Page 1
You Will Read About
Special Topics
Hemoperfusion Therapy in Children
Continues HP VS Intermittent HP
New Indications
Subarachnoid Hemorrhage (SAH)
Symmetrical Peripheral Gangrene (SPG)
Safety and Feasibility
Hemoperfusion on 183 Dialysis Patients
Single HP and HP + CRRT/ECMO
Page 2
FOREWORD
This clinical based evidence collection followsthe relevant regulations and policies of theJafron CREAT project, and is intended to promotethe clinical experience sharing, discussion andeducation of hemoperfusion.We thank the clinicians’ valuable sharing andtheir continuous attentions to this project withtheir creative thinking and exploration in thefield of hemoperfusion during clinical practice.
Page 3
Content
1. Recovery Of Symmetrical Peripheral Gangrene Of Limbs In A Patient After
Performing Hemoadsorption In Septic Shock, SCI, Turkey, New Indication
2. Subarachnoid Hemorrhage And Extracorporeal Blood Purification With
HA-380 And High-volume Hemofiltration: A New Therapeutic Challenge At
The Neurocritical Care Unit? A Case Report, SCI, Chile, New Indication
3. Case Series: Efficacy And Safety Of Hemoadsorption With HA-330
Adsorber In Septic Pediatric Patients With Cancer, SCI, Kazakhstan, Special
Topic
4. Efficacy Of Hemoperfusion In Severe And Critical Cases Of Covid-19, Iran,
Special Topic
5. Experience Of Application Of Combined Extracorporeal Blood Purification
With Hemoadsorption (HA330/HA330-II) At Patients With Severe Covid –
19, Kazakhstan, Safety & Feasibility
6. Blood Purification Techniques, Inflammatory Mediators And Mortality In
COVID-19 Patients, Iran
7. Effectiveness Of Hemoperfusion (HP) In Hemodialysis (HD) Patients With
Covid-19 Infection, Greece
8. Clinical Outcomes Of Hemoperfusion Using HA130 Cartridge Among
Maintenance Hemodialysis Patients In St. Luke’s Medical Center-qc
Dialysis Unit And Flora V Valisno De Siojo Dialysis Center Ofgat Andres
Memorial Medical Center: A Cross-sectional Study: Philippines, Safety &
Feasibility
9. Combination Hemodialysis- Hemoperfusion: Provides Benefit To Dialysis
Patients?, Greece
10. A Randomized Controlled Trial (Rct) Of Efficacy And Safety Of
Hemoperfusion Or Plasma Exchange Compared To Standard Medical
Therapy In Patients With Acute On Chronic Liver Failure, India
1
8
12
22
33
40
49
54
66
68
Page 4
Recovery of Symmetrical Peripheral Gangrene of Limbs in a
Patient After Performing Hemoadsorption in Septic Shock
1
Abstract
We report a 42-year-old patient who had Hodgkin lymphoma and developed bilateral symmetrical
peripheral gangrene (SPG) in the feet and hands, which occurred during septic shock after
autologous hematopoietic stem-cell transplantation. SPG is a rare but severe complication of
disseminated intravascular coagulation (DIC) and is frequently associated with sepsis. The
pathophysiology of SPG includes DIC-mediated intravascular thrombosis and thrombotic
occlusion of microcirculation, resulting in low blood flow. Sepsis-induced hypotension has been
suspected as one of the other causes of SPG, and it is thought to be aggravated by vasopressor
treatments given for hypotension. Our patient first experienced coldness, paleness, and cyanosis in
his body's acral parts, and then SPG later developed in both his feet and hands. Septic shock
management was performed with cytokine hemoadsorption, broad-spectrum antibiotics, and
massive fluid replacement rapidly. The patient fully recovered without the need for amputation.
Hemoadsorption is an extracorporeal cytokine-adsorption method for removing excess cytokines.
Prompt management of septic shock and early monitoring of peripheral ischemia are essential to
avoid SPG.
K E Y W O R D S
DIC, extracorporeal blood purification, hemoadsorption, sepsis, septic shock, symmetrical
peripheral gangrene
1 | INTRODUCTION
Symmetrical peripheral gangrene (SPG) is a rare but serious complication that involves bilateral
ischemic damage in the distal parts of the limbs in the absence of a major vascular occlusive
disease. The risk of mortality is high (up to 40%), and almost half of the survivors need
amputation.1 SPG is observed as a complication of disseminated intravascular coagulation (DIC)
in 85% of SPG cases.
Bahar Uncu Ulu1 | Tugçe Nur Yi geno glu 1 | Tuba Hacıbekiroglu2 |
Dursun Ali Saglam 3 | Ali Kılınç4 | Güls¸en Iskender 5 | Merih Kızıl Çakar1 |
Mehmet Sinan Dal1 | Fevzi Altuntas1
1Department of Hematology and Bone Marrow Transplantation Center, Ankara, Dr. Abdurrahman
Yurtaslan Oncology Training and Research Hospital, University of Health Sciences, Ankara, Turkey2Department of Hematology, Sakarya University Hospital, Sakarya, Turkey3Department of Intensive Care Unit, Ankara Dr. Abdurrahman Yurtaslan Oncology Training and Research
Hospital, University of Health Sciences, Ankara, Turkey4Apheresis Center, Ankara Dr. Abdurrahman Yurtaslan Oncology Training and Research Hospital,
University of Health Sciences, Ankara, Turkey5Department of Infectious Diseases, Ankara Dr. Abdurrahman Yurtaslan Oncology Training and Research
Hospital, University of Health Sciences, Ankara, Turkey
* Correspondence: Bahar Uncu Ulu, Department of Hematology and Bone Marrow Transplantation Center,
Ankara, Dr. Abdurrahman Yurtaslan Oncology Training and Research Hospital, University of Health
Sciences, 06200, Yenimahalle, Ankara, Turkey. Email: [email protected] .
01
Page 5
2
DIC is commonly associated with septicemia, and DIC-induced intravascular thrombosis causes
low blood flow and infarction of the skin and distal extremities.2-4
The use of vasopressors leads to spasm of the capillaries and impairment of microcirculation.4
Coldness, paleness, and cyanosis are the first signs of the SPG observed in the body's acral parts
and rapidly proceed to proximal areas.5-7 Currently, there is no specific treatment for SPG, and the
treatment priorities are usually the underlying condition and DIC.8 As sepsis is one of the leading
causes of DIC and SPG, there has been increasing interest in the use of extracorporeal devices for
the removal of pathogenic components observed during sepsis. Hemoadsorption (HA) is a method
of extracorporeal blood purification through a cartridge, where solutes are removed by direct
binding to the sorbent material.9-10 This case report presents a patient with Hodgkin Lymphoma
(HL) who developed SPG following septic shock. The patient fully recovered without amputation
in the follow-up.
2 | CASE PRESENTATION
A 42-year-old male patient with HL was admitted to the intensive care unit (ICU) for septic
shock on the 13th day after autologous hematopoietic stem-cell transplantation (ASCT). He was
neutropenic and thrombocytopenic when the first fever occurred. Cefoperazone sulbactam was
started. On the second day of febrile neutropenia, the patient progressed to sepsis, after which
meropenem, vancomycin, liposomal amphotericin B, and colistin were administered. The patient
needed nasal oxygen support because of hypoxia and was admitted to the ICU.
Despite extensive fluid replacement, the patient needed high doses of vasopressors to maintain
normotension. Even with infusion of noradrenaline at 3 μg/kg/min, his blood pressure remained
consistently low (80/40 mmHg). On the third day of febrile neutropenia, coldness, paleness, and
cyanosis started in the acral parts of the body and progressed to SPG in the feet and hands. The
patient had a score of 6 on the DIC scale of the International Society of Thrombosis and
Hemostasis (ISTH).11
Sepsis HA was started rapidly during the first hours in the ICU. The procedure was performed
using a hemoperfusion machine. One disposable hemoperfusion cartridge (HA330 resin, Styrene
divinylbenzene copolymers, Jafron Biomedical Co., Ltd., China) was used per day. The blood flow
rate was maintained at 200 mL/min. Each procedure continued for 150 minutes, and approximately
six total blood volumes were processed. Three absorbers were used over 3 days. The patient did
not receive any plasma components.
Due to thrombocytopenia, we did not administer routine systemic anticoagulation except for
priming the adsorption set. Then, 7500 IU of unfractionated heparin was used only for rinsing the
adsorption set to prevent clotting in the extracorporeal circuit. The changes of the patient's blood
parameters before and after HA are given in Figure 1. No microorganisms could be grown in
microbial cultures. The patient continued extended-spectrum antibiotics for empirical treatment.
By the third day of HA, the vasopressors were discontinued.
The progression of gangrene stopped with the withdrawal of vasopressors. Small blisters were
noticed in both feet over the next 10 days (Figures 2 and 3). SPG in both feet and hands started to
recover, and the patient was discharged from the hospital 38 days after ASCT. Three months after
autologous transplantation, the patient was in complete remission, and his bilateral distal
extremities fully recovered. His last follow-up was at 15 months after ASCT, and he was in
complete remission. The last view of his extremities is shown in Figure 4.
3 | DISCUSSION
We have reported a case of neutropenic fever with septic shock developing after ASCT. The
patient had SPG due to septicemia-associated DIC. We rapidly administered broad-spectrum
Page 6
3
antibiotics, massive fluid replacement, and vasopressor treatment. When we observed ischemic
lesions in his feet and hands, we increased supportive care by sepsis HA. The patient had such a
very impressive response the modalities that we stopped the vasopressor treatment afterward. HA
may contribute to decreasing cytokines and alleviate the septicemia associated with DIC.
The etiology of SPG is multifactorial, but septic shock and DIC are the leading causes.8,12-15
Sepsis is currently defined as a dysregulated host immune response to infection leading to organ
failure.16-18 The underlying pathophysiology is complex with both pathogenic and host factors.
Pathogen-associated molecular patterns and damage-associated molecular patterns play a
significant role in activating the endothelium and as a result inflammatory cytokines.19 The
activated endothelium becomes prothrombotic through increases in the expression of tissue factor
in the endothelium and monocytes.12,18 DIC develops in cases of impaired balance of anti- and
procoagulant factors. Early findings of septicemia-associated DIC include apparent coldness,
pallor, and pain. The ischemic lesions are often demarcated sharply and symmetric with initial
gray, blue, or purple discoloration that progresses to black as the skin undergoes necrosis.12,18
With more understanding about the pathophysiology of immune system factors in sepsis, interest
has been increasing in the use of extracorporeal devices for cytokine adsorption. It has been
hypothesized that a cytokine storm may be responsible for the self-destruction in sepsis, so the
removal of circulating cytokines is a sensible treatment option. The peak-concentration hypothesis
was first introduced with acute kidney injury and was subsequently generalized to sepsis more than
10 years ago.20 Since that time, it has been repeatedly hypothesized that there is a therapeutic
benefit of extracorporeal blood purification modalities, including forms of dialysis or therapeutic
apheresis regarding the cytokine storm.19-20
FIGURE 1 Changes of patient's blood parameters before and after hemoadsorption.
Abbreviations; HA: Hemoadsorption, CRP: C reactive protein, PT: prothrombin time,
LDH: lactate dehydrogenase
Page 7
4
HA330 (Jafron, Zhuhai City, China) is the one of the widely used adsorption cartridges in
China.9,10 Huang et al conducted small randomized controlled trials (RCTs) of adjuvant HA330
HA with 44 septic patients who had acute lung injury (ALI) in the ICU.21 Significant
reductions of IL-8 and IL-6 levels and length of stay was seen in patients when HA was performed
compared to standard therapy (defined as full intensive care management, including fluid
resuscitation, vasopressors, antimicrobial therapy, and ventilatory support). Nevertheless, length of
hospital stays and 28-day mortality did not differ between the two groups at day 3.21
In a later study by Huang et al, HA was compared to standard therapy in 46 patients with ALI
induced by extra-pulmonary sepsis.22 The HA group showed a significant reduction in IL-1 and
tumor necrosis factor-α in the broncho-alveolar lavage and plasma. Therefore, the improvement of
patients' hemodynamics was better, and the rate of mortality in the ICU and 28-day mortality were
lower in the HA group.22 But there is still no proof from a prospective RCT for any extracorporeal
treatment modality decreasing mortality in sepsis. Regarding sepsis, only therapeutic plasma
exchange appears to be potentially effective, but no recommendations have been made in the latest
international guidelines.18,23
An equivalent of HA330 is the extracorporeal wholeblood cytokine adsorber, which is currently
approved in the European Union.24 According to data from an international registry, whole-blood
cytokine adsorber therapy reduced IL-6 levels in 68% of patients with sepsis. No significant
decrease in organ failure was observed, but mortality was lower than predicted.25 A recent
prospective, randomized, pilot trial investigated the effects of early (<24 hours) extracorporeal
cytokine removal performed in 20 patients with septic shock. The results indicated a decrease in
norepinephrine requirements, an improvement in hemodynamics, and significantly lower levels of
procalcitonin and endothelin-1 precursor compared to controls.26 Despite showing a significant
reduction in circulating cytokine levels and improvement in clinical situations, there is a lack of
evidence, and it is not currently recommended by guidelines. Large prospective randomized trials
with carefully selected patient populations are needed to evaluate the efficacy of extracorporeal
HA.
The patient in the present case report had septic shock at 13 days after ASCT. In this case, early
management of septic shock with massive fluid replacement, antibiotics, and especially the
administration of sepsis HA within <24 hours might have prevented amputation from being
required. To the best of our knowledge, this is the first case report of successful HA in a patient
with SPG.
4 | CONCLUSIONS
In conclusion, early recognition and prompt management of septic shock are necessary to avoid
SPG. Vasopressors might exacerbate SPG, so clinicians should be careful, especially in the
presence of any sign of hypoperfusion in the extremities. Performing sepsis HA immediately may
be a good adjuvant option for the treatment of septic shock while avoiding destructive effects of
the cytokine storm and DIC, as in our patient. Nevertheless, RCTs are needed to prove this
hypothesized preventive effect.
ACKNOWLEDGMENTS
We would like to thank all staff and the nurses of the intensive care unit, stem cell transplantation
unit, and apheresis unit for their devoted work.
CONFLICT OF INTEREST
The authors declared no potential conflicts of interest with respect to the research, authorship,
and/or publication of this article.
Page 8
5
DATAAVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon
reasonable request.
ORCID
Bahar Uncu Ulu https://orcid.org/0000-0002-6230-9519 Tugçe Nur Yigenoglu
https://orcid.org/0000-0001-9962-8882
Page 9
6
REFERENCES
1.Sharma BD, Kabra SR, Gupta B. Symmetrical peripheral gangrene. Trop Doct. 2004;34(1):2-4.
2.Goodwin JN. Symmetrical peripheral gangrene. Arch Surg.
1974;108(6):780-784.
3.Molos MA, Hall JC. Symmetrical peripheral gangrene and disseminated intravascular
coagulation. Arch Dermatol. 1985;121 (8):1057-1061.
4.Joynt G, Doedens L, Lipman J, Bothma P. High-dose adrenaline with low systemic vascular
resistance and symmetrical peripheral gangrene. S Afr J Surg. 1996;34(2):99-101.
5.Ghosh SK, Bandyopadhyay D, Ghosh A. Symmetrical peripheral gangrene: a prospective study
of 14 consecutive cases in a tertiary-care hospital in eastern India. J Eur Acad Dermatol Venereol.
2010;24(2):214-218.
6.Applebaum RM, Kronzon I. Evaluation and management of cholesterol embolization and the
blue toe syndrome. Curr Opin Cardiol. 1996;11(5):533-542.
7.Parmar MS. Symmetrical peripheral gangrene: a rare but dreadful complication of sepsis. CMAJ.
2002;167(9):1037-1038.
8.Tsuji Y, Hiroto T, Kitano I, Tahara S, Sugiyama D. Importance of skin perfusion pressure in
treatment of critical limb ischemia. Wounds. 2008;20(4):95-100.
9.Honoré PM, De Bels D, Barreto Gutierrez L, Spapen HD. Hemoadsorption therapy in the
critically ill: solid base but clinical haze. Ann Intensive Care. 2019;9(1):22.
10. Ankawi G, Fan W, Pomarè Montin D, et al. A new series of sorbent devices for multiple
clinical purposes: current evidence and future directions. Blood Purif. 2019;47(1-3):94-100.
11.Toh CH, Hoots WK. SSC on disseminated intravascular coagulation of the ISTH. The scoring
system of the scientific and standardisation committee on disseminated intravascular coagulation
of the international society on thrombosis and haemostasis: a 5-year overview. J Thromb Haemost.
2007;5(3):604-606.
12.Ennis J, Ahmed O, Khalid M, Boland PA, Allen M. Meningococcal sepsis complicated by
symmetrical peripheral gangrene: a case report. Cureus. 2020;12(7):e9470. https://doi.org/10.7759/
cureus.9470.
13.Warkentin TE. Ischemic limb gangrene with pulses. N Engl J Med. 2015;373(7):642-655.
14. Foead AI, Mathialagan A, Varadarajan R, Larvin M. Management of symmetrical peripheral
gangrene. Indian J Crit Care Med. 2018;22(12):870-874.
15. Shenoy R, Agarwal N, Goneppanavar U, Shenoy A, Sharma A. Symmetrical peripheral
gangrene—a case report and brief review. Indian J Surg. 2013;75(Suppl 1):163-165.
16. Perner A, Gordon AC, De Backer D, et al. Sepsis: frontiers in diagnosis, resuscitation and
antibiotic therapy. Intensive Care Med. 2016;42(12):1958-1969.
17. Schefold JC, von Haehling S, Corsepius M, et al. A novel selective extracorporeal intervention
in sepsis: immunoadsorption of endotoxin, interleukin 6, and complement-activating product 5a.
Shock. 2007;28(4):418-425.
18.Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for
sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801-810.
19. Fajgenbaum DC, June CH. Cytokine Storm. N Engl J Med. 2020;383(23):2255-2273.
20.Ronco C, Kellum JA, Bellomo R, House AA. Potential interventions in sepsis-related acute
kidney injury. CJASN. 2008;3(2): 531-544.
21. Huang Z, Wang SR, Su W, Liu JY. Removal of humoral mediators and the effect on the
survival of septic patients by hemoperfusion with neutral microporous resin column. Ther Apher
Dial.
22.Huang Z, Wang SR, Yang ZL, Liu JY. Effect on extrapulmonary sepsis-induced acute lung
injury by hemoperfusion with neutral microporous resin column. Ther Apher Dial. 2013;17:454-
461.
Page 10
7
23.Padmanabhan A, Connelly-Smith L, Aqui N, et al. Guidelines on the use of therapeutic
apheresis in clinical practice – evidence-based approach from the writing Committee of the
American Society for apheresis: the eighth special issue. J Clin Apher. 2019;34:171-354.
24.Morris C, Gray L, Giovannelli M. Early report: the use of Cytosorb™ haemabsorption column
as an adjunct in managing severe sepsis: initial experiences, review, and recommendations. J
Intensive Care Soc. 2015;16(3):257-264.
25. Friesecke S, Träger K, Schittek GA, et al. International registry on the use of the CytoSorb®
adsorber in ICU patients: study protocol and preliminary results. Med Klin Intensivmed
Notfmed. 2019;114(8):699-707. English.
26. Hawchar F, László I, Öveges N, Trásy D, Ondrik Z, Molnar Z. Extracorporeal cytokine
adsorption in septic shock: a proof of concept randomized, controlled pilot study. J Crit Care.
2019;49:172-178.
How to cite this article:
Uncu Ulu B, Yigenoglu TN,Hacıbekiroglu T, et al. Recovery of Symmetrical Peripheral Gangrene
of Limbs in a Patient After Performing Hemoadsorption in Septic Shock. J Clin Apher. 2021;1–5.
https://doi.org/10.1002/jca.21893
Page 11
Subarachnoid Hemorrhage and Extracorporeal Blood
Purification with HA-380 and High-Volume Hemofiltration: A
New Therapeutic Challenge at the Neurocritical Care Unit? A
Case Report
8
Keywords
Subarachnoid hemorrhage · Interleukin-6 · Hemadsorption
Abstract
We present the case of a patient with subarachnoid hemorrhage (SAH) secondary to a ruptured
cerebral aneurysm and a refractory shock with high doses of vasopressors without a proven source
of infection. This patient received therapy with high-volume hemofiltration plus adsorption,
resolving the hemodynamic deterioration and with good neurological evolution. Our clinical case
proposes that extracorporeal therapies may have a feasibility role in the management of
complications of SAH. © 2021 S. Karger AG, Basel
Introduction
Neurocritical pathologies such as subarachnoid hemorrhage (SAH) have shown a correlation
between levels of cytokines and their outcomes [1]. Early elevation of cytokines at the central and
peripheral levels, mainly interleukin-6 (IL-6), with a first peak at 24–48 h after the event, along
with other inflammatory events such as neutrophil activation, is associated with neurological
deterioration and development of delayed cerebral ischemia [1– 3]. Furthermore, severe systemic
inflammatory states can lead to significant circulatory impairment with multiple organ failure and
death [4]. Our group proposes that the use of extracorporeal therapies for immunomodulation
could have a role in preventing complications in patients with SAH and significant elevation of
cytokines, improving neurological outcomes.
Case Presentation
A 57-year-old man with aneurysmal SAH of the right posterior communicating artery and
excluded with clipping was admitted to the critical care unit. Initial CT shows modified Fisher
scale IV and World Federation of Neurological Surgeons grading scale IV. On postoperative day 4,
fever, hypotension, and a rise of the inflammatory parameters began (Table 1) with a negative
microbiological study and normal chest radiography, highlighting an inflammatory cerebrospinal
fluid (CSF), without isolated microorganisms. Broad-spectrum antibiotics were started, but he
evolved with greater hemodynamic deterioration (norepinephrine 1.5 μg/kg/min and adrenaline 1
μg/kg/min), requiring a guided resuscitation with advanced hemodynamic monitoring (PiCCO),
not achieving adequate values (CI 4 L/min/m2, SVRI 850 dyn s/cm5/m2, and MAP <70 mm Hg),
Gonzalo Ramírez-Guerreroa,b Rocio Oliva Alarcóna Francisco Villagrán Cortésa,b Vicente Torres
Cifuentesa,b Romyna Baghetti Hernándeza Pablo Flores Fernandeza Cristian Godoy Telloa Francisco Torres
Moyanoc Cristian Lucero Córdovaa Simón Rojas Dolla Osvaldo Garay Colomaa
aCritical Care Unit, Carlos Van Buren Hospital, Valparaíso, Chile; bDialysis and Renal Trasplant Unit,
Carlos Van Buren Hospital, Valparaíso, Chile; cNeuroradiology Unit, Imagenology Service, Carlos Van
Buren Hospital, Valparaíso, Chile
02
Page 12
9
despite optimizing predictors of volume response and therefore suboptimal monitoring parameters,
highlighting a tissue oxygen pressure of 16 mm Hg and abnormal peripheral perfusion with
abnormal capillary refill time. A second microbiological study was negative. Due to
hyperinflammatory phenotype, blood purification therapy was considered.
A 12-h session of hemoperfusion (HP) pulse was performed (HA-380 cartridge, Jafron
Biomedical Co.) in combination with high-volume hemofiltration (HVHF) in a Prismaflex monitor
(Baxter) with blood flow 250 mL/min and effluent dose 70 mL/ kg/h, with prefilter replacement
and heparin. The HP cartridge was installed post filter. According to local protocol, in the second
and in the third day, only an 8-h isolated HVHF was performed, with same parameters.
Replacement solutions were adjusted according to the protocol for target natremia [5].
Page 13
10
A significant decrease in vasoactive drugs and improvement in inflammatory parameters were
achieved (Fig. 1). Brain CT showed no vasospasm or delayed cerebral ischemia. On postoperative
day 39, he was discharged from hospital without neurological sequelae.
Discussion and Conclusion
In SAH, neuroinflammation, evidenced by high levels of cytokines and a high lactate-pyruvate
ratio, correlates with delayed cerebral ischemia [6]. Loss of the bloodbrain barrier integrity and
break down products of hemoglobin activate cellular immunity, leading to the production of pro
inflammatory cytokines and adhesion molecules at the CSF and plasma levels [7–9].
Blood purification therapies are proposed in systemic inflammatory syndrome with refractory
shock [10]. We carried out HP using a macroporous resin sphere cartridge capable of adsorbing
interleukins through size sieving and hydrophobic interactions, and it was combined with HVHF to
enhance its effect [11–13]. Studies have shown that neutralization of peripheral IL-1 is associated
with better neurological outcomes [8].
