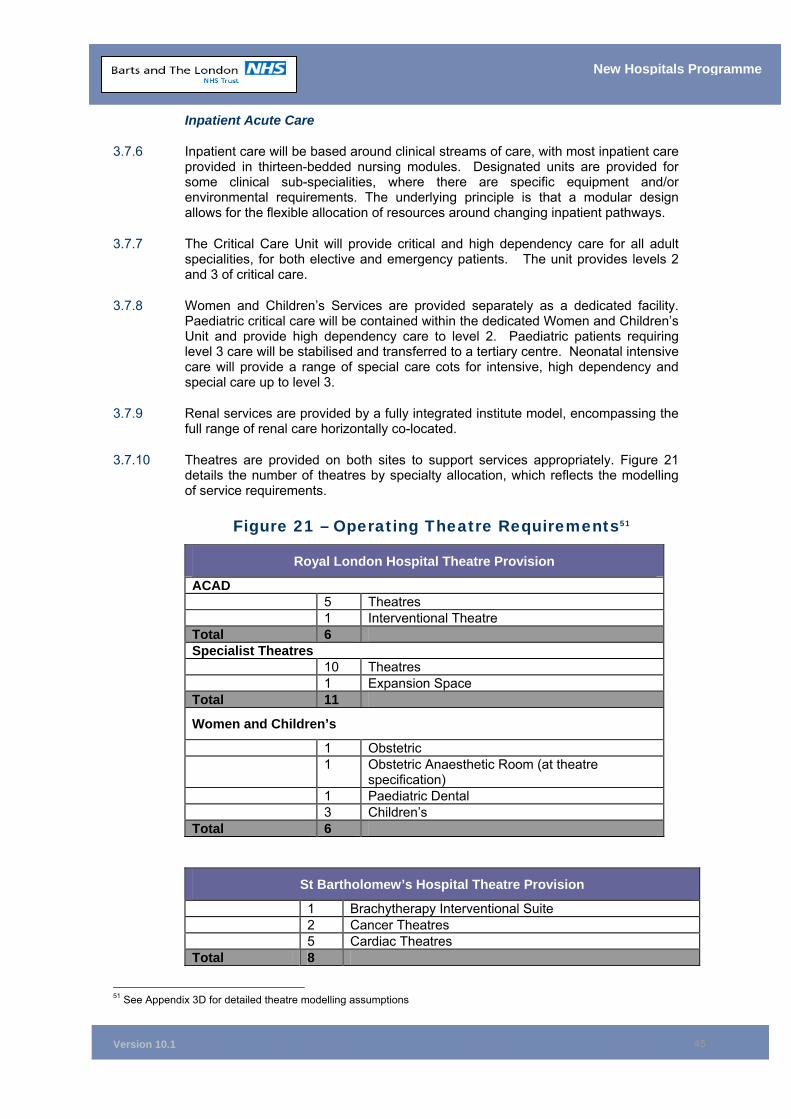
Version 10.1
45
New Hospitals Programme
Inpatient Acute Care
3.7.6 Inpatient care will be based around clinical streams of care, with most inpatient care provided in thirteen-bedded nursing modules. Designated units are provided for some clinical sub-specialities, where there are specific equipment and/or environmental requirements. The underlying principle is that a modular design allows for the flexible allocation of resources around changing inpatient pathways.
3.7.7 The Critical Care Unit will provide critical and high dependency care for all adult specialities, for both elective and emergency patients. The unit provides levels 2 and 3 of critical care.
3.7.8 Women and Children’s Services are provided separately as a dedicated facility. Paediatric critical care will be contained within the dedicated Women and Children’s Unit and provide high dependency care to level 2. Paediatric patients requiring level 3 care will be stabilised and transferred to a tertiary centre. Neonatal intensive care will provide a range of special care cots for intensive, high dependency and special care up to level 3.
3.7.9 Renal services are provided by a fully integrated institute model, encompassing the full range of renal care horizontally co-located.
3.7.10 Theatres are provided on both sites to support services appropriately. Figure 21 details the number of theatres by specialty allocation, which reflects the modelling of service requirements.
Figure 21 – Operating Theatre Requirements51
Royal London Hospital Theatre Provision
ACAD 5 Theatres 1 Interventional Theatre Total 6 Specialist Theatres 10 Theatres 1 Expansion Space Total 11
Women and Children’s
1 Obstetric 1 Obstetric Anaesthetic Room (at theatre
specification) 1 Paediatric Dental 3 Children’s Total 6
St Bartholomew’s Hospital Theatre Provision
1 Brachytherapy Interventional Suite 2 Cancer Theatres 5 Cardiac Theatres Total 8
51 See Appendix 3D for detailed theatre modelling assumptions
Version 10.1
46
New Hospitals Programme
Teaching and Education
3.7.11 The Trust is a teaching institution and works in conjunction with Barts and The London, Queen Mary’s School of Medicine and Dentistry and the City University St Bartholomew School of Nursing and Midwifery, in the provision of undergraduate and postgraduate education of healthcare professionals. The Trust has worked closely with the schools in the development of the new hospitals, to ensure that the teaching and educational needs of these professionals is integrated into the models of care and reflected in the design of the hospitals.
Research and Development
3.7.12 Research and Development (R&D) is an integral part of the delivery of healthcare, with around 1,000 research projects undertaken in the Trust at any one time. Currently these are undertaken in disparate locations which do not facilitate the co-ordination of teaching and research. Access to patients is difficult and is often undertaken at a location that is remote from treatment and the supporting clinical team.
3.7.13 The primary aims of the Trust’s R&D strategy are:
• To increase the expertise and reputation of the Trust as a centre of excellence in R&D, by ensuring that R&D is relevant, high quality and influences clinical practice;
• To maintain existing NHS R&D funding; and
• To maximise research income from non-NHS sources.
3.7.14 To achieve these strategic aims, there is a dedicated Clinical Research Centre (CRC) that is compliant with the Clinical Trials Directive 2001/20/EC, supporting the implementation of good clinical practice in the conduct of clinical trials. Work within the centre will be undertaken in line with Research Governance Framework, Health and Social Care DOH 2001.
3.7.15 The CRC consolidates all clinical research, maximising economies and providing a focus for expertise in research. It provides an integrated inpatient and outpatient centre for commercial and academic research, with a central facility (‘hub’) at The Royal London co-located with medical inpatients and a smaller unit (‘spoke’) at Barts.
3.8 The Clinical Facilities for the Models of Care Introduction
3.8.1 Services will be provided from the newly developed and refurbished Royal London Hospital in Whitechapel and St Bartholomew’s Hospital in The City of London. The Royal London is a major teaching general hospital and trauma centre and includes a major Dental Hospital, while the focus at Barts will be as a specialised cancer and cardiac centre.
3.8.2 The design of both hospitals has been developed around the new patient-centred models of care, putting the patient experience at the centre of care pathways and clinical co-locations. The new environment will fully support the delivery of the Trust’s clinical strategy and the provision of 21st century healthcare. Figure 22 shows the relationship between service models and the design concept for the new hospital at The Royal London.
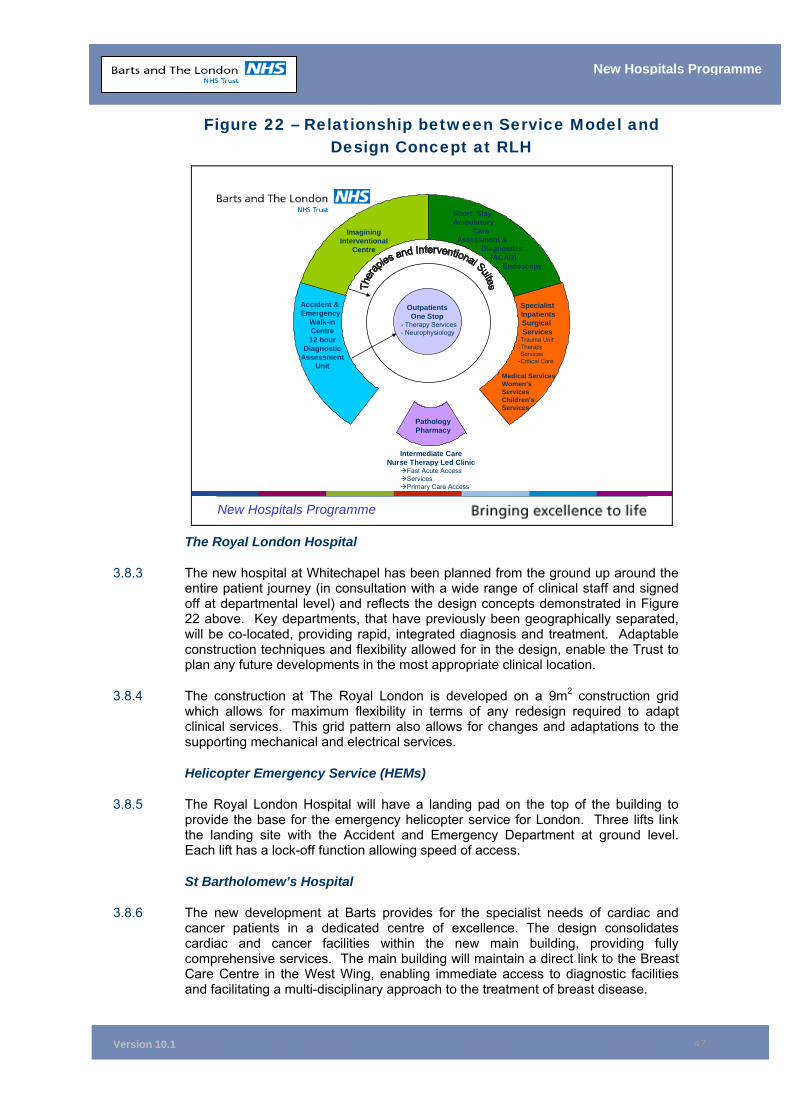
Version 10.1
47
New Hospitals Programme
Figure 22 – Relationship between Service Model and Design Concept at RLH
New Hospitals Programme
Intermediate CareNurse Therapy Led Clinic
Fast Acute AccessServicesPrimary Care Access
OutpatientsOne Stop
- Therapy Services- Neurophysiology
Accident & Emergency
Walk-in Centre12 hour
Diagnostic Assessment
Unit
Short StayAmbulatory
Care Assessment &
Diagnostics (ACAD)
Endoscopy
Specialist InpatientsSurgical Services
-Trauma Unit-Therapy Services
-Critical Care
Medical ServicesWomen’s Services Children’s Services
ImaginingInterventional
Centre
PathologyPharmacy
The Royal London Hospital
3.8.3 The new hospital at Whitechapel has been planned from the ground up around the entire patient journey (in consultation with a wide range of clinical staff and signed off at departmental level) and reflects the design concepts demonstrated in Figure 22 above. Key departments, that have previously been geographically separated, will be co-located, providing rapid, integrated diagnosis and treatment. Adaptable construction techniques and flexibility allowed for in the design, enable the Trust to plan any future developments in the most appropriate clinical location.
3.8.4 The construction at The Royal London is developed on a 9m2 construction grid which allows for maximum flexibility in terms of any redesign required to adapt clinical services. This grid pattern also allows for changes and adaptations to the supporting mechanical and electrical services.
Helicopter Emergency Service (HEMs)
3.8.5 The Royal London Hospital will have a landing pad on the top of the building to provide the base for the emergency helicopter service for London. Three lifts link the landing site with the Accident and Emergency Department at ground level. Each lift has a lock-off function allowing speed of access.
St Bartholomew’s Hospital
3.8.6 The new development at Barts provides for the specialist needs of cardiac and cancer patients in a dedicated centre of excellence. The design consolidates cardiac and cancer facilities within the new main building, providing fully comprehensive services. The main building will maintain a direct link to the Breast Care Centre in the West Wing, enabling immediate access to diagnostic facilities and facilitating a multi-disciplinary approach to the treatment of breast disease.
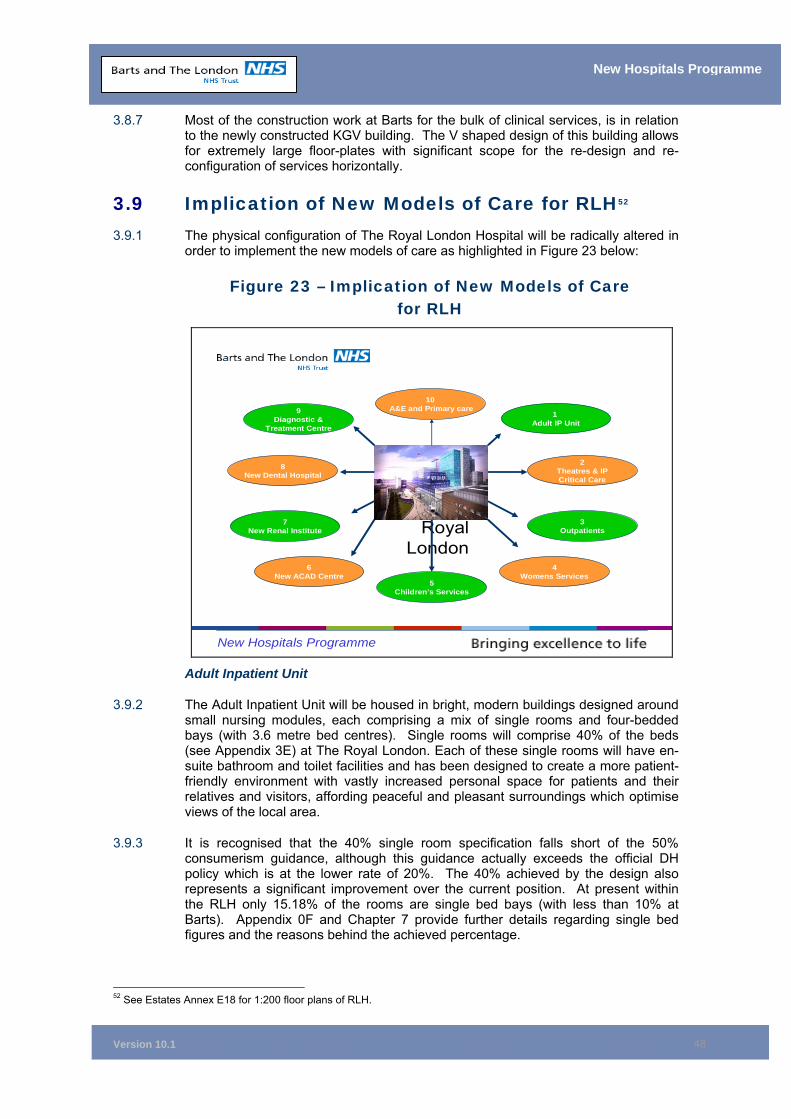
Version 10.1
48
New Hospitals Programme
3.8.7 Most of the construction work at Barts for the bulk of clinical services, is in relation to the newly constructed KGV building. The V shaped design of this building allows for extremely large floor-plates with significant scope for the re-design and re-configuration of services horizontally.
3.9 Implication of New Models of Care for RLH52 3.9.1 The physical configuration of The Royal London Hospital will be radically altered in
order to implement the new models of care as highlighted in Figure 23 below:
Figure 23 – Implication of New Models of Care for RLH
New Hospitals Programme
Royal London
9Diagnostic &
Treatment Centre
8New Dental Hospital
3Outpatients
7New Renal Institute
4Womens Services
1 Adult IP Unit
6New ACAD Centre
2Theatres & IP Critical Care
5Children’s Services
10A&E and Primary care
Adult Inpatient Unit
3.9.2 The Adult Inpatient Unit will be housed in bright, modern buildings designed around small nursing modules, each comprising a mix of single rooms and four-bedded bays (with 3.6 metre bed centres). Single rooms will comprise 40% of the beds (see Appendix 3E) at The Royal London. Each of these single rooms will have en-suite bathroom and toilet facilities and has been designed to create a more patient-friendly environment with vastly increased personal space for patients and their relatives and visitors, affording peaceful and pleasant surroundings which optimise views of the local area.
3.9.3 It is recognised that the 40% single room specification falls short of the 50% consumerism guidance, although this guidance actually exceeds the official DH policy which is at the lower rate of 20%. The 40% achieved by the design also represents a significant improvement over the current position. At present within the RLH only 15.18% of the rooms are single bed bays (with less than 10% at Barts). Appendix 0F and Chapter 7 provide further details regarding single bed figures and the reasons behind the achieved percentage.
52 See Estates Annex E18 for 1:200 floor plans of RLH.
Version 10.1
49
New Hospitals Programme
3.9.4 Chapter 7 and Appendix 0F also expand on the ways in which flexibility has been built into the scheme to accommodate future changes to models of care. In summary, the 9m2 construction grid in the proposed design solution allows for flexibility to re-configure services, as it makes it easier to re-plan internal areas. For example, this allows four-bedded bays within the generic inpatient modules to be converted very easily into two single rooms. However, if the changing model of care could not be accommodated due to the resultant loss in capacity, embedded and co-located non-clinical space and open-plan office accommodation could alternatively be converted to inpatient accommodation.
3.9.5 Notwithstanding the improvements in the patient environment, the inpatient area will incorporate the latest in clinical design, maximising staff visualisation and access to patients and is specifically designed to reduce cross-infection and contracting of iatrogenic diseases (infections caused by, or with origins in, the hospital environment). Appendix 0F provides further information regarding infection control. The key points are detailed below:
Patients will be cared for in the appropriate setting for their needs. The design of the new hospitals’ facilities allows “best practice” to be followed including ’cleanability“ and ease of maintenance.
The design of each pod ensures that the distance between beds supports current guidelines for control of infection. At the entrance to each single room and four-bedded bay there are apron and glove dispensers in addition to alcohol hand gel dispensers. There are clinical hand wash facilities available in all rooms, with a minimum of a 1:4 hand wash to bed ratio, increasing to 1:1 in critical care areas. The number of single rooms has been increased to ensure that patients can be easily isolated on each ward to prevent cross-infection.
For patients with more serious infections there is a ten-bedded isolation ward with lobbied single negative pressure rooms. Negative pressure facilities are also available within the renal inpatient service for inpatient haemodialysis patients who have tuberculosis. There is also a 10 cubicle area within haemodialysis, to isolate those patients with blood borne virus infections from other dialysis patients, in addition to 4 single rooms for isolation.
3.9.6 A dedicated Coronary Care Unit, adjacent to its own catheter laboratory and cardiac non-invasive testing unit, will offer cardiac patients the high level of monitoring and access to key diagnostic tests that they require.
3.9.7 Acutely ill elderly patients, currently cared for at Mile End Hospital, will be managed and integrated with the acute general and emergency service at The Royal London. An integrated acute elderly and general emergency medical service will offer on-site access to high technology diagnostic tests and dedicated therapy services within an acute hospital environment. This re-location will allow the PCT to further develop primary care facilities at Mile End Hospital.
IP Theatres & Critical Care
3.9.8 Inpatient theatres and critical care will be brought together in one place for the first time, allowing rapid access for patients and ensuring close monitoring of critical patients by anaesthetic staff.
3.9.9 The new theatre complex will comprise:
Version 10.1
50
New Hospitals Programme
• A suite of 10 operating theatres (with spatial capacity for expansion to 11) and capable of being equipped with specialised MRI and CT scanners and angiography equipment;
• A receiving area with bays for 15 beds; and
• A recovery area with bays for 15 beds.
3.9.10 The Critical Care Unit will be expanded from its current 25 beds (17 level 3 ITU and 8 level 2 HDU) to a 44 bed unit divided into four 11-bed modules for patients requiring level 2 and level 3 care. All of these beds will have capacity to care for patients requiring level 3 care. The care can be downgraded to level 2 according to clinical need without having to move the patient to another ward.
3.9.11 The current 25-bed Critical Care Unit at The Royal Hospital has an occupancy level in excess of 95%. In addition, in 2004/05 over 50 patients were transferred to other hospitals due to shortage of capacity at The Royal London. The Trust is currently examining capital options for increasing capacity in ITU by 4 beds over the interim period, until Phase 1 of RLH is completed. Any costs would be met by the Trust’s 2006/7 capital programme, assuming a move from SHA strategic capital to an FT capital regime. This interim additional provision is required urgently to reduce the need to transfer critically ill patients. The impact on the Trust’s I&E position is covered in Appendix 11D. Additional costs will be met from additional activity receipts, which have been modelled in this Appendix. The 44 critical care beds in the new build account for all level 3 and level 2 (HDU) beds which are co-located in the new scheme to afford maximum flexibility. The increase in critical care capacity at The Royal London is required for two reasons;
• The growth in population means a 25% increase in admitted patient care. Due to the predicted impact of the independent sector, more complex casemix patients will be admitted in the future (circa 10 beds).
• The critical care bed total also allows for the fact that the sector is under-provided for in terms of critical care. This means that, on occasions, patients are either stepped down from intensive care earlier than would be clinically optimal, or are required to be transferred to other critical care centres. Both of these points are evidenced by the high occupancy rates in ITU, high levels of transfer to other critical care facilities and the comparatively low ITU bed totals when BLT is compared with other teaching hospitals. All of these issues are understood and are noted at the North East London Critical Care Board and together equate to the need for more capacity (circa 9 beds).
Outpatients
3.9.12 The majority of specialist outpatient facilities, at present located in many different buildings (many of which are remote from the main part of the hospital) will be brought together in the main body of the hospital, co-located with diagnostic departments so as to offer a one-stop outpatient and diagnostic facility. The design will create efficiency and a more pleasant experience for the patient. Natural zoning for treatments will be developed which will maximise patient privacy and dignity and will engender a safe, pleasant environment that will improve recruitment and maximise retention of staff. Clinics being provided in the New Build include:
■ A large Dermatology Unit with dedicated wound care clinic;
■ A Fracture Clinic adjacent to an Outpatient Imaging and Bone Mineral Density Scanning Unit;
■ A Diabetes Centre, with a one-stop service for routine diabetes care;
Version 10.1
51
New Hospitals Programme
■ A specialised, discrete GUM, HIV & Immunology Unit offering high standards of patient privacy and dignity;
■ An Ophthalmology Unit which consolidates services on one site and will enhance the patient journey. This will be located on the ground floor, making it easily accessible for visually impaired patients; and
■ A Neurophysiology department housed in a dedicated modern facility, suitable for high technology equipment.
Women's Services
3.9.13 Women & Children’s services, presently scattered throughout the hospital, will be brought together into one combined unit, with its own entrance and dedicated space, offering an appropriate environment catering for the needs of these patient groups.
3.9.14 Co-locations have been carefully planned so as to minimise patients’ journey times. The obstetric theatre will be located close to the neonatal department to offer rapid access and postnatal wards will be located close by, so that mothers can be close to newborn infants who require specialist care. At present, these functions are located in separate buildings, which means that mothers have to wait until they are sufficiently recovered from surgery before being taken out of the main building and across a courtyard to visit their newborn baby.
3.9.15 The birth rate in Tower Hamlets is increasing annually. The present labour ward was designed for a much lower birth rate, and ward offices and other staff space have had to be used to cater for the larger turnover of patients. There is nowhere for families to wait or get refreshments while female relatives are in labour. The new build will have the capability to meet demand in Tower Hamlets and to expand to meet potential increases in demand through the flexibility of the grid pattern (see section 3.8.4 above). It will also provide separately defined and managed areas for terminations/miscarriages/assisted conception to birthing/post-natal areas.
3.9.16 The development of an Emergency Gynaecology Unit (EGU) will bring a vast improvement to Tower Hamlets services. The EGU will be much more accessible to women, allowing them to be diagnosed and treated quickly.
Women’s: Key Facilities • A 30-bed dedicated Labour Delivery Respite Post-partum (LDRP) Unit,
providing expectant mothers with a modern facility specifically designed to meet their needs during delivery
• A 31-bed ante/post-natal ward
• A 10-bed Gynaecology Unit and Early Pregnancy Advisory Unit
• A dedicated Women's outpatient service, including Gynaecology Outpatients, Antenatal Outpatients and Maternal and Foetal Assessment and Ultrasound
• A dedicated obstetric operating theatre suite
• A four-bed recovery area including two high dependency beds.
Children’s Services
3.9.17 Children’s services will be housed in a specially designed environment which is child-orientated and offers dedicated facilities for diagnosis and treatment. All
Version 10.1
52
New Hospitals Programme
children’s services will be easily reached from a central point, making access for everyone, especially for non-English speaking patients and parents, much easier through significantly improved wayfinding.
ACAD Centre
3.9.18 A new “Ambulatory Care“ unit will offer significantly increased capacity for day and short stay surgery. Located in a dedicated part of the hospital, with rapid access to all support services, the unit will have 6 theatres. One of these will be a dedicated ophthalmic and dental theatre and another will be equipped with pre-operative imaging equipment, allowing complex, minimally invasive, interventional treatments. Patients will recover in a specially designed recovery ward area with 47 beds and 30 chairs, for stays of up to 36 hours.
3.9.19 Co-located with the theatre complex will be an endoscopy suite with 5 procedure rooms and a separate recovery area, along with a Haematology Day Unit with four beds, six chairs and a cell separator unit.
Renal Unit
3.9.20 Renal services will be brought together on one site within a dedicated “renal institute“ with its own entrance. This represents a major improvement on the current split-site system with renal services at both The Royal London and Barts presenting clinical issues and resulting in a waste of resources. The unit will offer emergency access from the A&E Department, together with dedicated outpatient clinics and a CAPD patient training centre, which offers enhanced privacy and dignity for patients, for self management of their dialysis.
3.9.21 The Institute will provide a single point of access to all renal services and create a patient-centred service with enhanced patient flow, through therapy changes and timely surgical access provision, that can be easily monitored and maintained to achieve maximum longevity. Dialysis services will be centralised and enlarged from 66 to 88 stations, enabling an expanded service to be designed around individual needs and preferences.
3.9.22 These developments will enable the Trust to meet the requirements of the National Service Framework for renal services.
Dental Hospital
3.9.23 It is intended as part of Phase Two of the Project that The Dental Hospital will be housed within a new, specially designed unit with its own entrance and identity. The unit will offer a more logical patient journey and enhanced standards of privacy & dignity for patients. Routine and emergency dental treatments will be provided to
Children’s: Key Facilities A dedicated paediatric operating theatre suite comprising of: • Two inpatient theatres
• One daycase theatre and 25 beds for daycase recovery
• One dental theatre and Daycase Unit
• 75 beds, including a specially designed Adolescent Unit
• A larger Neonatal Unit with potential for further expansion of 10 additional cots
• An 10-bed High Dependency Unit
Version 10.1
53
New Hospitals Programme
both adults and children from the local community and beyond. It will achieve this by bringing several disparate clinics, distributed on separate floors of the Dental Institute, together in a multi-bay generic clinic environment, offering increased flexibility for clinical and teaching use.
Diagnostic & Treatment Centre (DTC)
3.9.24 Diagnostic and treatment services are at present scattered across the site (5 departments at Barts, 3 at The Royal London and 2 at The London Chest), making patient access difficult and hampering the ability of the Trust to offer an integrated service. Rapidly developing technology and increasing use of these services by all patient groups, has made the provision of an integrated diagnostic and treatment centre a key and essential asset for any modern hospital. Accordingly, a whole floor of the new development at the Royal London will be concentrating on serving patients” needs with regard to diagnostic tests and treatments that are best undertaken with imaging guidance. The centre will have extensive facilities for clinico-radiological conferences and case meetings, which will support the further development of multi-disciplinary patient care.
DTC: Key Facilities The new centre offers the following services as a one stop facility: Diagnostic Services • Plain film imaging via direct digital imaging • Ultrasound • Computerised tomography scanning • Magnetic resonance scanning • Fluoroscopy and minor specialised procedures • Angiography Interventional (Treatment) • Biopsies (under CT, MRI, Fluoroscopic and Ultrasound control) • Line insertions • Dilatations • Angioplasty
Accident & Emergency and Primary Care
3.9.25 The Accident & Emergency Unit at The Royal London Hospital is one of the busiest units in the UK and is a major level one trauma centre for the London M25 area. The residents of Tower Hamlets and surrounding boroughs thus have access to one of the UK’s best Accident & Emergency Units, offering rapid diagnosis and treatment for major trauma, minor injury and acute medical and surgical conditions.
3.9.26 Whilst the existing unit has been upgraded and expanded over recent years, it remains cramped, with recent increases in demand for A&E services at The Royal London Hospital placing additional strain on the system.
3.9.27 The new development on The Royal London site offers the opportunity to expand the capacity of both the adult and children’s A&E units and to integrate them with other primary care services, including the Emergency Dental Service, the Tower
Version 10.1
54
New Hospitals Programme
Hamlets Walk-In Centre and the Tower Hamlets Emergency Doctor Service. For the first time, local residents will have access to all of these services in an integrated unit in a single building. This will enable clinicians to ’stream’ all patients to the most appropriate A&E service, e.g. to local pharmacists, their general practitioner or to discharge them home.
3.9.28 The new A&E department is designed to optimise patient flows and to enable staff to deliver the most effective, efficient service. The design work has been informed by the consultancy firm McKinsey, with Strategic Health Authority endorsement and funding.
3.9.29 A number of key McKinsey recommendations have already been implemented in advance of the new build, including:
■ ’Streaming” (as described above)
■ New internal processes
■ Staff establishment
■ Skill mix review
■ A move to geographically located teams, responsible for managing a cohort of patients in their designated area
3.9.30 The impact of ’streaming“ has placed additional pressure on the Walk-in Centre (WIC). It is acknowledged that the current design does not provide sufficient capacity. However, it will be possible to provide the WIC with a larger footprint/4 additional consulting rooms with minimal re-design of the minors/majors area immediately adjacent to the WIC.
3.9.31 McKinsey have also worked with A&E clinicians and acute physicians to refine the proposal for a short stay facility for patients who require further investigation or a short period of treatment, but who will not require admission. “Streaming“ these patients to an appropriate clinical setting will avoid unnecessary admission. A Clinical Decision Unit (CDU) is to be established in the existing A&E department. This will be replaced by an Adult Diagnostic Unit in the new build, also co-located with A&E.
3.9.32 McKinsey have proposed that a more “open“ flexible space should be incorporated into the design, to be utilised in the event of a major incident. This proposal should not require fundamental re-design and the solution will be flexible design of cubicles allocated in the major area.
A&E: Key Facilities
• Two ’streaming’ cubicles at the front door.
• Seven initial treatment cubicles, including one equipped for ophthalmology.
• An Adult Decision Unit (ADU) - 14 beds, eight couches and one consultation room with a maximum length of stay of 12 hours, for patients who do not require full admission.
• Minors bays - 14 flexible-use spaces, of which eight will be trolley bays, one designated ENT/Ophthalmology, one will accommodate a dental chair

Version 10.1
55
New Hospitals Programme
and four will have reclining couches for suturing and other minor treatments
• One minor procedure room for intermediate suturing / treatment. This room will provide standard medical gases and suction, but no anaesthesia.
• Majors – 20 flexible space areas. All will have cardiac and non-invasive monitoring equipment. Emphasis on timely transfer to an appropriate bed should full admission or intervention be required.
• Resus – three medical, three polytrauma and two paediatric. Medical patients will be isolated from polytrauma to minimise distress. Adult resus can be accessed from paediatric A&E so that children with polytrauma can be easily transferred.
• Decontamination area at the entrance with negative pressure and hepafiltration to avoid contamination within the main department.
• Mental health room with en-suite facilities
• Security will be given a high priority, with modern seating systems provided to protect staff and patients
• All facilities will incorporate patient-focussed design, with improved auditory and visual privacy and integrated interior designs to create pleasant surroundings with privacy and dignity being of the highest priority
• Separate children's facilities with inbuilt children's observation suite
• Opportunity to develop sophisticated patient pathways supported by design
3.10 Implication of New Models of Care for SBH53
Figure 24 – Implication of New Models of Care for SBH
New Hospitals Programme
St Barts
3Respiratory Medicine
7Minor Injuries unit
4Endocrinology
1New Cardiac Centre
6Diagnostic &
Treatment Centre
2New Cancer
Centre
5Outpatients
New Cardiac Centre
3.10.1 Incorporating the specialities of cardiac surgery, thoracic surgery and tertiary cardiology in new accommodation, the Cardiac Centre will be consolidated on one site, enabling the largest cardiac service in the UK to deliver clinical excellence to the population it serves.
53 See Estates Annex E18 for 1:200 floor plans of Barts
Version 10.1
56
New Hospitals Programme
3.10.2 A dedicated cardiology floor co-locates the Coronary Care Unit, catheterisation laboratories, Cardiac Non-Invasive Unit, an outpatient suite and inpatient wards.
3.10.3 The inpatient wards comprise a mix of single rooms (40.9% at Barts54) together with four-bedded rooms, all with en-suite bathroom and toilet facilities. The wards have been designed to create a more patient-friendly environment, with vastly increased personal space for patients, their relatives and their visitors, peaceful, pleasant surroundings and optimised views of the local area.
3.10.4 Notwithstanding the improvements in patient environment, the inpatient area will also incorporate the latest in clinical design, maximising staff visualisation and access to patients and have been specifically designed to reduce cross-infection and the contracting of iatrogenic diseases.
3.10.5 Cardiac inpatient theatres and critical care will be brought together in one place for the first time, allowing rapid access for patients and ensuring close monitoring of critical patients by anaesthetic staff.
3.10.6 The new theatre complex will comprise:
• A suite of eight operating theatres, with five dedicated for cardiac surgery, capable of being equipped with specialised MRI and CT scanners and angiography equipment;
• A receiving area with bays for six beds; and
• A recovery area with bays for eight beds.
3.10.7 Cardiac surgery patients will go direct to the Cardiac Intensive Recovery Unit (CIRU) on the same floor, which has 16 beds. These recovery spaces will also be used by patients from the three cancer theatres.
3.10.8 A unit of 15 cardiothoracic HDU beds will provide the next step in patient recovery from surgery. The 9-bed intensive care unit is provided on this floor, enabling swift access to theatres and associated support.
New Cancer Centre
3.10.9 The multi-tier and multi-disciplinary approach to the care of cancer patients requires the provision of a sophisticated centre, with genuinely comprehensive services. The design for Barts delivers a repository of both expertise and specialist facilities needed for the care of patients with cancer.
3.10.10 The design of the building has been developed to be sympathetic to the client group, taking into account the feelings of both patients and relatives in such an environment, particularly in the event of news of a positive diagnosis. Practical efficiency has been combined with an appropriately sensitive and patient-focused approach. Some key features are:
• At lower ground level, in part of the large atrium space, is the radiotherapy department. This department is easily accessed and integrates itself with all other support services;
• The cancer information centre is situated on the ground floor and provides information and support for patients and visitors. It is strategically positioned to encourage the public to seek advice and help;
54 Note: This figure represents single rooms as a % of all inpatient beds excluding beds in Critical Care Areas
Version 10.1
57
New Hospitals Programme
• At level 1, the three cancer theatres are situated in a suite of eight theatres, sharing support facilities with cardiac services. A dedicated theatre for brachytherapy treatments is provided, with discreet outpatient access; and
• The inpatient wards are co-located at levels 4 and 5. They comprise a mix of single rooms together with two-bed and four-bed rooms. Each of these rooms will have en-suite bathroom and toilet facilities and have been designed to create a more patient friendly environment, with vastly increased personal space for patients, relatives and visitors.
3.10.11 Each ward area has been designed to meet its specialist needs. The design includes a bone marrow transplant unit and radioisotope treatment rooms. Specialist surgery for breast, endocrine and gynae-oncology is provided in dedicated ward areas.
Respiratory Medicine
3.10.12 The London Chest Hospital opened in 1855 and became world renowned for the treatment of diseases of the heart and lung. The new design provides 21st century facilities to deliver respiratory medicine.
3.10.13 The respiratory service is consolidated on level 4 at Barts, maintaining close links with the cardiac centre. It provides specialist inpatient facilities, including a sleep study centre and cystic fibrosis unit, designed to facilitate a self-referral service in a design that meets the needs of this client group.
3.10.14 The bronchoscopy and lung function laboratories are situated on the same level and, with the incorporation of the consultant offices, this maximises the approach to delivering patient-centred care.
Endocrinology
3.10.15 The endocrinology department is the largest provider of clinical endocrinology services in the UK and one of only three departments offering complex endocrinology services. The original design combined inpatient accommodation with an outpatient investigation unit, bridged by specialist laboratory services. The co-location of the academic arm provided teaching and research on all endocrine diseases and neoplasms referred to and treated at Barts, underpinning the delivery of clinical care. However, as a result of descope, the facilities will be provided in the Trust’s retained estate at Barts as complex endocrinology is closely clinically associated with cancer services and the two areas share many support services.
Outpatients
3.10.16 Outpatient facilities are located in a number of different buildings at present, many of which are remote from the main part of the hospital. These will be brought together in the main body of the hospital and will be co-located with diagnostic departments to offer a “one-stop” outpatient and diagnostic facility. The design will create a logical flow for patients and create a more pleasant experience. It will create natural zoning for treatments that maximise patient privacy and dignity and will create a safe, pleasant environment that will improve recruitment and maximise retention of staff. Both generic clinic modules and specialised dedicated clinic areas will be provided, and these include:
• A gynae-oncology outpatient service with integrated colposcopy suite;
• A cardiac OPD suite co-located with the Non-Invasive Diagnostic Unit; and
• An advanced lung function laboratory.
Version 10.1
58
New Hospitals Programme
Minor Injuries Unit
3.10.17 The Minor Injuries Unit provides a service to the local population around Barts. The new design delivers purpose-built accommodation at the ground floor level of the new build, with immediate access to imaging and diagnostic facilities. The new design delivers 21st century accommodation to enable the unit to respond to changes in the transient population that enter The City each day. The new unit is easily accessible with a dedicated waiting area and accommodation that has been designed to enable the delivery of a full range of minor injury services.
3.11 Chapter Conclusion 3.11.1 New facilities at Barts and The London are planned on the basis of modern models
of care. The combination of these new models and modern facilities will transform the patient experience, improve clinical outcomes and deliver greater efficiency.
3.12 Chapter Appendices 3A Pathfinder Clinical Strategy 2004/09 3B Assumptions and Data to Support Number of Beds 3C Clinical Groups by Specialty 3D Theatre Modelling Assumptions 3E Bed Allocation SBH and RLH
Version 10.1
59
New Hospitals Programme
4 REVIEW OF THE OUTLINE BUSINESS CASE
4.1 Introduction Synopsis – Review of the Outline Business Case (OBC)
This chapter provides:
Confirmation that the recommendations in the OBC for the development of an acute hospital on The Royal London (RLH) site, the development of a specialist cardiac and cancer centre on the St Bartholomew’s (Barts) site and the closure of The London Chest Hospital (LCH) remains robust.
Details of the changes to the bed numbers from OBC to FBC as a result of:
■ The review of the Clinical Development Plan (CDP), which resulted in an increase in overall beds by 76 to 1,248 (905 at RLH and 343 at Barts).
■ The recent repatriation of 37 cardiac beds to the Basildon Cardiac Centre in Essex which is due to open in 2007/08 (the impact of this is reflected in the above bed numbers at Barts).
■ The Descoping of the scheme required by DH (notably the mothballing of 250 beds within the 1,248 beds previously planned by the PFI)
Details of the changes to the Capital costs of the scheme since OBC approval..
4.2 Summary of the Outline Business Case Introduction
4.2.1 The previous chapters have set out clearly the need for the new development at Barts and The London. This chapter revisits the initial OBC option appraisal in the light of subsequent local and national developments since the OBC was approved in February 2000. Project objectives, non-financial benefits and recommended changes to the original OBC are reviewed to ascertain if they remain valid.
Overall Project Objectives
4.2.2 The redevelopment of Barts and The London has been, and remains, a key element in the Government’s wider plans for modernising the NHS in East London and the agenda for improving cancer and cardiac services nationwide. The aim of the redevelopment is to provide 21st century hospitals that will meet the specific needs of the people of East London, as well as to provide a range of specialist services for patients beyond the local population. Within the context of the size of the development, the overall intention of achieving these aims as set out in the objectives of the OBC, have not altered. The Trust is addressing the Department of Health’s 10 High Impact Changes as part of its existing financial planning in order to break even within the Trust’s current general efficiency programme. These High Impact Changes are therefore not explicitly modelled in entirety within the activity and efficiency modelling for the New Hospital Project.
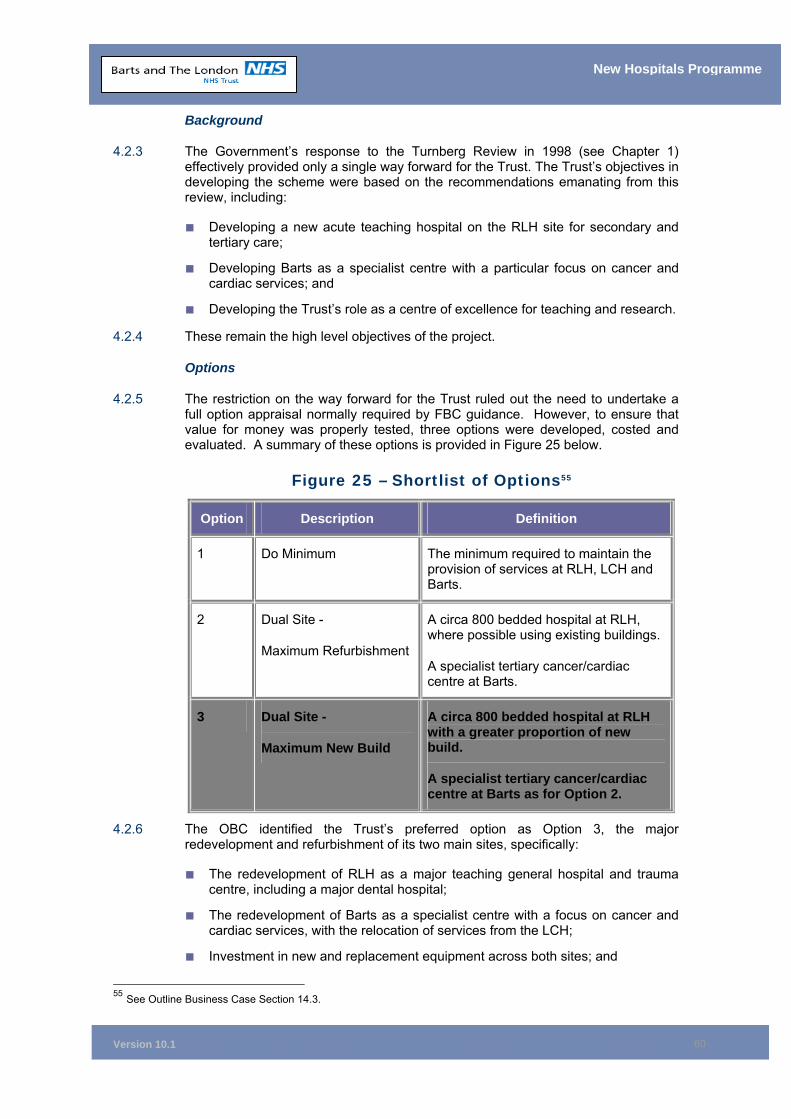
Version 10.1
60
New Hospitals Programme
Background
4.2.3 The Government’s response to the Turnberg Review in 1998 (see Chapter 1) effectively provided only a single way forward for the Trust. The Trust’s objectives in developing the scheme were based on the recommendations emanating from this review, including:
■ Developing a new acute teaching hospital on the RLH site for secondary and tertiary care;
■ Developing Barts as a specialist centre with a particular focus on cancer and cardiac services; and
■ Developing the Trust’s role as a centre of excellence for teaching and research.
4.2.4 These remain the high level objectives of the project.
Options
4.2.5 The restriction on the way forward for the Trust ruled out the need to undertake a full option appraisal normally required by FBC guidance. However, to ensure that value for money was properly tested, three options were developed, costed and evaluated. A summary of these options is provided in Figure 25 below.
Figure 25 – Shortlist of Options55
Option Description Definition
1 Do Minimum The minimum required to maintain the provision of services at RLH, LCH and Barts.
2 Dual Site -
Maximum Refurbishment
A circa 800 bedded hospital at RLH, where possible using existing buildings.
A specialist tertiary cancer/cardiac centre at Barts.
3 Dual Site -
Maximum New Build
A circa 800 bedded hospital at RLH with a greater proportion of new build.
A specialist tertiary cancer/cardiac centre at Barts as for Option 2.
4.2.6 The OBC identified the Trust’s preferred option as Option 3, the major redevelopment and refurbishment of its two main sites, specifically:
■ The redevelopment of RLH as a major teaching general hospital and trauma centre, including a major dental hospital;
■ The redevelopment of Barts as a specialist centre with a focus on cancer and cardiac services, with the relocation of services from the LCH;
■ Investment in new and replacement equipment across both sites; and
55 See Outline Business Case Section 14.3.

Version 10.1
61
New Hospitals Programme
■ Investment in information management and technology across both sites through separate, publicly-funded procurement.
4.2.7 This option, which received the approval of the NHS Executive London Region in 2000, has been regularly reviewed. Activity assumptions have been remodelled as and when necessary and the impact of health policy changes and other issues have been taken into account as they arise. Although some changes have been made in the content of the scheme, due to the work undertaken to remodel the clinical requirements based on evolving models of care and a refreshed view of the Trust’s activities, the strategic case for Option 3 remains unchanged and robust.
4.2.8 The reasons cited in the OBC for the selection of Option 3 (the dual site option) continue to stand in the FBC. In fact, the grounds for the selection of this option have been strengthened by the advent of the proposed Thames Gateway development. The Trust, therefore, has not fully re-appraised the options which were evaluated in the OBC in the FBC. The reasons for this ultimately fall to the increased bed requirement which flows from the Thames Gateway development. Option 1 (Do Minimum) is even less fit for purpose, as increased beds are now required (this is in addition to all the factors cited against this option in the OBC). The need for more beds in the scheme leads, within Options 1 and 2, to a less economic case and gives less scope for the clinical redesign work which the Trust originally proposed and continues to propose as a necessary condition to enhance and improve the delivery of its services.
4.3 Review of OBC Introduction
4.3.1 In its approval of the OBC in February 2000, the NHS Executive recommended a number of significant changes to the scheme56. The main recommendations were that the Trust review the basis for its activity assumptions in the OBC and include additional beds for cardiac and acute elderly services.
4.3.2 The Trust’s response was to undertake a full-scale review of its requirements and, in conjunction with the East London and The City Health Authority (ELCHA), GPs and the Trust’s clinical staff, the Trust revised its assumptions for clinical requirements. Figure 26 details the recommendations and conditions attached to OBC approval and how they have been addressed by the Trust.
56 See Appendix 4E or Estates Annex E5 for copies of NHS approvals letters.
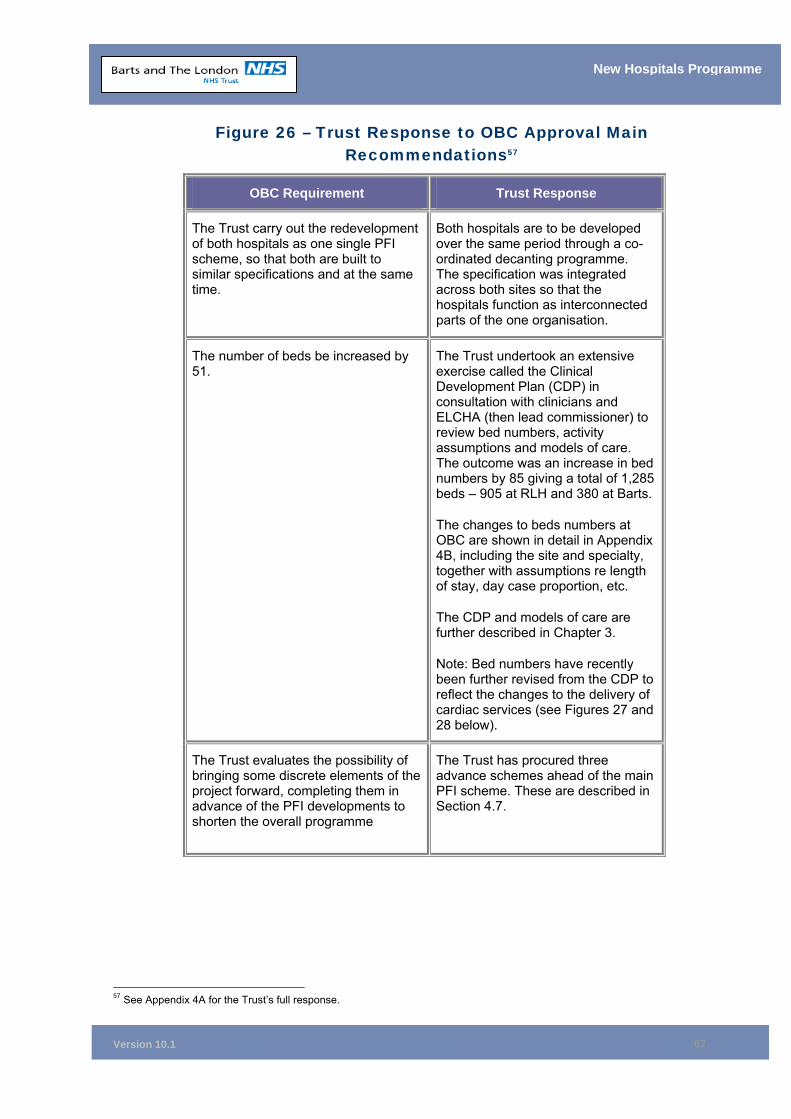
Version 10.1
62
New Hospitals Programme
Figure 26 – Trust Response to OBC Approval Main Recommendations57
OBC Requirement Trust Response
The Trust carry out the redevelopment of both hospitals as one single PFI scheme, so that both are built to similar specifications and at the same time.
Both hospitals are to be developed over the same period through a co-ordinated decanting programme. The specification was integrated across both sites so that the hospitals function as interconnected parts of the one organisation.
The number of beds be increased by 51.
The Trust undertook an extensive exercise called the Clinical Development Plan (CDP) in consultation with clinicians and ELCHA (then lead commissioner) to review bed numbers, activity assumptions and models of care. The outcome was an increase in bed numbers by 85 giving a total of 1,285 beds – 905 at RLH and 380 at Barts.
The changes to beds numbers at OBC are shown in detail in Appendix 4B, including the site and specialty, together with assumptions re length of stay, day case proportion, etc.
The CDP and models of care are further described in Chapter 3.
Note: Bed numbers have recently been further revised from the CDP to reflect the changes to the delivery of cardiac services (see Figures 27 and 28 below).
The Trust evaluates the possibility of bringing some discrete elements of the project forward, completing them in advance of the PFI developments to shorten the overall programme
The Trust has procured three advance schemes ahead of the main PFI scheme. These are described in Section 4.7.
57 See Appendix 4A for the Trust’s full response.
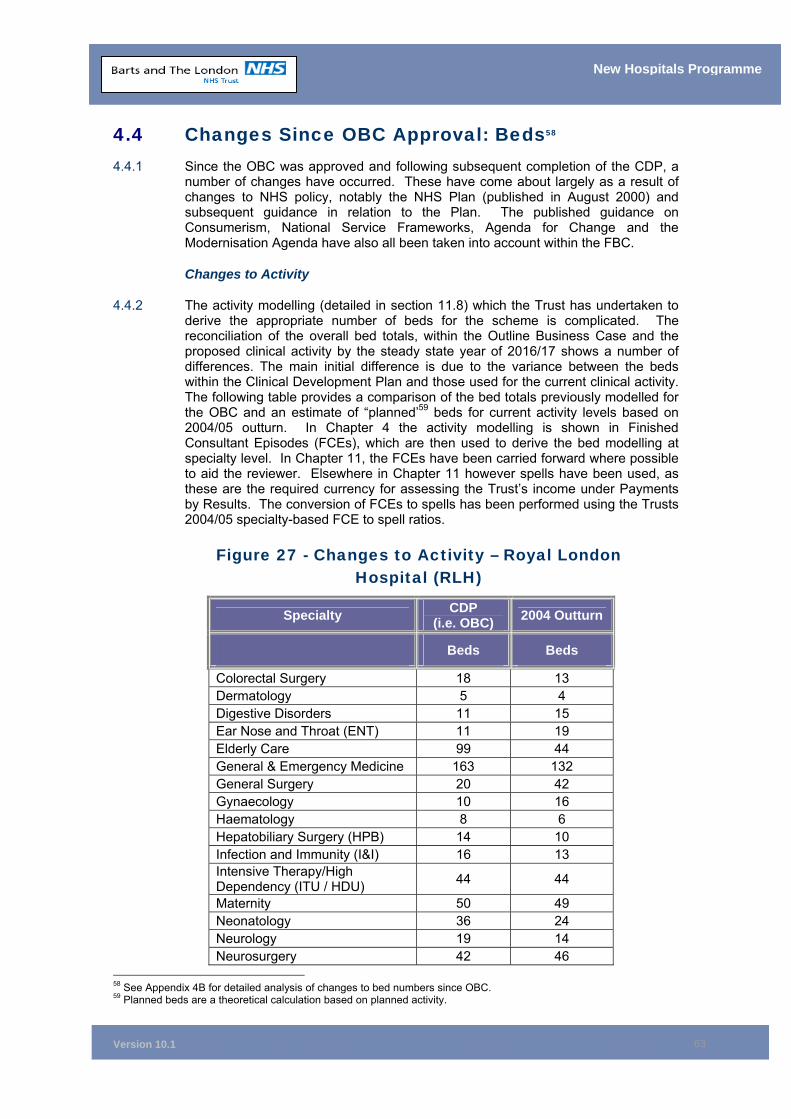
Version 10.1
63
New Hospitals Programme
4.4 Changes Since OBC Approval: Beds58 4.4.1 Since the OBC was approved and following subsequent completion of the CDP, a
number of changes have occurred. These have come about largely as a result of changes to NHS policy, notably the NHS Plan (published in August 2000) and subsequent guidance in relation to the Plan. The published guidance on Consumerism, National Service Frameworks, Agenda for Change and the Modernisation Agenda have also all been taken into account within the FBC.
Changes to Activity
4.4.2 The activity modelling (detailed in section 11.8) which the Trust has undertaken to derive the appropriate number of beds for the scheme is complicated. The reconciliation of the overall bed totals, within the Outline Business Case and the proposed clinical activity by the steady state year of 2016/17 shows a number of differences. The main initial difference is due to the variance between the beds within the Clinical Development Plan and those used for the current clinical activity. The following table provides a comparison of the bed totals previously modelled for the OBC and an estimate of “planned’59 beds for current activity levels based on 2004/05 outturn. In Chapter 4 the activity modelling is shown in Finished Consultant Episodes (FCEs), which are then used to derive the bed modelling at specialty level. In Chapter 11, the FCEs have been carried forward where possible to aid the reviewer. Elsewhere in Chapter 11 however spells have been used, as these are the required currency for assessing the Trust’s income under Payments by Results. The conversion of FCEs to spells has been performed using the Trusts 2004/05 specialty-based FCE to spell ratios.
Figure 27 - Changes to Activity – Royal London Hospital (RLH)
Specialty CDP (i.e. OBC) 2004 Outturn
Beds Beds
Colorectal Surgery 18 13 Dermatology 5 4 Digestive Disorders 11 15 Ear Nose and Throat (ENT) 11 19 Elderly Care 99 44 General & Emergency Medicine 163 132 General Surgery 20 42 Gynaecology 10 16 Haematology 8 6 Hepatobiliary Surgery (HPB) 14 10 Infection and Immunity (I&I) 16 13 Intensive Therapy/High Dependency (ITU / HDU) 44 44
Maternity 50 49 Neonatology 36 24 Neurology 19 14 Neurosurgery 42 46
58 See Appendix 4B for detailed analysis of changes to bed numbers since OBC. 59 Planned beds are a theoretical calculation based on planned activity.
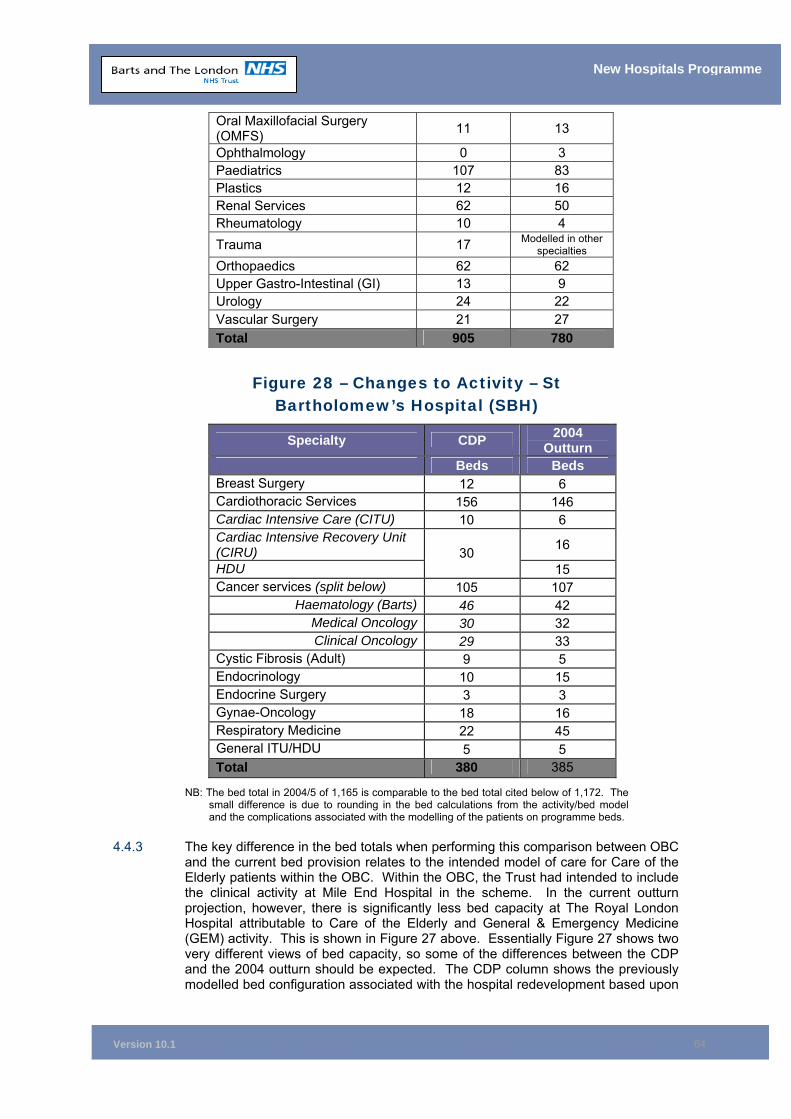
Version 10.1
64
New Hospitals Programme
Oral Maxillofacial Surgery (OMFS) 11 13
Ophthalmology 0 3 Paediatrics 107 83 Plastics 12 16 Renal Services 62 50 Rheumatology 10 4 Trauma 17 Modelled in other
specialties Orthopaedics 62 62 Upper Gastro-Intestinal (GI) 13 9 Urology 24 22 Vascular Surgery 21 27 Total 905 780
Figure 28 – Changes to Activity – St Bartholomew’s Hospital (SBH)
Specialty CDP 2004 Outturn
Beds Beds Breast Surgery 12 6 Cardiothoracic Services 156 146 Cardiac Intensive Care (CITU) 10 6 Cardiac Intensive Recovery Unit (CIRU) 16
HDU 30
15 Cancer services (split below) 105 107
Haematology (Barts) 46 42 Medical Oncology 30 32 Clinical Oncology 29 33
Cystic Fibrosis (Adult) 9 5 Endocrinology 10 15 Endocrine Surgery 3 3 Gynae-Oncology 18 16 Respiratory Medicine 22 45 General ITU/HDU 5 5 Total 380 385
NB: The bed total in 2004/5 of 1,165 is comparable to the bed total cited below of 1,172. The small difference is due to rounding in the bed calculations from the activity/bed model and the complications associated with the modelling of the patients on programme beds.
4.4.3 The key difference in the bed totals when performing this comparison between OBC and the current bed provision relates to the intended model of care for Care of the Elderly patients within the OBC. Within the OBC, the Trust had intended to include the clinical activity at Mile End Hospital in the scheme. In the current outturn projection, however, there is significantly less bed capacity at The Royal London Hospital attributable to Care of the Elderly and General & Emergency Medicine (GEM) activity. This is shown in Figure 27 above. Essentially Figure 27 shows two very different views of bed capacity, so some of the differences between the CDP and the 2004 outturn should be expected. The CDP column shows the previously modelled bed configuration associated with the hospital redevelopment based upon
Version 10.1
65
New Hospitals Programme
the 2002 CDP. The 2004 outturn column shows actual bed usage now. The general surgery difference is due to the trauma modelling approach in part and the balance is due to the changing local specialty code definitions of what is general and specialist surgery (colorectal, HPB, upper GI and urology have all gone down). Please note that the impact of the mothballed beds on specialities has not yet been modelled. This can only be done once it is clear that elements are being taken out of the scheme (see paras 4.4.21-4.4.33)
4.4.4 Appendix 4C shows the summary activity in FCEs, along with average length of stays for the CDP and 2004/05 outturn, which is the start point for the activity modelling. This modelling is then projected forward to include the modelled clinical activity for 2011 and 2016.
4.4.5 In summary, Appendix 4C shows the interaction of all the modelling variables to derive the activity and bed numbers used in the FBC.
Table 1 – Shows the activity, bed numbers and beds days which were the start point of the activity modelling in the OBC.
Table 2 - Shows the activity, bed numbers and beds days which were the start point of the activity modelling in the FBC 2003/4 outturn, but with the THPCT activity baseline set to 2004/5 outturn, after agreement with THPCT.
Table 3 – Shows the activity, bed numbers and beds days which result from taking the 2011 modelled activity using existing throughput assumptions.
Table 4 – Shows the activity, bed numbers and beds days which result from taking the 2016 modelled activity using existing throughput assumptions.
Table 5 – Shows the activity, bed numbers and beds days which result from taking the 2016 modelled activity and the proposed productivity levels using the benchmarked throughput assumptions. The approach taken to productivity assumptions is explained in section 11.9.
Table 6 – Shows the bed requirements under a range of these different scenarios for comparison purposes.
Table 7 – Shows the population projections used in the activity model, which are a key driver for the clinical activity modelling given the nature of the proposed Thames Gateway development.
4.4.6 The major complicating factor in this exercise is the modelling approach adopted for critical care. The Trust continues to have a modelled bed requirement for critical care which was set at the OBC stage and which acknowledged the under-provision of critical care in the North East London health economy.
4.4.7 In order to reconcile the start point of the bed requirement within the hospital at 2004/05 and the modelled bed requirement via clinical activity, the following reconciliation needs to be performed.

Version 10.1
66
New Hospitals Programme
Figure 28A – Reconciliation
Current beds as per computation via admitted patient care60 1,085
Current Trust critical care capacity 52
Beds currently used for patients on programme and other 35
Current Trust Total Bed Capacity at 2004/5 1172
4.4.8 This computed bed total of 1085 has then been used as the starting bed modelling and has been adjusted for a range of changes to service provision. The activity and performance assumptions underpinning the CDP were developed with the best available evidence at the time. Since then, a number of factors have challenged these assumptions:
■ Changes in clinical practice and service configuration such as the development of clinical networks in urology;
■ In cardiac services the development of the Essex Cardiac Centre, revised proposals for optimal revascularisation rates and the prominence of interventional cardiology;
■ The 2001 census provided a more detailed and accurate projection of the demography of the health economy; and
■ The Modernisation Agenda and the Trust’s drive towards improved efficiency has reduced length of stay and improved day case rates across key bed-holding specialties.
4.4.9 As a consequence of these and other developments, new benchmarks for length of stay and day case rates were set using the outturn for 2003/04 (2004/05 for Tower Hamlets PCT activity) as the baseline for projection to 2011 and 2016 as the steady state position. Similarly, the assumptions in the CDP relating to demographic change have been adjusted to the 2001 census with local validation from NELSHA.
4.4.10 Four other factors in relation to the management of demand for acute services have been taken into account in the projection to 2011:
■ An increase in demand of 3% a year in non-elective activity to 2008 and reduction to 0.5% a year thereafter to 2016;
■ A 5% total reduction in acute demand/intervention through management of patients in primary care with long-term conditions by 2008;
■ A 10% migration of short stay elective activity to Independent Sector Treatment Centres (ISTCs) by 2010 (this equates to 7.6% of overall elective work.); and
■ A reduction in non-elective admissions of 0.5% for under 65s to General Medicine, Cardiology, Rheumatology and Diabetology.
4.4.11 See Chapter 11, section 11.8 for further details on the 12-year activity modelling.
Cardiac Services
4.4.12 The Trust’s 12-year activity model, agreed with PCTs, includes the activity projections used in the FBC for the Essex Heart Centre at Basildon Hospital. In line
60 As per Appendix 4D Table 1.
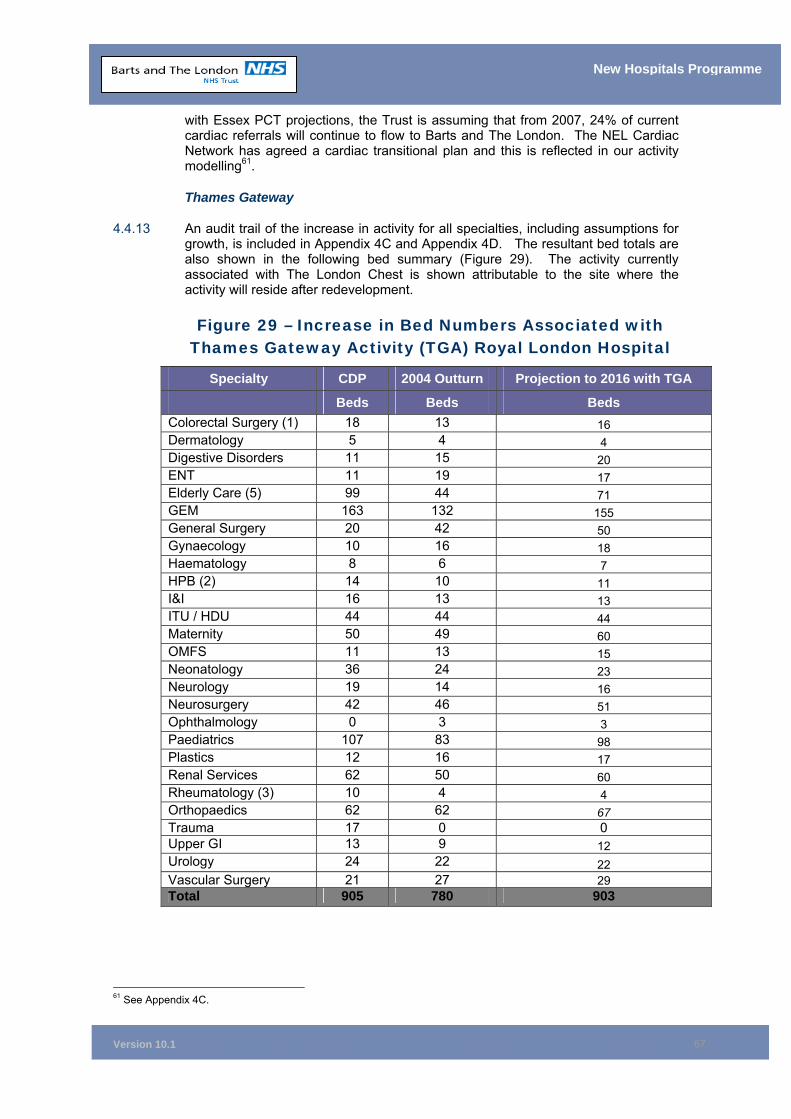
Version 10.1
67
New Hospitals Programme
with Essex PCT projections, the Trust is assuming that from 2007, 24% of current cardiac referrals will continue to flow to Barts and The London. The NEL Cardiac Network has agreed a cardiac transitional plan and this is reflected in our activity modelling61.
Thames Gateway
4.4.13 An audit trail of the increase in activity for all specialties, including assumptions for growth, is included in Appendix 4C and Appendix 4D. The resultant bed totals are also shown in the following bed summary (Figure 29). The activity currently associated with The London Chest is shown attributable to the site where the activity will reside after redevelopment.
Figure 29 – Increase in Bed Numbers Associated with Thames Gateway Activity (TGA) Royal London Hospital
Specialty CDP 2004 Outturn Projection to 2016 with TGA
Beds Beds Beds Colorectal Surgery (1) 18 13 16 Dermatology 5 4 4 Digestive Disorders 11 15 20 ENT 11 19 17 Elderly Care (5) 99 44 71 GEM 163 132 155 General Surgery 20 42 50 Gynaecology 10 16 18 Haematology 8 6 7 HPB (2) 14 10 11 I&I 16 13 13 ITU / HDU 44 44 44 Maternity 50 49 60 OMFS 11 13 15 Neonatology 36 24 23 Neurology 19 14 16 Neurosurgery 42 46 51 Ophthalmology 0 3 3 Paediatrics 107 83 98 Plastics 12 16 17 Renal Services 62 50 60 Rheumatology (3) 10 4 4 Orthopaedics 62 62 67 Trauma 17 0 0 Upper GI 13 9 12 Urology 24 22 22 Vascular Surgery 21 27 29 Total 905 780 903
61 See Appendix 4C.
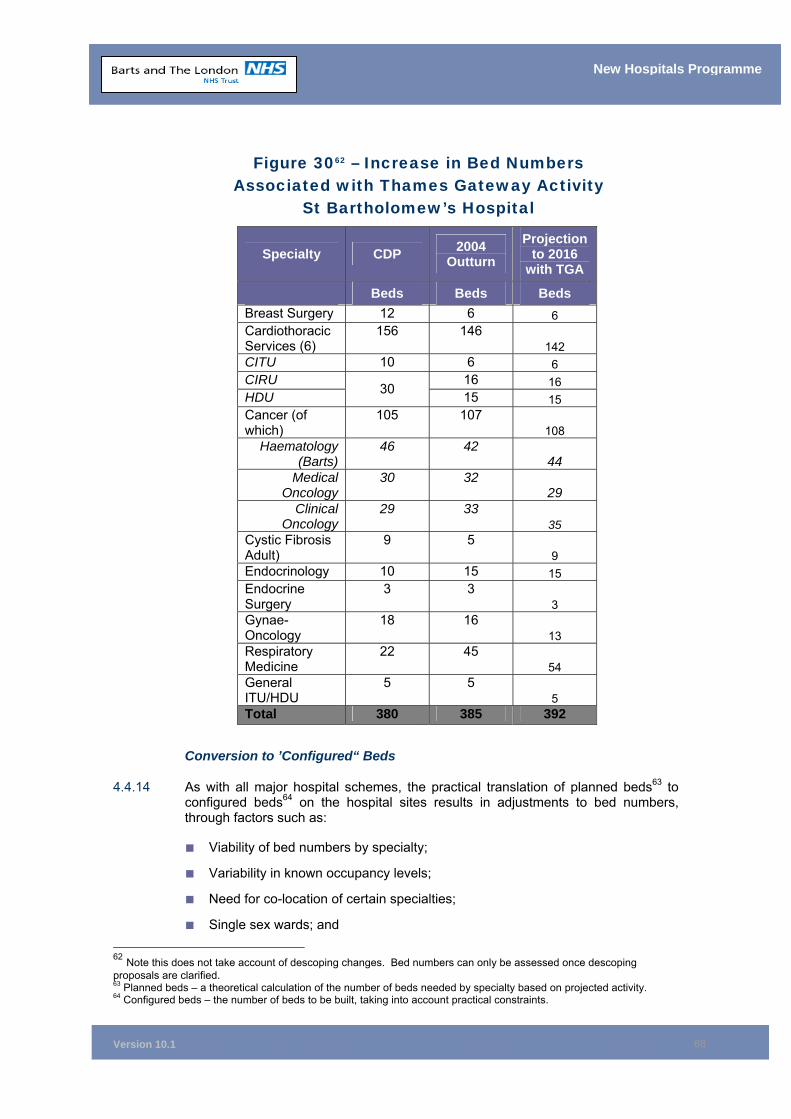
Version 10.1
68
New Hospitals Programme
Figure 3062 – Increase in Bed Numbers Associated with Thames Gateway Activity
St Bartholomew’s Hospital
Specialty CDP 2004 Outturn
Projection to 2016
with TGA
Beds Beds Beds Breast Surgery 12 6 6 Cardiothoracic Services (6)
156 146 142
CITU 10 6 6 CIRU 16 16 HDU 30 15 15 Cancer (of which)
105 107 108
Haematology (Barts)
46 42 44
Medical Oncology
30 32 29
Clinical Oncology
29 33 35
Cystic Fibrosis Adult)
9 5 9
Endocrinology 10 15 15 Endocrine Surgery
3 3 3
Gynae-Oncology
18 16 13
Respiratory Medicine
22 45 54
General ITU/HDU
5 5 5
Total 380 385 392
Conversion to ’Configured“ Beds
4.4.14 As with all major hospital schemes, the practical translation of planned beds63 to configured beds64 on the hospital sites results in adjustments to bed numbers, through factors such as:
■ Viability of bed numbers by specialty;
■ Variability in known occupancy levels;
■ Need for co-location of certain specialties;
■ Single sex wards; and 62 Note this does not take account of descoping changes. Bed numbers can only be assessed once descoping proposals are clarified. 63 Planned beds – a theoretical calculation of the number of beds needed by specialty based on projected activity. 64 Configured beds – the number of beds to be built, taking into account practical constraints.
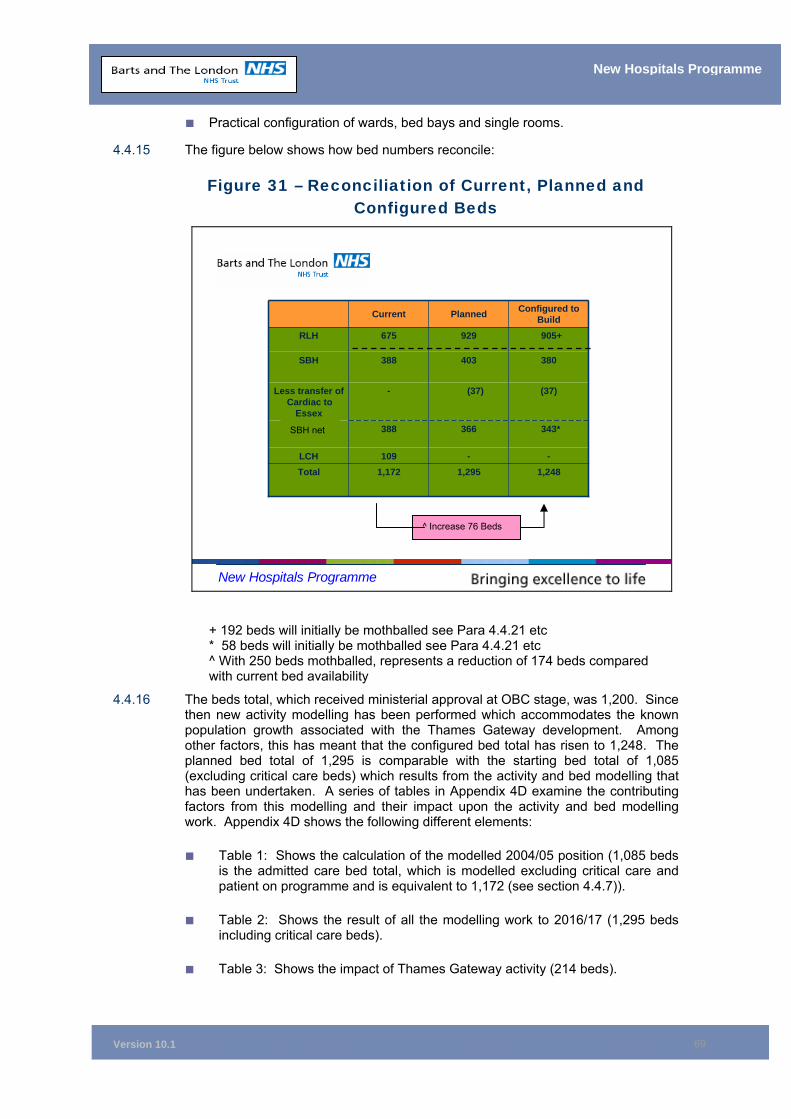
Version 10.1
69
New Hospitals Programme
■ Practical configuration of wards, bed bays and single rooms.
4.4.15 The figure below shows how bed numbers reconcile:
Figure 31 – Reconciliation of Current, Planned and Configured Beds
New Hospitals Programme
+ 192 beds will initially be mothballed see Para 4.4.21 etc * 58 beds will initially be mothballed see Para 4.4.21 etc ^ With 250 beds mothballed, represents a reduction of 174 beds compared with current bed availability
4.4.16 The beds total, which received ministerial approval at OBC stage, was 1,200. Since then new activity modelling has been performed which accommodates the known population growth associated with the Thames Gateway development. Among other factors, this has meant that the configured bed total has risen to 1,248. The planned bed total of 1,295 is comparable with the starting bed total of 1,085 (excluding critical care beds) which results from the activity and bed modelling that has been undertaken. A series of tables in Appendix 4D examine the contributing factors from this modelling and their impact upon the activity and bed modelling work. Appendix 4D shows the following different elements:
■ Table 1: Shows the calculation of the modelled 2004/05 position (1,085 beds is the admitted care bed total, which is modelled excluding critical care and patient on programme and is equivalent to 1,172 (see section 4.4.7)).
■ Table 2: Shows the result of all the modelling work to 2016/17 (1,295 beds including critical care beds).
■ Table 3: Shows the impact of Thames Gateway activity (214 beds).
--109LCH
343* 366388
(37)(37)-Less transfer of Cardiac to
Essex
905+ 929675RLH
380403388SBH
1,248 1,2951,172Total
Configured to Build PlannedCurrent
SBH net
^ Increase 76 Beds
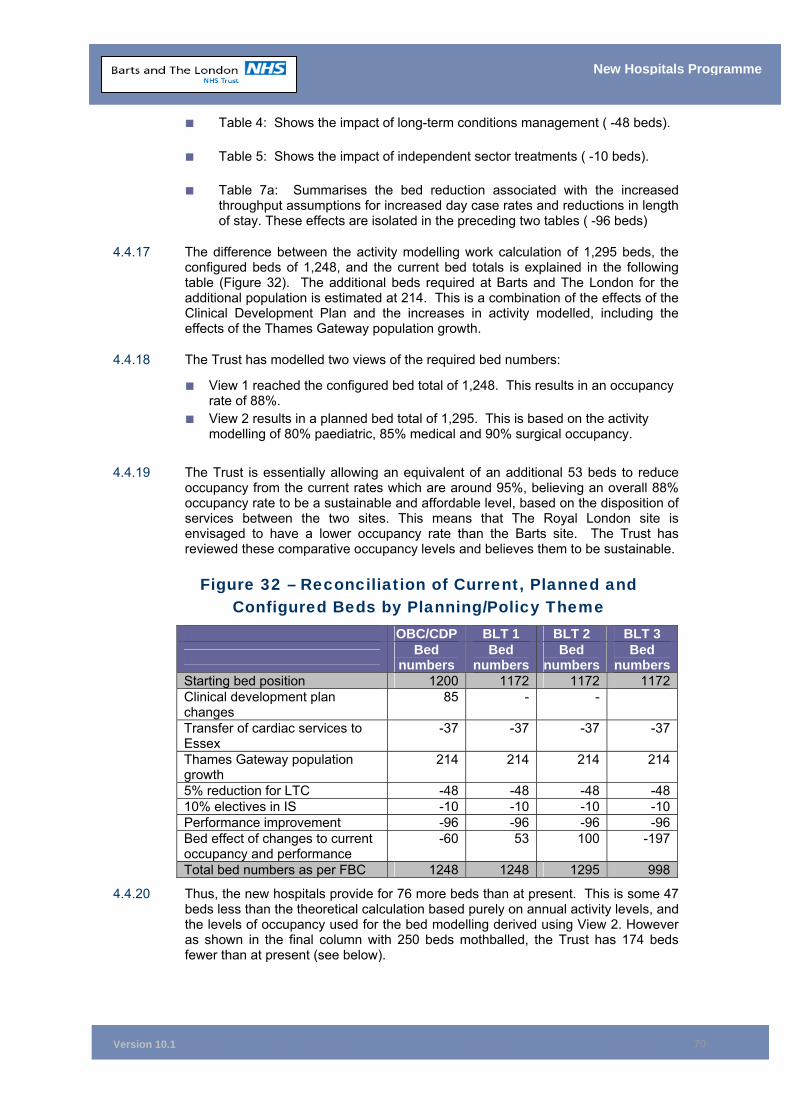
Version 10.1
70
New Hospitals Programme
■ Table 4: Shows the impact of long-term conditions management ( -48 beds).
■ Table 5: Shows the impact of independent sector treatments ( -10 beds).
■ Table 7a: Summarises the bed reduction associated with the increased throughput assumptions for increased day case rates and reductions in length of stay. These effects are isolated in the preceding two tables ( -96 beds)
4.4.17 The difference between the activity modelling work calculation of 1,295 beds, the configured beds of 1,248, and the current bed totals is explained in the following table (Figure 32). The additional beds required at Barts and The London for the additional population is estimated at 214. This is a combination of the effects of the Clinical Development Plan and the increases in activity modelled, including the effects of the Thames Gateway population growth.
4.4.18 The Trust has modelled two views of the required bed numbers:
■ View 1 reached the configured bed total of 1,248. This results in an occupancy rate of 88%.
■ View 2 results in a planned bed total of 1,295. This is based on the activity modelling of 80% paediatric, 85% medical and 90% surgical occupancy.
4.4.19 The Trust is essentially allowing an equivalent of an additional 53 beds to reduce occupancy from the current rates which are around 95%, believing an overall 88% occupancy rate to be a sustainable and affordable level, based on the disposition of services between the two sites. This means that The Royal London site is envisaged to have a lower occupancy rate than the Barts site. The Trust has reviewed these comparative occupancy levels and believes them to be sustainable.
Figure 32 – Reconciliation of Current, Planned and Configured Beds by Planning/Policy Theme
OBC/CDP BLT 1 BLT 2 BLT 3
Bed numbers
Bed numbers
Bed numbers
Bed numbers
Starting bed position 1200 1172 1172 1172Clinical development plan changes
85 - -
Transfer of cardiac services to Essex
-37 -37 -37 -37
Thames Gateway population growth
214 214 214 214
5% reduction for LTC -48 -48 -48 -4810% electives in IS -10 -10 -10 -10Performance improvement -96 -96 -96 -96Bed effect of changes to current occupancy and performance
-60 53 100 -197
Total bed numbers as per FBC 1248 1248 1295 998
4.4.20 Thus, the new hospitals provide for 76 more beds than at present. This is some 47 beds less than the theoretical calculation based purely on annual activity levels, and the levels of occupancy used for the bed modelling derived using View 2. However as shown in the final column with 250 beds mothballed, the Trust has 174 beds fewer than at present (see below).
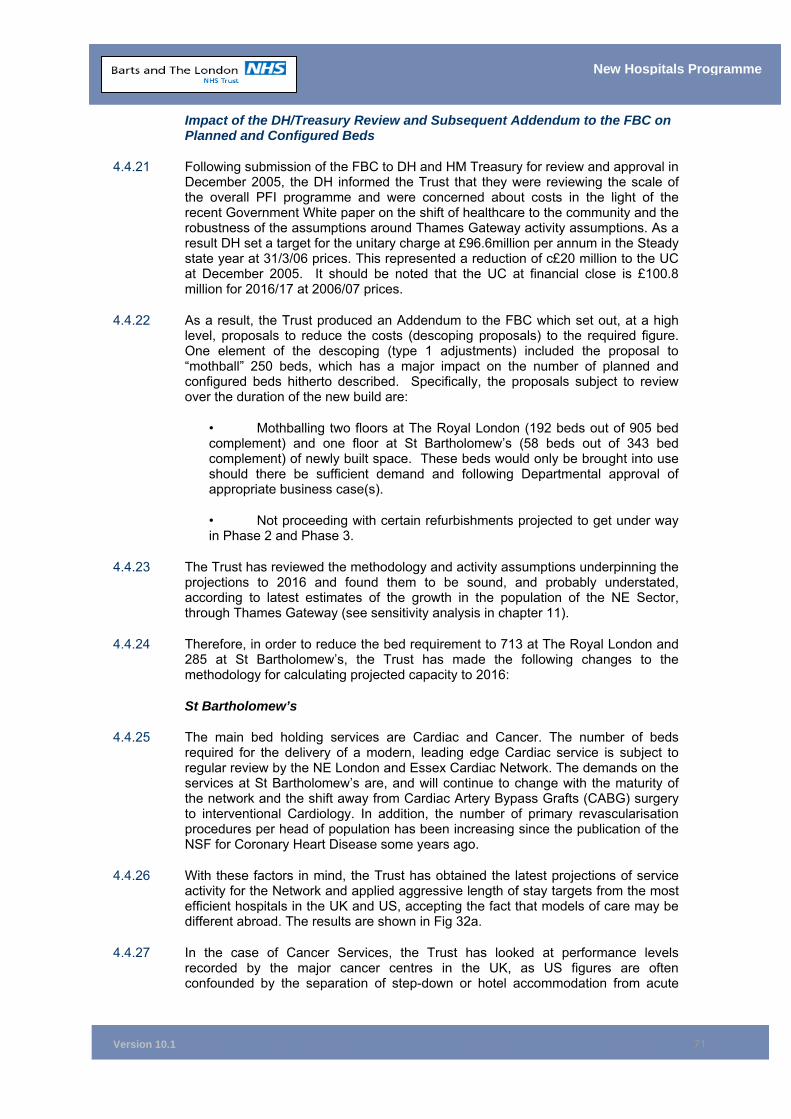
Version 10.1
71
New Hospitals Programme
Impact of the DH/Treasury Review and Subsequent Addendum to the FBC on Planned and Configured Beds
4.4.21 Following submission of the FBC to DH and HM Treasury for review and approval in December 2005, the DH informed the Trust that they were reviewing the scale of the overall PFI programme and were concerned about costs in the light of the recent Government White paper on the shift of healthcare to the community and the robustness of the assumptions around Thames Gateway activity assumptions. As a result DH set a target for the unitary charge at £96.6million per annum in the Steady state year at 31/3/06 prices. This represented a reduction of c£20 million to the UC at December 2005. It should be noted that the UC at financial close is £100.8 million for 2016/17 at 2006/07 prices.
4.4.22 As a result, the Trust produced an Addendum to the FBC which set out, at a high level, proposals to reduce the costs (descoping proposals) to the required figure. One element of the descoping (type 1 adjustments) included the proposal to “mothball” 250 beds, which has a major impact on the number of planned and configured beds hitherto described. Specifically, the proposals subject to review over the duration of the new build are:
• Mothballing two floors at The Royal London (192 beds out of 905 bed complement) and one floor at St Bartholomew’s (58 beds out of 343 bed complement) of newly built space. These beds would only be brought into use should there be sufficient demand and following Departmental approval of appropriate business case(s).
• Not proceeding with certain refurbishments projected to get under way in Phase 2 and Phase 3.
4.4.23 The Trust has reviewed the methodology and activity assumptions underpinning the projections to 2016 and found them to be sound, and probably understated, according to latest estimates of the growth in the population of the NE Sector, through Thames Gateway (see sensitivity analysis in chapter 11).
4.4.24 Therefore, in order to reduce the bed requirement to 713 at The Royal London and 285 at St Bartholomew’s, the Trust has made the following changes to the methodology for calculating projected capacity to 2016:
St Bartholomew’s
4.4.25 The main bed holding services are Cardiac and Cancer. The number of beds required for the delivery of a modern, leading edge Cardiac service is subject to regular review by the NE London and Essex Cardiac Network. The demands on the services at St Bartholomew’s are, and will continue to change with the maturity of the network and the shift away from Cardiac Artery Bypass Grafts (CABG) surgery to interventional Cardiology. In addition, the number of primary revascularisation procedures per head of population has been increasing since the publication of the NSF for Coronary Heart Disease some years ago.
4.4.26 With these factors in mind, the Trust has obtained the latest projections of service activity for the Network and applied aggressive length of stay targets from the most efficient hospitals in the UK and US, accepting the fact that models of care may be different abroad. The results are shown in Fig 32a.
4.4.27 In the case of Cancer Services, the Trust has looked at performance levels recorded by the major cancer centres in the UK, as US figures are often confounded by the separation of step-down or hotel accommodation from acute
Version 10.1
72
New Hospitals Programme
care. Only one Trust has recently achieved performance targets in excess of those hitherto used in the FBC – the Christie Hospital in Manchester. It is likely that the Hospital’s relationship with the local cancer network will be rather different as a standalone cancer centre to the profile of service delivery of St Bartholomew’s. Nevertheless, Fig 32a shows the impact of applying the Christie’s length of stay profile to the activity projections for St Bartholomew’s.
The Royal London
4.4.28 Conducting a similar exercise for the Royal London achieved little in the way of bed savings as target levels of performance in the FBC are already amongst the best in class. Instead, a more radical approach was taken to re-profile length of stay by specialty by identifying two patient cohorts whose post acute care could, theoretically, be delivered in a step down setting:
• Medium to long term rehabilitation
• Post acute outliers by length of stay
4.4.29 The first group were identified by condition; the latter by applying the national median length of stay by HRG with an additional time envelope for the resettlement to primary care or repatriation to the local community. It should be noted that NEL PCTs have not, as yet, been party to this modelling exercise (though the activity remains the same at steady state as explained in chapter 11). This will need to be progressed with them as the detail of the descoping is worked through over the next 15 months.
Figure 32a – Impact of Descoping Exercise on Bed Numbers
NB- as detailed in chapter 11, the affordability position at steady state does not include any income for the Mile End beds transferred into the RLH (rehabilitation)
4.4.30 In practice, neither option presents a pragmatic resolution to the descoping exercise whilst maintaining activity levels projected to 2016. The figure of 142 beds taken from The Royal London scheme falls far short of the 192 required.
4.4.31 Appendix 4G shows the assumptions behind the models, which will need to be reviewed in liaison with the clinical directorates, over the next 15 months, as the detailed and final descoping variations are worked up to deliver the necessary reduction to the UC .
4.4.32 An alternative scenario considered in sensitivity testing at OBC stage was to project demand and activity for acute beds to 2016, assuming no increase in admissions for the Thames Gateway development. The results of this model, where activity is driven by the trends in the Trust’s current catchment population and referral patterns, can be seen at Appendix 4D, Table 3. The net increase to contain the
Configured beds
Acute phase beds
Possible Transfer of post acute rehab to primary care
Variance from
configured beds
SBH 343 284 0 59
RLH 905 788 25 142
Version 10.1
73
New Hospitals Programme
Thames Gateway development to 2016 is 214 beds across the Trust, compared with the 250 required by the descoping exercise.
4.4.33 Therefore, as can be seen, if the population assumptions in the FBC do not come to fruition, and the consequent activity assumptions outlined in the FBC and endorsed by the PCTs are not realised, the proposed reduction in beds across the new development is feasible. However, if the base case activity assumptions are accurate, with the RLH mothballed beds, the Trust will need to become the best of class (not just in the UK) and even more radically innovate the models of care, for example
• full implementation of fast track surgery with the length of stay for complex surgery reducing from the current average of 10 days to 6 days and the introduction of trauma, elective and emergency surgery wards.
• Patient care for Physician led admitted care (medical wards) moved to a consultant team approach i.e. patients admitted under a consultant team rather than an individual so that decision making is faster.
4.4.34 At present, PCTs are working to the original Thames Gateway population projects and activity levels employed by the Trust. They are however, aware of the issues the Trust will need to address once specific descoping proposals have been agreed, the Trust will consult with PCTs on the proposals and the impact on activity. This will include discussions on the feasibility and efficacy of step-down facilities.
4.5 Changes Since OBC Approval: Capital Costs 4.5.1 The paragraphs below describe the factors which have changed capital costs since
OBC.
Changes in External Factors
4.5.2 These are cost changes to the scheme beyond Trust control. They are a result of three variables:
■ Increases to national indices e.g. construction pricing;
■ Changes to NHS policy; and
■ Changes required as a result of the planning process to attain planning consent.
4.5.3 The details of the external factors that have affected the scheme are set out below:
■ The capital cost of the OBC at approval in February 2000 was based on MIPS 295. At FBC, the Trust has been required to use MIPS 415. As the building of the new hospitals is being undertaken over a nine year period, an estimate of inflation during this period has assumed a total cost of £1.216 billion. This is the capital cost and, including financing and development costs, it would increase to a figure comparable to the £1.8 billion reflected in the Unitary Charge (UC).
■ The increase in Departmental Cost Allowance Guidance (DCAGs) and Improving the Patient Experience increased the cost by £149m.
■ From OBC to FBC, the location factor for inner London has increased from 19% to 23%, as advised by NHS Estates (£17m).
Version 10.1
74
New Hospitals Programme
■ The Greater London Authority (GLA) notified the Trust during the planning approval process that without significant amendments to the new hospital development on The Royal London site, the GLA were minded to direct the London Borough of Tower Hamlets (LBTH) to refuse planning permission. The following changes were therefore agreed and incorporated into the scheme:
Moving the new hospital tower blocks to provide a better sight line.
The redesign of the A&E department to enhance the environment and provide increased security.
The demolition of East Wing to enhance wayfinding to those areas of the hospital which will have separate entrances. This has the additional benefit of improving the public realm/open spaces on The Royal London site.
4.5.4 These changes have been included in the PSC to ensure that the PSC and the PFI solution are comparable.
4.5.5 In total, the increase in capital costs as a result of regeneration and improvement due to wider stakeholder engagement have added £211 million to the cost of the project (see Appendix 4E for more detail). This cost has been factored into the affordability position and is included in the annual UC of £100.8 million (at 2006/07 prices in steady state).
4.5.6 The Trust removed the proposed investment of £27 million in ICT. The cabling and infrastructure for ICT therefore remain within the construction costs of the project. This was following the advent of the National Programme.
4.5.7 The DH has been kept fully informed of the changes to the costs of the scheme throughout the development and procurement process and these changes have been included in the PSC to ensure that the PSC and the PFI solution are comparable.
Derivation of Non-Works Costs and Contingencies
4.5.8 These costs are derived as a percentage of the capital cost and are therefore driven upwards/downwards with any change in capital costs resulting from either external factors or changes to the Trusts requirements. Those that have had an impact on the scheme are:
■ Removal costs;
■ Decommissioning;
■ Decanting;
■ Statutory changes to building regulations; and
■ Planning costs.
4.5.9 Contingencies and fees are driven by changes to the construction cost. The rise in MIPS has therefore impacted on these costs which are £116.4 million within the total indexation to MIPS 415 in the PSC.
Changes to Trust Requirements
4.5.10 Increased/decreased costs can be generated by Trust-driven changes to the scope and size of the project. These variables are, by definition, factors within the control of the Trust.
Version 10.1
75
New Hospitals Programme
4.5.11 There have been several changes to the Trust requirements since the approval of the OBC (see also Chapter 11, paragraph 11.15.9):
■ An increase of 48 beds at a cost of £24 million following the outcome of the CDP;
■ The decision to seal the buildings at a cost of £17 million65
■ The risk assessed planning contingency was as a result of reviewing contingencies with NHS Estates, who felt the Trust was £15m too light.
■ Similarly, the design development relates mainly to the NHS Estates’ view that the scheme’s costs for cladding at a high level (using a technique called curtain walling) were too low, as they were based on an NHS average (DCAG plus a height allowance) and our buildings are higher than the norm for hospitals.
■ Value engineering subsequent to the selection of the preferred bidder:
The omission of the provision of a new nursery (retaining the current one), demolition of the unused boiler house and landscaping the area;
The decision to demolish the Ambrose King building and re-locate the
functions within the remaining planned space;
The omission of the refurbishment of the pathology building at Barts by integrating (with very minor exceptions) all of the Trust’s pathology service at The Royal London;
The removal of a proportion of non-lifecycle, loose equipment from the
scope of PFI leaving the Trust to fund, procure and install;
The relocation of corporate directorate staff located at Prescot Street (which can be handed back on lease expiry) through the addition of one floor onto the new outpatients building at The Royal London Hospital;
The modification of deductions that arise under the payment mechanism
and reduction in the number of performance standards that attract deductions; and
Skanska Innisfree increasing the level of car parking income guaranteed
to the Trust by agreeing to provide more spaces, at its own risk, than the number consented to by the London Borough of Tower Hamlets.
4.5.12 The changes to bed numbers have been agreed with the Trust’s local commissioners. The Trust’s approach to the provision of clinical services and the supporting evidence for the bed numbers are described in Chapter 3. The Trust changes also include an additional linear accelerator (£5m) at SBH to reflect projections of radiotherapy treatments.
4.5.13 The Trust’s ICT strategy is described in Chapter 17. In addition to the removal of the capital costs of ICT, the revenue costs and potential benefits and savings associated with it have been removed from the business case. Appendix 11A details the efficiency savings and this does not detail any ICT savings.
65 Note: Only this change took place during the competition, all others were taken into account prior to launching the procurement.
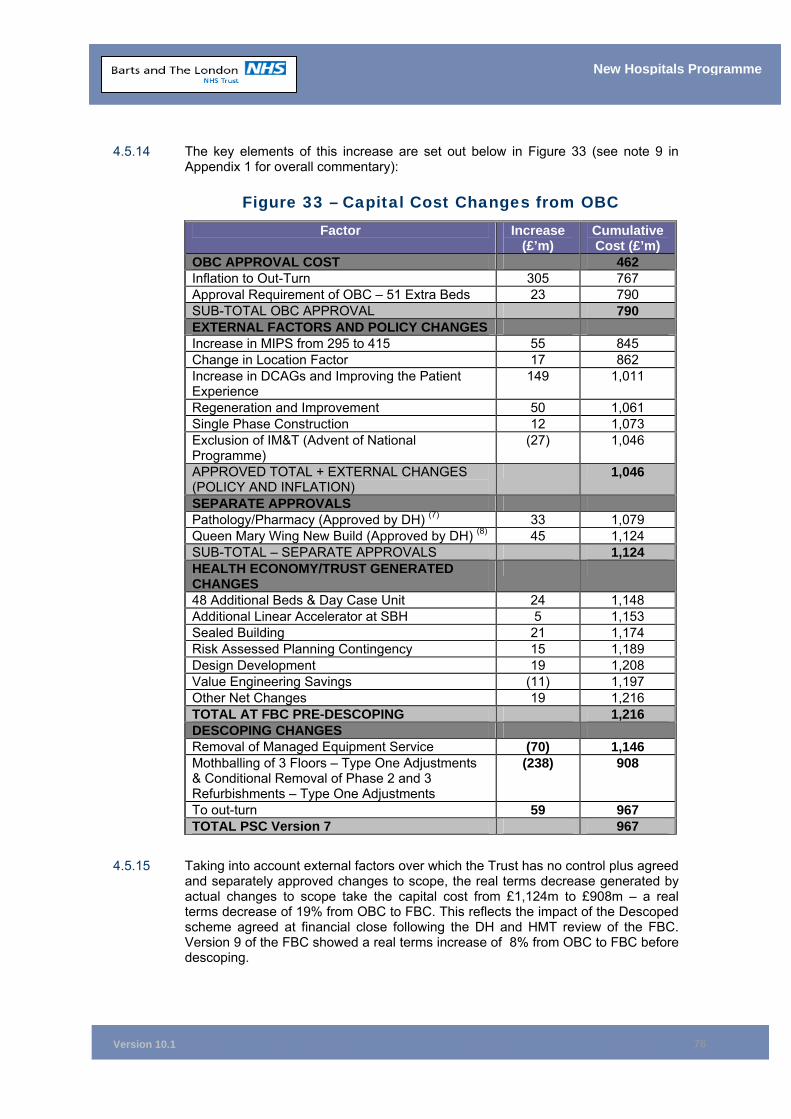
Version 10.1
76
New Hospitals Programme
4.5.14 The key elements of this increase are set out below in Figure 33 (see note 9 in Appendix 1 for overall commentary):
Figure 33 – Capital Cost Changes from OBC Factor Increase
(£’m) Cumulative Cost (£’m)
OBC APPROVAL COST 462 Inflation to Out-Turn 305 767 Approval Requirement of OBC – 51 Extra Beds 23 790 SUB-TOTAL OBC APPROVAL 790 EXTERNAL FACTORS AND POLICY CHANGES Increase in MIPS from 295 to 415 55 845 Change in Location Factor 17 862 Increase in DCAGs and Improving the Patient Experience
149 1,011
Regeneration and Improvement 50 1,061 Single Phase Construction 12 1,073 Exclusion of IM&T (Advent of National Programme)
(27) 1,046
APPROVED TOTAL + EXTERNAL CHANGES (POLICY AND INFLATION)
1,046
SEPARATE APPROVALS Pathology/Pharmacy (Approved by DH) (7) 33 1,079 Queen Mary Wing New Build (Approved by DH) (8) 45 1,124 SUB-TOTAL – SEPARATE APPROVALS 1,124 HEALTH ECONOMY/TRUST GENERATED CHANGES
48 Additional Beds & Day Case Unit 24 1,148 Additional Linear Accelerator at SBH 5 1,153 Sealed Building 21 1,174 Risk Assessed Planning Contingency 15 1,189 Design Development 19 1,208 Value Engineering Savings (11) 1,197 Other Net Changes 19 1,216 TOTAL AT FBC PRE-DESCOPING 1,216 DESCOPING CHANGES Removal of Managed Equipment Service (70) 1,146 Mothballing of 3 Floors – Type One Adjustments & Conditional Removal of Phase 2 and 3 Refurbishments – Type One Adjustments
(238) 908
To out-turn 59 967 TOTAL PSC Version 7 967
4.5.15 Taking into account external factors over which the Trust has no control plus agreed and separately approved changes to scope, the real terms decrease generated by actual changes to scope take the capital cost from £1,124m to £908m – a real terms decrease of 19% from OBC to FBC. This reflects the impact of the Descoped scheme agreed at financial close following the DH and HMT review of the FBC. Version 9 of the FBC showed a real terms increase of 8% from OBC to FBC before descoping.
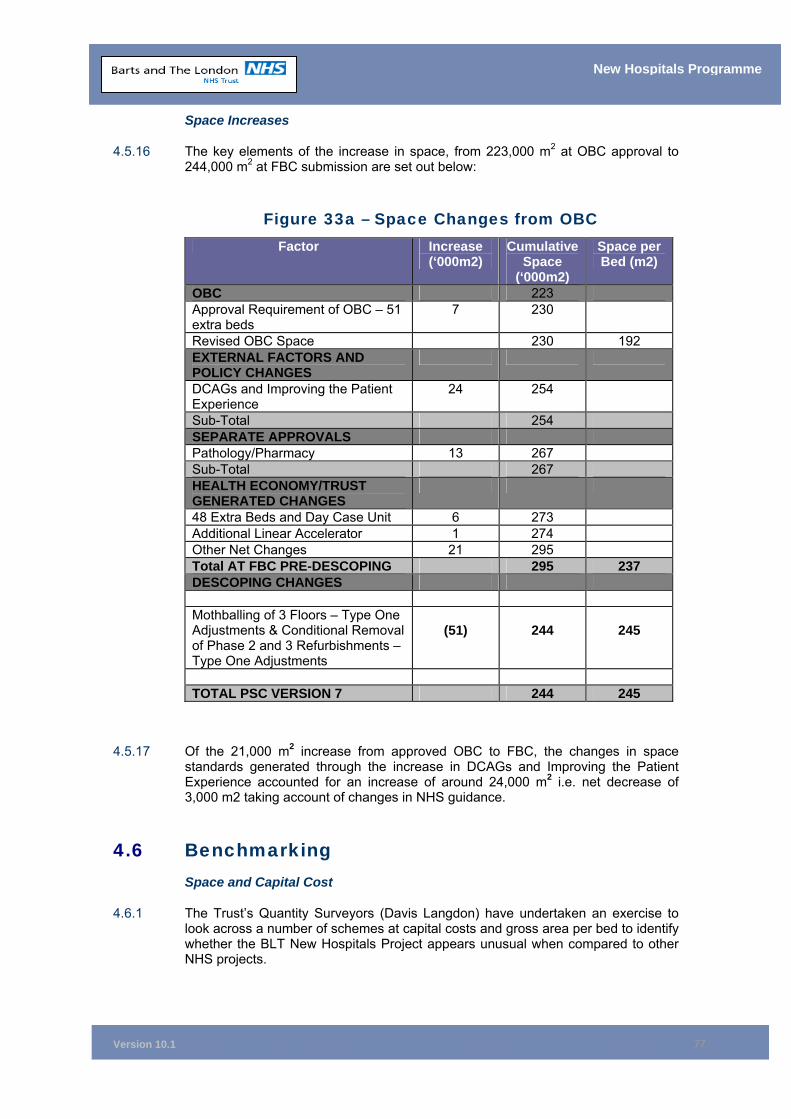
Version 10.1
77
New Hospitals Programme
Space Increases
4.5.16 The key elements of the increase in space, from 223,000 m2 at OBC approval to 244,000 m2 at FBC submission are set out below:
Figure 33a – Space Changes from OBC Factor Increase
(‘000m2) Cumulative
Space (‘000m2)
Space per Bed (m2)
OBC 223 Approval Requirement of OBC – 51 extra beds
7 230
Revised OBC Space 230 192 EXTERNAL FACTORS AND POLICY CHANGES
DCAGs and Improving the Patient Experience
24 254
Sub-Total 254 SEPARATE APPROVALS Pathology/Pharmacy 13 267 Sub-Total 267 HEALTH ECONOMY/TRUST GENERATED CHANGES
48 Extra Beds and Day Case Unit 6 273 Additional Linear Accelerator 1 274 Other Net Changes 21 295 Total AT FBC PRE-DESCOPING 295 237 DESCOPING CHANGES Mothballing of 3 Floors – Type One Adjustments & Conditional Removal of Phase 2 and 3 Refurbishments – Type One Adjustments
(51)
244
245
TOTAL PSC VERSION 7 244 245
4.5.17 Of the 21,000 m2 increase from approved OBC to FBC, the changes in space
standards generated through the increase in DCAGs and Improving the Patient Experience accounted for an increase of around 24,000 m2 i.e. net decrease of 3,000 m2 taking account of changes in NHS guidance.
4.6 Benchmarking Space and Capital Cost
4.6.1 The Trust’s Quantity Surveyors (Davis Langdon) have undertaken an exercise to look across a number of schemes at capital costs and gross area per bed to identify whether the BLT New Hospitals Project appears unusual when compared to other NHS projects.
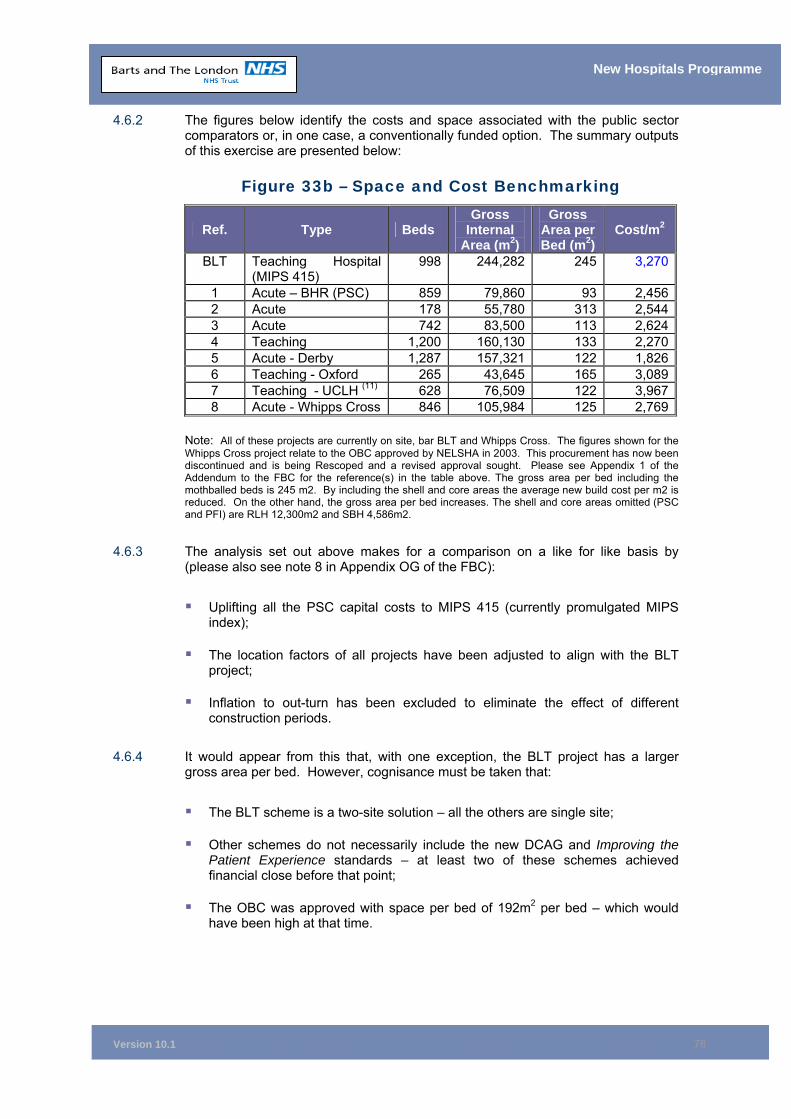
Version 10.1
78
New Hospitals Programme
4.6.2 The figures below identify the costs and space associated with the public sector comparators or, in one case, a conventionally funded option. The summary outputs of this exercise are presented below:
Figure 33b – Space and Cost Benchmarking
Ref. Type Beds Gross
Internal Area (m2)
Gross Area per Bed (m2)
Cost/m2
BLT Teaching Hospital (MIPS 415)
998 244,282 245 3,270
1 Acute – BHR (PSC) 859 79,860 93 2,4562 Acute 178 55,780 313 2,5443 Acute 742 83,500 113 2,6244 Teaching 1,200 160,130 133 2,2705 Acute - Derby 1,287 157,321 122 1,8266 Teaching - Oxford 265 43,645 165 3,0897 Teaching - UCLH (11) 628 76,509 122 3,9678 Acute - Whipps Cross 846 105,984 125 2,769
Note: All of these projects are currently on site, bar BLT and Whipps Cross. The figures shown for the Whipps Cross project relate to the OBC approved by NELSHA in 2003. This procurement has now been discontinued and is being Rescoped and a revised approval sought. Please see Appendix 1 of the Addendum to the FBC for the reference(s) in the table above. The gross area per bed including the mothballed beds is 245 m2. By including the shell and core areas the average new build cost per m2 is reduced. On the other hand, the gross area per bed increases. The shell and core areas omitted (PSC and PFI) are RLH 12,300m2 and SBH 4,586m2.
4.6.3 The analysis set out above makes for a comparison on a like for like basis by (please also see note 8 in Appendix OG of the FBC):
Uplifting all the PSC capital costs to MIPS 415 (currently promulgated MIPS
index);
The location factors of all projects have been adjusted to align with the BLT project;
Inflation to out-turn has been excluded to eliminate the effect of different
construction periods.
4.6.4 It would appear from this that, with one exception, the BLT project has a larger gross area per bed. However, cognisance must be taken that:
The BLT scheme is a two-site solution – all the others are single site;
Other schemes do not necessarily include the new DCAG and Improving the
Patient Experience standards – at least two of these schemes achieved financial close before that point;
The OBC was approved with space per bed of 192m2 per bed – which would
have been high at that time.
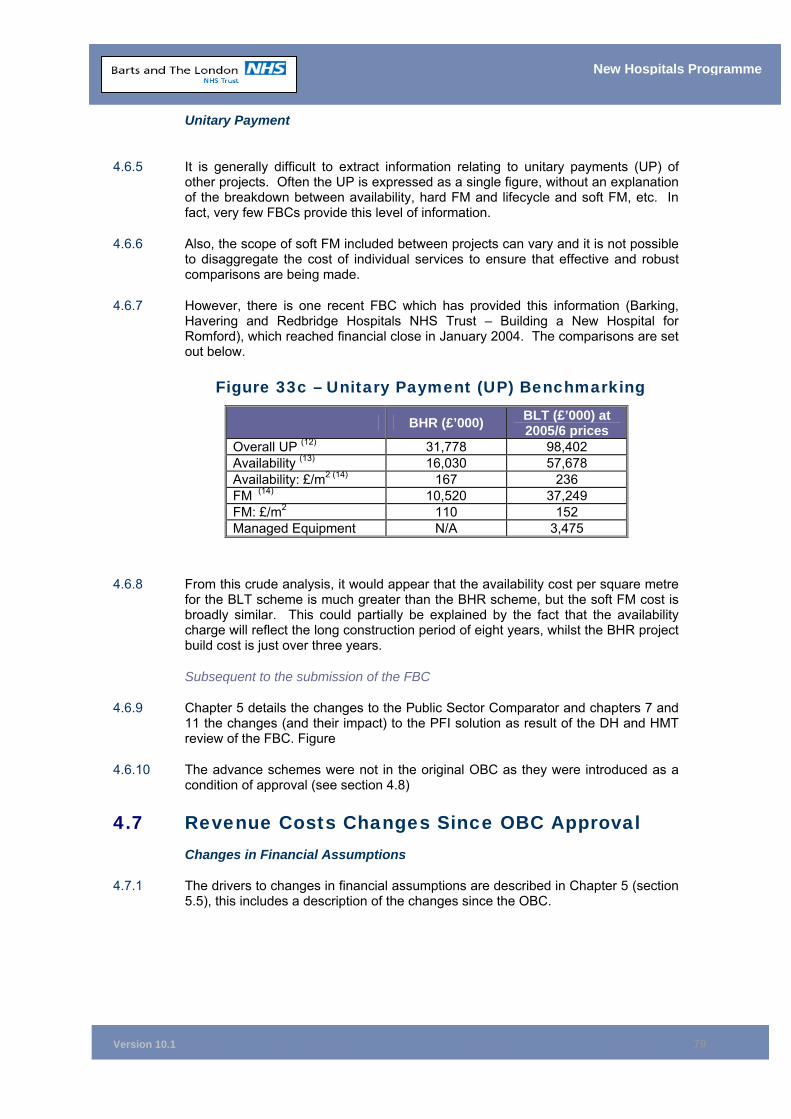
Version 10.1
79
New Hospitals Programme
Unitary Payment
4.6.5 It is generally difficult to extract information relating to unitary payments (UP) of other projects. Often the UP is expressed as a single figure, without an explanation of the breakdown between availability, hard FM and lifecycle and soft FM, etc. In fact, very few FBCs provide this level of information.
4.6.6 Also, the scope of soft FM included between projects can vary and it is not possible to disaggregate the cost of individual services to ensure that effective and robust comparisons are being made.
4.6.7 However, there is one recent FBC which has provided this information (Barking, Havering and Redbridge Hospitals NHS Trust – Building a New Hospital for Romford), which reached financial close in January 2004. The comparisons are set out below.
Figure 33c – Unitary Payment (UP) Benchmarking
BHR (£’000) BLT (£’000) at 2005/6 prices
Overall UP (12) 31,778 98,402 Availability (13) 16,030 57,678 Availability: £/m2 (14) 167 236 FM (14) 10,520 37,249 FM: £/m2 110 152 Managed Equipment N/A 3,475
4.6.8 From this crude analysis, it would appear that the availability cost per square metre for the BLT scheme is much greater than the BHR scheme, but the soft FM cost is broadly similar. This could partially be explained by the fact that the availability charge will reflect the long construction period of eight years, whilst the BHR project build cost is just over three years.
Subsequent to the submission of the FBC
4.6.9 Chapter 5 details the changes to the Public Sector Comparator and chapters 7 and 11 the changes (and their impact) to the PFI solution as result of the DH and HMT review of the FBC. Figure
4.6.10 The advance schemes were not in the original OBC as they were introduced as a condition of approval (see section 4.8)
4.7 Revenue Costs Changes Since OBC Approval Changes in Financial Assumptions
4.7.1 The drivers to changes in financial assumptions are described in Chapter 5 (section 5.5), this includes a description of the changes since the OBC.
Version 10.1
80
New Hospitals Programme
4.8 Advance Schemes 4.8.1 Ahead of the main PFI build, the Trust has undertaken three separate building
projects, together with a major decant scheme, to provide accommodation for relocating services. These are:
■ The construction of a new Pathology and Pharmacy building at The Royal London;
■ The refurbishment of the West Wing at Barts; and
■ The refurbishment of the Kenton and Lucas block at Barts.
4.8.2 The principal aim of the advance schemes was to reduce the overall development timetable thereby reducing costs and the complexity of the construction and decant programmes. The advance schemes provide a substantially vacated area at the eastern end of The Royal London site. At Barts, they allow for services to be decanted from the Horder Wing at the start of the main development programme. All three of the advance schemes are funded through a combination of NHS capital and charitable funds and do not form part of this business case. In addition, the funding for the decant schemes was also approved as a separate business case. The decant schemes provide temporary accommodation over the nine year construction period. Key decant schemes are off site office accommodation at Prescot Street and office accommodation in John Harrison House.
4.8.3 These schemes were the subject of separate business cases totalling £83 million. These business cases were approved by the London Regional Office in November 200166 and the schemes are either complete or near completion.
Pathology and Pharmacy - RLH
4.8.4 The new Pathology and Pharmacy block at The Royal London was commissioned in January 2006. All the Trust’s RLH pathology and pharmacy services are centralised in this building.
4.8.5 As the existing buildings housing Pathology and Pharmacy staff are not in the footprint of the hospitals redevelopment programme, the commissioning, occupation and decant programme for Pathology and Pharmacy has no impact on the main scheme.
West Wing - Barts
4.8.6 The West Wing at Barts has been refurbished and developed to bring together all the Trust’s breast care, diagnostic and screening services in a patient environment to rival the best in the world. Opened in September 2004, it provides state of the art digital mammography technology and co-located services.
Kenton and Lucas - Barts
4.8.7 The Kenton and Lucas block at Barts has been refurbished. Three discrete Trust services, an integrated rehabilitation unit (the Sexual Health Service and the Centre for Reproductive Medicine) moved into the building between January and June 2004. Each has its own separate entrance and provides an environment appropriate to the client needs. Sexual health and reproductive medicine will continue to be provided from the recently refurbished accommodation. Barts will
66 The Pathology and Pharmacy Scheme was subject to DH approval. Received in January 2002
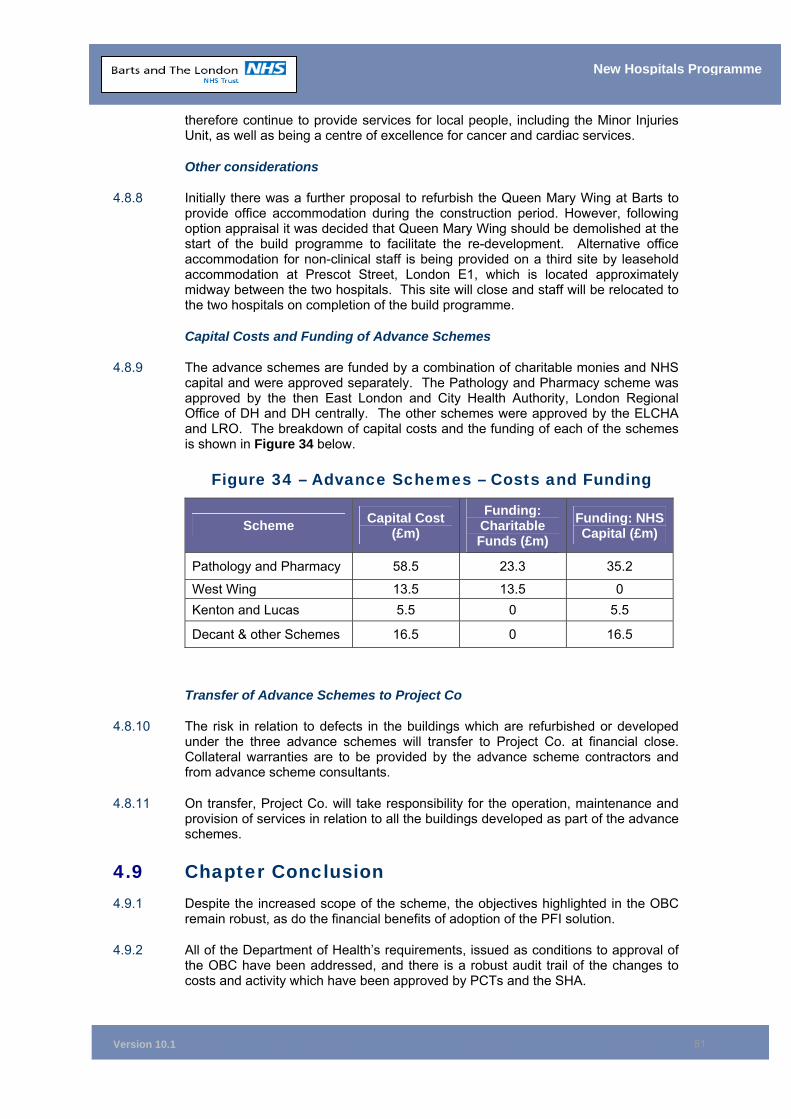
Version 10.1
81
New Hospitals Programme
therefore continue to provide services for local people, including the Minor Injuries Unit, as well as being a centre of excellence for cancer and cardiac services.
Other considerations
4.8.8 Initially there was a further proposal to refurbish the Queen Mary Wing at Barts to provide office accommodation during the construction period. However, following option appraisal it was decided that Queen Mary Wing should be demolished at the start of the build programme to facilitate the re-development. Alternative office accommodation for non-clinical staff is being provided on a third site by leasehold accommodation at Prescot Street, London E1, which is located approximately midway between the two hospitals. This site will close and staff will be relocated to the two hospitals on completion of the build programme.
Capital Costs and Funding of Advance Schemes
4.8.9 The advance schemes are funded by a combination of charitable monies and NHS capital and were approved separately. The Pathology and Pharmacy scheme was approved by the then East London and City Health Authority, London Regional Office of DH and DH centrally. The other schemes were approved by the ELCHA and LRO. The breakdown of capital costs and the funding of each of the schemes is shown in Figure 34 below.
Figure 34 – Advance Schemes – Costs and Funding
Scheme Capital Cost (£m)
Funding: Charitable Funds (£m)
Funding: NHS Capital (£m)
Pathology and Pharmacy 58.5 23.3 35.2
West Wing 13.5 13.5 0 Kenton and Lucas 5.5 0 5.5
Decant & other Schemes 16.5 0 16.5
Transfer of Advance Schemes to Project Co
4.8.10 The risk in relation to defects in the buildings which are refurbished or developed under the three advance schemes will transfer to Project Co. at financial close. Collateral warranties are to be provided by the advance scheme contractors and from advance scheme consultants.
4.8.11 On transfer, Project Co. will take responsibility for the operation, maintenance and provision of services in relation to all the buildings developed as part of the advance schemes.
4.9 Chapter Conclusion 4.9.1 Despite the increased scope of the scheme, the objectives highlighted in the OBC
remain robust, as do the financial benefits of adoption of the PFI solution.
4.9.2 All of the Department of Health’s requirements, issued as conditions to approval of the OBC have been addressed, and there is a robust audit trail of the changes to costs and activity which have been approved by PCTs and the SHA.
Version 10.1
82
New Hospitals Programme
4.10 Chapter Appendices 4A Trust Response to OBC Approval Recommendations 4B Audit Trail of Changes to Bed Numbers 4C Activity Modelling for All Specialities 4D Full Activity/Bed Specialty Audit Trail from CDP/OBC to FBC 4E Appendix Reference Not Used 4F OBC Approval Letters
Version 10.1
83
New Hospitals Programme
5 THE PUBLIC SECTOR COMPARATOR Synopsis – Public Sector Comparator (PSC)
This chapter provides:
■ An explanation of the fully costed and updated PSC, forming the baseline against which the private finance initiative (PFI) scheme has been evaluated;
■ Supporting information in respect of the assumptions which underpin the PSC;
■ A description of the changes since the Outline Business Case (OBC) and an explanation of the updated capital costs (£799 million at MIPS 415 VOP) and outturn costs of £967 million (including VAT). The PSC version 7 as described in this chapter includes the changes from the December 2005 FBC (version 9) following the review of the business case by DH & HMT. Thus PSC 7 includes the impact of the type 1 Descoping adjustments (mothballing of 250 beds and non refurbishment of certain phase 2 and 3 buildings);
■ A description of the changes since the Outline Business Case (OBC) and an explanation of the updated capital costs (£751 million (MIPS 415 VOP) and outturn costs of £908 million at out-turn, £967 million (including VAT), PSC version 7 as described in this chapter includes the changes from the December 2995 FBC (version 9) following the review of the business case by DH &HMT. Thus PSC7 includes the impact of the type 1 descoping adjustments (mothballing of 250 beds and non refurbishment of certain phase 2 and 3 buildings); and
■ The detail of the revenue costs associated with the PSC.
5.1 Introduction 5.1.1 The PSC represents the developed expression of the Trust’s design requirements
and provides a publicly financed benchmark against which the PFI solution has been assessed in terms of value for money (VfM) and clinical and overall functionality.
5.2 Description of the PSC 5.2.1 The PSC has been amended considerably to reflect the changes to the scheme that
have had to be accommodated since the approval of the OBC. This has ensured that it continues to provide an appropriate benchmark for assessing bids and, in the latter stages the preferred PFI solution, in terms of VfM, together with clinical and overall functionality.
5.2.2 The PSC seeks to give effect to the OBC, taking into account the developments identified at the time of approval of the OBC (e.g. the Clinical Development Plan (CDP)) and subsequent events such as Thames Gateway and the planning requirements of the Greater London Authority. In summary, the PSC reflects:
• A reconfiguration of services to provide a critical mass of key services on the respective sites, with Barts becoming a dedicated Cancer and Cardiac Centre and The London Chest Hospital becoming surplus;

