49
New Payment Models: What Does This Mean for Cardiology Paul N. Casale, MD, MPH, FACC Executive Director, NewYork Quality Care New York-Presbyterian • Columbia • Weill Cornell
New Payment Models:What DoesThisMean for Cardiology
Paul N. Casale, MD, MPH, FACCExecutive Director, NewYork Quality CareNew York-Presbyterian • Columbia • Weill Cornell

Alternative Payment Models

Quality Payment Program
Alternative Payment Models
• An Alte rna tive PaymentModel (APM) is a paymentapproach that provides addedincentives to clinicians toprovide high-qua lity and cos t-e fficient care .
• APMs can apply to
- Care episode (PCMH)
- Specific clinica l condition(episode /bundled payment)
- Popula tion (ACO)
Advanced APMs are a Subs e t of
APMs
APMs
Advanced
APMs


Fragmenta tion Of Care
Specia lty Care
PrimaryCare
In-patient &Out-patient
Hospita l
HomeHealth
HospicePost-acute
Care
Adverse DrugEvents
Hospita lReadmiss ion
DiagnosticErrors
Lack of Communicationand Appropria te
Follow-up

▪Established by HHS–
◦ to accelerate the health care system’s transition to alternative payment models
◦ capture best practices, disseminate information, and apply lessons learned

7
HealthierPeople
Requires theparticipation of theentire health care
community.
SmarterSpending
Shift payment structureto pay for quality of
care rather thanindividual services.
Better CareMove from current fee-for-service payment to amodel that paysclinicians
for quality care andimproved health.
Nationa l Quality S tra tegy

8
Better Care, Smarter Spending, Healthier People
Adoption of Alternative PaymentModels(APMs)
At least 50%of U.S.health care paymentsare so linked.
2018
50%
At least 30%of U.S. healthcare paymentsare linkedto quality and valuethrough APMs.
2016
30%
Goals for U.S. Health Care

9
Category 1
Fee for Se rvice –No Link to
Qua lity & Value
Ca tegory 2
Fee for Se rvice –Link to
Qua lity & Value
Ca tegory 3
APMs Built onFee -for-Se rvice Architecture
Category 4
Popula tion-BasedPayment
A
Foundational Payments forInfrastructure & Operations
B
Pay for Reporting
C
Rewards for Performance
D
Rewards and Penaltiesfor Performance
A
APMs withUpside Gainsharing
B
APMs with UpsideGainsharing/Downside Risk
A
Condition-SpecificPopula tion-Based Payment
B
ComprehensivePopula tion-Based
Payment
Population-Based Accountability
APM Framework

10
For Payment ReformAPM Goals

CMS Charting a Pa th Toward Grea te r Ris k
Cardiac EPM, MSSP Track 3, and Next-Gen ACO Filling Out the Continuum
Continuum of Medicare Ris k Models
BundledPayments
SharedSavings
SharedRis k
FullRis k
• Merit-BasedIncentive PaymentSystem
• MSSP Track 1(50% sharing)
• MSSP Track 2(60% sharing)
• MSSP Track 3(up to 75% sharing)
• Next Genera tionACO Model(80-85% sharedsavings option)
• Next Genera tionACO Model(full risk option)
• Medica reAdvantage(provide r-sponsored)
Pay-fo r-Performance
• Bundled Paymentsfor CareImprovementInitia tive (BPCI)
• Comprehens iveCare for JointReplacement(CJR) Model
• Card iac Epis odePayment Models
©2016 Advisory Board • All RightsReserved • advisory.com
CMS Charting a Path Toward Greater Risk

12

ACOs by Contract Type in the US

14

15

Bundled PaymentsSavingsPotential16

BPCI Cardiac Episodes
• Acute MyocardialInfarction
• Percutaneous CoronaryIntervention
• Coronary Artery BypassGraft
• Cardiac Arrhythmia
• Cardiac Defibrillator
• Cardiac Valve
• Congestive Heart Failure
• Chest pain
• Major CardiovascularProcedure
• Pacemaker
• Pacemaker devicereplacement or revision
• AICD generator or leadrevision
17

Bundled Payment for Care Improvement (BPCI) Model

Medicare , Medica id, Commercia l, and Employer Participants
Where Are Bundled Payments Happening?
Medicare BundledPayments for CareImprovement (“BPCI”)
Medicaid Bundled PaymentPrograms
ArkansasOhioTennessee
Employer Bundled PaymentPrograms
Commercial Bundled PaymentPrograms

