3/17/19 1 Super Bugs Need Super Drugs, or Do They? George Dresden, MSN, ACNP, DNP Objectives ØDetermine which antibiotic to use based on pharmacodynamic category: time dependent, concentration dependent, time dependent/concentration enhanced ØImprove your prescribing of antibiotics for bacteria with resistance to beta lactams, including penicillin. ØAssess for all gram negative and positive bacteria, as well as viral etiologies with secondary bacterial infections. Recognize, isolate, and treat the superbugs early. ØIn immunocompromised patients test for fungal etiologies, and be prepared to treat them. Differentiate between opportunistic and non-opportunistic systemic infections. Antibiotic/Antimicrobial Resistance Biggest Threats in 2013 Urgent Threats Ø Carbapenem-resistant Enterobacteriaeae (CRE) Ø Drug-resistant Neisseria Gonorrhoeae Ø Clostridiodes Difficile Serious Threats Ø Multidrug-resistant Acinetobacter Ø Drug-resistant Campylobacter Ø Fluconazole-resistant Candida Ø Extended-spectrum Beta-lactamase producing Enterobacteriaceae Ø Vancomycin-resistant Enterococcus (VRE) Ø Multidrug-resistant Pseudomonas aerginosa Ø Drug-resistant non-typhoidal Salmonella Ø Drug-resistant Shigella Ø Methicillin-resistant Staphyococcus aureus (MRSA) Ø Drug-resistant Streptococcus pneumoniae Ø Drug-resistant Tuberculosis Concerning Threats Ø Vancomycin-resistant Staphylocccus aureus (VRSA) Ø Erythromycin-Resistant Group A Streptococcus Ø Clindamycin-resistant Group B Streptococcus CDC is working toward releasing an updated Threats Report in the Fall of 2019.
Transcript
3/17/19
1
Super Bugs Need Super Drugs, or Do They?George Dresden, MSN, ACNP, DNP
ObjectivesØDetermine which antibiotic to use based on
pharmacodynamic category: time dependent, concentration dependent, time dependent/concentration enhanced
ØImprove your prescribing of antibiotics for bacteria with resistance to beta lactams, including penicillin.
ØAssess for all gram negative and positive bacteria, as well as viral etiologies with secondary bacterial infections. Recognize, isolate, and treat the superbugs early.
ØIn immunocompromised patients test for fungal etiologies, and be prepared to treat them. Differentiate between opportunistic and non-opportunistic systemic infections.
Antibiotic/Antimicrobial Resistance Biggest Threats in 2013Urgent Threats
So, How Did We Get Here?Quick Terminology Review-Take a Nap if this is Old Hat for you› Bacteriostatic-inhibition of bacterial growth› Bactericidal-killing of bacteria› Minimum inhibitory concentration (MIC)-the lowest concentration
of antibiotic that completely inhibits growth of the specific organism being tested
› Minimum bactericidal concentration (MBC)- the lowest concentration of antibiotic at which bacteria are killed
Evidence supports killing when treating endocarditis, meningitis and osteomyelitis, otherwise, inhibition of growth is generally sufficient.
So How Did We Get Here?› Overuse or misuse of antibiotics, i.e. giving antibiotics for a
viral infection (#1 misuse)› Patients not completing courses of antibiotics when they start
feeling better, so they get re-infected› Saving antibiotics and sharing them with others or taking
them later for a different illness
3/17/19
3
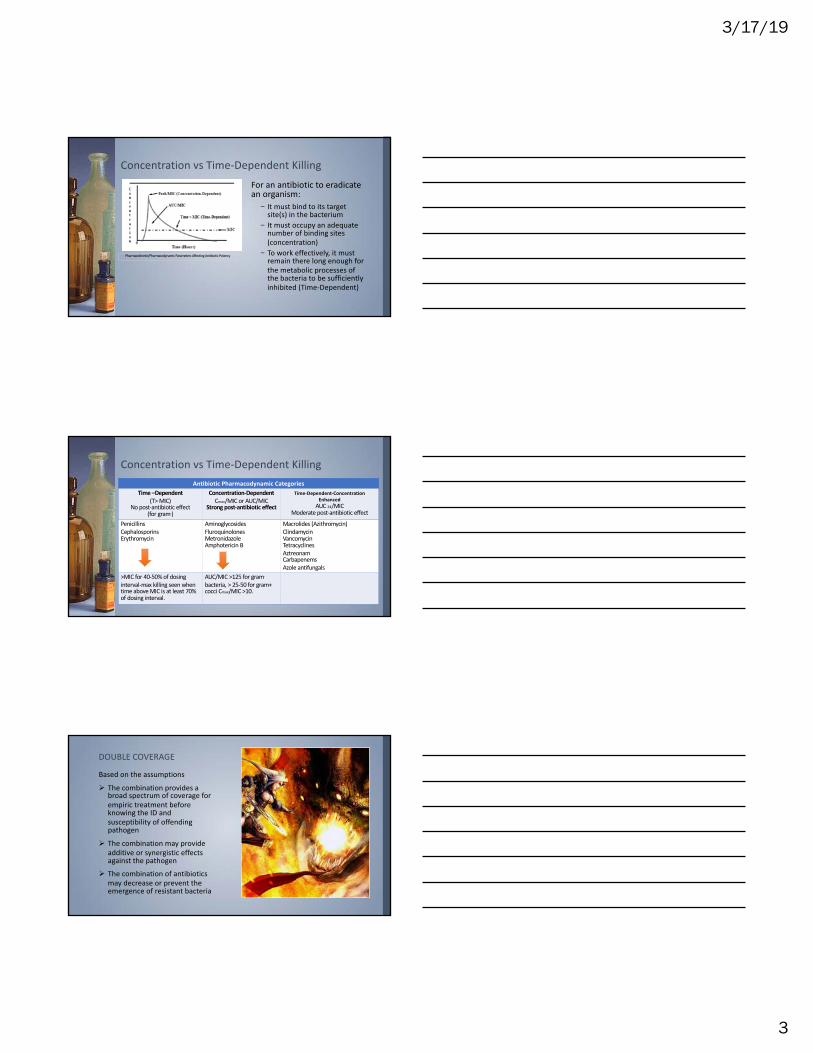
Concentration vs Time-Dependent KillingFor an antibiotic to eradicate an organism:
– It must bind to its target site(s) in the bacterium
– It must occupy an adequate number of binding sites (concentration)
– To work effectively, it must remain there long enough for the metabolic processes of the bacteria to be sufficiently inhibited (Time-Dependent)
>MIC for 40-50% of dosing interval-max killing seen when time above MIC is at least 70% of dosing interval.
