46
New Perspective of SERM in Postmenopausal Women Health Daniel Thiebaud MD, Medical Fellow, Global Osteoporosis Strategy, Eli Lilly, Australia
| Date post: | 15-Dec-2015 |
| Category: |
Documents |
| Upload: | dakota-fearn |
| View: | 215 times |
| Download: | 0 times |
New Perspective of SERM in Postmenopausal Women Health
Daniel Thiebaud MD, Medical Fellow,
Global Osteoporosis Strategy, Eli Lilly, Australia

Case Study• 63 year old woman presents with a history of acute low
back pain.
• Menopause at 44 years of age, but never received postmenopausal HRT.
• Reported a history of a Colles’ fracture at age of 60 years.
What additional questions would you ask?
• Lumbar spine films reveal a recent vert fracture (L1)
• DXA of the hip shows a BMD T-score of –1.8 SD, and of -2.7 at LS (L2-L4).
How should her case be managed?How should her case be managed?
Case Study : How should it be managed?
• What other questions should you ask?
• What other tests would you like to know?
• What general advice would you give ?
• What treatment would you consider?
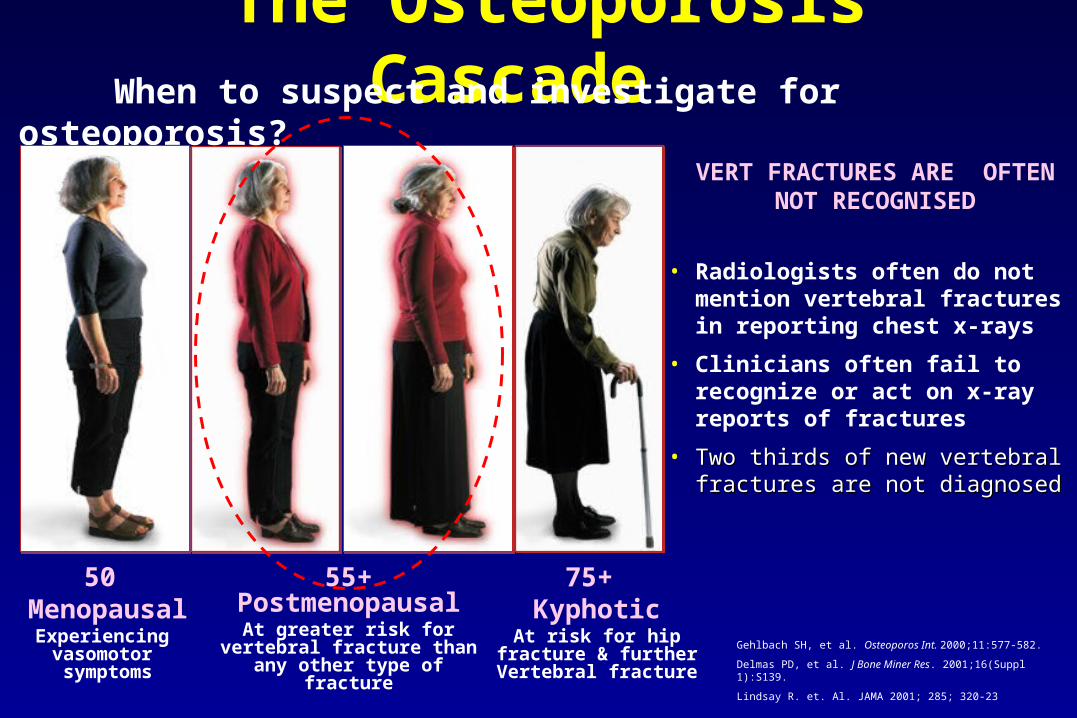
The Osteoporosis Cascade
75+ Kyphotic
At risk for hip fracture & further Vertebral
fracture
55+ PostmenopausalAt greater risk for vertebral
fracture than any other type of fracture
50 Menopausal
Experiencing vasomotor symptoms
When to suspect and investigate for osteoporosis?
• Radiologists often do not mention vertebral fractures in reporting chest x-rays
• Clinicians often fail to recognize or act on x-ray reports of fractures
• Two thirds of new vertebral Two thirds of new vertebral fractures are not diagnosedfractures are not diagnosed
Gehlbach SH, et al. Osteoporos Int. 2000;11:577-582.
Delmas PD, et al. J Bone Miner Res. 2001;16(Suppl 1):S139.
Lindsay R. et. Al. JAMA 2001; 285; 320-23
VERT FRACTURES ARE OFTEN NOT RECOGNISED
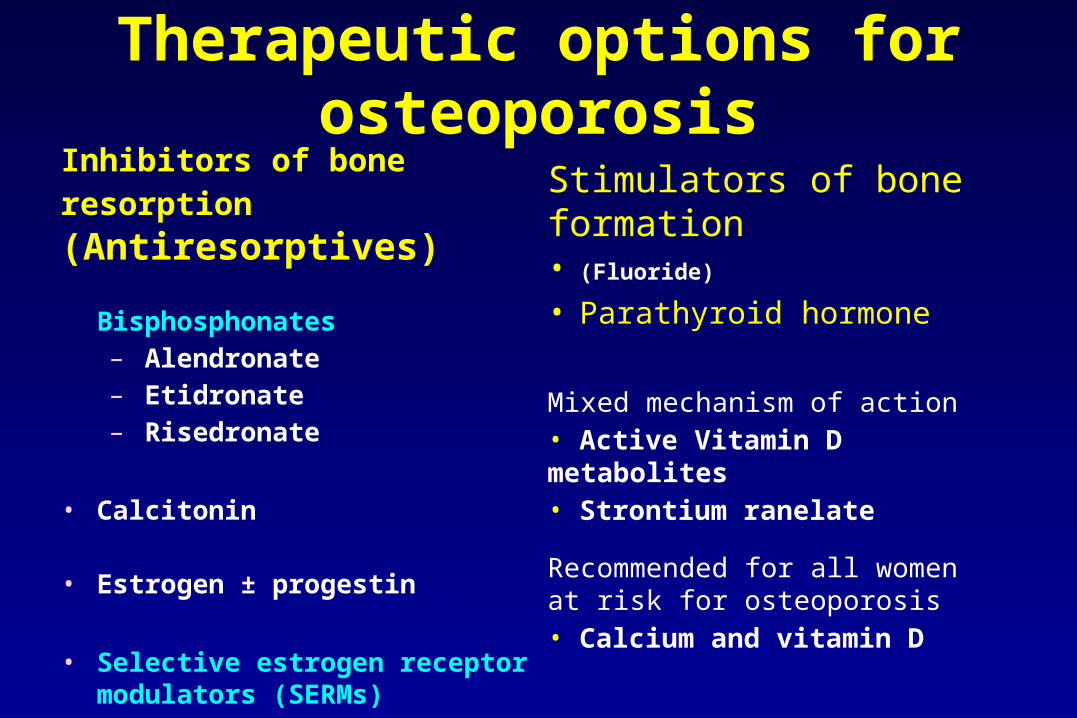
Therapeutic options for osteoporosis
Stimulators of bone formation• (Fluoride)
• Parathyroid hormone
Mixed mechanism of action• Active Vitamin D metabolites• Strontium ranelate
Recommended for all women at risk for osteoporosis• Calcium and vitamin D
Inhibitors of bone resorption (Antiresorptives)
Bisphosphonates– Alendronate– Etidronate– Risedronate
• Calcitonin
• Estrogen ± progestin
• Selective estrogen receptor modulators (SERMs)– Raloxifene
SSelective
EEstrogen
RReceptor
MModulatorodulator
Concept of a SERM
• Not an estrogen, progestin or other hormoneNot an estrogen, progestin or other hormone• Binds to estrogen receptorsBinds to estrogen receptors• Has estrogen-like effects in some tissuesHas estrogen-like effects in some tissues• Blocks estrogen effects in some tissuesBlocks estrogen effects in some tissues