Quality Payment Program
Advanced APMsin 2017
Oncology Care Model(Two-sided Risk Arrangement)
Comprehensive Primary Care Plus (CPC+)
Next Generation ACOModelShared Savings Program Track 2 and 3 ACO
Comprehensive Care for Joint Replacement(CJR) Payment Model
Future Advanced APM Opportunities
Advancing Care Coordination throughEpisode Payment Models
Acute Myocardial Infarction (AMI)
Coronary Artery Bypass Surgery(CABG)
New Voluntary Bundled Payment Model
ACOTrack 1+
Comprehensive ESRDCare Model

How Did We Get Here?
CMS Has Been Building to Mandatory Cardiac Bundles for Years
Medicare Partic ipa ting HeartBypas s Demo
Acute Care Epis ode (ACE) Demo
Bund led Payment for CareImprovement (BPCI)
1991-1996• Seven hospita ls• Tes ted bundled Part A and B payments
for two CABG DRGs
2013 – ongoing• 4 Models , includes medica l and surgica l
cardiac episodes1
2
3
CMS Evolution to Card iac Bundling
2009-2012• 3-years , 5 participants• Bundled Part A and B payments for
nine cardiac DRGs
Card iovas cu lar a Familia r Targe t fo rQuality Meas u res
• Readmissions Reduction Programincludes AMI, HF, CABG
• Hospita l-based VBP includes AMI,HF 30-day morta lity ra tes
• AMI, HF 30-Day payment reporting
• AMI, HF excess days metric
©2016 Advisory Board • All RightsReserved • advisory.com
How Did We Get Here?

Cardiac EPM Checklis t
Unders tanding Key Components of the New Cardiac EPM Proposa l
Composition of the cardiac EPM episode
Trans fer rules
Retrospective payment mode l mechanics
Quality requirements
Regula tory waive rs
Ga insharing opportunities
©2016 Advisory Board • All RightsReserved • advisory.com
Cardiac Episode Payment Models

Centra l Elements of Cardiac EPM Bundles
Composition of the ca rdiac EPM episode
Episode ofCare
Target Price
Reconcilia tionProcess
Quality
All care (Part A & B) re la ted to anchor hospita liza tion(AMI & CABG) and 90 days pos t-discharge
Episode ta rget - up to a 3% discount off ofhis torica l/regiona l spending performance
Calcula te diffe rence between episode spend andta rge t price
Specific measures tha t CMS has defined as importantindica tors of qua lity for ca rdiac EPMs
©2016 Advisory Board • All RightsReserved • advisory.com
Central Elements of Cardiac EPM Bundles

Partic ipa ting Markets Would Be Selec ted Randomly
Eligibility Crite ria Based on AMI Volumes
Key Elements of Cardiac EPM Market Se lec tion
• 98 marke ts would be chosenrandomly from 284 eligibleMetropolitan S ta tis tica lAreas(MSAs)
• Eligible MSAs:
• >75 AMIs per year
• The AMI and CABG episodeswould be implemented toge therin selected marke ts
©2016 Advisory Board • All RightsReserved • advisory.com
Participating Markets Randomly Selected

Taking a Long View of Pa tient Care
EPMs Would Track Cos ts , Outcomes Up to 90 Days Pos t-Discharge
AnchorHospitalization
Episode Trigger Episode Ends
EPM Propos ed Epis ode and Inc luded Services
90 DaysPost-Discharge
©2016 Advisory Board • All RightsReserved • advisory.com
Taking a Long View of Patient Care

CMS Would Use Retrospective Reconcilia tion to Adjus t Hospita l PaymentsPropos ed Hos pita l Payment Proces s Under Cardiac EPM
1 32Fee-fo r-Service Billing Payment Reconcilia tionComparis on to Targe t
Hospita l bills FFS ,ece ive payment assua l; CMS tracks
claims
Tota l cos tsmpared toge t price based
on his toric cla ims
If over ta rge t hospita lays CMS; ifer, rece ives
reconcilia tion
Phas es in Ups ide andDowns ide Financia l Ris k
Incorporates Blend of Regional and FacilityHis toric Claims Data
• Target price based on 3 years of his toric cla ims
• Hospita l & regional cla ims define targe t price
• In 2020 and 2021, only regional data used
• Partia l ups ide risk in year 1Phased to 20% by year 4
• Partia l downs ide risk in year 2 & 3Full risk (20%) in years 4 & 5
©2016 Advisory Board • All RightsReserved • advisory.com
No Immediate Change in Billing