Version 10.1
84
New Hospitals Programme
• Development of new service models of care;
• Creation of a new generation of state-of-the-art hospitals referred to in the NHS Plan;
• An increase in the number of single rooms in response to the consumerism guidance;
• A more strategic layout to The Royal London site, with an improved overall internal and external appearance;
• An improved layout at the Barts site, while maintaining the listed buildings and improving the environment within the square;
• Improved physical integration of services;
• Improved quality of patient accommodation for adults and children in line with the consumerism agenda;
• Improved quality and configuration of accommodation and the elimination of £46 million (MIPS 415) backlog maintenance on the two sites;
• A dedicated Ambulatory Care and Diagnostic Treatment Centre; and
• The provision of a range of non-clinical services and a structured lifecycle programme.
• The PSC at May 2006 (PSC 7) has been updated to reflect impact of the type 1 descoping adjustments (mothballing of 250 beds and non refurbishment of certain phase 2 and 3 buildings)
5.2.3 The total capital cost (including VAT) for the PSC is now £967 million (at out-turn). A reconciliation of OBC to PSC capital costs is included in section 5.15.
5.2.4 Figure 35 details new and refurbished facilities on both sites.
Figure 35 – New and Refurbished Facilities
New Hospitals Programme
Royal London Site (905 beds but 192 mothballed)
New Build £551m for the initial construction
phase of the main blocks together with £19m for phase two.
The total gross floor area for the new build is 263000m². See Estates Annex
E2.
Refurbishment£88m for the refurbishment of
properties primarily to the west of the site.
Barts Site (343 beds but 58 mothballed)
New Build £142m for the demolition of both
Horder and Queen Mary Wings and the construction of new blocks on these
sites.
Refurbishment£104m for the refurbishment of the
remaining sites other than Queen Mary and Horder Wings. The most
significant in cost being King George V Block.
5.2.5 The above totals £906 million. To this is added £2 million for the off-site catering
refurbishment and £61 million for equipment, giving a total of £967 million at out-turn excluding advance schemes.67
67 Further details of the costs are provided in Estates Annex Ref E9

Version 10.1
85
New Hospitals Programme
5.3 Phasing for the PSC 5.3.1 The PSC is a phased solution due to the complexity of the sites and the need to
maintain operational hospitals throughout the construction period. The key phases are outlined in Figure 36.
Figure 36 – Key Opening Dates
Enabling Works 2003/2005
Contract Award 2005/6 New Build of Blocks A B C - The Royal London Site 2010/11 Adaptation of Front Block etc - The Royal London Site 2012/13 New Build Car Park - The Royal London Site 2013/14 New Build QMW - Barts Site 2008/9 New Build Horder - Barts Site 2010/11 Adaptation of Pathology/OPD – Barts Site68 2008/9
5.4 Calculation of the PSC – Capital Costs Methodology
5.4.1 The capital costs for the PSC have been calculated adopting the approach outlined in How to Cost a Hospital, dated June 2001, as published by NHS Estates.
5.4.2 The costs are based on the Trust’s output specifications and operational policies, included within the Invitation to Negotiate (ITN). These have been priced using DH Departmental Cost Allowance Guides (DCAGs), as set out within the Healthcare Capital Investment (HCI) publication (version 2.0).
5.5 Changes Following OBC 5.5.1 The OBC was submitted in November 1999 and received approval in February
2000. Following approval of the OBC, the PSC has been developed in order to respond to several drivers for change, which are listed below and discussed in more detail in Chapter 4:
• The Clinical Development Plan;
• National Service Frameworks (NSFs);
• NBI Growth/Access, Booking and Choice – Plurality;
• Consumerism;
• The NHS Plan;
• Thames Gateway;
• Long-Term Conditions Management;
• Independent Sector Treatment Centres;
• Equipment to Support Service Changes; and
• Descoping of the scheme following the review of the business case by the DH and HMT.
68 In the PSC the Pathology Block would be used for: (In approx order of size, starting with biggest function) - General Pathology, Admin, Medical School embedded space, Medical School Museum, Medical School Library, Mortuary, Medical Photography.
Version 10.1
86
New Hospitals Programme
Delivery of the New Hospitals
5.5.2 In view of the scale and complexity of the scheme, another key driver was the timing of the delivery of the new hospitals and the costs involved.
5.5.3 As a consequence, approval of the OBC was conditional on the Trust reviewing the phasing of the scheme, in order to provide for earlier delivery of the project.
5.5.4 Following this review, it was determined that undertaking a number of enabling works would assist the development and facilitate the availability of the main footprint of the new build for an early start on site. This would additionally assist with the decanting problems.
5.5.5 The Trust has reworked the OBC in order to address this. The proposals were approved as part of the addendum OBC, the advance schemes FBC and the Pathology and Pharmacy FBC. Chapter 4 provides further detail in respect of the scope and timing of the advance works.
5.5.6 Earlier completion of the new hospitals can be achieved as the advance schemes enable the Trust to provide a significantly larger vacant site to the private sector at financial close than was proposed at OBC. This enables a much larger first phase of construction.
5.5.7 The advance schemes referred to are:
West Wing
5.5.8 This is the development of a specialist Cancer Centre (primarily breast cancer) on the Barts site. The FBC for this project was approved in 2001. The development is now complete and has been operational since September 2004.
Kenton and Lucas
5.5.9 This is the development of a Therapies, Fertility and Sexual Health Centre on the Barts site. The FBC for this project was approved in 2001. The development is now complete and has been operational since September 2004.
Pathology and Pharmacy
5.5.10 This is the construction of a new building, which will consolidate both the Pathology and Pharmacy functions on The Royal London site. The FBC for this project was approved in January 2002. The development is now underway with an expected operational date of January 2006.
Decant Facilities
5.5.11 These provide both on and off-site accommodation for Trust staff, freeing up on-site buildings either for site-essential staff decants or for early demolition/refurbishment. The FBC for this project was approved in May 2003 with a subsequent addendum approval of the FBC in May 2005. The off-site development is now complete and has been operational since March 2004. It is primarily office space based in Prescot Street, near Aldgate. The Trust’s medical simulator is also based at Prescot Street.
5.5.12 On-site facilities are being provided in areas which are peripheral and are not within the footprint of the Phase 1 buildings. At The Royal London site this is primarily John Harrison House which is providing office accommodation. At Barts work is
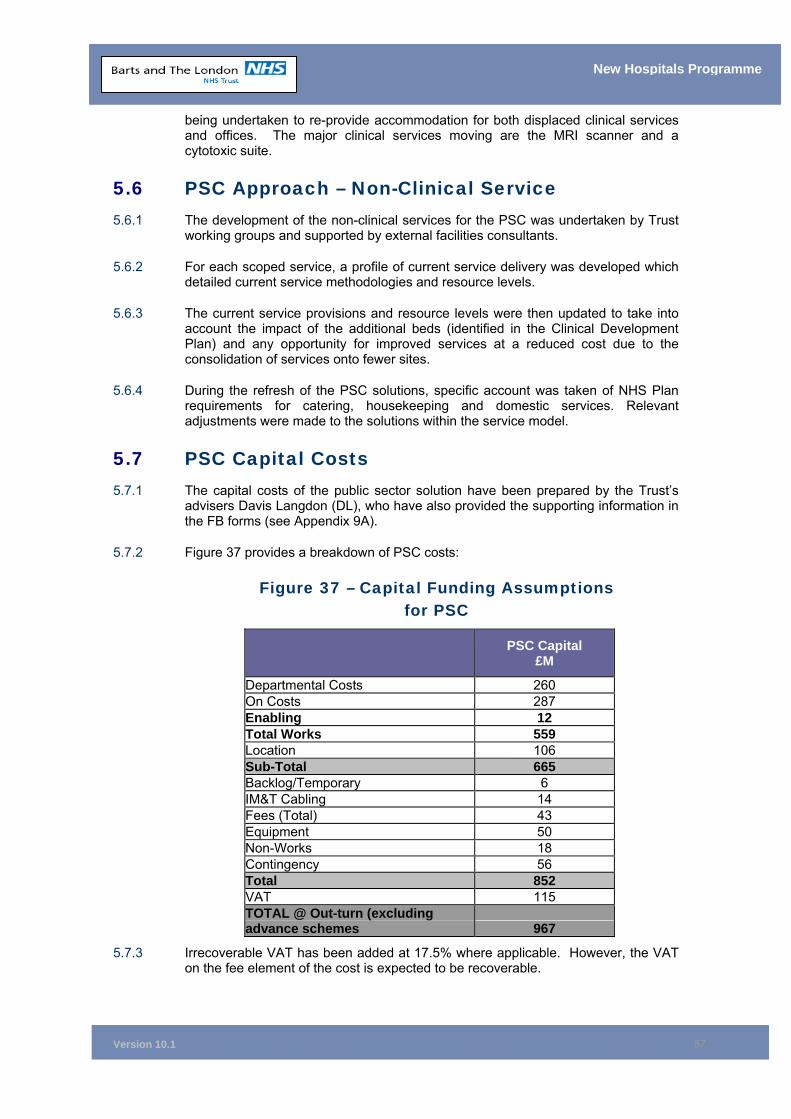
Version 10.1
87
New Hospitals Programme
being undertaken to re-provide accommodation for both displaced clinical services and offices. The major clinical services moving are the MRI scanner and a cytotoxic suite.
5.6 PSC Approach – Non-Clinical Service 5.6.1 The development of the non-clinical services for the PSC was undertaken by Trust
working groups and supported by external facilities consultants.
5.6.2 For each scoped service, a profile of current service delivery was developed which detailed current service methodologies and resource levels.
5.6.3 The current service provisions and resource levels were then updated to take into account the impact of the additional beds (identified in the Clinical Development Plan) and any opportunity for improved services at a reduced cost due to the consolidation of services onto fewer sites.
5.6.4 During the refresh of the PSC solutions, specific account was taken of NHS Plan requirements for catering, housekeeping and domestic services. Relevant adjustments were made to the solutions within the service model.
5.7 PSC Capital Costs 5.7.1 The capital costs of the public sector solution have been prepared by the Trust’s
advisers Davis Langdon (DL), who have also provided the supporting information in the FB forms (see Appendix 9A).
5.7.2 Figure 37 provides a breakdown of PSC costs:
Figure 37 – Capital Funding Assumptions for PSC
PSC Capital
£M
Departmental Costs 260 On Costs 287 Enabling 12 Total Works 559 Location 106 Sub-Total 665 Backlog/Temporary 6 IM&T Cabling 14 Fees (Total) 43 Equipment 50 Non-Works 18 Contingency 56 Total 852 VAT 115 TOTAL @ Out-turn (excluding advance schemes 967
5.7.3 Irrecoverable VAT has been added at 17.5% where applicable. However, the VAT on the fee element of the cost is expected to be recoverable.
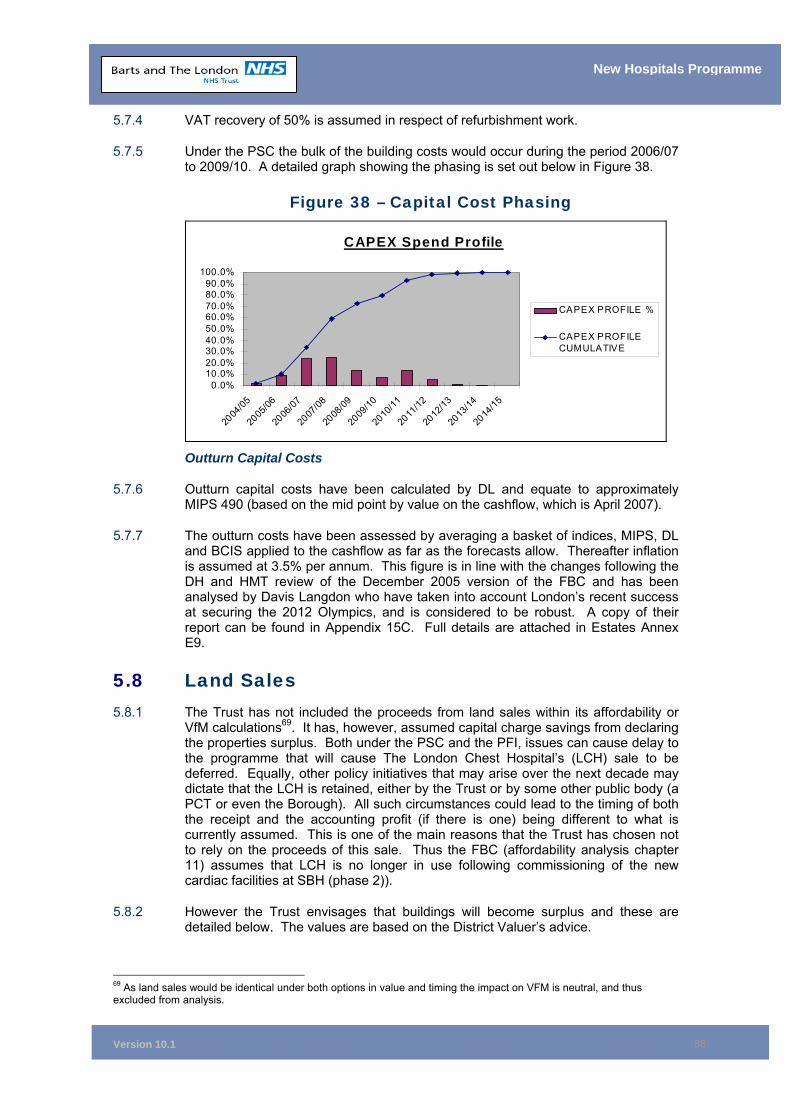
Version 10.1
88
New Hospitals Programme
5.7.4 VAT recovery of 50% is assumed in respect of refurbishment work.
5.7.5 Under the PSC the bulk of the building costs would occur during the period 2006/07 to 2009/10. A detailed graph showing the phasing is set out below in Figure 38.
Figure 38 – Capital Cost Phasing
CAPEX Spend Profile
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%90.0%
100.0%
2004
/05
2005
/06
2006
/07
2007
/08
2008
/09
2009
/10
2010
/11
2011
/12
2012
/13
2013
/14
2014
/15
CAPEX PROFILE %
CAPEX PROFILECUMULATIVE
Outturn Capital Costs
5.7.6 Outturn capital costs have been calculated by DL and equate to approximately MIPS 490 (based on the mid point by value on the cashflow, which is April 2007).
5.7.7 The outturn costs have been assessed by averaging a basket of indices, MIPS, DL and BCIS applied to the cashflow as far as the forecasts allow. Thereafter inflation is assumed at 3.5% per annum. This figure is in line with the changes following the DH and HMT review of the December 2005 version of the FBC and has been analysed by Davis Langdon who have taken into account London’s recent success at securing the 2012 Olympics, and is considered to be robust. A copy of their report can be found in Appendix 15C. Full details are attached in Estates Annex E9.
5.8 Land Sales 5.8.1 The Trust has not included the proceeds from land sales within its affordability or
VfM calculations69. It has, however, assumed capital charge savings from declaring the properties surplus. Both under the PSC and the PFI, issues can cause delay to the programme that will cause The London Chest Hospital’s (LCH) sale to be deferred. Equally, other policy initiatives that may arise over the next decade may dictate that the LCH is retained, either by the Trust or by some other public body (a PCT or even the Borough). All such circumstances could lead to the timing of both the receipt and the accounting profit (if there is one) being different to what is currently assumed. This is one of the main reasons that the Trust has chosen not to rely on the proceeds of this sale. Thus the FBC (affordability analysis chapter 11) assumes that LCH is no longer in use following commissioning of the new cardiac facilities at SBH (phase 2)).
5.8.2 However the Trust envisages that buildings will become surplus and these are detailed below. The values are based on the District Valuer’s advice.
69 As land sales would be identical under both options in value and timing the impact on VFM is neutral, and thus excluded from analysis.
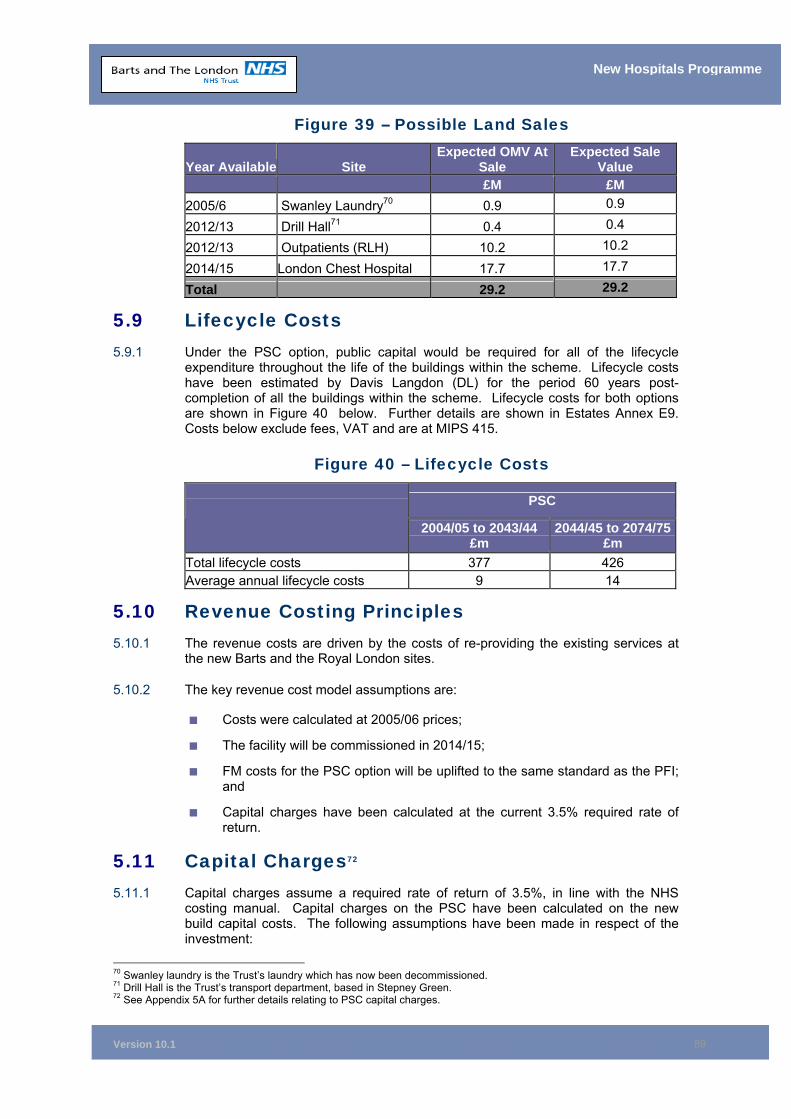
Version 10.1
89
New Hospitals Programme
Figure 39 – Possible Land Sales
Year Available Site Expected OMV At
Sale Expected Sale
Value £M £M
2005/6 Swanley Laundry70 0.9 0.9
2012/13 Drill Hall71 0.4 0.4
2012/13 Outpatients (RLH) 10.2 10.2
2014/15 London Chest Hospital 17.7 17.7
Total 29.2 29.2
5.9 Lifecycle Costs 5.9.1 Under the PSC option, public capital would be required for all of the lifecycle
expenditure throughout the life of the buildings within the scheme. Lifecycle costs have been estimated by Davis Langdon (DL) for the period 60 years post-completion of all the buildings within the scheme. Lifecycle costs for both options are shown in Figure 40 below. Further details are shown in Estates Annex E9. Costs below exclude fees, VAT and are at MIPS 415.
Figure 40 – Lifecycle Costs
PSC
2004/05 to 2043/44 £m
2044/45 to 2074/75£m
Total lifecycle costs 377 426 Average annual lifecycle costs 9 14
5.10 Revenue Costing Principles 5.10.1 The revenue costs are driven by the costs of re-providing the existing services at
the new Barts and the Royal London sites.
5.10.2 The key revenue cost model assumptions are:
■ Costs were calculated at 2005/06 prices;
■ The facility will be commissioned in 2014/15;
■ FM costs for the PSC option will be uplifted to the same standard as the PFI; and
■ Capital charges have been calculated at the current 3.5% required rate of return.
5.11 Capital Charges72 5.11.1 Capital charges assume a required rate of return of 3.5%, in line with the NHS
costing manual. Capital charges on the PSC have been calculated on the new build capital costs. The following assumptions have been made in respect of the investment:
70 Swanley laundry is the Trust’s laundry which has now been decommissioned. 71 Drill Hall is the Trust’s transport department, based in Stepney Green. 72 See Appendix 5A for further details relating to PSC capital charges.
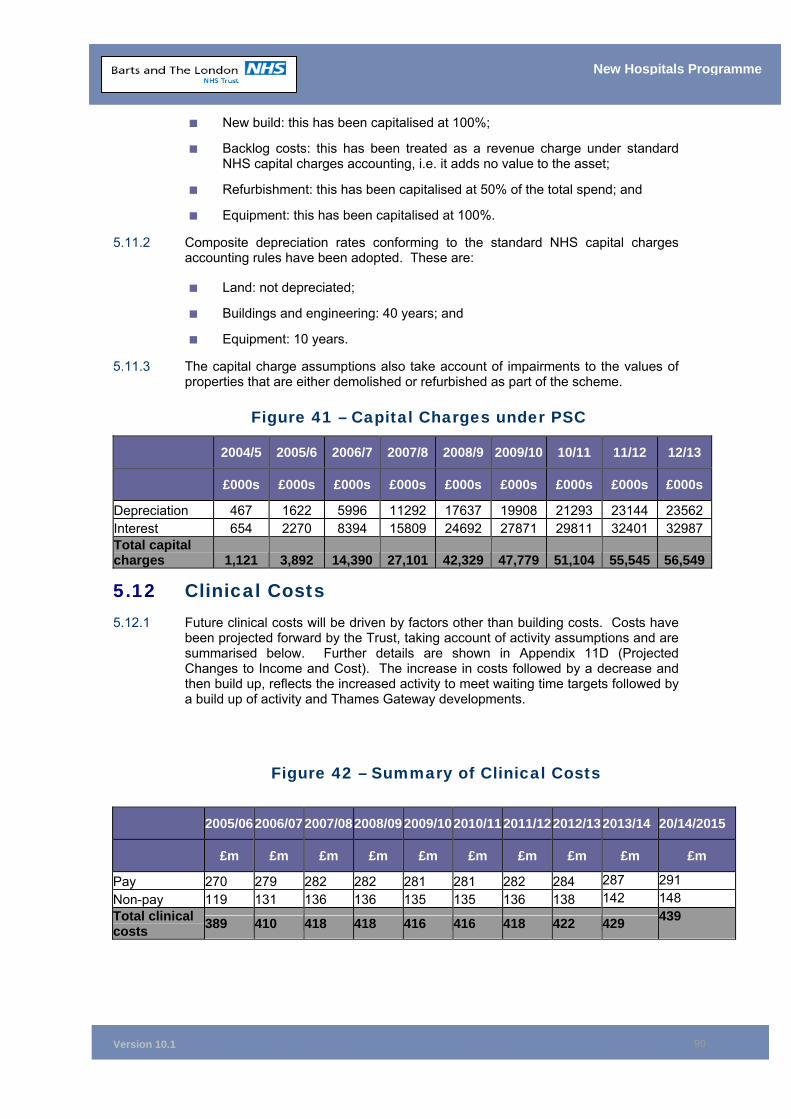
Version 10.1
90
New Hospitals Programme
■ New build: this has been capitalised at 100%;
■ Backlog costs: this has been treated as a revenue charge under standard NHS capital charges accounting, i.e. it adds no value to the asset;
■ Refurbishment: this has been capitalised at 50% of the total spend; and
■ Equipment: this has been capitalised at 100%.
5.11.2 Composite depreciation rates conforming to the standard NHS capital charges accounting rules have been adopted. These are:
■ Land: not depreciated;
■ Buildings and engineering: 40 years; and
■ Equipment: 10 years.
5.11.3 The capital charge assumptions also take account of impairments to the values of properties that are either demolished or refurbished as part of the scheme.
Figure 41 – Capital Charges under PSC
2004/5 2005/6 2006/7 2007/8 2008/9 2009/10 10/11 11/12 12/13
£000s £000s £000s £000s £000s £000s £000s £000s £000s
Depreciation 467 1622 5996 11292 17637 19908 21293 23144 23562 Interest 654 2270 8394 15809 24692 27871 29811 32401 32987 Total capital charges 1,121 3,892 14,390 27,101 42,329 47,779 51,104 55,545 56,549
5.12 Clinical Costs 5.12.1 Future clinical costs will be driven by factors other than building costs. Costs have
been projected forward by the Trust, taking account of activity assumptions and are summarised below. Further details are shown in Appendix 11D (Projected Changes to Income and Cost). The increase in costs followed by a decrease and then build up, reflects the increased activity to meet waiting time targets followed by a build up of activity and Thames Gateway developments.
Figure 42 – Summary of Clinical Costs
2005/06 2006/07 2007/082008/092009/102010/112011/122012/13 2013/14 20/14/2015
£m £m £m £m £m £m £m £m £m £m
Pay 270 279 282 282 281 281 282 284 287 291 Non-pay 119 131 136 136 135 135 136 138 142 148 Total clinical costs 389 410 418 418 416 416 418 422 429 439
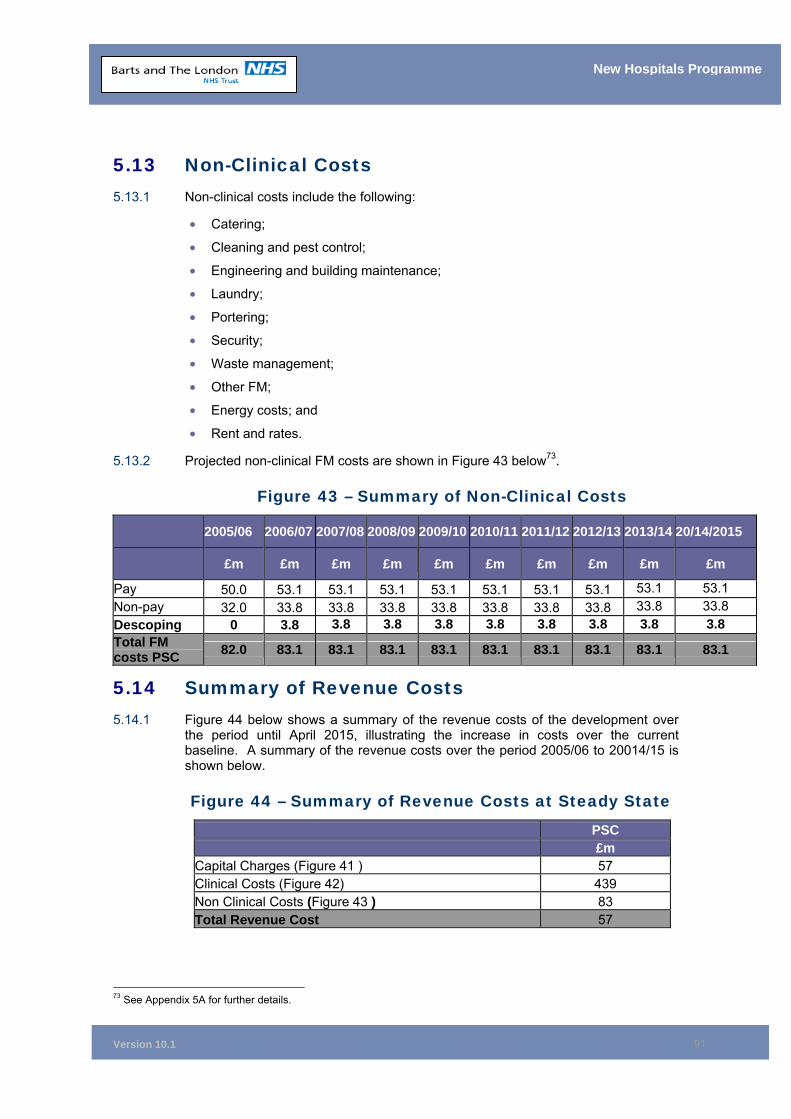
Version 10.1
91
New Hospitals Programme
5.13 Non-Clinical Costs 5.13.1 Non-clinical costs include the following:
• Catering;
• Cleaning and pest control;
• Engineering and building maintenance;
• Laundry;
• Portering;
• Security;
• Waste management;
• Other FM;
• Energy costs; and
• Rent and rates.
5.13.2 Projected non-clinical FM costs are shown in Figure 43 below73.
Figure 43 – Summary of Non-Clinical Costs
2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14 20/14/2015
£m £m £m £m £m £m £m £m £m £m
Pay 50.0 53.1 53.1 53.1 53.1 53.1 53.1 53.1 53.1 53.1 Non-pay 32.0 33.8 33.8 33.8 33.8 33.8 33.8 33.8 33.8 33.8 Descoping 0 3.8 3.8 3.8 3.8 3.8 3.8 3.8 3.8 3.8 Total FM costs PSC 82.0 83.1 83.1 83.1 83.1 83.1 83.1 83.1 83.1 83.1
5.14 Summary of Revenue Costs 5.14.1 Figure 44 below shows a summary of the revenue costs of the development over
the period until April 2015, illustrating the increase in costs over the current baseline. A summary of the revenue costs over the period 2005/06 to 20014/15 is shown below.
Figure 44 – Summary of Revenue Costs at Steady State
PSC £m
Capital Charges (Figure 41 ) 57 Clinical Costs (Figure 42) 439 Non Clinical Costs (Figure 43 ) 83 Total Revenue Cost 57
73 See Appendix 5A for further details.
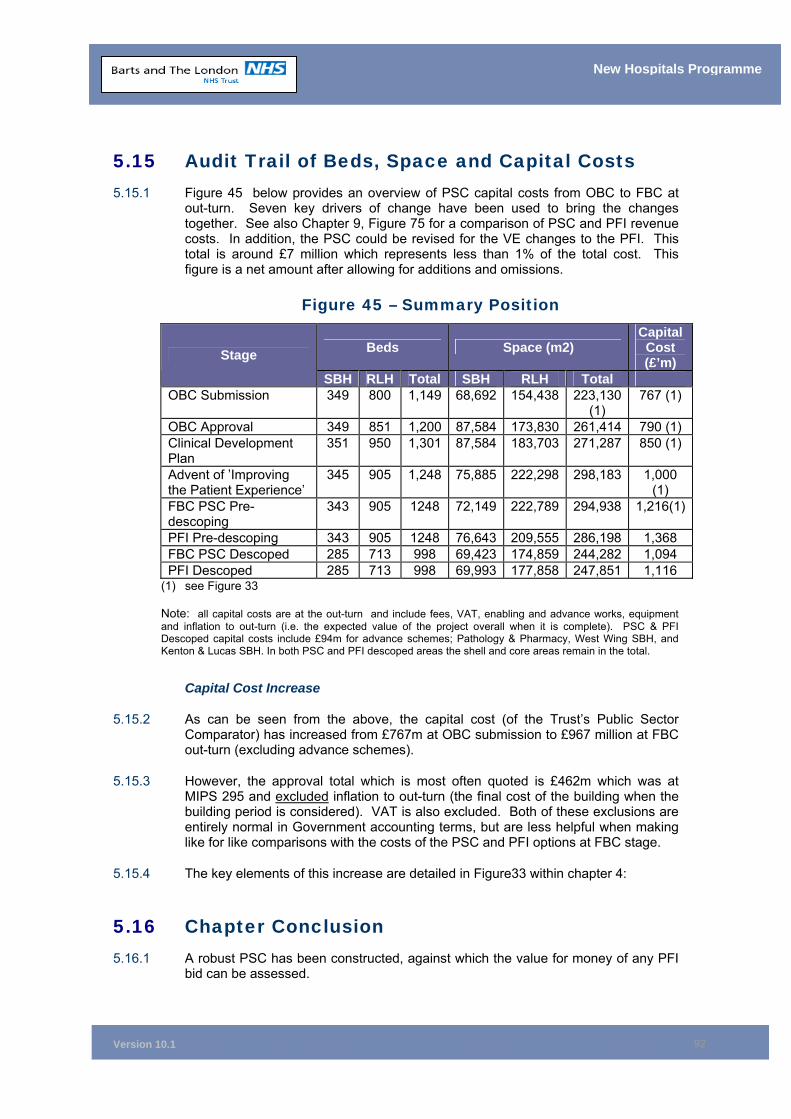
Version 10.1
92
New Hospitals Programme
5.15 Audit Trail of Beds, Space and Capital Costs 5.15.1 Figure 45 below provides an overview of PSC capital costs from OBC to FBC at
out-turn. Seven key drivers of change have been used to bring the changes together. See also Chapter 9, Figure 75 for a comparison of PSC and PFI revenue costs. In addition, the PSC could be revised for the VE changes to the PFI. This total is around £7 million which represents less than 1% of the total cost. This figure is a net amount after allowing for additions and omissions.
Figure 45 – Summary Position
Beds Space (m2) Capital
Cost (£’m) Stage
SBH RLH Total SBH RLH Total OBC Submission 349 800 1,149 68,692 154,438 223,130
(1) 767 (1)
OBC Approval 349 851 1,200 87,584 173,830 261,414 790 (1) Clinical Development Plan
351 950 1,301 87,584 183,703 271,287 850 (1)
Advent of ’Improving the Patient Experience’
345 905 1,248 75,885 222,298 298,183 1,000 (1)
FBC PSC Pre-descoping
343 905 1248 72,149 222,789 294,938 1,216(1)
PFI Pre-descoping 343 905 1248 76,643 209,555 286,198 1,368 FBC PSC Descoped 285 713 998 69,423 174,859 244,282 1,094 PFI Descoped 285 713 998 69,993 177,858 247,851 1,116
(1) see Figure 33 Note: all capital costs are at the out-turn and include fees, VAT, enabling and advance works, equipment and inflation to out-turn (i.e. the expected value of the project overall when it is complete). PSC & PFI Descoped capital costs include £94m for advance schemes; Pathology & Pharmacy, West Wing SBH, and Kenton & Lucas SBH. In both PSC and PFI descoped areas the shell and core areas remain in the total.
Capital Cost Increase
5.15.2 As can be seen from the above, the capital cost (of the Trust’s Public Sector Comparator) has increased from £767m at OBC submission to £967 million at FBC out-turn (excluding advance schemes).
5.15.3 However, the approval total which is most often quoted is £462m which was at MIPS 295 and excluded inflation to out-turn (the final cost of the building when the building period is considered). VAT is also excluded. Both of these exclusions are entirely normal in Government accounting terms, but are less helpful when making like for like comparisons with the costs of the PSC and PFI options at FBC stage.
5.15.4 The key elements of this increase are detailed in Figure33 within chapter 4:
5.16 Chapter Conclusion 5.16.1 A robust PSC has been constructed, against which the value for money of any PFI
bid can be assessed.
Version 10.1
93
New Hospitals Programme
5.16.2 A detailed audit trail has also been maintained, showing all changes since the OBC was approved in 2000. The apparently large increase in capital cost of the scheme over the past five years has been fully justified in this analysis.
5.17 Chapter Appendices 5A Capital Charges 5B Comparison of Beds, Space and Costs
Version 10.1
94
New Hospitals Programme
6 THE PFI PROCUREMENT PROCESS Synopsis – The PFI Procurement Process
This chapter:
• Describes the structure of the project;
• Details the process of procurement and confirms that it has been conducted in accordance with legislation and all relevant guidance;
• Confirms the detail of the process employed for evaluation of the bids, which was robust and subject to audit opinion and approval;
• Confirms the substantial involvement of staff in the analysis and evaluation of the bids;
• Describes the best and final offer (BaFO) process from beginning to end, including the evaluation methodology employed;
• Describes the process employed in the finalisation of the contract negotiations with the preferred bidder; and
• Confirms that the procurement process has been subject to and under the scrutiny of, the Trust’s internal audit processes.
6.1 Introduction 6.1.1 This chapter sets out the procedures that the Trust has undertaken in the
management of the procurement process and verifies that the scheme has progressed through the various stages of the project in accordance with Government regulations and good practice.
6.2 Outline of the Scheme 6.2.1 Although the scheme started out as a single project to redevelop both The Royal
London (RLH) and the St Bartholomew’s (SBH) sites, the need to undertake a number of advance works to facilitate the main PFI project and to assist in the delivery of the necessary decant programme, meant that the scheme has developed into a programme of works consisting of the following projects.
• The main private finance initiative (PFI) project;
• The delivery of a new Pathology and Pharmacy (P&P) building at the Royal London;
• The West Wing and Kenton & Lucas advance schemes at Barts; and
• The necessary works to deliver the pre-Phase 1 decant programme.
6.2.2 Each of these projects is, or has been, governed by its own Project Board which, in turn is, or has been, accountable to the New Hospitals Programme Board (NHPB) and the New Hospitals Programme Investment Board (NHPIB).
6.2.3 This chapter focuses on the process employed for the procurement of the main PFI project.
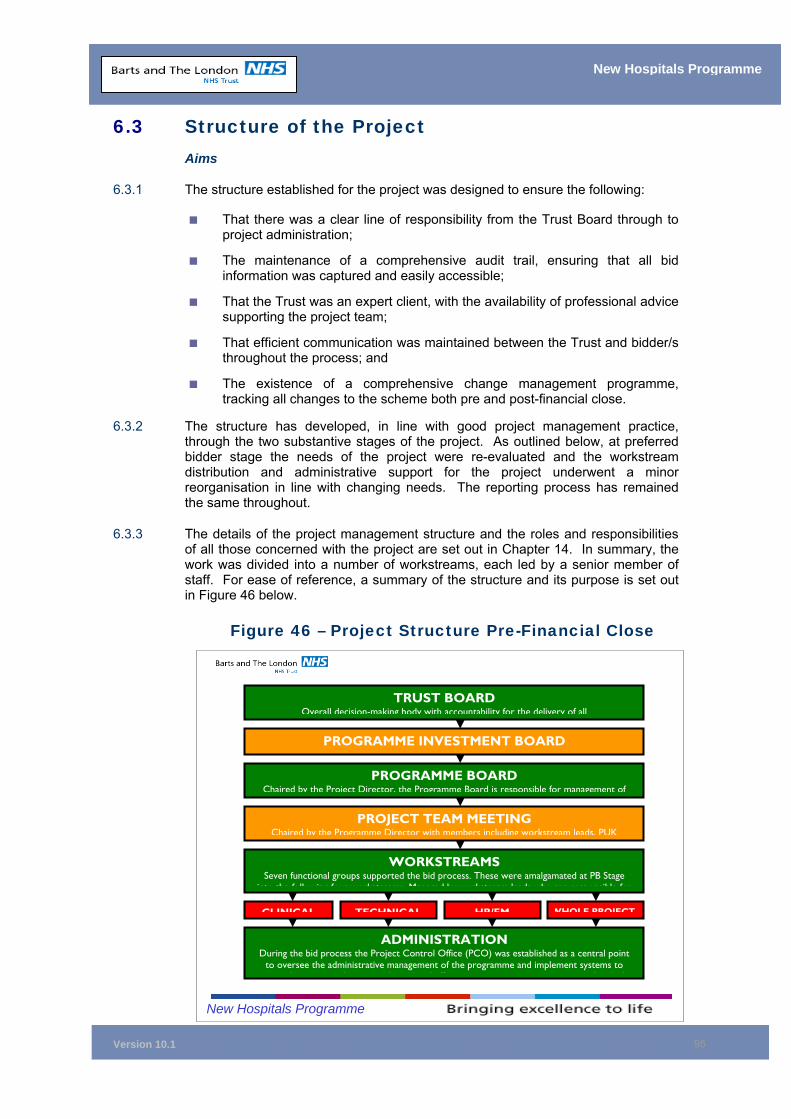
Version 10.1
95
New Hospitals Programme
6.3 Structure of the Project Aims
6.3.1 The structure established for the project was designed to ensure the following:
■ That there was a clear line of responsibility from the Trust Board through to project administration;
■ The maintenance of a comprehensive audit trail, ensuring that all bid information was captured and easily accessible;
■ That the Trust was an expert client, with the availability of professional advice supporting the project team;
■ That efficient communication was maintained between the Trust and bidder/s throughout the process; and
■ The existence of a comprehensive change management programme, tracking all changes to the scheme both pre and post-financial close.
6.3.2 The structure has developed, in line with good project management practice, through the two substantive stages of the project. As outlined below, at preferred bidder stage the needs of the project were re-evaluated and the workstream distribution and administrative support for the project underwent a minor reorganisation in line with changing needs. The reporting process has remained the same throughout.
6.3.3 The details of the project management structure and the roles and responsibilities of all those concerned with the project are set out in Chapter 14. In summary, the work was divided into a number of workstreams, each led by a senior member of staff. For ease of reference, a summary of the structure and its purpose is set out in Figure 46 below.
Figure 46 – Project Structure Pre-Financial Close
TRUST BOARD Overall decision-making body with accountability for the delivery of all
PROGRAMME INVESTMENT BOARD
PROGRAMME BOARD Chaired by the Project Director, the Programme Board is responsible for management of
PROJECT TEAM MEETING Chaired by the Programme Director with members including workstream leads, PUK
WORKSTREAMS Seven functional groups supported the bid process. These were amalgamated at PB Stage
into the following four workstreams Managed by workstream leads who are responsible for
CLINICAL TECHNICAL HR/FM WHOLE PROJECT
ADMINISTRATION During the bid process the Project Control Office (PCO) was established as a central point
to oversee the administrative management of the programme and implement systems to h h d l d ff d h h
New Hospitals Programme
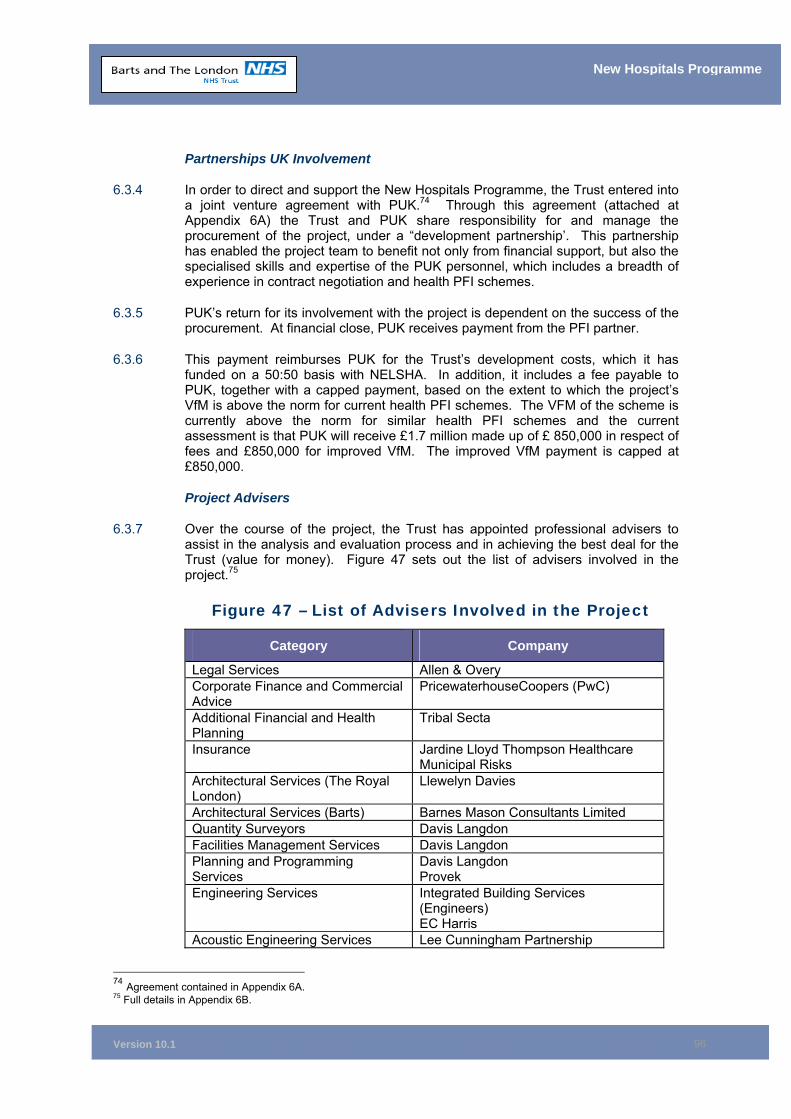
Version 10.1
96
New Hospitals Programme
Partnerships UK Involvement
6.3.4 In order to direct and support the New Hospitals Programme, the Trust entered into a joint venture agreement with PUK.74 Through this agreement (attached at Appendix 6A) the Trust and PUK share responsibility for and manage the procurement of the project, under a “development partnership’. This partnership has enabled the project team to benefit not only from financial support, but also the specialised skills and expertise of the PUK personnel, which includes a breadth of experience in contract negotiation and health PFI schemes.
6.3.5 PUK’s return for its involvement with the project is dependent on the success of the procurement. At financial close, PUK receives payment from the PFI partner.
6.3.6 This payment reimburses PUK for the Trust’s development costs, which it has funded on a 50:50 basis with NELSHA. In addition, it includes a fee payable to PUK, together with a capped payment, based on the extent to which the project’s VfM is above the norm for current health PFI schemes. The VFM of the scheme is currently above the norm for similar health PFI schemes and the current assessment is that PUK will receive £1.7 million made up of £ 850,000 in respect of fees and £850,000 for improved VfM. The improved VfM payment is capped at £850,000.
Project Advisers
6.3.7 Over the course of the project, the Trust has appointed professional advisers to assist in the analysis and evaluation process and in achieving the best deal for the Trust (value for money). Figure 47 sets out the list of advisers involved in the project.75
Figure 47 – List of Advisers Involved in the Project
Category Company
Legal Services Allen & Overy Corporate Finance and Commercial Advice
PricewaterhouseCoopers (PwC)
Additional Financial and Health Planning
Tribal Secta
Insurance Jardine Lloyd Thompson Healthcare Municipal Risks
Architectural Services (The Royal London)
Llewelyn Davies
Architectural Services (Barts) Barnes Mason Consultants Limited Quantity Surveyors Davis Langdon Facilities Management Services Davis Langdon Planning and Programming Services
Davis Langdon Provek
Engineering Services Integrated Building Services (Engineers) EC Harris
Acoustic Engineering Services Lee Cunningham Partnership
74 Agreement contained in Appendix 6A. 75 Full details in Appendix 6B.
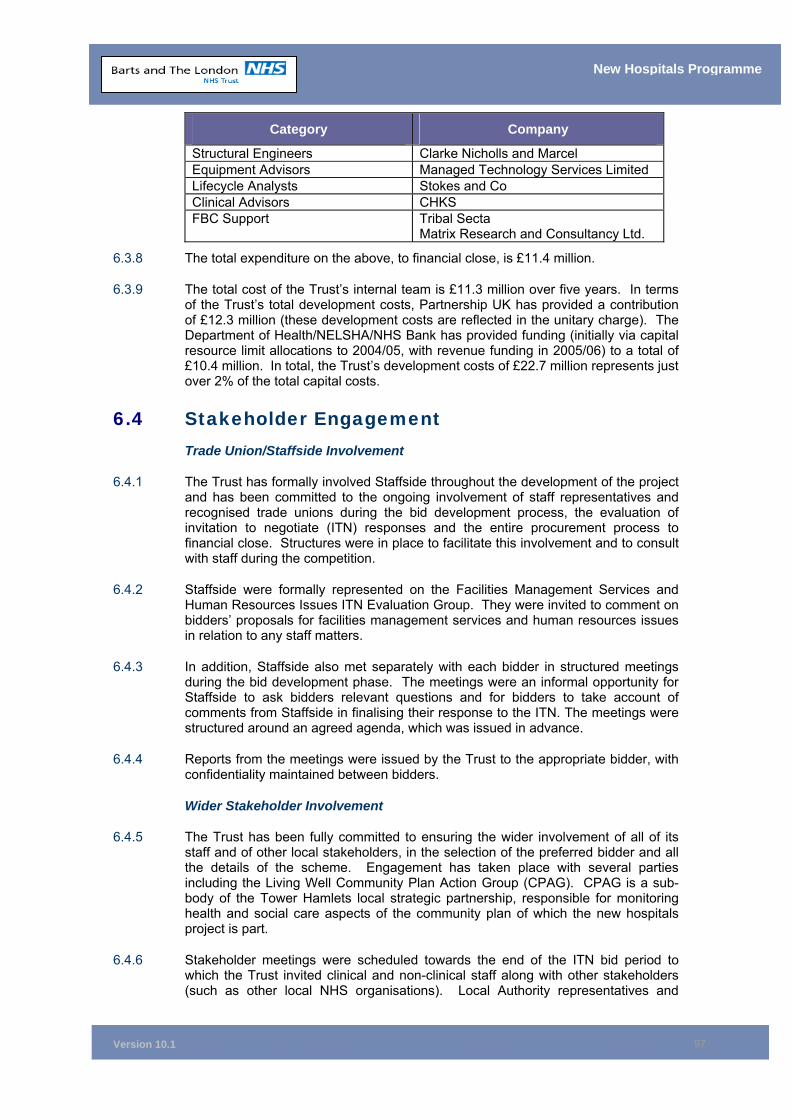
Version 10.1
97
New Hospitals Programme
Category Company
Structural Engineers Clarke Nicholls and Marcel Equipment Advisors Managed Technology Services Limited Lifecycle Analysts Stokes and Co Clinical Advisors CHKS FBC Support Tribal Secta
Matrix Research and Consultancy Ltd.
6.3.8 The total expenditure on the above, to financial close, is £11.4 million.
6.3.9 The total cost of the Trust’s internal team is £11.3 million over five years. In terms of the Trust’s total development costs, Partnership UK has provided a contribution of £12.3 million (these development costs are reflected in the unitary charge). The Department of Health/NELSHA/NHS Bank has provided funding (initially via capital resource limit allocations to 2004/05, with revenue funding in 2005/06) to a total of £10.4 million. In total, the Trust’s development costs of £22.7 million represents just over 2% of the total capital costs.
6.4 Stakeholder Engagement Trade Union/Staffside Involvement
6.4.1 The Trust has formally involved Staffside throughout the development of the project and has been committed to the ongoing involvement of staff representatives and recognised trade unions during the bid development process, the evaluation of invitation to negotiate (ITN) responses and the entire procurement process to financial close. Structures were in place to facilitate this involvement and to consult with staff during the competition.
6.4.2 Staffside were formally represented on the Facilities Management Services and Human Resources Issues ITN Evaluation Group. They were invited to comment on bidders’ proposals for facilities management services and human resources issues in relation to any staff matters.
6.4.3 In addition, Staffside also met separately with each bidder in structured meetings during the bid development phase. The meetings were an informal opportunity for Staffside to ask bidders relevant questions and for bidders to take account of comments from Staffside in finalising their response to the ITN. The meetings were structured around an agreed agenda, which was issued in advance.
6.4.4 Reports from the meetings were issued by the Trust to the appropriate bidder, with confidentiality maintained between bidders.
Wider Stakeholder Involvement
6.4.5 The Trust has been fully committed to ensuring the wider involvement of all of its staff and of other local stakeholders, in the selection of the preferred bidder and all the details of the scheme. Engagement has taken place with several parties including the Living Well Community Plan Action Group (CPAG). CPAG is a sub-body of the Tower Hamlets local strategic partnership, responsible for monitoring health and social care aspects of the community plan of which the new hospitals project is part.
6.4.6 Stakeholder meetings were scheduled towards the end of the ITN bid period to which the Trust invited clinical and non-clinical staff along with other stakeholders (such as other local NHS organisations). Local Authority representatives and
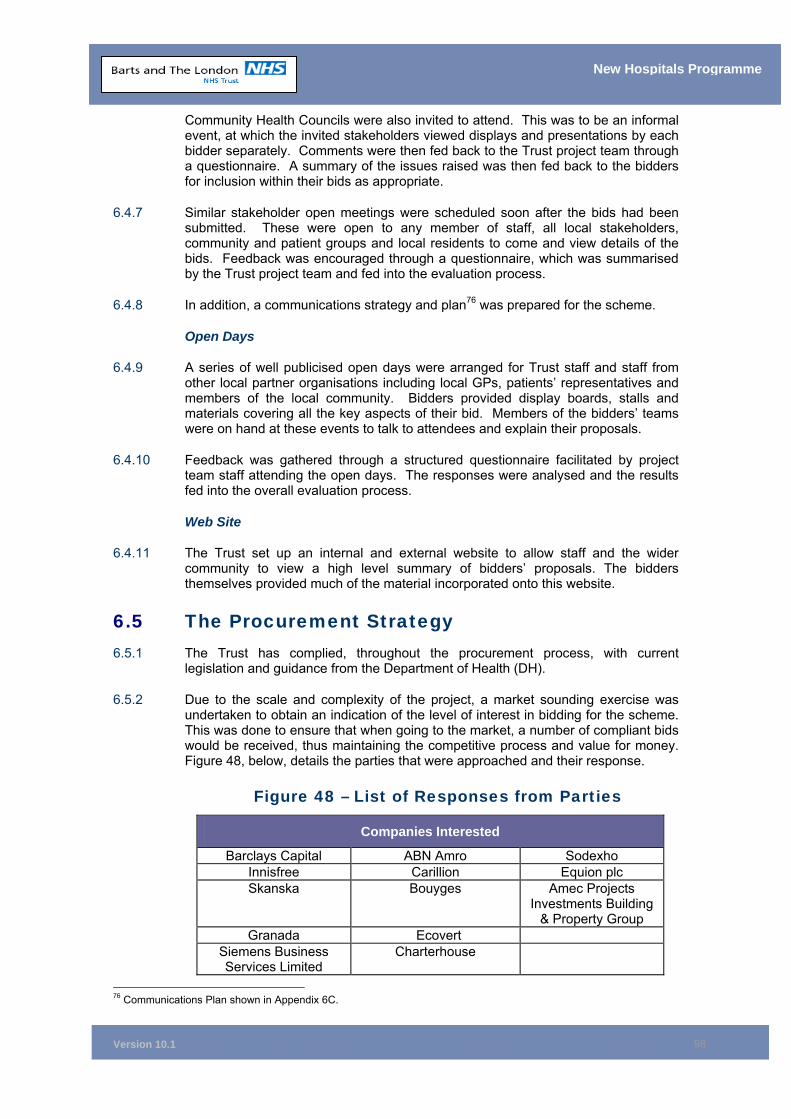
Version 10.1
98
New Hospitals Programme
Community Health Councils were also invited to attend. This was to be an informal event, at which the invited stakeholders viewed displays and presentations by each bidder separately. Comments were then fed back to the Trust project team through a questionnaire. A summary of the issues raised was then fed back to the bidders for inclusion within their bids as appropriate.
6.4.7 Similar stakeholder open meetings were scheduled soon after the bids had been submitted. These were open to any member of staff, all local stakeholders, community and patient groups and local residents to come and view details of the bids. Feedback was encouraged through a questionnaire, which was summarised by the Trust project team and fed into the evaluation process.
6.4.8 In addition, a communications strategy and plan76 was prepared for the scheme.
Open Days
6.4.9 A series of well publicised open days were arranged for Trust staff and staff from other local partner organisations including local GPs, patients’ representatives and members of the local community. Bidders provided display boards, stalls and materials covering all the key aspects of their bid. Members of the bidders’ teams were on hand at these events to talk to attendees and explain their proposals.
6.4.10 Feedback was gathered through a structured questionnaire facilitated by project team staff attending the open days. The responses were analysed and the results fed into the overall evaluation process.
Web Site
6.4.11 The Trust set up an internal and external website to allow staff and the wider community to view a high level summary of bidders’ proposals. The bidders themselves provided much of the material incorporated onto this website.
6.5 The Procurement Strategy 6.5.1 The Trust has complied, throughout the procurement process, with current
legislation and guidance from the Department of Health (DH).
6.5.2 Due to the scale and complexity of the project, a market sounding exercise was undertaken to obtain an indication of the level of interest in bidding for the scheme. This was done to ensure that when going to the market, a number of compliant bids would be received, thus maintaining the competitive process and value for money. Figure 48, below, details the parties that were approached and their response.
Figure 48 – List of Responses from Parties
Companies Interested
Barclays Capital ABN Amro Sodexho Innisfree Carillion Equion plc Skanska Bouyges Amec Projects
Investments Building & Property Group
Granada Ecovert Siemens Business Services Limited
Charterhouse
76 Communications Plan shown in Appendix 6C.
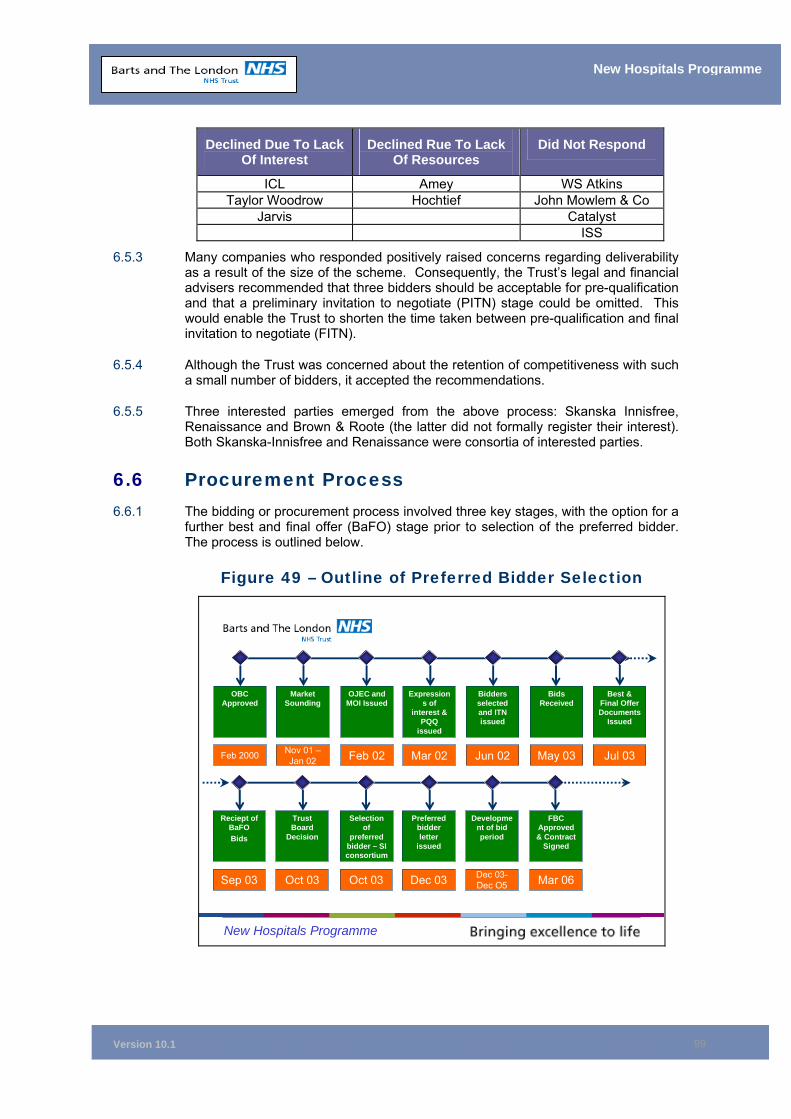
Version 10.1
99
New Hospitals Programme
Declined Due To Lack Of Interest
Declined Rue To Lack Of Resources
Did Not Respond
ICL Amey WS Atkins Taylor Woodrow Hochtief John Mowlem & Co
Jarvis Catalyst ISS
6.5.3 Many companies who responded positively raised concerns regarding deliverability as a result of the size of the scheme. Consequently, the Trust’s legal and financial advisers recommended that three bidders should be acceptable for pre-qualification and that a preliminary invitation to negotiate (PITN) stage could be omitted. This would enable the Trust to shorten the time taken between pre-qualification and final invitation to negotiate (FITN).
6.5.4 Although the Trust was concerned about the retention of competitiveness with such a small number of bidders, it accepted the recommendations.
6.5.5 Three interested parties emerged from the above process: Skanska Innisfree, Renaissance and Brown & Roote (the latter did not formally register their interest). Both Skanska-Innisfree and Renaissance were consortia of interested parties.
6.6 Procurement Process 6.6.1 The bidding or procurement process involved three key stages, with the option for a
further best and final offer (BaFO) stage prior to selection of the preferred bidder. The process is outlined below.
Figure 49 – Outline of Preferred Bidder Selection
New Hospitals Programme
Feb 2000 Feb 02 Mar 02 Jun 02 May 03 Jul 03Nov 01 –Jan 02
OBC Approved
OJEC and MOI Issued
Expressions of
interest & PQQ
issued
Bidders selected and ITN issued
Bids Received
Best & Final Offer Documents
Issued
Market Sounding
Sep 03 Oct 03 Dec 03 Dec 03-Dec O5 Mar 06Oct 03
Reciept of BaFOBids
Selection of
preferred bidder – SIconsortium
Preferred bidder letter
issued
Development of bid period
FBC Approved & Contract
Signed
Trust Board
Decision
Version 10.1
100
New Hospitals Programme
Initiation - Official Journal of the European Community (OJEC) Advertisement
6.6.2 The advertisement seeking private sector interest in the scheme was placed in the OJEC two years after approval of the OBC, in February 2002. The delay was due to the need to address the range of qualifications attached to the approval of the OBC, in particular the increase in the number of beds for cardiac services and acute elderly services. Chapter 4 contains further details of this work.
6.6.3 The response to OJEC resulted in two parties registering their interest, namely the Skanska-Innisfree consortium and the Renaissance consortium.77
Stage 1 – Pre-Qualification
6.6.4 These two consortia responded to the Trust’s invitation to submit a pre-qualification questionnaire (PQQ). The PQQ stage tested their economic and financial standing, ability and technical capacity. The responses were evaluated and both consortia qualified to proceed to the next stage of the procurement process. A paper was taken to the then Project Board78, recommending that competition proceed with both consortia.79 The Project Board endorsed the recommendations, as did the Trust Board.
Stage 2 – Preparation of Bids in Response to ITN
6.6.5 The Trust issued the ITN to both consortia, allowing them a 48-week period to prepare and submit their bids. The bidding process was designed to maximise the probability that two compliant bids, with firm price commitment, were received in a timely fashion. In order to achieve this, the above binding timetable was issued to bidders and a detailed schedule was put together setting out meetings that the Trust considered essential to hold with each bidder, the Trust’s functional groups and external advisers. The meetings were designed to comprehensively cover the reasonable requirements of bidders and the Trust, up to the submission of bids.
6.6.6 An interim submission was requested from each bidder 12 weeks into the bid development process to enable the Trust to check on progress and design development, as well as to develop user/consortia interface. This was followed by a presentation at which each bidder was invited to describe and discuss their initial design, engineering and operational concepts and the philosophies and policies that guided the further development of their bid. Bidders were also asked to provide specific proposals for any requested amendments to the draft project agreement.
6.6.7 This allowed the Trust to get an early opportunity to review and provide feedback to bidders on:
• Clinical, architectural and building design issues;
• Equipment provision;
• Operational policies; and
• Organisation of operational services.
77 Appendix 6D details consortia membership. 78 Known at this stage as the Capital Developments Project Board. See Chapter 14 for details of the levels of governance and project structure’s development. 79 Appendix 6E contains the Capital Developments Project Board paper on the outcome of the Pre-Qualification Exercise.
Version 10.1
101
New Hospitals Programme
ITN - Submission of Bids
6.6.8 Bidders submitted bids in accordance with the agreed procedure on 17 May 2003. Bids were required to remain open for acceptance by the Trust, with no price or other adjustment up to three months after the intended date of contract signature. Thereafter, bids were to remain open for acceptance by the Trust for a further period of 12 months, with only the construction costs subject to adjustment using the MIPS indices.
ITN Evaluation
6.6.9 The detailed bid evaluation process was overseen by the Invitation to Negotiate Evaluation Group (ITNEG) who made recommendations to the Trust’s Project Board, Strategic Management Group and Trust Board80. Beneath the ITNEG there were five main evaluation sub-groups, covering each major aspect of the bids. These five sub-groups evaluated the bids against the Trust’s requirements (as specified in the ITN) and made recommendations to ITNEG. The sub-groups were:
■ Design, Build and Clinical This sub-group evaluated the bidders’ proposed designs for clinical functionality, technical functionality, compliance, design quality, aesthetics and future flexibility. Views from each of the clinical sub-specialities on the design proposals for their areas were fed into this sub-group. ■ Facilities Management Services and Human Resources This sub-group focused on the detail of the bidders’ proposals for the delivery of FM services and on their proposals for dealing with human resources issues relating to transferred and seconded staff. This sub-group included representatives from Staffside. Views from representative FM service users, current facilities managers and staff were fed into the evaluation. Professional human resources and pensions views were also fed into this sub-group. ■ Equipment Proposals for the provision of a managed equipment service (MES) were evaluated by this sub-group. ■ Financing This was a specialist sub-group looking at the bidders' proposals for funding their bid and assessing whether the funding proposals were robust. ■ Commercial Issues and the Whole Bidder The commercial and legal aspects of the bids were evaluated by this sub-group, together with a number of “whole bidder issues’, such as the cohesiveness of the bidding consortia and views on the future working relationship with the Trust.
6.6.10 In addition, there was a sixth, separate sub-group focusing on the affordability of the bids. It was decided to keep the evaluation of affordability separate from assessing the other aspects of the bids. When the five main sub-groups above completed their evaluations and the affordability sub-group had assessed the costs, all the results were combined and the ITNEG took an overall view on which of the bids best met the Trust’s requirements within the constraints of affordability.
6.6.11 Each of the sub-groups were supported by the Trust’s external advisers who provided professional input. A number of internal evaluation working groups also fed their views on specific issues into the overall process. In total, over 400 staff (a
80 See Chapter 14 for details of the levels of governance and project structure’s development.
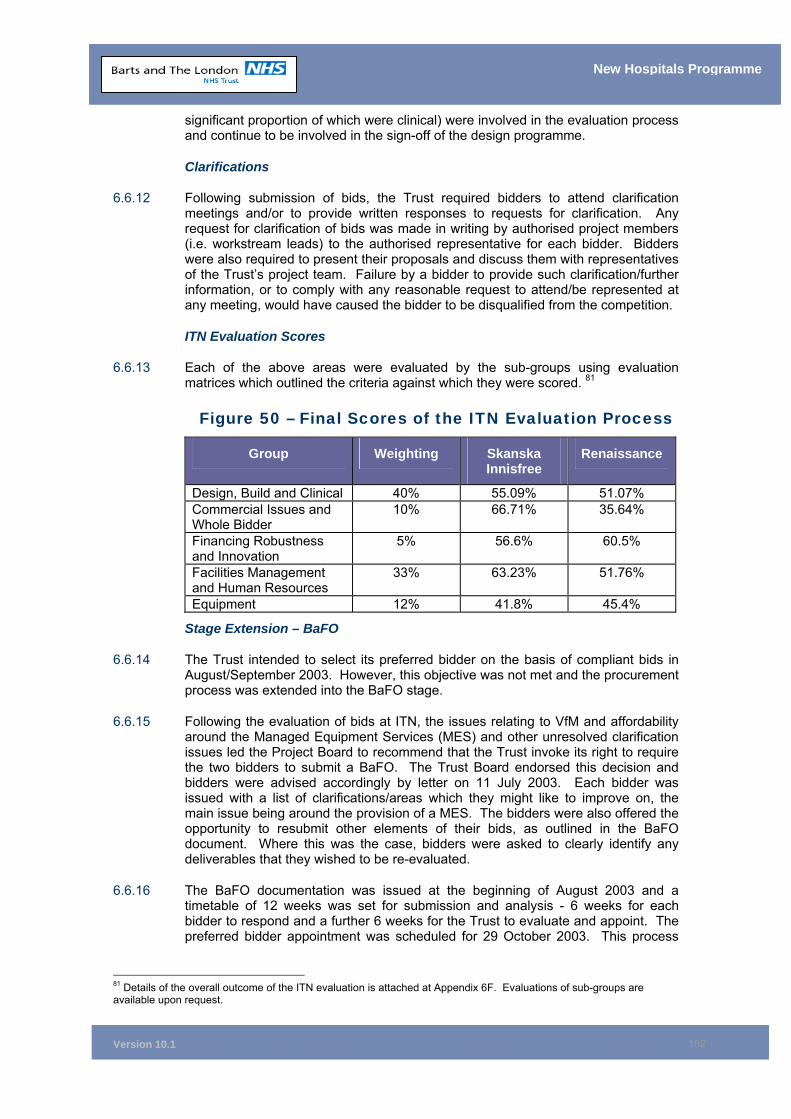
Version 10.1
102
New Hospitals Programme
significant proportion of which were clinical) were involved in the evaluation process and continue to be involved in the sign-off of the design programme.
Clarifications
6.6.12 Following submission of bids, the Trust required bidders to attend clarification meetings and/or to provide written responses to requests for clarification. Any request for clarification of bids was made in writing by authorised project members (i.e. workstream leads) to the authorised representative for each bidder. Bidders were also required to present their proposals and discuss them with representatives of the Trust’s project team. Failure by a bidder to provide such clarification/further information, or to comply with any reasonable request to attend/be represented at any meeting, would have caused the bidder to be disqualified from the competition.
ITN Evaluation Scores
6.6.13 Each of the above areas were evaluated by the sub-groups using evaluation matrices which outlined the criteria against which they were scored. 81
Figure 50 – Final Scores of the ITN Evaluation Process
Group Weighting Skanska Innisfree
Renaissance
Design, Build and Clinical 40% 55.09% 51.07% Commercial Issues and Whole Bidder
10% 66.71% 35.64%
Financing Robustness and Innovation
5% 56.6% 60.5%
Facilities Management and Human Resources
33% 63.23% 51.76%
Equipment 12% 41.8% 45.4%
Stage Extension – BaFO
6.6.14 The Trust intended to select its preferred bidder on the basis of compliant bids in August/September 2003. However, this objective was not met and the procurement process was extended into the BaFO stage.
6.6.15 Following the evaluation of bids at ITN, the issues relating to VfM and affordability around the Managed Equipment Services (MES) and other unresolved clarification issues led the Project Board to recommend that the Trust invoke its right to require the two bidders to submit a BaFO. The Trust Board endorsed this decision and bidders were advised accordingly by letter on 11 July 2003. Each bidder was issued with a list of clarifications/areas which they might like to improve on, the main issue being around the provision of a MES. The bidders were also offered the opportunity to resubmit other elements of their bids, as outlined in the BaFO document. Where this was the case, bidders were asked to clearly identify any deliverables that they wished to be re-evaluated.
6.6.16 The BaFO documentation was issued at the beginning of August 2003 and a timetable of 12 weeks was set for submission and analysis - 6 weeks for each bidder to respond and a further 6 weeks for the Trust to evaluate and appoint. The preferred bidder appointment was scheduled for 29 October 2003. This process
81 Details of the overall outcome of the ITN evaluation is attached at Appendix 6F. Evaluations of sub-groups are available upon request.
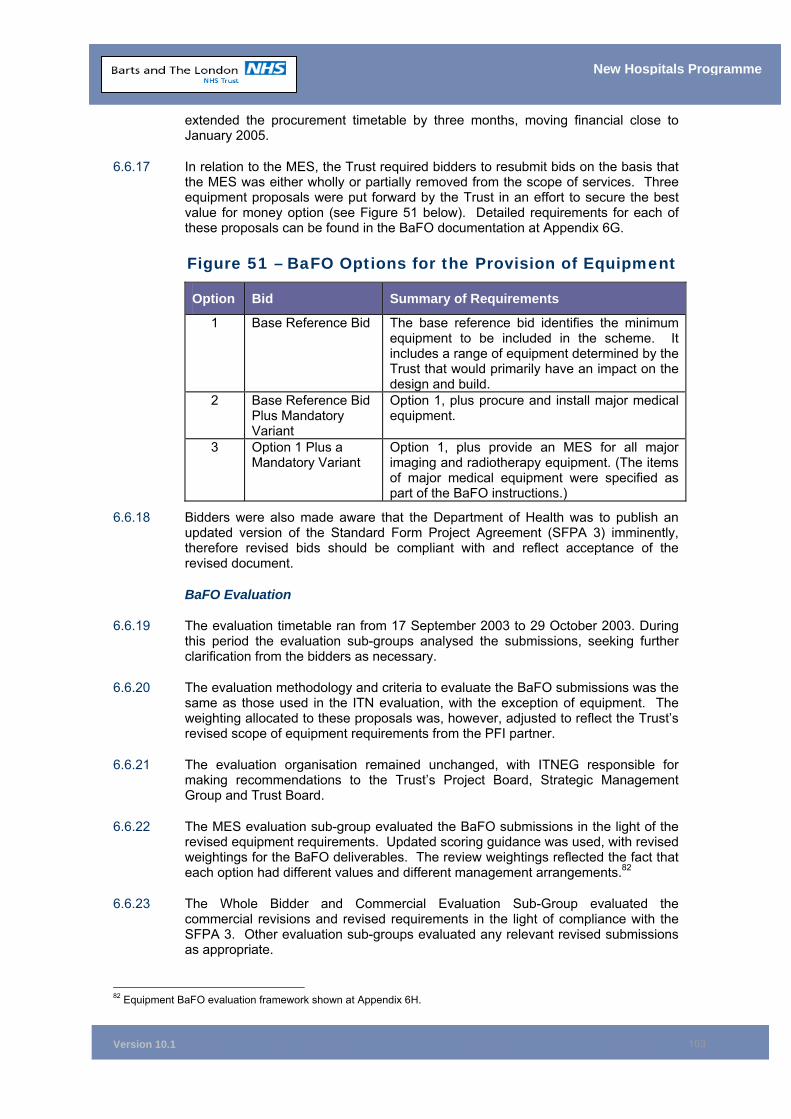
Version 10.1
103
New Hospitals Programme
extended the procurement timetable by three months, moving financial close to January 2005.
6.6.17 In relation to the MES, the Trust required bidders to resubmit bids on the basis that the MES was either wholly or partially removed from the scope of services. Three equipment proposals were put forward by the Trust in an effort to secure the best value for money option (see Figure 51 below). Detailed requirements for each of these proposals can be found in the BaFO documentation at Appendix 6G.
Figure 51 – BaFO Options for the Provision of Equipment
Option Bid Summary of Requirements
1 Base Reference Bid The base reference bid identifies the minimum equipment to be included in the scheme. It includes a range of equipment determined by the Trust that would primarily have an impact on the design and build.
2 Base Reference Bid Plus Mandatory Variant
Option 1, plus procure and install major medical equipment.
3 Option 1 Plus a Mandatory Variant
Option 1, plus provide an MES for all major imaging and radiotherapy equipment. (The items of major medical equipment were specified as part of the BaFO instructions.)
6.6.18 Bidders were also made aware that the Department of Health was to publish an updated version of the Standard Form Project Agreement (SFPA 3) imminently, therefore revised bids should be compliant with and reflect acceptance of the revised document.
BaFO Evaluation
6.6.19 The evaluation timetable ran from 17 September 2003 to 29 October 2003. During this period the evaluation sub-groups analysed the submissions, seeking further clarification from the bidders as necessary.
6.6.20 The evaluation methodology and criteria to evaluate the BaFO submissions was the same as those used in the ITN evaluation, with the exception of equipment. The weighting allocated to these proposals was, however, adjusted to reflect the Trust’s revised scope of equipment requirements from the PFI partner.
6.6.21 The evaluation organisation remained unchanged, with ITNEG responsible for making recommendations to the Trust’s Project Board, Strategic Management Group and Trust Board.
6.6.22 The MES evaluation sub-group evaluated the BaFO submissions in the light of the revised equipment requirements. Updated scoring guidance was used, with revised weightings for the BaFO deliverables. The review weightings reflected the fact that each option had different values and different management arrangements.82
6.6.23 The Whole Bidder and Commercial Evaluation Sub-Group evaluated the commercial revisions and revised requirements in the light of compliance with the SFPA 3. Other evaluation sub-groups evaluated any relevant revised submissions as appropriate.
82 Equipment BaFO evaluation framework shown at Appendix 6H.
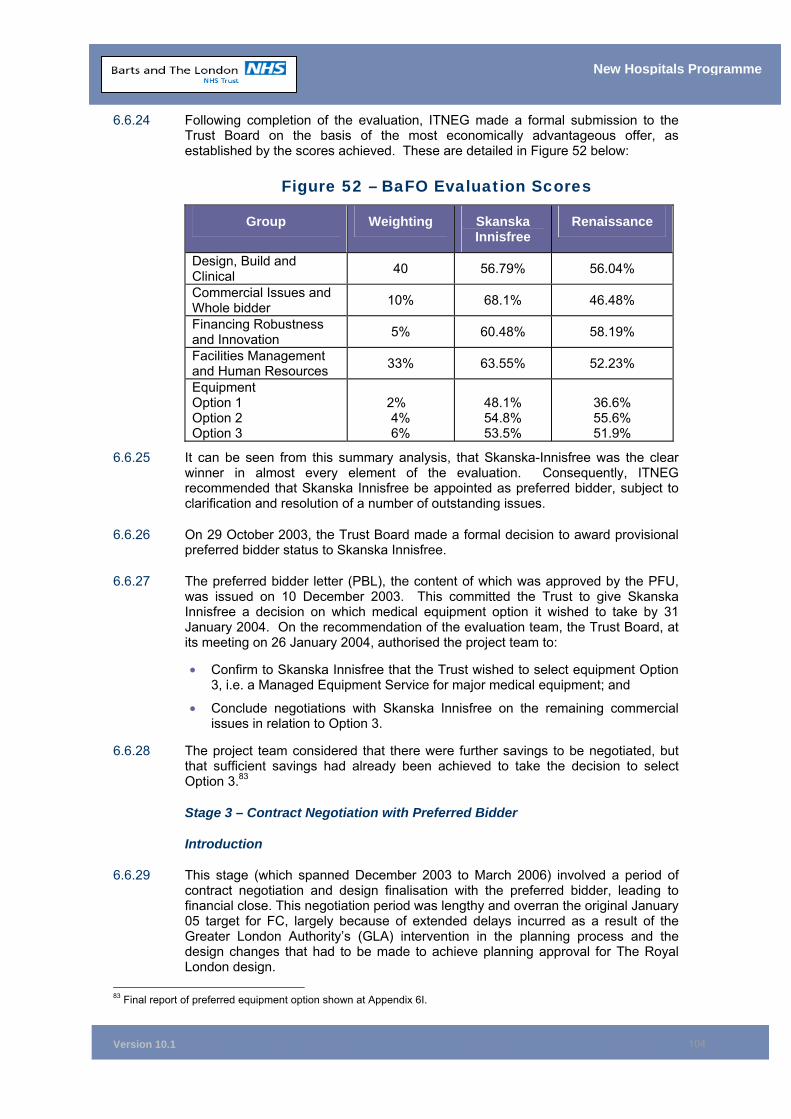
Version 10.1
104
New Hospitals Programme
6.6.24 Following completion of the evaluation, ITNEG made a formal submission to the Trust Board on the basis of the most economically advantageous offer, as established by the scores achieved. These are detailed in Figure 52 below:
Figure 52 – BaFO Evaluation Scores
Group Weighting Skanska Innisfree
Renaissance
Design, Build and Clinical 40 56.79% 56.04%
Commercial Issues and Whole bidder 10% 68.1% 46.48%
Financing Robustness and Innovation 5% 60.48% 58.19%
Facilities Management and Human Resources 33% 63.55% 52.23%
Equipment Option 1 Option 2 Option 3
2% 4% 6%
48.1% 54.8% 53.5%
36.6% 55.6% 51.9%
6.6.25 It can be seen from this summary analysis, that Skanska-Innisfree was the clear winner in almost every element of the evaluation. Consequently, ITNEG recommended that Skanska Innisfree be appointed as preferred bidder, subject to clarification and resolution of a number of outstanding issues.
6.6.26 On 29 October 2003, the Trust Board made a formal decision to award provisional preferred bidder status to Skanska Innisfree.
6.6.27 The preferred bidder letter (PBL), the content of which was approved by the PFU, was issued on 10 December 2003. This committed the Trust to give Skanska Innisfree a decision on which medical equipment option it wished to take by 31 January 2004. On the recommendation of the evaluation team, the Trust Board, at its meeting on 26 January 2004, authorised the project team to:
• Confirm to Skanska Innisfree that the Trust wished to select equipment Option 3, i.e. a Managed Equipment Service for major medical equipment; and
• Conclude negotiations with Skanska Innisfree on the remaining commercial issues in relation to Option 3.
6.6.28 The project team considered that there were further savings to be negotiated, but that sufficient savings had already been achieved to take the decision to select Option 3.83
Stage 3 – Contract Negotiation with Preferred Bidder
Introduction
6.6.29 This stage (which spanned December 2003 to March 2006) involved a period of contract negotiation and design finalisation with the preferred bidder, leading to financial close. This negotiation period was lengthy and overran the original January 05 target for FC, largely because of extended delays incurred as a result of the Greater London Authority’s (GLA) intervention in the planning process and the design changes that had to be made to achieve planning approval for The Royal London design.
83 Final report of preferred equipment option shown at Appendix 6I.

