New Technique Combined with Suture andIncision Method for Creating a MorePhysiologically Natural Double-Eyelid
Byung Chae Cho, M.D.Jin Suk Byun, M.D.
Daegu, Korea
Background: A combination of incision and nonincision surgical approaches isnecessary to create a more physiologically natural double-eyelid.Methods: The location of the partial incision and the burying location aredetermined. Through a partial incision, the levator aponeurosis is isolated andfixed to the tarsal plate. A single-knot continuous suture is performed. Thelocation of the continuous suture passing through the tarsal plate is at a levelthat is slightly lower than that at which the levator aponeurosis is fixed to thetarsal plate.Results: A total of 562 patients were operated on from November of 2006through October of 2008. The double-eyelid operation was performed on 386patients, the upper blepharoplasty with skin excision was performed in 91patients, and a secondary operation was performed in 85 patients. Combinedmild to moderate blepharoptosis was corrected simultaneously in all cases. Thefollow-up period ranged from 6 months to 2 years. Individual patient recoverytime varied from 2 weeks to 2 months.Conclusions: The advantages of the authors’ technique are as follows: (1) theprocess of forming a double-eyelid is natural; (2) the power of the levatorpalpebrae muscle regarding the eye-opening process is transmitted to pull upthe entire lid margin, allowing the eyes to be easily opened with minimal effort;and (3) there is minimal surgical scarring when the eyes are closed. (Plast.Reconstr. Surg. 125: 324, 2010.)
Double-eyelid surgery, including epicantho-plasty, is the most common aesthetic surgicalprocedure in Korea.1–14 Many procedures re-
garding the Asian double-eyelid operation describedin research studies can be classified as incision andnonincision techniques. In the early surgical proce-dures, a complete incision was considered to be themain surgical technique. However, because of pa-tient demands in which surgical marks should beminimized and postsurgical recovery should be swift,the trends are changing from a complete incision toa partial incision, and from partial incision to theburied suture (nonincision) method.
Generally, a buried suture (nonincision)method leaves no visible scar and has a shorteroperative time, less morbidity, and faster recovery.
However, this method is not suitable in everycase.1–7 This method is difficult to apply in caseswith a weak function of the levator palpebrae mus-cle. In contrast, a complete or partial incisionmethod may result in a strengthening of the le-vator palpebral muscle, in which patients will havea sense of a wide-open feeling of the eyes. How-ever, the levator-to-dermal suture technique andthe tarsodermal fixation method both leave a scar,have long-lasting edema, and require a long re-covery time.
The authors believe that an appropriate com-bination of these two surgical approaches is nec-essary to create a more physiologically naturaldouble-eyelid. The strength of eye opening may beachieved and at the same time surgical scarringmay be minimized. In addition, when the eyes areopen, the double-eyelid line would not be deepFrom the Department of Plastic and Reconstructive Surgery,
Disclosure: The authors have no financial interestto declare in relation to the content of this article.
www.PRSJournal.com324
but rather gently and gradually formed. The pro-cess of forming a double-eyelid is natural andspontaneous. There are no procedures that de-scribe the combination suture and incision tech-nique regarding double-eyelid operations. The au-thors introduce a new technique and report onthe surgical results.
PATIENTS AND METHODSDesign
Careful review of the current state of both eyesis necessary before the operation. A decision mustbe reached regarding the location of the double-eyelid line and an appropriate dimension of it.Once the line for the double-eyelid has been de-termined, the location of the partial incision andthe burying location are decided on (Fig. 1). Aminor incision may be applicable to individualswho have thin skin and a protruding eyelid (Fig.1, b and c). A half incision may be applicable topatients with thick skin, sunken-type eyelids, orblepharoptosis, and in cases in which the double-eyelid line should be changed because of a re-cessed double-eyelid or scar (Fig. 1, a, b, and c). Afull incision may be applicable to patients with (1)redundant skin with droopy eyelids, (2) severelyscarred secondary upper lid blepharoplasty, and(3) high fold correction procedures (Fig. 1, athrough e).