AUC/MIC >125 for gram-
bacteria, > 25-50 for gram+ cocci Cmax/MIC >10.
DOUBLE COVERAGE
Based on the assumptions
Ø The combination provides a broad spectrum of coverage for empiric treatment before knowing the ID and susceptibility of offending pathogen
Ø The combination may provide additive or synergistic effects against the pathogen
Ø The combination of antibiotics may decrease or prevent the emergence of resistant bacteria
3/17/19
4
Beta Lactams
Development of Beta Lactam Resistance› Decreased penetration to the target site
– Permeability of the outer membrane no longer allows the antibiotic through such as with Pseudomonas aeruginosa
› Alteration of the target site– Penicillin binding proteins (PBPs) may be changed so that they no
longer have an affinity for the beta-lactam antibiotics so that the bacterial cell is no longer inhibited. Examples are pneumococci, methicillin resistance in staphylococci, and Haemophilus influenzae.
› Inactivation by a bacterial enzyme (ESBL)– Chromosomal beta-lactamases– Plasmid-mediated beta-lactamases
How to Use Beta Lactams EffectivelyNatural Penicillin › Pen V
– Gm+, less effective against gm -, narrow spectrum, PO, prone to ß-lactamase (tonsillitis, anthrax, rheumatic fever, streptococcal skin infections)
Amino-Penicillin› Ampicillin
– Gm+ & gm -, broad spectrum PO and IV, prone to ß-lactamase (ear infections, sinusitis, UTI, menigitis)
› Amoxicillin– Gm+ & gm -, broad spectrum PO and IV,
prone to ß-lactamase (skin infection, sinusitis, UTI, streptococcal pharyngitis)
Anti-Staphylococcal Penicillin › Methcillin
– Gm+, very narrow spectrum, should be given IV, may cause interstitial nephritis
› Oxacillin– Gm+, treatment for PCN-resistant Staphyloocus
aureus, very narrow spectrum, should be given IV
› Nafcillin– Gm+, treatment for staphylococcal infections, very
narrow spectrum, should be given IV
› Cloxacillin– Effective against staphylococci that produce ß-
lactamase, very narrow spectrum, should be given PO
› Dicloxacillin and Flucloxacillin– Gm+, and Staphyococci that produce ß-
lactamase, very narrow spectrum, should be given PO
3/17/19
5
How to Use Beta Lactams EffectivelyAnti-Pseudomonal Penicillin› Pipercillin
– Gm+ & Gm-, extended spectrum, should be given IV or IM if given with tazobactam a ß-lactamase inhibitor, further strengthens its effectiveness
› Carbenicillin– Gm- & limited Gm+, mainly useful for
UTI› Ticarcillin
– Mainly Gm-, particularly Pseudomonas aeruginosa, also stenotrophomonasmaltophilia infections
Cephalosporin› 1st generation predominantly active
against Gm+ bacteria, the 3 successive generations have increased activity against Gm- bacteria, reducing Gm+ activity.
structure, so bind to the ß-lactamase and protect the antibiotic from destruction
› They are most successful when the binding is irreversible
› 3 Most Important: Clavulanic acid, Sulbactam, & Tazobactam
Beta-Lactamase Enzyme
3/17/19
6
Why Is It Important To Detect ESBL’s?› The presence of an ESBL-producing organism in a clinical infection
can result in treatment failure if the wrong antibiotic is used.› ESBL’s can be difficult to detect because they have varying levels of
activity against the cephalosporins. It is crucial to choose wisely which antibiotics to test against. For example, one enzyme may have a minimum inhibitory concentration (MIC) of 4 μg/ml on ceftazidime but have poor activity on cefotaxime with a MIC of 256 μg/ml.
› If an ESBL is detected, ALL PENICILLIN’S, CEPHALOSPORINS, AND AZTREONAM SHOULD BE REPORTED AS RESISTANT, even if in vitro test results indicate they have susceptibility.
