CARBOHYDRATE METABOLISM IN ADDISON'S DISEASE1 By GEORGE W. THORN, GEORGE F. KOEPF, ROGER A. LEWIS,2 AND ELIZABETH F. OLSEN (From the Chemical Division, Medical Clinic, The Johns Hopkins University and Hospital, Baltimore) (Received for publication July 15, 1940) Our understanding of the nature of the dis- ordered carbohydrate metabolism in Addison's disease has advanced little since the original dem- onstration by Porges in 1910 (1) of the frequent occurrence of hypoglycemic reactions and the studies of Eppinger, Falta and Rudinger in which an increase in glucose tolerance was noted (2). Subsequently, however, it was shown that patients with Addison's disease developed marked symp- toms of hypoglycemia following the administra- tion of small doses of insulin (3) and failed to show a rise of blood sugar as great as normnal subjects following the injection of a standard dose of epinephrin (4). Recently Long, Katzin and Fry (5) reported in detail their studies relating to the effect of adrenal cortical hormone on the carbohydrate metabolism of experimental animals. From their own studies, as well as those of others, these authors concluded that " the administration of cortical extract apparently decreases the propor- tion of glucose oxidized while there is an in- creased proportion deposited as liver glycogen. . . . It is suggested that one of the properties of the cortical hormone is a stimulation of protein catabolism and that the increased carbohydrate levels, nitrogen and potassium excretion following its injection into animals is an expression of this effect." A study of carbohydrate metabolism in un- treated patients with Addison's disease is difficult because of the poor clinical condition of these patients. In the present study we have had the good fortune to be able to complete carefully con- trolled metabolic studies on a limited number of untreated patients and on a larger number of pa- tients who were maintained in good condition by 1 This study was aided by a grant from the Committee on Research in Endocrinology, National Research Coun- cil. 2John D. Archbold, Fellow in Medicine. means of synthetic desoxycorticosterone acetate therapy.8 METHODS Before these studies were undertaken, normal subjects and patients with Addison's disease were maintained for a period of 1 to 2 weeks on a standard diet of adequate caloric intake. The ratio of carbohydrate: protein: fat was kept constant. In most instances patients received 5.0 grams of carbohydrate, 1.3 grams of protein and 1.5 grams of fat per kgm. of body weight. Respiratory metabolism During a preliminary period of 1 to 2 weeks, both the normal subjects and patients were trained for respiratory metabolic studies. Expired air was collected for 10-min- ute periods in a modified Baily gasometer and samples were analyzed in duplicate for carbon dioxide and oxygen by means of a Haldane-Henderson gas analyzer. Differ- ential derivation of calories was made with the aid of Lusk's table (6). In addition to determining the standard metabolism after a 15-hour fast, the respiratory metabo- lism, blood sugar (7) and urinary nitrogen (kjeldahl) were determined throughout the day at 2-hour intervals during a total fasting period of 22 hours. These de- terminations were repeated following the injection of adrenal cortical extract (Wilson, 50 cc.).4 The respira- tory quotient, blood sugar and urinary nitrogen excretion were determined at hourly intervals following the intra- venous administration of glucose before and after treat- ment with adrenal cortical extract (50 cc.), desoxycorti- costerone acetate (30 mgm.), corticosterone (85 mgm.) ,5 and 17-hydroxy-1l-dehydrocorticosterone (33 mgm.) (Kendall's Compound E).5 Standard intravenous glucose tolerance test A test was adopted in which 0.5 gram of glucose per kgm. of body weight was injected intravenously as a 20 8 The synthetic desoxycorticosterone acetate used in this study was provided through the courtesy of Doctor E. Oppenheimer, of the Ciba Pharmaceutical Products, Inc., Summit, N. J. 4 The adrenal cortical extract used in this study was supplied by Doctor David Klein of the Wilson Company, Chicago, Ill. 5We are indebted to Doctor E. C. Kendall of the Mayo Clinic, Rochester, Minn., for the crystalline cortico- sterone and 17-hydroxy-l1-dehydrocorticosterone (Com- pound E). 813
Transcript
CARBOHYDRATEMETABOLISMIN ADDISON'S DISEASE1
By GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS,2 ANDELIZABETH F. OLSEN
(From the Chemical Division, Medical Clinic, The Johns Hopkins Universityand Hospital, Baltimore)
(Received for publication July 15, 1940)
Our understanding of the nature of the dis-ordered carbohydrate metabolism in Addison'sdisease has advanced little since the original dem-onstration by Porges in 1910 (1) of the frequentoccurrence of hypoglycemic reactions and thestudies of Eppinger, Falta and Rudinger in whichan increase in glucose tolerance was noted (2).Subsequently, however, it was shown that patientswith Addison's disease developed marked symp-toms of hypoglycemia following the administra-tion of small doses of insulin (3) and failed toshow a rise of blood sugar as great as normnalsubjects following the injection of a standard doseof epinephrin (4).
Recently Long, Katzin and Fry (5) reportedin detail their studies relating to the effect ofadrenal cortical hormone on the carbohydratemetabolism of experimental animals. From theirown studies, as well as those of others, theseauthors concluded that " the administration ofcortical extract apparently decreases the propor-tion of glucose oxidized while there is an in-creased proportion deposited as liver glycogen.. . . It is suggested that one of the properties ofthe cortical hormone is a stimulation of proteincatabolism and that the increased carbohydratelevels, nitrogen and potassium excretion followingits injection into animals is an expression of thiseffect."
A study of carbohydrate metabolism in un-treated patients with Addison's disease is difficultbecause of the poor clinical condition of thesepatients. In the present study we have had thegood fortune to be able to complete carefully con-trolled metabolic studies on a limited number ofuntreated patients and on a larger number of pa-tients who were maintained in good condition by
1 This study was aided by a grant from the Committeeon Research in Endocrinology, National Research Coun-cil.
2John D. Archbold, Fellow in Medicine.
means of synthetic desoxycorticosterone acetatetherapy.8
METHODS
Before these studies were undertaken, normal subjectsand patients with Addison's disease were maintained fora period of 1 to 2 weeks on a standard diet of adequatecaloric intake. The ratio of carbohydrate: protein: fatwas kept constant. In most instances patients received5.0 grams of carbohydrate, 1.3 grams of protein and 1.5grams of fat per kgm. of body weight.
Respiratory metabolismDuring a preliminary period of 1 to 2 weeks, both the
normal subjects and patients were trained for respiratorymetabolic studies. Expired air was collected for 10-min-ute periods in a modified Baily gasometer and sampleswere analyzed in duplicate for carbon dioxide and oxygenby means of a Haldane-Henderson gas analyzer. Differ-ential derivation of calories was made with the aid ofLusk's table (6). In addition to determining the standardmetabolism after a 15-hour fast, the respiratory metabo-lism, blood sugar (7) and urinary nitrogen (kjeldahl)were determined throughout the day at 2-hour intervalsduring a total fasting period of 22 hours. These de-terminations were repeated following the injection ofadrenal cortical extract (Wilson, 50 cc.).4 The respira-tory quotient, blood sugar and urinary nitrogen excretionwere determined at hourly intervals following the intra-venous administration of glucose before and after treat-ment with adrenal cortical extract (50 cc.), desoxycorti-costerone acetate (30 mgm.), corticosterone (85 mgm.) ,5and 17-hydroxy-1l-dehydrocorticosterone (33 mgm.)(Kendall's Compound E).5
Standard intravenous glucose tolerance test
A test was adopted in which 0.5 gram of glucose perkgm. of body weight was injected intravenously as a 20
8 The synthetic desoxycorticosterone acetate used inthis study was provided through the courtesy of DoctorE. Oppenheimer, of the Ciba Pharmaceutical Products,Inc., Summit, N. J.