InfiltrationA small amount of 1% lidocaine containing
1:100,000 epinephrine is infiltrated into the skinat the surgical site. The side with a stronger levatorfunction is selected preferentially, a skin incisionis made, and then a slightly higher amount ofanesthesia is injected to the area below the muscle
layer. First, one side is separated and the levatoraponeurosis is fixed to the tarsal plate. Local an-esthesia is allowed to infiltrate into the area belowthe muscle layer by injecting it into the surgicalincision site contralaterally.
IncisionThe orbicularis oculi muscle is dissected in a
perpendicular direction through a partial inci-sion. While lifting the skin margin, using a skinhook, the tarsal plate’s upper border is exposed byseparating the internal and external aspectsdeeply and perpendicularly, in small steps, one ata time (Fig. 2). The anterior septum is opened andthen separated from the levator aponeurosis. Ifthere is herniated orbital fat, the fat is removed.
Tarsal FixationThe levator aponeurosis is disinserted after
isolating it by opening the anterior septum. In thecase of a normal or mild ptosis, the levator apo-neurosis is disinserted between partial incisionline b-c. In the case of moderate or severe ptosis,the disinsertion is slightly extended medially andlaterally from the partial incision line b–c. Thelevator aponeurosis is fixed to the tarsal plate byadjusting the position of the levator aponeurosis.The fixation sutures between the levator aponeu-rosis and the tarsal plate are performed at incisionpoints b and c (Fig. 3). In certain cases, when thelevator function is weak, the levator sheath is af-fixed to the tarsal plate to provide more strength.The location of the tarsal fixation is determined byeither the position of the lid margin before the
Fig. 1. Drawing demonstrating the preoperative design. a, Me-dial limbus; b, medial pupil; c, lateral limbus; b and c, partial inci-sion; a, d, and e, stab incisions.
Fig. 2. Drawing demonstrating the operative procedure.Through a partial incision, the upper border of the tarsal plate isexposed by separating the internal and external aspects deeplyand perpendicularly.
Volume 125, Number 1 • Physiologically Natural Double-Eyelid
325
operation or by the extent of the levator function.By observing the condition of the right and lefteyes, a tarsal fixation is performed first on the sidein which the levator function is somewhat better.Thus, tarsal fixation regarding the side with aweaker levator function is conducted in as close aproximity as possible to the normal side, based onthe principle that this induces a good result. Theside with weaker levator function may be moresensitive to lidocaine. Thus, there is a possibility ofa wrong decision being made if it is fixed to aweaker area rather than the actual fixation height.Therefore, in adjusting the actual strength of theopened eyes, one should pay attention to the factthat the tarsal plate should not be fixed toostrongly, as opposed to that of the normal side.The immediate postoperative height of the lidmargin should be verified by opening the eyeswithout the function of the frontalis muscle.
Suture TechniqueOnce the site of the tarsal fixation is verified
bilaterally, a single-knot continuous suture is per-formed (Fig. 4, above). The medial (Fig. 4, a–b)and lateral (Fig. 4, d–e) locations of the continu-ous suture pass through the tarsal plate (Fig. 4,above and center). The location of the continuoussuture should be at a slightly lower level than thatat which the levator aponeurosis is fixed to thetarsal plate (Fig. 4, below). The location of the knot
should be at the central part of the partial incision,with the knot fitted loosely to the distal end of thelevator aponeurosis. The knot is located beneaththe orbicularis oculi muscle and the levator apo-neurosis (Fig. 4, center and below).