Consequently, we proposed hemadsorption plus HVHF as rescue therapy for SAH with
refractory shock, achieving reduction of vasoactive drugs, plasma IL-6 from 34.4 to 4.8 pg/mL,
and CSF lactate levels, maintaining adequate cerebral perfusion parameters, without evidence of
delayed cerebral ischemia or cerebral infarction (Fig. 2).
Acknowledgements
The authors wish to thank the ICU staff at Carlos Van Buren Hospital.
Statement of Ethics
Biochemical and clinical parameters were collected under the approval of the scientific Ethics
Committee of the health service of Valparaiso – San Antonio. Written informed consent for
publication was authorized by the patient of this case report and for any accompanying images.
The consent document was authorized and reviewed by the local Ethics Committee.
Page 14
11
Conflict of Interest Statement
The authors report no conflicts of interest. The authors alone are responsible for the content and
writing of this article.
Funding Sources
There was no funding for the study.
Authors Contributions
G.R.G., R.O.A., and F.V.C. designed the work; G.R.G., R.O.A., and F.V.C. collected and
analyzed the data; G.R.G., R.O.A., R.B.H., V.T.C., F.V.C., F.T.M., S.R.D., C.G.T., P.F.F., and
O.G.C. drafted the work or substantively revised it; and all authors read and approved the final
manuscript.
Availability of Data and Materials
All data generated or analyzed during this study are included in this published article.
References
1.McMahon CJ, Hopkins S, Vail A, King AT, Smith D, Illingworth KJ, et al. Inflammation as a
predictor for delayed cerebral ischemia after aneurysmal subarachnoid haemorrhage. J Neurointerv
Surg. 2013;5(6): 512–7.
2.Savarraj JPJ, Parsha K, Hergenroeder GW, Zhu L, Bajgur SS, Ahn S, et al. Systematic model of
peripheral inflammation after subarachnoid hemorrhage. Neurology. 2017; 88(16):1535–45.
3.Mc Girt MJ, Mavropoulos JC, McGirt LY, Alexander MJ, Friedman AH, Laskowitz DT, et al.
Leukocytosis as an independent risk factor for cerebral vasospasm following aneurysmal
subarachnoid hemorrhage. J Neurosurg. 2003;98(6):1222–6.
4.Rimmelé T, Kellum JA. Clinical review: blood purification for sepsis. Crit Care. 2011;15(1):205.
5.Dangoisse C, Dickie H, Tovey L, Ostermann M. Correction of hyper- and hyponatraemia
during continuous renal replacement therapy. Nephron Clin Pract. 2014;128(3–4):394–8.
6.Sarrafzadeh A, Schlenk F, Gericke C, Vajkoczy P. Relevance of cerebral interleukin-6 after
aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2010;13(3):339–46. 7 Zhiyuan V, Kwok G.
Neuroinflammation responses after subarachnoid hemorrhage: a review. J Clin Neurosci.
2017;42:7–11.
8.Galea J, Ogungbenro K, Hulme S, Patel H, Scarth S, Hoadley M, et al. Reduction of
inflammation after administration of interleukin-1 receptor antagonist following aneurysmal
subarachnoid hemorrhage: results of the subcutaneous interleukin-1Ra in SAH (SCILSAH) study. J
Neurosurg. 2018;128(2):515–23.
9.Thornton P, Pinteaux E, Gibson RM, Allan SM, Rothwell NJ. Interleukin-1-induced
neurotoxicity is mediated by glia and requires caspase activation and free radical release. J
Neurochem. 2006;98(1):258–66.
10.Poli EC, Rimmelé T, Schneider AG. Hemoadsorption with CytoSorb®. Intensive Care Med.
2019;45(2):236–9.
11.Malard B, Lambert C, Kellum JA. In vitro comparison of the adsorption of inflammatory
mediators by blood purification devices. Intensive Care Med Exp. 2018;6(1):12.
12.Chu L, Li G, Yu Y, Bao X, Wei H, Hu M. Clinical effects of hemoperfusion combined with
pulse high-volume hemofiltration on septic shock. Medicine. 2020;99(9): e19058.
13.Sun S, He L, Bai M, Liu H, Li Y, Li L, et al. High-volume hemofiltration plus hemoperfusion
for hyperlipidemic severe acute pancreatitis: a controlled pilot study. Ann Saudi Med.
2015;35(5):352–8.
Page 15
Case Series: Efficacy and Safety of Hemoadsorption With HA-
330 Adsorber in Septic Pediatric Patients With Cancer
12
Background: Sepsis is a frequent cause of death in hospitalized patients and, in detail, in neonatal,
pediatric, and adult intensive care units (ICUs). Severe sepsis has a very poor prognosis. Indeed,
the mortality rate varies between 30 and 70% during the first 7–14 days. Despite a timely and
appropriate therapy, the prognosis of severe sepsis is too often negative. Therefore, new
therapeutic resources are under investigation in order to further improve prognosis.
Case series: Here, we reported three septic children in whom we used extracorporeal blood
purification therapy with hemoadsorption device HA330 (Jafron Biomedical Co., Ltd., China),
aiming to scavenge and eliminate bacterial toxins and inflammatory mediators from the blood.
Discussion and Conclusion: This small case series first showed that hemoperfusion with HA330
cartridge may be an effective and relatively safe adjunctive treatment to counterbalance the
cytokine storm in septic children with hematological disorders. Further studies are needed to
confirm and further support its safety and efficacy in a large number of pediatric patients.
Keywords: sepsis, pediatric cancer, blood purification, hemoadsorption, HA-330 adsorber
INTRODUCTION
Sepsis is a frequent cause of death in hospitalized patients and, in detail, in neonatal, pediatric, and
adult intensive care units (ICUs). According to WHO, almost 49 million people were hospitalized
with sepsis worldwide in 2017, and 11 million patients died; importantly, almost half of these
hospitalized patients were children under 5 years of age (1). According to a recent
systematicreview with meta-analysis, sepsis incidence and prevalence were estimated to be 48 per
Vitaliy Sazonov1,2*, Ramazan Abylkassov2,3, Zaure Tobylbayeva2, Askhat Saparov2, Olga Mironova2 and
Dimitri Poddighe3,4
1Department of Biomedical Sciences, Nazarbayev University School of Medicine, Nur-Sultan, Kazakhstan,2Pediatric Anesthesiology and Intensive Care Unit, National Research Center for Maternal and Child
Health, “University Medical Center”, Nur-Sultan, Kazakhstan, 3Department of Medicine, Nazarbayev
University School of Medicine, Nur-Sultan, Kazakhstan, 4Department of Pediatrics, National Research
Center for Maternal and Child Health, “University Medical Center”, Nur-Sultan, Kazakhstan
Edited by: Julie Fitzgerald, Children’s Hospital of Philadelphia, United States
Reviewed by: E. Scott Halstead, Pennsylvania State University (PSU), United States Andrea Moscatelli,
Giannina Gaslini Institute (IRCCS), Italy
*Correspondence: Vitaliy Sazonov [email protected]
Specialty section: This article was submitted to Pediatric Critical Care, a section of the journal Frontiers in
Pediatrics
Received: 25 February 2021, Accepted: 19 April 2021, Published: 11 June 2021
Citation: Sazonov V, Abylkassov R, Tobylbayeva Z, Saparov A, Mironova O and Poddighe D (2021) Case
Series: Efficacy and Safety of Hemoadsorption With HA-330 Adsorber in Septic Pediatric Patients With
Cancer. Front. Pediatr. 9:672260.
doi: 10.3389/fped.2021.672260
03
Page 16
13
100,000 persons-year and 22 per 100,000 people, respectively (2).
Sepsis can lead to life-threatening multiple organ dysfunction due to a dysregulated immunologic
and metabolic host response to an infection (3). In pathophysiological terms, sepsis can be defined
as a dysregulated systemic inflammatory response syndrome (SIRS) associated with an infection
(usually bacterial). Clinically, SIRS is diagnosed by the presence of at least two of the following
criteria (including one of the first two, mandatorily): abnormal temperature (>38.5 or <36◦C),
abnormal leukocyte count (leukocytosis or leukopenia for age-appropriate reference values),
tachycardia [>2 standard deviations (SDs) above the normal age-related values], tachypnea (>2 SD
above the normal age-related values). In severe sepsis, children develop cardiovascular (systolic
blood pressure <-2 SD for age and need for vasoactive drug, which correspond to the definition of
septic shock) or respiratory (PaO2/FiO2 <300 with need for mechanical ventilatory support)
insufficiency, along with multiple organ dysfunction. Severe sepsis has a very poor prognosis.
Indeed, the mortality rate varies between 30 and 70% during the first 7–14 days (4, 5).
The pathophysiological mechanisms of sepsis are very complex and have not been completely
elucidated yet. Once the causing pathogen enters the bloodstream, if it cannot be
appropriately and timely cleared for several and variable reasons, bacterial toxins may lead to the
uncontrolled production of a cascade of pro-inflammatory cytokines [including interleukin
(IL)-1β, IL-6, IL-12, tumor necrosis factor (TNF)-α)] (6, 7). This “cytokine storm” progressively
damages several tissues and organs and, importantly, creates an “endothelial dysfunction,”
which alters the balance between the coagulation process and fibrinolysis, and finally results in the
aggravation of tissue hypoperfusion, leading to an irreversible and multiple organ dysfunction (6).
Indeed, septic patients are often affected by underlying diseases that cause host immunodepression.
For instance, sepsis can complicate the clinical picture of patients affected with hematological
malignancies, as it is in our case series.
In general, the mainstay of sepsis treatment in children consists of antibiotic and supportive
therapies (including intravenous fluid replacement, mechanical ventilation, cardiotonic drugs, etc.).
Unfortunately, the prognosis of severe sepsis is too often negative, despite a timely and appropriate
therapy, as previously mentioned. Therefore, new therapeutic resources are under investigation in
order to further improve prognosis. Here, we reported three septic children in whom we used
extracorporeal blood purification therapy with hemoadsorption device HA330 (Jafron Biomedical
Co., Ltd., China), aiming to scavenge and eliminate bacterial toxins and inflammatory mediators
from the blood.
CLINICAL CASES
Patient 1
A 6-month-old girl was previously diagnosed with pure red cell aplasia. She developed fever,
anuria, and progressive skin necrosis on the abdominal wall and buttock areas. Based on clinical
(persistent hyperthermia, hypotension, oliguria), laboratory (leukocytosis and elevated
inflammatory parameters), and microbiological (blood cultures positive for Staphylococcus
epidermidis) findings, this patient was diagnosed with sepsis and transferred to the pediatric
intensive care unit (PICU). Despite the antibiotic therapy (meropenem, amikacin, metronidazole)
and the supportive therapy, her clinical conditions gradually worsened and, on day 10 after the
PICU admission, the patient also needed respiratory support [non-invasive ventilation (NIV)]
and showed a drastic increase of plasmatic urea/creatinine and all the inflammatory markers.
Therefore, this clinical condition of acute kidney injury led to the initiation of pediatric continuous
venovenous hemodiafiltration (CVVHDF) with the “Prismaflex” device (Baxter, US) (with the
following prescription parameters: flow rate, 50 ml/min; both pre-dilution and post-dilution, -150
ml/h; ultrafiltration, 20 ml/h; prolonged heparinization, 5–30 IU/kg/h; effluent, 600 ml/h; dialysate
fluid, 300 ml/h) by using disposable hemoperfusion cartridge HA 330 (Jafron Biomedical Co.,
Page 17
14
Ltd., China) for 4 h. An appropriate (for child’s size) hemodialysis catheter was inserted into the
right subclavian vein. Normal saline was used for the priming of the circuit and system testing;
before connecting the device to the patient, normal saline was replaced with red blood cell
suspension.
After this first session of CVVHDF, all renal and inflammatory parameters rapidly improved, as
summarized in Table 1. Importantly, the patient was also able to wean from the ventilatory support,
and the FiO2 decreased from 60 to 30%; moreover, catecholamines were gradually discontinued.
However, 5 days after the above treatment (day 15), the patient’s clinical condition worsened
again. Therefore, a second session of CVVHDF with HA-330 was performed, which resulted in
similar improvements as reported in the previous episode (as shown in Table 1). No further
CVVHF sessions were required, and the patient was discharged from the PICU 2 weeks later (day
29).
Patient 2
A 14-year-old boy diagnosed with drug-resistant and relapsed acute lymphoblastic leukemia (ALL)
was admitted for chemotherapy according to FLAG-IDA protocol (fludarabine, cytarabine,
idarubicin) (8). On the eighth day after completing the chemotherapy, the patient developed sepsis
sustained by (extended-spectrum β lactamase-producing) Escherichia coli. Because of the
development of multiorgan failure (including anuria and respiratory failure), he was transferred to
the PICU.
Despite the antibacterial treatment (trimethoprim/sulfamethoxazole, piperacillin tazobactam,
and amikacin), the patient showed no improvement. Due to persistent fever (associated with high
and increasing values of the inflammatory markers) and constantly high levels of plasmatic urea
along with anuria (despite the high dose of furosemide, 3 mg/kg/day) on day 7 from PICU
admission, he underwent CVVHDF (with the following prescription parameters: flow rate, 120
ml/min; both pre-dilution and post-dilution, -800 ml/h; ultrafiltration, 60 ml/h; prolonged
heparinization, 5–30 IU/kg/h; effluent, 3,200 ml/h; dialysate fluid, 1,600 ml/h) with HA 330
cartridge for 4 h. At the end of this procedure (as summarized in Table 2), this patient’s
inflammatory and renal parameters significantly improved, as well as his respiratory function.
Interestingly, all the inflammatory markers decreased, except for S100 protein. The patient was
weaned from mechanical ventilation on day 9 and achieved hemodynamic stability without any
catecholamines on day 10. He was discharged from the PICU on day 12.
Patient 3
A 2.5-year-old girl diagnosed with ALL was admitted for chemotherapy with high-dose
methotrexate according to ALL BFM IC 2002 Block HR1 protocol (9). After the 24-h high-dose
methotrexate infusion (HD-MTX), she developed severe toxic mucositis, epidermolysis, and
hepatitis.
Therefore, this patient was transferred to the PICU. On day 4, she developed sepsis
characterized by acute kidney injury and bilateral pneumonia, even though no clear
microbiological agents were identified. Indeed, the blood culture samples were obtained during
antibiotic therapy. The diagnosis of sepsis was made on the basis of the clinical picture and a high
level of procalcitonin (848 ng/L). Despite the antibacterial treatment with cefixime and amikacin,
no improvement was noticed, and the patient required respiratory support with mechanical
ventilation [synchronized intermittent mandatory ventilation with adaptive pressure ventilation
(APVSIMV) mode]. Thus, the patient underwent CVVHDF (with the following prescription
parameters: flow rate, 80 ml/min; both pre-dilution and post-dilution, -500 ml/h; ultrafiltration, 100
ml/h; prolonged heparinization, 5–30 IU/kg/h; effluent, 2,000 ml/h; dialysate fluid, 1,000 ml/h)
with HA-330 cartridge for 4 h on day 7. After the procedure, the patient’s general condition and
Page 18
15
laboratory parameters (Table 3) improved significantly. Importantly, the respiratory support was
switched to synchronized intermittent mandatory ventilation (SIMV), and her dopamine
requirement decreased twice compared to the previous days. In addition, there was good clinical
dynamics and healing of necrotic skin sites.
Unfortunately, despite such a positive response to CVVHDF procedure, the patient had a fatal
outcome on day 28 (namely, 21 days after the CVVHDF session) because of the underlying
hematologic malignancy, which became drug resistant.
Page 19
16
DISCUSSION
Sepsis is a frequent cause of PICU admission and mortality for children affected with leukemia
and, in general, severe hematologic diseases (10, 11). In detail, Aljabari et al. (12) still reported
high rates of morbidity and mortality among this group of patients despite the improvements in
supportive care and microbiological treatment: 8% of children develop severe sepsis requiring
treatment in the PICU, and 34% of them die or develop multiple organ dysfunction syndrome.
Therefore, additional strategies against sepsis should be sought. One of these therapeutic resources
is CVVHDF through disposable hemoperfusion cartridge HA 330.
There are different techniques for extracorporeal blood purification used during a cytokine
storm, such as highvolume hemofiltration (HVHF), plasma exchange (PE), high-cut-off (HCO)
membrane, hemoadsorption (with filters and adsorption columns, including selective polymyxin B,
Page 20
17
nonselective CytoSorb, HA, etc.). To date, several papers on the use of HVHF in children with
sepsis have been published; some authors concluded that such a procedure can improve the
outcome of sepsis (13). Actually, Miao et al. (14) reported no significant difference on 28-day
mortality, improvement of hemodynamic profile, and clearing of inflammatory factors in critically
ill pediatric patients with severe sepsis when using HVHF compared to the standard-volume
continuous venovenous hemofiltration (14). Moreover, other authors were against HVHF over
standard hemofiltration in children with septic shock or sepsis-associated organ dysfunction (15).
PE can potentially improve organ function in septic patients; however, a multicenter retrospective
study including patients younger than 18 years did not show any decrease in mortality in both
patients with continuous renal replacement therapy and PE usage (16). Additionally, PE can lead to
a deficiency of coagulation factors and hypoalbuminemia, in addition to further risk of infections.
Regarding HCO, the review by Ankawi et al. (17) concluded that there is no evidence to support its
use in sepsis, although a study in adults suggested a decrease in inflammatory cytokines and
improvement of hemodynamics (18).
HA330 is characterized by a hemoperfusion cartridge with an electrically porous resin used
specifically to remove cytokines, complements, and other endotoxins with molecular weight of
10–60 kDa. It is used primarily during acute and severe clinical conditions associated with a
cytokine storm, as it can occur during sepsis (19). This cartridge was also effective in the treatment
of hepatitis (decreased levels of IL-8, ammonia, bilirubin) and pancreatitis (decreased level of
lipids and amylase) (19). Conversely, the Prismaflex hemofilter used for CVVHDF eliminates low-
and medium-molecular weight compounds and only partially eliminates beta 2-microglobulinin
(12 kDa), TNF- α (17 kDa), IL-6 (26 kDa), and IL-10 (30 kDa) (20). For this reason, a CVVHDF
session alone is not usually effective to eliminate these inflammatory mediators. Therefore, the
appropriate selection of cartridges can play a significant role in the treatment of specific clinical
conditions. For example, the elimination of endotoxins is best carried out by selective polymyxin
B, rather than a non-selective cartridge, because their molecular weight cutoff point is higher than
the non-selective (∼100 vs. ∼60 kDa, respectively) (21). HA330 and CytoSorb are very similar
cartridges functionally; however, CytoSorb is the only approved extracorporeal technique in
European Union, whereas HA330 is mainly used in China (21).
Our previous experience with CytoSorb showed a 32% reduction rate of IL-6 (22). Here, HA330
appeared to be more effective in eliminating IL-6 from the bloodstream compared
to CytoSorb. The issue of the effectiveness of Cytosorb in reducing the plasmatic levels of
inflammatory cytokines remains controversial based on the available publications. According
to Schadler et al. (23), CytoSorb did not reach a statistically significant decrease in IL-6 blood
levels when compared to the control group with no hemoperfusion. Conversely, a recent study
done by Bottari et al. (24) showed a significant reduction of Il-6 and IL-10 by using Cytosorb with
continuous renal replacement therapy as blood purification strategy in pediatric septic shock.
To date, hemoadsorption using the HA-330 cartridge has been well-studied in adult patients with
inflammatory conditions such as sepsis, acute lung injury, hepatitis, and pancreatitis (19).
In these clinical settings, a marked reduction of inflammatory mediators, noticeable clinical
improvement, and, importantly, no significant side effects were reported (19). Moreover, several
reports suggested some benefits from this procedure even in patients affected with septic shock
(17, 25–27). However, large clinical studies on the use of extracorporeal methods in pediatric
sepsis are currently missing (17). Therefore, the indication and choice of specific extracorporeal
methods, such as hemofiltration or hemoadsorbtion, in septic patients can be based on the clinical
assessment of individual clinical cases.
To our knowledge, here we reported the first small case series of septic children treated with
CVVHDF by using HA330 cartridge. In all our three cases, we noted a combination of acute
kidney injury (combined with or without multiple organ failure), which was the reason for
Page 21
18
initiating the pediatric CVVHDF by using the Prismaflex hemofiltration system and poly
membrane (AN69) filters. The HA-330 adsorber was installed after the hemofilter. Heparin
titration rate was corrected on the basis of the activated partial thromboplastin time and maintained
at 60–80 seconds. In all these cases, normal saline was used for the priming of the circuit and
system testing; however, in two cases (Patient 1 and Patient 3), before connecting the device to the
patient, normal saline was replaced with red blood cell suspension. Before the procedure, double-
lumen central venous catheters were percutaneously placed to the right subclavian vein under
sedation and analgesia; the correct location was confirmed by chest X-ray.
The response to the treatment was positive in all three cases based on inflammatory markers (as
summarized in Table 4) and clinical improvements (including the weaning from the ventilatory
support and vasoactive drugs). Despite the small number of procedures performed (n = 4, in one
patient, the procedure was performed twice), we noted a remarkable decrease in all the
inflammatory markers. In all these patients, the antibiotic therapy alone did not seem to be enough,
but the CVVHDF with disposable hemoperfusion cartridge HA 330 administered in 4-h sessions
apparently rescued— or contributed to rescue at least—the clinical situation: they experienced a
stabilization of hemodynamics with half of the pretreatment dosage to none at all. As for the lung
function, after hemoperfusion, these patients required much milder regimens of mechanical
ventilation to none at all, and their blood gas values returned to age-appropriate normal ranges. As
recommended by the Pediatric Acute Lung Injury Consensus Conference Group, the improvement
of the respiratory failure was described by showing the variations in time of the S/F ratio or
oxygen saturation index (28). Moreover, all children also showed remarkable improvement of
diuresis and kidney function tests, as well as a decrease of transaminases, if altered.
Sepsis mortality is greatly affected by the development of multiorgan (cardiovascular,
pulmonary, renal, etc.) failure during its clinical course (2). Moreover, patients with leukemia and
sepsis showed much higher mortality rates than other general (non-hematologic) PICU patients
(11). Early empiric antibiotic treatment and life-supportive therapies are crucial for the successful
management of septic children (29). However, adjunctive therapies, like hemoperfusion, may
greatly increase the survival rate. A randomized controlled trial by Huang et al. (25) showed a
significant decrease in ICU and hospital mortality among a group of septic patients who underwent
hemoperfusion with HA330 compared to that of the control group receiving standard treatment
(12.5 vs. 45.0% and 37.5 vs. 50.0%, respectively) (25). This approach can effectively counteract
the cytokine storm that characterizes sepsis as an additional therapeutic tool to the “conventional”
immune-modulatory therapies (25, 30). In our small case series, extracorporeal purification
methods seem to represent a promising adjunctive therapy for severe sepsis in children. However,
this is currently the only experience with HA330-related blood purification in septic children.
Therefore, additional and independent reports and, possibly, clinical studies are needed to make
final conclusions on the effectiveness and safety of this procedure in children with hematological
diseases and malignancies. Indeed, the typical complications of extracorporeal methods (e.g.,
catheter bleeding and infection, heparinization side effects, decreased platelets, etc.) can be
encountered, but the shorter procedure time required by HA330-related blood purification can
reduce these risks.
CONCLUSION
This small case series first suggested that the hemoperfusion with HA330 cartridge may be an
effective and relatively safe adjunctive treatment to counterbalance the cytokine storm in septic
children affected with hematological disorders. However, further clinical studies are needed to
support our first and preliminary experience.
Page 22
19
DATAAVAILABILITY STATEMENT
The original contributions presented in the study are included in the article/supplementary
material, further inquiries can be directed to the corresponding author/s.
ETHICS STATEMENT
Ethical review and approval was not required for the study on human participants in accordance
with the local legislationand institutional requirements. This case series complies with the
guidelines for human studies, and the research was conducted ethically in accordance with the
World Medical Association Declaration of Helsinki. Written informed consent was obtained from
the patients’ parents. The report is fully anonymized.
AUTHOR CONTRIBUTIONS
VS contributed to the literature search, collecting of data, and writing and editing of the
manuscript. RA contributed to the literature search, collecting of data, and drafting of the
manuscript. ZT participated in patient care and collecting of data. AS and OM contributed to
collecting of data. DP contributed to writing the draft and critically revised the manuscript. All
authors reviewed the draft, modified it accordingly, and approved the final version.
FUNDING
The article publication charge was supported by Nazarbayev University School of Medicine.
