NHS 111 Stakeholder Briefing Contact: Programme Manager: Dr Kathryn MacDermott, Assistant Director Strategy & QIPP Communications & Engagement Project Lead: Alex Louis “NHS 111 can be designed locally to reach far beyond the initial vision” NHS 111 Lessons learnt and shared understanding, NHS 111 Programme, Version 1.2, September 2011
Transcript
NHS 111 Stakeholder Briefing
Contact:
Programme Manager: Dr Kathryn MacDermott, Assistant Director Strategy & QIPP
Communications & Engagement Project Lead: Alex Louis
“NHS 111 can be designed locally to reach far beyond the initial vision” NHS 111 Lessons learnt and shared understanding, NHS 111 Programme, Version 1.2, September 2011
A reminder…what is NHS 111?
• A new 24/7 telephone service which aims to make it easier for people to access local health services when they urgently need medical help or advice but it's not a life-threatening situation (i.e. not a 999 emergency)
The strategic context
• Coalition government commitment to introduce a three digit number to access non-urgent care nationwide by 2013.
“We will develop a coherent 24/7 urgent care service in every area in England that makes sense to patients when they have to make choices about their care. This will incorporate GP out of hour’s services and provide urgent medical care for people registered with a GP elsewhere. We will make care more accessible by introducing, informed by evaluation, a single telephone number for every kind of urgent and social care and by using technology to help people communicate with their clinicians.”
• Consultation for a three-digit number carried out in 2009 showed clear evidence of support from patient representative groups and clinicians.
• Early pilots introduced in 2010.
• London pilots due 2012
What are the benefits of NHS 111?
• Introduction of a consistent clinical assessment tool and referral management.
• Reduction in attendances at A&E and an increase in patients being directed and conveyed to the most appropriate care setting for their needs.
• Activity shifted to more clinically appropriate, lower cost care settings.
• Reduction in ambulance ‘999’ activations and conveyances to A&E.
• Reduction in unscheduled admissions by directing patients to home-based nursing/care services.
• Information on the capacity of, and demand for, urgent care provision available via Directory of Services (DoS) reporting, allowing commissioners to respond more intelligently to local needs/demands.
• Improved clinical governance of all general practice and community services through caller outcome information.
• Signposting of access to NHS dentistry in hours as well as Out of Hours (OOH).
• Improved end of life care services through coordination of individual patient care.
• An increased percentage of patients achieving preferred place of death.
Support for a three digit number
• DoH started work in 2008 scoping a single number to access NHS urgent healthcare services
• Included public research which showed overwhelming support for a ‘999 style’ memorable number
• Public support for introduction of 111 very high; 88% of people interviewed said likely to use the new service
• Public support matched with extensive support from British Medical Association, Royal College of General Practitioners & Royal College of Physicians
• Provider organisations including LAS, NHS Direct and out of hours providers are positively engaged in 111 pilot
• All SHAs support the introduction of single number to access urgent healthcare services.
NHS 111: more than a number
• Provides a definitive clinical assessment at the first point of contact, without the need to call patients back.
• The service will direct people to the right NHS service, first time, without the need for them to be re-triaged.
• It will be able to transfer clinical assessment data to other providers and book appointments for patients when locally agreed and appropriate.
• It works alongside the London Ambulance Service (LAS) and will be able to despatch an ambulance without delay and without the need for the patient to repeat any information.
Unplanned care
• Review use of urgent care centres
• Review use of walk in centres • Develop and implement unscheduled care
strategy
• Implement 111
Key deliverables:
• Reduce the level of unscheduled secondary care activity
• Reduce inappropriate A&E attendances
• Reduce A&E conversion rates
• Increase the volume of activity undertaken in primary and community based services and local settings (at home/hospices)
Directory of local skills and services (CMS) Provided by each NHS organisation in a PCT area, including
opening hours, referral criteria, and real- time capacity
999 A&E MIU GP
in hrs GP
OOH DN WiC
Midwife Pharmacy Rapid response
nursing Palliative care
services, hospices
The future of Urgent and Emergency Care
NHS 111 national pilots so far
• NHS 111 launched in Aug 2010 in County Durham & Darlington, and December 2010 in Nottingham City, Lincolnshire and Luton in total, over quarter million calls received.
• System impact data released monthly by the Department of Health reviewing the impact of NHS 111 services on A&E, UCC, Primary Care, ambulance services and NHS Direct. – Durham and Darlington data compared with the same period from the previous year
shows that A&E attendances decreased by 1%, in comparison to a 9% increase in A&E attendances for the same time period in the control site. This is equal to a net 10% reduction
– OOH, WiC and UCC contacts have increased by 4% per cent compared to control site where contacts increased by 19% over the same time period. This is equal to a net reduction of 15%.