Fig. 4. Drawings demonstrating the procedure of a single-knotcontinuous suture. (Above) Cross-sectional view of a single-knotcontinuous suture. The location of the knot should be at the cen-tral part of the partial incision, and the knot should not be tight atall. (Center) The location of the continuous suture passingthrough the tarsal plate should be at a level slightly lower thanthe level at which the levator aponeurosis is fixed to the tarsalplate. (Below) Final view. The knot loosely fitting to the distal endof the levator aponeurosis is located at a level that is below theorbicularis oculi muscle and the levator aponeurosis. a, Mediallimbus; b, medial pupil; c, lateral limbus; a, d, and e, stab incisions;L, levator aponeurosis; T, tarsal plate.
Fig. 3. Drawings demonstrating the operative procedure. Thelevator aponeurosis is fixed to the tarsal plate by adjusting theposition of the levator aponeurosis. If the levator function is weakin certain cases, the strength of the levator sheath is used to fix itto the tarsal plate. L, levator aponeurosis; T, tarsal plate.
Plastic and Reconstructive Surgery • January 2010
326
After the completion of a continuous suture,the skin is closed after verifying that the eyelidlevels are symmetrical bilaterally in a sitting posi-tion (Fig. 5). If the eyelid levels are not aligned,the eyelid level is adjusted to either a weak orstrong side by means of levator plication or levatorloosening or the eyelid levels are corrected by anadditional fixation procedure.
RESULTSA total of 562 patients were operated on from
November of 2006 to October of 2008. The dou-ble-eyelid operation alone was performed in 386patients, an upper blepharoplasty with skin exci-sion was performed in 91 patients, and a secondaryoperation was performed in 85 patients, using theauthors’ technique. Mild to moderate cases ofblepharoptosis were corrected in conjunction withthe double-eyelid operation and upper blepharo-plasty. In particular, 21 patients presented with mod-erate to severe blepharoptosis. The follow-up periodranged from 6 months to 2 years.
The length of the operation was 40 minutes.Total stitch-out was performed on the third dayafter the operation. The patient’s general recoverytime to achieve a more naturally physiologic dou-ble-eyelid was within approximately 2 weeks to 2months (Figs. 6 through 10). Four hundred thirty-six patients were able to be followed-up between6 months and 2 years. The final results were eval-uated on the basis of the degree of symmetry and the shape of the double-eyelid and the degree
of patient satisfaction. Excellent results wereachieved in 395 patients (90.6 percent), with sym-metry of both double-eyelids and excellent levelsof satisfaction; 32 patients (7.3 percent) showedgood results, nine patients (2.1 percent) achievedfair results, and no patients achieved poor results.
Postoperative complications included double-eyelid asymmetry in 25 cases, loosening of thedouble-eyelid in three cases, and exposure of su-ture material in one case. In 23 cases, in which theheights of lid margins differed bilaterally, the eye-lid levels were corrected by adjusting the levatortension 1 week after the operation. The maincause of the postoperative difference of lid levelsis supposed to be preoperative anatomical struc-tural differences of the levator palpebrae muscleand unreflected levator palpebrae muscle func-tion in both eyes. It is not appropriate to inject thelidocaine mixed with epinephrine solution intothe deep and wide operative field during the op-erative procedure because of the nature of thepostoperative difference regarding both lid levels,which was shown in cases with an overinfiltrationof lidocaine with an epinephrine solution in oneFig. 5. Final view of skin closure.
Fig. 6. Photographs of a 23-year-old woman with a single-eyelid(above) preoperatively and (below) 20 months postoperatively.
Volume 125, Number 1 • Physiologically Natural Double-Eyelid
327
eye. The three cases with weakening or looseningof the double-eyelid fold were corrected with anadditional buried technique. One case exhibitedexposure of the suture material at 4 months afterthe operation. The double-eyelid was maintainedafter removal of the suture material. To avoid ex-posure of suture material, it is important to takecare not to make a superficial passage of the suturematerial in the patient with very thin skin of theupper eyelid.