ACKNOWLEDGMENTS
The authors express their special gratitude to all those involved in the treatment and care of the
patients in this difficult time: parents, doctors, nurses, and clinic staff.
REFERENCES
1. Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al. Global,
regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global
Burden of Disease Study. Lancet. (2020) 395:200–11. doi: 10.1016/S0140-6736(19)32989-7
2. Fleischmann-Struzek C, Goldfarb DM, Schlattmann P, Schlapbach LJ, Reinhart K, Kissoon N.
The global burden of paediatric and neonatal sepsis: a systematic review. Lancet Respir Med.
(2018) 6:223–30. doi: 10.1016/S2213-2600(18) 30063-8
3. Matot I, Sprung CL. Definition of sepsis. Intens Care Med. (2001) 27(Suppl. 1):S3–9. doi:
10.1007/PL00003795
4. Studnek JR, Artho MR, Garner CL, Jr, Jones AE. The impact of emergency medical services on
the ED care of severe sepsis. Am J Emerg Med. (2012) 30:51–6. doi:
10.1016/j.ajem.2010.09.015
5. Goldstein B, Giroir B, Randolph A, International Consensus Conference on Pediatric Sepsis.
International pediatric sepsis consensus conference: definitions for sepsis and organ
dysfunction in pediatrics. Pediatr Crit Care Med. (2005) 6:2–8. doi: 10.1097/00130478-
200501000-00049
6. Chousterman BG, Swirski FK, Weber GF. Cytokine storm and sepsis disease pathogenesis.
Semin Immunopathol. (2017) 39:517–28. doi: 10.1007/s00281-017-0639-8
7. Dandona P, Nix D, Wilson MF, Aljada A, Love J, Assicot M, et al. Procalcitoninincrease after
endotoxin injection in normal subjects. J Clin Endocrinol Metab. (1994) 79:1605–8. doi:
10.1210/jcem.79.6.7989463
Page 23
20
8. Tavil B, Aytac S, Balci YI, Unal S, Kuskonmaz B, Yetgin S, et al. Fludarabine, cytarabine,
granulocyte colony-stimulating factor, and idarubicin (FLAG-IDA) for the treatment of
children with poor-prognosis acute leukemia: the Hacettepe experience. Pediatr Hematol
Oncol. (2010) 27:517–28. doi: 10.3109/08880018.2010.493578
9. Moricke A, Zimmermann M, Reiter A, Henze G, Schrauder A, Gadner H, et al. Long-term
results of five consecutive trials in childhood acute lymphoblastic leukemia performed by the
ALL-BFM study group from 1981 to 2000. Leukemia. (2010) 24:265–84. doi:
10.1038/leu.2009.257
10. Haase R, Lieser U, Kramm C, Stiefel M, Vilser C, Bernig T, et al. Management of oncology
patients admitted to the paediatric intensive care unit of a general children’s hospital - a single
center analysis. Klin Padiatr. (2011) 223:142–6. doi: 10.1055/s-0031-1275291
11. Singer K, Subbaiah P, Hutchinson R, Odetola F, Shanley TP. Clinical course of sepsis in
children with acute leukemia admitted to the pediatric intensive care unit. Pediatr Crit Care
Med. (2011) 12:649– 54. doi: 10.1097/PCC.0b013e31821927f1
12. Aljabari S, Balch A, Larsen GY, Fluchel M, Workman JK. Severe sepsis-associated morbidity
and mortality among critically ill children with cancer. J Pediatr Intens Care. (2019) 8:122–9.
doi: 10.1055/s-0038-1676658
13. Ning B, Ye S, Lyu Y, Yin F, Chen Z. Effect of high-volume hemofiltration on children with
sepsis. Transl Pediatr. (2020) 9:101–7. doi: 10.21037/tp.2020.03.13
14. Miao H, Wang F, Xiong X, Wang C, Zhang Y. Clinical benefits of high-volume hemofiltration
in critically ill pediatric patients with severe sepsis: a retrospective cohort study. Blood Purif.
(2018) 45:18– 27. doi: 10.1159/000481249
15. Weiss SL, Peters MJ, Alhazzani W, Agus, M.S.D, Flori HR, et al. Surviving
sepsis campaign international guidelines for the management of septic shock and sepsis
associated organ dysfunction in children. Pediatr Crit Care Med. (2020) 21:e52–106. doi:
10.1097/PCC.0000000000002198
16. Aygun F, Varol F, Durak C, Talip Petmezci M, Kacar A, Dursun H, et al. Evaluation of
continuous renal replacement therapy and therapeutic plasma exchange, in severe sepsis or
septic shock in critically ill children. Medicina. (2019) 55:350. doi:
10.3390/medicina55070350
17. Ankawi G, Neri M, Zhang J, Breglia A, Ricci Z, Ronco C. Extracorporeal techniques for the
treatment of critically ill patients with sepsis beyond conventional blood purification therapy:
the promises and the pitfalls. Crit Care. (2018) 22:262. doi: 10.1186/s13054-018-2181-z
18. Villa G, Zaragoza JJ, Sharma A, Neri M, De Gaudio AR, Ronco C. Cytokine removal with high
cut-off membrane: review of literature. Blood Purif. (2014) 38:167–73. doi: \
10.1159/000369155
19. Ankawi G, Fan W, Pomare Montin D, Lorenzin A, Neri M, Caprara C, et al. A new series of
sorbent devices for multiple clinical purposes: current evidence and future directions. Blood
Purif. (2019) 47:94–100. doi: 10.1159/0004 93523
20. Thomas M, Moriyama K, Ledebo I. AN69: evolution of the world’s first high permeability
membrane. Contrib Nephrol. (2011) 173:119– 29. doi: 10.1159/000328961
21. Honore PM, De Bels D, Barreto Gutierrez L, Spapen HD. Hemoadsorption therapy in the
critically ill: solid base but clinical haze. Ann Intens Care. (2019) 9:22. doi: 10.1186/s13613
019-0491-1
22. Saparov A, Sazonov V, Tobylbaeva Z, Isakov S, Bekpan A, Autalipov D, et al. First successful
hemoadsorption using CytoSorb((R)) in a septic pediatric patient in Kazakhstan: a case report.
Int J Artif Organs. (2019) 42:315– 7. doi: 10.1177/0391398818819953
Page 24
21
23. Schadler D, Pausch C, Heise D, Meier-Hellmann A, Brederlau J, Weiler N, et al. The effect of a
novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic patients: a
randomized controlled trial. PLoS ONE. (2017) 12:e0187015. doi
10.1371/journal.pone.0187015
24. Bottari G, Guzzo I, Marano M, Stoppa F, Rava L, Di Nardo M, et al. Hemoperfusion with
Cytosorb in pediatric patients with septic shock: a retrospective observational study. Int J Artif
Organs. (2020) 43:587– 93. doi: 10.1177/0391398820902469
25. Huang Z, Wang SR, Su W, Liu JY. Removal of humoral mediators and the effect on the
survival of septic patients by hemoperfusion with neutral microporous resin column. Ther
Apher Dial. (2010) 14:596– 602. doi: 10.1111/j.1744-9987.2010.00825.x
26. 26. Huang Z, Wang SR, Yang ZL, Liu JY. Effect on extrapulmonary sepsisinduced acute lung
injury by hemoperfusion with neutral microporous resin
column. Ther Apher Dial. (2013) 17:454–61. doi: 10.1111/j.1744-9987.2012.
01083.x
27. Kacar CK, Uzundere O, Kandemir D, Yektas A. Efficacy of HA330 hemoperfusion adsorbent
in patients followed in the intensive care unit for septic shock and acute kidney injury and
treated with continuous venovenous hemodiafiltration as renal replacement therapy. Blood
Purif. (2020) 49:448– 56. doi: 10.1159/000505565
28. Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress
syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus
Conference. Pediatr Crit Care Med. (2015) 16:428–39. doi: 10.1097/PCC.00000000000 00350
29. Alexander S, Fisher BT, Gaur AH, Dvorak CC, Villa Luna D, Dang H, et al. Effect of
levofloxacin prophylaxis on bacteremia in children with acute leukemia or undergoing
hematopoietic stem ell transplantation: a randomized clinical trial. JAMA. (2018) 320:995–
1004. doi: 10.1001/jama.2018.12512
30. Zhang J, Peng Z, Maberry D, Volpe J, Kimmel JD, Federspiel WJ, et al. Effects of
hemoadsorption with a novel adsorbent on sepsis: in vivo and in vitro study. Blood Purif.
(2015) 39:239–45. doi: 10.1159/000381006
Conflict of Interest: The authors declare that the research was conducted in the absence of any
commercial or financial relationships that could be construed as a potential conflict of interest.
Copyright © 2021 Sazonov, Abylkassov, Tobylbayeva, Saparov, Mironova and
Poddighe. This is an open-access article distributed under the terms of the Creative Commons
Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted,
provided the original author(s) and the copyright owner(s) are credited and that the original
publication in this journal is cited, in accordance with accepted academic practice. No use,
distribution or reproduction is permitted which does not comply with these terms.
Page 25
Efficacy of Hemoperfusion in Severe and Critical
Cases of COVID-19
22
Keywords: COVID-19, SARS-CoV-2, Hemoperfusion, acute respiratory distress syndrome,
Cytokine storm
Abstract
Introduction: In critically ill COVID-19 patients, uncontrolled over-production of inflammatory
mediators is observed, dominantly. The excessive immune response give rise to multiple organ
dysfunction. Implementing extracorporeal therapies may be useful in omitting inflammatory
mediators and supporting different organ systems. We aimed to investigate the effectiveness of
hemoperfusion in combination with standard therapy in critically ill COVID-19 patients.
Method: We conducted a single-center, matched control retrospective study on patients with
confirmed SARS-CoV- 2 infection. Patients were treated with hemoperfusion in combination with
standard therapy (hemoperfusion group) or standard treatment (matched group). Hemoperfusion or
hemoperfusion and CRRT (continuous renal replacement therapy) therapies were initiated in
hemoperfusion group. The patients in the matched group were matched one by one with the
hemoperfusion group for age, sex, the oxygen saturation (SPO2) at the admission and the
frequency of using invasive mechanical ventilation during hospitalization. Two types of
hemoperfusion cartridges used in this study were Jafron© (HA330) or cytosorb® 300.
Result: A total number of 128 COVID- 19 confirmed patients were enrolled in this study; 73
patients were allotted to the matched group and 55 patients received hemoperfusion. The median
SPO2 at the admission in control and hemoperfusion groups was 80% and 75%, respectively (P-
value=0.113). The mortality rate was significantly lower in hemoperfusion group compared to the
matched group (67.3% vs. 89%; P.value=0.002). The median length of ICU stay was statistically
different in studied groups (median, 12 days for hemoperfusion group vs. 8 days for the matched
group; P<0.001). The median of final oxygen saturation was statistically higher and median of
PaCO2 was lower in hemoperfusion group compared to the matched group.
Conclusion: Among critically ill COVID-19 patients, the use of hemoperfusion reduces the
mortality rate and improves oxygen saturation and PaCO2.
Introduction
On 11th March 2020, COVID-19 was declared a global pandemic by World Health Organization
(WHO). Infected cases with COVID-19 represent a wide spectrum of symptoms ranging from mild
to severe forms. Although the number of infected cases with mild or no symptoms is significant,
COVID-19 leads to Page 4/16 critical illness in some cases. Multiple organ failure can be expected
Ilad Alavi Darazam1*, Muhanna Kazempour1, Mohamad Amin Pourhoseingholi1, Firouze Hatami1,
Mohammad Mahdi Rabiei1, Farid Javandoust Gharehbagh1, Mahdi Amirdosara1, Mohammadreza
Hajiesmaeili1, Minoosh Shabani1, Shervin Shokouhi1, Legha Lotfollahi1, Masoud Mardani1, Maryam
Haghighi-Morad1, Davoud Rangraz1, Hassan Falahaty1, Hosein Syami1, Yaghoob Irannejad1, Maryam
fallah1, Masoud Zangi1, Navid Shaigh1
1 Shahid Beheshti University of Medical Sciences https://orcid.org/0000-0002-4440-335X
* ([email protected]
04
Page 26
23
among severe forms of infection with COVID-19. Therefore, extracorporeal organ support may be
required (1, 2). In some patients, excessive immune response against SARS-CoV-2 results in
cytokine storm characterized by uncontrolled overproduction of pro-inflammatory cytokines (e.g.,
Interferon γ, interleukin (IL-) 1B, IL-6, IL-12) (3). Increased circulating levels of pro inflammatory
cytokines and chemokines are associated with endothelial dysfunction and microvascular and
macrovascular thrombosis (4). Therefore, cytokine storm can result in multiple organ failure
including acute respiratory distress syndrome (ARDS) and acute kidney injury (AKI). Multiple
organ failure is responsible for high mortality among at least severe cases of COVID-19 (5). It has
been shown that there is a positive association between mortality rate and levels of pro-and anti-
inflammatory cytokines (6).
Based on the pathophysiology of COVID-19, implementing of sequential extracorporeal
therapies is worthwhile in order to eliminating of extra inflammatory mediators (7).
Hemoperfusion is an extracorporeal blood purification modality. Throughout hemoperfusion
process, anticoagulated blood is circulated through a sorbent containing cartridge (or column) and
large endogenous and exogenous molecules including targeting cytokines, endotoxin and virus
particles are removed depending on the type of sorbent (for example, pure resins, polymyxin-
coated resins, or heparin-coated resins)(1, 8). Hemoperfusion devices adsorb and remove both pro-
inflammatory and anti-inflammatory cytokines nonselectively. Therefore, the other side of coin is
excessive immunosuppression or removing anti-inflammatory mediators (7). A study by De Vriese
et al. showed that levels of pro- and anti-inflamatory cytokines decreased significantly after
performing continuous veno-venous hemofiltration in patients with septic shock and acute kidney
injury(9). However, based on a recent expert review, information regarding
the fact that implementing of hemoperfusion provides beneficial effects in quenching cytokine
storm products is limited and sporadic.
The Emergency Use Authorization (EUA) authority allowed FDA to grant temporary
authorization for four hemoperfusion devices for treatment of severe COVID-19 with cytokine
storm (10). To date, there is no effective and promising treatment, hence extracorporeal therapies
can be a treatment option for improving COVID-19 outcomes and prevent organ dysfunction. We
performed a matched control retrospective study to investigate the efficacy of hemoperfusion in
combination with standard therapy in critically ill COVID-19 patients.
Material And Methods
Study design
We conducted a single-center, matched control retrospective study on cases with con¦rmed
SARS CoV-2 infection (positive reverse transcriptase polymerase-chain-reaction (RT-PCR) and/or
positive computed tomography scan (CT Scan findings)). The study’s participants were selected
from those who hospitalized between 17 October, 2020 and 17 January,2021 at our hospital (a
major referral medical center for COVID-19 outbreak). The study was approved by Medical
Research Committee for Research Ethics and signed informed consents were obtained from all
patients or their legally authorized representatives. This study is registered with IRCT (Iranian
registry of clinical trial), IR.SBMU.RETECH.REC.1399.582.
Patients
Inclusion Criteria for this study were 1) Adults≥18 years old 2) Oxygen saturation (SPO2) ≤
86% or respiratory rate ≥30 3) Diffuse bilateral pulmonary opacities without effusions in chest CT
scan 4) Respiratory failure not fully explained by cardiac failure or §uid overload 5) Within 1 week
of a known clinical insult or new/worsening respiratory symptom and 6) Hospitalization days ≤14
from the sign and symptom onset. The manifestations were including at least one of the radiation
contactless body temperature ≥37.8, cough, shortness of breath, nasal congestion/ discharge,
Page 27
24
myalgia/arthralgia, diarrhea/vomiting, headache or fatigue on admission.
Patients in the matched group also meet the same criteria defined for hemoperfusion group and
were selected from the same patients within similar time period. Patients in matched group were
also matched one by one with the hemoperfusion group for age, sex, the oxygen saturation (SPO2)
at the admission and the frequency of using invasive mechanical ventilation during hospitalization.
Treatment
Hemoperfusion and matched groups received IFN-β1a (Recigen) (Subcutaneous injections of 44
μg (24,000 IU) on days 1, 3, 6) + remdesivir (200mg first dose then 100 mg daily dose for 5 days)
+ methylprednisolone pulse therapy (1000 mg for three days then 1 mg/kg twice daily) and
standards of care including the necessary oxygen support, non-invasive, or invasive mechanical
ventilation. In addition, hemoperfusion or hemoperfusion and CRRT (continuous renal
replacement therapy) therapies were initiated in the hemoperfusion group.
Hemoperfusion treatment: The patients were administered hemoperfusion through femoral
venous catheters at a blood §ow rate of 250-300 mL/min. Two types of hemoperfusion cartridges
used in this study were Jafron© (HA330) for 4 hours or cytosorb® 300 for 8 to 12 hours.
Hemoperfusion + CRRT: Blood was filtered and returned to the patient with replacement fluid.
The modality of CRRT was pre-dilution continuous venovenous hemofiltration (CVVH). The
volume of the CRRT dose was adjusted according to individual patient requirements nevertheless
the CRRT dose was usually 20-25 ml/kg per hour and access was achieved through a central
venous catheter placed in one of the large central veins. The cartridges were used in this method
were Jafron© (HA330) for 8 hours or CytoSorb® 300 for 12-24 hours.
Based on the improvement in patient's clinical status after hemoperfusion, including being able
to reduce mechanical ventilation support in the intubated patients or improve oxygen saturation in
non-intubated patients, the medical team decided to perform second or third course of
hemoperfusion.
Sodium heparin was used as an anticoagulant and administered as a bolus dose and continues
and try to maintain activated partial thromboplastin time ratio (APTTr) ≤2. The loading dose of
heparin in hemoperfusion therapy was 3000-1000 IU and the maintenance dose was between 1000
to 2000 IU per hour. The loading dose of heparin in hemoperfusion plus CRRT therapy was
between 2000 to 5000 IU and the maintenance dose was between 500-1000 IU per hour (11). In
patients with coagulopathy and patients treated with other anticoagulants the heparin was not used.
Outcome Measures
We studied the clinical progression of two groups during their hospital admission. The mortality
rate in the late phase of admission (including the survival time), duration of hospitalization,
intubation length, oxygen saturation, arterial blood gas findings, complete blood count ¦ndings and,
C-Reactive Protein (CRP) have been compared between two groups.
Statistical analysis
Frequency rates and percentages were used for categorical variables, and Interquartile Ranges
(IQRs) and median were used for continuous variables. For comparison the non-normal continuous
variables, Mann–Whitney U test was used. Chi-Square test was used for comparing the frequency
of categorical variables. Cox proportional hazard regression model and Kaplan–Meier curve (with
logrank test) were also applied to calculate the Hazard rate (HR) with 95% Confidence Intervals
(CIs). STATA software version 14.0 was used to perform the statistical analyses and 0.05 was
considered as statistically significant level.
Page 28
25
Results
Of all recruited patients (n = 128), 55 patients received hemoperfusion and 73 patients were
allotted to the control group who were matched for age, gender, oxygen saturation and incubation
rate with hemoperfusion group. Mean (SD) age of total participants was 59.6 (10.92). Distribution
of male and female gender was 64.1% and 35.9%, respectively. No significant difference was
observed in terms of age and gender between hemoperfusion and matched control group. Table 1
outlines demographic and baseline clinical factors in two studied groups. Although Majority of
clinical factors did not reach a significant difference between two groups, hypertension rate,
ischemic heart disease as the underlying conditions, PH, PaCO2, lymphocyte count, platelet count
and creatine phosphokinase were significantly different (Table 1).
Page 30
27
The total number of deaths in our study was 102 (70.9%). In the hemoperfusion group, the
mortality rate was significantly lower as opposed to matched control group (67.3% vs 89%; P-
value = 0.002). As outlined in Table 2, median length of ICU stay and duration of incubation were
significantly higher in hemoperfusion group. Final oxygen saturation was significantly higher in
hemoperfusion group whilst PaCO2 was found to be lower in the respect group compared to
control group. In addition, C-reactive protein (CRP) were also different between two groups (Table
2).
Page 31
28
To evaluate the effect of hemoperfusion on survival of severe COVID-19 patients, long-rank test
was conducted on survival time of hospitalized patients which was statistically different between
two groups (median, 12 days for hemoperfusion group vs 8 days for the control group; P < 0.001)
and the Kaplan– Meier curve indicated that the cumulative survival was higher for patients in
hemoperfusion group compared to their matches (Fig. 1).
Of 55 patients in hemoperfusion group, the number of patients received one, two and three or
four courses of hemoperfusion was 18 (32.7%), 14 (25.4%) and 23 (41.9%), respectively. Number
of patients received hemoperfusion with cartridge 300 and 330 was 9 and 46, respectively. The
number of deaths among patients who had cartridge 300 was 4 (44.4%) and the respect number for
patients who had cartridge 330 was 14 (30.4%). No significant association was found between
cartridge type and mortality rate in hemoperfusion group.
Cox regression model was employed to calculate hazard of death for patients in matched group
compared to hemoperfusion group. Analyses were done in crude and adjusted models. Two
significant underlying diseases (hypertension and ischemic heart disease) were not included in
multivariate model since the Cochran's Mantel-Haenszel test indicated conditional independence
across these two underling diseases for both hypertension (P.value = 0.646) and Ischemic Heart
Disease (P.value = 0.400), but age, sex, oxygen saturation and lymphocyte count at the baseline
were included as the adjusting factors. According to the analysis in crude model, the hazard rate
(HR) of death in matched groups compared to hemoperfusion group was 2.54 (95% CI: 0.1.67–
3.87, P < 0.001) and the adjusted HR was 2.39 (95% CI: 1.49–3.83, P < 0.001). Both crude and
adjusted analyses revealed that patients who treated in matched group were at higher risk of death
Page 32
29
compared to patients who treated in hemoperfusion group.
Discussion
Hemoperfusion has been suggested as an effective treatment for COVID-19 patients in
conjunction with other conventional remedies. In this study, hemoperfusion group exhibited higher
O2 saturation but lower PaCO2 and CRP levels compared to matched control group. An interesting
finding of this study was that lower mortality rate was observed among the patients in
hemoperfusion group. Jafron® and CytoSorb® are two different manufacturers of hemoperfusion
cartridges. Although they employ different methodology for preforming hemoperfusion, their
cartridge efficacy has not been compared so far in a study.
Cytokine storm and intensive immune responses have been addressed as the root causes of
severe form of COVID-19 infection (12). It has been observed that cytokine storm plays crucial
role in exerting endorgan damage and increasing mortality rate among patients with COVID-19.
Of all series of cytokines, IL- 1, IL-6, IL-10, and TNF-beta are the most remarkable inflammatory
factors through the cytokine storm phenomenon (13–15). Furthermore, the most critical role in
cytokine storm, patients mortality and the severity of the disease have been attributed to IL-6 (16).
At early stages of COVID-19, increased levels of CRP can be associated with sever pulmonary
complication like acute respiratory distress syndrome (ARDS)(17). Therefore, timely clearance of
cytokines and inflammatory factors can decrease patients’ complications and mortality in COVID
19 infection (18).
Hemoperfusion, an extracorporeal blood purification modality, is used for circulating of
patients’ anticoagulated blood through a circuit that contains an absorbent filter which reduces
toxic agents and inflammatory factors like inflammatory cytokines(1, 19). The absorbent system in
hemoperfusion usually is a cartridge which has been loaded with absorbent ingredients including
charcoal (for water-soluble materials) and resins (for lipid-soluble materials) (20). HA 330 and HA
380 cartridges are two types of hemoperfusion cartridges which are used in inflammatory
conditions. These cartridges have the capability of inflammatory cytokines absorption (21). In
addition, HA 280 cartridges are capable to absorb smaller particle size(22). In the current study,
Jafron® (HA 330) and CytoSorb® 300 cartridges were used for the hemoperfusion. In a systematic
review in 2013 by Borthwick et al., it has been suggested that hemoperfusion may has significant
effects on ICU stay and mortality rate in sepsis patients (13). In addition, in the pandemic era, there
are some studies which have suggested the positive effects of hemoperfusion in COVID-19
patients (23, 24). In a study by Vardanjani et al., hemoperfusion and continuous renal replacement
therapies were effective in ceasing ARDS progression, decreasing patient intubation and patient’s
oxygen dependency in addition to their preventive effects on AKI and septic shock. Moreover, it
reduced mortality and length of hospital stay(25). In the study of De Rosa et al., hemoperfusion
with polymyxin in COVID-19 patients with endotoxic shock was associated with organ function
recovery and hemodynamic improvement(26).
