Page 1
Non-castrate Metastatic Prostate Cancer: Have theTreatment Options Changed?
Phillip L. Palmbos and Maha Hussain
Over the past 7 decades androgen-deprivation therapy (ADT) has been the cornerstone of
treatment for metasta
achieve this goal have
but also gonadotropinandrogen receptor (A
castrate-resistant prost
CRPC have emerged. Tthis review, we outline
for NCPC, and discuss
Semin Oncol 40:337-3
0270-9295/& 2013 Elshttp://dx.do
Conflicts opFizer, Lillconsultant
DepartmenUniversi
Address cInternalof MichiMI 4810
Seminars
tic non-castrate prostate cancer (NCPC); however, the mechanisms to
evolved over time to include not only bilateral orchiectomy and estrogens,
-releasing hormone (GnRH) agonists, antagonists, and the inclusion ofR) blockade. Despite treatment with ADT, most men will progress to
ate cancer (CRPC). Over the last decade many new treatment options for
hese new treatments also could have a meaningful role earlier in NCPC. Inthe biologic drivers of NCPC, review current standard therapy available
the evolving role of new therapeutics in metastatic disease.
46 & 2013 Elsevier Inc. All rights reserved.
Despite many decades of research, metastatic
prostate cancer remains a lethal disease,claiming 28,170 lives per year in the United
States and representing the second most common
malignancy-related death in men.1 Prostate cancer isan androgen-dependent tumor and the vast majority
of new metastatic prostate cancers (non-castrate
prostate cancer [NCPC]), are initially responsive toandrogen-deprivation therapy (ADT). However, ADT
is not curative and most patients will ultimately
progress to castration-resistant prostate cancer(CRPC).2 The last decade has seen the approval of
multiple new treatments for CRPC, but these new
therapeutic modalities are not curative and their rolein NCPC remains to be defined.3 To advance pros-
tate cancer care, we must now move these novel
therapies to earlier stages of disease, determine theoptimal timing and use of existing therapies, and
develop biomarkers that identify patients likely to
benefit from new targeted therapies. In this reviewwe will outline the biologic drivers of NCPC, review
current standard therapy available for NCPC, and
- see front matterevier Inc. All rights reserved.i.org/10.1053/j.seminoncol.2013.04.007
f interest: Dr Hussain receives research support from Abbot,y, EMD Sorrano, Astellas, Takeda and Millenium. She is afor: Genmab, Exelexis.
t of Internal Medicine, Division of Hematology/Oncology,ty of Michigan, Ann Arbor, MI.
orrespondence to Maha Hussain, MD, Department ofMedicine, Division of Hematology/Oncology, Universitygan, 1500 E Medical Center Dr, 7314 CCGC, Ann Arbor,9-5946. E-mail: [email protected]
in Oncology, Vol 40, No 3, June 2013, pp 337-346
discuss the evolving role of new therapeutics in
metastatic disease.
ANDROGENS AND THE PROSTATE
The prostate gland requires androgens for forma-
tion and patients who lack the enzymes responsiblefor androgen biosynthesis do not develop a prostate.4
Prostate adenocarcinoma also requires androgen-
induced activation of androgen receptors (ARs) forgrowth and survival; disruption of this pathway stops
prostate cancer proliferation and induces apoptosis.2
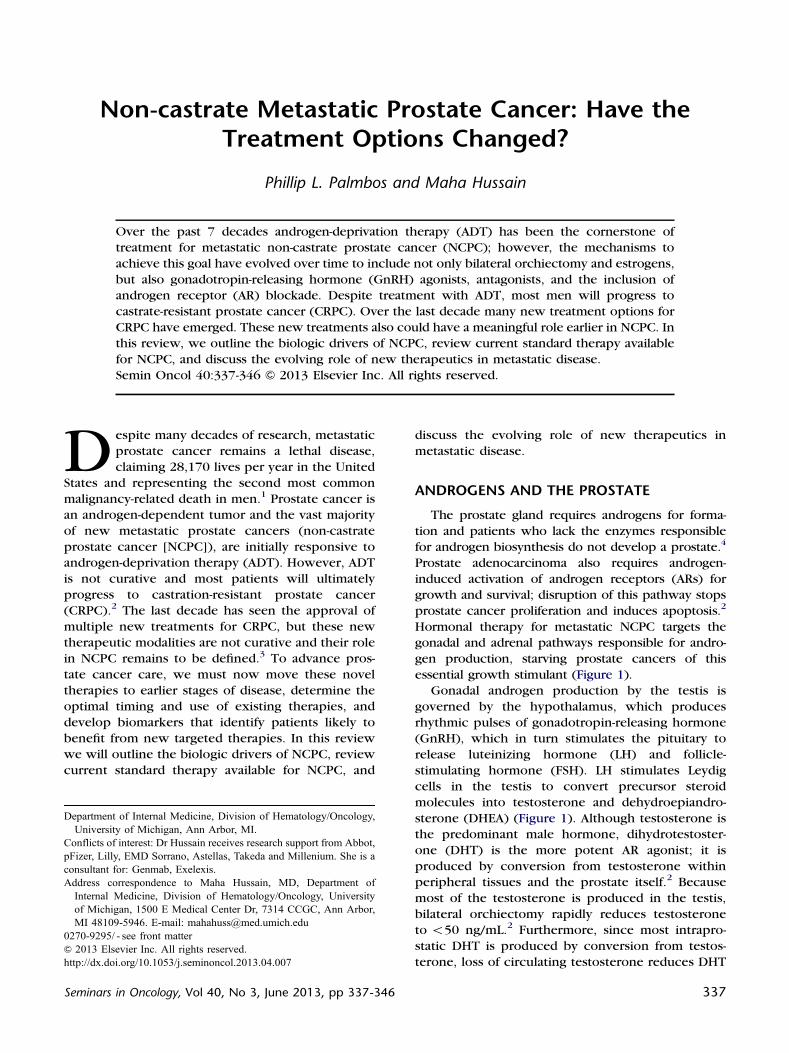
Hormonal therapy for metastatic NCPC targets thegonadal and adrenal pathways responsible for andro-
gen production, starving prostate cancers of this
essential growth stimulant (Figure 1).Gonadal androgen production by the testis is
governed by the hypothalamus, which produces
rhythmic pulses of gonadotropin-releasing hormone(GnRH), which in turn stimulates the pituitary to
release luteinizing hormone (LH) and follicle-
stimulating hormone (FSH). LH stimulates Leydigcells in the testis to convert precursor steroid
molecules into testosterone and dehydroepiandro-
sterone (DHEA) (Figure 1). Although testosterone isthe predominant male hormone, dihydrotestoster-
one (DHT) is the more potent AR agonist; it is
produced by conversion from testosterone withinperipheral tissues and the prostate itself.2 Because
most of the testosterone is produced in the testis,
bilateral orchiectomy rapidly reduces testosteroneto o50 ng/mL.2 Furthermore, since most intrapro-
static DHT is produced by conversion from testos-
terone, loss of circulating testosterone reduces DHT
337
Page 2
Hypothalamus
Pituitary
Tes�sAdrenal
Prostate Cancer
TestosteroneDHEAS
DHT
LHACTH
GnRHCRH Leuprolide, Goserelin, DES,
DegarelixGlucocor�coids
Ketoconazole, Abiraterone CYP17A1CYP17A1
Biclutamide, Nilutamide, Flutamide,
EnzalutamideARN-509
Androgen Receptor
Figure 1. Androgen regulation and prostate cancer.