4 The adrenal cortical extract used in this study wassupplied by Doctor David Klein of the Wilson Company,Chicago, Ill.
5We are indebted to Doctor E. C. Kendall of theMayo Clinic, Rochester, Minn., for the crystalline cortico-sterone and 17-hydroxy-l1-dehydrocorticosterone (Com-pound E).
813
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
per cent solution in distilled water. The flow was ad-justed so that the infusion was completed in 30 minutes.This rate of glucose administration (0.5 gram per kgm.per % hour) approximated the maximum rate of in-testinal absorption of glucose and hence provided anintravenous glucose test which was within physiologicallimits. Capillary blood for sugar determinations wastaken in the fasting state and at 30-minute intervals dur-ing a 4-hour period following the glucose infusion. Urinespecimens were collected at appropriate intervals andanalyzed for sugar.
Oral glucose tolerance testA solution of glucose, 1.75 grams per kgm. of body
weight, was given. Capillary blood for sugar deter-minations was taken during the fasting state and 30, 60,120 and 180 minutes after the ingestion of glucose.
Epinephrin test
Epinephrin, 0.007 mgm. per kgm. of body weight, wasinjected subcutaneously. The site of the injection wasmassaged vigorously for a period of 2 minutes. Capil-lary blood for sugar determinations was taken duringthe fasting state and 15, 30, 60 and 90 minutes after theinjection of epinephrin.
OBSERVATIONS
Increased appetite for carbohydrateIt is of interest to note that many patients with
Addison's disease had formed the habit of sup-
plementing their regular diet with intermediatenourishment of foods containing readily availablecarbohydrate (Patient E. L., see protocol). Inthis respect there is a parallel to the increasedappetite for salt and salty foods which has beennoted clinically by many observers, and confirmedexperimentally by the studies of Richter andEckert on adrenalectomized rats (8).
Fasting blood glucoseThe fasting blood glucose level of untreated
patients with Addison's disease was observed tobe in the low-normal range in most instances. Ina group of 20 patients the average blood glucosevalue a (108 determinations) was observed to be80 mgm. per 100 cc. before treatment. Prolongedtreatment with desoxycorticosterone acetate didnot affect the fasting blood glucose level since theaverage value observed during treatment was also
*All blood sugar values determined by the modifiedmicromethod of Folin and Malmros are arbitrarily re-ferred to in this study as " blood glucose values."
80 mgm. per 100 cc. (166 determinations). Theseobservations confirm earlier studies (9, 10).
Treatment with adrenal cortical extract (Wil-son, 4 to 10 cc. daily, injected subcutaneously)was associated with an appreciable rise in theaverage fasting blood glucose level (Table I).
TABLE I
Effect of adrenal cortical hormone therapy onfasting blood glucose
3-20gz. 4-10 cc. 8-12 c. 33 i__________ ~~dal dail dail __ ____5 patents 76 77 81 83(Number of de-
teminatIons). (43) (60) (20) (30) _Patent E. L .. 75 75 84 99 95Rage.. (6-81) (72-81)
Includes values observed during treatment with eitherdaily intramuscular injection of a solution of hormone inoil, or subcutaneously implanted pellets of crystallinedesoxycorticosterone acetate.
t Massive dose, 50-70 cc., during a 24-hour period.
The oral administration of larger quantities ofadrenal cortical extract in glycerol solution (8 to12 cc. daily, 1 cc. representing 50 grams ofadrenal gland) was likewise associated with a risein the average value for fasting blood glucose.Treatment with large quantities of adrenal corti-cal extract (Wilson, 20 to 50 cc. daily, injectedsubcutaneously and intravenously), corticosterone(85 mgm.) and 17-hydroxy-11-dehydrocortico-sterone (33 mgm.) in oil, injected intramuscularlyin divided doses, was followed by a much greaterelevation in fasting blood glucose level (PatientE. L., Table I).
The efficacy of treatment with adrenal corticalextract (50 to 70 cc.) in preventing the gradualfall in blood glucose during a prolonged fast isillustrated in Figure 1. The rise in blood glucosewhich reached its maximum 6 to 8 hours afterinjection of extract did not appear to be due totraces of epinephrin which may have been presentin the extract, since there was no immediate risein blood glucose as might have been anticipatedfollowing an injection of epinephrin.
814
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
M.B.ADD/5ON'3 DI3EA3
Ex+ract_I
"01 bNo treatment-~M Adrenal Cortical
extract
I,---___________------7
I5 18 21
FIG. 1. EFFECT OF ADRENALCORTICAL EXTRACTON BLooD GLUCOSELEVEL(PROLONGEDFAST)
Oral glucose toleranceThe striking intolerance of patients with Addi-
son's disease to the oral administration of glucoseis well known (11). Not infrequently an adrenalcrisis has been precepitated by this test.
A comparison between the blood glucose valuesof 8 control subjects and 4 untreated patients withAddison's disease following the oral administra-tion of glucose, is shown in Figure 2. The low-normal initial fasting sugar level, the " flat-type "of glucose curve, and the striking hypoglycemiawhich was frequently noted 2 to 3 hours follow-ing the administration of glucose are of particular
BLOOD - -
GLUCOSEMG. i5operp
*100 CC.
125
10C .)75
50
25 _
0
MINUTE5 0
significance in the response of patients with Ad-dison's disease. At the time of initial examina-tion, approximately 75 per cent of a group of 30patients with Addison's disease were found tohave an abnormal oral glucose tolerance curve.
The symptoms of pylorospasm which so fre-quently followed the oral administration of glu-cose to these patients suggest that the apparentincrease in glucose tolerance (flat-type of curve)was in a large measure due to an abnormality inthe intestinal absorption of glucose. This- was
confirmed by the normal height to which the bloodglucose level rose following the intravenous ad-
60 12O
FIG. 2. ORLGLUCOSETOLERANcE TEST
180
BloodGlucoseMgc.per
00OO'C.C
100
80
401
0Hours
815
o0
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN ,.
4 PATIENTSADDISON'S DISEASE
.-- BEFORE TREATMENT..ee... AM1R TREATMENT
[AVERAGE DURATIONOF3kTREATMENT-IYEAR I
4? .
0*S*
0S* *@SS@*0S@0000%
*0 *%96iXf"'40%90690I-~~~~~~~~~~~~1a
M-INUTES 0 60 120
FIG. 3. ORAL GLUCOSETOLERNCETEST. THE EFFECT OFDESOXYCORTICOSTERoNETREATMENT
186
ministration of a standard dose of glucose (seeFigure 5).
Following prolonged treatment (1 year ormore) with desoxycorticosterone acetate, we ob-served a marked change in the oral glucose toler-ance curve in 4 patients (Figure 3). The clini-cal condition of these patients was markedly
improved at the time the second glucose curvewas determined. It would seem likely that thechange in the glucose curve was due primarily toimproved absorption of glucose from the intes-tinal tract and not to a marked or specific effectof desoxycorticosterone acetate on the internalmetabolism of glucose, inasmuch as desoxycortico-
sterone acetate therapy had no demonstrable effecton the blood glucose curve following the intra-venous administration of glucose.
Intravenous glucose toleranceIn order to eliminate the obvious disadvantages
of glucose administered orally, we used a standardintravenous glucose tolerance test (see methods).One consideration seemed essential, viz., that therate of glucose solution introduced intravenouslyshould not exceed the maximum rate of intestinalabsorption of glucose, if physiological studies were
to be made. Experience now indicates that, underconstant conditions, the blood glucose curve fol-lowing the intravenous administration of 0.5gram of glucose per kgm. of body weight duringa 30-minute period is constant for a given indi-vidual (Figure 4).