DISCUSSIONThe mechanism of creating a natural-appear-
ing double-eyelid is known as following the pro-cess. In observing inherently natural double-eye-lids, they begin to form slightly in the process ofeye opening as the levator palpebrae muscle con-tracts and the double-eyelid lines become distinc-tive when the eyes open widely. However, as theeyes are closed, the distinctive fold disappears andeven the buried line cannot be seen. The pro-
cesses of creating a double-eyelid after the oper-ation may be different, depending on the fixationposition and strength of connections from thelevator aponeurosis to the tarsal plate and thelevator aponeurosis to the skin (Fig. 11). There-fore, there are differences regarding the strengthrequired to open the eyes and the depth of adouble-eyelid.
A double-eyelid created by a buried methodhas a loose connection between the levator pal-pebrae muscle and the skin. Thus, this exhibits asimilar process in creating an inherent double-eyelid. However, creating a double-eyelid using aburied technique to an eye with a weak levatorfunction would lead to the patient having a lidmargin level that is lower than that of a normalposition. Application of the buried technique islimited to situations in which the sizes of both eyesare different or in cases where the size of thedouble-eyelid should be changed. In cases inwhich the buried nonincision method is used, the
Fig. 7. Photographs of a 25-year-old woman with a high double-eyelid and moderate ptosis. In this patient, a double-eyelidoperation and ptosis correction were performed at another clinic. However, high double-eyelid and uncorrected ptosis werepresented. (Above, left). Preoperative view with uncorrected ptosis. (Above, right). Preoperative eye closing view showing adeep intense previous double-eyelid operation line. (Below, left) Four-month postoperative view. (Below, right) Four-monthpostoperative eye closing view shows no intense double-eyelid line.
Plastic and Reconstructive Surgery • January 2010
328
process of strengthening the levator function isabsent, and the levator function becomes distinc-tively weaker after the operation (Fig. 11, above).
The mechanism of creating a double-eyelidusing an incision method involves a technique bywhich the dermis or muscle layer of the lower flapis fixed directly to the levator aponeurosis. In thisway, the degree of strength regarding eye openingis transmitted from the levator aponeurosis to thetarsal plate, thereby lifting the lid margin. How-ever, in the process of transmitting this strength,because the power is dispersed and redistributedto the lower flap that is connected to the centralpart, the power of eye opening would not be trans-mitted efficiently. The higher the height of fixa-tion of the lower flap, the greater the loss of thestrength of the eye opening, because significantdispersion of the strength before the eye whileopening is transmitted to the lid margin at theearly stage (Fig. 11, below). Furthermore, the lowerflap that retains tension after the operation con-tains edema, acting as another hindering factorthat further limits the power of the eye while open-ing. If double-eyelid folds are created by means ofusing an incision method along the incision line
by fixing the muscle layer or dermis portion of thelower flap to the levator aponeurosis or the levatorsheath, the strong force of the eye opening isapplied, especially to the fixed area in the line ofthe double-eyelid. As a result, a depression fre-quently develops in the fixed area as opposed tothat of the unfixed area.
When reviewing the mechanism of openingthe eyes after an operation using the authors’method, the levator palpebrae muscle strength,exhibited when the eyes are open immediatelyafter closure, is not affected by the skin and istransmitted directly to the tarsal plate. As a result,the lid margin is preferentially lifted and thestrength of the levator palpebrae muscle that opensthe eye is totally transmitted to pull the lid margin.Thus, the eyes are opened easily with minimal effort,because the strength of the levator palpebrae musclein the early stage of the eye-opening process is firsttransmitted to the tarsal plate.
In the mechanism proposed in this article,unlike the incision method, the lower flap is con-nected loosely with suture material to the distalend of the levator aponeurosis to a level that is
Fig. 8. Photographs of a 26-year-old woman with single-eyelidand mild ptosis (above) preoperatively and (below) 6 monthspostoperatively.
Fig. 9. Photographs of a 25-year-old woman with ptosis and asym-metry of the double-eyelid by suture technique (above) preopera-tively and (below) 17 months postoperatively, with simultaneouscorrection of ptosis and asymmetry of the double-eyelid.