P.L. Palmbos and M. Hussain338
levels by 70%–80%, thereby reducing the prolifer-
ative stimulus within the tumor tissue.4
Adrenal androgen production is also regulatedby the hypothalamic-pituitary axis. Secretion of cor-
ticotropin-releasing hormone (CRH) by the hypothal-
amus stimulates the pituitary to release adrenocorti-cotropic hormone (ACTH), which in turn stimulates
the adrenal cortex to produce the androgen, DHEA
(Figure 1). Similar to testosterone, DHEA can beconverted to DHT in peripheral tissues and the
prostate.4 Adrenal production of androgens likely
accounts for the observation that prostate tumorsretain DHT levels 20%–30% of normal even after
medical or surgical castration.4 This alternative path-
way of androgen production can be targeted bytreatment with exogenous corticosteroids, which
block production of ACTH and subsequent adrenal
production of androgens or by drugs that inhibit theadrenal enzymes responsible for androgen production
(Figure 1). Indeed, corticosteroids do have intrinsic
activity in CRPC and are frequently used after diseaseprogression following medical or surgical castration
or in conjunction with cytotoxic chemotherapy,
although they have not been tested in randomizedtrials.5 Most current treatments for metastatic NCPC
target various aspects of these two pathways.
TREATMENT OF METASTATIC NCPC:HISTORICAL PERSPECTIVE
Orchiectomy and Estrogens
The first treatment for men with advanced prostateadenocarcinoma was described more than 70 years
ago by Huggins and Hodges who found that men
treated with bilateral orchiectomy or with the estrogen,
diethylstilbestrol (DES) displayed clinical improve-ments.6 Both orchiectomy and DES resulted in suppres-
sion of gonadal androgen production; orchiectomy,
by removal of the androgen-secreting tissue, and DES,by provoking negative feedback on the GnRH/LH
regulatory pathway (Figure 1). This Nobel Prize win-
ning observation established hormonal therapy as theprimary treatment for metastatic NCPC and is founda-
tional to all current therapy for prostate cancer. In the
1960s, a large clinical trial conducted by the Veteran'sAdministration Cooperative Urological Research Group
(VACURG) randomized patients with advanced or
metastatic prostate cancer to either orchiectomy, DES,or both to determine which was most effective.7
Interestingly, DES did not confer a survival advantage
when compared to orchiectomy, primarily due toincreased risk of cardiovascular events. These toxicities
were in part due to the high dose of estrogens, which is
now a recognized risk factor for cardiovascular diseaseand thrombosis.8
GnRH Agonist/Antagonists
In the early 1980s synthetic peptide analogues of
GnRH were developed that targeted the pituitaryregulation of androgen production and allowed
medical castration. The most commonly used agents,
leuprolide or goserelin, are synthetic GnRH agoniststhat replace the normal pulsatile secretion of GnRH
with a continual agonism resulting in an initial pulse
of LH and androgen production, followed by sup-pression of both LH and testosterone to below 50
Page 3
Non-castrate metastatic prostate cancer 339
ng/dL, a level of suppression similar to orchiectomy
(Figure 1).2 Randomized trials comparing GnRHagonists to DES in patients with metastatic prostate
cancer demonstrated that they were equally effica-
cious in reducing serum testosterone levels, hadsimilar overall survival and TTP and avoided many
of the limiting cardiovascular and thrombotic toxic-
ities associated with DES.9 Patient preference hasmade medical castration with GnRH agonists the
standard of care for newly diagnosed metastatic
prostate cancer.More recently, GnRH antagonists have been devel-
oped. Degarelix, is a GnRH antagonist that directly
blocks GnRH stimulation of the pituitary.10 A random-ized phase III trial of degarelix versus leuprolide
demonstrated that degarelix treatment produces
more rapid reduction in testosterone levels (castratelevels by day 3 of treatment), whereas patients treated
with leuprolide had a 65% increase in testosterone on
day 3 and required 28 days to achieve castratelevels.11 Another putative advantage of degarelix is
the absence of LH micro-surges associated with GnRH
agonist administration even after castrate levels oftestosterone are achieved. Whether these micro-
surges have an impact on patient outcomes remains
unclear. Further evaluation of the patients treatedwith degarelix has suggested that degarelix may
reduce the risk of prostate-specific antigen (PSA)
relapse in patients with more extensive disease butdid not alter survival.12
AR
+
AR
Prolifera�on
Transcrip�on
Survival
Apoptosis
BCL2 Clusterin
DNA Repair
Androgens IGF-1R c-MET
PI3K
AKT
mTOR
PTENRAS
RAF
MAPK
SRC
DNA
Nucleus
Cytoplasm
Amplifica�on, Muta�on
Figure 2. Signaling pathways governing growth andsurvival in prostate cancer.