Patients with Addison's disease frequently de-veloped marked symptoms of hypoglycemia 2 to 3hours after the administration of glucose intra-venously (Table II). In some patients coma andvasomotor collapse occurred and additional glu-
utes utes utes utes utes utes utes utesF. H. M 21 77 210 182 163 123 86 65 50 48*Y. E. F 39 79 225 177 120 118 84 66 59*S. W. F 55 111 426 235 171 100 77 69*J. P. M 21 79 270 202 192 163 99 75 62*M. B. F 31 78 250 135 77 56 48* 61*0. 0. M 43 78 241 182 140 100 74 52 50*E. L. F 51 76 235 183 153 103 77 61 50*A. H. M 39 89 140 113 72 61*0. Q. M 62 81 241 182 149 118 90 76 68 62B. W. M 26 86 264 215 196 142 105 86 69 69A S. M 33 78 200 164 131 105 84 68 62 77S. P. M 27 80 206 156 105 80 68 60 72A. H. F 20 78 222 194 164 131 97 70 60 64H. H. M 38 99 254 225 153 112 104 78 78 80
NORMALStBJIECTS
F. A. M 23 81 282 204 164 88 67 69 82 106A. K. M 23 84 194 91 78 71 76 84C. D. M 26 89 220 123 70 55 78 80 84 87R. L. M 28 95 290 202 164 106 75 73 64 68S. A. M 25 87 220 155 110 81 76 83 81 78
* Hypoglycemic reaction.
817
818 GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS., ANDELIZABETH F. OLSEN
F- u~~~~~~~~~~I
usU
o -
0 ~~~j!- [ 8~~-
o (oZ<0~~~~~
x z~~WV~~~~SW'
0~~~~~~~u 8~~~~
or ~ *o
a-~~~~~~~~~~~atA*~~~~~~~~~~
~~~ hi~a
0~~~~Z~~~~~~~~j ). ig~~~
hi
z
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
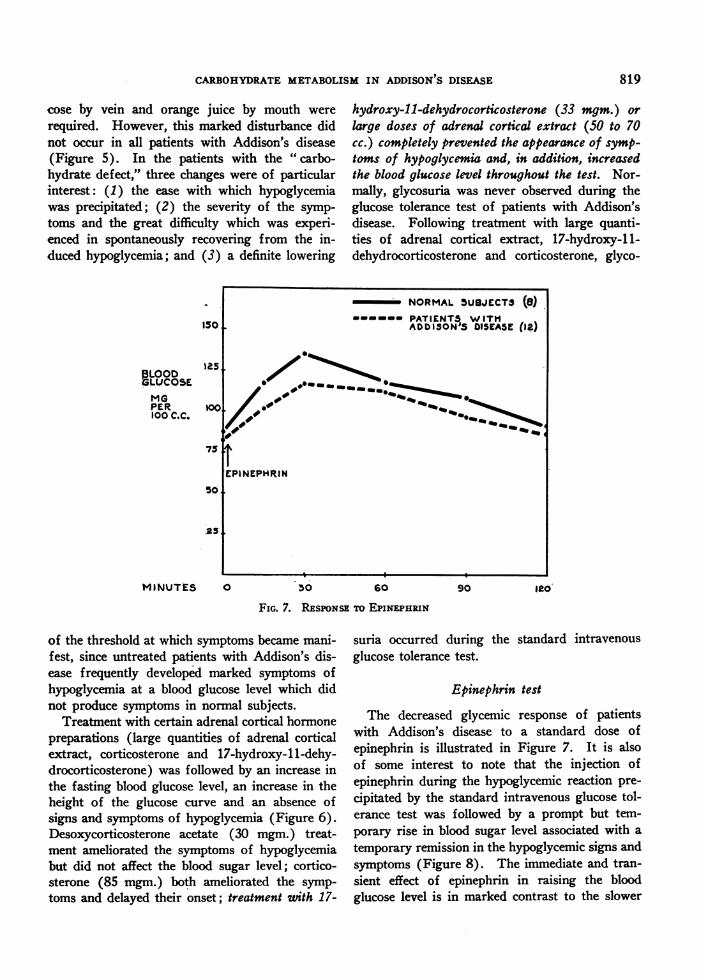
cose by vein and orange juice by mouth wererequired. However, this marked disturbance didnot occur in all patients with Addison's disease(Figure 5). In the patients with the "carbo-hydrate defect," three changes were of particularinterest: (1) the ease with which hypoglycemiawas precipitated; (2) the severity of the symp-toms and the great difficulty which was experi-enced in spontaneously recovering from the in-duced hypoglycemia; and (3) a definite lowering
BLOODBLUCOSEMGPER100 C.C.
MINUTES 0
hydroxy-11-dehydrocorticosterone (33 mgm.) orlarge doses of adrenal cortical extract (50 to 70cc.) completely prevented the appearance of symp-toms of hypoglycemia and, in addition, increasedthe blood glucose level throughout the test. Nor-mally, glycosuria was never observed during theglucose tolerance test of patients with Addison'sdisease. Following treatment with large quanti-ties of adrenal cortical extract, 17-hydroxy-11-dehydrocorticosterone and corticosterone, glyco-
120
of the threshold at which symptoms became mani-fest, since untreated patients with Addison's dis-ease frequently developed marked symptoms ofhypoglycemia at a blood glucose level which didnot produce symptoms in normal subjects.
Treatment with certain adrenal cortical hormonepreparations (large quantities of adrenal corticalextract, corticosterone and 17-hydroxy-11-dehy-drocorticosterone) was followed by an increase inthe fasting blood glucose level, an increase in theheight of the glucose curve and an absence ofsigns and symptoms of hypoglycemia (Figure 6).Desoxycorticosterone acetate (30 mgm.) treat-ment ameliorated the symptoms of hypoglycemiabut did not affect the blood sugar level; cortico-sterone (85 mgm.) both ameliorated the symp-toms and delayed their onset; treatment wuth 17-
suria occurred duringglucose tolerance test.
the standard intravenous
Epinephrin test
The decreased glycemic response of patientswith Addison's disease to a standard dose ofepinephrin is illustrated in Figure 7. It is alsoof some interest to note that the injection ofepinephrin during the hypoglycemic reaction pre-cipitated by the standard intravenous glucose tol-erance test was followed by a prompt but tem-
porary rise in blood sugar level associated with a
temporary remission in the hypoglycemic signs andsymptoms (Figure 8). The immediate and tran-sient effect of epinephrin in raising the bloodglucose level is in marked contrast to the slower
50 60 90
FIG. 7. RESPONSETO EPINEPHRIN
819
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
and more prolonged action of adrenal corticalhormone (4 to 24 hours).
In one patient the response to epinephrin fol-lowing an overnight fast was observed in theuntreated state and again after several days oftreatment with adequate doses of adrenal corticalhormone (20 cc. daily, injected subcutaneously).Associated with treatment there was a small butdefinite increase in the height of the blood glucosecurve, an increment of 27, 15, 11, 3 mgm., re-spectively, at 15, 30, 60 and 90 minutes followingthe subcutaneous injection of epinephrin (seemethods).
Response to insulinBecause of the profound reaction of patients
with Addison's disease to relatively small dosesof insulin, we did not study the action of thishormone in human subjects. In bilaterally ad-renalectomized dogs (to be reported elsewhere),it was demonstrated that treatment (6 to 18 hoursbeforehand) with 50 to 80 cc. of adrenal corticalextract completely prevented the severe and oftenfatal hypoglycemic reaction which followed theintravenous injection of 0.25 units of insulin perkggm. Large quantities of desoxycorticosteroneacetate (50 mgm. or more) were ineffective inpreventing convulsions. Treatment with 17-hy-droxy-11-dehydrocorticosterone, however, in adose of 10 mgm., permitted the animal to survive
the test without supplementary glucose therapy.The limited quantity of crystalline hormone avail-able did not permit an exact determination ofequivalent quantities of adrenal cortical extractand crystalline 17-hydroxy-1 1-dehydrocortico-sterone.
