18
NHS Library Services to support Commissioning in the South West: a Workshop Lyngford House 21 st March 2013
| Date post: | 03-Jan-2016 |
| Category: |
Documents |
| Upload: | david-allen |
| View: | 220 times |
| Download: | 0 times |

NHS Library Services to support Commissioning in the South West: a Workshop
Lyngford House 21st March 2013

The new NHS landscape requires NHS Library Services to review their service offering and adapt their service provision to meet the needs of a wider user base.
Clinical commissioners have been identified as a group of potential library users that our Library Services could support more effectively
The work will have a bearing on the ways in which we approach other specific user group requiring specialist knowledge services
Background to the Workshop
• 11.00am - Welcome, objectives and outline of the Workshop• 11.05am - Explores the world of clinical commissioners and their need for
high quality information.• 11.20am - Helping Library Managers to understand the skills that they
require to provide a tailored knowledge service to meet clinical commissioning needs.
• 12.30pm - Lunch• 13.15pm - The West Sussex Knowledge and Library Team to provide details
on how this specialist service has been developed.• 14.15pm - How this service could be introduced in the South West• 14.45pm - Recommendations and next steps• 15.15pm - Summary and feedback
Agenda for Today’s Work Shop

• An understanding of the need for engagement with clinical commissioners.
• A key stakeholder map of the South West, with established leads as contacts and channels for future engagement with each clinical commissioning group
• Consideration of promotional opportunities to be developed for commissioners
• An understanding of the process of synthesized knowledge to support commissioners
• A training needs analysis of the skills and knowledge required to undertake specialist support for commissioners
• Agreed actions for individuals and/or groups, including requirement for further facilitation/external support
Outputs from the Workshop

• An understanding of the need for engagement with clinical commissioners.
Output 1

• From April 2013, the NHS Commissioning Board (NHSCB) will be established with an overarching role to ensure that the NHS delivers better outcomes for patients within its available resources and upholds and promotes the NHS Constitution.
• The NHSCB will work through its national, regional and local area teams to discharge these responsibilities
• NHS Commissioning Board has a budget of £95.6 billion to deliver the mandate. Within this overall funding, it has allocated £65.6 billion to local
health economy commissioners: CCGs and local authorities.• £25.4 billion has been allocated for the NHS CB’s commissioning of
specialised healthcare, primary care and military and offender services. These are being commissioned nationally for the first time to ensure increased quality of care for patients through increased consistency of provision
The World of Commissioning

• The NHSCB will work in partnership with CCGs and other local networks; and will ensure that there is a locally responsive approach, supported by joint health and wellbeing strategies, joint strategic needs assessments (JSNAs) and pharmaceutical needs assessments (PNAs)
• CCGs will commission the majority of NHS services for their populations, drawing on the unique role of general practice in connecting with patients and acting as the intermediary for most of their care.
• CCGs will have a statutory responsibility to support the NHSCB to improve the quality of primary medical care. Even though they are responsible for local services, to commission primary care as well would create a conflict of interests
NHS Commissioning Board

The national measures are based on measures in the NHS Outcomes Framework and quality premiums are paid to CCGs for
• reducing potential years of lives lost through amenable mortality • reducing avoidable emergency admissions • ensuring roll-out of the Friends and Family Test and improving patient
experience of hospital services • preventing healthcare associated infections (12.5% of quality premium)But... total payment for a CCG based on its performance against these 4
national measures will be reduced if they do not meet the NHS Constitution rights or pledges for patients in relation to
(a) maximum 18-week waits from referral to treatment(b) maximum four-hour waits in A&E departments(c) maximum 62-day waits from urgent GP referral to first definitive
treatment for cancer, and (d) maximum 8-minute responses for Category A red 1 ambulance calls.
National Measures of quality in commissioning

• A key stakeholder map of the South West, with established leads as contacts and channels for future engagement with each clinical commissioning group
Output 2

Geographic profile
Source: Oxford Consultants for Social Inclusion (OCSI)
The South West region is approximately 250 miles long and covers 9,200 square miles – excluding Dorset
Urban areas have the highest rates of deprivation, though there are pockets of rural deprivation - 2.2% of the regional rural South West population living in the most deprived areas.
More than 130,000 people in rural areas in the South West have no access to a car or van (8.1% of all people living in rural areas in the South West).
Less than 2,000 households in the South West are more than 10km from the nearest GP. More than half of these households are located in North Cornwall, where 2.6% of households (1,000 households) are more than 10km from the nearest GP.
757,000 households in the South West are more than one hour travel time from a hospital by public transport (including 127,000 households with no access to a car or van).