Chemical Structures of Estradiol andCurrently Available SERMs
SOH
OH
O
ON
Raloxifenepost-menopausal osteoporosis
prevention and treatment
ON
Tamoxifenprevention and treatment of
breast cancer
Cl
ON
Clomiphenefertility induction
ON
Cl
Toremifenetreatment of breast cancer
OH
OH
17-estradiol
New SERMs in Phase 3 trials:
- Lasofoxifene- Basedoxifene- Arzoxifene
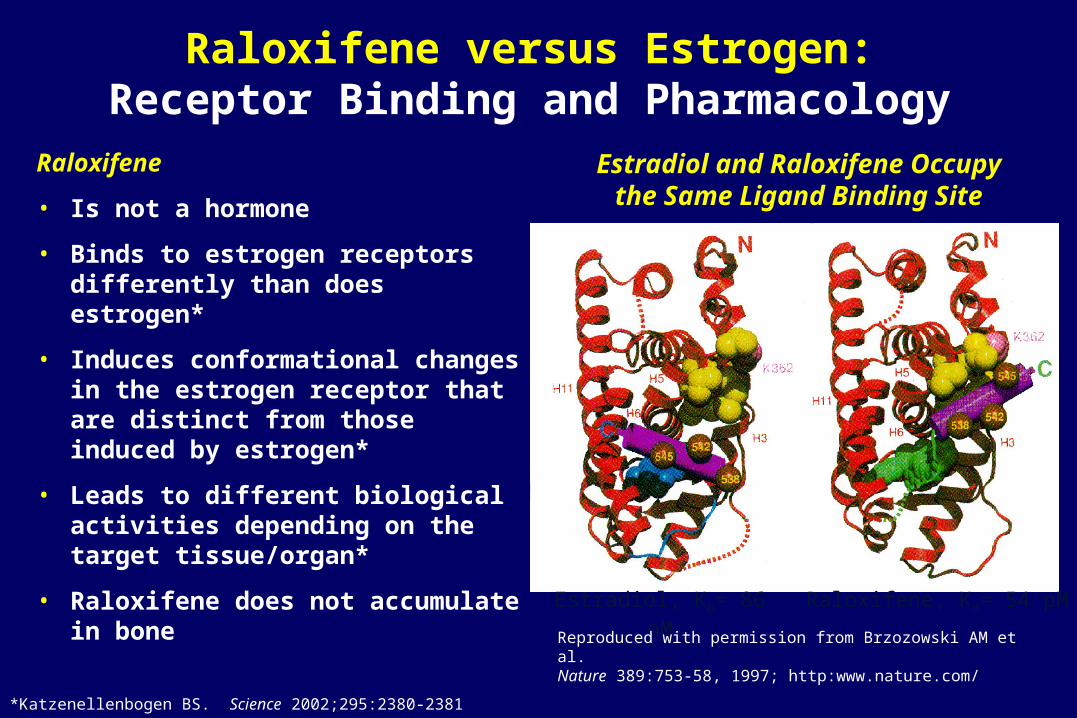
Raloxifene
• Is not a hormone
• Binds to estrogen receptors differently than does estrogen*
• Induces conformational changes in the estrogen receptor that are distinct from those induced by estrogen*
• Leads to different biological activities depending on thetarget tissue/organ*
• Raloxifene does not accumulate in bone
Raloxifene versus Estrogen:Receptor Binding and Pharmacology
*Katzenellenbogen BS. Science 2002;295:2380-2381
Raloxifene, Kd= 54 pMEstradiol, Kd= 86 pM
Reproduced with permission from Brzozowski AM et al. Nature 389:753-58, 1997; http:www.nature.com/
Estradiol and Raloxifene Occupythe Same Ligand Binding Site
N
OH
O
O
HO S
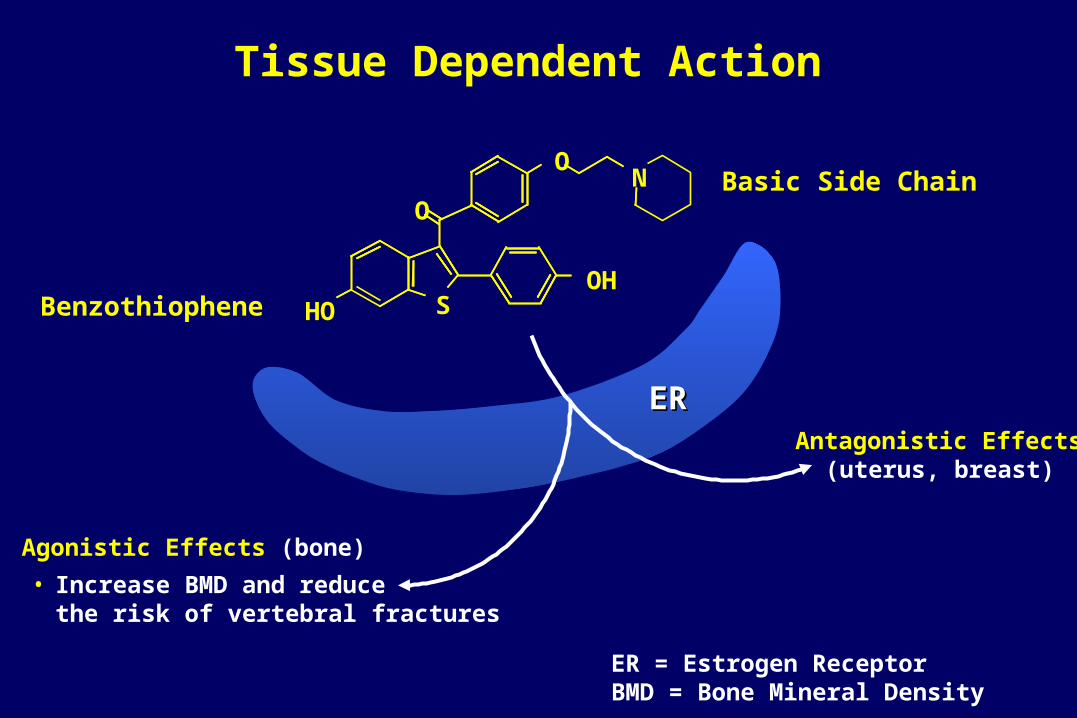
Tissue Dependent Action
Antagonistic Effects(uterus, breast)
Agonistic Effects (bone)
Basic Side Chain
Benzothiophene
ER = Estrogen ReceptorBMD = Bone Mineral Density
ERER
• Increase BMD and reducethe risk of vertebral fractures
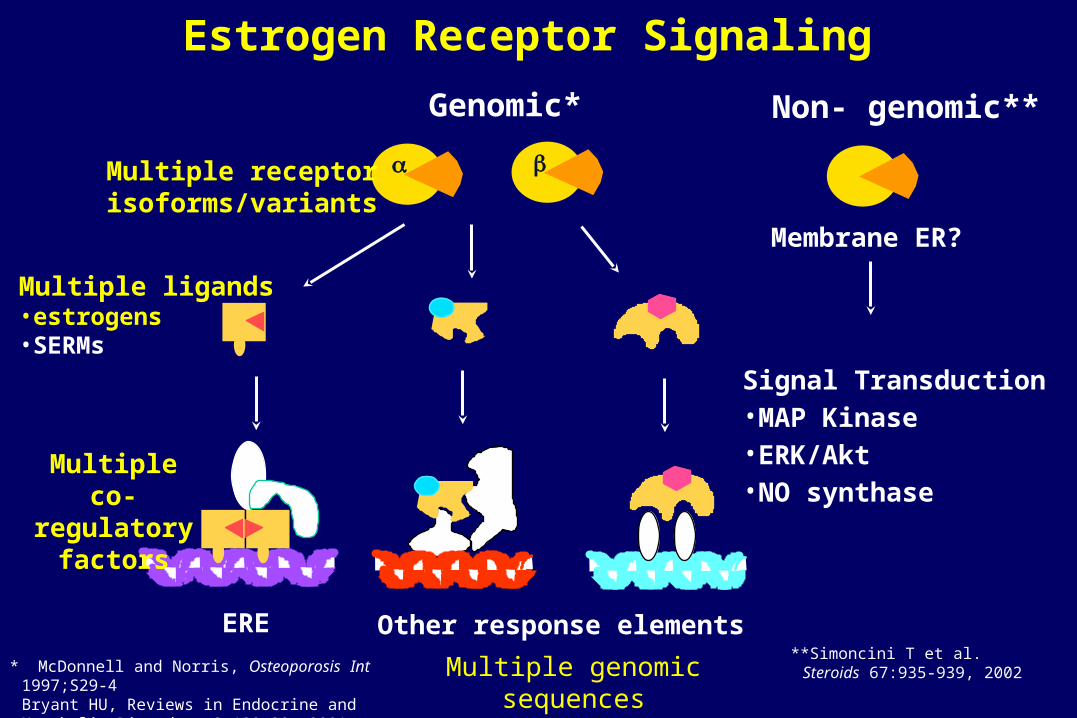
Estrogen Receptor Signaling
Other response elementsERE
Multiple co-regulatory
factors
Multiple ligands•estrogens•SERMs
Multiple receptor isoforms/variants
Genomic* Non- genomic**
Signal Transduction•MAP Kinase•ERK/Akt•NO synthase
Membrane ER?
Multiple genomic sequences**Simoncini T et al. Steroids
67:935-939, 2002* McDonnell and Norris, Osteoporosis Int 1997;S29-4Bryant HU, Reviews in Endocrine and Metabolic Disorders 2:129-38, 2001
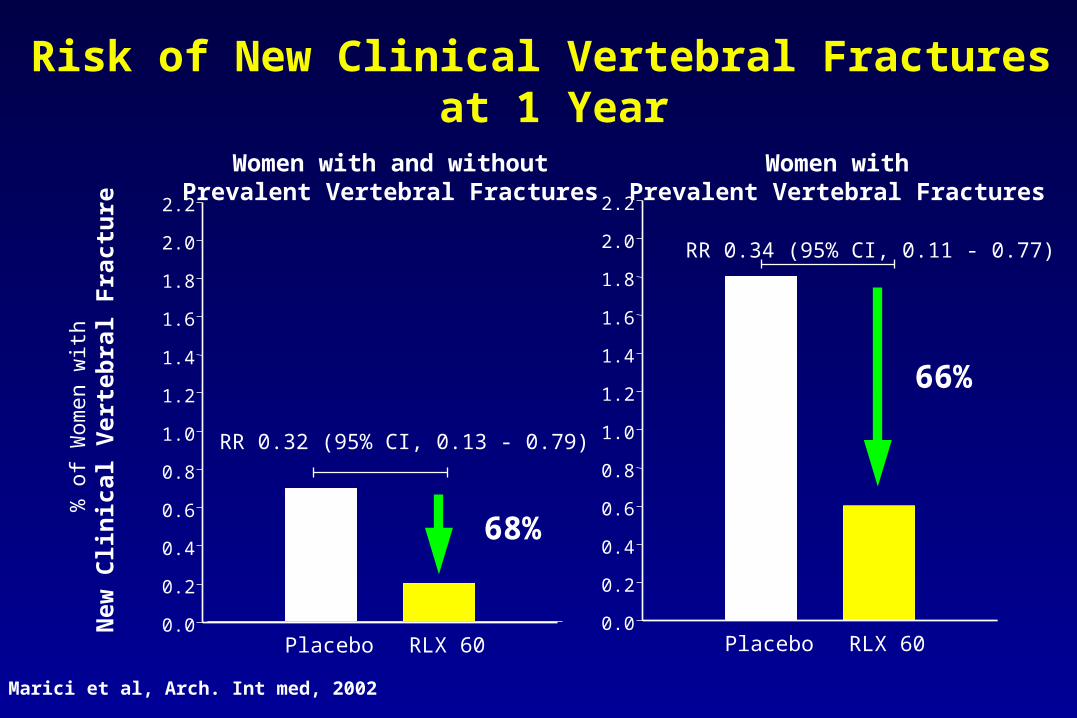
Women with and withoutPrevalent Vertebral Fractures
Women withPrevalent Vertebral Fractures
Placebo RLX 60
% o
f Wom
en w
ith
New
Cli
nic
al V
erte
bra
l F
ract
ure
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
RR 0.32 (95% CI, 0.13 - 0.79)
Placebo RLX 600.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
RR 0.34 (95% CI, 0.11 - 0.77)
66%
68%
Risk of New Clinical Vertebral Fractures at 1 Year
Marici et al, Arch. Int med, 2002
0
1
2
% o
f Pat
ient
s
Placebo
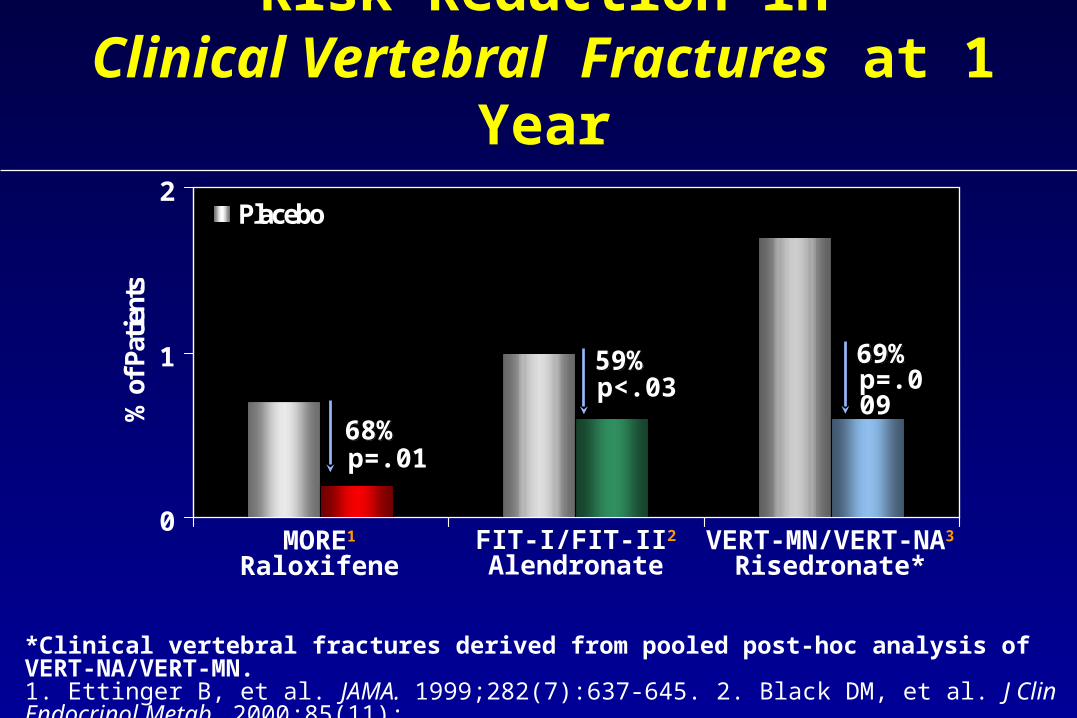
Risk Reduction inClinical Vertebral Fractures at 1 Year
59%59%p<.03
69%69%p=.009
p=.0168%68%
MORE1
RaloxifeneFIT-I/FIT-II2
AlendronateVERT-MN/VERT-NA3
Risedronate*
*Clinical vertebral fractures derived from pooled post-hoc analysis of VERT-NA/VERT-MN.1. Ettinger B, et al. JAMA. 1999;282(7):637-645. 2. Black DM, et al. J Clin Endocrinol Metab. 2000;85(11):4118-4124. 3. Data on file, Procter & Gamble.
