Not Only Chemotherapy Not Only Chemotherapy Anti-Tumor Vaccines for Anti-Tumor Vaccines for Tumor Eradication Tumor Eradication Irit Avivi Irit Avivi Department of Hematology and Department of Hematology and BMT BMT Rambam Medical Health Care Rambam Medical Health Care Campus Campus
Transcript
Not Only ChemotherapyNot Only Chemotherapy
Anti-Tumor Vaccines for Tumor Anti-Tumor Vaccines for Tumor EradicationEradication
Irit AviviIrit Avivi
Department of Hematology and BMTDepartment of Hematology and BMT
Rambam Medical Health Care CampusRambam Medical Health Care Campus
Haifa Haifa
Talk PlanTalk Plan The immune system in the healthy personThe immune system in the healthy person Why does the immune system fail to eradicate Why does the immune system fail to eradicate
cancer ?cancer ? Strategies to overcome this immunological Strategies to overcome this immunological
impairmentimpairment Vaccine studies in MyelomaVaccine studies in Myeloma Future directionsFuture directions
Current Approach to CancerCurrent Approach to Cancer Targeting tumor cellsTargeting tumor cells
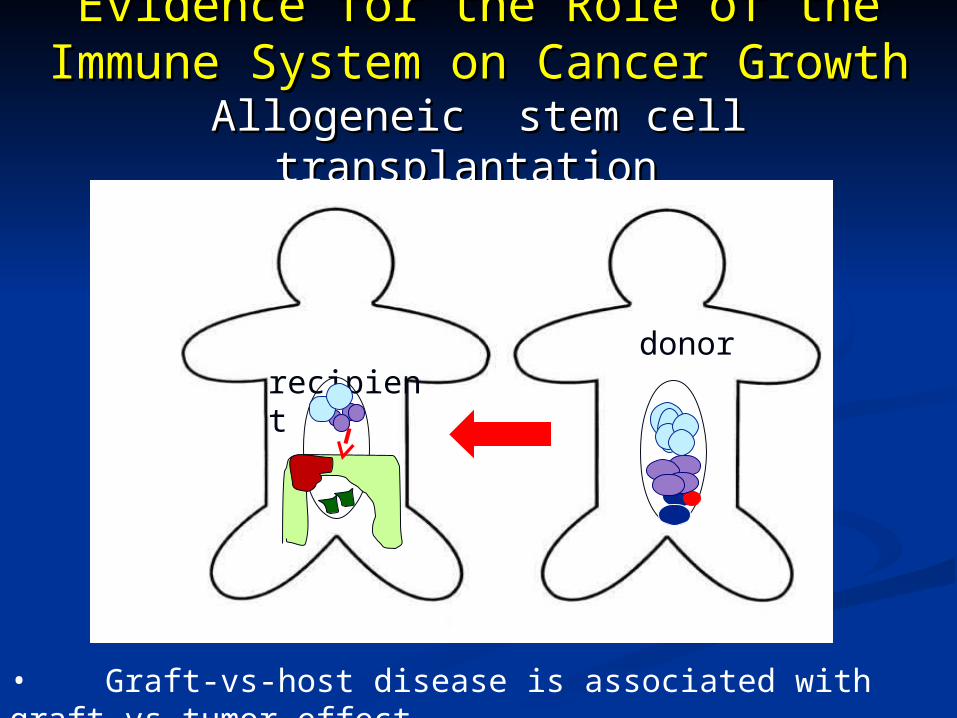
• Graft-vs-host disease is associated with graft vs tumor effect•