Androgen Receptor Blockade
The emergence of castration resistance in men
treated with gonadal suppression is now understoodto depend in part on stimulation by androgens
produced by the adrenal glands. It was therefore
hypothesized that inhibition of the AR itself mightimprove outcomes in patients with metastatic NCPC
by blocking AR signaling mediated by adrenal andro-
gens. Since the late 1980s multiple trials of com-bined androgen blockade using primary gonadal
suppression, with and without concomitant AR
blockers, cyproterone acetate, flutamide, nilutamide,and biclutamide, were conducted to test this hypoth-
esis.13 Although some of these trials demonstrated a
survival or progression-free survival benefit, oppo-nents of this approach note that not all trials showed
significant benefits and that their cost and potential
for side effects limit their overall clinical utility. Ameta-analysis of 21 randomized clinical trials assess-
ing GnRH agonists alone or in combination with AR
blockade concluded that while there was no benefitto combined androgen blockade at 2 years when
compared to monotherapy, there was a modest and
statistically significant survival advantage to com-bined androgen blockade at 5 years.14 Therefore,
because of this survival advantage and minimal
added toxicity, combined androgen blockade hasbecome one of the standard treatment considera-
tions for metastatic disease.
BIOLOGY AND PREVENTION OF CASTRATE-RESISTANT PROSTATE CANCER
Progression from NCPC to CRPC requires evolu-tion from an androgen-dependent state to an
androgen-independent state. The mechanisms that
drive this progression include reactivation of ARsignaling or upregulation of other cellular pathways
controlling growth (Figure 2).15 Reactivation of AR
signaling in prostate cancer cells may be multifacto-rial but can involve genetic amplification or muta-
tional activation of the AR receptor, increased
intratumoral androgen production and upregulationof AR coactivators, all of which increases transcrip-
tional activation and proliferation (Figure 2).16
It has been suggested that androgen-independentcancer cells are present early in disease and
androgen-independent growth is driven by clonal
selection of these cells.17 If these androgen-independent clones could be targeted while the bulk
of the tumor is sensitive to androgen loss, then
eventual progression could be delayed or prevented.Two approaches to date to delay or prevent the
development of CRPC have been the subject of large
clinical trials. The first approach is based on thehypothesis that CRPC arises due to selective
pressure-induced ADT and that by limiting exposure
to selective pressure CRPC can be delayed oravoided. The second approach attempts to eliminate
resistant clones present early in disease using cyto-
toxic chemotherapy in combination with ADT.
Reducing Selective Pressure
Continuous androgen deprivation (CAD) maydrive Darwinian selection of androgen-insensitive
Page 4
P.L. Palmbos and M. Hussain340
clones, leading ultimately to CRPC. Therefore, inter-
mittent androgen deprivation (IAD), which removescontinuous selective pressure could delay develop-
ment of CRPC in addition to reducing the side effects
related to ADT. This theory was supported bypreclinical mouse models in which androgen sup-
pression drove formation of androgen-independent
tumors.18 In addition, ADT has been associated withseveral toxicities, including osteoporosis, weight
gain, diabetes, cholesterol, and coronary artery dis-
ease, which potentially could be reduced by IAD.19
Prior to this year, four randomized trials had
addressed this question, with three supporting equiv-
alent survival and less adverse events in most patientsreceiving IAD when compared to continuous therapy
and one showing worse survival in a subset of
patients with higher risk disease (high pretreatmentPSA, more extensive/bulky disease).20–23 Although
intriguing, each of these trials was small with
heterogeneous populations and not adequately pow-ered to determine comparability/non-inferiority. The
definitive prospective randomized controlled study
regarding this question, Southwest Oncology Group(SWOG) 9346 (INT-0162) was recently reported.24
In this study, 1,535 patients with metastatic NCPC
who achieved PSA o4 following ADT were ran-domly assigned to either intermittent or continuous
ADT and survival, adverse events, and quality of life
were assessed. Interestingly, although this trial con-firmed some quality of life improvements in patients
in the IAD arm, it did not meet its primary endpoint,
which was IAD non-inferiority as compared to CAD.These findings suggest that contrary to preclinical
modeling and theory, patients receiving IAD may
have worse overall survival. In this context, it wouldseem that IAD is not a routine therapy and patients
wishing to undergo IAD must be carefully counseled.
Targeting “De Novo” Androgen-Dependentand -Independent Disease
A second strategy to delay or prevent CRPC is to
eliminate androgen-insensitive clones using cyto-
toxic therapy given concurrently with ADT inpatients with newly metastatic NCPC. Historically,
the addition of alkylating agents and anthracyclines
to ADT demonstrated improved response rates andpalliation but no survival advantage.25,26 In 2004,
two phase III studies demonstrated a survival benefit
in CRPC patients treated with docetaxel.27,28 Sincedocetaxel conferred a survival advantage in CRPC, it
was postulated that docetaxel might confer a sur-
vival advantage when combined with ADT in meta-static NCPC. This question is currently being
addressed in Eastern Cooperative Oncology Group
(ECOG) E3805 (CHAARTED), which randomizespatients with newly diagnosed metastatic prostate
cancer to either docetaxel plus prednisone with
ADT or ADT alone. Whether docetaxel offers asurvival advantage to patients who are starting ADT
or instead the toxicity of therapy outweighs
improved response will be determined.29
NEXT-GENERATION HORMONAL AGENTS
The realization that CRPC relies on reactivation of
AR signaling via AR amplification, mutation, and
extragonadal production of androgens made morepotent suppression of AR signaling a prime thera-
peutic target in patients with CRPC.30 Two success-
ful strategies have been developed to target thisresidual androgenic signaling in metastatic CRPC:
inhibition of the extragonadal synthetic pathways,
and more potent blockade of the AR.CYP17A, a 17α-hydroxylase/17,20-lyase, is present
in both testicular tissue and adrenal cortex and is
responsible for the conversion of pregnenolone intoDHEA and testosterone (Figure 1).4 Historically,
ketoconazole was used to block this enzymatic
pathway and represents a second-line hormonaltherapy for metastatic prostate cancer. Abiraterone
acetate is a newer CYP17A inhibitor that irreversibly
blocks CYP17A production of DHEA from steroidprecursors (Figure 1).31 Interestingly, inhibition of
CYP17A also blocks production of cortisol, resulting
in increased ACTH and overproduction of othermineralocorticoid precursors. For this reason, all
patients must also receive corticosteroids to sup-
press ACTH production and prevent symptoms ofmineralocorticoid excess.31 Importantly, when
administered with corticosteroids, abiraterone
extends survival in patients with CRPC who havepreviously received docetaxel (14.8 months v 10.9
months, P o.0001).32 Abiraterone now has been
approved for CRPC after docetaxel and the data forits use in early CRPC prior to chemotherapy also has
been reported.33 Although trials in metastatic NCPC
are proposed or ongoing, there is reason to assumethat such agents will have even a better anti-tumor
effect in NCPC.