• Multicenter, double-blind, placebo-controlled trial
• 25 countries, 180 centers, 3 years with 1 year extension
• 7705 postmenopausal women with osteoporosis
• Mean age 66.5 years
• Raloxifene 60 mg =Evista, 120 mg, or placebo
• All patients given daily calcium (500 mg) and vitamin D (600 IU)
• Primary endpoints: radiographic vertebral fracture, BMD, safety
• Secondary endpoints: all osteoporotic fractures, cardiovascular health, breast cancer, cognitive function
Ettinger B et al. JAMA 282:637-45, 1999Cummings SR et al. JAMA 281:2189-97, 1999
MOREMOREMMultiple ultiple OOutcomes of utcomes of RRaloxifene aloxifene EEvaluationvaluation
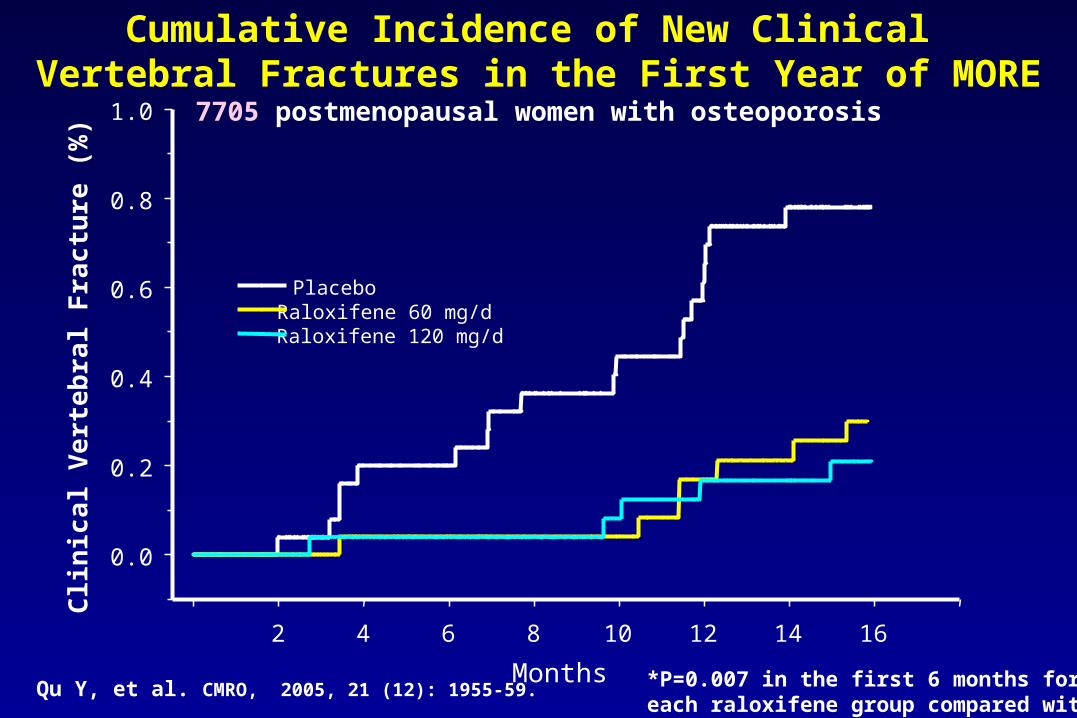
Cumulative Incidence of New Clinical Vertebral Fractures in the First Year of MORE
7705 postmenopausal women with osteoporosis
*P=0.007 in the first 6 months foreach raloxifene group compared with placebo
Qu Y, et al. CMRO, 2005, 21 (12): 1955-59.Months
2 4 6 8 10 12 14 16
0.0
0.2
0.4
0.6
0.8
1.0
PlaceboRaloxifene 60 mg/dRaloxifene 120 mg/d
Clin
ica
l Ve
rte
bra
l Fra
ctu
re (
%)
Wom
en w
ith N
ew
Clin
ical V
ert
ebra
l F
ractu
re (
%)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
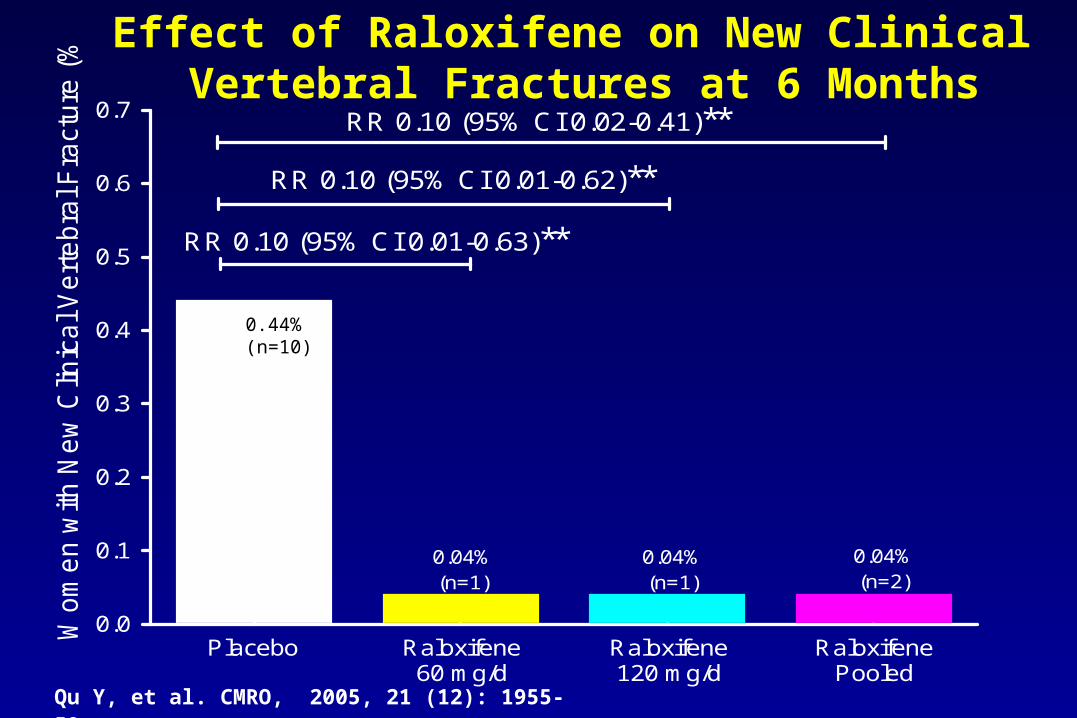
0.04%(n=1)
0.04%(n=1)
0.04%(n=2)
RR 0.10 (95% CI 0.02-0.41)**
RR 0.10 (95% CI 0.01-0.62)**
RR 0.10 (95% CI 0.01-0.63)**
0.44%(n=10)
Placebo Raloxifene60 mg/d
Raloxifene120 mg/d
RaloxifenePooled
0.44%(n=10)
Effect of Raloxifene on New Clinical Vertebral Fractures at 6 Months
Qu Y, et al. CMRO, 2005, 21 (12): 1955-59.

Effect of raloxifene on clinical fractures in Asian (China, Japan) women with osteoporosis
Baseline Characteristics a Japan (N=284)b China (N=204)c
Age (years) 64.8±6.3 65.3±6.0
Years Postmenopausal 15.2±6.5 16.9±7.3
Body Mass Index (kg/m2) 21.8±2.8 23.0±2.9
Prevalent Vertebral Fracture (%) 26.4 13.7
Lumbar Spine BMD (g/cm2)
T-score0.63±0.05
-3.77±0.460.69±0.07
-3.52±0.51
a : Mean ± standard deviation for continuous variables presentedb : N=97 for placebo ; N=92 for raloxifene 60 mg/d ; N=95 for raloxifene 120 mg/dc : N=102 for placebo ; N=102 for raloxifene 60 mg/d
T.Nakamura et al.JBMM, 24:414-418, 2006
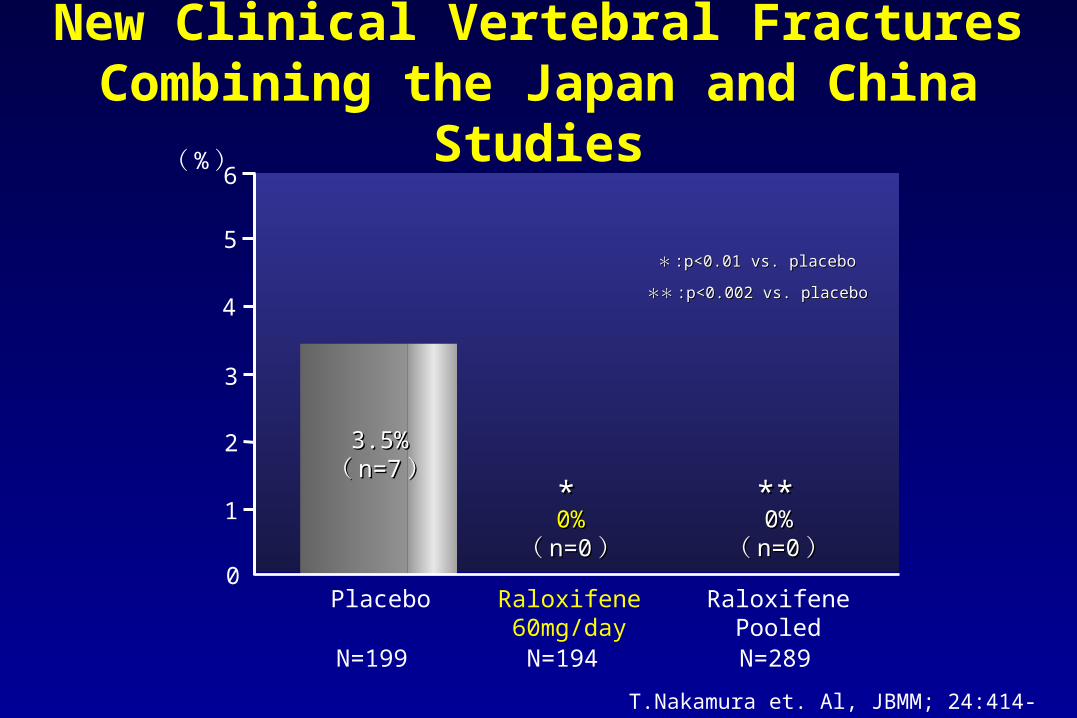
New Clinical Vertebral Fractures Combining the Japan and China Studies
RaloxifenePooled
3
2
1
0
(%)
3.5%3.5%(( n=7n=7))
0%0%(( n=0n=0))
Placebo Raloxifene60mg/day
4
5
6
0%0%(( n=0n=0))
******
**** :p<0.002 vs. placebo:p<0.002 vs. placebo
** :p<0.01 vs. placebo:p<0.01 vs. placebo
N=199 N=194 N=289
T.Nakamura et. Al, JBMM; 24:414-418; 2006

RaloxifenePooled
7
6
5
4
3
2
1
0
(%)
6.0%6.0%(( n=12n=12)) 1.0%1.0%
(( n=2n=2)) 0.7%0.7%(( n=2n=2))
RRRR:: 0.110.11(( 0.03 - 0.510.03 - 0.51))
RRRR:: 0.170.17(( 0.04 - 0.750.04 - 0.75))
Placebo Raloxifene60mg/day
8
9