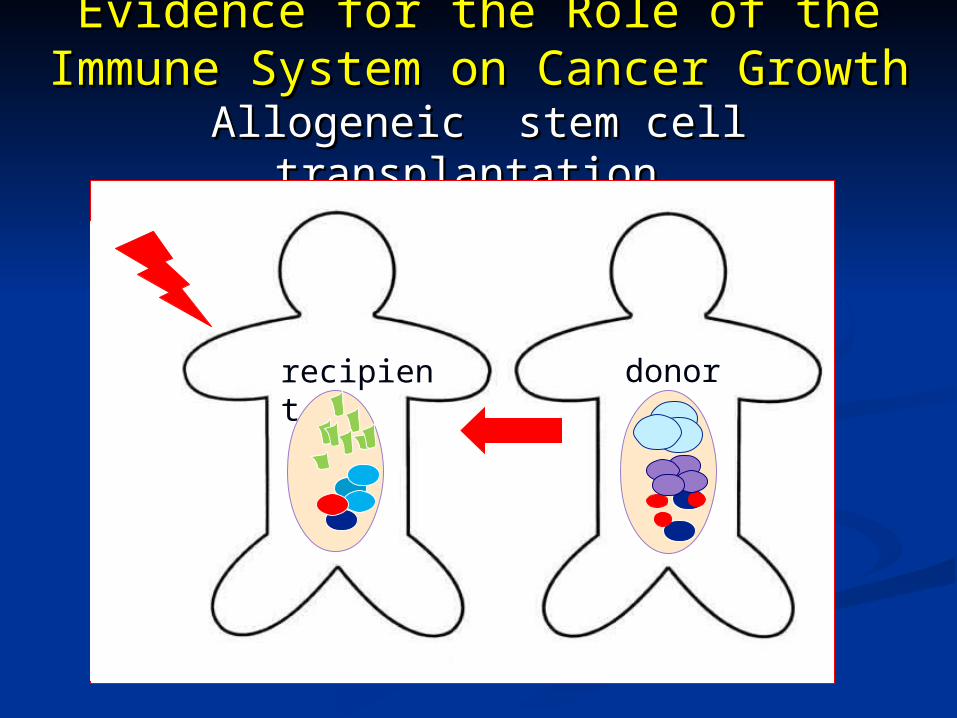
More Evidence for the Role of the More Evidence for the Role of the Immune System on Cancer GrowthImmune System on Cancer Growth
T cells & Antibodies directed against tumor cellsT cells & Antibodies directed against tumor cells
exist in the circulationexist in the circulation
HoweverHowever
Immune responses are ineffective in Immune responses are ineffective in
preventing disease establishment and progressionpreventing disease establishment and progression
Why ?Why ?
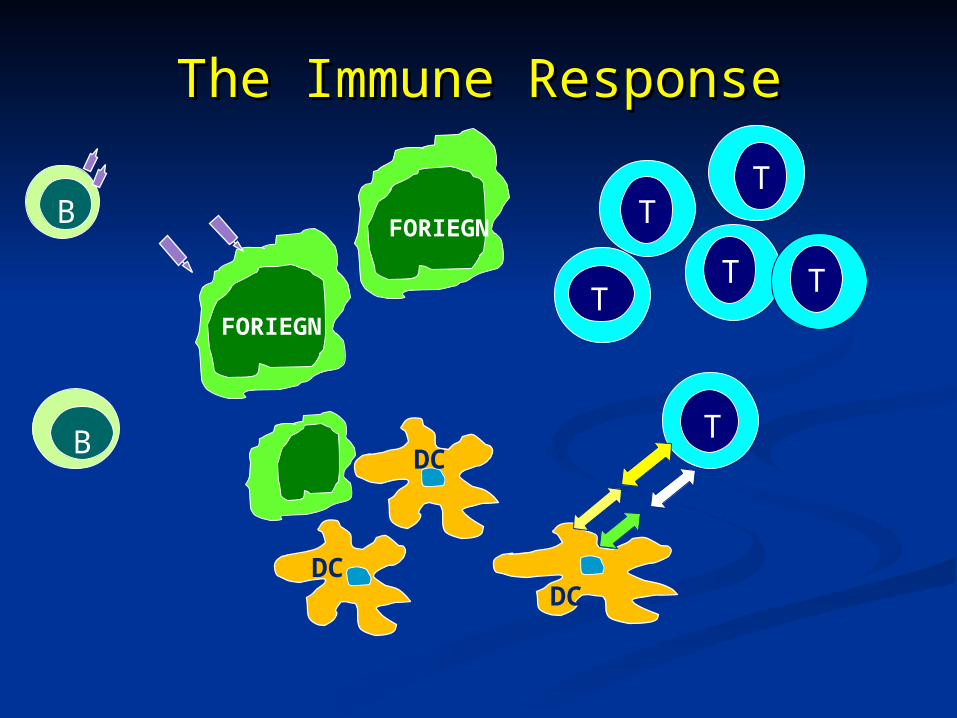
The Immune ResponseThe Immune Response
B
DC
DCDC
T
FORIEGN
B
T
FORIEGN
T
T
T T
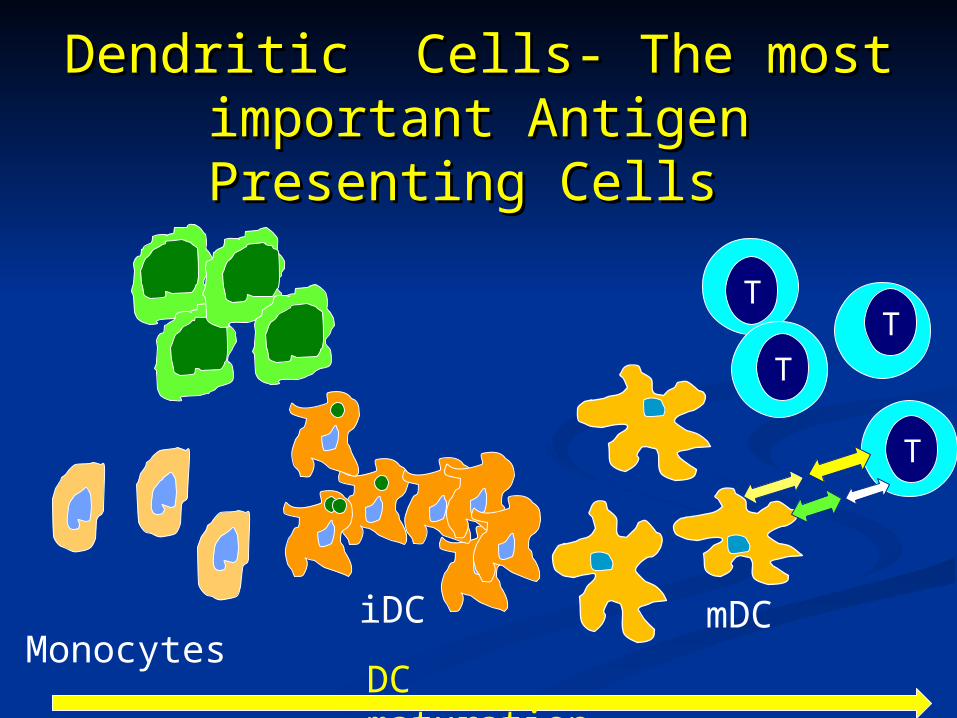
Dendritic Cells- The most Dendritic Cells- The most important Antigen Presenting Cells important Antigen Presenting Cells
T
T
T
T
DC maturation
iDC Monocytes mDC
Berzofsky et al JCI 2004
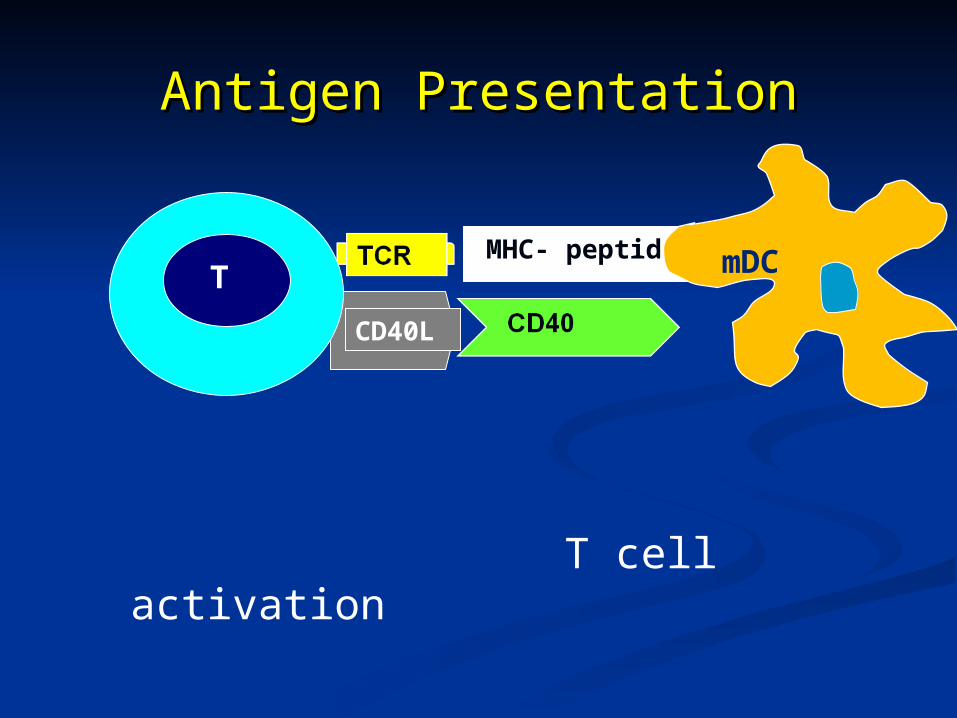
CD40L
MHC- peptide
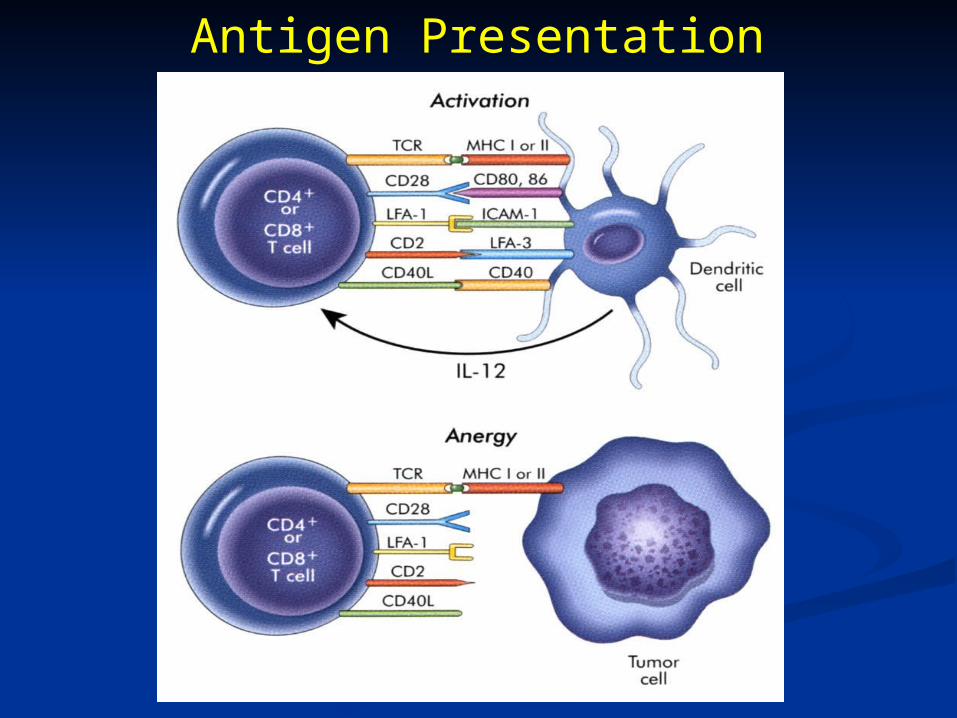
Antigen PresentationAntigen Presentation
mDCT
T cell activation
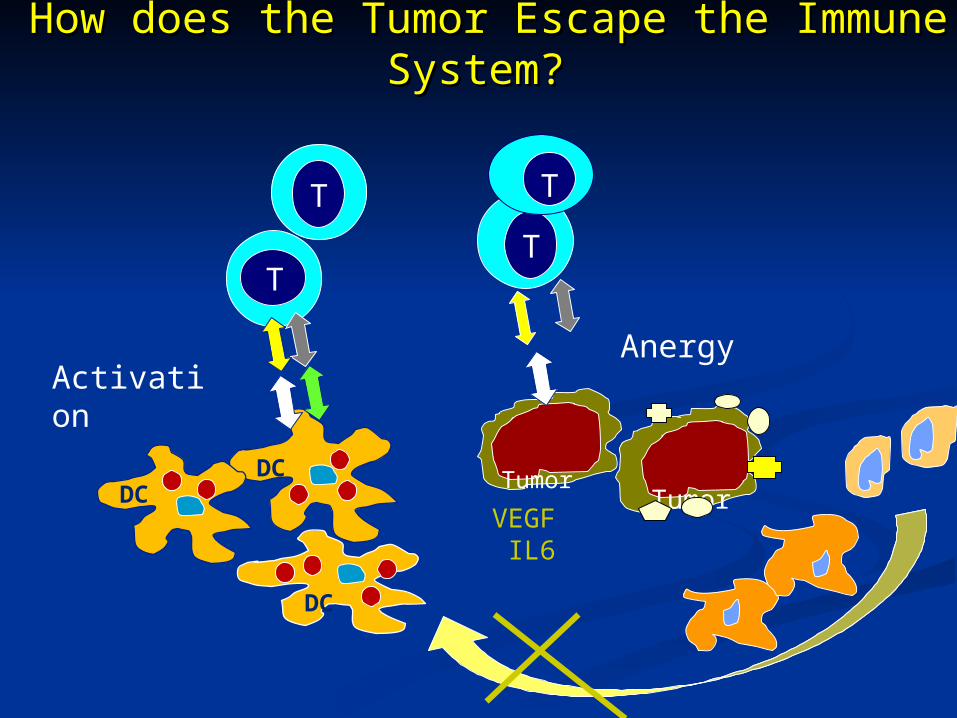
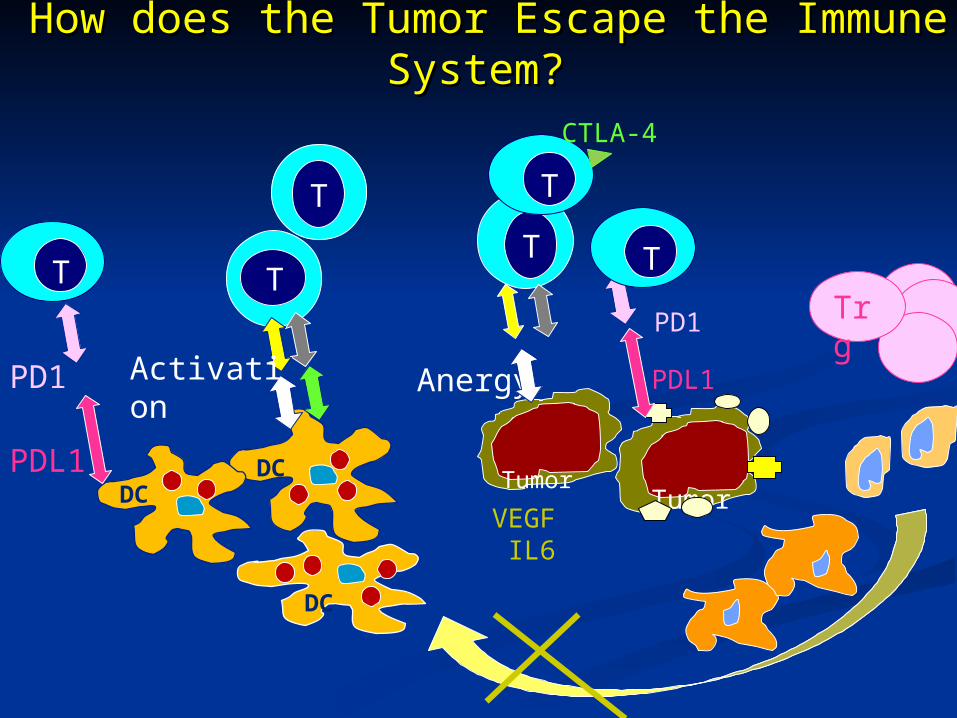
How does the Tumor Escape the Immune System?How does the Tumor Escape the Immune System?