Version 10.1
105
New Hospitals Programme
Trust Conditions Attaching to the Award of Preferred Bidder Status
6.6.30 Skanska Innisfree’s selection as provisional preferred bidder was contingent upon certain conditions. These conditions were set out in the preferred bidder letter (PBL) (see Appendix 6J) and agreed through the co-signature of the letter, by both parties, in a timely fashion.
6.6.31 The main purpose of the PBL was to catalogue and agree the main matters that remained open for discussion and negotiation following the preferred bidder appointment. Moreover the PBL:
• Provided protection to a procuring authority that matters which were settled during competition would not be re-opened at a time when competitive tension had been reduced;
• Provided protection to the consortium that, should the procuring authority seek to make changes to the basis upon which the bid had been put together, the consortium was able to compute the practical and financial impact of such changes and discuss and negotiate their inclusion with the Trust; and
• Identified those matters that still remained outside the control of both parties (for example, the level of prevailing interest rates), the impact of which would need to be accommodated in the terms of the agreement prior to financial close.
Consortium Conditions Attaching to the Award of Preferred Bidder Status
6.6.32 The project directors from the Trust and PUK met with Skanska Innisfree’s “Principals” on 04 November 2003 to discuss the PBL. The consortium agreed to the contents of the letter as then drafted.
6.6.33 At this time the consortium registered concern that the PBL failed to refer to certain matters that it judged were essential to its agreement. The omissions covered:
• Affordability;
• Town planning; and
• Bid development costs.
6.6.34 Almost all of the discussions between the Trust and the consortium, from the award of provisional preferred bidder status to the issue of the PBL, focused on how these three issues were to be accommodated in the letter. Each is described in more detail below.
1. Affordability
6.6.35 Both DH and SI requested that the Trust secure the formal support of the three main PCTs to the affordability implications of its bid, so that it could assure itself that the current scheme was affordable. With the assistance of the North East London Strategic Health Authority (NELSHA), the Trust secured the appropriate commitments from the three local Primary Care Trusts (PCTs). Letters of support from Newham and Tower Hamlets are attached as Appendix 6K.
6.6.36 However, despite the approval of both PCTs and the SHA, concerns continued to be raised by the Department of Health in December 2005 in relation to:
i. Affordability in general, taking into account the annual UC as a proportion of the Trust’s income; and
Version 10.1
106
New Hospitals Programme
ii. Capacity, particularly whether that being provided at Barts was required, given cardiac capacity across North London.
6.6.37 This resulted in a review of the Project’s affordability, particularly the Barts development. Matrix Management Consultants were appointed by the SHA to conduct an independent review of cancer and cardiac activity. The outcome of which endorsed the Trust’s assumptions.
2. Planning
6.6.38 Outline planning permission for the Trust’s own design had not been secured at the time of issue of the PBL. The London Borough of Tower Hamlets (LBTH) made it clear that, as the redevelopment involved listed buildings in a conservation area, it was not prepared to provide any formal approval to outline proposals. The Trust received the same feedback from the Corporation of London in relation to Barts. Such a stance is not unusual in major capital developments, particularly where listed buildings are involved.
6.6.39 In view of this, the Trust elected to commission a “planning brief” for The Royal London Hospital redevelopment which was submitted to and considered by LBTH. This planning brief was informally supported by the Borough’s Policy & Implementation Committee.
6.6.40 Skanska Innisfree was of the view that the absence of formal outline planning permission (even in the light of the planning brief) fundamentally changed the risks associated with the planning process, which fell to it to manage. The consortium was reluctant to accept the normal level of risks with regard to its design, should town planning have taken considerably longer than envisaged or, ultimately, should it prove impossible to achieve.
6.6.41 In recognition of the greater level of uncertainty, the Trust sought to continue to oblige the consortium to obtain planning permission, but identified a number of excusing causes that would hold the consortium harmless should planning permissions be delayed or prove impossible to secure. The consortium refused to accept any obligation to obtain planning permission, arguing that even normal planning processes are highly politicised in nature. It agreed to pursue the planning process diligently and in accordance with best planning practice, so that if it could be demonstrated that it had acted in a dilatory fashion in pursuit of planning, then it would suffer the financial consequences.
3. Bid Development Costs
6.6.42 The issue of costs was intertwined with the consortium’s concern regarding planning. The consortium had estimated that it could incur costs of approximately £44 million between issue of the PBL and financial close, in developing its design and securing planning permissions, etc., to reach financial close.
6.6.43 The consortium sought to reduce the exposure it had to writing-off bid development costs should either delay, or cancellation occur, for reasons that were outside its control. Of the two scenarios, delay was by far the more probable.
6.6.44 The Trust responded to the consortium’s concerns by suggesting a risk sharing mechanism that reflected the fact that many of the matters that remained outside the consortium’s control were also outside the Trust’s control. The notion of Trust risk, shared risk and consortium risk was established in the PBL (see Appendix 6J, section 13).
Version 10.1
107
New Hospitals Programme
6.6.45 The potential causes of delay and/or cancellation or withdrawal were divided as follows:
• Trust risks were defined as those risks which are clearly within the control of the Trust (eg changes in the Trust's requirements), or which are entirely outside the control of the consortium, but within the control of the public sector. Trust risk therefore included:
Any change in funding allocated to the project;
Any change in the Government's policy framework or change in law (including in relation to tax): (1) specifically affecting hospital projects or (2) discriminating against PFI/Public Private Partnership (PPP) and in the case of either (1) or (2) affecting the project;
Any change in the proposed configuration of hospital services in East London;
Any judicial review, appeal or other proceedings instituted in relation to any planning consent or application;
Any calling in by the Secretary of State or decision to hold a planning inquiry or direction, objection or other intervention by the Mayor of London;
Any planning decision motivated by concerns that either site should not be developed with the hospital services proposed by the Trust;
Any planning decision or delay in reaching a decision, which is not a decision or delay in reaching a decision, which a reasonable authority assessing the project would take or cause;
Any planning condition relating to any off-site matter which is not within the reasonable control of the consortium to fulfil;
Any extraordinary, unscheduled intervention which would not reasonably be expected as part of the normal planning process for a project of this nature;
Any decision to list or to change the listing status of any building or structure on the sites which has a material adverse effect on the consortium's design for the project, or the ability of the consortium to obtain planning permission for the project;
Any decision by the Trust to materially change any of the Trust's requirements;
Any failure by the Trust to give the consortium access to premises at agreed times (this includes both vacant possession for buildings needed at financial close and access to complete the survey programme prior to financial close);
Unforeseen ground conditions (archaeology risk);
Any changes resulting from the funding competition referred to in paragraph 20 of the PBL; and
Any material failure by the Trust to comply with the terms of the PBL following reasonable notice in writing given by the consortium to the Trust.
• Consortium risks were defined as those risks which are clearly within the consortium's control (eg a unilateral substantive change in the risk allocation of the consortium's BaFO or delay/refusal of planning permission as a direct result of the consortium's design).
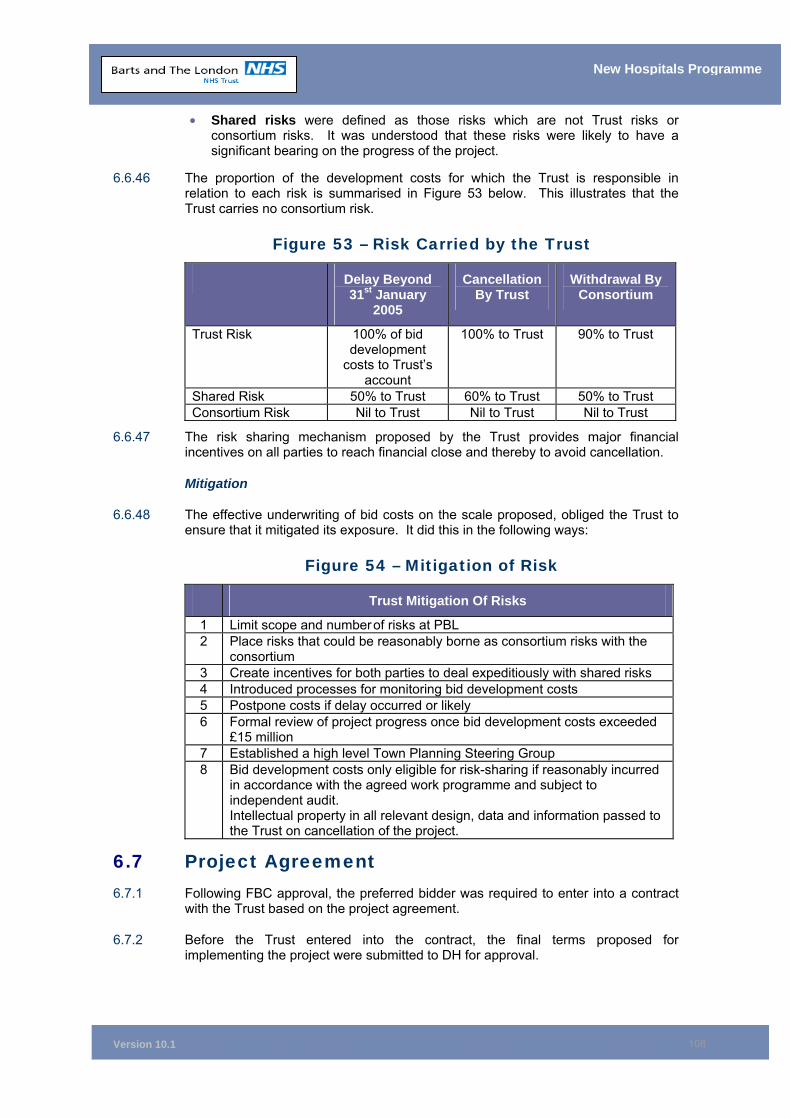
Version 10.1
108
New Hospitals Programme
• Shared risks were defined as those risks which are not Trust risks or consortium risks. It was understood that these risks were likely to have a significant bearing on the progress of the project.
6.6.46 The proportion of the development costs for which the Trust is responsible in relation to each risk is summarised in Figure 53 below. This illustrates that the Trust carries no consortium risk.
Figure 53 – Risk Carried by the Trust
Delay Beyond 31st January
2005
Cancellation By Trust
Withdrawal By Consortium
Trust Risk 100% of bid development
costs to Trust’s account
100% to Trust 90% to Trust
Shared Risk 50% to Trust 60% to Trust 50% to Trust Consortium Risk Nil to Trust Nil to Trust Nil to Trust
6.6.47 The risk sharing mechanism proposed by the Trust provides major financial incentives on all parties to reach financial close and thereby to avoid cancellation.
Mitigation
6.6.48 The effective underwriting of bid costs on the scale proposed, obliged the Trust to ensure that it mitigated its exposure. It did this in the following ways:
Figure 54 – Mitigation of Risk
Trust Mitigation Of Risks
1 Limit scope and number of risks at PBL 2 Place risks that could be reasonably borne as consortium risks with the
consortium 3 Create incentives for both parties to deal expeditiously with shared risks 4 Introduced processes for monitoring bid development costs 5 Postpone costs if delay occurred or likely 6 Formal review of project progress once bid development costs exceeded
£15 million 7 Established a high level Town Planning Steering Group 8 Bid development costs only eligible for risk-sharing if reasonably incurred
in accordance with the agreed work programme and subject to independent audit. Intellectual property in all relevant design, data and information passed to the Trust on cancellation of the project.
6.7 Project Agreement 6.7.1 Following FBC approval, the preferred bidder was required to enter into a contract
with the Trust based on the project agreement.
6.7.2 Before the Trust entered into the contract, the final terms proposed for implementing the project were submitted to DH for approval.
Version 10.1
109
New Hospitals Programme
6.7.3 As part of this approval process, the proposed commercial arrangements and contract terms were considered by the Private Finance Unit (PFU) of the DH. The PFU had specifically instructed the Trust that substantive amendment of the Standard Form Project Agreement (SFPA) were not acceptable, except to the extent that any such amendment could be justified on project-specific grounds. Those aspects of the project that give rise to project-specific matters are outlined in Volume III of the draft project agreement. See Chapter 15 for full details of the project agreement arrangements.
6.8 Funding Support 6.8.1 At the time of the PBL, the DH agreed to provide cash support for any obligations
that arose under this risk-sharing mechanism in a timely fashion. This, together with the continuing arrangement on development costs with PUK, has covered the cash required support.
6.8.2 DH also indicated that, depending on the cause leading to the obligation, cash would be provided to the Trust either by way of grant (if the cause sat outside the control of the local health system) or loan (if the cause of the delay/cancellation was within the control of the local health system). This is covered in more detail in Chapter 11.
Support from PCTs
6.8.3 At the time of the PBL, the Trust received confirmation of overall support from the PCTs, including a commitment to provide an additional £30.6 million per annum (£21.9 million of which is attributed to Tower Hamlets PCT) to cover anticipated Thames Gateway population growth84. (See also section 11.3)
6.9 CABE 6.9.1 The NHS Estates Design Review Panel (DRP) was set up by the Secretary of State
for Health, its remit being to provide advice, guidance and support to the NHS in the form of a design review and subsequent report.
6.9.2 The Commission for Architecture and the Built Environment (CABE) published Better Public Buildings in 200085, as part of an initiative to improve the design of public buildings. This was followed by conferences at which the Trust was represented and at which contact with CABE was established. The Trust approached CABE regarding design comment and when CABE instigated its enabling programme as part of a funding agreement between CABE and NHS Estates, the Trust was selected as one of the five PFI hospitals to have an “Enabler’. Barts and The London was a suitable project in that it met many of CABE's overall involvement criteria.
6.9.3 The advantage to the Trust was in:
• Helping to establish CABE's aspirations in terms of design and function;
• Assisting in the selection process; and
• Having an ongoing role in terms of briefing design teams and reviews of progress in relation to design issues as appropriate.
84 See Appendix 6K for copy of the relevant letter from the Tower Hamlets PCT (THPCT). 85 Better Public Buildings – A proud legacy for the future: Department for Culture, Media and Sport 2000.
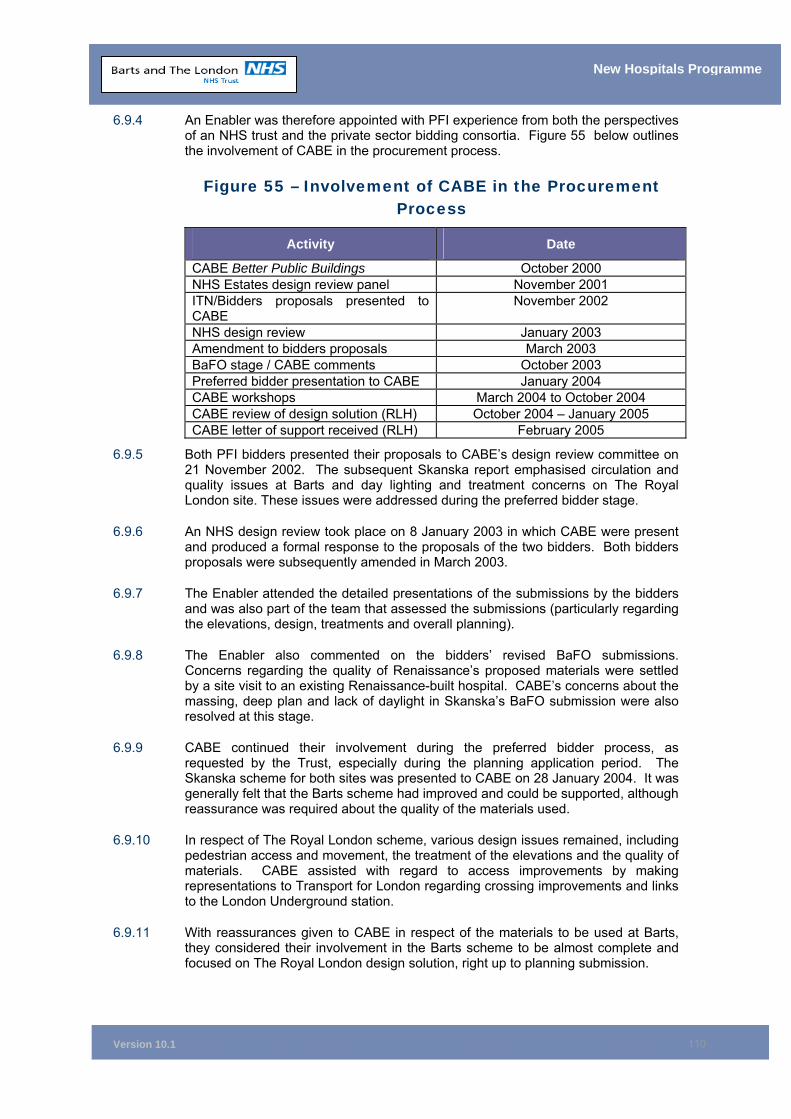
Version 10.1
110
New Hospitals Programme
6.9.4 An Enabler was therefore appointed with PFI experience from both the perspectives of an NHS trust and the private sector bidding consortia. Figure 55 below outlines the involvement of CABE in the procurement process.
Figure 55 – Involvement of CABE in the Procurement Process
Activity Date
CABE Better Public Buildings October 2000 NHS Estates design review panel November 2001 ITN/Bidders proposals presented to CABE
November 2002
NHS design review January 2003 Amendment to bidders proposals March 2003 BaFO stage / CABE comments October 2003 Preferred bidder presentation to CABE January 2004 CABE workshops March 2004 to October 2004 CABE review of design solution (RLH) October 2004 – January 2005 CABE letter of support received (RLH) February 2005
6.9.5 Both PFI bidders presented their proposals to CABE’s design review committee on 21 November 2002. The subsequent Skanska report emphasised circulation and quality issues at Barts and day lighting and treatment concerns on The Royal London site. These issues were addressed during the preferred bidder stage.
6.9.6 An NHS design review took place on 8 January 2003 in which CABE were present and produced a formal response to the proposals of the two bidders. Both bidders proposals were subsequently amended in March 2003.
6.9.7 The Enabler attended the detailed presentations of the submissions by the bidders and was also part of the team that assessed the submissions (particularly regarding the elevations, design, treatments and overall planning).
6.9.8 The Enabler also commented on the bidders’ revised BaFO submissions. Concerns regarding the quality of Renaissance’s proposed materials were settled by a site visit to an existing Renaissance-built hospital. CABE’s concerns about the massing, deep plan and lack of daylight in Skanska’s BaFO submission were also resolved at this stage.
6.9.9 CABE continued their involvement during the preferred bidder process, as requested by the Trust, especially during the planning application period. The Skanska scheme for both sites was presented to CABE on 28 January 2004. It was generally felt that the Barts scheme had improved and could be supported, although reassurance was required about the quality of the materials used.
6.9.10 In respect of The Royal London scheme, various design issues remained, including pedestrian access and movement, the treatment of the elevations and the quality of materials. CABE assisted with regard to access improvements by making representations to Transport for London regarding crossing improvements and links to the London Underground station.
6.9.11 With reassurances given to CABE in respect of the materials to be used at Barts, they considered their involvement in the Barts scheme to be almost complete and focused on The Royal London design solution, right up to planning submission.
Version 10.1
111
New Hospitals Programme
6.9.12 A series of CABE workshops were subsequently arranged to address the broad issues of facades, geometry of building forms and external and internal wayfinding.
6.9.13 Revisions were made and presented to CABE at a meeting on 29 September 2004. However, at that point in time, their concerns in relation to the main towers and building above plinth level could not be addressed due to cost and time restraints.
6.9.14 CABE was impressed by the strategy adopted for the public realm/open spaces and felt that it was a workable solution. The adaptation of the front block to address the accessibility issues was also welcomed. CABE requested that the clarity created with relation to the new public spaces continue into the treatment of the main building, with a simplification of the elements. They were also of the view that some cosmetic treatments could be explored to the main towers, without changing the blocks.
6.9.15 CABE considered that the new open space was a great opportunity for a “festive space” that could be used to engage with the local community as a performance/shared area. It was pointed out that the London Borough of Tower Hamlets required a basic scheme to be submitted for planning purposes. The detailed design of this important space could then be worked-up later.
6.9.16 As a result of the GLA intervention (see section 6.10 below), design changes to the main towers had to be made if the scheme was to achieve planning approval. As part of the process, further formal design reviews were held, which resulted in CABE providing their overall strategic support for the revisions made. This support was then communicated to Tower Hamlets Planning Authority.86
6.9.17 One or two issues remained in respect of circulation space and the positioning of lifts, which it was agreed would be the subject of further work and additional dialogue with CABE, regarding the detailed design.
6.10 GLA Involvement in the Planning Application 6.10.1 Shortly after the Trust tendered this project in the summer of 2002, consultation
commenced with the London Borough of Tower Hamlets and later with other bodies including English Heritage (EH), CABE and conservation, community and religious groups. Due to the strategic importance and scale of the proposed redevelopment, extensive consultation took place with the GLA, who have a statutory role to play in the planning process. The original planning application was submitted on 30 April 2004.
6.10.2 The GLA responded to the proposals in a letter dated 3 August 2004, stating that, if Tower Hamlets intended to approve the application in relation to the Royal London site, the Mayor of London was minded to direct refusal due to serious concerns. Those concerns included:
• Lack of accessibility and the provision of an inclusive environment;
• Inactive street frontages, encouraging anti-social behavior;
• Poor wayfinding; and
• Scale and massing (particularly in relation to the two towers).
6.10.3 Skanska Innisfree and the Trust responded to these concerns and to workshops held with the GLA Urbanism Unit, resulting in the following improvements:
86 Letter confirming CABE support shown in Appendix 6L.
Version 10.1
112
New Hospitals Programme
• The demolition of the listed East Wing, to create a large publicly-accessible square;
• Realignment of entrances to this square to animate the area;
• The expansion of the glazed health mall to provide more active facades to the square; and
• The lowering of the ground floor at the portico entrance to provide level access for people with disabilities.
6.10.4 These were incorporated in an amendment to the application submitted on 15 October 2004.
6.10.5 Following a further meeting with the GLA, it was clear that although most of their concerns had been addressed, the scale and mass remained a serious issue. Discussions with the GLA culminated in the following solutions to reduce the scale of the two towers forming the inpatient accommodation:
• The south block was moved eastwards by 9 meters, with the ground floor remaining in position;
• The FM yard was re-planned;
• St Phillip’s Square was extended slightly eastwards;
• 3 meter projections were added to parts of the east and west faces of the towers;
• The height of part of the roof top plant rooms was increased to line up with the projections;
• The elevations were articulated to give the impression of four tall, slim towers; and
• An entrance was added to the ground floor from St Phillip’s Square, thereby animating this space further.
6.10.6 On 3 December 2004, following a design review meeting between Skanska Innisfree, the Trust, the London Borough of Tower Hamlets and the GLA, all parties agreed to the design proposals. These formed the basis of the planning amendment submitted on 4 February 2005.
6.11 Audit of PFI Procurement Process 6.11.1 Internal audit reviewed the procurement process for the main PFI New Hospitals
Project from the issue of the invitation to negotiate (ITN) in June 2002 to the selection of the provisional preferred bidder in October 2003. External auditors had also conducted a compliance check on the audit requirements, originally set out as part of the ITN, which were found to be satisfactory.
6.11.2 Internal audit developed a “control evaluation framework” for the procurement processes in early 200287. Compliance with the framework was checked through a programme of testing as the procurement progressed.
6.11.3 The overall objective of the audit was to ascertain whether robust procurement processes were operated in accordance with relevant NHS and HM Treasury Guidance. In particular, audit testing examined whether:
• Transfers of information had been properly controlled and confidentiality maintained;
87 See Appendix 6M for Audit Report of PFI procurement process.
Version 10.1
113
New Hospitals Programme
• The receipt and evaluation of bids followed a robust process in accordance with EU procurement regulations, HM Treasury and NHS guidance and the Trust’s Standing Orders and Standing Financial Instructions;
• The evaluation of BaFO followed a robust process in accordance with HM Treasury and NHS guidance; and
• A robust process was followed for selection of the preferred bidder and final evaluation.
6.11.4 The audit concluded that the PFI procurement process on the New Hospitals Project, from the issue of the ITN to the selection of the provisional preferred bidder, was operated in accordance with relevant legislation, guidance and best practice and complied fully with the agreed internal audit control evaluation framework.
6.12 Gateway Review 6.12.1 The project has been the subject of three Gateway Reviews. Gates 2 and 3 have
been undertaken and completed. Gate 3 was conducted over the period 24 - 27 May 2005 and the scheme achieved amber status.
6.12.2 An action plan was drawn up for implementing the recommendations of the review (attached at Appendix 0D). All high priority recommendations have been addressed.
6.12.3 A further Gateway 0 is planned for summer 2006.
6.13 Chapter Conclusion 6.13.1 In conclusion, the procurement process has been comprehensive. All relevant
legislation and guidance has been followed and all relevant parties have been involved at the appropriate stages of the process.
6.13.2 The competition up to preferred bidder stage has been robust and the benefit of this has not been eroded during the preferred bidder stage.
6.14 Chapter Appendices 6A PUK Agreement 6B Trust Advisors to the Project 6C Communications Plan 2004 – 2005 6D Details of the Bidding Consortia 6E Outcome of Pre-Qualification Exercise 6F ITN Evaluation - Overall Scores 6G BaFO Requirements For Equipment Bids 6H Equipment BaFO Evaluation Framework 6I Equipment Evaluation Report 6J Preferred Bidder Letter 6K Newham and Tower Hamlets PCTs’ Letters of Support 6L CABE Letter of Support 6M Audit Report PFI Procurement Process
Version 10.1
114
New Hospitals Programme
7 THE PREFERRED SOLUTION Synopsis – The Preferred Solution
This chapter shows that: ■ The Skanska Innisfree consortium is the preferred partner;
■ The Funding structure is robust;
■ The Preferred PFI solution is designed to provide clinical functionality and maximise flexibility of design;
■ The solution proposes access and wayfinding that represent a considerable improvement on the existing facilities;
■ The approach to the provision of FM services and equipment meets the Trust’s requirements;
■ The decant, commissioning and phasing programme associated with the construction programme is complex but manageable; and
■ The impact of the descoping proposals will be assessed and any changes detailed in the addendum to the FBC.
7.1 Introduction 7.1.1 This chapter details the PFI solution, including details of the consortium, the
structure of the Special Purpose Vehicle (SPV), funding arrangements, design principles, decant and commissioning programme, IT, equipment and FM arrangements. This chapter also provides a summary of PFI-specific benefits, and details, at a high level, the impact of the descoping proposals.
7.2 The Consortium Members Skanska
7.2.1 Skanska UK is a business unit within the Skanska Group, a global construction services company. Skanska offers a range of services, from project development to construction and facilities management (FM). The group currently has 70,000 employees and operates in 11 home markets. Group sales in 2003 totalled US $16.4 billion while Skanska UK had net sales of £850 million and employs 3,500 staff.
7.2.2 Skanska UK’s core activity is construction, combining design, building and civil engineering with a range of specialist skills to provide integrated project solutions. The company is a market leader in PFI and the primary provider of healthcare PFI projects. Skanska has recently signed contracts with and are currently building on sites at the University Hospital of Coventry and Walsgrave and the South Derbyshire Hospitals NHS Trust. Other PFI hospitals successfully completed are King’s College Hospital (London), Queen Elizabeth Hospital (London) and Chepstow Neighbourhood Health Unit (Wales).
7.2.3 Skanska Integrated Projects (SIP) is a trading name of Skanska Construction UK Limited (the principal design and construction company of Skanska UK). Skanska Rashleigh Weatherfoil Limited (SRW) is the hard FM services arm of Skanska UK. SIP and SRW have a successful track record in the construction and long-term maintenance of PFI hospital projects.
Version 10.1
115
New Hospitals Programme
7.2.4 Skanska BOT Investment UK Ltd is the UK arm of the investment division of Skanska BOT AB, which is a business unit of Skanska AB. Skanska BOT are active investors in PFI and infrastructure projects in a variety of locations around the world. Skanska BOT Investment UK Ltd will hold Skanska’s investment in the project.
Innisfree
7.2.5 Established in 1995, Innisfree is an infrastructure investment group in the UK, investing in PFI and Public Private Partnership (PPP) infrastructure projects.
Mowlem Aqumen
7.2.6 Mowlem Aqumen is a provider of facilities management and outsourcing solutions to owners and users of premises and facilities. Mowlem provides services to a wide spectrum of clients and operates and develops FM solutions in healthcare, defence, education, retail, commerce, industry, financial services and PFI projects.
7.2.7 Mowlem provides services under a PFI contract at the James Cook University Hospital and is at the preferred bidder stage on two other hospital projects (Lewisham Hospital and Cornwall LIFT projects).
7.2.8 In 2006 Carillion Plc acquired Mowlem Plc. This has brought much wider PFI experience to the Project. Carillion have entered into the agreement with the same risks and obligations taken by Mowlem.
Siemens
7.2.9 Siemens Healthcare Services is a business unit within Siemens plc. Siemens Healthcare Services provides managed technology services to the UK healthcare sector. These services include provision of medical equipment, IT and PACS solutions, as well as electro biomedical engineering services.
7.2.10 Siemens first signed a contract for operating an NHS hospital Managed Equipment Service (MES) within a PFI contract in 1998. It now has five operational contracts with terms of up to 40 years, such as Worcester Royal Infirmary NHS Trust and Dudley Group of Hospitals NHS Trust. Siemens has recently signed contracts with Blackburn Hyndburn & Ribble Valley NHS Trust and Barking, Havering & Redbridge Hospitals NHS Trust and is the preferred equipment provider at North Staffordshire NHS Trust.
Synergy Healthcare
7.2.11 Synergy Healthcare plc is a supplier of sterile services in the healthcare sector. The surgical business is a significant supplier of sterile and other surgical support services to the NHS, while Group Company Healthtex supplies linen management services to the NHS.
7.2.12 The sterile services division operates 12 sterile services units, providing clinical sterile services department (CSSD) instrument trays throughout England. The division operates as a fully managed service or as a service partner. Synergy is providing sterile services under the South Derbyshire Hospitals NHS Trust PFI project.
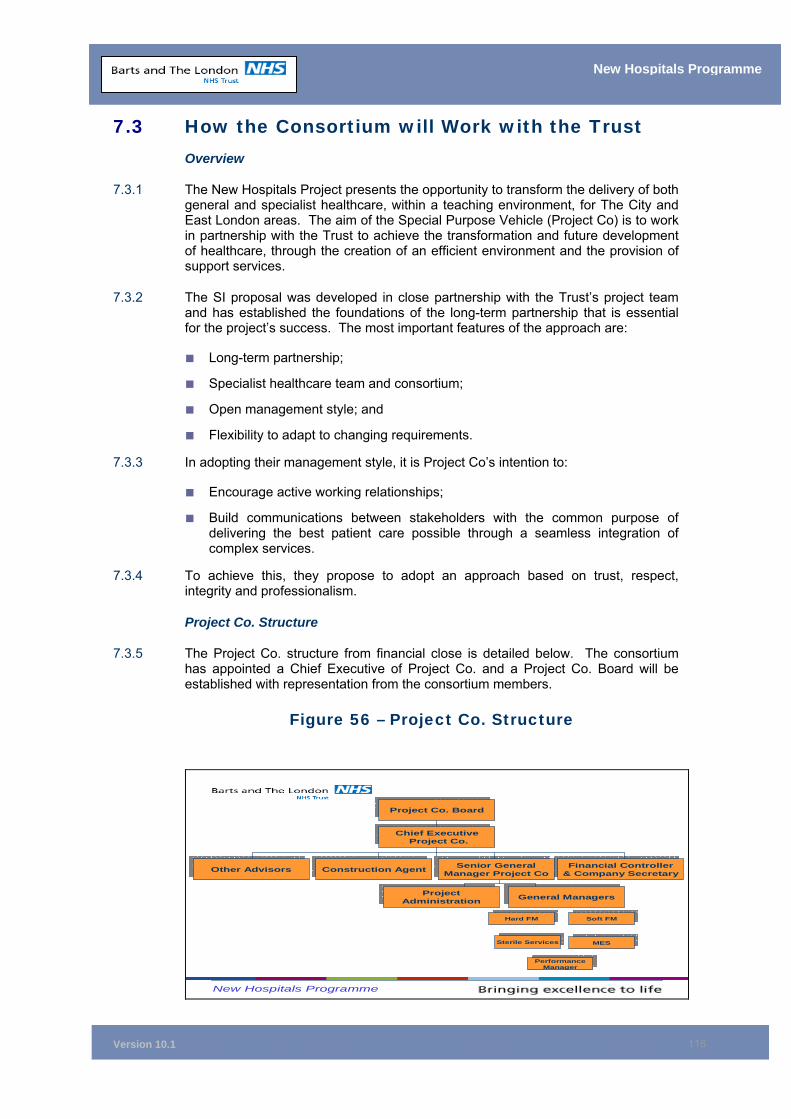
Version 10.1
116
New Hospitals Programme
7.3 How the Consortium will Work with the Trust Overview
7.3.1 The New Hospitals Project presents the opportunity to transform the delivery of both general and specialist healthcare, within a teaching environment, for The City and East London areas. The aim of the Special Purpose Vehicle (Project Co) is to work in partnership with the Trust to achieve the transformation and future development of healthcare, through the creation of an efficient environment and the provision of support services.
7.3.2 The SI proposal was developed in close partnership with the Trust’s project team and has established the foundations of the long-term partnership that is essential for the project’s success. The most important features of the approach are:
■ Long-term partnership;
■ Specialist healthcare team and consortium;
■ Open management style; and
■ Flexibility to adapt to changing requirements.
7.3.3 In adopting their management style, it is Project Co’s intention to:
■ Encourage active working relationships;
■ Build communications between stakeholders with the common purpose of delivering the best patient care possible through a seamless integration of complex services.
7.3.4 To achieve this, they propose to adopt an approach based on trust, respect, integrity and professionalism.
Project Co. Structure
7.3.5 The Project Co. structure from financial close is detailed below. The consortium has appointed a Chief Executive of Project Co. and a Project Co. Board will be established with representation from the consortium members.
Figure 56 – Project Co. Structure
New Hospitals Programme
Project Co. BoardProject Co. Board
Chief ExecutiveProject Co.
Chief ExecutiveProject Co.
Financial Controller& Company Secretary
Financial Controller& Company Secretary
Senior GeneralManager Project Co
Senior GeneralManager Project Co
Construction AgentConstruction AgentOther AdvisorsOther Advisors
ProjectAdministration
ProjectAdministration
General ManagersGeneral Managers
Hard FMHard FM Soft FMSoft FM
Sterile ServicesSterile Services MESMES
PerformanceManagerPerformance
Manager
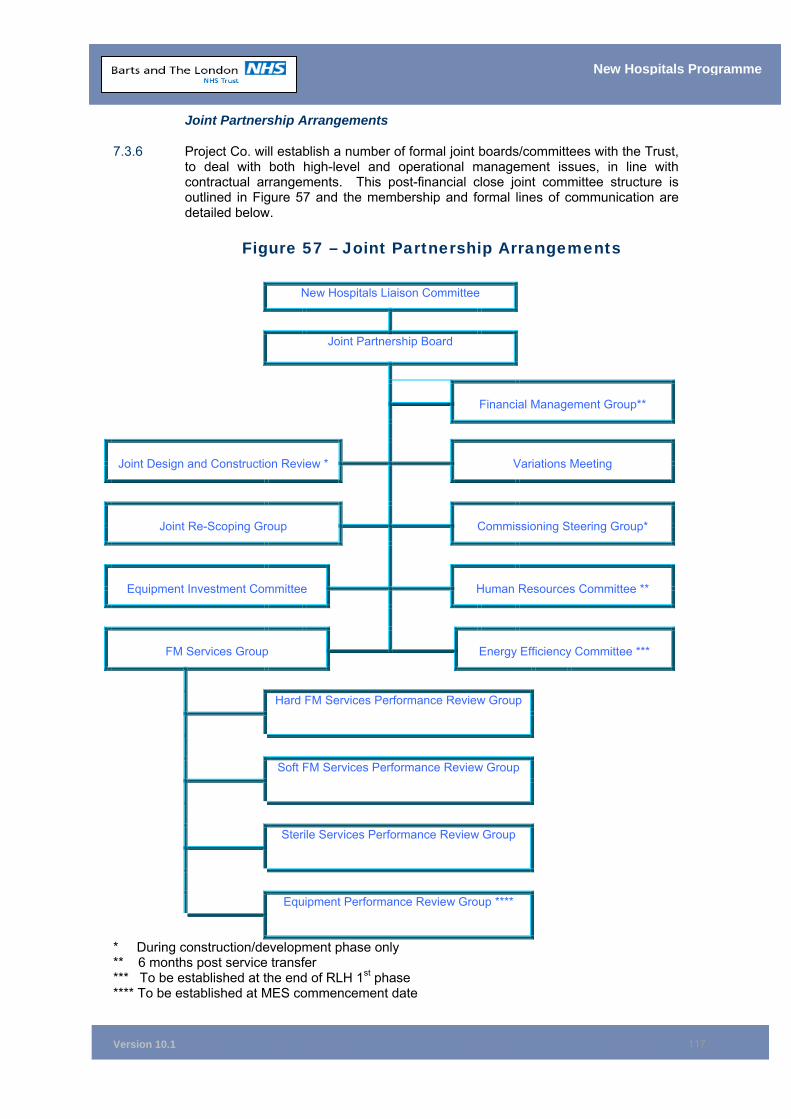
Version 10.1
117
New Hospitals Programme
Joint Partnership Arrangements
7.3.6 Project Co. will establish a number of formal joint boards/committees with the Trust, to deal with both high-level and operational management issues, in line with contractual arrangements. This post-financial close joint committee structure is outlined in Figure 57 and the membership and formal lines of communication are detailed below.
Figure 57 – Joint Partnership Arrangements
New Hospitals Liaison Committee
Joint Partnership Board
Financial Management Group**
Joint Design and Construction Review *
Variations Meeting
Joint Re-Scoping Group
Commissioning Steering Group*
Equipment Investment Committee
Human Resources Committee **
FM Services Group
Energy Efficiency Committee ***
Hard FM Services Performance Review Group
Soft FM Services Performance Review Group
Sterile Services Performance Review Group
Equipment Performance Review Group ****
* During construction/development phase only ** 6 months post service transfer *** To be established at the end of RLH 1st phase **** To be established at MES commencement date
Version 10.1
118
New Hospitals Programme
7.3.7 The purpose of the Liaison Committee is to oversee and manage the contractual relationship as set out in the Project Agreement (Clause 12). The Project Agreement (known as the PA) is the contract between the Trust and Capital Hospitals Limited for the New Hospitals Programme (see chapter 15). The Liaison Committee comprises three Trust and three Project Co. nominees under the chairmanship of the Trust. Membership is as follows:
Trust
■ Chief Executive ■ Director of Finance and Investment ■ Further Executive or Non Executive Director (TBA)
Capital Hospitals Ltd
Non Executive Chairman Director of Innisfree Further Director (TBA)
7.3.8 The functions of the Liaison Committee are:
To provide a means for the joint review of issues relating to the performance of the PA;
To provide a forum for joint strategic discussion, considering actual and anticipated changes in the market and business of the Trust and possible variations of the PA to reflect those changes or for more efficient performance of this Agreement; and
In certain circumstances, pursuant to Schedule 26 (Dispute Resolution Procedure), to provide a means of resolving disputes or disagreements between the parties amicably.
Joint Partnership Board
7.3.9 The purpose of the Joint Partnership Board (JPB)88 is to ensure that the project proceeds to a successful conclusion. It is this forum which will monitor progress in both the construction programme and the delivery of service and address any operational/service issues which can not been resolved at a lower level.
7.3.10 The Project Co. membership of the Joint Partnership Board would include the chief executive officers and senior operational managers.
7.3.11 The Trust membership will be drawn on similar lines, with the Trust’s Programme Director, together with senior managers responsible for the delivery of the project.
7.3.12 A report covering progress in the various elements of the project will be presented to the Joint Partnership Board in advance of the meeting. This will cover design and construction, services, financial and any other matters.
7.3.13 For day-to-day administration, it is recommended that four key committees are established: a Commissioning Steering Group, the Equipment Investment Committee, the HR Committee for staffing/transfer agreement issues and a Design
88 Further detail relating to the membership and function of the JPB can be found in Chapter 14, section 14.11.
Version 10.1
119
New Hospitals Programme
and Construction Committee for matters relating to design and construction. All of these committees will comprise Trust and Project Co. personnel.
7.3.14 The Commissioning Steering Group, HR Committee and Equipment Investment Committee, once established, will continue for the life of the project. The Design and Construction Committee will naturally cease to be required once the new facilities are operational.
Commissioning Steering Group
7.3.15 The primary purpose of the Commissioning Steering Group (CSG) is to coordinate and oversee the commissioning process for the new facilities in accordance with Schedule 12 of the PA. This will include interim services arrangements, decanting operations and service delivery itself. This group will be chaired by the Trust.
7.3.16 The Commissioning Steering Group will be led within Project Co. by the Senior General Manager with input from Project Co’s construction team, together with representatives from the equipment providers. The Trust representation will consist of the Programme Director, the Director of Operations, the Head of Clinical Commissioning and the service leads for equipment and soft FM.
7.3.17 For specific issues, the CSG may decide to establish sub-committees, with the ability to draw on additional appropriate specialists as necessary. In the early stages these are likely to include specific groups for decanting and service moves.
Equipment Investment Committee
7.3.18 The main purpose of the Equipment Investment Committee (EIC) is to ensure that the obligations of the parties as set out in the Project Agreement and Schedule 13 are met, such that key pieces of equipment (particularly medical equipment) are both specified and chosen to the agreed programme timetable, with full involvement of the Trust’s personnel. The Committee will be chaired by the Trust and will meet periodically, as necessary, to make recommendations to the Joint Partnership Board. Above all, this committee will be charged with ensuring there is:
• Flexibility to adapt to changing requirements;
• Appropriate equipment specifications;
• Relevant application of technology refreshment criteria;
• Lifecycling of equipment;
• Robust evaluation of tenders for short listed suppliers; and
• The highest level of maintenance.
7.3.19 The Trust representatives will be the Programme Director, the Head of Clinical Design Development, the Trust Equipment Lead, the Director of Finance (or nominee), the Medical Director (or nominee), Senior Nurse/Radiographer and the General Manager of Diagnostics and Therapeutics.
HR Committee
7.3.20 The primary purpose of the HR Committee is to oversee the transfer agreement for TUPE and ROE personnel.
7.3.21 The membership of the HR Committee for Project Co. will be led by the Senior General Manager with general managers from Project Co.’s operational management team, together with representatives from the service providers. The
Version 10.1
120
New Hospitals Programme
Trust lead will be the Director of Human Resources, supported by the PFI Performance Lead and Programme Director. It is envisaged that the pre-financial close HR Strategy Group will naturally move towards this structure, ensuring continuity for the project.
Design and Construction Committee
7.3.22 During the construction stage, a Design and Construction Committee will operate with the remit of ensuring that the design and construction operations are implemented successfully, with the minimum of inconvenience to the Trust’s ongoing operations.
7.3.23 The Trust representatives will be the Programme Director, the Technical Lead and two Construction Project Managers. Project Co.’s membership would include the Chief Executive, Construction Agent and other appropriate representatives from the building contractor and Project Co.’s operational team.
7.3.24 The Design and Construction Committee will meet on a regular basis. The agenda will include overall monitoring of the design and construction process, including progress, design development, interim works (phasing and decanting), equipment, IT, safety, quality and environmental issues, variations and commissioning.
7.3.25 The Design and Construction Committee may set up a number of sub-committees to address specific issues. Should this be the case, the committee will monitor the work and receive reports from these various sub-groups.
Financial Management Group
7.3.26 The Financial Management Group (FMG) will oversee the establishment of the systems and procedures necessary to ensure that the provisions of the Project Agreement and Schedule 18 are applied in a consistent and agreed manner between the parties. It will also ensure agreement on FM aspects of variations are maintained and clarify, quantify and agree the financial implications of any disputes.
7.3.27 The FMG is under the chairmanship of Project Co. with the following membership:
Project Co. Senior General Manager; Project Co. Accountant; Trust Nominees; Four Service Providers’ Nominees (as required)
7.3.28 The minutes of the FMG are submitted to the Joint Partnership Board for review
and outstanding issues requiring Joint Partnership Board action will be highlighted.
Service Performance Steering Group (SPSG)
7.3.29 The purpose of the SPSG is to coordinate and oversee the performance of hard, soft and sterile services and to resolve issues and disputes. In recognition of the different service requirements and coordination of these services, the SPSG will be supported by:
■ The Hard FM Performance Review Group
■ The Soft FM Performance Review Group
■ Sterile Services Performance Review Group
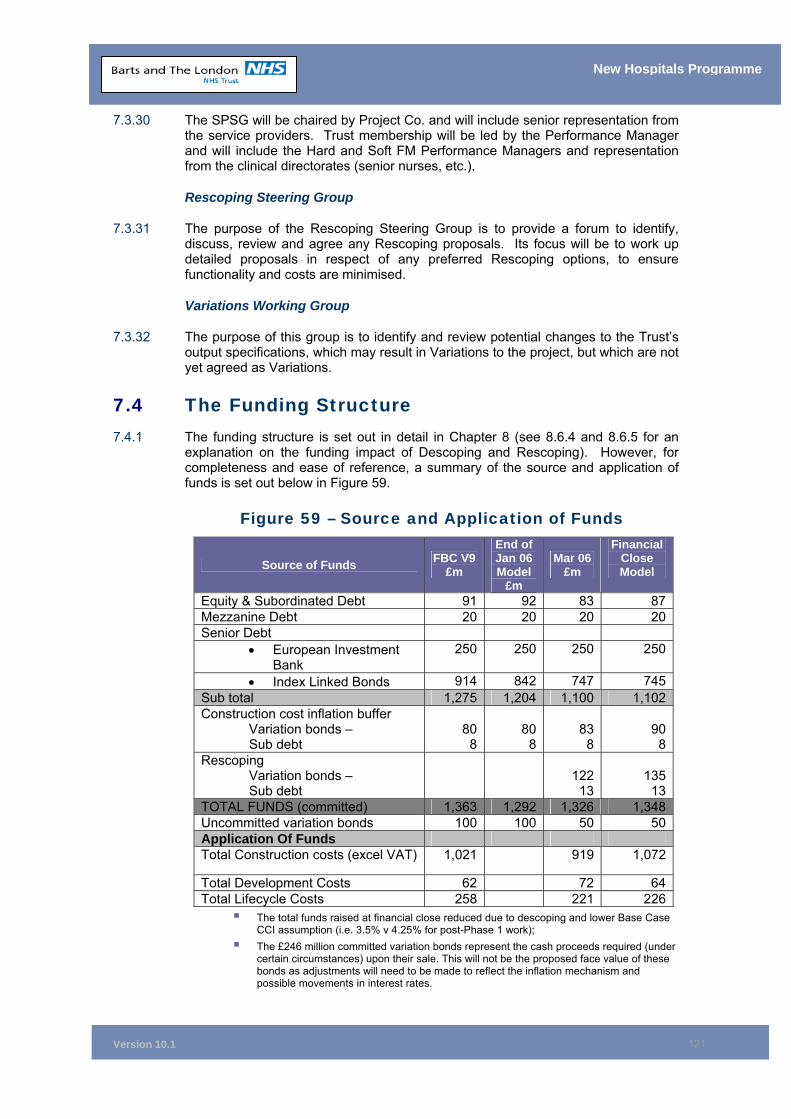
Version 10.1
121
New Hospitals Programme
7.3.30 The SPSG will be chaired by Project Co. and will include senior representation from the service providers. Trust membership will be led by the Performance Manager and will include the Hard and Soft FM Performance Managers and representation from the clinical directorates (senior nurses, etc.).
Rescoping Steering Group
7.3.31 The purpose of the Rescoping Steering Group is to provide a forum to identify, discuss, review and agree any Rescoping proposals. Its focus will be to work up detailed proposals in respect of any preferred Rescoping options, to ensure functionality and costs are minimised.
Variations Working Group
7.3.32 The purpose of this group is to identify and review potential changes to the Trust’s output specifications, which may result in Variations to the project, but which are not yet agreed as Variations.
7.4 The Funding Structure 7.4.1 The funding structure is set out in detail in Chapter 8 (see 8.6.4 and 8.6.5 for an
explanation on the funding impact of Descoping and Rescoping). However, for completeness and ease of reference, a summary of the source and application of funds is set out below in Figure 59.
Figure 59 – Source and Application of Funds
Source of Funds FBC V9 £m
End of Jan 06 Model
£m
Mar 06 £m
Financial Close Model
Equity & Subordinated Debt 91 92 83 87Mezzanine Debt 20 20 20 20Senior Debt
• European Investment Bank
250 250 250 250
• Index Linked Bonds 914 842 747 745Sub total 1,275 1,204 1,100 1,102Construction cost inflation buffer
Variation bonds – Sub debt
808
808
83
8 90
8Rescoping
Variation bonds – Sub debt
122
13 135
13TOTAL FUNDS (committed) 1,363 1,292 1,326 1,348Uncommitted variation bonds 100 100 50 50Application Of Funds Total Construction costs (excel VAT) 1,021 919 1,072
Total Development Costs 62 72 64Total Lifecycle Costs 258 221 226
The total funds raised at financial close reduced due to descoping and lower Base Case CCI assumption (i.e. 3.5% v 4.25% for post-Phase 1 work);
The £246 million committed variation bonds represent the cash proceeds required (under certain circumstances) upon their sale. This will not be the proposed face value of these bonds as adjustments will need to be made to reflect the inflation mechanism and possible movements in interest rates.
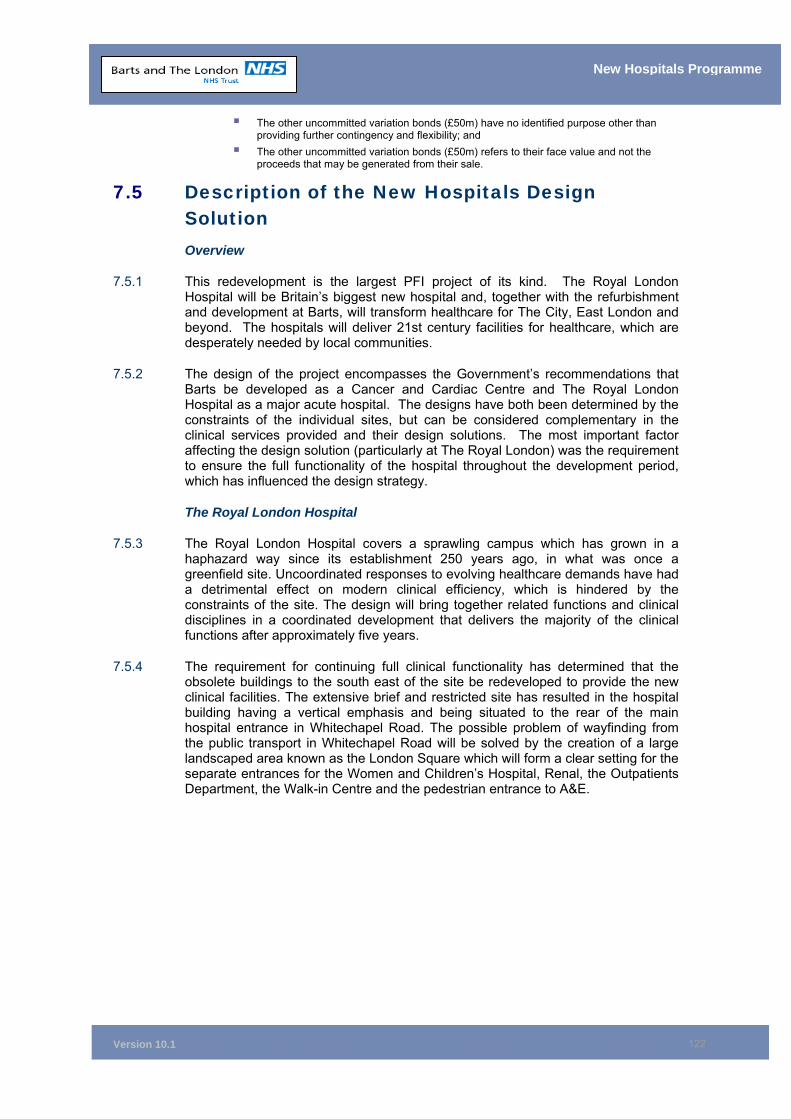
Version 10.1
122
New Hospitals Programme
The other uncommitted variation bonds (£50m) have no identified purpose other than providing further contingency and flexibility; and
The other uncommitted variation bonds (£50m) refers to their face value and not the proceeds that may be generated from their sale.
7.5 Description of the New Hospitals Design Solution Overview
7.5.1 This redevelopment is the largest PFI project of its kind. The Royal London Hospital will be Britain’s biggest new hospital and, together with the refurbishment and development at Barts, will transform healthcare for The City, East London and beyond. The hospitals will deliver 21st century facilities for healthcare, which are desperately needed by local communities.
7.5.2 The design of the project encompasses the Government’s recommendations that Barts be developed as a Cancer and Cardiac Centre and The Royal London Hospital as a major acute hospital. The designs have both been determined by the constraints of the individual sites, but can be considered complementary in the clinical services provided and their design solutions. The most important factor affecting the design solution (particularly at The Royal London) was the requirement to ensure the full functionality of the hospital throughout the development period, which has influenced the design strategy.
The Royal London Hospital
7.5.3 The Royal London Hospital covers a sprawling campus which has grown in a haphazard way since its establishment 250 years ago, in what was once a greenfield site. Uncoordinated responses to evolving healthcare demands have had a detrimental effect on modern clinical efficiency, which is hindered by the constraints of the site. The design will bring together related functions and clinical disciplines in a coordinated development that delivers the majority of the clinical functions after approximately five years.
7.5.4 The requirement for continuing full clinical functionality has determined that the obsolete buildings to the south east of the site be redeveloped to provide the new clinical facilities. The extensive brief and restricted site has resulted in the hospital building having a vertical emphasis and being situated to the rear of the main hospital entrance in Whitechapel Road. The possible problem of wayfinding from the public transport in Whitechapel Road will be solved by the creation of a large landscaped area known as the London Square which will form a clear setting for the separate entrances for the Women and Children’s Hospital, Renal, the Outpatients Department, the Walk-in Centre and the pedestrian entrance to A&E.
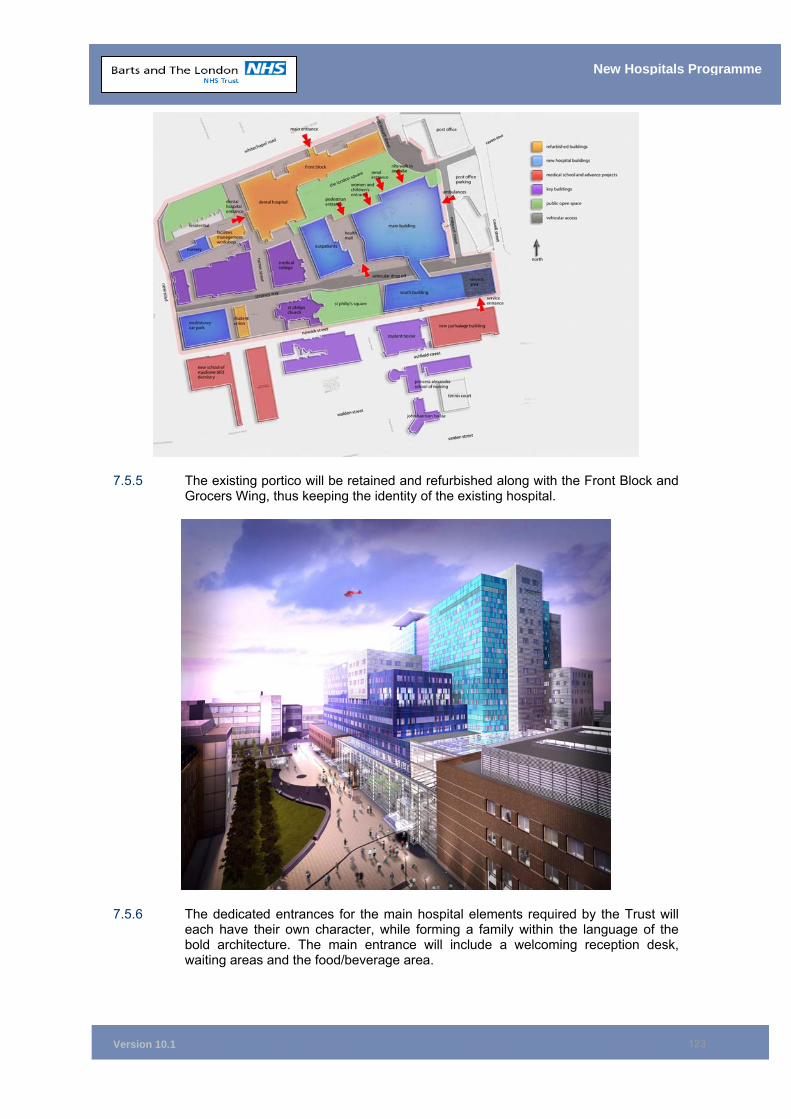
Version 10.1
123
New Hospitals Programme
7.5.5 The existing portico will be retained and refurbished along with the Front Block and Grocers Wing, thus keeping the identity of the existing hospital.
7.5.6 The dedicated entrances for the main hospital elements required by the Trust will each have their own character, while forming a family within the language of the bold architecture. The main entrance will include a welcoming reception desk, waiting areas and the food/beverage area.
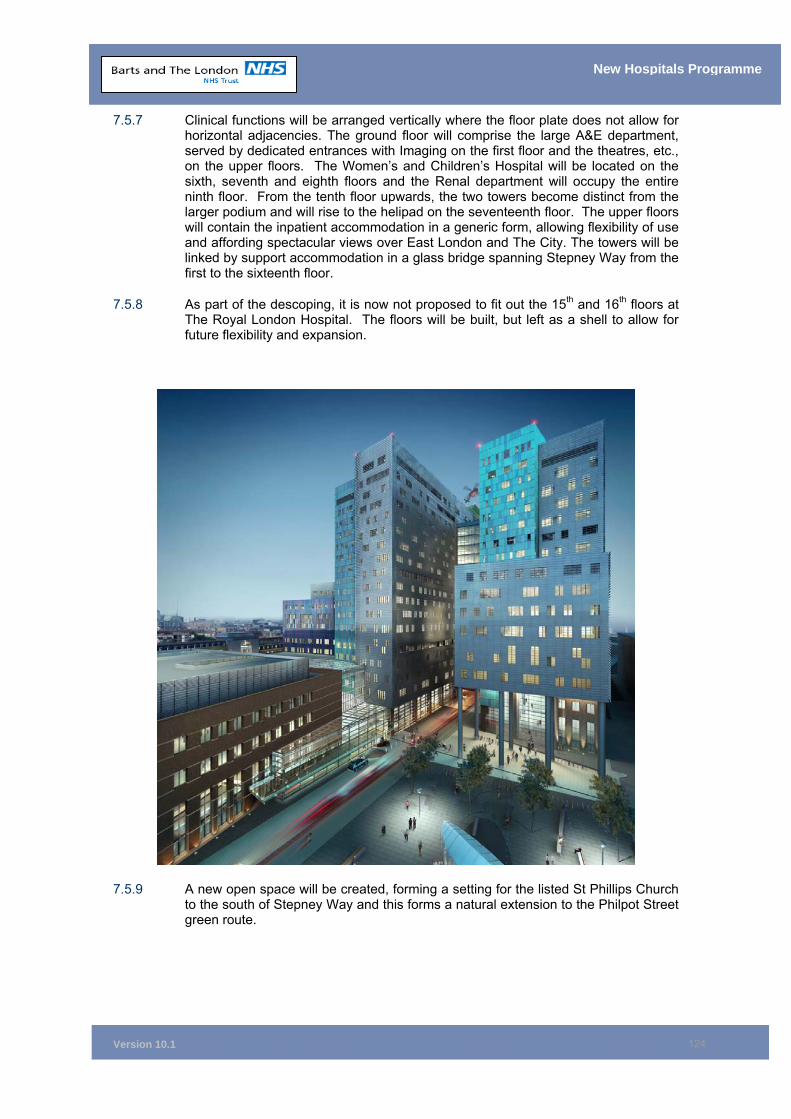
Version 10.1
124
New Hospitals Programme
7.5.7 Clinical functions will be arranged vertically where the floor plate does not allow for horizontal adjacencies. The ground floor will comprise the large A&E department, served by dedicated entrances with Imaging on the first floor and the theatres, etc., on the upper floors. The Women’s and Children’s Hospital will be located on the sixth, seventh and eighth floors and the Renal department will occupy the entire ninth floor. From the tenth floor upwards, the two towers become distinct from the larger podium and will rise to the helipad on the seventeenth floor. The upper floors will contain the inpatient accommodation in a generic form, allowing flexibility of use and affording spectacular views over East London and The City. The towers will be linked by support accommodation in a glass bridge spanning Stepney Way from the first to the sixteenth floor.
7.5.8 As part of the descoping, it is now not proposed to fit out the 15th and 16th floors at The Royal London Hospital. The floors will be built, but left as a shell to allow for future flexibility and expansion.
7.5.9 A new open space will be created, forming a setting for the listed St Phillips Church to the south of Stepney Way and this forms a natural extension to the Philpot Street green route.