Metallo Beta-Lacamase› Resistant against a broad spectrum of beta-lactam antibiotics.› This includes those in the carbapenem family.› This particular class is characterized by its ability to hydrolyze
carbapenems and by their resistance to available ß-lactamase inhibitors (tazobactam, sulbactam, clavulanic acid) but susceptibility by metal ion chelators (vitamin B12, ascorbic acid).
› The most common bacteria that are responsible for this enzyme are Gm- such as Escherichia coli, Klebsiella pneumoniae and Pseudomonas aeruginosa.
Penicillin-under or over utilized?› Penicillin allergy is the most common, reported by up to 15%
of hospitalized patients› Clinically-can they be safely given structurally related
cephalosporins or carbapenems› Do they need allergy consultation first?
3/17/19
7
Approach to the Patient with a Past PCN Reaction Who Requires Antibiotics
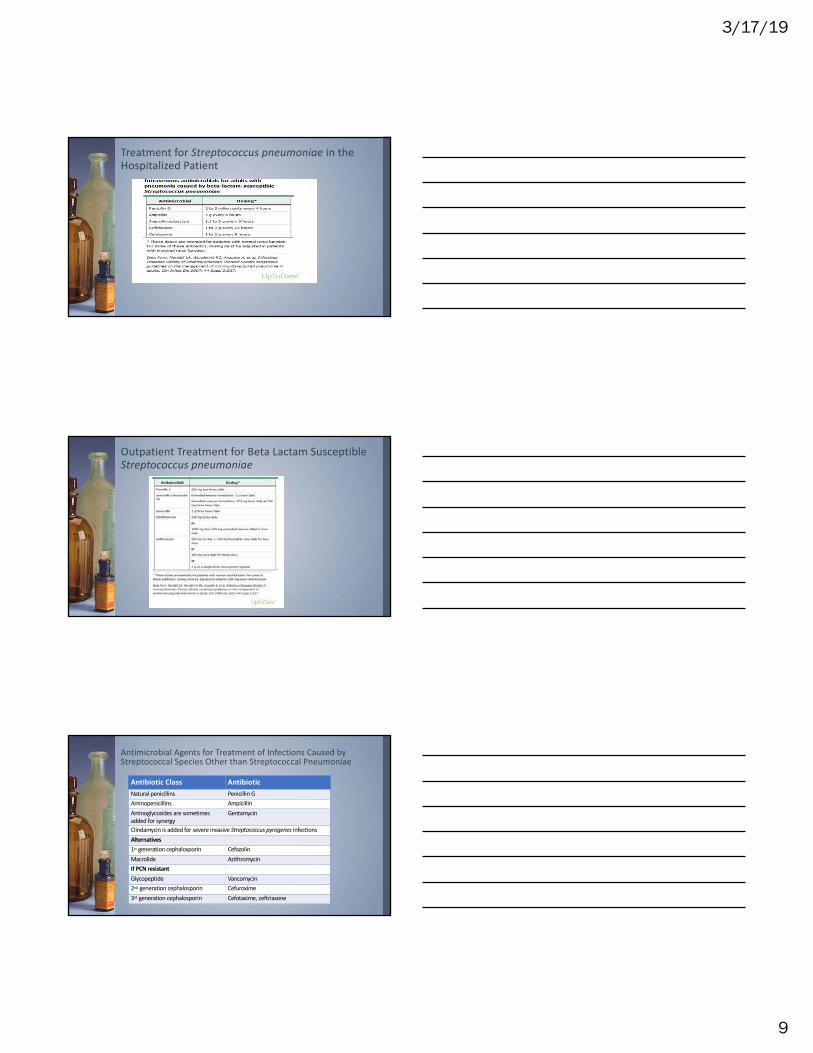
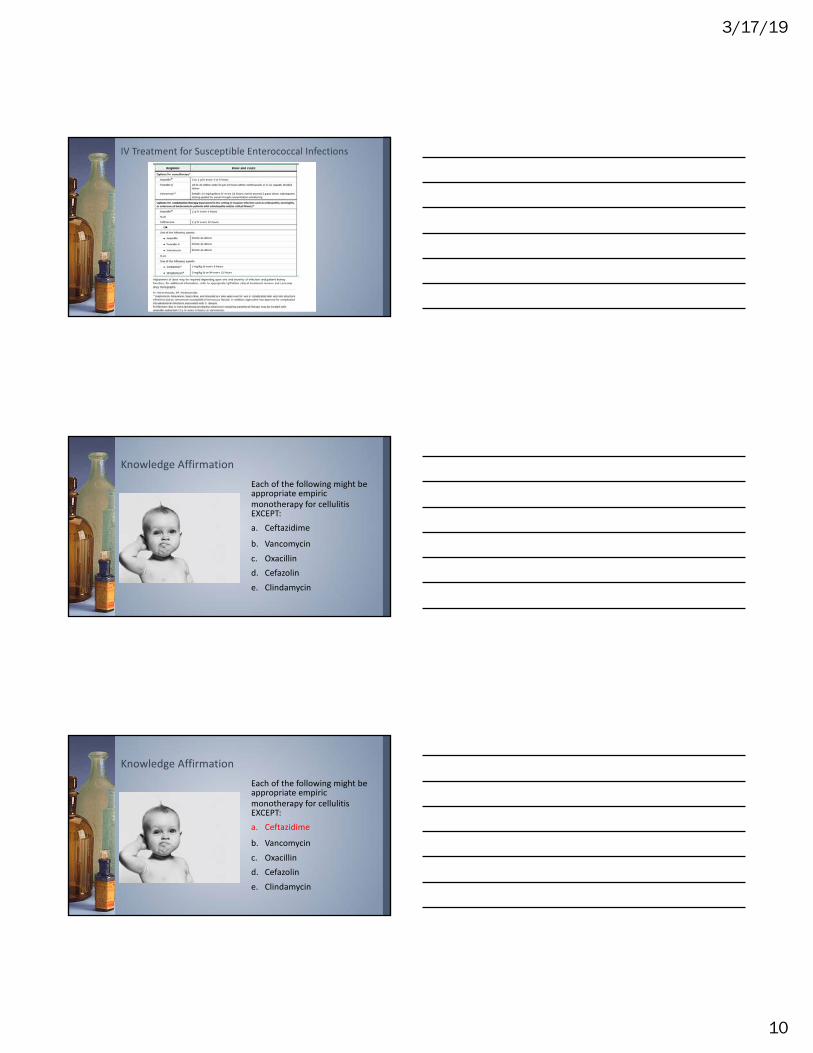