DCDC
DC
T
TT
T
Tumor Tumor
ActivationAnergy
VEGF IL6
Antigen Presentation
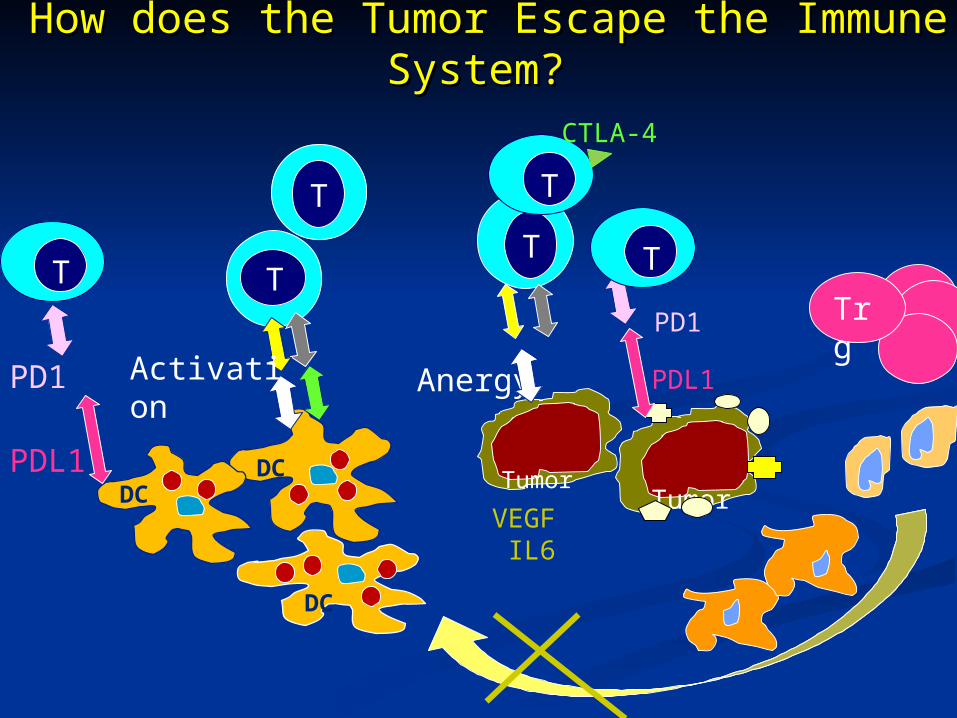
How does the Tumor Escape the Immune System?How does the Tumor Escape the Immune System?
DCDC
DC
T
TT
T
Tumor Tumor
Activation Anergy
VEGF IL6
CTLA-4
Trg
PDL1
PD1
PDL1
PD1
TT
How Does the Tumor Escape How Does the Tumor Escape the Immune System?the Immune System?
The tumor expresses Host AgsThe tumor expresses Host Ags
It impairs DC maturation and functionIt impairs DC maturation and function
Interferes with Antigen presentationInterferes with Antigen presentation
The tumor interacts with T cells AnergyThe tumor interacts with T cells Anergy
The tumor express inhibitory moleculesThe tumor express inhibitory molecules
The tumor induces accumulation of regulatory T cellsThe tumor induces accumulation of regulatory T cells
Strategies to Overcome Strategies to Overcome Tumor-Induced Immunological Defects Tumor-Induced Immunological Defects
Tumor escape OvercomingTumor escape Overcoming Host Ags Host Ags Tumor specific AgsTumor specific Ags
Immunogenic stimulatorsImmunogenic stimulators
Impaired DCs Maturation Impaired DCs Maturation Ex vivo DCs maturation Ex vivo DCs maturation
T cell Anergy T cell Anergy Interfere with Interfere with
mechanisms involvedmechanisms involved
in anergyin anergy
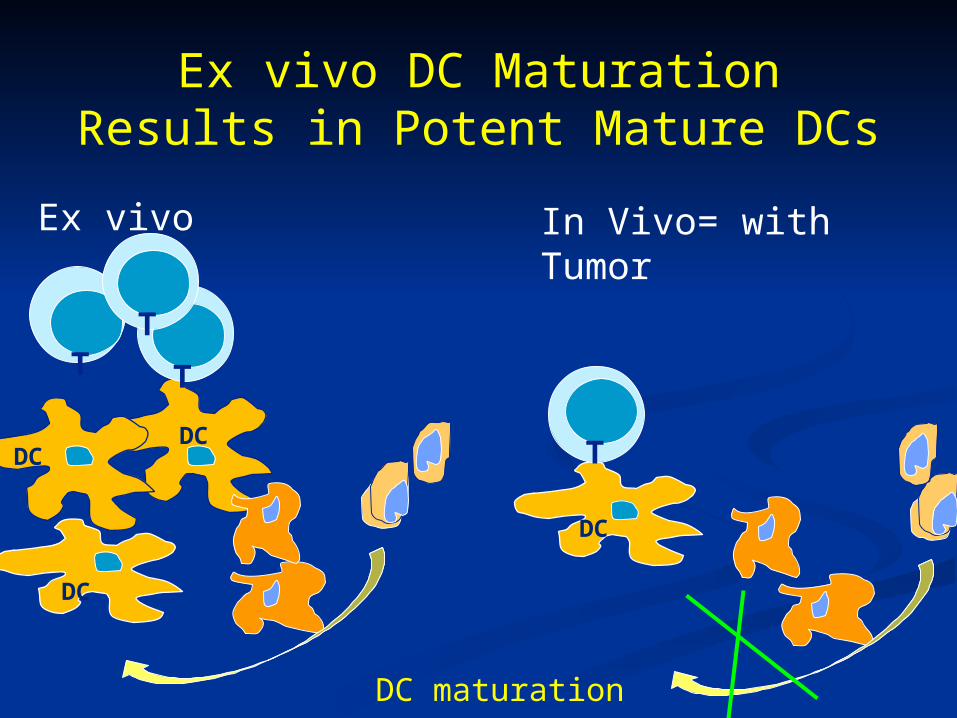
Ex vivo DC Maturation Results in Potent Mature DCs
DC
DC
DC
DC
T T
T
Ex vivo In Vivo= with Tumor
T
DC maturation
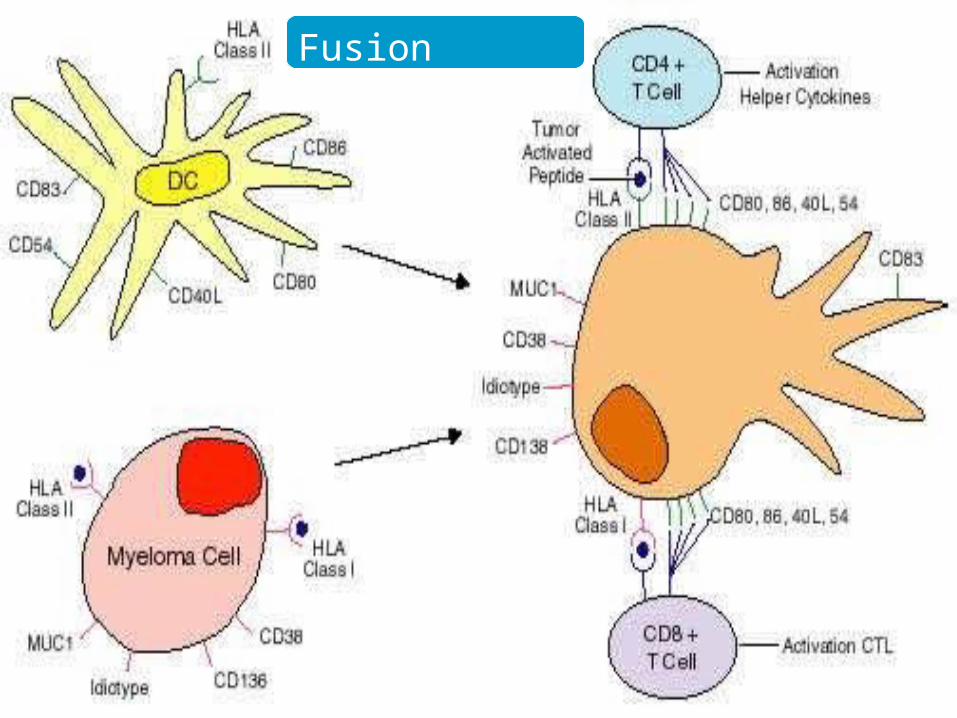
Strategies to Load Tumor Antigens onto DC