– 45% drop in NHSD 0845 calls
• Majority of calls receive a primary care disposition this includes pharmacy, community nursing, out of hours as well as in-hours primary care dispositions.
• The Secretary of State set a deadline of April 2013 for NHS 111 service to be available across England.
• DH requested firm 111 roll-out plans from SHAs be submitted in September 2011 plans needed to include the financial case.
• To ensure universal coverage by 2013 DH have said that where plans do not exist, commissioners be expected to engage with NHS Direct as an ‘opt-in’ to work in partnership with ambulance and local GP out of hours providers to provide 111 services on an interim basis until a formal procurement process takes place.
• All London clusters have now submitted plans that ensure NHS 111 service coverage through pilots by January 2013. London CCGs must endorse local plans.
• London is planning formal procurement of NHS 111 post pilots from 2014 – with the early pilots intended a high quality, efficient 111 service integrated with primary and community urgent care systems.
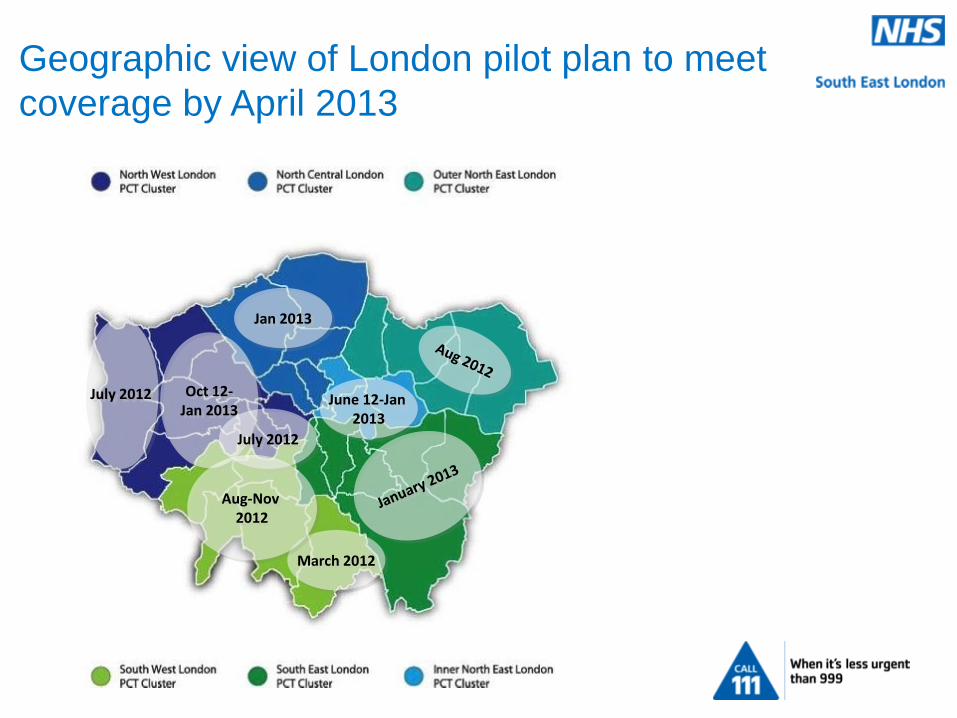
July 2012 Oct 12- Jan 2013
July 2012
Jan 2013
June 12-Jan 2013
March 2012
Aug-Nov 2012
Geographic view of London pilot plan to meet
coverage by April 2013
London
plan by
cluster
North Central London
Geographic Coverage: 17% of London population: Camden/ Haringey/ Islington/ Barnet/ Enfield
Approach to identify a pilot partner :
Plans to use a limited/closed competitive process to deliver a two- year pilot ahead of a pan London Plans to adopt Part B Restricted Accelerated procurement process to deliver a 2 year pilot ahead of a pan London procurement. Cluster initially secured commitment from CCG during October/ November 2011 of a procurement approach that limits supplier base and a111 go-live in January 2013. Newly proposed procurement approach encourages an open procurement process and earlier go-live to mitigate slippage . CCGs will need to confirm revisions to the plan during January 2012. Cluster then finalise local 111 service specification by March ‘12 based on local urgent care strategies Contract award planned for mid April 2012 contract mobilisation period from April to January 2013.