Population The South West population was just over 5.2 m in 2011, an
increase of 7.3% since 2001. This compares with an overall increase of 7.9% for the UK over the same period.
Population density was 222 / km2 (570 /sq mile) People aged 65+ in the South West in 2011 was 19.6% of the
population, compared with 17.6% for the under-16s. This compares with averages for the UK of 16.4 and 18.7% respectively.
In the South West men aged 65 in 2007–09 could expect to live another 18.6 years and women 21.3 years. This compares with 17.8 and 20.4 years in the UK as a whole.
employment rate was 74.0 per cent in Q4 2011, compared with 70.3 per cent for the UK as a whole.
unemployment rate was one of the lowest of the regions at 6.1 per cent, compared with 8.4 per cent for the UK.
Density2,500 or over1,000 – 2,499500 – 999250 – 499100 – 249< 99
Within the region, the unemployment rate was lowest in Cotswold at 3.9 per cent and highest in Torbay unitary authority (UA) at 8.8 per cent for the year to September 2011.

NHS Organisations
NHS provider organisations in the South West:
12 acute trusts3 healthcare trusts5 partnership trusts2 ambulance trusts1 specialist trust1 community services trust (potential)
Other NHS organisations/ networks:6 Cluster PCTs – 11 CCGs4 Local Area Teams2 Academic Health Science networks1 Clinical senate2 Public health centres1 West Local Delivery Partnership1 CLAHRC 2 HIECs
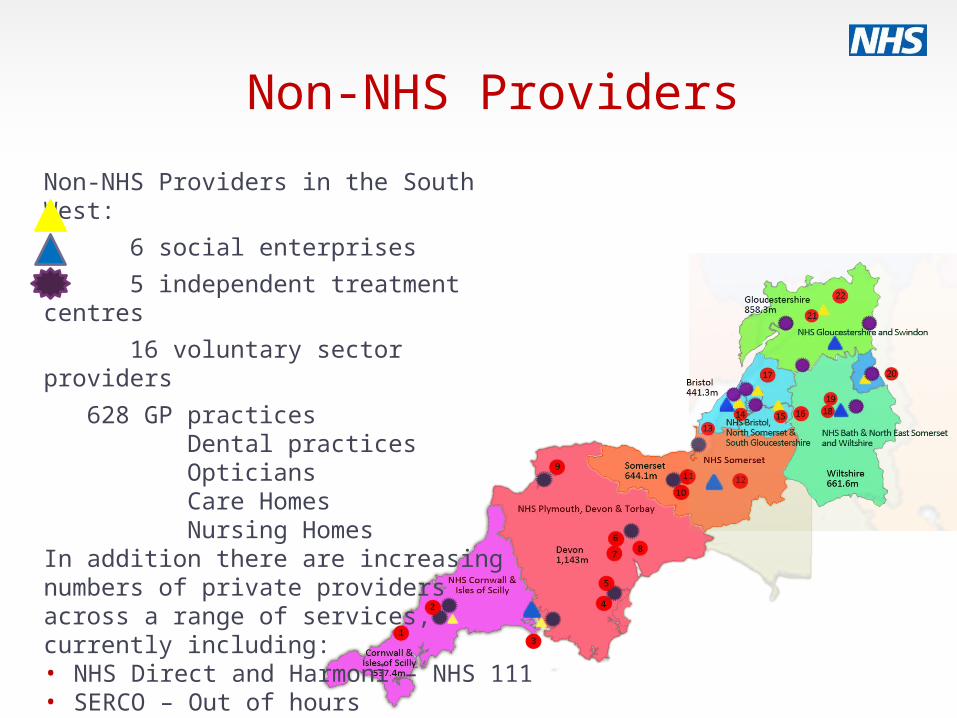
Non-NHS Providers
Non-NHS Providers in the South West:
6 social enterprises
5 independent treatment centres
16 voluntary sector providers
628 GP practices Dental practices Opticians Care Homes Nursing HomesIn addition there are increasing numbers of private providers across a range of services, currently including:• NHS Direct and Harmoni – NHS 111• SERCO – Out of hours• Virgin Care – Children’s services• South West Pathology services

Local Authorities The South West has a good record of working
closely with Local Authorities Swindon, Torbay, Bath & North East Somerset all have combined health and care services
13 Health & Wellbeing Boards
Consideration of promotional opportunities to be developed for commissioners
Output 3

• An understanding of the process of synthesized knowledge to support commissioners
• A training needs analysis of the skills and knowledge required to undertake specialist support for commissioners
Output 4
Agreed actions for individuals and/or groups, including requirement for further facilitation/external support
Output 5
Recommendations and Feedback




![NHS ST HELENS CLINICAL COMMISSIONING GROUP CONSTITUTION · 2018-11-27 · NHS St Helens Clinical Commissioning Group’s Constitution - 4 - Version: [4] | NHS England Effective Date:](https://static.documents.pub/doc/80x56/5ec82fa56a6d915d871ef75d/nhs-st-helens-clinical-commissioning-group-constitution-2018-11-27-nhs-st-helens.jpg)