Tumor cell fusion
Loading of Tumor lysate
Loading of Tumor peptides
Individual Ag Whole Cell
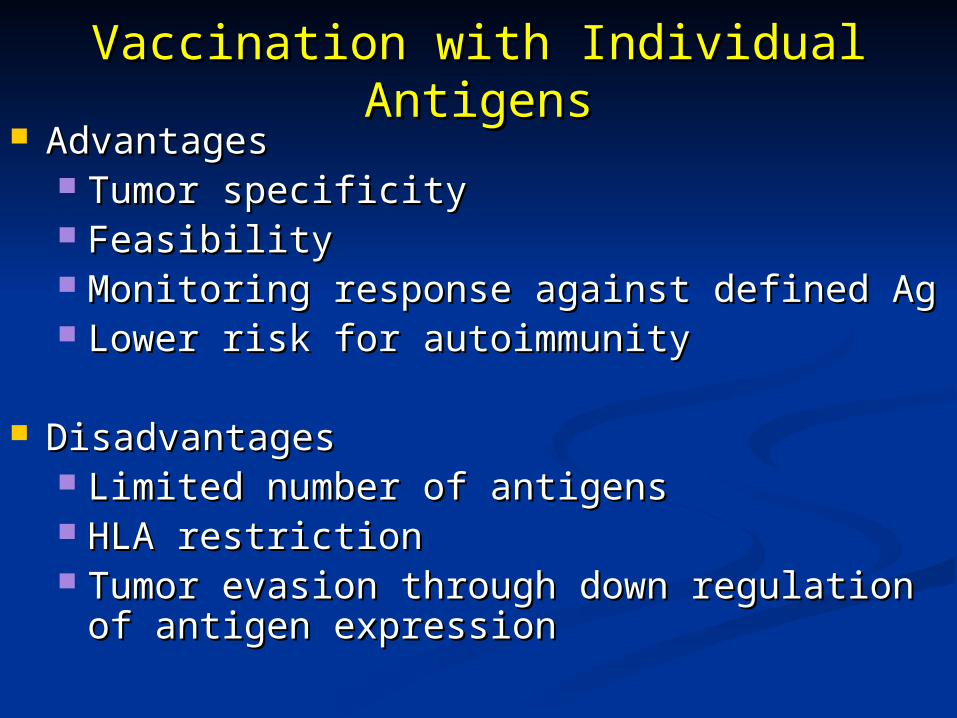
Vaccination with Individual AntigensVaccination with Individual Antigens AdvantagesAdvantages
Tumor specificityTumor specificity FeasibilityFeasibility Monitoring response against defined AgMonitoring response against defined Ag Lower risk for autoimmunityLower risk for autoimmunity
DisadvantagesDisadvantages Limited number of antigensLimited number of antigens HLA restrictionHLA restriction Tumor evasion through down regulation of antigen Tumor evasion through down regulation of antigen
expressionexpression
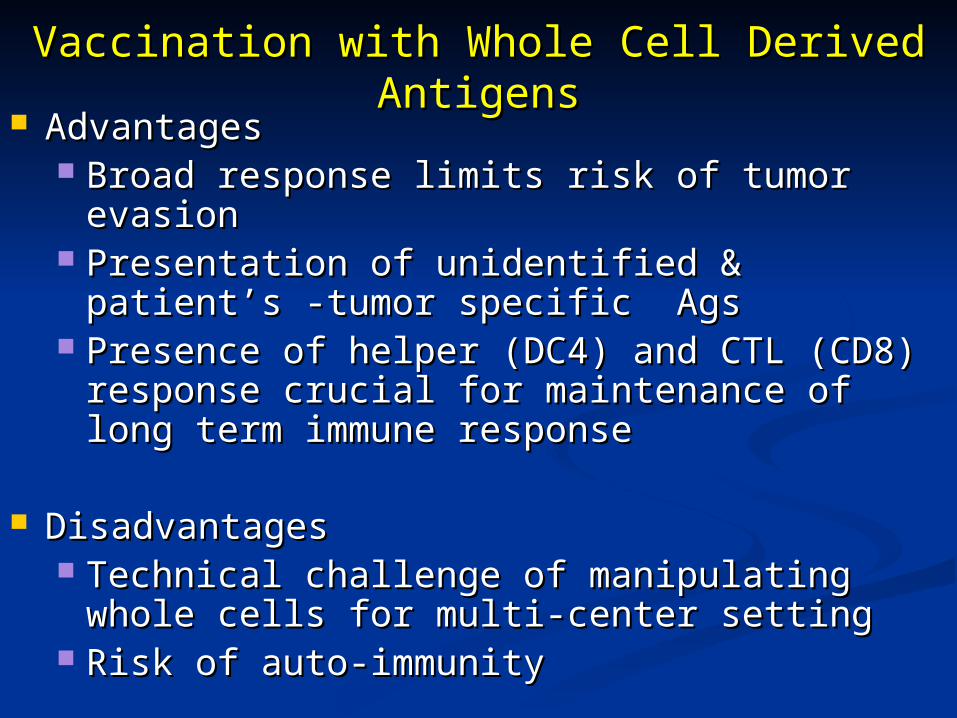
Vaccination with Whole Cell Derived AntigensVaccination with Whole Cell Derived Antigens AdvantagesAdvantages
Broad response limits risk of tumor evasionBroad response limits risk of tumor evasion Presentation of unidentified & patient’s -tumor Presentation of unidentified & patient’s -tumor
specific Agsspecific Ags Presence of helper (DC4) and CTL (CD8) Presence of helper (DC4) and CTL (CD8)
response crucial for maintenance of long term response crucial for maintenance of long term immune responseimmune response
DisadvantagesDisadvantages Technical challenge of manipulating whole cells for Technical challenge of manipulating whole cells for
multi-center settingmulti-center setting Risk of auto-immunityRisk of auto-immunity
Fusion Vaccines
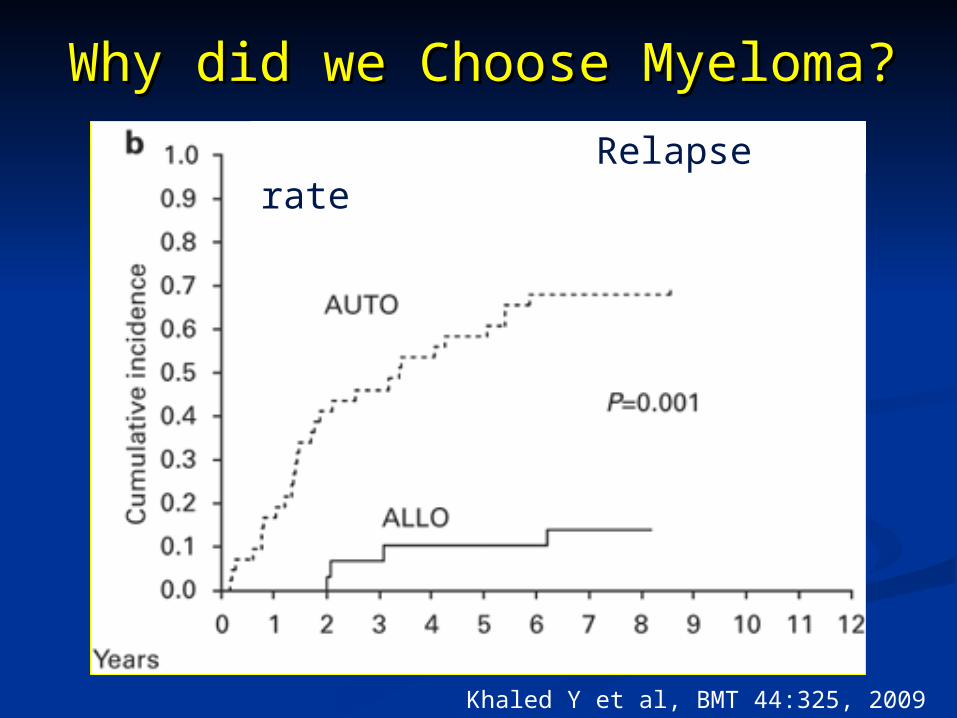
Why did we Choose Myeloma?Why did we Choose Myeloma?
““Vaccination” with Vaccination” with DC/MM Fusions DC/MM Fusions