******
**** :p<0.001 vs. placebo:p<0.001 vs. placebo** :p<0.01 vs. placebo:p<0.01 vs. placebo
Any New Clinical Fractures Combining the Japan and China Studies
T.Nakamura et. al.JBMM; 24:414-418, 2006
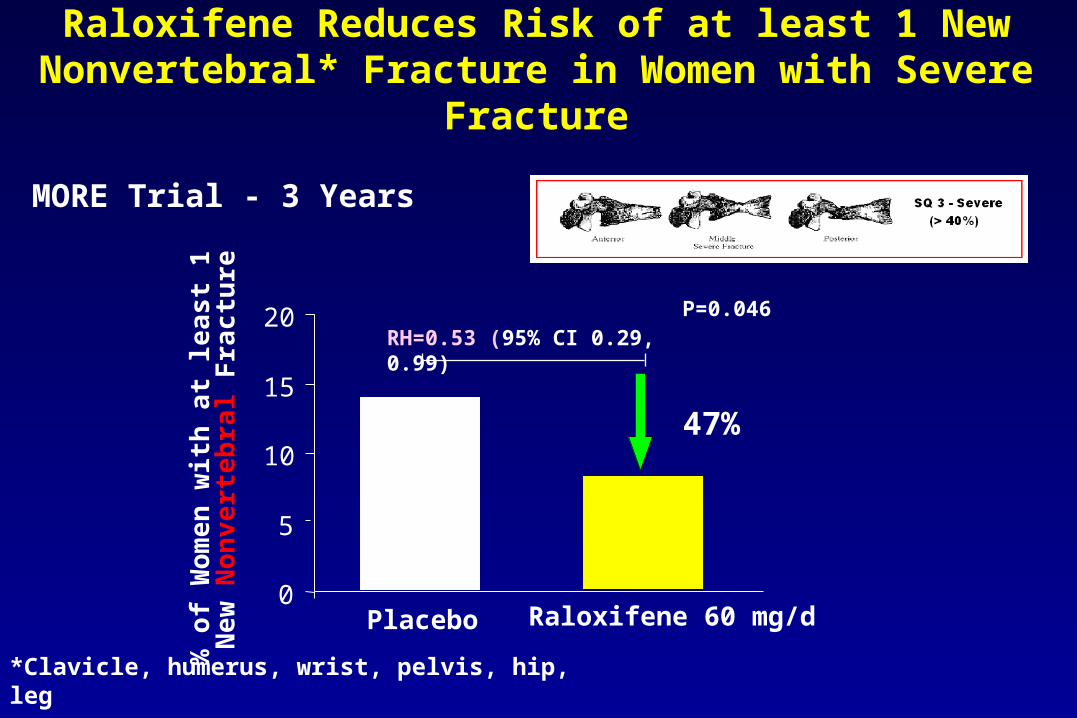
Raloxifene Reduces Risk of at least 1 New Nonvertebral* Fracture in Women with Severe Fracture
*Clavicle, humerus, wrist, pelvis, hip, leg
Delmas PD et al. Bone 2003;33;4:522-532
0
5
10
15
20
% o
f W
om
en
wit
h a
t le
ast
1
Ne
w N
on
vert
eb
ral F
rac
ture
RH=0.53 (95% CI 0.29, 0.99)
Placebo Raloxifene 60 mg/d
47%
MORE Trial - 3 Years
P=0.046
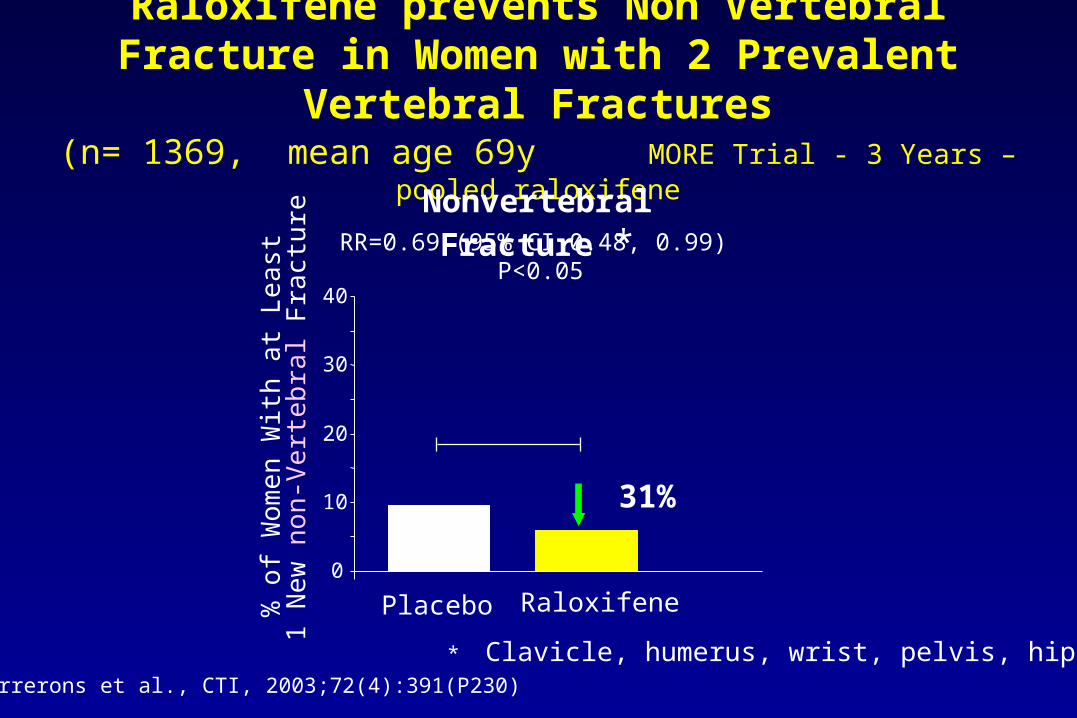
Raloxifene prevents Non Vertebral Fracture in Women with 2 Prevalent Vertebral Fractures
(n= 1369, mean age 69y MORE Trial - 3 Years – pooled raloxifene
Nonvertebral Fracture *
Farrerons et al., CTI, 2003;72(4):391(P230)
0
10
20
30
40%
of W
om
en
With
at L
ea
st
1 N
ew n
on-V
ert
ebra
l Fra
ctur
e RR=0.69 (95% CI 0.48, 0.99) P<0.05
Placebo Raloxifene
31%
* Clavicle, humerus, wrist, pelvis, hip, leg
EVA Trial (Evista Versus Alendronate)
• First ever head-to-head fracture outcome trial• Compare the osteoporotic fracture risk reduction
efficacy of raloxifene and alendronate• Approximately 2000 postmenopausal women with
osteoporosis • Double-blind, randomized, controlled, 1-3 year trial with
raloxifene 60 mg/d vs alendronate 10 mg/d– Calcium 500 mg/d + vitamin D 400 IU/d to all patients– Sites in US, Canada, and Puerto Rico
Recker RR, et al. J Bone Miner Res. 2005;20(suppl 1):S97, Bone in press 2007.

Baseline CharacteristicsCharacteristic Raloxifene
(N=707)
Alendronate
(N=716)
P-value
Age (years) 65.5 65.7 0.56
Caucasian (%) 86.7 86.9 0.83
BMI (kg/m2) 24.8 24.6 0.42
LS BMD (g/cm2)
0.82 0.82 0.79
T-score -2.32 -2.34 0.65
FN BMD (g/cm2) 0.61 0.61 0.98
T-score -2.39 -2.39 0.77
Hip BMD (g/cm2) 0.71 0.71 0.71
T-Score -1.99 -2.01 0.64
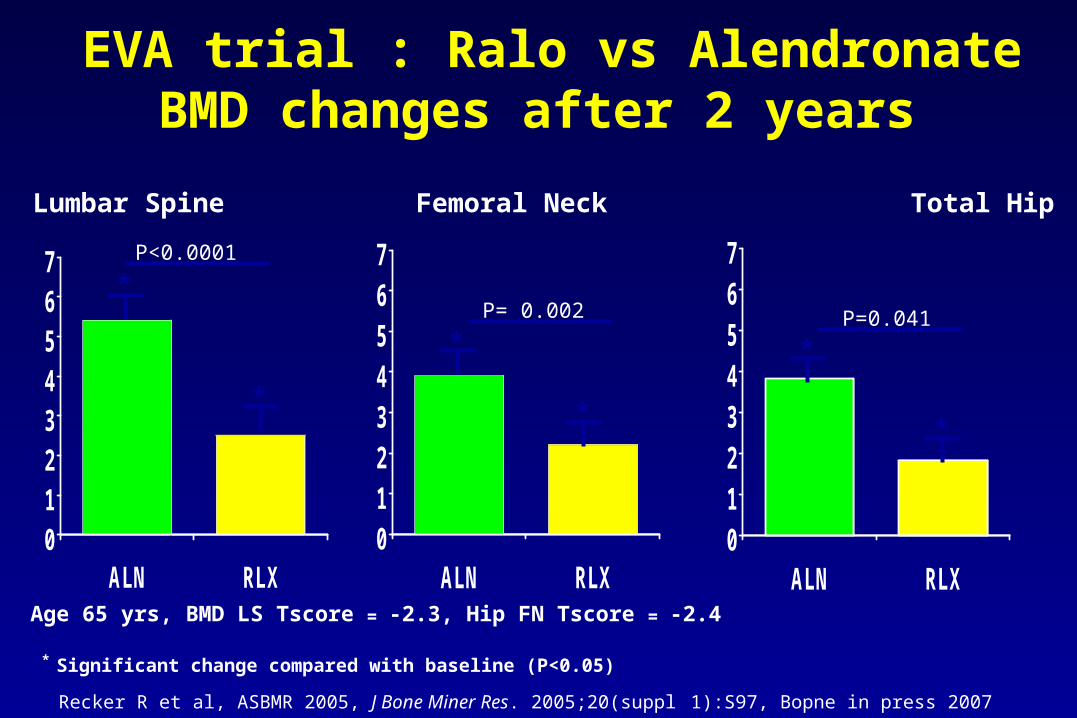
EVA trial : Ralo vs AlendronateBMD changes after 2 years
01234567
ALN RLX01234567
ALN RLX01234567
ALN RLX
Recker R et al, ASBMR 2005, J Bone Miner Res. 2005;20(suppl 1):S97, Bopne in press 2007
Lumbar Spine Femoral Neck Total Hip
*
*
*
*
*
*
P<0.0001
P= 0.002 P=0.041
Age 65 yrs, BMD LS Tscore = -2.3, Hip FN Tscore = -2.4
* Significant change compared with baseline (P<0.05)
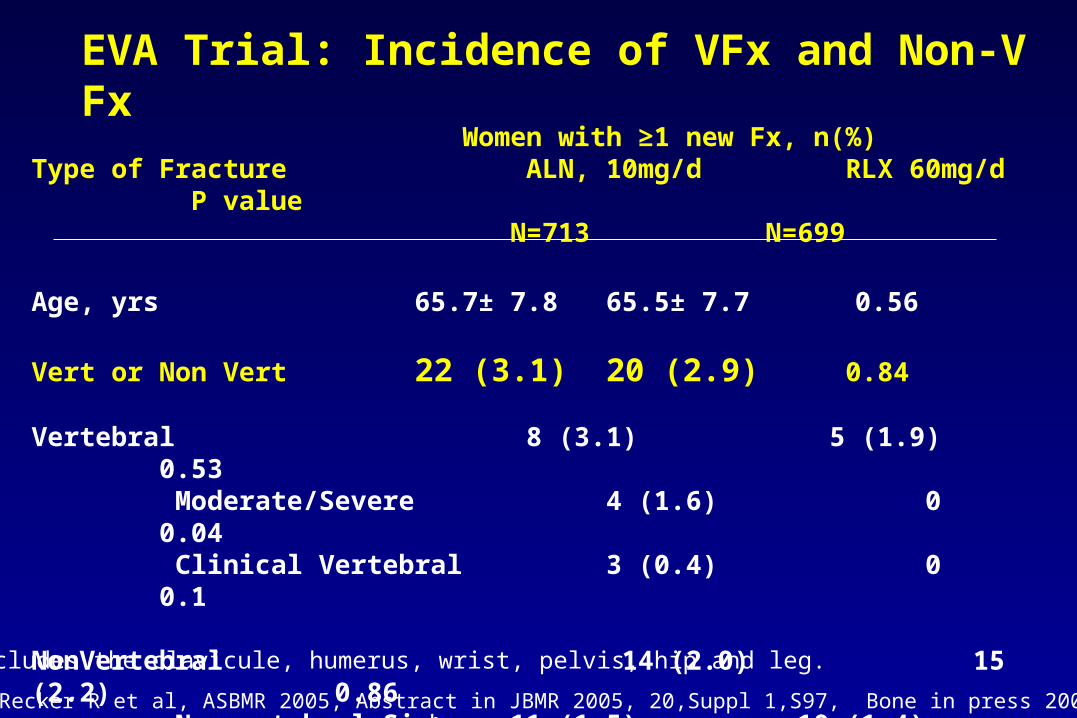
EVA Trial: Incidence of VFx and Non-V Fx
Women with ≥1 new Fx, n(%)Type of Fracture ALN, 10mg/d RLX 60mg/d P value
N=713 N=699
Age, yrs 65.7± 7.8 65.5± 7.7 0.56
Vert or Non Vert 22 (3.1) 20 (2.9) 0.84
Vertebral 8 (3.1) 5 (1.9) 0.53 Moderate/Severe 4 (1.6) 0 0.04 Clinical Vertebral 3 (0.4) 0 0.1
NonVertebral 14 (2.0) 15 (2.2) 0.86 Nonvertebral-Sixb 11 (1.5) 10 (1.4) 0.89
b Includes the clavicule, humerus, wrist, pelvis, hip and leg.