The PenicillinsCategory Parenteral Agents Oral AgentsNatural Penicillins Penicillin G Penicillin VAntistaphylococcal penicillins Nafcillin, oxacillin DicloxacillinAminopenicillins Ampicillin Amoxacillin, ampicillinAminopenicillins+ß-lactamaseinhibitors
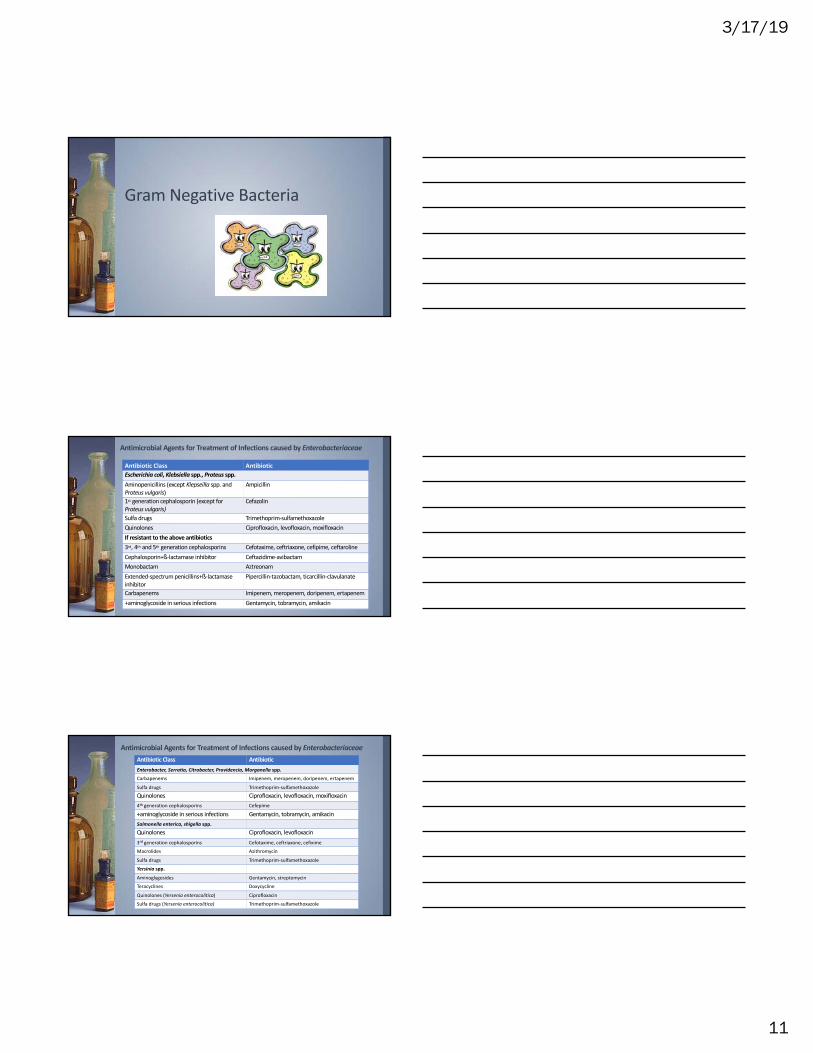
Antimicrobial Agents for Treatment of Infections caused by EnterobacteriaceaeAntibiotic Class AntibioticEnterobacter, Serratia, Citrobacter, Providencia, Morganella spp.Carbapenems Imipenem, meropenem, doripenem, ertapenem
Antibiotic Class AntibioticTreatment of ChoiceMacrolides Erythromycin, azithromycin, clarithromycinQuinolones Ciprofloxacin, leofloxacinAlternativesTetracyclines Tetracycline, doxycyclineAminoglycosides Gentamycin, tobramycin, amikacinAminopenicillin+ß-lactamase inhibitor Amoxicillin+clavulanic acidChloramphenicol
Treatment only indicated for a subset of patients –those with high fevers, bloody or profuse diarrhea, prolonged symptoms, or immunocompromised.