Version 10.1
125
New Hospitals Programme
7.5.10 The existing historic buildings, such as the Front Block, will be refurbished to provide more suitable non-medical accommodation such as offices. Alexandra Wing is 30 years old and will be refurbished to provide accommodation for the Dental Hospital89.
7.5.11 The design of the buildings will reflect the environment and vibrancy of Whitechapel by the bold use of colour in the modular glazing system. The glazing will allow for the flexible planning of the interiors of the hospital, yet provide a varied treatment to the faces of the large towers. The addition of the stainless steel filigree features on the south, east and west elevations will reduce the scale of the towers. The lower floors of the main building will use terracotta facing, acknowledging the masonry construction prevalent in the Whitechapel area.
7.5.12 The proposals at The Royal London Hospital represent an opportunity to substantially improve the clinical adjacencies and the healthcare environment for patients and staff. The iconic nature of the development will give a new public identity to the hospital making the hospital a vital part of the regeneration of Whitechapel.
St Bartholomew’s Hospital
7.5.13 Barts in Smithfield will be developed as a Cancer and Cardiac Centre. The present poor adjacencies, caused by important departments being located off the “island” site, will be addressed by the construction of a co-ordinated medical facility situated in the south eastern corner of the site. This will remove the need to move patients across public roads, as is the case at present. The new building will contain the majority of the clinical functions and the existing buildings will be refurbished to provide generally non-clinical accommodation such as offices. East Wing will be retained and sympathetically refurbished as cardiac offices, a function more suited to a listed building.
89 This is dependant on the Trust seeking approval to proceed with Phase 3 of the development at The London (see para. 7.7.8)
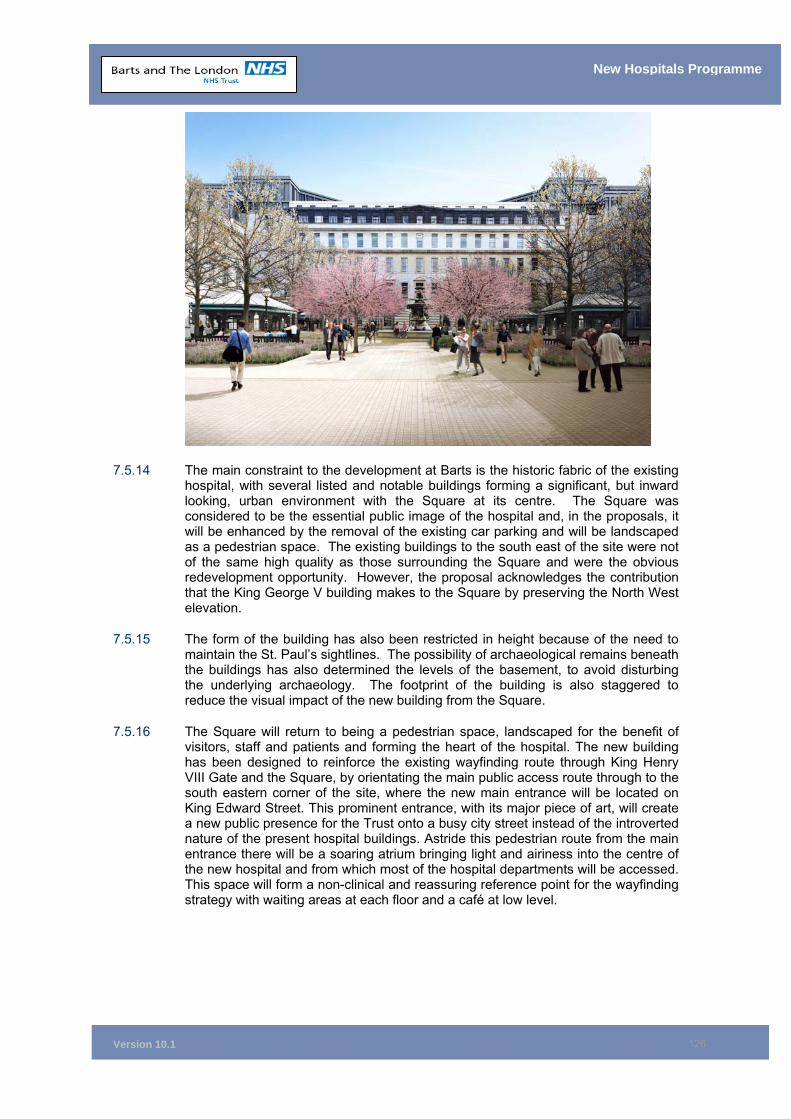
Version 10.1
126
New Hospitals Programme
7.5.14 The main constraint to the development at Barts is the historic fabric of the existing hospital, with several listed and notable buildings forming a significant, but inward looking, urban environment with the Square at its centre. The Square was considered to be the essential public image of the hospital and, in the proposals, it will be enhanced by the removal of the existing car parking and will be landscaped as a pedestrian space. The existing buildings to the south east of the site were not of the same high quality as those surrounding the Square and were the obvious redevelopment opportunity. However, the proposal acknowledges the contribution that the King George V building makes to the Square by preserving the North West elevation.
7.5.15 The form of the building has also been restricted in height because of the need to maintain the St. Paul’s sightlines. The possibility of archaeological remains beneath the buildings has also determined the levels of the basement, to avoid disturbing the underlying archaeology. The footprint of the building is also staggered to reduce the visual impact of the new building from the Square.
7.5.16 The Square will return to being a pedestrian space, landscaped for the benefit of visitors, staff and patients and forming the heart of the hospital. The new building has been designed to reinforce the existing wayfinding route through King Henry VIII Gate and the Square, by orientating the main public access route through to the south eastern corner of the site, where the new main entrance will be located on King Edward Street. This prominent entrance, with its major piece of art, will create a new public presence for the Trust onto a busy city street instead of the introverted nature of the present hospital buildings. Astride this pedestrian route from the main entrance there will be a soaring atrium bringing light and airiness into the centre of the new hospital and from which most of the hospital departments will be accessed. This space will form a non-clinical and reassuring reference point for the wayfinding strategy with waiting areas at each floor and a café at low level.
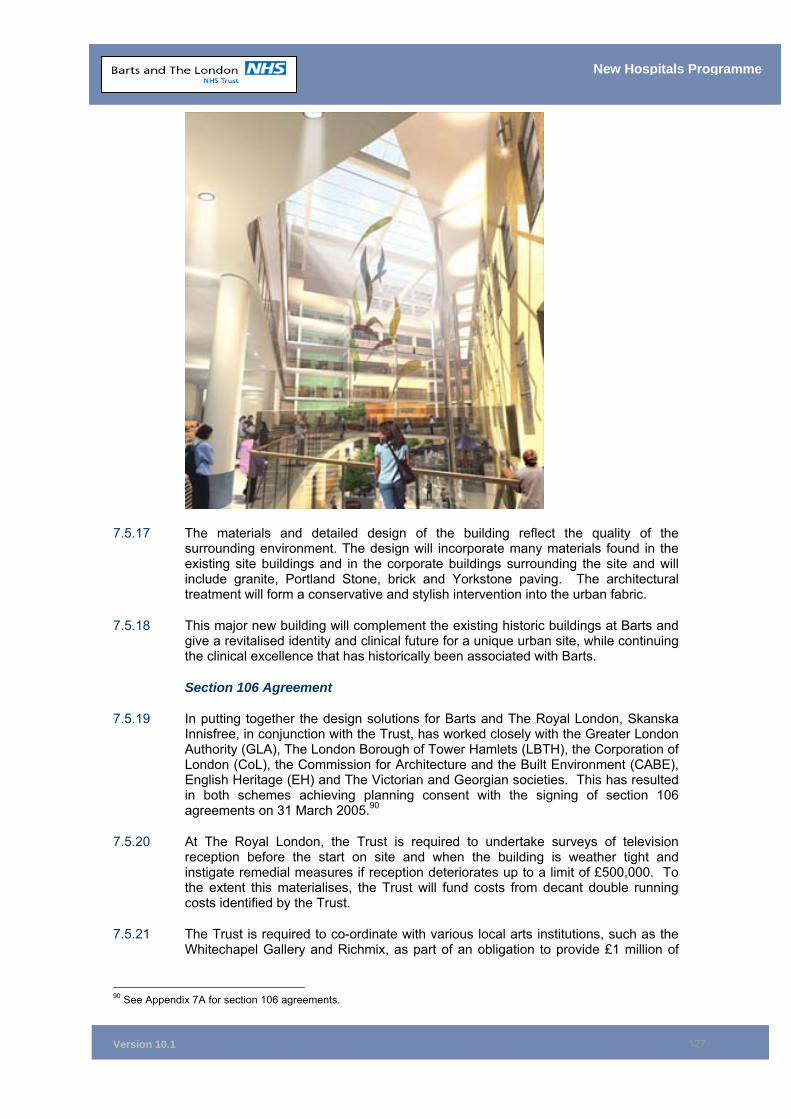
Version 10.1
127
New Hospitals Programme
7.5.17 The materials and detailed design of the building reflect the quality of the surrounding environment. The design will incorporate many materials found in the existing site buildings and in the corporate buildings surrounding the site and will include granite, Portland Stone, brick and Yorkstone paving. The architectural treatment will form a conservative and stylish intervention into the urban fabric.
7.5.18 This major new building will complement the existing historic buildings at Barts and give a revitalised identity and clinical future for a unique urban site, while continuing the clinical excellence that has historically been associated with Barts.
Section 106 Agreement
7.5.19 In putting together the design solutions for Barts and The Royal London, Skanska Innisfree, in conjunction with the Trust, has worked closely with the Greater London Authority (GLA), The London Borough of Tower Hamlets (LBTH), the Corporation of London (CoL), the Commission for Architecture and the Built Environment (CABE), English Heritage (EH) and The Victorian and Georgian societies. This has resulted in both schemes achieving planning consent with the signing of section 106 agreements on 31 March 2005.90
7.5.20 At The Royal London, the Trust is required to undertake surveys of television reception before the start on site and when the building is weather tight and instigate remedial measures if reception deteriorates up to a limit of £500,000. To the extent this materialises, the Trust will fund costs from decant double running costs identified by the Trust.
7.5.21 The Trust is required to co-ordinate with various local arts institutions, such as the Whitechapel Gallery and Richmix, as part of an obligation to provide £1 million of
90 See Appendix 7A for section 106 agreements.
Version 10.1
128
New Hospitals Programme
public art (including any necessary infrastructure). The Trust intends to raise the money for the art projects from voluntary donations over the construction period.
7.5.22 The pavements, etc., surrounding the site are to be renewed as an obligation on the Trust to renovate the public highway in the conservation area. The cost (£1.6 million) is within Project Co’s bid.
7.5.23 The Trust has also entered into an obligation regarding the helipad operations, based upon the existing section 106 agreement for the temporary helipad, restricting hours of use and flight paths to minimise disturbance to the neighbours.
7.5.24 At Barts, the Trust is again to provide public art to the value of £300,000 with at least one major piece to be located in the main entrance in King Edward Street. This will be met by voluntary donations.
7.5.25 The Trust is also required to renew the pavement around the perimeter of the site to a value of £400,000. This cost has been the subject of discussions between Project Co. and the Trust and a 50/50 split has been agreed with the Trust funding the £200,000. This will be in 2014/15 and the Trust will use either its block capital allocation or borrowings if the FT regime is applicable.
7.5.26 The Trust is also required to permanently remove all parking from the Barts Square, returning it to a landscaped pedestrian space for the benefit of patients, staff and visitors.
Clinical Output Specifications
7.5.27 The overall design philosophy adopted for the project was to make the patient the central focus of healthcare provision.
7.5.28 This philosophy required the mapping and understanding of patient flows for each specialty, encompassing:
How patients enter the system;
The types of investigation undertaken; and
What happens during a patient's stay and discharge process.
7.5.29 The outcome of this work, which involved clinicians from across the Trust, was a model for patient flow requirements which identified:
‘Best fit” of departmental adjacencies to facilitate effective and efficient care pathways for patients from the moment they enter the hospitals; and
The location of essential rooms, all of which were identified in the clinical and departmental output specifications for the project.
7.5.30 The PFI solution has been developed to meet these clinical specifications.
Quality of the Internal and External Environment
7.5.31 The architectural output specifications identified the Trust’s requirements in relation to construction, external and internal finishes, external and courtyard landscaping, access requirements and wayfinding.
7.5.32 The building services engineering output specification identified the Trust’s requirements with regard to the full range of engineering services. These specifications support the provision of healthcare, create the optimum environment
Version 10.1
129
New Hospitals Programme
for the care of patients and provide a safe and healthy working environment for staff.
7.5.33 The PFI solution has been developed to reflect these specifications. Full design specifications have been obtained and tested against the Achieving Excellence in Design Evaluation Toolkit (AEDET)91.
Engineering Solution
7.5.34 The Trust has agreed the design with the preferred partner and it largely meets the Trust’s original requirements. Engineering policies have been reviewed and discussed with certain changes and modifications having been incorporated to comply with HTM’s, HBN’s, other mandatory standards and to meet the Trust’s expectations. A programme of workshops has been undertaken with the Preferred Bidder, to ensure that Project Co.’s proposals fully reflect the requirements and expectations of the Trust. All of the agreed engineering solutions are reflected in the Trust’s construction requirements. For example, the lift solution proposed by Project Co. was analysed by the Trust, then discussed in a workshop with Project Co. The result of this process was a substantial increase in the lift provision for the new hospitals. The 38 fully developed and refined Project Co. engineering proposals are detailed in the Estates Annex (See Appendix E15).
7.5.35 To facilitate agreement of the engineering solution, SI provided the following:
■ Policy documents which reflect (in full) the agreed detailed engineering solution including the revised lift provision, energy efficient design solutions and agreed refinements;
■ Schematics and drawn information, which provide detail of the agreed proposals and the refined Trust construction requirements. Hard detail of the components of the plant and equipment, etc., have been included, the final refinement of which will be addressed in the agreed schedule of Reviewable design date (RDDs);
■ Plans for some of the building engineering solution, which identify main horizontal and vertical service distribution routes and set out the proposed maintenance arrangements;
■ Site layouts, which show (to an extent) the provision and disposition of the services. Detailed information of some areas remain outstanding and will be the subject of review in the schedule of reviewable design data; and
■ Specifications proposed by SI and detailed in Project Co.’s proposals, although these will not be fully developed until after financial close as specified in the reviewable design data schedule.
Energy
7.5.36 The PFI solution offers a simple approach to energy use, including simple cost effective energy conservation measures.
7.5.37 Whilst it is true that the majority of the existing estate is of poor energy performance, much of the existing estate does not form part of the final steady state scheme, through either demolition/replacement, new build or discontinued use. Significant sections of the existing estate to be retained will either undergo major refurbishment as part of the scheme or have already been refurbished by the Trust as advance works. Therefore, within the constraints of listed building consent, which
91 The results of the AEDET analysis is contained in the Estates Annex E14.
Version 10.1
130
New Hospitals Programme
applies to a proportion of the advance works/scheme refurbishments, certain improvements to the energy efficiency of the building and services are incorporated. Furthermore, the use of the refurbished buildings within the PFI scheme are utilised primarily as non-clinical space, whose energy demands and hours of operation are reduced compared with clinical space, which has a reducing effect on the overall energy consumptions and targets
7.5.38 The buildings were not designed as sealed buildings from the outset. In the ITN, the Trust specified minimising mechanical ventilation and maximising natural ventilation where possible. However, during the design development stage this was reconsidered due to a number of factors, including:
• Changing standards; • Increasing summertime standards; • The structure of the building made natural ventilation inappropriate – for
example, the height of the towers at The Royal London; • Concerns in respect of poor air quality in Whitechapel; • Concerns in respect of noise pollution; and • The Trust Board’s concern about high temperatures and patient/staff comfort.
7.5.39 Consequently, partial cooling of the building was proposed, ie the building would be ’sealed’. Adoption of this proposal was approved by the Trust Board.
7.5.40 This approach provides some advantages in terms of environmental control. In general, it is estimated that this method will deliver a 3˚C reduction in room temperature (in the summer) compared to employing natural ventilation in all areas. From the clinical perspective, it will also result in improved infection control. The current construction energy level is 58.65 GJ/100m3 per annum (excluding SSD) which is a significant improvement on current energy levels, despite the hospitals being heavily serviced. This target has been approved by the PFU and DH Estates. SSD will be included in setting operational targets, and energy usage will be monitored and regulated by the proposed Energy Forum, a joint body drawn from elected members of the Trust and Project Co.
7.5.41 Although it does not specifically meet the current government targets of 35-55 GJ/100m3 per annum, it is recognised that certain design aspects, such as deep plan, height and position of the towers (solar gain), full mechanical ventilation and partial cooling throughout the new build and some refurbished estate, impose pressures on the energy targets due to improved conditions over and above the NHS “norm” of maximising natural ventilation and minimising cooling. The Trust and Project Co. have agreed a range of energy conservation measures that have limited any increased use of energy. These measures include extensive building energy management systems, resulting in efficient running of plant and equipment. The most significant investment to reduce energy consumption is the development of the heat recovery scheme, which recovers large quantities of heat energy from the boiler flues, making a substantial contribution to energy efficiency at both sites. NHS Estates have been apprised of the measures taken and are of the view that all has been done from an engineering perspective to achieve maximum energy efficiency. However, they are unable to endorse the energy levels as they exceed government targets.
7.5.42 Consumerism guidance suggests that the provision of individual room control is commendable, however, there are overriding clinical requirements that may be compromised by such an approach. Both Barts and The Royal London are acute referral hospitals which, in conjunction with elderly patient requirements, make it important to ensure that the correct environmental conditions are maintained to assist the recovery process. Full temperature control of rooms would also have an adverse impact on energy targets and increases energy costs would be directly attributable to the Trust.
Version 10.1
131
New Hospitals Programme
7.5.43 It should also be noted that the NHS Estates environmental assessment tool has been applied and that the scheme complies with the Government’s requirements, as set out in Achieving Sustainability In Construction Procurement – Sustainability Action Plan.
7.5.44 The requirement to reduce the size of the scheme will have an impact on energy targets, however, until such time as the detail of the preferred re-scoping option is worked up, the impact on energy targets is not known. The Trust has until April 2007 to flesh out the detail of the Rescoping proposals and understand the impact of the scheme, all of which will be provided in an addendum to this Full Business Case.
Compliance with Guidance and Legislation
7.5.45 Both the PSC and PFI solutions have been designed to comply with the appropriate guidance and legislation.
7.5.46 Where SI have not complied in the design, a schedule of non-compliance has been provided and agreed by the Trust. In general terms, derogations have been agreed where clinical functionality and other criteria have not been compromised. The updated compliance schedule is included within the Estates Annex at Appendix E21.
Consumerism
7.5.47 In addition, the Trust and the PFI partner have complied with consumerism requirements as far as possible given the proportion of retained estate. The Trust is developing the new hospitals on its existing sites, therefore the solution is, of necessity, subject to significant site constraints and has to be a deep plan and high rise solution. The consumerism requirement in relation to space around the beds is compliant and 40% of the beds will be in single rooms.92
7.5.48 Overall, the solution works from a clinical, risk management and manual handling perspective. Details of the proforma issued at ITN and a completed consumerism report can be found in the Estates Annex93.
Flexibility
7.5.49 The new hospital buildings are designed to allow for changes to the internal configuration. At Barts, this is achieved by having a standard internal 9 metre x 9 metre grid of columns throughout. The only exception is where the grid is adapted to follow the curve of Little Britain in the south east wing and where the grid is trimmed on the northern face by the adaptation of the south west wing to the King George V building (which is retained and refurbished).
7.5.50 The structural floor slab has been designed principally as a slab to enable a degree of flexibility for relocation of internal walls and services. To some extent, wall location flexibility is also attained by having numerous mullion/solid panels to position internal walls.
7.5.51 Floor slabs are increased in thickness on the lower storey floors, where large/sensitive equipment may be placed in the future. There are also greater floor-to-floor heights at basement, ground and first floor levels to accommodate activities requiring diagnostic, imaging and therapeutic equipment (such as X-ray, MRI, CT, linear accelerators and surgical theatres).
92 See Appendix 0F for further details in relation to the Trust’s compliance with consumerism. 93 See Estates Annex Ref E22, E23 and E24.
Version 10.1
132
New Hospitals Programme
7.5.52 At Barts, flexibility is achieved through varied floor-to-floor heights to maintain horizontal continuity with the existing King George V building.
7.5.53 Full details of the design solutions at The Royal London and Barts are contained in the Estates Annex.94
7.6 Communicating the design solution 7.6.1 The Trust and the preferred partner recognised the importance of engaging with
stakeholders and the wider public around the design solution. With this in mind a comprehensive Communications Strategy (Appendix 6C) was drawn up and implemented. The strategy included:
■ Two editions of a special Newsletter, Neighbourhood Link, which was distributed to around 12,000 homes and businesses in the vicinity of the hospitals;
■ A freephone helpline 0800 028 1323;
■ Public exhibitions on the town planning applications at both hospitals in 2004 and 2005;
■ Mobile exhibitions in key community locations such as the East London Mosque, Sainsbury’s at Whitechapel and local health centres;
■ Permanent displays at all three of the Trust’s hospital sites;
■ Meetings and presentations to a wide range of key individuals and local organisations as well as statutory bodies; and
■ Websites set up by both the Trust and the preferred partner, providing details of the scheme.
7.6.2 The Communications Strategy was underpinned by a detailed matrix listing the different elements involved with each section of the strategy against a timeframe for implementation.
7.6.3 The preferred partner also produced an artist’s impression of the new hospitals and engaged a public relations firm who produced comprehensive consultation statements for both hospitals.
7.7 Decanting, Construction and Commissioning Programme
7.7.1 The scheme comprises two separate, but interdependent, building programmes, one for Barts and the other for The Royal London. The overarching need is to maintain the provision of services at full capacity during the rebuilding programme for each of the fully operational hospitals.
7.7.2 As part of the enabling works, a number of existing buildings have had to be vacated, involving the relocation of more than 1,000 staff. This work was a project in its own right (the Pre-Phase 1 Decant Project) and was managed as part of the New Hospitals Programme. It was funded separately and does not form part of this
94 See Estates Annex Ref E27 and E28.
Version 10.1
133
New Hospitals Programme
FBC. It is not, therefore, discussed in detail here, although there are obvious links to the delivery of this project and the construction programme for the PFI. As of June 2006, pre-Phase 1a decant has been completed, which included the majority of the buildings to be cleared prior to Phase 1. All that now remains to be completed, is pre-Phase 1b decant, which involves the decant of the East Wing at the RLH for which there is a 12 month programme attached at Appendix 7D.
7.7.3 The construction programme has been divided into three discrete phases, each phase incorporates decant, construction and commissioning periods. The overall construction programme at both sites is approximately 9 years.
7.7.4 Following the GLA modifications, the visual appearance of The Royal London has been enhanced by a significant refinement to the massing of the towers. The main enhancement to the scheme as a result of the GLA planning requirements, is the provision of a large public open space to the front of the new buildings. This approach enhances the flow of space and reduces the visual impact of these major structures.
The Royal London Phasing95
7.7.5 Phase 1 at The Royal London comprises two (multi-storey) towers and a 10-storey podium building. This significant construction will provide all of the new inpatient areas at the hospital, some 905 beds (192 of which will be mothballed initially (15th and 16th Floors), unless activity demands operationalising the full capacity of the building and the necessary approvals and additional funding have been secured). In fact, Phase 1 provides 70% of the overall clinical area of the entire PFI project and covers an area of 174,000 m2. The current programme indicates that Phase 1 will be completed within 4 years 8 months.
7.7.6 Phase 2 is fundamentally the refurbishment of the existing buildings on The Royal London site which are to remain and the provision of a significant new building development. A new Outpatients Department (OPD) will be provided, with a large atrium joining the first phase and the second phase developments together. Phase 2 is currently programmed to be completed within a further 2 years and 8 months.
7.7.7 Phase 3 is limited to car parking and landscaping and is programmed to be completed within a further two years.
7.7.8 However, as part of the cost reduction solution, Phases 2 and 3 will only be undertaken if the Trust can show that activity demands it and necessary funding is available and approved.
Barts Phasing
7.7.9 The initial stage of the Barts project is to demolish the Queen Mary Wing (QMW), building on the Barts site, the tower and the majority of King George V (KGV). The external façade facing the square will remain intact, as an integral part of the conservation of the Barts square. The Barts development will provide a state of the art Oncology Unit and extensive, highly advanced, cardiac facilities. The Barts development will provide 343 beds over Phases 1 and 2 (68 of which will initially be mothballed). Phase 1 provides 23,000m2 (125 beds approximately), which are predominately the advanced cardiac facilities. The remaining 218 beds will be provided during Phase 2, which will provide a state of the art cancer care centre.
95 A high level site map showing the detail of the phased developments at Barts and The Royal London is attached at Appendix 7B.
Version 10.1
134
New Hospitals Programme
7.7.10 Phase 2 includes the western area of the new build site, the residential staff quarters and Pathology. This phase is programmed to be completed within a further 2 years 6 months.
7.7.11 Phase 3 comprises the redevelopment of the energy centre, car parking and landscaping and is programmed to be completed within a further 2 years 6 months.
7.7.12 As with the RLH development, certain elements of phases 2 and 3 will now only be undertaken if the Trust can show that activity is as predicted and the additional capacity is required and then only if the necessary DH and HMT approvals and funding are secured.
Overall
7.7.13 Completion of Phase 1 on each site provides about 70% of all clinical accommodation (66% by capital cost).
7.7.14 The Trust has gone to great lengths and involved relevant critical stakeholders to ensure that the programme enables clinical functionality to be maintained throughout the construction phase at both sites. This same engagement will continue in assessing the descoping options which will be assessed for clinical functionality. All interdependencies in relation to cross-site decanting activities are reflected in the programmes appended at Appendices 7D and 14F. The Trust is therefore confident that the need to provide best clinical care while meeting the bidder’s construction programme, can be successfully achieved.
7.8 Fire Strategy 7.8.1 The Fire Strategy has been endorsed by NHS Estates and the Trust subject to the
rectification of those issues raised within the IBS (Trust’s advisors) report regarding fire compartmentation. Following initial concerns with SI’s fire solution in the towers, they redesigned the buildings by adding further bridge links between them. NHS Estates have indicated that they are content (in principle) with the solution, subject to a review of final floorplates at 1:200 level. The final comments from the Trust's advisers and NHS estates have been analysed by the Trust and Project Co. and do not impact on the overall design, but have been included in the agreed reviewable design data schedule to ensure their inclusion in the final detailed design. The fire strategy will be revisited in respect of the descoping solution, to ensure the proposals meet all necessary requirements.
7.8.2 It is anticipated that a reasonable and practicable level of fire safety will be achieved for both sites.
7.9 Transport and Access Arrangements Overview
7.9.1 The Trust recognises the importance of minimising private car use as a means of transport to and from the Trust’s properties and the beneficial effects that this would have on both community health and the local environment. To this end, it has produced a Green Travel Plan96 in conjunction with the preferred provider.
7.9.2 The Green Travel Plan demonstrates a commitment to improving the health of the individual and the community, as well as helping the environment. Although it is difficult to quantify in a financial context, encouraging staff to walk and cycle means
96 Shown in Estates Annex E13.
Version 10.1
135
New Hospitals Programme
that they are likely to be fitter, healthier and less stressed. This potentially has a beneficial effect on:
■ Sickness absenteeism;
■ Parking spaces (land that could be utilised for new buildings); and, in the wider context
■ Traffic congestion and a reduction of pollutants in the atmosphere, which reduces the number of admissions to hospital for respiratory diseases.
7.9.3 The objectives of the Green Travel Plan are to:
■ Encourage staff, patients and visitors to adopt healthy modes of transport (walking and cycling) as a key part of a shift towards a healthier, more active and safer lifestyle;
■ Lead by example with an exemplary Green Travel Plan and to work in partnership with other organisations on the Trust's sites;
■ Minimise car use and facilitate healthier and more sustainable travel by improving facilities and providing information;
■ Eliminate unnecessary travel; and
■ Create an alliance with local authorities, transport providers and other major employers to promote sustainable travel in the Trust’s area.
Pedestrian/Cyclist
7.9.4 The Local Authority (LA) and allied agencies are keen to ensure that there is proper provision of pedestrian and cycle routes, both in the vicinity of the hospitals and on site. Currently there is recognition of the need to improve these on both of the Trust sites when the new hospitals are built. In particular, it is suggested within the broader streetscape proposals to provide a cycle path along the south side of Stepney Way.
7.9.5 Provision has also been made within the scheme for secure bicycle parking lockers, which are clustered around the site in various locations. Other facilities will include provision of staff changing accommodation with showers.
Public Transport
7.9.6 Both Barts and The Royal London are well served by London Transport buses. Bus stops are located outside both hospitals and there is easy access to the hospitals from these.
7.9.7 Additionally, discussions have been held with London Underground with regard to improving access to The Royal London from the Whitechapel tube station, located virtually opposite to the entrance of the existing hospital, across the busy Whitechapel Road. This station is to be refurbished and modernised. It is hoped to ensure that London Underground’s proposals will facilitate easy access to the new hospital at The Royal London.
Car Parking
7.9.8 The scheme provides for no long-term patient and visitor parking. The Trust’s original aspiration was for 1,200 car parking spaces. However, the ITN specified 600 spaces and following discussion with the preferred bidder, this was subsequently reduced to 450 based on reproviding like for like. The approved
Version 10.1
136
New Hospitals Programme
application allows for 322 spaces at The Royal London, all of which are required for staff usage. There are 49 spaces provided at Barts.
7.9.9 Provision at The Royal London for six short stay places has been provided. There are also drop off and pick up areas, concentrated along Stepney Way, accessed from a dedicated road lane.
7.9.10 However, as a result of DH intervention and the need to reduce the UC, much of this parking capacity is now at risk. For example, car parking within The London was facilitated by transfer of the Dental Hospital to refurbished premises in Alex Wing. If Phase 2 does not proceed, no parking will be available for staff on site. This is a planning issue which will require careful management. However, the Trust has 15 months to work up the detail of the descoping variations and initial proposals may well have to change to ensure that the Trust is not in breach of any planning applications.
7.9.11 The only other facilities available are public parking spaces for patients and visitors on neighbouring streets. The cost of using these facilities is controlled by the respective Local Authorities.
Disabled Parking
7.9.12 Provision has been made for disabled bays at ground floor level across the sites (6 at Barts and 28 at The Royal London).
Wayfinding
7.9.13 Due to the size and complexity of the hospital developments on both sites, the Trust was particularly concerned that patients and visitors should be able to find their way within the hospitals easily. The Trust has put wayfinding as a key priority for both the exterior and interior design solutions. The scheme therefore necessitates the adoption of a number of different strategies to assist wayfinding, as outlined briefly below.
7.9.14 Wayfinding at both Barts and the The Royal London is based on a system of landmarks, or iconographics, as an aid to orientation and identification. Use of external signs will not only be directional, but provide a visual identity to the environment through the use of colour, materials and form. At Barts, wayfinding is orientated around the atrium and the existing square and south eastern entrance to King Edward Street. At The Royal London, the primary wayfinding route is a landscaped route that links the main access routes through the hospital from Whitechapel Road to Commercial Road.
7.9.15 Separate, but complementary, signage will be used to assist with wayfinding for essential supplies, deliveries and services. Artwork, colour schemes, signage and furniture have been developed by the design team to create functional, aesthetically pleasing environments.
7.10 FM Services – The Approach Adopted FM Services
7.10.1 The consortium has provided an integrated solution to FM services, based on the “neighbourhood concept’. This concept centres on the provision of FM services to a zone, using dedicated staff who work closely with and are part of, the ward team. At the centre of the team is the housekeeping service, which co-ordinates and takes responsibility for the delivery of FM services at ward level. Within ward areas there
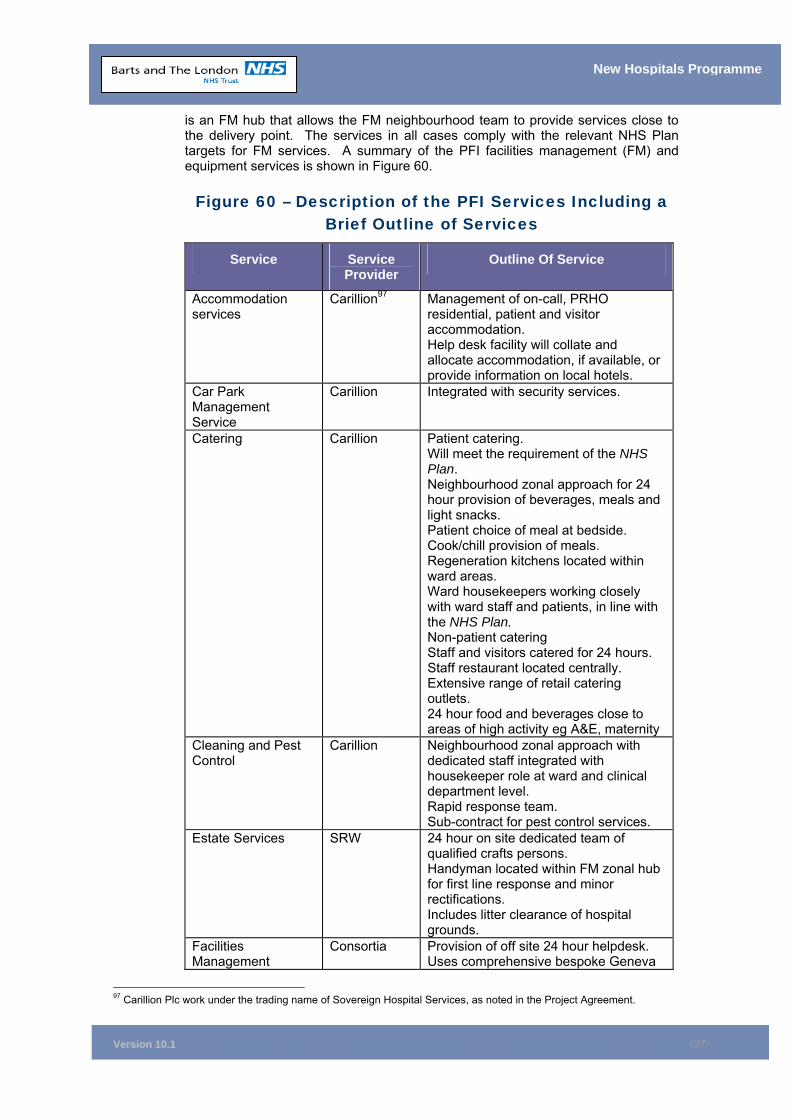
Version 10.1
137
New Hospitals Programme
is an FM hub that allows the FM neighbourhood team to provide services close to the delivery point. The services in all cases comply with the relevant NHS Plan targets for FM services. A summary of the PFI facilities management (FM) and equipment services is shown in Figure 60.
Figure 60 – Description of the PFI Services Including a Brief Outline of Services
Service Service Provider
Outline Of Service
Accommodation services
Carillion97 Management of on-call, PRHO residential, patient and visitor accommodation. Help desk facility will collate and allocate accommodation, if available, or provide information on local hotels.
Car Park Management Service
Carillion Integrated with security services.
Catering Carillion Patient catering. Will meet the requirement of the NHS Plan. Neighbourhood zonal approach for 24 hour provision of beverages, meals and light snacks. Patient choice of meal at bedside. Cook/chill provision of meals. Regeneration kitchens located within ward areas. Ward housekeepers working closely with ward staff and patients, in line with the NHS Plan. Non-patient catering Staff and visitors catered for 24 hours. Staff restaurant located centrally. Extensive range of retail catering outlets. 24 hour food and beverages close to areas of high activity eg A&E, maternity
Cleaning and Pest Control
Carillion Neighbourhood zonal approach with dedicated staff integrated with housekeeper role at ward and clinical department level. Rapid response team. Sub-contract for pest control services.
Estate Services SRW 24 hour on site dedicated team of qualified crafts persons. Handyman located within FM zonal hub for first line response and minor rectifications. Includes litter clearance of hospital grounds.
Facilities Management
Consortia Provision of off site 24 hour helpdesk. Uses comprehensive bespoke Geneva
97 Carillion Plc work under the trading name of Sovereign Hospital Services, as noted in the Project Agreement.
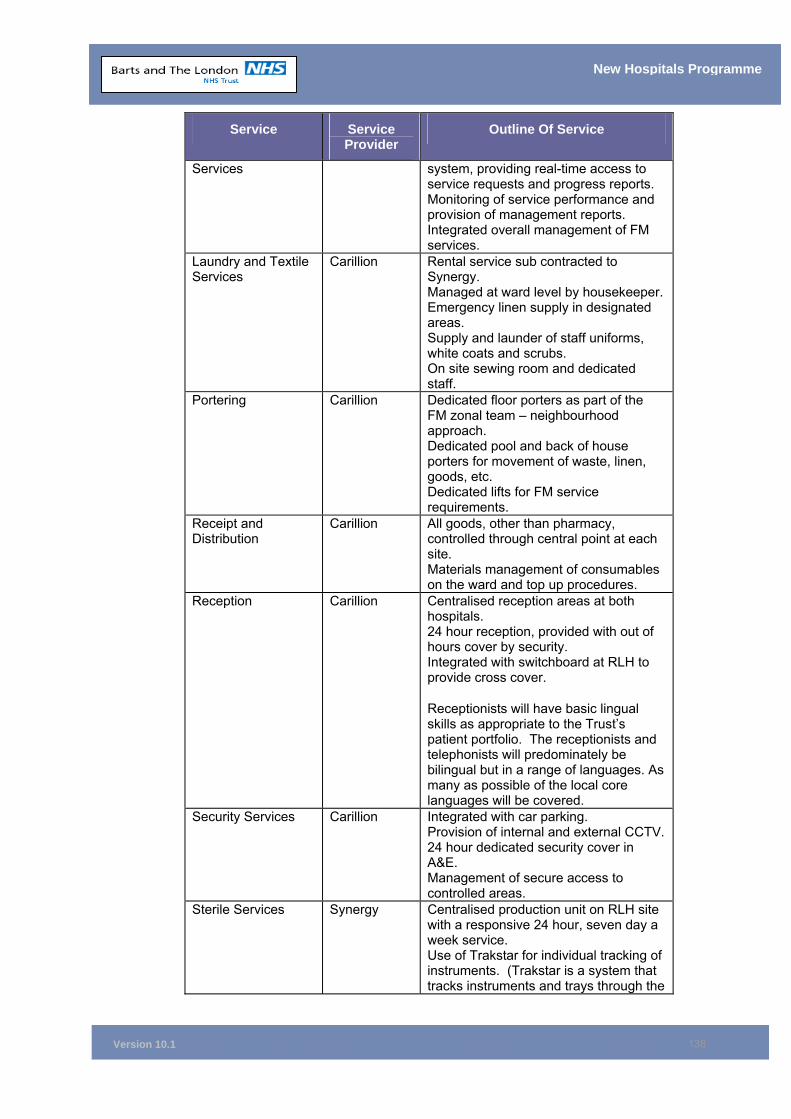
Version 10.1
138
New Hospitals Programme
Service Service Provider
Outline Of Service
Services system, providing real-time access to service requests and progress reports. Monitoring of service performance and provision of management reports. Integrated overall management of FM services.
Laundry and Textile Services
Carillion Rental service sub contracted to Synergy. Managed at ward level by housekeeper. Emergency linen supply in designated areas. Supply and launder of staff uniforms, white coats and scrubs. On site sewing room and dedicated staff.
Portering Carillion Dedicated floor porters as part of the FM zonal team – neighbourhood approach. Dedicated pool and back of house porters for movement of waste, linen, goods, etc. Dedicated lifts for FM service requirements.
Receipt and Distribution
Carillion All goods, other than pharmacy, controlled through central point at each site. Materials management of consumables on the ward and top up procedures.
Reception Carillion Centralised reception areas at both hospitals. 24 hour reception, provided with out of hours cover by security. Integrated with switchboard at RLH to provide cross cover.
Receptionists will have basic lingual skills as appropriate to the Trust’s patient portfolio. The receptionists and telephonists will predominately be bilingual but in a range of languages. As many as possible of the local core languages will be covered.
Security Services Carillion Integrated with car parking. Provision of internal and external CCTV. 24 hour dedicated security cover in A&E. Management of secure access to controlled areas.
Sterile Services
Synergy Centralised production unit on RLH site with a responsive 24 hour, seven day a week service. Use of Trakstar for individual tracking of instruments. (Trakstar is a system that tracks instruments and trays through the
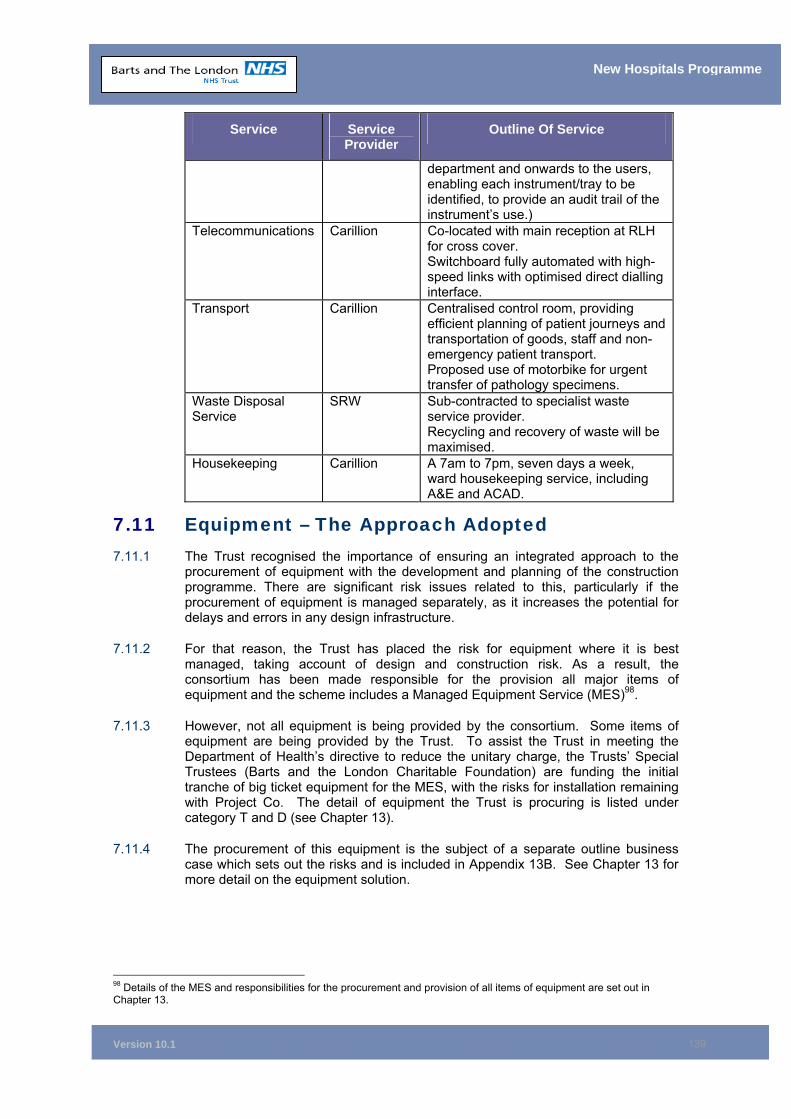
Version 10.1
139
New Hospitals Programme
Service Service Provider
Outline Of Service
department and onwards to the users, enabling each instrument/tray to be identified, to provide an audit trail of the instrument’s use.)
Telecommunications Carillion Co-located with main reception at RLH for cross cover. Switchboard fully automated with high-speed links with optimised direct dialling interface.
Transport Carillion Centralised control room, providing efficient planning of patient journeys and transportation of goods, staff and non-emergency patient transport. Proposed use of motorbike for urgent transfer of pathology specimens.
Waste Disposal Service
SRW Sub-contracted to specialist waste service provider. Recycling and recovery of waste will be maximised.
Housekeeping Carillion A 7am to 7pm, seven days a week, ward housekeeping service, including A&E and ACAD.
7.11 Equipment – The Approach Adopted 7.11.1 The Trust recognised the importance of ensuring an integrated approach to the
procurement of equipment with the development and planning of the construction programme. There are significant risk issues related to this, particularly if the procurement of equipment is managed separately, as it increases the potential for delays and errors in any design infrastructure.
7.11.2 For that reason, the Trust has placed the risk for equipment where it is best managed, taking account of design and construction risk. As a result, the consortium has been made responsible for the provision all major items of equipment and the scheme includes a Managed Equipment Service (MES)98.
7.11.3 However, not all equipment is being provided by the consortium. Some items of equipment are being provided by the Trust. To assist the Trust in meeting the Department of Health’s directive to reduce the unitary charge, the Trusts’ Special Trustees (Barts and the London Charitable Foundation) are funding the initial tranche of big ticket equipment for the MES, with the risks for installation remaining with Project Co. The detail of equipment the Trust is procuring is listed under category T and D (see Chapter 13).
7.11.4 The procurement of this equipment is the subject of a separate outline business case which sets out the risks and is included in Appendix 13B. See Chapter 13 for more detail on the equipment solution.
98 Details of the MES and responsibilities for the procurement and provision of all items of equipment are set out in Chapter 13.
Version 10.1
140
New Hospitals Programme
7.12 Approach to IT/Telecommunications Introduction
7.12.1 The ICT design is specific to the particular needs of the Trust and combines Project Co.’s previous best practice with an in-depth knowledge of new and emerging technologies, to provide a comprehensive infrastructure strategy for the Trust.
7.12.2 The Trust provides a very broad range of voice and data services to a wide range of users, covering many medical and administrative disciplines, in several locations. The potential complexity of this environment demands a well-defined business approach, supported by a comprehensive and forward looking ICT strategy.
7.12.3 The technical infrastructure for the data communications network will allow the Trust to connect active communications equipment at designated communications closets.
7.12.4 Data and telecommunications data outlet points are determined by staff setting out the room data sheets, to ensure that appropriate outlets are provided according to the functional requirement of the area. Further detail about the approach to and management of the IT selection is detailed in Chapter 17.
Design Goal and Philosophy
7.12.5 The key elements of the philosophy defined and agreed by Project Co. are:
Two sites one network (but each site to be capable of independent operation);
No single point of failure;
Integrated disaster recovery;
High performance providing investment protection; and
Support to the Trust’s systems plan and beyond.
7.12.6 Proposals are based on technologies currently available and generally accepted within the market. However, owing to the project’s long implementation timetable, new technology may be available at the time that procurement and deployment is required. In addition, some technologies proposed by Project Co. may be superseded.
7.12.7 Technologies that are superseded will be replaced, where required, with technologies that are in place at that time, in liaison and discussion with the Trust’s ICT Department. Any additional costs will be managed through the change control process.
7.12.8 No allowance is made in Project Co.’s proposals for ICT network hardware. This is subject to separate procurement. However, Project Co. has paid consideration to the integration of trust equipment and will liaise with the preferred supplier to ensure they meet with the contractual timescales and networks specified by the Trust and/or its ICT partners99.
7.12.9 Within the North East London Strategic Health Authority, London NHS Connecting for Health and the Capital Care Alliance there is commitment and support for Barts and The London to progress rapidly to implementation of the Care Record Service (CRS) to replace the existing PAS/HISS.
99 Full details of the ICT strategy can be found in Chapter 17.
Version 10.1
141
New Hospitals Programme
7.12.10 The Trust has planned its CRS Programme to correlate with the New Hospitals Programme. It depends on a clinical management system being available to provide support, eg the system is key to providing the sophisticated booking and scheduling and data access functionality required to manage the patients’ journey effectively.
7.13 The Sustainability of the Preferred Solution 7.13.1 The Trust adopted its Environmental Policy in August 2004. Among other
objectives the policy aims to:
■ Implement and maintain an environmental management system, in conjunction with the New Hospitals Project, which will ultimately achieve ISO 14001 accreditation;
■ Comply with all relevant environmental legislation, regulations and other NHS-specific requirements;
■ Develop an education and training programme for employees (both clinical and non-clinical), in order to inform staff of good practice, increase control of and reduce the Trust’s impact on, the environment;
■ Seek to reduce pollution, where reasonably practicable, by use of non-polluting techniques and practices;
■ Design new services and buildings to minimise their environmental impact;
■ Maximise the efficient use of energy, resources and raw materials in all activities;
■ Put into place economically viable waste segregation, recycling and waste minimisation schemes;
■ Improve the environmental impacts associated with the purchase and supply of products and services;
■ Develop, in conjunction with its partners, an environmentally sound fleet management and transportation strategy as part of the Green Transport Plan;
■ Promote the use of contracts arranged by the NHS Purchasing and Supply Agency, thereby benefiting from their environmental procurement work programme;
■ Integrate environmental considerations into the procurement process for contracts arranged at Trust level;
■ Encourage the purchase of goods manufactured from recycled products, i.e. purchasing of office stationery made from recycled paper where practicable;
■ Purchase goods with good durability and long, useful life;
■ Encourage the use of minimal packaging/re-usable packaging;
■ Require that only timber and wood products from sustainable and legal sources are purchased;
■ Avoid use of disposable non-clinical items where practicable, unless infection control guidelines would indicate otherwise; and
■ Consider alternatives to non-biodegradable cleaning agents and chlorine-based bleaches where practicable, in conjunction with infection control.
Version 10.1
142
New Hospitals Programme
7.13.2 To ensure this policy is implemented in relation to the New Hospitals Project, the Trust has engaged in dialogue with the preferred partner over a range of sustainability issues, including those where the consortium has a clear lead role such as:
■ Design and build of the new hospitals;
■ Waste management;
■ Energy and water use; and
■ Estate management.
7.13.3 It is also engaging in dialogue over areas where a partnership arrangement is necessary to achieve its objectives, including:
■ Green Transport Plan;
■ Sustainable regeneration;
■ Green purchasing; and
■ Community employment.
7.13.4 To structure this wide range of workstreams, a matrix has been developed that sets out the range of optimum sustainability outcomes against the operation and development of the Trust. 100
7.13.5 This approach allows for the most sustainable solutions to emerge, within the context of the design and affordability considerations. This process has been developed by the Implementing Sustainability Group, which includes both Trust and SI personnel. SI has supported this process through adopting a programme of “sustainability champions” for its design and construction team. This group meets regularly to track progress on sustainability targets. SI are also partners with Forum for the Future and its education arm, The Natural Step. The Natural Step and SI have held a series of workshops to raise awareness of the sustainability agenda.
7.14 Benefits to the Hospital Community 7.14.1 The Benefits of the scheme to both the hospital community and patients are set out
in Chapter 18.
7.15 Chapter Conclusion 7.15.1 The preferred solution is demonstrably robust and sustainable.
7.16 Chapter Appendices 7A Section 106 Agreements 7B High Level Site Map Showing Construction Phases 7C Sustainability Matrix 7D Pre-Phase 1B Decant Programme 7E Phase Breakdown SBH and RLH
100 See Appendix 7C for Sustainability Matrix.
Version 10.1
143
New Hospitals Programme
8 FINANCING THE SCHEME Synopsis – Financing the Scheme
This Chapter sets out: • The term of the agreement is (42 years from financial close) with the full
operational phase being approximately 32 years.
• The detail and outcome of the Trust’s decision to run a funding competition which resulted in improved terms from those submitted at BaFO.
• The contribution of the Barts and the London Charitable Foundation to the scheme.
• The detail of the funding sources are being used to finance the scheme with 90.3% coming from debt and 9.7% from equity. This includes a European Investment Bank (EIB) index-linked load of £250 million.
• Post-financial close, interest rate risk will lie with Skanska Innisfree.
• The Project Company’s (Project Co.) assumed internal real rate of return is 4.1% post-tax.
• Skanska Innisfree’s financial model assumes the composite trader tax status in addition to finance debtor accounting treatment.
• 100% of the service payment will be indexed annually in line with the Retail Prices Index (RPI). There is no fixed-rate inflator.
8.1 Introduction 8.1.1 This chapter sets out a high level breakdown of the costs of the scheme and how
the Unitary Charge is made up. It also details:
■ The consortium’s funding structure; ■ Their approach to funding the scheme; ■ The detail of the terms offered; and ■ The detail of the Charitable Foundation’s contribution to the scheme.
8.1.2 The chapter also provides an analysis and commentary on the funding structure from the Trust’s financial advisers.
8.2 Overview of the PFI Deal Term of the Agreement
8.2.1 The contract for the New Hospitals Project is based on version 3 of the NHS Standard Form Project Agreement (SFPA3).
8.2.2 The project term (concession period) is 42 years, inclusive of the construction period. In line with standard practice, the concession will commence from financial close.
8.2.3 The annual service payment payable by the Trust at steady state (2016/17) is £98.4 million a year at 1st April 2005 prices (£100.8 million at 2006/07 prices). Payment by the Trust is quarterly in advance as approved by the Department of Health Private Finance Unit (PFU) (see Appendix 8C).
Version 10.1
144
New Hospitals Programme
8.2.4 The service payment quoted above is the contracted amount payable by the Trust, as determined by the financial model at bond launch. This reflects a yield on the benchmark 2035 gilt of 1.188%, a spread to the gilt of 0.515% and an interest rate on the EIB loan of 1.55% as at bond launch.
Inflation
8.2.5 The typical position in health PFI projects is that the service payment will be adjusted each year only for the impact of inflation. The instructions to bidders advised that indexation should be related to the annual increase in the Retail Price Index (RPI), with the base assumption being set at 2.5% per annum. On this basis, the service payment would be subject to inflation increases from 01 April 2006 and annually thereafter, until the end of the concession. As the senior funding requirement is met entirely from index-linked funding (index-linked project bond and EIB loan), 100% of the service payment is indexed at RPI annually. No proportion of the service payment will be indexed annually by a fixed inflator. This is dealt with in more detail below.
Taxation
8.2.6 Skanska Innisfree has assumed composite trader tax status as well as finance debtor accounting. This is in line with current PFU guidance101.
8.3 Approach and Solution to Funding Barts and the London Charitable Foundation’s Contribution
8.3.1 To assist the Trust in achieving the reduction to the Unitary Charge required by DH and HMT, the Barts and the London Charitable Foundation were asked to assist in funding the capital requirement in respect of the provision of equipment for the Managed Equipment Service. Following discussions, the Charitable Foundation agreed to donate equipment covering the capital cost consequences of the initial tranche of medical equipment (i.e. up to the point when the first equipment refresh requirements arise). In financial terms this equates to approximately £25 - £30 million, thereby reducing the UC by £3.2 million per annum. The Trust has further assumed that all the MES equipment will be funded directly over the life of the MES contract, resulting in a total deduction to the UC of £3.8 million, but with a fall back that, within 2 years of financial close, the Trust can default to Project Co. funding the capital consequences of MES following initial installation (see Chapter 13 Equipment). More over in terms of adjustment:
• It would not be appropriate for the Charitable Foundation (CF) to commit to fund the full £70 million required to fund equipment purchases over the 15 year period of the initial MES contract at this stage. However, as per the letter from the Chairman of the CF (see annexe to Appendix 0G), it has agreed to look sympathetically on future requests from BLT for funding MES equipment depending on its available reserves at the time. The refresh costs will have an approximate capital cost of £25 million - £30 million (at current prices).
• The Trust would continue to expect to receive capital allocations either as Capital Resource Limit of under NHS Foundation Trust borrowing arrangements. There is capacity to borrow funds modelling the FT borrowing rules against the Trust’s I&E and balance sheets of between £3.2 million and £3.8 million per annum depending on negotiation and timing and if fully funded
101 Confirmation from the Inland Revenue (a code of practice 10 clearance) regarding the initial acceptability of this approach for this project is included in Appendix 8.A
Version 10.1
145
New Hospitals Programme
via the Unitary Charge. In the overall context of prudent assumptions on income growth, it is expected this would be affordable.
Project Co’s Funding Solution
8.3.2 As encouraged by the Trust, Skanska Innisfree maintained flexibility in its final funding solution beyond the BaFO period. Skanska Innisfree’s BaFO submission was based on a 100% wrapped fixed-rate bond with RPI swaps, to hedge the inflation risk inherent in the service payment indexation as, at the time, this appeared to offer the lowest financing cost to the Trust.
8.3.3 In addition, Skanska Innisfree will utilise the full £250 million of EIB index-linked funding. At the invitation to negotiate (ITN) stage, Skanska Innisfree assumed that the index-linked bond market would only have the economic capacity to absorb 50% of the proposed senior debt, with the remaining senior funding requirement being raised through the fixed-rate bond market.
8.3.4 However, experience with the Southern Derbyshire Hospital scheme’s transaction highlighted the fact that the market for index-linked bonds may not be able to absorb this proportion of index-linked paper. The Trust and Skanska Innisfree agreed to continue monitoring the market (through the selected bond managers) to ensure the most appropriate mix of funding at financial close.
8.3.5 At both ITN and BaFO stages, Skanska Innisfree provided a number of funding variants. These included a bank funded case, a floating rate case and a two tranche funding case. However these cases did not appear to provide the Trust with the best value for money and, on this basis, the most appropriate way forward was bond financing with a suitable mix of index-linked and fixed-rate bonds being issued.
8.3.6 In the run-up to bond launch, demand for index-linked monoline-wrapped project bonds was found to be strong and the spread over the gilt to be competitive compared with fixed rate bonds. Therefore, the final funding structure reflected 100% index-linked senior funding.
8.4 Funding Competition 8.4.1 The Trust maintained the option to require the preferred bidder to run a funding
competition post-appointment. This was in order to maintain flexibility in the mix of products for as long as possible and to obtain the most economically advantageous funding terms. The funding competition consisted of a competition for bond managers and a separate competition for monolines. The preliminary information memorandum (PIM) was issued in May 2004 in respect of the bond underwriter competition and in October 2004 in respect of the monoline competition.
8.4.2 Ten bids were received for the bond manager competition. Each of the bids was evaluated by Investec (Skanska Innisfree’s financial advisers) and PwC (the Trust’s financial advisers). From the initial submission a short list was agreed to take forward to the second stage of the process. The pricing of the short listed bidders compared with the BaFO pricing is set out below. Given the size of the transaction, the objective was to appoint joint bond managers.
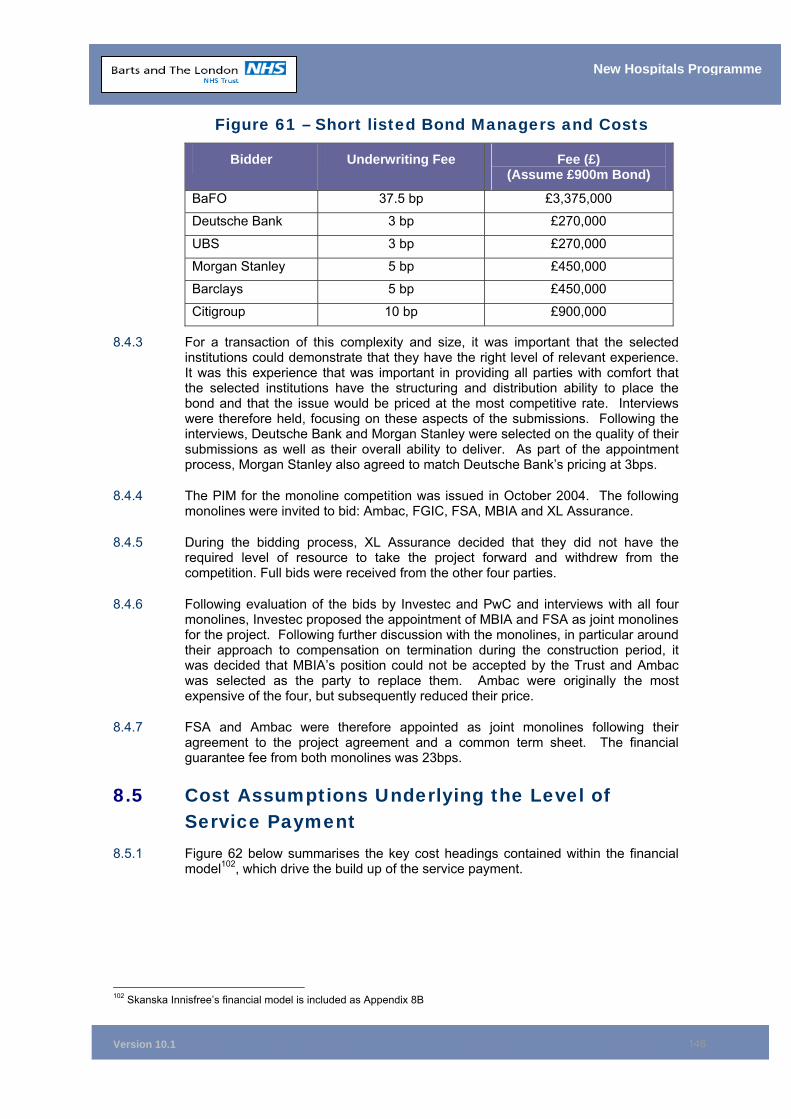
Version 10.1
146
New Hospitals Programme
Figure 61 – Short listed Bond Managers and Costs
Bidder Underwriting Fee Fee (£) (Assume £900m Bond)
BaFO 37.5 bp £3,375,000
Deutsche Bank 3 bp £270,000
UBS 3 bp £270,000
Morgan Stanley 5 bp £450,000
Barclays 5 bp £450,000
Citigroup 10 bp £900,000
8.4.3 For a transaction of this complexity and size, it was important that the selected institutions could demonstrate that they have the right level of relevant experience. It was this experience that was important in providing all parties with comfort that the selected institutions have the structuring and distribution ability to place the bond and that the issue would be priced at the most competitive rate. Interviews were therefore held, focusing on these aspects of the submissions. Following the interviews, Deutsche Bank and Morgan Stanley were selected on the quality of their submissions as well as their overall ability to deliver. As part of the appointment process, Morgan Stanley also agreed to match Deutsche Bank’s pricing at 3bps.
8.4.4 The PIM for the monoline competition was issued in October 2004. The following monolines were invited to bid: Ambac, FGIC, FSA, MBIA and XL Assurance.
8.4.5 During the bidding process, XL Assurance decided that they did not have the required level of resource to take the project forward and withdrew from the competition. Full bids were received from the other four parties.
8.4.6 Following evaluation of the bids by Investec and PwC and interviews with all four monolines, Investec proposed the appointment of MBIA and FSA as joint monolines for the project. Following further discussion with the monolines, in particular around their approach to compensation on termination during the construction period, it was decided that MBIA’s position could not be accepted by the Trust and Ambac was selected as the party to replace them. Ambac were originally the most expensive of the four, but subsequently reduced their price.
8.4.7 FSA and Ambac were therefore appointed as joint monolines following their agreement to the project agreement and a common term sheet. The financial guarantee fee from both monolines was 23bps.
8.5 Cost Assumptions Underlying the Level of Service Payment
8.5.1 Figure 62 below summarises the key cost headings contained within the financial model102, which drive the build up of the service payment.
102 Skanska Innisfree’s financial model is included as Appendix 8B
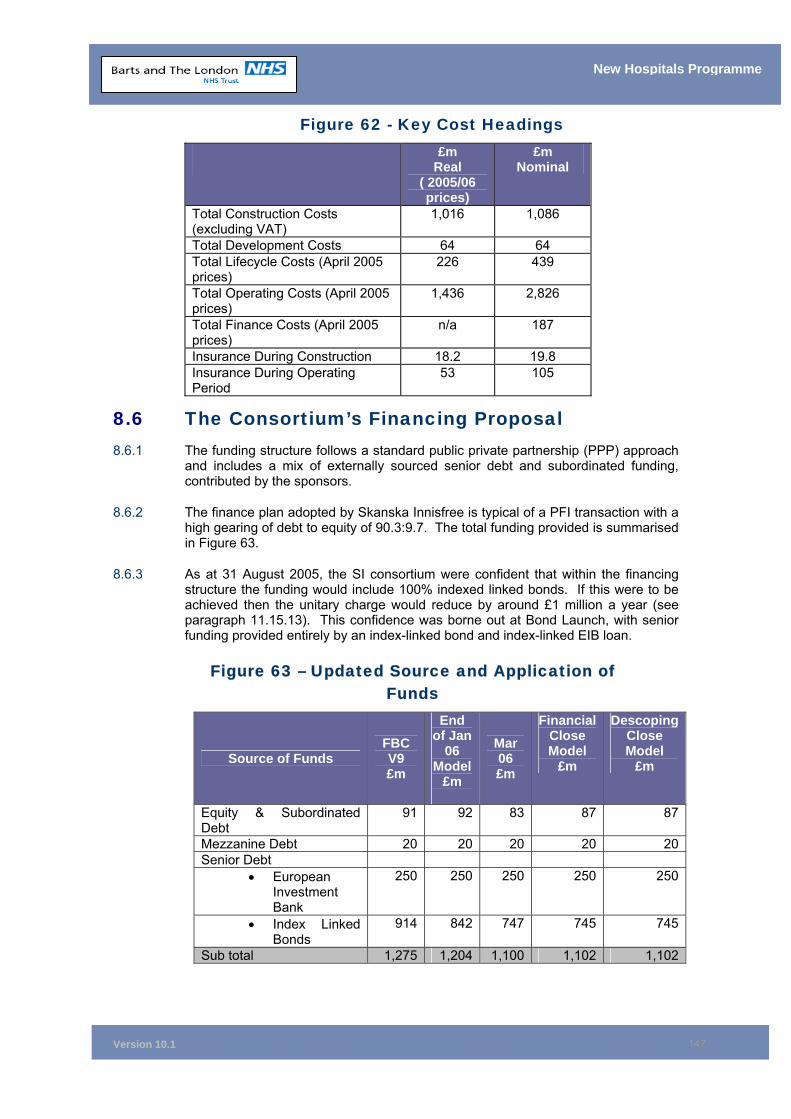
Version 10.1
147
New Hospitals Programme
Figure 62 - Key Cost Headings
£m Real
( 2005/06 prices)
£m Nominal
Total Construction Costs (excluding VAT)
1,016 1,086
Total Development Costs 64 64 Total Lifecycle Costs (April 2005 prices)
226 439
Total Operating Costs (April 2005 prices)
1,436 2,826
Total Finance Costs (April 2005 prices)
n/a 187
Insurance During Construction 18.2 19.8 Insurance During Operating Period
53 105
8.6 The Consortium’s Financing Proposal 8.6.1 The funding structure follows a standard public private partnership (PPP) approach
and includes a mix of externally sourced senior debt and subordinated funding, contributed by the sponsors.
8.6.2 The finance plan adopted by Skanska Innisfree is typical of a PFI transaction with a high gearing of debt to equity of 90.3:9.7. The total funding provided is summarised in Figure 63.
8.6.3 As at 31 August 2005, the SI consortium were confident that within the financing structure the funding would include 100% indexed linked bonds. If this were to be achieved then the unitary charge would reduce by around £1 million a year (see paragraph 11.15.13). This confidence was borne out at Bond Launch, with senior funding provided entirely by an index-linked bond and index-linked EIB loan.
Figure 63 – Updated Source and Application of Funds
Source of Funds FBC V9 £m
End of Jan
06 Model
£m
Mar 06 £m
Financial Close Model
£m
Descoping Close Model
£m
Equity & Subordinated Debt
91 92 83 87 87
Mezzanine Debt 20 20 20 20 20Senior Debt
• European Investment Bank
250 250 250 250 250
• Index Linked Bonds
914 842 747 745 745
Sub total 1,275 1,204 1,100 1,102 1,102
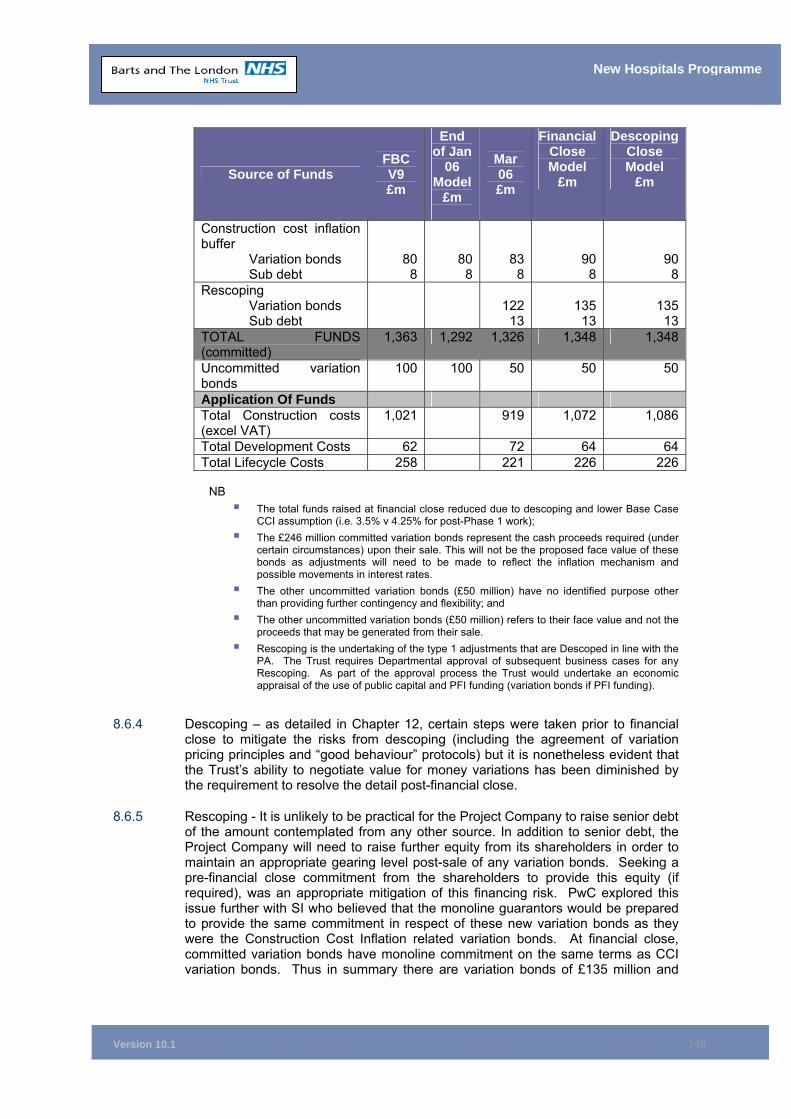
Version 10.1
148
New Hospitals Programme
Source of Funds FBC V9 £m
End of Jan
06 Model
£m
Mar 06 £m
Financial Close Model
£m
Descoping Close Model
£m
Construction cost inflation buffer
Variation bonds Sub debt
808
808
838
90 8
908
Rescoping Variation bonds Sub debt
12213
135
13 135
13TOTAL FUNDS (committed)
1,363 1,292 1,326 1,348 1,348
Uncommitted variation bonds
100 100 50 50 50
Application Of Funds Total Construction costs (excel VAT)
1,021 919 1,072 1,086
Total Development Costs 62 72 64 64Total Lifecycle Costs 258 221 226 226
NB
The total funds raised at financial close reduced due to descoping and lower Base Case CCI assumption (i.e. 3.5% v 4.25% for post-Phase 1 work);
The £246 million committed variation bonds represent the cash proceeds required (under certain circumstances) upon their sale. This will not be the proposed face value of these bonds as adjustments will need to be made to reflect the inflation mechanism and possible movements in interest rates.
The other uncommitted variation bonds (£50 million) have no identified purpose other than providing further contingency and flexibility; and
The other uncommitted variation bonds (£50 million) refers to their face value and not the proceeds that may be generated from their sale.
Rescoping is the undertaking of the type 1 adjustments that are Descoped in line with the PA. The Trust requires Departmental approval of subsequent business cases for any Rescoping. As part of the approval process the Trust would undertake an economic appraisal of the use of public capital and PFI funding (variation bonds if PFI funding).
8.6.4 Descoping – as detailed in Chapter 12, certain steps were taken prior to financial
close to mitigate the risks from descoping (including the agreement of variation pricing principles and “good behaviour” protocols) but it is nonetheless evident that the Trust’s ability to negotiate value for money variations has been diminished by the requirement to resolve the detail post-financial close.
8.6.5 Rescoping - It is unlikely to be practical for the Project Company to raise senior debt of the amount contemplated from any other source. In addition to senior debt, the Project Company will need to raise further equity from its shareholders in order to maintain an appropriate gearing level post-sale of any variation bonds. Seeking a pre-financial close commitment from the shareholders to provide this equity (if required), was an appropriate mitigation of this financing risk. PwC explored this issue further with SI who believed that the monoline guarantors would be prepared to provide the same commitment in respect of these new variation bonds as they were the Construction Cost Inflation related variation bonds. At financial close, committed variation bonds have monoline commitment on the same terms as CCI variation bonds. Thus in summary there are variation bonds of £135 million and
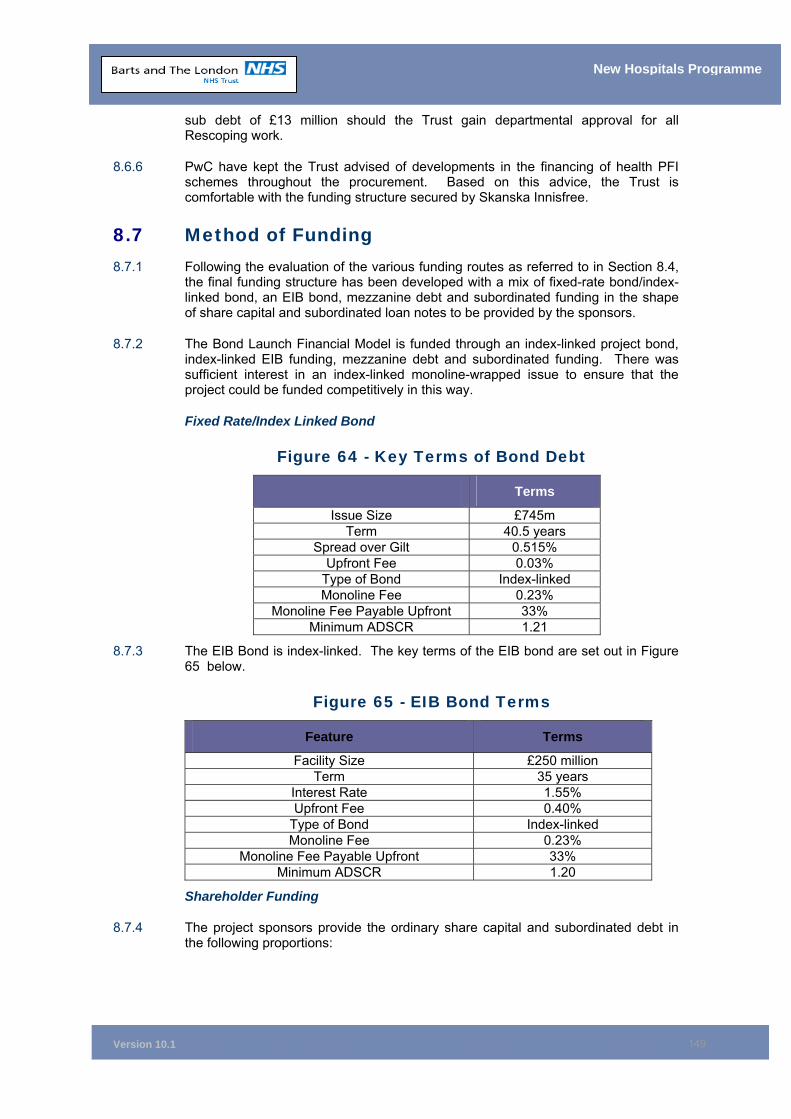
Version 10.1
149
New Hospitals Programme
sub debt of £13 million should the Trust gain departmental approval for all Rescoping work.
8.6.6 PwC have kept the Trust advised of developments in the financing of health PFI schemes throughout the procurement. Based on this advice, the Trust is comfortable with the funding structure secured by Skanska Innisfree.
8.7 Method of Funding 8.7.1 Following the evaluation of the various funding routes as referred to in Section 8.4,
the final funding structure has been developed with a mix of fixed-rate bond/index-linked bond, an EIB bond, mezzanine debt and subordinated funding in the shape of share capital and subordinated loan notes to be provided by the sponsors.
8.7.2 The Bond Launch Financial Model is funded through an index-linked project bond, index-linked EIB funding, mezzanine debt and subordinated funding. There was sufficient interest in an index-linked monoline-wrapped issue to ensure that the project could be funded competitively in this way.
Fixed Rate/Index Linked Bond
Figure 64 - Key Terms of Bond Debt
Terms
Issue Size £745m Term 40.5 years
Spread over Gilt 0.515% Upfront Fee 0.03%
Type of Bond Index-linked Monoline Fee 0.23%
Monoline Fee Payable Upfront 33% Minimum ADSCR 1.21
8.7.3 The EIB Bond is index-linked. The key terms of the EIB bond are set out in Figure 65 below.
Figure 65 - EIB Bond Terms
Feature Terms
Facility Size £250 million Term 35 years
Interest Rate 1.55% Upfront Fee 0.40%
Type of Bond Index-linked Monoline Fee 0.23%
Monoline Fee Payable Upfront 33% Minimum ADSCR 1.20
Shareholder Funding
8.7.4 The project sponsors provide the ordinary share capital and subordinated debt in the following proportions:
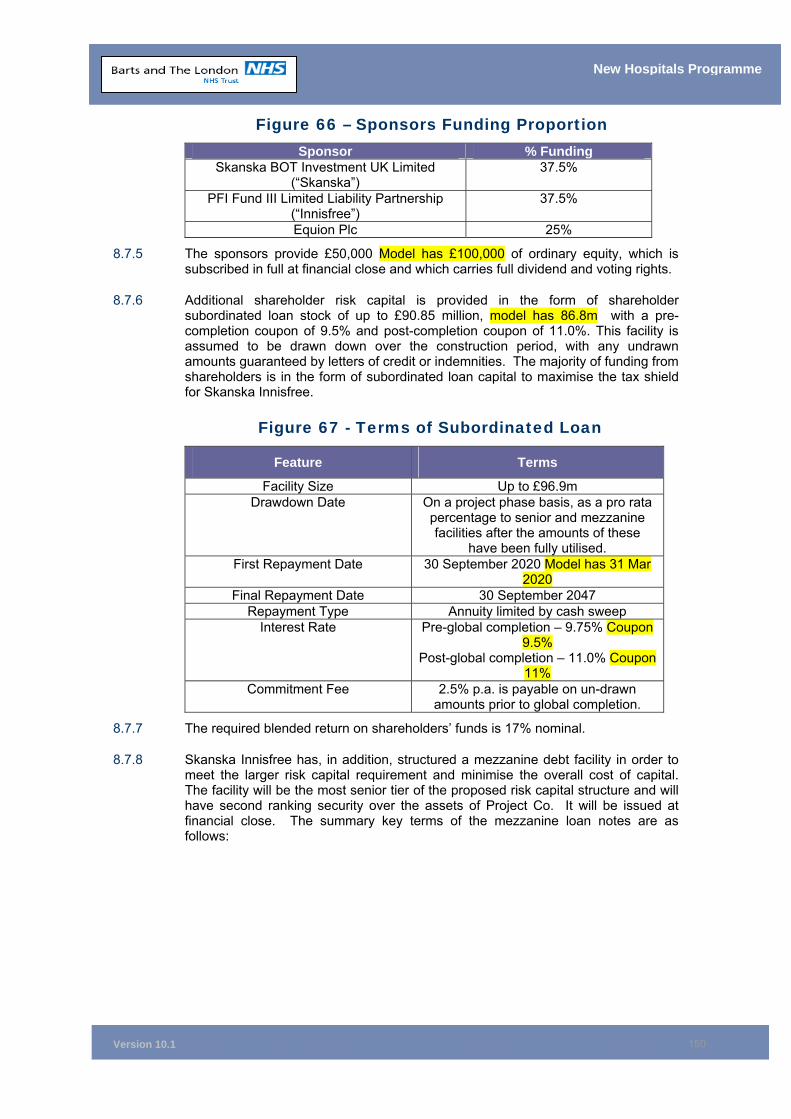
Version 10.1
150
New Hospitals Programme
Figure 66 – Sponsors Funding Proportion Sponsor % Funding
Skanska BOT Investment UK Limited (“Skanska”)
37.5%
PFI Fund III Limited Liability Partnership (“Innisfree”)
37.5%
Equion Plc 25%
8.7.5 The sponsors provide £50,000 Model has £100,000 of ordinary equity, which is subscribed in full at financial close and which carries full dividend and voting rights.
8.7.6 Additional shareholder risk capital is provided in the form of shareholder subordinated loan stock of up to £90.85 million, model has 86.8m with a pre-completion coupon of 9.5% and post-completion coupon of 11.0%. This facility is assumed to be drawn down over the construction period, with any undrawn amounts guaranteed by letters of credit or indemnities. The majority of funding from shareholders is in the form of subordinated loan capital to maximise the tax shield for Skanska Innisfree.
Figure 67 - Terms of Subordinated Loan
Feature Terms
Facility Size Up to £96.9m Drawdown Date On a project phase basis, as a pro rata
percentage to senior and mezzanine facilities after the amounts of these
have been fully utilised. First Repayment Date 30 September 2020 Model has 31 Mar
2020 Final Repayment Date 30 September 2047
Repayment Type Annuity limited by cash sweep Interest Rate Pre-global completion – 9.75% Coupon
9.5% Post-global completion – 11.0% Coupon
11% Commitment Fee 2.5% p.a. is payable on un-drawn
amounts prior to global completion.
8.7.7 The required blended return on shareholders’ funds is 17% nominal.
8.7.8 Skanska Innisfree has, in addition, structured a mezzanine debt facility in order to meet the larger risk capital requirement and minimise the overall cost of capital. The facility will be the most senior tier of the proposed risk capital structure and will have second ranking security over the assets of Project Co. It will be issued at financial close. The summary key terms of the mezzanine loan notes are as follows:
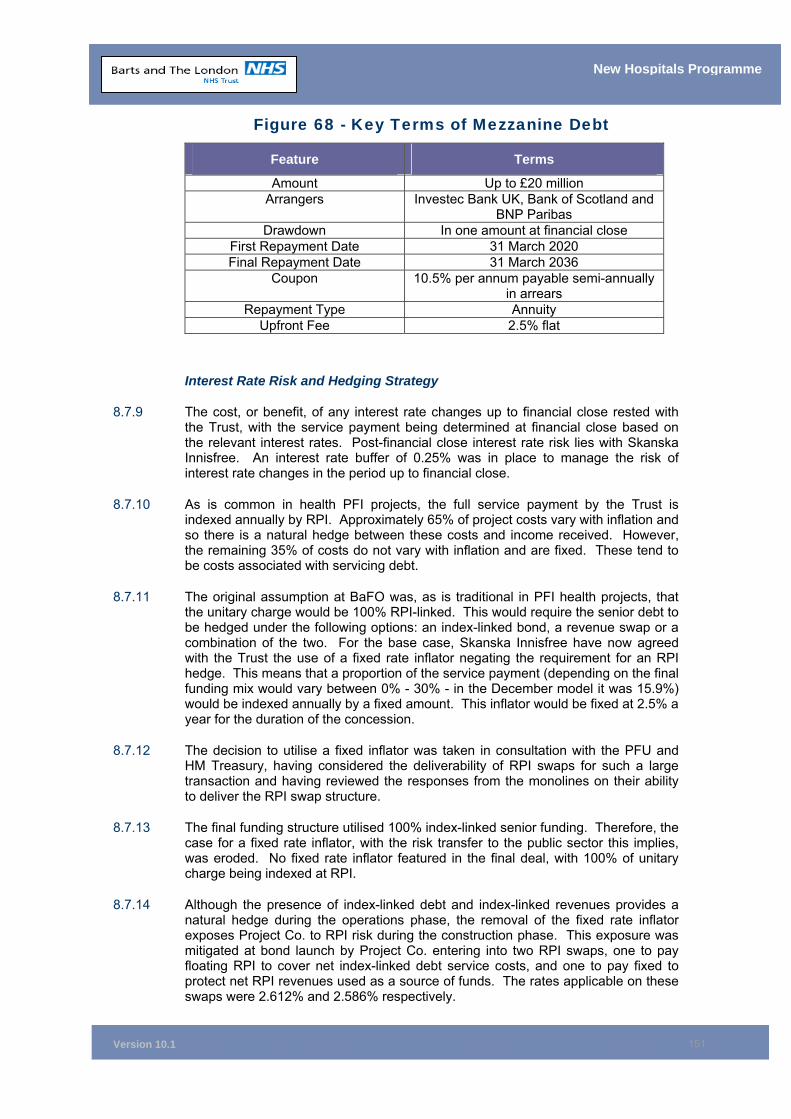
Version 10.1
151
New Hospitals Programme
Figure 68 - Key Terms of Mezzanine Debt
Feature Terms
Amount Up to £20 million Arrangers Investec Bank UK, Bank of Scotland and
BNP Paribas Drawdown In one amount at financial close
First Repayment Date 31 March 2020 Final Repayment Date 31 March 2036
Coupon 10.5% per annum payable semi-annually in arrears
Repayment Type Annuity Upfront Fee 2.5% flat
Interest Rate Risk and Hedging Strategy
8.7.9 The cost, or benefit, of any interest rate changes up to financial close rested with the Trust, with the service payment being determined at financial close based on the relevant interest rates. Post-financial close interest rate risk lies with Skanska Innisfree. An interest rate buffer of 0.25% was in place to manage the risk of interest rate changes in the period up to financial close.
8.7.10 As is common in health PFI projects, the full service payment by the Trust is indexed annually by RPI. Approximately 65% of project costs vary with inflation and so there is a natural hedge between these costs and income received. However, the remaining 35% of costs do not vary with inflation and are fixed. These tend to be costs associated with servicing debt.
8.7.11 The original assumption at BaFO was, as is traditional in PFI health projects, that the unitary charge would be 100% RPI-linked. This would require the senior debt to be hedged under the following options: an index-linked bond, a revenue swap or a combination of the two. For the base case, Skanska Innisfree have now agreed with the Trust the use of a fixed rate inflator negating the requirement for an RPI hedge. This means that a proportion of the service payment (depending on the final funding mix would vary between 0% - 30% - in the December model it was 15.9%) would be indexed annually by a fixed amount. This inflator would be fixed at 2.5% a year for the duration of the concession.
8.7.12 The decision to utilise a fixed inflator was taken in consultation with the PFU and HM Treasury, having considered the deliverability of RPI swaps for such a large transaction and having reviewed the responses from the monolines on their ability to deliver the RPI swap structure.
8.7.13 The final funding structure utilised 100% index-linked senior funding. Therefore, the case for a fixed rate inflator, with the risk transfer to the public sector this implies, was eroded. No fixed rate inflator featured in the final deal, with 100% of unitary charge being indexed at RPI.
8.7.14 Although the presence of index-linked debt and index-linked revenues provides a natural hedge during the operations phase, the removal of the fixed rate inflator exposes Project Co. to RPI risk during the construction phase. This exposure was mitigated at bond launch by Project Co. entering into two RPI swaps, one to pay floating RPI to cover net index-linked debt service costs, and one to pay fixed to protect net RPI revenues used as a source of funds. The rates applicable on these swaps were 2.612% and 2.586% respectively.
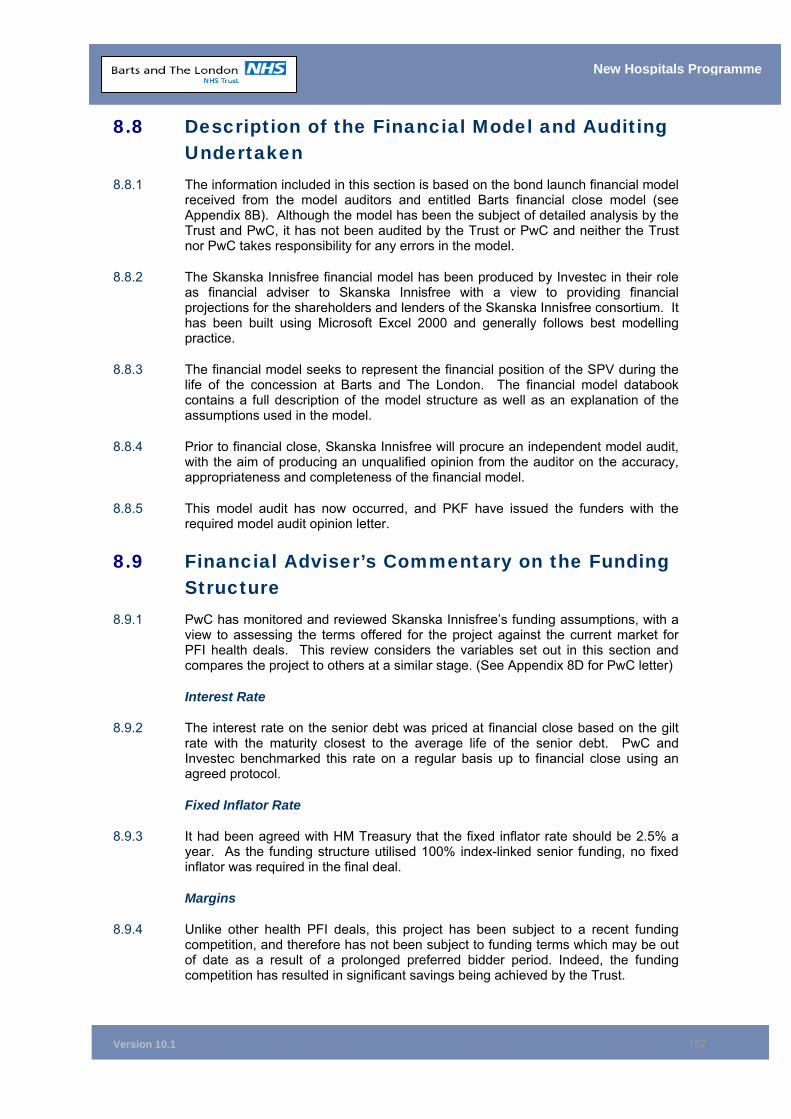
Version 10.1
152
New Hospitals Programme
8.8 Description of the Financial Model and Auditing Undertaken
8.8.1 The information included in this section is based on the bond launch financial model received from the model auditors and entitled Barts financial close model (see Appendix 8B). Although the model has been the subject of detailed analysis by the Trust and PwC, it has not been audited by the Trust or PwC and neither the Trust nor PwC takes responsibility for any errors in the model.
8.8.2 The Skanska Innisfree financial model has been produced by Investec in their role as financial adviser to Skanska Innisfree with a view to providing financial projections for the shareholders and lenders of the Skanska Innisfree consortium. It has been built using Microsoft Excel 2000 and generally follows best modelling practice.
8.8.3 The financial model seeks to represent the financial position of the SPV during the life of the concession at Barts and The London. The financial model databook contains a full description of the model structure as well as an explanation of the assumptions used in the model.
8.8.4 Prior to financial close, Skanska Innisfree will procure an independent model audit, with the aim of producing an unqualified opinion from the auditor on the accuracy, appropriateness and completeness of the financial model.
8.8.5 This model audit has now occurred, and PKF have issued the funders with the required model audit opinion letter.
8.9 Financial Adviser’s Commentary on the Funding Structure
8.9.1 PwC has monitored and reviewed Skanska Innisfree’s funding assumptions, with a view to assessing the terms offered for the project against the current market for PFI health deals. This review considers the variables set out in this section and compares the project to others at a similar stage. (See Appendix 8D for PwC letter)
Interest Rate
8.9.2 The interest rate on the senior debt was priced at financial close based on the gilt rate with the maturity closest to the average life of the senior debt. PwC and Investec benchmarked this rate on a regular basis up to financial close using an agreed protocol.
Fixed Inflator Rate
8.9.3 It had been agreed with HM Treasury that the fixed inflator rate should be 2.5% a year. As the funding structure utilised 100% index-linked senior funding, no fixed inflator was required in the final deal.
Margins
8.9.4 Unlike other health PFI deals, this project has been subject to a recent funding competition, and therefore has not been subject to funding terms which may be out of date as a result of a prolonged preferred bidder period. Indeed, the funding competition has resulted in significant savings being achieved by the Trust.
Version 10.1
153
New Hospitals Programme
Upfront and Commitment Fees
8.9.5 The bond has upfront fees of 3bps and credit enhancement premium of 23bps, with a third paid up front on a discounted basis, and the remainder paid over the life of the bond. Due to the recent funding competition, it can be assured that this reflects the current market.
Debt Service Reserve Account
8.9.6 Consistent with most PFI projects and the current market, the senior debt providers require a debt service reserve account covering the following six months’ principal and interest.
Cover Ratios
8.9.7 The bond term sheet requires that the base case project cash flows meet certain cover ratios. The cover ratios required for this project are a minimum ADSCR of 1.20 and a minimum Bond Life Cover Ratio (BLCR) of 1.24. These requirements are partially complied with in the financial model and reflect the current market due to the recent funding competition.
Gearing
8.9.8 The project is highly geared at 90.3% debt to 9.7% equity. This is considered to be consistent with projects in the PFI market.
Equity Return
8.9.9 The equity internal rate of return (IRR) in the current model is 14.0% real post-tax. This level of return is slightly higher than might be seen on other recent health transactions, but given the risk profile of this project with a nine year construction period we believe this to be reasonable.
Project Internal Rate of Return (IRR)
8.9.10 The project IRR is a measure of the overall cost of external capital to the project. The current model shows a project IRR of 4.1% (real post-tax). This is reflective of the overall cost of capital to projects in the PFI market.
8.10 Conclusion 8.10.1 The funding structure is robust and the funding competition has secured significant
savings to the Trust. The Trust’s advisers (PwC) have reviewed the funding solution and have confirmed that it is acceptable and in line with market norms.
8.11 Chapter Appendices
8A Code of Practise 10 Clearance 8B Skanska Innisfree’s Financial Model 8C Quarterly in Advance Letter 8D PwC Commentary on Funding Structure 8E Glossary of Finance Terms
Version 10.1
154
New Hospitals Programme
9 ECONOMIC APPRAISAL
Synopsis – Economic Appraisal
This Chapter demonstrates that:
• A discounted cash flow analysis, employing the Generic Economic Model (GEM), was used in order to test the Public Sector Comparator (PSC) and Private Finance Initiative (PFI) options for value for money (VfM)
• The analysis was conducted in accordance with the relevant edition of the Green Book – Appraisal and Evaluation in Central Government
• The results of the financial analysis concluded that the PFI option has a marginally lower net present cost (NPC) over both the 43 and 69 year appraisal periods (PFI - £7.802 billion and £8.349 billion; PSC - £8.111 billion and £8.670 billion respectively)
• In conclusion, the PFI solution offers better Value for Money then the PSC.
9.1 Introduction 9.1.1 An economic appraisal was carried out to compare value for money for the PFI
option with the PSC. The economic analysis has been based on the guidance issued by the Department of Health entitled Principles of Generic Economic Model for Full Business Case Option Appraisal (Department of Health, September 2002).
9.1.2 Discounted cash flow analysis using the Net Present Cost (NPC) method was used to compare the options. Cash flows exclude capital charges and VAT.
9.1.3 As the Invitation to Negotiate (ITN) for this project was issued prior to April 2003, it would be expected that the 1997 version of the Green Book would be used. The use of the 1997 Green Book methodology has been confirmed by the Trust with the Capital Investment Unit (CIU).
9.1.4 The start point for the economic appraisal is assumed to be 1 April 2006, as financial close occurred in 2006/07.
9.2 Green Book Methodology 9.2.1 A discount factor of 6% has been applied to cash flows for each option in line with
the 1997 Treasury Green Book103.
9.2.2 Cash flows have been discounted over two periods, the period from financial close until the end of the concession (the concession is for 42 years, including the build, but spans 43 financial years) and the period from financial close until the end the expected life of the facilities – 69 years including the build. Non-cashflow aspects of the revenue costs have been excluded, for example capital charges are not a real cash flow and are thus not included in the economic appraisal.
9.2.3 Only costs to the public sector are considered. Thus VAT is excluded as this represents a circular cash flow for the public sector.
9.2.4 A price base of 2005/06 has been used. 103 Green Book: Appraisal and Evaluation in Central Government, HM Treasury
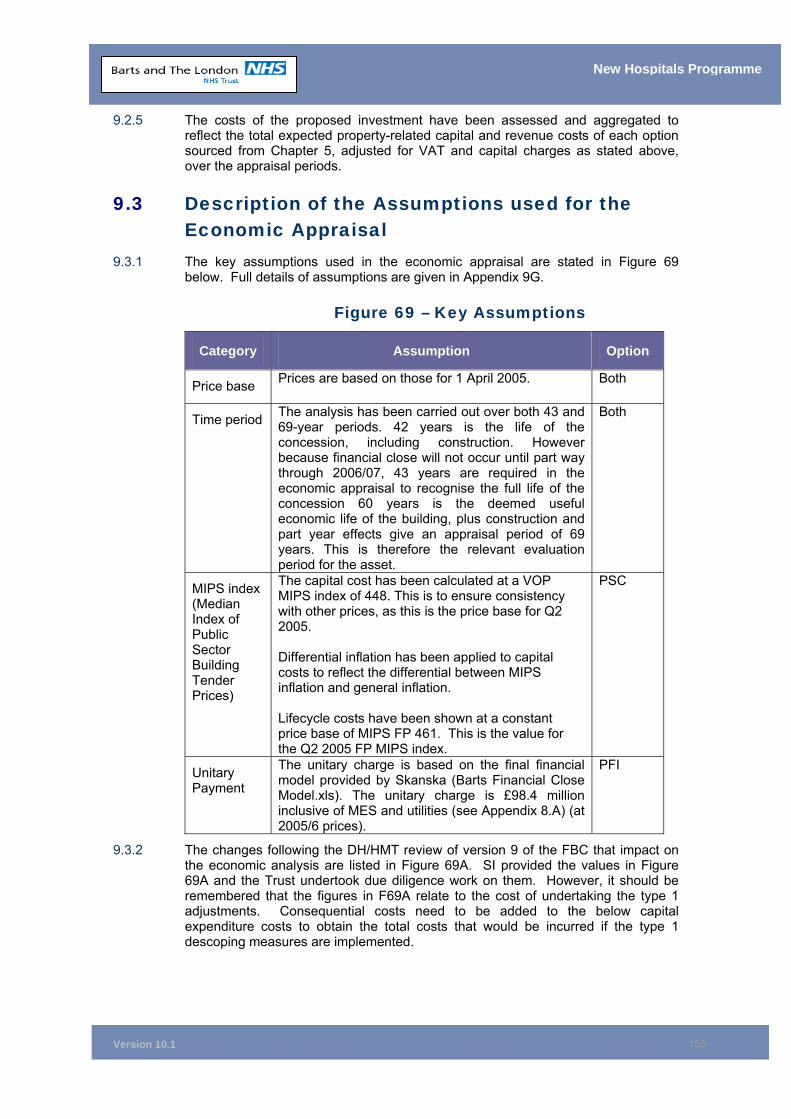
Version 10.1
155
New Hospitals Programme
9.2.5 The costs of the proposed investment have been assessed and aggregated to reflect the total expected property-related capital and revenue costs of each option sourced from Chapter 5, adjusted for VAT and capital charges as stated above, over the appraisal periods.
9.3 Description of the Assumptions used for the Economic Appraisal
9.3.1 The key assumptions used in the economic appraisal are stated in Figure 69 below. Full details of assumptions are given in Appendix 9G.
Figure 69 – Key Assumptions
Category Assumption Option
Price base Prices are based on those for 1 April 2005. Both
Time period The analysis has been carried out over both 43 and 69-year periods. 42 years is the life of the concession, including construction. However because financial close will not occur until part way through 2006/07, 43 years are required in the economic appraisal to recognise the full life of the concession 60 years is the deemed useful economic life of the building, plus construction and part year effects give an appraisal period of 69 years. This is therefore the relevant evaluation period for the asset.
Both
MIPS index (Median Index of Public Sector Building Tender Prices)
The capital cost has been calculated at a VOP MIPS index of 448. This is to ensure consistency with other prices, as this is the price base for Q2 2005. Differential inflation has been applied to capital costs to reflect the differential between MIPS inflation and general inflation. Lifecycle costs have been shown at a constant price base of MIPS FP 461. This is the value for the Q2 2005 FP MIPS index.
PSC
Unitary Payment
The unitary charge is based on the final financial model provided by Skanska (Barts Financial Close Model.xls). The unitary charge is £98.4 million inclusive of MES and utilities (see Appendix 8.A) (at 2005/6 prices).
PFI
9.3.2 The changes following the DH/HMT review of version 9 of the FBC that impact on the economic analysis are listed in Figure 69A. SI provided the values in Figure 69A and the Trust undertook due diligence work on them. However, it should be remembered that the figures in F69A relate to the cost of undertaking the type 1 adjustments. Consequential costs need to be added to the below capital expenditure costs to obtain the total costs that would be incurred if the type 1 descoping measures are implemented.
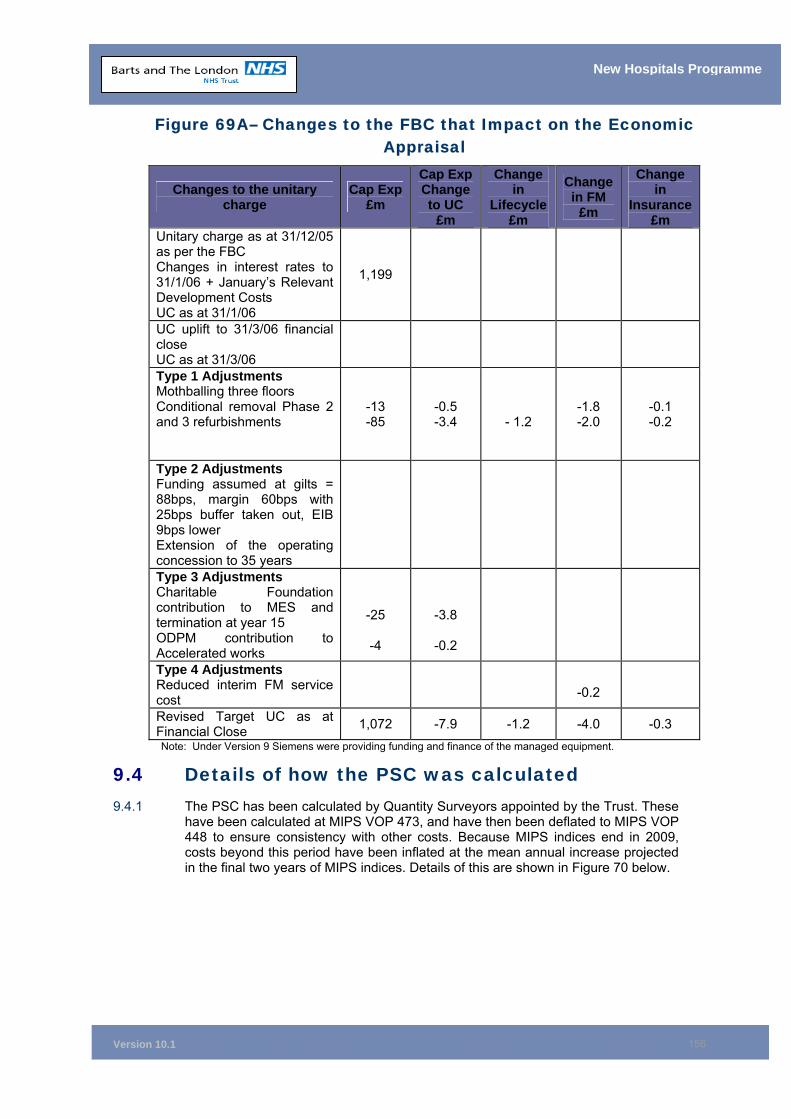
Version 10.1
156
New Hospitals Programme
Figure 69A– Changes to the FBC that Impact on the Economic Appraisal
Changes to the unitary charge
Cap Exp £m
Cap Exp Change to UC
£m
Change in
Lifecycle £m
Change in FM
£m
Change in
Insurance £m
Unitary charge as at 31/12/05 as per the FBC Changes in interest rates to 31/1/06 + January’s Relevant Development Costs UC as at 31/1/06
1,199
UC uplift to 31/3/06 financial close UC as at 31/3/06
Type 1 Adjustments Mothballing three floors Conditional removal Phase 2 and 3 refurbishments
-13 -85
-0.5 -3.4
- 1.2
-1.8 -2.0
-0.1 -0.2
Type 2 Adjustments Funding assumed at gilts = 88bps, margin 60bps with 25bps buffer taken out, EIB 9bps lower Extension of the operating concession to 35 years
Type 3 Adjustments Charitable Foundation contribution to MES and termination at year 15 ODPM contribution to Accelerated works
-25
-4
-3.8
-0.2
Type 4 Adjustments Reduced interim FM service cost
-0.2
Revised Target UC as at Financial Close 1,072 -7.9 -1.2 -4.0 -0.3
Note: Under Version 9 Siemens were providing funding and finance of the managed equipment.
9.4 Details of how the PSC was calculated 9.4.1 The PSC has been calculated by Quantity Surveyors appointed by the Trust. These
have been calculated at MIPS VOP 473, and have then been deflated to MIPS VOP 448 to ensure consistency with other costs. Because MIPS indices end in 2009, costs beyond this period have been inflated at the mean annual increase projected in the final two years of MIPS indices. Details of this are shown in Figure 70 below.
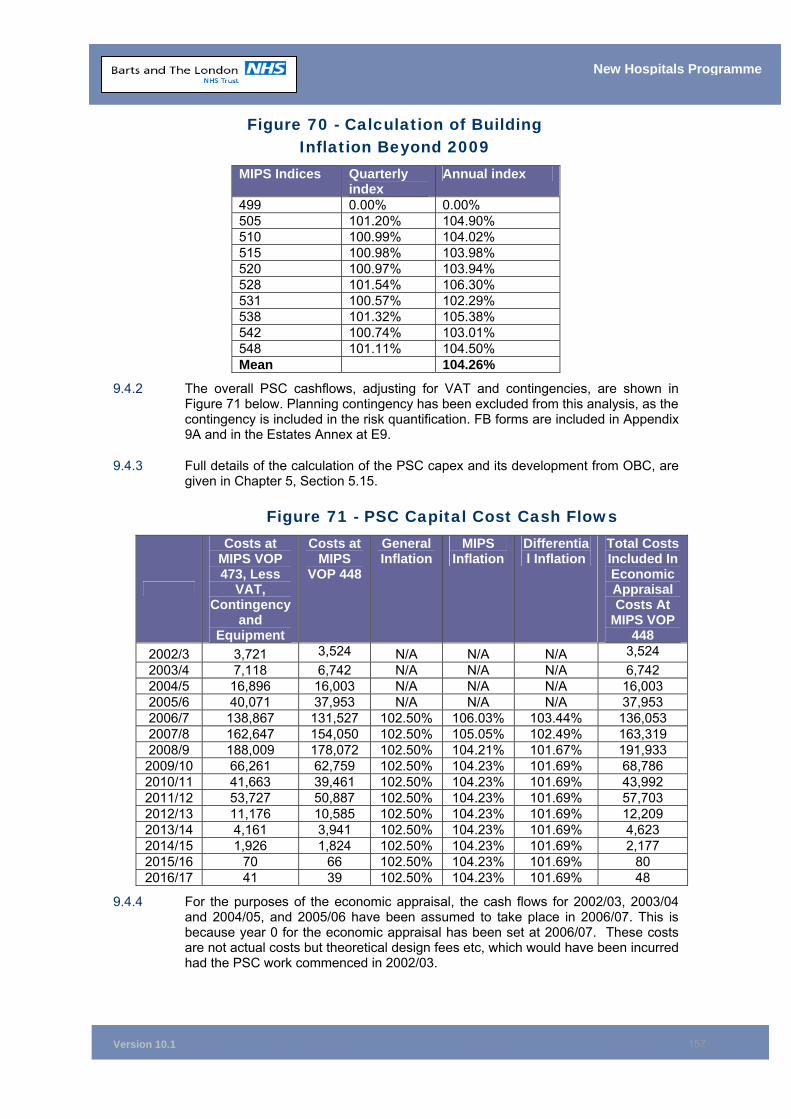
Version 10.1
157
New Hospitals Programme
Figure 70 - Calculation of Building Inflation Beyond 2009
MIPS Indices Quarterly index
Annual index
499 0.00% 0.00% 505 101.20% 104.90% 510 100.99% 104.02% 515 100.98% 103.98% 520 100.97% 103.94% 528 101.54% 106.30% 531 100.57% 102.29% 538 101.32% 105.38% 542 100.74% 103.01% 548 101.11% 104.50% Mean 104.26%
9.4.2 The overall PSC cashflows, adjusting for VAT and contingencies, are shown in Figure 71 below. Planning contingency has been excluded from this analysis, as the contingency is included in the risk quantification. FB forms are included in Appendix 9A and in the Estates Annex at E9.
9.4.3 Full details of the calculation of the PSC capex and its development from OBC, are given in Chapter 5, Section 5.15.
Figure 71 - PSC Capital Cost Cash Flows
Costs at MIPS VOP 473, Less
VAT, Contingency
and Equipment
Costs at MIPS
VOP 448
General Inflation
MIPS Inflation
Differential Inflation
Total Costs Included In Economic Appraisal Costs At
MIPS VOP 448
2002/3 3,721 3,524 N/A N/A N/A 3,524 2003/4 7,118 6,742 N/A N/A N/A 6,742 2004/5 16,896 16,003 N/A N/A N/A 16,003 2005/6 40,071 37,953 N/A N/A N/A 37,953 2006/7 138,867 131,527 102.50% 106.03% 103.44% 136,053 2007/8 162,647 154,050 102.50% 105.05% 102.49% 163,319 2008/9 188,009 178,072 102.50% 104.21% 101.67% 191,933 2009/10 66,261 62,759 102.50% 104.23% 101.69% 68,786 2010/11 41,663 39,461 102.50% 104.23% 101.69% 43,992 2011/12 53,727 50,887 102.50% 104.23% 101.69% 57,703 2012/13 11,176 10,585 102.50% 104.23% 101.69% 12,209 2013/14 4,161 3,941 102.50% 104.23% 101.69% 4,623 2014/15 1,926 1,824 102.50% 104.23% 101.69% 2,177 2015/16 70 66 102.50% 104.23% 101.69% 80 2016/17 41 39 102.50% 104.23% 101.69% 48
9.4.4 For the purposes of the economic appraisal, the cash flows for 2002/03, 2003/04 and 2004/05, and 2005/06 have been assumed to take place in 2006/07. This is because year 0 for the economic appraisal has been set at 2006/07. These costs are not actual costs but theoretical design fees etc, which would have been incurred had the PSC work commenced in 2002/03.
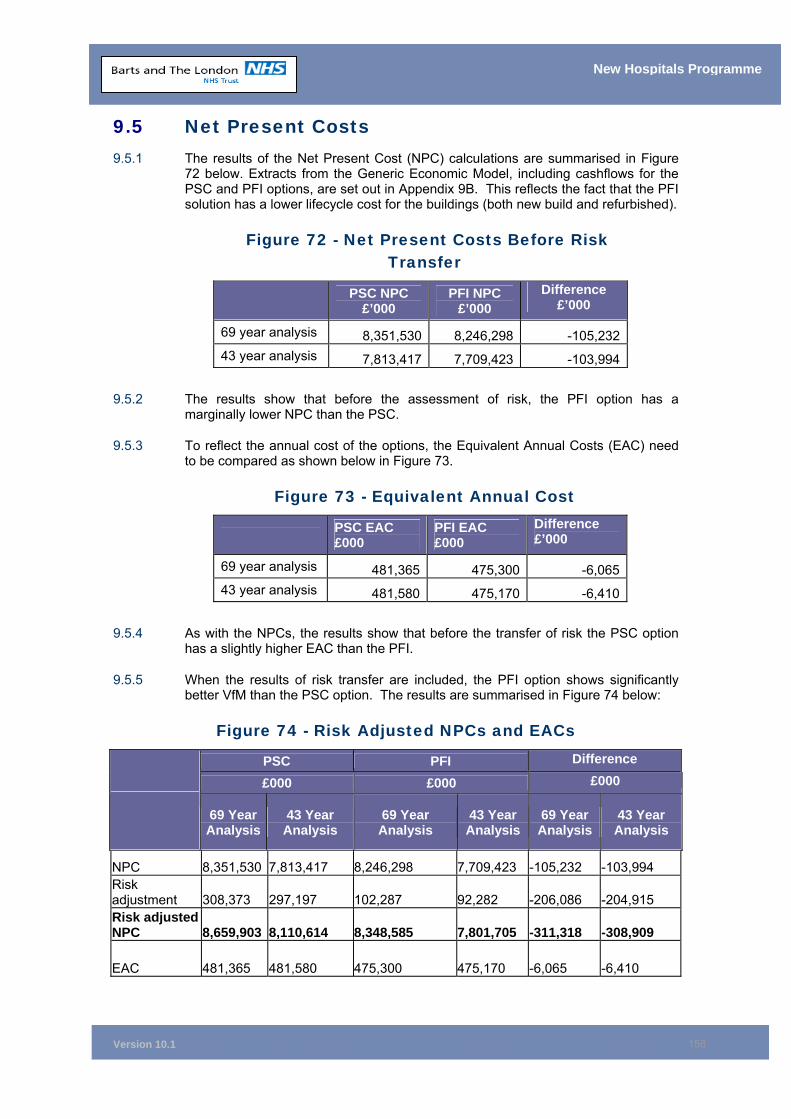
Version 10.1
158
New Hospitals Programme
9.5 Net Present Costs 9.5.1 The results of the Net Present Cost (NPC) calculations are summarised in Figure
72 below. Extracts from the Generic Economic Model, including cashflows for the PSC and PFI options, are set out in Appendix 9B. This reflects the fact that the PFI solution has a lower lifecycle cost for the buildings (both new build and refurbished).
Figure 72 - Net Present Costs Before Risk Transfer
PSC NPC £’000
PFI NPC £’000
Difference £’000
69 year analysis 8,351,530 8,246,298 -105,232 43 year analysis 7,813,417 7,709,423 -103,994
9.5.2 The results show that before the assessment of risk, the PFI option has a marginally lower NPC than the PSC.
9.5.3 To reflect the annual cost of the options, the Equivalent Annual Costs (EAC) need to be compared as shown below in Figure 73.
Figure 73 - Equivalent Annual Cost
PSC EAC £000
PFI EAC £000
Difference £’000
69 year analysis 481,365 475,300 -6,065 43 year analysis 481,580 475,170 -6,410
9.5.4 As with the NPCs, the results show that before the transfer of risk the PSC option has a slightly higher EAC than the PFI.
9.5.5 When the results of risk transfer are included, the PFI option shows significantly better VfM than the PSC option. The results are summarised in Figure 74 below:
Figure 74 - Risk Adjusted NPCs and EACs
PSC PFI Difference
£000 £000 £000
69 Year Analysis
43 Year Analysis
69 Year Analysis
43 Year Analysis
69 Year Analysis
43 Year Analysis
NPC 8,351,530 7,813,417 8,246,298 7,709,423 -105,232 -103,994 Risk adjustment 308,373 297,197 102,287 92,282 -206,086 -204,915 Risk adjusted NPC 8,659,903 8,110,614 8,348,585 7,801,705 -311,318 -308,909
EAC 481,365 481,580 475,300 475,170 -6,065 -6,410
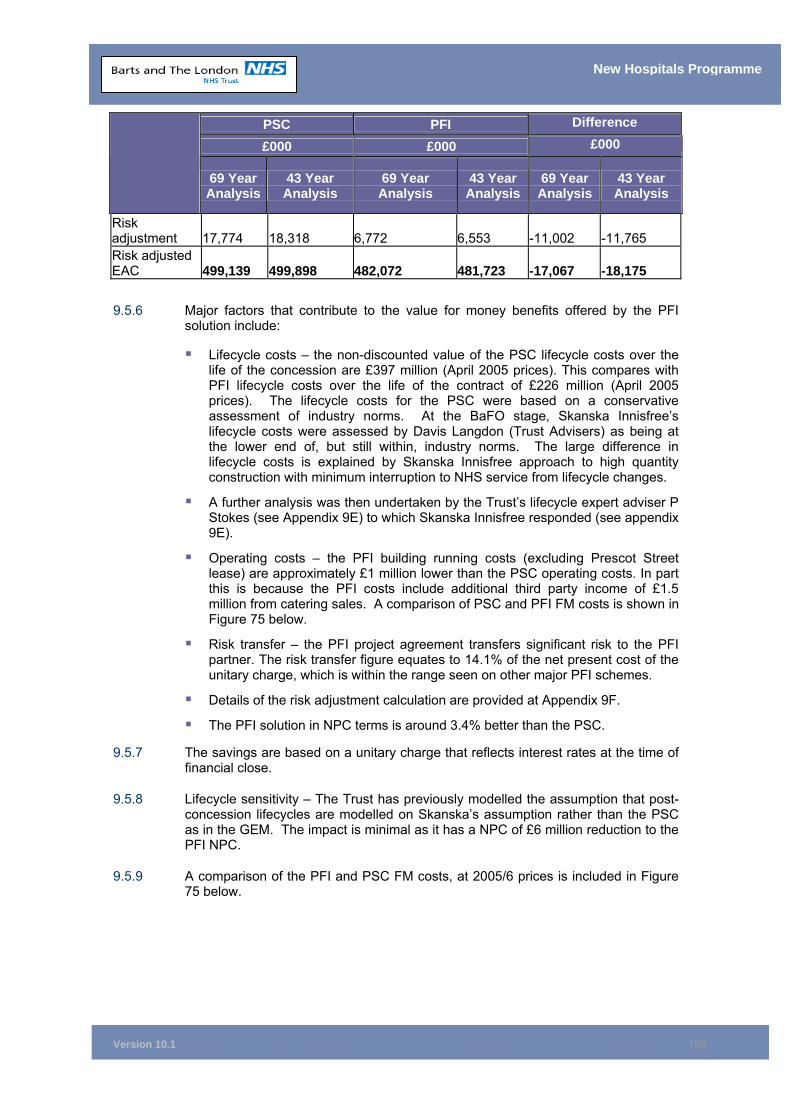
Version 10.1
159
New Hospitals Programme
PSC PFI Difference
£000 £000 £000
69 Year Analysis
43 Year Analysis
69 Year Analysis
43 Year Analysis
69 Year Analysis
43 Year Analysis
Risk adjustment 17,774 18,318 6,772 6,553 -11,002 -11,765 Risk adjusted EAC 499,139 499,898 482,072 481,723 -17,067 -18,175
9.5.6 Major factors that contribute to the value for money benefits offered by the PFI solution include:
Lifecycle costs – the non-discounted value of the PSC lifecycle costs over the life of the concession are £397 million (April 2005 prices). This compares with PFI lifecycle costs over the life of the contract of £226 million (April 2005 prices). The lifecycle costs for the PSC were based on a conservative assessment of industry norms. At the BaFO stage, Skanska Innisfree’s lifecycle costs were assessed by Davis Langdon (Trust Advisers) as being at the lower end of, but still within, industry norms. The large difference in lifecycle costs is explained by Skanska Innisfree approach to high quantity construction with minimum interruption to NHS service from lifecycle changes.
A further analysis was then undertaken by the Trust’s lifecycle expert adviser P Stokes (see Appendix 9E) to which Skanska Innisfree responded (see appendix 9E).
Operating costs – the PFI building running costs (excluding Prescot Street lease) are approximately £1 million lower than the PSC operating costs. In part this is because the PFI costs include additional third party income of £1.5 million from catering sales. A comparison of PSC and PFI FM costs is shown in Figure 75 below.
Risk transfer – the PFI project agreement transfers significant risk to the PFI partner. The risk transfer figure equates to 14.1% of the net present cost of the unitary charge, which is within the range seen on other major PFI schemes.
Details of the risk adjustment calculation are provided at Appendix 9F.
The PFI solution in NPC terms is around 3.4% better than the PSC.
9.5.7 The savings are based on a unitary charge that reflects interest rates at the time of financial close.
9.5.8 Lifecycle sensitivity – The Trust has previously modelled the assumption that post-concession lifecycles are modelled on Skanska’s assumption rather than the PSC as in the GEM. The impact is minimal as it has a NPC of £6 million reduction to the PFI NPC.
9.5.9 A comparison of the PFI and PSC FM costs, at 2005/6 prices is included in Figure 75 below.
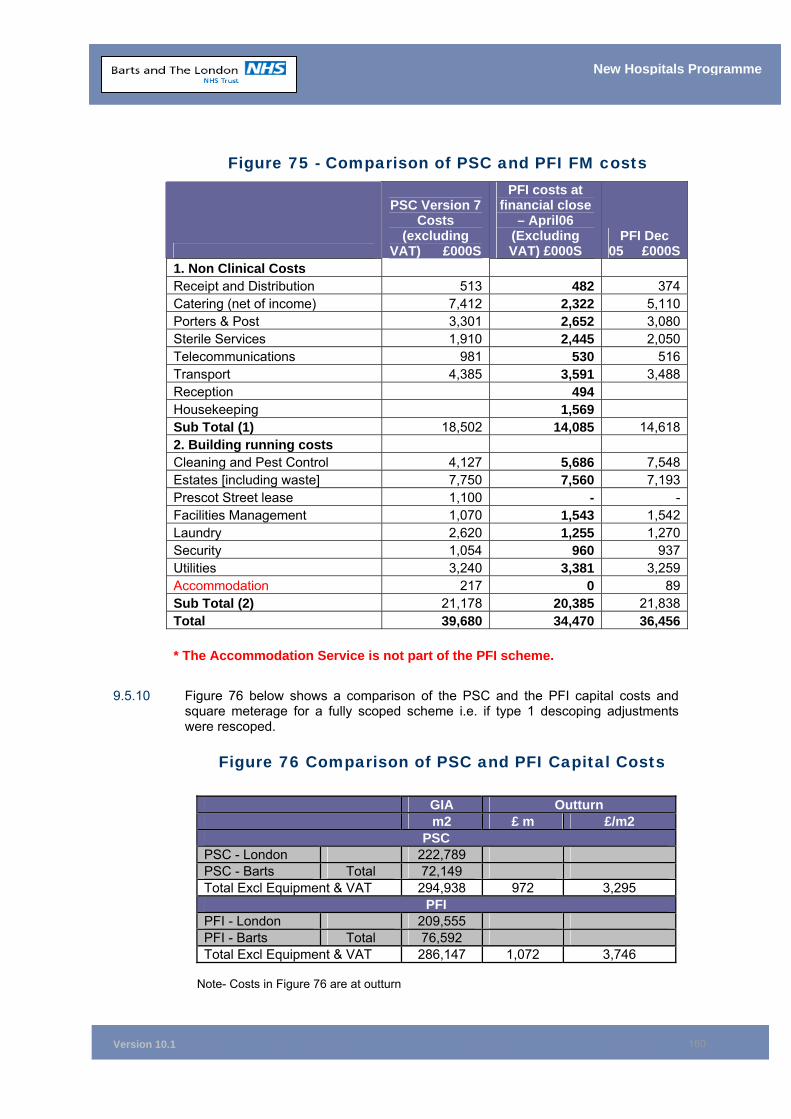
Version 10.1
160
New Hospitals Programme
Figure 75 - Comparison of PSC and PFI FM costs
PSC Version 7 Costs
(excluding VAT) £000S
PFI costs at financial close
– April06 (Excluding VAT) £000S
PFI Dec 05 £000S
1. Non Clinical Costs Receipt and Distribution 513 482 374Catering (net of income) 7,412 2,322 5,110Porters & Post 3,301 2,652 3,080Sterile Services 1,910 2,445 2,050Telecommunications 981 530 516Transport 4,385 3,591 3,488Reception 494 Housekeeping 1,569 Sub Total (1) 18,502 14,085 14,6182. Building running costs Cleaning and Pest Control 4,127 5,686 7,548Estates [including waste] 7,750 7,560 7,193Prescot Street lease 1,100 - -Facilities Management 1,070 1,543 1,542Laundry 2,620 1,255 1,270Security 1,054 960 937Utilities 3,240 3,381 3,259Accommodation 217 0 89Sub Total (2) 21,178 20,385 21,838Total 39,680 34,470 36,456 * The Accommodation Service is not part of the PFI scheme.
9.5.10 Figure 76 below shows a comparison of the PSC and the PFI capital costs and square meterage for a fully scoped scheme i.e. if type 1 descoping adjustments were rescoped.
Figure 76 Comparison of PSC and PFI Capital Costs
GIA Outturn m2 £ m £/m2
PSC PSC - London 222,789 PSC - Barts Total 72,149 Total Excl Equipment & VAT 294,938 972 3,295
PFI PFI - London 209,555 PFI - Barts Total 76,592 Total Excl Equipment & VAT 286,147 1,072 3,746
Note- Costs in Figure 76 are at outturn
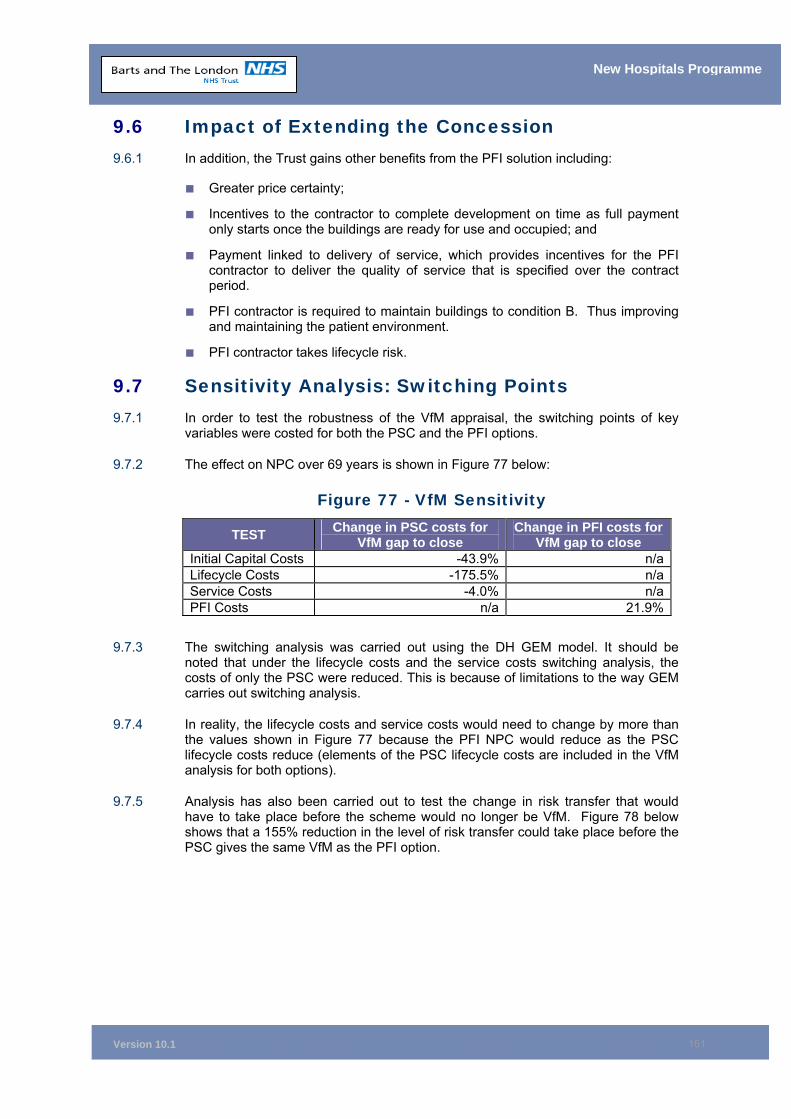
Version 10.1
161
New Hospitals Programme
9.6 Impact of Extending the Concession 9.6.1 In addition, the Trust gains other benefits from the PFI solution including:
■ Greater price certainty;
■ Incentives to the contractor to complete development on time as full payment only starts once the buildings are ready for use and occupied; and
■ Payment linked to delivery of service, which provides incentives for the PFI contractor to deliver the quality of service that is specified over the contract period.
■ PFI contractor is required to maintain buildings to condition B. Thus improving and maintaining the patient environment.
■ PFI contractor takes lifecycle risk.
9.7 Sensitivity Analysis: Switching Points 9.7.1 In order to test the robustness of the VfM appraisal, the switching points of key
variables were costed for both the PSC and the PFI options.
9.7.2 The effect on NPC over 69 years is shown in Figure 77 below:
Figure 77 - VfM Sensitivity
TEST Change in PSC costs for VfM gap to close
Change in PFI costs for VfM gap to close
Initial Capital Costs -43.9% n/aLifecycle Costs -175.5% n/aService Costs -4.0% n/aPFI Costs n/a 21.9%
9.7.3 The switching analysis was carried out using the DH GEM model. It should be noted that under the lifecycle costs and the service costs switching analysis, the costs of only the PSC were reduced. This is because of limitations to the way GEM carries out switching analysis.
9.7.4 In reality, the lifecycle costs and service costs would need to change by more than the values shown in Figure 77 because the PFI NPC would reduce as the PSC lifecycle costs reduce (elements of the PSC lifecycle costs are included in the VfM analysis for both options).
9.7.5 Analysis has also been carried out to test the change in risk transfer that would have to take place before the scheme would no longer be VfM. Figure 78 below shows that a 155% reduction in the level of risk transfer could take place before the PSC gives the same VfM as the PFI option.
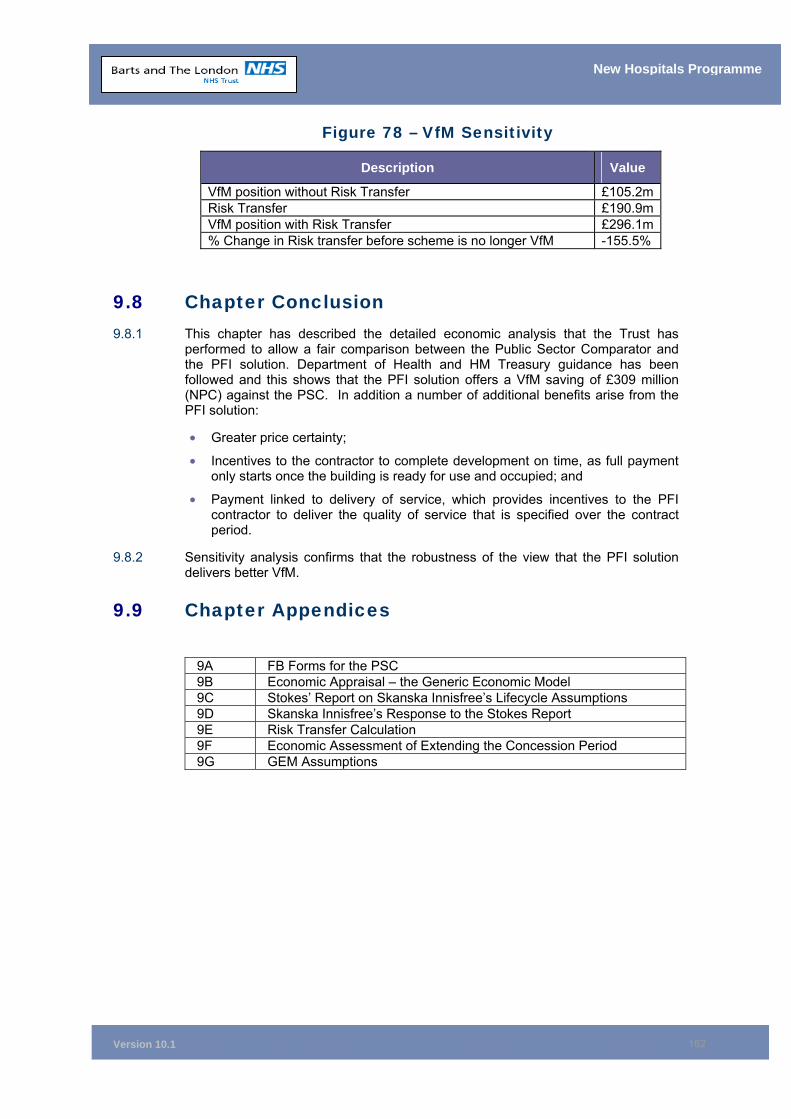
Version 10.1
162
New Hospitals Programme
Figure 78 – VfM Sensitivity
Description Value
VfM position without Risk Transfer £105.2m Risk Transfer £190.9m VfM position with Risk Transfer £296.1m % Change in Risk transfer before scheme is no longer VfM -155.5%
9.8 Chapter Conclusion 9.8.1 This chapter has described the detailed economic analysis that the Trust has
performed to allow a fair comparison between the Public Sector Comparator and the PFI solution. Department of Health and HM Treasury guidance has been followed and this shows that the PFI solution offers a VfM saving of £309 million (NPC) against the PSC. In addition a number of additional benefits arise from the PFI solution:
• Greater price certainty;
• Incentives to the contractor to complete development on time, as full payment only starts once the building is ready for use and occupied; and
• Payment linked to delivery of service, which provides incentives to the PFI contractor to deliver the quality of service that is specified over the contract period.
9.8.2 Sensitivity analysis confirms that the robustness of the view that the PFI solution delivers better VfM.
9.9 Chapter Appendices
9A FB Forms for the PSC 9B Economic Appraisal – the Generic Economic Model 9C Stokes’ Report on Skanska Innisfree’s Lifecycle Assumptions 9D Skanska Innisfree’s Response to the Stokes Report 9E Risk Transfer Calculation 9F Economic Assessment of Extending the Concession Period 9G GEM Assumptions
Version 10.1
163
New Hospitals Programme
10 ACCOUNTING TREATMENT Synopsis – Accounting Treatment
This chapter demonstrates that:
• The approach taken to accounting treatment conforms to the latest guidance.
• The freehold ownership of the land at both The Royal London site (RLH) and the Barts sites will remain with the Trust in its entirety.
• Responsibility for identified facilities will be taken by Skanska Innisfree (SI) for the duration of the concession. As they will also bear the risks associated with this property, it will not appear on the Trust’s balance sheet.
• The London Chest Hospital (LCH) is surplus to requirements but does not currently form part of a commercial proposal by Skanska Innisfree.
• Disposals, demolitions and impairments will reduce the value of the Trust’s net assets to £286 million.
• Skanska Innisfree is responsible for the provision of equipment as defined in the Managed Equipment Service. All other equipment will be the property of the Trust.
10.1 Accounting for Land and Buildings 10.1.1 The accounting treatment assumed within the financial and economic analyses for
the Trust’s land and buildings follows the guidance contained in Land and Buildings in PFI Schemes104.
10.1.2 All of the land and buildings affected by the project are in the ownership of the Trust, and the accounting treatment of the respective sites is as follows.
The Royal London and Bart Sites
10.1.3 The freehold and leasehold ownership of the land at the Royal London and Barts remain with the Trust. Full details are in Appendix 10F.
10.1.4 A significant number of building demolitions will take place during the early years of the agreement. During this time, the Trust will follow the current guidance for both impairment and accelerated depreciation of such assets. Buildings which are demolished soon after financial close have been impaired within the 2005/06 annual accounts (see paragraph 10.5). Those demolished later are subject to accelerated depreciation. This treatment has been agreed with the District Valuer and the Trust’s external auditors KPMG. Letters of agreement are in Appendix 10H.
10.1.5 The buildings remaining on the site have been categorised as either Trust, transferred or to be demolished. Details are provided in appendix 10E.
10.1.6 Responsibility for transferred facilities is Skanska Innisfree’s from transfer to the end of the concession and all building and maintenance risks rest with Skanska Innisfree. These will be accounted for as deferred assets.
104 Department of Health, Private Finance Unit guidance letter, 16 January 2003.
Version 10.1
164
New Hospitals Programme
10.1.7 Responsibility for the new buildings is Skanska Innisfree’s until the end of the concession. This will be accounted for as a residual interest building up to the end of the concession when it will appear as a fixed asset in the Trust’s accounts.
10.1.8 The Trust’s financial advisers and auditors have agreed that when the risks and rewards of ownership are assessed in line with FRS5, the correct accounting treatment is that the PFI is off balance sheet. See section 10.4 for the impact of the changes to the accounting treatment following the DN/HMT review of the FBC.
10.1.9 Two buildings have been identified as surplus to requirements, these are:
• the Outpatients Department on the Royal London site (NBV £8 million); and
• the Drill Hall on the Mile End Road (NBV £0.4 million.
10.1.10 These buildings do not currently form part of any commercial proposal with SI. Their usage will be reviewed annually and a final decision made by the Trust Board. This will inform the accounting treatment. The accounting treatment will be determined by the Trust’s use of these buildings in the future and the point at which the Trust declares them surplus to requirements. In practice, whilst the Trust may dispose of the Drill Hall, it is unlikely to dispose of the OPD as it is on the hospital site. There is a possibility, depending on Trust requirements, that the Trust will use the space in the drill hall for storage and convert the existing outpatients building as a type 1 post-financial close adjustment (as per schedule 22, part 7 in the Project Agreement, the Trust is reviewing the financial close, type 1 adjustments as it has the opportunity to agree a revised Descoping list with Capital Hospitals Ltd within 15 months post financial close). Hence, accelerated depreciation has not been assumed. The financial position in the FBC assumes the buildings are declared surplus when the PFI construction is complete and do not therefore incur capital charges. If this were not the case, capital charges of £600,000 per annum would be incurred. Alternatively capital receipts may be realised by sale, but this would not be until 2015/2016.
The London Chest Hospital (LCH) Site
10.1.11 On completion of the construction period, services currently at LCH will transfer to Barts. Therefore, the LCH will become surplus to requirements. No decision has been made as to how the anticipated proceeds from the sale will be utilised by the Trust and this has not been included in the affordability analysis. Where the proceeds exceed the Trust’s delegated limits a business case will be provided regarding utilisation of the proceeds as they would accrue to the Strategic Health Authority. Alternatively if the Foundation Trust regime applies they will accrue to the Trust. The capital charges manual guidance is that where there is uncertainty around timing the Trust may choose to impair the asset when and if it becomes surplus rather than accelerate depreciation. Although the Trust anticipates closing the LCH there is uncertainty around the timing as this is dependent on the PFI build being available to move into. Additional changes in activity levels may mean that the LCH does not close.
10.1.12 Both Project Co. and the Trust can cause delay to the programme that will cause the sale of LCH to be deferred. Equally, other policy initiatives that may arise over the next decade may dictate that LCH is retained either by the Trust or by some other public body (a PCT or even the Borough). All such circumstances could lead to the timing, both of the receipt and the accounting profit (if there is one), being different to what is currently assumed. This is one of the main reasons that the Trust has chosen not to rely on the proceeds.
10.1.13 The NBV of the London Chest Hospital is £14.4 million. The Trust anticipates the OMV would be a similar amount as indicated by Property Advisors. The PDC would
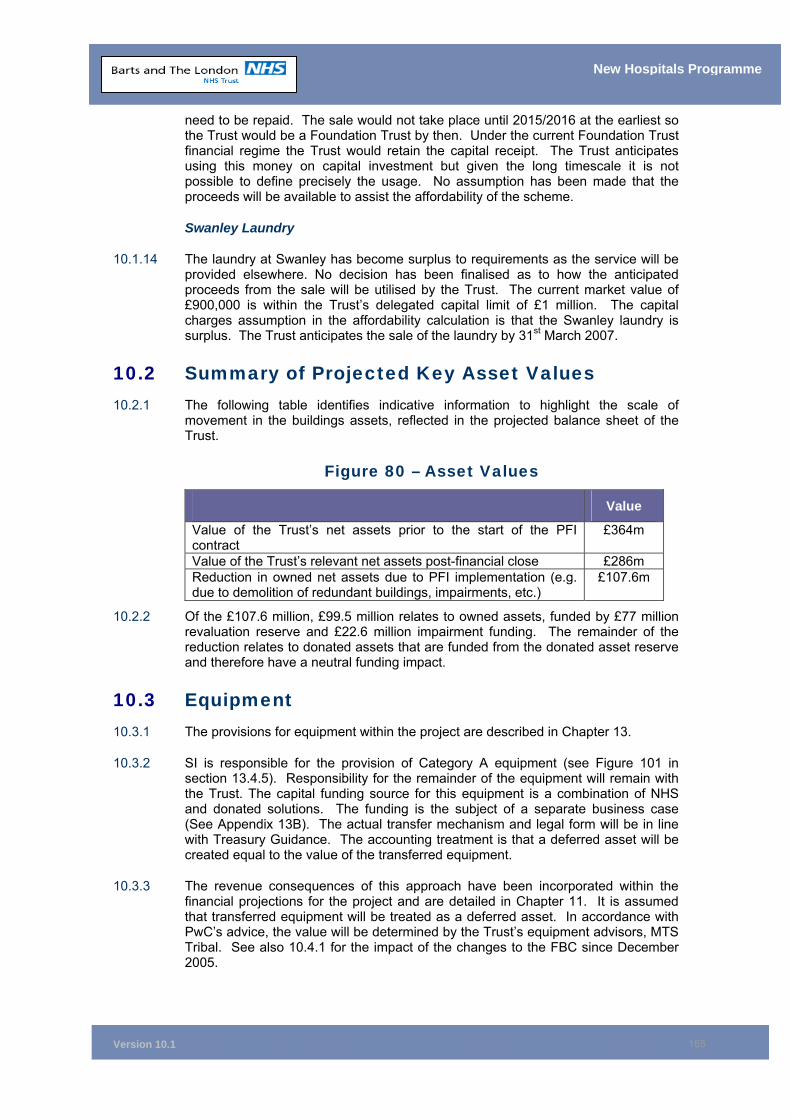
Version 10.1
165
New Hospitals Programme
need to be repaid. The sale would not take place until 2015/2016 at the earliest so the Trust would be a Foundation Trust by then. Under the current Foundation Trust financial regime the Trust would retain the capital receipt. The Trust anticipates using this money on capital investment but given the long timescale it is not possible to define precisely the usage. No assumption has been made that the proceeds will be available to assist the affordability of the scheme.
Swanley Laundry
10.1.14 The laundry at Swanley has become surplus to requirements as the service will be provided elsewhere. No decision has been finalised as to how the anticipated proceeds from the sale will be utilised by the Trust. The current market value of £900,000 is within the Trust’s delegated capital limit of £1 million. The capital charges assumption in the affordability calculation is that the Swanley laundry is surplus. The Trust anticipates the sale of the laundry by 31st March 2007.
10.2 Summary of Projected Key Asset Values 10.2.1 The following table identifies indicative information to highlight the scale of
movement in the buildings assets, reflected in the projected balance sheet of the Trust.
Figure 80 – Asset Values
Value
Value of the Trust’s net assets prior to the start of the PFI contract
£364m
Value of the Trust’s relevant net assets post-financial close £286m Reduction in owned net assets due to PFI implementation (e.g. due to demolition of redundant buildings, impairments, etc.)
£107.6m
10.2.2 Of the £107.6 million, £99.5 million relates to owned assets, funded by £77 million revaluation reserve and £22.6 million impairment funding. The remainder of the reduction relates to donated assets that are funded from the donated asset reserve and therefore have a neutral funding impact.
10.3 Equipment 10.3.1 The provisions for equipment within the project are described in Chapter 13.
10.3.2 SI is responsible for the provision of Category A equipment (see Figure 101 in section 13.4.5). Responsibility for the remainder of the equipment will remain with the Trust. The capital funding source for this equipment is a combination of NHS and donated solutions. The funding is the subject of a separate business case (See Appendix 13B). The actual transfer mechanism and legal form will be in line with Treasury Guidance. The accounting treatment is that a deferred asset will be created equal to the value of the transferred equipment.
10.3.3 The revenue consequences of this approach have been incorporated within the financial projections for the project and are detailed in Chapter 11. It is assumed that transferred equipment will be treated as a deferred asset. In accordance with PwC’s advice, the value will be determined by the Trust’s equipment advisors, MTS Tribal. See also 10.4.1 for the impact of the changes to the FBC since December 2005.
Version 10.1
166
New Hospitals Programme
10.4 Impact on accounting treatment of changes to the FBC from December 2005
10.4.1 The accounting treatment for the PFI remains unchanged from the position detailed in version 9 of the FBC (December 2005) with the exception of the Type 3 adjustment relating to the Managed Equipment Service. The Trust is to receive an initial donation from the St Bartholomew and The Royal London Charitable Foundation of £25m as direct funding towards the procurement of the first tranche of Managed Equipment. Thus the Trust has assumed a requirement to account for this equipment as donated assets.
10.4.2 Appendix 10B2 provides the accounting opinion from our financial advisers, PwC on the changes to the Managed Equipment Service, which has been forwarded to our External Auditors, KPMG. The advice confirms that the funding of the equipment by the Charitable Foundation should lead to them being treated as donated assets within the Trust’s balance sheet.
10.4.3 Appendix 10B3 details PwC’s advice with regard to the impact of type 1 adjustments. This confirms that there should be no change in treatment for the mothballed beds given that SI will be responsible for their lifecycle and maintenance. However, the Trust would be responsible in the steady state for maintaining the refurbished buildings within the type 1 adjustments (i.e. responsible for those buildings that are not refurbished in phases 2 and 3 at both sites) and hence these would be on balance sheet (unless and until being Re-scoped).
10.4.4 Appendix 10C3 provides KPMG’s final accounting opinion taking account of the changes to the FBC since December 2005.
10.5 Accounting Treatment of the Annual Service Charge
10.5.1 The Trust’s financial advisers, PricewaterhouseCoopers (PwC), have continually reviewed the proposed accounting treatment for the scheme. They have undertaken a detailed analysis of the risks retained and transferred105 and concluded that the appropriate treatment for the identified and newly constructed facilities by the Trust is off balance sheet.
10.5.2 This opinion was stated in their letter to the Trust dated January 2003 and has since been re-confirmed in July 2005106 and March 2006 (for adjustments to version 9 of the FBC). The Trust’s Director of Finance has considered the draft opinion and has liaised throughout the scheme’s development with the Trust’s external auditors (KPMG)107.
Residual interest
10.5.3 Under the PFI option, the Trust is required to build up the value of the asset to the estimated net book value (NBV) at the end of the concession. The District Valuer has estimated that the residual NBV at the end of the concessionary period as £452 million. The initial profile of residual interest (item in the Income and Expenditure Account) is shown in Figure 81 below. Thus £8.662 million is the estimated annual
105 See Appendix 10A for PwC’s analysis of risks. 106 See Appendix 10B for PwC’s letter confirming off balance sheet treatment. 107 See Appendix 10C for KPMG’s review of accounting treatment.
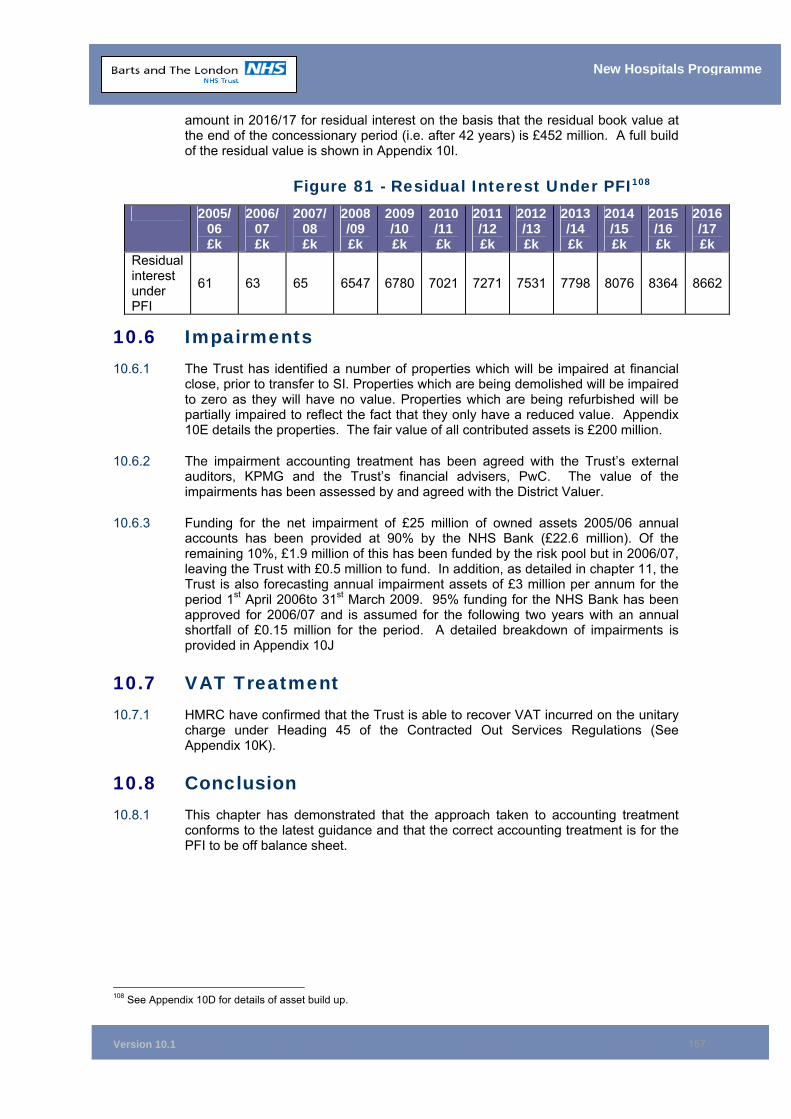
Version 10.1
167
New Hospitals Programme
amount in 2016/17 for residual interest on the basis that the residual book value at the end of the concessionary period (i.e. after 42 years) is £452 million. A full build of the residual value is shown in Appendix 10I.
Figure 81 - Residual Interest Under PFI108 2005/
06 £k
2006/ 07 £k
2007/ 08 £k
2008/09 £k
2009/10 £k
2010/11 £k
2011/12 £k
2012/13 £k
2013 /14 £k
2014 /15 £k
2015/16 £k
2016/17 £k
Residual interest under PFI
61 63 65 6547 6780 7021 7271 7531 7798 8076 8364 8662
10.6 Impairments 10.6.1 The Trust has identified a number of properties which will be impaired at financial
close, prior to transfer to SI. Properties which are being demolished will be impaired to zero as they will have no value. Properties which are being refurbished will be partially impaired to reflect the fact that they only have a reduced value. Appendix 10E details the properties. The fair value of all contributed assets is £200 million.
10.6.2 The impairment accounting treatment has been agreed with the Trust’s external auditors, KPMG and the Trust’s financial advisers, PwC. The value of the impairments has been assessed by and agreed with the District Valuer.
10.6.3 Funding for the net impairment of £25 million of owned assets 2005/06 annual accounts has been provided at 90% by the NHS Bank (£22.6 million). Of the remaining 10%, £1.9 million of this has been funded by the risk pool but in 2006/07, leaving the Trust with £0.5 million to fund. In addition, as detailed in chapter 11, the Trust is also forecasting annual impairment assets of £3 million per annum for the period 1st April 2006to 31st March 2009. 95% funding for the NHS Bank has been approved for 2006/07 and is assumed for the following two years with an annual shortfall of £0.15 million for the period. A detailed breakdown of impairments is provided in Appendix 10J
10.7 VAT Treatment 10.7.1 HMRC have confirmed that the Trust is able to recover VAT incurred on the unitary
charge under Heading 45 of the Contracted Out Services Regulations (See Appendix 10K).
10.8 Conclusion 10.8.1 This chapter has demonstrated that the approach taken to accounting treatment
conforms to the latest guidance and that the correct accounting treatment is for the PFI to be off balance sheet.
108 See Appendix 10D for details of asset build up.
Version 10.1
168
New Hospitals Programme
10.9 Chapter Appendices
10A PwC’s Analysis of Risks 10B PwC’s Letter Confirming Off Balance Sheet 10B2 PwC’s Final Letter on Managed Equipment Accounting Advice 10B3 PwC’s Letter on the Impact of Type 1 Adjustments on their Accounting
Advice 10C1 KPMG’s Review of Accounting Treatment 10C2 Letter from Trust Director of Finance to KPMG 10C3 KPMG’s Final Review of Accounting Treatment 10D Asset Build Up 10E Buildings Affected by the PFI 10F Land and Property 10G District Valuer’s Report 10H KPMG Impairment of Asset 10I Residual Interest Build Up 10J Impairment Figures 10K VAT Letter 10L Asset NBVs 10M District Valuer’s Letter – Valuation of Residual Asset
Version 10.1
169
New Hospitals Programme
11 AFFORDABILITY ANALYSIS Synopsis – Affordability
This chapter demonstrates that:
• Under Patient Choice and Payment by Results (PbR), the Trust will need to ensure its cost base is within predicted PbR funding levels.
• The Trust has worked alongside its main Primary Care Trust (PCT) commissioners in seeking their approval of the activity assumptions which have been used within the business case to generate these funding flows. The affordability modelling takes account of the reduced income as a result of the transfer of activity to primary care.
• The Trust has performed affordability analysis using a PbR methodology and recognises that affordability risks will transfer to the Trust while demand risks rest with the PCTs.
• By the time the new hospitals open fully, PbR will be in operation and the precise disposition of the sources of revenue funding will be determined by the Trust, its PCTs, education, training and research and development (R&D) commissioners, and the effects of Patient Choice.
• The outline business case (OBC) for the New Hospitals Project had a series of activity and efficiency assumptions. This chapter refreshes these assumptions and provides a reconciliation with the OBC position.
• The affordability position excludes transitional relief for the steady state year (2016/17), and is based on the income received for agreed activity in the base model and after Trust savings of around £30 million per annum (which takes into account the Trust being required to make annual cost savings to meet PbR and other pressures). The Trust has a track record on delivering cost reductions and the Trust Board and Strategic Management Group have signed up to achieving the £30 million savings over the next two years from the Best Value Review.
• The income and activity 12 year model provides a prudent base case, as the latest projections for population and housing in North East London indicate that the population growth estimates used in the model for Thames Gateway are likely to be under-estimated. The affordability chapter demonstrates that the Trust has robust handling strategies should the planned level of activity be under or over-stated.
• The Trust will review the FBC as income of the income risks and opportunities crystallise, and given the potential scale of variation, assertions about affordability may be transient.
• With the descoped scheme the same level of activity has to be undertaken but in a more efficient manner/higher bed occupancy so that income remains unchanged. This is reflected in the chapter 4 bed analysis which was updated in version 10 of the FBC for the Descoped scheme. Rescoping the mothballed beds would take place when sufficient activity and income over and above that detailed in chapter 11 warrants a business case to be made to the SHA & DH e.g. for a greater impact from Thames Gateway population increase than the prudent estimate used in chapter 11.
• The Trust has an agreed affordable unitary charge of £98.4 million (in the steady state year at 31/03/06 prices). This compares with the unitary charge stated in the Addendum to the FBC of £96.4 million (steady state year) as at 31 March 2006. Although the spread on the index-linked bonds is 51.5bps which compared with 55bps (assumed in the target UC), the
Version 10.1
170
New Hospitals Programme
bond gilt yield (interest rate) increased from mid-February and added £2.4 million to the final UC. However, the affordability envelope set by DH and HMT on 16 February 2006 has been met given the UC has only moved adversely due to interest rate movements in the two month period to financial close on 27 April 2006.
• This version of the FBC has been updated to 2006/07 price base so that it reflects the Trust’s planned 2006/07 income as the baseline. Thus the UC in the steady state year (20016/17) is now £100.8 million (ie in line with the agreed (Capital Hospitals Limited) financial model, i.e. the £ 98.4 million UC is indexed by 1.02426.
•
11.1 Overview 11.1.1 This chapter sets out the methodology for determining the level of funding available
at 2006/07 price levels to support the scheme; determines whether this will be sufficient to fund the scheme as currently envisioned; and shows how sensitive the affordability of the scheme is to changes in key cost and income drivers. Income, both tariff and non-tariff, will be the same under both PFI and public sector comparator (PSC) options in respect of the 12-year activity and income model that the Trust has developed and agreed with its main commissioners. All figures in the tables in this chapter are at 2006/07 pay and price levels. Funding for Agenda for Change is included. The baseline includes the impact of the 2006/07 PbR rebasing exercise.
11.1.2 The steady state year for the affordability is 2016/17, which is one full financial year after the completion of all construction phases. The reason for not using 2015/16 as the completion year for the affordability analysis is that the activity projection for the Thames Gateway population increases over the 12-year period from 2005 to 2017. Thames Gateway is complete by 2016 and therefore no significant population growth is expected beyond that date (this is in line with GLA London Plan). Thus, there is a further £7 million increase in income to 2017 associated with the population increase. The sensitivity analysis (see section 11.16) within this chapter addresses how the Trust would manage a downside risk of lower population growth. It should be noted that the Trust is anticipating the receipt of £83 million in transitional relief from 2006 – 2016 in line with PbR and PFI schemes’ guidance.
11.2 Financial Performance
11.2.1 The Trust has an excellent track record on financial management with break even achieved on the Income and Expenditure account over the last 6 years. In 2005/06 the Trust’s underlying position prior to the financial close transactions was breakeven because of over-performance against activity plans and use of non-recurrent reserves. After the inclusion of the New Hospitals financial close transactions, the Trust achieved a surplus of £3.4 million in its audited accounts. The Trust made a surplus of £6.1 million from the purchase of assets for the PFI scheme being moved to capital at financial close with a loss of £2.7 million from the shortfall of impairment funding from the NHS Bank (funds impairments at 90%)
11.2.2 SSAP 17 “Accounting for Post-Balance Sheet Events” requires that events arising after the balance sheet date need to be reflected in the financial statements if they provide additional evidence of conditions that existed at the balance sheet date and materially affect the amounts to be included. Clearly, the New Hospitals Programme (NHP) financial close (27 April 2006) is both material and proximate to
Version 10.1
171
New Hospitals Programme
the 31 March year end and needs to be accounted for accordingly. Financial close involved a number of high value transactions such as the impairment and transfer of fixed assets to the New Hospitals partner (The Partner) that have directly had an impact on the Final Accounts as follows;
■ Impairment of Assets - Initially the impairment of assets transferred to the
partner was forecast to generate an expenditure charge of c£31.8 million. These impairments would occur at financial close originally forecast to be early 2006. Under NHS funds flow rules, the Trust applied for NHS bank assistance to cover the impairments charge. The NHS Bank agreed to fund c£28.6 million. The Strategic Health Authority (SHA) contributed £1.8 million leaving the Trust with a c£1.4 million in year cost pressure to meet. However there are two consequences of financial close moving to 27 April 2006;
a) The assets did not transfer to the partner so continued to attract
depreciation. After off setting the c£1.8 million contribution made by the SHA the Trust has an in year cost pressure of c£1.5 million. This is similar to the expected impairment shortfall expected by the Trust.
b) The impairment figure, recalculated to take into account depreciation and additional unavoidable capital spend (fire precaution works etc) of £25.2 million was only funded by the NHS Bank at 90%. Therefore the Trust was required to meet a further in year cost pressure of £2.7 million in 2005/06.
■ Repayment of expenditure by the Partner - As part of the planning and
business case process, the Trust purchased three properties essential to accommodate the footprint of the new hospital, and paid for a number of advanced enabling works and reasonable developer’s costs in accordance with the project agreement. Most of this expenditure occurred in 2005/6 and totalled c£42 million. This was refunded to the Trust, by the Partner, on financial close. With the exception of c£6 million, all of the repayment counted as income to offset the expenditure and therefore has a nil impact on the accounts. However, £6 million was incurred in the early stages of the development of the business case and there was less certainty that the Trust would reach financial close, therefore the Trust had to fund the expenditure in 2003/04 financial year but could not include matching income. Correspondingly, on financial close, the Trust received c£6 million income for which there is no current expenditure. The accounting entries for this were agreed with our external auditors as part of their review of the 2005/06 annual accounts.
11.2.3 As reflected in the 2005/06 audited accounts, the net impact of the two transactions is an overall non recurrent surplus of c£3.4 million. Under the new rules introduced to encourage Trusts to achieve financial surpluses, the Trust will be guaranteed to receive its surplus back in 2006/07 together with 5% interest payment (£0.17 million) on the surplus. It is stressed this is a non recurrent surplus and the Trust has a great deal of change to make under the Best Value Review to achieve a satisfactory recurrent position in 2006/7.
11.2.4 As detailed in section 11.4 and in section 6 of the Addendum to the FBC (Appendix 0G to the Executive Summary), 2006/07 presents a challenging financial year given the scale of recurrent pressures against the level of initial income. The Trust has a target surplus of £5 million (1% of turnover) for 2006/07. The Patient Access and Financial Monitoring Group undertakes a thorough review of financial and patient care activity performance; this is reviewed by the Trust Executive on a fortnightly basis.
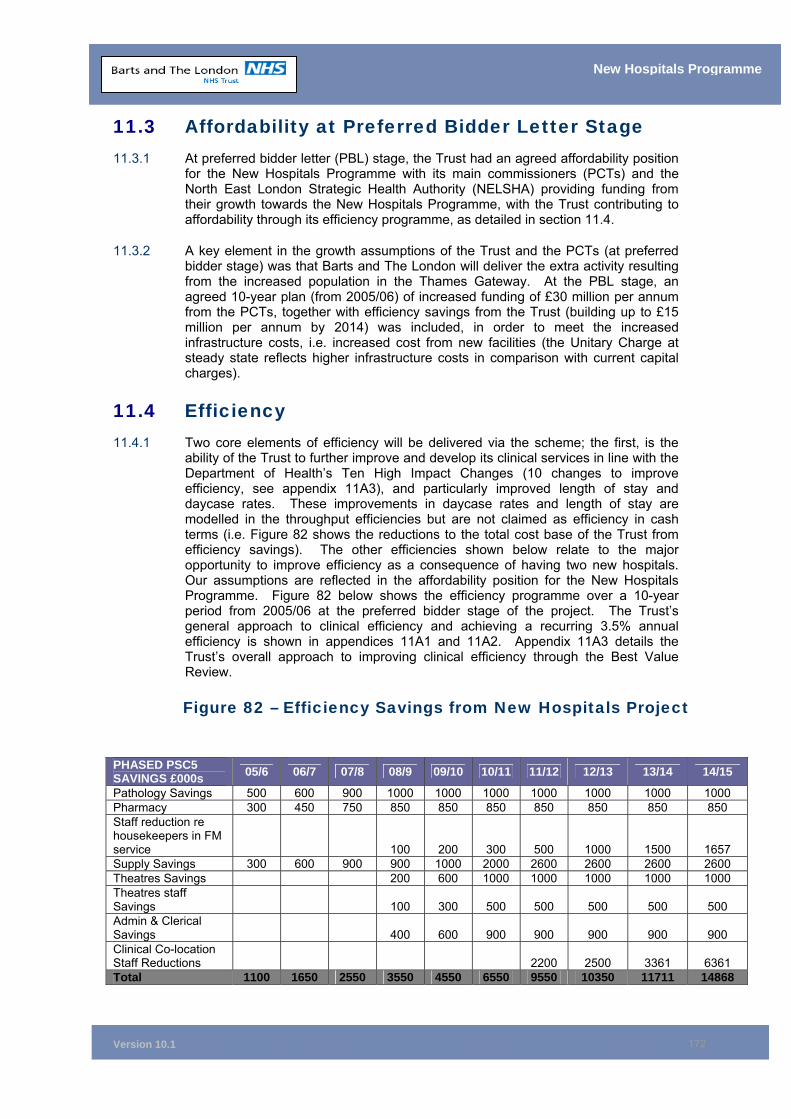
Version 10.1
172
New Hospitals Programme
11.3 Affordability at Preferred Bidder Letter Stage 11.3.1 At preferred bidder letter (PBL) stage, the Trust had an agreed affordability position
for the New Hospitals Programme with its main commissioners (PCTs) and the North East London Strategic Health Authority (NELSHA) providing funding from their growth towards the New Hospitals Programme, with the Trust contributing to affordability through its efficiency programme, as detailed in section 11.4.
11.3.2 A key element in the growth assumptions of the Trust and the PCTs (at preferred bidder stage) was that Barts and The London will deliver the extra activity resulting from the increased population in the Thames Gateway. At the PBL stage, an agreed 10-year plan (from 2005/06) of increased funding of £30 million per annum from the PCTs, together with efficiency savings from the Trust (building up to £15 million per annum by 2014) was included, in order to meet the increased infrastructure costs, i.e. increased cost from new facilities (the Unitary Charge at steady state reflects higher infrastructure costs in comparison with current capital charges).
11.4 Efficiency 11.4.1 Two core elements of efficiency will be delivered via the scheme; the first, is the
ability of the Trust to further improve and develop its clinical services in line with the Department of Health’s Ten High Impact Changes (10 changes to improve efficiency, see appendix 11A3), and particularly improved length of stay and daycase rates. These improvements in daycase rates and length of stay are modelled in the throughput efficiencies but are not claimed as efficiency in cash terms (i.e. Figure 82 shows the reductions to the total cost base of the Trust from efficiency savings). The other efficiencies shown below relate to the major opportunity to improve efficiency as a consequence of having two new hospitals. Our assumptions are reflected in the affordability position for the New Hospitals Programme. Figure 82 below shows the efficiency programme over a 10-year period from 2005/06 at the preferred bidder stage of the project. The Trust’s general approach to clinical efficiency and achieving a recurring 3.5% annual efficiency is shown in appendices 11A1 and 11A2. Appendix 11A3 details the Trust’s overall approach to improving clinical efficiency through the Best Value Review.
Figure 82 – Efficiency Savings from New Hospitals Project
PHASED PSC5 SAVINGS £000s 05/6 06/7 07/8 08/9 09/10 10/11 11/12 12/13 13/14 14/15
Pathology Savings 500 600 900 1000 1000 1000 1000 1000 1000 1000 Pharmacy 300 450 750 850 850 850 850 850 850 850 Staff reduction re housekeepers in FM service 100 200 300 500 1000 1500 1657 Supply Savings 300 600 900 900 1000 2000 2600 2600 2600 2600 Theatres Savings 200 600 1000 1000 1000 1000 1000 Theatres staff Savings 100 300 500 500 500 500 500 Admin & Clerical Savings 400 600 900 900 900 900 900 Clinical Co-location Staff Reductions 2200 2500 3361 6361 Total 1100 1650 2550 3550 4550 6550 9550 10350 11711 14868
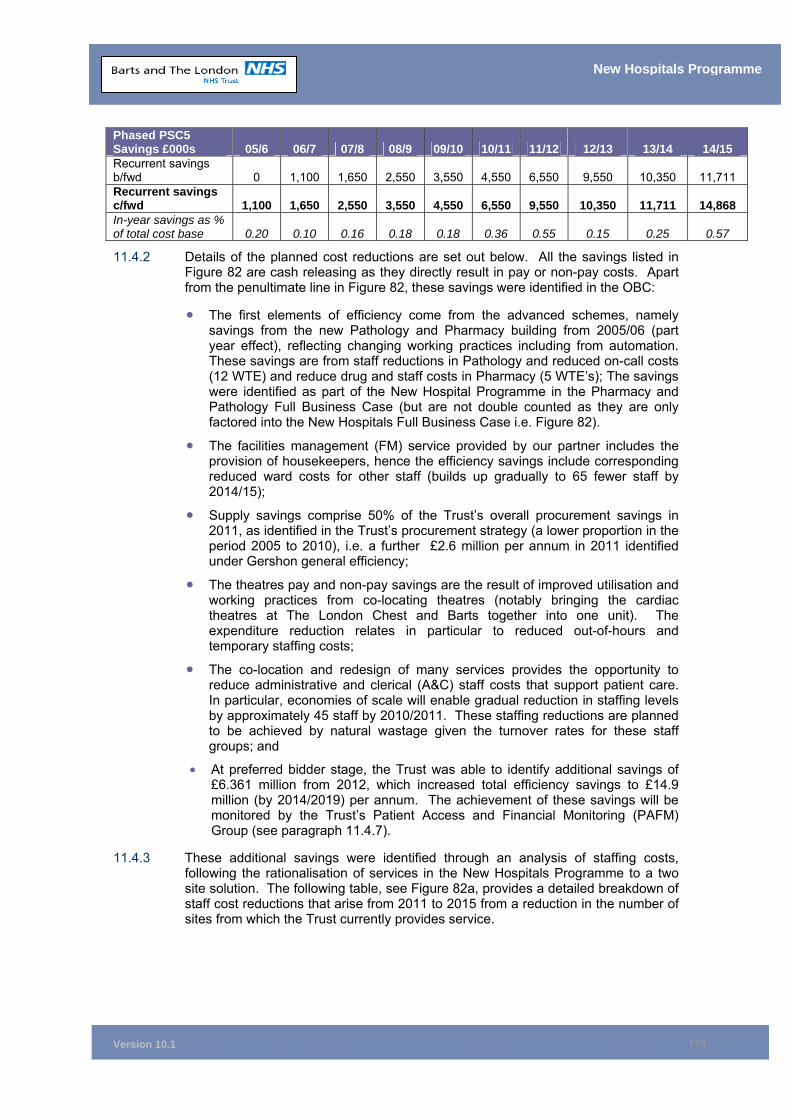
Version 10.1
173
New Hospitals Programme
Phased PSC5 Savings £000s 05/6 06/7 07/8 08/9 09/10 10/11 11/12 12/13 13/14 14/15 Recurrent savings b/fwd 0 1,100 1,650 2,550 3,550 4,550 6,550 9,550 10,350 11,711 Recurrent savings c/fwd 1,100 1,650 2,550 3,550 4,550 6,550 9,550 10,350 11,711 14,868 In-year savings as % of total cost base 0.20 0.10 0.16 0.18 0.18 0.36 0.55 0.15 0.25 0.57
11.4.2 Details of the planned cost reductions are set out below. All the savings listed in Figure 82 are cash releasing as they directly result in pay or non-pay costs. Apart from the penultimate line in Figure 82, these savings were identified in the OBC:
• The first elements of efficiency come from the advanced schemes, namely savings from the new Pathology and Pharmacy building from 2005/06 (part year effect), reflecting changing working practices including from automation. These savings are from staff reductions in Pathology and reduced on-call costs (12 WTE) and reduce drug and staff costs in Pharmacy (5 WTE’s); The savings were identified as part of the New Hospital Programme in the Pharmacy and Pathology Full Business Case (but are not double counted as they are only factored into the New Hospitals Full Business Case i.e. Figure 82).
• The facilities management (FM) service provided by our partner includes the provision of housekeepers, hence the efficiency savings include corresponding reduced ward costs for other staff (builds up gradually to 65 fewer staff by 2014/15);
• Supply savings comprise 50% of the Trust’s overall procurement savings in 2011, as identified in the Trust’s procurement strategy (a lower proportion in the period 2005 to 2010), i.e. a further £2.6 million per annum in 2011 identified under Gershon general efficiency;
• The theatres pay and non-pay savings are the result of improved utilisation and working practices from co-locating theatres (notably bringing the cardiac theatres at The London Chest and Barts together into one unit). The expenditure reduction relates in particular to reduced out-of-hours and temporary staffing costs;
• The co-location and redesign of many services provides the opportunity to reduce administrative and clerical (A&C) staff costs that support patient care. In particular, economies of scale will enable gradual reduction in staffing levels by approximately 45 staff by 2010/2011. These staffing reductions are planned to be achieved by natural wastage given the turnover rates for these staff groups; and
• At preferred bidder stage, the Trust was able to identify additional savings of £6.361 million from 2012, which increased total efficiency savings to £14.9 million (by 2014/2019) per annum. The achievement of these savings will be monitored by the Trust’s Patient Access and Financial Monitoring (PAFM) Group (see paragraph 11.4.7).
11.4.3 These additional savings were identified through an analysis of staffing costs, following the rationalisation of services in the New Hospitals Programme to a two site solution. The following table, see Figure 82a, provides a detailed breakdown of staff cost reductions that arise from 2011 to 2015 from a reduction in the number of sites from which the Trust currently provides service.
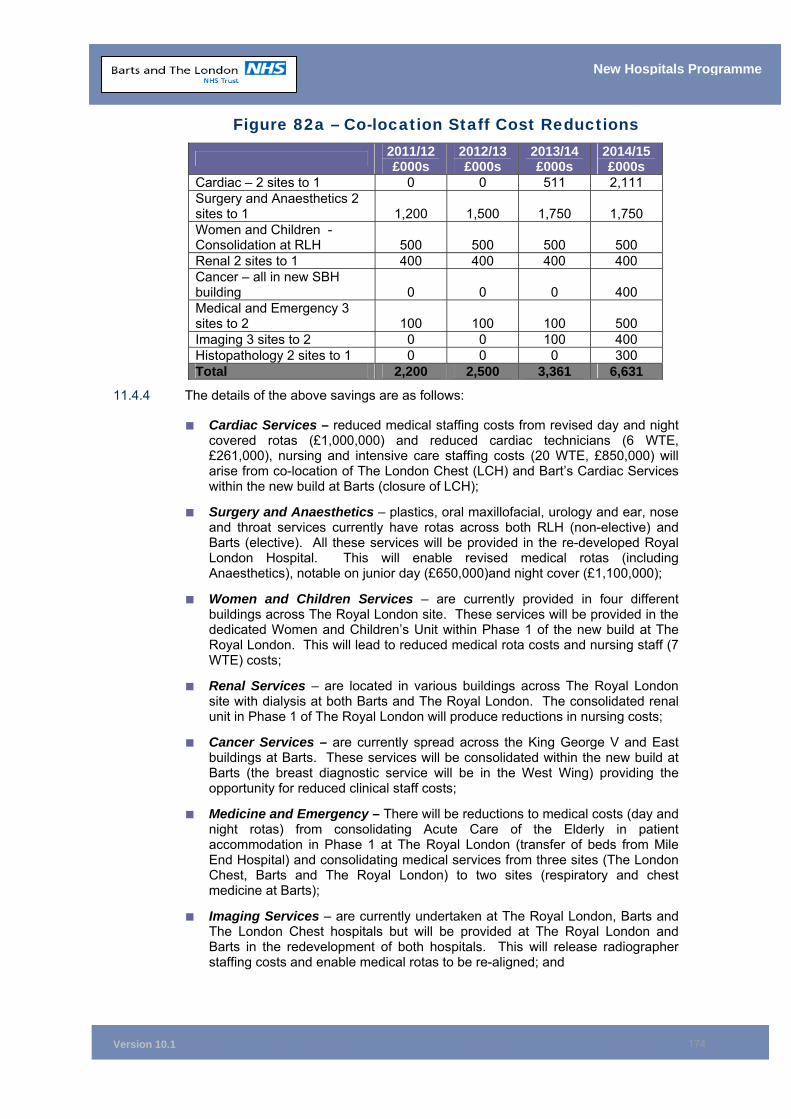
Version 10.1
174
New Hospitals Programme
Figure 82a – Co-location Staff Cost Reductions
2011/12 £000s
2012/13 £000s
2013/14 £000s
2014/15 £000s
Cardiac – 2 sites to 1 0 0 511 2,111 Surgery and Anaesthetics 2 sites to 1 1,200 1,500 1,750 1,750 Women and Children - Consolidation at RLH 500 500 500 500 Renal 2 sites to 1 400 400 400 400 Cancer – all in new SBH building 0 0 0 400 Medical and Emergency 3 sites to 2 100 100 100 500 Imaging 3 sites to 2 0 0 100 400 Histopathology 2 sites to 1 0 0 0 300 Total 2,200 2,500 3,361 6,631
11.4.4 The details of the above savings are as follows:
■ Cardiac Services – reduced medical staffing costs from revised day and night covered rotas (£1,000,000) and reduced cardiac technicians (6 WTE, £261,000), nursing and intensive care staffing costs (20 WTE, £850,000) will arise from co-location of The London Chest (LCH) and Bart’s Cardiac Services within the new build at Barts (closure of LCH);
■ Surgery and Anaesthetics – plastics, oral maxillofacial, urology and ear, nose and throat services currently have rotas across both RLH (non-elective) and Barts (elective). All these services will be provided in the re-developed Royal London Hospital. This will enable revised medical rotas (including Anaesthetics), notable on junior day (£650,000)and night cover (£1,100,000);
■ Women and Children Services – are currently provided in four different buildings across The Royal London site. These services will be provided in the dedicated Women and Children’s Unit within Phase 1 of the new build at The Royal London. This will lead to reduced medical rota costs and nursing staff (7 WTE) costs;
■ Renal Services – are located in various buildings across The Royal London site with dialysis at both Barts and The Royal London. The consolidated renal unit in Phase 1 of The Royal London will produce reductions in nursing costs;
■ Cancer Services – are currently spread across the King George V and East buildings at Barts. These services will be consolidated within the new build at Barts (the breast diagnostic service will be in the West Wing) providing the opportunity for reduced clinical staff costs;
■ Medicine and Emergency – There will be reductions to medical costs (day and night rotas) from consolidating Acute Care of the Elderly in patient accommodation in Phase 1 at The Royal London (transfer of beds from Mile End Hospital) and consolidating medical services from three sites (The London Chest, Barts and The Royal London) to two sites (respiratory and chest medicine at Barts);
■ Imaging Services – are currently undertaken at The Royal London, Barts and The London Chest hospitals but will be provided at The Royal London and Barts in the redevelopment of both hospitals. This will release radiographer staffing costs and enable medical rotas to be re-aligned; and