Recker R et al, ASBMR 2005, Abstract in JBMR 2005, 20,Suppl 1,S97, Bone in press 2007
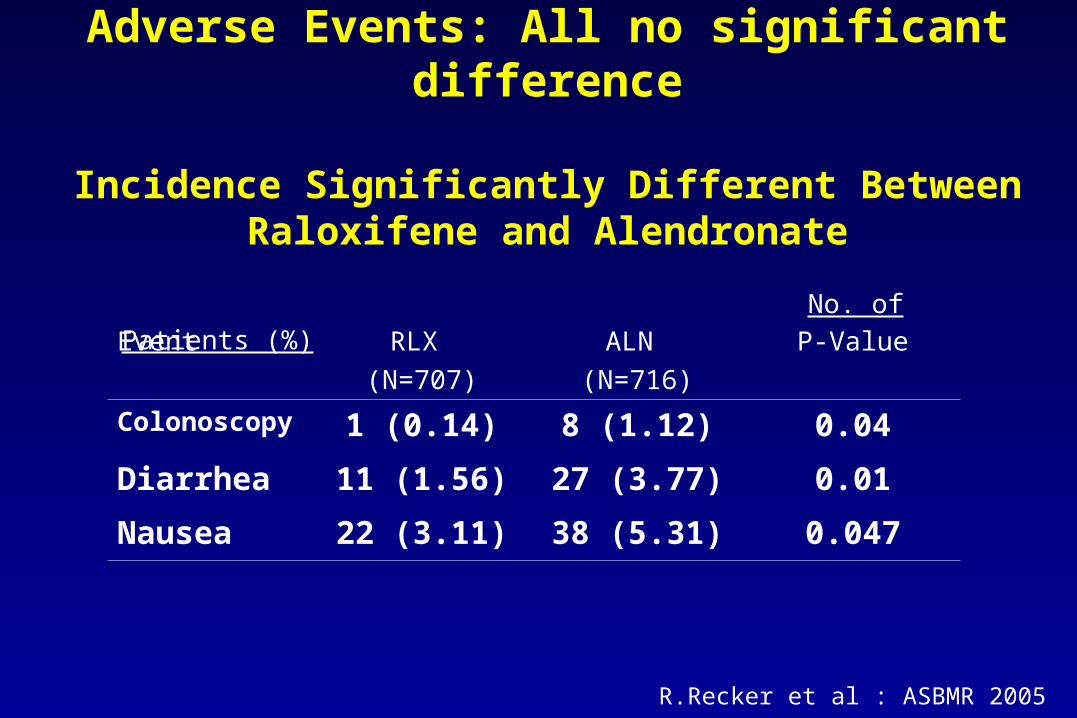
Adverse Events: All no significant difference
Incidence Significantly Different Between Raloxifene and Alendronate
No. of Patients (%)
Event RLX
(N=707)
ALN
(N=716)
P-Value
Colonoscopy 1 (0.14) 8 (1.12) 0.04
Diarrhea 11 (1.56) 27 (3.77) 0.01
Nausea 22 (3.11) 38 (5.31) 0.047
R.Recker et al : ASBMR 2005
Evista Safety
Daniel Thiebaud MD, Medical Fellow,
Global Osteoporosis Strategy, Eli Lilly, Australia

MORE, Multiple Outcomes of Raloxifene Evaluation; CORE, Continuing Outcomes Relevant to EVISTA; RUTH, Raloxifene Use for The Heart; STAR, Study of Tamoxifen and Raloxifene; EVA, EVISTA-Alendronate Comparison
0
5000
10000
15000
20000
1,764
7,705
4,011
10,101
19,747
Nu
mb
er
of E
nro
lled
Wo
men
OsteoporosisPrevention
MORE CORE RUTH STAR EVA
1,400
Large-Scale Raloxifene Clinical Trials
Rationale for the RUTH TrialRationale for the RUTH Trial
• Coronary outcomes, based on:– favorable impact of raloxifene on cardiovascular risk markers1 – evidence from observational studies that treatment with estrogen
was associated with a reduced risk of CHD in postmenopausal women2,3
• Invasive breast cancer, based on:– anti-estrogenic effects of raloxifene in the breast4
– 72% reduction in invasive breast cancer in a secondary analysis of data from the MORE trial5
RUTH was designed to determine the effect of raloxifene on:
1Blumenthal R et al. Am Heart J 20042Stampfer MJ et al. Prev Med 19913Grady D et al. Ann Intern Med 19924Brzozowski AM et al. Nature 19975Cauley J et al. Breast Cancer Res Treat 2001
Relevant Clinical Trial FindingsRelevant Clinical Trial FindingsAfter RUTH CommencedAfter RUTH Commenced
• Estrogen and Estrogen Plus ProgestinTherapy– HERS trial: Estrogen plus progestin did not reduce the overall rate of CHD
events in postmenopausal women with established coronary disease1
– WHI trial: Early increase in risk of coronary events with estrogen plus progestin therapy and estrogen alone in healthy postmenopausal women2,3
• Raloxifene– MORE trial results suggested no overall effect of raloxifene on
cardiovascular (CV) events, and a reduced risk for CV events in the subset of postmenopausal women retrospectively defined as at increased CV risk (post hoc analysis)4
1Hulley et al, JAMA 19982Writing Group for the Women's Health Initiative Investigators, JAMA 20023Anderson GL et al. JAMA 20044Barrett Connor et al, JAMA 2002
STAR Results: Invasive Breast Cancer
• The number of invasive breast cancers in the tamoxifen group (163 cases of 9,726) versus the raloxifene group (168 cases of 9,745) were statistically equivalent.
• Tamoxifen is known to reduce breast cancer risk by 50%, and STAR shows that raloxifene produces similar results.
Vogel et al, JAMA , 2006; 295, June 2006 2. Fisher B, et al. J Natl Cancer Inst 1998; 90:1371-1388.