Orteronel (TAK-700) is another 17α-hydroxylase/17,20-lyase inhibitor that is more selective for the
lyase function of CYP17A.34 This selectivity has the
advantage of reduced activation of the mineralocor-ticoid pathway and thus may have the benefit of not
requiring concomitant corticosteroids.35 Currently,
there are two large phase III clinical trials evaluatingthe efficacy of this compound in metastatic CRPC
before and after chemotherapy compared to placebo
(NCT01193257 and NCT01193244).Enzalutamide is a more potent AR blocker that
binds to AR with higher affinity than biclutamide and
prevents the AR from translocation to the nucleus.34
Enzalutamide now also has been reported to extend
Page 5
Table 1. Prostate Cancer Pathways and Targets
Pathway Target Agent
Androgen signaling CYP17, androgen receptor Abiraterone, enzalutamide, ARN-509, TAK-700,TOK-001
Angiogenesis VEGF, VEGFR, PDGFR Olaratumab, tasquinomod, ramucirumabApoptosis BCL-2, clusterin AT-101, custirsenDNA repair PARP VeliparibBone microenvironment Integrins, RANK ligand EMD 525797, denosumabImmune system CTLA-4, tumor antigen Ipilimumab, sipuleucel-TReceptor tyrosine kinases IGF-1R, c-MET, SRC Cixutumumab, cabozantinib, casatinib
Abbreviations: VEGF/R- vascular endothelial growth factor/receptor, PDGF- platelet derived growth factor receptor, BCL-2- B celllymphoma 2, PARP- poly ADP ribose polymerase, RANK- receptor activator of nuclear factor kappa B, CTLA-4- cytotoxic Tlypmphocyte antigen 4, Insulin like growth factor 1R.
Non-castrate metastatic prostate cancer 341
the survival of patients with CRPC in a phase III
randomized placebo-controlled trial (median overall
survival, 18.4 v 13.6 months, respectively; hazardratio [HR] 0.631; P o .0001).36 The activity of more
potent AR blockade in CRPC indicates that they are
very likely to also have a role in patients withhormone-sensitive cancers.
Although, abiraterone, TAK-700, and enzaluta-
mide all show promising clinical activity in CRPC,development is already underway on third-
generation more potent inhibitors of androgen sig-
naling. TOK-001, a combined CYP17/anti-androgen,targets both CYP17-mediated production of andro-
gens and has anti-AR activity.37 A phase I trial has
recently completed accrual and results are pending(ARMOR1, NCT00959959). In addition, ARN-509, an
anti-AR agent with higher affinity for AR than
biclutamide and higher anti-tumor efficacy thanenzalutamide in preclinical models, is now being
tested in a phase I/II trial in patients with CRPC
(NCT01171898).38
The efficacy of both CYP17A inhibitors and more
potent AR blockade, even after extensive prior treat-
ment, raises the important question of whether earlierand more potent androgen suppression/blockade with
abiraterone, enzalutamide, or TAK-700 and similar
next-generation agents could improve survival inpatients with metastatic NCPC when tumors remain
maximally dependent on androgens for survival.
Recently reported data from a phase II trial ofabiraterone in combination with ADT in high risk
prostate cancer prior to surgery demonstrated that
addition of abiraterone increased PSA responses anddecreased DHT and DHEA levels suggesting a poten-
tial role for abiraterone in newly diagnosed disease.
Studies to determine the efficacy of abiraterone inconjunction with GnRH agonists in neoadjuvant set-
tings and as sensitizing agents for radiation are
ongoing (NCT01088529, NCT01023061). Moreover,the STAMPEDE trial includes an arm in which patients
with advanced NCPC will receive abiraterone and
ADT (NCT00268476). A phase II single-arm trial
addressing the inclusion of enzalutamide in earlierhormone-sensitive disease is also underway
(NCT01302041). Similarly, a recently approved con-
cept by SWOG will evaluate gonadal suppression plusbicalutamide versus gonadal suppression plus TAK-
700, in metastatic NCPC. Hopefully these trials will
begin to define the role of more effective androgensuppression in earlier stage disease and offer the
promise of preventing progression to CRPC.
BEYOND ANDROGENS—NEW TARGETS ANDDRUGS
The relative “diminishing returns” (modest sur-
vival improvements and efficacy in subsets of
patients) from strategies targeting androgen signal-ing in the setting of CRPC highlights the importance
of not only moving these agents to NCPC where a
better impact maybe possible but also to focus onother cellular pathways that contribute to the devel-
opment of CRPC.32 Clearly a better understanding of
the biology of progression is needed; however, manypathways have been identified and drugs targeting
these pathways are currently being explored
(Figure 2 and Table 1). If tolerable and effective inhumans, these agents may represent new options for
patients with newly metastatic NCPC.
One such pathway is the insulin-like growthfactor-1 (IGF-1) signaling pathway. IGF-1 binds to
IGF-1R, a receptor tyrosine kinase involved in cellu-
lar survival and proliferation in multiple tumor types,including prostate cancer.39 IGF-1R subsequently
activates the PI3K/AKT, RAS/MAPK, and SRC kinase
pathways, which drive proliferation and survival(Figure 2). Elevated IGF-1 has been identified as a
possible risk for development of prostate cancer and
prostate tumors have increased expression of IGF-1R.39 Several methods to block the IGF-1 pathway
Page 6
P.L. Palmbos and M. Hussain342
have been explored, including anti-sense oligonu-
cleotides and more recently the monoclonal anti-body, cixutumumab (IMC-A12). Because IGF-1
signaling participates with androgenic signaling to
promote tumor growth, combination with ADTpromotes tumor response in preclinical models of
NCPC.40 This hypothesis is currently being evaluated
in SWOG S0925, a randomized phase II trial of ADTwith or without cixutumumab in metastatic NCPC
with the primary endpoint of undetectable PSA.