Version 10.1
175
New Hospitals Programme
■ Histopathology – is currently provided at The Royal London and Barts. At the end of Phase 3, these services will be centrally provided at The Royal London Hospital (with a hot laboratory at Barts). This will enable a reduction in scientific and technical staffing costs.
11.4.5 In total, savings of £15 million per annum are planned to be achieved by 2015. In addition, over the next 10 years, the Trust will have an efficiency programme that delivers financial stability under the PbR regime, in the context of:
■ The Pathfinder Clinical Strategy; ■ Care Record Service (CRS); ■ The New Hospitals Project; ■ Achieving procurement savings/reducing back office costs, in line with the
Gershon savings requirements; and ■ Efficiency savings from the 10 High Impact Changes
11.4.6 The Appendix 11A (3) details the Trust’s Medium Term Financial Strategy including its approach to clinical efficiency and Figure 82b provides an overall summary of the Trust’s cost improvement programme for the period 2005 to 2014.
Figure 82b – Trust Efficiency Programme
EFFICIENCY TOTAL TO 2014 £M New Hospitals 14.9 Care Records Service & Picture Archive Communications Service
0.6 (tbc) 1.4
PbR – cost Reduction 7.7 Sub total 24.6 Best Value Review 30 GRAND TOTAL 54.6
Note: New Hospital efficiency saving are achieved in full for 2014/15 and hence remain the same value for steady state (2016/17)
11.4.7 The Patient Access and Financial Monitoring Group (PAFM), which is jointly chaired by the Directors of Finance and Performance Management & Planning (and includes all the clinical directorate general managers), is responsible for co-ordinating the development of efficiency plans (including the 10 High Impact Changes and Gershon savings) and monitoring their delivery. The tracking schedule that PAFM uses for both the development and monitoring of the efficiency programme109, enables the Trust to ensure that there is no double counting of efficiency savings between the new hospitals project and the other workstreams.
11.4.8 Thus the Patient Access & Financial Monitoring Group has the task of reviewing the delivery of the above cost improvement plan. The December 2005 plan amounts to a reduction in the Trust’s cost base of nearly 3% by 2008 then a further reduction of 1.5% by 2014 from cost reductions related to the New Hospitals Programme (see Figure 82b). However, the trust is now also faced by the following additional pressures;
Uplift to tariffs – The uplift to the 2006/7 tariffs is 1.5% (6.5% generic uplift less
2.5% efficiency and less 2.5% tariff deflation). This entails less than full funding for pay and non-pay (notably power, heat and light and drug cost pressures).
Pay Drift - Although the trust has a benefits realisation plan for AfC it does not
result in sufficient cost reduction to offset the likely level of funding for the 109 See Appendix 11A for the Trust’s efficiency programme.
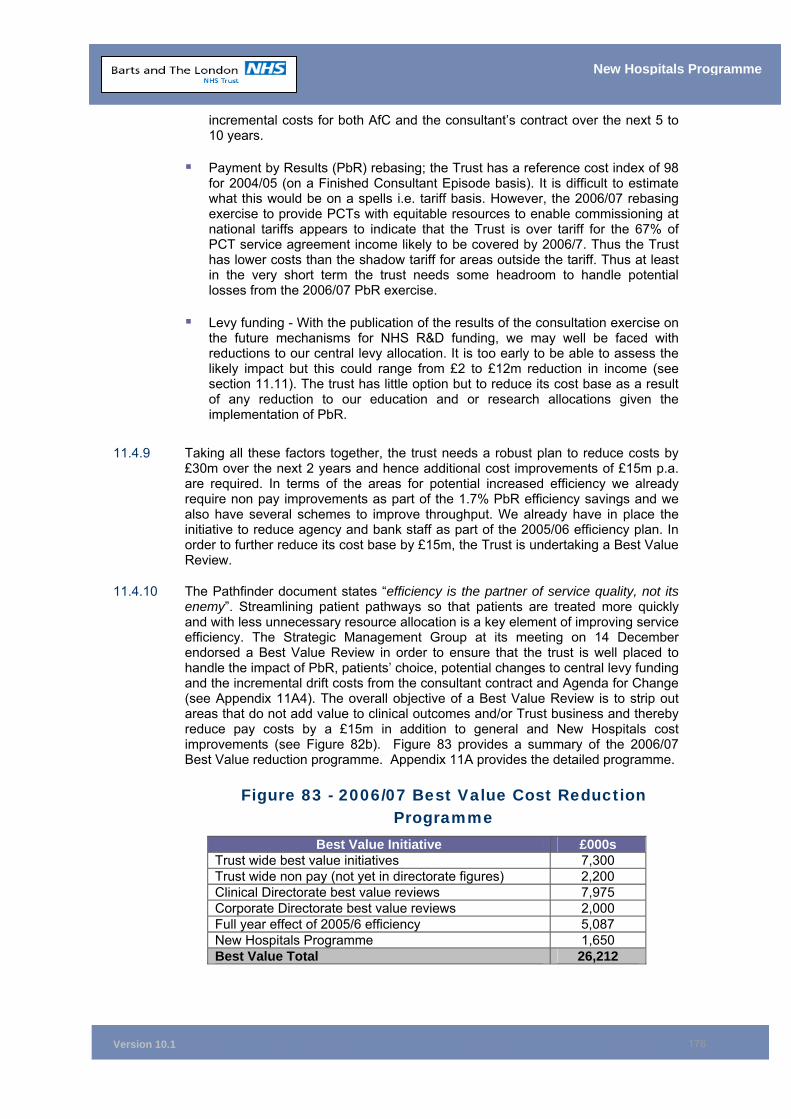
Version 10.1
176
New Hospitals Programme
incremental costs for both AfC and the consultant’s contract over the next 5 to 10 years.
Payment by Results (PbR) rebasing; the Trust has a reference cost index of 98
for 2004/05 (on a Finished Consultant Episode basis). It is difficult to estimate what this would be on a spells i.e. tariff basis. However, the 2006/07 rebasing exercise to provide PCTs with equitable resources to enable commissioning at national tariffs appears to indicate that the Trust is over tariff for the 67% of PCT service agreement income likely to be covered by 2006/7. Thus the Trust has lower costs than the shadow tariff for areas outside the tariff. Thus at least in the very short term the trust needs some headroom to handle potential losses from the 2006/07 PbR exercise.
Levy funding - With the publication of the results of the consultation exercise on
the future mechanisms for NHS R&D funding, we may well be faced with reductions to our central levy allocation. It is too early to be able to assess the likely impact but this could range from £2 to £12m reduction in income (see section 11.11). The trust has little option but to reduce its cost base as a result of any reduction to our education and or research allocations given the implementation of PbR.
11.4.9 Taking all these factors together, the trust needs a robust plan to reduce costs by £30m over the next 2 years and hence additional cost improvements of £15m p.a. are required. In terms of the areas for potential increased efficiency we already require non pay improvements as part of the 1.7% PbR efficiency savings and we also have several schemes to improve throughput. We already have in place the initiative to reduce agency and bank staff as part of the 2005/06 efficiency plan. In order to further reduce its cost base by £15m, the Trust is undertaking a Best Value Review.
11.4.10 The Pathfinder document states “efficiency is the partner of service quality, not its enemy”. Streamlining patient pathways so that patients are treated more quickly and with less unnecessary resource allocation is a key element of improving service efficiency. The Strategic Management Group at its meeting on 14 December endorsed a Best Value Review in order to ensure that the trust is well placed to handle the impact of PbR, patients’ choice, potential changes to central levy funding and the incremental drift costs from the consultant contract and Agenda for Change (see Appendix 11A4). The overall objective of a Best Value Review is to strip out areas that do not add value to clinical outcomes and/or Trust business and thereby reduce pay costs by a £15m in addition to general and New Hospitals cost improvements (see Figure 82b). Figure 83 provides a summary of the 2006/07 Best Value reduction programme. Appendix 11A provides the detailed programme.
Figure 83 - 2006/07 Best Value Cost Reduction Programme
Best Value Initiative £000s Trust wide best value initiatives 7,300 Trust wide non pay (not yet in directorate figures) 2,200 Clinical Directorate best value reviews 7,975 Corporate Directorate best value reviews 2,000 Full year effect of 2005/6 efficiency 5,087 New Hospitals Programme 1,650 Best Value Total 26,212
Version 10.1
177
New Hospitals Programme
11.4.11 In conclusion, the efficiency savings that are required for both the new hospitals project and “general efficiency” to sustain financial stability are challenging, but achievable.
11.5 Affordability at FBC/Financial Close Overview of Analysis
11.5.1 The following provides an overview of the affordability analysis. For the FBC, we have modelled a base case scenario as follows.
Income & Activity
11.5.2 The Trust has worked with the top 90% of its patient care commissioners, (which representing 80% of the Trust total income, see Appendix 0C and 1B) to agree income and activity assumptions in the FBC. The seven PCTs in North East London and the thirteen Essex PCTs have been provided with a 12-year activity plan that takes account of projected increases in activity for population growth, demand and productivity (taking into account Government policy and Department of Health planning specifications issued to PCTs and trusts).
11.5.3 As the national tariffs will be fully implemented by the steady state year, the key affordability issue for PCTs is confirmation that the activity projections are robust. The activity model agreed by the PCTs in 2005 has not been altered in this version of the FBC apart from 2006/07 to reflect SLA agreements. The base assumptions have been tested with our commissioners for supporting, undergraduate and postgraduate education and training. The base model also includes increases for RTA and external contract income increases of £800,000 per annum by 2011/2012.
Expenditure
11.5.4 The expenditure baseline is 2005/06 (unaudited accounts) updated to 2006/07 for inflation. The current Facilities Management (FM) costs (which are being transferred to the PFI partner) are removed from the Trust’s cost base. The cost base is then additionally adjusted for the net impact from the PFI contract; both the unitary charge and the impact on capital charges (including the capital charges for non-managed equipment and the advance schemes). Marginal costs are then also included for the additional patient care activity. Figure 88 in 11.12.4 provides a summary of the changes in costs and appendices 11D and 11M detail the Trust’s income and Expenditure Account (year by year over the period to 2016/2017).
Marginal Costs
11.5.5 Within the FBC, marginal costs in the medium term have been flexed upwards to reflect stepped costs for meeting the “18-weeks-to-treat” target. Marginal costs are assumed at 59% for 2006/7 but if there is a deferring of activity to meet the target, the marginal costs exceed 95% for the period 1/4/07 to 31/3/08 (97% in 2007/8). This is to ensure that the impact of any changes to activity to meet access targets is neutral. The other reason for assuming almost 100% is to neutralise any impact of the 2006/07 deflation of the national tariffs, i.e. there is no PbR gain available from the increased income to provide a contribution to the interim unitary charge.
Marginal Costs 2008/12
11.5.6 The FBC includes a marginal cost rate for additional activity at 55% for the period 2008/09 to 2010/11, given the low levels of activity growth (50% assumed in 2011/12). See Appendix 11D1 in Version 9 of the FBC.
Version 10.1
178
New Hospitals Programme
Marginal Costs 2010 – 2017
11.5.7 The marginal rate for increased activity for the period 2010 to 2015 is set at 40%. As the level of cost improvements related to the New Hospitals Programme (NHP) increases from 2010 to 2015 by £8m (over 5 years) and by 2016/17 the Trust will be a top performing teaching hospital in terms of productivity. The Trust considers that these marginal rates are robust in the sense that this should be the maximum level of additional costs for the required level of extra activity over the period.
11.5.8 The marginal costs assumptions are based on the Trust’s current marginal cost rates. There is wide variation across specialties with, for example, the marginal rate for acute elderly activity at around 20% whereas the marginal rate for medical oncology activity is in the region of 80% (impact of drug costs for chemotherapy treatments). The 40% is a weighted average.
Affordable Unitary Charge
11.5.9 The affordable unitary charge for the steady state year (2016/17) is therefore the difference between the income received from commissioners and the revised expenditure baseline. The Trust is able to afford a unitary charge of £100.8 million for the steady state year (at 2006/07 prices). This is exclusive of the transitional funding that the Trust should receive from the NHS Bank, in line with the DH guidance on PbR (see 11.13).
11.6 Affordability and Payment by Results 11.6.1 The PbR funding methodology is being phased in over the period to 2007/08 and
thus will be fully in place well before the completion of the scheme. The additional income available to the Trust for the New Hospitals Project will be largely dependent on the funding available under PbR, i.e. payment for additional activity at national tariffs.
11.6.2 The base case activity model for the FBC is priced at 2006/07 levels and hence includes a downward adjustment for 2006/07 national tariff deflation and local 2005/06 prices plus a 4% inflation uplift for non-PbR services110. This represents the starting income amount for each of the Trust’s PCTs. The overall uplift to 2005/06 equates to 4% when the impact of devices and drugs that are charged as exclusions to the tariff are included in income (as per 2006/07 actual SLA agreements). The base case model has 63% of Service Agreement (SLA) income on national tariffs and 37% increase at local prices, in line with 2006/07 planned SLA income.
11.6.3 The Trust’s local prices are lower than the 2006/07 shadow tariffs (national average costs 2004/05). See Appendix 11F for the sensitivity analysis. The prices used for the income modelling to 2016/17 have been subject to validation by the North East London Strategic Health Authority and have been reconciled back to the Trust’s PbR income plan for 2006/07.
11.6.4 In terms of the activity used, the model assumes:
■ Cardiac - activity changes in spells for cardiac activity at the proposed national tariff rates for 2006/07.
■ Non-cardiac - for the activity changes associated with “other” activity and Thames Gateway activity, the modelling work has been performed in finished consultant episodes (FCE). The Trust has calculated a PbR compliant FCE
110 Only activity outside of the original published 2006/07 PbR tariffs scope is at local prices
Version 10.1
179
New Hospitals Programme
cost, based on the weighted average FCE rate from the tariff (including an abatement for short stays and supplement for excess bed days and specialist services as defined in the PbR rebasing process), using 2006/07 tariff rates and local prices where the tariff is not yet in existence.
■ Critical Care - critical care costs are included in the associated FCE prices. Care has been taken to ensure that they are not “double- counted’, for example in an occupied bed day rate. See section 3.9.10 for explanation of increase in critical care capacity.
■ Market Forces Factor (MFF) – the MFF has been excluded from all pricing but has been subsequently added back at PCT level, and varies each year proportionally to PCT income.
11.7 Market Forces Factor 11.7.1 Although the Trust’s patient-related income will be derived from national tariffs, the
DH recognises unavoidable geographical input cost differences by means of a MFF. The MFF is set annually by DH, based on external comparators provided by the University of Warwick. It can therefore change independently of NHS costs and the Trust’s own cost base. The MFF does (or is expected to) cover the Trust’s overall income base including levies. The base case assumes no change from the Trust’s 2006/07 MFF (1.3455), which is 2% lower than the MFF for 2005/06.
11.7.2 The reduced MFF comes from the move from central London to PCT pay zones (for the staffing element of the MFF) and the increased level of the un-weighted element within the MFF. The Trust and NELSHA have requested a revision to the MFF zones, as there is no zone for the Corporation of London and Warwick has used Hackney as the proxy to set the zone for Barts. Barts is 28% of the total MFF for the Trust and we estimate that the adoption of a Corporation of London zone would add a minimum of 0.5% to our MFF (i.e. an MFF index of 1.35 for 2006/07). This would represent additional income of c£250k in 2006/07 under the originally proposed scope of Payments by Results.
11.8 Activity Modelling for PCTs 11.8.1 The activity analysis for the New Hospitals Project is very complex. Even before
the advent of Patient Choice, the environment that the Trust operates in is highly dynamic. The changes are driven by:
■ The proposed development of Thames Gateway;
■ New models of care within the primary, secondary and tertiary sectors;
■ The revised standard of a maximum 18 week wait from referral to treatment; and
■ The use of the independent sector for the provision of some health care services.
11.8.2 In line with the Addendum to the FBC, the activity analysis in the base case has not been altered in this final version of the FBC. This is because Version 09 of the FBC (December 2005) already included adjustments that foresaw the 2006 White Paper (treating patients closer to home), Moreover, as part of the review of version 10 of the FBC, the Trust has recently confirmed with THPCT that the activity assumptions remain robust following the publication of the White Paper. However, the productivity assumptions have changed (see section 11.9).
11.8.3 The starting point for the analysis, in both activity and finance terms, is the PbR rebasing position, i.e. 2003/4 outturn. In the case of Tower Hamlets PCT, however,
Version 10.1
180
New Hospitals Programme
the 2004/05 outturn activity has been used as this represents a material change from the 2003/04 position. This starting position is then adjusted for 2006/07 planned activity (as per SLAs) and then for the population changes and other factors to derive the activity level for each PCTs in each financial year up to 2016/17. This analysis has focused on the sustainability of the level of activity by 2016/17. This year has been chosen as it represents the end point of the population modelling associated with Thames Gateway, so is the most reliable estimate the Trust has for planning purposes of population derived demand for secondary care activity. The Business Case is predicated on the design solution providing sufficient capacity at this point, and this has been the focus of the Trusts bed modelling. In addition to this end point goal, the Trust is continuing to refine the view of required capacity during the transitional years to this point. The contract keeps the bed capacity during the construction phase of the scheme at current levels; and the Trust is now refining the collective view of capacity to meet the 18 week referral to treatment standard, to ensure the adequacy of the current bed total of 1,172 between now and 2016/17. If there is an increase in beds required over the interim period then this would increase the marginal costs associated with the activity model. This has been factored into 2007 to 2010 expenditure projections. If extra beds were to be needed for the base case activity during the interim then the Trust would manage this within the overall affordability envelope during the interim. (it is highly unlikely we would allow extra beds for planned level of activity unless casemix changed in which case would be linked to higher income).
11.8.4 The income and activity totals used as the start point for the modelling are recognisable to PCTs and there is an audit trail to the PbR summaries used for the 2004/05 to 2006/07 rebasing processes. A prudent model of activity growth has been derived, which assumes that all of the activity modelled in the Trust’s capacity plan for 2005-08 is non-recurrent in nature i.e. there will be a one off stock reduction to get to 4 week Out-Patient and 10 week In-Patient/Day Case waiting which will not have a recurrent impact on demand for secondary care services. This means that the activity modelling assumes that all the activity which is required to hit the 18 week referral to treatment target will have no impact recurrently on PCT referral and treatment patterns. The modelling for the activity projections to 2016/17 is the approach agreed with the East London & City Information Service (ELCIS). Appendix 11D(1) shows an additional option for PCT income for 2007/08 with the adding back of deferred activity (from 2006/07) growth to meet the 18 week to treat target. This is a non-recurrent change within the model. This option relates to the fact that London PCTs have deferred increased activity in 2006/07 towards reduced waiting times along the path to achieving 18 weeks to treat due to the need to provide 3% of their allocations to London SHA as part of London’s financial plan to balance. Hence there is a scenario whereby PCTs would add back the deferred activity into 2007/08 SLAs (treated as non recurrent increase in our PFI income and activity model).
11.8.5 The Trust currently (2004/05) has an overall reference cost index (RCI) of 98 on a FCE basis. The DH does not publish an index on a spells basis (NHS costs are on an FCE basis but the tariff is published on a spells basis) and there are different methodologies available to prepare a spells based RCI. The PbR team at DH have informally advised the Trust that we have an RCI of 97 on a spells basis, using the HES activity data (2004 calendar year). In line with PbR for 2006/07, the base income and activity model reflects 63% of our patient care services being charged at national tariffs and 37% charged at local prices.
11.8.6 Using CHKS data from our membership of the Inner London Teaching Hospitals Group, financial variance analysis shows that our FCE to admission ratio equates to the national average for 2004/05 based on 2004/05 reference costs submissions (i.e. uses 2004/05 activity outturn).
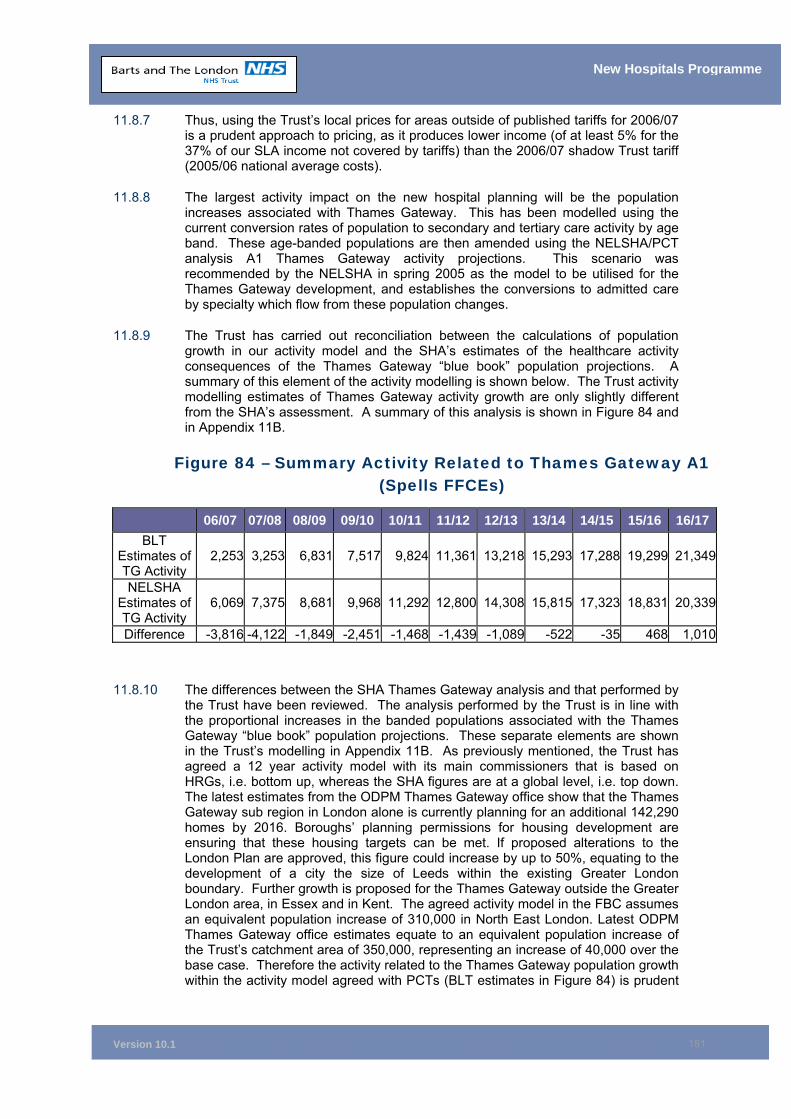
Version 10.1
181
New Hospitals Programme
11.8.7 Thus, using the Trust’s local prices for areas outside of published tariffs for 2006/07 is a prudent approach to pricing, as it produces lower income (of at least 5% for the 37% of our SLA income not covered by tariffs) than the 2006/07 shadow Trust tariff (2005/06 national average costs).
11.8.8 The largest activity impact on the new hospital planning will be the population increases associated with Thames Gateway. This has been modelled using the current conversion rates of population to secondary and tertiary care activity by age band. These age-banded populations are then amended using the NELSHA/PCT analysis A1 Thames Gateway activity projections. This scenario was recommended by the NELSHA in spring 2005 as the model to be utilised for the Thames Gateway development, and establishes the conversions to admitted care by specialty which flow from these population changes.
11.8.9 The Trust has carried out reconciliation between the calculations of population growth in our activity model and the SHA’s estimates of the healthcare activity consequences of the Thames Gateway “blue book” population projections. A summary of this element of the activity modelling is shown below. The Trust activity modelling estimates of Thames Gateway activity growth are only slightly different from the SHA’s assessment. A summary of this analysis is shown in Figure 84 and in Appendix 11B.
Figure 84 – Summary Activity Related to Thames Gateway A1 (Spells FFCEs)
11.8.10 The differences between the SHA Thames Gateway analysis and that performed by the Trust have been reviewed. The analysis performed by the Trust is in line with the proportional increases in the banded populations associated with the Thames Gateway “blue book” population projections. These separate elements are shown in the Trust’s modelling in Appendix 11B. As previously mentioned, the Trust has agreed a 12 year activity model with its main commissioners that is based on HRGs, i.e. bottom up, whereas the SHA figures are at a global level, i.e. top down. The latest estimates from the ODPM Thames Gateway office show that the Thames Gateway sub region in London alone is currently planning for an additional 142,290 homes by 2016. Boroughs’ planning permissions for housing development are ensuring that these housing targets can be met. If proposed alterations to the London Plan are approved, this figure could increase by up to 50%, equating to the development of a city the size of Leeds within the existing Greater London boundary. Further growth is proposed for the Thames Gateway outside the Greater London area, in Essex and in Kent. The agreed activity model in the FBC assumes an equivalent population increase of 310,000 in North East London. Latest ODPM Thames Gateway office estimates equate to an equivalent population increase of the Trust’s catchment area of 350,000, representing an increase of 40,000 over the base case. Therefore the activity related to the Thames Gateway population growth within the activity model agreed with PCTs (BLT estimates in Figure 84) is prudent
06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17BLT
Estimates of TG Activity
2,253 3,253 6,831 7,517 9,824 11,361 13,218 15,293 17,288 19,299 21,349
NELSHA Estimates of TG Activity
6,069 7,375 8,681 9,968 11,292 12,800 14,308 15,815 17,323 18,831 20,339
Difference -3,816 -4,122 -1,849 -2,451 -1,468 -1,439 -1,089 -522 -35 468 1,010
Version 10.1
182
New Hospitals Programme
given it is a bottom up analysis based on the original London plan (see section 1.4.3).
11.8.11 The other important reference point for the activity modelling in the FBC is to reappraise the activity modelling which was undertaken for the OBC, thus we have assumed choice has neutral overall impact. This has been conducted in conjunction with a review of the comparison of the efficiency throughput assumptions, in the productivity assumptions section of this chapter.
11.8.12 The central assumption in the activity modelling is that current referrals to the Trust are an adequate starting point, or proxy, for future referrals. In the absence of a completely new model defining the health economy in North East London, Essex and further afield, this projection methodology acts as a pragmatic starting point to the activity modelling. This model is then refined by the introduction of the other variables for the modelling of increased independent sector provision and changes to admissions due to new models of care for dealing with Long Term Conditions. This approach has allowed the Trust to perform a PCT-specific analysis of activity to 2016/17, based on the existing nature of their disparate referral patterns to the Trust.
11.8.13 The different balance of secondary care activity versus tertiary care activity is encompassed by this approach. These historic referrals are then adjusted proportionally to the changes in age and sex adjusted population to derive the likely healthcare demand associated with the planned changes to the North East London population. In addition to population changes, some element of referral growth is modelled into the activity projections, as per the capacity planning assumptions of NELSHA PCT Analysis A1 Thames Gateway population impact. The population and referral growth assumptions used for the baseline activity projections are summarised in Appendix 11B in spells. Appendix 11C then shows the activity and finance position by PCT which reconciles to these spell based totals. These are the activity and finance totals which have been agreed by the PCTs in the Full Business Case approval process.
11.8.14 The main components of the admitted patient care activity analysis are listed below. The first two impact particularly on the medium term, while Thames Gateway is the most significant factor in the longer term.
■ Cardiac Services - the model uses the revised cardiac activity plan for 2005/06-2008/09 issued by the North East London (NEL) and Essex Specialist Commissioning Groups. This models the effects of new angiography centres, conversions of the angiography numbers into surgery and the impact of the 18 week referral to treatment standard. It also takes into account the opening of the new Essex Cardiac Centre in Basildon (due to open in 2007/08), with 24% of current South Essex PCTs cardiac flows continuing to be referred to The Trust beyond 2008.
■ Other Activity – for other specialties, the Trust has performed its own assessment of the volume of activity required to achieve waiting list reductions necessary to deliver 18 weeks referral to treatment.
■ Thames Gateway Activity Changes – this is based on assumption A1 for NEL. The PCT level model uses the current five year banded age ranges conversion rates to admitted patient care. As these banded populations change, the activity changes proportionately.
Patients Choice
11.8.15 While Patients’ Choice may change detailed referral patterns, it has been assumed that the overall impact will be neutral in steady state. This is based on the experience to date of Patient Choice in London. The Trust has three years
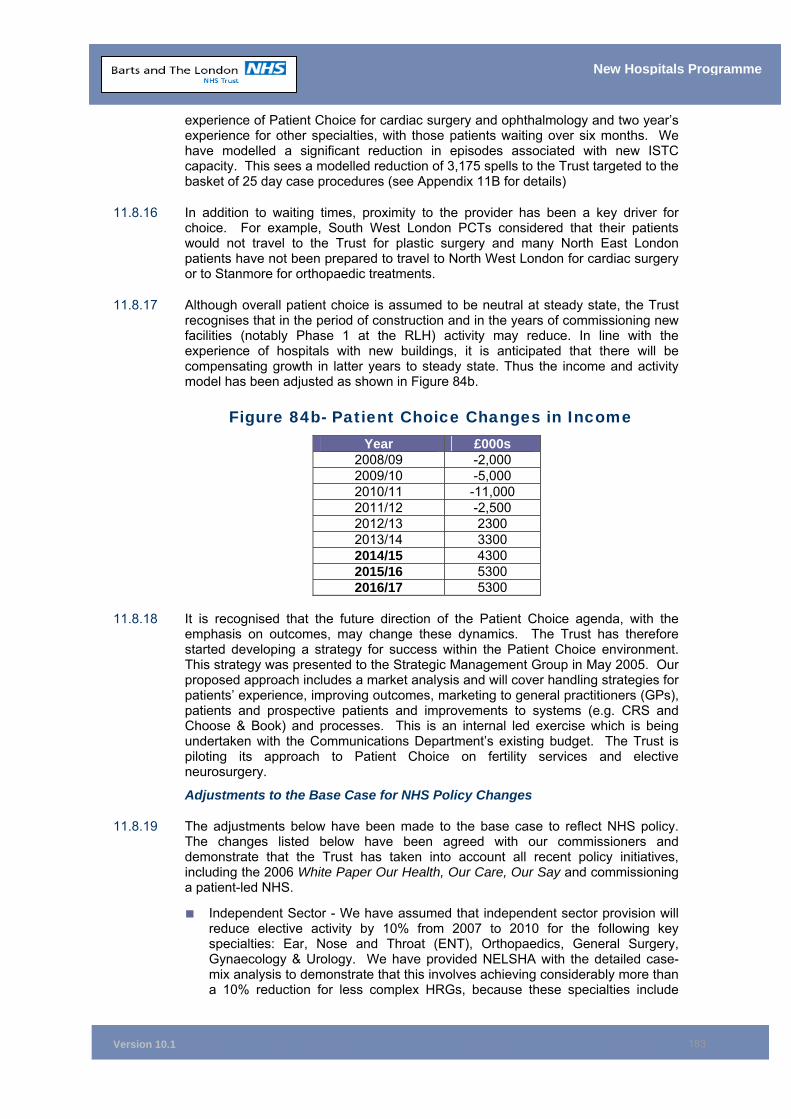
Version 10.1
183
New Hospitals Programme
experience of Patient Choice for cardiac surgery and ophthalmology and two year’s experience for other specialties, with those patients waiting over six months. We have modelled a significant reduction in episodes associated with new ISTC capacity. This sees a modelled reduction of 3,175 spells to the Trust targeted to the basket of 25 day case procedures (see Appendix 11B for details)
11.8.16 In addition to waiting times, proximity to the provider has been a key driver for choice. For example, South West London PCTs considered that their patients would not travel to the Trust for plastic surgery and many North East London patients have not been prepared to travel to North West London for cardiac surgery or to Stanmore for orthopaedic treatments.
11.8.17 Although overall patient choice is assumed to be neutral at steady state, the Trust recognises that in the period of construction and in the years of commissioning new facilities (notably Phase 1 at the RLH) activity may reduce. In line with the experience of hospitals with new buildings, it is anticipated that there will be compensating growth in latter years to steady state. Thus the income and activity model has been adjusted as shown in Figure 84b.
Figure 84b- Patient Choice Changes in Income Year £000s
2008/09 -2,000 2009/10 -5,000 2010/11 -11,000 2011/12 -2,500 2012/13 2300 2013/14 3300 2014/15 4300 2015/16 5300 2016/17 5300
11.8.18 It is recognised that the future direction of the Patient Choice agenda, with the
emphasis on outcomes, may change these dynamics. The Trust has therefore started developing a strategy for success within the Patient Choice environment. This strategy was presented to the Strategic Management Group in May 2005. Our proposed approach includes a market analysis and will cover handling strategies for patients’ experience, improving outcomes, marketing to general practitioners (GPs), patients and prospective patients and improvements to systems (e.g. CRS and Choose & Book) and processes. This is an internal led exercise which is being undertaken with the Communications Department’s existing budget. The Trust is piloting its approach to Patient Choice on fertility services and elective neurosurgery.
Adjustments to the Base Case for NHS Policy Changes
11.8.19 The adjustments below have been made to the base case to reflect NHS policy. The changes listed below have been agreed with our commissioners and demonstrate that the Trust has taken into account all recent policy initiatives, including the 2006 White Paper Our Health, Our Care, Our Say and commissioning a patient-led NHS.
■ Independent Sector - We have assumed that independent sector provision will reduce elective activity by 10% from 2007 to 2010 for the following key specialties: Ear, Nose and Throat (ENT), Orthopaedics, General Surgery, Gynaecology & Urology. We have provided NELSHA with the detailed case-mix analysis to demonstrate that this involves achieving considerably more than a 10% reduction for less complex HRGs, because these specialties include
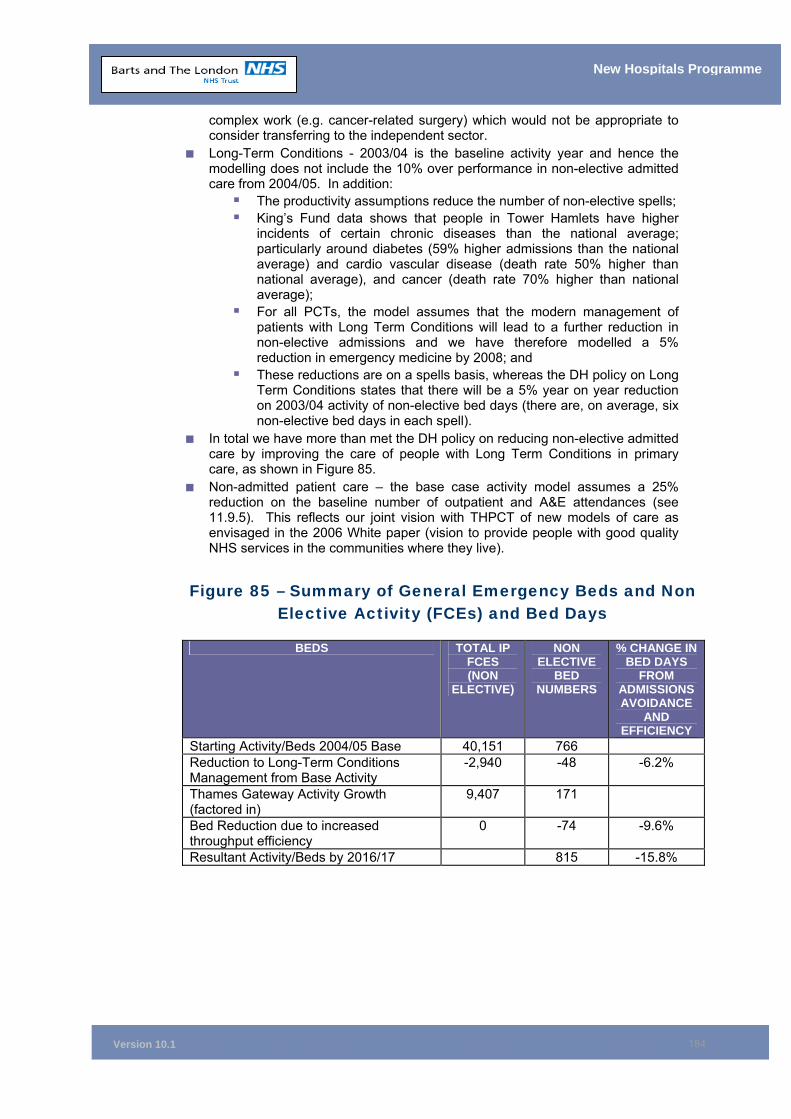
Version 10.1
184
New Hospitals Programme
complex work (e.g. cancer-related surgery) which would not be appropriate to consider transferring to the independent sector.
■ Long-Term Conditions - 2003/04 is the baseline activity year and hence the modelling does not include the 10% over performance in non-elective admitted care from 2004/05. In addition:
The productivity assumptions reduce the number of non-elective spells; King’s Fund data shows that people in Tower Hamlets have higher
incidents of certain chronic diseases than the national average; particularly around diabetes (59% higher admissions than the national average) and cardio vascular disease (death rate 50% higher than national average), and cancer (death rate 70% higher than national average);
For all PCTs, the model assumes that the modern management of patients with Long Term Conditions will lead to a further reduction in non-elective admissions and we have therefore modelled a 5% reduction in emergency medicine by 2008; and
These reductions are on a spells basis, whereas the DH policy on Long Term Conditions states that there will be a 5% year on year reduction on 2003/04 activity of non-elective bed days (there are, on average, six non-elective bed days in each spell).
■ In total we have more than met the DH policy on reducing non-elective admitted care by improving the care of people with Long Term Conditions in primary care, as shown in Figure 85.
■ Non-admitted patient care – the base case activity model assumes a 25% reduction on the baseline number of outpatient and A&E attendances (see 11.9.5). This reflects our joint vision with THPCT of new models of care as envisaged in the 2006 White paper (vision to provide people with good quality NHS services in the communities where they live).
Figure 85 – Summary of General Emergency Beds and Non Elective Activity (FCEs) and Bed Days
BEDS TOTAL IP FCES (NON
ELECTIVE)
NON ELECTIVE
BED NUMBERS
% CHANGE IN BED DAYS
FROM ADMISSIONS AVOIDANCE
AND EFFICIENCY
Starting Activity/Beds 2004/05 Base 40,151 766 Reduction to Long-Term Conditions Management from Base Activity
-2,940 -48 -6.2%
Thames Gateway Activity Growth (factored in)
9,407 171
Bed Reduction due to increased throughput efficiency
0 -74 -9.6%
Resultant Activity/Beds by 2016/17 815 -15.8%
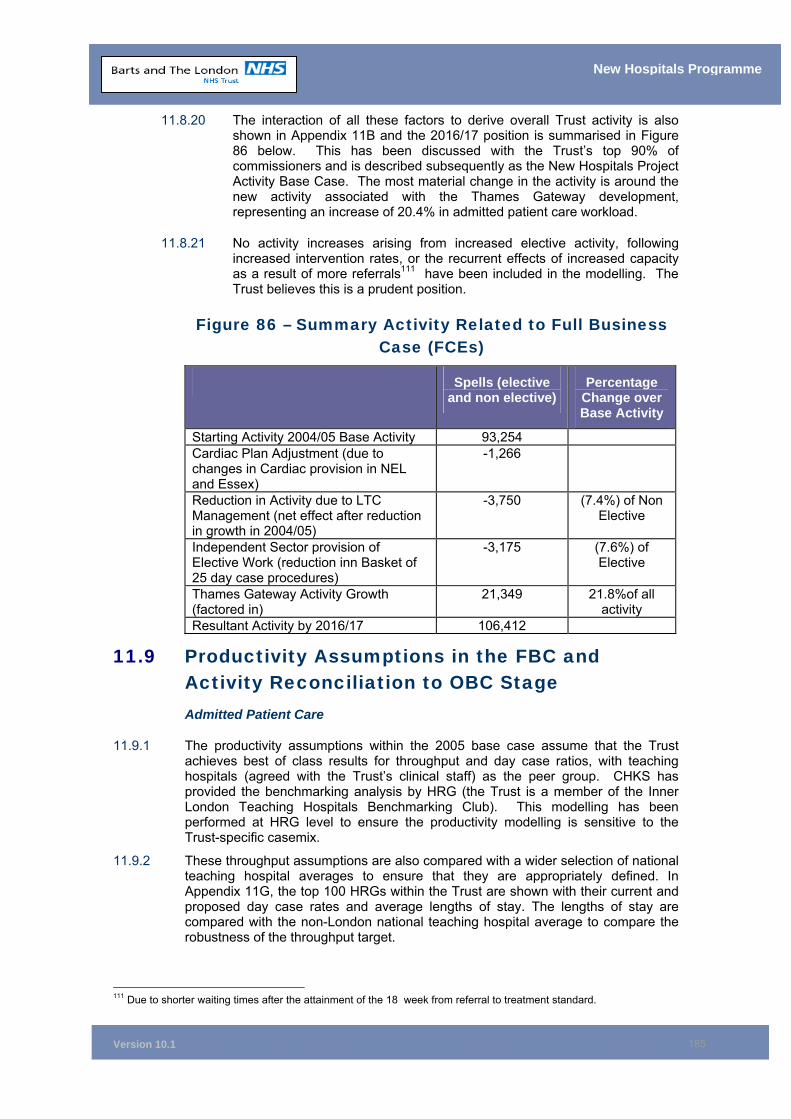
Version 10.1
185
New Hospitals Programme
11.8.20 The interaction of all these factors to derive overall Trust activity is also shown in Appendix 11B and the 2016/17 position is summarised in Figure 86 below. This has been discussed with the Trust’s top 90% of commissioners and is described subsequently as the New Hospitals Project Activity Base Case. The most material change in the activity is around the new activity associated with the Thames Gateway development, representing an increase of 20.4% in admitted patient care workload.
11.8.21 No activity increases arising from increased elective activity, following increased intervention rates, or the recurrent effects of increased capacity as a result of more referrals111 have been included in the modelling. The Trust believes this is a prudent position.
Figure 86 – Summary Activity Related to Full Business Case (FCEs)
Spells (elective and non elective)
Percentage Change over Base Activity
Starting Activity 2004/05 Base Activity 93,254 Cardiac Plan Adjustment (due to changes in Cardiac provision in NEL and Essex)
-1,266
Reduction in Activity due to LTC Management (net effect after reduction in growth in 2004/05)
-3,750 (7.4%) of Non Elective
Independent Sector provision of Elective Work (reduction inn Basket of 25 day case procedures)
-3,175 (7.6%) of Elective
Thames Gateway Activity Growth (factored in)
21,349 21.8%of all activity
Resultant Activity by 2016/17 106,412
11.9 Productivity Assumptions in the FBC and Activity Reconciliation to OBC Stage Admitted Patient Care
11.9.1 The productivity assumptions within the 2005 base case assume that the Trust achieves best of class results for throughput and day case ratios, with teaching hospitals (agreed with the Trust’s clinical staff) as the peer group. CHKS has provided the benchmarking analysis by HRG (the Trust is a member of the Inner London Teaching Hospitals Benchmarking Club). This modelling has been performed at HRG level to ensure the productivity modelling is sensitive to the Trust-specific casemix.
11.9.2 These throughput assumptions are also compared with a wider selection of national teaching hospital averages to ensure that they are appropriately defined. In Appendix 11G, the top 100 HRGs within the Trust are shown with their current and proposed day case rates and average lengths of stay. The lengths of stay are compared with the non-London national teaching hospital average to compare the robustness of the throughput target.
111 Due to shorter waiting times after the attainment of the 18 week from referral to treatment standard.
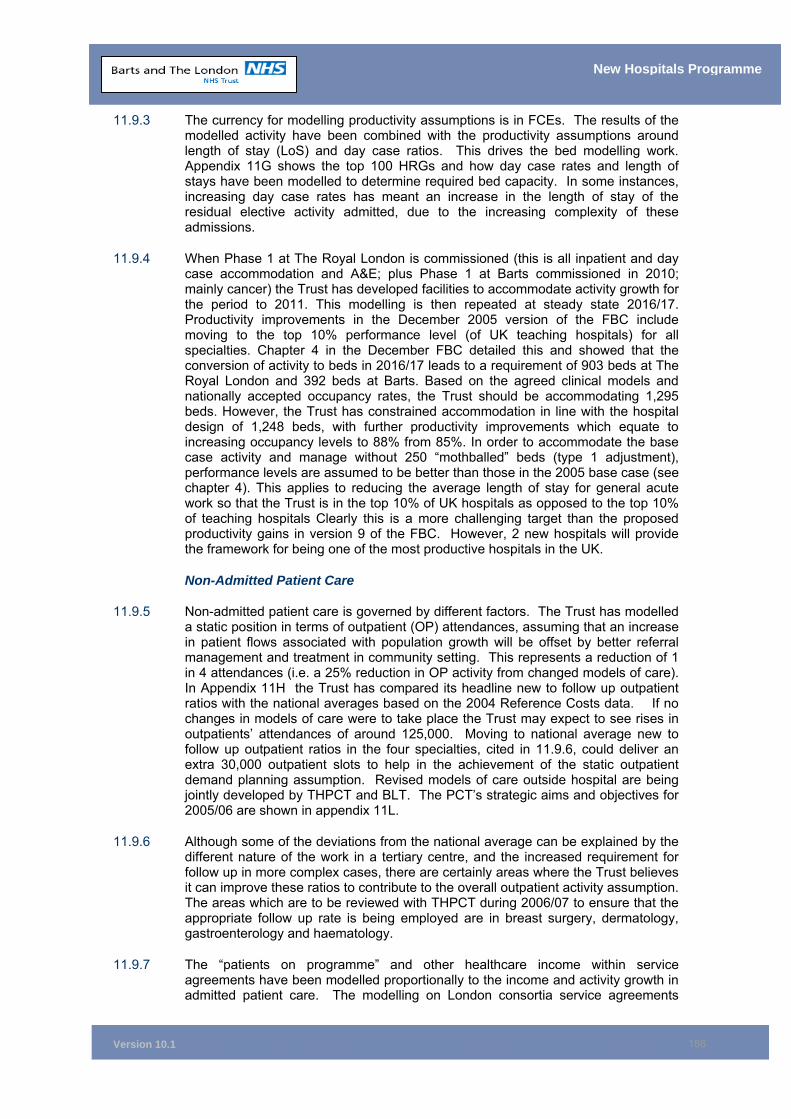
Version 10.1
186
New Hospitals Programme
11.9.3 The currency for modelling productivity assumptions is in FCEs. The results of the modelled activity have been combined with the productivity assumptions around length of stay (LoS) and day case ratios. This drives the bed modelling work. Appendix 11G shows the top 100 HRGs and how day case rates and length of stays have been modelled to determine required bed capacity. In some instances, increasing day case rates has meant an increase in the length of stay of the residual elective activity admitted, due to the increasing complexity of these admissions.
11.9.4 When Phase 1 at The Royal London is commissioned (this is all inpatient and day case accommodation and A&E; plus Phase 1 at Barts commissioned in 2010; mainly cancer) the Trust has developed facilities to accommodate activity growth for the period to 2011. This modelling is then repeated at steady state 2016/17. Productivity improvements in the December 2005 version of the FBC include moving to the top 10% performance level (of UK teaching hospitals) for all specialties. Chapter 4 in the December FBC detailed this and showed that the conversion of activity to beds in 2016/17 leads to a requirement of 903 beds at The Royal London and 392 beds at Barts. Based on the agreed clinical models and nationally accepted occupancy rates, the Trust should be accommodating 1,295 beds. However, the Trust has constrained accommodation in line with the hospital design of 1,248 beds, with further productivity improvements which equate to increasing occupancy levels to 88% from 85%. In order to accommodate the base case activity and manage without 250 “mothballed” beds (type 1 adjustment), performance levels are assumed to be better than those in the 2005 base case (see chapter 4). This applies to reducing the average length of stay for general acute work so that the Trust is in the top 10% of UK hospitals as opposed to the top 10% of teaching hospitals Clearly this is a more challenging target than the proposed productivity gains in version 9 of the FBC. However, 2 new hospitals will provide the framework for being one of the most productive hospitals in the UK.
Non-Admitted Patient Care
11.9.5 Non-admitted patient care is governed by different factors. The Trust has modelled a static position in terms of outpatient (OP) attendances, assuming that an increase in patient flows associated with population growth will be offset by better referral management and treatment in community setting. This represents a reduction of 1 in 4 attendances (i.e. a 25% reduction in OP activity from changed models of care). In Appendix 11H the Trust has compared its headline new to follow up outpatient ratios with the national averages based on the 2004 Reference Costs data. If no changes in models of care were to take place the Trust may expect to see rises in outpatients’ attendances of around 125,000. Moving to national average new to follow up outpatient ratios in the four specialties, cited in 11.9.6, could deliver an extra 30,000 outpatient slots to help in the achievement of the static outpatient demand planning assumption. Revised models of care outside hospital are being jointly developed by THPCT and BLT. The PCT’s strategic aims and objectives for 2005/06 are shown in appendix 11L.
11.9.6 Although some of the deviations from the national average can be explained by the different nature of the work in a tertiary centre, and the increased requirement for follow up in more complex cases, there are certainly areas where the Trust believes it can improve these ratios to contribute to the overall outpatient activity assumption. The areas which are to be reviewed with THPCT during 2006/07 to ensure that the appropriate follow up rate is being employed are in breast surgery, dermatology, gastroenterology and haematology.
11.9.7 The “patients on programme” and other healthcare income within service agreements have been modelled proportionally to the income and activity growth in admitted patient care. The modelling on London consortia service agreements

Version 10.1
187
New Hospitals Programme
assumes steady state for all areas apart from HIV, Haemophilia & HEMS, which show a modest increase of 3% in activity/income for the first three years of the analysis, and a 0.5% increase in years after that. This is in line with the increases in growth in Thames Gateway Scenario A1.
11.9.8 As a key provider of HIV/AIDS Services, if there was a radical change in the nature of the care provided for HIV/AIDS which required more bed based care, this steady state assumption does not adequately reflect that. The Trust has, however, reviewed the HIV/AIDS treatment and care pathway as part of the Clinical Development Plan, and it is not envisaged that the current model of care is likely to materially change. At the moment this income assumption is essentially neutral in the overall affordability in the model, as these income projections can be regarded as pass through costs associated with increased drug prescribing.
Reconciliation to Outline Business Case Position
11.9.9 In December 2005 the FBC proposed 1,248 beds compared with 1,200 beds in the OBC. This 4% increase reflected refinements in the Clinical Development Plan and increases in admitted patient care work since the OBC.
11.9.10 As detailed in the Addendum to the FBC, the Trust has reached financial close on the basis of 250 beds mothballed (192 beds out of 905 mothballed at RLH and 58 out of 343 mothballed at SBH) and hence a total revised bed complement of 998 in comparison with the OBC position.
11.10 Response of PCTs to the Activity Modelling 11.10.1 Tower Hamlets PCT has taken the lead in co-ordinating responses from North East
London PCTs to the activity modelling. They commissioned external consultants (Matrix) to review the model. Matrix, on behalf of NEL PCTs, developed three additional scenarios to test the robustness of the base model. The key variables of the scenarios are as follows:
■ Variation in demand; ■ Throughput efficiency; and ■ Alternative provision.
11.10.2 The result of the detailed activity analysis in income terms is included at Appendix 11D. The Trust, Tower Hamlets PCT, City & Hackney PCT, Newham PCT and the North East London specialised commissioning lead (on behalf of the four outer NEL PCTs), reviewed the impact of the scenarios in March 2005. The meeting concluded that the base activity model provides a prudent view of likely activity trajectories over the next 12 years, particularly given that the starting point is the 2003/04 outturn (i.e. 2003/04 represented at the time of the modelling the most comprehensive full year set of data available. For Tower Hamlets PCT the starting point was amended to 2004/05 (agreed with Tower Hamlets PCT in June 2005) due to the changes in non-elective activity).
11.10.3 Matrix issued their report in late March 2005. The report concludes that the Trust’s activity modelling process is robust and the baseline for the model is recognisable as local data (i.e. actual outturn data for 2003/04 and 2004/05). The report also concluded that scenario A fits closest to the national policy agenda and Local Delivery Plans (see Appendix 11F for sensitivity analysis - demand analysis).
11.10.4 As recognised in the Matrix report, a major risk for PCTs in the adoption of scenario A, is that they are based on 2003/04 outturn activity. At month 11, 2004/05 there was a 10% over performance in non-elective inpatient care within the Trust’s SLAs. This excluded the short stay admission ward (the Trust excluded Cambridge ward
Version 10.1
188
New Hospitals Programme
activity throughout 2004/05 as agreed with the East London & City Information Service (ELCIS). Moreover, the Trust has increased productivity for non-elective spells, by reducing the average length of stay to the best of class position of the inner London teaching hospitals.
11.10.5 After further discussion in April 2005, particularly with Tower Hamlets PCT, but also with others from the sector (via a quality assurance check on the activity work by Matrix Consulting (performed by the ELCIS), some changes to the base activity case was made. The base case reflected a 5% reduction in medical non-elective admissions of patients with Long Term Conditions by 2008, and inner North East London PCTs believed this over exaggerated the impact of changing models of care to the steady state year. The increase in non elective admissions in 2004/05 were thought to be atypically high in trend terms. Typically non elective workload growth has ran at 3% per annum for Tower Hamlets PCT. The PCT therefore believes that the revised activity model described in 11.10.8, to be sustainable after the planned investments in long term conditions management and community caseholding.
11.10.6 The base case scenario reflected the large reduction in non-elective admissions experienced in 2004/05. The total reduction in chronic conditions from the 2004/05 position would therefore have been 19.1% by the steady state year 2016/17. On discussion, this modelling work was not believed to be sufficiently sophisticated.
11.10.7 The discussions with PCTs highlighted two main areas for revision of the base case scenario activity model. The impact of the revisions are shown in Appendix 11B.
11.10.8 The first was a more appropriate assessment of non-elective care for all PCTs. Revised activity work was consequently undertaken which provides a more sophisticated model for chronic disease management and Long-Term Conditions. This equates to modelling a 0.5% per annum reduction in all admissions for the over 65s and a 0.5% reduction in key chronic specialties proposed by the PCTs. The impact of this revised scenario, described as scenario A by the PCTs, as opposed to scenario B (the Trust’s original base case), is an overall reduction in non-elective FCEs of 2,940 by the steady state year of 2016/17. Tower Hamlets PCT has a codified plan for the management of Long Term Conditions to deliver this scale of admission reductions. The PCT aims and objectives for 2005/06 are shown in Appendix 11L and strategic aim 4 refers. In particular the PCT has a strategic services development plan which includes primary care centre development throughout the PCT. Included in their supporting strategy are plans for the development of 4 stage one LIFT schemes and a 5th scheme at Strategic Outline Case stage (see Appendix 11L).
11.10.9 On reviewing this model, Tower Hamlets PCT started a separate process of reviewing the attainability of this figure in the context of their plans for management of Long-Term Conditions within primary care and other initiatives to avoid non-elective hospital admissions. The PCT came to the conclusion that a 26.9% reduction (the view from the Matrix report on the total reduction in non-elective bed days are the period 2005/06 to 2016/17) would not be deliverable.
11.10.10 The PCT has experienced year-on-year increases in non-elective admissions not attributable to population growth in recent years. This reflects the trend in deprived areas for year on year increase in emergency care. We agreed with THPCT to minimise this trend in the activity modelling with the proposed solution, therefore, to restate the non-elective activity baseline for Tower Hamlets PCT to include the actual level of non-elective care experienced in 2004/05. These spells have then been additionally abated under the same assumptions as the move from scenario B to scenario A. The overall effect of this change is to see a modest increase in non-

Version 10.1
189
New Hospitals Programme
elective admissions associated with the activity modelling (in summary overall, the Trust has deducted 15.8% of non-elective activity in the agreed adjusted model).
11.10.11 Over 80% of the Trust’s commissioners support the activity modelling assumptions and have written confirming this. Appendix 1B provides the details of the PCTs and the activity they commission and Appendix 0C provides their letters of support.
11.10.12 The second area where the Trust and Tower Hamlets PCT have revised the activity modelling work is around the view of care of the elderly (CoE), which is discussed separately below.
Care of the Elderly Beds
11.10.13 The OBC included the transfer of 99 beds from the Mile End Hospital (MEH) to the Royal London. MEH currently has 136 beds (18 for intermediate care, 96 for CoE and 22 continuing care beds).
11.10.14 The position agreed with Tower Hamlets is that an element of the MEH activity should now transfer into the New Hospitals Project, but at a lower level than previously assumed at OBC. There are currently 172 admissions to the MEH beds that are chronic/acute, which would be better handled in an acute context under the care of a medical consultant (this equates to 22 beds). Tower Hamlets PCT has provided a reconciliation of the change in the approach to the provision of care of the elderly activity from the OBC position to that which is currently proposed. Since the development of the model of care proposed in the OBC, the Trust and the PCT have continued to develop a shared view of intermediate and community care which has now resulted in a change from the OBC view of the appropriate location of the care currently provided in the Mile End beds. This is in line with the PCT’s strategy for older people. Overall it should be noted that the actual number of admissions are small and we would look to more proactively case manage these patients in the community; there is minimal risk that the strategy review will lead to a change to the base case.
11.10.15 The agreed position with Tower Hamlets PCT for the care of the elderly activity in the Trust for the steady state year equates to a total of 71 care of the elderly beds (22 transferring from Mile End and 49 acute Barts and the London beds).
Summary of PCT Income
11.10.16 Figure 87 provides a summary of the additional income from NEL and Essex PCTs over the period from 2006 to 2017. In the steady state year this shows a real increase of £40.5m (at 2006/07 prices) and a net contribution towards the unitary charge of £24 million (£16 million is 40% of £40.5 million) assuming an average rate of 40% for the marginal costs for undertaking the additional activity in 2016/17.
Figure 87 – Summary of Income 06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17
£m £m £m £m £m £m £m £m £m £m £m
Base Income 510 512 512 512 512 512 512 512 512 512 512Additional PCT
Income -9 13 1 -5 0 6 13 20 27 33 41
Other changes to income
11 -22 -38 -41 -39 -26 -21 -20 -20 -18 -19
Total Income 512 503 475 466 473 492 504 512 519 527 534
Version 10.1
190
New Hospitals Programme
11.10.17 The other changes to income figures include the impact of the 2006/7 PbR rebasing and the central levy deductions (see section 11.11). A further rebasing of the tariff is assumed to 2009/10 (£2 million negative impact increasing to £10m recurring negative impact for 2008/09, then reducing to £7.5 million for 2009/10). The other income changes also reflect the impact of patient choice (from Figure 84b) and the increase from other income (see section 11.11.3).
11.10.18 Although Payment by Results has inherent uncertainties, the Trust believes that it has constructed a well conceived model for admitted patient care income. Elsewhere, for areas where Payments by Results may be more difficult to implement, in terms of different approaches to counting more specialised areas of activity (i.e. for the 40% of our patient care services not covered by PbR in 2006/07), the Trust has assumed there will be no change in Trust income purely associated with the development of the Payment by Results policy or the introduction on HRG grouper version 4. The Trust has moreover not offset the losses from the PbR rebasing of 2006/07 until 2011/12 (then only by a reduction of £5 million to 2006/07 loss), even though our costs outside of national tariffs are below 2004/05 average reference costs (see Appendix 11D).
11.10.19 Figure 87 excludes the net impact of transferring care of the elderly activity from MEH (172 episodes). This would equate to £0.5 million extra (net gain on marginal costs) to support the unitary charge and hence represents part of our handling strategy to offset the more pessimistic scenarios (see Appendix 11F for sensitivity analysis).
11.10.20 Currently due to capacity constraints with level 3, critical care (ITU) beds at the Royal London, when our level 3 beds at RLH are full, patients in other NEL hospitals that should be transferred to RLH are instead transferred to other hospitals in London. PCTs will therefore see a reduction in their service agreements with other hospitals for critical care transfers when the new RLH critical care facility opens (within phase 1 of RLH). Therefore, in terms of affordability from a PCT perspective, all NEL PCTs will be able to reduce their SLAs with other providers for out of area intensive care transfers as the new hospitals will have sufficient capacity to avoid outflows.
11.11 Other Income Income Assumptions from Central Levies
11.11.1 Levy income (Service Increment for Teaching (SIFT), Dental SIFT, NMET and R&D) is paid by the DH and may be subject to rebasing (i.e. transfers to, or from, service income streams or uplifts that are different from the PbR tariffs). In line with the Addendum to the FBC the base case for the affordability analysis assumes a £12m loss of income from central levies (R&D and SIFT allocation). In particular, as detailed in 11.4.8, the Trust is at risk from a reduction in R&D income with the implementation of Best Research for Best Health.
Other income
11.11.2 In terms of other areas for income growth, Road Traffic Act (RTA) income is planned to increase by £320k (10% increase to £1.7m in total) in line with the 10% increase in emergency admissions over the interim period (over the past 3 years the trend for Road traffic act income has been in line with emergency admissions from A&E). This planned increase is net of the 6% bad debt provision. The trust’s other income plan also includes an additional £480k for contracts with the independent sector for the use of the trust’s facilities for the independent sector to undertake paying patient activity at weekends. This would be in the form of a
Version 10.1
191
New Hospitals Programme
contract for the provision of services. The Trust has checked that this is allowable by Monitor under the Foundation Trust regime and the Trust has already been approached by an interested company that is keen to enter into an agreement at SBH for Saturday lists.
11.12 Expenditure 11.12.1 Figure 88 provides a summary of the Trust’s expenditure basis over the next 12
years at 2006/07 price base, excluding the unitary charge. The relevant costs associated with the FM service within the contract are removed from the expenditure base, in line with start up of our partner’s FM services. It should be noted that the PFI FM costs exclude Agenda for Change uplifts, as these are to be separately agreed. The Trust has a reserve based on the estimated AfC costs for the staff transferring.
11.12.2 The changes to capital charges are detailed in the accounting treatment chapter of the FBC (Chapter 10). In summary, the major changes are as follows:
■ Movement to deferred assets (£8,741,000 at steady state); ■ There is an addition to capital charges of £500,000 as a result of the type one
adjustments, as the non-refurbished buildings in phases 2 and 3 remain on the balance sheet;
■ Capitalised element of the unitary charge, i.e. build up of residual interest (£8,662,000 at steady state). With the type one adjustments and the change in MES funding there is a £200,000 reduction to the capitalised element of the UC (residual interest)
■ The capital charge element for the Trust supplied equipment service OBC starts from 2008 and builds to a total of £4m by 2011/12. This is based on a prudent view of depreciation (in terms of the number of years for asset lives) and the current 3.5% return on capital. Although the Foundation Trust regime uses 4.5 to 5% as the assumed rate of borrowing by 2011 the national tariffs will reflect the actual costs of all FTs and hence any increase in the cost of capital would be offset by an increase in income. Appendix 13B provides a detailed breakdown of capital charges from the non MES OBC.
11.12.3 Impairments (of £26.5 million in 2005/06) are also detailed in the accounting treatment chapter (see section 10.5) and are assumed to be funded from the NHS Bank (90%). Of the remaining £2.65 million, £1.9 million is funded by the NEL risk pool in 2006/07. The pressure of £2.65 million is included in the Trust’s 2005/2006 annual accounts.
11.12.4 The marginal costs for the additional activity are over 80% for the period 2006 to 2009. This level of cost recognises the stepped costs associated with achieving the 18 week referral to treatment target by 31 December 2008. Marginal costs from 2010/11 are assumed to gradually reduce to be at a rate of 50% by steady state. The marginal costs include the flexed costs within the FM service for activity changes, e.g. linen and laundry. This 50% marginal cost rate is more prudent than the experience of the Trust in dealing with additional clinical workload in the last five years where the rate has been 4%. It has been further tested and collaborated by review of direct and indirect costs in the Trust’s costing model.
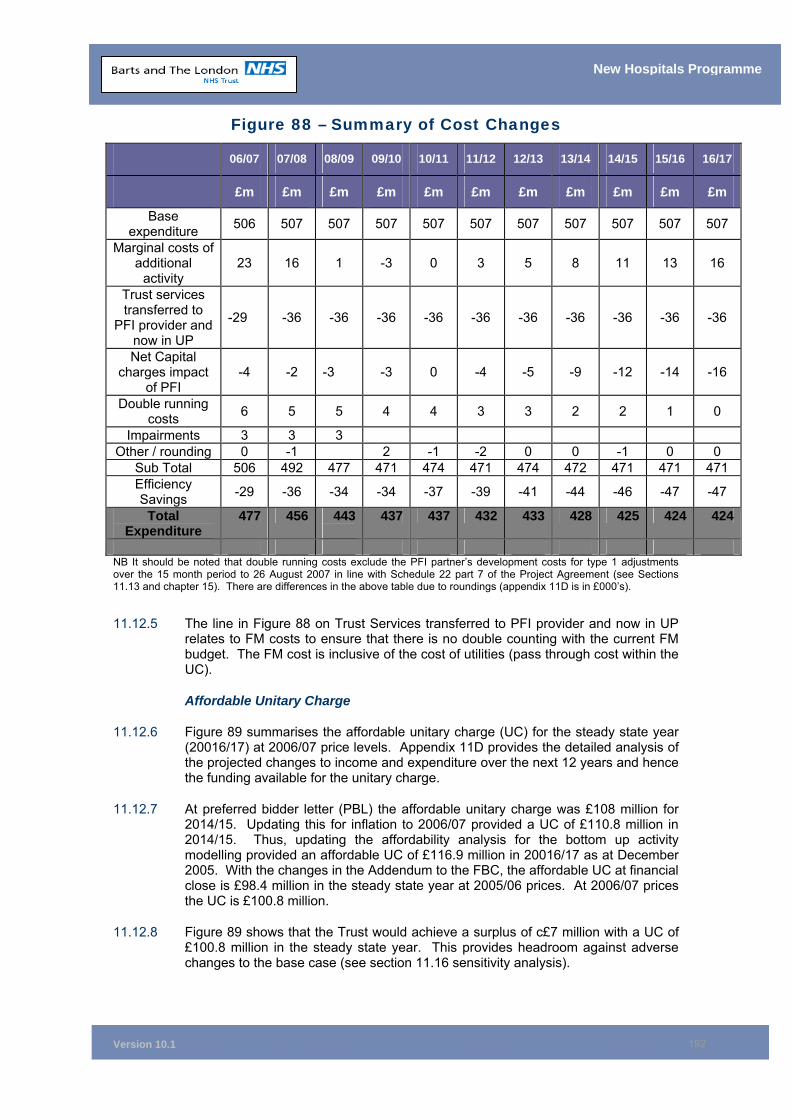
Version 10.1
192
New Hospitals Programme
Figure 88 – Summary of Cost Changes
06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17
£m £m £m £m £m £m £m £m £m £m £m
Base expenditure 506 507 507 507 507 507 507 507 507 507 507
Marginal costs of additional
activity 23 16 1 -3 0 3 5 8 11 13 16
Trust services transferred to
PFI provider and now in UP
-29 -36 -36 -36 -36 -36 -36 -36 -36 -36 -36
Net Capital charges impact
of PFI -4 -2 -3 -3 0 -4 -5 -9 -12 -14 -16
Double running costs 6 5 5 4 4 3 3 2 2 1 0
Impairments 3 3 3 Other / rounding 0 -1 2 -1 -2 0 0 -1 0 0
Sub Total 506 492 477 471 474 471 474 472 471 471 471 Efficiency Savings -29 -36 -34 -34 -37 -39 -41 -44 -46 -47 -47
Total Expenditure
477 456 443 437 437 432 433 428 425 424 424
NB It should be noted that double running costs exclude the PFI partner’s development costs for type 1 adjustments over the 15 month period to 26 August 2007 in line with Schedule 22 part 7 of the Project Agreement (see Sections 11.13 and chapter 15). There are differences in the above table due to roundings (appendix 11D is in £000’s).
11.12.5 The line in Figure 88 on Trust Services transferred to PFI provider and now in UP relates to FM costs to ensure that there is no double counting with the current FM budget. The FM cost is inclusive of the cost of utilities (pass through cost within the UC).
Affordable Unitary Charge
11.12.6 Figure 89 summarises the affordable unitary charge (UC) for the steady state year (20016/17) at 2006/07 price levels. Appendix 11D provides the detailed analysis of the projected changes to income and expenditure over the next 12 years and hence the funding available for the unitary charge.
11.12.7 At preferred bidder letter (PBL) the affordable unitary charge was £108 million for 2014/15. Updating this for inflation to 2006/07 provided a UC of £110.8 million in 2014/15. Thus, updating the affordability analysis for the bottom up activity modelling provided an affordable UC of £116.9 million in 20016/17 as at December 2005. With the changes in the Addendum to the FBC, the affordable UC at financial close is £98.4 million in the steady state year at 2005/06 prices. At 2006/07 prices the UC is £100.8 million.
11.12.8 Figure 89 shows that the Trust would achieve a surplus of c£7 million with a UC of £100.8 million in the steady state year. This provides headroom against adverse changes to the base case (see section 11.16 sensitivity analysis).
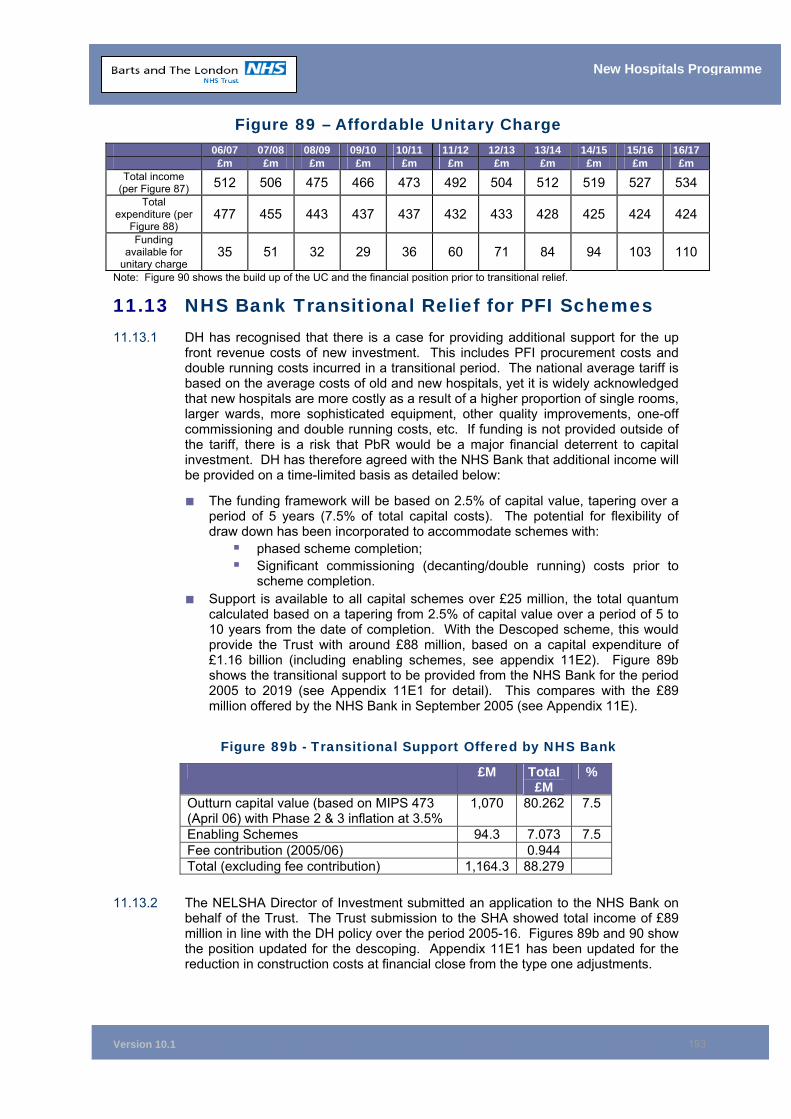
Version 10.1
193
New Hospitals Programme
Figure 89 – Affordable Unitary Charge 06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17 £m £m £m £m £m £m £m £m £m £m £m
Total income (per Figure 87) 512 506 475 466 473 492 504 512 519 527 534
Total expenditure (per
Figure 88) 477 455 443 437 437 432 433 428 425 424 424
Funding available for
unitary charge 35 51 32 29 36 60 71 84 94 103 110
Note: Figure 90 shows the build up of the UC and the financial position prior to transitional relief.
11.13 NHS Bank Transitional Relief for PFI Schemes 11.13.1 DH has recognised that there is a case for providing additional support for the up
front revenue costs of new investment. This includes PFI procurement costs and double running costs incurred in a transitional period. The national average tariff is based on the average costs of old and new hospitals, yet it is widely acknowledged that new hospitals are more costly as a result of a higher proportion of single rooms, larger wards, more sophisticated equipment, other quality improvements, one-off commissioning and double running costs, etc. If funding is not provided outside of the tariff, there is a risk that PbR would be a major financial deterrent to capital investment. DH has therefore agreed with the NHS Bank that additional income will be provided on a time-limited basis as detailed below:
■ The funding framework will be based on 2.5% of capital value, tapering over a period of 5 years (7.5% of total capital costs). The potential for flexibility of draw down has been incorporated to accommodate schemes with:
phased scheme completion; Significant commissioning (decanting/double running) costs prior to
scheme completion. ■ Support is available to all capital schemes over £25 million, the total quantum
calculated based on a tapering from 2.5% of capital value over a period of 5 to 10 years from the date of completion. With the Descoped scheme, this would provide the Trust with around £88 million, based on a capital expenditure of £1.16 billion (including enabling schemes, see appendix 11E2). Figure 89b shows the transitional support to be provided from the NHS Bank for the period 2005 to 2019 (see Appendix 11E1 for detail). This compares with the £89 million offered by the NHS Bank in September 2005 (see Appendix 11E).
Figure 89b - Transitional Support Offered by NHS Bank
11.13.2 The NELSHA Director of Investment submitted an application to the NHS Bank on behalf of the Trust. The Trust submission to the SHA showed total income of £89 million in line with the DH policy over the period 2005-16. Figures 89b and 90 show the position updated for the descoping. Appendix 11E1 has been updated for the reduction in construction costs at financial close from the type one adjustments.
£M Total £M
%
Outturn capital value (based on MIPS 473 (April 06) with Phase 2 & 3 inflation at 3.5%
1,070 80.262 7.5
Enabling Schemes 94.3 7.073 7.5 Fee contribution (2005/06) 0.944 Total (excluding fee contribution) 1,164.3 88.279
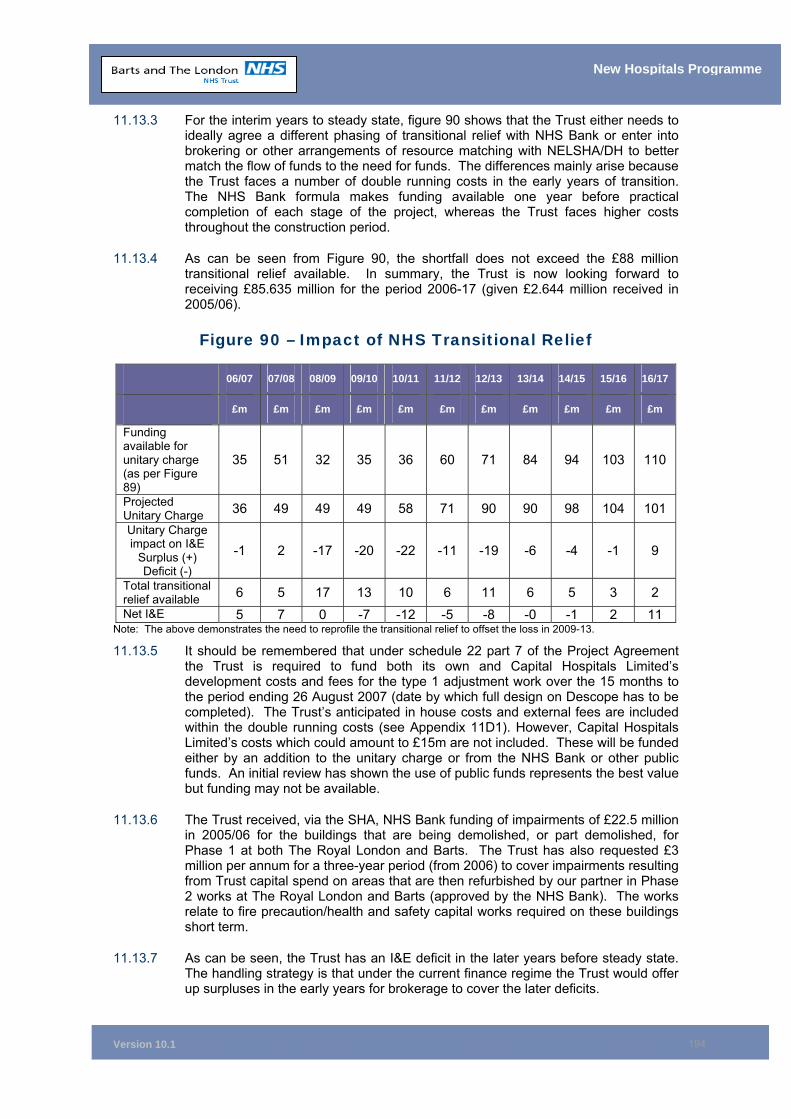
Version 10.1
194
New Hospitals Programme
11.13.3 For the interim years to steady state, figure 90 shows that the Trust either needs to ideally agree a different phasing of transitional relief with NHS Bank or enter into brokering or other arrangements of resource matching with NELSHA/DH to better match the flow of funds to the need for funds. The differences mainly arise because the Trust faces a number of double running costs in the early years of transition. The NHS Bank formula makes funding available one year before practical completion of each stage of the project, whereas the Trust faces higher costs throughout the construction period.
11.13.4 As can be seen from Figure 90, the shortfall does not exceed the £88 million transitional relief available. In summary, the Trust is now looking forward to receiving £85.635 million for the period 2006-17 (given £2.644 million received in 2005/06).
Figure 90 – Impact of NHS Transitional Relief
Note: The above demonstrates the need to reprofile the transitional relief to offset the loss in 2009-13.
11.13.5 It should be remembered that under schedule 22 part 7 of the Project Agreement the Trust is required to fund both its own and Capital Hospitals Limited’s development costs and fees for the type 1 adjustment work over the 15 months to the period ending 26 August 2007 (date by which full design on Descope has to be completed). The Trust’s anticipated in house costs and external fees are included within the double running costs (see Appendix 11D1). However, Capital Hospitals Limited’s costs which could amount to £15m are not included. These will be funded either by an addition to the unitary charge or from the NHS Bank or other public funds. An initial review has shown the use of public funds represents the best value but funding may not be available.
11.13.6 The Trust received, via the SHA, NHS Bank funding of impairments of £22.5 million in 2005/06 for the buildings that are being demolished, or part demolished, for Phase 1 at both The Royal London and Barts. The Trust has also requested £3 million per annum for a three-year period (from 2006) to cover impairments resulting from Trust capital spend on areas that are then refurbished by our partner in Phase 2 works at The Royal London and Barts (approved by the NHS Bank). The works relate to fire precaution/health and safety capital works required on these buildings short term.
11.13.7 As can be seen, the Trust has an I&E deficit in the later years before steady state. The handling strategy is that under the current finance regime the Trust would offer up surpluses in the early years for brokerage to cover the later deficits.
06/07 07/08 08/09 09/10 10/11 11/12 12/13 13/14 14/15 15/16 16/17
£m £m £m £m £m £m £m £m £m £m £m
Funding available for unitary charge (as per Figure 89)
35 51 32 35 36 60 71 84 94 103 110
Projected Unitary Charge 36 49 49 49 58 71 90 90 98 104 101 Unitary Charge impact on I&E
Surplus (+) Deficit (-)
-1 2 -17 -20 -22 -11 -19 -6 -4 -1 9
Total transitional relief available 6 5 17 13 10 6 11 6 5 3 2 Net I&E 5 7 0 -7 -12 -5 -8 -0 -1 2 11
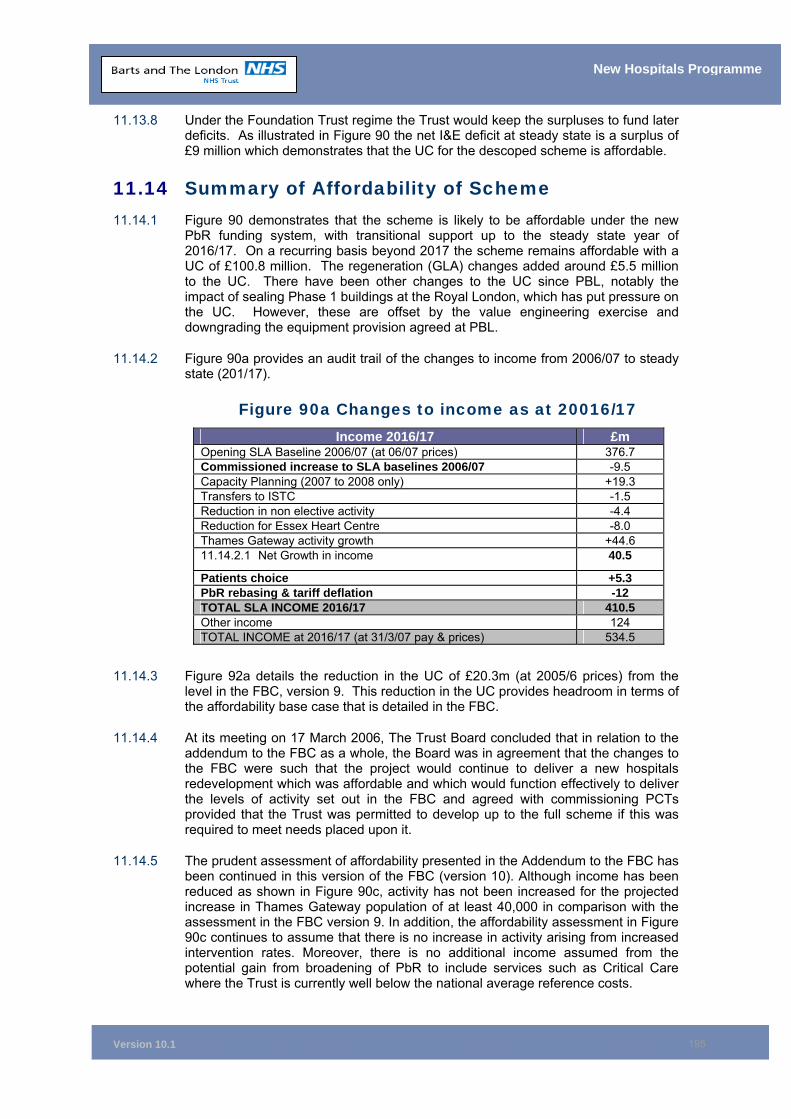
Version 10.1
195
New Hospitals Programme
11.13.8 Under the Foundation Trust regime the Trust would keep the surpluses to fund later deficits. As illustrated in Figure 90 the net I&E deficit at steady state is a surplus of £9 million which demonstrates that the UC for the descoped scheme is affordable.
11.14 Summary of Affordability of Scheme 11.14.1 Figure 90 demonstrates that the scheme is likely to be affordable under the new
PbR funding system, with transitional support up to the steady state year of 2016/17. On a recurring basis beyond 2017 the scheme remains affordable with a UC of £100.8 million. The regeneration (GLA) changes added around £5.5 million to the UC. There have been other changes to the UC since PBL, notably the impact of sealing Phase 1 buildings at the Royal London, which has put pressure on the UC. However, these are offset by the value engineering exercise and downgrading the equipment provision agreed at PBL.
11.14.2 Figure 90a provides an audit trail of the changes to income from 2006/07 to steady state (201/17).
Figure 90a Changes to income as at 20016/17 Income 2016/17 £m
Opening SLA Baseline 2006/07 (at 06/07 prices) 376.7 Commissioned increase to SLA baselines 2006/07 -9.5 Capacity Planning (2007 to 2008 only) +19.3 Transfers to ISTC -1.5 Reduction in non elective activity -4.4 Reduction for Essex Heart Centre -8.0 Thames Gateway activity growth +44.6 11.14.2.1 Net Growth in income 40.5
Patients choice +5.3 PbR rebasing & tariff deflation -12 TOTAL SLA INCOME 2016/17 410.5 Other income 124 TOTAL INCOME at 2016/17 (at 31/3/07 pay & prices) 534.5
11.14.3 Figure 92a details the reduction in the UC of £20.3m (at 2005/6 prices) from the level in the FBC, version 9. This reduction in the UC provides headroom in terms of the affordability base case that is detailed in the FBC.
11.14.4 At its meeting on 17 March 2006, The Trust Board concluded that in relation to the addendum to the FBC as a whole, the Board was in agreement that the changes to the FBC were such that the project would continue to deliver a new hospitals redevelopment which was affordable and which would function effectively to deliver the levels of activity set out in the FBC and agreed with commissioning PCTs provided that the Trust was permitted to develop up to the full scheme if this was required to meet needs placed upon it.
11.14.5 The prudent assessment of affordability presented in the Addendum to the FBC has been continued in this version of the FBC (version 10). Although income has been reduced as shown in Figure 90c, activity has not been increased for the projected increase in Thames Gateway population of at least 40,000 in comparison with the assessment in the FBC version 9. In addition, the affordability assessment in Figure 90c continues to assume that there is no increase in activity arising from increased intervention rates. Moreover, there is no additional income assumed from the potential gain from broadening of PbR to include services such as Critical Care where the Trust is currently well below the national average reference costs.
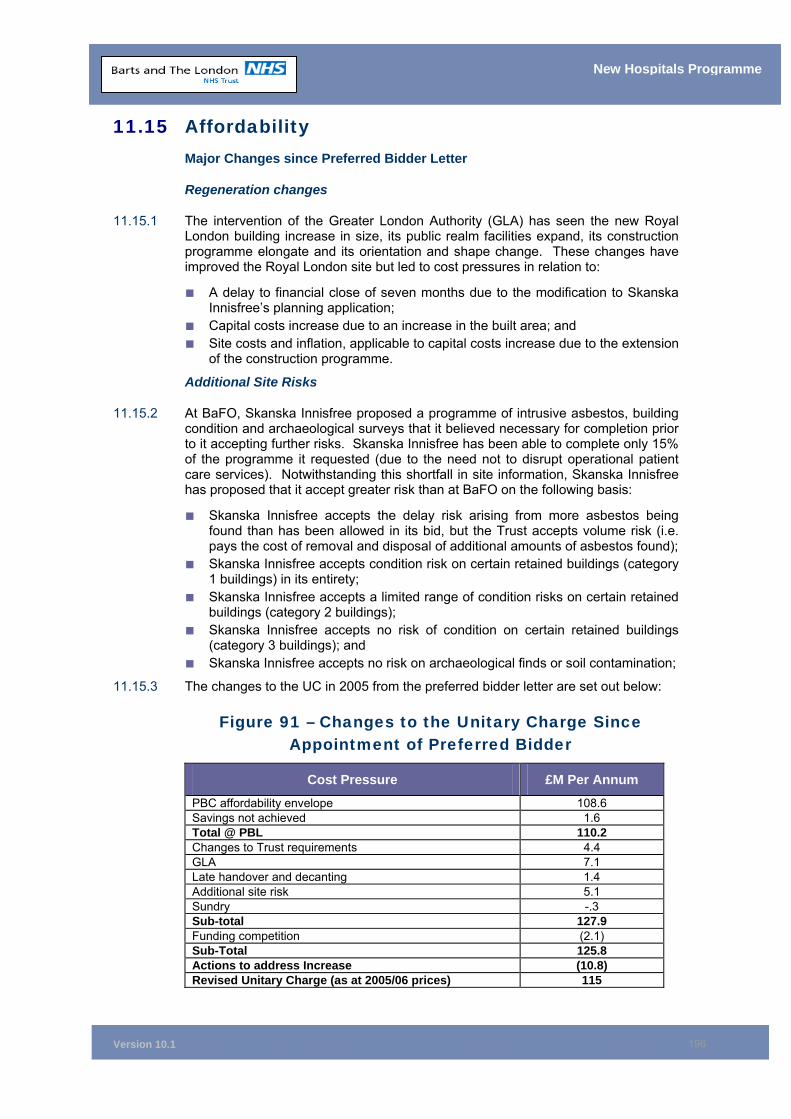
Version 10.1
196
New Hospitals Programme
11.15 Affordability Major Changes since Preferred Bidder Letter
Regeneration changes
11.15.1 The intervention of the Greater London Authority (GLA) has seen the new Royal London building increase in size, its public realm facilities expand, its construction programme elongate and its orientation and shape change. These changes have improved the Royal London site but led to cost pressures in relation to:
■ A delay to financial close of seven months due to the modification to Skanska Innisfree’s planning application;
■ Capital costs increase due to an increase in the built area; and ■ Site costs and inflation, applicable to capital costs increase due to the extension
of the construction programme.
Additional Site Risks
11.15.2 At BaFO, Skanska Innisfree proposed a programme of intrusive asbestos, building condition and archaeological surveys that it believed necessary for completion prior to it accepting further risks. Skanska Innisfree has been able to complete only 15% of the programme it requested (due to the need not to disrupt operational patient care services). Notwithstanding this shortfall in site information, Skanska Innisfree has proposed that it accept greater risk than at BaFO on the following basis:
■ Skanska Innisfree accepts the delay risk arising from more asbestos being found than has been allowed in its bid, but the Trust accepts volume risk (i.e. pays the cost of removal and disposal of additional amounts of asbestos found);
■ Skanska Innisfree accepts condition risk on certain retained buildings (category 1 buildings) in its entirety;
■ Skanska Innisfree accepts a limited range of condition risks on certain retained buildings (category 2 buildings);
■ Skanska Innisfree accepts no risk of condition on certain retained buildings (category 3 buildings); and
■ Skanska Innisfree accepts no risk on archaeological finds or soil contamination;
11.15.3 The changes to the UC in 2005 from the preferred bidder letter are set out below:
Figure 91 – Changes to the Unitary Charge Since Appointment of Preferred Bidder
Cost Pressure £M Per Annum PBC affordability envelope 108.6 Savings not achieved 1.6 Total @ PBL 110.2 Changes to Trust requirements 4.4 GLA 7.1 Late handover and decanting 1.4 Additional site risk 5.1 Sundry -.3 Sub-total 127.9 Funding competition (2.1) Sub-Total 125.8 Actions to address Increase (10.8) Revised Unitary Charge (as at 2005/06 prices) 115
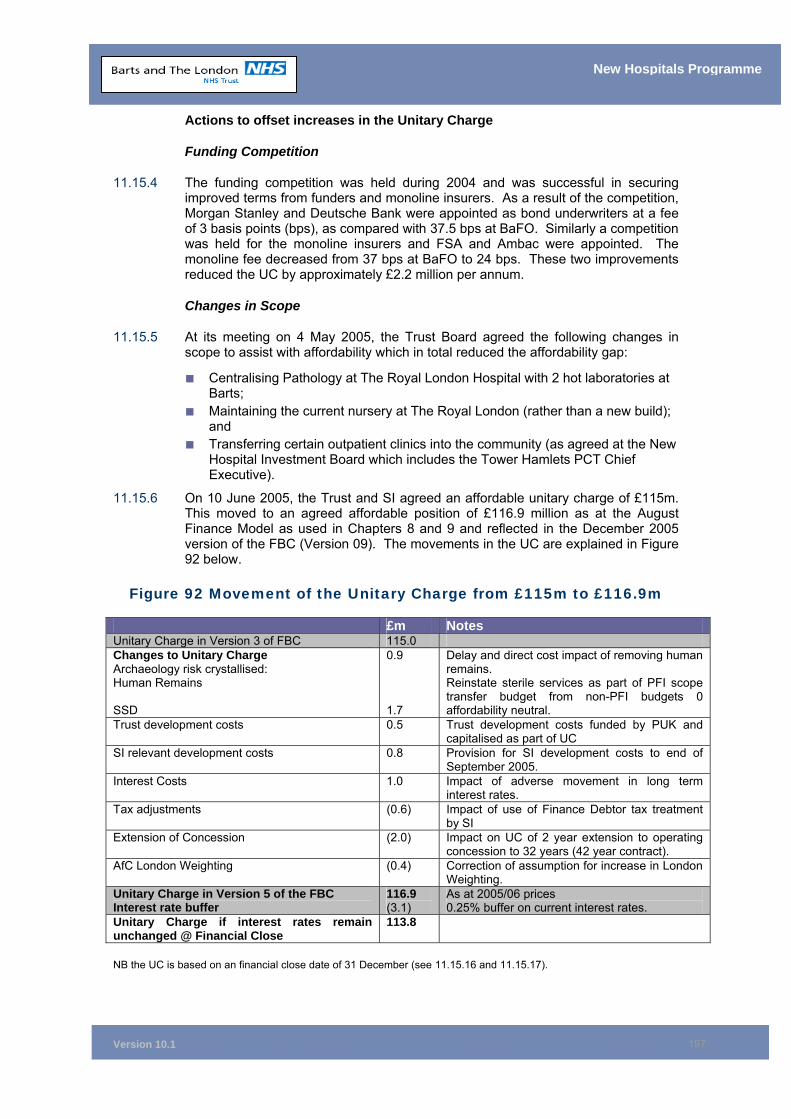
Version 10.1
197
New Hospitals Programme
Actions to offset increases in the Unitary Charge
Funding Competition
11.15.4 The funding competition was held during 2004 and was successful in securing improved terms from funders and monoline insurers. As a result of the competition, Morgan Stanley and Deutsche Bank were appointed as bond underwriters at a fee of 3 basis points (bps), as compared with 37.5 bps at BaFO. Similarly a competition was held for the monoline insurers and FSA and Ambac were appointed. The monoline fee decreased from 37 bps at BaFO to 24 bps. These two improvements reduced the UC by approximately £2.2 million per annum.
Changes in Scope
11.15.5 At its meeting on 4 May 2005, the Trust Board agreed the following changes in scope to assist with affordability which in total reduced the affordability gap:
■ Centralising Pathology at The Royal London Hospital with 2 hot laboratories at Barts;
■ Maintaining the current nursery at The Royal London (rather than a new build); and
■ Transferring certain outpatient clinics into the community (as agreed at the New Hospital Investment Board which includes the Tower Hamlets PCT Chief Executive).
11.15.6 On 10 June 2005, the Trust and SI agreed an affordable unitary charge of £115m. This moved to an agreed affordable position of £116.9 million as at the August Finance Model as used in Chapters 8 and 9 and reflected in the December 2005 version of the FBC (Version 09). The movements in the UC are explained in Figure 92 below.
Figure 92 Movement of the Unitary Charge from £115m to £116.9m
NB the UC is based on an financial close date of 31 December (see 11.15.16 and 11.15.17).
£m Notes Unitary Charge in Version 3 of FBC 115.0 Changes to Unitary Charge Archaeology risk crystallised: Human Remains SSD
0.9 1.7
Delay and direct cost impact of removing human remains. Reinstate sterile services as part of PFI scope transfer budget from non-PFI budgets 0 affordability neutral.
Trust development costs 0.5 Trust development costs funded by PUK and capitalised as part of UC
SI relevant development costs 0.8 Provision for SI development costs to end of September 2005.
Interest Costs 1.0 Impact of adverse movement in long term interest rates.
Tax adjustments (0.6) Impact of use of Finance Debtor tax treatment by SI
Extension of Concession (2.0) Impact on UC of 2 year extension to operating concession to 32 years (42 year contract).
AfC London Weighting (0.4) Correction of assumption for increase in London Weighting.
Unitary Charge in Version 5 of the FBC Interest rate buffer
116.9 (3.1)
As at 2005/06 prices 0.25% buffer on current interest rates.
Unitary Charge if interest rates remain unchanged @ Financial Close
113.8
Version 10.1
198
New Hospitals Programme
11.15.7 Changes to the December 2006 business case (version 9) have been made in response to the concerns expressed by DH and HM Treasury about affordability, and the consequent review of capital schemes announced in the NHS Operating Framework 2006/07. The financial environment in which the NHS operates has changed significantly since the Trust assessed affordability in September 2005, in particular further information on:
■ Lower levels of funding growth to the NHS from 2008 onwards; ■ Current financial overspend of the NHS, including difficulties being experienced
by hospitals with existing PFI schemes in operation; ■ The recent White Paper on care outside of hospitals; and ■ Financial Regime (Payment by Results 2006/07) and policy (Best Research for
Best Health, etc.) changes.
11.15.8 Although Barts and The London NHS Trust has attempted to address some of these issues through a further £15m workforce cost reduction programme (equivalent to 0.3% p.a. of turnover over the 10 years to steady state), there are further potential downside risks over the next 10 years, and these are best addressed by achieving a reduction in the unitary payment and having greater flexibility in the final scale of buildings and physical capacity.
11.15.9 Therefore, as detailed in the Addendum to the FBC, in February 2006, the Trust agreed four types of adjustments to version 9 of the FBC:
Type 1 adjustments involve the Trust modifying the PFI scheme in an innovative way. The Trust understands that the Department of Health has endorsed an approach whereby the Trust’s output requirements and SI’s proposals remain as set out in the current Project Agreement but that the funding provided under this contract is varied to allow flexibility in the extent to which these proposals are fully implemented within secured planning approvals. The two elements of SI’s proposals described below, mothballing and refurbishment in Phases 2 and 3 are included within the amended Variation Schedule (Schedule 22, part 7) so that there is no contractual obligation on SI to carry out the works unless instructed to do so by the Trust. The works will only be implemented on the basis that they are required to meet planning approvals; health need; and are affordable to the Trust and subject to Departmental and HMT approval. The schedule includes a capital figure to carry out the works and the price to go back on the UC for the services (Appendix 1 to Schedule 22, part 7). The parties are committed to ensuring that the consequential amendments will be made to the Trust’s Construction Requirements and relevant specifications within the Project Agreement.
Under this arrangement, the Department of Health expects the Trust to keep its requirements under review during the long construction period. If activity and associated income arise as projected, then additional funds will be raised. The two elements subject to specific review in this context are:
■ Mothballing two floors at The Royal London (192 beds out of 905 bed
complement) and one floor at St Bartholomew’s (58 beds out of 343 bed complement) of newly built space.
■ Not proceeding with certain refurbishments projected to get under way in Phase 2 and Phase 3.
Type 2 adjustments involved the following:
Version 10.1
199
New Hospitals Programme
■ Changing of funding assumptions, reduction of the buffer - the Trust preserved a 25bps interest rate buffer throughout the procurement. Given the closeness to financial close and following discussions with the Department of Health and SI, the buffer was reduced to 5bps. In addition the updated position on the European Investment Bank funding was 9 bps lower than in version 9 of the FBC.
■ Following due diligence, the reduction in the Unitary Charge associated with the
extension of the operating concession from 32 to 35 years was calculated to be £1.6m a year, compared with an initial estimate of £3m. This change reflected the erroneous omission by SI of the increase in lifecycle costs from extending the operating concession period. The Trust Board at its meeting on 17 March 2006 agreed that it could not accept an extension of the concession period to 35 years which generated a saving of only £1.6 million. The Board requested that the Director of Finance explore with SI alternative options in relation to the concession period, including a shorter extension or no extension from the previous 32 years. Following due diligence by the Trust’s technical advisers, the Trust asked SI to either revert to a 32 year operating concession and lose the £1.6m net benefit or SI to propose a best and final offer on the 35 year deal that the Trust could rapidly consider. SI confirmed that the position remains their final offer with regard to extending the concession period and so the Trust reverted to accepting a contract over 42 years with a 32 year operating concession period.
Type 3 adjustments reflect capital contributions to the costs of the scheme. They fall into two categories, namely medical equipment and enabling works:
■ Medical equipment – The St Bartholomew and The Royal London Charitable Foundation has agreed in principle that it will donate equipment covering the capital cost consequences of the initial tranche of medical equipment (i.e. up to the point when the first equipment refresh requirements arises) and the Trust’s advisers are looking at the ways in which the relevant contracts require amendment.
■ Enabling works - SI has undertaken a series of accelerated, enabling works which, together, total approximately £60m in capital value. The ODPM Thames Gateway office has contributed £4m towards these costs.
Type 4 adjustments represent minor modifications to the Project Agreement, notably the removal from the UC of the 0.7% construction cost inflation buffer for post-Phase 1 works. The UC will now fund construction cost inflation at an annual rate of 3.5% per annum. In addition there is a reduction in the interim service costs which had assumed an over-prudent level of double-running costs in the period prior to steady state.
11.15.10 Figure 92b shows the impact of each of the changes required to achieve a target reduction to the UC of £20m from the level at version 9 of the FBC (excluding movements in interest rates from February 2006 to financial close).
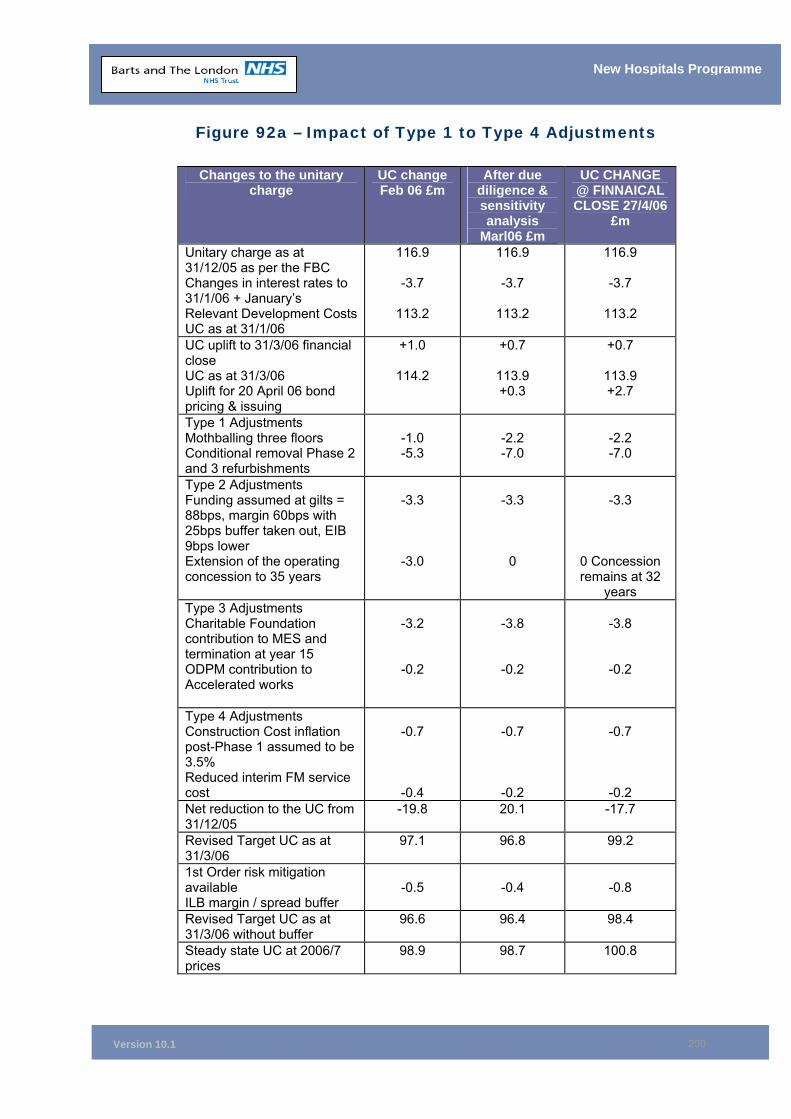
Version 10.1
200
New Hospitals Programme
Figure 92a – Impact of Type 1 to Type 4 Adjustments
Changes to the unitary charge
UC change Feb 06 £m
After due diligence & sensitivity analysis
Marl06 £m
UC CHANGE @ FINNAICAL CLOSE 27/4/06
£m
Unitary charge as at 31/12/05 as per the FBC Changes in interest rates to 31/1/06 + January’s Relevant Development CostsUC as at 31/1/06
116.9
-3.7
113.2
116.9
-3.7
113.2
116.9
-3.7
113.2
UC uplift to 31/3/06 financial close UC as at 31/3/06 Uplift for 20 April 06 bond pricing & issuing
+1.0
114.2
+0.7
113.9 +0.3
+0.7
113.9 +2.7
Type 1 Adjustments Mothballing three floors Conditional removal Phase 2 and 3 refurbishments
-1.0 -5.3
-2.2 -7.0
-2.2 -7.0
Type 2 Adjustments Funding assumed at gilts = 88bps, margin 60bps with 25bps buffer taken out, EIB 9bps lower Extension of the operating concession to 35 years
-3.3
-3.0
-3.3
0
-3.3
0 Concession remains at 32
years Type 3 Adjustments Charitable Foundation contribution to MES and termination at year 15 ODPM contribution to Accelerated works
-3.2
-0.2
-3.8
-0.2
-3.8
-0.2
Type 4 Adjustments Construction Cost inflation post-Phase 1 assumed to be 3.5% Reduced interim FM service cost
-0.7
-0.4
-0.7
-0.2
-0.7
-0.2 Net reduction to the UC from 31/12/05
-19.8 20.1 -17.7
Revised Target UC as at 31/3/06
97.1 96.8 99.2
1st Order risk mitigation available ILB margin / spread buffer
-0.5
-0.4
-0.8
Revised Target UC as at 31/3/06 without buffer
96.6 96.4 98.4
Steady state UC at 2006/7 prices
98.9 98.7 100.8
Version 10.1
201
New Hospitals Programme
11.15.11 Figure 92a shows that the UC amounts to £98.4m in the steady state year at 2005/6 prices which amounts to £100.8m at 2006/7 prices. The final UC reflects the lower margin on the index linked bonds from the mid February assessment but an increase in interest rates over the same period. Thus at financial close the Trust is able to meet the DH target UC reduction (excluding interest movements). Figure 92a does not include any costs associated with the descoping procedure (no consequential costs are included). While the figures are guaranteed in respect of Capital Expenditure and the provision of Global Services (this being the services provided by CHL on completion of all commissioned buildings i.e. services provided during the operating concession from year 11 to year 42 of the Project Agreement), the price does not include any consequential effects that would be required to be addressed prior to the adjustment being implemented (costs or savings associated with the implementation of the descoping procedure e.g. the need to retain premises which would otherwise no longer be required). Finalising the type 1 adjustments within 15 months of financial close (as agreed in Schedule 22 part 7 of the PA) will enable the consequential costs of type 1 adjustments (descoping) to be identified. The Trust is aware that it needs to live within the £100.8 million UC envelope including all consequential costs of Descoping.
11.16 Sensitivity Analysis 11.16.1 The timing of the FBC coincides with the introduction of PbR and Patient Choice.
PbR will be fully implemented over the next 2 years, with the national tariff extended in 2006/07 to cover more than just elective inpatient services (covers c60% of patient care services in 2006/07). The Trust has experience of dealing with the London Patient Choice project and is handling the full introduction of Patient Choice from December 2005.
11.16.2 The affordability analysis within the FBC shows the impact of one or more variables on the overall affordability position. It is extremely unlikely that all the changes in the high and low scenarios would arise together. Appendix 11F shows the sensitivity analysis in the form of variables to the base case.
11.16.3 The business case sets out the Barts and the London/ PCT view of the most likely scenario and explains that many of the scenarios modelled in the sensitivity analysis are likely to have offsetting impacts, for example if demand is lower in some specialties, there are other opportunities under Patient Choice to secure increases in others.
11.16.4 The probabilities used in the appendix are Trust judgements of the probabilities of each item arising. However, the Trust has also tested the analysis using two variations of Monte Carlo random number simulation.
11.16.5 This uses the random numbers to decide if the item will or will not occur. If the random number was equal or greater than the chosen probability, the event was deemed to arise and the full value of the risk factored in. If the random number was below the probability, the event was deemed not to arise and a nil value ascribed. Although a series of runs gave a wide distribution of results the variation from base case had a relatively low range (because many of the items generated a nil cost/gain as the random number indicated the event would not occur). The mean of outcomes was equity between adverse and favourable and supported the overall projection of income, costs and affordability.
11.16.6 Generating random probabilities for each item and applying to the specific cost/ income quantum produced significant variation in the overall impacts, but they
Version 10.1
202
New Hospitals Programme
clustered to a mean where pessimistic outcomes were balanced by optimistic outcomes.
Assumptions
11.16.7 The model initially uses 2016/17 income as the base case to represent steady state and the long-term position. Income changes are modelled at full cost (i.e. PbR basis) and are based on the activity and financial data agreed with PCTs in 2005:
11.16.8 The variables can impact on costs, income or both, as shown below:
■ Some of the variables will impact on the Trust cost base, e.g. if there is a reduction in activity, the Trust will reduce its variable costs (there may be a time lag between the changes and full achievement of staff reductions);
■ Some costs, e.g. availability fees, are fixed and will therefore not be affected by changes from the base assumptions.;
■ Population and demand variables will impact on income and costs; ■ Productivity variables are likely to impact only on costs under PbR. They may,
of course, restrict (or increase) effective capacity and drive “demand” variability; and
■ Tariff variability will impact only on income (although it may create further incentives or imperatives for the Trust to change its cost base). Cost variability will generally be costs incurred during, or before, construction and thus fixed once established.
11.16.9 The financial values in the base case represent the income/cost quantum that is subject to the specific variable, and therefore do not sum to total planned income. This is because the factors are not mutually exclusive. For example, population changes affect a large part of total income, as would tariff changes. Although in the worst and best case modelling the total impact of net changes is stated, the factors would not, nor cannot, all operate together.
11.16.10 Where costs will change when there are income changes, the scenarios assume marginal costs of more than 50% to 2011 then at 40% from 2012. In the pessimistic and optimistic cases, a simple average of these rates (47%) has been used to indicate the corresponding change in costs from the income change. In section E (cost variability) the impact of different marginal rates has been included as a further cost penalty or gain. In section E, the optimistic case models the impact of 50% marginal costs per annum in the pessimistic case for activity in steady state.
A. Analysis of Variables
Population Growth
Base Case
11.16.11 The base case uses Thames Gateway TGW A1 populations, as recommended by the SHA. This is considered the most likely scenario.
Admitted Patient Care
11.16.12 The activity associated with TGW A1 has been separated from other activity growth in the base model and valued. The Trust would be utilising 1,198 beds at 88% occupancy under TGW A1 (1,248 at 86% for a full rescoped scheme). Thus, the base case includes a net increase of 21,349 spells by 2016, which represents a 20% increase in admitted patient care. This reflects growth in admitted patient care of 3% for 2005 to 2008, then 0.5% growth in activity from 2009 to 2016, plus the