Standard metabolismThe standard metabolism of patients with Ad-
dison's disease has been considered to be definitelylower than that of normal subjects. The valueswhich were obtained in 15 untreated patients aregiven in Figure 9. In our experience a basal
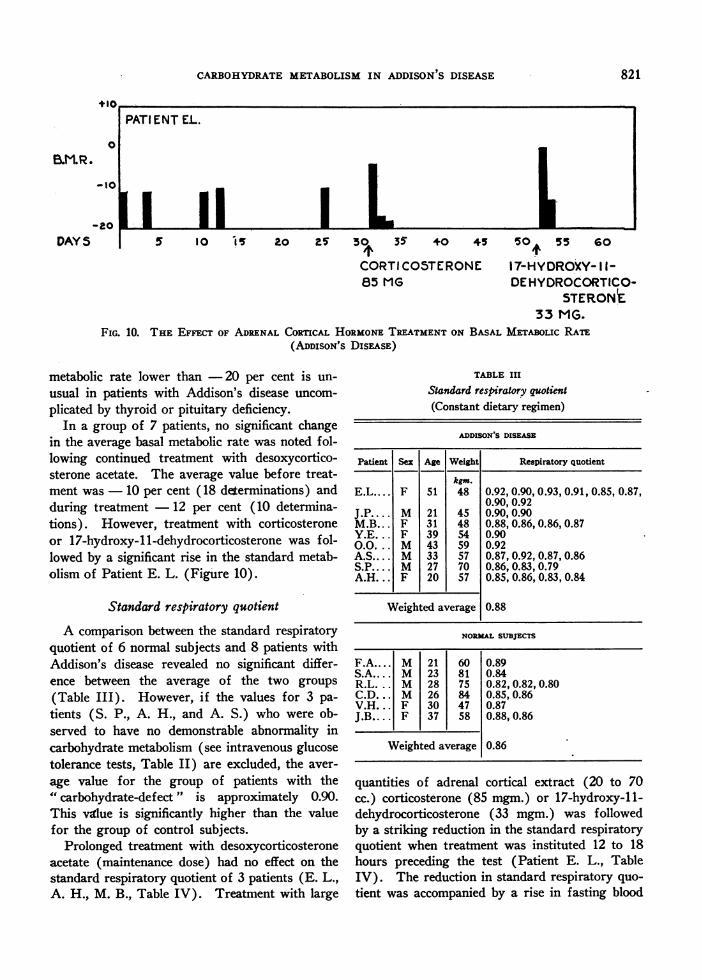
CORTICOSTERONE 17-lHYDROXY- I 1-85 MG DEHYDROCORTICO-
STERON£33 MG.
FIG. 10. THE EFFECT OF ADRENALCORTICAL HORMONETREATMENTON BASAL METABoLIc RATE(ADDISON's DIsEASE)
metabolic rate lower than -20 per cent is un-
usual in patients with Addison's disease uncom-
plicated by thyroid or pituitary deficiency.In a group of 7 patients, no significant change
in the average basal metabolic rate was noted fol-lowing continued treatment with desoxycortico-sterone acetate. The average value before treat-ment was 10 per cent (18 determinations) andduring treatment 12 per cent (10 determina-tions). However, treatment with corticosteroneor 17-hydroxy-11-dehydrocorticosterone was fol-lowed by a significant rise in the standard metab-olism of Patient E. L. (Figure 10).
Standard respiratory quotient
A comparison between the standard respiratoryquotient of 6 normal subjects and 8 patients withAddison's disease revealed no significant differ-ence between the average of the two groups
(Table III). However, if the values for 3 pa-
tients (S. P., A. H., and A. S.) who were ob-served to have no demonstrable abnormality incarbohydrate metabolism (see intravenous glucosetolerance tests, Table II) are excluded, the aver-
age value for the group of patients with the" carbohydrate-defect" is approximately 0.90.This value is significantly higher than the valuefor the group of control subjects.
Prolonged treatment with desoxycorticosteroneacetate (maintenance dose) had no effect on thestandard respiratory quotient of 3 patients (E. L.,A. H., M. B., Table IV). Treatment with large
TABLE III
Standard respiratory quotient(Constant dietary regimen)
ADDISON'S DISEASE
Patient Sex Age Weight Respiratory quotient
kgm.E.L.... F 51 48 0.92, 0.90, 0.93, 0.91, 0.85, 0.87,
0.90, 0.92J.P... M 21 45 0.90,0.90M.B.. . F 31 48 0.88, 0.86,0.86, 0.87Y.E... F 39 54 0.90O...O. M 43 59 0.92A.S... M 33 57 0.87, 0.92, 0.87, 0.86S.P. M 27 70 0.86, 0.83, 0.79A.H... F 20 57 0.85, 0.86, 0.83, 0.84
Weighted average 0.88
NORMLSUBJECTS
F.A.... M 21 60 0.89S.A.... M 23 81 0.84R.L... M 28 75 0.82, 0.82, 0.80C.D... M 26 84 0.85, 0.86V.H... F 30 47 0.87J.B.... F 37 58 0.88, 0.86
Weighted average 0.86
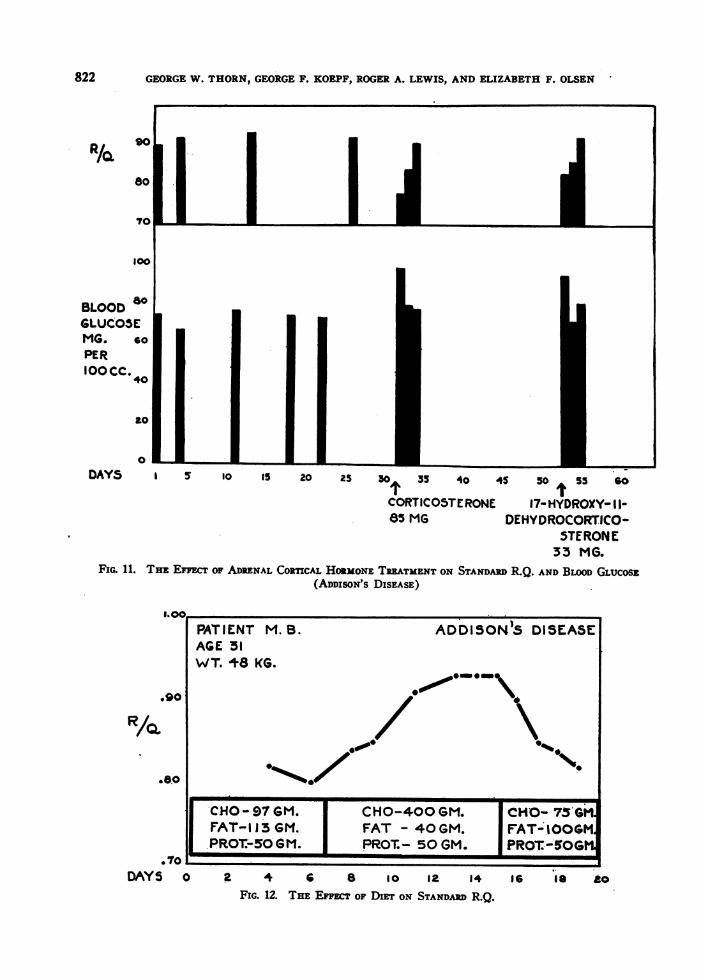
quantities of adrenal cortical extract (20 to 70cc.) corticosterone (85 mgm.) or 17-hydroxy-11-dehydrocorticosterone (33 mgm.) was followedby a striking reduction in the standard respiratoryquotient when treatment was instituted 12 to 18hours preceding the test (Patient E. L., TableIV). The reduction in standard respiratory quo-tient was accompanied by a rise in fasting blood
o
B.M.R.