This study was in the same line with the results of previous studies. In the current study, the
mortality rate was significantly lower in Hemoperfusion group compared to the matched group;
furthermore, it was observed that O2 saturation may be improved significantly after performing
hemoperfusion in COVID-19 patients. In this study, the median length of hospital stay was lower
in matched group. However, based on Kaplan model, we could find that the cumulative survival of
patients in the hemoperfusion group was associated with the median length of hospital stay.
Our study’s major strength was the high sample size of hemoperfusion group. A study by
Asgharpour et el. was conducted on 10 patients; whereas the current study was conducted on 55
patients which is the highest sample size in the literature(27). In addition, considering the high
costs of hemoperfusion for the patients, we could not implement this treatment option for every
patient due to ethical considerations, and this may be the reason for the lack of a high-sample
Page 33
30
clinical trial in this regard.
In fact, this treatment option was used in this study as a salvage treatment option in the
accompaniment of the ¦nal stage treatments. Furthermore, the hemoperfusion group and matched
group in this study was not homogenous. Some patients in this study received Tocilizumab which
can affect the mortality of patients(28). Moreover, patients in this study received different courses
of hemoperfusion (not same in the number and length of sessions) by two different cartridges. As
shown in this study, hemoperfusion by Jafron® 330 cartridge had lower mortality compared to
CytoSorb® cartridge; however, it failed to reach significant difference. The results can be changed
in future studies with homogeneous and higher sample sizes.
Limitation
Our data collection depended on physicians completing because our study is a respectively
study. This study is not a randomized clinical trial; therefore, there are not exact inclusion and
exclusion criteria. It was not possible to analyze arterial blood gas for some patients because of
technical procedures and trained staff limitation. In this study two types of hemoperfusion
cartridge were used due to lack of access to a certain type of hemoperfusion cartridge in various
times.
Conclusion
Among critically ill COVID-19 patients, we found a signi¦cant reduction in mortality rate and
improvement of oxygen saturation and pCO2 in hemoperfusion group. To evaluation of the e¨cacy
of hemoperfusion due to some limitations in this study, randomized controlled clinical trials are
needed.
Declarations
Ethics approval: The study was con¦rmed by the Ethics in Medical Research Committee of the
Shahid Beheshti University of Medical Sciences. This study is registered with IRCT (Iranian
registry of clinical trial), IR.SBMU.RETECH.REC.1399.582.
Consent for publication: Not applicable
Page 34
31
Availability of data and materials: The datasets generated during and/or analyzed during the
current study are available from the corresponding author on reasonable request.
Acknowledgments: The authors would like to thank the Clinical Research Development Unit
(CRDU) of Loghman Hakim Hospital, Shahid Beheshti University of Medical Sciences, Tehran,
Iran for their help and support in conducting this study.
Funding: Not applicable
Conflict of interests: We declare no competing interests
Authors' contributions: All authors contributed to conception and design of study; MMR, FH,
IAD, and KM contributed to the acquisition of data; MMR, FH, IAD and MAP contributed to the
analysis of data; all authors contributed to the drafting of the article and/or critical revision; and all
authors contributed to the finnal approval of manuscript.
References
1. Ronco C, Reis T. Kidney involvement in COVID-19 and rationale for extracorporeal therapies.
Nature Reviews Nephrology. 2020;16(6):308-10.
2. National Institutes of Health (NIH). Clinical Presentation of People with SARS-CoV-2
Infection October 9, 2020 [Available from:
https://www.covid19treatmentguidelines.nih.gov/overview/clinicalpresentation/.
3. Coperchini F, Chiovato L, Croce L, Magri F, Rotondi M. The cytokine storm in COVID-19: An
overview of the involvement of the chemokine/chemokine-receptor system. Cytokine &
growth factor reviews. 2020;53:25-32.
4. Li H, Liu L, Zhang D, Xu J, Dai H, Tang N, et al. SARS-CoV-2 and viral sepsis: observations
and hypotheses. The Lancet. 2020;395(10235):1517-20.
5. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological ¦ndings of COVID-19
associated with acute respiratory distress syndrome. The Lancet respiratory medicine.
2020;8(4):420-2. ½.
6. Kellum JA, Kong L, Fink MP, Weissfeld LA, Yealy DM, Pinsky MR, et al. Understanding the
in§ammatory cytokine response in pneumonia and sepsis: results of the Genetic and
In§amatory Markers of Sepsis (GenIMS) Study. Archives of internal medicine.
2007;167(15):1655-63.
7. Clark EG, Hiremath S, McIntyre L, Wald R, Hundemer GL, Joannidis M. Haemoperfusion
should only be used for COVID-19 in the context of randomized trials. Nature Reviews
Nephrology. 2020;16(12):697-9. ¾.
8. Ronco C, Bagshaw SM, Bellomo R, Clark WR, Husain Syed F, Kellum JA, et al.
Extracorporeal blood puri¦cation and organ support in the critically ill patient during COVID
19 pandemic: expert review and recommendation. Blood puri¦cation. 2021;50(1):17-27.
9. De Vriese AS, Colardyn FA, Philippe JJ, Vanholder RC, DE SUTTER JH, Lameire NH.
Cytokine removal during continuous hemo¦ltration in septic patients. Journal of the American
Society of Nephrology. 1999;10(4):846-53.
10. FDA Emergency Use Authorization Approval Documents. 2020 [Available from:
https://www.fda.gov/emergency-preparedness-and-response/mcm-legal-regulatory-and
policyframework/emergency-use-authorization#covidothermeddev.
11. Ostermann M, Dickie H, Tovey L, Treacher D. Heparin algorithm for anticoagulation during
continuous renal replacement therapy. Critical care. 2010;14(3):1-2.
Page 35
32
12. Ragab D, Salah Eldin H, Taeimah M, Khattab R, Salem R. The COVID-19 cytokine storm;
what we know so far. Frontiers in immunology. 2020;11:1446.
13. Cao X. COVID-19: immunopathology and its implications for therapy. Nature reviews
immunology. 2020;20(5):269-70.
14. Liu B, Li M, Zhou Z, Guan X, Xiang Y. Can we use interleukin-6 (IL-6) blockade for
coronavirus disease 2019 (COVID-19)-induced cytokine release syndrome (CRS)? Journal of
autoimmunity. 2020:102452.
15. 15. Han H, Ma Q, Li C, Liu R, Zhao L, Wang W, et al. Pro¦ling serum cytokines in COVID-19
patients reveals IL-6 and IL-10 are disease severity predictors. Emerging microbes &
infections. 2020;9(1):1123-30. 1½.
16. McElvaney OJ, McEvoy NL, McElvaney OF, Carroll TP, Murphy MP, Dunlea DM, et al.
Characterization of the in§ammatory response to severe COVID-19 illness. American journal
of respiratory and critical care medicine. 2020;202(6):812-21.
17. Mardani R, Vasmehjani AA, Zali F, Gholami A, Nasab SDM, Kaghazian H, et al. Laboratory
parameters in detection of COVID-19 patients with positive RT-PCR; a diagnostic accuracy
study. Archives of academic emergency medicine. 2020;8(1).
18. Koertge A, Wasserkort R, Wild T, Mitzner S. Extracorporeal hemoperfusion as a potential
therapeutic option for critical accumulation of rivaroxaban. Blood puri¦cation. 2018;45(1
3):126-8.
19. Vardanjani AE, Golitaleb M. COVID-19 Pandemic Hemoperfusion Therapy OR Plasma
Exchange Therapy in Intensive Care. Iranian Journal of Allergy, Asthma and Immunology.
2020:1-3.
20. Safari S, Salimi A, Zali A, Jahangirifard A, Bastanhagh E, Aminnejad R, et al. Extracorporeal
Hemoperfusion as a Potential Therapeutic Option for Severe COVID-19 patients; a Narrative
Review. Archives of academic emergency medicine. 2020;8(1).
21. Ankawi G, Fan W, Montin DP, Lorenzin A, Neri M, Caprara C, et al. A new series of sorbent
devices for multiple clinical purposes: current evidence and future directions. Blood
puri¦cation. 2019;47(1-3):94- 100.
22. Kogelmann K, Jarczak D, Scheller M, Drüner M. Hemoadsorption by CytoSorb in septic
patients: a case series. Critical Care. 2017;21(1):1-10.
23. Moradi H, Abbasi S. Hemoperfusion as a Supportive Treatment in a COVID-19 Patient with
Late Pulmonary Thromboembolism: A Case Report. International Medical Case Reports
Journal. 2020;13:341.
24. Shadvar K, Tagizadiyeh A, Gamari AA, Soleimanpour H, Mahmoodpoor A. Hemoperfusion as
a Potential Treatment for Critically Ill COVID-19 Patients with Cytokine Storm. Blood
Puri¦cation. 2020:1-3.
25. Vardanjani AE, Ronco C, Ra¦ei H, Golitaleb M, Pishvaei MH, Mohammadi M. Early
hemoperfusion for cytokine removal may contribute to prevention of intubation in patients
infected with COVID-19. Blood Puri¦cation. 2021;50(2):257-60.
26. De Rosa S, Cutuli SL, Ferrer R, Antonelli M, Ronco C, Group CEC, et al. Polymyxin B
hemoperfusion in COVID‐19 Patients with endotoxic shock: Case Series from EUPHAS II
registry. Arti¦cial organs. 2020.
27. Asgharpour M, Mehdinezhad H, Bayani M, Zavareh MSH, Hamidi SH, Akbari R, et al.
Effectiveness of extracorporeal blood puri¦cation (hemoadsorption) in patients with severe
coronavirus disease 2019 (COVID-19). BMC Nephrology. 2020;21(1):356.
28. Tleyjeh IM, Kashour Z, Damlaj M, Riaz M, Tlayjeh H, Altannir M, et al. E¨cacy and safety of
tocilizumab in COVID-19 patients: a living systematic review and meta-analysis. Clinical
Microbiology and Infection. 2020.
Page 36
Experience of application of combined extracorporeal blood
purification with hemoadsorption (HA330/HA330-II) at
patients with severe COVID - 19
33
Abstract:
The COVID-19 pandemic has faced all medical society to problems of various complication in
clinical picture substantial morbidity and mortality worldwide. Millions of people worldwide had
struggled with this disease, many of them unfortunately lost the battle. Diversity of this disease
have made therapy overly complicated. More than 1-year scientists worldwide try to solve the
riddles of the virus and find the key to the lock. Various approaches and combinations have been
tested in the intensive care of patients with COVID - 19. Unfortunately, mortality rate is still high
moreover there is no certain therapy or prevention from coronavirus. Ongoing advances in science
and progress in understanding of etiopathogenesis, development of complications such as a
cytokine storm, draw attention of medical society to extracorporeal methods of blood purification
as a variant of inflammatory activity reduction. According to literature data direction to
extracorporeal blood purification methods in intensive care was beneficial to patients. Thus, in our
center we have provided different combinations of blood purification to patients with severe
COVID – 19 and cytokine storm. We would like to share with our experience of blood purification
(hemadsorption) application to patients with severe COVID – 19 in ICU.
Keywords: Blood purification, hemadsorption, ECMO, COVID -19, MODS, cytokine storm.
Introduction:
COVID – 19 pandemics swept the world in 2019, until today, scientists have accumulated more
questions than answers. What is already known about the disease?
The first – extremely high level of mortality in intensive care unit (ICU). According to data of
systematic review it ranges from 31% in Spain, 35.2% in Italy, 41.2% in Denmark and more than
70% in China at patients with severe COVID – 19 and invasive mechanical ventilation [1-3].
Multifaced clinical picture - emerging data suggest that Novel Coronavirus disease particularly
dangerous for the human organism due to affection of multiple organs, leading to organ failure and
eventually death [4]. Furthermore, COVID-19 is associated with high mortality due to numerous
complications such as acute respiratory distress syndrome (ARDS), systemic inflammation (sepsis,
cytokine storm), multiorgan dysfunction (MODS), acute kidney injury (AKI) and liver damage
[5,6]. ARDS leads to severe respiratory failure, severe hypoxia and necessity of invasive
mechanical ventilation or even extracorporeal membrane oxygenation (ECMO) [7-9]. Cytokine
storm and sepsis often diagnosed at patients with severe COVID – 19 [10]. Elevated cytokine
levels result in endothelial dysfunction, vascular damage, and metabolic dysregulation, thereby
damaging multiple organ systems [11]. Extracorporeal blood purification methods obviously has
positive effect in the complex therapy of hyperinflammation [12, 13]. The timeliness and validity
Nilufar Jabaeva, Aidyn Kuanyshbek, Rymbay Kaliyev, Timur Kapyshev, Timur Lesbekov, Nurlan Smagulov,
Tatyana Li, Zhuldyz Nurmakhametova, Shaimurat Tulegenov, Bolat Bekishev, Ainamkoz Amanzholova.
NJSC National research cardiac surgery center. Turan ave 38. Nur-Sultan city. Kazakhstan. 010000
05
Page 37
34
of the start of extracorporeal procedures is crucial. The maximum effect can be achieved if
extracorporeal treatment is performed in the early stages of the clinical and laboratory
manifestation of the "cytokine storm" syndrome and MODS [14].
Numerous complications cumulatively and diversity of the COVID 19 course, have made
management of this disease extremely hard and tricky. This occasion has led our team to provide
this research. We would like to share our experience of combined extracorporeal blood purification
methods application as an option of severe COVID – 19 intensive care.
Materials and methods:
We conducted a retrospective analysis of 69 medical records of patients hospitalized in the ICU
of JSC National Research Cardiac Surgery Center (NRCSC) Nur-Sultan city, Kazakhstan because
of severe course of COVID 19.
Inclusion criteria: Patients with positive COVID - 19 in severe condition. Patients treated by blood
purification with hemadsorption.
Exclusion criteria: Patients with coagulopathy. Active bleeding. Hemorrhage stroke.
To all patients were provided extracorporeal blood purification with hemadsorption (HA 330/HA
330II (Jafron Biomedical, China) as an additional option to intensive care.
Jafron HA 330/ HA 330II - disposable cartridges are filled with an adsorbent material — a
copolymer of styrene and divinylbenzene. The adsorbing material of different models of cartridges
of the "HA" series has different porosity of granules. Due to this, as well as hydrophobic and ionic
interaction, the target molecules — toxins, cytokines, bilirubin, and others-are removed from the
bloodstream. Cartridge HA 330 recommended for sepsis therapy, HA 330II for therapy of liver
damage.
Hemoadsorption with a HA 330 column was effectively used in the treatment of CAVID-19
[14]. Methods and sequence of extracorporeal therapy
1. Hemoadsorption method (Picture #1 a).
The procedures were performed using the adsorbent HA 330 or HA 330II (Jafron Biomedical,
China) on a JAFRON apparatus (Jafron Biomedical, China). A double lumen dialysis catheter or
ECMO circuit was used as a vascular access. 5 patients underwent 4 hemoperfusion procedures of
180-200 duration each. The blood flow rate was maintained in the range of 180-200 ml/min.
Heparin dosage was titrated individually for every patient, and the indicators of activated clotting
time (ACT) before and during the procedure.
2. Combined method (Picture #1 b).
It was decided to carry out extracorporeal therapy at patients with AKI that required RRT (15
patients) in combination form of joint procedures of hemadsorption with HA330 or HA330II
cartridges and hemodiafiltration/hemofiltration in a single circuit.
Methodology of combined hemadsorption procedures with HA330 or HA330II (Jafron
Biomedical, China) + extended continuous hemofiltration/hemodiafiltration using the OMNI
device (BBraun, Germany). A double lumen dialysis catheter or ECMO circuit was used as a
vascular access. The blood flow rate at the level of 180-200 ml/min, the perfusion time of 1
cartridge HA330 for 180 minutes, then the extended hemofiltration procedure was continued until
the next connection of the cartridge HA330 after 12-24 hours according to the recommended by
Ronco et al [13] scheme, minimally 4 procedures HA330 or HA330II for 180 minutes were
performed with further continuation of extended hemofiltration/hemodiafiltration according to
indications. Heparin was used as an anticoagulant, the dose of which was selected individually for
each patient, depending on the initial state of the blood clotting system and ACT level before and
during the procedure. To maintain ACT within 180-200 s, 15-20 U /kg/h of heparin was required.
According to the recommendations of Ronco C, Huang C [14, 15], each patient was given 2
Page 38
35
procedures for the first day, lasting at least 180 min, with an interval of 12 hours, followed by 2nd
and 3d day with an interval of 24 hours. After the first 3 hours of the procedure, the HA330 or
HA330II hemadsorption circuit was switched off and the RRT procedure continued. Further
treatment of AKI was performed similarly to the protocol of sequential use of extracorporeal
procedures.
The scheme 2+1+1 HA330 columns was applied on the 1st day change it after 12 hours, on the
2nd and 3rd days-1 column change after 24 hours [15]
Results:
The total number of patients with COVID -19 – required blood purification or ECMO with HA
330 or HA 330 II (Jafron hemoadsorber)– 20 patients.
Mean age of patients- 53.57 [29, 70] years.
Distribution of comorbid pathology in our group: 40% of patients had high BP level, 35% had
Diabetes Insipidus, and more 20% had obesity on the moment of hospitalization to ICU. It
confirms that comorbid pathology exacerbates clinical picture. All patients in our research were in
extremely severe condition.
№ Comorbid pathology N = 20
1 Type 2 diabetes 7 (35%)
2 COPD 1 (5%)
3 Arterial hypertension 8 (40%)
4 Ischemic heart disease 3 (15%)
5 Obesity 5 (25%)
6 LVAD 1 (5%)
7 Gastric ulcer 1 (5%)
8 Chronic renal failure 1 (5%)
Table # 1. Distribution of the comorbid pathology.
Table # 2. Complications of COVID – 19.
# Type of complication N (20)
1 *Cytokine storm 13 (65%)
2 MODS 5 (25%)
3 SEPSIS 5 (25%)
4 Acute respiratory failure (ARDS) 14 (70%)
5 Acute kidney injury 2 (KDIGO 2018) 9 (45%)
6 Acute kidney injury 3 (KDIGO 2018) 6 (30%)
7 Acute liver failure 7 (35%)
* Cytokine storm at patients with COVID – 19 was diagnose on the basis of laboratory
data: elevation in blood probe of PCT , Presepsin, IL6, CRP level, and severe clinical
manifestation of COVID – 19.
Page 39
36
Complications of COVID – 19 in our group was distributed in the order: on the 1st place was
ARDS, what is why 15 patients had invasive mechanical ventilation and 14 patients had ECMO.
On the second place was cytokine storm – 65%, and AKI. All these complications had not
excluded the presence of each other and could be present simultaneously.
Depends on the type of complication, extracorporeal blood purification method was prescribed.
Consequently, 15patients in our research group had received - combined procedures of blood
purification -RRT with hemadsorption by HA 330 or HA 330 II cartridges.
Distribution and duration of extracorporeal blood purification methods presented in the table #3.
Picture #1. a)Hemadsorbtion by Hemoperfusion machine Model: JF-800A with cartridge HA 330,
b) combined method (OMNI BBraun) CVVHD with cartridge HA 330.
Laboratory data of patients with severe COVID – 19 had trends to improvement on the background
of intensive care and combined methods of extracorporeal blood purification. Decreasing of the
presepsin level had not significant value.
Mortality rate in the group of investigation 10 from 20 – 50%.
Type of procedure Quantity of procedures
(n=84)
Duration (hour)
HP (HA 330)+ CVVHF/CVVHDF 2+1+1 (n=33) >3 (24) h
HP (HA330II)+
CVVHF/CVVHDF
2+1+1 (n=31) > 3 (24)h
HP (HA 330/HA330II)+ECMO 2+1+1(n=20) > 3 (24)h
Table #3. Type, quantity and duration of the procedures
a b
Page 40
37
Chart#1 Laboratory data.
0.00
5.00
10.00
15.00
20.00
25.00
30.00
35.00
before procedure after 1 procedure after 2 procedure after 3 procedure Agter 4 procedure
Trends of laboratory data
Leuk CRP PCT Crea Bil T Bil D
Table #4. Laboratory data – trends of Leukocytes, CRP, IL - 6, PCT, Urea, Creatinine, and
bilirubin level. (Mean level [min;max]).
Laboratory
data
Before blood
purification
After 1
procedure
After 2
procedure
After 3
procedure
After 4
procedure
Р
value
Leukocytes
10*9/l
15.30
[5.8; 34.03]
13.31
[7.44;31.08]
10.68 [5.56;
15.55]
8.23 [5.13;
14.23]
6.54 [3.75;
12.44]
0.01
C-reactive
protein
mg/dL
19.78
[0.15; 54.86]
16.89
[0.46;
33.12]
12.43 [0.09;
29.07]
6.06
[0.054;
23.97]
5.78 [0.05;
18.76]
0.043
Interleukin-6
pg/mL
260.77
[54; 572]
205.82
[21.03; 403]
201.188
[12.56;
365.48]
108.9
[12.86;
290.45]
85.76
[10.53;
220.14]
0.027
Procalcitonin
ng/ml
30.38
[0.1; 38.28]
12.13
[0.1; 30.38]
4.34 [0.08;
12.73]
5.56
[0.054;
10.76]
3.82 [0.06;
8.12]
0.01
Creatinin
mg/dL 2.33
[0.77; 3.23]
1.77
[0.86;2.98]
1.89 [0.80;
2.93 ]
1.34 [0.86;
1.06 ]
1.22 [0.82;
1.03]
0.01
Presepsin
pg/mL
2420.24
[19.96;
16277]
2788.81
[657; 9834]
1783.56
[232.64;
11589]
2063.41
[217.12;
8653.45]
1980.65
[256.11;
6544.67]
0.18
Bilirubin
Total
mg/dL
5.83
[0.6; 12.93]
2.73 [0.71;
6.33]
2.58 [1.39;
5.33]
2.40 [1.35;
4.89]
1.58 [1.17;
4.25]
0.037
Bilirubin
Direct mg/dL
4.24
[0.15; 8.54]
2.44 [0.25;
5.16]
1.39 [0.72;
4.05]
1.18 [0.12;
3.58.05]
0.83 [0.13;
2.75]
0.014
Page 41
38
Discussion:
Mortality rate of patients with severe COVID – 19 was extremely high. It is impossible to compare
the mortality rate in our group with other relevant patients, due to lack of data. There were a small
number of patients with severe COVID – 19 who did not receive hemadsorption method of blood
purification. According to data of Zhou F, YuT, DuR, et al. and Yang, Xiaobo, et al which were
published in the Lancet and The Lancet Respiratory Medicine journals, the mortality rate of
patients with severe COVID - 19 in the ICU Wuhan China were on the level 65 - 78% [3,16].
According to Fawad Rahim et al the mortality rate of patients with severe COVID - 19 in the ICU
without the use of CRRT exceeds 70-77% [17].
Also our study confirmed numerous literature data that comorbid pathology as a diabetes may
significantly exacerbate the course of coronavirus disease [18, 19, 20].
Conclusions: Mortality rate at patients with severe COVID – 19 unfortunately stays on the high
level. Our experience of application of the combined extracorporeal blood purification methods
had shown positive effect in laboratory data, probably had impact in survival rate (comparing with
literature data) of extremely severe patients with COVID 19 in ICU. In our point of view
application of combined methods of extracorporeal blood purification methods has perspective for
development and requires further research.
References:
1. Quah, Pipetius, Andrew Li, and Jason Phua. "Mortality rates of patients with COVID-19 in
the intensive care unit: a systematic review of the emerging literature." Critical care 24
(2020): 1-4.
2. Wang Y, Lu X, Chen H, Chen T, Su N, Huang F, Zhou J, Zhang B, Li Y, Yan F, Wang J.
Clinical course and outcomes of 344 intensive care patients with COVID-19. Am J Respir
Crit Care Med. 2020. https://doi.org/10.1164/rccm. 202003-0736LE
3. Zhou F, YuT, DuR, et al. Clinical course and risk factors for mortality of adult inpatients with
COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–
1062. [Crossref], [PubMed], [Web of Science ®], [Google Scholar]
4. Sorbello, Massimiliano, and Robert Greif. "COVID-19 pandemic: A multifaceted challenge
for science and healthcare." Trends in Anaesthesia & Critical Care 34 (2020): 1.