Version 10.1
203
New Hospitals Programme
effects of the Thames Gateway population. The MFF associated with the relevant income is included.
Outpatients
11.16.13 Outpatient steady state activity is 395,000 attendances per annum. The MFF associated with the relevant income is included.
11.16.14 Variations to the base case are detailed in Figure 93 below.
Figure 93 – Population Growth & Variability
Low Scenario High scenario
A.1 & A.2: TGW A2 and A3 are higher population growth projections and would result in overall increases in demand. TGW 3 would require the Trust to use 1,396 beds to deliver indicative activity based on the model conversion rates. In practice, other changes would reduce the bed requirements, but activity under PbR will be paid at tariff. The optimistic case is an additional 6,000 spells by 2016, representing a 3% growth per annum from 2005 to 2016. The probability of A3 projections has increased since Version 09 of the FBC. The latest estimates from the ODPM Thames Gateway office show an increase in the proportion of TG housing in East London which would entail an increase In the Trust’s catchment population by a further 40,000 over TGW A1 from 310,000 to 350,000.
A.3: Lower demand. Relates to specific population reductions rather than reduced demand from specific morbidity and admission rates; these are covered under demand variability. It has been modelled as a 20% shortfall on TGW A1 projections. Thus the pessimistic case is a reduction of 5,000 spells by 2016. The probability of this scenario is reduced by the recent ODPM Thames Gateway analysis (as above).
A.4: It is not considered likely that outpatient activity will fall below current levels due to population growth, etc.
A.4: On historic trends, a 10% increase would be very conservative. If nationally OP growth is contained to these levels, OP tariffs are likely to be higher in real terms than now, because the intensity of consultations will increase. 50% of the income will be absorbed in cost increases.
B. Demand Variability
Base Case
11.16.15 Reductions in non-elective bed days (medical emergencies) as a consequence of Long-Term Conditions management initiatives and increases in NHS work undertaken by the independent sector are required to meet DH planning guidance and expectations. However, underlying growth in patients is still expected, in
Version 10.1
204
New Hospitals Programme
particular for specialised services that are less likely to be undertaken in the independent sector or outside tertiary centres. There is currently a significant outflow of patients to non-NEL providers, particularly in critical care. Treating a higher proportion of new patients within the Trust is feasible based on planned hospital capacity. The base case B.1 and B.2 includes a series of assumptions regarding reduced activity. The “pessimistic case” then models higher reductions to the base case (and the best case reduces the impact of the base case assumptions).
11.16.16 The key demand assumptions within the base case are as follows:
■ The base case does not include any increase for referral growth from either primary care or secondary care (for tertiary services);
■ The achievement of the 18-week from referral to treatment access target is treated as a one-off stock reduction between 2005 and 2008 within the base case;
■ The start point for the base case model is actual activity for 2003/04; ■ Cardiac services are modelled on version 8 of the North East London & Essex
Cardiac Transitional Plan. The cardiac activity for Essex is based on the activity in the business case for the Essex Cardiac Centre (which is due to open in 2007/08); and
■ Patient Choice has been assumed at steady state in aggregate, but the Trust accepts the premise that there are likely to be gains and losses between specialties.
Non Elective Admitted Patient Care in Base Case
11.16.17 In 2004/05 the Trust had a 10% over-performance against planned activity for non-elective inpatient services. The base model only takes account of the THPCT element of this over-performance, so takes a prudent view; hence the base model assumes that non-emergency spells are reduced by 10% for other PCTs against 2004/05 levels, with a further 5% reduction in bed days for emergency medicine to 2007/08. Although the activity model has been updated to 2006/07 planned SLA levels, the demand assumptions in the business case and in the sensitivity analysis remain robust. In terms of reducing non elective admitted care activity levels, THPCT plans include additional resources in the community (in addition to meeting the agreed activity levels in the BLT New Hospital base model) in line with the Long Term Conditions Strategy within the joint THPCT/BLT Integrated Service Improvement Plan.
Elective Admitted Patient Care in Base Case
11.16.18 The Trust also has over performance in a number of areas for elective inpatient services in 2004/05 (notably for cardiac services). Thus the start point for the base case (2006/07 planned SLA activity) does not include the 2004/05 over-performance. In addition, the base case assumes an outflow of 10% to the independent sector for key specialties - ENT, Orthopaedics, General Surgery, Gynaecology and Urology admissions to 2008/09.
Outpatients
11.16.19 The base case assumes that 1 in 4 outpatient appointments are no longer referred to The Trust outpatient clinics. This is phased in over the next 11 years to achieve steady state, i.e. no increase in outpatients for the increase in population. This equates to a 25% reduction in outpatient attendances (see appendix 11H).
11.16.20 The table below summarises the key demand variables to the base case.
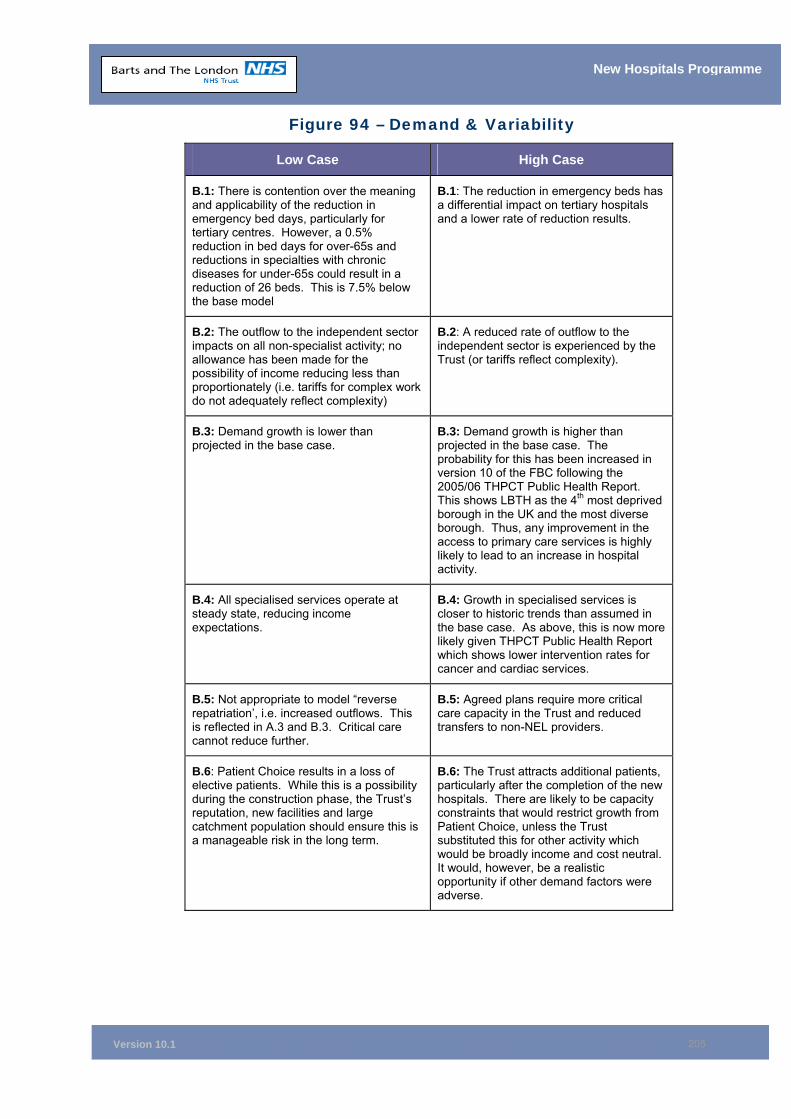
Version 10.1
205
New Hospitals Programme
Figure 94 – Demand & Variability
Low Case High Case
B.1: There is contention over the meaning and applicability of the reduction in emergency bed days, particularly for tertiary centres. However, a 0.5% reduction in bed days for over-65s and reductions in specialties with chronic diseases for under-65s could result in a reduction of 26 beds. This is 7.5% below the base model
B.1: The reduction in emergency beds has a differential impact on tertiary hospitals and a lower rate of reduction results.
B.2: The outflow to the independent sector impacts on all non-specialist activity; no allowance has been made for the possibility of income reducing less than proportionately (i.e. tariffs for complex work do not adequately reflect complexity)
B.2: A reduced rate of outflow to the independent sector is experienced by the Trust (or tariffs reflect complexity).
B.3: Demand growth is lower than projected in the base case.
B.3: Demand growth is higher than projected in the base case. The probability for this has been increased in version 10 of the FBC following the 2005/06 THPCT Public Health Report. This shows LBTH as the 4th most deprived borough in the UK and the most diverse borough. Thus, any improvement in the access to primary care services is highly likely to lead to an increase in hospital activity.
B.4: All specialised services operate at steady state, reducing income expectations.
B.4: Growth in specialised services is closer to historic trends than assumed in the base case. As above, this is now more likely given THPCT Public Health Report which shows lower intervention rates for cancer and cardiac services.
B.5: Not appropriate to model “reverse repatriation’, i.e. increased outflows. This is reflected in A.3 and B.3. Critical care cannot reduce further.
B.5: Agreed plans require more critical care capacity in the Trust and reduced transfers to non-NEL providers.
B.6: Patient Choice results in a loss of elective patients. While this is a possibility during the construction phase, the Trust’s reputation, new facilities and large catchment population should ensure this is a manageable risk in the long term.
B.6: The Trust attracts additional patients, particularly after the completion of the new hospitals. There are likely to be capacity constraints that would restrict growth from Patient Choice, unless the Trust substituted this for other activity which would be broadly income and cost neutral. It would, however, be a realistic opportunity if other demand factors were adverse.
Version 10.1
206
New Hospitals Programme
C. Productivity
Base Case
11.16.21 The base case therefore assumes a length of stay of 5 days and average occupancy of 88% (previously 5.5 days in Version 09 of the FBC). The position is complicated by the % day case rates. However, the absolute position is of less relevance than recognising that, under PbR, reductions in length of stay (provided they do not reduce quality and re-admission rates) will allow the Trust to reduce its variable costs for any given level of activity. Increasing day case rates to 55% is challenging given that certain elective services (such as cardiac surgery) have no day cases. Moreover, increasing the day case rate leads to an increase in the average length of stay, given that residual elective inpatients have a more complex case-mix.
11.16.22 If the capacity were re-used this would be reflected in “demand” income gains. For the purposes of this analysis, we assume that 5,000 cases are capable of seeing length of stay flexed by 1 day (enabling 1,000 additional cases to be treated or capacity reduced: costed at average cost per bed day). Similarly, 3,000 cases can flex to/from day cases over and above the base assumption.
D. Tariff and Levy Variability
Base Case
Pricing
11.16.23 The base case includes 2006/07 PbR services (i.e. elective and non-elective inpatient activity except specialised services e.g. renal transplants) priced at tariff (£238 million in 2006/07) with non PbR services (non-elective inpatients, outpatients and A&E services) at our local 2006/07 prices (£139 million in 2006/07). It should be noted that the Trust’s local price is lower than the national average costs for non-PbR activity. Thus there is a high probability of a gain on PbR to offset current losses when PbR is extended.
11.16.24 The Trust is currently at reference cost index (RCI) of 98. The tariffs may alter in real terms as the DH will set these annually. The base case assumes a deflation of the tariff of £10m for 2007-09 and £2 million thereafter.
Case-mix
11.16.25 The base case does not include any increase in income for the planned introduction from 2008/09 of the use of version 4 of the HRG grouper. This is on the basis that the Trust has used 2006/07 tariffs, including a case-mix adjustment (see sections 11.16.27-11.16.28 below on central levies). However, there is now a high probability of increased income from the use of version 4 of the HRG grouper, given its more sophisticated use of case mix and given that the Trust has not benefited from the use of specialist top ups in 2006/07. Specialist top ups were designed as an interim measure pending the implementation of HRG version 4 to recognise the deficiencies of HRG grouper 3.5 in taking account of case mix, but the top up is only received where the relevant HRG is signified as “with complications – unspecified”. The Trust, along with other teaching hospitals, specifies the complication within the secondary element of the clinical coding. Thus, in 2006/07 the Trust has received c£1 million from specialist top ups, whereas all other acute trusts in North East London have received greater income for specialist top ups with lower activity and less complex case mix.
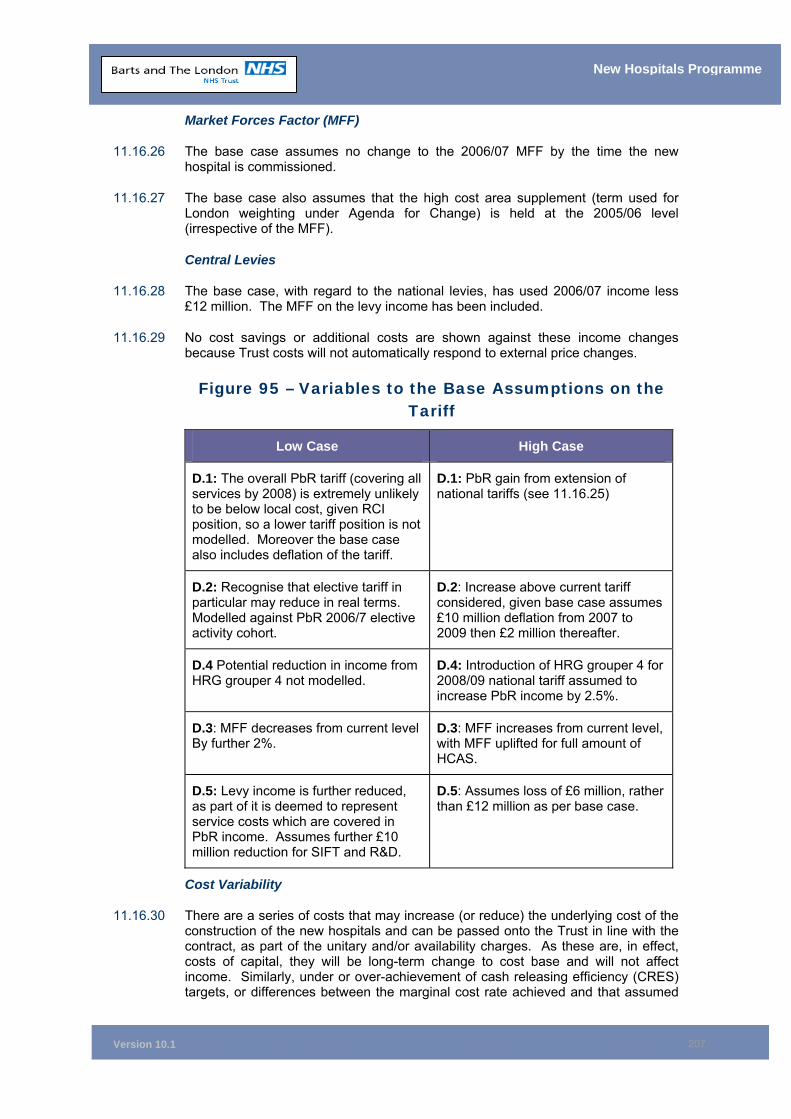
Version 10.1
207
New Hospitals Programme
Market Forces Factor (MFF)
11.16.26 The base case assumes no change to the 2006/07 MFF by the time the new hospital is commissioned.
11.16.27 The base case also assumes that the high cost area supplement (term used for London weighting under Agenda for Change) is held at the 2005/06 level (irrespective of the MFF).
Central Levies
11.16.28 The base case, with regard to the national levies, has used 2006/07 income less £12 million. The MFF on the levy income has been included.
11.16.29 No cost savings or additional costs are shown against these income changes because Trust costs will not automatically respond to external price changes.
Figure 95 – Variables to the Base Assumptions on the Tariff
Low Case High Case
D.1: The overall PbR tariff (covering all services by 2008) is extremely unlikely to be below local cost, given RCI position, so a lower tariff position is not modelled. Moreover the base case also includes deflation of the tariff.
D.1: PbR gain from extension of national tariffs (see 11.16.25)
D.2: Recognise that elective tariff in particular may reduce in real terms. Modelled against PbR 2006/7 elective activity cohort.
D.2: Increase above current tariff considered, given base case assumes £10 million deflation from 2007 to 2009 then £2 million thereafter.
D.4 Potential reduction in income from HRG grouper 4 not modelled.
D.4: Introduction of HRG grouper 4 for 2008/09 national tariff assumed to increase PbR income by 2.5%.
D.3: MFF decreases from current level By further 2%.
D.3: MFF increases from current level, with MFF uplifted for full amount of HCAS.
D.5: Levy income is further reduced, as part of it is deemed to represent service costs which are covered in PbR income. Assumes further £10 million reduction for SIFT and R&D.
D.5: Assumes loss of £6 million, rather than £12 million as per base case.
Cost Variability
11.16.30 There are a series of costs that may increase (or reduce) the underlying cost of the construction of the new hospitals and can be passed onto the Trust in line with the contract, as part of the unitary and/or availability charges. As these are, in effect, costs of capital, they will be long-term change to cost base and will not affect income. Similarly, under or over-achievement of cash releasing efficiency (CRES) targets, or differences between the marginal cost rate achieved and that assumed
Version 10.1
208
New Hospitals Programme
in the modelling in sections A-C of the sensitivity analysis, will impact on the cost base of the Trust.
11.16.31 Appendix 11F includes the potential impact if costs increase faster than expected. This shows up under the low scenario (See E2) with potential additional costs of £1.2million prior to probability analysis.
11.17 Handling Strategy for Changes to the Base Case Income & Expenditure Model
11.17.1 The sensitivity analysis shows that the overall base case income and expenditure modelling is prudent and robust. Indeed the sensitivity analysis demonstrates that, in terms of affordability, the Trust has headroom, in that the total value of the high case scenario (having taken into account probability analysis) is greater than the total value of the low case scenario. The Trust has the following handling strategies for any potential changes to base model:
Handling strategies for coping with more activity than planned
11.17.2 The Trust has the following potential strategies for dealing with more activity than is currently included in the planned level of activity in the steady state year.
a) Utilise the 250 mothballed beds and/or refurbish assets that are
currently descoped (type one adjustments) - the Trust would present further business case(s) for Rescoping in line with Schedule 22, Part 7 of the Project Agreement. The business case(s) would require approval from the DH.
b) Use of planned clinical research unit – both the Royal London and Barts includes clinical research centres with in patient beds (additional income of £2 million assumed from commercial trials). This could be used for NHS patients should activity be under estimated in the steady state year. Currently, the return on patient care beds is often greater than that from clinical trials depending on the case mix and throughput of the activity.
c) Convert non-clinical space into clinical space –the designs of both hospitals are flexible in terms of converting into generic clinical areas. In addition, non-clinical space can be converted into clinical space, e.g. office accommodation in outpatients could be converted into clinical space for outpatient clinics and study areas/offices within Phase 1 of The Royal London and both phases of Barts could be converted into inpatient or diagnostic accommodation, if required. This would give a contribution from the difference between the tariffs received and the marginal costs for undertaking the extra activity (the net contribution is likely to be less than for undertaking clinical trials).
d) Do not transfer MEH activity – the 22 beds that are to be used following the transfer from MEH of acute care of the elderly activity could be used for other inpatient activity (subject to discussion and agreement with Tower Hamlets PCT). The staff associated with the 22 beds at MEH would go back to Mile End Hospital if the trust could not accommodate the increase in activity. The base case affordability analysis does not include any net contribution from including the activity associated with the transfer of 22 MEH beds (see 11.10.13).
e) Additional facilities – at the end of all phases at both The Royal London and Barts, The London Chest Hospital and The Royal London outpatient building are surplus to requirements based on our base activity and income model.
Version 10.1
209
New Hospitals Programme
The London Chest could continue to remain as an inpatient facility should an extra 109 beds be required. It would be less than optimal to run a much smaller in patient facility at The London Chest. The Royal London outpatients building could be refurbished for extra out patient accommodation or a new clinical facility could potentially be built on the site. There is also the potential to purchase the Royal Mail site adjacent to Phase 1 at The Royal London.
Handling strategies for coping with less activity than planned and increases in cost
11.17.3 The Trust has the following potential strategies for dealing with less activity than is currently included in the planned level of activity in the steady state year.
a Cost Reduction to maintain Trust Income and Expenditure balance within a reduced activity scenario - The Trust will be able to save the marginal costs of reduced activity but recognises that except in volume related elements of the contract, it must maintain its Unitary Charge payments and therefore would need to identify additional savings to meet the full impact of reduced income resulting from reduced clinical activity.
A number of options have been considered and would be implemented if necessary. Some are in part non-recurrent in nature, but would be used to cover any period between income reduction and the longer term efficiency based savings to achieve recurrent balance. The range of potential savings is shown against each.
■ The Trust could rationalise services on the Bart’s site by only using the re-developed King George V block. Thus the Trust could vacate some or all of the other buildings around the Bart’s square (North Wing and Great Hall, East Wing: Clinical Offices, West Wing: Breast Cancer and Kenton and Lucas: Fertility and Sexual Health). This would lead to savings on power, heat and light and certain fixed costs along with potential income from letting these spaces (this could generate net cost reductions up to £1 million per annum, excluding income from letting.
■ On several benchmarking measures the trust has scope to change patterns of activity and reduce length of stay. This is discussed more fully in 11.4 and we recognise the risk of ”double counting“ potential savings, given the changes to throughput associated with the mothballing of 250 beds. However, it is likely that at least part of the achievable gains would be available to meet the reduced activity/reduced income scenario and it would manifest in reduced expenditure through ward closures and reduced staffing levels. (£1 million to £3 million per annum).
■ Recent external reports have indicated the trust frequently undertakes services for other organisations without commensurate reward and recognising the full commercial opportunities available to it i.e. not charged at full cost potential. Areas identified include Pathology services provided to other NHS bodies, but there are numerous other examples of the specialist expertise within the trust being made available to other organisations at little or no cost. The impact is likely to be particularly on the NHS and result in a transfer of costs from BLT to other NHS bodies. Moreover this is reflected by direct access costs being significantly below the national average and hence the Trust would increase income with the introduction of national tariffs for GP direct access services (due to be introduced from 2008/09). (£2 million - £3 million per annum)
■ The trust has not so far predicated any of its plans on out-sourcing corporate services. The development of NHS shared service centres and other market developments, including internet and intranet to reduce the reliance on direct contact may reduce the risks and increase the potential benefits of out-sourcing. Any changes would release for sale (or reduce the volume of commercially rented property) current NHS assets. This would be carried out in
Version 10.1
210
New Hospitals Programme
conjunction with local NHS bodies to ensure the space provided and covered by the unitary charge were fully utilised. BLTs current plans include some reliance on space outside the main PFI development, and there are other properties such as the pay consortiums office at Barking. (£1M-£3M per annum; saving on fixed costs, plus potential for 1-off sale benefits in health economy)
■ Deferring the replacement and upgrade of PC’s. Although these are capital expenditure, there are some other expenditure items including small equipment which could be capitalised. This would reduce revenue spend although undoubtedly a non-recurrent measure. Other non-recurrent savings would include further reductions to stock levels. (£750K - £1.5M for a year)
11.17.4 In addition to evaluating options for cost reduction the Trust will also be seeking areas to expand activity and consequently income, such as:
Reducing the outflow of patients to other sectors of London – NEL has an outflow of patients to other sectors of London as BLT has not had sufficient capacity to take these patients. The base case model is extremely prudent in terms of reducing these outflows, with steady state assumed for most specialist services. However, if activity was lower than in the base case, then the Trust would have the capacity to reduce the outflow of patients to other London teaching hospitals, without increasing the range of specialist services. Examples of where reductions in outflows of new patients from NEL could be achieved include:
ENT services from Newham: inpatients currently treated at The Royal National Throat Nose and Ear Hospital (RNTNEH);
Plastic surgery from Newham: currently there are elective treatments at Broomfield Hospital in Chelmsford;
Tertiary Neurology outflows to the National Hospital, notably from Whipps Cross Hospital; and
Renal services: due to a lack of capacity within the Trust, several NEL renal patients are currently treated by north central London providers.
b Ophthalmology – Tower Hamlets PCT currently has a contract for Ophthalmology with Moorfields (provided at MEH). Barts and The London provides ophthalmology services to City and Hackney and Newham PCTs. The Trust has significantly improved its ophthalmology services over the past 2 years, recruiting 2.5 new consultants and radically re-designing the service model. Patient Choice work has been undertaken for NEL PCTs over the past 12 months.
The Trust therefore considers that it is in a strong position to provide a quality service for Tower Hamlets PCT GPs and residents (which of course we will be entitled to do under Patient Choice) within our new hospitals. This would free up fixed costs at MEH for Tower Hamlets PCT.
c Paying patients – In 2004/2005 the Trust’s paying patient income totalled £1.5 million. This means that the Trust has a low level of paying patient income in comparison with other London teaching hospitals. Lower NHS activity could be offset by a dedicated paying patient unit at Barts and/or The Royal London. There is a strong market for specialised care from self payers (UK and overseas) in areas such as cancer treatment and procedures. This would require a change in legislation by 2017 but this seems likely given current policy pre-dates ISTC policy.
Version 10.1
211
New Hospitals Programme
A dedicated 25-bedded unit for specialised services could lead to gross income in the region £7 million and a net gain of around £1 million (assumes 14% margin). Such a unit could be run by the Trust or by a partner (which would result in less risk but reduced marginal gain). Although the margin on UK insured patients is too low to be a primary market, they could also make a contribution to fixed costs if there was unused capacity.
d Intervention rates – the activity model agreed with NEL PCTs leaves intervention rates unchanged. As stated earlier in this chapter this is a very prudent assumption given that intervention rates in inner North East London are below national averages. Moving to the national average would of course add pressure to occupancy rates without further changes in working practices/throughput but the advent of Practice Based Commissioning and the Public Health agenda of PCTs in NEL are likely to lead to increasing rates towards the national averages. A potential net gain on income of around £2 million by 2016 is therefore possible.
e Care of the elderly beds transferring from MEH – the current affordable UC calculations do include the net gain from including 172 acute / stroke episodes transferred from MEH. If acute activity was materially lower than planned then the Trust could enter into discussions with Tower Hamlets PCT for a greater transfer of activity from MEH. This could generate a net gain of around £1.7 million (623 additional admissions, which equates to 63 additional beds).
f Reduced loss of income from work to ISTC – the value of work transferring to the independent sector has been costed at average specialty rates. Thus this is likely to be an over-estimate of the income loss given the lower than average casemix of the work that is assumed to transfer.
11.18 Balance Sheet 11.18.1 The Trust is conscious that it will need to be able to operate within the Foundation
Trust regime from 1 April 2008 (at the latest). The Trust has therefore prepared a long-term balance sheet and reviewed the ratios used by FTs to demonstrate that post-FBC it will be able to live within the FT regime (see Appendix 11I)
11.19 Chapter Conclusion 11.19.1 The PFI option is affordable and is considered robust on the basis of the sensitivity
analysis undertaken. NEL and Essex PCTs have endorsed the base activity model. The base activity model and pricing of the activity provide a prudent view of the next 12 years and, therefore, present a sound financial platform for the Trust and our PFI partner. The sensitivity analysis confirms that the base case is a robust middle ground for affordability.
Version 10.1
212
New Hospitals Programme
11.20 Chapter Appendices
11A Best Value Cost Reduction Programme 05/06 11A1 Reviewing and Improving Clinical Efficiency SMG Paper Sept 2005 11A2 Payment by Results Risk Assessment Programme 11A3 Draft Medium Term Financial Strategy and Plan 06-07 11A4 Workforce Added Value Review Dec 05 11B Baseline Activity Projections 11C Scenario Analysis 11D Trust Income Assumptions by PCT 11E NHS Bank Funding 11E1 Request for NHS Bank Transitional Relief 11E2 Capital Enabling Schemes 11F Affordability in the FBC – Assumptions - Variables 11G Top 100 HRGs – Length of Stay Improvements 11H Outpatient New to Follow-up Comparison 11I Annual Plan 11J Episode to Spell Conversion Rates 11K Tower Hamlets PCT Affordability Analysis 11L Tower Hamlets PCT 05/06 Strategic Aims and Corporate Priorities 11M1 Trust’s Income and Expenditure Pro Forma to Steady State
(Marginal) 11M2 Trust’s Income and Expenditure Pro Forma to Steady State (TAC,
FT Format)

Version 10.1
213
New Hospitals Programme
12 RISK ANALYSIS Synopsis – Risk Analysis
This chapter sets out: • The approach to risk analysis and assessment of quantifiable and
unquantifiable risks;
• The key risk areas, their quantification, valuation and acceptability;
• The sensitivity analysis employed in relation to the analysis of risks;
• Assurance of the Trust’s robust approach to risk management in relation to project specific risks, post-FBC approval; and
• Contingency planning arrangements.
12.1 Introduction 12.1.1 All projects have risks associated with them and it is vital to identify these risks,
capture them, quantify them where possible, and establish for those risks with a high or medium ranking an action plan for mitigating them.
12.1.2 The New Hospitals Project is a large and complex PFI project, and consequently there are a significant number of risks associated with its delivery. Because of this, a detailed and robust approach has been taken to the identification of risk and risk management.
12.1.3 Thus the following paragraphs detail the risks faced by the Trust from the PFI contract, together with the risk handling strategies. Section 11.16 covers the sensitivity analysis on activity, income and cost assumptions associated with the Trust’s operating risks i.e. business risk. The handling strategies for dealing with income gain or loss (e.g. where patient care activity is greater or less than planned) are detailed in section 11.17. The overall risk assessment in terms of the impact from business and PFI risks is shown at the end of this chapter (see 12.10).
12.2 Risk Methodology 12.2.1 The methodology employed in relation to risk analysis for the project comprises four
steps. These are:
• Risk identification - developing a risk register covering key risk areas and individual risks within these areas;
• Risk assessment - estimating the likelihood and, where appropriate, the timing of each risk occurring and the impact if it should occur;
• Risk quantification - putting a value to each of the risks, using the estimates of likelihood, impact and timing; and
• Risk management - developing a plan to manage/mitigate all the risks identified in the risk register for the preferred option, including identification of responsible persons for managing each risk and setting up monitoring mechanisms.
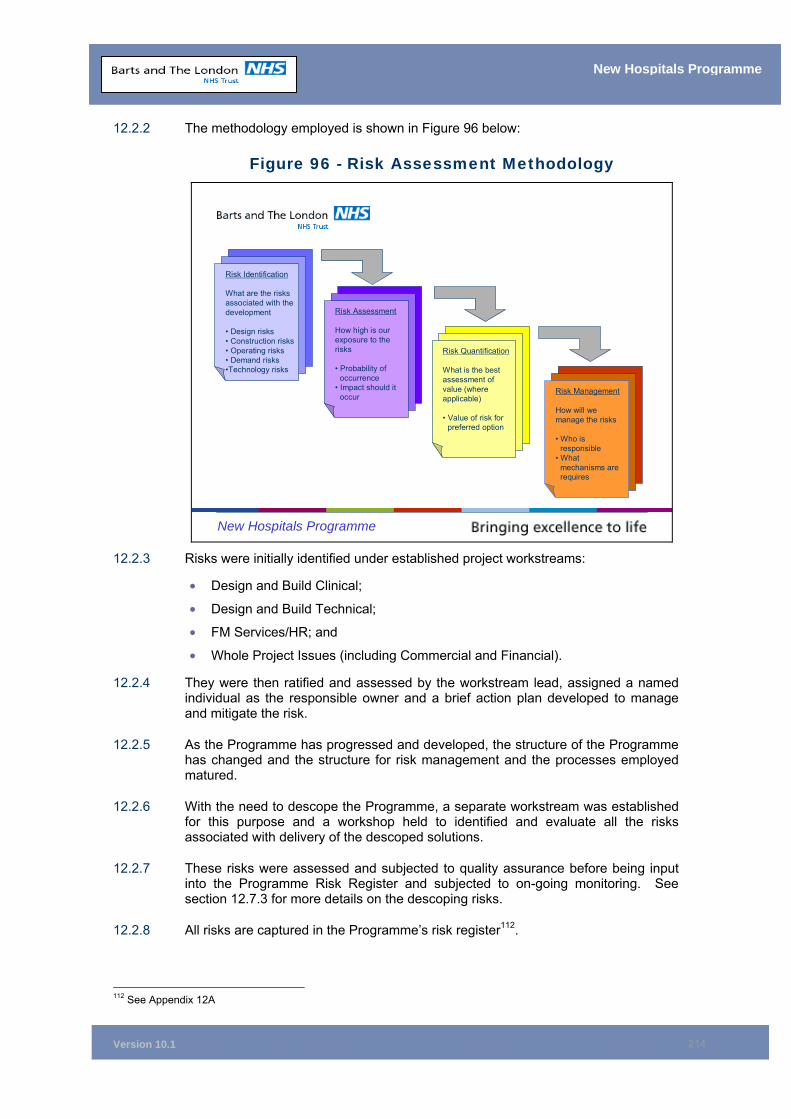
Version 10.1
214
New Hospitals Programme
12.2.2 The methodology employed is shown in Figure 96 below:
Figure 96 - Risk Assessment Methodology
New Hospitals Programme
Risk Identification
What are the risks associated with the development
• Design risks• Construction risks• Operating risks• Demand risks•Technology risks
Risk Assessment
How high is our exposure to the risks
• Probability of occurrence
• Impact should it occur
Risk Quantification
What is the best assessment of value (where applicable)
• Value of risk for preferred option
Risk Management
How will we manage the risks
• Who is responsible
• What mechanisms are requires
12.2.3 Risks were initially identified under established project workstreams:
• Design and Build Clinical;
• Design and Build Technical;
• FM Services/HR; and
• Whole Project Issues (including Commercial and Financial).
12.2.4 They were then ratified and assessed by the workstream lead, assigned a named individual as the responsible owner and a brief action plan developed to manage and mitigate the risk.
12.2.5 As the Programme has progressed and developed, the structure of the Programme has changed and the structure for risk management and the processes employed matured.
12.2.6 With the need to descope the Programme, a separate workstream was established for this purpose and a workshop held to identified and evaluate all the risks associated with delivery of the descoped solutions.
12.2.7 These risks were assessed and subjected to quality assurance before being input into the Programme Risk Register and subjected to on-going monitoring. See section 12.7.3 for more details on the descoping risks.
12.2.8 All risks are captured in the Programme’s risk register112.
112 See Appendix 12A
Version 10.1
215
New Hospitals Programme
12.3 Risk Identification 12.3.1 Initially, in 2002, external consultants were employed to assist in the development
of a comprehensive risk register. HVR Consulting Services, through workshops and interviews involving workstream leads and other key members of the project team, developed a risk register, which was presented to the Project Board for consideration and approval. The register was subsequently adopted.
12.3.2 Following the evaluation of the BaFO, subsequent appointment of provisional preferred bidder and issue of the preferred bidder letter, there was a need to extensively review the risk register to reassess those risks previously identified and to update it with newly identified risks. Using the SWOT analysis produced as part of the BaFO evaluation process, a significant number of additional risks were identified and added to the register. The risk register has been updated on a regular basis throughout the preferred bidder period.
12.3.3 Since then, and throughout the development of the project, the register has been continually updated and amended to reflect the changing risk profile.
12.3.4 The risk register details each risk and provides:
• Identification number;
• Description of risk;
• Risk level (as defined by the risk assessment matrix);
• Lead (senior responsible owner);
• Mitigation actions required, and target date;
• Achieved date; and
• Delay (reasons).
12.4 Risk Assessment and Quantification 12.4.1 The identified risks have been assessed using the Trust’s generic risk evaluation
system, used for scoring and managing risk across the Trust. The system was based on the methodology developed by the Controls Assurance Support Unit. Where appropriate, an assessment of the value/cost implication of the risk becoming an issue has been assessed.
12.4.2 Each identified risk is assessed for likelihood of occurrence (1 – 5) and impact or consequence (1 – 5). Scores are then multiplied to give an overall risk score between 1 and 25. Any risk assessment score of 8 or over is considered high, and if over 15, it is considered to be a significant risk.
12.4.3 A copy of the risk matrix employed to assess identified risks, which also provides a definition of the individual scores, is shown in Appendix 12B.
12.5 Risk Management 12.5.1 The risk register is a critical project management tool and is reviewed on a regular
basis by the project’s operational management team (project team) and the Project Board, where new risks are identified and existing risks re-evaluated. A dedicated risk/issue management group has been established to review and Quality Assure all risks and ensure they are being managed effectively. Any current significant risks and progresses against them is report on a monthly basis to the Trust Board.

Version 10.1
216
New Hospitals Programme
12.5.2 In addition, all project risks assessed as high or significant are included on the Trust’s risk register and subject to review by the Trust’s Risk Management Group and the board-level Healthcare Governance Steering Group. The Trust’s Programme Assurance Board reviews high-level risks and the strategy for management of the risks on a monthly basis (see Chapter 14).
12.6 Risks Transferred to the PFI Partner 12.6.1 A critical factor in the development and agreement of any PFI deal is identifying,
assessing and analysing those risks in relation to the Programme (construction and development) which are transferred to the preferred partner. This is critical to assessing the value for money (VfM) that the PFI solution delivers against the public sector comparator (PSC).
12.6.2 There are two main categories of risk to identify: quantifiable and unquantifiable. A qualitative and quantitative approach has been taken to assessment and analysis in relation to these risks. The VfM assessment has been undertaken by use of the Department of Health’s (DH’s) generic economic model (GEM) and associated guidance.
12.6.3 The risks to the Trust can be grouped under the categories in the standard form contract:
• Design;
• Construction and Development;
• Operating Cost;
• Variability of Revenue;
• Termination;
• Technology and Obsolescence;
• Control;
• Residual Value; and
• Other Project Risks.
12.6.4 The approach to the assessment and quantification of these risks is set out below.
Risk Assessment and Quantification
12.6.5 A fully-quantified risk assessment workshop, which was facilitated by PricewaterhouseCoopers (PwC), was undertaken and was periodically updated during the procurement process. Representatives included:
• Trust estates;
• Facilities management;
• Operational management;
• Human resources and finance staff;
• The Trust’s legal adviser’s Allen and Overy; and
• Trust’s quantity surveyors (DL).
12.6.6 For each risk option, the following factors were taken into account in calculating the financial impact of the risk:
• Basis for quantification - what area of cost will the risk impact upon if it occurs;
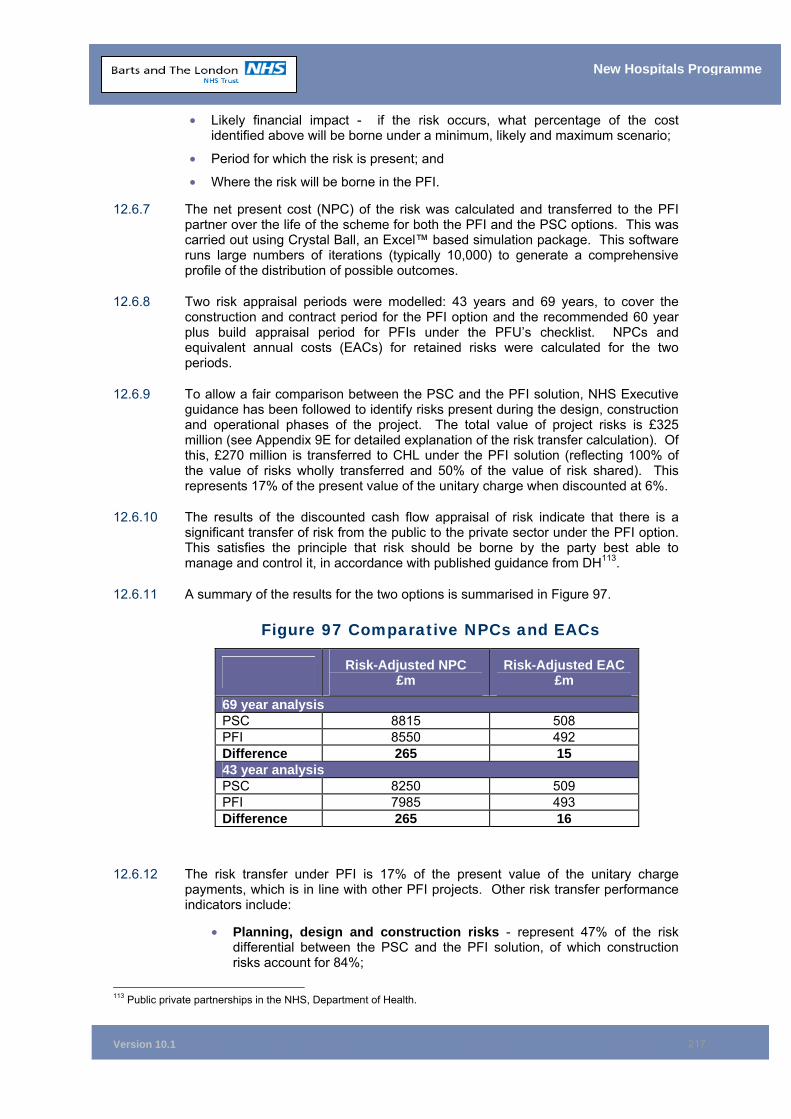
Version 10.1
217
New Hospitals Programme
• Likely financial impact - if the risk occurs, what percentage of the cost identified above will be borne under a minimum, likely and maximum scenario;
• Period for which the risk is present; and
• Where the risk will be borne in the PFI.
12.6.7 The net present cost (NPC) of the risk was calculated and transferred to the PFI partner over the life of the scheme for both the PFI and the PSC options. This was carried out using Crystal Ball, an Excel™ based simulation package. This software runs large numbers of iterations (typically 10,000) to generate a comprehensive profile of the distribution of possible outcomes.
12.6.8 Two risk appraisal periods were modelled: 43 years and 69 years, to cover the construction and contract period for the PFI option and the recommended 60 year plus build appraisal period for PFIs under the PFU’s checklist. NPCs and equivalent annual costs (EACs) for retained risks were calculated for the two periods.
12.6.9 To allow a fair comparison between the PSC and the PFI solution, NHS Executive guidance has been followed to identify risks present during the design, construction and operational phases of the project. The total value of project risks is £325 million (see Appendix 9E for detailed explanation of the risk transfer calculation). Of this, £270 million is transferred to CHL under the PFI solution (reflecting 100% of the value of risks wholly transferred and 50% of the value of risk shared). This represents 17% of the present value of the unitary charge when discounted at 6%.
12.6.10 The results of the discounted cash flow appraisal of risk indicate that there is a significant transfer of risk from the public to the private sector under the PFI option. This satisfies the principle that risk should be borne by the party best able to manage and control it, in accordance with published guidance from DH113.
12.6.11 A summary of the results for the two options is summarised in Figure 97.
Figure 97 Comparative NPCs and EACs
Risk-Adjusted NPC £m
Risk-Adjusted EAC £m
69 year analysis PSC 8815 508 PFI 8550 492 Difference 265 15 43 year analysis PSC 8250 509 PFI 7985 493 Difference 265 16
12.6.12 The risk transfer under PFI is 17% of the present value of the unitary charge payments, which is in line with other PFI projects. Other risk transfer performance indicators include:
• Planning, design and construction risks - represent 47% of the risk differential between the PSC and the PFI solution, of which construction risks account for 84%;
113 Public private partnerships in the NHS, Department of Health.
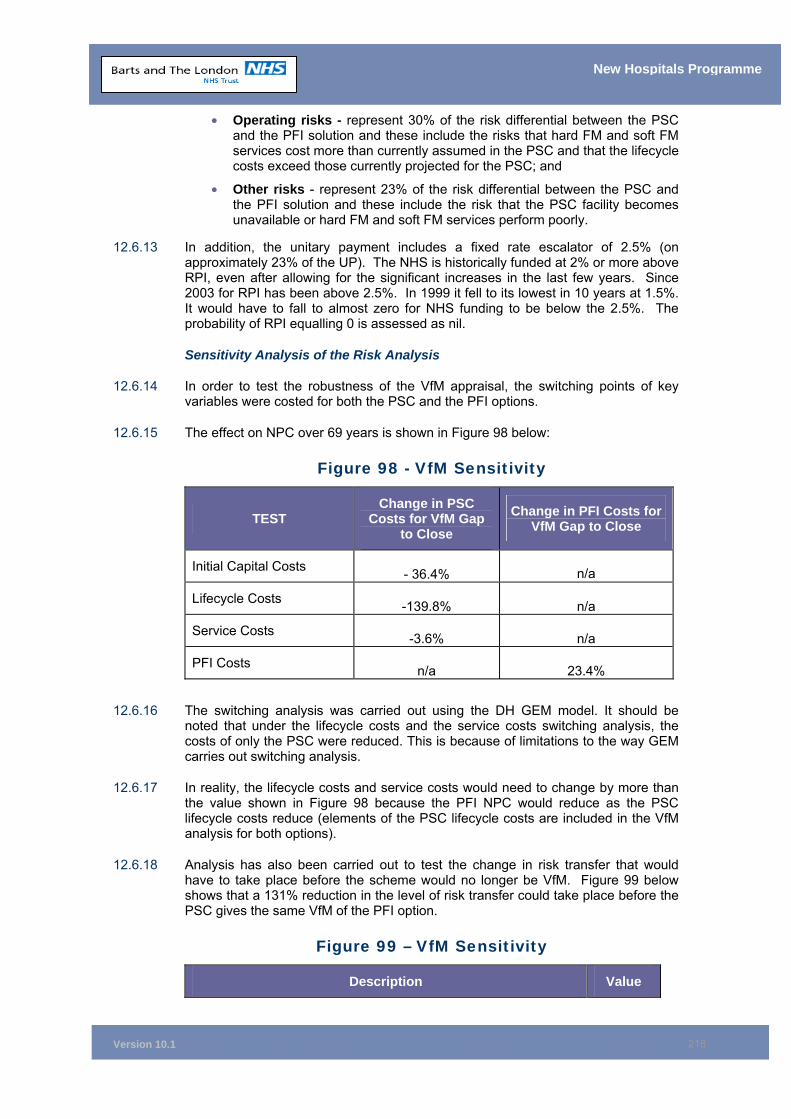
Version 10.1
218
New Hospitals Programme
• Operating risks - represent 30% of the risk differential between the PSC and the PFI solution and these include the risks that hard FM and soft FM services cost more than currently assumed in the PSC and that the lifecycle costs exceed those currently projected for the PSC; and
• Other risks - represent 23% of the risk differential between the PSC and the PFI solution and these include the risk that the PSC facility becomes unavailable or hard FM and soft FM services perform poorly.
12.6.13 In addition, the unitary payment includes a fixed rate escalator of 2.5% (on approximately 23% of the UP). The NHS is historically funded at 2% or more above RPI, even after allowing for the significant increases in the last few years. Since 2003 for RPI has been above 2.5%. In 1999 it fell to its lowest in 10 years at 1.5%. It would have to fall to almost zero for NHS funding to be below the 2.5%. The probability of RPI equalling 0 is assessed as nil.
Sensitivity Analysis of the Risk Analysis
12.6.14 In order to test the robustness of the VfM appraisal, the switching points of key variables were costed for both the PSC and the PFI options.
12.6.15 The effect on NPC over 69 years is shown in Figure 98 below:
Figure 98 - VfM Sensitivity
TEST Change in PSC
Costs for VfM Gap to Close
Change in PFI Costs for VfM Gap to Close
Initial Capital Costs - 36.4%
n/a
Lifecycle Costs -139.8% n/a
Service Costs -3.6% n/a
PFI Costs n/a 23.4%
12.6.16 The switching analysis was carried out using the DH GEM model. It should be noted that under the lifecycle costs and the service costs switching analysis, the costs of only the PSC were reduced. This is because of limitations to the way GEM carries out switching analysis.
12.6.17 In reality, the lifecycle costs and service costs would need to change by more than the value shown in Figure 98 because the PFI NPC would reduce as the PSC lifecycle costs reduce (elements of the PSC lifecycle costs are included in the VfM analysis for both options).
12.6.18 Analysis has also been carried out to test the change in risk transfer that would have to take place before the scheme would no longer be VfM. Figure 99 below shows that a 131% reduction in the level of risk transfer could take place before the PSC gives the same VfM of the PFI option.
Figure 99 – VfM Sensitivity
Description Value

Version 10.1
219
New Hospitals Programme
Description Value
VfM Position Without Risk Transfer £47.5m Risk Transfer £218.3m VfM Position with Risk Transfer £265.7m % Change in Risk Transfer Before Scheme is no Longer VfM - 131.7%
12.6.19 Finally, analysis has been performed to assess the impact of changes in interest rates. The interest rate within the current model reflects market conditions on 10 August 2005:
• UK Index 4.124% 2030 (for EIB and index-linked bonds) – 1.514%; and
• UK Gilt 4.25% 2036 (fixed rate bond) – 4.368%.
12.6.20 The financial model assumes a buffer of 25 basis points (bps) applied to each of the three bonds highlighted above. Investec, on behalf of Skanska, have modelled the impact of removing the interest rate buffer and this results in a reduction in the UC of £2.95 million. Removing the interest rate buffer increases the VfM benefit of PFI by £38 million over the lifetime of the contract.
12.6.21 An additional sensitivity has been performed to model the impact of interest rates above the buffer. In doing this it has been assumed that the tariff responds linearly to changes in the interest rate. It has therefore been assumed that a 25bps increase in interest rates will increase the UC by £2.95 million, and a 50 bps increase in interest rate will increase the UC by £5.9 million. It can be seen from the results below that the PFI solution would still be value for money.
Figure 99a – Impact of Changes in Interest Rate Description PSC NPC
(£m) PFI NPC (£m) Difference VfM
Base scenario (inclusive of 0.25% buffer)
8,815,005 8,549,261 -265,744 Yes
Interest rate with no buffer 8,815,005 8,511,646 -303,359 Yes
NB: Base Scenario: UK Index 4.125% 2030 (for EIB and I/L bonds) – 1.514%, UK Gilt 4.25% 2036 (for fixed rate bond) – 4.368%
12.7 Retained Risks 12.7.1 Following financial close, the Trust retains a number of risks during the construction
period. Appendix 12C sets out the Trust’s general approach to management of risks arising during the construction period and the steps taken to reduce retained risks since BaFO. It also identifies the time and cost provisions already included within the Trust’s affordability envelope and quantifies the risks not covered by such specific provisions. The most significant risks are summarised in this chapter. These relate to:
• Descoping risks;
• Site risks;
• Adjustments to construction costs after Phase 1 on each site;
• Design development;

Version 10.1
220
New Hospitals Programme
• Completion and commissioning;
• Non-PFI equipment; and
• The provision of ICT equipment.
12.7.2 The scale of these risks, together with the risk handling strategies are as follows:
Descoping Risks
12.7.3 Concerns have been expressed about long-term affordability of the scheme, particularly in the light of the review of NHS hospital redevelopment schemes announced as part of the NHS Operating Framework 2006/07. It was determined that affordability concerns are best addressed by achieving a reduction in the UC at financial close and then retaining greater flexibility in the final scale of buildings and physical capacity, rather than seek to achieve modifications to the scheme during the construction period.
12.7.4 A descoping UC reduction was determined and stands at £9.5m per annum. The amount was determined in agreement with the DH, to reduce the annual UC to it’s target maximum of £96.6 million (subsequently modified to £98.4 million following interest rate movements between 31st March 2006 and the date of Financial Close). Prior to the introduction of the target maximum, the annual UC totalled £113.2 million. A number of adjustments to the annual UC reduced the amount required from descoping to £9.5 million. Other adjustments included:
• Removal of the interest buffer (£2.6 million annual UC equivalent);
• Reduction in the provision for Phase 2 inflation to 3.5% (£0.7 million annual UC equivalent);
• Introduction of ODPM grant funding (£0.2 million annual UC equivalent);
• Reduction in interim FM services costs (£0.2 million annual UC equivalent);
• Reduction in UC due to scope change for MES (£3.4 million annual UC equivalent).
12.7.5 The descoped savings (£9.5 million) will be removed from the recurrent UC impact of the PFI scheme at steady state. The descoped scheme forms the basis of SI’s contractual obligations at financial close. The detail of the descoping proposals contained within the Project Agreement (PA) are set out in Appendix 12C. The Variation Schedule (Schedule 22, part 7) in the PA governs the way in which the descoping proposals will be implemented.
12.7.6 Schedule 22 Part 7 provides for a rapid assessment of the descoping proposals, with a view either to affirming them (and clarifying the consequential effects) or identifying substitutes and completing similar analysis on these, within 16 months of financial close114.
12.7.7 This work will be led by the Descoping Project Sub-Committee, which will report to the New Hospitals Investment Board. A supporting Descoping Work Group is to be established with dedicated resources assigned to it. SI has also set up its own dedicated descoping project team to work alongside the Trust’s team. The main functions of the Descoping Work Group are:
114 This work was subsequently completed to time, the original descoping proposal having been confirmed.
Version 10.1
221
New Hospitals Programme
To develop, in conjunction with SI, an activity and resource plan and associated timetable which will allow the Trust to discharge its obligations under Schedule 22 Part 7 in a way that is clinically, operationally and commercially feasible;
To complete the programme of work associated with the descoping so that BLT’s obligations, as set out in Schedule 22 Part 7, are properly discharged, in a timely fashion.
12.7.8 The descoping proposals present risks for the Trust. These risks are:
A shortfall in accommodation, with some departments now being homeless at global completion;
Planning obligations and the discharge of the conditions; and
The affordability of any necessary Rescoping to meet clinical/patient needs.
Site Risks
12.7.9 These comprise risks associated with the site and buildings being used by SI to complete the scheme. The standard contractual PFI position seeks to transfer those risks that the PFI partner has had the opportunity to survey. In some instances, the Trust has managed to transfer more site risk to SI than this standard requires. The principal site risks retained are set out below. The site risks have been assessed in Appendix 12C, which encompasses a range of scenarios with their probability. The range of values is shown in each case below. Further detail of the costs and how the risks are managed, is available in Appendix 12C.
I. Archaeological Risk (including human remains) – this risk remains with the Trust. The age of the sites suggests that this risk is significant and will need to be actively managed. The Trust has sought to interrogate this risk by conducting archaeological surveys, including a number of trial pits dug on both sites where access is available. The Museum of London Archaeological Services (MOLAS) has undertaken trial digs on both sites (the detailed reports are included at Appendix 15D). Findings show that an area at The Royal London (Bedstead Square) is estimated to contain the buried remains of up to 600 people. The impact of this has been estimated by SI as adding 14 weeks to the construction programme at The Royal London. This period has been built into the works programme. The inspection of the other principal area of interest at The Royal London (Garden Square) can be accommodated without further delay to the programme.
II. At Barts, the principal areas of interest for MOLAS are accessible only as part of Phases 2 and 3 of the construction programme. A period of one month has already been included in Phase 3 to enable an archaeological dig in the area adjacent to where Merrill Lynch discovered remnants of the old London Wall. MOLAS will retain a watching brief as the construction site is opened up, and this function has been allowed for in SI’s programme. (Range value £0 to £360k). See Appendix 12C paragraph 2.3.1 for further detail.
III. Soil Contamination – the principal retained risk relates to the identification and removal of radioactive material buried beneath the ground. The Trust has sought to interrogate this risk by conducting radioactive contamination surveys (see Appendix 15E). Surveys already conducted show that a number of radioactive benches were buried in concrete cases at Barts some decades ago. The area where these benches are located is required
Version 10.1
222
New Hospitals Programme
during Phase 3. The Trust will be able to secure access to the site and remove the contaminated benches well before SI requires the site as part of Phase 3. The potential impact on SI’s programme (and costs) therefore is low. A further five areas of radioactive interest have been located by the survey, although each of these present considerably easier obstacles than the contaminated benches.
The Trust has commissioned a more detailed survey which is being completed by a specialist radioactive material disposal company, Aurora. Aurora has reported its findings to date, which indicates no evidence of radioactive materials. There is one area left to survey, which is currently occupied. Efforts are being made to re-house staff to complete this survey by January 2007. (Range value £0 to £180k). See Appendix 12C, paragraph 2.3.3 for further detail.
IV. Asbestos –– asbestos identification and removal affects buildings that are demolished and retained. The Trust has for some years now maintained an asbestos risk register for all buildings. It has sought to interrogate the risk it is retaining through two recent updates to the register via non-intrusive surveys, the first conducted by the Trust in 2004 and the second completed by SI. SI has priced to remove the amount of asbestos recorded in the Trust’s asbestos register, unless it has been able to complete its own intrusive surveys. At financial close, SI has completed over 25% of the surveys it requires, although this equates to more than 80% of surveys required for Phase 1.
SI will complete its intrusive asbestos survey programme, either as part of the accelerated works programme, or immediately following SI securing vacant possession of the Trust’s buildings after financial close (some of which will not be handed over until the end of Phase 1). The results of surveys conducted so far, albeit on a relatively small sample (around 24%), indicate that the non-intrusive surveys are a reasonable reflection of the quantum of asbestos being found. Notwithstanding this, the Trust retains the cost risk on the net increase/decrease of actual asbestos found. The Trust and SI has agreed the asbestos baseline, the rate that will be applied to newly discovered asbestos and the methodology by which the quantum of asbestos is computed. As part of an agreed risk share package, SI has agreed to take delay risk on asbestos discovered in excess of that currently shown in the asbestos register. (Range value £63k to £378k). See Appendix 12C paragraph 2.3.4 for more detail.
V. Retained refurbished buildings – SI’s works programme involves the refurbishment of a number of the Trust’s buildings. SI’s proposals for these buildings involve a comprehensive redevelopment to the internal environment, including the replacement of all mechanical and engineering services. As many of these buildings remain occupied (until the Phase 1 works programme is completed), SI has been unable to conduct intrusive surveys on their superstructure (roofs, foundations, walls, etc.). Notwithstanding this, SI has accepted all risks (other than latent defects) relating to five of the nine retained and refurbished buildings (known as Category A buildings).
The level of risk accepted by SI in relation to the remaining four buildings (Front Block, Grocers Wing and West Wing at The Royal London and East Wing at Barts) is determined by the level of access enjoyed by SI to conduct intrusive surveys in advance of the commencement of the works associated with each building. For the East Wing at Barts (known as a Category B building for the purpose of the project agreement), the Trust is able to grant SI the access it requires to survey, well in advance of the
Version 10.1
223
New Hospitals Programme
commencement of works. SI has therefore accepted all risks other than the cost consequences that the condition of the superstructure is not as assumed. The assumptions made by SI with regard to this are explicit and set out in the project agreement. The Trust is unable to provide SI with access to conduct surveys in the other three buildings (known as Category C buildings for the purpose of the project agreement) prior to providing vacant possession. Unlike for Category A and Category B buildings, SI is therefore unable to accept either the time or cost consequences in the event that, following the completion of surveys, its assumptions relating to superstructure are proved incorrect.
A baseline set of assumptions relating to the condition of the superstructure of Category B and Category C buildings has been established and is included in the project agreement. An agreed survey programme will be used to validate only these assumptions. Changes to condition, other than those set out in the assumptions, will be SI’s risk. The Trust bears the risk that the surveys show the assumptions to be incorrect. If there is a capital cost impact and this is so material that Project Co. is unable to proceed, then a variation to the Trust's requirements will need to be made. Given the potentially high cost impact of delay, the project agreement allows for the Trust to pre-fund the capital cost impact of a change in the Trust’s requirements which would fall to be treated as a Trust works variation. If not required for their principle purpose (i.e. to fund CCI in excess of 3.5%), committed CCI variation bonds (totalling £80m) can be used to fund the capital cost impact of the assumptions proving to be incorrect. The project agreement also places a reasonable endeavours obligation on SI to issue uncommitted variation bonds to cover such costs if not funded from committed variation bonds, up to the limit of the pool of uncommitted variation bonds (i.e. £100m). Where (committed or uncommitted) variation bonds are issued, the project agreement provides that they can be used to repay the amount pre-funded by the Trust where this has taken place. Similar provisions apply also to Trust works variation arising as a result of other Trust risks crystallising in relation to site risks (such as asbestos and soil contamination) and the completion and commissioning programme.
The Trust and SI have examined contingency plans aimed at reducing the cost of Category B and Category C buildings should material risks crystallise following the completion of intrusive surveys. These involve relatively minor reductions to the Trust’s requirements for these buildings, but which would reduce capital costs by around £6 million.
• Once the survey programme is complete and SI’s proposals (modified or not in the light of these proposals) are accepted, then SI will accept all risk other than for latent defects (i.e. from this point in time all Category B and Category C buildings are treated similarly to Category A buildings). (Range value £0 - £300k). See Appendix 12C, paragraph 2.3.5 for more detail.
• VI. Latent defects - First, latent defects risk has been defined as “that which cannot be discovered from surveys competently carried out” (i.e. the risk that a risk was discoverable remains with SI). Second, if a latent defect is discovered during the works to the retained refurbished buildings, then this gives rise to a compensation event. If the impact of the latent defect is so material that Project Co. is unable to proceed, then a variation to the Trust's requirements will be made. As following the completion of Phase 1, the PA allows for the Phase 2 buildings to give rise to their own UC, the impact of delay is limited to individual buildings (and not the whole phase). The Trust has completed a ”hypothetical“ descoping exercise on the retained refurbished buildings that could be deployed in the event that latent defects are discovered during the works period. Latent defects (but only in the
Version 10.1
224
New Hospitals Programme
superstructure) that come to light following the works period remain a Trust risk.
• Given its remoteness in time, no specific risk mitigation measures have been put in place to address this element of latent defect risk. Typically, it is not NHS policy to create general provisions to set against unforeseeable and remote risks (e.g. backlog maintenance).
Post-Phase 1 Construction Costs
12.7.10 SI has provided a fixed price construction contract for the whole construction period except that, in relation to Phase 2 and Phase 3, SI’s construction costs can be adjusted to take account of construction cost inflation and change in law. Transferring these risks to the private sector was both practically difficult (i.e. there was little or no appetite from the private sector) and judged to be poor value for money. As neither of these risks would be capable of being transferred under the PSC, neither reflects risks to the Trust that would be avoidable using alternative procurement routes.
■ Construction Cost Inflation - the Trust retains risk of construction cost inflation (CCI) applied to post-Phase 1 construction costs. The risk relates to the indexation of Phase 2 and Phase 3 construction costs in line with the Davis Landon buildings cost index. For affordability purposes, the Trust has allowed an annual uplift of 3.5% (an increase from 3% on the index set during the competition) (which takes account of the impact of the 2012 Olympics). In broad terms a 0.25% increase/decrease in the Davis Langdon buildings cost index would lead to a change in the unitary charge of £400,000. The Trust’s advisers (who also happen to be Davis Langdon) have indicated that the 3.5% per annum represents a robust estimate of the level of inflation over the relevant period, i.e. 3.5% per annum would represent a central estimate (see Appendix 15C). The initial funding level and the unitary charge presume that CCI will run at 3.5%. To the extent that CCI actually falls below 3.5% and, together with any associated change in law liabilities, the Project proves to be over-funded, the project agreement provides mechanisms for the Trust to ”claw back“ the economic benefit. If CCI exceeds 3.5%, Project Co. has committed construction variation bonds totalling £90 million (providing headroom equivalent to CCI running at 6.5%) In the unlikely circumstances that CCI exceeds 6.5%, the Trust will need to make a call on the pool of uncommitted variation bonds, which totals £50m.
■ Change in Law - SI’s Phase 2 and Phase 3 construction cost can be adjusted by changes in law that are not currently reasonably foreseeable, or which can be foreseen as Phase 2 or Phase 3 approach. The proportion of the construction costs subject to this adjustment is 33%. SI will inform the Trust of any adjustment driven by change in law six months in advance of embarking on later phases at each site. If, and when, an adjustment is agreed (which is subject to the disputes resolution procedure) then the construction price for the relevant phase and site is fixed.
Completion and Commissioning
12.7.11 SI has produced a detailed programme of works by site and by phase. The programme further breaks down the phases into a number of sections on each site. The purpose of the sectional approach is to allow the Trust to conduct its pre-completion commissioning in a staggered way. Pre-completion commissioning activities by the Trust include the installation and testing of equipment and ICT and training and orientation programmes for the Trust’s operational staff. The Trust has completed its own programme of moves (including decanting, decommissioning and handover of vacated buildings) that dovetails with SI’s works programme. The
Version 10.1
225
New Hospitals Programme
management and implementation of operational aspects of the Trust’s transfer, decommissioning and building vacation programme will be undertaken by the Trust’s Director of Operations and be overseen by the New Hospitals Programme Board. Three elements of the programme stand out currently as presenting operational risks to the Trust. These are:
The installation of equipment to be provided by Siemens, elements of which are ring-fenced;
The procurement and installation of medical and non-medical equipment not installed by SI; and
The procurement and installation of ICT equipment.
Design Development Programme
12.7.12 In many PFI schemes, there remains considerable risk that the cost of the preferred design solution increases prior to the commencement of works. This risk presents typically through the detailed design development process, much of which can still be outstanding following financial close. The Trust and SI will complete 95% sign-off of all clinical areas at the 1:50s level on each site by financial close. The 95% figure includes all complex areas, e.g. theatres, ITU and Clinical Physics, with generic areas such as non-specialist outpatients within the remaining 5%. In addition to this, 100% of 1:200s (in clinical and non-clinical areas) will be complete and signed-off as will 100% of all room data sheets. This is a substantially higher figure than is typically seen on PFI schemes and acts to reduce the risk substantially that changes in the Trust’s requirements or in SI’s design will lead to unforeseen cost pressures. The Trust and SI agreed a programme that will achieve the sign-off of the remaining 5% of clinical 1:50s within two months of financial close. This programme is now complete and 100% of areas are signed off at 1:50 (B status). This forms part of the reviewable design data process as set out in the project agreement.
MES Equipment
12.7.13 The contractual ring-fencing of the managed equipment service results in some element of project completion risks remaining with the Trust. The main consequence is that the building may be completed but not be occupied by the Trust due to the late installation of equipment.
12.7.14 In these circumstances, while the MES provider (Siemens) is not paid, the unitary charge in relation to the building commences. The Trust faces double-running costs on a new (but unoccupiable) building, as well as supporting the estate which it is due to vacate. In the Trust’s case, the impact of this risk is compounded by the delay on vacant possession of buildings in Phase 2.
12.7.15 The Trust and its advisers have completed analyses that indicate that the clinical occupation of new clinical facilities will be achievable if a relatively small number of significant pieces of equipment are installed. The main pieces of equipment are to be installed in advance of the Trust taking occupation (for example, a minimum buffer of three weeks applies to all imaging equipment).
12.7.16 The principal risk identified by the Trust’s advisers is that the building is not adequately complete for Siemens to commence its installation work, yet practical completion has taken place. However, completion tests conducted by the Independent Tester are to include state of readiness tests for the installation of MES. Equally, the interface agreement between Siemens and Skanska Construction gives Siemens access, inspection and sign-off rights prior to it accepting the building for its installation work. These contractual rights should act
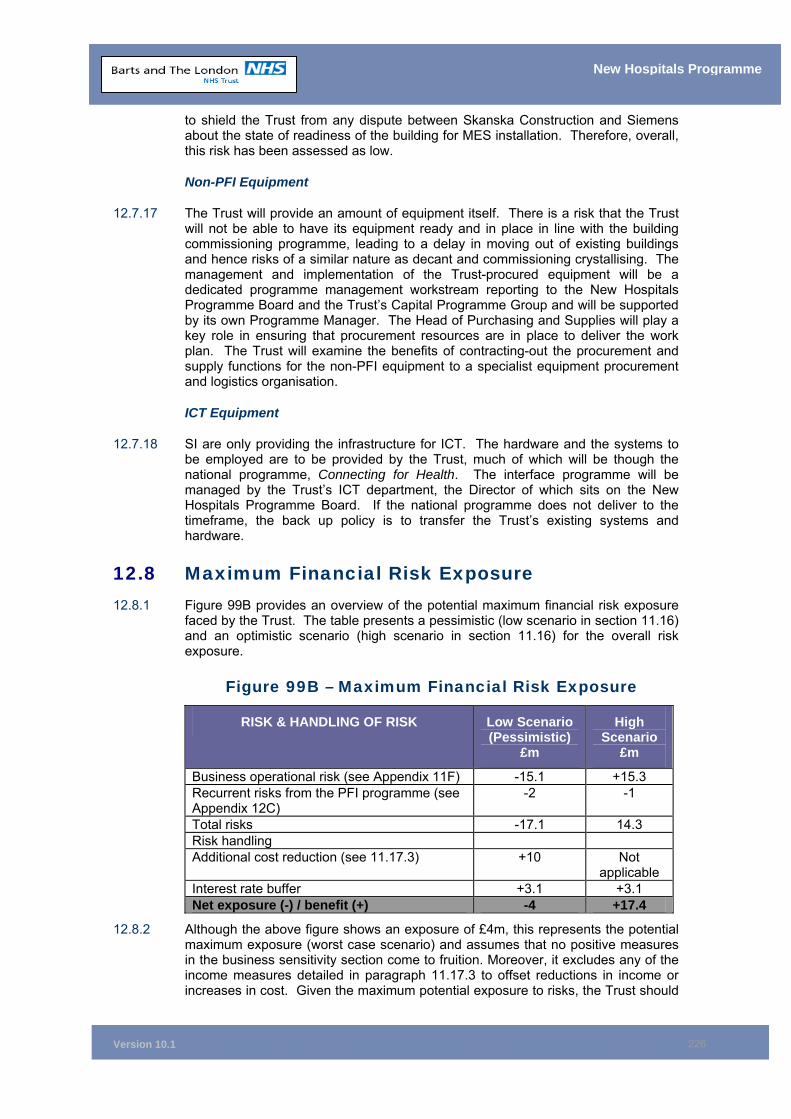
Version 10.1
226
New Hospitals Programme
to shield the Trust from any dispute between Skanska Construction and Siemens about the state of readiness of the building for MES installation. Therefore, overall, this risk has been assessed as low.
Non-PFI Equipment
12.7.17 The Trust will provide an amount of equipment itself. There is a risk that the Trust will not be able to have its equipment ready and in place in line with the building commissioning programme, leading to a delay in moving out of existing buildings and hence risks of a similar nature as decant and commissioning crystallising. The management and implementation of the Trust-procured equipment will be a dedicated programme management workstream reporting to the New Hospitals Programme Board and the Trust’s Capital Programme Group and will be supported by its own Programme Manager. The Head of Purchasing and Supplies will play a key role in ensuring that procurement resources are in place to deliver the work plan. The Trust will examine the benefits of contracting-out the procurement and supply functions for the non-PFI equipment to a specialist equipment procurement and logistics organisation.
ICT Equipment
12.7.18 SI are only providing the infrastructure for ICT. The hardware and the systems to be employed are to be provided by the Trust, much of which will be though the national programme, Connecting for Health. The interface programme will be managed by the Trust’s ICT department, the Director of which sits on the New Hospitals Programme Board. If the national programme does not deliver to the timeframe, the back up policy is to transfer the Trust’s existing systems and hardware.
12.8 Maximum Financial Risk Exposure 12.8.1 Figure 99B provides an overview of the potential maximum financial risk exposure
faced by the Trust. The table presents a pessimistic (low scenario in section 11.16) and an optimistic scenario (high scenario in section 11.16) for the overall risk exposure.
Figure 99B – Maximum Financial Risk Exposure
RISK & HANDLING OF RISK Low Scenario (Pessimistic)
£m
High Scenario
£m
Business operational risk (see Appendix 11F) -15.1 +15.3 Recurrent risks from the PFI programme (see Appendix 12C)
-2 -1
Total risks -17.1 14.3 Risk handling Additional cost reduction (see 11.17.3) +10 Not
applicable Interest rate buffer +3.1 +3.1 Net exposure (-) / benefit (+) -4 +17.4
12.8.2 Although the above figure shows an exposure of £4m, this represents the potential maximum exposure (worst case scenario) and assumes that no positive measures in the business sensitivity section come to fruition. Moreover, it excludes any of the income measures detailed in paragraph 11.17.3 to offset reductions in income or increases in cost. Given the maximum potential exposure to risks, the Trust should
Version 10.1
227
New Hospitals Programme
be able to adequately handle the likely degree of risks. This gives assurance that the Trust can manage potential variations to both the planned activity and income modelling agreed with PCTs and to the unitary charge from risks of delay (recurrent risks).
12.9 Chapter Conclusion 12.9.1 All risks have been identified and, where appropriate, costed and transferred to the
PFI provider. The PFI solution represents VfM compared to the PSC.
12.9.2 Robust systems are in place for the ongoing identification and management of risk.
12.10 Chapter Appendices 12A Risk Register 12B Risk Matrix and Evaluation Methodology 12C Construction Period Risks and Risk Management
Version 10.1
228
New Hospitals Programme
13 EQUIPMENT Synopsis – Equipment
This chapter shows that:
• Skanska Innisfree will be responsible for provision and the installation of all equipment that impacts on the design and construction, including imaging and radiotherapy equipment;
• Project Co. will provide a managed equipment service (MES) for major medical equipment; and
• The Trust will manage the procurement of all other medical and non-medical equipment.
13.1 Introduction 13.1.1 This chapter provides details of the Trust’s solution for the provision and
management of equipment within the context of the redevelopment of the hospitals. It sets out the following:
• The equipment included in the PFI and how it will be provided and managed;
• The equipment outside the scope of the PFI and how it will be provided and managed;
• How it is intended to fund that equipment which is not included in the PFI; and
• The changes made to the provision of equipment to meet the DH and Treasury approval requirements and thereby demonstrate that the Trust has an affordable scheme in the long term.
13.2 Trust Approach to Equipment Introduction
13.2.1 The Trust envisaged that, as part of the redevelopment, there would be considerable investment in new equipment and that existing equipment (with a useful remaining life) would be transferred to new and refurbished areas. The funding of the equipment and its timely replacement for new or updated technology, is key to the delivery of clinical services. Securing a value for money solution for the provision of this equipment has been a critical element throughout the development and procurement of the New Hospitals Project.
13.2.2 As there is no standard model for the provision of equipment for PFI schemes, the Trust identified its own strategy for the provision and maintenance of equipment for the redevelopment. This strategy seeks, where possible, to pass the risk to Skanska Innisfree for:
• Provision of major medical equipment; and
• Coordinating the supply and installation of certain other categories of equipment.
13.2.3 Evidence from other PFI projects indicated that there were limited numbers of providers who could manage and provide value for money on a wide ranging equipment portfolio within a PFI consortium. In particular, the supply of medical equipment is a less mature element of the PFI market, as most medical equipment
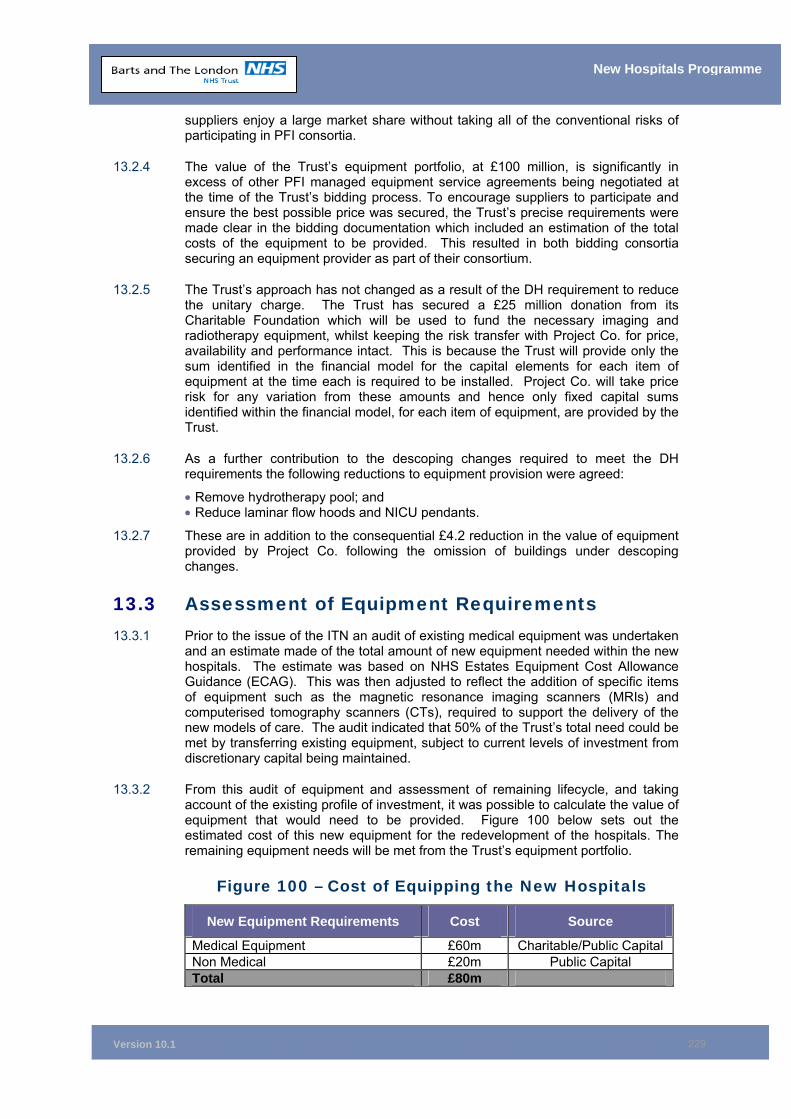
Version 10.1
229
New Hospitals Programme
suppliers enjoy a large market share without taking all of the conventional risks of participating in PFI consortia.
13.2.4 The value of the Trust’s equipment portfolio, at £100 million, is significantly in excess of other PFI managed equipment service agreements being negotiated at the time of the Trust’s bidding process. To encourage suppliers to participate and ensure the best possible price was secured, the Trust’s precise requirements were made clear in the bidding documentation which included an estimation of the total costs of the equipment to be provided. This resulted in both bidding consortia securing an equipment provider as part of their consortium.
13.2.5 The Trust’s approach has not changed as a result of the DH requirement to reduce the unitary charge. The Trust has secured a £25 million donation from its Charitable Foundation which will be used to fund the necessary imaging and radiotherapy equipment, whilst keeping the risk transfer with Project Co. for price, availability and performance intact. This is because the Trust will provide only the sum identified in the financial model for the capital elements for each item of equipment at the time each is required to be installed. Project Co. will take price risk for any variation from these amounts and hence only fixed capital sums identified within the financial model, for each item of equipment, are provided by the Trust.
13.2.6 As a further contribution to the descoping changes required to meet the DH requirements the following reductions to equipment provision were agreed:
• Remove hydrotherapy pool; and • Reduce laminar flow hoods and NICU pendants.
13.2.7 These are in addition to the consequential £4.2 reduction in the value of equipment provided by Project Co. following the omission of buildings under descoping changes.
13.3 Assessment of Equipment Requirements 13.3.1 Prior to the issue of the ITN an audit of existing medical equipment was undertaken
and an estimate made of the total amount of new equipment needed within the new hospitals. The estimate was based on NHS Estates Equipment Cost Allowance Guidance (ECAG). This was then adjusted to reflect the addition of specific items of equipment such as the magnetic resonance imaging scanners (MRIs) and computerised tomography scanners (CTs), required to support the delivery of the new models of care. The audit indicated that 50% of the Trust’s total need could be met by transferring existing equipment, subject to current levels of investment from discretionary capital being maintained.
13.3.2 From this audit of equipment and assessment of remaining lifecycle, and taking account of the existing profile of investment, it was possible to calculate the value of equipment that would need to be provided. Figure 100 below sets out the estimated cost of this new equipment for the redevelopment of the hospitals. The remaining equipment needs will be met from the Trust’s equipment portfolio.
Figure 100 – Cost of Equipping the New Hospitals
New Equipment Requirements Cost Source
Medical Equipment £60m Charitable/Public Capital Non Medical £20m Public Capital Total £80m
Version 10.1
230
New Hospitals Programme
13.3.3 In the run up to financial close, the Trust’s equipment portfolio was regularly reviewed and adjusted to reflect changes. The list of equipment that needs to be procured is being continually updated and adjusted with the development of the detailed design on a room-by-room basis and any subsequent changes to the clinical requirements to deliver the models of care. The adjustments to date have resulted in a unitary charge reduction of £732k per annum. The main two changes have been:
• Changes to specification for Linear Accelerators; and
• Reduction in provision for Planar X-ray imaging rooms and specification changes.
13.3.4 These changes were enhanced by the optimisation of lifecycles for each modality and the Trust providing some durables.
13.4 Procurement Options The Preferred Solution
13.4.1 The Trust’s aim to secure the best value for money for equipment and transfer maximum risk was achieved at BaFO, with the acceptance of the proposal that Skanska Innisfree would provide:
• A range of equipment that primarily has an impact on design and build; and
• A managed equipment service for all major imaging and radiotherapy equipment.
13.4.2 Affordability has now been further enhanced through securing a £25 million donation from the Charitable Foundation which has been used to fund the major imaging and radiotherapy equipment, thus securing a significant reduction to the annual UC.
Equipment Categorisation
13.4.3 The Trust has a clear and unambiguous approach to equipment through the use of bespoke categories to describe the Trust's and Project Co.’s responsibilities for the provision and maintenance of equipment. The categorisation, detailed in Figure 101, ensures clarity in relation to the range of equipment needed and individual responsibilities to provide and maintain equipment. Commissioning risk is in accordance with the definitions identified in Figure 97 and handling strategies are summarised in section 12.9.10.
13.4.4 The only equipment not included in this categorisation is the equipment which is required for the provision of facilities management (FM) services, which are the responsibility of the service provider, and ICT equipment which is the subject of a separate CRS business case.
13.4.5 Equipment identified as Category, T. MT and D is to be supplied by the Trust, with details of its procurement further described in the Trust Supplied Equipment Business Case (see Appendix 13B).
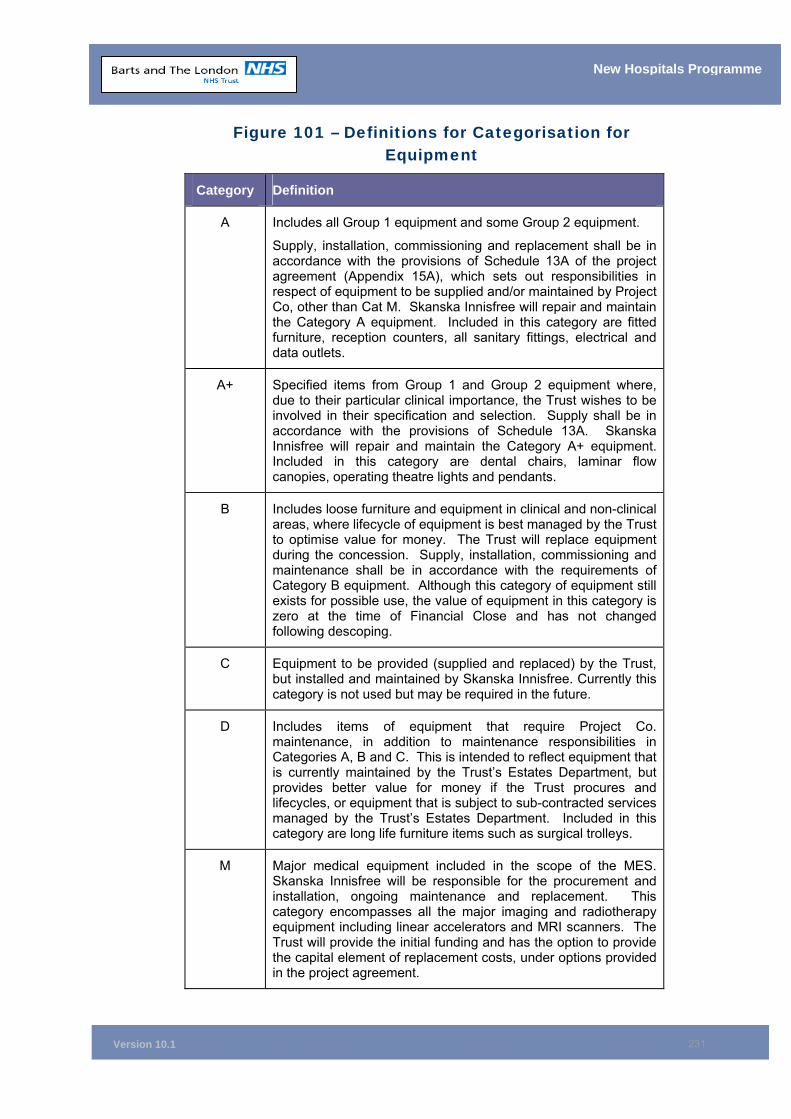
Version 10.1
231
New Hospitals Programme
Figure 101 – Definitions for Categorisation for Equipment
Category Definition
A Includes all Group 1 equipment and some Group 2 equipment.
Supply, installation, commissioning and replacement shall be in accordance with the provisions of Schedule 13A of the project agreement (Appendix 15A), which sets out responsibilities in respect of equipment to be supplied and/or maintained by Project Co, other than Cat M. Skanska Innisfree will repair and maintain the Category A equipment. Included in this category are fitted furniture, reception counters, all sanitary fittings, electrical and data outlets.
A+ Specified items from Group 1 and Group 2 equipment where, due to their particular clinical importance, the Trust wishes to be involved in their specification and selection. Supply shall be in accordance with the provisions of Schedule 13A. Skanska Innisfree will repair and maintain the Category A+ equipment. Included in this category are dental chairs, laminar flow canopies, operating theatre lights and pendants.
B Includes loose furniture and equipment in clinical and non-clinical areas, where lifecycle of equipment is best managed by the Trust to optimise value for money. The Trust will replace equipment during the concession. Supply, installation, commissioning and maintenance shall be in accordance with the requirements of Category B equipment. Although this category of equipment still exists for possible use, the value of equipment in this category is zero at the time of Financial Close and has not changed following descoping.
C Equipment to be provided (supplied and replaced) by the Trust, but installed and maintained by Skanska Innisfree. Currently this category is not used but may be required in the future.
D Includes items of equipment that require Project Co. maintenance, in addition to maintenance responsibilities in Categories A, B and C. This is intended to reflect equipment that is currently maintained by the Trust’s Estates Department, but provides better value for money if the Trust procures and lifecycles, or equipment that is subject to sub-contracted services managed by the Trust’s Estates Department. Included in this category are long life furniture items such as surgical trolleys.
M Major medical equipment included in the scope of the MES. Skanska Innisfree will be responsible for the procurement and installation, ongoing maintenance and replacement. This category encompasses all the major imaging and radiotherapy equipment including linear accelerators and MRI scanners. The Trust will provide the initial funding and has the option to provide the capital element of replacement costs, under options provided in the project agreement.
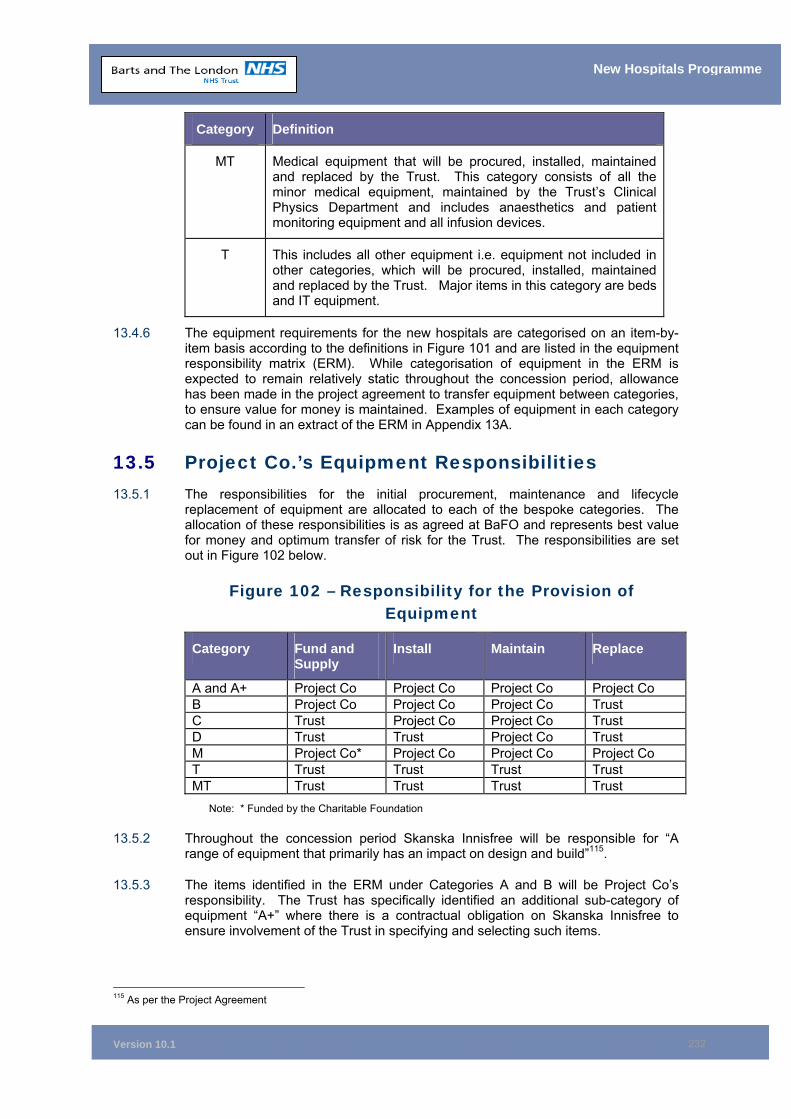
Version 10.1
232
New Hospitals Programme
Category Definition
MT Medical equipment that will be procured, installed, maintained and replaced by the Trust. This category consists of all the minor medical equipment, maintained by the Trust’s Clinical Physics Department and includes anaesthetics and patient monitoring equipment and all infusion devices.
T This includes all other equipment i.e. equipment not included in other categories, which will be procured, installed, maintained and replaced by the Trust. Major items in this category are beds and IT equipment.
13.4.6 The equipment requirements for the new hospitals are categorised on an item-by-item basis according to the definitions in Figure 101 and are listed in the equipment responsibility matrix (ERM). While categorisation of equipment in the ERM is expected to remain relatively static throughout the concession period, allowance has been made in the project agreement to transfer equipment between categories, to ensure value for money is maintained. Examples of equipment in each category can be found in an extract of the ERM in Appendix 13A.
13.5 Project Co.’s Equipment Responsibilities 13.5.1 The responsibilities for the initial procurement, maintenance and lifecycle
replacement of equipment are allocated to each of the bespoke categories. The allocation of these responsibilities is as agreed at BaFO and represents best value for money and optimum transfer of risk for the Trust. The responsibilities are set out in Figure 102 below.
Figure 102 – Responsibility for the Provision of Equipment
Category Fund and Supply
Install Maintain Replace
A and A+ Project Co Project Co Project Co Project Co B Project Co Project Co Project Co Trust C Trust Project Co Project Co Trust D Trust Trust Project Co Trust M Project Co* Project Co Project Co Project Co T Trust Trust Trust Trust MT Trust Trust Trust Trust
Note: * Funded by the Charitable Foundation
13.5.2 Throughout the concession period Skanska Innisfree will be responsible for “A range of equipment that primarily has an impact on design and build”115.
13.5.3 The items identified in the ERM under Categories A and B will be Project Co’s responsibility. The Trust has specifically identified an additional sub-category of equipment “A+” where there is a contractual obligation on Skanska Innisfree to ensure involvement of the Trust in specifying and selecting such items.
115 As per the Project Agreement
Version 10.1
233
New Hospitals Programme
13.5.4 As an example, the A + Category equipment will include theatre pendants, theatre lighting and canopies, dental chairs and sterilisers. These items of equipment sit at the interface of clinical services and therefore the clinical body should be able to influence the choice of equipment. However, their installation, their maintenance and their replacement are integral to the way the building works and therefore Skanska Innisfree retains primary responsibility for them. All other items will be procured by Skanska Innisfree with minimal input from the Trust and installed as part of the construction programme.
13.5.5 Project Co. will also equip, maintain and provide ongoing replacement of specific items of medical equipment to the Trust through the MES. The equipment included within the MES is specifically identified as Category M in Appendix 13A.
13.6 The Managed Equipment Service Overview
13.6.1 The MES will commence in full on completion of Phase 1 of the construction programme in 2009/10 with Project Co. (Siemens) being responsible for:
• The initial procurement of major medical equipment for the new hospitals;
• The initial transfer of major medical legacy equipment as agreed with the Trust;
• Replacement of all equipment included within the service, according to an agreed equipment replacement plan;
• Equivalency at the point of replacement, such that equipment is replaced with like equipment that incorporates all standard features available at the time;
• Maintenance of all equipment included within the service; and
• Updates and upgrades where these are provided by the equipment manufacturer within comprehensive service contract arrangements to their normal customer base.
13.6.2 Following the changes introduced in March 2006, an additional option for the Trust to provide the capital element of the replacement costs for the equipment included in the MES was also agreed. Under these revised funding options all of the elements of risk transfer and service delivery identified above, and further described in the following paragraphs, will remain in place.
13.6.3 The length of the concession will be 35 years, with market testing at 15 and 25 years. Market testing is set to take place at these intervals to reflect the considerable level of capital expenditure by Siemens in the first 4 to 5 years of the contract. The interval to the first market test was determined so as to allow Siemens an approximate period of 10 years of “full” service delivery, by which time lifecycle replacement of key items of equipment will have taken place, Market testing at these intervals also provides the Trust with a period of operational continuity following the initial capital investment. Ten years has become an acceptable precedent for market testing an MES service where there is a large capital investment. The level of capital investment differentiates the MES from more orthodox FM services.
13.6.4 In order to maximise the reduction in unitary charge arising from the £25 million donation from the Charitable Foundation, a step up in unitary charge was introduced at year 15 (2025). A value for money MES after this period is ensured by the Trust having the right to instigate a market test after 15 years.
Version 10.1
234
New Hospitals Programme
13.6.5 The Trust also has the right to revert to Project Co. funding the equipment requirement (initial tranche and replacement) at any time prior to two years post-financial close.
MES Service Provider
13.6.6 Siemens Healthcare Services (SHS) is Project Co’s service provider, who will provide the MES. SHS has experience of providing these services in the acute sector of the NHS and is considered to be of sufficient size and experience to provide the service to the Trust. SHS’s experience includes five PFI contracts for the provision of equipment/managed equipment service, which range from total asset management to the provision of specialised imaging equipment.
Benefits of the MES
13.6.7 The SHS proposal provides significant benefits to the Trust in terms of risk transfer for a relatively small number of high value items of medical equipment. SHS will be required to initially equip the new hospitals to pre-defined specifications and to maintain agreed availability and standards of performance throughout the concession period to ensure that the Trust can meet its clinical obligations.
13.6.8 Benefits to the Trust are identified as follows:
• Substantial risk transfer on the availability of equipment;
• Substantial risk transfer on the performance of the equipment;
• Subject to the ring-fencing provisions in the project agreement (see section 15.11), the risk of coordinating the procurement, supply and installation of equipment and the build programme is passed to Project Co.;
• Project Co. is incentivised to take account of equipment requirements in the design of the hospitals, including facilitating ease of maintenance for large and fixed installation equipment; and
• Technology refresh on equipment replacement.
13.6.9 The incentive is based on the fact that costs of fitting out works and delivery into the buildings falls to Project Co. and installing and maintaining equipment falls to SHS. The scheme identifies architecturally significant equipment for which Project Co. are contractually bound to provide space, and all services, to allow the Trust to select equipment from any supplier.
Key Features of the MES
13.6.10 It is of paramount importance that the Trust is able to meet changing healthcare needs and to provide its ongoing clinical service requirements, supported by technology that is up to date, reliable and efficient. To ensure that, throughout the concession period, SHS provides the Trust with a MES that supports these requirements and continues to provide value for money, a range of criteria is agreed for the service. The key features are as follows:
Equipment Investment Committee (EIC)
The Trust has sought to retain an appropriate level of control and involvement in equipment choice through the EIC. The Trust, Skanska Innisfree and SHS will be represented on this committee and will together make equipment procurement decisions.
Supporting the EIC will be several specialist planning sub-groups whose
Version 10.1
235
New Hospitals Programme
membership will include Project Co, clinical staff and users. The planning groups will be tasked with informing the committee’s procurement decisions, preparing clinical specifications and undertaking user evaluations. These groups will make recommendations to the EIC on the most suitable equipment to meet the equipment and service specifications.
Lifecycles
SHS will replace equipment in accordance with agreed lifecycles which have been developed based on a combination of current Royal College of Radiologists’ guidelines, equipment manufacturer recommendations and Trust requirements to improve the lifecycle management of key items of diagnostic equipment.
Replacement of Equipment
SHS will replace equipment at regular intervals under a rolling capital investment programme contained within the Investment Plan and in accordance with the lifecycles agreed with the Trust. Within the Investment Plan, flexibility has been allowed to review the expected life of equipment and replacement dates so that the Trust can respond to the changing needs of its clinical services. The Trust will have the ability to flex the plan to bring forward or extend replacement, introduce new technology and withdraw items of equipment that are no longer clinically required. There will also be the flexibility to introduce charitable and other types of funding.
Technical Refreshment
SHS’s proposal is based on clinical output-based specifications, developed by the Trust for all MES equipment. These specifications will be the baseline for initial supply during the construction period and for future replacement. In the future, where there have been technological advancements that are now standard features, these will form part of the updated baseline specification. This is the basis of equivalency, e.g. where top of the range was originally specified items will be replaced by the same, including any advances and technological features. Where there is a clearly identifiable technological change above that provided by equivalency, or where the equipment is fundamentally different, the risk will remain with the Trust.
Legacy Equipment
Under the MES, SMS will be responsible for supplying Category M equipment to furnish the new hospitals. Some of this equipment will be new and some will be transferred from the old hospitals. Detailed planning regarding suitability for transfer and current lifecycles by the Trust has ensured that transferred equipment will provide value for money. SHS’s proposal is based on a list of Category M equipment, with assumptions that the Trust considers to be transferable in 2008/09. Any changes to the list of equipment arising from Trust purchases will be incorporated into a revised transfer list which will inform the financial models and changes to the cost of the service.
Payment Mechanism
A coordinated approach is established by the Trust across all FM and equipment services by the inclusion of the MES into the standard form payment mechanism. Details of the payment mechanism are in the project agreement, Schedule 18. The MES will supply equipment to the Trust. The Trust has opted for 50% compliance to Siemens product on the basis that this strikes the best balance between economy and clinical choice. The 50% compliance solution provides a degree of certainty for Siemens when pricing risk, such that choice can be achieved for the remaining 50%.
Version 10.1
236
New Hospitals Programme
Clinical Choice
The Trust’s requirements for radiotherapy equipment will be met from a single supplier nominated by the Trust 27 months prior to completion of Phase 1, in accordance with a defined programme for selection included within Project Co.’s proposals. Project Co. will ensure that the built environment does not limit the choice of equipment supplier.
Equipment Management
SHS will be responsible for the maintenance of MES equipment. Planned preventative maintenance (PPM) will be in accordance with manufacturer’s guidelines/industry norms, and to a timetable that allows the Trust to maximise clinical activity. This maintenance will be provided by SHS and will not involve the transfer of any Trust staff.
To support clinical requirements and ensure continuity of service, there will be a
first line reactive response to equipment breakdowns by on-site technical staff, directly employed by SHS.
For radiotherapy equipment where quality control and calibration services have
a direct clinical impact and cannot be disaggregated from reactive maintenance, the first line response will be provided by Trust staff, although the risk of availability remains with the nominated supplier. This service is provided under a service level agreement (SLA) with SHS, which includes a strict escalation procedure to SHS. Downtime commences when the fault is reported to the helpdesk. The full risk of availability and performance on all MES equipment, including services provided under the SLA for radiotherapy equipment, remains with SHS.
The reactive maintenance service for all MES equipment including
radiotherapy, will be fully comprehensive and be required to meet specified rectification times and a guaranteed up time.
Training
A programme will be agreed for each item of equipment as part of the selection process. SHS will provide the agreed programme at no additional cost and as part of the MES.
MES Help Desk
13.6.11 All equipment faults will be logged by Project Co.’s centralised helpdesk and automatically sent to the service provider (SHS). The reporting of faults will provide the basis for management information reports on performance and the information for the payment mechanism.
Interim Period Arrangements
13.6.12 The interim period will be from financial close up to transfer of the equipment service at the end of Phase 1 of the construction at Barts in 2009/10. The length of this period means that, in the time leading up to transfer, it will be necessary to regularly review the assumptions provided at BaFO for the initial procurement and the transferability of the equipment.
13.6.13 The Trust, together with SHS, will agree any future changes to the timing of lifecycle replacements or the introduction of new technology during the interim period for major medical and imaging equipment. The changes will be reflected in the pricing structure and therefore be subject to a change control mechanism.
Version 10.1
237
New Hospitals Programme
Maintenance of Non-Medical Equipment
13.6.14 Skanska Innisfree, through its estates services provider Skanska Rashleigh Weatherfoil (SRW), will also be responsible for the maintenance of non-medical equipment. This is currently maintained by the Trust’s Estates Department or is subject to sub-contracted services managed by the Estates Department. The Trust will be responsible for the replacement of this equipment as the short-term nature of the expected life does not warrant lifecycle replacement. These items have been separately identified as Category D and include such items as trolleys, some furniture and office equipment.
The Trust’s Equipment Responsibilities
13.6.15 In addition to the £25 million which the Trust will be providing to fund the initial tranche of MES equipment, the Trust will need to procure an estimated £30 million for the equipping of the new hospitals (see Appendix 13B Trust Supply Equipment Business Case),. This equipment is in Categories D, T and MT and throughout the concession period the Trust will be responsible for the maintenance (except Category D) and replacement of this equipment. The maintenance of Category D equipment will be undertaken by SRW.
Equipping the New Hospitals
13.6.16 New equipment will be required to equip the hospitals when they are commissioned in 2009/10. The Trust is developing a strategy for the funding of this equipment, and has considered several options to achieve this. The preferred option is for a capital funding bid to the Strategic Health Authority. Details of the supporting business case are in Appendix 13B. This separate business case has been drafted adopting the new capital funding arrangements.
Charitable Donations and NHS Initiatives
13.6.17 The Trust receives significant donations from the St Bartholomew and The Royal London Charitable Foundation to support the purchase of new and innovative medical technology. The Trust can use these future donations to purchase Trust-owned equipment or equipment provided by Skanska Innisfree through the flexible arrangements within the MES Investment Plan. Similarly, any NHS initiatives for equipment can be applied to equipment in Category M without penalty to the Trust or changing the obligations of the service provider.
13.6.18 The changes introduced following the DH requirement to reduce the unitary charge allow for the option to introduce a £25 million donation. This clearly demonstrates the flexibility provided within the MES Investment Plan.
Management of Trust Equipment
13.6.19 The Trust’s Clinical Physics Department staff and other specialist staff (such as renal technicians) will continue to provide services directly to the Trust for the management of equipment not included within the arrangements with Skanska Innisfree. Items identified in Category T (such as patient beds) will continue to be managed through current arrangements.
Lifecycle Responsibilities
13.6.20 The Trust has responsibility for the replacement of Category D, T and MT equipment, with estimated capital investment as shown in Figure 102 above. The
Version 10.1
238
New Hospitals Programme
cycle of equipment replacement will be according to the clinical requirements of the Trust.
13.6.21 Category B items will be procured and managed by Skanska Innisfree. However, replacement will be funded by the Trust as the normal lifecycle arrangements are not appropriate to the management of this type of equipment. Furniture and other non clinical equipment was initially included in this category, but was changed to Category D, as a cost saving measure prior to Financial Close.
13.6.22 Categories A, A+ and M equipment will be procured, managed and replaced by Skanska Innisfree under the terms of the project agreement.
13.7 Transfer of equipment 13.7.1 The Trust is developing an Equipment Replacement Strategy for the period leading
up to the transfer of equipment to the new hospitals. This strategy will take account of value for money, changes to clinical models of care and aspects of the design and physical location when procuring equipment during the interim period.
Trust Supplied Equipment
13.7.2 For the categories of equipment for which the Trust is solely responsible (D, T and MT), the Trust will determine the suitability for transfer by undertaking a condition survey. This will be done at an appropriate time before the items of equipment are required to be moved. To prepare for the transfer of equipment, the Trust will embark on a programme of replacement between financial close and the commencement of the MES. As these items do not require fixing into the building fabric, the survey and physical transfer will be linked to the operational phasing and decanting timetable as each service moves to the new facilities.
13.7.3 There has been an assumption that 50% (by value) of all these items will be suitable for transfer. An audit carried out by the Trust’s equipment advisers has shown that, based on current levels of spending, the Trust could reasonably expect to transfer 50%. When the final evaluation is performed, there will be a need to consider the equipment's condition and suitability for use within the new facilities. The 50% transfer assumption may not be appropriate for all items. In some categories, the transfer assumption may be lower, due to the existing equipment not being suitable for reasons of design and aesthetics. In other categories, the transfer assumption may be much higher, because of Trust investment in medical equipment. The transfer equipment will be treated as a deferred asset.
Project Co. Supply Equipment
13.7.4 It is not intended to transfer categories A, A + and B equipment to the new facilities. It is possible that the Trust will need to evaluate a small number of cases where there could be a marked financial benefit in transferring these items. However, in the period leading up to occupation of the new facilities, procurement of these items will be managed so as reduce this need to a minimum.
MES Equipment
13.7.5 Major medical equipment (Category M) required for the new facilities will be provided by a combination of new and transferred items. Assumptions on the equipment suitable for transfer have been made on the basis of current age and condition. Due to the length of the construction period, some of the items for transfer are currently Trust-owned equipment and others will be planned replacements of existing equipment. The assumptions will be reviewed in

Version 10.1
239
New Hospitals Programme
conjunction with Skanska Innisfree shortly before commencement of the MES , at the completion of Phase 1 at Barts.
13.7.6 The detailed programme of equipment installation identifies new equipment being installed before the transfer of legacy equipment. The small number (ten) of legacy items requiring uninstalling, moving, and re-installing will be moved at the end of the period for Trust decanting of services. New equipment makes up 90% of the Trust requirements for fixed equipment and will provide the level of support to allow near full clinical activity The impact of any delay in the transfer of legacy equipment is therefore unlikely to adversely affect the Trust's decanting of services.
13.8 Equipment Costs 13.8.1 The value of equipment for which the Trust is solely responsible and outside the
remit of the MES will be £30 million. This will be funded from NHS borrowing and donations and is subject to a separate business case. A copy of the business case is attached at Appendix 13B.
13.9 IT Costs 13.9.1 The Trust's IT costs are the subject of a separate business case and the benefits
have been captured in the IT business case to avoid double counting.
13.9.2 The PFI project provides the IT cabling “up to the socket'.
13.10 Chapter Conclusion 13.10.1 The measures described in this chapter will ensure that the Trust benefits from fully
equipped medical facilities for the term of the contract. Performance and lifecycle risk is passed to Skanska Innisfree for all fixed equipment, including major medical items.
13.10.2 Planned replacements of this major equipment will ensure that the Trust also benefits from technological advances in equipment supporting the clinical activity throughout this period.
13.11 Chapter Appendices 13A Examples of Equipment in Each Category 13B Outline Business Case for Trust Supply Equipment

Version 10.1
240
New Hospitals Programme
14 PROGRAMME MANAGEMENT ARRANGEMENTS Synopsis – Programme Management Arrangements
This chapter:
• Shows that the structure established to manage the scheme from post-financial close to successful completion and into the operational phase is robust;
• Details the key objectives of the programme management team, which will ensure the delivery of a successful project;
• Shows that the costs of maintaining the structure is affordable and details the funding arrangements;
• Shows that the interface with Project co./Capital Hospitals Ltd is seamless;
• Details the programme implementation plan;
• Details the governance and monitoring arrangements that have been established to ensure issues are addressed in a timely fashion; and
• Demonstrates that the agreed change control process ensures changes are captured, costed, managed and approved.
14.1 Introduction 14.1.1 This section sets out the Trust’s proposed arrangements for management of the
programme. They have changed since Financial Close, to reflect the Programme’s ongoing requirements, and will be regularly reviewed to ensure the programme proceeds smoothly through the build and procurement phase to completion in 2015 and post-programme/project evaluation.
14.1.2 This Chapter covers:
• Objectives for the implementation phase;
• Project management milestones;
• Programme management structure;
• Programme implementation (team) structure;
• Roles and responsibilities;
• Programme management costs;
• Control arrangements;
• The interface with Capital Hospitals and the Service Providers; and
• The programme implementation plan.
14.1.3 This chapter will act as a reference point against which the Programme Board and Trust Board will audit and evaluate progress.

Version 10.1
241
New Hospitals Programme
14.2 Objectives for the Implementation Phase 14.2.1 Key objectives have been identified from the implementation of the project to
completion. Figure 103 below sets out the general, construction, change management, service transformation and operational objectives for the programme.
Figure 103 - Objectives for the Project Implementation Phase
General Objectives
1 To successfully build and maintain joint partnerships between the Trust and Capital Hospitals, their constructors and service providers.
2 To maintain a clear audit trail of all decisions (changes to output specs, etc.).
3 To keep internal and external stakeholders informed of progress in all aspects of the programme by the most appropriate means.
Construction and Commissioning
4 Ensure the Trust meets it contractual obligations. 5 To successfully manage the decanting and commissioning process
without compromising the day-to-day activities of the Trust. 6 To move departments/services once only, wherever possible. 7 To minimise the disruption and inconvenience factors for staff, patients
and our neighbours.
Change Management and Service Transformation
8 Seamless progression through the main stages of the construction/ decanting and commissioning programme
9 To achieve successful implementation of the HR change management programme and the introduction of new models of care.
10 Maintenance of service standards throughout the mobilisation period. 11 To ensure an integrated approach to delivery of services. 12 To ensure service continuity and certainty at all times. 13 To ensure benefits are realised.
Operational
14 Monitor overall project performance. 15 Ensure key stakeholders are fully informed of progress and issues. 16 Share the learning experience with other Trust PFI schemes.
14.2.2 Achieving these objectives will be the main focus of the Programme Management Team.
14.3 Project Management Milestones -Timetable to Completion
14.3.1 The project has a number of distinct phases (milestones) from financial close to full commissioning and completion. These are set out in Figure 104 below.
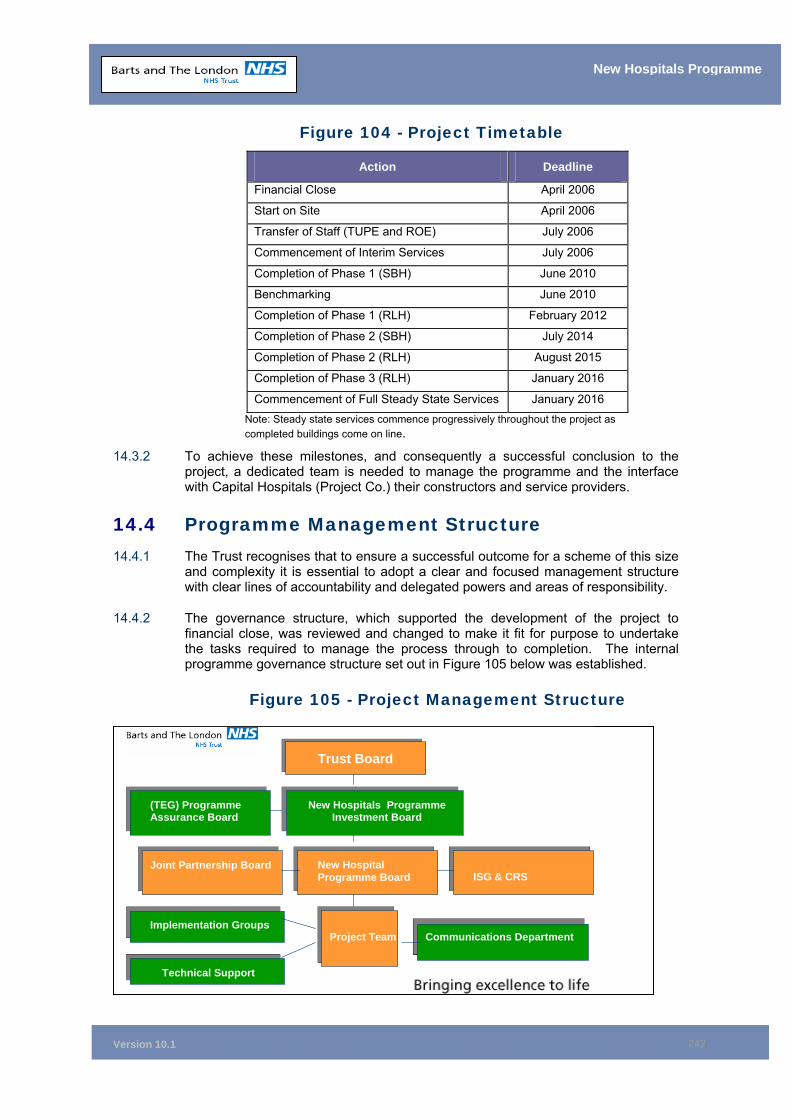
Version 10.1
242
New Hospitals Programme
Figure 104 - Project Timetable
Action Deadline
Financial Close April 2006
Start on Site April 2006
Transfer of Staff (TUPE and ROE) July 2006
Commencement of Interim Services July 2006
Completion of Phase 1 (SBH) June 2010
Benchmarking June 2010
Completion of Phase 1 (RLH) February 2012
Completion of Phase 2 (SBH) July 2014
Completion of Phase 2 (RLH) August 2015
Completion of Phase 3 (RLH) January 2016
Commencement of Full Steady State Services January 2016 Note: Steady state services commence progressively throughout the project as completed buildings come on line.
14.3.2 To achieve these milestones, and consequently a successful conclusion to the project, a dedicated team is needed to manage the programme and the interface with Capital Hospitals (Project Co.) their constructors and service providers.
14.4 Programme Management Structure 14.4.1 The Trust recognises that to ensure a successful outcome for a scheme of this size
and complexity it is essential to adopt a clear and focused management structure with clear lines of accountability and delegated powers and areas of responsibility.
14.4.2 The governance structure, which supported the development of the project to financial close, was reviewed and changed to make it fit for purpose to undertake the tasks required to manage the process through to completion. The internal programme governance structure set out in Figure 105 below was established.
Figure 105 - Project Management Structure
Trust Board
New Hospitals Programme Investment Board
(TEG) Programme(TEG) Programme Assurance Board
ISG & CRSNew Hospital Programme Board
Joint Partnership Board
Implementation Groups
Technical Support
Project Team Communications Department
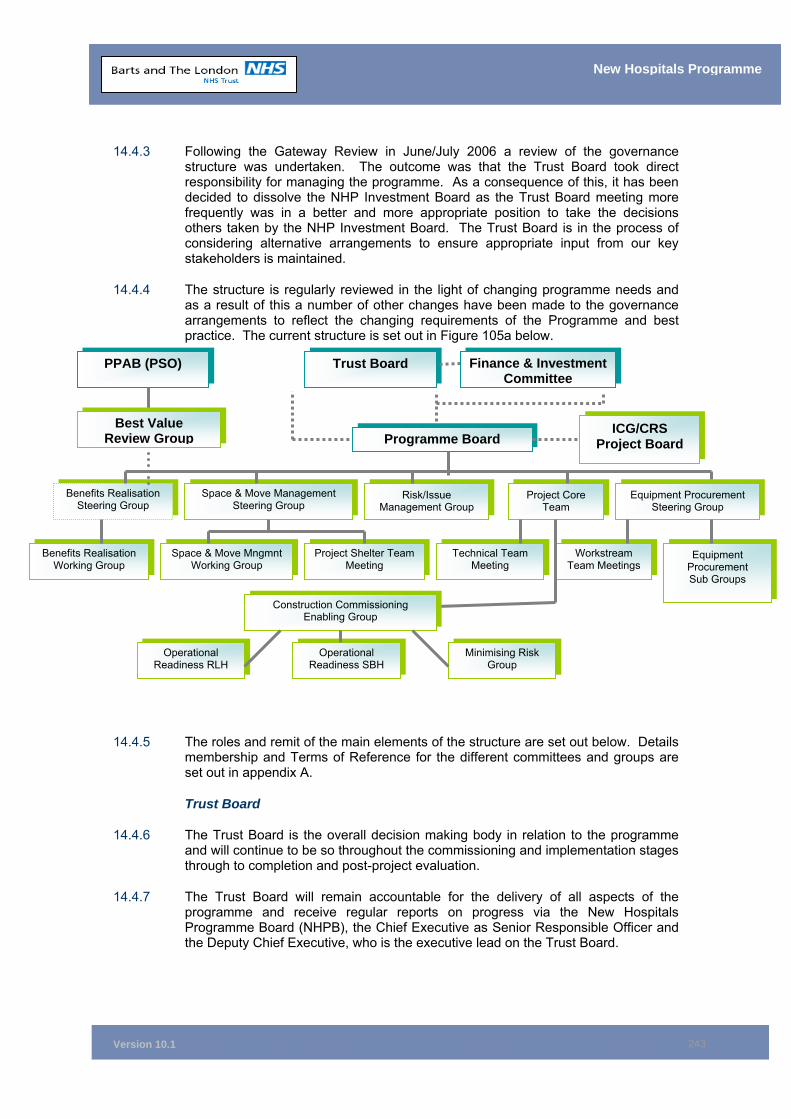
Version 10.1
243
New Hospitals Programme
14.4.3 Following the Gateway Review in June/July 2006 a review of the governance structure was undertaken. The outcome was that the Trust Board took direct responsibility for managing the programme. As a consequence of this, it has been decided to dissolve the NHP Investment Board as the Trust Board meeting more frequently was in a better and more appropriate position to take the decisions others taken by the NHP Investment Board. The Trust Board is in the process of considering alternative arrangements to ensure appropriate input from our key stakeholders is maintained.
14.4.4 The structure is regularly reviewed in the light of changing programme needs and as a result of this a number of other changes have been made to the governance arrangements to reflect the changing requirements of the Programme and best practice. The current structure is set out in Figure 105a below.
14.4.5 The roles and remit of the main elements of the structure are set out below. Details membership and Terms of Reference for the different committees and groups are set out in appendix A.
Trust Board
14.4.6 The Trust Board is the overall decision making body in relation to the programme and will continue to be so throughout the commissioning and implementation stages through to completion and post-project evaluation.
14.4.7 The Trust Board will remain accountable for the delivery of all aspects of the programme and receive regular reports on progress via the New Hospitals Programme Board (NHPB), the Chief Executive as Senior Responsible Officer and the Deputy Chief Executive, who is the executive lead on the Trust Board.
Trust Board Finance & Investment Committee
Programme Board ICG/CRS
Project Board
PPAB (PSO)
Best Value Review Group
Risk/Issue Management Group
Space & Move Management Steering Group
Benefits Realisation Steering Group
Project Core Team
Equipment Procurement Steering Group
Benefits Realisation Working Group
Space & Move Mngmnt Working Group
Project Shelter Team Meeting
Equipment Procurement Sub Groups
Technical Team Meeting
Workstream Team Meetings
Construction Commissioning Enabling Group
Operational Readiness RLH
Operational Readiness SBH
Minimising Risk Group
Version 10.1
244
New Hospitals Programme
Pathfinder Programme Assurance Board
14.4.8 The Trust Executive Group has established a Pathfinder Programme Assurance Board (PPAB) to monitor the delivery and to quality assure all major programmes and projects within the Trust, and to ensure that all are working towards delivery of the Trust’s strategic objectives. One of the most important objectives is delivery of the Trust’s Pathfinder five year clinical strategy. Pathfinder aims to achieve excellence in:
• Clinical quality;
• Service efficiency; and
• Patient experience.
14.4.9 Delivery of the New Hospitals Project is a major element of achieving Pathfinder.
14.4.10 PPAB, which is chaired by the Trust's Chief executive and attended by all the corporate directors, is responsible for:
• Oversight and coordination of the various Project Boards and Senior Responsible Officers (SROs) of the projects;
• Cross-Trust project quality assurance and coordination;
• Setting a common strategic framework for all programmes/projects;
• Compliance with programme/project control standards;
• Setting quality assurance standards for programmes/projects; and
• Specifying mandatory documentation standards, etc.
14.4.11 Thus, the role of PPAB is to ensure that there are no “gaps” and that all the individual projects/programmes deliver the expected benefits. This board will commission new work to ensure the coordinated delivery of whole Trust benefits from development activity. The Board will also approve the scope of new programmes/projects (including their deliverables and milestones) and consider the interface with other projects/programmes.
14.4.12 PPAB receive a copy of the monthly Trust Board Report and New Hospital Programme highlight reports, which includes updates on costs, issues, risks and product completion.
The New Hospitals Programme Board (NHPB)
14.4.13 The Programme Board is the body that has direct responsibility for overseeing the management of all aspects of the redevelopment of Barts and The Royal London Hospitals. It is responsible for the successful delivery of the programme, including the benefits. It formally reports to the Trust Board.
14.4.14 The NHPB has established a number of sub-groups/committees to take forward elements of the programme and manage the interfaces with Project Co. One of the most important is the Construction and Commissioning Enabling Group which is chaired by the Director of Operations. This group will oversee and manage the operational interface with the construction programme.
Benefits Realisation Steering Group
14.4.15 The role of the Benefits Realisation Steering Group is to take responsibility for the benefits realisation programme for the New Hospitals Programme, and to manage, monitor and oversee implementation to ensure achievement. One of the first steps
Version 10.1
245
New Hospitals Programme
was to revisit the benefits identified in the Business Case to ensure they were robust and then to develop a vision for the New Hospitals and a strategy to deliver the Benefits Realisation programme (Appendix 14H).
14.4.16 A close link with ICT will be in place to ensure efficiencies are delivered through the use of new technologies.
Space and Move Management Steering Group
14.4.17 The purpose of the Space and Move Management Working Group is to provide a forum to discuss and generate ideas for resolving space and move management issues, and to manage the Space and Move Management workstream. The group are responsible for identifying solutions and putting together option appraisals in liaison with colleagues, for consideration and approval prior to the development of business cases I respect of any agreed capital schemes.
14.4.18 A specific output of this workstream is the development of an Estates Utilisation Strategy that will inform the Trust’s capital investment programme.
Core Programme Team
14.4.19 Day-to-day operational management of the programme will continue to be undertaken by the workstream leads, who constitute the ‘Core Programme Team’. This group will be chaired by the Programme Director and meets fortnightly to assess progress.
ISG & CRS Project Board
14.4.20 The ISG and CRS Project Board will be tasked with ensuring that the information and communication technology (ICT) aspects of the project are delivered appropriately and to the agreed timescales, and that the delivery of ICT dovetails with the New Hospitals Project construction and commissioning programme. Further information on this can be found in Chapter 17 of this business case, along with the relationship between this Project Board and the overall ICT implementation structure for the Trust. Its membership is likely to be:
• Director of ICT (Trust Board responsibility for ICT services) (Chair);
• Head of Clinical Design;
• CRS Lead (ICT);
• Senior Technical Manager (D&B Team – New Hospitals Project);
• Deputy Director for ICT;
• Clinical Lead for ICT;
• Senior Nursing Representative; and
• Skanska ICT Lead.
14.4.21 As can be seen from the organisation chart above (Figure 105a), this board will work alongside the New Hospital Programme Board to ensure that the overall project objectives are met effectively.
14.4.22 The terms of reference of the ISG and CRS project board are to:
• To provide costs for active communication and IT infrastructure providing the appropriate level of date outlets required for use in the new buildings(s) aligned to the build programme;
Version 10.1
246
New Hospitals Programme
• Ensure that the ICT implementation proceeds as per the timescale required to support the opening of the new hospitals;
• Ensure that a detailed implementation plan is established and monitored;
• Ensure that the Trust fulfils its obligations under the contract;
• Ensure that appropriate training programmes are in place for Trust staff and that resources for this are identified; and
• Monitor the outputs of the implementation and ensure that these meet the assessed needs of the Trust in clinical and management terms. To inform the New Hospitals Programme Board of developing technologies that could deliver efficiencies and improved service delivery.
14.4.23 In addition to the internal governance structure detailed above, a joint governance structure has been set up with Capital Hospitals to manage and oversee the different elements of the programme they are responsible for delivering. The details of this structure is set out in Chapter 7. The two main committees responsible for the delivery of the programme are:
The Liaison Committee (Joint Principals Board)
14.4.24 This board is responsible for overseeing the management of the contractual relationship with the consortium. Details of terms of reference and membership are set out in section 14.11 below.
The Joint Partnership Group
14.4.25 This forum is responsible for the operational management of the contractual relationship with the consortium and monitoring progress with the construction programme. Details of terms of reference and membership are set out in Section 14.11 below.
Stakeholder Engagement
14.4.26 Stakeholder engagement is considered to be very important and is conducted in a variety of ways in accordance with the project’s Stakeholder Engagement Strategy, a copy of which is provided at Appendix 14B. Implementation of the strategy is the responsibility of the Trust’s Communications Manager whose role is detailed in paragraph 14.6.2. One element of the strategy, communicating the design solution, is set out in detail in Chapter 7, paragraph 7.6.
14.5 Programme Support Office 14.5.1 In addition to the dedicated structure to oversee and manage the implementation of
the project, the Trust’s Programme Support Office (PSO) provides advice and guidance and ensures that consistent standards are maintained with regard to programme control.
14.5.2 The PSO was established to support and coordinate the activities of the major programmes and projects undertaken by the Trust.
14.5.3 The objectives of the PSO are:
• To provide a central function to support and coordinate programmes and projects in the Trust;
• To take a leading role in setting and monitoring standards in this area and make recommendations regarding best practice as appropriate;