-10l
DAYS
821
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
glucose (Figure 11). It is particularly significantthat 48 hours after treatment with these substanceshad been discontined the standard respiratory quo-
tient and the fasting blood glucose value hadreturned to the previous untreated level (Figure11 ). No ketonuria was observed during the shortperiod of treatment with adrenal cortical extract,corticosterone or 17-hydroxy-11-dehydrocortico-sterone. The possibility of ketonemia was notexcluded.
In another type of experiment the effect of dietwas observed on the standard respiratory quotientof normal subjects and patients with Addison'sdisease. An increase in the proportion of carbo-hydrate in the diet (protein and total caloriesbeing kept constant) resulted in a striking rise inthe standard respiratory quotient of untreated pa-
tients with Addison's disease (Patient M. B.,Figure 12) as well as in normal control subjects.
Respiratory quotient following the intravenousadministration of glucose
Because of the striking abnormality which was
observed in the intravenous glucose curve of pa-
tients with Addison's disease, it seemed desirableto follow closely the changes in respiratory me-
tabolism which occurred during this test. Therespiratory quotient, total urinary nitrogen excre-
tion and blood glucose values of 4 normal subjectsand 5 patients with Addison's disease were fol-lowed during the standard intravenous glucosetolerance test (Table V). The respiratory quo-tient rose to 0.90 or above in only one of the 4normal subjects, whereas it exceeded 0.90 in all
5 of the patients with Addison's disease. Particu-larly noteworthy was the sudden and striking fallin respiratory quotient in Patients E. L., J. P.,and M. B., as marked hypoglycemic symptoms be-
TABLE V
Changes in respiratory quotient, urinary nitrogen andblood glucose following the intravenous administration ofglucose
* Total urinary nitrogen, expressed as grams per hour.t Blood glucose expressed as mgm. per 100 cc.
came manifest. It is obvious that determinationsof respiratory quotient made at this time are sub-ject to error, but the fact that all 3 of the patientshad such sudden and striking changes in the samedirection may be of some significance.
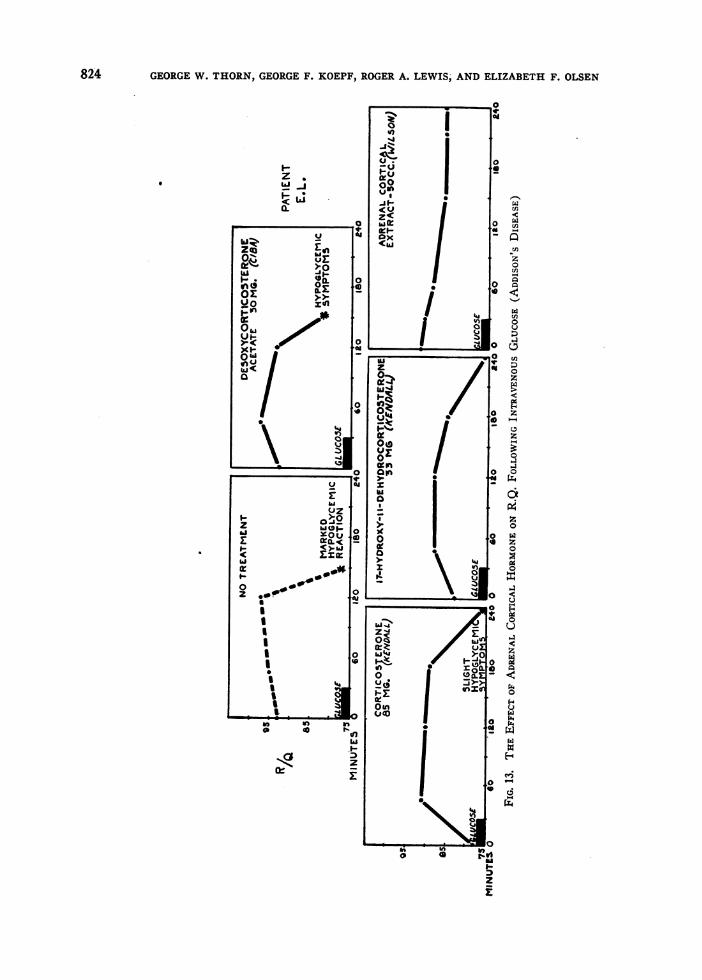
The effect of treatment with large quantitiesof adrenal cortical extract (Wilson's 50 to 70cc.), crystalline desoxycorticosterone acetate (30mgm.), corticosterone (85 mgm.) and 17-hy-droxy-11-dehydrocorticosterone (33 mgm.) onthe respiratory quotient of Patient E. L., is re-corded in Figure 13. Continued treatment withmaintenance doses of desoxycorticosterone acetateor treatment immediately beforehand with a mod-
823
824 GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS; ANDELIZABETH F. OLSEN
0
0u
ze r
z<
w(t ~~~~0X o
ge >.0 0~~~~~~~~01
0/~~~oz >>-- 0
0~~~~~~~~~~~
o -~~~~~~~~~oz 0o*M4 Li(IC
0~~~~~
S '4 ~~~~~~~%0
5 ~~00* 0~~~
It
uz
i
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
INITIAL / HOUR 2 HOUR5
s~t0;>Q s
CONTROLNOTRfATtM1ENT
DESOXYCORT/CO5ERONEACETATE 30 MG.
CORTICOSTERONE85 MG.
/7-IYDROXY -//-OL/9YOROCOPT/CO-
5TERONE33 IVG.
ADRENAL CORTiCAL.XTRACT 50 CC.
3HOUR5 1 HOURS
HYPOGLYCEMICREACTION
HYPOGLYCEM/C- 5YtMPTOMS
jb
FIG. 14: ADDISON'S DISEASL E. L. CALORIC CHANGESFOLLOWINGINTRAVENOUS GLUCOSE
erately large dose of this compound (30 mgm.)was not associated with any change in the re-
spiratory quotient. Treatment with 50 cc. ofadrenal cortical extract, injected 4 to 6 hoursprevious to the test, did not affect the initialstandard respiratory quotient but was associatedwith a marked change in the subsequent respira-tory quotient values (Figure 13, Patient E. L.).In another experiment (Figure 11) it was ob-served that treatment with 50 to 70 cc. of adrenalcortical extract during a 12- to 24-hour periodpreceding the test significantly affected the initialrespiratory quotient. Treatment with corticoster-one and with 17-hydroxy-11-dehydrocorticoster-one (dissolved in oil and injected intramuscularlyduring a 12-hour period prior to the standard in-travenous glucose tolerance test) was followed bya marked reduction in initial standard respiratory
quotient, as well as in the values following theintravenous glucose tolerance test (Figure 13).
Differential derivation of calories (Lusk's ta-ble) indicated that in the untreated state (PatientE. L., Figure 14) a high proportion of calorieswas derived from carbohydrate oxidation follow-ing the intravenous administration of glucose,particularly during the second hour of the test.During the third hour of the test, in the untreatedpatient, there was a sudden reduction in the pro-portion of calories derived from carbohydrate(low R/Q) immediately preceding the onset ofmarked symptoms of hypoglycemia. Treatmentwith desoxycorticosterone acetate had no effect onthese changes. Treatment with adrenal corticalextract, 17-hydroxy-11-dehydrocorticosterone andcorticosterone (in order of potency) was followedby a significant reduction in the proportion of
825
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
MINUTLS 0 60 I1O 160 240 300 360
FIG. 15. EFFECT OF ADRENALCORTICAL HORMONETHERAPYON URINARY EXCRETION OF NITROGEN DURINGSTANDARDINTRAVENOUSGLUCOSETOLERANCETEST
calories derived from carbohydrate during theinitial periods of the test (first and second hours).During the third and fourth hours of the test, fol-lowing treatment with these three substances,there was an increase in the proportion of caloriesderived from carbohydrate and protein. The in-crease in calories derived from protein was par-ticularly striking following adrenal cortical ex-
tract therapy.The excellent clinical condition of patient E. L.
at the termination of the intravenous glucosetolerance test following treatment with adrenalcortical extract and 17-hydroxy-11-dehydrocorti-costerone warrants mention (see Figure 6). Fur-thermore, it is significant that signs and symptomsof hypoglycemia did not become manifest duringtreatment with these substances although the bloodglucose, on some occasions, was reduced to the
level at which signs and symptoms had appeared inthe untreated state.