MORE plus CORE Study Design
0 1 2 3 4 5 6 7 8
Placebo
Raloxifene HCl 60 mg/day
Raloxifene HCl 120 mg/day
Placebo
Raloxifene HCl 60 mg/day
Year
8 Years Total Follow-up
MORE (N=7705)Three Treatment
Groups
CORE (n=4011)Two Treatment
Groups
GapMORE ConclusionCORE Screening
Martino S, et al. J. Natl. Cancer Inst. 2004;96(23):1751-1761
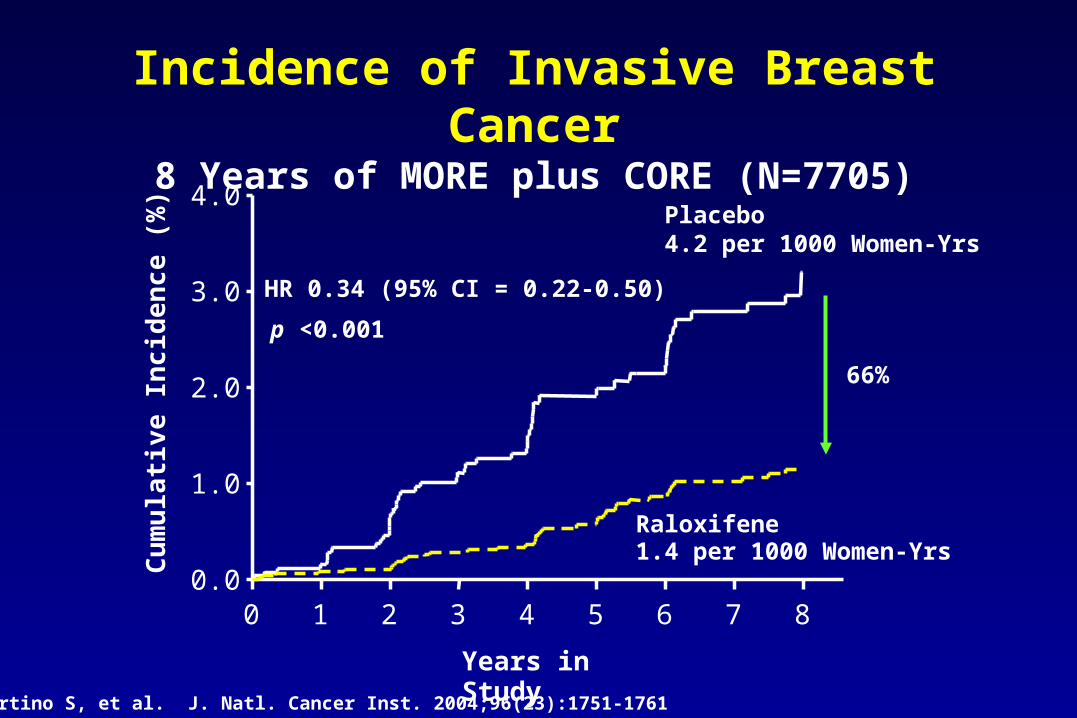
Incidence of Invasive Breast Cancer8 Years of MORE plus CORE (N=7705)
Years in Study
0 1 2 3 4 5 6 7 80.0
1.0
2.0
3.0
4.0
HR 0.34 (95% CI = 0.22-0.50)
Placebo4.2 per 1000 Women-Yrs
Raloxifene1.4 per 1000 Women-Yrs
p <0.001
Cu
mu
lati
ve In
cid
enc
e (%
)
66%
Martino S, et al. J. Natl. Cancer Inst. 2004;96(23):1751-1761
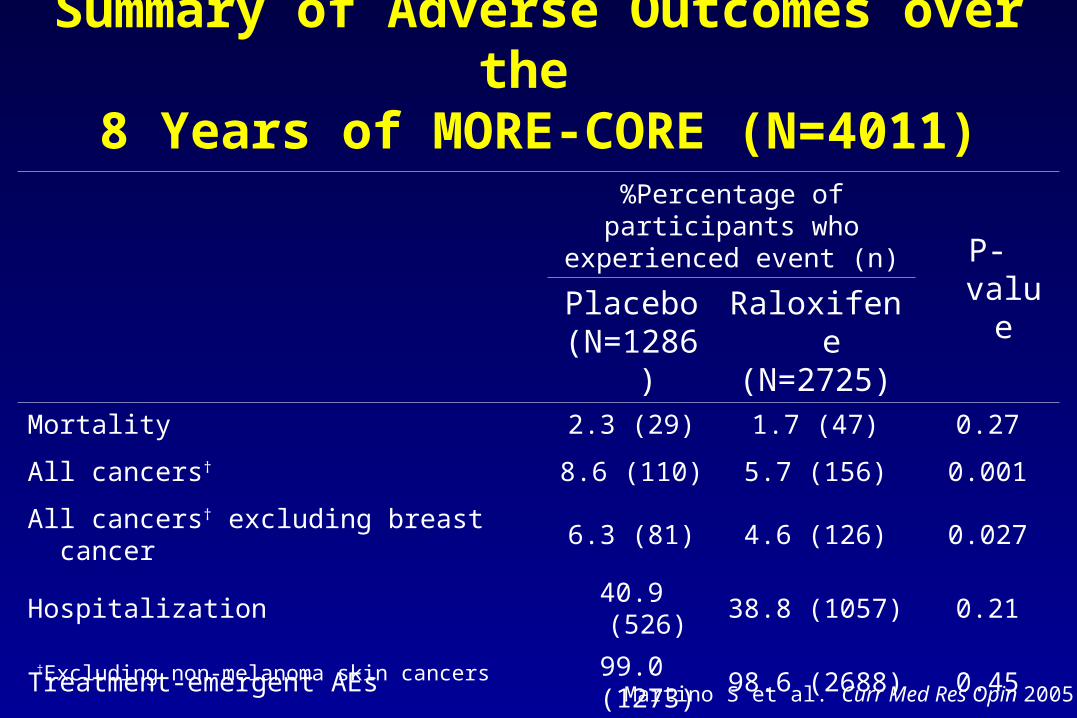
Summary of Adverse Outcomes over the 8 Years of MORE-CORE (N=4011)
%Percentage of participants who experienced event (n)
P-valuePlacebo(N=1286)
Raloxifene(N=2725)
Mortality 2.3 (29) 1.7 (47) 0.27
All cancers† 8.6 (110) 5.7 (156) 0.001
All cancers† excluding breast cancer 6.3 (81) 4.6 (126) 0.027
Hospitalization 40.9 (526) 38.8 (1057) 0.21
Treatment-emergent AEs 99.0 (1273) 98.6 (2688) 0.45
Treatment-emergent serious AEs 45.5 (585) 42.3 (1154) 0.07
Study discontinuation CORE due to AE 2.4 (31) 1.9 (53) 0.35
†Excluding non-melanoma skin cancersMartino S et al. Curr Med Res Opin 2005
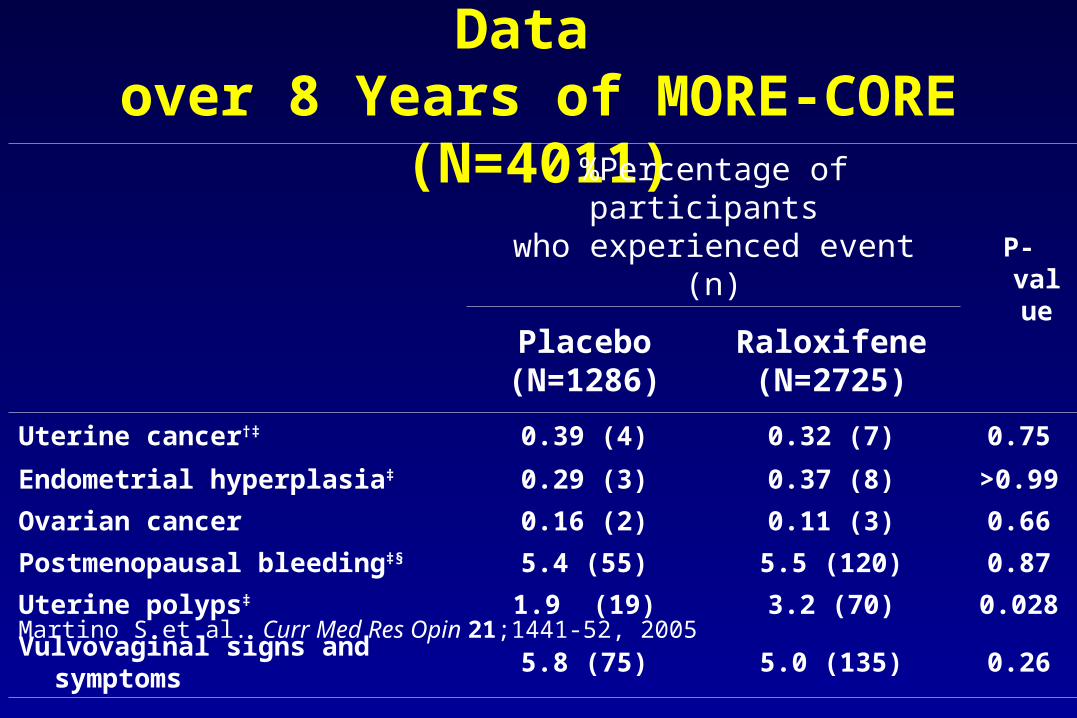
Summary of Gynecological AE Data over 8 Years of MORE-CORE (N=4011)
%Percentage of participants who experienced event (n)
P-valuePlacebo(N=1286)
Raloxifene(N=2725)
Uterine cancer†‡ 0.39 (4) 0.32 (7) 0.75
Endometrial hyperplasia‡ 0.29 (3) 0.37 (8) >0.99
Ovarian cancer 0.16 (2) 0.11 (3) 0.66
Postmenopausal bleedingठ5.4 (55) 5.5 (120) 0.87
Uterine polyps‡ 1.9 (19) 3.2 (70) 0.028
Vulvovaginal signs and symptoms 5.8 (75) 5.0 (135) 0.26
Martino S et al. Curr Med Res Opin 21;1441-52, 2005
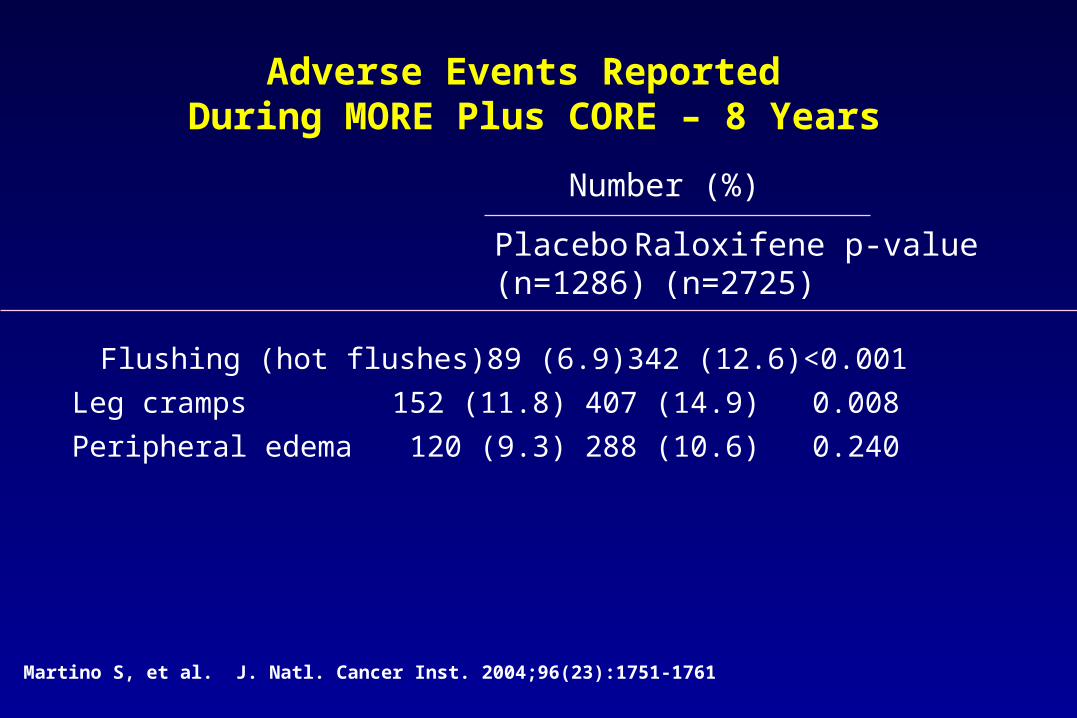
Flushing (hot flushes) 89 (6.9) 342 (12.6) <0.001
Leg cramps 152 (11.8) 407 (14.9) 0.008
Peripheral edema 120 (9.3) 288 (10.6) 0.240
Adverse Events Reported During MORE Plus CORE – 8 Years