Volume 125, Number 1 • Physiologically Natural Double-Eyelid
329
lower than that of the fixation position of thelevator aponeurosis. In such a structure, the powerof eye opening is efficiently transmitted withoutdiminishing its strength in the early phase of theeye-opening process. In addition, postoperativeswelling on the lower flap is minimal, without lossof the power of eye opening, which allows foreffective correction of ptosis in the event of weaklevator function. This allows for easy lifting of thelid margin as a dynamic lid crease (Fig. 11, below).
With the eyes open somewhat (if the lid mar-gin is moved to the upper direction), tension istriggered gradually by the suture material,therefore gently creating the eyelid folds. At thismoment, the upper eyelid skin, including the lidmargin, has already been moved to the upperdirection. Thus, a soft and natural double-eye-lid, instead of a deep and intense fold, is createdalong the suture material. In addition, becauseonly a little tension is required by the lower flapafter the operation, the advantages of lessedema and a faster recovery process in mostcases are evident. The possibility of weakeningor loosening of the double-eyelid fold in the
authors’ proposed technique is rare comparedwith the suture method alone over the 2-yearfollow-up period.
The proposed technique allows the strengthof the eye opening to be transmitted first and
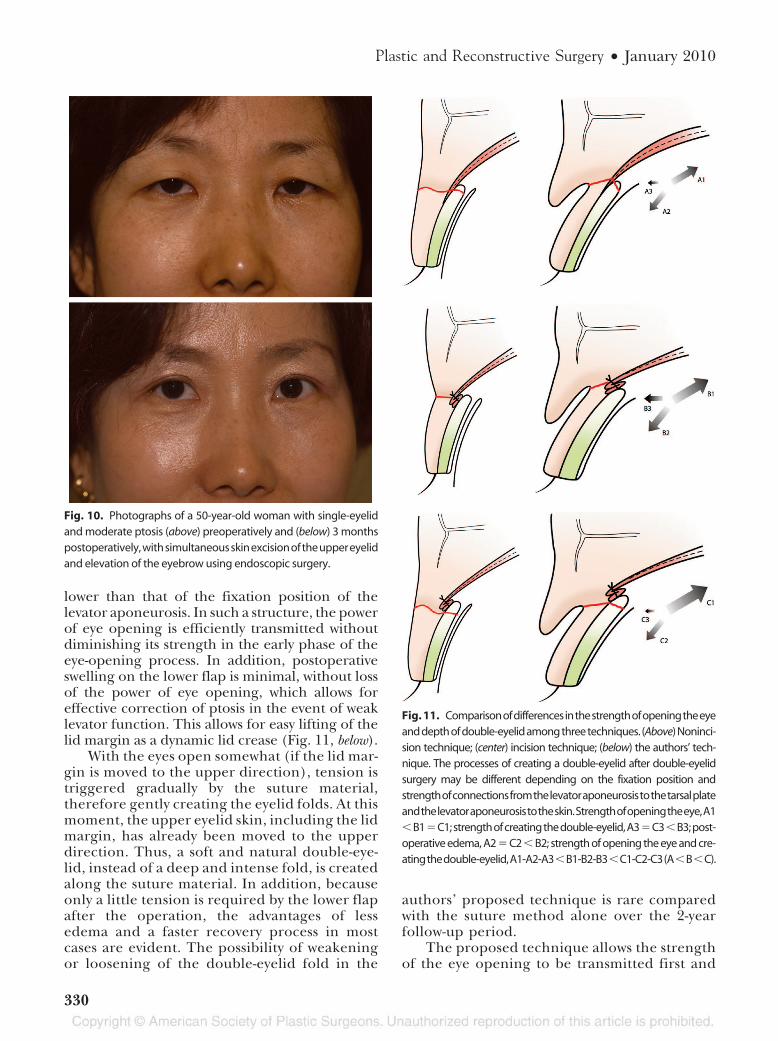
Fig. 10. Photographs of a 50-year-old woman with single-eyelidand moderate ptosis (above) preoperatively and (below) 3 monthspostoperatively,withsimultaneousskinexcisionoftheuppereyelidand elevation of the eyebrow using endoscopic surgery.