Antimicrobial Agents for Treatment of Infections Caused by Helicobacter pyloriAntibiotic Class AntibioticAminopenicillins AmoxicillinMacrolides ClarithromycinMetronidazoleTetracyclines TetracyclineBismuth subsalicylate (Pepto Bismol)Recommended Regimens *Duration of treatment is generally 2 weeksAmoxicillin+clarithromycin+PPIMetronidazole+clarithromycin+PPIBismuth subsalicylate+metronidazole+tetracycline+PPI
3/17/19
14
Antimicrobial Agents To Treat Infection from HaemophilusinfluenzaeAntibiotic Class AntibioticTreatment of ChoiceAminopenicillins+ß-lactamase inhibitor Amoxicillin+clavulanate, ampicillin+sulbactam2nd generation cephalosporins Cefuroxime3rd generation cephalosporins Ceftriaxone, cefotaximeAlso activeTetracyclines Tetracycline, doxycyclineMacrolide-like agents Azithromycin, telithromycinQuinolones Ciprofloxacin, levofloxacin, moxifloxacin,
Antimicrobial Agents For Infection Due to Moraxella catarhalisAntibiotic Class AntibioticExtended-spectrum penicillins PiperacillinAminopenicillins+ß-lactamase inhibitor Amoxicillin+clavulanate, ampicillin+sulbactam2nd generation cephalosporins Cefuroxime3rd generation cephalosporins Ceftriaxone, cefotaximeMacrolides Azithromycin, clarithromycinAminoglycosides Gentamycin, tobramycin, amikacinSulfa drugs Trimethoprim-sulfamethoxazoleQuinolones Ciprofloxacin, levofloxacin, moxifloxacinTetracyclines Tetracycline, doxycycline