Go live date: January 2013
Outer North East London
Geographic Coverage: 12% of London population: Barking& Dagenham/ Haringey/ Redbridge/ Waltham Forest
Approach to identify a pilot partner :
Previously nominated existing GP OOH provider to deliver a two year 111 pilot ahead of a pan London procurement. However CCG and Cluster agreed to cancel pilot arrangements with existing GPOOH provider following legal advice on single tender award and risk of challenge. Plan to implement Part B Restricted Accelerated procurement process to deliver a 2 year pilot ahead of a pan London procurement. Revised plan to be agreed at ONEL Urgent Care Board, chaired and attended by the CCGs on 29th November. Once endorsed will require final sign off at Joint PCT Boards in January 2012.
Go live date: Issue tender January 12; contract award end Feb; mobilisation and go-live March to August 2012
East London & City
Geographic Coverage: 9% of London population by Tower Hamlets, City & Hackney, Newham
Approach to identify a pilot partner :
Completed limited competitive process to let an initial/ pilot phase contract for two years in line with future pan-London procurement. Cluster Board and CCG approved process, content they have sufficiently justified limiting supplier base. Preferred supplier now identified, to secure final Board and CCG sign off 8 Dec.
Go live date: June 2012 City and Hackney; Tower Hamlets & Newham phased implementation from October 2012 – January 2013 (i.e. post Olympics)
South East London
Geographic Coverage: 21% of London population: Bexley/ Bromley / Greenwich/ Lambeth / Lewisham / Southwark
Approach to identify a pilot partner :
Plans to adopt Part B Restricted Accelerated procurement process to deliver a 2 year pilot ahead of a pan London procurement. CCG confirmation obtained on on accelerated procurement as earlier discussion supported a partnership arrangement between SEL existing GP OOH providers and NHS Direct. If insufficient progress made CCGs agreed to implement a limited procurement process to let a pilot contract for two years. CCG need to agree to revised open procurement approach.
Go live date: Jan uary 2013
South West London
Geographic Coverage: 17% of London population: Croydon/ Richmond/ Wandsworth/ Kingston/ Sutton & Merton
Approach to identify a pilot partner :
Croydon - completed limited competitive process to let pilot contract for two years in line with future pan-London procurement. Cluster Board and CCG’s approved process , content with commissioner justification for limiting supplier base. Preferred supplier now identified, in contract discussions, go live planned for March / April 2012 tbc with DH.
Remaining SWL Boroughs plan to adopt Part B Restricted Accelerated procurement process to deliver two year pilot ahead of a pan London procurement. Secured initial support for go-live timelines and procurement in September, CCG Chairs sighted on change in procurement process but remain committed to go-live planned timelines will need final confirmation with all SWL CCGs following November 2011 change in CCG configuration.
Go live date: Croydon – March 2012; remaining SWL boroughs phased from August 2012 to November 2012.
Inner North West London
Geographic Coverage: 8% of London population: Hammersmith & Fulham/ Westminster/ Kensington & Chelsea
Approach to identify a pilot partner :
Previously nominated existing GP OOH provider to deliver a two year 111 pilot ahead of a pan London procurement. However CCG and Cluster agreed to cancel pilot arrangements with existing GPOOH provider following legal advice identifying potential breach of financial SFI ‘s/ SO’s and PRCC Guidelines Have implemented Part B Restricted Accelerated procurement process to deliver a 2 year pilot ahead of a pan London procurement. Tender published on Supply2Health; contract award planned for 23 January. Mobilisation to commence Feb to July 2012
Go live date: Up to July 2012.
Outer North West London
Geographic Coverage: Geographic coverage: 10% of London population: Hillingdon/ Hounslow/ Ealing
Approach to identify a pilot partner :
Hillingdon previously nominated existing GP OOH provider to deliver a two year 111 pilot ahead of a pan London procurement. CCG and Cluster agreed to cancel pilot arrangements with existing GPOOH provider following legal advice identifying potential breach of financial SFI ‘s/ SO’s and PRCC guidelines Now implemented Part B Restricted Accelerated procurement process to deliver a 2 year pilot ahead of a pan London procurement. Tender published on Supply2Health; contract award planned for 23 January. Mobilisation to commence Feb to July 2012 Hounslow and Ealing plan to adopt Part B Restricted Accelerated procurement process to deliver two year pilot ahead of a pan London procurement. Secured initial support for go-live timelines and procurement in September, CCG Chairs to confirm change in procurement process and go-live planned timelines. Hounslow plan to integrate procurement of 111 provider with re-tendering GP OOH services
Go live date: Hillingdon went live March 2012
Hounslow/ Ealing phased go-live approach between October and January 2013.