Urinary nitrogen excretionThe rise in urinary nitrogen excretion which
was observed during the standard intravenous
TABLE VI
Total urinary nitrog,en excretion (grams per hour) duringstandard intravenous glucose tokrance test
Fsig 1 2 3 4Fasting hour hours hours hours
4 Control subjects... 0.40 0.58 0.63 0.66 0.564 Patients with Addi-
son's disease ...... 0.36 0.45 0.35 0.29 0.35
glucose tolerance test was greater and more sus-tained in control subjects than in patients withAddison's disease (Table VI). In Patient E. L.
0 1-
826
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
(Figure 15), treatment with 17-hydroxy-11-de-hydrocorticosterone and with adrenal cortical ex-tract was followed by a striking rise in the urinaryexcretion of nitrogen during the intravenous glu-cose tolerance test. Treatment with desoxycorti-costerone acetate was without effect, and treat-ment with corticosterone was followed by achange, intermediate between that of desoxycorti-costerone acetate and 17-hydroxy-11-dehydro-corticosterone (Figure 15). It is of interest tonote that the greatest increases in urinary nitrogenexcretion followed treatment with those adrenalcortical hormone preparations which had previ-ously been shown to be the most potent in regu-lating carbohydrate metabolism. It is possible,however, that the changes in the renal excretionof nitrogen following hormone treatment may bedue in part to changes in renal " function."
Prolonged fast
Prolonged fasting was associated with a de-crease in blood glucose, respiratory quotient andurinary nitrogen excretion (Patient M. B., Fig-ure 16). Treatment with adrenal cortical extractwas followed by a rise in blood glucose, a furtherdecrease in respiratory quotient, and an increasein urinary nitrogen excretion.
It would appear that the efficacy of adrenalcortical hormone therapy in raising the blood glu-cose level during fasting was the result of in-creased glycogenesis without an equivalent in-crease in glucose utilization.
Necessity for adequate carbohydrate in diet
Studies (M. B., Figure 12) indicate that pa-tients with Addison's disease can utilize the read-ily available carbohydrate contained in their diet.It has been suggested (9, 12) that patients withAddison's disease should be provided with a diethigh in readily available carbohydrate, if hypo-glycemia is to be avoided. A diet high in carbo-hydrate would appear to be essential for the suc-cessful treatment of Addison's disease, at leastuntil treatment with hormone possessing carbohy-drate-regulating property is available at a costwhich most patients can afford.
The striking inability of these patients to derivesufficient carbohydrate from endogenous and ex-ogenous non-carbohydrate sources was vividly
BLOODGLUCOSEMGPelt100 CC.
URINARYWITROGEN
GM.PER 2HOUR
B. ---UNTREATEDADD1OWNS EXTRACT SOCC.
90aS
so
70
80 *70.
10 ___________
0
HRS.OFFAST 15 I. to 2*
FIG. 16. PROLONGEDFAST
demonstrated by the course of events which oc-curred when Patient J. P., under carefully con-trolled conditions, was fed a diet low in carbo-hydrate. The composition of the diet was asfollows:
Throughout this study the patient received treat-ment with desoxycorticosterone acetate. On theevening of the third day, one hour after theingestion of tea and cream, a severe hypoglycemicreaction occurred. This was characterized bydeep respiration, profuse perspiration, hunger,
827
I
4
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
weakness and nervousness progressing rapidly tomarked mental confusion. The following dataobtained at this time indicated that the reactionwas specifically related to a disturbance in carbo-hydrate metabolism and not to a loss of sodium,chloride and water with subsequent dehydration:
1. No appreciable loss in body weight duringthe 3 days of the experiment.
2. Rapid recovery following intravenous glu-cose therapy without additional sodium chloride oradrenal cortical hormone therapy.
3. Hypoglycemia (55 mgrm.) was associatedwith a normal concentration of sodium and chlo-ride in the blood with evidence of only slighthemoconcentration: serum sodium 140 m.eq., chlo-ride 101.4 m.eq., and potassium 6.1 m.eq., perliter; carbon dioxide combining power 49 volumesper cent; non-protein nitrogen 27 mgm. per 100cc. The urine contained acetone bodies 4 +.
The slightly higher-than-normal serum potas-sium value may be of some significance in asso-ciation with the low blood glucose level (13).
Thus within a period of 72 hours, during whichhe received a diet of adequate caloric content, andduring a period in which blood pressure, plasmavolume and electrolyte balance were maintained bymeans of desoxycorticosterone acetate treatment,this patient developed a severe hypoglycemic re-action. This study demonstrates the decreasedglycogenesis which is associated with Addison'sdisease, as well as the inability of desoxycortico-sterone acetate treatment to increase the forma-tion of glucose from non-carbohydrate sources.
Hypoglycemia precipitated by intercurrentinfections
Acute respiratory infections and gastro-enteritisconstitute the most frequent complications whichprecipitate hypoglycemia in patients with Addi-son's disease. If not recognized and treated thiscomplication may result in a fatal outcome.
In the absence of complications, treatment withdesoxycorticosterone acetate maintained a majorityof patients with Addison's disease (12) in goodclinical condition without supplementary treat-ment with specific carbohydrate-regulating factor.The frequent ingestion of food provided an ade-
quate supply of readily available carbohydrate.However, when this source of supply was re-stricted (fasting, nausea, vomiting), or when thedemand for carbohydrate was increased (fever,infection), the blood glucose level rapidly declinedand severe hypoglycemic symptoms appeared de-spite adequate desoxycorticosterone acetate ther-apy. The reasons for the rapid onset of hypo-glycemia in these patients appeared to be two-fold:(a) oxidation of carbohydrate which rapidly de-pleted available stores; and (b) inability to formadequate quantities of carbohydrate from non-glucose sources.
At present the only form of specific hormonetherapy possessing carbohydrate-regulating factorwhich is available commercially is adrenal corticalextract. This must be used in large doses, 20 to50 cc. daily, in the presence of severe infection.In addition, it is desirable to provide carbohydrateby parenteral administration of glucose solutions,if patients are unable to take adequate quantitiesof fruit juice, lactose, gingerale, etc., by mouth.
Lactic acid
Because of the position of lactic acid as a transi-tion substance between protein and glycogen, andits importance in glucose oxidation, it seemed de-sirable to study its glycogenic action in patientswith Addison's disease and in adrenalectomizedanimals.
In Patient 0. 0. treatment with lactic acid (18grams of racemic lactic acid administered intrave-nously as the sodium salt dissolved in 1000 cc. ofwater) failed to alleviate the symptoms of hypo-glycemia which were initiated by the standardintravenous glucose tolerance test. Glucose ad-ministered intravenously 1 hour after the lactatesolution had been started promptly corrected thehypoglycemia. These observations on patientswere confirmed by experiments on adrenalecto-mized dogs (14) in which d-lactic acid adminis-tered intravenously failed to prevent the convul-sions induced by insulin, whereas treatment withglucose completely prevented signs of hypogly-cemia. Direct evidence of the diminished abilityof untreated adrenalectomized animals to convertlactic acid to glucose has also been obtained inphlorhizinized adrenalectomized rats (14).