Acinetobacter species Infection Treatment
3/17/19
15
Knowledge AffirmationWhich of the following antibiotic regimens would be appropriate for a patient with a severe infection caused by Pseudomonas aerugnosa prior to knowledge of the isolate’s susceptibilities?a. Ceftazidime+tobramycinb. Ceftriaxone+gentamycinc. Pipercillin+rifampind. Ertapenem+amikacine. Ampicillin+tobramycin
Knowledge AffirmationWhich of the following antibiotic regimens would be appropriate for a patient with a severe infection caused by Pseudomonas aerugnosa prior to knowledge of the isolate’s susceptibilities?a. Ceftazidime+tobramycinb. Ceftriaxone+gentamycinc. Pipercillin+rifampind. Ertapenem+amikacine. Ampicillin+tobramycin
Anaerobic Bacteria
3/17/19
16
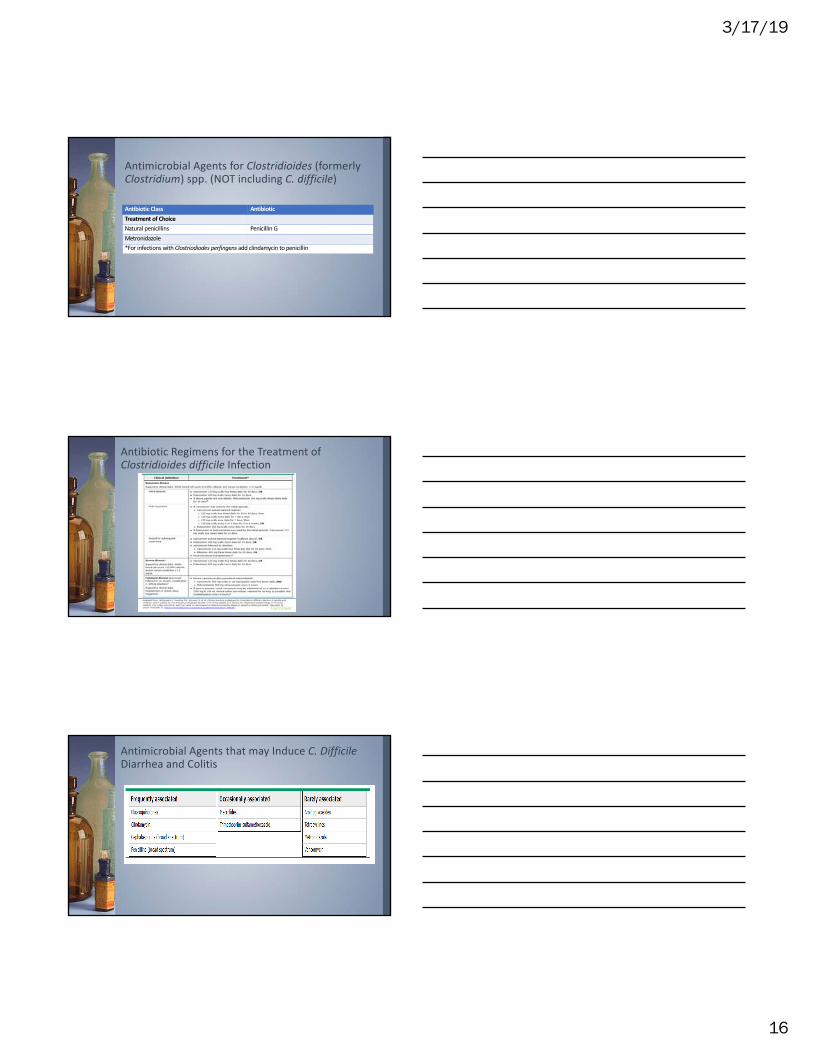
Antimicrobial Agents for Clostridioides (formerly Clostridium) spp. (NOT including C. difficile)
Antibiotic Class AntibioticTreatment of ChoiceNatural penicillins Penicillin GMetronidazole*For infections with Clostriodiodes perfingens add clindamycin to penicillin
Antibiotic Regimens for the Treatment of Clostridioides difficile Infection
Antimicrobial Agents that may Induce C. Difficile Diarrhea and Colitis
3/17/19
17
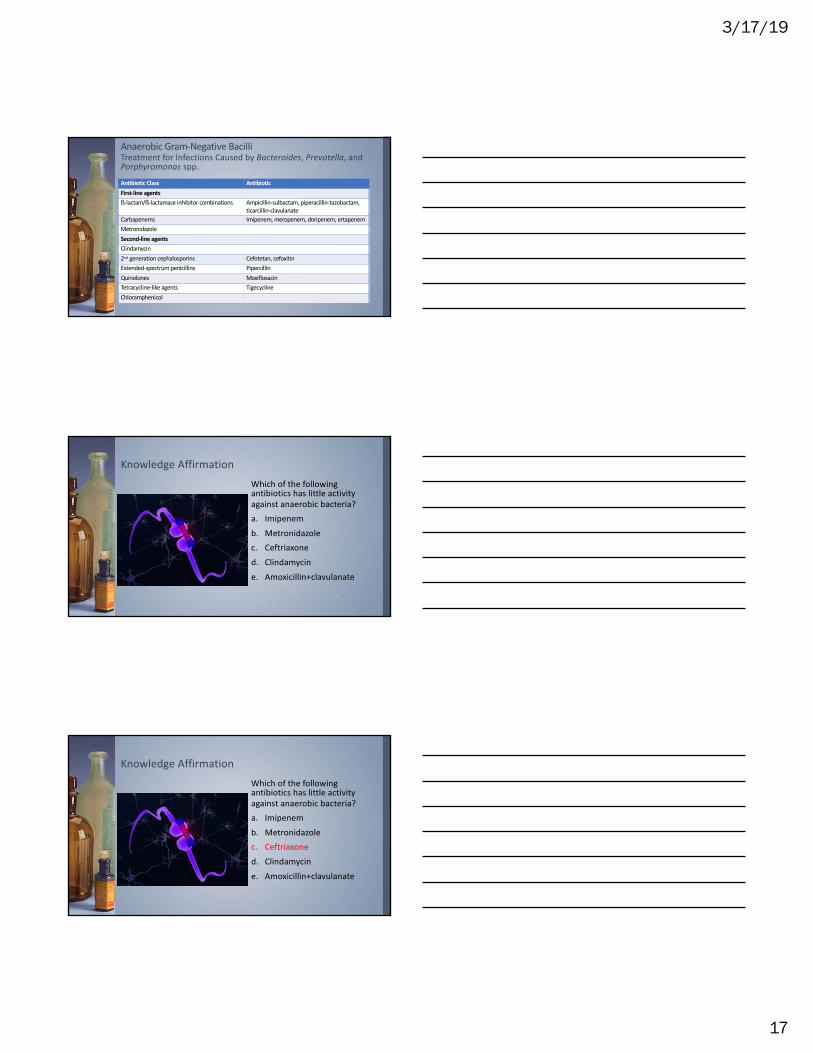
Anaerobic Gram-Negative BacilliTreatment for Infections Caused by Bacteroides, Prevotella, and Porphyromonas spp.