5. Robba C., Battaglini D., Pelosi P., Rocco P.R.M. Multiple organ dysfunction in SARS-CoV-
2: MODS-CoV-2. Expet Rev. Respir. Med. 2020:1–4. doi:
10.1080/17476348.2020.1778470. [PMC free article] [PubMed] [CrossRef] [Google
Scholar] [Ref list]
6. WuZ, McGooganJM. Characteristics of and important lessons from the coronavirus disease
2019 (COVID-19) outbreak in China: summary of a report of 72314 cases from the Chinese
Center for Disease Control and Prevention.
JAMA. 2020;323(13):1239. [Crossref], [PubMed], [Web of Science ®], [Google Scholar]
7. HuangC, WangY, LiX, et al. Clinical features of patients infected with 2019 novel
coronavirus in Wuhan, China. Lancet. 2020;395:497–506. [Crossref], [PubMed], [Web of
Science ®], [Google Scholar]
8. Ñamendys-Silva, Silvio A. "ECMO for ARDS due to COVID-19." Heart & Lung: The
Journal of Cardiopulmonary and Acute Care 49.4 (2020): 348-349.
Page 42
39
9. Peiris, Sasha, et al. "Pathological findings in organs and tissues of patients with COVID-19: A
systematic review." PLoS One 16.4 (2021): e0250708.
10. Bhaskar, Sonu, et al. "Cytokine storm in COVID-19—immunopathological mechanisms,
clinical considerations, and therapeutic approaches: the REPROGRAM consortium position
paper." Frontiers in immunology 11 (2020): 1648.
11. Panigrahy D, Gilligan MM, Huang S, Gartung A, Cortés-Puch I, Sime PJ, et al.
Inflammation resolution: a dual-pronged approach to averting cytokine storms in COVID-
19? Cancer Metastasis Rev. (2020) 39:337–40. doi: 10.1007/s10555-020-09889-4
12. Panagiotou, Anthi, Sérgio Gaiao, and Dinna N. Cruz. "Extracorporeal therapies in
sepsis." Journal of Intensive Care Medicine 28.5 (2013): 281-295.
13. Zhou, Feihu, et al. "Blood purification and mortality in sepsis: a meta-analysis of randomized
trials." Critical care medicine 41.9 (2013): 2209.
14. Huang C., Wang Y., Li X., et al. Clinical features of patients infected with 2019 novel
coronavirus in Wuhan, China. Lancet. 2020. DOI: 10.1016/S0140-6736(20)30183-5
15. Ronco C., Reis T., De Rosa S. Coronavirus Epidemic and Extracorporeal Therapies in
Intensive Care: sivis pacem para bellum. Blood Purif. 2020 Mar 13: 1–4. DOI:
10.1159/000507039.
16. Yang, Xiaobo, et al. "Clinical course and outcomes of critically ill patients with SARS-CoV-2
pneumonia in Wuhan, China: a single-centered, retrospective, observational study." The
Lancet Respiratory Medicine (2020).
17. Fawad Rahim et al, Cureus . 2020 Oct 12;12(10):e10906. doi: 10.7759/cureus.10906.
18. Feldman, E. L., Savelieff, M. G., Hayek, S. S., Pennathur, S., Kretzler, M., & Pop-Busui, R.
(2020). Covid-19 and diabetes: a collision and collusion of two diseases. Diabetes, 69(12),
2549-2565.
19. Moccia, F., et al. "COVID-19-associated cardiovascular morbidity in older adults: a position
paper from the Italian Society of Cardiovascular Researches." GeroScience 42.4 (2020):
1021-1049.
20. Peiris, Sasha, et al. "Pathological findings in organs and tissues of patients with COVID-19:
A systematic review." PLoS One 16.4 (2021): e0250708.
Page 43
Blood Purification Techniques, Inflammatory Mediators
and Mortality in COVID-19 Patients
40
Background: Inflammatory mediators are an important component in the pathophysiology of the
coronavirus disease 2019 (COVID-19). This study aimed to assess the effects of reducing
inflammatory mediators using hemoperfusion (HP) and continuous renal replacement therapy
(CRRT) on the mortality of patients with COVID-19.
Materials and Methods: Twelve patients with confirmed diagnosis of COVID-19 were included.
All patients had acute respiratory distress syndrome (ARDS). Patients were divided into three
groups, namely, HP, CRRT and HP+CRRT. The primary outcome was mortality and the secondary
outcomes were oxygenation and reduction in inflammatory mediators at the end of the study.
Results: Patients were not different at baseline in demographics, inflammatory cytokine levels,
and the level of acute phase reactants. Half of the patients (3 out of 6) in the HP+CRRT group
survived along with the survival of one patient (1 out of 2) in the HP group. All four patients in the
CRRT group died. Serum creatinine (SCr), Interleukin-1 (IL1), Interleukin-6 (IL6), Interleukin-8
(IL8), partial pressure of oxygen (PaO2), O2 saturation (O2 sat), and hemodynamic parameters
improved over time in HP+CRRT and CRRT groups, but no significant difference was observed in
the HP group (All Ps > 0.05).
Conclusion: Combined HP and CRRT demonstrated the best result in terms of mortality, reduction
of inflammatory mediators and oxygenation. Further investigations are needed to explore the role
of HP+CRRT in COVID-19 patients.
Seyed Mohammadreza Hashemian1, Navid Shafigh2, Golnaz Afzal3, Hamidreza Jamaati1, Esmaeil Mortaz4,
Payam Tabarsi4, Majid Marjani4, Majid Malekmohammad5, Farzaneh Dastan1,3, Seyed Mehdi Mortazavi6,
Makan Sadr7, Esmaeil Idani1, Batoul Khoundabi8, Abdolreza Mohamadnia1, Atefeh Abedini1, Arda Kiani1,
Afshin Moniri7, Seyed Alireza Nadji7, Fatemeh Yassari1, Mojtaba Mokhber Dezfuli9, Mihan Pourabdollah1,
Mohammad Varahram10, Faezeh Eshaghi1, Mahdi Malekpour11 , Aliakbar Velayati1
1Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung
Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran., 2Department of
Anesthesiology and Critical Care Medicine, School of Medicine, Shahid Beheshti University of Medical
Sciences, Tehran, Iran, 3Department of Clinical Pharmacy, School of Pharmacy, Shahid Beheshti University
of Medical Sciences, Tehran, Iran, 4Clinical Tuberculosis and Epidemiology Research Center, NRITLD,
Shahid Beheshti University of Medical Sciences, Tehran, Iran, 5Tracheal Diseases Research Center
(TDRC), NRITLD, Shahid Beheshti University of Medical Sciences, Tehran, Iran, 6Department of Nursing,
Shahid Beheshti University of Medical Sciences, Tehran, Iran, 7Virology Research Center
(VRC), NRITLD, Shahid Beheshti University of Medical Sciences, Tehran, Iran, 8Iran-Helal Institute of
AppliedScience and Technology, Research Center for Health Management in Mass Gathering, Red Crescent
Society of the Islamic Republic of Iran, Tehran, Iran., 9Lung Transplantation Research Center, NRITLD,
Shahid Beheshti University of Medical Sciences, Tehran, Iran, 10Mycobacteriology Research Center,
NRITLD, Shahid Beheshti University of Medical Sciences, Tehran, Iran, 11Geisinger Medical Center,
Danville, PA , USA
*Correspondence to:HashemianSMR,Malekpour M Address: Chronic Respiratory Diseases Research
Center, NRITLD, Shahid Beheshti University of Medical Sciences, Tehran, Iran Email address:
[email protected] [email protected]
Received: 15 July 2020
Accepted: 30 September 2020
06
Page 44
41
Key words: Coronavirus disease 2019; COVID-19; Acute respiratory distress syndrome; ARDS;
Inflammatory marker; Hemoperfusion; Continuous renal replacement therapy; Cytokine;
Oxygenation; Mortality
INTRODUCTION
Following the official recognition of the novel coronavirus disease 2019 (COVID-19), it rapidly
turned into a pandemic overwhelming most of the healthcare systems. The clinical spectrum of
COVID-19 pneumonia ranges from mild upper respiratory tract involvement to severe acute
respiratory syndrome coronavirus 2 (SARSCoV-2) and ultimately death. Critically ill patients with
COVID-19 are more likely to develop acute respiratory distress syndrome (ARDS) related to
systemic proinflammatory cytokine responses over a short period of time. ARDS is a dreaded
complication of COVID-19 patients with high mortality (1-3). In February 2020, Masih
Daneshvari Hospital reported its first COVID-19 patient and became the referral center for
COVID-19 cases in Iran. The pursuing high load of patients was inevitably associated with a
significant mortality of patients in the intensive care unit (ICU) due to severe ARDS (4). Data
suggests that increased mortality of COVID-19 patients is associated with a profound systemic
inflammatory response (5).
Various cytokines are linked to COVID-19 and associated with COVID-19 induced lung injury
and ARDS. The production of a wide array of proinflammatory cytokines is significantly elevated
in patients with COVID- 19 compared to healthy individuals (6). Hypercytokinemia, also known as
a cytokine storm, is shown to be related to an alarming incidence of ARDS and critical illness
requiring ICU admission. Plasma levels of several cytokines in COVID-19 patients could serve as
potential biomarkers of disease severity in COVID-19 (7). These findings have demonstrated the
immunopathological mechanisms of COVID-19 (8).
Various therapeutic techniques should be applied to control the inflammatory storm as
confounding factors exist in patients with ARDS requiring invasive mechanical ventilation (IMV).
Hemoperfusion (HP) and continuous renal replacement therapy (CRRT) can increase inflammatory
cytokine elimination from the bloodstream and modulate immune function and, thus, improve
patient prognosis (9).
In this study, we aimed to assess the effects of CRRT, HP, and their combination on mortality in
COVID-19 patients undergoing IMV admitted to Masih Daneshvari Hospital in Tehran, Iran.
Various clinical indices, including the time of treatment and biochemical parameters, were
analyzed to assess the effects of HP and CRRT on the patient survival and to compare the effects of
these techniques to remove plasma inflammatory factors.
MATERIALS AND METHODS
Study design and participants
This study was conducted at Masih Daneshvari Hospital, Shahid Beheshti University of Medical
Sciences after the approval of the study protocol by the Clinical Research Ethics Committee
(IR.SBMU.NRITLD.REC.1399. 011). We included 12 adult patients who required mechanical
ventilation and had a partial pressure of arterial oxygen/fraction of inspired oxygen ratio
(PaO2/FiO2) under 150 with a confirmed diagnosis of COVID-19 using reverse transcription
polymerase chain reaction RT-PCR. The initial blood sample was collected immediately after the
patient was admitted to the ICU and prior to receiving any treatment.
Patients were divided into three groups (HP, CRRT, and HP+CRRT) based on their initial kidney
function, glomerular filtration rate (GFR), and neutrophil gelatinaseassociated lipocalin (NGAL)
as a specific biomarker of acute kidney injury (AKI), diagnosed by an increase in the serum
creatinine (SCr) level of at least 0.3 mg/dL within 48 hours. Estimated GFR (eGFR) in the HP
group was > 60 mL/min. In the setting of AKI, CRRT was performed. Two patients were in the HP
Page 45
42
group, four patients were in the CRRT group and six patients were in the HP+CRRT group. All
clinical data were recorded and standardized in a spreadsheet by two critical care physicians who
were unaware of the purpose of this study.
Medical care in ICU
All patients received conventional ICU care including ventilator support, enteral or parenteral
nutrition, correction of water-electrolyte imbalances, intravascular fluid replacement, and control
of body temperature. Patients received hydroxychloroquine sulfate 400 mg twice-a-day on day 1
followed by 200 mg twice-a-day. To prevent untoward pulmonary injury patients were started on
atazanavir and ritonavir once daily for 7–14 days. Vancomycin (25 mg/kg loading dose, 15 mg/kg
twice-aday), imipenem (500 mg every six hours) IV infusion combined with azithromycin 500 mg
daily for three days were administered to treat the bacterial and atypical pneumonia.
Norepinephrine was administered in the range of 0.5 to 2.5 mcg/kg/min IV infusion to improve
blood perfusion and cardiac function.
The therapeutic effect was assessed via blood indices including arterial blood gas, PaO2 and O2
saturation, hemodynamic parameters (central venous oxygen saturation [ScvO2], oxygen delivery
[DO2]), plasma levels of three cytokines (interleukin 1 [IL1], interleukin-6 [IL6], and interleukin-8
[IL8]), and kidney function (blood urea nitrogen [BUN] and SCr). Acceptable treatment outcome
was defined as a marked improvement of ARDS severity demonstrated by increase in PaO2/FiO2
ratio, O2 saturation, DO2, ScvO2, improvement of renal function, and reduction of inflammatory
cytokines, norepinephrine, and ultimately improved mortality. The survival time was calculated
from the time of ICU admission to hospital discharge.
Blood purification
HP and/or CRRT therapies were initiated to improve O2 saturation and reduce proinflammatory
cytokine levels (10,11). Hemoperfusion (HP): Elevated IL-6 levels in ARDS patients with normal
kidney function suggested its role in lethal lung injury. HP was carried out with a cutoff value of
100 pg/mL (12) for IL-6, through femoral venous catheters at a blood flow rate of 100–300
mL/min. HP was implemented over six hours per day and the number of HP treatments was
determined by the plasma levels of the IL- 1, IL-6 and IL-8 along with clinical assessment of the
patient. A fully automated dialysis machine and a HA380 membrane filter (Jafron Biomedical Co)
were used for the HP.
Continuous renal replacement therapy (CRRT): Among patients with direct kidney involvement
and a high level of IL-6, the most important causative cytokine in ARDS, a recombinant
humanized anti-IL-6 monoclonal antibody, tocilizumab (8 mg/kg, at a maximum dose of 800 mg
per infusion, with an intravenous drip time longer than 1 h) was used to treat cytokine storm
followed by continuous venovenous hemofiltration (CVVH), whereas in the setting of AKI,
continuous venovenous hemodiafiltration (CVVHDF) was performed. CRRT was performed with
an ultrafiltration rate of 50–200 cc/h for 24 h every other day. A dedicated machine (PrismaFlex
system) and filter (ST150, Baxter) were used for the CRRT. The blood flow rate was set at 50–250
mL/min, and the dialysis rate was set at 25–35 mL/kg/h. Vascular access was obtained using arrow
double lumen hemodialysis (12 Fr × 20 cm) and central venous catheters (CV-15122-F) in the
femoral vein.
Combined hemoperfusion and continuous renal replacement therapy (HP+CRRT): In this group,
patients underwent CRRT plus HP using a HA380 membrane filter, which was changed routinely
after 6 hours over the course of 24 hours of CCRT due to the saturation of the adsorptive sites in
the aseptic technique step.
During each blood purifying technique, continuous infusion of heparin (ranging from 5 to 20
Page 46
43
units/kg/h) was used to prevent clotting. Therapeutic level was defined as an activated partial
thromboplastin time (aPTT) ranging between 15 and 20 times the normal.
Data collection
For every patient, sequential (sepsis-related) organ failure assessment (SOFA) score, and acute
physiology and chronic health evaluation II (APACHE II) score were calculated on the day of ICU
admission. Serum NGAL levels were measured using a commercially available ELISA kit
(Antibody Shop, Gentofte, Denmark). Ethylene diamine tetra acetic acid (EDTA) blood samples
were collected in sterile (endotoxin-free) tubes before and after the therapeutic techniques.
Samples destined for cytokine detection were placed in ice and transported immediately to the
laboratory. The plasma was separated by centrifugation (2000 ×g for 10 min) at 4 °C and stored in
300 µL aliquots at -70 °C until analysis. Serum concentrations of IL-1, IL-6, and IL-8 were
measured by ELISA using Quantikine kits. The minimum detectable concentration of all cytokines
with the R&D kits was less than 10 pg/mL. The operating procedure provided by the manufacturer
was strictly followed. Pulse contour cardiac output (PiCCO) was used to detect ScvO2 and DO2
through a central venous catheter and an arterial line. Measuring DO2 is dependent upon
hemoglobin/hematocrit, cardiac output, and saturation of the individual hemoglobin molecules.
The obtained blood samples were analyzed with an automatic biochemical analyzer for the
measurement of acute phase reactants (procalcitonin [PCT] and ferritin], kidney function (BUN,
SCr), and blood gas factors (PaO2, O2 sat) at the same time as cytokine level determination.
Data analysis
Results were presented as mean ± standard deviation. A P < 0.05 was considered statistically
significant. Categorical variables were analyzed using the chi-squared test. Other indices were
analyzed using ANOVA. To assess the relationship between the therapeutic techniques and the
mortality rate, multivariate Cox regression survival curves with the Cox proportional hazard model
were generated. The primary dependent variable was mortality. The treatment outcome was
recorded as categorical variables (1: Better; 0: Worse or death). Multivariate adjustment was made
separately for age, sex, ICU length of stay, time of the first treatment and number of treatments,
SOFA and APACHE II scores, ferritin, PCT, arterial blood gas indices, hemodynamic parameters,
and renal function tests.
RESULTS
Table 1 summarizes demographics and baseline characteristics of the patients. At baseline, there
was no significant difference (All Ps > 0.05) in age, sex, SOFA and APACHE II scores, ferritin,
PCT, and time of the first treatment between the three groups. A significant difference was seen the
mean SCr and BUN levels at baseline (Ps = 0.010 and 0.035, respectively). Changes in the
biochemical and hemodynamic parameters, cytokine levels, and blood gas factors are summarized
in table 2 showing before and after treatment measurements. With progression of hypoxemia,
multi-organ damage became a serious concern. There were significant differences in the mean
BUN, O2 sat (at a 0.10 level), and norepinephrine dosage (at a 0.05 level) among the three groups
over the study period. The CRRT group had the best result in clearing BUN and the HP+CRRT
group showed the best outcome on the improvement in O2 saturation and reduction of
norepinephrine dosage.
The median ICU length of stay was not different (P=0.737) between the three groups (7.5±2.1,
7.0±1.4, and 8.0±2.2 days for HP, CRRT, and HP+CRRT groups, respectively). The three groups
were also similar in the number of interventions they received (1.5 ± 0.7, 2.0 ± 0.0, and 3.0 ± 1.1
for HP, CRRT, and HP+CRRT groups, respectively). As shown in figure 1, CRRT and HP+CRRT
Page 47
44
groups were superior to HP in improving patients' PaO2, O2 sat, ScvO2, and DO2. Patients in the
HP+CRRT group demonstrated a marked improvement in IL-6 and IL-8 levels.
The overall mortality was 66.6% (8 out of 12 patients). Mortality rates were 50% in the HP
group (n=2), 100% in the CRRT group (n=4), and 50% in the HP+CRRT group (n=6). The
HP+CRRT group had the best overall primary and secondary outcomes. The Cox proportional
hazards model for overall survival is shown in figure 2.
Page 49
46
DISCUSSION
Acute lung injury and ARDS in COVID-19 patients have a higher mortality rate than what is
observed in other diseases. To date, the management of ARDS in COVID-19 patient remains
supportive, while no effective therapeutics, including antivirals or vaccines, is shown to improve
mortality. In previous studies, COVID-19 patients have received antimicrobial agents, antiviral,
antimalarial, and corticosteroid therapy with variable dosage depending on disease severity,
however, no effective outcomes is observed (13-15). Hence, our study was designed to evaluate the
blood purification therapies using HP, CRRT, and their combination on inflammatory mediator
elimination from plasma and improvement of survival. Significant elevation in plasma
inflammatory cytokines and chemokines was seen in severe COVID-19 patients, associated with
higher mortality rates in moderate-tosevere ARDS. HP, CRRT, and HP+CRRT techniques were
designed to remove cytokines and other circulating inflammatory mediators from the bloodstream.
An earlier study has demonstrated that increased plasma level of cytokines was associated with
extensive lung inflammation in COVID-19 pneumonia (16). IL-1 is the most important cytokine in
the early stage of ARDS, associated with increasing pro-inflammatory chemokines leading to
edema; and the therapeutic target could be achieved by removing it (17). Also, higher plasma
levels of IL-6 and IL-8 in bronchoalveolar lavage fluid are associated with a higher mortality rate
(18). We noted that patients with ARDS had higher levels of IL1, IL6, and IL8, probably leading to
an activated systemic inflammatory response. Moreover, patients requiring ICU admission had
higher concentrations of proinflammatory mediators than those not requiring ICU admission,
suggesting that the cytokine storm might play a crucial role in the severity of the disease (19).
The initial concentration of IL1, IL6, and IL8 was elevated and could be used as an index for
assessing the blood purifying techniques and hypoxemia prognosis. Therefore, in this study, we
divided patients into three groups (HP, CRRT, and HP+CRRT), and the measured cytokines were
evaluated to compare the efficacy of each techniques. Data from Italy and China showed
extracorporeal organ support therapies, including hemoperfusion, could remove plasma
inflammatory cytokines, broadly used in clinical settings to support hemodynamic and organ
function recovery (11,19). HP and CRRT achieved high solute clearance rates across a
semipermeable membrane and they could eliminate inflammatory mediators from the bloodstream
(9).
Page 50
47
Although it is still controversial whether HP or CRRT is beneficial in viral pneumonia, CRRT is
reported to have a positive effect on the reduction of the mortality risk in COVID-19 patients
requiring IMV, (10) while other studies found that CRRT is a risk factor for mortality in COVID-
19 (20). To compare the efficacy of HP and CRRT, we set up
groups based on the GFR cutoff, and further divided patients into three groups for comparing
plasma cytokine levels, blood gas factors, hemodynamic parameters, BUN,
SCr, and the mortality rate. There was no significant differences in the overall survival during ICU
stay among the three groups (P > 0.05). Our study has several limitations. First, the sample size
of this study was not large. Second, this was a single-center study. Although potentially more
patients could be involved in such a study, resource limitation is the main
factor limiting this investigation to only one center. Third, patient data was only available until
time of discharge which was included in the analysis. This study lacked long-term data.
CONCLUSION
The best clinical outcome in COVID-19 patients was observed in the HP+CRRT group which
not only had a comparatively better survival rate but also demonstrated better improvement in
plasma cytokine levels, blood gas factors, and hemodynamic parameters. Role of HP+CRRT
needs to be investigated in larger and preferably randomized studies.
Ethical Approval and Consent to participate
Clinical Research Ethics Committee approval was IR.SBMU.NRITLD.REC.1399.011. Patients
and/or next of kin provided consent for participation.
Consent for publication
Patients and/or next of kin provided consent for participation and publication of clinical data. All
authors approved the final manuscript and consented for publication.
Availability of supporting data
All the data provided in the manuscript no additional supporting data.
Competing interests
Not applicable.
Funding
Not applicable.
Acknowledgements
We wish to thank Jafron Biomedical Co. for providing all the required equipment for HP and
CRRT free of charge to COVID-19 patients.
REFERENCES
1. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of
adult inpatients with COVID- 19 in Wuhan, China: a retrospective cohort study. Lancet
2020;395(10229):1054-1062.
2. Phua J, Weng L, Ling L, Egi M, Lim CM, Divatia JV, et al. Intensive care management of
coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med
2020;8(5):506-517.
3. Zumla A, Hui DS, Azhar EI, Memish ZA, Maeurer M. Reducing mortality from 2019-nCoV:
host-directed therapies should be an option. Lancet 2020;395(10224):e35-e36.
Page 51
48
4. Jamaati H, Dastan F, Tabarsi P, Marjani M, Saffaei A, Hashemian SM. A Fourteen-day
Experience with Coronavirus Disease 2019 (COVID-19) Induced Acute Respiratory Distress
Syndrome (ARDS): An Iranian Treatment Protocol. Iran J Pharm Res 2020;19(1):31-36.
5. Gralinski LE, Baric RS. Molecular pathology of emerging coronavirus infections. J Pathol
2015;235(2):185-95.
6. Liu Y, Zhang C, Huang F, Yang Y, Wang F, Yuan J, et al Elevated plasma level of selective
cytokines in COVID-19 patients reflect viral load and lung injury. National Science Review
2020.
7. Blondonnet R, Constantin JM, Sapin V, Jabaudon M. A Pathophysiologic Approach to
Biomarkers in Acute Respiratory Distress Syndrome. Dis Markers 2016; 2016: 3501373.
8. McGonagle D, Sharif K, O'Regan A, Bridgewood C. The Role of Cytokines including
Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like
Disease. Autoimmun Rev 2020;19(6):102537.
9. Han F, Sun R, Ni Y, Hu X, Chen X, Jiang L, et al. Early initiation of continuous renal
replacement therapy improves clinical outcomes in patients with acute respiratory distress
syndrome. Am J Med Sci 2015;349(3):199-205.
10. Yang Y, Shi J, Ge S, Guo S, Xing X, Wang Y, et al. Effect of continuous renal replacement
therapy on all-cause mortality in COVID-19 patients undergoing invasive mechanical
ventilation: a retrospective cohort study. medRxiv 2020.