828
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
Physiological actizity of steroid compoundsobtained from the adrenal cortex
To date numerous crystalline compounds havebeen isolated from adrenal cortical extracts. Inthe present study we have compared the effect ofthree of these compounds on carbohydrate metabo-lism in man. Desoxycorticosterone, which ap-pears to be the most active adrenal cortical com-pound thus far isolated as measured by its abilityto maintain the life of adrenalectomized animals,is very potent in electrolyte-regulating property(9). It appeared from this study that desoxy-corticosterone treatment had little, if any, specificeffect on carbohydrate metabolism in man. Corti-costerone, a compound similar to desoxycortico-sterone, but with an additional hydroxyl group,probably at C11, had less electrolyte-regulatingproperty (15) than desoxycorticosterone, but itwas much more potent in its carbohydrate-regu-lating effect. Seventeen-hydroxy-ll-dehydrocorti-costerone was more potent in carbohydrate-regu-lating property than either corticosterone ordesoxycorticosterone, but appeared from animalexperiments to be much less effective than eitherof these compounds in regulating electrolyte bal-ance and in maintaining the life of adrenalec-tomized animals. Thus oxygenation of desoxy-corticosterone in positions 11 and 17 greatlyincreased carbohydrate-regulating potency but atthe same time greatly decreased electrolyte-regu-lating and life-maintaining properties.
Potent adrenal cortical extracts appeared tocontain appreciable quantities of both electrolyteand carbohydrate-regulating factors. However,in man, relatively large quantities of extract mustbe given to demonstrate either effect. Doctor E.C. Kendall of the Mayo Clinic kindly supplieddata regarding the approximate steroid content ofWilson's adrenal extract (50 cc. contains approxi-mately 3 mgm. corticosterone, 3 mgm. dehydrocor-ticosterone, 3 mgm. 17-hydroxy-11-dehydrocorti-costerone, 1 mgm. 17-hydroxycorticosterone, aswell as unidentified substances). Our experi-ments suggest that the carbohydrate-regulatingpotency of this extract (50 cc. being as effectiveas 85 mgm. of corticosterone or 33 mgm. of17-hydroxy-11-dehydrocorticosterone) is muchgreater than can be explained by its content ofthese two constituents.
DISCUSSION
A comparison between the oral and intravenousglucose tolerance curves indicates that the so-called " flat-curve " following orally administeredglucose actually represents delayed or poor ab-sorption of glucose. Similar changes have beenobserved in a patient with idiopathic steatorrhea(non-tropical sprue). It appears from thesestudies that a " flat-curve " following orally ad-ministered glucose is of little diagnostic signifi-cance.
The striking hypoglycemia which occurs inmany patients with Addison's disease followingthe standard intravenous glucose tolerance test isof great clinical significance since it implies theexistence of a marked disturbance in carbohydratemetabolism. The test is of considerable aid indiagnosis, although it is not specific. Its greatestusefulness lies in the ease with which it permitsa disturbance in carbohydrate metabolism to bedetected. The changes which were observed inpatients following intravenous glucose adminis-tration were in many ways similar to the changesobserved by Kendall et al (13) in adrenalecto-mized dogs. A comparison between intravenousglucose tolerance curves performed before andafter specific hormone therapy indicates that withadequate treatment there is a marked increase inthe threshold at which severe hypoglycemic symp-toms occur. Thus the adequately treated patientwith Addison's disease and the normal subjectfrequently do not manifest symptoms at a bloodglucose level which may be associated with markedsigns and symptoms of hypoglycemia in the un-treated patient. The exact mechanism for thisdifference in threshold is not known at present.Its clinical significance, however, is apparent.
The increase in fasting blood glucose level whichwas observed following the administration ofcrystalline corticosterone and 17-hydroxy-1 1-de-hydrocorticosterone precludes the inference thata rise in blood glucose following adrenal corticalhormone therapy is necessarily due to contaminat-ing substances, viz., epinephrin.
The increased height to which the blood glucoselevel rose, and the glycosuria which was observedfollowing specific hormone therapy in PatientE. L. (Figure 6), substantiate the studies ofLukens (16) and others regarding the nature of
829
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
the diabetes in patients with adrenal cortical hy-perfunction (tumor and hyperplasia).
Preliminary studies on lactic acid metabolismindicate that the ability of patients with Addison'sdisease to form glucose from this substance isgreatly impaired. These studies have -been con-firmed experimentally in phlorhizinized rats and,in addition, it appears that the formation of glu-cose from pyruvate and from glycogenic aminoacids is also impaired (14). Treatment with po-tent adrenal cortical hormone restores to normalthe capacity of these animals to form glucosefrom lactic acid, pyruvate and glycogenic aminoacids.
It is suggested that in adrenal cortical insuffi-ciency carbohydrate oxidation is adequate, al-though the ability to form glucose and glycogenfrom intermediate products of carbohydrate andprotein metabolism is impaired. As a result, theglycogen depots in the body are soon exhausted,and ingested preformed carbohydrate is requiredto maintain the blood glucose level and to providea readily available source of energy. Hormonetherapy increases the ability of the body to formglucose and glycogen from the intermediate prod-ucts of both carbohydrate and protein metabolismand apparently increases the proportion of caloriesderived from protein and fat.
SUMMARY
Some or all of the following abnormalities incarbohydrate metabolism were observed in a largeproportion of patients with Addison's disease:
1. A low-normal fasting blood glucose level.2. Striking hypoglycemia:
(a) Following the oral or intravenous ad-ministration of glucose
(b) Following a 24-hour fast(c) During fever or infections(d) On a diet high in fat and low in car-
bohydrate.3. Decreased threshold at which hypoglycemic
symptoms appeared.4. Flat type of oral glucose tolerance curve.5. Absence of "rebound" in blood glucose
curve following the administration of intravenousglucose.
6. Decreased glycemic response to epinephrin.
7. High standard respiratory quotient.8. Increase over normal in respiratory quotient
following glucose administration.9. Low-normal basal metabolic rate.
With the exception of its effect on the oralglucose tolerance curve, the abnormalities in car-bohydrate metabolism were not significantly al-tered by desoxycorticosterone acetate (Ciba) ther-apy. Treatment with large quantities of adrenalcortical extract (Wilson, 50 cc.), 17-hydroxy-11-dehydrocorticosterone (Compound E, Kendall, 33mgm.), and corticosterone (85 mgm.), in orderof potency, was observed to
(a) Increase the fasting blood glucose level.(b) Decrease the standard respiratory quotient.(c) Increase the blood glucose level and renal
excretion of nitrogen and decrease the respiratoryquotient following the standard intravenous glu-cose tolerance test.
(d) Increase the threshold at which hypogly-cemic symptoms appeared.
(e) Increase the basal metabolic rate.
Treatment with adrenal cortical extract was alsoobserved to
(a) Increase the glycemic response to epineph-rin.
(b) Increase the fasting blood glucose levelduring fever and infections.
These experiments suggest that the adrenalcortical hormone has a direct action on carbohy-drate metabolism in man, and are in agreementwith the animal experiments reported by Long,Katzin and Fry (5). Our experimental data sug-gest that the adrenal cortical hormone increasesthe ability of the organism to form glucose andglycogen from intermediate products of both car-bohydrate and protein metabolism and in thismanner regulates the utilization of carbohydrate.
CONCLUSION
A high proportion of untreated patients withAddison's disease was observed to have a dis-turbed carbohydrate metabolism. This defectcould be most readily demonstrated by the appli-cation of a standard intravenous glucose tolerancetest. The abnormality in carbohydrate metabo-lism appeared to be specific since it persisted de-
830
CARBOHYDRATEMETABOLISM IN ADDISONS DISEASE
spite the correction of the disturbance in electro-lyte balance, plasma volume and blood pressure bymeans of desoxycorticosterone acetate therapy.Treatment with large quantities of adrenal cor-tical extract, 17-hydroxy-1 1-dehydrocorticosterone(Compound E) and corticosterone, in order ofpotency, corrected the abnormal carbohydratemetabolism.