Antibiotic Class AntibioticFirst-line agentsß-lactam/ß-lactamase inhibitor combinations Ampicillin-sulbactam, piperacillin-tazobactam,
Knowledge AffirmationWhich of the following antibiotics has little activity against anaerobic bacteria?a. Imipenemb. Metronidazolec. Ceftriaxoned. Clindamycine. Amoxicillin+clavulanate
Knowledge AffirmationWhich of the following antibiotics has little activity against anaerobic bacteria?a. Imipenemb. Metronidazolec. Ceftriaxoned. Clindamycine. Amoxicillin+clavulanate
3/17/19
18
Atypical Bacteria
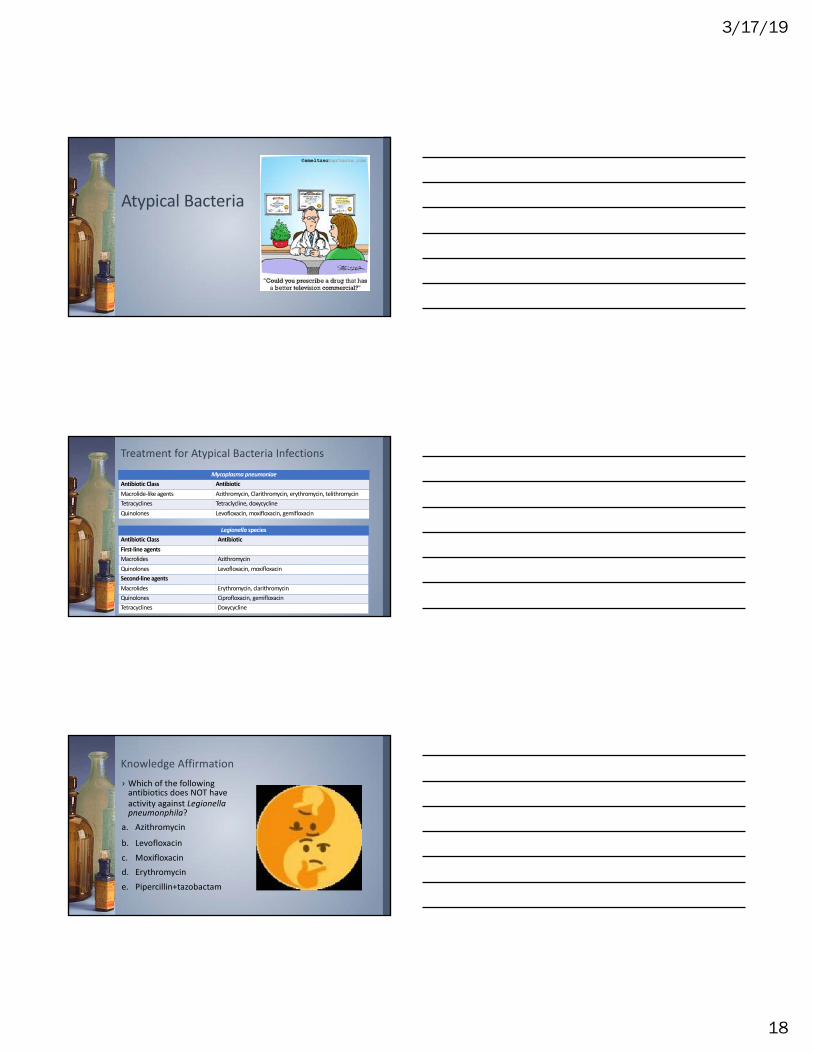
Treatment for Atypical Bacteria InfectionsMycoplasma pneumoniae
antibiotics does NOT have activity against Legionella pneumonphila?
a. Azithromycin
b. Levofloxacinc. Moxifloxacind. Erythromycine. Pipercillin+tazobactam
3/17/19
19
Knowledge Affirmation› Which of the following
antibiotics does NOT have activity against Legionella pneumonphila?
a. Azithromycin
b. Levofloxacinc. Moxifloxacind. Erythromycine. Pipercillin+tazobactam
Myobacteria
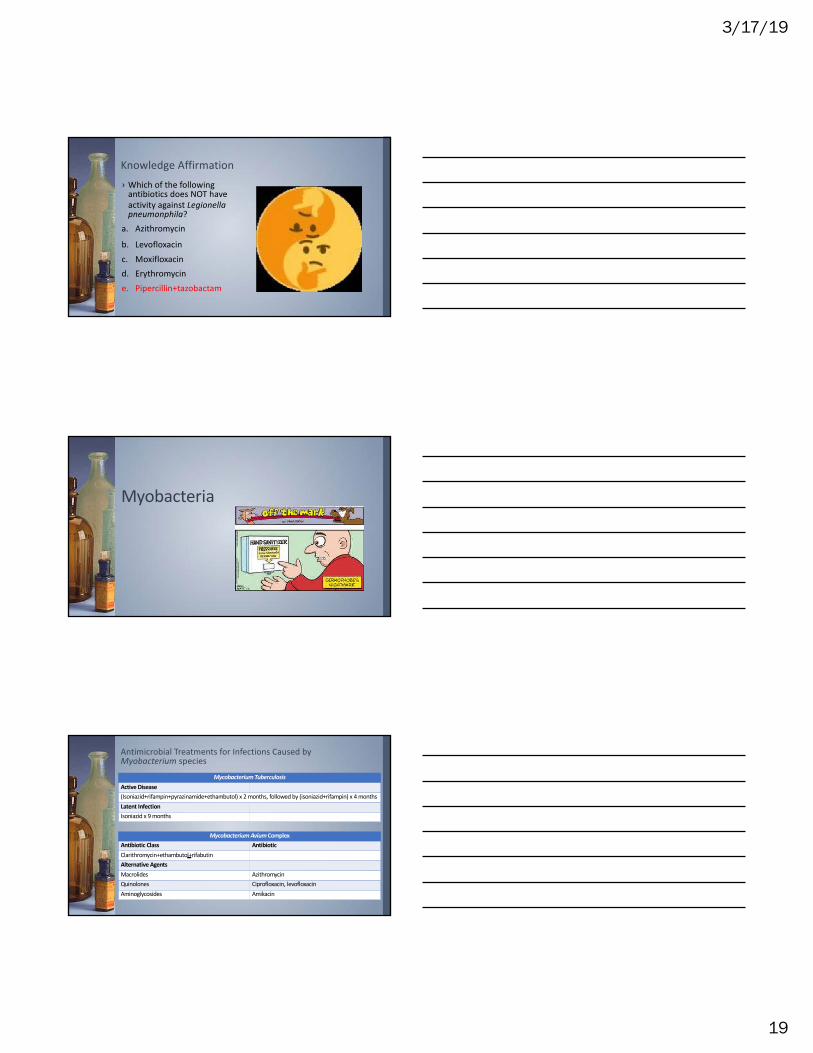
Antimicrobial Treatments for Infections Caused by Myobacterium species
Mycobacterium TuberculosisActive Disease(Isoniazid+rifampin+pyrazinamide+ethambutol) x 2 months, followed by (isoniazid+rifampin) x 4 monthsLatent InfectionIsoniazid x 9 months
Mycobacterium Avium ComplexAntibiotic Class AntibioticClarithromycin+ethambutol+rifabutinAlternative AgentsMacrolides AzithromycinQuinolones Ciprofloxacin, levofloxacinAminoglycosides Amikacin
3/17/19
20
Antimicrobial Treatment for Myobacterium leprae
Antibiotic Class AntibioticDapsone+rifampin+clofaximineAlternative AgentsTetracyclines MinocyclineQuinolones OfloxacinMacrolides Clarithromycin
Knowledge AffirmationAll of the following are used to treat patients with tuberculosis EXCEPT:a. Pyrazinamideb. Isoniazidc. Rifampind. Dapsonee. Ethambutol
Knowledge AffirmationAll of the following are used to treat patients with tuberculosis EXCEPT:a. Pyrazinamideb. Isoniazidc. Rifampind. Dapsonee. Ethambutol
3/17/19
21
Fungal Infections
Antifungal Agents for Candida speciesAntifungal Class AntifungalEchinocandins Caspofungin, anidulafungin, micafunginAzoles Fluconazole, voriconazole, posaconazole, itraconazole, isavuconazolePolyene Amphotericin B
• If your patient is not improving on standard antibacterial therapy, despite new negative cultures, look for an underlying fungal infection.
• At risk patients include: those with IV lines of catheters, bone marrow transplant recipients, ICU patients , patients with implanted joint prostheses, or who are immunosuppressed.
• Mortality of invasive candidiasis is 30%.
Opportunistic Infections-PJP
3/17/19
22
Antifungal Agents for Nonmeningeal Cryptococcal Infection