Mid North West London
Geographic Coverage: 6% of London population: Brent/ Harrow
Approach to identify a pilot partner :
Brent & Harrow to adopt Part B Restricted Accelerated procurement process to deliver two year pilot ahead of a pan London procurement. Secured initial support for go-live timelines and procurement in September, CCG Chairs to confirm change in procurement process and go-live planned timelines.
Go live date: Phased implementation with Brent and Harrow from October and January 2013 linked with Ealing (above)
Directory of Services: resilience and benefits
Resilience plans
• Additional services to be profiled: Mental Health (both Pathways and other referral), Specialist palliative care service (for Co-ordinate My Care), LES/DES ( consistent with ‘Once for London’ management of LES and DES plans) and Emergency/OOH Dental (potential front-end service reconfiguration to use 111/DoS)
• Additional 111-readiness testing plans using London Top 10 Patient Journey scenarios
• Implementation of 111-DoS testing lessons learned
• Searching and reporting functionality developed for full user roll-out, with cost-effective training solution
• Cluster infrastructure (e.g. governance, workforce planning) proposals to be approved and implemented
• Sustainable provider profiling solution, e.g. London library of service templates
• Expansion of DoS to include social care, jointly commissioned health & social care services, voluntary sector and grant funded services.
Benefits • Cost savings from signposting high-volume ED patient flows to appropriate primary and community-
based services
• Robust 111-readiness testing pack for clusters roll-out to all London pilots
• Added value for stakeholders, especially clinicians (searching tool) and commissioners (reporting)
• Resilient and sustainable Cluster-based infrastructure
Directory of Services: attributes
•A timely and accurate suite of standard and bespoke reports offering users, in particular commissioners, a powerful tool for transforming the patient journey cost-effectively
•A safe and accurate tool that is valued by a wide range of stakeholders, and returns consistent service results whether used in 111 or by clinicians
•A safe and accurate directory of London services to support 111, commissioning integration and other strategic health and social care initiatives
•A well-managed, London-wide user community of commissioners, clinicians, providers and DoS administrators
Users Services
Reporting Searching
DoS Implementation Milestones and Timescales
December 2011
•Additional services profiling
•Additional 111 readiness testing
•Review of implementation and Cluster infrastructure proposals
January 2012
•Additional services profiling
•Implementation of 111-DoS lessons learned
•Emergency/ OOH dental services profiling
•Searching and reporting roll-out, with training
February 2012
•Additional services profiling
•Searching and reporting roll-out, with training
March 2012
•Additional services profiling
•Sign-off of London library of service templates
April 2012 onwards
•DoS implementation/handover to Clusters complete
111 pilot go-live
111 pilot go-live
CmC go-live
CMS DoS
Partner Additional call demand handled by external organisation. Includes health information and web during the pilot phase.
The SEL 111 model
111 999 Cat C OOH NHS Direct Provider(s) Crisis Line
111 telephony cloud
Provider(s)
111 call advisors
NHS Pathways Triage
Ambulance needed?
End of life register
Repeat caller
Pathways disposition
LAS dispatches
Clinicians
3
5
GP OOH Provider(s)
2
1
1. Calls are prioritised to be answered. 2. Additional capacity is provided by
an agreed partner, who also takes health information call.
3. The provider(s) acts as ‘virtual’ call centre for SEL 111 calls.
4. When a speak to/contact primary care provider disposition is OOH, the call is directed to the OOH GP
5. The model supports the links to the End of Life Register
Other service providers
4
No Yes
SEL approach and progress
• The SEL 111 Programme Board will report to the clinical commissioning
groups and the SEL Clinical Strategy Group.
• 111 implementation group overseeing delivery of the project
• Profiling workshops to populate the directory of services (DoS) and
‘break the system’ events to allow clinicians and providers to test the
voracity of the system have been held in south east London.
• A joint mental health profiling/discussion event with south west London
was held in October.
• Engagement with stakeholders is on-going – three clinical engagement
leads: Dr Ben Pert, Dr Kapil Mahna and Programme Board Chair, David
Parkins
Stakeholder engagement activity
clinical
individual GP practice visits by SEL 111 clinical engagement leads, implementation team and cluster primary care contracting staff
Break the system and DoS profiling workshops held September-October – more events and consultation planned for 2012
Updates and attendance at cluster unscheduled care boards
LMC briefings via primary care contracting team
Patient/public
Regular presentations and updates to Stakeholder Reference Group
Stakeholder update bulletins once provider appointed
Presentations to HOSCs, community and patient groups
Two community representatives on procurement panel (Greenwich & Southwark)
Questions? Please contact the project team for further information or for a more detailed briefing on NHS 111 [email protected] Tel: 020 3049 3951 Alex Louis [email protected] Communications & Engagement project lead