11. Ronco C, Navalesi P, Vincent JL. Coronavirus epidemic: preparing for extracorporeal organ
support in intensive care. Lancet Respir Med 2020;8(3):240-241.
12. Gong J, Dong H, Xia SQ, Huang YZ, Wang D, Zhao Y, et al. Correlation analysis between
disease severity and inflammation-related parameters in patients with COVID-19 pneumonia.
MedRxiv 2020.
13. de Wit E, van Doremalen N, Falzarano D, Munster VJ. SARS and MERS: recent insights into
emerging coronaviruses. Nat Rev Microbiol 2016;14(8):523-34.
14. Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical
Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia
in Wuhan, China. JAMA 2020;323(11):1061-1069.
15. Molina JM, Delaugerre C, Le Goff J, Mela-Lima B, Ponscarme D, Goldwirt L, et al. No
evidence of rapid antiviral clearance or clinical benefit with the combination of
hydroxychloroquine and azithromycin in patients with severe COVID-19 infection. Med Mal
Infect 2020;50(4):384.
16. Wong CK, Lam CW, Wu AK, Ip WK, Lee NL, Chan IH, et al. Plasma inflammatory cytokines
and chemokines in severe acute respiratory syndrome. Clin Exp Immunol 2004;136(1):95- 103
17. Hashemian SM, Mortaz E, Tabarsi P, Jamaati H, Maghsoomi
Z, Khosravi A, et al. Elevated CXCL-8 expression in bronchoalveolar lavage correlates with
disease severity in patients with acute respiratory distress syndrome resulting from
tuberculosis. J Inflamm (Lond) 2014;11:21.
18. Donnelly SC, Strieter RM, Kunkel SL, Walz A, Robertson CR, Carter DC, et al. Interleukin-8
and development of adult respiratory distress syndrome in at-risk patient groups. Lancet
1993;341(8846):643-7.
19. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with
2019 novel coronavirus in Wuhan, China. Lancet 2020;395(10223):497-506.
20. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill
patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective,
observational study. Lancet Respir Med 2020;8(5):475-481.
Page 52
Effectiveness of hemoperfusion (HP) in hemodialysis (HD)
patients with Covid-19 infection
49
Abstract
Introduction: The aims of this study are to observe clinical course of all patients affected by
infection with SARS-CoV-2 undergoing HD focusing on the impact of HP on them.
Methods: Patients divided to Group A: HD sessions with HP and Group B: patients without HP.
We registered all the data regarding patients’ clinical course.
Results: 13 patients have been enrolled in group A. 9 patients discharged from the hospital after
43 days (range: 35-56). 30 days were the mean hospitalization stay for the deceased ones. We did
not observe any side effects with HP cartridges. 9 patients did not receive HP during their
hospitalization. All of them were presented symptomatic. 8 out of 9 patients died after 6 days of
hospitalization (range: 1-14), 2 of them in ICU.
Conclusion: HP seems to be a helpful, safe and quite efficient tool in the battle against Covid-19
in HD patients.
Key words: hemodialysis, covid-19, hemoperfusion
Introduction
In December 2019 a new strain of coronavirus, officially named severe acute respiratory
syndrome coronavirus 2 (SARS-Cov-2), was first isolated from three patients with coronavirus
disease 2019 (covid-19) by the Chinese Center for Disease Control and Prevention connected to
the cluster of acute respiratory illness cases from Wuhan, China 1,2. On 30 January 2020, the
World Health Organization declared that the outbreak of SARS-Cov-2 constituted a public health
emergency of international concern.
End-Stage-Renal Disease patients under hemodialysis (HD) are at increased risk for
coronavirus disease 2019 (COVID-19) and its complications, owing to the presence of multiple
comorbid conditions. Patients receiving kidney replacement therapy are a vulnerable population as
those receiving dialysis are usually older with significant co-morbidity, have impaired immune
responses 3 and require regular attendance at a healthcare facility. The logistical aspects within a
dialysis facility further increase the risk of disease transmission 4. There are data suggesting a
more severe disease course in patients with chronic kidney disease (CKD) 5. Still outcomes in
End-Stage-Renal Disease patients under HD are unclear, with small case series suggesting a
milder course6. On the other hand HD patients are usually old and affected by several
comorbidities such as diabetes mellitus and hypertension that are known to be associated with high
risk of poor outcomes in patients with coronavirus disease 2019 (COVID-19).
Ioannis Griveas
Army Share Fund Hospital of Athens, Greece, 417 NIMTS
Address: 362 Kifisias Ave, 15233, Chalandri, Athens, Greece,
E-mail: [email protected]
07
Page 53
50
It has been demonstrated that at the beginning of sepsis process following Covid-19 invasion,
the overshoot of multiple pro-inflammatory mediators is frequently observed, and patient mortality
will be much higher when the serum level of pro-inflammatory and anti-inflammatory cytokines is
considerable 7,8. Blocking the overshoot of these inflammatory mediators can stop the sepsis
process and improve patient outcomes 8. One of the treatment approaches that can be taken to
reduce these cytokines is extracorporeal blood purification, also referred to as hemoperfusion
(HP)9. HP is an extracorporeal technique involving the passage of blood through a cartridge where
solutes are removed by direct binding to the sorbent material. HP acts by adsorption mechanism,
related to different cartridges which have been provided in its structure. The effectiveness of
hemoperfusion on serum level of IL-6, IL-8, IL-1β, and tumor necrosis factor has been
demonstrated in several studies10.
Our Nephrology Department during spring period on the first wave of COVID-19 was the
referral Dialysis Unit for Covid-19 positive HD patients in the district area of Athens, Greece. We
used HP as a therapeutic option in our patients. The aims of this study are to report characteristics,
rates and outcomes of all patients affected by infection with SARS-CoV-2 undergoing HD and
treated under our care focusing on the impact of HP on them.
Methods
This is an observational study. Our Dialysis Unit has been assigned as a referral unit for Covid-
19 positive HD patients. Patients divided to 2 groups: first group of patients underwent HD
sessions with Hemoperfusion (A) and the second one received HD sessions without any other
extracorporeal blood purification method (B). We used resin-directed hemoadsorption cartridges
(HA-330 and HA-130) manufactured by the Jafron Biomedical Company, China. We registered all
the data regarding the clinical course of our patients population. Age, primary cause of end stage
renal disease, weight, clinical presentation, HD history, outcome, days of hospitalization.
Results
22 Covid-19 positive HD patients were treated under the care of our facility during the period 8
April 2020-17 June 2020. 16 patients were symptomatic at admission and 13 patients admitted
with or developed during their stay pleural effusions. 12 patients (8 male) of our group died during
their hospitalization. 3 out of 12 were admitted to Intensive Care Unit (ICU). 6 patients were
septic, 4 had respiratory failure and 2 developed cardiovascular events. 14.5 days were the mean
hospitalization days (range: 1-38 days) for the diceased ones.
2 out of 3 patients that admitted to ICU had quick deterioration, incubated and stayed in ICU for
48 hours. The third one with severe cormobidities (multiple myeloma, cancer of bladder)
developed respiratory failure after 8 days of hospitalization, incubated, became septic and died
after 20 days in ICU.
Mean age of our patients was 74.5 years. It has to be pointed out that 13 patients were over 75
years old. Mean age was higher in those who died compared with those who were discharged with
double negative Covid-19 tests (79 vs 74,5 years old respectively). Median dialysis vintage for our
patients was 63 months and for the diceased ones was 89 months. Average weight of our patients
was 69 kgrs. Weight of diceased patients was 63 kgrs. 11 out of 22 patients and 5 out of 12
diceased patients were diabetic. 14 patients were hypertensive and 16 had official cardiovascular
backround. 10 out of total 22 patients under our care discharged after 43 days of hospitalization (
range:35-56 days).
Page 54
51
Group A
13 patients (4 males) have been enrolled in this group with mean age of 74 years old. 5 of them
were presented asymptomatic at admission and 7 of them admitted with or developed during their
stay pleural effusions. 4 of them were asymptomatic without effusions during the whole hospital
stay.
12 patients received HP for 3 hours in our Dialysis Unit during the planned HD session and one
patient received Hemoperfusion in ICU during CRRT.
6 patients had one session of Hemoperfusion (with HA130, 4 patients and with HA 330, 2
patients).
6 patients had 2 sessions (7 days interval) either with HA 130 both sessions (3 patients) or with
HA 330 followed 7 days after with HA 130 (3 patients).
The patients that admitted in ICU started HP the third day of her admission. The pattern was as
follows:
We used HA330 in 3 consecutive days during CRRT. In Day 10 we used HA130 and in Day 13
HA330. HP was performed for 3 hours.
24 days was the average hospitalization stay before starting HP for the 12 patients in boards. 9
patients discharged from the hospital after 43 days of hospitalization (range: 35-56 days). 30 days
were the mean hospitalization stay for the diceased ones.
We did not observe any side effects with HP cartridges (hypotension, reduction of platelets,
bleeding).
Group B
9 patients (7 males) with mean age of 75 years old did not receive HP during their
hospitalization. All of them were presented symptomatic. 8 out of 9 patients died after 6 days of
hospitalization (range: 1-14 days), 2 of them in ICU.
Discussion
To our knowledge this is the first study that demonstrates the experience of performing HP in
end-stage renal disease under HD patients without admission in ICU. Our general impression is
that the method definitely helped our patients without severe or minor side effects.
We all are familiar with the so called "cytokine storm syndrome" (CSS). In many life-
threatening conditions such as sepsis, if homeostasis has not restored, uncontrolled pro-
inflammatory response along with an unbalanced anti-inflammatory feedback causes production of
excess inflammatory mediators, particularly cytokines 11. Cytokines are a family of
immunoregulatory molecules that play roles in regulation of pro and anti-inflammatory responses.
Cytokine storm has been frequently reported to occur in severe COVID-19. Available data
suggest that elevated levels of mediators such as interleukin-6 (IL-6), IL-8, tumour necrosis factor
an others indicate a severe course or fatality of the disease 7. Accordingly, it has been recently
suggested to screen COVID-19 patients for cytokine storm and a secondary form of
hemophagocytic lymphohistiocytosis (HLH) 12. Identified patients may be candidates for anti-
inflammatory intervention, in order to mitigate an excessive host response and thereby reduce
organ damage.
In our patients population we used hemoperfusion cartridges HA130 and HA330 (Jafron,
China) which are among the widely used HP devices in China. The cartridges contain highly
biocompatible sorbents and neutro-macroporous resin made of styrene-divinylbenzene
Page 55
52
copolymer. HA 330 cartridges are mainly used in acute inflammatory conditions and HA 130
provide new therapeutic options for end-stage renal disease under HD patients (e.g cardiovascular
disease, increased CRP, TNF, IL, malnutrition etc).
Their adsorbing beads’ pore size ranged from 500 D to 60 kD, giving them the ability to absorb
various medium sized factors, including most inflammatory cytokines (IL-1, IL-6, IL-8, and TNF-
a) 13. The results of multiple studies
have demonstrated that application of HA 330 to eliminate circulating and alveolar levels of pro-
inflammatory cytokines in severe sepsis, septic shock, or acute lung injury patients significantly
improved patients’ hemodynamics, reduced the length of intensive care unit stay, and intensive
care unit mortality 13,14,15.
Cartridges which are used in hemoperfusion process are divided in selective and non-selective
types. The Jafron resin hemoperfusion cartridges are classified as nonselective group. These
cartridges are different based on the pore size distribution which determines their cutoff points for
adsorption of different materials, and makes them applicable for different clinical outputs; for
example HA-130 was used for improvement of uremic symptoms in chronic hemodialysis and HA-
330 was effective on modulation of severe inflammatory processes, as mentioned above.
As it has been pointed out at the beginning, the above study is the first one in end-stage renal
disease under HD patients with Covid-19 infection using HP. Our study groups were both similarly
old with severe cormobidities. The ones that received HP clearly benefited from the method.
Randomized trial data about the effectiveness of hemoperfusion in COVID-19 patients is lacking
in general, however, evidence shows that this therapeutic approach is tolerable
to most patients if conducted with the assistance of nephrology specialists, in order to minimize
side effects of the method which are generally rare 16. Despite our ratherly late start of the method
even patients that presented with severe clinical features, old in age, managed to overcome the
infection and discharge from the hospital.
Blood Purification therapies such as HP are proposed as promising adjunctive treatments,
designed for elimination of toxins and removal of inflammatory mediators. Even though a growing
body of evidence indicates the beneficial impact of their use, at this stage, there are controversial
reports on these techniques that should be explored 17. Our notice that corresponds with references
of the literature is that connection of HP and direct virus- mediated damage is not sufficiently
checked. Another query according to the literature data is whether HP can alter cytokine,
endotoxin or pathogen levels sufficiently. That is why form many researchers its biological
impact is unclear 18.
To sum up, HP seems to be a helpful, safe and quite efficient tool in the battle against Covid-19
in HD patients. Despite the method is unspecific, our lack of strong evidence, our views are with
the opinion that is an reliable alternative therapy. However, the real impact of HP on the patient’s
clinical course (time of initiation, therapeutic protocols, tools to evaluate response) has yet to be
determined. The above notice does not minimize the great interest for the method that renal
community should give.
BIBLIOGRAPHY
1. Zhu N, Zhang D, Wang W, et al, China Novel Coronavirus Investigating and Research Team.
A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med
2020;382:727-33. doi:10.1056/NEJMoa2001017
2. Gralinski LE, Menachery VD. Return of the Coronavirus: 2019-nCoV. Viruses
Page 56
53
3. Kato S, Chmielewski M, Honda H, Pecoits-Filho R, Matsuo S, Yuzawa Y, et al. Aspects of
immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol. 2008;3(5):1526–33.
4. Kliger AS, Cozzolino M, Jha V, et al. Managing the COVID-19 pandemic: international
comparisons in dialysis patients. Kidney Int. 2020;98:12–16.
5. Henry BM, Lippi G. Chronic kidney disease is associated with severe coronavirus disease
2019 (COVID-19) infection [e-pub ahead of print]. Int Urol Nephrol.
https://doi.org/10.1007/s11255-020-02451-9.
6. Wang R, Liao C, He H, et al. COVID-19 in hemodialysis patients: a report of 5 cases [e-pub
ahead of print]. Am J Kidney Dis. https://doi.org/10.1053/j.ajkd.2020.03.009.
7. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with
2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506.
8. Schadler D, Pausch C, Heise D, Meier-Hellmann A, Brederlau J, Weiler N, et al. The effect of
a novel extracorporeal cytokine hemoadsorption device on IL-6 elimination in septic
patients: a randomized controlled trial. PLoS One. 2017;12(10):e0187015.
9. Ronco C, Reis, T. Kidney involvement in COVID-19 and rationale for extracorporeal
therapies. Nat Rev Nephrol. 2020;16:308–10. https://doi.org/10.1038/s41581-020-0284-7.
10. Harm S, Schildbock C, Hartmann J. Cytokine removal in extracorporeal
blood purification: an in vitro study. Blood Purif. 2020;49(1–2):33–43.
11. Anand D, Ray S, Bhargava S, Das S, Garg A, Taneja S, et al. Proinflammatory versus anti-
inflammatory responsein sepsis patients: looking at the cytokines. Critical Care.
2014;18(Suppl 2):P13-P.
12. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ, Hlh Across
Speciality Collaboration UK. COVID-19: consider cytokine storm syndromes and
immunosuppression. Lancet. 395(10229):1033-4, 2020.
13. Ankawi G, Fan W, Pomare Montin D, Lorenzin A, Neri M, Caprara C, et al. A New Series of
Sorbent Devices forMultiple Clinical Purposes: Current Evidence and Future Directions.
Blood purification. 2019;47(1-3):94-100.
14. Huang Z,Wang SR, SuW, Liu JY. Removal of humoral mediators and the effect on the
survival of septic patients by hemoperfusion with neutral microporous resin column.
Therapeutic apheresis and dialysis : official peer reviewed journal of the International
Society for Apheresis, the Japanese Society for Apheresis, the Japanese Society for Dialysis
Therapy. 2010;14(6):596-602.
15. Huang Z, Wang SR, Yang ZL, Liu JY. Effect on extrapulmonary sepsis-induced acute lung
injury by hemoperfusion with neutral microporous resin column. Therapeutic apheresis and
dialysis : official peer-reviewed journal of the International Society for Apheresis, the
Japanese Society for Apheresis, the Japanese Society for Dialysis Therapy. 2013;17(4):454-
61.
16. Ma J, Xia P, Zhou Y, Liu Z, Zhou X, Wang J, et al. Potential effect of blood purification
therapy in reducing cytokine storm as a late complication of critically ill COVID-19. Clin
Immunol. 2020;214:108408.
17. Ankawi G, Neri M, Zhang J, Breglia A, Ricci Z, Ronco C. Extracorporeal techniques for the
treatment of critically ill patients with sepsis beyond conventional blood purification therapy:
the promises and the pitfalls. Critical Care. 2018;22(1):262.
18. Schadler, D. et al. The effect of a novel extracorporeal cytokine hemoadsorption device on
IL-6 elimination in septic patients:
Page 57
Clinical Outcomes of Hemoperfusion Using HA130 Cartridge
Among Maintenance Hemodialysis Patients in St. Luke’s
Medical Center-QC Dialysis Unit and Flora V Valisno De Siojo
Dialysis Center ofGat Andres Memorial Medical Center: A
Cross-sectional Study.
54
ABSTRACT
Objective: This study aimed to compare the clinical outcomes of patients who underwent
hemoperfusion using HA-130 cartridge with hemodialysis to those with hemodialysis alone among
maintenance hemodialysis patients in St. Luke’s Medical Center Quezon City dialysis unit and
Flora V Valisno De Siojo Dialysis Center of Gat Andres Bonifacio Memorial Medical Center from
August 2018–May 2019.
Methods: This cross-sectional study included 183 patients who underwent hemodialysis(HD) and
hemoperfusion(HP) using HA-130 cartridge and 156 patients on hemodialysis alone. Serum
phosphorous, albumin, hemoglobin, erythropoietin(EPO) dose, Kt/V, hospitalizations, and
mortality were compared from baseline, at the start and end of hemoperfusion when appropriate
and between these two groups.
Results: Significant differences in baseline characteristics were the patients in HD alone group
were older(p=0.002), predominantly had diabetic kidney disease(p=0.002), and hemoglobin of
<9.5 g/dl(p=0.0001). While most patients in HD+HP group had hypertensive
nephrosclerosis(p=0.003), with hemoglobin 9.5 to 11.5 g/dl(p=0.001) and >11.5 g/dl(p=0.038).
Main indication for hemoperfusion was an elevated serum phosphorous which was increased in
HD+HP group(p=0.0001). From baseline values, these variables improved after hemoperfusion:
EPO dose (mean=9448+3626.4 versus 10092+3405.6 units/week, p=0.050, 95%CI-1286.4 to-
0.95); hemoglobin (mean=10.8+1.5 versus 10.5+1.7g/dl, p=0.016, 95%CI 0.1to 0.7); and albumin
(mean=3.9+0.5 versus 3.7+0.6 g/dl, p=0.010, 95%CI 0.03to 0.2). There was no significant
difference with phosphorous (mean=2.04+0.7 versus 2.08+0.6mmol/L, p=0.520, 95%CI-0.2 to
0.1) at the end of the study, although there was a significant difference in the second and third
months of treatment(p=0.0001). At the end of the study; albumin(p=0.0001, 95%CI-0.4to-0.03)
and hemoglobin(p=0.0004, 95%CI-1.0 to-0.3) were significantly higher in HD+HP group. The
percentage of patients with hemoglobin <9.5 g/dl was significantly lower(p=0.0001) in HD+HP
group(10.9%) than in HD alone group(34.2%). Although the phosphorous in HD alone group was
lower(p=0.017, 95%CI -0.4to-0.03) than in HD+HP group, it increased in HD alone group from
baseline(mean=1.84+0.70 versus 1.56+0.66mmol/L). There was no significant difference in EPO
dose (p=NS) and Kt/V(p=NS) in both groups. Hospitalization rate OR=4.23(p=0.0104, 95%CI
1.93 to 9.27) and mortality rate OR=4.07(p=0.0001, 95%CI 1.30 to12.75) such that patients in HD
alone group were four times more likely to be hospitalized and to die than those in HD+HP group.
Conclusion: Patients who underwent hemodialysis and hemoperfusion using HA-130 cartridge
Floin Jade M. Quibo-Galvadores, MD Arlene C. Crisostomo, MD, MSc, MMHoA, FPCP, FPSN
Department of Medicine, SECTION OF NEPHROLOGY St. Luke’s Medical Center – Quezon City, 279 E.
Rodriguez Sr. Boulevard, New Manila, Quezon City, Philippines
08
Page 58
55
had a lower risk of hospitalization and mortality than those on hemodialysis alone. There were
significant improvements in hemoglobin, erythropoietin dose, albumin, and phosphorous values
from baseline in HD+HP patients.
Keywords: Hemodialysis, hemoperfusion, hemoglobin, phosphorous, albumin, EPO
1. INTRODUCTION
Hemodialysis is the most common treatment of patients with End Stage Renal Disease
(ESRD). It effectively removes small water-soluble molecules that circulate without significant
protein binding. Molecules that are larger and/or protein-bound are much more difficult to remove
[1]. These molecules are uremic toxins that are classified by the European Uremic Toxin Work
group into three major categories: (a) small, water-soluble molecules such as urea and creatinine,
which can be efficiently removed by HD; (b) middle molecules larger than 500 Da such as
parathyroid hormone, 2-macroglobulin and C reactive protein (CRP), which can be removed by
peritoneal dialysis or high-flux HD or hemofiltration (HF); and (c) protein-bound molecules such
as phenolic and indolic compounds, homocysteine that are difficult to remove via HD or HF.
Studies have shown that these uremic toxins are associated with significant morbidity and
mortality in ESRD patients [2]. Clinical applications of various models of extracorporeal blood
purification technology show the clearance rates of middle and large uremic toxins in the
following descending order: hemodialysis (HD) + hemoperfusion (HP) > HP alone >
hemodiafiltration (HDF) > hemofiltration (HF) > HD.
Hemoperfusion (HP) is the removal of uremic toxins through adsorption wherein there is
direct contact of the molecules with activated charcoal or resin [3]. HA cartridges particularly HA-
130 were found to be effective in reducing uremic symptoms in chronic hemodialysis (HD)
patients. In a randomized controlled trial by Li et al., HP combined with HD resulted in
improvement of pruritus score (p < 0.05) and decreased parathyroid hormone (p<0.05) and calcium
phosphate product (p<0.05) [4].
In a prospective, randomized, controlled trial involving 100 maintenance hemodialysis patients
by Chen et al, HP (using HA-130 cartridge) combined with HD was found to be superior in
removing middle and large molecules. Serum concentration levels of patients’ leptin, hsCRP,
iPTH, IL-6, B2-MG and TNF alpha significantly dropped (p<0.05 respectively) in HP combined
HD group compared to HD alone after a 2-year study period. Systolic blood pressure,
erythropoietin doses, and number of antihypertensive drug used were lower in HP combined HD
group (p<0.05 for all) than in the control group. HP combined with HD patients had higher values
of hemoglobin (p<0.01). This study also showed that at the end of the 2-year study period, HP
combined with HD group had higher total score of quality of life assessment and lower mortality
rate compared with HD alone (p<0.01for both) [3].
No local studies have evaluated the clinical outcomes of maintenance hemodialysis patients
using HA-130 cartridge combined with hemodialysis hence this study. This is a dual center study
involving St. Luke’s Medical Center, Quezon City and Flora V Valisno De Diojo Dialysis Center
of Gat Andres Bonifacio Memorial Medical Center. St Luke’s Medical Center, Quezon City is a
leading tertiary academic hospital with a dialysis unit that can accommodate 13 patients per
treatment shift with 500 – 600 treatments a month. Gat Andres Bonifacio Memorial Medical
Center is a primary government hospital that offers free medical services to Manila residents. It
has a 150-200 bed capacity and is located in Tondo, Manila. It’s outpatient dialysis unit, called
Flora V Valisno De Siojo Dialysis Center, during this study period had 55 patients per treatment
shift with 3500-3700 treatments a month.