Two Factors Would Dete rmine Whether You Pay CMS, or CMS Pays You
1 2Medicare Paymen tBelow Targe t
Meet Quality S tandards
EPM episode paymentsmust be below CMS ’ta rge t
Hospita l performance on EPMquality compos ite determinesdiscount ta rget and reconcilia tionpayment eligibility
Reconcilia tion paymen t e lig ib ility dependenton min imum quality s tandard
If hospita l comes in below target price but doesnot achieve a t leas t “Acceptable ” ra ting, they willnot be e ligible for reconcilia tion payment.
©2016 Advisory Board • All RightsReserved • advisory.com
Reconciliation to be Based on Payment and Quality
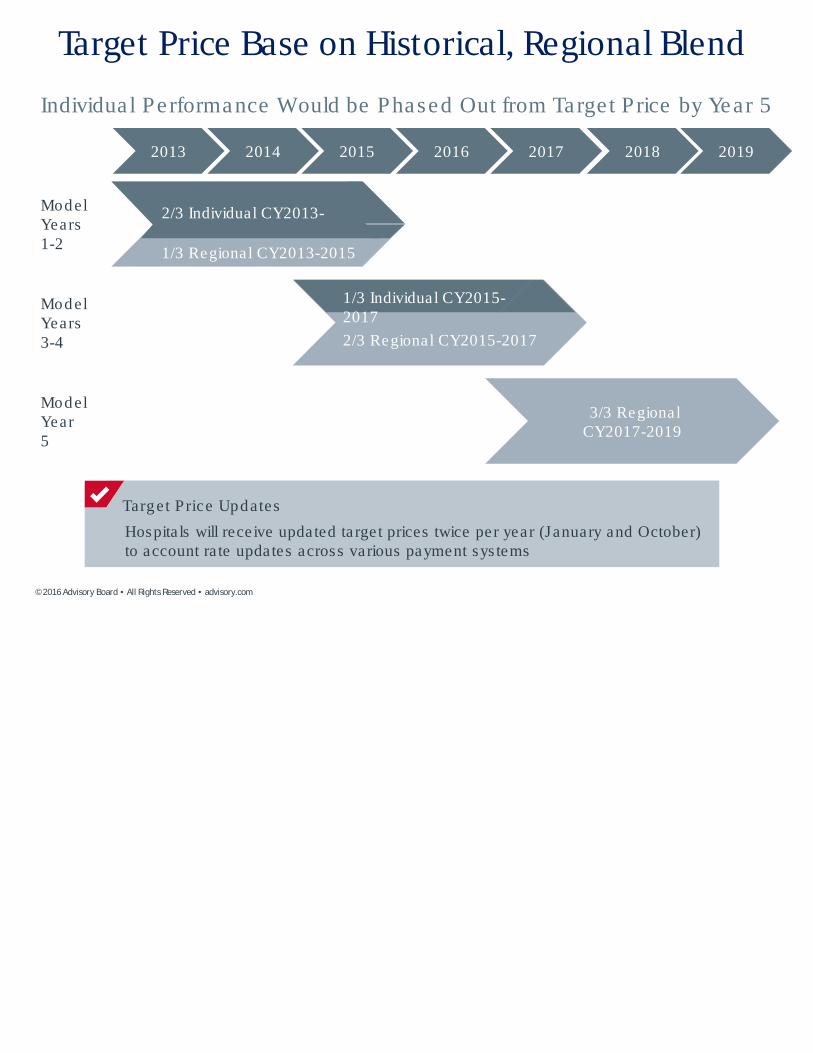
Individua l Performance Would be Phased Out from Target Price by Year 5
20162015 2017 2018 2019
ModelYears1-2
ModelYears3-4
20142013
ModelYear5
1/3 Individual CY2015-2017
2/3 Regional CY2015-2017
2/3 Individual CY2013-2015
1/3 Regional CY2013-2015
3/3 RegionalCY2017-2019
Hospita ls will rece ive updated targe t prices twice per year (January and October)to account ra te updates across various payment sys tems
Target Price Updates
©2016 Advisory Board • All RightsReserved • advisory.com
Target Price Base on Historical, Regional Blend