Treatment for AspergillosisAntifungal Class AntifungalInitial Therapy Voriconazole+ echinocandin (NOT fluconazole)If intolerant of voriconazole Amphotericin B or isavuconazoleSalvage Therapy
+ Voriconazole, isavuconazole, OR liposomal amphotericin B
Duration of therapy at a minimum is 6-12 weeks. For most immunosuppressed patients it will continue for months to years.If the etiology was endocarditis, the patient should stay on a lifelong azole at a treatment dose.
Questions???? Headaches?
3/17/19
23
References• Antimicrobial fundamental concepts. Obtained from https://www.asp.mednet.ucla.edu/files/view/guidebook/AntimicrobialFundamentalConcepts.pdf
• Blumenthal, K. G., & Solensky, R. (2017). Choice of antibiotics in penicillin-allergic hospitalized patients. www.uptodate.com
• Cox, G.M. & Perfect, J. R. (2017). Cryptococcus neoformans infection outside the central nervous system. www.uptodate.com
• Hauser, A. R. (2019). Anaerobic bacteria. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA.
• Hauser, A. R. (2019). Antibiotics that target the cell envelope. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA.
• Hauser, A. R. (2019). Atypical bacteria. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA
• Hauser, A. R. (2019). Gram negative bacteria. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA.
• Hauser, A. R. (2019). Gram positive bacteria. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA.
• Hauser, A. R. (2019). Mycobacteria. In Antibiotic Basics for Clinicians, Wolters Kluwer: Philadelphia, PA.
• Kanafani, Z. A. & Kanj, S. S. (2018). Acinetobacter infection: Treatment and prevention. www.uptodate.com.
• Kauffman, C. A. (2018). Management of candidemia and invasive candidiasis in adults. www.uptodate.com
• Kauffman, C. A. (2018). Treatment and prevention of invasive aspergillosis. www.uptodate.com
• Kelly, C. P. , Lamont, J. T. & Bakkan, J. S. (2019). Clostridioides (formerly Clostridium) difficile infection in adults: Treatment and prevention. www.uptodate.com
• Letourneau, A. R. (2017). Beta-lactam antibiotics: Mechanisms of action and resistance and adverse effects. www.uptodate.com
• Marrie, T. J., & Tuomanen, E. I. (2018). Pneumococcal pneumonia in adults. www.uptodate.com
• Melin, J. A., Kunins, L., Givens, J., & Sokol, H. N. (2019). What’s new in hospital medicine. www.uptodate.com
• Quindós-Andrés, G. (2016). Environmental Mycology in Public Health. https://doi.org/10.1016/B978-0-12-411471-5.00006-5
• Quintiliani, R. (2010). Pharmacodynamics of antimicrobial agents: Time-dependent vs. concentration dependent killing. www.antimicrobe.org.
• Sarma, S. C. (2015). Beta Lactam Antibiotics. Presentation. https://www.slideshare.net/saurav9119/beta-lactam-antibiotics-43630735