Apoptosis is another important mechanismwhereby tumors avoid cell death after treatment. In
CRPC, upregulation of bcl-2 and clusterin blocks
apoptotic pathways and may provide a partialexplanation of resistance to cytotoxic chemotherapy
(Figure 2). AT-101 binds to bcl-2 and its related
family of anti-apoptotic proteins lowering cellularapoptotic threshold. A phase I clinical trial of AT-101
suggested disease-specific activity and a phase II trial
of AT-101 in combination with ADT in newlydiagnosed metastatic NCPC suggested a modest
increase in PSA response in patients with aggressive
disease.41,42 Likewise, the protein, clusterin,increases after androgen ablation and/or chemother-
apy, increasing cellular resistance to apoptosis.43
Custersin is an antisense oligonucleotide directedagainst clusterin, which lowers clusterin levels in
tumors. In a phase II trial of patients with CRPC
treated with docetaxel plus/minus custersin, therewas a suggestion of better survival for patients
receiving custersin (median survival, 23.8 v 16.9
months).44 These data led to a phase III trial ofcustersin in CRPC, which is currently enrolling
subjects. Because ADT induces upregulation of
anti-apoptotic proteins and induces apoptosis, itmay be reasonable to consider combining agents
targeting this pathway with ADT in metastatic NCPC
as well.Vascular endothelial growth factor (VEGFR) and
c-MET are receptor tyrosine kinases that govern
prostate cancer growth, angiogenesis, and boneremodeling. Although small trials testing agents that
target the VEGFR pathway (bevacizumab, sunitinib)
suggested possible anti-tumor activity in prostatecancer, confirmatory phase III trials have failed to
demonstrate survival benefits in patients with
CRPC.45–47 Other VEGF inhibitors are being eval-uated (Table 1). Interestingly, cabozantinib, a small-
molecule inhibitor of c-MET, VEGFR2, and multiple
tyrosine kinases, has shown promise in CRPC.A phase II trial of patients with metastatic CRPC
treated with cabozantinib demonstrated remarkable
reduction in metastatic bone disease and relief ofbone pain.48 c-MET expression increases with pros-
tate cancer progression and is associated with meta-
static disease, as well as angiogenesis (Figure 2).49,50
Interestingly, AR signaling also appears to repress
c-MET expression, and castration actually increases
c-MET expression.50 These findings imply that ADTdirectly participates in the emergence of castrate
resistance by upregulation of c-MET. Therefore, it is
rational to postulate that the combination of ADTwith c-MET multi-targeting agents like cabozantinib
or others might offer the potential of delaying the
development of CRPC.In patients with CRPC and bone metastasis,
inhibitors targeted at osteoclast activation have
proven to be an important adjunct to therapy.Specifically, bisphosphonate therapy with zolen-
dronic acid or the RANK ligand inhibitor, denosu-
mab, reduces skeletal-related events (SRE) in patientswith CRPC.51–53 These findings could suggest that
bone-protective agents might benefit patients with
metastatic NCPC. Despite this, a trial of thebisphosphonate, clodronate, did not show statisti-
cally significant improvements in survival or bone-
related events in patients with newly diagnosedmetastatic prostate cancer.54 A larger study, Cancer
and Leukemia Group B (CALGB) 90202, randomly
assigned 680 men with metastatic NCPC to eitherzolendronic acid or placebo and measured time to
first SRE or death. This study may help define
whether there is a role for bone-targeted agents inNCPC, but results are pending. Until then, the only
role for bone-stabilizing agents in metastatic NCPC is
for osteoporosis induced by ADT.Provoking the immune system to recognize and
exert an anti-tumor effect has been an important goal
for many years. Sipuleucel-T is an active cellularimmunotherapy consisting of host antigen-
presenting cells (APCs), which have been sensitized
to recognize prostate cancer by co-culture withprostatic acid phosphatase and granulocyte–macro-
phage colony-stimulating factor. This agent received
US Food and Drug Administration approval based ona survival advantage in a phase III trial.55–57 The
survival advantage in CRPC provokes interest in
using immunotherapy earlier in the course of pro-state cancer to prevent development of metastatic
disease or CRPC when disease burden is low. The
PROTECT trial is a phase III study randomizingpatients with biochemically recurrent prostate can-
cer after prostatectomy to either sipuleucel-T or
placebo with a primary endpoint of time to pro-gression and may begin to elucidate the optimal
timing of this controversial therapeutic in non-
castrate disease (NCT00779402).Ipilumimab is an anti-cytotoxic T-lymphocyte
antigen-4 (CTLA4) monoclonal antibody. Normally,
CTLA4 deactivates cytotoxic T lymphocytes, andipilumimab interferes with this process allowing
development of an anti-tumor cytotoxic response.
Early studies suggest that treatment of patients withprostate cancer can induce a cytotoxic immune
Page 7
Non-castrate metastatic prostate cancer 343
response directed at tumor.58 A phase II trial in
patients with advanced prostate cancer demon-strated that addition of ipilumimab to ADT improved
PSA responses and resulted in significant disease
down-staging in a fraction of patients.59 Additionaltrials are ongoing to explore the role of ipilumimab
in both CRPC and NCPC (NCT01377389 and
NCT00170157).
STRATEGIES FOR SUCCESS: EVALUATINGNOVEL THERAPIES IN METASTATIC NCPC
The large number of new hormonal and targetedagents make it essential to develop rational strategies
to approach clinical evaluation in metastatic NCPC
patients. Many patients will do well on traditionalADT for years and therefore the risks, costs, and
benefits of potential treatments must be weighed
carefully. For these reasons, several factors must beconsidered when designing trials to test these novel
agents.
First, trials must be designed with the under-standing that many patients with NCPC have a
relatively long survival. The overall survival for
newly diagnosed metastatic prostate cancer patientshas improved markedly over the last 20 years. In a
recent comparison of SWOG phase III clinical trials
(S8494, S8894, S9346) conducted in newly meta-static NCPC patients sequentially between 1985 and
2009, patients in S9346 demonstrated improved
median survivals compared to the earlier trials (49months v 30 and 34 months in the earlier trials) and
a 22% lower risk of death in S9346 compared to
S8894 (hazard ratio, 0.78; 95% confidence interval,0.70–0.87; P o.001).60 Indeed, patients in the S9346
study who achieved a PSA o0.2 ng/mL at 6–7months after ADT had a median survival of 75months.61 These results illustrate that many patients
with newly metastatic NCPC can expect to live 5–10years following diagnosis. Because of this, trialsassessing new drugs and treatment strategies in
NCPC must be designed and powered to detect
survival advantages that may not be apparent formore than 5–10 years.