QualityMeas ure
Defin itionWeight inCompos ite
Co llec tion
30-DayMorta lity
30-day, a ll cause , risk-s tandardized morta lity ra tefollowing a hospita liza tion for AMI
50% Claims -based perInpa tient QualityReporting (IQR)(NQF #0230)
AMI Exces sDays
Excess days in acute care (ER,observa tion, and readmis s ion daysfollowing a hospita liza tion for AMI
20% Cla ims -based perIQR
HCAHPSSurvey
Patient experience (not specific toDRGs).Communica tion, painmanagement, cleanliness ,quie tness etc.
20% Patient Survey(NQF #0166)
Hybrid AMIMorta lityVoluntaryData
30-day, risk-s tandardized AMImorta lity ra te , us ing a combina tionof cla ims data and EHR datasubmitted by hospita ls
10% Volunta rysubmis sion(NQF #2473)
©2016 Advisory Board • All RightsReserved • advisory.com
AMI Quality Measures

A Potentia l Replacement for the Current 30-Day Morta lity Measure
30-Day AMI Morta lityMeasure (NQF #0230)
• Same measure cohortand outcome
Claims Data EHR Data
Five core clinical data elements :
• Age
• Heart ra te
• Sys tolic blood pressure
• Troponin
• Creatinine
Hybrid AMI Morta lity Meas u re
©2016 Advisory Board • All RightsReserved • advisory.com
Hybrid AMI Mortality to Measure Clinical Status

Gainsharing opportunitie s
Ris k-Sharing Res tric tions
Hospita l may only share funds from in te rna ls avings or fina l reconc ilia tion /repayment
Maximum phys ic ian ga ins ha re is 50% ofPart B phys ic ian fee s chedule
Gainsharing payments must be partly bas edon qua lity metrics s e t by the hos pita l (notre fe rra ls /pa tient volumes)
If sharing downs ide risk, the hos p ita l mus tre ta in 50% of repayment ris k.
Maximum repayment amount for onepartner is 25%
©2016 Advisory Board • All RightsReserved • advisory.com
CMS Proposes Options for Gainsharing

Waiver of “Inc ident To”Direc t Supervis ion Requirement fo rpos t d is charge home vis its
Non-phys ician and clinica l s ta ff can provide home vis its (phys iciandoesn’t have to be present) - for pa tients not e ligible for homehealth services . 13 vis its for AMI and 9 vis its for CABG EPM.
Telehealth Services
Waive the geographic s ite requirement for te lehea lth, a llowingpa tients to receive te lehea lth services no matte r where they areloca ted. Also would waive the originating s ite requirement.
Skilled Nurs ing Fac ility Three -Day Rule
CMS will waive the SNF 3-day rule only for the AMI EPM ifa pa tient is dis charged to a SNF with a t leas t a three s tarquality ra ting (s tarting in performance year 2)
©2016 Advisory Board • All RightsReserved • advisory.com
Proposed Cardiac EPM Program Waivers