Number (%)
Placebo Raloxifene p-value(n=1286) (n=2725)
Martino S, et al. J. Natl. Cancer Inst. 2004;96(23):1751-1761
Therapeutic options for osteoporosis
Stimulators of bone formation• (Fluoride)• Parathyroid hormone
Mixed mechanism of action• Vitamin D and metabolites• Strontium ranelate
Recommended for all women at risk for osteoporosis• Calcium and vitamin D
Inhibitors of bone resorption
Bisphosphonates– Alendronate– Etidronate– Risedronate
• Calcitonin
• Estrogen ± progestin
• Selective estrogen receptor modulators (SERMs)– Raloxifene
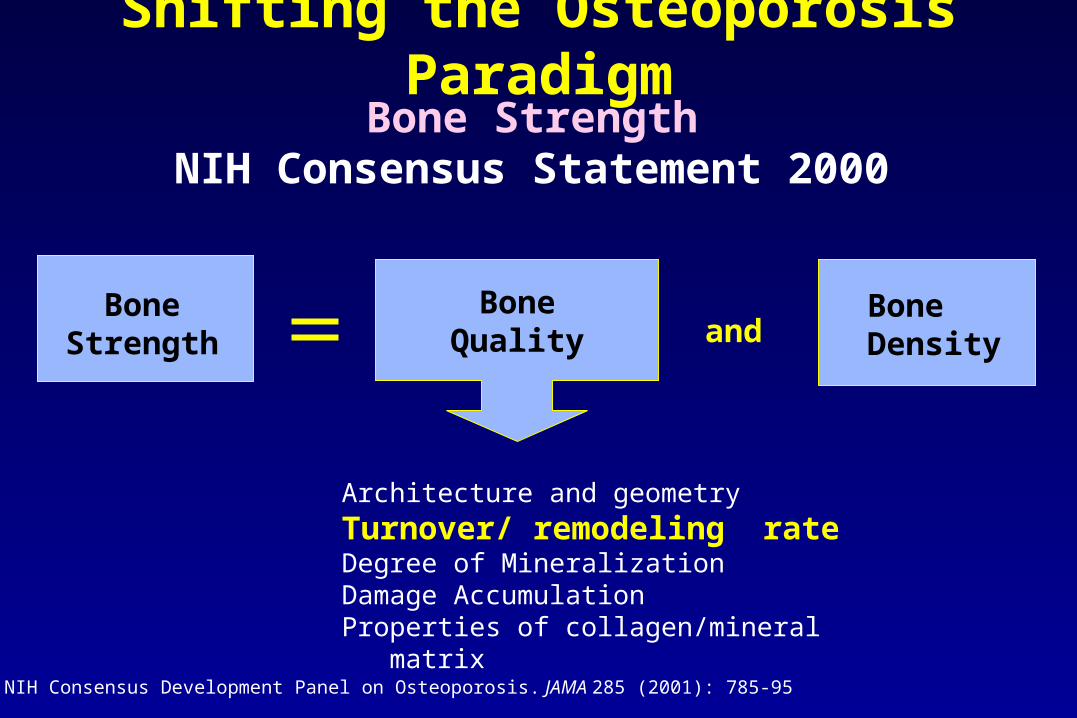
Bone StrengthNIH Consensus Statement 2000
BoneQuality
BoneStrength and
Architecture and geometry
Turnover/ remodeling rateDegree of MineralizationDamage AccumulationProperties of collagen/mineral matrix
Shifting the Osteoporosis Paradigm
BoneDensity
NIH Consensus Development Panel on Osteoporosis. JAMA 285 (2001): 785-95
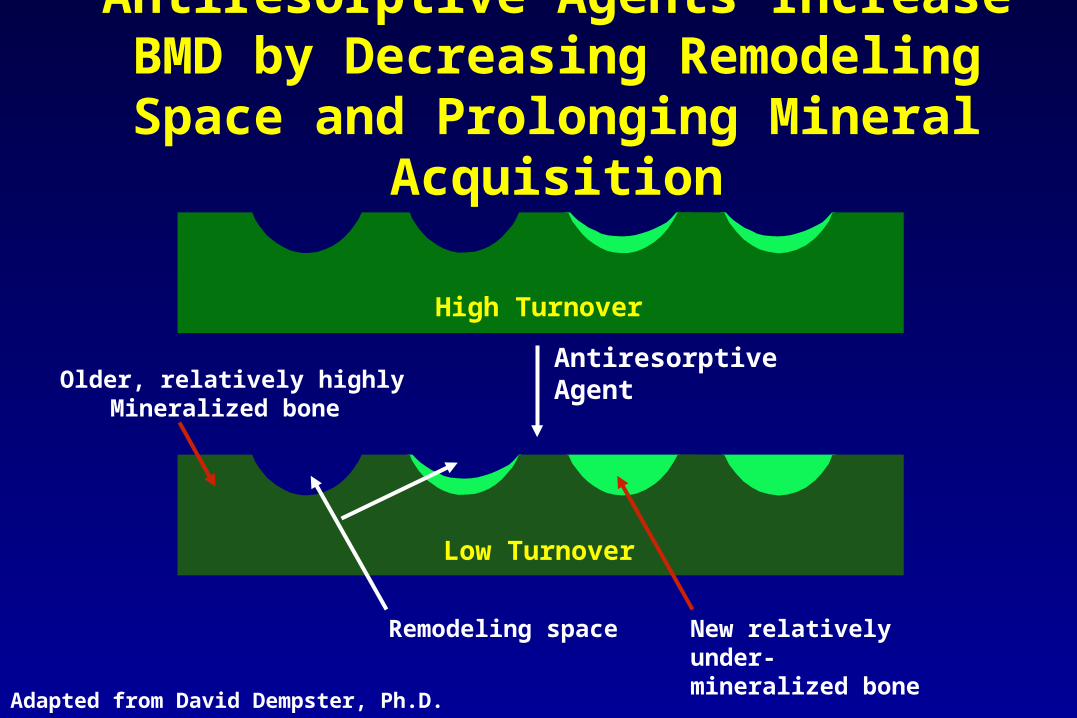
Antiresorptive Agents Increase BMD by Decreasing Remodeling Space and
Prolonging Mineral Acquisition
Remodeling space
Antiresorptive Agent
High Turnover
Low Turnover
New relatively under-mineralized bone
Adapted from David Dempster, Ph.D.
Older, relatively highlyMineralized bone

Markers of collagen degradation and synthesis in women treated with raloxifene or alendronate
Stepan J, Vokrouhlicka J, CCA 288, 1999, 121-135
Resorption Formation
Stepan et al, ASBMR 2002
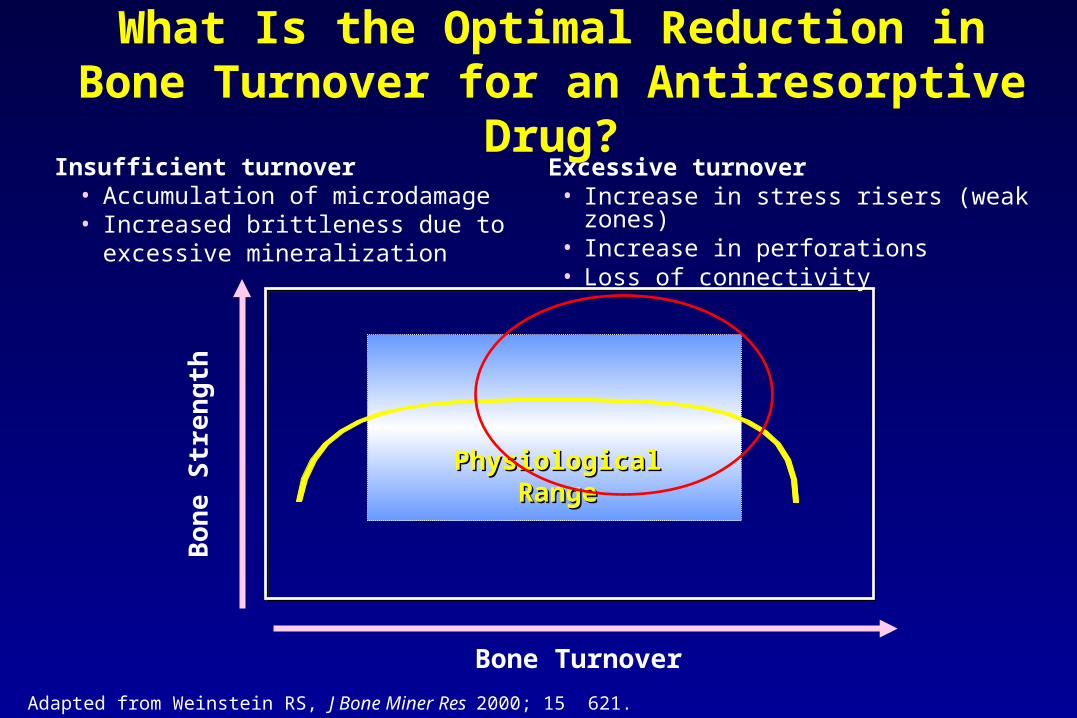
What Is the Optimal Reduction in Bone Turnover for an Antiresorptive Drug?
Adapted from Weinstein RS, J Bone Miner Res 2000; 15 621.
Physiological Physiological RRangeange
Bo
ne
Str
en
gth
Bone Turnover
Excessive turnover• Increase in stress risers (weak zones)• Increase in perforations• Loss of connectivity
Insufficient turnover• Accumulation of microdamage• Increased brittleness due to excessive
mineralization
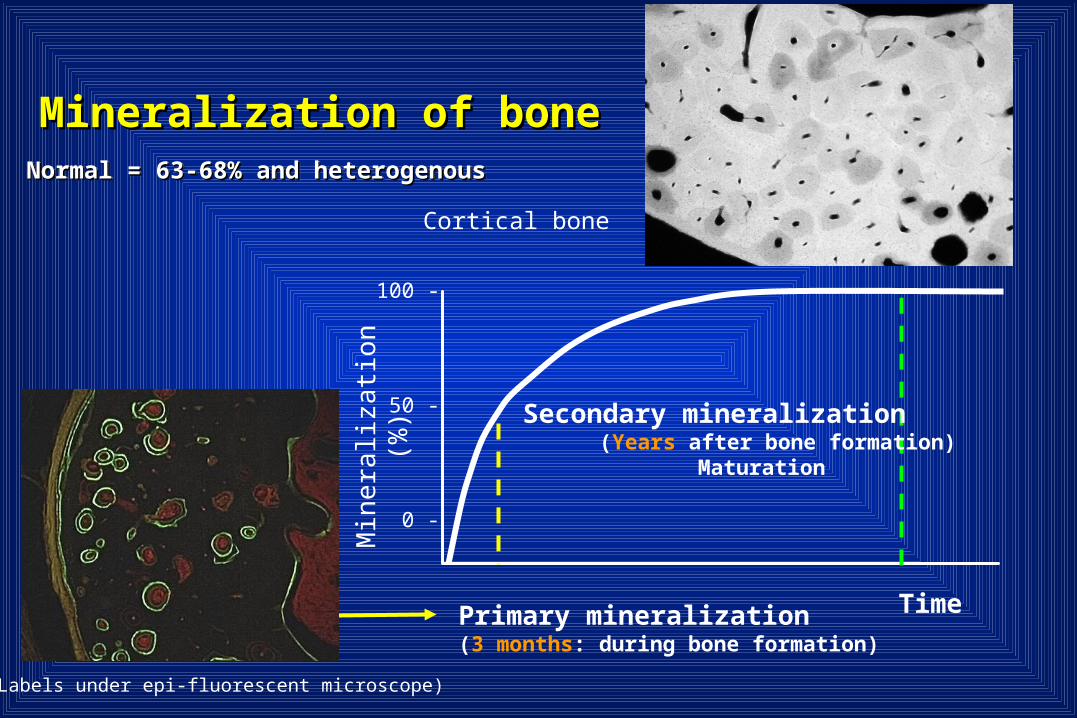
Time
100 -
50 -
0 -
Min
eral
iza
tion
(%
)
Primary mineralization(3 months: during bone formation)
Cortical bone