Second, future trials should target high-risk
patient populations or those who are most likely torespond to therapy. Metastatic NCPC is a diverse
disease and while some patients never progression
on ADT, others rapidly progress and die fromdisease. Unlike some other cancers, we currently
have very limited tools to determine good and poor
prognosis at the time of diagnosis of metastaticdisease.62 One such tool is PSA response to initial
ADT. In S9346 (INT-0162), patients who did not
achieve a PSA o4 ng/mL after 6–7 months had amedian survival of less than 2 years, whereas
patients with a PSA o0.2 ng/mL had a median
survival of over 75 months.61 Clearly, patients withpoor PSA response to initial ADT are a group that
could derive benefit from improved therapy and may
therefore represent a group for which intensificationof therapy is justified using novel agents such as
abiraterone or enzalutamide to potentially improve
outcomes.Third, the pathways that drive prostate cancer
progression and growth are complicated and often
redundant and it is unlikely that single targetedagents will be effective (Figure 2). As trials to
examine newer targeted therapies in NCPC con-
tinue, it is essential to develop the correlativescience to define which patient groups will benefit
from single or combined targeted therapies. The
advent of personalized medicine, including molec-ular categorization and tumor genome sequencing,
may allow us to further target treatments to sub-
groups. To develop meaningful treatments, we willneed to define the pathways that drive an individual
tumor and then target them accordingly.
Fourth, although overall survival remains the goldstandard for phase III trials, the relatively long overall
survival for patients with newly diagnosed metastatic
NCPC makes survival endpoints impractical forsmaller phase II trials, which are necessary for
evaluation of novel agents. Therefore, the develop-
ment of accurate and predictive surrogate markers ofsurvival is essential. Pending the development of
better predictive biomarkers it is possible that using
PSA decline rates as an intermediate biomarker toefficiently test new treatment strategies before
embarking on large phase III trials is a reasonable
approach.Finally, all treatments must be judged not only by
their ability to prolong life but also on their associ-
ated costs, both side effect profile and cost-effectiveness. In CRPC patients, where survival is
measured in months, a small survival benefit and
greater toxicity could be tolerated, whereas NCPCpatients, who may live a decade or longer, may not
wish to suffer similar toxicities for proportionally
smaller benefits.
BEYOND CASTRATION—EXPLORING THEEVOLVING LANDSCAPE OF PROSTATECANCER CARE
In truth, the principles of treatment for metastatic
NCPC have not changed yet, but we now have more
tools to deliver standard care. Over the last decadecreative approaches to cytotoxic therapy and
improved molecular targeting of androgen signaling
have resulted in many treatment options for patientswith CRPC who previously had a grim prognosis.
Page 8
P.L. Palmbos and M. Hussain344
The challenge for the next decade will be to
determine the optimal sequencing and combinationsof these novel agents, potentially moving them ear-
lier in the disease course either as adjuvant therapies
or at presentation with metastatic NCPC. Although asubset of NCPC patients currently enjoys survival
estimates of 5–10 years, it is feasible that more
profound androgen suppression earlier in diseasewill specifically benefit patients with higher-risk
disease (poor PSA response) improving their dismal
prognosis. Based on our current understanding ofthe biologic drivers of prostate cancer progression, it
is reasonable to expect that deeper androgen depri-
vation in prostate cancer at an early stage when it ismost sensitive to androgen stimulus may produce
better and more durable disease responses, resulting
in prolonged survival and delayed progressionto CRPC.
In addition, we are starting to glimpse the path-
ways that drive prostate cancer to lose dependenceon androgen signaling. New drugs targeting these
pathways that drive survival and proliferation are
constantly being developed. The challenge of thesenew targeted drugs will be selecting and combining
agents in subsets of patients most likely to benefit
from them. To better define these categories, adeeper understanding of the biology of NCPC is
required. Perhaps next-generation sequencing and
molecular techniques will allow us to target path-ways instead of histology. While the role for these
novel hormonal and targeted agents remains to be
defined in clinical trials, it is likely that the biologicprocesses that they target are relevant in both NCPC
and CRPC, and therefore they may ultimately join a
growing armamentarium in the fight against prostatecancer.
REFERENCES1. Siegel R, Naishadham D, Jemal A. Cancer statistics,
2012. CA Cancer J Clin. 2012;62(1):10–29.
2. Harris WP, Mostaghel PS, Nelson B, et al. Androgen
deprivation therapy: progress in understanding mech-
anisms of resistance and optimizing androgen deple-
tion. Nat Clin Pract Urol. 2009;6(2):76–85.
3. Ruch JM, Hussain MH. Evolving therapeutic paradigms
for advanced prostate cancer. Oncology (Williston
Park). 2011;25(6):496–504.
4. Sharifi N, Auchus RJ. Steroid biosynthesis and prostate
cancer. Steroids. 2012;77(7):719–26.
5. Venkitaraman R, Thomas K, Huddart RA, et al. Efficacy
of low-dose dexamethasone in castration-refractory
prostate cancer. BJU Int. 2008;101(4):440–3.
6. Huggins C, Hodges CV. Studies on prostatic cancer: I.
The effect of castration, of estrogen and of androgen
injection on serum phosphatases in metastatic carci-
noma of the prostate. J Urol. 2002;168(1):9–12.
7. Byar DP. Proceedings: The Veterans Administration
Cooperative Urological Research Group's studies of
cancer of the prostate. Cancer. 1973;32(5):1126–30.
8. Cox RL, Crawford ED. Estrogens in the treatment of
prostate cancer. J Urol. 1995;154(6):1991–8.
9. Leuprolide versus diethylstilbestrol for metastatic pros-
tate cancer. The Leuprolide Study Group. N Engl J
Med. 1984;311(20):1281–6.
10. Van Poppel H, Klotz L. Gonadotropin-releasing hor-
mone: an update review of the antagonists versus
agonists. Int J Urol. 2012;19(7):594–601.
11. Klotz L, Boccon-Gibod L, Shore ND, et al. The efficacy
and safety of degarelix: a 12-month, comparative,
randomized, open-label, parallel-group phase III study
in patients with prostate cancer. BJU Int. 2008;102
(11):1531–8.
12. Tombal B, Miller K, Boccon-Gibod L, et al. Additional
analysis of the secondary end point of biochemical
recurrence rate in a phase 3 trial (CS21) comparing
degarelix 80 mg versus leuprolide in prostate cancer
patients segmented by baseline characteristics. Eur
Urol. 2010;57(5):836–842.