Version 10.1
247
New Hospitals Programme
• To set and maintain consistent and practical sets of standards for project management that will enhance the Trust’s ability to deliver changes on time, to budget and to ensure that benefits are fully realised;
• To provide a central facility for monitoring project delivery and for reporting progress to senior management;
• To provide a central and structured storage capability for programme/project information which will allow project executives and staff to have instant access to the latest version of relevant documents; and
• To promote the use of formal methodologies and a programme for continuous improvement in the Trust’s programme/project delivery capability in the use of:
PRINCE2
MSP (Managing Successful Programmes)
MoR (Management of Risk).
14.6 Programme Implementation (Team) Structure 14.6.1 The structure of the team has been reviewed for the period post-financial close.
Attached at Appendix 14C is the detail of the structure adopted currently. This structure has been approved by the Trust Board and funding has been secured. Some of the detail relating to the main roles is set out below.
14.6.2 The structure of the team will change over time to reflect the needs of the programme.
Chief Executive
14.6.3
Director of Finance and Investment
14.6.4 The Director of Finance and Investment has executive leadership of the Programme and is responsible for monitoring the Programme and ensuring it is on track for delivery of its objectives. In particular he is responsible for:
• Governance of the Programme including chairing the programme board;
• Ownership of the delivery of the Business Case;
• Ensure the project is subject to internal and external review;
• Problem resolution and referral; and
• Post Project Evaluation
Programme Director
14.6.5 The Programme Director reports to the Chief Executive (Trust Board Executive lead for the programme) and is accountable to the Chief Executive. The Programme Director is accountable to PPAB and Project Board for delivery of the project, and is the named Trust representative in the project agreement. The Programme Director is responsible for:
• Providing leadership;
• Setting work programmes and objectives for the workstreams;
Version 10.1
248
New Hospitals Programme
• Ensuring the Trust meets its contractual obligations;
• Reporting progress; and
• Managing communications and stakeholder engagement.
14.6.6 For clarity in respect of the decision making process, and to ensure that the project is managed effectively and to time, the Programme Board has agreed a clear scheme of delegation of responsibility to the Programme Director (see Appendix 14G). Critical decisions outside of these parameters are reserved for the NHPB or NHPIB.
Workstream Leads
14.6.7 There are three main workstreams (clinical design and clinical commissioning; technical and construction; and FM contract management), each headed by a senior manager (Workstream Lead) who is directly accountable to the Programme Director. Workstream Leads are responsible for:
• Managing their workstreams;
• Setting responsibilities and work programmes/objectives for team members which ensure the delivery of project objectives;
• Monitoring delivery against objectives;
• Identifying any issues which could affect project deliverables;
• Ensuring the Programme Control processes and tools are complied with;
• Identifying any possible solutions for resolution for consideration by Core Project Team; and
• Managing the input from, and interface with, external advisers.
14.6.8 Workstream Leads are responsible for managing issues arising within their areas of responsibility throughout implementation and commissioning. The Trust will ensure the necessary continuity and hopefully ensure that corporate memory is not lost.
Head of Clinical Design and Clinical Commissioning
14.6.9 This role has been critical throughout the project in ensuring that the design solution provided by the Capital Hospitals consortium reflected clinical and patient needs and in overseeing the sign-off of 1:200 and 1:50 plans. The Head of Clinical Design and Clinical Commissioning provides the key link with the change team responsible for the necessary business re-engineering and the technical commissioning team to ensure that plans for service transfer are manageable and appropriate. The post holder has overall responsibility for:
• Coordination of the design process for those areas with a clinical interface;
• Detailed migration and decant programmes;
• Equipment; and
• Arts and interior design.
14.6.10 The post holder is supported by a number of clinical advisers.
PFI Technical and Construction Lead
14.6.11 This post holder is responsible for ensuring that the Trust meets its obligations with regard to all construction and technical matters in the project agreement, i.e.
Version 10.1
249
New Hospitals Programme
management of the construction programme, and will be required for the duration of the construction period. The post holder is also responsible for:
• Providing the Trust with expert technical advice;
• Managing Trust obligations that have an impact on construction;
• Managing the existing capital programme;
• Decommissioning of existing buildings;
• Space planning with the clinical leads;
• Non-clinical reviewable design;
• Managing implementation of the advanced works;
• Day-to-day site liaison with Skanska Innisfree;
• Coordination of the delivery of the IT interface; and
• Technical commissioning.
14.6.12 The post holder is supported by two experienced Construction Project Managers, Capital Project Managers, a Decant and Commissioning Manager, a Space and Property Manager and a professional consultancy support where necessary.
PFI Performance Manager
14.6.13 This post holder is responsible for contract performance and management of the SSD, soft and hard FM services. Main responsibilities include:
• Contract management;
• Implementation of the payment mechanism;
• Interim services;
• SSD, soft and hard FM monitoring including management of the helpdesk; and
• Ensuring a high level of service is maintained.
14.6.14 As the structure shows, the post holder is supported by an appropriate number of monitoring staff.
Programme Control Office
14.6.15 In addition, a dedicated Programme Control Office (PCO) has been be established.
14.6.16 The PCO is headed by a senior manager who is accountable to the Programme Director and responsible for:
• Project control;
• Risk and issues coordination and management;
• Programme Reporting;
• Management of Advisors;
• Audit of the Programme;
• Monitoring implementation of the programme plan;
• Maintaining the governance infrastructure; and
• Provision of programme administrative support.
Version 10.1
250
New Hospitals Programme
External Advisers
14.6.17 The Trust has employed a number of external advisers to complement in-house skills and experience. Their input was reviewed following financial close and the approval of the full business case. Following review it was decided to appoint a lead technical advisor and E.C. Harris were appointed to this work under their OGC Framework Agreement. A number of advisors have also been retained on a call-off basis to ensure that continuity and past experience and knowledge of the programme is not lost and to ensure that the Trust is always able to access high quality technical advice.
The Project Team
14.6.18 Project team members, under the workstream leads, have responsibility for implementing the project plan and delivering their individual work programmes. Each project team member has agreed objectives set by the workstream leads. Progress against these will be monitored regularly.
14.6.19 Project team members will undertake the tasks required to complete the programme, involving staff in other directorates in the Trust as appropriate.
The Equipment Adviser
14.6.20 The Programme had one dedicated Medical Equipment Adviser, supported by Managed Technology Services Limited (MTS). However, the programme of works involved in management of the MES and Trust supply equipment programme is huge and too much for one individual to manage. A second Equipment Advisor has therefore been appointed and this work will be split between them. It is intended to retain this resource throughout implementation to:
• Ensure that the Trust makes timely decisions with regard to equipment procurement, in line with Skanska Innisfree’s construction programme;
• Work with the Trust's clinicians to draw up the necessary output specifications for equipment as part of the MES;
• Manage the process of procurement of equipment not provided through the MES; and
• Work with other Trust managers on ensuring equipment earmarked for transfer is decommissioned and re-commissioned appropriately.
14.6.21 The Equipment Advisers are responsible and accountable to the Head of Clinical Design and Clinical Commissioning.
Communications and Stakeholder Engagement
14.6.22 The Trust’s Director of Communications is responsible for managing the communications strategy in relation to the New Hospitals Programme. Crucial to this role is ensuring that the benefits which the development will provide to the local community and the wider NHS, are championed at every opportunity, both internally and externally.
14.6.23 Main responsibilities include:
• To develop comprehensive channels and tools of communication with all stakeholders, including the wider community, to ensure they are fully informed of progress with the project;
• To publish regular bulletins (Neighbourhood Link) on the project’s progress;
Version 10.1
251
New Hospitals Programme
• To manage all national media and press-related interest;
• To generate opportunities for public involvement in the project during implementation;
• To manage major events at key stages of project implementation; and
• To develop and maintain the Trust’s internet/intranet pages on the project.
Art and Interior Design
14.6.24 The Trust’s Vital Arts Director is responsible for developing and managing the Arts Strategy in relation to the New Hospitals Programme with the aim of using art to enhance the hospital environment and experience for patients, staff and visitors, providing an atmosphere of comfort, healing and wellbeing.
14.6.25 Main responsibilities include:
• Delivering a landmark arts programme that helps to provide a local focus for the new hospitals and beautiful environments that are responsive to the needs of building users;
• Maximising the opportunities to include art of all kinds and at all stages of project implementation;
• Working with the Trust Fundraising Team and project partners to generate the necessary funding to deliver the art programme;
• Commissioning and managing artists to deliver the art programme; and
• Creating opportunities to use the arts to involve public and staff in the project.
Other Directorate Support
14.6.26 In addition, the programme will be supported by staff from Communications, Human Resources and ICT. These staff members are vital in ensuring the smooth implementation of the programme.
14.7 Project Management Costs 14.7.1 The costs associated with the management of the project, including contract
performance management arrangements to global completion and post-project evaluation, and including the costs of any necessary consultancy fees, are estimated to be £3.0 million per annum, (2005/06 prices) (£2.4 million retained structure first year). Costs will be met from the transitional funding monies available, or from Trust internal resources. The affordability analysis in Chapter 11, Figure 88 includes the project management costs within the double running costs figure.
14.7.2 In addition to direct Programme management costs, the Trust is putting mechanisms in place to assist with the management of any variations.
14.8 The Descoping Project Team 14.8.1 As a consequence of the DH/HM Treasury’s decision that the Trust should reduce
the costs of the scheme by 17% (approximately £20 million per annum) there was a need to undertake a descoping exercise. Because of the size and complexity of the task, and the short timeframe for delivery (15 months), it was necessary to set up a separate, dedicated project team to manage the exercise. Following the successful completion of Descoping this workstream has now been disbanded.
Version 10.1
252
New Hospitals Programme
14.9 Programme Management – Business Continuity 14.9.1 The Trust recognises the importance of completing the recruitment appropriately
skilled individuals into the programme team. Prior to FC there were a number of vacancies in the team which were being covered by external consultants. A vigorous recruitment exercise was conducted which included the appointment of a recruitment agency.
14.9.2 Despite best endeavours, one or two of the posts proved difficult to recruit to, and found no applicants suitable for appointment.
14.10 Control Arrangements 14.10.1 To help ensure the project runs smoothly, controls have been established:
• To monitor the activities within workstreams;
• To monitor the costs of the scheme;
• To monitor risks and issues;
• For the interface with Capital Hospitals; and
• To monitor expenditure against budgets for the project.
14.10.2 The Programme Board have agreed the project plan timetable and targets (objectives) have been established for the successful delivery of the programme. No tolerances or variances from the established target dates will be permitted without reference to the NHPB and, where appropriate, the Trust Board. The Core Project Team will monitor progress against workstream deliverables regularly. Any variances against project milestones and recommendations for addressing these will be submitted to the NHPB and Trust Board where necessary for consideration and a decision as to the way forward.
14.10.3 The Board receives reports on progress through a monthly highlight report via the Programme Board, which provides quality assurance. The highlight report includes a report on the progress in the workstreams, costs to date, any potential issues, an update on risks and the next major steps to be taken in the programme expenditure. This Highlight Report is fed from the Programmes reporting structure. Each workstream lead is required to produce a highlight report in respect of their workstream, these reports are amalgamated into a single report to the Board.
The Project Control Tools
14.10.4 A number of project control tools have been established for management of the programme. They include:
• The overall programme plan which details key milestones and deliverables for the project to completion;
• The project control handbook which details:
The procedures and control processes for project implementation and for monitoring and reporting progress (highlight and checkpoint report);
The roles and responsibilities of individuals in the project team, ensuring that everyone understands, accepts and carries out their responsibilities; and
The mechanisms for audit and review.
Version 10.1
253
New Hospitals Programme
14.10.5 The project control processes include the maintenance of comprehensive risk and issues logs and the programme plan which identified dependencies. These are project-critical documents, which are reviewed regularly by the Programme Team. Risks and issues of concern are reported to the NHPB and escalated higher if necessary. Workstream leads are responsible for regularly reviewing the risks and issues identified under their workstream and updating the logs with activity to be undertaken to address and mitigate the risks.
14.11 Interface with Capital Hospitals Limited (CHL) 14.11.1 It is critical to the success of the project that the Trust and Capital Hospitals work
closely together in partnership throughout the implementation period to completion. The consortium has established its own implementation structure for the management of the project post-financial close, in liaison with the Trust. This is complementary to the Trust’s arrangements and is set out in their Contract Management Plan116.
14.11.2 The Contract Management Plan, which has also been agreed with the Trust, sets out the arrangements for joint working following financial close.
14.11.3 Representatives from CHL and the service providers sit on many of the implementation groups and Trust committees and a partnership approach is being developed.
14.11.4 At the highest level there is a Liaison Committee (Joint Principals Board) responsible for managing the contractual relationship between the two organisations and any dispute resolution. Membership of this committee is small, consisting of three representatives from the Trust and three from CHL. Trust members are the Chief Executive, the Director of Finance and Investment and a Non Executive Director.
14.11.5 The key interfaces will be with the clinical design and build teams and FM performance teams, all of which will report at executive level to the Joint Partnership Group, which is the mechanism for the management of the day-to-day contractual relationship, and will oversee overall implementation of the project and address and resolve any issues of concern.
14.11.6 Membership and Terms of Reference of the Joint Partnership Group are contained within the Contract Management Plan attached at Appendix 14D.
14.11.7 Because of the scale and complexity of the project, the Joint Partnership is supported by a number of specific sub-groups as follows:
• Joint Design and Construction Review;
• Equipment Investment Committee;
• MES Steering Group;
• Commissioning Steering Group;
• Safety, Health, Environment and Fire Group;
• Energy Efficiency Committee;
• Variations Group; and
• Services’ Performance Steering Group;
116 See Appendix 14D.
Version 10.1
254
New Hospitals Programme
Hard FM Services
Soft FM Services
Sterile Services
14.11.8 A summary of the roles and memberships of these groups is set out in Chapter 7 paragraph 7.3.
14.11.9 The detailed membership and terms of reference for these groups and the relationship with the Joint Partnership Group is set out in the Contract Management Plan at Appendix 14D.
Communications
14.11.10 In addition to regular face-to-face meetings and exchange of email, etc., a number of electronic processes have been established to aid and speed communications between the project team and the consortium.
14.11.11 In addition, to simplify and improve access to, and sign-off of, drawings and plans between Capital Hospitals Ltd and the Trust, a web based document management system (Skandocs) has been adopted and protocols have been developed with regard to use of the system.
Decisions – Maintaining Control and the Audit Trail
14.11.12 Another key aspect of the interface with the consortium is in relation to the decision making process. It is important that there is an audit trail of key decisions made and that any changes to output specifications are logged, priced and approved.
14.11.13 A detailed project control handbook117 has been put together and agreed with the Project Board and the consortium. This sets out the protocols for control and individual responsibilities.
14.11.14 The project agreement is compliant with the NHS standard form of contract (SFPA3) with regard to the upper limit for variations arising during implementation, (the lesser of 1% of project costs or £1 million). However, for the New Hospital Project, affordability is a key factor and, therefore, a variation up to £10 million is a real issue. A strict change control procedure has therefore been established and agreed with the consortium. This procedure ensures all agreed changes to output specifications are controlled and managed and that a clear audit trail exists.
14.11.15 One of the disciplines in the interface procedure is a requirement for all changes to be approved by the Project Team before a change control form can be submitted to the consortium. Increasingly it is thought that there is a need to establish a scheme of delegation for minor changes, and proposals have recently been approved by the Trust board, the detail of which remains to be agreed with Finance.
14.11.16 A further discipline being worked through with the consortium to control cost is a fixed price for minor work amendments, such as provision of an additional power or data outlet, light fitting, etc.
14.11.17 These interface procedures have been reviewed by Internal Audit and are considered to be robust.
117 See Appendix 14E.
Version 10.1
255
New Hospitals Programme
Commissioning Arrangements
14.11.18 Management of the commissioning arrangements for the new build is a critical element in the programme. A detailed decanting and commissioning programme118 for Phase 1 at both Barts and The Royal London hospitals has been put together in liaison with the consortium. Adherence to this programme will ensure delays to the building programme are minimised.
14.11.19 As a result of descoping, there is a need to review and refresh the commissioning plans. This work is being undertaken, and drawings are being revised and agreed with CHL.
14.11.20 The methodology to be employed for making this happen smoothly will involve detailed planning with the users for: decommissioning existing equipment; training; the transfer of patients and staff to the new facilities; and commissioning new equipment. This work is being taken forward and managed by the clinical and technical teams under the Head of Clinical Development.
Managing the implementation of Interim Services
14.11.21 The management of the interim services will be to the same robust standard as that for steady state. Service level specifications have been drawn up, together with method statements and a service quality plan. All of these documents have been approved and signed up to by the Trust, Skanska Innisfree and the FM service providers. This mirrors the steady state arrangements with specific stated derogations.
14.11.22 The Trust’s retained management structure for FM services will provide input to the informed client role for statutory, mandatory, advisory and good practice on FM matters. Clinical service developments will be assessed, and following consultation with the FM service providers, appropriate variations issued. The role will also be to support the project and complement Project Co.’s self-monitoring arrangement. This will include programme management and performance monitoring.
14.12 Post-Project Evaluation 14.12.1 It is recognised that clear arrangements need to be in place, beyond global
completion for post-project evaluation. It is intended that this process will be overseen by the Programme Director. Detailed arrangements are contained in Chapter 19.
14.13 Chapter Conclusion 14.13.1 This chapter demonstrates that sound systems and processes are in place for the
management of the project from financial close to global completion and that the necessary funding is in place to support the proposals.
118 See Appendix 14F.
Version 10.1
256
New Hospitals Programme
14.14 Appendices 14A New Hospitals Programme Governance Structure – Terms of Reference
and Membership 14B Stakeholder Engagement Strategy 14C Post-Financial Close Project Management Structure 14D Contract Management Plan Capital Hospitals Ltd 14E The Project Control Handbook 14F Decant and Commissioning Programme 14G Scheme of Delegation 14H Benefits Realisation Steering Group Terms of Reference
Version 10.1
257
New Hospitals Programme
15 PROJECT AGREEMENT SUMMARY
Synopsis – Project Agreement Summary
This chapter:
• Confirms that the Standard Form Project Agreement Version 3 (SFPA3) has been followed with minimal exceptions;
• Confirms that where these exceptions have occurred, they have been agreed by the Private Finance Unit (PFU); and
• Outlines the detail of material project specific modifications to the SFPA3.
15.1 Introduction 15.1.1 The project agreement (PA) (see Appendix 15A) is in all material respects in the
form of version three of the standard form project agreement (SFPA3) issued by the Department of Health (DH), with the exception of certain project specific points. The Trust has continually updated DH on the development of the PA during the procurement.
15.1.2 A summary of SFPA3 is published by the DH and a copy of this is attached at Appendix 15B. Consistent with the drafting of SFPA3 but contrary to the summary in Appendix 15B, the land arrangements in the PA do not use a leaseback structure. Instead the Trust grants a licence to Project Co. in order to allow it to obtain more favourable tax treatment.
15.1.3 The principal project specific provisions are summarised below.
15.2 Change in Law 15.2.1 SFPA3 is designed for a typical PPP hospital project with a construction period of
up to four years. In such a project, it is generally accepted that Project Co. will accept the risk of change in law (other than NHS specific change in law and discriminatory change in law) arising during the entire construction phase.
15.2.2 The SFPA3 risk allocation for change in law is not commercially acceptable in the context of a very long construction programme such as the approximately nine and a half year period anticipated for this project. This is because, if Project Co. was required to accept change in law risk for the entire construction period, it would have to price a significant risk premium to cover the unforeseeable consequences of change in law occurring outside the standard horizon of foreseeability (generally between four and five years).
15.2.3 The approach adopted in the PA is therefore effectively to treat the project as two shorter projects for the purposes of change in law. In practice, this means that Project Co. has an opportunity to revise its price for the second and third phases of the construction works to reflect the impact on its capital expenditure of:
• Changes in law after the date of the PA which could not reasonably have been foreseen at that date; and
• Changes in law during the second half of construction which are foreseeable at the price revision date.
Version 10.1
258
New Hospitals Programme
15.2.4 SI has accepted change in law risk for the first phase of construction at both Barts and The Royal London. As Barts Phase 1 construction is approximately 4 years and The Royal London Phase 1 is just under 5 years, SI has accepted change in law risk for a longer period than most conventional projects anticipated by SFPA3.
15.2.5 Six months before the beginning of Barts Phase 2, and 6 months before The Royal London Phase 2, Project Co. will have the opportunity to adjust the construction price of Phase 2 and Phase 3 works in relation to the changes in law referred to above. This adjusted price is then fixed and Project Co. accepts change in law risk for the rest of the construction period.
15.3 Construction Cost Inflation 15.3.1 As stated above, SFPA3 is designed for a project with a construction period
substantially shorter in duration than that of this project. Similarly, it would not deliver value for money for the Trust to require Project Co. to take the risk of construction cost inflation for the entire construction period. This judgement was arrived at following both extensive discussions with potential bidders prior to competition (which revealed no appetite whatsoever on the part of the private sector to accept this risk) and discussions with the DH PFU regarding the project specific challenges faced by the Barts and The London PFI scheme. From these, it was concluded that the private sector should be required to provide a fixed construction cost for the first five years, but that due to the uncontrollability and unforseeability of inflation further ahead the risk of inflation, after five years should remain with the Trust. The Trust has retained the risk of construction cost inflation applied to post-Phase 1 construction costs. The Trust has therefore provided that the price for the construction of the second and third phases of the project will be adjusted in accordance with an agreed index.
15.3.2 At BaFO bidders were required to price on the assumption that construction cost inflation will be 3% per annum. To reflect a more prudent affordability and risk position, this assumption has been adjusted to 3.5% per annum. The PA provides that three months before construction of each second phase this assumption is tested against the Davis Langdon buildings cost index for the period up to the revision date and for the next two years.
15.3.3 The Trust will pay any increase in cost compared to the base assumption and will take the benefit of any reduction in cost. The costs subject to indexation are those modelled by Skanska Innisfree as part of their bid. Therefore the Trust will not incur additional indexation costs as a result of delays caused by the contractor.
15.3.4 This process will be repeated again two years later to reflect forecast construction cost inflation over the next two years and, if necessary, a third time two years after that date. In practice, there will probably be two adjustments during the Barts Phase 2 & 3 works and three adjustments during the Phase 2 and 3 works at The Royal London. The need to repeat this process every two years is dictated by the fact that, historically, forecasts of construction cost inflation for longer periods have been unacceptably inaccurate.
15.3.5 The Davis Langdon index is based on building costs and is considered less volatile than a tender price index. Technical advice indicates that the Trust’s current inflation assumption is prudent (see Appendix 15C). The index takes account of the Government’s existing infrastructure investment programme and is weighted for local London factors such as Crossrail.
15.3.6 The initial funding level and the unitary charge presume that CCI will run at 3.5% per annum, equating to a CCI-driven capital expenditure requirement of £70.8m.
Version 10.1
259
New Hospitals Programme
To the extent that CCI actually falls below 3.5% and together with any associated change in law liabilities, the project proves to be over-funded, the project agreement provides mechanisms for the Trust to ‘claw back’ the economic benefit.
15.3.7 If CCI exceeds 3.5% Project Co. has committed construction variation bonds totalling £90m to provide the additional funding requirement. In addition, the Trust will be able to make a call on the pool of uncommitted variation bonds which totals over £100m. However, if indexation is running at such excessive levels, it is much more likely that the Trust will respond by seeking to rescope the project to remain within the affordability envelope and therefore is unlikely to need to call upon further funding. This risk would apply equally to both the PFI and conventionally funded options.
15.4 Look Forward Test 15.4.1 In a typical PFI project, and in accordance with SFPA3, NHS trusts generally do not
have any remedy in respect of poor performance of the construction works until such time as completion has not been achieved by an agreed longstop date. In a typical PFI project, with a construction period of two to three years, the longstop date would generally fall around 9 to 18 months after the scheduled date for completion.
15.4.2 In view of the very long construction period of the project, the Trust considered that it would be unacceptable if it was effectively powerless to exercise any remedy in the event of poor progress until the expiry of a longstop date, which would be over 10 years after the commencement of construction of the project. The solution to this is the ”look forward test“ which is operable by the Trust in the event that Project Co. has failed to achieve either:
The actual “Royal London first phase completion date” within a period of 18 months after the scheduled “Royal London first phase completion date’; or
The actual “Barts first phase completion date” within a period of 18 months after the scheduled “Barts first phase completion date’.
15.4.3 In either of the circumstances described above the Trust will have a right to terminate the PA if it is agreed, or in the absence of agreement, determined (by an independent expert) that there is no reasonable prospect of Project Co. achieving the actual substantial completion date (defined as the completion of Barts Phases 1 and 2 and The Royal London Phases 1 and 2) within a period of 36 months after the scheduled substantial completion date.
15.5 Delay Events/Excusing Causes 15.5.1 Delay events are events affecting the progress of the works, in respect of which
Project Co. is given an extension of the time allowed to complete the works (but no compensation for the any additional cost of working or additional finance cost).
15.5.2 Excusing causes are events which prevent Project Co. from performing the services. Project Co. will be paid for the services which it is prevented from performing, as if such prevention had not occurred.
15.5.3 In contrast with typical projects, the project will have a long interim period during which both construction works and services will be provided simultaneously on the sites. The Trust has acknowledged that certain delay events may also have an adverse impact on the ability of Project Co. to provide the services. As a result an additional ‘excusing causes“ have been introduced which is triggered by certain
Version 10.1
260
New Hospitals Programme
delay events. The additional ‘excusing causes“ relates to the occurrence of any project specific ground risk in an inaccessible area.
15.5.4 In addition, as discussed below, the Trust has agreed a specific regime dealing with its retained estate where Project Co. is required to provide certain interim services. It has not been possible to allow Project Co. to carry out comprehensive intrusive surveys of these buildings. Therefore, the Trust has from the outset retained lifecycle risk in them until handed over to Project Co. for refurbishment. Consequently, the Trust has accepted that where interim service provision is materially affected by deterioration in the condition of these buildings, or by latent defects, Project Co. is entitled to relief.
15.5.5 This relief may take the form of derogation to the relevant interim service level requirement, or the Trust remedying the deterioration or defect. If the Trust does not elect either of these, and before the relief is implemented, Project Co. is entitled to an excusing cause. To assist the Trust in controlling and managing these risks Project Co. is required, on an annual basis, to notify the Trust of any such problems it is aware of or foresees occurring in the existing buildings. If subsequently a problem that was not so notified occurs, Project Co. is only entitled to relief if it could not reasonably have foreseen that problem.
15.6 Interim Services 15.6.1 As mentioned above, the PA requires Project Co. to provide services during the
prolonged construction period. In general, the provision of these interim services is treated in the same way as the ‘steady state“ services, subject to a number of exceptions which recognise the greater risk and uncertainty attached to the provision of services in existing buildings at a time when Project Co. is also carrying out substantial construction works. These include:
• The Trust is not entitled to terminate the PA for poor performance of the interim services, although individual service providers can be terminated;
• The Trust has agreed to a number of service derogations where the service providers cannot perform the service to the steady state standards due to the inherent condition of the existing buildings. The service providers will also be protected by the measures described in paragraphs 15.5.4 and 15.5.5, in relation to deterioration of the existing buildings during the interim period; and
• The payment mechanism for interim services is based on SFPA Schedule 18 but separate from that for the steady state services. Compared with the steady state provisions, the interim payment mechanism has a higher tolerance for Project Co. failures, while ensuring that failures in delivering the interim services cannot lead to deductions against the main service payment in periods when both interim and steady state services are being provided (for example once Phase 1 on either site has been completed). Additionally, the Trust does not have use parameters against which availability can be measured and there will not, therefore, be any Category D or E unavailability deductions during the first 12 months of service. During this period the Trust and Project Co. will work together to develop a set of use parameters which will be used to measure availability during the remainder of the interim period.
Version 10.1
261
New Hospitals Programme
15.7 Insurance and Indemnities of Existing Buildings 15.7.1 The portfolio of buildings for which Project Co. is responsible under the PA includes
existing buildings, a number of which are of particular and distinct historic and aesthetic value. In addition, the long construction phase means that Project Co. makes use of a number of the Trust's buildings on a temporary basis before returning them to the Trust in a decommissioned state. There are also a number of buildings scheduled for demolition as part of the project, but where the obligations of Project Co, which are reflected in the insurance arrangements, are to provide alternative temporary facilities, rather than to rebuild.
15.7.2 The Trust has recognised that it does not represent value for money to impose on Project Co. comprehensive insurance and reinstatement obligations in relation to all these buildings during the construction phase of the project. Consequently these obligations have been modified and in places removed in relation to certain buildings. Generally speaking in all these buildings, Project Co. is still required to maintain public liability insurance covering its activities.
15.7.3 In addition Project Co. is required to take out limited material damage cover for those buildings which are scheduled to form part of the construction programme, allowing it to reinstate those buildings to the condition required in the construction programme.
15.7.4 The proposed insurance arrangements for existing buildings are designed to put the Trust in no better and no worse a position than they currently are. However, the Trust is potentially exposed to the risk that damage to the existing buildings not caused by Project Co. could cause delay to Phase 2 of the construction works. Therefore the Trust investigated the cost of Project Co. obtaining Delay in Start Up insurance for existing buildings to cover this risk and has decided to take up this option to mitigate the Trust’s exposure to programme risk. A second Trust risk relates to damage to existing buildings that prevents the Trust decanting services to these buildings prior to Phase 2 construction, thereby delaying the commencement of the Phase 2 works. The Trust has required Project Co. to take out insurance cover to provide funds to make available alternative accommodation in the event that this situation arises.
15.7.5 These changes have resulted in consequential modifications to the indemnity obligations of Project Co. by restricting the scope of its indemnity obligations for damage to the Trust's assets in these buildings to the scope of its insurance during the interim period.
15.8 Insurance Price Adjustments 15.8.1 The SFPA3 mechanism for adjusting the price of and sharing the risk in relation to
insurance premia has been modified in two ways:
Consistent with the treatment of change in law and construction cost inflation, the price of Project Co's construction insurances is fixed for Phase 1 on both sites only. At the beginning of each Phase 2, Project Co. is required to take out a new set of construction insurances for the remainder of the construction period. The increased or decreased cost of this (as compared to the modelled cost) falls to the Trust, except to the extent that an increase arises because of a poor claims record; and
The project involves concurrent construction and operation phases rather than the consecutive phases envisaged by SFPA3 – this therefore requires a more complex mechanism for dealing with the cost sharing mechanism for
Version 10.1
262
New Hospitals Programme
changes to operational insurance premiums starting to apply and what the applicable baseline is for assessing cost changes. Although the precise timing and details of how the cost sharing mechanism will operate will be determined at the time, the basic principles have been settled and incorporated in the PA. Adjustment dates for operational insurance are set by the completion of major phases of the construction works. It is believed that in practical terms this is the simplest approach and also the most economical as the Trust will benefit from economies of scale as greater areas of the facilities become operational. The cost sharing arrangement is the same as agreed on several recent NHS PFI deals (e.g. Manchester), other than the adjustment will take place every two years.
15.9 Advance Works 15.9.1 The New Hospitals Programme included three advance works schemes (the
Pathology and Pharmacy Building, the West Wing and Kenton & Lucas Block) which have been procured by the Trust in advance of the procurement of the main PFI project. The rationale for procuring these works was to allow a shorter programme for the main project.
15.9.2 The contractors for each of these buildings do not form part of the preferred bidder consortium. Accordingly, in order to allow for maximum risk transfer in relation to the advance works from the Trust to Project Co, the Trust has procured collateral warranties from the contractors and professional advisers for each advance building in favour of Skanska Innisfree. To the extent that Project Co. benefits from these collateral warranties, the Trust will receive the full PFI service from day one of service transfer. However, there is a period of time between completion of the advance works and handover of these buildings to Project Co. During this period, the Trust has maintenance obligations. Some defects, not covered by the advance works collateral warranties, have also become apparent such as water leakage into an area of the Kenton & Lucas basement. Where a defect is the result of the Trust not carrying out proper maintenance or where a defect is not covered by the collateral warranties, the Trust will provide the estates service provider with a derogation from the service provisions. For those advance schemes now complete (i.e. the West Wing and Kenton and Lucas) the process of identifying these derogations is complete and a definitive list of specific derogations is included in the Project Agreement. The specific derogations will fall away once the Trust has undertaken any necessary remedial work.
15.9.3 The advance works schemes have been designed without input from Project Co, and in a small number of cases the service delivery methodology proposed for the new and refurbished PFI works is not appropriate to the advanced works. Where this is the case, the Trust and Project Co. have agreed an alternative service methodology to meet the service standard. As an example the lifts within the advanced works are smaller than those in the new build and therefore the waste collections bins required to service the advanced works will be smaller and the collection frequency will be higher. The necessary amendments to the service methodologies is complete and for those advance schemes now complete a specific list has been agreed and is included in the Project Agreement.
15.10 Site and Ground Risk Allocation 15.10.1 The SFPA current at the time of the ITN was drafted on the assumption that the
development site is a greenfield site, where comprehensive site investigation is possible. However, SFPA3 also recognises the situation whereby development takes place on a brownfield site where survey access is limited and where there is redevelopment of existing buildings. The New Hospitals Programme is significantly
Version 10.1
263
New Hospitals Programme
more complex than the assumed greenfield model and, as a result, the following risk allocation has been agreed. Project Co. has accepted responsibility for all site risks identified by survey work prior to financial close.
15.10.2 Site risks comprise those risks associated with the site and buildings being used by SI to complete the scheme. The standard contractual PFI position seeks to transfer those risks that the PFI partner has had the opportunity to survey. In some instances, the Trust has managed to transfer more site risk to SI than this standard requires. The principal site risks retained by the Trust relate to:
Archaeological risk (including human remains) – this risk remains with the
Trust. The age of the sites suggests that this risk is significant and will need to be actively managed. The Museum of London’s Archaeological Service (MOLAS) has already completed detailed examinations of both sites involving a series of exploratory digs. Findings set out in MOLAS’s reports for each site (included at Appendix 15D) show that an area in Bedstead Square at The Royal London is estimated to contain the buried remains of up 600 people. The programme impact of this has already added 9 weeks to the programme at The Royal London. The inspection of the other principal area of interest at The Royal London (Garden Square), where the remains of another 600 people are estimated to be buried, can be accommodated within the current programme.
At Barts, the principal areas of interest for MOLAS are accessible only as part of Phase 2 and 3 of the construction programme. A period of one month has already been included in the Phase 3 programme to enable an archaeological dig in the area adjacent to where Merrill Lynch discovered remnants of the old London Wall when constructing its new building some years ago.
MOLAS will retain a watching brief as the construction site is opened up and this function has been allowed for in SI’s programme.
• Soil contamination – The principal risk the Trust is retaining in this area relates
to the identification and removal of radioactive material buried beneath the ground. Surveys already conducted shows that a number of radioactive benches were buried in concrete cases at Barts some decades ago. The area where these benches are located is required during Phase 3 and therefore, the potential impact on SI’s programme (and costs) is likely to be low. A further five areas of radioactive interest have been located by the survey (see Appendix 15E).
The Trust has commissioned a more detailed survey which is to be completed by a specialist radioactive material disposal company, Aurora. Aurora is due to report its findings towards the end of September 2005. This will include a detailed estimate of the scale of radioactivity, the recommended methodology, timing and cost of removal and disposal.
• Asbestos – asbestos identification and removal affects buildings that are
demolished and retained. The Trust’s asbestos register has been updated for the results of three survey programmes in the last five years and this has been priced by SI. SI is currently completing its own intrusive asbestos survey programme. SI has agreed to take delay risk on asbestos discovered in excess of that currently shown in the asbestos register. The Trust retains the cost risk on the net increase/decrease of actual asbestos found. The Trust and SI have agreed the asbestos baseline, the rate that will be applied to newly discovered asbestos and the methodology by which the quantum of asbestos is computed.

Version 10.1
264
New Hospitals Programme
• Retained refurbished buildings – with the exception of the Front Block, Grocers
Wing and West Wing at The Royal London and East Wing at Barts, SI has accepted all risks (other than latent defects) relating to the condition of retained refurbished buildings. These buildings, that number five, are known as Category A buildings for the purpose of the Project Agreement.
The level of risk accepted by SI in relation to Front Block, Grocers Wing and West Wing at The Royal London and East Wing at Barts is determined by the level of access enjoyed by SI to conduct surveys in advance of the commencement of the works associated with each building. For the East Wing at Barts (known as a Category B building for the purpose of the PA), the Trust is able to grant SI the access it requires to survey well in advance of the commencement of works. SI has therefore accepted all risks other than the cost consequences that the condition of the superstructure (e.g. foundations, roof, etc.) is not as assumed. The assumptions made by SI with regard to this are explicit and set out in the PA. The Trust is unable to provide SI with access to conduct surveys in the other three buildings (known as Category C buildings for the purpose of the PA) prior to providing vacant possession. Unlike for Category A and Category B buildings, SI is unable to accept either the time or cost consequences if, following the completion of surveys, its assumptions relating to superstructure are proved incorrect.
A baseline set of assumptions relating to the condition of the superstructure of Category B and Category C buildings has been established and is included in the PA. An agreed survey programme will be used to validate only these assumptions. Changes to condition other than those set out in the assumptions will be SI’s risk. The Trust bears the risk that the surveys show the assumptions to be incorrect. If there is a capital cost impact and this is so material that Project Co. is unable to proceed, then a variation to the Trust's requirements will need to be made. Given the potentially high cost impact of delay, the Project Agreement allows for the Trust to pre-fund the capital cost impact of a change in the Trust’s requirements which would fall to be treated as a Trust Works Variation. If not required for their principle purpose (i.e. to fund CCI in excess of 4.25%), committed CCI Variation Bonds (totalling £80m) can be used to fund the capital cost impact of the assumptions proving to be incorrect. The Project Agreement also places a reasonable endeavours obligation on SI to issue uncommitted Variation Bonds to cover such costs if not funded from committed Variation Bonds, up to the limit of the pool of uncommitted Variation Bonds (i.e. £100m). Where (committed or uncommitted) Variation Bonds are issued, the Project Agreement provides that they can be used to repay the amount pre-funded by the Trust where this has taken place. Similar provisions apply also to Trust Works Variation arising as a result of other Trust risks crystallising in relation to site risks (such as asbestos and soil contamination) and the completion and commissioning programme.
The Trust and SI have examined contingency plans aimed at reducing the cost of Category A and Category B buildings should material risks crystallise following the completion of intrusive surveys. These involve relatively minor reductions to the Trust’s requirements for these buildings but which would reduce capital costs by around £6 million.
Once the survey programme is complete and SI’s proposals, modified or not in the light of these proposals, are accepted then SI will accept all risk other than for latent defects (i.e. from this point in time all Category B and Category C buildings are treated similarly to Category A buildings).
Version 10.1
265
New Hospitals Programme
15.11 Managed Equipment Service 15.11.1 The PA requires Project Co. to provide a Managed Equipment Service (the MES)
whereby, in return for a flat annual payment, it provides and maintains certain items of clinical equipment meeting a generic output specification.
15.11.2 The Trust has recognised that bidders perceive additional risk in providing this service and that consequently it does not necessarily represent value for money to treat the MES identically to the other services Project Co. is required to provide. In particular it is accepted that the MES should be ‘ring-fenced“ from Project Co's other services, the main effects being that:
In the event of poor performance by the provider of the MES, the Trust is not entitled to terminate the PA, but only to require the termination of the MES component or the termination by Project Co. of the MES provider's sub-contract;
Conversely if the PA is terminated for reasons unrelated to the MES, the MES provider is protected from the impact of that termination, so that the Trust must (at its option), either continue with the MES service (contracting directly with the MES provider) or purchase the MES equipment at net book value. Net book value is calculated from the MES provider’s financial model which is updated on an open book basis to reflect the actual equipment investment programme;
If the MES provider is late in completing the installation of the MES equipment, thus delaying the Trust in handing over buildings for the next phase of construction, Project Co. will be entitled to additional time and money from the Trust – which it is unlikely the Trust will be able to recover from the MES provider; and
In the event that the MES provider is terminated either on the Trust's instructions or by Project Co. for certain limited defaults, Project Co. has no absolute obligation to re-provide the MES service, but is instead required to re-tender the MES sub-contract and only to absorb any increased cost up to the MES termination cap (see next paragraph).
15.11.3 In addition, the Trust has also agreed to certain caps on the liability imposed on Project Co. in relation to the MES. These include caps on the deductions that may be imposed in a month, a year and in a market testing period, as well as caps on the liability arising on any termination of the MES. In the event that any of these caps are reached, either the MES provider can decide to increase the level of the cap or the Trust can choose to terminate the MES provider.
15.11.4 The contractual ring-fencing of the MES results in some element of project completion risks remaining with the Trust. The main consequence is that the building may be completed but not be occupiable by the Trust due to the late installation of the MES.
15.11.5 In these circumstances, while the MES provider is not paid, the Unitary Charge in relation to the unoccupied building commences. The phased nature of the construction programme means that the Trust incurs (a) double-running costs on a new (but unoccupiable) building as well as supporting the estate, which it is due to vacate and (b) the programme impact of delay on vacant possession of buildings in Phase 2.
15.11.6 The Trust and its advisers have completed analysis that indicates that, following the introduction of sectional completion to each individual phase (during which the Trust’s pre-completion commissioning activities can take place), clinical occupation of new clinical facilities will be achievable if a relatively small number of significant pieces of equipment are installed. The main pieces of equipment are to be installed well in advance of the Trust taking occupation (for example, a minimum buffer of
Version 10.1
266
New Hospitals Programme
three weeks applies to all imaging equipment). The Trust and its equipment advisers have concluded that the risk of the Trust being unable to occupy the new buildings due to a MES delay is very small (see Appendix 15F).
15.11.7 The principal risk identified by the Trust is that the building is not adequately complete for Siemens to commence its installation work yet practical completion has taken place. However, this risk will be mitigated through the Completion Tests conducted by the Independent Tester which include state of readiness tests for the installation of MES. Project Co. will be unable to obtain a completion certificate until the areas in which Siemens install equipment have met agreed equipment installation criteria. Equally, the Interface Agreement between Siemens and Skanska Construction gives Siemens access, inspection and sign-off rights prior to it accepting the building for its installation work. These contractual rights should act to shield the Trust from any dispute between Skanska Construction and Siemens about the state of readiness of the building for MES installation.
15.11.8 The Trust is to provide an amount of equipment itself. There is a risk that the Trust will not able to have its equipment ready and in place in line with the building commissioning programme, leading to a delay in moving out of existing buildings and hence risks of a similar nature as those in 15.11.5 crystallising. The management and implementation of the Trust-procured equipment will be a dedicated Programme Management Workstream reporting to the New Hospitals Programme Board and the Trust’s Capital Programme Group and be supported by its own Programme Manager. The Head of Purchasing & Supplies will play a key role in ensuring that procurement resources are in place to deliver the work plan.
15.11.9 To address affordability concerns raised by the Department of Health, the Trust has decided to provide funding to cover the capital element of the MES. The first tranche of this funding will be provided by the Charitable Foundation. The introduction of this capital was designed to improve the overall affordability to the Trust, whilst having minimal impact on the VfM of the previously agreed MES deal. The intention of the parties was to alter the risk profile of the MES agreement as little as possible, whilst acknowledging that introducing public capital into this element of the project raises a number of new risks.
15.11.10 The appendices at 15H, 15I and 15J provide detail of the impact on the MES agreement of introducing public capital. However the main changes are described below:
MES Options
■ A number of potential options were discussed by the Trust and Project Co. The Project Agreement at financial close is based on what is known as Option 9, where the Trust provides all capital throughout the concession. The Trust also has the option, within two years, to opt for variations known as Option 1 (Project Co. provide all capital) and Option 6 (Trust provides capital for first install only). The financial models for options 1 and 6 are included within the agreement and therefore the Trust is aware of the cost of these options.
Termination
■ There is a right for Project Co. to terminate the MES only where the Trust fails to provide capital funding. This is subject to a materiality threshold of £300,000 and the Trust has a 120 day rectification period. If the Trust is aware that capital is not available, it can vary the MES to remove equipment and hence the requirement for funding. However, this is subject to a threshold and Project Co.

Version 10.1
267
New Hospitals Programme
has a second MES-only termination right if the value of the MES falls below 80% of the basecase capital value.
Balancing Payment
The benefit to the Trust of introducing public capital is derived through a reduction in the MES Unitary Payment. The full benefit to the Trust is only realised after year 15. Therefore an early termination will mean that Project Co. derives an unearned financial benefit. To rectify this, the parties have agreed a balancing formula whereby the “unexpired” value of the capital funding is paid back to the Trust.
15.12 Sterile Services 15.12.1 As with the MES, the Trust has accepted that bidders perceive additional risk in
relation to the provision of sterile services and has therefore accepted both:
The ‘ring-fencing“ of the sterile services from Project Co’s other services;
Caps on Project Co's liability arising from the sterile services; and
In each case, on similar terms to those described for the MES.
15.13 Benchmarking and Market Testing 15.13.1 The Trust has included benchmarking during the interim services period and at
steady state as well as market testing. The rationale for including interim services is that these services are being provided during the long construction period and that it is in the interests of both parties to have these costs benchmarked rather than getting a fixed price cost for the whole period. Market testing during the interim period is impractical as it will not be possible to replace a service provider during the interim period and then let the original provider back to provide steady state services. The interim services benchmark will occur on the fifth anniversary of service commencement.
15.13.2 The Trust has decided to include benchmarking as well as market testing for steady state services. The reasoning is that this provides the opportunity for both parties not to undertake the market testing exercise if the Trust is content that it is receiving good services in a manner and for a cost that represents value for money. If this is not the case then the services will be market tested.
15.13.3 Figure 106A sets out where the market-tested services are subject to either benchmarking or market-testing during the interim period and once in steady state.
Figure 106A – Benchmarking and Market Testing of PFI Services
Market Tested Service
Interim Period Steady State
Soft FM services (other than waste) but including the estates management service in
Benchmarking after 5 years after service commencement
Benchmarking and/or market testing 6 years after interim benchmarking and every 5 years thereafter
Version 10.1
268
New Hospitals Programme
Existing Buildings Waste Benchmarking after 5 years after
service commencement Benchmarking and/or market testing every 5 years after interim benchmarking
SSD Benchmarking and/or market testing on the later of the 6th anniversary of Financial close or 3 months after relocation of SSD service to the Royal London site
Benchmarking and/or market testing 6 years after interim benchmarking/market testing and every 5 years thereafter
Managed Equipment Service
Benchmarking and/or market testing on the 15th anniversary of service commencement
Benchmarking and/or market testing every 10 years after first benchmarking/market testing exercise
15.14 Compensation on Termination 15.14.1 The Compensation on Termination provisions follow the drafting of SFPA3 except
for three project specific amendments:
The preferred bidder's funding solution includes bond funding and therefore the PA follows the PFU approved drafting used on the Manchester and Newcastle PFI projects;
The preferred bidder's funding solution also includes £20 million mezzanine finance – the Trust has agreed to treat this in the same way as senior funding for the purposes of the compensation on termination and refinancing provisions; and
The compensation provisions also reflect the particular provisions agreed in relation to the MES – where on termination these services are carved out of the termination arrangements, the compensation calculations are adjusted to reflect the fact that certain elements of the funding stream are thus being treated separately.
15.15 Payment Mechanism 15.15.1 The payment mechanism is based on the standard form payment mechanism
issued with SFPA3, although the draft issued with the ITN was based on an earlier version of the Standard Form. The overall structure of the Trust’s payment mechanism (in terms of overall payments, deductions, calculation of service deficiency points, etc.) is in most material aspects the same and has been approved by the PFU.
15.15.2 The Payment Mechanism has been adapted in such a way that it deviates from SFPA3. The main areas where this occurs are:
Interim Period. As detailed in section 15.5, the Payment Mechanism is applied to the Interim Services period although in a modified form. The standard form payment mechanism does not include provision for interim services, but given the length of the interim period it was considered appropriate to include a payment mechanism as close as possible in operation to the steady state payment mechanism.

Version 10.1
269
New Hospitals Programme
Fixed escalator. The service payment includes an element that is escalated by a fixed percentage of 2.5%. This has been included to reflect the funding strategy that will almost certainly include a large proportion of fixed rate bonds. Indexing a percentage of the Unitary Charge by a fixed amount provides a natural hedge for the debt service on these fixed rate bonds, avoiding the cost and complexity of purchasing an RPI swap, and offers both affordability and value for money benefits to the project. In the unlikely event that the senior debt consists only of index-linked bonds, the fixed escalator will be removed.
MES and SSD caps. As detailed above, there are financial caps on the deductions that can be made for service failures relating to the ring-fenced services. In the event that a cap is reached, either the service provider can increase the level of the cap or the Trust can terminate the service provider.
Bedding in period percentages. SFPA3 has a very short bedding in period from the commencement date of global services. The Trust has agreed to amend the bedding in period percentages such that they are lower and apply for longer than the SFPA3 provisions. This is to reflect the scale and anticipated complexity of establishing service provision over such a large hospital site. The agreed bedding in principles mirror the new provisions of the PFU consultation payment mechanism.
The Key Unit principle has been amended so that for category D failure events, it will only apply where the Unit is substantially unavailable for its clinical function. As part of the deal in agreeing to this, Project Co. agreed that when the Key Unit principle is ‘active“ the Trust can still make deductions for further failure events within the Functional Area. This is thought to incentivise Project Co. to respond to other Failure Events within the Functional Area and effectively takes the total area weighting above 100%.
Temporary Repairs. The Trust has agreed that it should “act reasonably” in permitting Project Co. to carry out temporary repairs, which is a departure from SFPA3 where the Trust can act at its “absolute discretion.” The Trust believes this has no commercial impact and was agreed as part of a series of measures between the Trust and Project Co.
15.15.3 The Trust has consulted the PFU in detail on the position reached with the Payment Mechanism and has secured approval in all areas where the Payment Mechanism deviates from Standard Form.
15.16 Payment in Advance 15.16.1 SFPA3 envisages Project Co. receiving payment monthly in arrears. On affordability
grounds, the Trust has accepted a proposal from Project Co. to make payments quarterly in advance. The Unitary Payment saving associated with this is £610,000 a year. The PA contains suitable claw-back protections in the event that Project Co. defaults while in receipt of an advance payment. Payments are made to a blocked account secured in favour of the Trust from which money may be withdrawn at the rate of one third at the end of each month.
15.16.2 Following certain Project Co. Events of Default, the payment mechanism reverts to the monthly in arrears principle and any payments in advance then standing to the credit of the blocked account are immediately repayable to the Trust.
Version 10.1
270
New Hospitals Programme
15.17 Descoping Variations 15.17.1 In January 2006, the Department of Health confirmed that the Unitary Payment for
the year 2015/2016 should be no greater than £96.6 million (indexed) per annum (which was updated on Financial Close to £98.4 million) (the Base Global Service Payment). At such time, the Unitary Payment was calculated to have been approximately £116.92 million (indexed) per annum. Prior to signing the Project Agreement, the Trust agreed with Project Co. to financial savings worth approximately £10.86 million (indexed) per annum, which were achieved through changing interest rate assumptions, amending the deal on the Managed Equipment Service and [list other type variations]) (the extent of such works and services are known as the Maximum Scope of Works and Services and these works and services equate to a Unitary Payment of £107.86 million). This left a shortfall in the savings needed of £9.46 million (indexed) per annum: this is therefore the savings that the Trust still needs to make from the construction and service costs, to achieve the target descoping saving.
15.17.2 Project Co. and the Trust agreed, as set out in Schedule 22, part 7 (descoping variations), to a methodology that enabled them, working together, to amend the scope of the Project from that set out in the Project Agreement on 27 April 2006 to a reduced scope that enabled the Trust to achieve the Target Descoping Saving (each variation required to achieve the target descoping saving being a descoping variation and each descoping variation having its own descoping saving). In broad terms, the principles applying to Schedule 22, part 7 followed the principles contained within Schedule 22 of SFPA3. For example, any descoping variation should leave neither party in no better nor worse position than it would have been in had such descoping variation been implemented.
15.17.3 Included within the Project Agreement were a set of various descoping variations that, should the Trust decide to pursue, were intended to achieve the target descoping saving. These were known as initial descoping variations. The Trust was mindful of the fact, however, that, as the initial descoping variations were identified within a relatively short period of time, the descoping savings and operational impact attributable to the initial descoping variations might be improved on (i.e. produce the same or better savings with less operational impact).
15.17.4 Schedule 22 Part 7 set out the method by which the Trust and Project Co. were to examine the feasibility of the initial descoping variations and other descoping variations and, where agreed to be feasible, developed to a level that could be implemented in order to achieve the target descoping saving in the most economically efficient manner, having regard to the operational impact and the value for money that each such descoping variation offers.
15.17.5 The Project Agreement set out that, by a date no later than 27th July 2007, the Trust and Project Co. were to have agreed a set of Descoping Savings that they know will achieve the target descoping saving and were developed to a level that could be implemented. Each such descoping variation was known as an agreed descoping variation. Whilst there was no penalty for the Trust failing to achieve this deadline, it is obliged to continue progressing such agreed descoping variations, although they may not be its preferred set of descoping variations, until it has identified other descoping variations to a level of detail that could be implemented.
15.17.6 The Trust may, due to certain events, be entitled to reduce the target descoping saving. If this occurred, then:
Version 10.1
271
New Hospitals Programme
a) the Trust could instruct Project Co. to proceed with an agreed descoping variation; and
b) the Trust (upon confirmation from the Department of Health) would authorise that the base global service payment be increased119.
15.17.7 The extent of the reduction in the target descoping saving was directly related the value of the descoping saving of the relevant agreed descoping variation and the increase in the base global service payment (as applicable).
15.17.8 It should also be noted that, should the Department of Health confirm that the base global service payment may be increased the level that would require Project Co. to perform the maximum scope of works and services, then the value of the unitary payment is guaranteed to be £107.86 million (but remains subject to the cost of Project Co. obtaining any additional funding required to perform the maximum scope of works and services that have not been funded to date).
15.17.9 The main risks that affected the operation of Schedule 22 part 7 were:
a) Planning Consents – Project Co. only had planning consent to perform the maximum scope of works and services. Therefore, should a descoping variation require planning consent then this was to be a Trust risk and the Trust was not permitted to require Project Co. to perform a descoping variation where such planning consent is required but had not been obtained. Project Co. is obliged to use all reasonable endeavours to obtain all necessary planning consents. Failure to use all reasonable endeavours would have an adverse consequences for Project Co. in the event of termination of the Project Agreement (see below).
b) Additional Funding Arrangements – Project Co. had only obtained funding to the extent of the base global service payment. Where the Target descoping saving was reduced as a result of the base global service payment increasing, then Project Co. was required, on an all reasonable endeavours basis, to obtain funding equivalent to the extent of such increase. To reduce the risk that the Project cannot be descoped due to a planning consent (see above) but equally cannot not be continued due to lack of funding, Project Co. agreed to make available the level of equity that it would have committed for the maximum scope of works and services. Whilst the Trust acknowledged that this may be an expensive source of funding, it constituted its risk mitigation strategy to prevent termination in such a scenario. Where additional funding was required, the Trust would also look to see whether variation bonds and, failing that, public money were available prior to relying on additional Project Co. equity.
c) Termination – Where the target descoping saving had not been achieved by the actual phased completion date relating to Royal London Phase 1, Project Co. was entitled to terminate the Project Agreement. In such circumstances, the Trust would be liable to pay Project Co. compensation for the termination of the Project Agreement. The quantum of such termination would be sufficient to cover the cost of repaying the senior debt and, subject to the exceptions set out below, Project Co. share capital and junior debt (as if it
119 The Trust subsequently agreed the descoping variations to time.
Version 10.1
272
New Hospitals Programme
were a Trust voluntary termination). The exceptions to this rule are set out in paragraph 11.5 of Schedule 22 part 7 and are as follows:
i. where Project Co. has failed to comply with its obligations under Schedule 22 Part 7 and such failure is the direct cause of termination, Project Co. shall not receive any amount in respect of its share capital and the Junior Debt
ii. where Project Co. has been dilatory in the performance of its obligations under Schedule 22 Part 7 and such failure is the direct cause of termination, Project Co. shall only receive fifty percent (50%) of the amount for which its share capital and the Junior Debt could have been sold on an open market basis based on certain assumptions;
iii. where Project Co. has failed to comply with its obligations to provide additional equity (see above), Project Co. shall not receive any amount relating to its share capital or the Junior Debt.
15.17.10 In the event, the target descoping saving was achieved, which makes the termination Clause now irrelevant.
15.18 Chapter Conclusion 15.18.1 This chapter confirms that the Standard Form Project Agreement Version 3
(SFPA3) has been followed. The Department of Health’s Private Finance Unit has been consulted and involved in any exceptions and project specific amendments have developed where these exceptions/amendments have been included.
15.19 Chapter Appendices 15A Project Agreement 15B Summary of Standard Form Project Agreement 3 15C Davis Langdon Inflation Report 15D MOLAS Reports on Each Site 15E STATS Radiation Report 15F MTS MES Installation Delay Risk Report 15G No longer required by the Department of Health 15H Trust Paper to DH Describing the Amended MES Agreement 15I Legal Outline of Contractual Changes to the MES Agreement 15J Affordability and VFM Assessment of Amended MES
Version 10.1
273
New Hospitals Programme
16 WORKFORCE, HUMAN RESOURCES AND CHANGE MANAGEMENT Synopsis – Human Resources
This chapter demonstrates that:
• A workforce plan has been developed which identifies staffing changes and facilitates succession planning. Changes in staffing:
Nursing and midwifery posts – expected reduction of 57 whole time equivalents (WTEs)
Admin and clerical posts - expected growth by 90 WTEs
MLSOs – no expected growth
• The Trust has implemented a range of strategies and policies to achieve:
The HR elements of the National Plan
Change management to support models of care
The Trust being the first choice for patients under Patient Choice
A stable, appropriate and contented workforce
• Comprehensive arrangements have been worked up and agreed with the preferred bidder and FM staff in relation to the transfer and secondment arrangements under:
The Retention of Employment model
TUPE transfers
Transfer Agreement and Agenda for Change – which will assist in eliminating two-tierism
16.1 Introduction 16.1.1 The workforce plan is based, in the initial years, on the Local Development Plan
(LDP) 2005/08 and shows staff-in-post (whole time equivalents). From 2008 onwards, a reduced growth rate has been estimated, based on the expected delivery of “Gershon” efficiency savings. The impact of new policies and developments is identified in section 16.3 (Workforce Planning Strategy).
16.1.2 This chapter also describes the Trust’s Human Resources (HR) Strategy and approach to:
• The change management processes to introduce new models of care; and
• Working in partnership.
16.1.3 Key aspects of the HR strategy are:
• Achieving the HR elements of the NHS Plan;
• Workforce planning and transformation for the new models of care; and
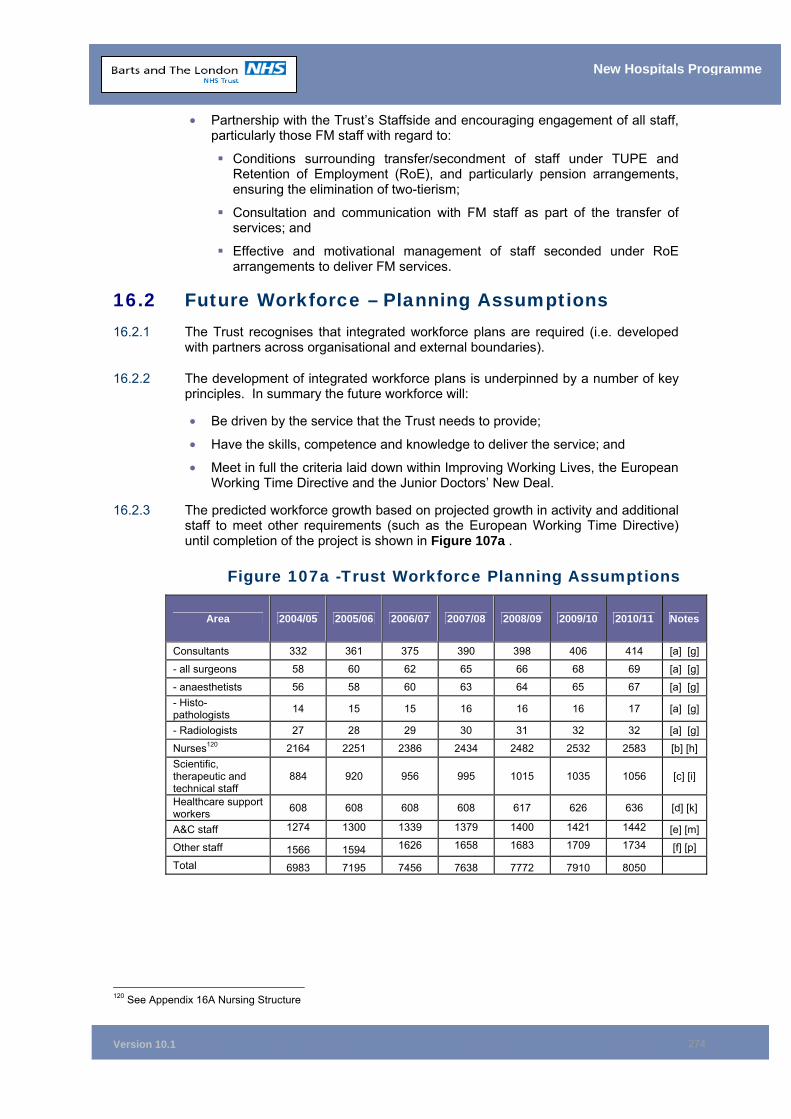
Version 10.1
274
New Hospitals Programme
• Partnership with the Trust’s Staffside and encouraging engagement of all staff, particularly those FM staff with regard to:
Conditions surrounding transfer/secondment of staff under TUPE and Retention of Employment (RoE), and particularly pension arrangements, ensuring the elimination of two-tierism;
Consultation and communication with FM staff as part of the transfer of services; and
Effective and motivational management of staff seconded under RoE arrangements to deliver FM services.
16.2 Future Workforce – Planning Assumptions 16.2.1 The Trust recognises that integrated workforce plans are required (i.e. developed
with partners across organisational and external boundaries).
16.2.2 The development of integrated workforce plans is underpinned by a number of key principles. In summary the future workforce will:
• Be driven by the service that the Trust needs to provide;
• Have the skills, competence and knowledge to deliver the service; and
• Meet in full the criteria laid down within Improving Working Lives, the European Working Time Directive and the Junior Doctors’ New Deal.
16.2.3 The predicted workforce growth based on projected growth in activity and additional staff to meet other requirements (such as the European Working Time Directive) until completion of the project is shown in Figure 107a .
Figure 107a -Trust Workforce Planning Assumptions
Area 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 Notes
Consultants 332 361 375 390 398 406 414 [a] [g]
- all surgeons 58 60 62 65 66 68 69 [a] [g]
- anaesthetists 56 58 60 63 64 65 67 [a] [g] - Histo-pathologists 14 15 15 16 16 16 17 [a] [g]
- Radiologists 27 28 29 30 31 32 32 [a] [g]
Nurses120 2164 2251 2386 2434 2482 2532 2583 [b] [h] Scientific, therapeutic and technical staff
884 920 956 995 1015 1035 1056 [c] [i]
Healthcare support workers 608 608 608 608 617 626 636 [d] [k]
A&C staff 1274 1300 1339 1379 1400 1421 1442 [e] [m]
Other staff 1566 1594 1626 1658 1683 1709 1734 [f] [p]
Total 6983 7195 7456 7638 7772 7910 8050
120 See Appendix 16A Nursing Structure
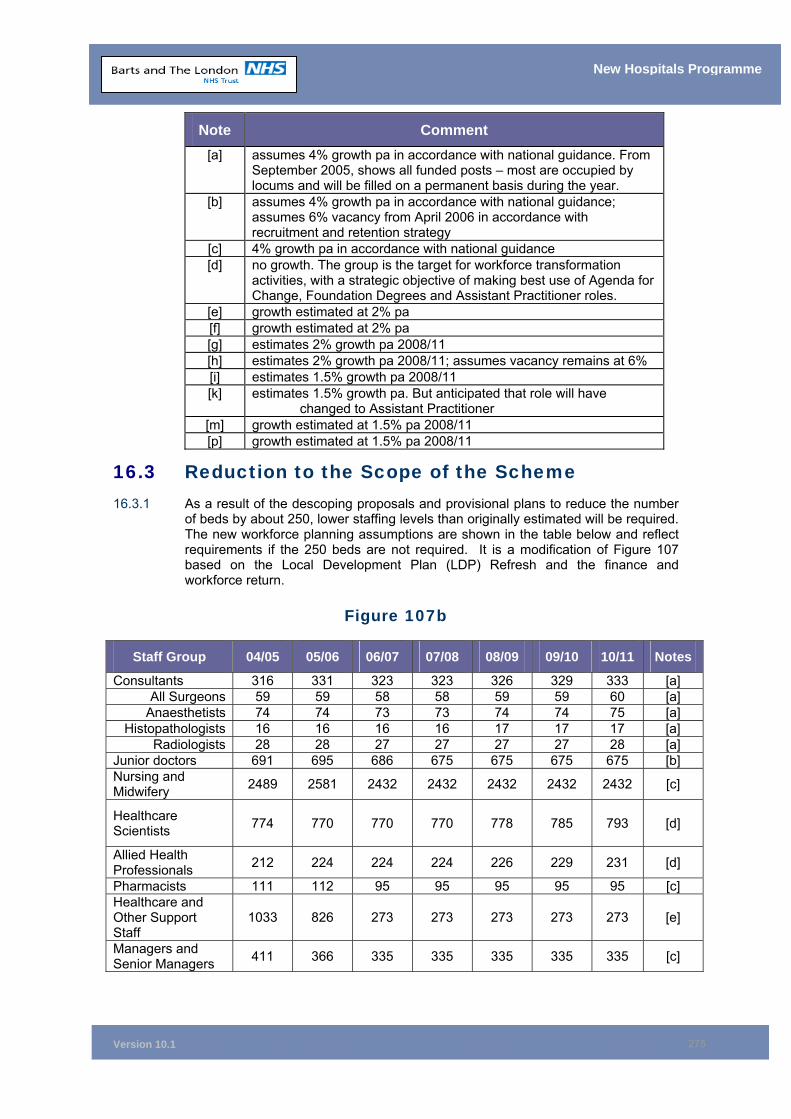
Version 10.1
275
New Hospitals Programme
Note Comment [a] assumes 4% growth pa in accordance with national guidance. From
September 2005, shows all funded posts – most are occupied by locums and will be filled on a permanent basis during the year.
[b] assumes 4% growth pa in accordance with national guidance; assumes 6% vacancy from April 2006 in accordance with recruitment and retention strategy
[c] 4% growth pa in accordance with national guidance [d] no growth. The group is the target for workforce transformation
activities, with a strategic objective of making best use of Agenda for Change, Foundation Degrees and Assistant Practitioner roles.
[e] growth estimated at 2% pa [f] growth estimated at 2% pa [g] estimates 2% growth pa 2008/11 [h] estimates 2% growth pa 2008/11; assumes vacancy remains at 6% [i] estimates 1.5% growth pa 2008/11 [k] estimates 1.5% growth pa. But anticipated that role will have
changed to Assistant Practitioner [m] growth estimated at 1.5% pa 2008/11 [p] growth estimated at 1.5% pa 2008/11
16.3 Reduction to the Scope of the Scheme 16.3.1 As a result of the descoping proposals and provisional plans to reduce the number
of beds by about 250, lower staffing levels than originally estimated will be required. The new workforce planning assumptions are shown in the table below and reflect requirements if the 250 beds are not required. It is a modification of Figure 107 based on the Local Development Plan (LDP) Refresh and the finance and workforce return.
Figure 107b
Staff Group 04/05 05/06 06/07 07/08 08/09 09/10 10/11 Notes
Consultants 316 331 323 323 326 329 333 [a] All Surgeons 59 59 58 58 59 59 60 [a]
Anaesthetists 74 74 73 73 74 74 75 [a] Histopathologists 16 16 16 16 17 17 17 [a]
Radiologists 28 28 27 27 27 27 28 [a] Junior doctors 691 695 686 675 675 675 675 [b] Nursing and Midwifery 2489 2581 2432 2432 2432 2432 2432 [c]
Healthcare Scientists 774 770 770 770 778 785 793 [d]
Allied Health Professionals 212 224 224 224 226 229 231 [d]
Pharmacists 111 112 95 95 95 95 95 [c] Healthcare and Other Support Staff
1033 826 273 273 273 273 273 [e]
Managers and Senior Managers 411 366 335 335 335 335 335 [c]
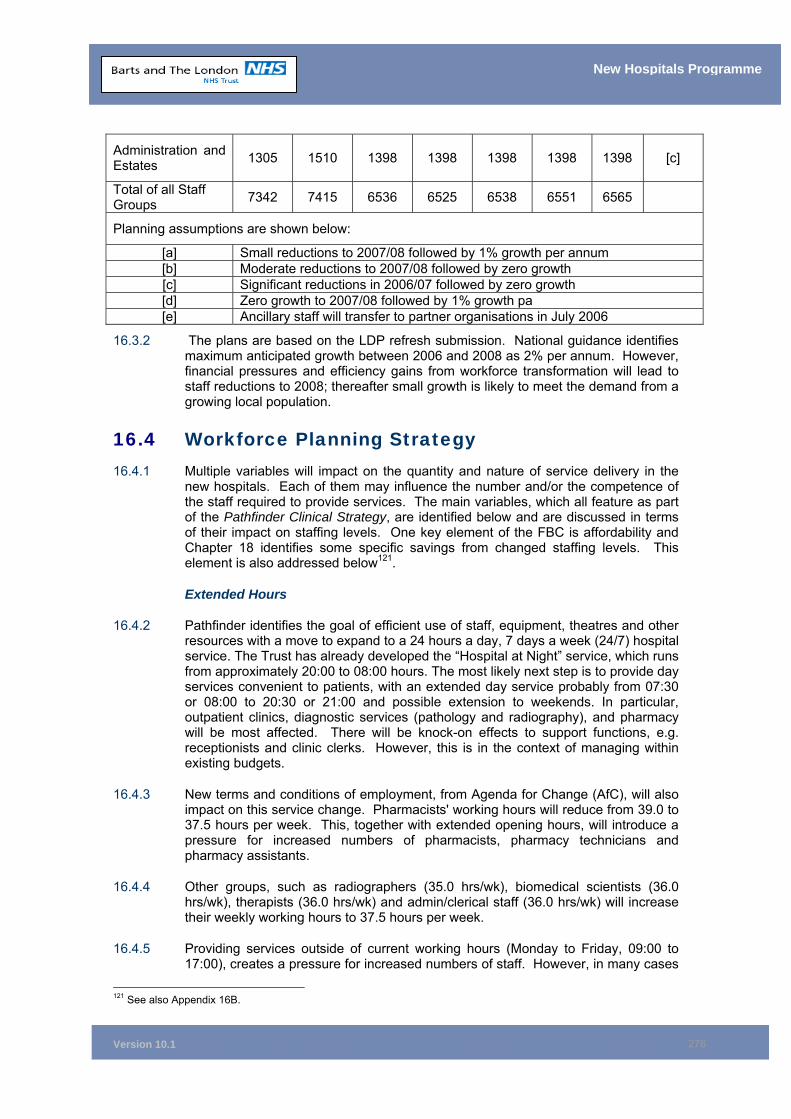
Version 10.1
276
New Hospitals Programme
16.3.2 The plans are based on the LDP refresh submission. National guidance identifies maximum anticipated growth between 2006 and 2008 as 2% per annum. However, financial pressures and efficiency gains from workforce transformation will lead to staff reductions to 2008; thereafter small growth is likely to meet the demand from a growing local population.
16.4 Workforce Planning Strategy 16.4.1 Multiple variables will impact on the quantity and nature of service delivery in the
new hospitals. Each of them may influence the number and/or the competence of the staff required to provide services. The main variables, which all feature as part of the Pathfinder Clinical Strategy, are identified below and are discussed in terms of their impact on staffing levels. One key element of the FBC is affordability and Chapter 18 identifies some specific savings from changed staffing levels. This element is also addressed below121.
Extended Hours
16.4.2 Pathfinder identifies the goal of efficient use of staff, equipment, theatres and other resources with a move to expand to a 24 hours a day, 7 days a week (24/7) hospital service. The Trust has already developed the “Hospital at Night” service, which runs from approximately 20:00 to 08:00 hours. The most likely next step is to provide day services convenient to patients, with an extended day service probably from 07:30 or 08:00 to 20:30 or 21:00 and possible extension to weekends. In particular, outpatient clinics, diagnostic services (pathology and radiography), and pharmacy will be most affected. There will be knock-on effects to support functions, e.g. receptionists and clinic clerks. However, this is in the context of managing within existing budgets.
16.4.3 New terms and conditions of employment, from Agenda for Change (AfC), will also impact on this service change. Pharmacists' working hours will reduce from 39.0 to 37.5 hours per week. This, together with extended opening hours, will introduce a pressure for increased numbers of pharmacists, pharmacy technicians and pharmacy assistants.
16.4.4 Other groups, such as radiographers (35.0 hrs/wk), biomedical scientists (36.0 hrs/wk), therapists (36.0 hrs/wk) and admin/clerical staff (36.0 hrs/wk) will increase their weekly working hours to 37.5 hours per week.
16.4.5 Providing services outside of current working hours (Monday to Friday, 09:00 to 17:00), creates a pressure for increased numbers of staff. However, in many cases
121 See also Appendix 16B.
Administration and Estates 1305 1510 1398 1398 1398 1398 1398 [c]
Total of all Staff Groups 7342 7415 6536 6525 6538 6551 6565
Planning assumptions are shown below:
[a] Small reductions to 2007/08 followed by 1% growth per annum [b] Moderate reductions to 2007/08 followed by zero growth [c] Significant reductions in 2006/07 followed by zero growth [d] Zero growth to 2007/08 followed by 1% growth pa [e] Ancillary staff will transfer to partner organisations in July 2006
Version 10.1
277
New Hospitals Programme
AfC extends the basic working week for many employees and careful re-allocation of these additional hours, together with the development of creative rotas to provide high staff numbers at peak activity times, could make this organisational change neutral in terms of staffing numbers and costs. However, travelling time to work could be a counter-pressure to the flexible deployment of staff for short evening or weekend shifts.
16.4.6 A further factor that will be considered is independent sector provision (ISP) of diagnostic services, which will commence in 2006. This is designed to release additional capacity outside the Trust. It allows for partnerships which may translate into private sector or foundation hospitals, providing out of hours services in NHS hospitals. While this might ease the pressure of the labour market, it would be a cost pressure.
16.5 New Models of Care 16.5.1 This is expected to embrace some or all of the following:
Supplementary Prescribing
16.5.2 The main impact will be on training time for nurses and pharmacists.
One Stop Clinics/See and Treat
16.5.3 The service provision is staff and cost neutral. This is predicated upon the new service being instead of, not in addition to, an old one. This will require attention to the fine detail of project management and benefits realisation.
Long Term Illnesses
16.5.4 The national strategy for the care of people with chronic illnesses is based on case management by community matrons. In principle, this should relieve pressure on both A&E and outpatient clinics. However, it will be difficult to isolate its impact from other multiple issues. In practice, therefore, it is unlikely to release staff time or funds.
Discharge Planning and Reduced Lengths of Stay
16.5.5 Pathfinder identifies reduced length of stay as a key measure of improved efficiency in certain areas. The consequence of this is that average patient acuity will rise which might require a rise in the nurse/bed ratio and skill mix and a growth in the level of support services, (e.g. pathology and imaging, pharmacy, clerical, laundry, portering and cleaning). It could also impact on follow-up, outpatient clinic work.
New Roles
16.5.6 The modernisation agenda identifies multiple opportunities for new roles. Chief among them is the Assistant Practitioner. This is being tested in diagnostic imaging and could resolve vacancy rates of over 20 per cent among radiographers.
16.5.7 In nursing, there is a well-established staff balance between qualified nurses and healthcare support workers (HCSWs). Currently, HCSWs are trained to NVQ level 3, but use of Foundation degrees is under active consideration. The Trust has developed many services by use of Specialist Nurse Practitioners and there is much evidence to demonstrate the value of Nurse Surgical Practitioners, capable of doing independent minor surgery.
Version 10.1
278
New Hospitals Programme
16.5.8 Staffing in pharmacy has changed considerably with an expanded role of pharmacy technicians and moves for them to be a registered profession. There is probably little scope for major modernisation initiatives.
16.5.9 In all these areas, workforce transformation and the appropriate use of new roles will be central to the benefits realisation strategy.
16.6 Thames Gateway 16.6.1 The Thames Gateway is a major urban regeneration project. The population of
North East London is projected to grow by 310,500, and the population of Tower Hamlets alone is expected to experience a growth in population of some 100,000 residents. This will create a demand for healthcare equivalent to that made upon a medium-sized (650 bed) district general hospital. NELSHA estimates increased demand of 66,000 outpatient appointments and 91,000 A&E attendances.
16.6.2 The NELSHA strategy, however, precludes the building of a new hospital and places less reliance on acute hospital beds. It focuses on primary care and the use of community service provision (see long term illness strategy above). The risk to the Trust is that, if the primary and community care strategy does not deliver the expected benefits, the demand placed on The Trust will rise substantially.
16.6.3 The underlying workforce plan will therefore include a risk assessment and contingency plans for various scenarios to enable the Trust to manage excess healthcare demand and additional demand for staff within the capacity of the new hospitals.
16.7 Technology and Design Computerised Prescribing/Robotic dispensing
16.7.1 The effect will be to reduce a part of the workload in pharmacy. These tools are expected to reduce prescribing and dispensing errors and therefore save time in correcting errors and reducing clinical risk.
IV Additives
16.7.2 This should lead to a marked reduction in infections and other clinical risks with a saving on nurse time.
LIMS and Modern Technology in Pathology
16.7.3 The business case for the Pathology and Pharmacy new build project identified savings from reduced staffing levels, amounting to £1 million arising from centralisation, a modern ICT system and new analytical technology. It was identified that these savings would be used to fund the affordability of the new hospitals, and they are therefore factored into the affordability position in Chapter 11 (see Figure 82). These benefits are also set out in Figure 117 in paragraph 18.4.3.
16.7.4 However, additional service demand pressures from reduced lengths of stay and Thames Gateway population increases (identified above) may impact on these savings. Close project management will be required to ensure realisation of these benefits.
Version 10.1
279
New Hospitals Programme
16.7.5 The underlying workforce plan will need to address the risk from escalating service demand, identify strategies to meet various contingencies and deliver the financial benefits.
CRS
16.7.6 The business case for CRS identifies future benefits in the form of staff savings. Clearly, the provision of an integrated database of patient information will preclude the need to search for missing health records and to retrieve test results. This will reduce the work of health records clerks, junior doctors, and ward support staff. However, there will be increased work in the realm of CRS training and the registration authority to cope with the annual turnover of say 15% in nursing, therapy and diagnostic staff and the bi-annual change of house for junior doctors.
16.7.7 Savings will be made, particularly in A&C staff, but close project management will be required to realise the benefits and prevent work expanding to fill the vacuum and increase the quality of care.
PACS
16.7.8 Implementation of PACS would negate the need to have reporting radiologists in the same location as the hardcopy images. It could lead to external provision of reporting services (e.g. overseas staff reporting overnight or a regional service with efficiencies of scale). It should lead to savings and reduced demand for staff benefits which are not included in this business case are included under the CRS project benefits. The Trust is an early adopter of a Radiology Information System and PACS. Work is in progress for the procurement and implementation of these systems with a projected “go live” date of June 2006. (The Trust has made provision for some onsite storage of hard copy images, both co-located with Imaging and remotely which, if not required in the future allows for some restricted soft space areas.)
Ward Design in New Hospital
16.7.9 The design of wards in the new hospitals will raise the level of privacy, which should in turn enhance the quality of the patient experience.
16.7.10 Single rooms (which are more easily cleaned) will reduce hospital acquired infection rates and lower the incidence of diarrhoea outbreaks. This will increase the quality of the patient experience and will also reduce the workload of nursing staff.
16.7.11 On balance, the impact of the ward design might be on staff numbers. However, this will require more detailed consideration as part of the underlying workforce plan. The assumption from an affordability perspective is that it is cost neutral.
Consolidation on to Two Sites
16.7.12 Closure of The London Chest Hospital (LCH) will reduce the number of operating theatre suites. Economies of scale will therefore reduce the staffing levels of theatre staff (junior doctors required for 24 hour a day cover and nurses) and realise the benefits identified in Chapter 18, Figure 117 and Appendix 18A.
16.8 Efficiency Gains 16.8.1 A national workforce modelling initiative conducted as a back-drop to local
development planning identifies an expected growth of 4% per annum across all specialties and functions. These forecasts draw upon commitments for expansion
Version 10.1
280
New Hospitals Programme
made in Delivering the NHS Plan and planning and priorities guidance 2002/03. However, these “targets” are indicative and not absolute.
16.8.2 Balanced against these forecasts of expansion are efficiency gains of 2.7% per annum (see Chapter 11, paragraph 11.4.6 and Figure 83) arising from the report Releasing Resources to the Front Line – Independent Review of Public Sector Efficiency, commonly known as the Gershon Report. Cost pressures for the New Hospital Project arising from the expected increase in front-line staff have been identified above. However, most of the finance to support expansion will have to be found from efficiency gains from “back room” services, or from workforce transformation gains. These will contribute to the additional efficiency savings of £6.4 million required by 2014/15 (see Chapter 11, Figure 82).
16.9 The HR Strategy
Figure 109 -Trust HR Strategy
New Hospitals Programme
Trust HR Strategy– Three Elements
HR in th
e NHS P
lan
Change Management to support Models of Care
Working in Partnership
16.9.1 The Trust’s HR strategy has three main elements as shown in Figure 109.
16.10 Delivering HR in the NHS Plan 16.10.1 The first element is delivering HR in the NHS Plan, under the four pillars shown in
Figure 110 below.
Version 10.1
281
New Hospitals Programme
Figure 110 HR in the NHS Plan - the Four Pillars
New Hospitals Programme
Making the NHS a Model Employer
Model Employer
Improving Working Lives and Beyond
Ensuring the NHS provides a Model Career. The Skills
Escalator
Model Career
Four Modernisations Workforce Planning Pay
RegulationLearning and Personal
Development
Improving Staff Morale
Improving the image of the NHS as an
employer
HRM Development
Building CapacityQuality and ‘Attitude’
Pillar One – making the NHS a model employer
• Ensuring staff involvement and partnership working through interim services, steady state and beyond;
• Ensuring achievement of IWL Practice Plus status and gaining ongoing commitment of private partners;
• Ensuring diversity of the workforce through robust strategies agreed with private partners that embrace the community and regeneration initiatives;
• Ensuring best practice human resource management especially in relation to dignity and safety at work;
• Providing uninterrupted, accessible, affordable and good quality childcare support; and
• Through the Retention of Employment (ROE) model, ensuring continuing access to membership of the NHS pension scheme and encouraging participation in modernisation of the scheme through partnership working.
Pillar Two – the four modernisations
• Ensuring that Agenda for Change (AfC) is applied throughout the transferred workforce, and for replacement posts, using the Trust’s Transfer Agreement, which is incorporated into the Project Agreement concluded with Project Co.;
• Ensuring that consultants embrace the new Consultant Contract and its associated transformation opportunities sufficiently in advance to support new models of care, patient choice and new funding streams;
• Achieving working time regulation compliance for junior doctors by successful implementation of the Hospital at Night Project and redesign of rotas in advance of the new build and during interim services, while ensuring participation in and achievement of, modernisation of medical training;
• Securing private partner commitment to the Trust’s training and development strategy. In particular developing the commitment, skill and competence of
Version 10.1
282
New Hospitals Programme
managers within the Knowledge and Skills Framework and annual appraisal/personal development planning; and
• Working with the private partners to share resources and enhance access to training and development opportunities including sourcing initiatives through regeneration.
Pillar Three – improving staff morale
• Ensuring robust workforce planning to reach agreed targets and aspirations of patients and staff, including ongoing engagement of NE London SHRINE and the Strategic Health Authority to ensure a regional perspective;
• Ensuring staff engagement at all levels in initiatives for working differently;
• Ensuring commitment of private partners to flexible working initiatives and continuing access to a broad range of staff benefits;
• Implementing national communication strategies in addition to local, targeted communications regarding the new build; and
• Ensuring ongoing commitment to annual staff survey by private partners and monitoring of resultant action planning.
Pillar Four – building people management skills
• Ensuring development of HR capacity and capability to underpin organisational development during an 8 year building programme;
• Developing HR leadership capabilities to ensure delivery of major priorities, e.g. increasing workforce numbers; working differently; implementing Working Time Regulations, Agenda for Change and Consultant Contract and developing the appropriate culture to support achievement of the Trust’s clinical strategy; and
• Ensuring effective and timely implementation of IT solutions and underpinning training of staff.
16.11 Change Management to Support Models of Care 16.11.1 The second element of the strategy is to facilitate change management to support
the new models of care by:
• Ensuring that patients choose to be treated at Barts and The London;
• Implementing the Trust’s Pathfinder strategy to support achievement of excellence throughout the Trust in everything we do; and
• Confirming the role of service transformation and workforce transformation in supporting modernisation and working differently.
16.12 Working in Partnership 16.12.1 The third element is to develop a partnership approach with the staff
representatives (Staffside) and indeed all staff.
16.12.2 More detail about the different elements of the strategy is set out in Appendix 16C.
Version 10.1
283
New Hospitals Programme
16.13 Implementing the HR Strategy HR Staff Capability and Capacity
16.13.1 Successful implementation of the HR strategy will be underpinned by the ongoing development of HR staff throughout the Trust. The Trust is actively engaged in the NE London SHRINE Project on enhancing HR capability and capacity. During 2004 the HR Directorate launched an HR Graduate Rotational Programme to support the Trust’s devolved HR structure and ensure career development. This also supports succession planning, which is an underpinning strategy to ensure that motivated, competent and experienced HR staff are retained to support organisational development. The HR Directorate currently has 4 graduates employed on the programme, with a further 2 graduates employed within the Agenda for Change Project Team.
Recruitment and Retention
16.13.2 The Trust has a continuing drive to recruit and retain the highest calibre staff. Amongst the initiatives to be carried forward are: the recruitment of nurses and other healthcare professionals from abroad the rotational programme for newly qualified nurses; and the support provided for nurses to take on greater responsibilities and progress from D to E grade. Two staff are employed within recruitment Services to lead on recruitment and retention for nursing, the largest staff group, which has a formal exit interview process.
16.13.3 It is intended to embed the exit interview process throughout the Trust during 2005/06 using the partnership arrangements for consultation. Strategic implementation of Agenda for Change and realising the benefits identified will also enhance recruitment and retention of all staff.
Recruiting from the Local Community
Regeneration and Community Employment
16.13.4 The Trust scoped out its regeneration potential in Reaping the Benefit in 2003. This work led to the appointment of a Regeneration Manager in 2004. Following on from this, the Trust adopted an outline regeneration strategy in May 2004 – Improving Health, Growing and Sustaining Prosperity attached at Appendix 2B.
16.13.5 This sets out a series of objectives in relation to the Trust’s role as an employer, buyer of goods and services, developer and community institution. In response to this the consortium have appointed a Community Relations Manager and a joint approach is planned in leading regeneration activity. Central to the strategy is the aim of supporting community employment. The Trust has established an Actions for Community Employment (ACE) group chaired by the Regeneration Manager. The ACE entry level project has established a targeted local recruitment process in jobs requiring an NVQ2 or less, including A & C 3 and 4 grades, ancillaries, HCSWs, MLAs and junior technician staff. The ACE Project is expected to fill over 240 jobs per year with local people and will supply additional training where required at pre-employment and vocational levels. Since the project started in January 2005 26 people have been offered work through the process. ACE has been implemented in collaboration with Job Centre Plus and Employment Solutions (a local brokerage partnership).
16.13.6 The Trust recognises its role in the local community as one of the major employers in the area. Apart from jobs in health and facilities management, the construction programme will create 1,500 vacancies. The consortium has committed to filling
Version 10.1
284
New Hospitals Programme
these posts locally with a target of ensuring that 20% are filled by the local community within three years of the start of construction. Employment and training programmes are being negotiated with funders such as the Local Authority and Job Centre Plus. Costs associated with monitoring arrangements are under discussion with Skanska. This will not be a cost pressure to the Trust. However, systems will be established post-financial close to monitor the costs.
16.13.7 To raise the profile of the employment opportunities at entry level, both within the Trust and created by the construction, a locally accessible recruitment facility (“job shop”) will be set up that will provide details on employment opportunities as well as a range of support functions, e.g. information on NVQs and other qualifications and support in completing application forms. It is planned that the facility will be an on-site, drop-in recruitment “shop” at The Royal London site.
16.13.8 By raising the profile of opportunities at entry level, the Trust is focused on increasing the numbers of staff from the local population and, in particular, those from disadvantaged backgrounds, to ensure that the workforce within the Trust and the opportunities presented by the construction better represent the ethnic mix of the community. The Trust also promotes the “skills escalator”. The skills escalator is a framework for people to gain skills and knowledge to enhance their current role and promote career development through learning. It recognises that individuals need different things at different stages in their life and adopts a “step on, step off” ethos to cope with changing life styles.
16.13.9 The Trust continues to build on the links with local schools and agencies to provide and support career and employment opportunities within the Trust. The Trust is working jointly with Project Co. to strengthen these relationships and provide further opportunities for the local population as building work proceeds. The Trust is working in collaboration with local agencies on the following:
Workwise
16.13.10 The Trust has recruited 26 people to the Volunteers in Partnership (VIP) programme that is designed to help people find employment and increase the number of volunteers working in the organisation. The Trust places the volunteers in “real work” environments with a view to helping them gain employment within the organisation. Some volunteers receive training for an NVQ Level 2 qualification. 16 participants have now been place into employment through Work Wise.
16.13.11 The Trust has also commenced a partnership with Groundwork East London whereby Groundwork submit applicants for extended work placement. During this time (which lasts for up to six months) Groundwork pay the participants and provide training and support with a view to the Trust taking them on when vacancies occur, assuming performance is satisfactory. The Trust has highlighted portering and domestics as potential placement areas. This scheme has been merged with the Actions for Community Employment (ACE) programme with the Community Employment Manager acting as the liaison point.
Apprenticeship Schemes
16.13.12 The Trust introduced an Estates Apprenticeship Scheme in 2001. Initially, prospective candidates were selected from trainees attending an 18-week foundation engineering course in partnership with the training provider.
16.13.13 The apprenticeship scheme is a three-year training programme across the Trust sites. It works towards completing an EMTA NVQ level 3, as well as providing day release for a formal City and Guilds qualification in electrical or mechanical engineering.
Version 10.1
285
New Hospitals Programme
16.13.14 The Trust currently employs 7 trainees, four electrical and three mechanical. Four are scheduled to complete their training in 2005 and three in 2007. Plans include further recruitment every two years. The private provider is fully committed to continuing with the scheme with the potential to expand the numbers and roles, this commitment was included in SI’s bid submission. Costs for the training elements of the apprenticeships are expected to be borne by the Learning Skills Council.
Training and Education
16.13.15 The Trust has a large Training and Development department that offers a diverse range of courses and seminars for staff and supports nationally recognised external courses, e.g. post graduate qualifications including MBAs. Within the current training and development decanting suite are dedicated areas for ICT training (including ECDL qualifications) and the Medical Simulation Centre. The department also provides training and development support to those staff who are impacted by the new hospitals programme and in particular the staff at Swanley Laundry, which has now closed.
16.13.16 An example of the success of the support provided to the laundry staff is included at Appendix 16D. The department has a key role in supporting continuing professional development for staff, which is identified through the appraisal process and personal development planning. Training and development will also be fundamental to broadening the horizons of staff who, as a result of the planned changes to the NHS pension scheme, remain at work for longer that anticipated and may need, or aspire to, a change of career. The department will transfer to a purpose-built facility in the new hospitals build that will provide efficient use of resources by co-locating all departments offering training and education and the sharing of resources.
16.14 Change Management Introduction
16.14.1 The Service Transformation Directorate has been responsible for delivering and supporting a number of Trust-wide change projects. These have been driven by the changes required by the new models of care. The changes that have been introduced cover a range of system, process, cultural and people changes. These have included the streaming of hospital services (trauma ward, short stay surgery and day surgery), more efficient diagnostics, building organisational capacity for change, introducing the Care Record Service (CRS) and developing a more effective organisational culture.
16.14.2 The Trust’s Pathfinder clinical strategy (attached at Appendix 3A to the FBC) provides a framework for strategic planning over the next five years. Business plans will continue to be developed annually to ensure that priorities are set and progress is sustained. For further information see Chapter 3.
16.14.3 The Service Transformation Directorate has been responsible for delivering and supporting a number of Trust-wide change projects. These projects have been driven by the changes required by the new models of care.
The Change Management Approach
16.14.4 The change approach will be led by the Director of Operations (who also leads on Benefits Realisation), underpinned by the following principles:

Version 10.1
286
New Hospitals Programme
• Strategy: all change effort must contribute towards the realisation of Pathfinder.
• Benefits realisation: building on the benefits in the FBC to further quantify benefits, establish ownership and drive realisation.
• Scoped to meet future needs and a good fit for the new hospitals: shaped by the clinical output specifications produced by the relevant clinical specialties and the Capital Strategy Team/PFI Clinical Team and drivers in the wider environment that will further affect models of care.
• Learning from the change experience associated with other large new hospital projects: this should include both NHS and private sector experience.
• Systems, Processes, People, Culture, Partnerships: projects will be established to plan and implement changes to systems and processes, set direction from the top and engage the people below. These will focus simultaneously on the hard (structures and systems) and the soft (corporate culture e.g., leadership, decision making), and encourage appropriate internal and external partnerships (including engagement of patients, the PCT and the Medical School). Evidence-based process improvement techniques (e.g. the 10 High Impact Changes, capacity and demand analysis and statistical process control) will be used.
• Integration: with the new hospital team and with wider organisational change in the Trust.
• Enabling business needs: ensuring targets are met. Operational issues must be considered when designing the detailed plans.
• Financial limitations: working within any limitations imposed by the current hospital design.
• Incremental approach, not big bang: that takes into account business needs and the organisation’s capacity to deal with change. Early action will be taken on those changes that can be implemented prior to the move.
• Dedicated change managers: an expert and highly skilled resource that will ensure employees remain motivated and effective within the change process.
16.14.5 A full project plan is in development based on the approach detailed above. It is anticipated that this plan will identify the following products to be completed by June 2006:
• Potential benefits: these have been identified at a high level within the business case for the new hospitals. A detailed benefits management strategy will define, in detail, how the project will monitor, deliver and realise the expected benefits. By September 2006 we will have developed individual benefits profiles and a benefits register populated with detail and responsible owners. A final benefits realisation implementation plan will be produced by June 2006122.
• A risk and issues log associated with change management.
• A full register of the design assumptions that have been made that require a change in systems and processes. This register will need to be integrated with the benefits register and future projected activity. For example, efficiency savings as a result of reduced lengths of stay and the assumption that 25% of current outpatient work will not be undertaken with the hospitals. This register should be separated into those changes that are Trust-wide (such as the introduction of housekeepers and the new shape of wards) and those changes
122 See Appendix 18B.
Version 10.1
287
New Hospitals Programme
that are specialty-specific. It must focus on both non-clinical and clinical changes.
• A consolidated plan of future national and local changes that are likely to influence the future of how clinical care will be provided. Local changes will include planning assumptions of the Medical School and referring PCTs.
• A report on lessons learned from other large changes associated with new building projects. This will be drawn from desk research, interviews with key people from a variety of different sectors and seminars with external speakers.
• A change project plan for the new hospitals based on each of the points above. This plan will scope those changes that must take place in order to move into the new hospitals and those changes that the new hospitals enable. It will detail both those changes that are not dependent upon the new buildings and could therefore be implemented earlier and those changes that could take place at the time of the move or even after. In this way we will ensure a phased approach rather than a big bang approach. The plan will demonstrate clear priorities and be targeted at those areas that will deliver the most benefits.
• A Change Management/Benefits Realisation Steering Group, has been established, accountable to the New Hospitals Programme Board, with clear terms of reference to approve and deliver the change plan. Members of this Board (see Appendix 18C) include representatives from clinical and corporate directorates to ensure critical integration with other change projects in the Trust.
• Dedicated change managers, initially to scope the project (including any need for further dedicated change resource) and then to deliver it.
• Change champions identified in each specialty. Ideally, these should be people who have worked with the PFI Clinical Team to develop the specifications and sign-off the drawings.
• Process maps of the priority changes with change impacts identified. These will have been produced by the change manager and relevant staff working in those areas.
Care Record Service (CRS)
16.14.6 The Trust is one of the “fast track” sites to implement the Care Record System (CRS), which provides electronic access to a comprehensive history of patients’ health and care information. It gives immediate access to medical records and care notes 24/7, including patient access to their own records.
16.14.7 Implementation of CRS will improve patient care by providing clearly defined clinical standards; electronic requests for tests and procedures and electronic results; discharge planning; on-line bed management and management information. The system contains the “choose and book” system to underpin patient choice; improve communication between patients and health professionals; provide faster and more efficient services and an assurance that individual care history is up-to-date.
16.14.8 The benefits to staff include:
• Instant access to patient records, diagnostic images and results 24 hours a day, seven days a week;
• Improved information about patients, including knowledge of all care providers involved in the treatment of the patient;
• Greater support in diagnosis and easier access to up-to-date information;
Version 10.1
288
New Hospitals Programme
• Reduced time taken for admin tasks;
• More efficient and appropriate referrals between care sectors;
• Increased safety in prescribing, the monitoring of prescriptions and alerts to contraindicated therapies;
• Better data to support clinical audit and research; and
• These benefits have not been attributed to this business case as they are benefits attributable to the implementation of CRS.
16.14.9 CRS provides a further catalyst for change by engaging staff in role redesign and the practicalities of clinical design in the new build to optimise this significant development in the national programme for IT Connecting for Health. The project is underpinned by a dedicated CRS team, a Programme Board and inclusion of all stakeholders at all levels. The project is overseen by the Programme Assurance Board.
16.14.10 A major strand of the project is the clinical transformation work and associated “benefits realisation” (details of which are included as Appendix 18A). Roll-out of the necessary training (and ongoing training needs of new and temporary staff) is being carefully planned to ensure the minimal disruption to service delivery. However, once CRS is embedded in the NHS, all relevant staff will have undergone the necessary training and registration, leaving only new staff and some temporary staff to be trained.
16.14.11 The Programme Assurance Board ensures that projects such as CRS integrate with all other projects underway or planned within the Trust.
New Roles for Staff
16.14.12 Service and workforce transformation necessitates creative role design and services delivered by high performing teams. Catalysts for change such as Agenda for Change, the implementation of CRS (and Choose and Book), the Consultant Contract and the new hospital build, provide an unprecedented opportunity to redesign roles. For example, nurses taking on responsibilities traditionally undertaken by medical staff, clinicians accessing patient notes and x-rays electronically at the bedside, NVQs for radiographic support workers to undertake simple examinations (e.g. chest x-rays),and enriching the role of medical secretaries as booking patients into clinics diminishes.
16.14.13 A dedicated post of Role Design Facilitator has been established in Training and Development to ensure that all opportunities to modernise and enrich are identified and followed through, supported by consultation arrangements and working in partnership. Re-organisation and restructuring of departments is already underway in advance projects such as Pharmacy and Pathology who moved into newly built premises early in 2006, providing good learning experiences for the major new build opportunities.
Transition (to new environment)
16.14.14 This is a nine-year build that requires detailed interim arrangements and complex decanting arrangements to ensure continued delivery of high quality, responsive services. It is also of the utmost importance to engage staff throughout the process. Regular exhibitions of the plans and opportunities for staff to visualise and question the outcomes have been provided. Included in the bid submission are “mock-ups” of wards and clinical areas where staff can familiarise themselves with the design, layout and the clinical specifications throughout the construction phase. There is