1.1 Significance of the study
Page 59
56
Despite the advancement in blood purification technology, the mortality rates of maintenance
hemodialysis patients is still high with cardiovascular disease as the leading cause of death. Large
middle molecules are a diverse group of uremic toxins that contribute significantly to the high
cardiovascular disease burden and are associated with significant morbidity and mortality in
patients with ESRD. Hemodialysis can effectively remove small and middle molecules through
diffusion and convection. However, larger and protein bound molecules cannot be eliminated via
hemodialysis or hemofiltration [5]. Hemoperfusion allows for removal of uremic toxins by direct
contact with activated charcoal or resin via adsorption. Hence combination of hemoperfusion and
hemodialysis can effectively eliminate all uremic toxins associated with increased cardiovascular
risk. This study determined the clinical outcome of maintenance hemodialysis patients who
underwent combined hemoperfusion using HA-130 cartridge and hemodialysis in St. Luke’s
Medical Center Quezon City dialysis unit and Flora V Valisno De Siojo Dialysis Center of Gat
Andres Bonifacio Memorial Medical Center from August 2018 to May 2019.
1.2 Rationale for doing the study
Results from previous small-scale studies demonstrated that hemoperfusion combined with
hemodialysis is an effective approach to remove small water-soluble solutes, middle molecules
and protein bound uremic toxins. With the effective removal of uremic toxins, HP plus HD will
improve clinical outcomes of maintenance hemodialysis patients. With these promising results,
the researchers were encouraged to further investigate the effect of combined hemoperfusion with
hemodialysis among our End Stage Renal Disease Filipino patients.
1.3 Background of the study and brief literature review
Adsorption, a complementary mechanism for solute removal, relies on direct binding of solutes
to membranes or sorbent materials contained within a cartridge (adsorption unit). Adsorption can
be applied both alone and in combination with other blood purification techniques. An important
characteristic of sorbent materials is minimizing unwanted molecule loss (such as nutrients and
antibiotics), which is frequently encountered using other extracorporeal blood purification
techniques [6]. The sorbent devices have the ability to remove endogenous and exogenous
materials such as middle uremic toxins, protein bound uremic toxins, hydrophobic or protein
bound exogenous substances, cytokines, complements, free hemoglobin, and residual drugs by
means of adsorption [7]. HA cartridges, HA-130 in particular, were found to be effective in
reducing uremic symptoms in chronic hemodialysis patients.
In a randomized controlled trial done by Li et al. involving 90 maintenance hemodialysis
patients diagnosed of uremic pruritus, HP combined with HD not only resulted in improvement of
pruritus in comparison to HD alone (p < 0.05) but also decreased parathyroid hormone and calcium
phosphate product (p < 0.05) [4].
In a prospective randomized controlled trial done by Chen et al involving 100 maintenance
hemodialysis patients followed for total of 2 years, there was significant improvement in the
combined HP using HA-130 with HD in terms of blood pressure control (p<0.05), erythropoietin
dose (p<0.05), and hemoglobin levels (p<0.05). There was significant decrease in the serum
concentration of leptin, hsCRP, iPTH, IL-6, B2-MG and TNF alpha (p<0.05, respectively) at the
end of the 2-year observation period. There was also significant improvement in the quality of life
(p<0.05) in the HP combined with HD group. There was significant reduction in 2-year mortality
rate (p<0.05) in the HP plus HD group compared to control group [3].
In a retrospective cohort study done by Lu et al with 150 maintenance hemodialysis patients,
serum calcium and phosphorous levels were significantly lower in the HP (using HA-130)
combined with hemodialysis group compared to hemodialysis alone after six months of treatment
Page 60
57
(p<0.05). FGF-23 and iPTH were also found to be significantly decreased in the HP combined
with HD group after six months of treatment(p<0.05) [8].
2. OBJECTIVES:
General Objective:
To compare the clinical outcomes of hemodialysis patients who underwent hemoperfusion
using HA-130 cartridge (HD + HP) to those who underwent hemodialysis (HD) alone among
maintenance hemodialysis patients in St. Luke’s Medical Center Quezon City dialysis unit and
Flora V Valisno De Siojo Dialysis Center of Gat Andres Bonifacio Memorial Medical Center
from August 2018 – May 2019.
Specific Objective:
To compare the clinical outcomes of hemodialysis patients who underwent hemoperfusion
using HA-130 cartridge to those who underwent hemodialysis alone among maintenance
hemodialysis patients in St. Luke’s Medical Center Quezon City dialysis unit and Flora V
Valisno De Siojo Dialysis Center of Gat Andres Bonifacio Memorial Medical Center from
August 2018 – May 2019 in terms of:
a. Mean and median serum phosphorous
b. Mean and median erythropoietin dose
c. Mean and median hemoglobin level
d. Mean and median serum albumin
e. Percentage of anemia with hemoglobin levels less than 9.5 g/dl; 9.5 to 11.5 g/dl; >11.5 g/dl
f. Number of Hospital admissions
g. Percentage of Mortality
3. METHODOLOGY
3.1 Study design and population
This is a cross-sectional study of adult maintenance hemodialysis patients who underwent
hemoperfusion using HA-130 cartridge combined with hemodialysis at least twice and those who
underwent hemodialysis alone in St. Luke’s Medical Center Quezon City dialysis unit and Flora
V Valisno De Siojo Dialysis Center of Gat Andres Bonifacio Memorial Medical Center from
August 2018 – May 2019.
3.2 Inclusion and Exclusion Criteria
3.3 Operational Definitions:
Hemoperfusion - is an extracorporeal blood purification modality that consists of the passage of
anticoagulated whole blood through a device, usually a column, that contains adsorbent particles
Page 61
58
[9]. It allows removal of uremic toxins by direct contact with activated charcoal or resin via
adsorption.
HA-130 – is a sorbent device that has the ability to remove endogenous and exogenous material
such as uremic toxins by means of adsorption. It is mainly used in chronic conditions.
Maintenance Hemodialysis – is a process of purifying blood and the most common renal
replacement modality for ESRD patients.
Hyperphosphatemia – serum phosphorous value above 4.5 mg/dl (1.45 mmol/L)
Mean and Median serum phosphorous – average and middle value of serum phosphorous in
patients who underwent hemoperfusion using HA-130 combined with regular dialysis and patients
who had hemodialysis alone.
Mean and median erythropoietin dose - average and middle value of erythropoietin dose in
patients who underwent hemoperfusion using HA-130 combined with regular dialysis and patients
who had hemodialysis alone.
Mean and median hemoglobin level - average and middle value of hemoglobin level in patients
who underwent hemoperfusion using HA-130 combined with regular dialysis and patients who
had hemodialysis alone.
Percentage of anemia with hemoglobin levels less than 9.5 g/dl; 9.5 to 11.5 g/dl; >11.5 g/dl –
number of patients with hemoglobin levels less than 9.5 g/dl, 9.5 to 11.5 g/dl, >11.5 g/dl
respectively divided by total number of patients in each group (patients who underwent
hemoperfusion using HA-130 combined with regular dialysis and patients who had hemodialysis
alone) multiplied by 100.
Hospital admissions mean and median – average and middle value of the number of hospital
admissions in patients who underwent hemoperfusion using HA-130 combined with regular
dialysis and patients who had hemodialysis alone.
Percentage of Mortality – number of death of patients divided by total number of patients in each
group (patients who underwent hemoperfusion using HA-130 combined with regular dialysis and
patients who had hemodialysis alone) multiplied by 100.
3.4 Description of Study Procedure
3.4.1 Method of subject selection
Data from the quality assurance report of patients who had HD alone and those who
underwent HD + HP at least twice from August 2018 to May 2019 in St. Luke’s Medical Center
dialysis Unit and Flora V Valisno De Siojo Dialysis Center of Gat Andres Bonifacio Memorial
Medical Center were obtained and included in the study. Hemodialysis alone group served as the
control group.
3.4.2 Data Gathering
This study included demographic data such as age, sex, duration on hemodialysis, and
causes of renal failure such as hypertension, diabetes mellitus, and chronic glomerulonephritis.
Laboratory data included mean and median hemoglobin, serum albumin, serum phosphorous,
erythropoietin dose, hospital admissions, mortality, and Kt/V.
3.4.3 Sample Size Estimation
Using the study of Lu, et al [8], the change in phosphorous of 15% among hemoperfusion
combined with hemodialysis patients in China, a total of 195 hemodialysis patients per group (HD
+ HP, HD alone) were needed as shown in the formula below:
Page 62
59
for a total sample size of 390 patients.
3.4.4 Subject recruitment process
The quality assurance forms included data like age, sex, years on dialysis, causes of end
stage renal disease, number of hospital admissions and mortality. They also included laboratory
data like hemoglobin levels, erythropoietin dose, serum albumin, serum phosphorous, and
adequacy of dialysis expressed as Kt/V. Quality assurance data of patients that fulfilled the
inclusion criteria were included in the study.
3.4.5 Study procedures
The quality assurance data forms were reviewed. The independent variables included age,
sex, number of years on dialysis, and causes of end stage renal disease. Dependent variables
included serum phosphorous and albumin, erythropoietin dose, hemoglobin levels, number of
hospital admissions, and mortality rates of patients who underwent hemoperfusion using HA-130
combined with regular dialysis and patients who had hemodialysis alone.
3.4.6 Description of Outcome Measures
The primary outcomes in this study included the mean and median serum phosphorous,
mean and median erythropoietin dose, mean and median hemoglobin, mean and median serum
albumin, percentage of anemia, number of hospital admissions, and percentage of mortality of
patients.
3.4.7 Data Analysis
Demographic and clinical characteristics were reported as frequencies and percentages for
nominal/categorical variables, and mean difference and standard deviation for numerical variables.
Paired t-test was used to compare numerical values before and after the treatment. In
comparing all months, ANOVA on repeated measures was utilized. Chi-square/fisher test with
odds ratio was used to determine the association of hospitalizations and mortality with treatment.
P-values of equal to or less than 0.05 was considered statistically significant. Medcalc Statistical
software was used to carry out computations.
3.4.8 Ethical Consideration
The study abided by the Principles of the Declaration of Helsinki (2013) and was conducted
along the Guidelines of the International Conference on Harmonization – Good Clinical Practice
(ICH-GCP). The Clinical Protocol and all relevant documents were reviewed and approved by the
SLMC Institutional Ethics Review Committee. There was no violation of data privacy because no
patient identifiers were present since monthly quality assurance reports were used.
All study data were recorded and investigators are responsible for the integrity of the data
i.e. accuracy, completeness, legibility, originality, timeliness, and consistency. The manner of
disseminating and communicating the study results guaranteed the protection of the confidentiality
of the patient’s data. All study-related documents such as all versions of the protocol, ethical
clearance, data collection forms hard copies of source documents, were kept and stored by the
Principal Investigator in strict confidentiality for at least 5 years, after which they will be shredded.
Page 63
60
4. RESULTS:
A total of 183 dialysis patients underwent HD + HP using HA130 and 156 HD alone
patients were included in the study. The baseline characteristics of patients are shown in Table 1.
Patients under HD + HP group were significantly younger (51 years old) than HD patients alone
(56 years old). Male gender was predominant for both groups. No significant difference existed on
duration of ESRD. There were more patients with ESRD secondary to Hypertensive
nephrosclerosis in the HD + HP group compared to HD alone group (39.3% vs 24% respectively,
p=0.003). While those with ESRD secondary to diabetic kidney disease was significantly higher
for hemodialysis alone patients than HD + HP (49.4% vs 32.8% respectively, p=0.002).
Phosphorous was significantly lower among patients in the hemodialysis alone group compared to
HP + HD (p=0.0001) at the start of the study. Percentage of patients with hemoglobin less than 9.5
g/dl was higher in HD alone group (p=0.0001).
There was a significant difference in terms of hemoglobin levels (p=0.016), erythropoietin
(EPO) dose per week (p = 0.050) and serum albumin (p = 0.0095) before and after treatment of
hemoperfusion using HA-130 (Table 2). A non-statistically significant downward trend for serum
phosphorous at the end of treatment was seen (p = 0.520). Percentage of patients with hemoglobin
Page 64
61
less than 9.5 g/dl was significantly lower at the end of the treatment (p= 0.033).
Table 3 shows a downward trend in the level of serum phosphorous although there was no
significant difference at the end of treatment (4th month) with hemoperfusion. However, the
serum, phosphorous was significantly lower in the 2nd and 3rd months of treatment. Serum
albumin and, hemoglobin levels were significantly higher in the 3rd and 4th months of treatment
together with significantly lower doses of erythropoietin.
Comparing HD + HP group and HD alone group at the end of treatment (Table 4), there
was a significant difference in the serum phosphorous levels (p = 0.017). Serum albumin and
hemoglobin levels (p= 0.0001, p = 0.0004 respectively) were significantly higher in the HD + HP
group than HD alone group. Kt/V and EPO dose (p = 0.766, p = 0.3697 respectively) did not have
Page 65
62
significant difference in the HD+HP group and HD alone group. Percentage of patients with
hemoglobin less than 9.5 was significantly higher in the HD alone than HD + HP group (34.2 %
vs 10.9 %, p = 0.0001).
The number of hospitalizations and percentage of mortalities were significantly lower (p
<0.05) in the HD + HP group compared to those in the HD alone group (Table 5). Those who were
treated with HD alone were four times more likely to be hospitalized or to die as compared to
those who were treated with HD + HP.
5. DISCUSSION
The reduction in serum phosphorous levels, EPO doses, and significant improvement with
Page 66
63
hemoglobin and albumin levels at the end of the study among patients in the HD + HP group
compared to those in the HD alone group may be due to the removal of toxins including
proinflammatory cytokines by HP, as these protein-bound small molecules, middle and large
molecules are not efficiently removed by hemodialysis alone.
The reduction in serum phosphorous with HP is similar to the study done by Li, et al [4],
in which there was a significant decrease in serum phosphorous levels at the end of 4 weeks of
treatment (p<0.05) with one hemoperfusion treatment given every 2 weeks. Lu, et al also reported
significant improvement in the serum phosphorous of hemodialysis patients treated with
hemoperfusion after 6 months of treatment (p < 0.05). While phosphorous is a small molecular
substance, it often forms a complex with other macromolecular substances making its clearance
with hemodialysis alone limited [8]. In this study, serum phosphorous was significantly reduced
in the second and third months of treatment. However, at the end of the fourth month, there was
an increase in the levels of serum phosphorous among the HD + HP group making the difference
from the start of study insignificant. This could be probably due to complacency of the patients in
observing a low phosphorous diet.
In our study, anemia was more prevalent among the HD group alone. An important cause
is the presence of systemic inflammation which leads to functional iron deficiency and inhibition
of erythrocyte maturation by proinflammatory factors like TNF-alpha and IL-6. A combination of
hemodialysis and hemoperfusion not only ensured the thorough clearance of small molecule toxins
but also the removal of middle and large molecules which would help alleviate systemic
inflammation and increase the effect of treatment on uremic anemia [3]. As shown in our study,
there is a significant increase in the hemoglobin levels of patients at the end of treatment.
Similarly, in a study done by Chen, et al; patients who were treated with hemoperfusion had a
significant increase in the hemoglobin levels from baseline [3].
Systemic inflammation among hemodialysis patients affects serum albumin levels. There
is a relationship between an increase in the blood levels of inflammatory markers and a decrease in
albumin levels [11]. Hemoperfusion adsorbs middle and large molecules including inflammatory
cytokines [3]. Hence alleviation of inflammation with HP could lead to improved
serum albumin levels as observed in our study.
Despite similar Kt/V in both HD + HP group and HD alone group, the increased number
of hospitalizations and percentage of mortality among patients in the HD alone group could be due
to retention of a wide range of small protein-bound molecules, middle and large molecules
including inflammatory cytokines - molecules not well removed by dialysis alone. Chen, et al
reported a significant decrease (p<0.05) in the inflammatory markers (hsCRP, iPTH, IL-6, beta2-
MG, TNF-alpha) of patients who had hemoperfusion at the end of treatment. There was also a
higher total score of quality of life and lower mortality rate in the HD + HP group compared with
the HD alone group. Reduction in the inflammatory markers also led to better control of blood
pressure and heart rate which can lead to decreased cardiovascular events [3]. Effective removal
of uremic toxins of combined hemodialysis and hemoperfusion leads to a better prognosis.
This study showed that patients in the HP + HD group were four times less likely to be
hospitalized and die. The same findings were found in a study by Dung et al, wherein the
combination of HD and HP helped to reduce the cardiovascular-related mortality rate after a 3-
year follow-up. Mortality rate in the HD + HP group was 4.3 % while in HD alone group, the
mortality was 17% (p = 0.049) [12]. In another study by Yan, et al; during the 24-month followup
period, HD + HP group had a lower number of first hospitalizations compared to HD alone
group (20 out of 78 patients in the HD + HP group while in HD group, 31 out of 80 patients were
hospitalized) where infectious diseases and cardiovascular events were the main causes for
hospitalizations. Fifteen patients died during the 24-month follow-up period (3 in the HD + HP
.
Page 67
64
group; 12 in the HD group) with cardiovascular diseases, cerebrovascular events, and pulmonary
infections being the main reasons for mortality [13]. In our study, however, causes for
hospitalizations and mortality were not specified in the monthly quality assurance reports of most
dialysis patients.
Another factor that could also contribute to the increased hospitalization and mortality was
the significant number of patients with diabetic kidney disease in the HD alone group. Studies
have shown that the survival rate among diabetic hemodialysis patients is significantly lower than
their non-diabetic counterparts. Beladi-Mousavi, et al reported the one-year survival rate was
significantly lower among diabetic HD patients (79.2% versus 85%, p = 0.01) [14]. Another study
by Soleymanian, et al, the annual hospitalization rate was higher in diabetic hemodialysis patients
(median: 0.86 versus 0.43, p = <0.001). The death rate was two folds higher in diabetics (24 versus
12 per 100 patient-years). Cardiovascular diseases comprised 80.5% of death in diabetics and
54.5% in non-diabetics [15].
Other factors to consider for increased morbidity and mortality are older age and higher
prevalence of anemia among patients in the HD alone group. In a study by Locatelli, et al; dialysis
patients with hemoglobin <10 g/dl were 29% more likely to be hospitalized than those with
hemoglobin 11 – 12 g/dl (p<0.001) [16]. As to older age, studies have shown that age is associated
with mortality among hemodialysis patients. Msaad, et al reported that survival was higher in
younger dialysis patients (p=0.001). Patients aged over 65 are 1.26 times more likely at risk
to die than patients under 65 years of age (p=0.002) [17].
6. LIMITATIONS OF THE STUDY
The data were obtained from monthly quality assurance reports. Reasons for
hospitalizations and causes of mortality were not specified. The indication for hemoperfusion was
elevated serum phosphorous. This would explain the markedly elevated serum phosphorous levels
in the HD + HP group than in the HD alone group. Furthermore, there were significant differences
in the baseline characteristics of the patients which could not be addressed by the cross-sectional
study design. And this study did not include other inflammatory markers such as hsCRP, beta2-
MG, TNF-alpha which would affect the prognosis and well-being of HD patients. It did not include
other markers of Chronic Kidney Disease-Metabolic Bone Disorder such as calcium, iPTH, FGF-
23, and vitamin D levels.
7. CONCLUSION
Patients in the hemodialysis with hemoperfusion group had a lower risk of hospitalization
and mortality compared to those in the HD alone group. There were significant improvements in
the laboratory parameters of HF + HD patients in terms of hemoglobin levels, erythropoietin dose,
serum albumin, and serum phosphorous.
8. RECOMMENDATIONS
It is recommended to do a large randomized prospective trial with longer duration of study.
Laboratory parameters like hsCRP, beta2-MG, TNF-alpha levels, calcium, iPTH, FGF-23,
vitamin D levels may also be included in the study to further evaluate the efficiency of
hemoperfusion among maintenance hemodialysis patients.
Page 68
65
9. REFERENCES:
1. Wolley, MJ., Hutchison, CA: Large Uremic Toxins: an unsolved problem in end-stage
kidney disease; Nephrol Dial Transplant (2018) 33: iii6–iii11
2. Vanholder R, De Smet R, Glorieux G, et al. Review on uremic toxins: classification,
concentration, and interindividual variability. Kidney Int 2003;63:1934–43
3. Chen SJ, Jiang GR, Shan JP, Lu W, Huang HD, Ji G, et al: Combination of maintenance
hemodialysis with hemoperfusion: A safe and effective model of artificial kidney. Int J
Artif Organs 2011; 34: 339–347
4. Li WH, Yin YM, Chen H, et al. Curative effect of neutral macroporous resin
hemoperfusion on treating hemodialysis patients with refractory uremic pruritus. Medicine
2017;96: e6160.
5. Matsushita K, van der Velde M, Astor BC, et al. Association of estimated glomerular
filtration rate and albuminuria with all-cause and cardiovascular mortality in general
population cohorts: a collaborative meta-analysis. Lancet 2010;375:2073–81
6. Clark WR, Ferrari F, La Manna G, Ronco C: Extracorporeal sorbent technologies: basic
concepts and clinical application. Contrib Nephrol 2017; 190: 43–57
7. Pomarè Montin D, Ankawi G, Lorenzin A, Neri M, Caprara C, Ronco C: Biocompatibility
and Cytotoxic Evaluation of New Sorbent Cartridges for Blood Hemoperfusion. Blood
Purif 2018; 46: 187–195
8. Lu Hua, Wei Qingmin, Guo Gengxin, Liu Qian, Wang Mingming: Effects of different
blood purification techniques on interleukin-28 and mineral levels in patients. Int J Clin
Exp Med 2018;11(10):11198-11204
9. www. Uptodate.com
10. Winchester JF, Silberzweig J, Ronco, C: Sorbents in Acute Renal Failure and End-Stage
Renal Disease: Middle Molecule and Cytokine Removal. Blood Purif 2004; 22:73–77
11. Fouque D, Mitch WE. (2016). Brenner & Rector’s The Kidney. 10th ed. USA: Elsevier,
Inc.
12. Dung NH, Quyen DBQ, Hai NTT, et al: A Combination of Hemodialysis with
Hemoperfusion Helped to Reduce the Cardiovascular-Related Mortality Rate after a 3-
Year Follow-Up: A Pilot Study in Vietnam. Blood Purif 2020 Jul 2;1-8
13. Yan HG, Xiu HY, Li HP et al: Additional Hemoperfusion is Associated with Improved
Overall Survival and Self-Reported Sleep Disturbance in Patients on Hemodialysis. The
International Journal of Artificial Organs 2019, feb 1-7 DOI: 10.1177/0391398819837546
14. Beladi Mousavi SS, Alemzadeh Ansari MJ, Alemzadeh Ansari MH, BeladiMousavi M.
Long-term survival of patients with end-stage renal disease on maintenance hemodialysis.
A multicenter study in Iran. Iran J Kidney Dis. 2012; 6:452-6.
15. Soleymanian T, Kokabeh Z, Mahjoub A, Ramaghi R, Argani H. Clinical outcomes and
quality of life in hemodialysis diabetic patients versus non-diabetics. J Nephropathol.
2017;6(2):81-89. DOI: 10.15171/jnp.2017.14.
16. Locatelli F, Pisoni R, Combe C, Bommer J, et al: Anaemia in haemodialysis patients of
five European countries: Association with morbidity and mortality in the Dialysis
Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant. 2004 Jan;
19(1):121-32.
17. Msaad R, Essadik R, Mohtadi K, Meftah H, Lebrazi H, et al: Predictors of mortality in
hemodialysis patients. Pan Afr Med J. 2019; 33:61
Page 69
Combination Hemodialysis- Hemoperfusion: Provides benefit
to dialysis patients?
66
Objective: Classic dialysis (HD) with low flux membranes does not provide adequate clearance of
the middle molecular uremic toxins (MMB). Investigated the possibility of better removal of
parathormone (iPTH) and β2-microglobulin (β2Μ) in combination with low flux HD and
hemoperfusion (HP).
Material and methods: Were studied for 6 months, 12 hemodialysis men patients, dialyzed with
low-flux polysulfone membranes, without infections, malignancies / hematological disorders,
under constant treatment for anemia and hyperparathyroidism. Were randomized to 2 groups of 6
patients: group A (HD+HP) and group B only HD. To patients of group A added a cartridge HP
type HA130 with the dialyzer once a week for the 1st month, once every 2 weeks for the 2nd
month and once a month for 4 months. A 3rd group C studied at the same time, with 6 men
received on line hemodiafiltration (OL-HDF). In all patients measured the serum levels of β2Μ
and iPTH in months 0 (M0) and 6 (M6), before (preD) and after (postD) the second weekly
session.