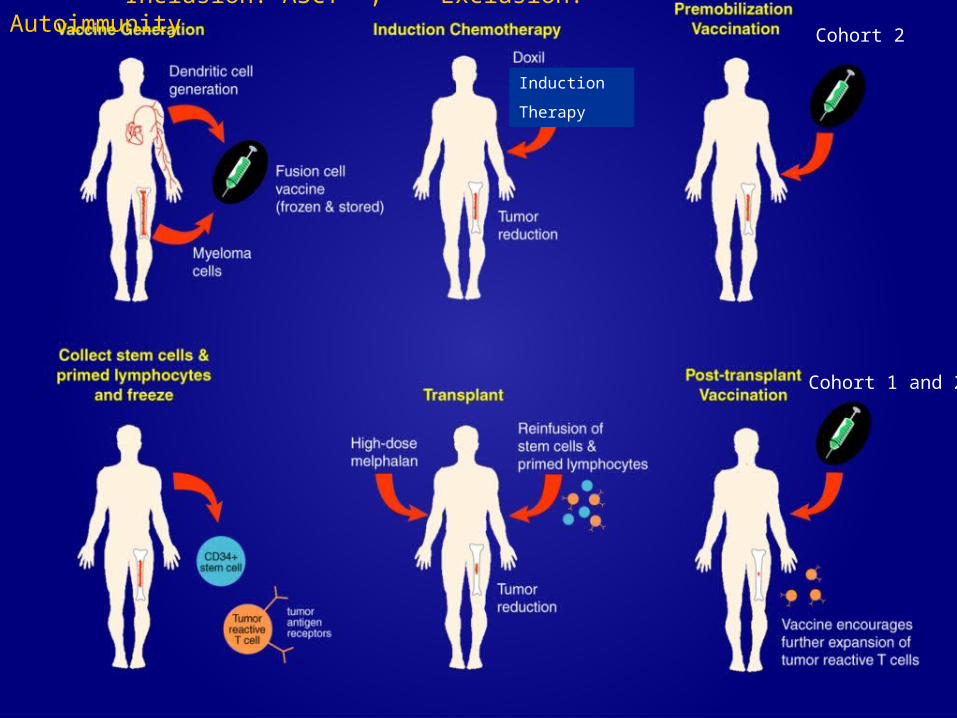
Vaccination with DC/MM Fusions: Vaccination with DC/MM Fusions: Trial DesignTrial Design
Phase I dose escalation trialPhase I dose escalation trial
EligibilityEligibility Patients with advanced stage myelomaPatients with advanced stage myeloma Presence of measurable diseasePresence of measurable disease > 20% plasma cells in bone marrow for > 20% plasma cells in bone marrow for
vaccine generationvaccine generation
Vaccination Schedule: Vaccination Schedule: 3 subcutaneous vaccinations in conjunction 3 subcutaneous vaccinations in conjunction
with GM-CSF administered every 3 weekswith GM-CSF administered every 3 weeks
Adherent PBMCs cultured for 5-7 days with GM-CSF & IL-4; TNF- added for 48-72 hours
Myeloma cells isolated
DCs assessed for DC & tumor specific markers
Myeloma cells assessed for tumor & DC specific markers
DC & myeloma fused with 50% PEG at DC: tumor, 3:1 to 10:1
Fusion cells quantified by measuring dual expression ofunique DC & tumor markers
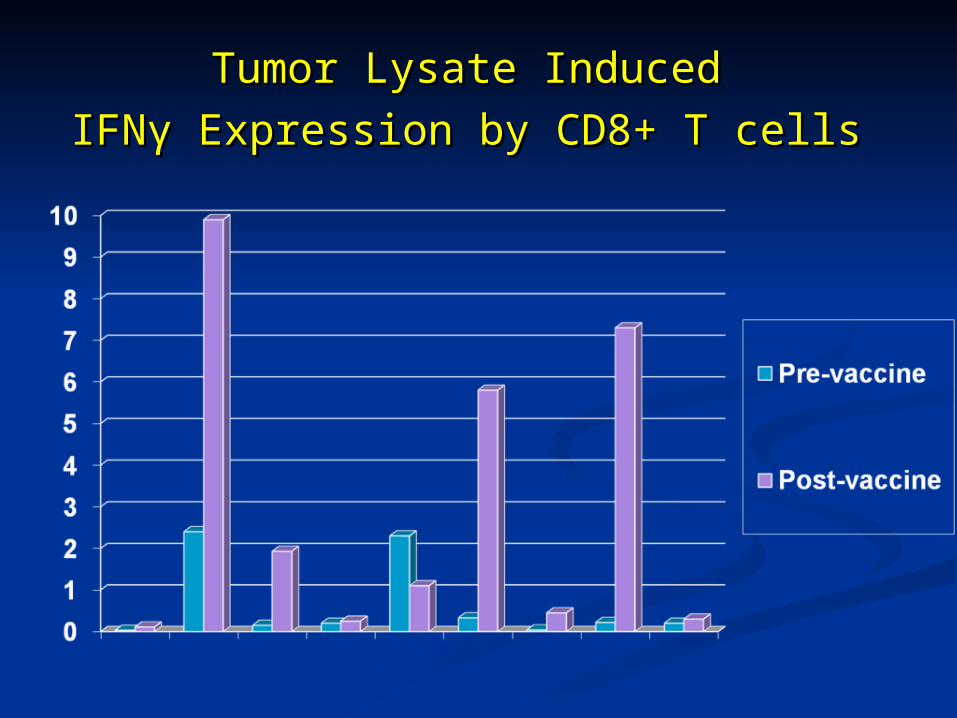
IFNIFNγγ Expression by CD8+ T cells Expression by CD8+ T cells
100 101 102 103 104
FL1-H
Pre-vaccination#3
55.8
10.8
100 101 102 103 104
FL1-H
1 month postvaccination
57
4.5
100 101 102 103 104
FL1-H
Pre-mobilization
51
1.78
100 101 102 103 104
FL1-H
Post-transplantation
72
4.1
IFN
CD8 FITC
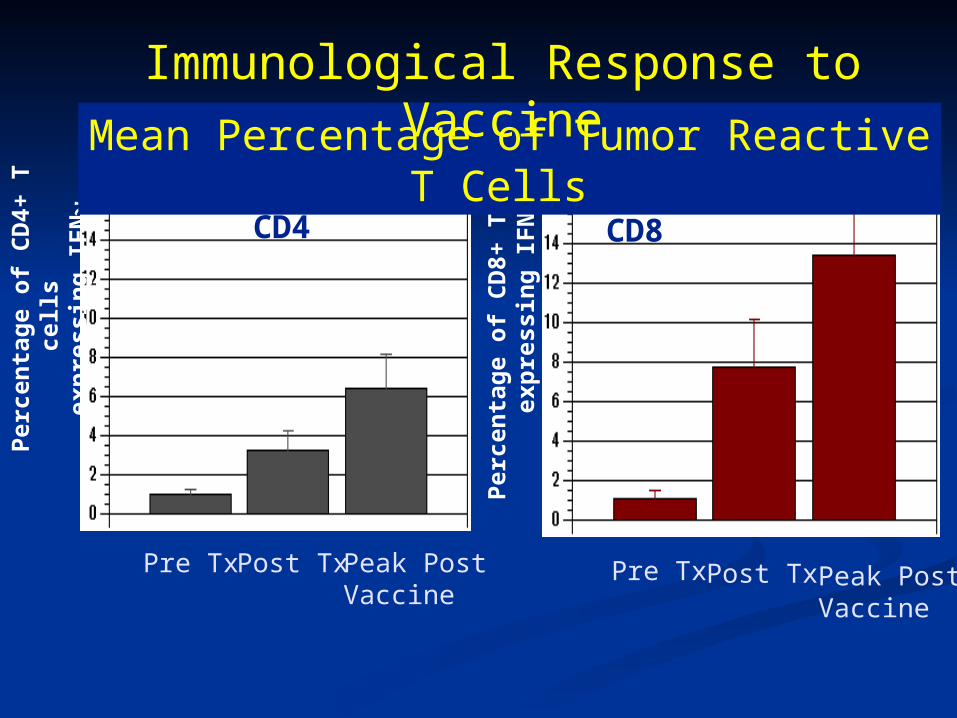
Vaccination Induced Immune Response
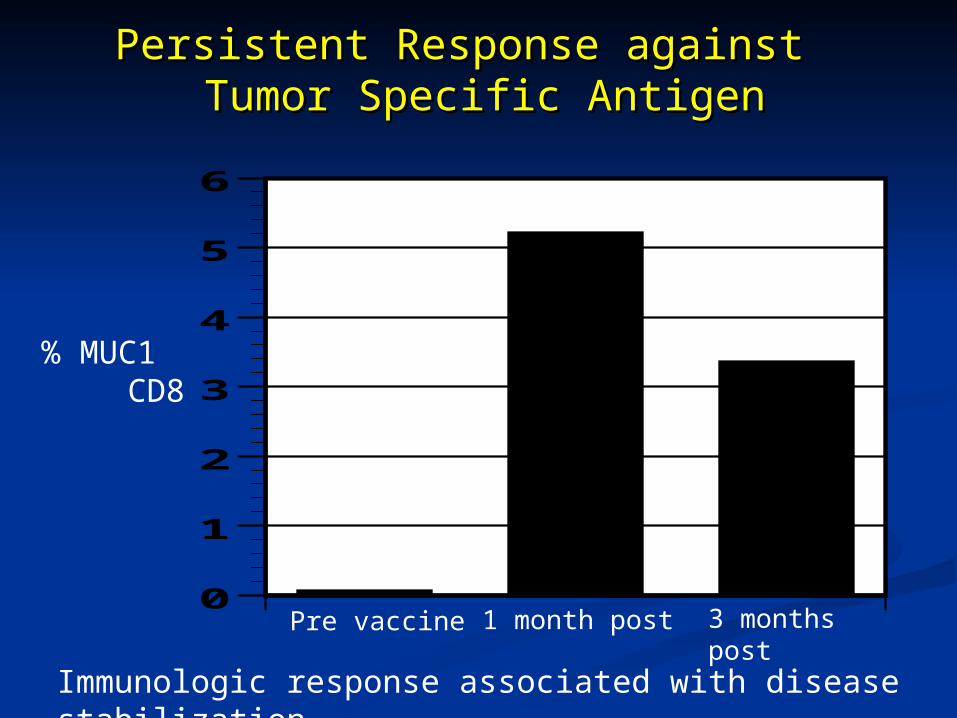
Persistent Response against Persistent Response against Tumor Specific Antigen Tumor Specific Antigen