13. Akaza H. Combined androgen blockade for prostate
cancer: review of efficacy, safety and cost-effectiveness.
Cancer Sci. 2011;102(1):51–6.
14. Samson DJ, Seidenfeld J, Schmitt B, et al. Systematic
review and meta-analysis of monotherapy compared
with combined androgen blockade for patients with
advanced prostate carcinoma. Cancer. 2002;95
(2):361–76.
15. Koupparis A, Casey RG, Casey R, Robinson M, Gleave
ME. Novel targeted agents on the horizon for
castration-resistant prostate cancer. Future Oncol.
2010;6(12):1883–95.
16. Ryan CJ, Tindall DJ. Androgen receptor rediscovered:
the new biology and targeting the androgen receptor
therapeutically. J Clin Oncol. 2011;29(27):3651–8.
17. Isaacs JT, Coffey DS. Adaptation versus selection as the
mechanism responsible for the relapse of prostatic
cancer to androgen ablation therapy as studied in the
Dunning R-3327-H adenocarcinoma. Cancer Res.
1981;41(12 Pt 1):5070–5.
18. Bruchovsky N, Rennie PS, Coldman AJ, Goldenberg SL,
To M, Lawson D. Effects of androgen withdrawal on
the stem cell composition of the Shionogi carcinoma.
Cancer Res. 1990;50(8):2275–82.
19. Saylor PJ, Smith MR. Adverse effects of androgen
deprivation therapy: defining the problem and pro-
moting health among men with prostate cancer. J Natl
Compr Canc Netw. 2010;8(2):211–23.
20. Calais da Silva FEC, Bono AV, Whelan P, et al. Inter-
mittent androgen deprivation for locally advanced and
metastatic prostate cancer: results from a randomised
phase 3 study of the South European Uroncological
Group. European Urology. 2009;55(6):1269–77.
21. Mottet N, Van Damme J, Loulidi S, Russel C, Leiten-
berger A, Wolff JM. Intermittent hormonal therapy in
the treatment of metastatic prostate cancer: a random-
ized trial. BJU Int. 2012;110(9):1262–9.
22. Salonen AJ, Taari K, Ala-Opas M, Viitanen J, Lundstedt
S, Tammela TLJ. The FinnProstate Study VII: intermit-
tent versus continuous androgen deprivation in
Page 9
Non-castrate metastatic prostate cancer 345
patients with advanced prostate cancer. J Urol.
2012;187(6):2074–81.
23. Langenhuijsen JF, Badhauser D, Schaaf B, Kiemeney
LALM, Witjes JA, Mulders PFA. Continuous vs. inter-
mittent androgen deprivation therapy for metastatic
prostate cancer. Urol Oncol. 2011. [Epub ahead of
print].
24. Hussain M, Tangen CM, Celestia HS, et al. Intermittent
(IAD) versus continuous androgen deprivation (CAD)
in hormone sensitive metastatic prostate cancer
(HSM1PC) patients (pts): results of S9346 (INT-
0162), an international phase III trial. J Clin Oncol.
2012;30 suppl: abstr 4.
25. Osborne CK, Blumenstein B, Crawford ED, et al.
Combined versus sequential chemo-endocrine therapy
in advanced prostate cancer: final results of a random-
ized Southwest Oncology Group study. J Clin Oncol.
1990;8(10):1675–82.
26. Kantoff PW, Halabi S, Conaway M, et al. Hydrocorti-
sone with or without mitoxantrone in men with
hormone-refractory prostate cancer: results of the
Cancer and Leukemia Group B 9182 study. J Clin
Oncol. 1999;17(8):2506–13.
27. Petrylak DP, Tangen CM, Hussain MH, et al. Docetaxel
and estramustine compared with mitoxantrone and
prednisone for advanced refractory prostate cancer. N
Engl J Med. 2004;351(15):1513–20.
28. Tannock IF, de Wit R, Berry WR, et al. Docetaxel plus
prednisone or mitoxantrone plus prednisone for
advanced prostate cancer. N Engl J Med. 2004;351
(15):1502–12.
29. Dorff TB, Tangen CM, Crawford ED, et al. Cooperative
Group Trials—Southwest Oncology Group (SWOG)
innovations in advanced prostate cancer. Ther Adv
Med Oncol. 2009;1(2):69–77.
30. Bluemn EG, Nelson PS. The androgen/androgen recep-
tor axis in prostate cancer. Curr Opin Oncol. 2012;24
(3):251–7.
31. Rehman Y, Rosenberg JE. Abiraterone acetate: oral
androgen biosynthesis inhibitor for treatment of
castration-resistant prostate cancer. Drug Des Devel
Ther. 2012;6:13–8.
32. de Bono JS, Logothetis CJ, Molina A, et al. Abiraterone
and increased survival in metastatic prostate cancer. N
Engl J Med. 2011;364(21):1995–2005.
33. Ryan C, Smith M, DeBono J, et al. Interim analysis (IA)
results of COU-AA-302, a randomized, phase III study of
abiraterone acetate (AA) in chemotherapy-naive patients
(pts) with metastatic castration-resistant prostate cancer
(mCRPC). J Clin Oncol. 2012;30 suppl: abstr LBA4518.
34. Massard C, Fizazi K. Targeting continued androgen
receptor signaling in prostate cancer. Clin Cancer Res.
2011;17(12):3876–83.
35. Yamaoka M, Hara T, Hitaka T, et al. Orteronel (TAK-
700), a novel non-steroidal 17,20-lyase inhibitor:
effects on steroid synthesis in human and monkey
adrenal cells and serum steroid levels in cynomolgus
monkeys. J Steroid Biochem Mol Biol. 2012;129(3-
5):115–28.
36. Scher HI, Saad F, Taplin ME, et al. Effect of MDV3100,
an androgen receptor signaling inhibitor (ARSI), on
overall survival in patients with prostate cancer
postdocetaxel: results from the phase III AFFIRM
study. J Clin Oncol. 2012;30 suppl 5: abstr LBA1.
37. Vasaitis T, Belosay A, Schayowitz A, et al. Androgen
receptor inactivation contributes to antitumor efficacy
of 17{alpha}-hydroxylase/17,20-lyase inhibitor 3beta-
hydroxy-17-(1H-benzimidazole-1-yl)androsta-5,16-
diene in prostate cancer. Mol Cancer Ther. 2008;7
(8):2348–57.