PROTOCOL
E. L. (Number 193336), a 51-year-old single businesswoman, was admitted to The Johns Hopkins Hospitalon March 3, 1940, complaining of "weakness and sickstomach" for 6 months. She had first noticed loss ofstrength and weight in 1935 and since then had been trou-bled with spells of nausea. In November 1938 she hadhad an attack of bilateral bronchopneumonia, necessitat-ing hospitalization for 18 days. Since then she had neverrecovered her strength. While in the hospital a nurse hadcommented on the darkness of her skin and she herselfhad noted increasing pigmentation of the gums, nipples,abdomen and hands. She also had experienced spells ofhunger associated with nervousness and sweating whichwere relieved by food and she had developed the habit ofeating fruit or milk between breakfast and lunch. Onoccasions it was necessary for her to stop on her wayhome from work late in the afternoon for a sandwichbecause of extreme hunger.
Her father had suffered from chronic bronchitis andhad had an arrested pulmonary tuberculous lesion. Shehad had malaria in 1901, a partial thyroidectomy in 1914,and typhoid fever in 1919. In 1932 she had had anappendix drained and a subsequent repair of the incision.A cyst had been removed from the left breast in 1934.During the past two years her menstrual periods hadbecome irregular.
Physical examination on admission, March 3, 1940, re-vealed an undernourished middle-aged woman who ap-peared chronically ill. Her temperature was 99° F., pulserate 92 per minute, respirations 20 per minute and bloodpressure 86/70 mm. Hg. There was generalized darkbrown pigmentation of the skin, most marked over theelbows, hands, knees and in the axillary folds. Therewere many small black freckles and the areolae werealmost black in color. There was pigmentation of thegums and external genitalia. Some tortuosity of theretinal arteries was noted. The tonsils were small.There was a small amount of thyroid tissue palpable.The lungs were clear. The pulses were of poor volume.The heart was small and the sounds distant. The secondpulmonic sound was reduplicated and louder than theaortic second sound. There were no cardiac murmurs.No abdominal organs or masses were felt. Pelvic andrectal examination revealed no abnormality. The neuro-logical examination was normal.
The essential laboratory data were as follows:
Hemoglobin 80 per cent (12 grams), red blood cells 3.7million, hematocrit 33 per cent cells, white blood cells
6,000 with polymorphonuclears 58 per cent, eosinophiles4 per cent, monocytes 3 per cent and lymphocytes 35 percent, the sedimentation rate 29 mm. in one hour, cor-rected. The blood Wassermann was negative. Theblood non-protein nitrogen was 32 mgm. per 100 cc. andthe blood glucose 72 mgm. per 100 cc. On admission shewas given intravenous hypertonic sodium chloride. Thefollowing morning the serum carbon dioxide combiningpower was 52.2 volume per cent. Chloride was 1092m.eq. per liter, sodium 139 m.eq. per liter and potassium5.1 m.eq. per liter of serum.
The urine was found to have a specific gravity of1.010 and no albumin or sugar. There were no formedelements. Cultures were negative for acid fast bacilli.A phenolsulfonphthalein test showed a dye excretion of48 per cent in 2 hours.
X-rays revealed fibroid infiltration at the left apex, noadrenal calcification and a normal sella turcica. Thebasal metabolic rate was minus 15 per cent. Gastricanalysis showed no free hydrochloric acid until afterhistamine when it rose to 40°. The electrocardiogramwas normal. Venous pressure was 95 mm. of water.Circulation time with sodium cyanide was 18 secondsand with paraldehyde was 8 seconds. Tuberculin testswere negative at a dilution of 1 to 100,000 and 1 to10,000. Carbohydrate studies are recorded in the text.
Course. During the first month in hospital this patientwas maintained on supplementary sodium chloride ther-apy by mouth (10 grams) and frequent intravenous in-fusions of sodium chloride and glucose solution. On thisregimen she was unable to be up and about for morethan very brief periods. Her appetite was poor, herblood pressure 88/50 mm. of Hg, and her weight 44.0kgm. During her course of hospitalization she had onerather severe episode of vomiting and diarrhea, and inaddition an urinary tract infection. During these periodsshe was given desoxycorticosterone acetate and adrenalcortical extract. With the subsidence of the infectionthe patient was started on a regimen of 5 grams ofadded sodium chloride by mouth and a single daily intra-muscular injection of 4 mgm. of Percorten (desoxy-corticosterone acetate in oil). On this regimen herstrength improved, she gained 4 kgm. in weight and herblood pressure increased to a level of 130/85 mm. of Hg.On June 23, 1940, 8 pellets of crystalline desoxycortico-sterone acetate (125 mgm. each) were implanted in thesubcutaneous tissues of the left infrascapular region.The daily injections of Percorten were discontinued.The added sodium chloride therapy (5 grams daily) wasmaintained and the patient was discharged.
The authors wish to acknowledge the cooperation andassistance of Doctor Carlos Delbue and Miss MildredCaldwell, and the technical assistance of Mr. HarryEisenberg.
BIBLIOGRAPHY
1. Porges, O., Ueber Hypoglykamie bei Morbus Addi-son sowie bei nebennierenlosen Hunden. Ztschr. f.klin. Med., 1910, 69, 341.
831
GEORGEW. THORN, GEORGEF. KOEPF, ROGERA. LEWIS, ANDELIZABETH F. OLSEN
2. Eppinger, H., Falta, W., and Rudinger, C., Ueber dieWechselwirkung der Driisen mit innerer Sekretion.Ztschr. f. klin. Med., Berlin, 1908, 66, 380.
3. Maranion, G., Action de L'insuline dans L'insuffisanceSurrenale. Presse Med., 1925, 33, 1665.
4. Levy Simpson, S., Addison's disease and its treatmentby cortical extract. Quart. J. Med., 1932, 1, 99.
5. Long, C. N. H., Katzin, B., and Fry, E. G., Theadrenal cortex and carbohydrate metabolism. En-docrinology, 1940, 26, 309.
6. Lusk, G., Animal calorimetry; analysis of the oxida-tion of mixtures of carbohydrate and fat. A cor-rection. J. Biol. Chem., 1924, 59, 41.
7. Folin, O., and Malmros, H., An improved form ofFolin's micro method for blood sugar determina-tions. J. Biol. Chem., 1929, 83, 115.
8. Richter, C. P., and Eckert, J. F., Mineral metabolismof adrenalectomized rats studied by the appetitemethod. Endocrinology, 1938, 22, 214.
9. Thorn, G. W., Howard, R. P., and Emerson, K., Jr.,Treatment of Addison's disease with desoxycor-ticosterone acetate, a synthetic adrenal corticalhormone (preliminary report). J. Clin. Invest.,1939, 18, 449.
10. Ferrebee, J. W., Ragan, C., Atchley, D. W., andLoeb, R. F., Desoxycorticosterone esters; certaineffects in the treatment of Addison's disease. J.A. M. A., 1939, 113, 1725.
11. Rowntree, L. G., and Snell, A. M., A Clinical Studyof Addison's Disease. W. B. Saunders Company,Philadelphia, 1931.
12. Thorn, G. W., and Firor, W. M., Desoxycortico-sterone acetate therapy in Addison's disease: Clini-cal considerations. J. A. M. A., 1940, 114, 2517.
13. Kendall, E. C., Flock, E. V., Bollman, J. L., andMann, F. C., The influence of cortin and sodiumchloride on carbohydrate and mineral metabolismin adrenalectomized dogs. J. Biol. Chem., 1938,126, 697.
14. Lewis, R. A., Kuhlmann, D., Delbue, C. A., Koepf,G. F., and Thorn, G. W., Adrenal cortex andcarbohydrate metabolism. Endocrinology. (Inpress.)
15. Thorn, G. W., Engel, L. L., and Eisenberg, H., Theeffect of corticosterone and related compounds onthe renal excretion of electrolytes. J. Exper. Med.,1938, 68, 161.
16. Lukens, F. D. W., and Palmer, H. D., Adrenal corti-cal virilism. Endocrinology, 1940, 26, 941.