0
1
2
3
4
5
6
% MUC1 CD8
Pre vaccine 1 month post 3 months post
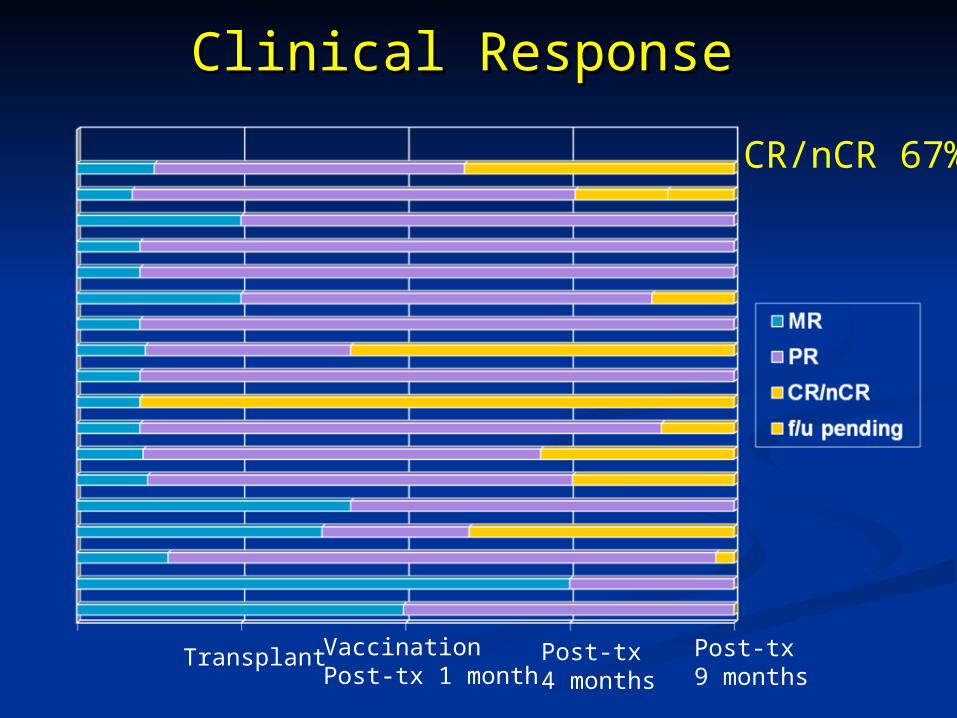
Immunologic response associated with disease stabilization
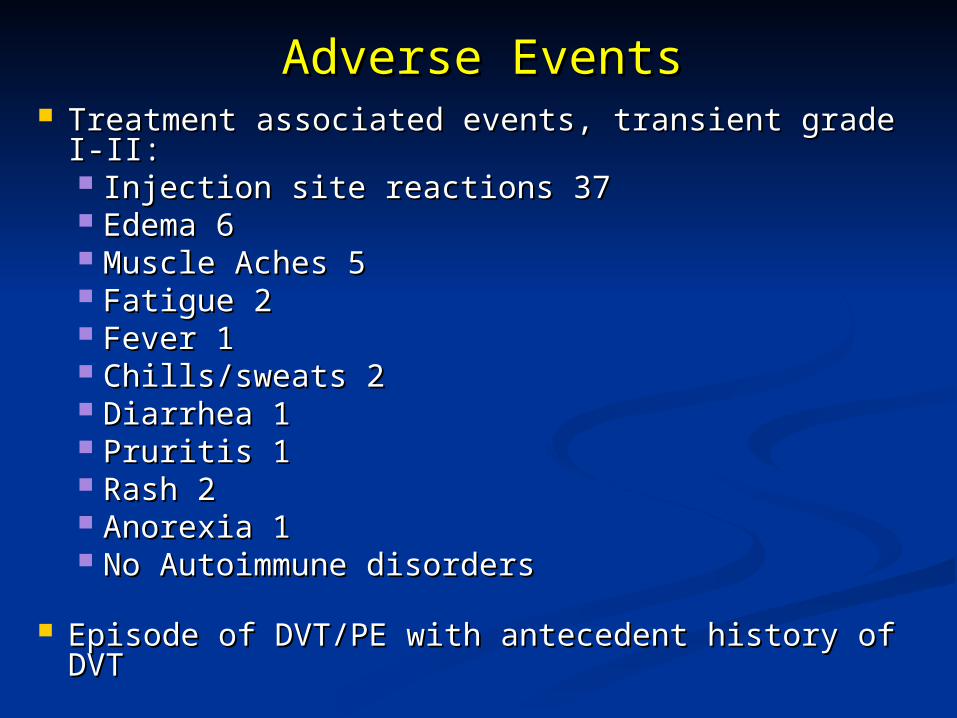
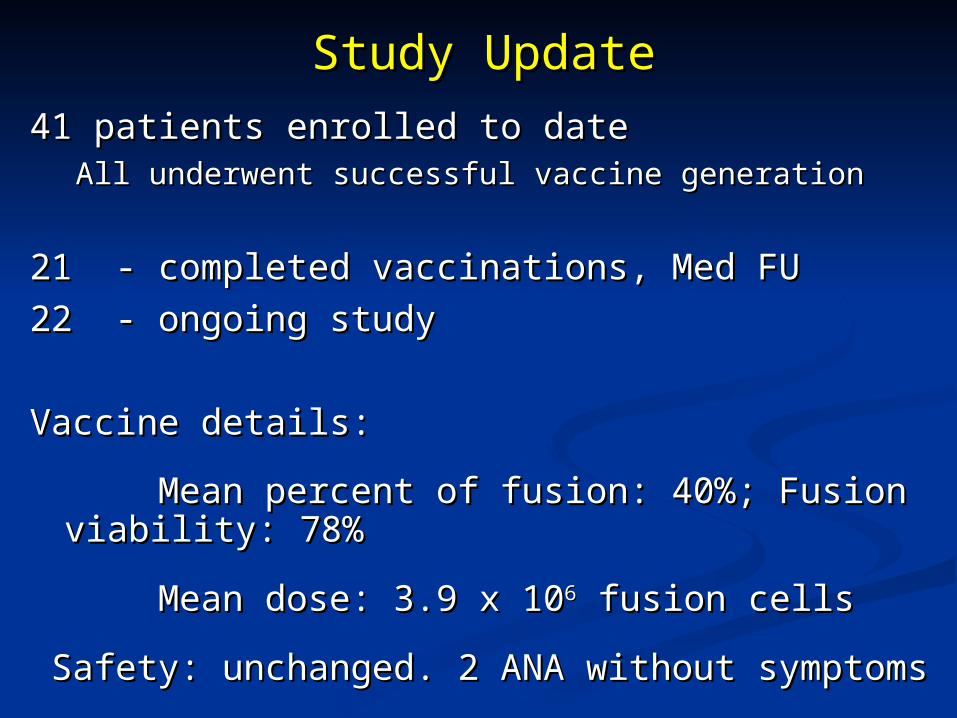
Vaccination with DC/Myeloma Fusions: Vaccination with DC/Myeloma Fusions: Conclusions Conclusions
Vaccination is feasible and well toleratedVaccination is feasible and well tolerated Majority of patients show immunologic Majority of patients show immunologic
responseresponse Disease stabilization in a majority of patientsDisease stabilization in a majority of patients
How to Improve the Efficacy of How to Improve the Efficacy of Fusion Vaccines?Fusion Vaccines?
Administer to patients with Administer to patients with
minimal residual disease minimal residual disease
Administer after eliminating Regulatory T cellsAdminister after eliminating Regulatory T cells
Binds effector memory Tcs, resulting in their activation Binds effector memory Tcs, resulting in their activation and inhibition of apoptosis and inhibition of apoptosis
Clinical Trials:Clinical Trials: Phase I trial : tolerated with evidence of clinical benefitPhase I trial : tolerated with evidence of clinical benefit Administration post ASCT results in increased CD4+ Administration post ASCT results in increased CD4+
effector memory T cells effector memory T cells (Rotem-Yehudar et al., A1216; Ash 2009)(Rotem-Yehudar et al., A1216; Ash 2009)
% E
xpre
ssio
n
of
PD
-1 (
CD
4 T
cel
ls)
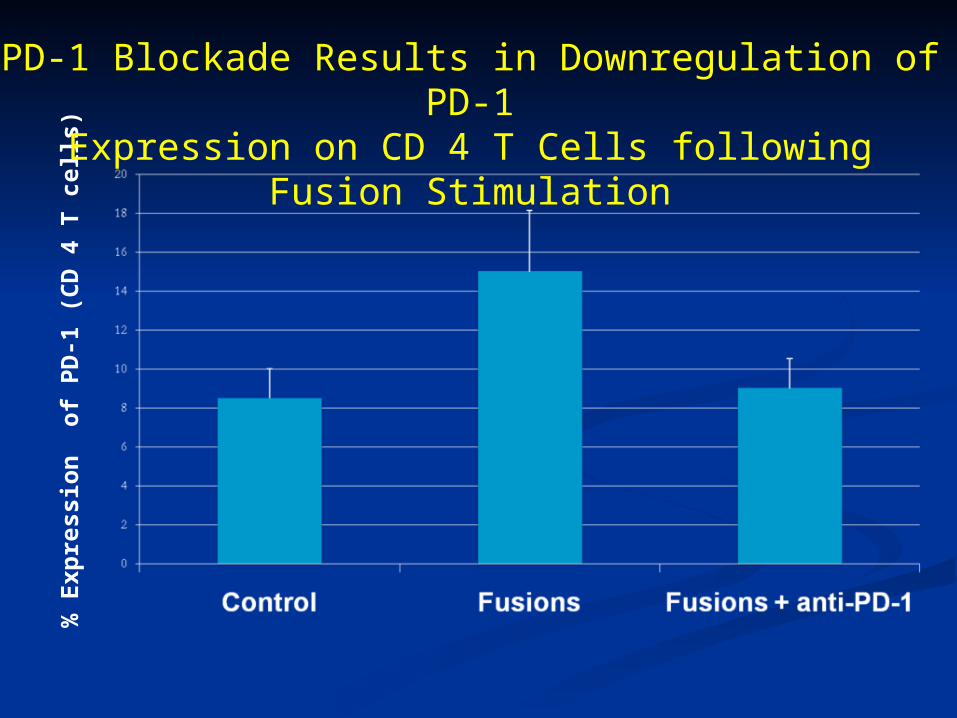