Secondary mineralization (Years after bone formation) Maturation
Labels under epi-fluorescent microscope)
Mineralization of boneMineralization of boneNormal = 63-68% and heterogenousNormal = 63-68% and heterogenousNormal = 63-68% and heterogenousNormal = 63-68% and heterogenous

(Adopted from Wainwright, Biggs, Currey and Gosline, 1976 modified)
Ash density (degree of mineralization)
Stiffness(Young’s Modulus)
HighLow
Work to Failure (Toughness)
65 66 67 68 (%)
Effects of long-term anti-resorptive therapy
• increased bone mass• increased degree of mineralization
time dependent
increase bone strength
stiffer
decrease bone strength
brittle
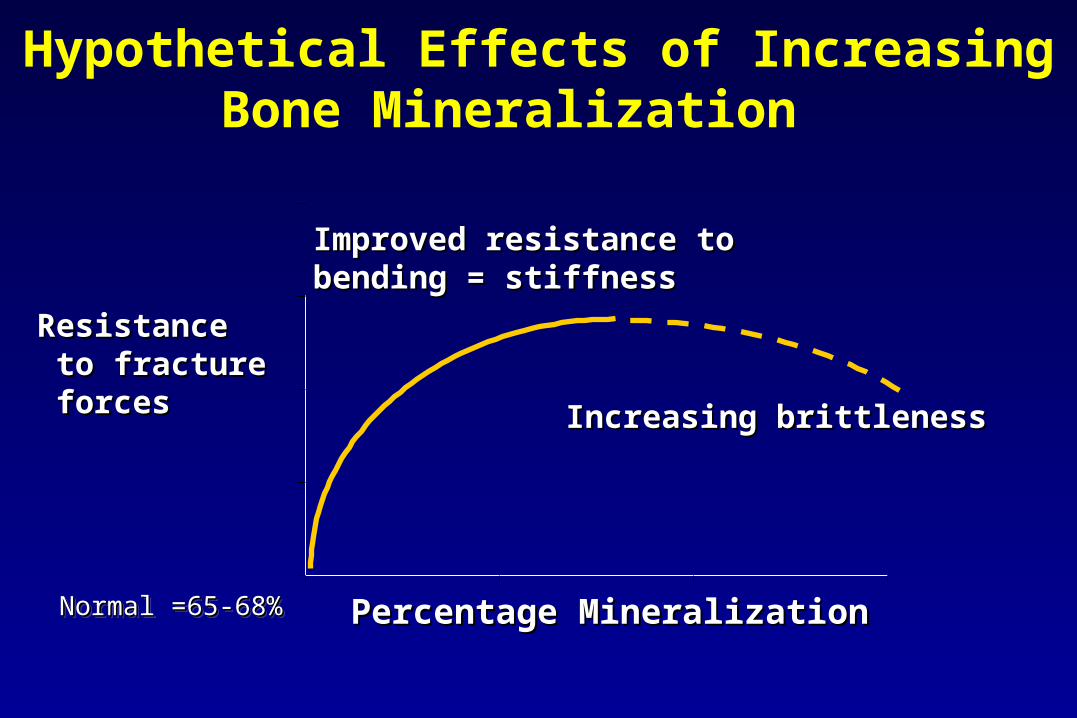
Hypothetical Effects of Increasing Bone Mineralization
Percentage MineralizationPercentage Mineralization
ResistanceResistance to fracture to fracture forcesforces
Improved resistance to Improved resistance to bending = stiffnessbending = stiffness
Increasing brittlenessIncreasing brittleness
Normal =65-68%Normal =65-68%Normal =65-68%Normal =65-68%
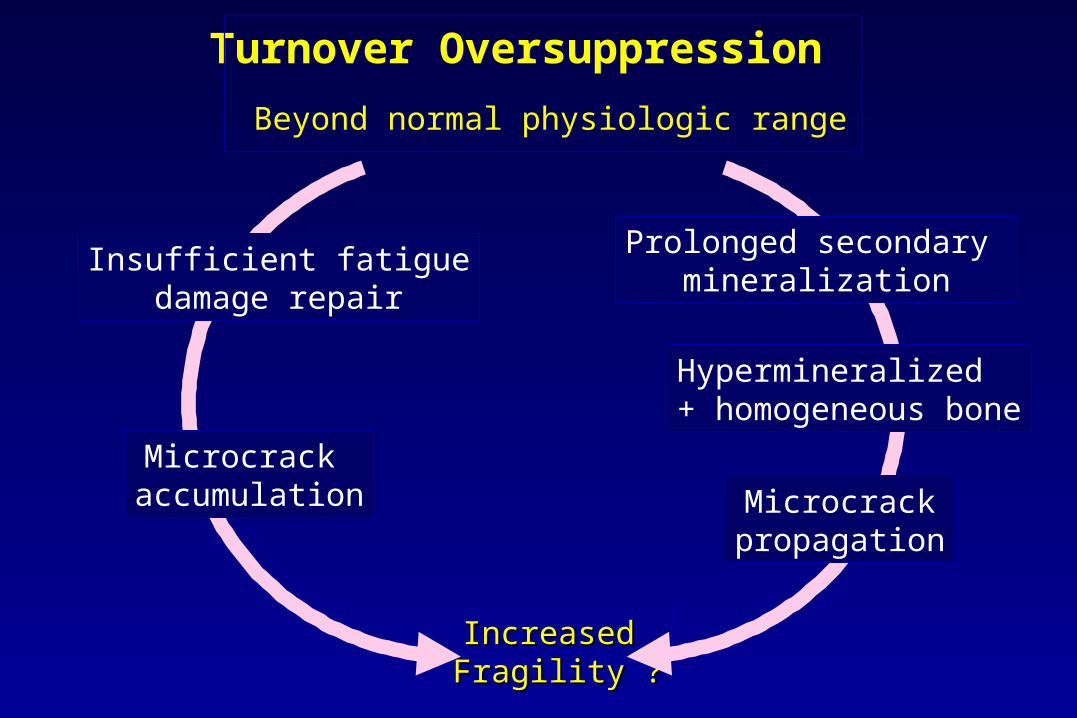
Turnover Oversuppression
Beyond normal physiologic range
Increased Increased Fragility ?Fragility ?
Insufficient fatiguedamage repair
Microcrack accumulation Microcrack
propagation
Prolonged secondary mineralization
Hypermineralized + homogeneous bone
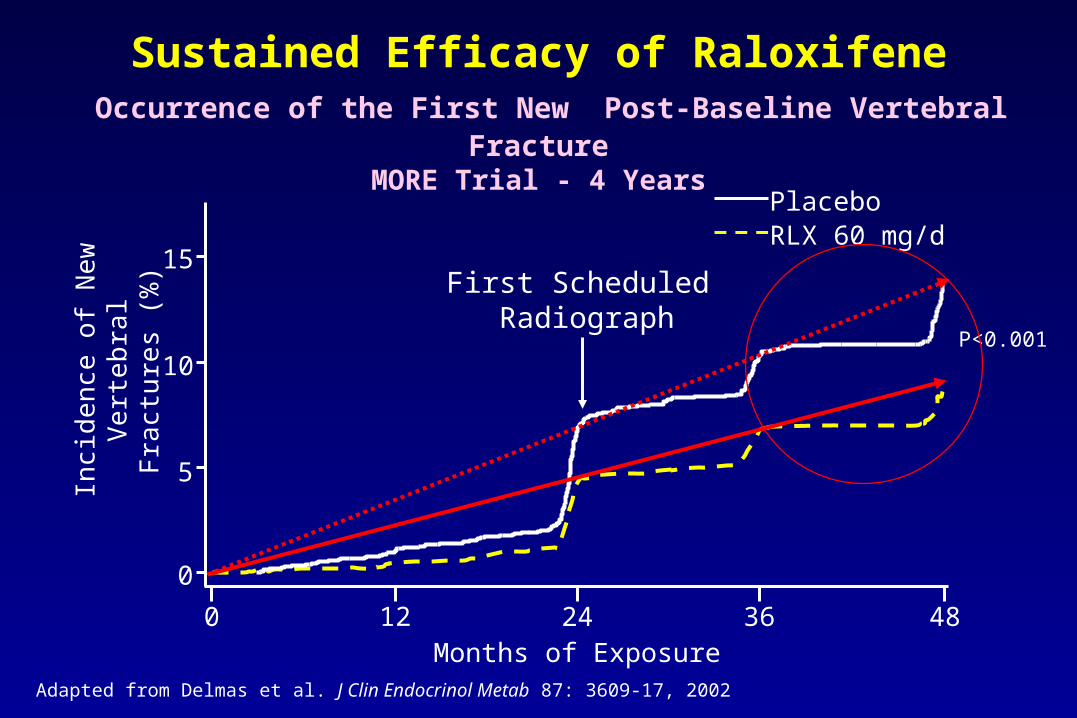
Sustained Efficacy of Raloxifene Occurrence of the First New Post-Baseline Vertebral Fracture
MORE Trial - 4 Years
Adapted from Delmas et al. J Clin Endocrinol Metab 87: 3609-17, 2002
Months of Exposure0 24 36 48
0
5
10
15
Inci
den
ce o
f Ne
w
Ve
rte
bra
l Fra
ctu
res
(%)
PlaceboRLX 60 mg/d
12
First Scheduled Radiograph
P<0.001
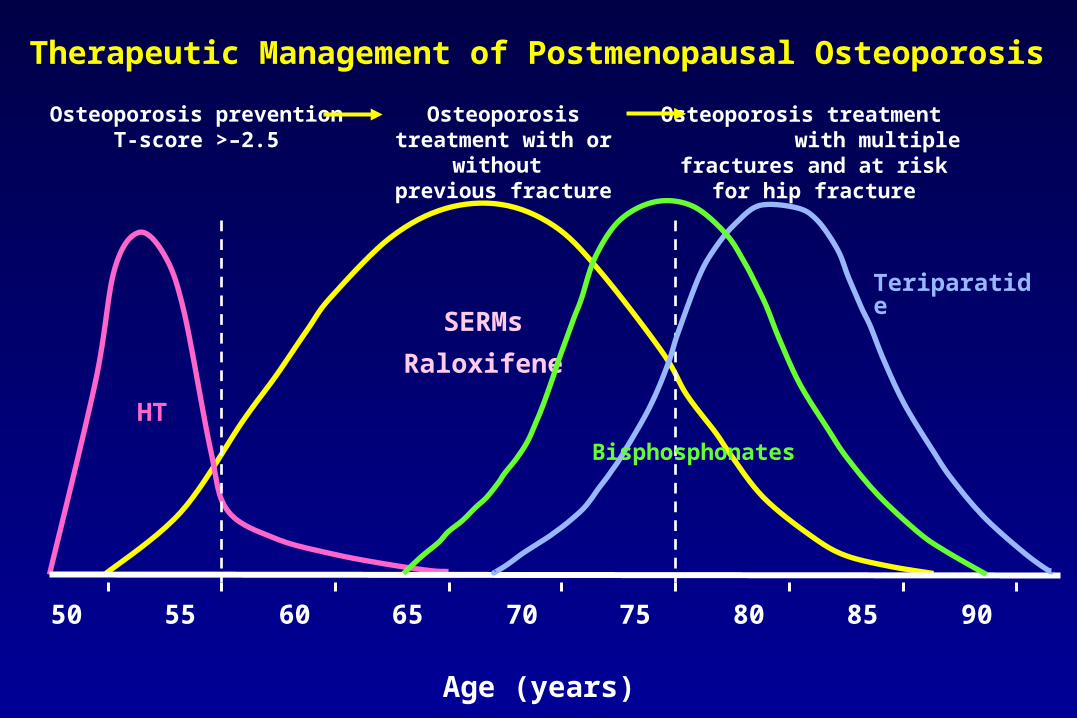
SERMs
Raloxifene
HT
Osteoporosis preventionT-score >–2.5
Osteoporosis treatment with or without
previous fracture
Osteoporosis treatment with multiple fractures and at
risk for hip fracture
50 55 60 65 70 75 80 85 90
Age (years)
Teriparatide
Bisphosphonates
Therapeutic Management of Postmenopausal Osteoporosis

