Results: The levels of preD- β2Μ were similar in groups A and B at M0 and M6. In group C were
lower in comparison with group A at M0 (p=0,008) and at M6 (p=0,02). The levels postD- β2Μ
decreased significantly in group C at M0 (p<0,001) and at M6 (p<0,001) and the improvement/
reduction was maintained, with no difference between M0-M6. Improvement/ reduction of the
levels of β2Μ between M0-M6 found only in group A (p=0,03) and not to group B. The levels of
preD- iPTH did not differ between group A, B, C at M0 (p=NS) and at M6 (p=NS). The levels post
D- iPTH decreased at M6 in group A (p=0,04), not at group B and were a marginal decrease in
group C (p=0,05), with marginal improvement of the reduction between M0-M6 in group C
(p=0,046).
Conclusions: OL-HDF is undoubtedly the most effective method of purification of uraemic toxins
(MMB), but also the combination HP-low flux HD seems more effective than low flux HD alone,
so it could be useful in daily clinical practice.
References:
1. Lesaffer G., De Smet R., Lameire N., et al. Intradialytic removal of protein-bound uraemic
toxins: role of solute characteristics and of dialyser membrane. NDT 2000; 15:50-7
2. Ikuto Masakane and Kenji Sakurai. Current approaches to middle molecule removal: room for
innovation Nephrol Dial Transplant. 2018; 33(Suppl 3): iii12-iii21
3. Li WH, Yin YM, Chen H et al. Curative effect of neutral macroporous resin hemoperfusion on
treating hemodialysis patients with refractory uremic pruritus. Medicine (Baltimore) 2017;
96:e6160.
M. Sonikian, E. Karakou, A. Velentza, A. Barbatsi, Th. Chiras, M-E Papadaki, P. Arvanitakis, N.
Trakas, M. Martsoukou
Renal Unit, Biochemical Laboratory, Biopathology Laboratory of Sismanogleio General Hospital of Athens.
09
Page 70
67
c,dp<0,001ep=0,04fp=0,05gp=0,03hp=0,46
Page 71
A Randomized Controlled Trial (Rct) of Efficacy And Safety of
Plasma Adsorption or Plasma Exchange Compared to
Standard Medical Therapy in Patients with Acute on Chronic
Liver Failure
68
Background: Acute‐on‐chronic liver failure (ACLF) has very high 28‐day mortality of almost
30‐40%. Exaggerated hepatic necrosis, inflammation and immune response lead to early organ
failure and mortality. We aimed to remove high levels of toxic bile acids, bilirubin, DAMPS and
metabolites from circulation and to modulate the immune mechanisms to improve survival of
patients with ACLF.
Methods: Patients with ACLF with bilirubin >12 mg/dl and INR > 1.5 without any infection or
extrahepatic organ failure were screened for enrolment. Total of 32 ACLF patients were
randomized into 3 groups; standard medical treatment (SMT) (Gr A, n=11), SMT with plasma
adsorption [Jafron BS330] (Gr B, n=11) and SMT with plasma‐exchange (Gr C, n=10). The
primary endpoint was transplant free survival at day 28 and secondary objectives were assessment
of new onset sepsis, organ failure and safety and complications associated with the treatment.
Results: The baseline characteristics were comparable [mean age 50.2± 11.5, 44 ± 12 and 47±12.3
yr., male 10:9:8, baseline bilirubin 21.7±7, 26.9±6.1 and 27.6±8.8 mg/dl, bile acid levels 131±7,
126.8±11 and 138 ±10.8 mg/dl, CTP – 10.7 ± 1.5, 11.5 ± 1 and 11.4 ± 1.1, MELD score 29±4.2,
28±3.5 and 31.4±3.4, AARC score 9.5 ±1.8, 8.9±1, 10±0.92]. There was no statistical difference in
survival SMT vs PA vs PE (89%, 0, 89% and 63.3 %, 90%, 72%, respectively) at day 7 and 28
[p=0.12]. In comparison with Gr. A, Gr. B had significantly lower incidence at day 7 and 28 of new
onset sepsis (27%, 10%, 20% and 45.5%, 20%, 36%) and AKI (27%, 0%, 11% and 45%, 10%,
27%) respectively. In comparison with Gr A, B and C, there was (3.5 and 2.5‐fold, p=0.03) and
(1.64 and 1.4‐fold, p=0.18) reduction in bilirubin and bile acids which were associated with
improved survival. Further, bile acid profiling identified persistent increase in cholic acid,
glycocholic acid, chenodeoxycholic acid, taurochenodeoxycholic acid, tauroursodeoxy cholate and
lithocholic acid (p<0.05), amongst the survivors specially in Gr. B. As compared to SMT, in Gr. B,
Vinay kumar B R1, Rakhi Maiwall2, Ashok Kumar Choudhury3, Jaswinder Singh Maras4, Meenu Bajpai5,
Nirupama Trehanpati1,4, Guresh Kumar6 and Shiv Kumar Sarin7, (1)Hepatology, Ilbs, (2)Hepatology,
Institute of Liver and Biliary Sciences, New Delhi, India, (3)Hepatology, Institute of Liver and Biliary
Sciences , New Delhi, (4)Molecular and Cellular Medicine, Institute of Liver and Biliary Sciences,
(5)Hematology, Institute of Liver & Biliary Sciences, New Delhi, (6)Clinical Research, Institute of Liver and
Biliary Sciences, New Delhi, India, (7)Hepatology, Institute of Liver & Biliary Sciences
10
Page 72
69
there was significant increase in phenylacetate, ketone bodies riboflavin and sphingolipid
metabolism (p<0.05). PE in Gr. C resulted in significant increase in metabolites linked to energy
metabolism (Carnitine, pantothenate, Beta oxidation of fatty acid), methionine spermidine and
spermine metabolism (p<0.05) while metabolites linked to nicotinamide and nicotinamide
metabolism, arginine and proline metabolism and malate aspartate were significantly decreased in
comparison to SMT in PA and PE (p<0.05).
Conclusion: Artificial liver support in the form of plasma adsorption and plasma exchange, can
safely be used in severely sick ACLF patients. These modalities significantly improve the bile acid
and metabolic profile of ACLF patients. There was low incidence of new onset sepsis and AKI
especially using hemoperfusion. Further studies with larger sample size are warranted.
Disclosures:
The following people have nothing to disclose: Vinay kumar B R, Rakhi Maiwall, Ashok Kumar
Choudhury, Guresh Kumar, Shiv Kumar Sarin
Disclosure information not available at the time of publication: Jaswinder Singh Maras, Meenu
Bajpai, Nirupama Trehanpati
Submitter's E-mail Address:
[email protected]
Presentation Type:
Oral or Poster
Category:
Acute Liver Failure and Artificial Liver Support
Description:
Acute Liver Failure and Artificial Liver Support
Corresponding Presenting Author
Dr. Vinay Kumar B R
Email: [email protected] -- Will not be published
Ilbs
Hepatology
Trainee/Fellow










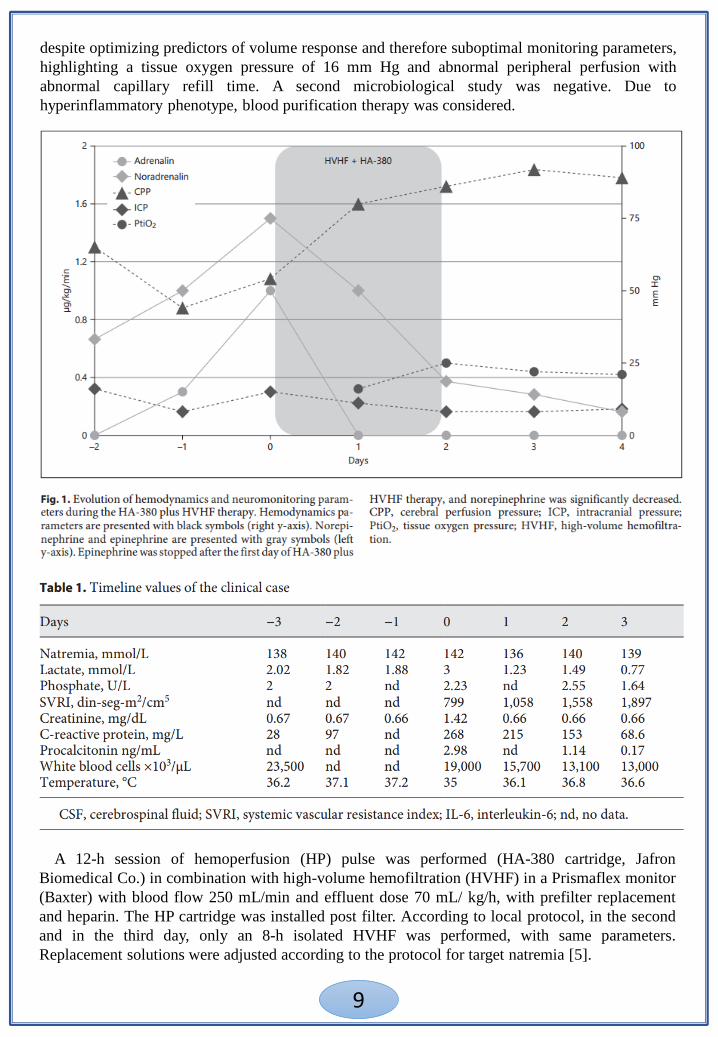
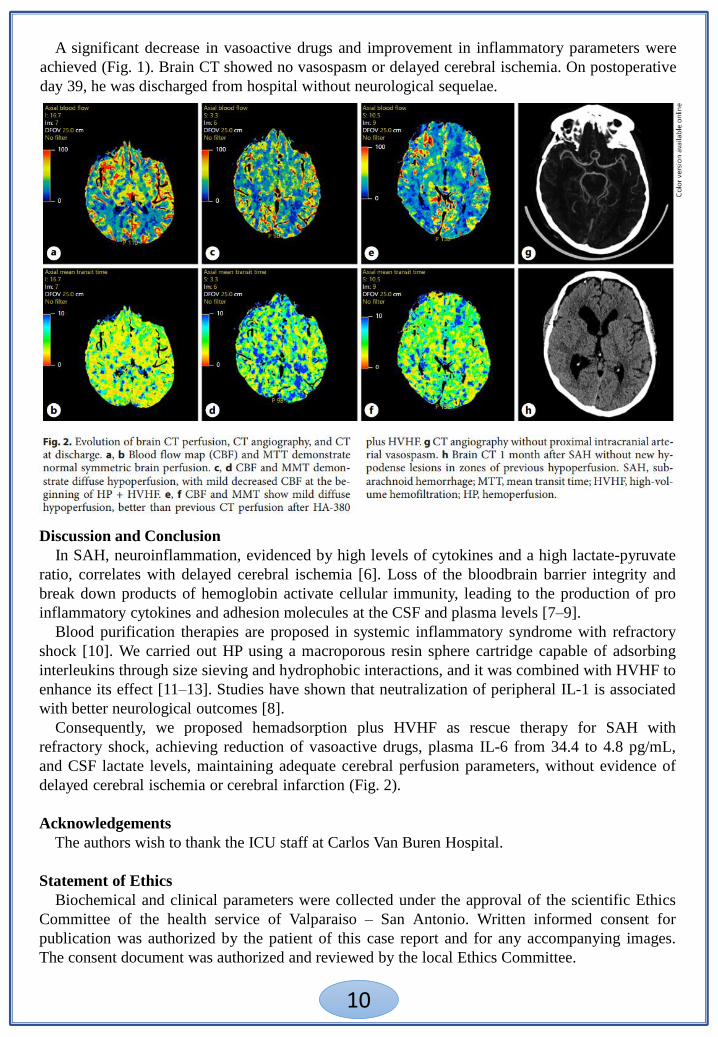















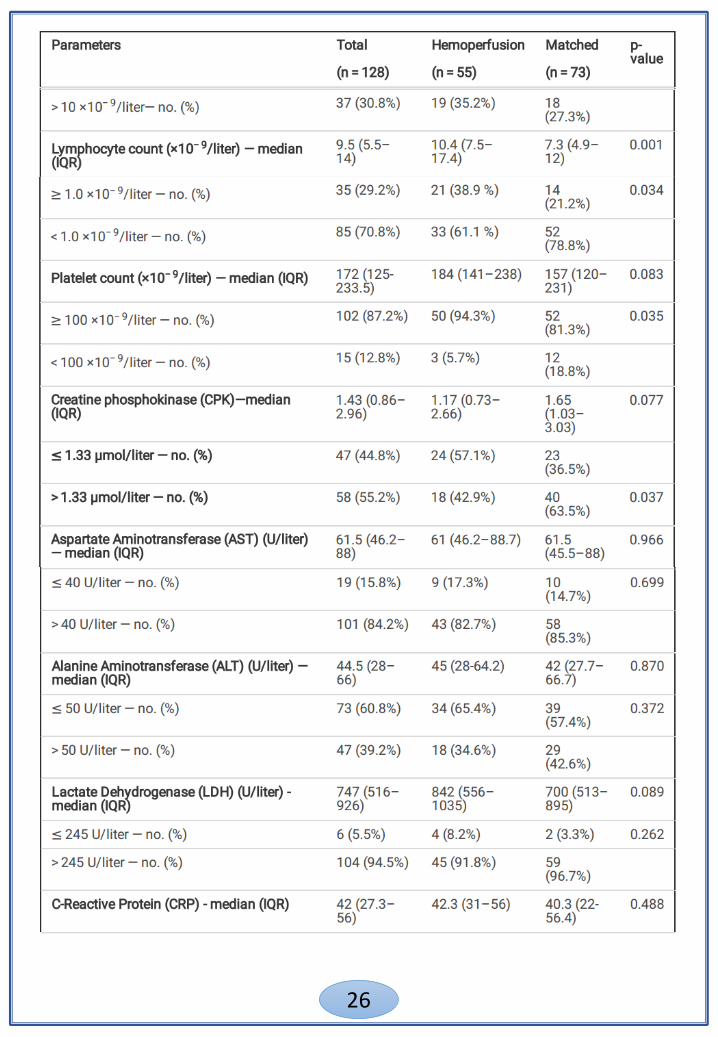








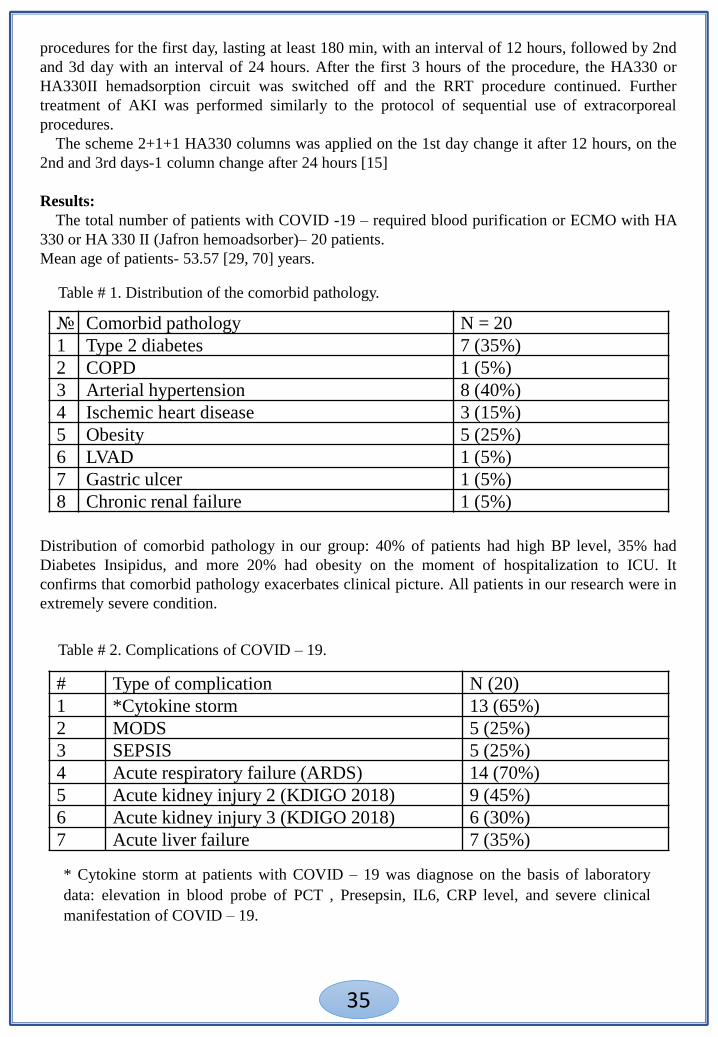








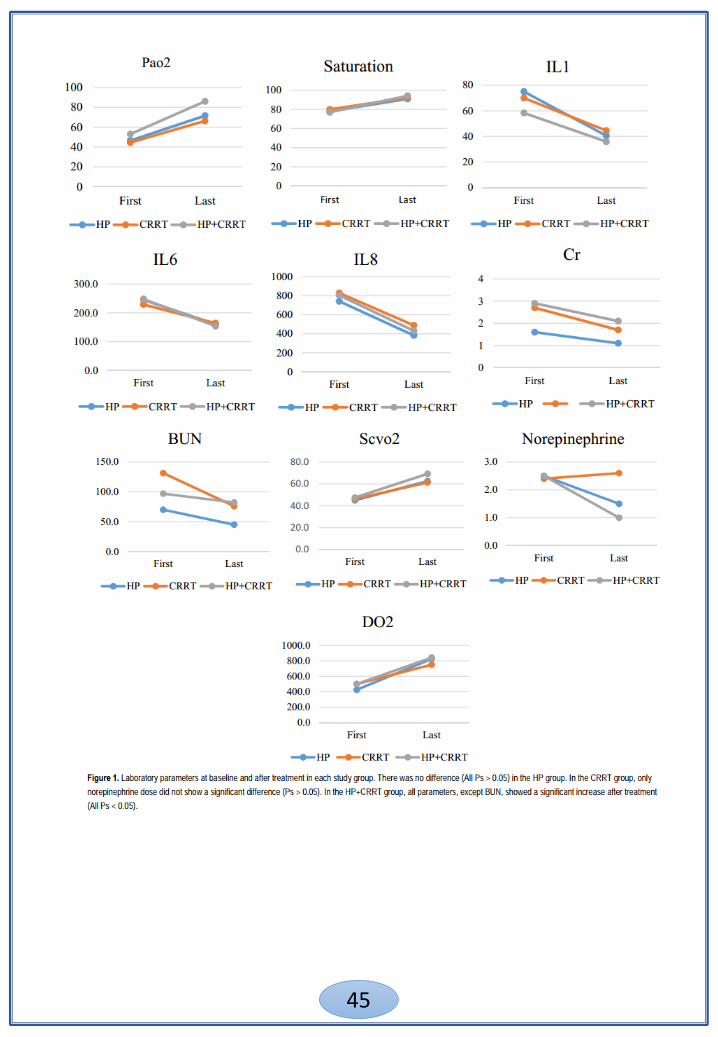











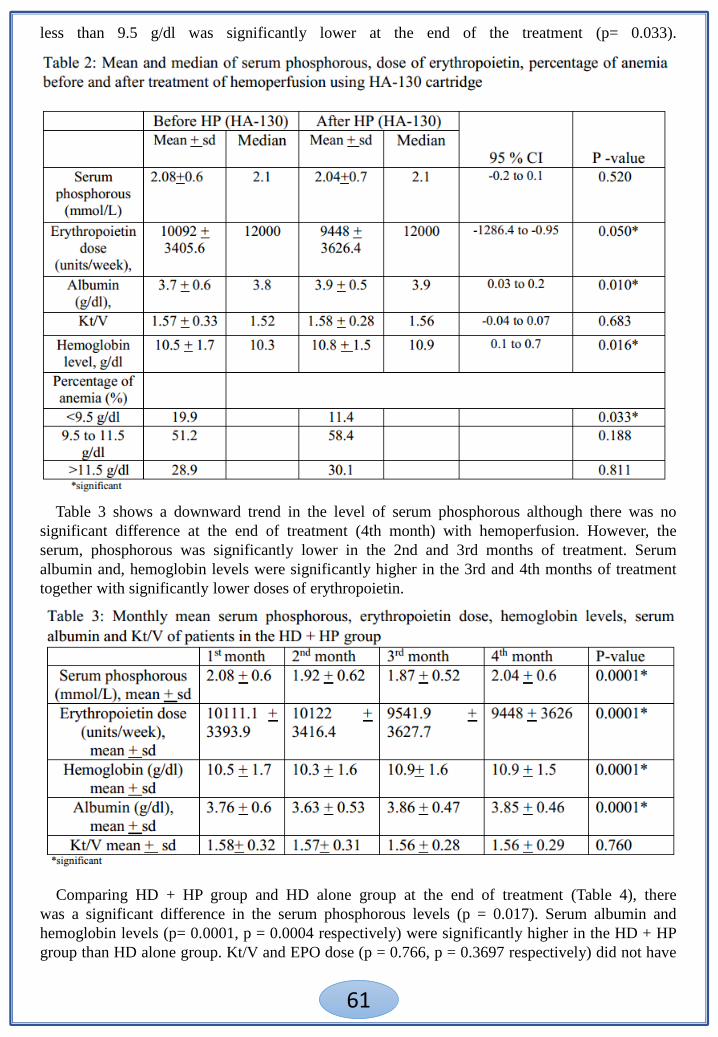




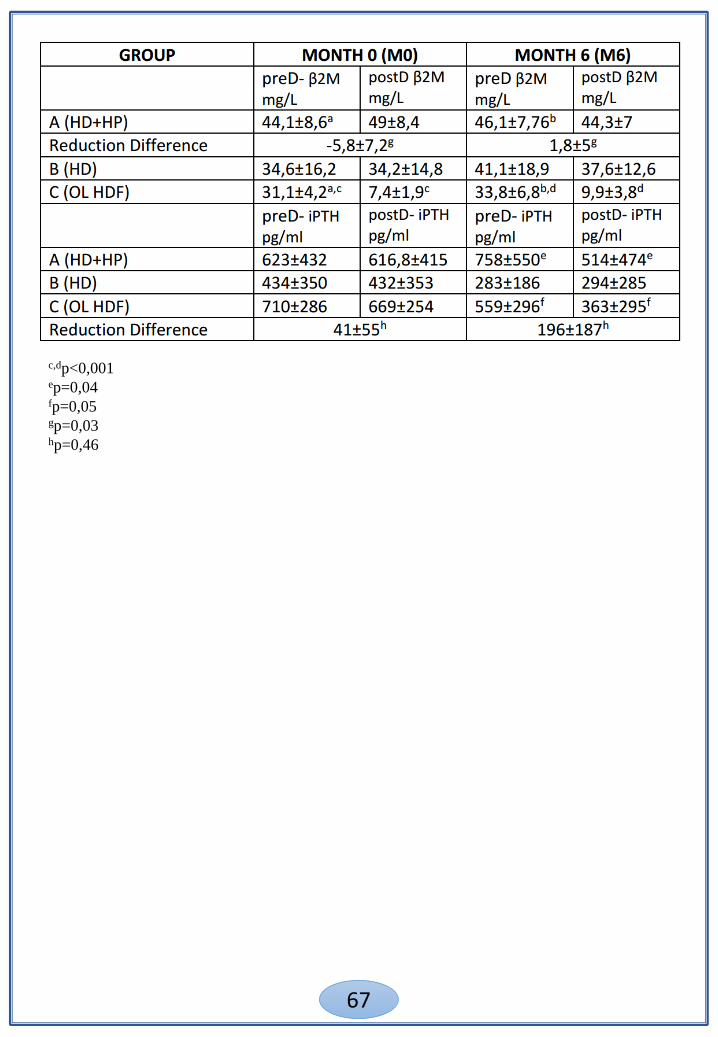









![S-7200C SERVICE MANUAL...S-7200C i SAFETY INSTRUCTIONS [1] Safety indications and their meanings This service manual and the indications and symbols that are used on the machine itself](https://static.documents.pub/doc/80x56/6076f01ef2b0c80afb0fbd63/s-7200c-service-manual-s-7200c-i-safety-instructions-1-safety-indications.jpg)








![BAS-300G INSTRUCTION MANUAL BAS-311G BAS … BAS-311G, BAS-326G iSAFETY INSTRUCTIONS [1] Safety indications and their meanings This instruction manual and the indications and symbols](https://static.documents.pub/doc/80x56/5ad1f1607f8b9a05208c18a3/bas-300g-instruction-manual-bas-311g-bas-bas-311g-bas-326g-isafety-instructions.jpg)