PD-1 Blockade Results in Downregulation of PD-1Expression on CD 4 T Cells following Fusion Stimulation
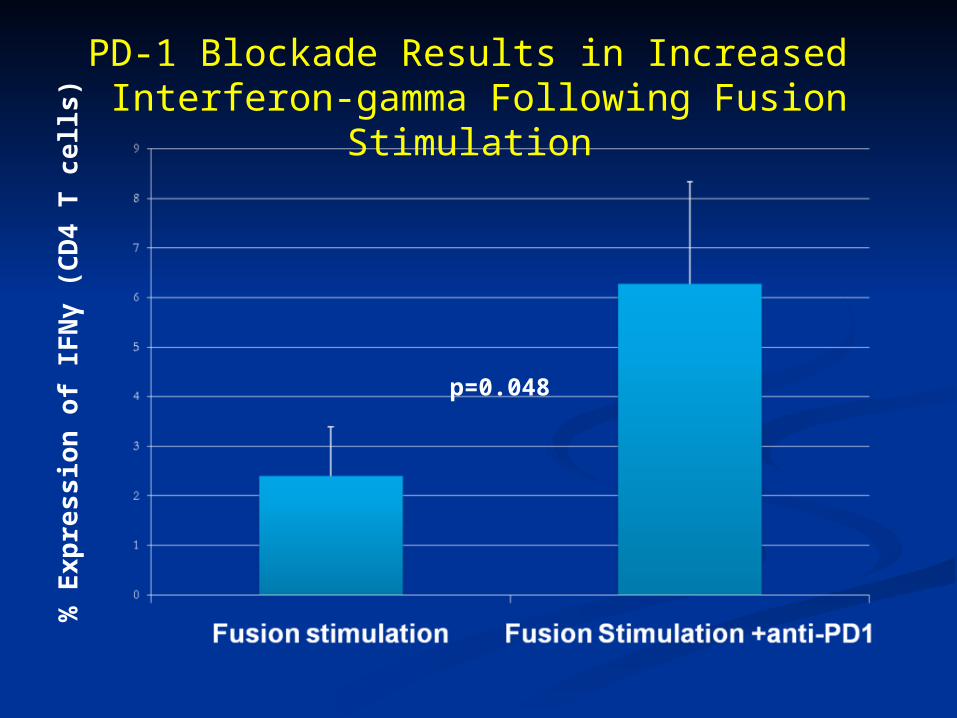
p=0.048
% E
xp
ress
ion
of
IFN
γ (
CD
4 T
ce
lls)
PD-1 Blockade Results in Increased Interferon-gamma Following Fusion Stimulation
100 101 102 103 104
FL1-H100 101 102 103 104
FL1-H100 101 102 103 104
FL1-H
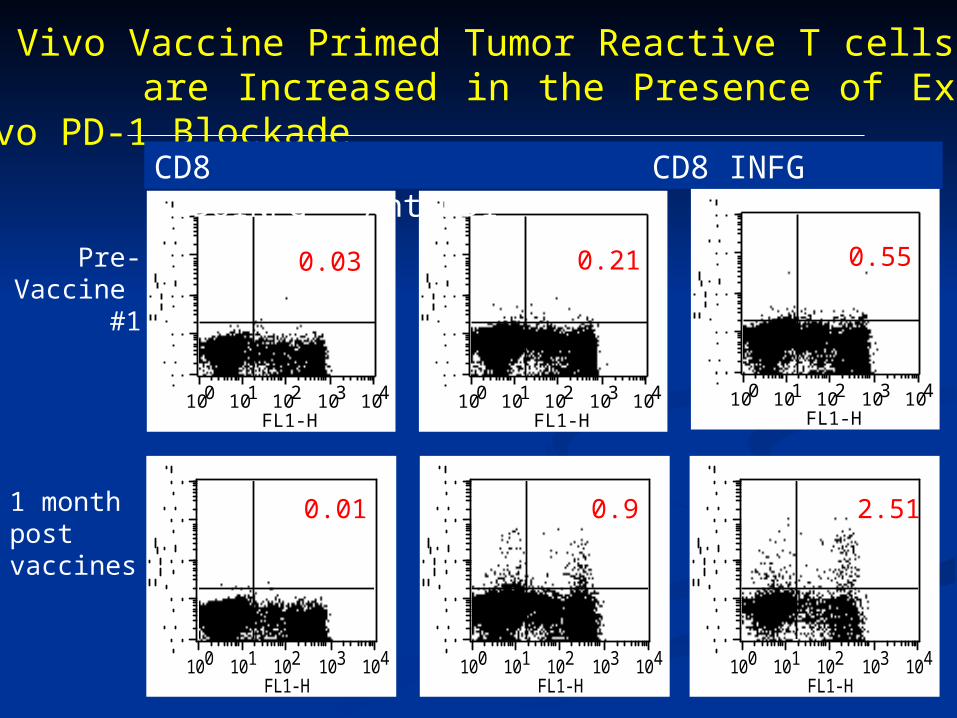
0.210.03 0.55
2.510.90.01
CD8/IFNgCD8/IgG CD8/IFNg
In Vivo Vaccine Primed Tumor Reactive T cells are Increased in the Presence of Ex-vivo PD-1 Blockade
)
Pre-Vaccine #1
1 month post vaccines
100 101 102 103 104
FL1-H100 101 102 103 104
FL1-H100 101 102 103 104
FL1-H
0.03 0.21 0.55
CD8 CD8 INFG CD8INFG + AntiPD1
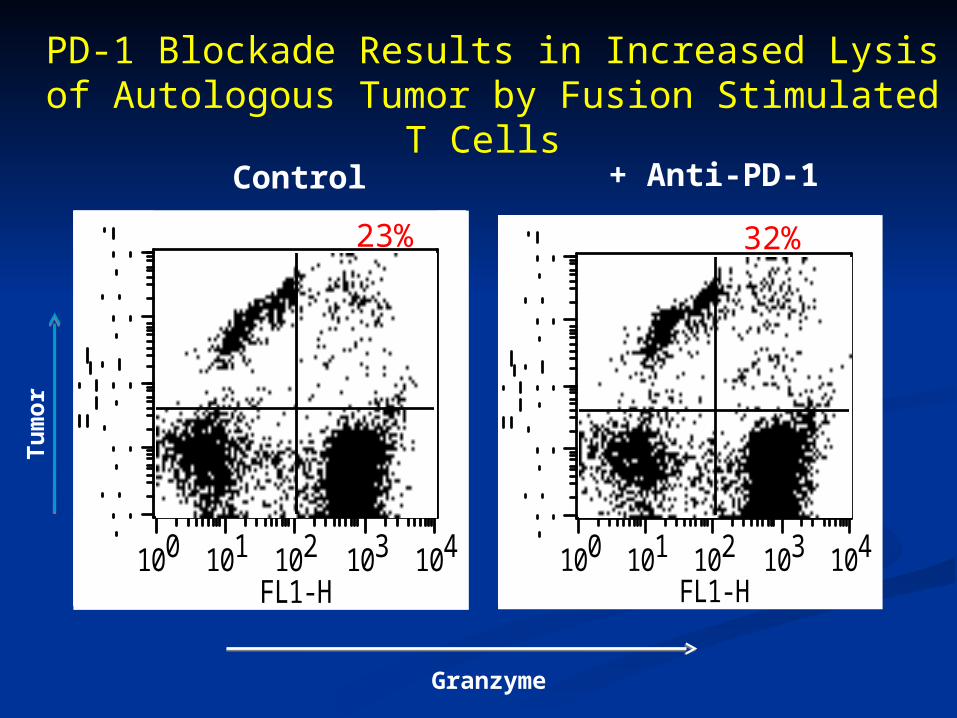
PD-1 Blockade Results in Increased Lysis of Autologous Tumor by Fusion Stimulated T Cells
Granzyme
Tu
mo
r
+ Anti-PD-1 Control
100 101 102 103 104
FL1-H100 101 102 103 104
FL1-H
23% 32%
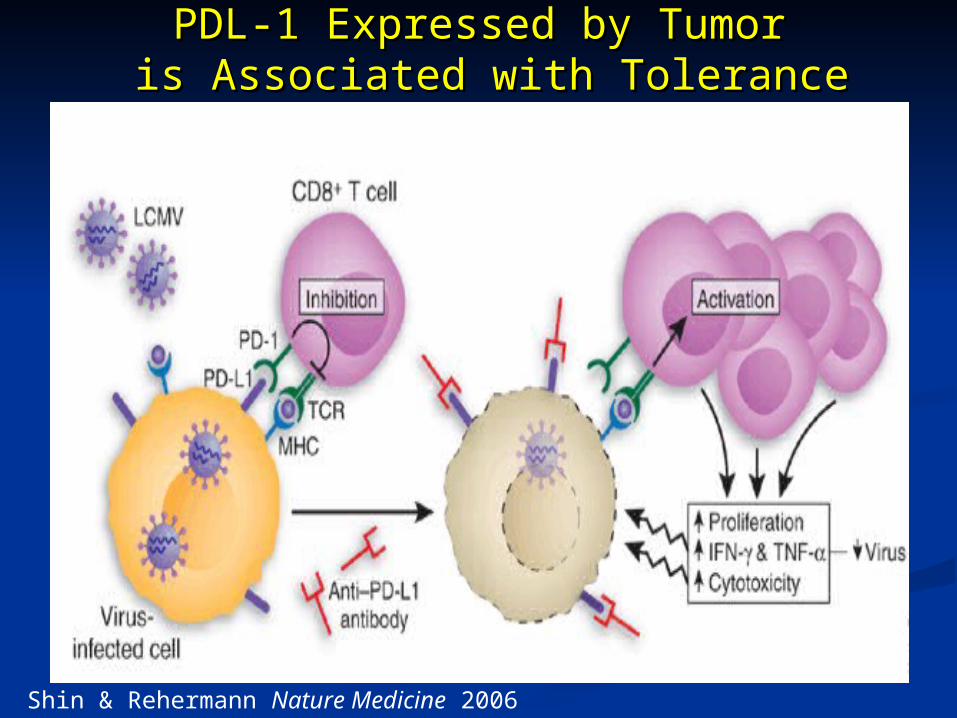
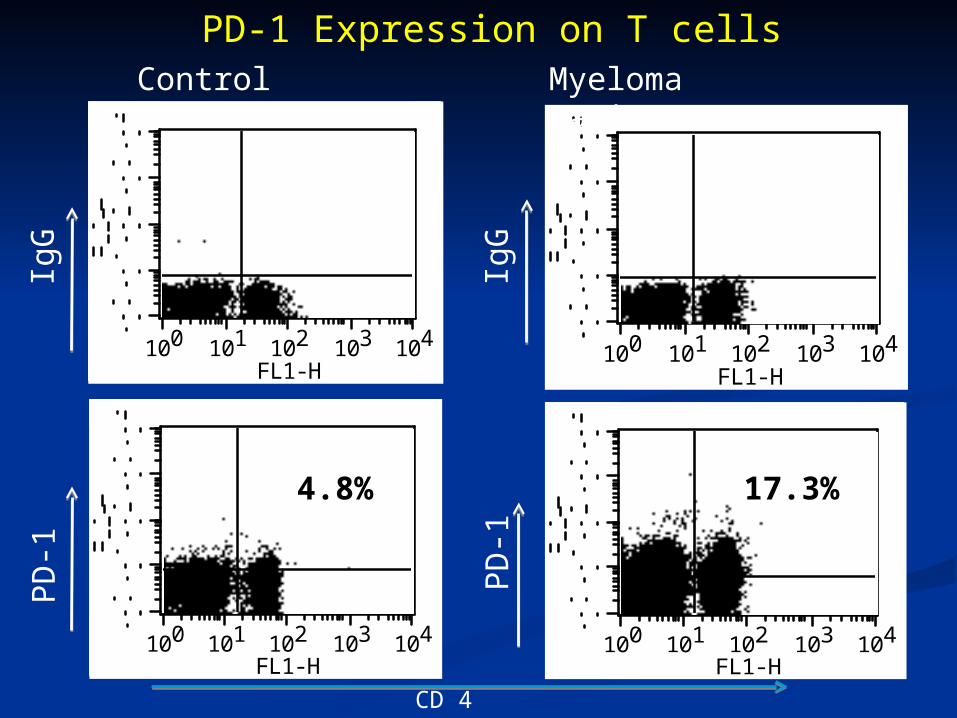
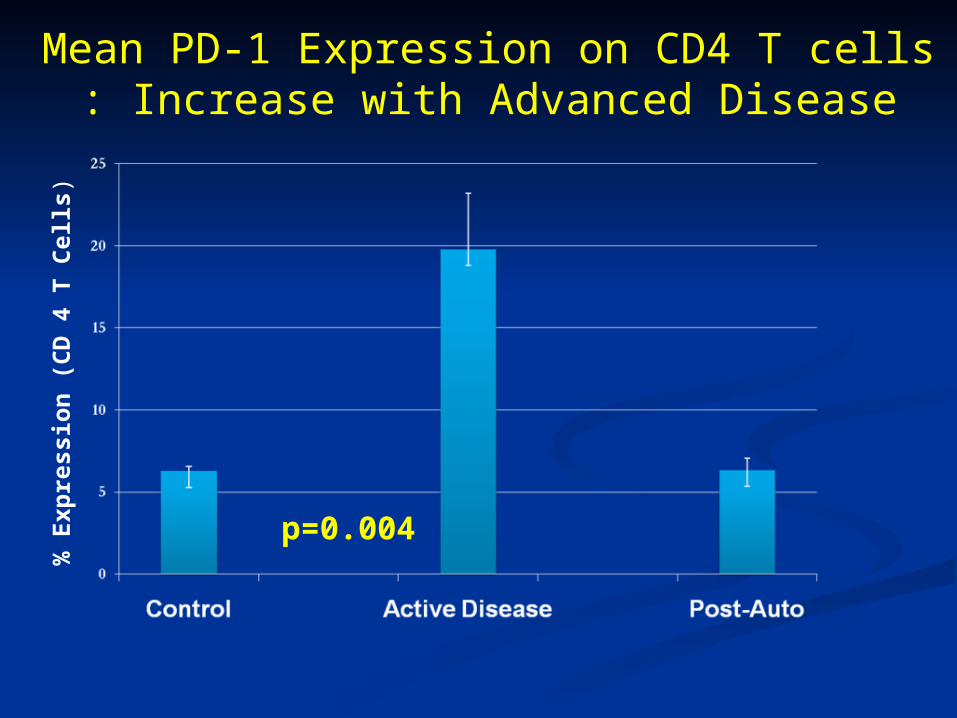
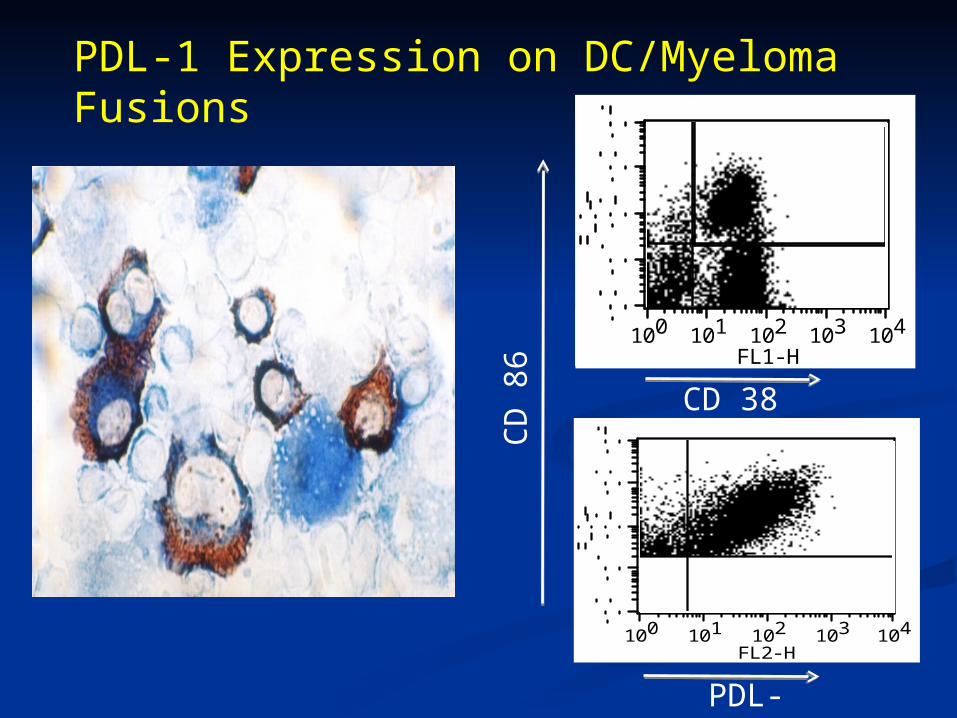
PD1-PDL1 pathway in MyelomaPD1-PDL1 pathway in Myeloma Strong in vitro data supporting the potential role Strong in vitro data supporting the potential role
of PD1-PDL1 pathway in myelomaof PD1-PDL1 pathway in myeloma
- High expression of PDL1 on DCs & MM cells- High expression of PDL1 on DCs & MM cells
- High expression of PDL on T cells- High expression of PDL on T cells PD1-PDL1 blockade improved anti-tumor PD1-PDL1 blockade improved anti-tumor