Fig. 11. Comparisonofdifferencesinthestrengthofopeningtheeyeanddepthofdouble-eyelidamongthreetechniques. (Above)Noninci-sion technique; (center) incision technique; (below) the authors’ tech-nique. The processes of creating a double-eyelid after double-eyelidsurgery may be different depending on the fixation position andstrengthofconnectionsfromthelevatoraponeurosistothetarsalplateandthelevatoraponeurosistotheskin.Strengthofopeningtheeye,A1�B1�C1;strengthofcreatingthedouble-eyelid,A3�C3�B3;post-operative edema, A2 � C2 � B2; strength of opening the eye and cre-atingthedouble-eyelid,A1-A2-A3�B1-B2-B3�C1-C2-C3(A�B�C).
Plastic and Reconstructive Surgery • January 2010
330
the double-eyelid folds are created during theeye-opening process. Thus, the eye-openingstrength does not become weakened and thedouble-eyelid lines are created distinctively atthe eye-opening phase. In addition, the levatorpalpebrae muscle is connected weakly to thelower flap by the suture material. Thus, the foldscreated by indirect power are gentle but are noteasily disconnected or dissolved in the casesstudied (Fig. 11, below).
CONCLUSIONSIn conclusion, the advantages of the authors’
technique are as follows. First, the power of thelevator palpebrae muscle regarding the eye-open-ing process is transmitted to pull up the entire lidmargin, allowing the eyes to be easily opened withminimal effort. Second, there is minimal surgicalscarring when the eyes are closed. When the eyesare open, the double-eyelid line would not bedeep, and is gently and gradually formed. Third,the difference between the left and right eyelidlevels can be easily adjusted.
4. Megumi Y. Double-eyelid procedure by removal of transcon-junctival orbital fat and buried sutures combined with slingtechnique to avoid wounding the eyelid. Aesthetic Plast Surg.1997;21:254–257.
5. Shiao IS. Oriental double-eyelid: A simplified nonincisionaltechnique using the twin-needle suturer. Plast Reconstr Surg.1995;96:179–182.
6. Shirakabe Y, Kinugasa T, Kawata M, Kishimoto T, ShirakabeT. The double-eyelid operation in Japan: Its evolution asrelated to cultural changes. Ann Plast Surg. 1985;15:224–241.
7. Baek SM, Kim SS, Tokunaga S, Bindiger A. Oriental bleph-aroplasty: Single-stitch, nonincision technique. Plast ReconstrSurg. 1989;83:236–242.
8. Sayoc BT. Plastic construction of the superior palpebral fold.Am J Ophthalmol. 1954;38:556–559.
9. Boo-Chai K. Plastic construction of the superior palpebralfold. Plast Reconstr Surg. 1963;31:74–78.
10. Fernandes LR. The double-eyelid operation in the Orientalin Hawaii. Plast Reconstr Surg. 1960;25:257–264.
12. Lee JS, Park WJ, Shin MS, Song IC. Simplified anatomicmethod of double-eyelid operation: Septodermal fixationtechnique. Plast Reconstr Surg. 1997;100:170–178; discussion179–181.
13. Kim SJ, Song IG, Choi JH, Lee JH, You YJ, Koh IS. Epican-thoplasty using Y-V advancement flap method. J Korean SocPlast Reconstr Surg. 2009;36:200.
14. Baik BS, Suhk JH, Choi WS, Yang WS. Treatment of blepha-roptosis by the advancement procedure of the Muller’s mus-cle-Levator aponeurosis composite flap. J Korean Soc PlastReconstr Surg. 2009;36:211.
Volume 125, Number 1 • Physiologically Natural Double-Eyelid