Unders tanding the Issues , Defining the Terms
Trans fe r rules
Before Going Further, DefineYour Terms
• Partic ipant: Hospita l in se lectedMSA for EPMs
• Nonpartic ipant: Hospita l not inselected MSA for EPMs
• Inpa tien t to inpa tien t trans fe r:Patient admitted at initia l hospita l,then trans fe rred to differenthospita l
• Outpa tien t to inpa tien t trans fer:Patient not admitted a t initia lhospita l then trans ferred todifferent hospita l (e .g., s een in ERand immediate ly trans fe rred),
Key Ques tions Regard ing Trans fe rs
If an AMI patient s ta rts a tone hospita l and then issent e ls ewhere for care ,who is financia llyrespons ible?
If the DRG at the initia lhospita l is diffe rent thanthe DRG at the trans fe rhospita l (e .g., if AMI patienthad a CABG), how is theepisode ta rget price set?
©2016 Advisory Board • All RightsReserved • advisory.com
Hospital Transfers a Concern
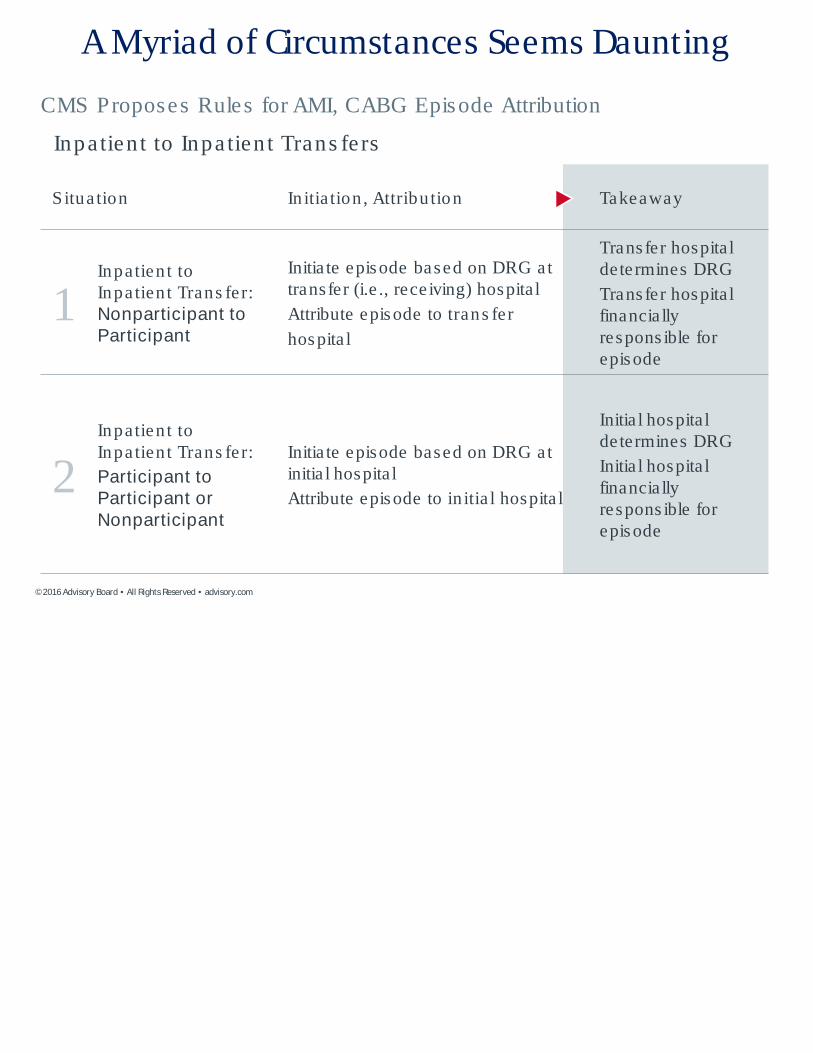
CMS Proposes Rules for AMI, CABG Episode Attribution
Situa tion In itia tion , Attribu tion Takeaway
1Inpatien t toInpa tien t Trans fe r:Nonparticipant toParticipant
Initia te episode based on DRG attrans fer (i.e ., rece iving) hospita l
Attribute episode to trans fer
hospita l
Trans fer hospita ldete rmines DRG
Trans fer hospita lfinancia llyrespons ible forepisode
2Inpatien t toInpa tien t Trans fe r:
Participant toParticipant orNonparticipant
Initia te episode based on DRG atinitia l hospita l
Attribute episode to in itia l hospita l
Initia l hospita lde termines DRG
Initia l hospita lfinancia llyrespons ible forepisode
Inpa tien t to Inpa tien t Trans fe rs
©2016 Advisory Board • All RightsReserved • advisory.com
AMyriad of Circumstances Seems Daunting

CMS Proposes Rules for AMI, CABG Episode Attribution
Situa tion In itia tion , Attribution Takeaway
3
Outpa tien t toInpa tien t Trans fer:
Nonparticipant orparticipant toParticipant
Initia te episode based on DRG attrans fe r (i.e ., receiving) hospita l
Attribute episode to trans fer
hospita l
Trans fe r hospita lde termines DRG
Trans fe r hospita lfinancia llyrespons ible forepisode
4Outpa tien t toInpa tien t Trans fe r:
Participant toNonparticipant
No AMI or CABG model initia ted No episode initia ted
Outpa tien t to Inpa tient Trans fe rs
©2016 Advisory Board • All RightsReserved • advisory.com
AMyriad of Circumstances Seems Daunting (Cont.)

Responding to the Proposed Rule for Cardiac EPMs
1 Unders tand the s ources of cos ts in epis odes ; identifyhigh areas of episodic cos t and eva lua te inte rna l e fficienciesand loca l PAC provider outcomes .
2 Patien t engagement; eva luate care management program,access to care , communica tion tools including EMR patientporta l.
3 Phys ic ian leaders hip ; engage and educa te cardiovascula rspecia lis ts and team members on the ca rdiac EPM program,deve lop coherent s tra tegy and organiza tiona l s tructure .
Even if not chosen for participa tion, ca rdiologis ts shouldcons ider this proposa l to be a s igna l tha t future bundling orepisodic payment re form is like ly to occur
©2016 Advisory Board • All RightsReserved • advisory.com
Preparing for Cardiac Episode Payment Models