Version 10.1
289
New Hospitals Programme
robust engagement of clinicians at all levels, particularly in the process of achieving signed-off 1:50 drawings.
16.14.15 Wherever possible, the Trust is adopting a “one decanting only” approach to the movement of staff and patients to facilitate demolition and rebuild. Each decanting is supported by full engagement of the staff and the unions which will continue through to the new environment.
16.14.16 The Trust will reflect and learn from each discrete transition a process which started with redevelopment initiatives that were completed during 2004. At Barts, a centre of excellence for breast care has been created in the West Wing. The centralisation of radiology services has brought the Breast Unit and the patients it treats, major benefits in improvements in efficiency and communications. This has in turn created much more efficient and effective working relationships, providing a major positive impact on team. High performing teams support excellence in service delivery, recruitment and retention and high morale in staff. The knock-on and immediate benefit to the patients, is the ease with which they now move through the system.
Trust’s Relationship with Educational Institutions
16.14.17 The Trust is working closely with City University, QMUL and other educational institutions to ensure that:
• The workforce needed for tomorrow is secured;
• The use of the MPET levy is prioritised to ensure that education is fit for purpose;
• The planning process for service delivery is robust and reflects educational requirements; and
• Increases in training commissions for nurses, doctors and midwives are accommodated, including supporting return to practice and refugee professionals.
16.14.18 Significant investment has been made to enhance development opportunities for all grades of staff through investment in continuing professional development and establishment of nurse rotations. Priorities for investment are jointly generated through the Trust and the SHA through the WDC.
16.14.19 Our principles for delivery focus on:
• Doing things differently;
• Being focused on patient pathway and needs;
• Workforce roles that are more flexible and based on competencies;
• Full use of the skills escalator;
• A workforce to reflect our local communities; and
• Driving new ways of commissioning education and training that is multi disciplinary, competency and outcome based and measurable.
16.14.20 Through our partnership arrangements with City University, plans have been agreed in relation to changes to our commissions and the timing of intakes to the benefit of both the service and education provider. The partnership arrangement is being continuously strengthened through regular meetings and open dialogue to ensure that there is a greater understanding of workforce requirements through our planning process.
Version 10.1
290
New Hospitals Programme
16.14.21 Our role on the WDC Board has helped to shape the way in which educational funding is used to meet future service need and is measured by a shift in funding to support non-professional routes including Foundation Degrees as a means to widening access and supporting advancement.
16.14.22 Our work with the Medical School has been strengthened through the Joint Strategy Group and the establishment of a joint R & D office. There is agreement to establish a joint education office which will support our common agendas. The establishment of the NE London Foundation School for MMC will help build the base for this work, along with the roll-out of the generic training programme for F1 and F2 posts. The delivery of the generic training of these doctors will include other professionals which supports our strategy for integrated learning.
16.14.23 We continue to work with other education providers, local schools and colleges to ensure that we offer opportunities to local students who are interested in careers in health and have established work experience programmes, taster days and summer schools. This underpins our plans to widen access and raise awareness of the wide range of careers that are on offer and the educational programmes that we offer to support these roles.
Closure of Trust Sites
16.14.24 As the construction progresses, some of the sites from which staff will be working will be closed. Namely these are:
• Laundry at Swanley in August 2005;
• Central Production Unit (CPU) at Wapping lease expires in 2009;
• London Chest Hospital in 2014/15; and
• Prescot Street lease expires in 2015.
16.14.25 The London Chest Hospital will remain open for the delivery of clinical services, namely Cardiac Services, until the construction on the two main sites is completed in 2014/15. Following completion of the Cardiac Department at Barts, the clinical and administrative staff will be relocated to their new base at Barts.
16.14.26 A change management process will be agreed nearer the time of transfer that is in line with Trust policies and procedures and with full consultation of staff and Trade Unions. This will draw on the experiences of the moves into the Advance Works and ongoing decanting arrangements. The Trust has not planned for any redundancies as a result of the relocation.
16.14.27 While the service provider has not indicated the preferred option for the CPU when the lease expires in 2009, they have indicated that it is likely that the lease will not be renewed due to the need for significant capital investment. However, the consortium has provided a commitment to the Trust that it will avoid compulsory redundancies and the Trust’s Security of Employment Policy will apply. It is anticipated that the length of the time prior to closure of these two sites will allow sufficient planning of manpower, to ensure that the service providers can redeploy any affected staff within the Trust.
16.15 Staffside Involvement 16.15.1 Throughout the bidding stage, regular meetings facilitated by HR were arranged
with each of the bidders and Staffside. This enabled Staffside to raise areas of concern and to gather information on such issues as pensions and the bidder’s employee relations’ history. Staffside were also able to visit other PFI project sites
Version 10.1
291
New Hospitals Programme
such as Queen Elizabeth Hospital NHS Trust in Greenwich and South Tees NHS Trust in Middlesbrough to talk to their trade union colleagues and other staff to gain an understanding of previous staff transfers.
16.15.2 Members of Staffside formed one of the evaluation teams that provided input to the selection of the preferred bidder. They were therefore able to influence the outcome to the same extent as other user groups involved in the process. As well as participating in the evaluation process, two members of Staffside (as part of the ITN FM Evaluation Group) were involved in the final decision on the FM preferred partner put forward to the Trust Board.
16.15.3 At preferred bidder stage a series of tripartite meetings have been established between Staffside, the consortia and the Trust. These will be the main consulting forums for the transfer of staff and the agreement on other issues, such as HR policies. Representatives from the third party contracts are to be part of the forum, which is known as the Tripartite Staff Forum. This Forum will continue after transfer of staff and provide the consultative and negotiating machinery for all RoE staff. The service providers have committed to continue to recognise all relevant trade unions and will engage in their own joint consultative and negotiation arrangements, which the Trust will monitor as part of the overall monitoring arrangements put into place.
16.15.4 An HR Operational Group has also been formed with representatives from the Trust and the consortia to oversee the Transfer Agreement for TUPE and RoE personnel and take forward developing HR strategy. Staffside colleagues are invited to participate in this group as appropriate (see Chapter 14).
Future Consultation Pre/Post- Financial Close
16.15.5 The consultation arrangements fall into five discrete areas, as follows:
Overarching consultation through the Tripartite arrangements
16.15.6 Regular formal and informal meetings continue and include the provision of pension briefings for TUPE’d staff. The pension briefings commenced with group, “new company”, pension arrangements and continue with “one-to-one” advice with support from GAD, the NHS pension scheme and the private provider pension schemes, where appropriate. Staffside colleagues have an open invitation to all meetings and briefings.
Formal consultation with the staff at Swanley Laundry
16.15.7 Informal consultation commenced with the staff at Swanley laundry pre-preferred bidder stage, as the potential closure of the site formed part of both bidders’ submissions. Regular interactive briefings have been provided to the staff, in addition to comprehensive “question and answer” sheets and the provision of a “communications box” where staff felt unable to ask their questions direct. Formal consultation commenced in March 2005 and redundancy payments have been made available to staff. Staffside colleagues have participated in all briefings and meetings.
Formal consultation with the 5 trades included in RoE
16.15.8 The Trust’s RoE agreement has been adopted by the Tripartite Staff Forum and is attached to the project agreement. Formal consultation with staff commenced in March 2005 through group presentations and “one-to-ones” on a small group or individual basis. Staffside colleagues fully participated in these arrangements.
Version 10.1
292
New Hospitals Programme
Formal consultation with staff who will TUPE transfer
16.15.9 Formal consultation commenced in for March 2005. Staff who will be subject to TUPE transfer were provided with individual letters in the autumn of 2004 with questions and queries dealt with by the project team and Staffside colleagues. The private providers have delivered informative staff briefings, followed up by copies of slides and question and answer sheets. The TUPE transfer documentation has been drafted by the HR Operational Group and staff members have received individual one-to-one briefings.
Formal consultation with Contractor (third party staff)
16.15.10 The Trust has agreed to TUPE transfer all existing third party FM staff back into the NHS prior to transfer to the private provider The staff affected are domestic and security staff who will therefore benefit from RoE arrangements and the “transfer agreement” that the private provider is obliged to accept. Formal letters ending the contractual arrangements were sent to ISS Mediclean and First Security in the first week of March 2005. A three-month formal consultation period commenced at the same time. The transfers back into the NHS have now been affected and trade union representatives from both groups of staff have been invited to join the tripartite arrangements. A detailed project plan is currently being finalised by the Trust to underpin all future consultative arrangements.
16.15.11 The consultation arrangements impact on Payroll, who are fully engaged in the transfer process and advising on timelines to achieve successful transfers both in and out of the NHS. The private provider has committed to utilising the Trust’s own payroll consortium to pay the RoE staff and so ensure the correct application of Agenda for Change.
16.15.12 Individual support is being given to staff that will be very close to retirement at the date of transfer.
Recognition Agreement
16.15.13 HR Clinics have been established across the 3 main sites, in partnership with the private providers. They provide a drop-in centre to address individual staff questions and concerns. Flyers are sent out on a regular basis.
16.15.14 The introduction of the Trust’s new Partnership Agreement will include the provision of the Tripartite Staff Forum as a formal sub-group of the Partnership Board and will include representatives of the service providers. The partnership agreement and facilities arrangements are scheduled to be adopted a series of facilitated workshops with ACAS (funded by the Charitable Foundation). Scoping of these workshops have been undertaken and they are due to commence early in 2006 after full consultation with Staffside colleagues. Until adopted, the existing recognition arrangements remain as the status quo123.
16.16 TUPE and ROE Provisions Facilities Services
16.16.1 The Trust has some 1,000 FM staff (including third party staff) employed across its 6 sites. All FM services and staff across the Trust’s sites are subject to transfer to the consortia, with the exception of risk management staff, supplies procurement staff and a core facilities management function, all of which are to be retained as
123 See appendix 16E for the Trust’s Recognition and Procedural Agreement.
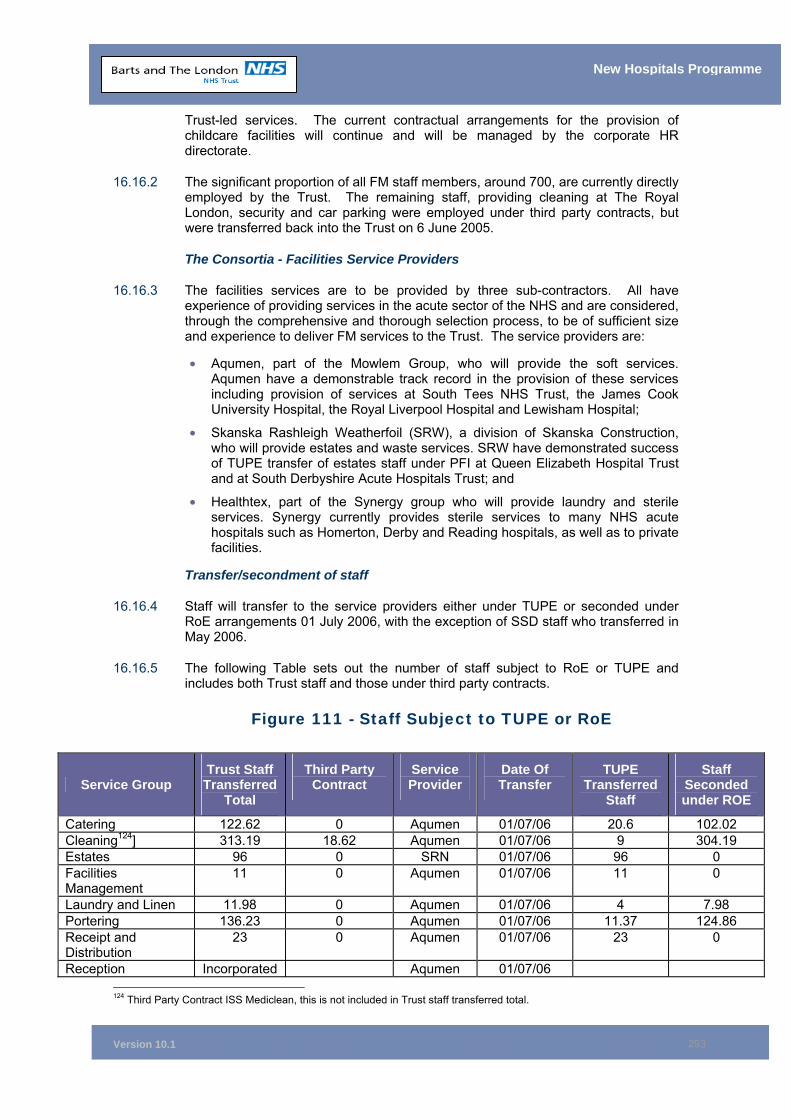
Version 10.1
293
New Hospitals Programme
Trust-led services. The current contractual arrangements for the provision of childcare facilities will continue and will be managed by the corporate HR directorate.
16.16.2 The significant proportion of all FM staff members, around 700, are currently directly employed by the Trust. The remaining staff, providing cleaning at The Royal London, security and car parking were employed under third party contracts, but were transferred back into the Trust on 6 June 2005.
The Consortia - Facilities Service Providers
16.16.3 The facilities services are to be provided by three sub-contractors. All have experience of providing services in the acute sector of the NHS and are considered, through the comprehensive and thorough selection process, to be of sufficient size and experience to deliver FM services to the Trust. The service providers are:
• Aqumen, part of the Mowlem Group, who will provide the soft services. Aqumen have a demonstrable track record in the provision of these services including provision of services at South Tees NHS Trust, the James Cook University Hospital, the Royal Liverpool Hospital and Lewisham Hospital;
• Skanska Rashleigh Weatherfoil (SRW), a division of Skanska Construction, who will provide estates and waste services. SRW have demonstrated success of TUPE transfer of estates staff under PFI at Queen Elizabeth Hospital Trust and at South Derbyshire Acute Hospitals Trust; and
• Healthtex, part of the Synergy group who will provide laundry and sterile services. Synergy currently provides sterile services to many NHS acute hospitals such as Homerton, Derby and Reading hospitals, as well as to private facilities.
Transfer/secondment of staff
16.16.4 Staff will transfer to the service providers either under TUPE or seconded under RoE arrangements 01 July 2006, with the exception of SSD staff who transferred in May 2006.
16.16.5 The following Table sets out the number of staff subject to RoE or TUPE and includes both Trust staff and those under third party contracts.
Figure 111 - Staff Subject to TUPE or RoE
Service Group Trust Staff Transferred
Total
Third Party Contract
Service Provider
Date Of Transfer
TUPE Transferred
Staff
Staff Seconded under ROE
Catering 122.62 0 Aqumen 01/07/06 20.6 102.02 Cleaning124] 313.19 18.62 Aqumen 01/07/06 9 304.19 Estates 96 0 SRN 01/07/06 96 0 Facilities Management
11 0 Aqumen 01/07/06 11 0
Laundry and Linen 11.98 0 Aqumen 01/07/06 4 7.98 Portering 136.23 0 Aqumen 01/07/06 11.37 124.86 Receipt and Distribution
23 0 Aqumen 01/07/06 23 0
Reception Incorporated Aqumen 01/07/06 124 Third Party Contract ISS Mediclean, this is not included in Trust staff transferred total.
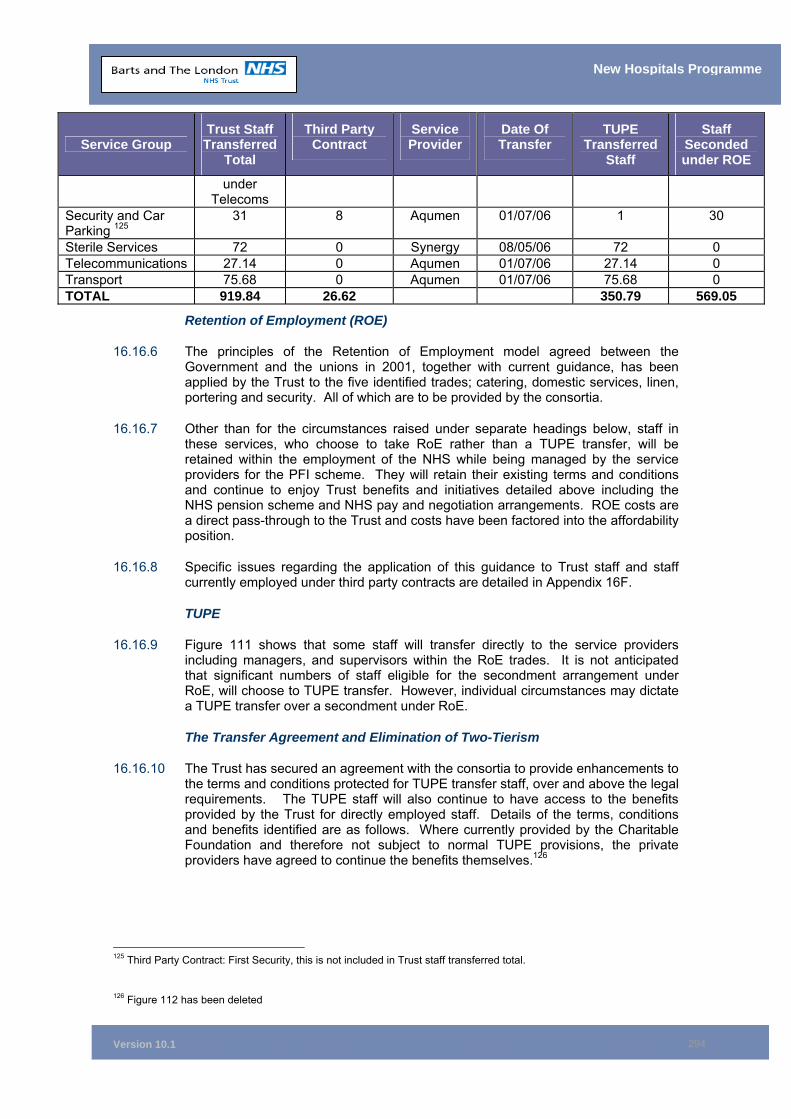
Version 10.1
294
New Hospitals Programme
Service Group Trust Staff Transferred
Total
Third Party Contract
Service Provider
Date Of Transfer
TUPE Transferred
Staff
Staff Seconded under ROE
under Telecoms
Security and Car Parking 125
31 8 Aqumen 01/07/06 1 30
Sterile Services 72 0 Synergy 08/05/06 72 0 Telecommunications 27.14 0 Aqumen 01/07/06 27.14 0 Transport 75.68 0 Aqumen 01/07/06 75.68 0 TOTAL 919.84 26.62 350.79 569.05
Retention of Employment (ROE)
16.16.6 The principles of the Retention of Employment model agreed between the Government and the unions in 2001, together with current guidance, has been applied by the Trust to the five identified trades; catering, domestic services, linen, portering and security. All of which are to be provided by the consortia.
16.16.7 Other than for the circumstances raised under separate headings below, staff in these services, who choose to take RoE rather than a TUPE transfer, will be retained within the employment of the NHS while being managed by the service providers for the PFI scheme. They will retain their existing terms and conditions and continue to enjoy Trust benefits and initiatives detailed above including the NHS pension scheme and NHS pay and negotiation arrangements. ROE costs are a direct pass-through to the Trust and costs have been factored into the affordability position.
16.16.8 Specific issues regarding the application of this guidance to Trust staff and staff currently employed under third party contracts are detailed in Appendix 16F.
TUPE
16.16.9 Figure 111 shows that some staff will transfer directly to the service providers including managers, and supervisors within the RoE trades. It is not anticipated that significant numbers of staff eligible for the secondment arrangement under RoE, will choose to TUPE transfer. However, individual circumstances may dictate a TUPE transfer over a secondment under RoE.
The Transfer Agreement and Elimination of Two-Tierism
16.16.10 The Trust has secured an agreement with the consortia to provide enhancements to the terms and conditions protected for TUPE transfer staff, over and above the legal requirements. The TUPE staff will also continue to have access to the benefits provided by the Trust for directly employed staff. Details of the terms, conditions and benefits identified are as follows. Where currently provided by the Charitable Foundation and therefore not subject to normal TUPE provisions, the private providers have agreed to continue the benefits themselves.126
125 Third Party Contract: First Security, this is not included in Trust staff transferred total. 126 Figure 112 has been deleted
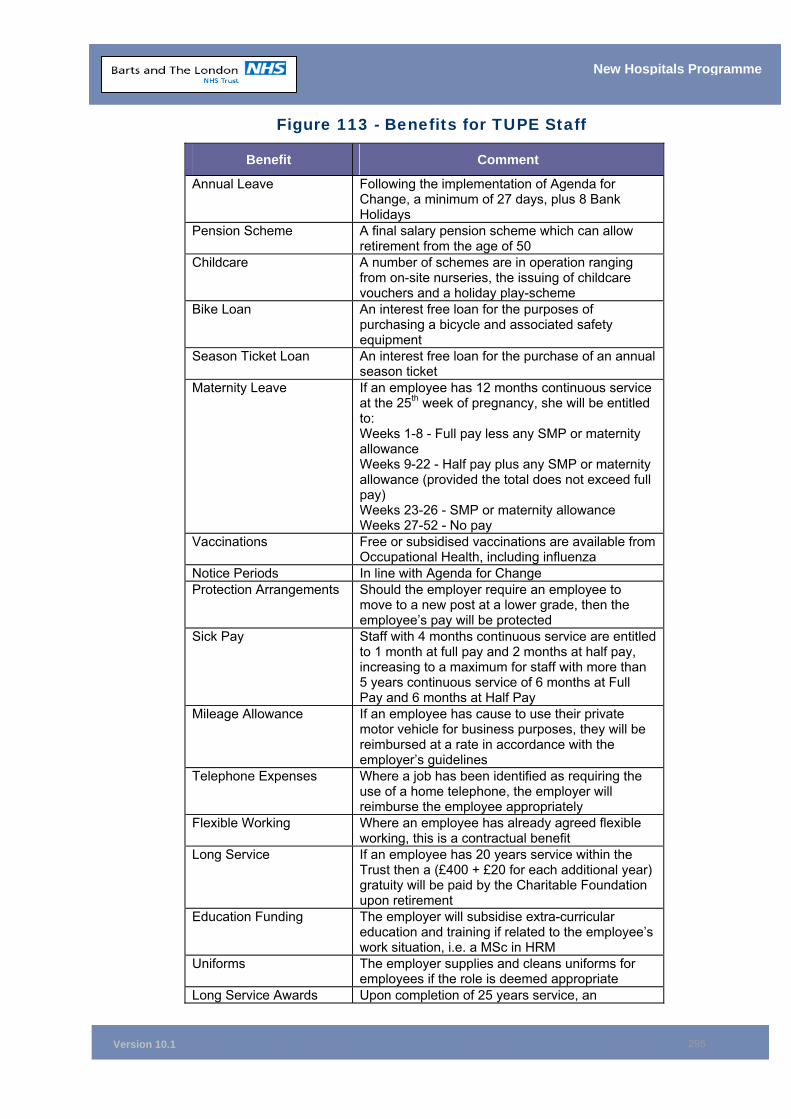
Version 10.1
295
New Hospitals Programme
Figure 113 - Benefits for TUPE Staff
Benefit Comment
Annual Leave Following the implementation of Agenda for Change, a minimum of 27 days, plus 8 Bank Holidays
Pension Scheme A final salary pension scheme which can allow retirement from the age of 50
Childcare A number of schemes are in operation ranging from on-site nurseries, the issuing of childcare vouchers and a holiday play-scheme
Bike Loan An interest free loan for the purposes of purchasing a bicycle and associated safety equipment
Season Ticket Loan An interest free loan for the purchase of an annual season ticket
Maternity Leave If an employee has 12 months continuous service at the 25th week of pregnancy, she will be entitled to: Weeks 1-8 - Full pay less any SMP or maternity allowance Weeks 9-22 - Half pay plus any SMP or maternity allowance (provided the total does not exceed full pay) Weeks 23-26 - SMP or maternity allowance Weeks 27-52 - No pay
Vaccinations Free or subsidised vaccinations are available from Occupational Health, including influenza
Notice Periods In line with Agenda for Change Protection Arrangements Should the employer require an employee to
move to a new post at a lower grade, then the employee’s pay will be protected
Sick Pay Staff with 4 months continuous service are entitled to 1 month at full pay and 2 months at half pay, increasing to a maximum for staff with more than 5 years continuous service of 6 months at Full Pay and 6 months at Half Pay
Mileage Allowance If an employee has cause to use their private motor vehicle for business purposes, they will be reimbursed at a rate in accordance with the employer’s guidelines
Telephone Expenses Where a job has been identified as requiring the use of a home telephone, the employer will reimburse the employee appropriately
Flexible Working Where an employee has already agreed flexible working, this is a contractual benefit
Long Service If an employee has 20 years service within the Trust then a (£400 + £20 for each additional year) gratuity will be paid by the Charitable Foundation upon retirement
Education Funding The employer will subsidise extra-curricular education and training if related to the employee’s work situation, i.e. a MSc in HRM
Uniforms The employer supplies and cleans uniforms for employees if the role is deemed appropriate
Long Service Awards Upon completion of 25 years service, an
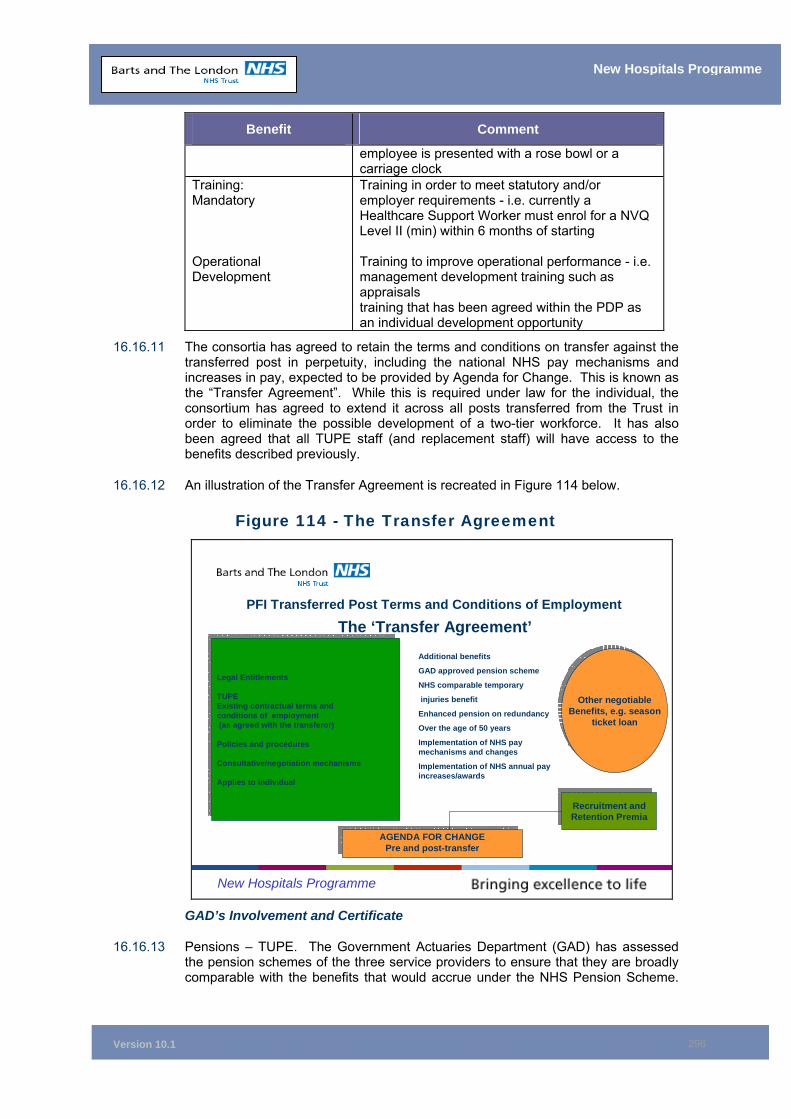
Version 10.1
296
New Hospitals Programme
Benefit Comment
employee is presented with a rose bowl or a carriage clock
Training: Mandatory Operational Development
Training in order to meet statutory and/or employer requirements - i.e. currently a Healthcare Support Worker must enrol for a NVQ Level II (min) within 6 months of starting Training to improve operational performance - i.e. management development training such as appraisals training that has been agreed within the PDP as an individual development opportunity
16.16.11 The consortia has agreed to retain the terms and conditions on transfer against the transferred post in perpetuity, including the national NHS pay mechanisms and increases in pay, expected to be provided by Agenda for Change. This is known as the “Transfer Agreement”. While this is required under law for the individual, the consortium has agreed to extend it across all posts transferred from the Trust in order to eliminate the possible development of a two-tier workforce. It has also been agreed that all TUPE staff (and replacement staff) will have access to the benefits described previously.
16.16.12 An illustration of the Transfer Agreement is recreated in Figure 114 below.
Figure 114 - The Transfer Agreement
New Hospitals Programme
PFI Transferred Post Terms and Conditions of Employment
The ‘Transfer Agreement’
Legal Entitlements
TUPEExisting contractual terms and conditions of employment(as agreed with the transferor)
Policies and procedures
Consultative/negotiation mechanisms
Applies to individual
Legal Entitlements
TUPEExisting contractual terms and conditions of employment(as agreed with the transferor)
Policies and procedures
Consultative/negotiation mechanisms
Applies to individual
AGENDA FOR CHANGEPre and post-transferAGENDA FOR CHANGE
Pre and post-transfer
Additional benefits
GAD approved pension scheme
NHS comparable temporary
injuries benefit
Enhanced pension on redundancy
Over the age of 50 years
Implementation of NHS pay mechanisms and changes
Implementation of NHS annual pay increases/awards
Other negotiableBenefits, e.g. season
ticket loan
Other negotiableBenefits, e.g. season
ticket loan
Recruitment andRetention Premia
Recruitment andRetention Premia
GAD’s Involvement and Certificate
16.16.13 Pensions – TUPE. The Government Actuaries Department (GAD) has assessed the pension schemes of the three service providers to ensure that they are broadly comparable with the benefits that would accrue under the NHS Pension Scheme.
Version 10.1
297
New Hospitals Programme
GAD has issued certificates providing confirmation to this effect for all three service providers’ schemes. The current certificates are attached at Appendix 16G.
16.16.14 All staff transferred under TUPE arrangements will be offered the opportunity to join the respective Government Actuaries Department (GAD) certified pension schemes of each of the service providers. This includes:
• All managerial and supervisory staff transferring in compliance with the definition agreed between the Trust and the consortia;
• Any operational staff who choose to TUPE transfer from ISS Mediclean or First Security to Mowlem Aqumen; and
• Any operational staff that chose to TUPE transfer in preference to RoE.
16.16.15 It has further been agreed with the consortium that all transferring NHS staff will be provided with a broadly comparable pension at any second or subsequent transfer, if the service provider changes for whatever reason (Clause 31.5 of the Project Agreement (Version dated 2 March 2005) refers).
16.16.16 Prior to the appointment of the preferred bidder and while there was still a competitive element to the bidding process, GAD dealt with negotiating and securing the bulk transfer terms for Trust staff who would be transferring their NHS Pensions to the relevant service provider as part of the TUPE transfer. Bulk transfer terms with the consortia were therefore agreed before appointment as preferred bidder.
Pensions Advice
16.16.17 The Trust, in conjunction with GAD and the trade unions, will provide access to independent, objective advice for all staff, whether transferring under TUPE or being seconded to the service provider under RoE. This ensures staff will be able to make informed decisions regarding the best pension’s option to take based on their personal circumstances.
Communication and Consultation
16.16.18 The internal communication strategy for the new hospitals programme encompasses all Trust staff and specifically those staff who will be affected by the transfer of services to the consortia.
16.16.19 Throughout the PFI process from the beginning through to financial close, open and regular communications with staff have been provided to ensure that staff members are fully informed and aware of progress. Communication has been by a variety of media, including:
• Periodic issue of a New Hospital Build news sheet;
• Redevelopment Link – A paper communication issued to all staff periodically;
• The Trust’s weekly Bulletin – an electronic news sheet detailing what is happening in the Trust;
• The Trust’s intranet site;
• Comprehensive Q&A briefings – targeted at key staff groups and including a specific set for Swanley laundry;
• Provision of “communication boxes” across the sites; and
• A series of open days for staff and stakeholders to view proposals at bidding stage and after the appointment of preferred bidder.
Version 10.1
298
New Hospitals Programme
16.16.20 In addition, the consortia has provided several exhibitions of the proposed development showing models of the new hospitals and providing other information such as ward layouts and copies of the planning applications. These exhibitions have been available to staff throughout the Trust. In addition, a static exhibition is planned as part of the construction phase, which will be open to patients, visitors, staff, and interested members of the public.
Communications with Staff Subject To Transfer
16.16.21 From the placing of the OJEC advertisement and throughout the bidding process, those staff subject to transfer have been kept informed of progress by personal invitation to staff meetings attended by the Chief Executive, Directors and senior members of the Facilities, HR and Project Team. Any issues raised at these meetings have been addressed through question and answer sheets, distributed to relevant staff and placed on the Trust’s intranet site.
16.16.22 During the bidding phase, the HR department made available an independent Staff Adviser, with experience in staff relations, to directly respond to an individual or departmental request (in confidence if necessary) for information on the project. The intention being to enable equity of access to information about the PFI, in particular for FM staff who would be subject to transfer and who were not members of a Trade Union. A special briefing was also prepared and sent to all applicants for FM jobs to appraise them of the developments and any potential impact on the role for which they might apply. This was updated at preferred bidder stage.
16.16.23 At preferred bidder, the service providers made a series of focused presentations to staff identified for transfer by staff group and method of planned transfer. Staff who attended and those who were unable or chose not to attend, have been provided with copies of the slides used and detailed question and answer sheets.
16.16.24 Other forms of communication include HR Clinics, regular discrete meetings/presentations to the FM senior managers, the publication of newsletters led by the consortia, and “communication” boxes located throughout the Trust, which have been made available for staff to raise issues of concern. Additional dedicated notice boards have also been provided.
16.16.25 Specific communication needs for the Swanley Laundry have been addressed by:
• A series of group meetings and question and answer sessions (followed up in writing) and supported by senior and line management; senior HR representatives and Staffside colleagues;
• One-to-ones with staff;
• Personal skills analysis; and
• Trust funding of development initiatives for displaced staff.
16.16.26 The overall consultation and communication strategy “time plan” also includes further group meetings with FM senior managers and staff; one-to-ones and small groups regarding transfer arrangements and group and individual pensions advice. The Trust is also developing an interactive web site to support the move to a formal partnership agreement and this will embrace the new hospitals programme.
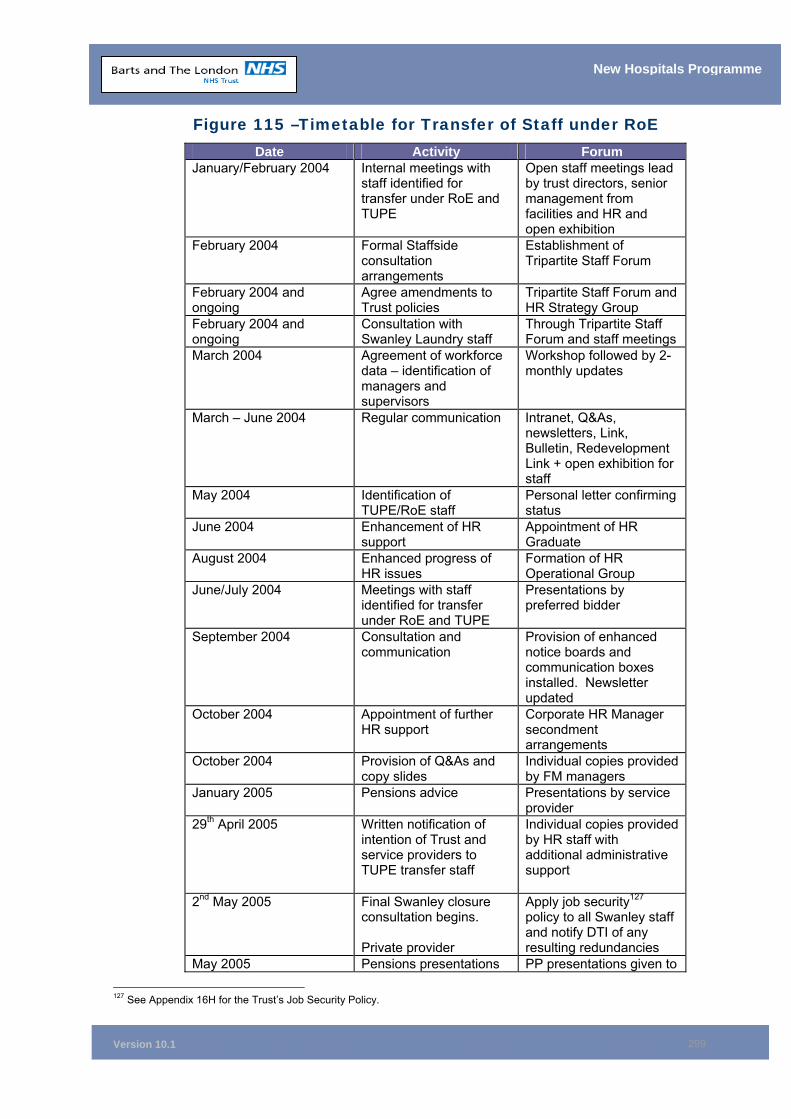
Version 10.1
299
New Hospitals Programme
Figure 115 –Timetable for Transfer of Staff under RoE Date Activity Forum
January/February 2004 Internal meetings with staff identified for transfer under RoE and TUPE
Open staff meetings lead by trust directors, senior management from facilities and HR and open exhibition
February 2004 Formal Staffside consultation arrangements
Establishment of Tripartite Staff Forum
February 2004 and ongoing
Agree amendments to Trust policies
Tripartite Staff Forum and HR Strategy Group
February 2004 and ongoing
Consultation with Swanley Laundry staff
Through Tripartite Staff Forum and staff meetings
March 2004 Agreement of workforce data – identification of managers and supervisors
Workshop followed by 2-monthly updates
March – June 2004 Regular communication Intranet, Q&As, newsletters, Link, Bulletin, Redevelopment Link + open exhibition for staff
May 2004 Identification of TUPE/RoE staff
Personal letter confirming status
June 2004 Enhancement of HR support
Appointment of HR Graduate
August 2004 Enhanced progress of HR issues
Formation of HR Operational Group
June/July 2004 Meetings with staff identified for transfer under RoE and TUPE
Presentations by preferred bidder
September 2004 Consultation and communication
Provision of enhanced notice boards and communication boxes installed. Newsletter updated
October 2004 Appointment of further HR support
Corporate HR Manager secondment arrangements
October 2004 Provision of Q&As and copy slides
Individual copies provided by FM managers
January 2005 Pensions advice Presentations by service provider
29th April 2005 Written notification of intention of Trust and service providers to TUPE transfer staff
Individual copies provided by HR staff with additional administrative support
2nd May 2005 Final Swanley closure consultation begins. Private provider
Apply job security127 policy to all Swanley staff and notify DTI of any resulting redundancies
May 2005 Pensions presentations PP presentations given to
127 See Appendix 16H for the Trust’s Job Security Policy.
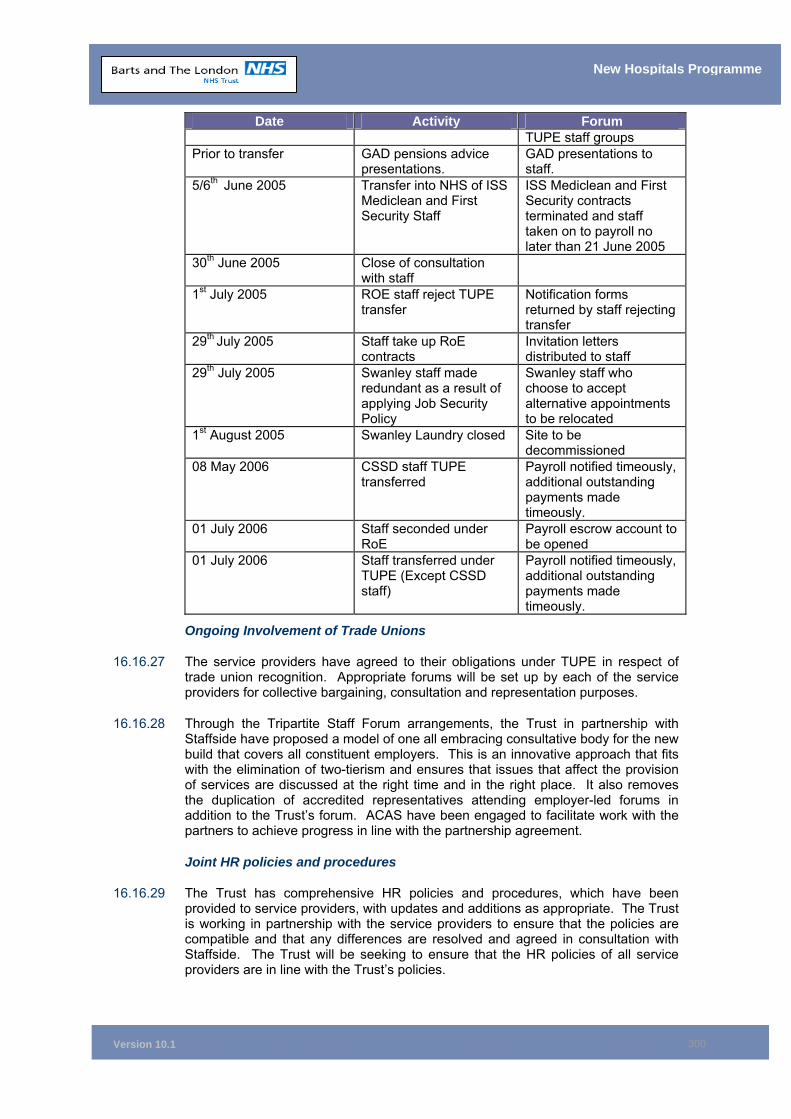
Version 10.1
300
New Hospitals Programme
Date Activity Forum TUPE staff groups
Prior to transfer GAD pensions advice presentations.
GAD presentations to staff.
5/6th June 2005 Transfer into NHS of ISS Mediclean and First Security Staff
ISS Mediclean and First Security contracts terminated and staff taken on to payroll no later than 21 June 2005
30th June 2005 Close of consultation with staff
1st July 2005 ROE staff reject TUPE transfer
Notification forms returned by staff rejecting transfer
29th July 2005 Staff take up RoE contracts
Invitation letters distributed to staff
29th July 2005 Swanley staff made redundant as a result of applying Job Security Policy
Swanley staff who choose to accept alternative appointments to be relocated
1st August 2005 Swanley Laundry closed Site to be decommissioned
08 May 2006 CSSD staff TUPE transferred
Payroll notified timeously, additional outstanding payments made timeously.
01 July 2006 Staff seconded under RoE
Payroll escrow account to be opened
01 July 2006 Staff transferred under TUPE (Except CSSD staff)
Payroll notified timeously, additional outstanding payments made timeously.
Ongoing Involvement of Trade Unions
16.16.27 The service providers have agreed to their obligations under TUPE in respect of trade union recognition. Appropriate forums will be set up by each of the service providers for collective bargaining, consultation and representation purposes.
16.16.28 Through the Tripartite Staff Forum arrangements, the Trust in partnership with Staffside have proposed a model of one all embracing consultative body for the new build that covers all constituent employers. This is an innovative approach that fits with the elimination of two-tierism and ensures that issues that affect the provision of services are discussed at the right time and in the right place. It also removes the duplication of accredited representatives attending employer-led forums in addition to the Trust’s forum. ACAS have been engaged to facilitate work with the partners to achieve progress in line with the partnership agreement.
Joint HR policies and procedures
16.16.29 The Trust has comprehensive HR policies and procedures, which have been provided to service providers, with updates and additions as appropriate. The Trust is working in partnership with the service providers to ensure that the policies are compatible and that any differences are resolved and agreed in consultation with Staffside. The Trust will be seeking to ensure that the HR policies of all service providers are in line with the Trust’s policies.
Version 10.1
301
New Hospitals Programme
16.16.30 Some of the Trust’s HR policies have been reviewed to reflect the status of the staff covered under RoE, and the fact that staff not employed by the Trust will manage them. Key areas to address included:
• The application of recruitment processes;
• Appraisal and performance management;
• Disciplinary and grievance procedures;
• Claims of bullying and harassment;
• Termination provisions in situations such as disciplinary issues, fixed term contracts and redundancy;
• Security of employment;
• The management of sickness absence; and
• Capability.
16.16.31 The Trust has worked with the preferred bidder to establish appropriate policy and procedure amendments to deal with issues in full consultation with Staffside representatives.
16.16.32 It is also of the utmost importance to consider the impact of developing employment law, e.g. the new Statutory Disciplinary and Grievance Procedures and the ACAS Code of Practice effective from 1st October 2004. Such developments are progressed initially through the Tripartite Staff Forum.
16.16.33 The Trust has strict procedures in place in relation to the application and approval of policies. All the Trust’s policies are subject to a 3-year review programme and all new and revised/amended policies are subject to consultation and approval through the Trust’s Policies and Procedures Working Group, which has representation from both management and Staffside.
Equality and Diversity
16.16.34 The preferred bidder has committed to adopting the Trust’s Race Equality Scheme, Equal Opportunities Policy and Equality and Diversity Strategy and is working in partnership with the HR Department, the Head of Recruitment Services, the Head of Work/Life Balance and the Trust’s Regeneration Manager to ensure the Trust’s Equality and Diversity Strategy is developed to its full potential. This is of course in conjunction with Staffside colleagues and representatives from the community and community organisations.
Agenda for Change
16.16.35 The preferred bidder has committed to adopting the new national NHS pay and job evaluation mechanism for all TUPE transferred staff and replacement/new staff employed to deliver FM services in the Trust’s new hospitals. To ensure a smooth transition, the Trust is working in partnership with service providers to ensure common understanding of the new system the appropriate and timely training of staff in job evaluation and matching, and training of line managers in the Knowledge and Skills Framework and appraisal.
16.16.36 Part of the rationale of retaining the RoE payroll services in house is to ensure a smooth transition to Agenda for Change and minimum disruption to staff pay arrangements. Working in partnership also enables timely and effective management of appeals against grading. Full adoption of Agenda for Change, and any subsequent developments, ensures the elimination of “two-tierism”.
Version 10.1
302
New Hospitals Programme
16.17 Chapter Conclusions 16.17.1 The manpower planning for providing clinical and support staffing for the new
hospitals is robust.
16.17.2 The best interests of staff affected by PFI arrangements have been secured by the Trust. The transfer of staff is in accordance with Government policy. No staff working in clinical services will transfer and the Trust has secured:
• A comprehensive transfer agreement that protects the posts covered by TUPE;
• The application of the RoE agreement;
• The reintegration of third party contractor staff to the NHS;
• The adoption of Agenda for Change in full;
• The raising of the minimum wage to NHS standards; and
• Uninterrupted and continuing formal trade union engagement.
16.18 Chapter Appendices 16A Nursing Structure 16B Common Interest Groups’ Benefits Realisation Work 16C Detail Elements of the HR Strategy 16D Example of the Support Provided to Swanley Staff 16E Staffside Recognition Arrangements 16F Specific Issues for Trust Staff and Third Party Contractors 16G GAD Certificates 16H Trust’s Job Security Policy
Version 10.1
303
New Hospitals Programme
17 INFORMATION COMMUNICATION & TECHNOLOGY Synopsis – Information Communication and Technology
This chapter:
• Explains the relationship between the Trust’s ICT strategy and the National Programme for Information Technology “Connecting for Health”
• Describes the national and local context for ICT
• Gives a high-level overview of the ICT strategy, what it contains and how it contributes to the New Hospital Project objectives
• Discusses some risks at a strategic level
• Describes the ICT cabling infrastructure that Skanska Innisfree is expected to deliver as part of the PFI scheme
• Provides assurance that robust systems and processes are in place for managing the implementation of ICT
17.1 The Trust’s Information Communication and Technology Strategy
17.1.1 The Trust’s Information Communication and Technology (ICT) strategy (Appendix 17A) will contribute to the successful implementation and operation of the new hospital development. It is based on participation in the National Programme Connecting for Health, with the majority of systems being selected and procured centrally for the whole of London. The strategy, approved by the Trust Board 07 December 2005 was a five year strategy, which is now being updated to reflect changes in the Connecting for Health Programme.
17.1.2 The investment in new ICT systems does not form part of this FBC. Current Department of Health (DH) guidance is that ICT should be excluded from PFI build projects, except for the cabling infrastructure. The ICT procurement is therefore the subject of a separate business case, being developed by the Trust in parallel with the main hospital PFI.
17.1.3 Trust IT strategy demands that all ICT systems have fallback and contingency built into their design. The network infrastructure will provide alternative routes in the case of primary route failure with no single point of failure on the core network infrastructure. The fallback and assurance arrangements for the systems that are to host the CRS application are as set out in the National Program for IT LSP contract which, in London's case, mean Cerner Millennium systems which are designed to run 24 hours a day, 365 days a year without disruption. There are two data centres where the Cerner Millennium systems are located with one centre acting as a fallback for the other. All local trust systems are reviewed in terms of risk and impact of loss and appropriate resilience is built into their configuration. The ICT department is fully ISO 27001, Part 2 certified and this standard requires that we have a business continuity plan and a full disaster recovery plan for critical systems.
17.1.4 The design of the Trust network is such that the “core” network has redundancy routes in place which allow for alternate routing should a primary route become
Version 10.1
304
New Hospitals Programme
compromised. The inter-site routes currently are triangulated, providing alternative routes in the case of failure of a primary route. Moving to a two-site operation, it is intended to have two inter-site links which will take different routes and will provide redundancy for each other in case of failure.
17.1.5 The external link to national CRS services is connected via N3 which has two separate connections - one active and one passive. This configuration is currently enhanced with the introduction of a third connection thereby supporting triangulation. This facilitates increased resilience ensuring Trust systems are essentially always connected. The N3 infrastructure is fully fault-tolerant and has service level performance targets in terms of availability set by CFH.
17.1.6 Trust strategy accepts that ICT systems are critical to the smooth operation of clinical services; there is therefore a close interface between the delivery of both schemes. The Trust’s strategic approach to ICT is outlined below. This section describes:
the national and local context for ICT; how the ICT strategy contributes to the objectives of the PFI scheme; and the link with the building PFI.
17.2 Strategic context for ICT 17.2.1 At the time the Outline Business Case (OBC) was developed and written for the
Care Record System (CRS), the Trust was working to the agenda set out in Information for Health (1998), the NHS National Information Strategy.
17.2.2 In November 2002, the Trust revised its ICT strategy on the basis of procuring rather than building its own modern integrated hospital information system. In preparation for this, the Trust made the decision to cease investment in its ageing Patient Administration System (PAS)/Hospital Information System Services (HISS) and under-powered departmental systems, and focused resources on implementing a programme of improvement to the ICT technical infrastructure.
17.2.3 The Trust’s revised ICT strategy was shared with local partner organisations and the Strategic Health Authority (SHA) via the Local Implementation Strategy (LIS) Boards. The strategy was supported by all partners. Currently the ICT strategy is being updated; when completed this too will be shared with all organisations in the health community.
17.3 National Context 17.3.1 Delivering the NHS Plan (April 2002) developed the vision which had been set out
in The NHS Plan (July 2001). This described a service designed around meeting the needs of patients. Patients were to be offered choices of where and when they receive treatment, and clinical management systems would need to be developed to support that vision. Such choices were to include the opportunity and ability to book diagnostic and consultation appointments electronically while visiting GP surgeries. Modern ICT systems would also be needed to support the frontline delivery of care and treatment.
17.3.2 Delivering 21st Century IT Support for the NHS (July 2002) outlined the National IT approach to enable the NHS to meet the requirements outlined above. The principles of “Information for Health” remained, but this was to be supported by a national programme of information and IT priorities (the National Implementation Programme (NIP)) which became a reality in the NHS in April 2003.
Version 10.1
305
New Hospitals Programme
17.3.3 NIP set out a shift to a national approach to IT standards and provision and the programme provides for:
• National direction and leadership;
• Procurement of standardised IT systems;
• Private sector delivery through Local Service Providers (LSPs); and
• Local co-ordination through regional “clusters” of SHAs.
17.3.4 Central control will also extend to resource management, performance management and implementation.
17.3.5 A fundamental element of the NHS programme is a move towards a Care Records System (CRS). For health records, this means a national approach to procurement and implementation, conforming to national standards and interoperability with emerging national infrastructures such as the Electronic Staff Record and a formal registration authority to manage clinical access to patient information.
17.3.6 The Trust’s ICT strategy is entirely consistent with the National Implementation Programme.
17.4 London Context 17.4.1 As part of the National Implementation Programme, it was agreed that the five
SHAs in the pan London programme would be one of the two first wave clusters to select a Local Service Provider (LSP) and then implement the NHS CRS. Development of the strategy to achieve this was completed in May 2003, in parallel with this business case development. The LSP for London was selected in December 2003.
17.4.2 The selected LSP for London is British Telecom (BT). A copy of the letter from NPfIT confirming that the Trust should proceed to deployment is attached at Appendix 17B.
17.4.3 Within the NHS London Programme for IT (LPfIT) and BT, there is commitment and support for the Trust to progress rapidly to implementation of systems to replace the existing PAS/HISS.
17.5 The Trust’s ICT Culture 17.5.1 The Trust has undertaken considerable work on improving hospital-wide networks,
including its Intranet and desktop access, meeting all national targets on time. This strategy has provided the tools and created the environment for clinicians to use new technology, while laying the foundation for CRS, information sharing and patient access.
17.5.2 In common with comparable organisations, the Trust has developed an extensive and diverse portfolio of information systems over the past few years. Many of these have provided considerable benefits, not least in developing the awareness of staff of the opportunities and potential benefits from the use of ICT in healthcare, and the ambition to exploit ICT to improve the effectiveness and efficiency of the organisation.

Version 10.1
306
New Hospitals Programme
17.6 Scope and Timing of the CRS Implementation 17.6.1 The Trust Executive agreed for the Trust to be one of the deployment sites for the
BT Acute Care Solution in 2006/07 subject to the following four constraints:
Functionality – all outstanding matters are resolved satisfactorily; That the various deployment plans are merged into a single plan (i.e.
conformation of a robust project plan to deliver within the timescales); That the deployment is demonstrated as affordable within the resources
available to the Trust (hence no adverse impact over efficiency savings plans for CRS; and
LPfIT will pursue BT for compensation for any contractual slippage under the terms of the National LSP contract.
17.6.2 As required by the Trust Board and LPfIT, a revised CRS business case was prepared and this was approved by the SHA 24th January 2006 (see Appendix 17E). A further revision of the Business Case was presented and approved by the Trust board on 27th June 2007. The acute solution will replace the existing PAS functionality and associated services (e.g. theatre and maternity scheduling and orders) with a fully integrated patient record in the winter of 2007. Interfaces with existing systems will be reduced to a minimum but will include key clinical systems supporting services not provided for in the CRS portfolio.
17.6.3 SHA approval for the Trust Picture Archiving and Communication System (PACS) project was granted on 8th November 2005 and the project was successfully concluded in November 2006.
17.6.4 Transfer of PACS equipment will be timetabled to co-ordinate with the move into the new hospitals when they are ready.
17.6.5 The PACS business case generates a potential adverse net cash impact as the savings to be generated in directorates are unlikely to deliver their full year benefit until 2008/9. This is likely to impact on all Trusts implementing PACS and BLTs preferred solution is for CFH to recognise this and amend the LSP service charge timings to reduce net cash outflow in 2007/8 with it being recovered later in the programme.
17.6.6 Other CRS components, such as Advanced Maternity, Advanced Clinicals and Prevention, Screening and Surveillance will be deployed in the following years as they become available. Advanced clinicals are multi-disciplinary assessments, decision support and integrated care pathway systems or access as set out in the NHS CRS Functionality specifications produced by Connecting for Health (CFH).
17.6.7 The CRS Programme is on schedule to deliver the foundation release in December 2007, with the first upgrade being applied in April 2008. The CRS implementation timetable is aligned with the New Hospitals build programme in as much as there is a requirement for CRS to be installed before the Trust moves into the new accommodation. Procurement and Installation of IT equipment will be managed in-house and the New hospitals ICT Infrastructure sub group and will report to the main New Hospitals Programme board to ensure integration and the best programme fit is achieved.
17.6.8 The main risk to the Trust in connection with the build programme is one of organisational capacity, where plans are required for staff training, changes in working practices, undertaking the move to the new premises and maintaining patient care. Enabling work is underway with BT to mitigate these risks by front-loading the CFH impact analysis and organisational change.
Version 10.1
307
New Hospitals Programme
17.6.9 By taking ICT provision out of the PFI scheme in accordance with NHS guidance, the Trust recognises it has taken on the associated responsibility for delivery. By engaging fully with CFH, the Trust is able to benefit from its support and commitment to deliver the systems it needs.
17.6.10 The Trust also acknowledges that it needs to manage any future affordability issues in relation to implementing its strategy. Such issues would be assessed in light of the Wanless report, which suggests the NHS requires an increase from 2% to 4% of revenue to support ICT expenditure. CFH will supply, as a free gift to the Trust, services which the Trust currently funds, such as PAS. Full functionality is being provided for the PACS solution by CFH. It is intended that funds released through the provision of CFH services, be utilised to provide ICT service expansion and accommodate any revenue consequences of maintaining the CFH provided CRS solution within the Trust.
17.7 ICT’s Contribution to the Objectives of the PFI Scheme
17.7.1 Implementation of the ICT strategy will bring many benefits to the Trust, independent of the New Hospitals Project. Some of these benefits will be realised before the new hospitals become available. However, maximum exploitation of CRS will be achieved through the organisational changes envisaged as part of the New Hospitals Project. The Trust has been careful to separate out the benefits and ensure that there is no double counting. All benefits attributed to the implementation of CRS have not been included in this scheme.
17.7.2 Specific high level considerations are as follows:
• The Trust will remain on split sites, therefore the cross-site availability of electronic patient records, electronic scheduling of appointments and diagnostic tests will be important;
• The design concept reflects the inter-relationships and complex co-locations of the sites. The importance of ICT to support virtual co-locations is paramount;
• The Ambulatory Care and Diagnostic Centre and the Imaging and Interventional block, will exploit the provision of advanced Information Technology systems for appointment and theatre scheduling, request and real-time scheduling of diagnostic tests and instant communication of results;
• The level of outpatient activity at The Royal London already makes it one of the busiest departments in the UK. The ICT systems will allow efficient management of this intensely busy service; and
• The chronic shortage of trained staff is already impacting upon the ability of the Trust to meet performance targets, and this situation is not anticipated to improve in the future. Efficiency gains offered by the innovative application of ICT will maximise the utilisation of trained staff.
17.8 ICT Training 17.8.1 The full ICT programme, including all the advanced components, is phased to be
rolled-out over a 5 year period from 2006 to 20010 inclusive. As modules are implemented, the Trust will run a series of training programmes for staff (clinical and administrative) that will use the new systems. The Trust has already completed a Strategic Needs Analysis with the help of the Local Service Provider. This analysis has provided pointers to success criteria for the training plan when it is developed.
Version 10.1
308
New Hospitals Programme
A training project has been established to take forward the next stage, which includes a detailed training needs analysis.
17.8.2 An important feature of the training programme will be the inclusion of Best Practice as defined by the user groups and incorporated into the systems by the Local Service Provider. This is one way in which the benefits of the new systems will be realised in daily clinical practice.
17.9 Management of Risks 17.9.1 CRS Project risks have been identified and recorded in line with PRINCE 2
methodology. The risks are assessed by the CRS programme team and a management action identified. Current, forthcoming and potential risks will be reviewed by this team throughout the period of the project.
17.9.2 One of the main risks identified to the New Hospitals Programme was delay in implementation of the CRS Programme. However, the Trust is in the fortunate position of having a broad range of existing systems in place which adequately support service delivery. Maintaining these existing systems are the Trust’s fall-back position should there be any delay in implementation of the CRS programme.
17.9.3 The existing extensive Patient Administration and Clinical Systems which currently support the Trust will continue to be used until replaced by CRS. No additional work is required for these systems to function should they still be in use when the new hospital is occupied, as the cabling infrastructure being provided by the Consortium will enable the functionality of existing systems. This fall-back position allows the new hospital to be fully functional but would delay achievement of the new hospitals vision. Delay in the deployment of the CRS system will delay the benefits realisation. Many of the claimed benefits will be gained through estate enabled changes to clinical processes and procedures but until the full functions of the CRS system are being used in tandem with the clinical changes complete benefit realisation will not be seen.
17.9.4 Any new system will be hosted in the main ICT building and not the new build. End user devices will be procured and installed in accordance with the overall build commission and release programme (see Appendix 17D for implementation programme).
17.9.5 As detailed in Paragraphs 17.6 – 17.8 above, there is a sufficient time buffer between replacement of the current, enterprise-wide systems and occupation of the new hospital. The major CRS components are planned for deployment during 2006 through to 2010. These include PAS, Maternity, Theatres, Test Requesting, Results Reporting, Pharmacy Stock Control, Radiology and PACS (Imaging). These deployments have been confirmed by LPfIT.
17.9.6 A further risk identified was in relation to the decanting programme and the availability of resources within the Trust’s ICT Department to ensure that ICT systems can be installed within the constraints set by Skanska Innisfree’s phased construction programme. However, this is not considered to be an issue (see section on decanting below).
17.10 Approach to ICT in the PFI Scheme 17.10.1 As the provision of new systems is to be through participation in the national
strategy, only the local hardware and network infrastructure remain to be procured. For the PFI scheme, this means that only the cabling infrastructure, up to the wall outlets, is to be included.
Version 10.1
309
New Hospitals Programme
17.10.2 Fallback and contingency has been built into the design of the network infrastructure to provide alternative routes in the case of primary route failure. The intention is to have no single points of failure on the core network infrastructure. The systems that are to host the CRS application are Cerner Millennium systems which are designed to run 24 hours a day, 365 days a year without disruption. There are two data centres where the Cerner Millennium systems are located with one centre acting as a fallback for the other. Other systems are reviewed in terms of risk and impact of loss and appropriate resilience is built into the configuration. A business continuity plan is created and a full disaster recovery plan is designed for critical systems. A solution is implemented based on a risk analysis and affordability.
17.10.3 There are two elements to the issue of network redundancy. Firstly, the design of the Trust network is such that the “core” network has redundancy routes in place which allows for alternate routing should a primary route be affected. The inter-site routes currently are triangulated, providing alternative routes in the case of failure of a primary route. Moving to a two-site operation, it is intended to have two inter-site links which will take different routes and will provide redundancy for each other in case of failure.
17.10.4 Secondly, the external link to national services is connected via N3 which has two separate connections - one active and one passive. This configuration is currently being enhanced with the introduction of a third connection, thereby supporting triangulation. This facilitates increased resilience ensuring Trust systems are essentially always connected. The N3 infrastructure is fully fault-tolerant and has service level performance targets in terms of availability set by CFH.
17.10.5 The PFI ITN specified:
• The minimum requirements for terminal access points, plus a stated spare capacity;
• The design and topology constraints for hub rooms and communications rooms;
• Fall-back and redundancy requirements;
• Technical specifications for compatibility with the Trust’s active equipment;
• Environmental requirements; and
• Documentation, change control and monitoring approach.
17.10.6 The PFI partner is responsible for the installation of passive Cat6 UTP copper and fibre optic cabling terminating at designated wiring closets / communications rooms to passive patch panels. The Trust is responsible for the installation of the active data communications equipment (hubs/routers, etc.). No software or applications are involved in the cabling infrastructure element.
17.10.7 The Trust will migrate systems into the new build where the system is in operation and is managed locally by the department. However, the number of instances of this is rare, as most “systems” are hosted centrally in the main ICT building which is not affected by the build. A new communications area has been identified which will form part of the Trust’s business continuity and disaster recovery arrangements.
17.10.8 The Public Sector Comparator (PSC) was based on an independently costed assessment of the ICT specification. Skanska Innisfree was able to propose a solution which met the technical specification within the scope of the PSC. The proposal also allows for more than the minimum cabled outlets plus a greater use of wireless technology.
Version 10.1
310
New Hospitals Programme
17.11 Future Expansion and Technologies 17.11.1 The infrastructure specification within the PFI project relates specifically to the
provision of saturation coverage of wireless transceiver points throughout the estate, horizontal cat6 copper cabling (industry standard cable specification) and fibre optic cabling connecting buildings and on floors in the new build. Patch panels, patch leads and Cabinets are included in the scope of work. This allows scope for the final ICT standards to reflect the “state of the art”, while being an integral part of the hospital building. The Trust can take advantage of the national strategy as it develops over the coming years. The PFI thereby aims to provide an ICT infrastructure which will ensure that as yet unforeseen technological developments can be introduced.
17.12 Managing the IT Infrastructure 17.12.1 Skanska Innisfree will:
• Provide the infrastructure cabling (wallports, local cabling between wallports and hub room, patch blocks, main data and voice cables, etc.) as well as tray-work and containment (sign off and inspection checkpoints are built in with final certification of all data points);
• Provide equipment cabinets and patch leads, all active components of the voice (but not data) network including hardware and software, and the PABX (Private Automatic Branch Exchange Telephone System);
• Install and maintain electrical cables, sockets and connections and provide the supply of electrical power, including back-up generators and the Uninterrupted Power Supply (UPS). Local UPS units will be provided and maintained by the Trust or its IT services supplier; and
• Provide and operate equipment and services as follows:
Monitoring and control of temperature and humidity, detection of water, smoke or fire in hub rooms, main hub rooms, and the computer suite;
Provide and maintain an automatic fire smothering gas installation(s) in the computer suite and main hub rooms; and
Provide and maintain a system of intruder detection in all IT spaces.
17.12.2 Once operational, Skanska Innisfree and the Trust will hold frequent and regular service management meetings to review performance, service levels and requirements concerning all the services provided by Skanska Innisfree. ICT will be included in that process, so that all issues in relation to the infrastructure will be addressed in a formal way. Details of the interface and working arrangements are set out in Chapter 14.
17.12.3 Skanska Innisfree has agreed to comply with the Trust’s accreditation process for attachment of systems and devices to the network. This process is performed by the Trust’s ICT staff.
17.12.4 The process of oversight of implementation of ICT in the new hospitals will be managed by the ISG/CRS Project Board, which reports in relation to ICT in the new hospitals to the New Hospitals Programme Board. Chapter 14 provides a summary of the Terms of Reference and further detail.
17.12.5 The chair of this Project Board (the Trust’s Director of ICT), who is also the Programme Director for the CRS project, is a member of the New Hospitals
Version 10.1
311
New Hospitals Programme
Programme Board. A copy of the job description for the CRS Programme Director is attached at Appendix 17C.
17.13 Decanting Programme 17.13.1 The Trust’s technical team has been working with Skanska Innisfree to develop a
decanting programme which aims to safeguard existing services, while implementing the new networks. The Trust’s technical team is therefore conversant with the detailed plans for the network during the decanting period, as well as with the scheduling. Full details of the ICT Commissioning Programme can be found at Appendix 17D.
17.13.2 The decanting programme includes the identification and sourcing of any additional or temporary equipment to allow the new network to be tested and made available without degrading existing services.
17.13.3 The Trust is currently planning to strengthen its network staff to increase support to the PFI project and ensure the ICT resource is in place to support the decanting programme. There will be named staff allocated to the project that will be responsible for the coordination, liaison and implementation of the ICT components. This work will be monitored by the CRS/ISG Project Board.
17.14 Chapter Conclusion 17.14.1 The Trust has adopted the NPfIT programme and is an early implementer. The
interface required between ICT and the construction and commissioning of the new hospitals has been carefully considered, appropriate systems and processes for managing the interface have been established and plans made for making the necessary resources for commissioning hardware available.
17.14.2 The Trust has identified a robust fallback position which will ensure that the new hospitals can be commissioned and be operational should the NPfIT programme not be delivered to time.
17.15 Chapter Appendices 17A ICT Strategy 17B Letter of Authorisation from NPfIT to Proceed to Deployment 17C Job Description for the Trust’s CRS Programme Director 17D ICT Commissioning Programme 17E SHA Approval of CRS Business Case
Version 10.1
312
New Hospitals Programme
18 BENEFITS REALISATION Synopsis – Benefits Realisation This chapter sets out: • Comprehensive details of the high level benefits to be realised through
implementation of the project - both cash releasing and non-cash releasing;
• An analysis of the financial and non-financial benefits to be realised;
• The Benefits Realisation Plan and how assessment of delivery of the high level benefits will be achieved; and
• The ongoing programme of work to identify those detailed benefits that underpin the high level benefits and the development of an action plan for delivery.
18.1 Introduction 18.1.1 This chapter details the high level benefits to be realised through completing the
project and the Trust’s approach to benefits management. Many of the benefits have been outlined in the preceding chapters but they are brought together here for completeness.
18.1.2 This Chapter includes:
• The project’s investment objectives;
• The benefits detailed in the outline business case and how they have changed/been enhanced;
• The benefits to be realised and how they flow from the project objectives;
• Financial benefits;
• Non-financial benefits;
• The Trust’s approach to benefits management:
Benefits identification
Benefits management
Benefits realisation planning
Benefits realisation
Benefits reviews; and
• The reference points against which the Trust Board will evaluate outcomes.
18.2 The Overall Investment Objectives 18.2.1 The agreed objective for the project is to provide services in accordance with the
recommendations of the London Review, including:
O1 To provide 21st century healthcare in an environment which staff, patients and our local communities can be proud;
O2 To have facilities for patients and staff that truly reflect the Trust’s long tradition of clinical excellence;
Version 10.1
313
New Hospitals Programme
O3 To replace many of the existing buildings with a coherent structure, purpose built to support the delivery of 21st century clinical care, while sympathetic to historical buildings;
O4 To reduce the backlog of today’s ageing building stock and introduce output-based standards that will ensure a “nearly new” quality for at least 30 years;
O5 To design and provide buildings that will be able to respond flexibly to the Trust’s evolving clinical strategy and advances in modern healthcare provision;
O6 To ensure that services and activities performed by the Trust will continue during construction, 24 hours a day, 365 days a year, safely and with the minimum of disruption and inconvenience;
O7 To ensure that the scheme can support the delivery of the Pathfinder clinical strategy for services, with particular emphasis on clinical excellence, patient experience, and service efficiency;
O8 To ensure that the scheme takes into account the impact of key national NHS policies and initiatives, such as Patient Choice, Payment by Results, Agenda for Change and the Consultant Contract, as well as local developments such as the Thames Gateway expansion, the GLA’s population forecasts and ensuring these dovetail with the Strategic Health Authority's assumptions by working closely with Tower Hamlets PCT and other partner organisations;
O9 To protect the terms and conditions of staff being seconded or transferred to the private sector partner under the terms of TUPE (Transfer of Undertakings Protection of Employment) and RoE (Retention of Employment) legislation; and
O10 To put patients at the heart of the new hospitals and transform the hospital experience for millions of patients from London and beyond.
18.2.2 Achieving these objectives will result in the following benefits to patients and staff of the Trust:
• Better access to services;
• Improved clinical quality of hospital services;
• Improved environmental quality within which to provide hospital services;
• Service improvements and new models of care;
• Improved strategic fit of services with other health bodies in acute and primary care settings;
• Ability to meet national, regional and local policy imperatives;
• Improved recruitment and retention and training and development of staff; and
• Achievement of efficiency savings.
18.2.3 Appendix 18A sets out the benefits to be achieved against the desired objectives from which they flow.
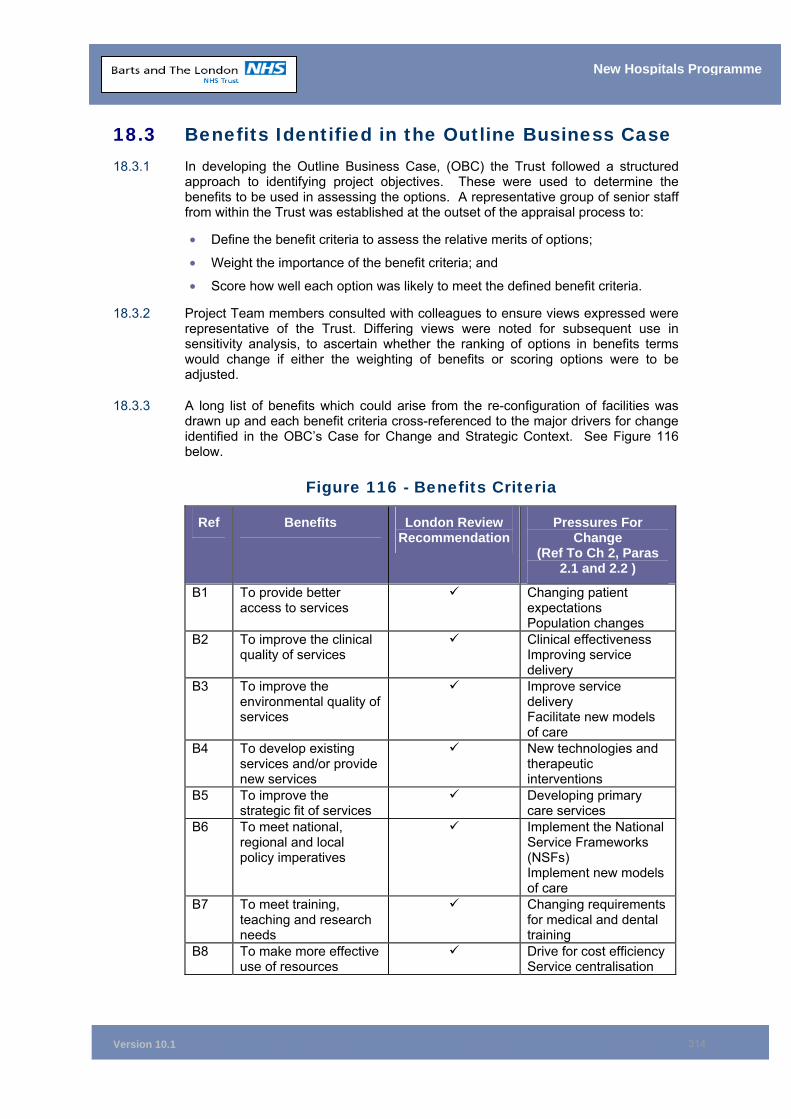
Version 10.1
314
New Hospitals Programme
18.3 Benefits Identified in the Outline Business Case 18.3.1 In developing the Outline Business Case, (OBC) the Trust followed a structured
approach to identifying project objectives. These were used to determine the benefits to be used in assessing the options. A representative group of senior staff from within the Trust was established at the outset of the appraisal process to:
• Define the benefit criteria to assess the relative merits of options;
• Weight the importance of the benefit criteria; and
• Score how well each option was likely to meet the defined benefit criteria.
18.3.2 Project Team members consulted with colleagues to ensure views expressed were representative of the Trust. Differing views were noted for subsequent use in sensitivity analysis, to ascertain whether the ranking of options in benefits terms would change if either the weighting of benefits or scoring options were to be adjusted.
18.3.3 A long list of benefits which could arise from the re-configuration of facilities was drawn up and each benefit criteria cross-referenced to the major drivers for change identified in the OBC’s Case for Change and Strategic Context. See Figure 116 below.
Figure 116 - Benefits Criteria
Ref Benefits London Review Recommendation
Pressures For Change
(Ref To Ch 2, Paras 2.1 and 2.2 )
B1 To provide better access to services
Changing patient expectations Population changes
B2 To improve the clinical quality of services
Clinical effectiveness Improving service delivery
B3 To improve the environmental quality of services
Improve service delivery Facilitate new models of care
B4 To develop existing services and/or provide new services
New technologies and therapeutic interventions
B5 To improve the strategic fit of services
Developing primary care services
B6 To meet national, regional and local policy imperatives
Implement the National Service Frameworks (NSFs) Implement new models of care
B7 To meet training, teaching and research needs
Changing requirements for medical and dental training
B8 To make more effective use of resources
Drive for cost efficiency Service centralisation
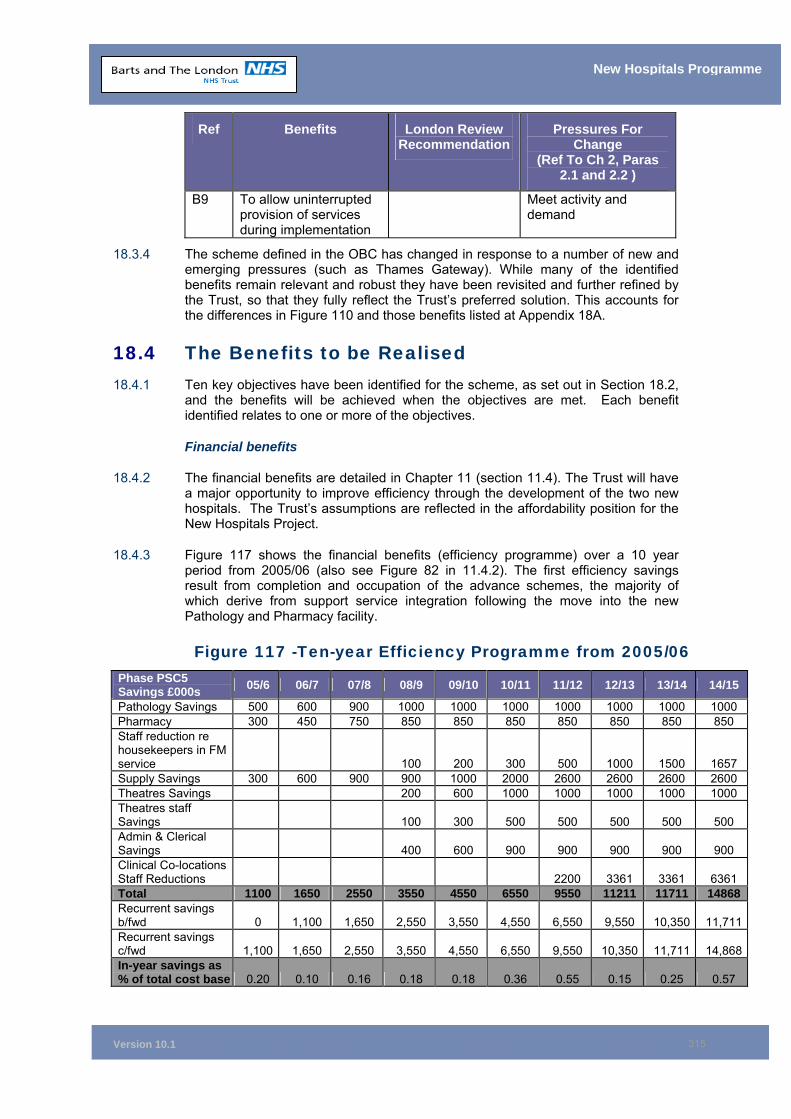
Version 10.1
315
New Hospitals Programme
Ref Benefits London Review Recommendation
Pressures For Change
(Ref To Ch 2, Paras 2.1 and 2.2 )
B9 To allow uninterrupted provision of services during implementation
Meet activity and demand
18.3.4 The scheme defined in the OBC has changed in response to a number of new and emerging pressures (such as Thames Gateway). While many of the identified benefits remain relevant and robust they have been revisited and further refined by the Trust, so that they fully reflect the Trust’s preferred solution. This accounts for the differences in Figure 110 and those benefits listed at Appendix 18A.
18.4 The Benefits to be Realised 18.4.1 Ten key objectives have been identified for the scheme, as set out in Section 18.2,
and the benefits will be achieved when the objectives are met. Each benefit identified relates to one or more of the objectives.
Financial benefits
18.4.2 The financial benefits are detailed in Chapter 11 (section 11.4). The Trust will have a major opportunity to improve efficiency through the development of the two new hospitals. The Trust’s assumptions are reflected in the affordability position for the New Hospitals Project.
18.4.3 Figure 117 shows the financial benefits (efficiency programme) over a 10 year period from 2005/06 (also see Figure 82 in 11.4.2). The first efficiency savings result from completion and occupation of the advance schemes, the majority of which derive from support service integration following the move into the new Pathology and Pharmacy facility.
Figure 117 -Ten-year Efficiency Programme from 2005/06 Phase PSC5 Savings £000s 05/6 06/7 07/8 08/9 09/10 10/11 11/12 12/13 13/14 14/15
Pathology Savings 500 600 900 1000 1000 1000 1000 1000 1000 1000 Pharmacy 300 450 750 850 850 850 850 850 850 850 Staff reduction re housekeepers in FM service 100 200 300 500 1000 1500 1657 Supply Savings 300 600 900 900 1000 2000 2600 2600 2600 2600 Theatres Savings 200 600 1000 1000 1000 1000 1000 Theatres staff Savings 100 300 500 500 500 500 500 Admin & Clerical Savings 400 600 900 900 900 900 900 Clinical Co-locations Staff Reductions 2200 3361 3361 6361 Total 1100 1650 2550 3550 4550 6550 9550 11211 11711 14868Recurrent savings b/fwd 0 1,100 1,650 2,550 3,550 4,550 6,550 9,550 10,350 11,711Recurrent savings c/fwd 1,100 1,650 2,550 3,550 4,550 6,550 9,550 10,350 11,711 14,868In-year savings as % of total cost base 0.20 0.10 0.16 0.18 0.18 0.36 0.55 0.15 0.25 0.57
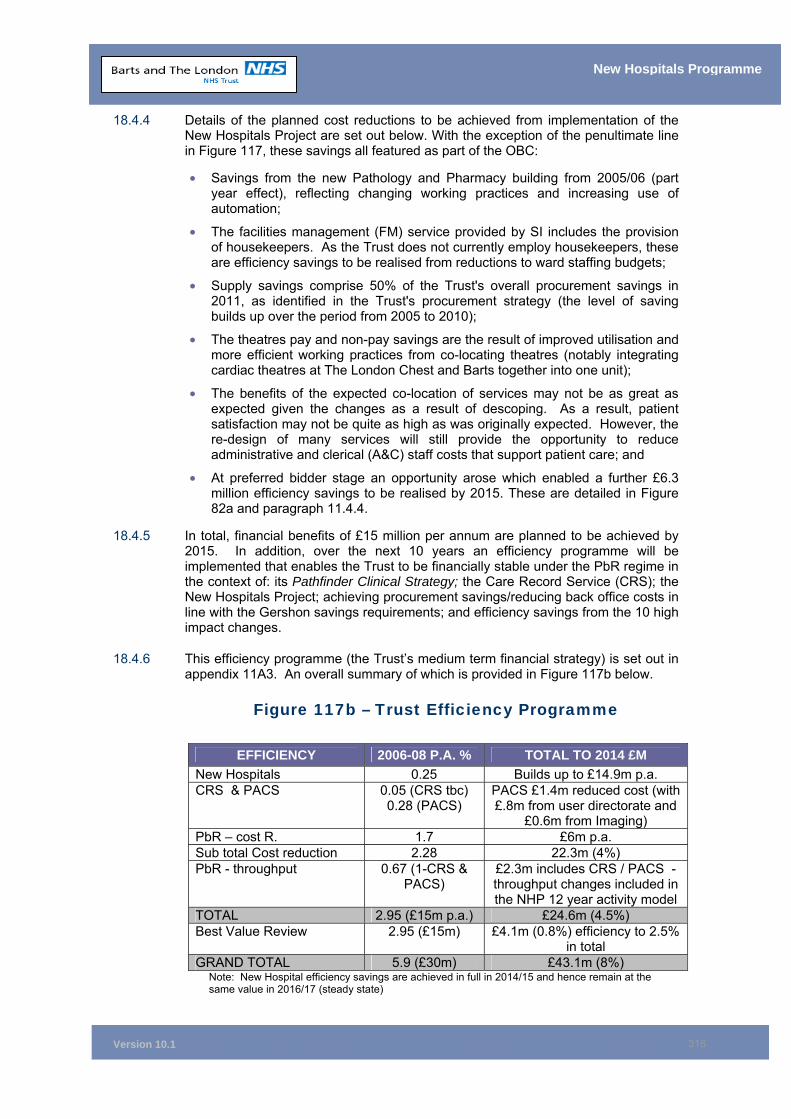
Version 10.1
316
New Hospitals Programme
18.4.4 Details of the planned cost reductions to be achieved from implementation of the New Hospitals Project are set out below. With the exception of the penultimate line in Figure 117, these savings all featured as part of the OBC:
• Savings from the new Pathology and Pharmacy building from 2005/06 (part year effect), reflecting changing working practices and increasing use of automation;
• The facilities management (FM) service provided by SI includes the provision of housekeepers. As the Trust does not currently employ housekeepers, these are efficiency savings to be realised from reductions to ward staffing budgets;
• Supply savings comprise 50% of the Trust's overall procurement savings in 2011, as identified in the Trust's procurement strategy (the level of saving builds up over the period from 2005 to 2010);
• The theatres pay and non-pay savings are the result of improved utilisation and more efficient working practices from co-locating theatres (notably integrating cardiac theatres at The London Chest and Barts together into one unit);
• The benefits of the expected co-location of services may not be as great as expected given the changes as a result of descoping. As a result, patient satisfaction may not be quite as high as was originally expected. However, the re-design of many services will still provide the opportunity to reduce administrative and clerical (A&C) staff costs that support patient care; and
• At preferred bidder stage an opportunity arose which enabled a further £6.3 million efficiency savings to be realised by 2015. These are detailed in Figure 82a and paragraph 11.4.4.
18.4.5 In total, financial benefits of £15 million per annum are planned to be achieved by 2015. In addition, over the next 10 years an efficiency programme will be implemented that enables the Trust to be financially stable under the PbR regime in the context of: its Pathfinder Clinical Strategy; the Care Record Service (CRS); the New Hospitals Project; achieving procurement savings/reducing back office costs in line with the Gershon savings requirements; and efficiency savings from the 10 high impact changes.
18.4.6 This efficiency programme (the Trust’s medium term financial strategy) is set out in appendix 11A3. An overall summary of which is provided in Figure 117b below.
Figure 117b – Trust Efficiency Programme
EFFICIENCY 2006-08 P.A. % TOTAL TO 2014 £M New Hospitals 0.25 Builds up to £14.9m p.a. CRS & PACS 0.05 (CRS tbc)
0.28 (PACS) PACS £1.4m reduced cost (with £.8m from user directorate and
£0.6m from Imaging) PbR – cost R. 1.7 £6m p.a. Sub total Cost reduction 2.28 22.3m (4%) PbR - throughput 0.67 (1-CRS &
PACS) £2.3m includes CRS / PACS -throughput changes included in the NHP 12 year activity model
TOTAL 2.95 (£15m p.a.) £24.6m (4.5%) Best Value Review 2.95 (£15m) £4.1m (0.8%) efficiency to 2.5%
in total GRAND TOTAL 5.9 (£30m) £43.1m (8%)
Note: New Hospital efficiency savings are achieved in full in 2014/15 and hence remain at the same value in 2016/17 (steady state)
Version 10.1
317
New Hospitals Programme
18.4.7 These savings, although cash releasing, are required to offset the cost pressures from quality improvements associated with the transfer of services into new facilities; the provision of new models of care and meeting additional cost pressures which arise from the uplift to 2006/07 tariffs (only 1.6%); pay drift; PbR rebasing; and reductions to the R&D central levy allocation. The savings would need to be used in this way regardless of whether the project was funded from public monies or from the private sector (PFI).
18.4.8 Although many of these efficiencies are not attributable to the New Hospitals Project, achieving them does impact on the affordability of the scheme, therefore the detail as to the methodology of approach for realising these efficiencies is set out in Chapter 11.
18.4.9 The PAFM Group which is jointly chaired by the Directors of Finance and Performance Management and Planning and includes all the clinical directorate general managers is responsible for co-ordinating the development of efficiency plans and monitoring their delivery including those to be realised from the New Hospitals Programme. The tracking schedule that PAFM uses for both the development and monitoring of the efficiency programme will ensure that there is no double counting of efficiency between the New Hospitals Project and the other workstreams.
18.4.10 In conclusion, the efficiency savings that are required for both the New Hospitals Project and “general efficiency” to sustain financial stability are challenging, but achievable.
Non Financial Benefits
18.4.11 The eight high level benefits identified are set out in Appendix 18A. This appendix also sets out:
The impact of the benefit; Risks to achieving the benefit; The measures applicable to each; Named responsible individuals (owners of the benefits); and Timeframe for delivery, etc., i.e. a high level Benefits Realisation Plan.
18.4.12 These high level benefits are underpinned by a number of more detailed benefits that will be achieved from the delivery of the scheme and which can be grouped under the six headings listed below. These will be developed further as part of the Benefits Realisation Planning phase in line with the Trust’s Benefits Management Strategy.
Benefits to Patients
Patients will be treated in a modern, purpose built environment, with an average of 40% single rooms128. This new environment will ensure that privacy and dignity standards can be met.
The higher specification to the finish on the new and refurbished buildings will allow for better cleaning and further improvement in the Trust’s already impressive track record in minimising hospital acquired infection.
The quality of food provision will also improve as a result of better catering facilities, ensuring that the Trust meets and exceeds the “Better Hospital Food Standards”.
There is separation of servicing from patient traffic and services have been located in a manner that allows for easy way-finding which will be further
128 Note: This figure represents single rooms as a % of all inpatient beds excluding beds in Critical Care Areas.
Version 10.1
318
New Hospitals Programme
facilitated through well-sited reception points and the use of art. Art will also be used to enhance the therapeutic environment funded through charitable donations.
Better provision has been made for patient advice services, multi-faith facilities, shops and other services.
The hospital will have a number of gardens and quiet areas for patients and their visitors to use. Hostel accommodation will continue to be available for parents, carers and patients who have to travel.
Physical access will be improved with improved wayfinding, designated drop off zones and increased parking, including disabled parking. Access from the underground station to The Royal London Hospital will be improved.
Access to care will be improved through the increased number of beds, improved day-care and ambulatory provision of additional improved equipment.
In summary, the patient pathway and thus personal experience of patients treated in the hospitals will be greatly improved.
Benefits to staff
• All clinical staff will benefit from a “fit for purpose environment”. They have been involved in specifying the co-location of clinical services, thus allowing for the most efficient delivery of care. These co-locations have been achieved in the design.
• Staff will also have access to the most modern medical equipment which, for the major items, will be replaced on a regular basis in accordance with their recommended life.
• Staff changing facilities are co-located with their work areas as well as access to the improved catering, retail and multi-faith facilities.
• Improved parking facilities will benefit essential car users.
• The modern environment will improve the recruitment and retention of staff. In particular, the security of the two sites will be much improved. Security is a major concern of staff at the present time.
• The majority of facilities service staff will remain Trust employees under the Retention of Employment arrangements and therefore be covered by Agenda for Change. For those that transfer, the Trust has negotiated terms that achieve comparability with those in Agenda for Change (including GAD approved final salary pensions), thus ensuring a two-tier workforce does not develop.
Benefits to clinical quality and performance
• The design facilitates the separation of emergency from planned care. The Barts site will be almost entirely for planned care and within The Royal London, the planned care facilities are physically separated from those for emergency patients. This, together with the increased number of beds and ambulatory and short stay care facilities, will enable the two hospitals to run more effectively. In particular, it will eliminate the inefficiencies caused by the 98% occupancy currently experienced at The Royal London.
• The modern clinical environment provides the Trust with the opportunity to optimise clinical care, leading to an improvement in the Trust’s already strong performance in clinical outcomes.
• The new easy to clean and maintain environment will reduce hospital acquired infection.
• The modern and well-maintained plant and equipment will be more reliable, thereby reducing the clinical risks that can be caused by breakdowns.
Version 10.1
319
New Hospitals Programme
• Better clinical co-locations and a closer fit between facilities available will enable clinical performance to be optimised (for example, an increased proportion of care undertaken on a day-care or short stay basis). While the residual cases requiring inpatient care will be more complex, some reduction in length of stay will be achievable through the more effective use of clinical facilities and an improved therapeutic environment.
• The much improved environment will enable the Trust to attract leading clinical practitioners, which will further enhance clinical performance.
Benefits to the physical environment
• The redevelopment eliminates £100 million of backlog maintenance.
• Systematic refurbishment and maintenance of clinical areas will be undertaken leading to an improved environment for staff and patients.
• Security will improve - the design solution enables better security of the site and improves the safety of staff and property. This should help to improve staff morale and reduce the number of security incidents.
• The design solution facilitates better wayfinding.
• The artwork and gardens will provide an improved therapeutic environment (to be funded from charitable donations).
• The new hospitals have been designed with future flexibility in mind. The construction uses a large 9m2 grid (compares to 7m2 in most standard schemes), which provides greater flexibility in reconfiguring internal space. Universal floor loadings capable of supporting the heaviest equipment currently available means that changing use will not be constrained by equipment requirements. Services space and risers are generous, facilitating re-routing if necessary.
Benefits to commissioners
18.4.13 Clearly all the benefits that accrue to the Trust’s patients and staff are equally beneficial to commissioners, in terms of ensuring their populations continue to receive a high standard of healthcare.
18.4.14 Opportunity is provided to increase the throughput of patients to meet additional acute hospital requirements resulting from the population growth in the Thames Gateway regeneration scheme. The Trust will be able to provide the majority of demand for increased secondary and tertiary care for Tower Hamlets and the increased tertiary care for the other local PCTs. This would eliminate the need for further investment in acute care infrastructure, particularly if the local health economy develops models of, care that promote the management of chronic illness as far as possible in patients homes or local healthcare facilities.
18.4.15 The clinical performance assumptions that underpinned the planning of the new hospitals represented a reasonably challenging agenda in the period in which they were developed (calendar year 2000 – clinical performance benchmarked against the upper quartile of teaching hospital performance). Since then, the Trust has done considerable work on developing its clinical strategy. In addition, the Modernisation Agency has disseminated a large amount of good practice on improving clinical efficiency which the Trust is progressing through the work of its Transformation Team. Such developments will allow it to process additional work over and above that originally planned.
Version 10.1
320
New Hospitals Programme
Socio-economic benefits
18.4.16 The redevelopment of Barts and The London will also create substantial regeneration benefits for East London.
18.4.17 In relation to employment and training, the development will expand the number of jobs available. Indeed it has already stimulated the Trust to recruit and train local people in order to contribute to a first class workforce alongside first class buildings. This is being addressed through an Actions for Community Employment Strategy that entails partnership with regeneration and education agencies, including the London Development Agency, Job Centre Plus and the London Health Commission, alongside partners from the local health economy and the London Borough of Tower Hamlets.
18.4.18 Alongside these initiatives, the Trust will be working with Skanska Innisfree to ensure that a similar offer is made to local communities in respect of construction employment, with over 1,500 construction jobs planned to be created in the course of the development.
18.4.19 The Trust and Skanska Innisfree will also ensure that local businesses are informed of the opportunities available to them through the development and operation of the new hospitals.
18.4.20 The redevelopment offers a new set of options to local communities in respect of job and business opportunities in areas of high deprivation and economic inactivity.
18.4.21 A second set of opportunities relates to the physical impact of the development, especially in regard to The Royal London Hospital. The Royal London is placed within the strategically important City Fringe area, regarded by the London Borough of Tower Hamlets as a key development area. The planned hospital development, alongside complementary developments such as the new Pathology and Pharmacy and Medical College buildings, will create a health and education campus for the area. This will form a key component for the future regeneration of the area, which will include a new London Underground Station opposite the hospital to serve the new East London Line Extension and, in due course, Crossrail.
18.4.22 The dramatic physical change to the landscape of Whitechapel will act as a catalyst for further regeneration and business development, also providing a basis for improved retail and leisure opportunities.
Trust approach to benefits management
18.4.23 Benefits management is about enabling business performance improvement and is focused on the actual realisation of the benefits as opposed to merely forecast benefits as outlined in the FBC. Therefore, the Trust’s focus will not be just the delivery of the physical programme, but also the changes required in the business to realise the benefits.
18.4.24 It is for this reason that the work programme for the delivery of benefits will be led by the Director of Operations, an Executive Director of the Trust Board. The Director of Operations will be supported by the trust’s Clinical Service Transformation Team and the Programme’s Head of Clinical Service Development.
18.4.25 The Trust approach is as follows:
Benefits planning including developing a Benefits Management Strategy; Benefits identification; Benefits realisation planning;
Version 10.1
321
New Hospitals Programme
Benefits realisation; and Benefits Review,
Benefits Planning
18.4.26 The Trust is in the process of developing the benefits realisation strategy and setting up the structures, systems and detailed plans needed to realise the high level strategic benefits. A detailed programme of work has been identified, which includes development of detailed directorate-specific benefit realisation plans, signed up and agreed at an operational level, which will ensure delivery of the high level strategic benefits. A copy of the work programme can be found at Appendix 18B.
18.4.27 A governance structure has been developed to support the realisation of the benefits. A Benefits Realisation Steering Group (BRSG), led by the Director of Operations has been established to oversee and manage delivery of the benefits. The terms of reference for this group are set out in Appendix 18C. The BRSG will report to the New Hospitals Programme Board and will be responsible for: producing the Benefits Management Strategy; identifying those elements of work necessary to achieve the high level benefits and operational changes required to realise them; and monitoring benefits actually delivered. The work of the BRSG will be supported by the results of parallel business change work programmes proceeding in the Trust. These will result in key deliverables, including the Trust’s revised Stakeholder Management Strategy, its Business Change Strategy and a new Communications and Marketing Strategy.
18.4.28 In addition, day-to-day support will also be provided by the Trust’s Programme Support Office and progress monitored by the Pathfinder Programme Assurance Board (see Chapter 14).
Benefits Identification
18.4.29 This is an ongoing activity throughout the programme from the strategic benefits used in the production of the FBC to the operational benefits identified once in operation. The Trust currently has identified eight strategic benefits (see Appendix 18A). These are specific, measurable, achievable, realistic and time bound. In addition, they are focused on the Trust's strategic aims and objectives.
18.4.30 The benefits are appropriate to stakeholders, balanced and cover all significant areas of work. The Trust believes that the benefits delivery will be resilient to organisational changes as the benefits management strategy will be integrated into the Trust’s wider organisational processes. In addition, the Trust believes that the benefits realisation processes it has put in place are cost-effective and represent a reasonable balance between the benefits derived and the effort required to collect and collate relevant information.
Benefits Realisation Planning
18.4.31 The Trust is in the process of developing a detailed benefits realisation plan which governs how the benefits will be managed. This detailed plan will include timescales for delivery, plans for measuring and analysing benefit data, and timescales for formal reviews including OGC Gateways. A necessary input for this plan will be a baseline programme delivery plan, albeit at a programme milestone level. A key current task is completing a baseline measurement of the benefit (the as-is state), before any new processes or procedures are put in place.
Version 10.1
322
New Hospitals Programme
Benefits Realisation
18.4.32 The purpose of this phase is to implement the business changes required in order to maximise the realisation of benefits. The Director of Operations will be the business change owner and will have responsibility for ensuring the planned business change actually occurs. The Programme Support Office will assist in supporting the business change owner.
18.4.33 This phase will also comprise ongoing monitoring and measurement of benefits and is supported by training and communications plans to raise awareness of the benefits.
Benefits Review
18.4.34 The Trust considers it important to regularly review the benefits being delivered to ensure their effect and benefit is maximised and that good practice in the delivery of these benefits is shared. This will be an ongoing process. Typical activities will be business change reviews, sharing of best practice, sharing lessons learned and communications with stakeholders and key operational users and areas. This will be used to both identify ongoing benefits and maximise and assure the realisation of identified benefits.
18.4.35 Achieving the benefits and maximising the potential of the new hospitals development is something that the Trust is determined to realise. Because of this, it is thought essential to undertake some training in the delivery of benefits and the Cranfield School of Business Managements have been engaged to assist in this process.
18.5 Chapter Conclusion 18.5.1 This chapter has set out the main objectives and benefits to be realised from the
project. It has shown that there are robust and comprehensive plans in place to monitor their delivery.
18.6 Chapter Appendices 18A High Level Benefits Realisation Plan 18B Benefits Realisation – Programme of Work 18C Benefits Realisation Steering Group Terms of Reference
Version 10.1
323
New Hospitals Programme
19 POST-PROJECT EVALUATION Synopsis – Post-Project Evaluation • A phased process for post-project evaluation has been developed
• Deliverables have been set against the phased evaluation process
• Resources for undertaking the evaluation process have been identified and agreement reached on funding the work
19.1 Introduction 19.1.1 Post-project evaluation (PPE) is a mandatory requirement for all trusts undertaking
a project of this scope and scale.
19.1.2 PPE will evaluate the outcomes, not only to establish whether the overarching objectives outlined in the Full Business Case (FBC) have been met, but also to understand the impact the scheme has had on the organisation and ensure that lessons are learnt from the implementation of the project for the benefit of others.
19.1.3 This chapter details the PPE process to be employed by the Trust, and will act as a reference point against which the Trust Board will evaluate the process129.
19.1.4 The Programme Director will take responsibility for the evaluation process and deliverables and be accountable to the Programme Board.
19.2 Post-Project Evaluation Objectives 19.2.1 The main objectives of PPE are to assess:
• Whether the project is running to plan;
• Whether the identified benefits of the project are being realised;
• Whether Value for Money (VfM) is being delivered and achieved; and
• Opportunities for improving current and future performance, i.e. learning lessons.
19.2.2 The PPE process is therefore closely mapped to:
• The project’s global objectives (see Figure 118);
• The timetabled phases of the project (See Figure 119); and
• The Benefits Realisation Plan (see Appendix 18A).
129 See also Appendix 19A for the PFI Post-Implementation Framework.
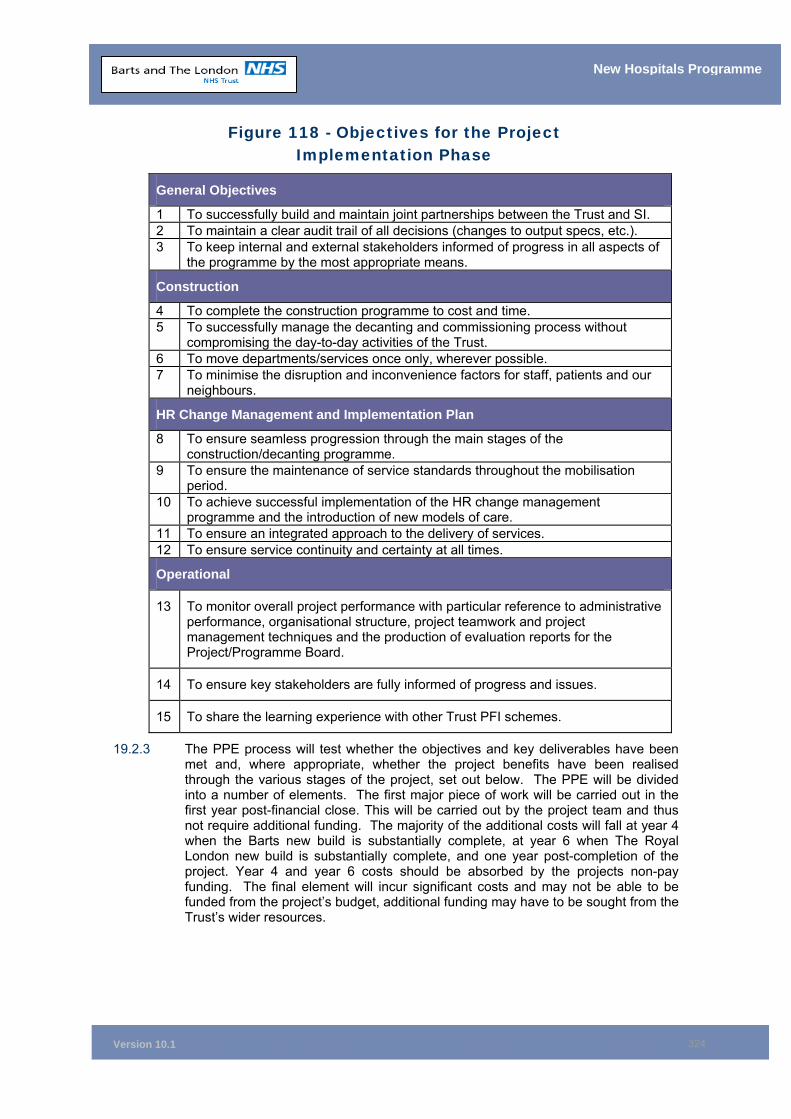
Version 10.1
324
New Hospitals Programme
Figure 118 - Objectives for the Project Implementation Phase
General Objectives
1 To successfully build and maintain joint partnerships between the Trust and SI. 2 To maintain a clear audit trail of all decisions (changes to output specs, etc.). 3 To keep internal and external stakeholders informed of progress in all aspects of
the programme by the most appropriate means.
Construction
4 To complete the construction programme to cost and time. 5 To successfully manage the decanting and commissioning process without
compromising the day-to-day activities of the Trust. 6 To move departments/services once only, wherever possible. 7 To minimise the disruption and inconvenience factors for staff, patients and our
neighbours.
HR Change Management and Implementation Plan
8 To ensure seamless progression through the main stages of the construction/decanting programme.
9 To ensure the maintenance of service standards throughout the mobilisation period.
10 To achieve successful implementation of the HR change management programme and the introduction of new models of care.
11 To ensure an integrated approach to the delivery of services. 12 To ensure service continuity and certainty at all times.
Operational
13 To monitor overall project performance with particular reference to administrative performance, organisational structure, project teamwork and project management techniques and the production of evaluation reports for the Project/Programme Board.
14 To ensure key stakeholders are fully informed of progress and issues.
15 To share the learning experience with other Trust PFI schemes.
19.2.3 The PPE process will test whether the objectives and key deliverables have been met and, where appropriate, whether the project benefits have been realised through the various stages of the project, set out below. The PPE will be divided into a number of elements. The first major piece of work will be carried out in the first year post-financial close. This will be carried out by the project team and thus not require additional funding. The majority of the additional costs will fall at year 4 when the Barts new build is substantially complete, at year 6 when The Royal London new build is substantially complete, and one year post-completion of the project. Year 4 and year 6 costs should be absorbed by the projects non-pay funding. The final element will incur significant costs and may not be able to be funded from the project’s budget, additional funding may have to be sought from the Trust’s wider resources.
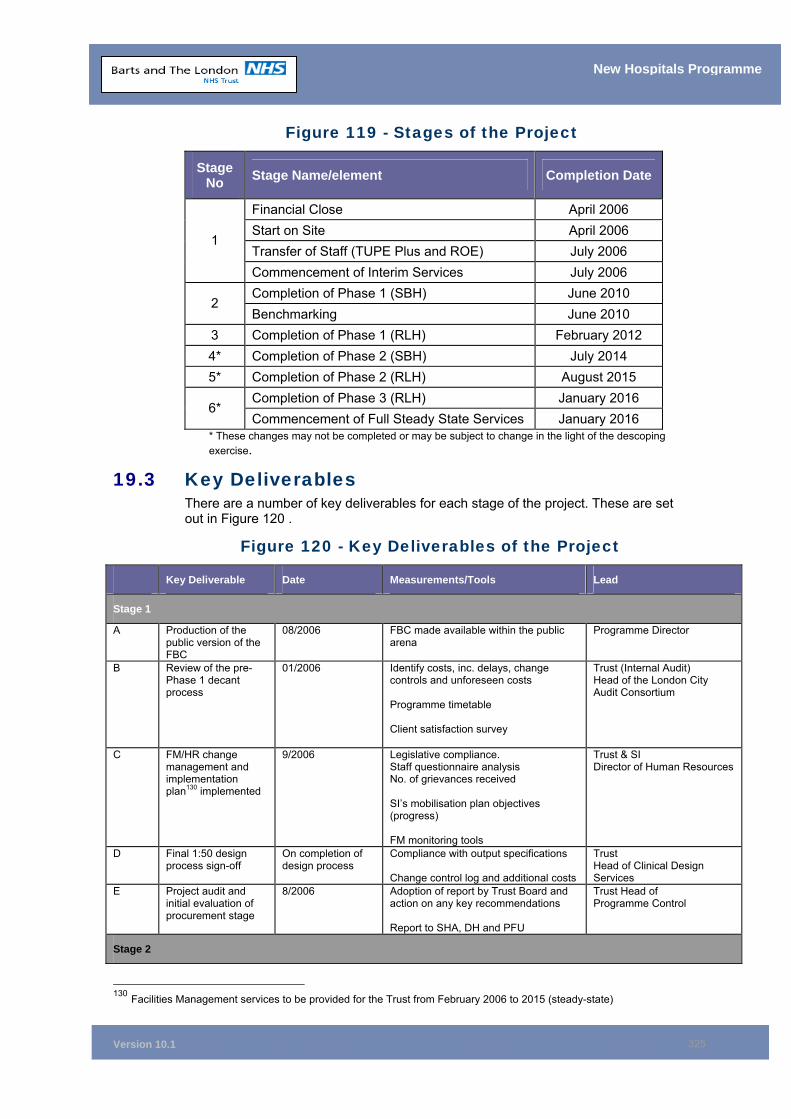
Version 10.1
325
New Hospitals Programme
Figure 119 - Stages of the Project
Stage No Stage Name/element Completion Date
Financial Close April 2006 Start on Site April 2006 Transfer of Staff (TUPE Plus and ROE) July 2006
1
Commencement of Interim Services July 2006 Completion of Phase 1 (SBH) June 2010
2 Benchmarking June 2010
3 Completion of Phase 1 (RLH) February 2012 4* Completion of Phase 2 (SBH) July 2014 5* Completion of Phase 2 (RLH) August 2015
Completion of Phase 3 (RLH) January 2016 6*
Commencement of Full Steady State Services January 2016 * These changes may not be completed or may be subject to change in the light of the descoping exercise.
19.3 Key Deliverables There are a number of key deliverables for each stage of the project. These are set out in Figure 120 .
Figure 120 - Key Deliverables of the Project
Key Deliverable Date Measurements/Tools Lead
Stage 1
A Production of the public version of the FBC
08/2006 FBC made available within the public arena
Programme Director
B Review of the pre-Phase 1 decant process
01/2006 Identify costs, inc. delays, change controls and unforeseen costs Programme timetable Client satisfaction survey
Trust (Internal Audit) Head of the London City Audit Consortium
C FM/HR change management and implementation plan130 implemented
9/2006 Legislative compliance. Staff questionnaire analysis No. of grievances received SI’s mobilisation plan objectives (progress) FM monitoring tools
Trust & SI Director of Human Resources
D Final 1:50 design process sign-off
On completion of design process
Compliance with output specifications Change control log and additional costs
Trust Head of Clinical Design Services
E Project audit and initial evaluation of procurement stage
8/2006 Adoption of report by Trust Board and action on any key recommendations Report to SHA, DH and PFU
Trust Head of Programme Control
Stage 2
130 Facilities Management services to be provided for the Trust from February 2006 to 2015 (steady-state)
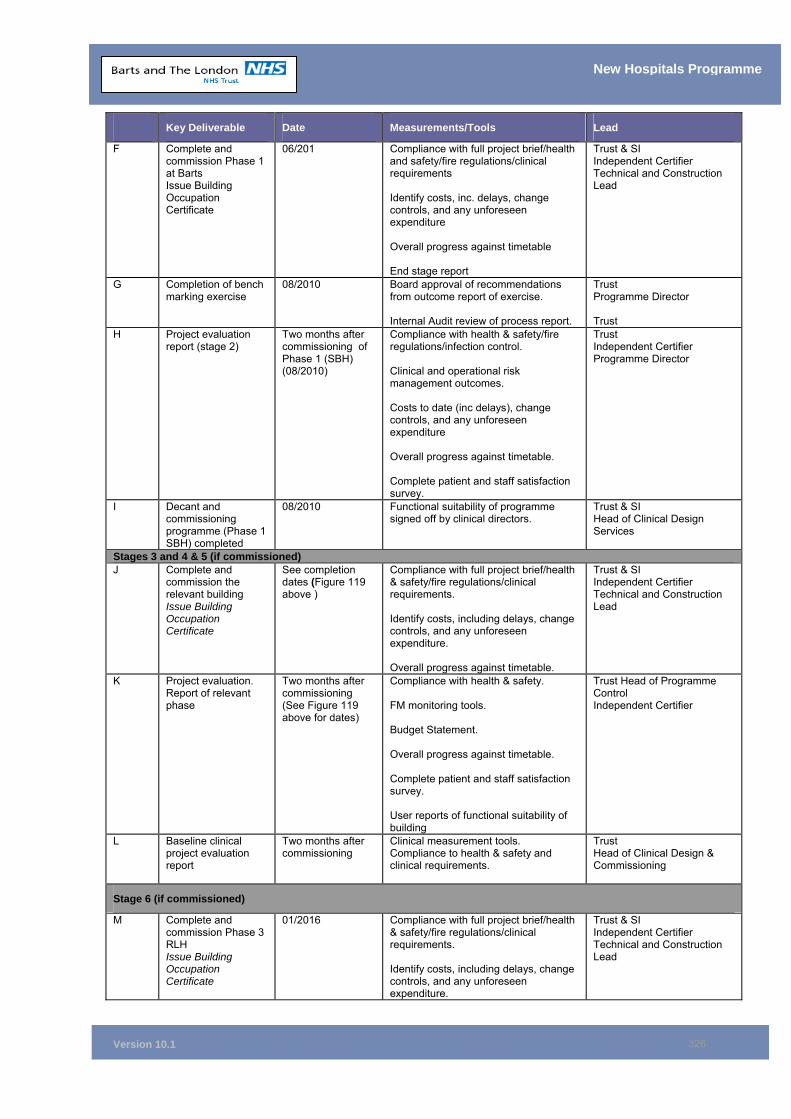
Version 10.1
326
New Hospitals Programme
Key Deliverable Date Measurements/Tools Lead
F Complete and commission Phase 1 at Barts Issue Building Occupation Certificate
06/201 Compliance with full project brief/health and safety/fire regulations/clinical requirements Identify costs, inc. delays, change controls, and any unforeseen expenditure Overall progress against timetable End stage report
Trust & SI Independent Certifier Technical and Construction Lead
G Completion of bench marking exercise
08/2010
Board approval of recommendations from outcome report of exercise. Internal Audit review of process report.
Trust Programme Director Trust
H Project evaluation report (stage 2)
Two months after commissioning of Phase 1 (SBH) (08/2010)
Compliance with health & safety/fire regulations/infection control. Clinical and operational risk management outcomes. Costs to date (inc delays), change controls, and any unforeseen expenditure Overall progress against timetable. Complete patient and staff satisfaction survey.
Trust Independent Certifier Programme Director
I Decant and commissioning programme (Phase 1 SBH) completed
08/2010 Functional suitability of programme signed off by clinical directors.
Trust & SI Head of Clinical Design Services
Stages 3 and 4 & 5 (if commissioned) J Complete and
commission the relevant building Issue Building Occupation Certificate
See completion dates (Figure 119 above )
Compliance with full project brief/health & safety/fire regulations/clinical requirements. Identify costs, including delays, change controls, and any unforeseen expenditure. Overall progress against timetable.
Trust & SI Independent Certifier Technical and Construction Lead
K Project evaluation. Report of relevant phase
Two months after commissioning (See Figure 119 above for dates)
Compliance with health & safety. FM monitoring tools. Budget Statement. Overall progress against timetable. Complete patient and staff satisfaction survey. User reports of functional suitability of building
Trust Head of Programme Control Independent Certifier
L Baseline clinical project evaluation report
Two months after commissioning
Clinical measurement tools. Compliance to health & safety and clinical requirements.
Trust Head of Clinical Design & Commissioning
Stage 6 (if commissioned)
M Complete and commission Phase 3 RLH Issue Building Occupation Certificate
01/2016 Compliance with full project brief/health & safety/fire regulations/clinical requirements. Identify costs, including delays, change controls, and any unforeseen expenditure.
Trust & SI Independent Certifier Technical and Construction Lead
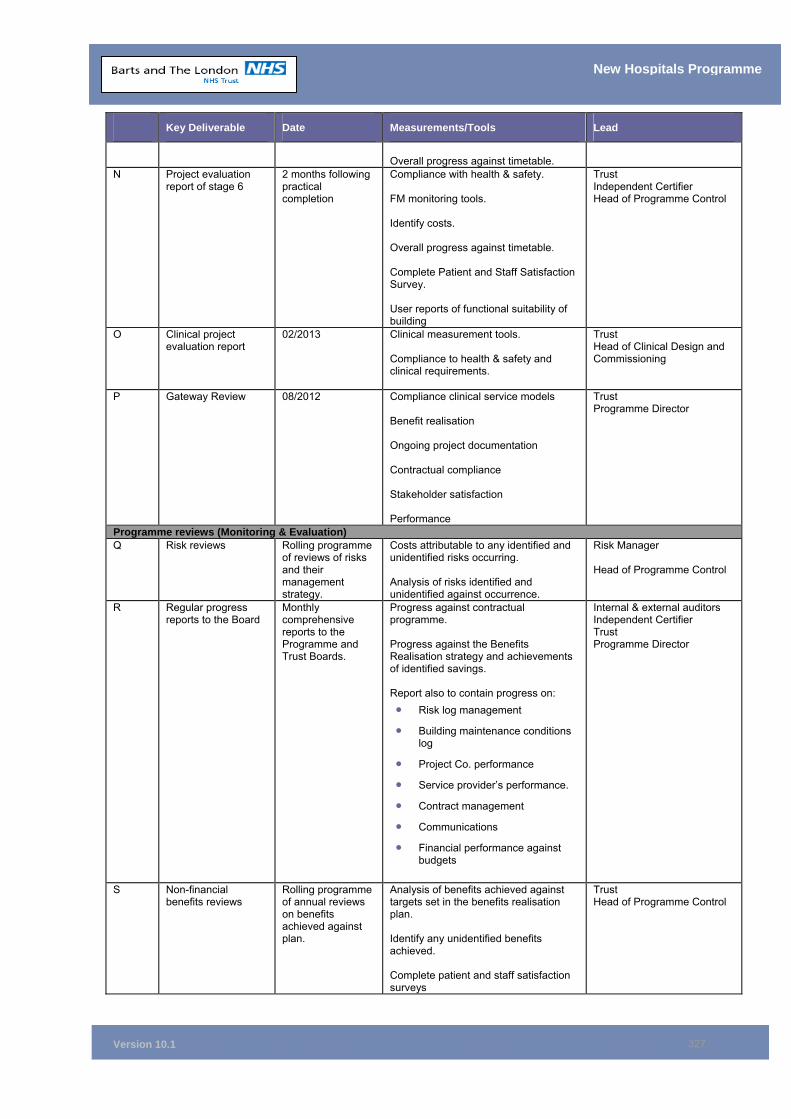
Version 10.1
327
New Hospitals Programme
Key Deliverable Date Measurements/Tools Lead
Overall progress against timetable.
N Project evaluation report of stage 6
2 months following practical completion
Compliance with health & safety. FM monitoring tools. Identify costs. Overall progress against timetable. Complete Patient and Staff Satisfaction Survey. User reports of functional suitability of building
Trust Independent Certifier Head of Programme Control
O Clinical project evaluation report
02/2013 Clinical measurement tools. Compliance to health & safety and clinical requirements.
Trust Head of Clinical Design and Commissioning
P Gateway Review 08/2012 Compliance clinical service models Benefit realisation Ongoing project documentation Contractual compliance Stakeholder satisfaction Performance
Trust Programme Director
Programme reviews (Monitoring & Evaluation) Q Risk reviews Rolling programme
of reviews of risks and their management strategy.
Costs attributable to any identified and unidentified risks occurring. Analysis of risks identified and unidentified against occurrence.
Risk Manager Head of Programme Control
R Regular progress reports to the Board
Monthly comprehensive reports to the Programme and Trust Boards.
Progress against contractual programme. Progress against the Benefits Realisation strategy and achievements of identified savings. Report also to contain progress on: • Risk log management
• Building maintenance conditions log
• Project Co. performance
• Service provider’s performance.
• Contract management
• Communications
• Financial performance against budgets
Internal & external auditors Independent Certifier Trust Programme Director
S Non-financial benefits reviews
Rolling programme of annual reviews on benefits achieved against plan.
Analysis of benefits achieved against targets set in the benefits realisation plan. Identify any unidentified benefits achieved. Complete patient and staff satisfaction surveys
Trust Head of Programme Control
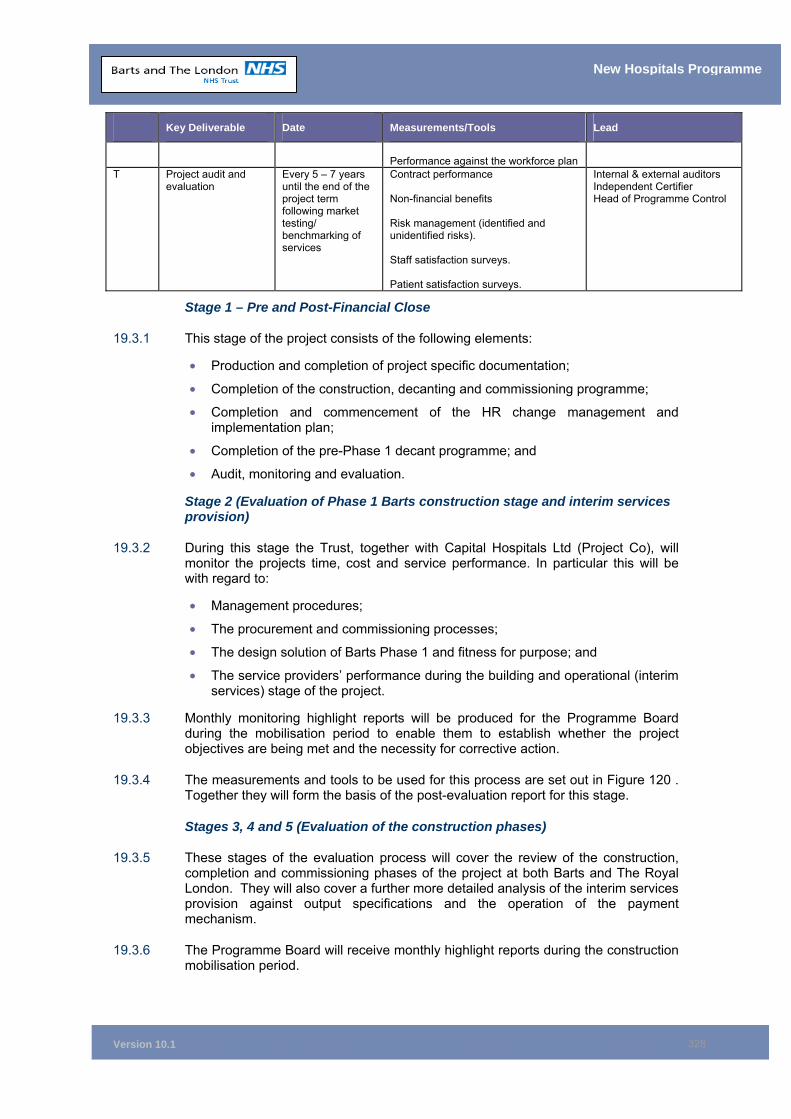
Version 10.1
328
New Hospitals Programme
Key Deliverable Date Measurements/Tools Lead
Performance against the workforce plan
T Project audit and evaluation
Every 5 – 7 years until the end of the project term following market testing/ benchmarking of services
Contract performance Non-financial benefits Risk management (identified and unidentified risks). Staff satisfaction surveys. Patient satisfaction surveys.
Internal & external auditors Independent Certifier Head of Programme Control
Stage 1 – Pre and Post-Financial Close
19.3.1 This stage of the project consists of the following elements:
• Production and completion of project specific documentation;
• Completion of the construction, decanting and commissioning programme;
• Completion and commencement of the HR change management and implementation plan;
• Completion of the pre-Phase 1 decant programme; and
• Audit, monitoring and evaluation.
Stage 2 (Evaluation of Phase 1 Barts construction stage and interim services provision)
19.3.2 During this stage the Trust, together with Capital Hospitals Ltd (Project Co), will monitor the projects time, cost and service performance. In particular this will be with regard to:
• Management procedures;
• The procurement and commissioning processes;
• The design solution of Barts Phase 1 and fitness for purpose; and
• The service providers’ performance during the building and operational (interim services) stage of the project.
19.3.3 Monthly monitoring highlight reports will be produced for the Programme Board during the mobilisation period to enable them to establish whether the project objectives are being met and the necessity for corrective action.
19.3.4 The measurements and tools to be used for this process are set out in Figure 120 . Together they will form the basis of the post-evaluation report for this stage.
Stages 3, 4 and 5 (Evaluation of the construction phases)
19.3.5 These stages of the evaluation process will cover the review of the construction, completion and commissioning phases of the project at both Barts and The Royal London. They will also cover a further more detailed analysis of the interim services provision against output specifications and the operation of the payment mechanism.
19.3.6 The Programme Board will receive monthly highlight reports during the construction mobilisation period.
Version 10.1
329
New Hospitals Programme
19.3.7 These highlight reports, together with the other measurements/tools identified in Figure 120 , will be used to assist the production of an appropriate stage evaluation report.
Stage 6 (Evaluating longer-term outcomes)
19.3.8 This stage will re-assess the preliminary outcomes identified in the previous phases and will additionally address changes in operating costs, risk allocation and transfer activity rates in various specialities.
19.3.9 Ongoing PPE will be undertaken throughout the life of the project to identify continuous improvement.
19.4 The Process 19.4.1 Successful evaluation begins with clear, specific and measurable goals. In
accordance with the Good Practice Guide, Learning Lessons from Post-Project Evaluation, the Trust will develop a post-project evaluation tool to assess the performance of the project through a systematic analysis of the outcomes against the expected benefit criteria identified in the FBC.
19.4.2 Evaluation is an essential tool to improve the overall project performance, achieve best VfM and improve decision-making. The evaluation of the project will also:
• Ascertain whether the project is running smoothly so that corrective action can be taken;
• Promote organisational learning both within the Trust and also in the wider NHS PFI environment;
• Avoid repeating costly mistakes;
• Improve decision-making and resource allocation; and
• Improve accountability by demonstrating to internal and external parties that resources have been used efficiently and effectively.
19.4.3 This will, in part, necessitate a continual reflective learning process, not only to ensure that the project is delivered within quality, time and cost standards, but also to help improve the standards of business case development, project appraisal, design, management and implementation within the Trust and the wider NHS.
19.4.4 This will be achieved by a combination of interim progress reports through the governance structure to the Trust Board and highlight reports to the Trust’s Programme Assurance Board. These reports, together with the formal evaluation process at set stages in the project following completion of major milestones, form the basis of the PPE process.
19.4.5 Audit reports will be prepared after each of these key milestones. These key project evaluations will form part of the annual audit programme.
19.5 Organisation Project management approach
19.5.1 A proactive approach to the management of this phase of the project will be supported by agreement of the following before each stage occurs:
• What the key tasks are;
Version 10.1
330
New Hospitals Programme
• Who is best placed to lead and undertake the task;
• An agreed structure for any deliverables;
• Agreed quality measures for the task; and
• The cost of the activity.
19.5.2 These agreements will be reflected within the products of the project and will be monitored by the Programme Director and Project Management Team.
Outputs of the Project
19.5.3 Outputs will be required periodically as described within the key deliverables. The production of these reports will be supported by ongoing management of the project and will be delivered to an agreed quality standard and reviewed accordingly.
19.5.4 The different elements/tools to be employed in the PPE process are set out below:
• Management outputs – to set up, manage, monitor and deliver the project;
• Quality criteria – the quality assessment for the individual reports so that the individuals responsible for the delivery of the reports are clear from the outset as to their priorities; and
• Quality methods – the process necessary to evaluate the quality of the reports which, in some areas, will require approval from the Trust Board and in other cases will require quality assurance by individual members of the project team or the Trust's executive team.
19.6 Chapter Conclusion 19.6.1 The Trust’s process for PPE is phased and robust and consistent with the “Good
Practice Guide: Learning Lessons from Post-Project Evaluation”.
19.6.2 It will enable a full evaluation during and after functional completion of the project on the extent of achievement of the original objectives and benefits.
19.7 Chapter Appendices 19A PFI Post-Implementation Framework

