38. Clegg NJ, Wongvipat J, Joseph JD, et al. ARN-509: a
novel antiandrogen for prostate cancer treatment.
Cancer Res. 2012;72(6):1494–503.
39. Kojima S, Inahara M, Suzuki H, Ichikawa T, Furuya Y.
Implications of insulin-like growth factor-I for prostate
cancer therapies. Int J Urol. 2009;16(2):161–7.
40. Plymate SR, Haugk K, Coleman I, et al. An antibody
targeting the type I insulin-like growth factor receptor
enhances the castration-induced response in androgen-
dependent prostate cancer. Clin Cancer Res. 2007;13
(21):6429–39.
41. MacVicar GR, Somer B, Greco FA, Brill K, Leopold L.
An open-label, multicenter, phase I/II study of AT-101
in combination with docetaxel (D) and prednisone
(P) in men with hormone refractory prostate cancer
(HRPC). J Clin Oncol. 2008;26 suppl: abstr 16043.
42. Stein MN, Khan I, Hussain M, et al. Phase II study of AT-
101 to abrogate Bcl-2-mediated resistance to androgen-
deprivation therapy (ADT) in patients (pts) with newly
diagnosed androgen-dependent metastatic prostate can-
cer (ADMPC). J Clin Oncol. 2011;29(suppl 7); abstr 137.
43. July LV, Akbari M, Zellweger T, Jones EC, Goldenberg
SL, Gleave ME. Clusterin expression is significantly
enhanced in prostate cancer cells following androgen
withdrawal therapy. Prostate. 2002;50(3):179–88.
44. Chi KN, Hotte SJ, Yu EY, et al. Randomized phase II
study of docetaxel and prednisone with or without
OGX-011 in patients with metastatic castration-
resistant prostate cancer. J Clin Oncol. 2010;28
(27):4247–54.
45. Kelly WK, Halabi S, Carducci M, et al. Randomized,
double-blind, placebo-controlled phase III trial com-
paring docetaxel and prednisone with or without
bevacizumab in men with metastatic castration-
resistant prostate cancer: CALGB 90401. J Clin Oncol.
2012;30(13):1534–40.
46. Sonpavde G, Periman PO, Bernold D, et al. Sunitinib
malate for metastatic castration-resistant prostate can-
cer following docetaxel-based chemotherapy. Ann
Oncol. 2010;21(2):319–24.
47. Dror Michaelson M, Regan MM, Oh WK, et al. Phase II
study of sunitinib in men with advanced prostate
cancer. Ann Oncol. 2009;20(5):913–20.
48. Smith DC, et al. Phase II study of XL184 in a cohort of
patients (pts) with castration-resistant prostate cancer
(CRPC) and measurable soft tissue disease. J Clin
Oncol. 2011;29 suppl 7: abstr 127.
49. Humphrey PA, Zhu X, Zarnegar R, et al. Hepatocyte
growth factor and its receptor (c-MET) in prostatic
carcinoma. Am J Pathol. 1995;147(2):386–96.
50. Verras M, Lee J, Xue H, Li TH, Wang Y, Sun Z. The
androgen receptor negatively regulates the expression
of c-Met: implications for a novel mechanism of
Page 10
P.L. Palmbos and M. Hussain346
prostate cancer progression. Cancer Res. 2007;67
(3):967–75.
51. Smith MR, Saad F, Coleman R, et al. Denosumab and
bone-metastasis-free survival in men with castration-
resistant prostate cancer: results of a phase 3, rando-
mised, placebo-controlled trial. Lancet. 2012;379
(9810):39–46.
52. Fizazi K, Carducci M, Smith M, et al. Denosumab
versus zoledronic acid for treatment of bone metasta-
ses in men with castration-resistant prostate cancer: a
randomised, double-blind study. Lancet. 2011;377
(9768):813–22.
53. Saad F, Gleason DM, Murray R, et al. Long-term
efficacy of zoledronic acid for the prevention of
skeletal complications in patients with metastatic
hormone-refractory prostate cancer. J Natl Cancer
Inst. 2004;96(11):879–82.
54. Dearnaley DP, Sydes MR, Mason MD, et al. A double-
blind, placebo-controlled, randomized trial of oral
sodium clodronate for metastatic prostate cancer
(MRC PR05 Trial). J Natl Cancer Inst. 2003;95
(17):1300–11.
55. Small EJ, Schellhammer PF, Higano CS, et al. Placebo-
controlled phase III trial of immunologic therapy with
sipuleucel-T (APC8015) in patients with metastatic,
asymptomatic hormone refractory prostate cancer. J
Clin Oncol. 2006;24(19):3089–94.
56. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T
immunotherapy for castration-resistant prostate can-
cer. N Engl J Med. 2010;363(5):411–22.
57. Higano CS, Schellhammer PF, Small EJ, et al. Integrated
data from 2 randomized, double-blind, placebo-con-
trolled, phase 3 trials of active cellular immunotherapy
with sipuleucel-T in advanced prostate cancer. Cancer.
2009;115(16):3670–9.
58. Small EJ, Tchekmedyian NS, Rini BI, Fong L, Lowy I,
Allison JP, et al. A pilot trial of CTLA-4 blockade with
human anti-CTLA-4 in patients with hormone-
refractory prostate cancer. Clin Cancer Res. 2007;13
(6):1810–5.
59. Tollefson MK, Karnes RJ, Thompson RH, et al. A
randomized phase II study of ipilimumab with andro-
gen ablation compared with androgen ablation alone
in patients with advanced prostate cancer. Genito-
urinary Cancers Symposium. 2010 Abstract 168.
March 5-7, 2010, San Francisco, USA.
60. Tangen C, Hussain M, Higano C, et al. Improved
overall survival trends of men with newly diagnosed
M1 prostate cancer. a SWOG phase III trial experience
(S8494, S8894 & S9346). J Urol. 2012;188(4):1164–9.
61. Hussain M, Tangen CM, Higano C, et al. Absolute
prostate-specific antigen value after androgen depriva-
tion is a strong independent predictor of survival in
new metastatic prostate cancer: data from Southwest
Oncology Group trial 9346 (INT-0162). J Clin Oncol.
2006;24(24):3984–90.
62. Grivas PD, Robins DM, Hussain M. Predicting response
to hormonal therapy and survival in men with hor-
mone sensitive metastatic prostate cancer. Crit Rev
Oncol Hematol. 2012.