Unders tanding Costs a Crucia l Step to Deve loping an EPM Stra tegy
Percen tage of To ta l Cos ts Attribu ted to Each Setting
Medicare, 2014
©2016 Advisory Board • All RightsReserved • advisory.com
Assessing Costs At 90 Days After Admission

ACCKey Comment Areas:Proposed Rule for Cardiac EPMs
• Clinical homogeneity in the AMI model
• AMI model quality measures
• Advanced APMs
• Special policies for hospital transfers ofbeneficiaries with AMI
• Risk sharing and financial arrangements underEPMs
• Additional care coordination considerations

Clinical Homogeneity
CMS proposes to include beneficiaries who aredischarged under AMI (MS-DRGs 280-282) and PCI(MS-DRGs 246-251) with an AMI ICD-10 CMdiagnosis code in the principal or secondarydiagnosis position.
ACC strongly recommends limiting the AMI model toSTEMI patients discharged with AMI code only in theprincipal diagnosis position.
39

Proposed AMI Quality Measures
4 measures: 3 required, 1 voluntary
Measure Weight
• MORT-30-AMI (NQF #0230) 50%
• AMI Excess Days 20%
• HCAHPS Survey (NQF #0166) 20%
• Hybrid AMI Mortality (NQF #2473) 10%
Voluntary Data
40

AMI Quality Measures and Role of NCDR
• The ACC recommends reducing the weighting forthe MORT-30-AMI measure to no more than 30%ofthe composite quality performance score
• The ACC recommends reallocating the remaining20%of the weight to the Core Quality MeasureCollaborative (CQMC) cardiovascular measures setand measures reported through NCDR.

Transfer Policy
• The ACC strongly recommends attributing patientsto the hospital where revascularization proceduresare performed rather than the anchor hospital
• The admitting hospital that transfers the patientfor treatment has little or no control over the rest ofthe episode and thus should not be heldaccountable.
42

Other Positions
Risk Sharing and Financial Arrangements underEPMs
• The ACC recommends including both Part AandPart B services in gainsharing arrangements toachieve truly meaningful risk sharing.
Additional Care Coordination Considerations
• The ACC urges CMS to make resources for carecoordination strategies available to supportadvancing care coordination.
43

Bundled Payment Model: Opportunities
• Representscontinued movement towardsa value-based payment system that focuseson improvedquality and value – key elementsof ACC’sstrategicplan.
• ReflectsCMS’ continued efforts to find new waysforspecialists to be rewarded for deliveringquality care
• May qualify asan Advanced Alternative PaymentModel (APM) under MACRA.
• Opportunity to extend the value of NCDR(ACTION,Cath-PCI) and ACCquality programs.

Bundled Payment Model: Challenges
• Different from previousCMSbundlespayment models:
– Higher-risk patients
– Surgeriesare not elective (Physicianshave lesscontrol overtiming/planning)
• Those without experience with bundles will have littletime to adapt or plan in advance.
• Changes in payment structuresmust be driven byclinical practices that improve patient outcomes.
• Potential for unintended consequences

Program Would Sta rt J uly 1, 2017
2016 2017 2018 2019 2020 2021
6 Months 12 Months 12 Months 12 Months 12 Months
Card iac EPM Performance Periods
Downside riskcommences on
April 1, 2018
©2016 Advisory Board • All RightsReserved • advisory.com
Program Would Start July 1, 2017

Quality Payment Program
• MACRA established the Phys ician-Focused Payment Model
Technica l Advisory Committee (PTAC) to review and assess
Phys ician-Focused Payment Models based on proposa ls
submitted by s takeholde rs to the committee .
• The PTAC is a federa l advisory committee tha t provides
independent advice to the Secre ta ry. The PTAC is supported
by HHS Office of the Ass is tant Secre ta ry for P lanning and
Evalua tion.
• This committee provides a unique opportunity for s takeholde rs
to pa rticipa te in the deve lopment of new models and to he lp
de te rmine priorities for the phys ician community
Physician-Focused Payment Model TechnicalAdvisory Committee

Quality Payment Program
PFPM =Phys ic ian -Focus ed Payment
Model
Goal to encourage new APM options forMedicare clinicians
PFPM Technical Advisory Committee (PTAC)
Submiss ion ofmode l
proposa ls byStakeholders 11 appointed care
delivery experts tha treview proposals , submitrecommenda tions to HHS
Secre tary
Secre tarycomments onCMS webs ite ,
CMScons iders
tes tingproposedmode ls
Mode ls withfavorable
response go toCMS
InnovationCenter
49

