response in vitroresponse in vitro The in vitro data provide strong platform for The in vitro data provide strong platform for
combining anti PD1-PDL1 hrapy with combining anti PD1-PDL1 hrapy with
DirectionsDirections
Choose the right tumor: Choose the right tumor:
Immunogenic vs “Non Immunogenic?Immunogenic vs “Non Immunogenic?
Improve the immunogenic target: Improve the immunogenic target:
specific peptides vs whole tumor ?specific peptides vs whole tumor ?
Control the inhibitory environment Control the inhibitory environment
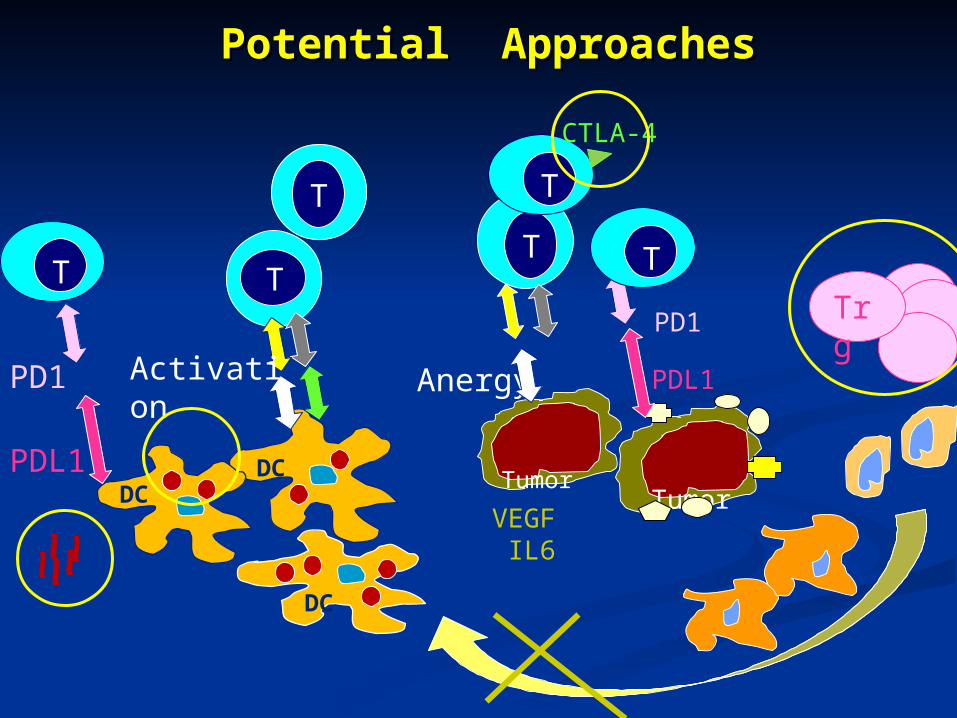
Potential ApproachesPotential Approaches
DCDC
DC
T
TT
T
Tumor Tumor
Activation Anergy
VEGF IL6
CTLA-4
Trg
PDL1
PD1
PDL1
PD1
TT
The Rambam- Harvard Vaccine Program The Rambam- Harvard Vaccine Program
DC/MM – anti PD1L Myeloma vaccine studyDC/MM – anti PD1L Myeloma vaccine study DC/MM- immuno-mudulatory drug studyDC/MM- immuno-mudulatory drug study DC/AML- anti PD1L Myeloma vaccine study DC/AML- anti PD1L Myeloma vaccine study DC/RCC – Sunitinib StudyDC/RCC – Sunitinib Study
Sunitinib -kinase inhibitor of Flt3, Kit, VEGFSunitinib -kinase inhibitor of Flt3, Kit, VEGF
and PDGF receptors and PDGF receptors Pre-clinical study for vaccination for CLL Pre-clinical study for vaccination for CLL


























![[PPT]TUMOR TRAKTUS UROGENITAL - FK UWKS 2012 C | … · Web viewTUMOR TRAKTUS UROGENITAL I. Tumor Ginjal A. Tumor Grawitz B. Tumor Wilms II. Tumor Urotel III. Tumor Testis IV. Karsinoma](https://static.documents.pub/doc/80x56/5ade93b87f8b9ad66b8bb718/ppttumor-traktus-urogenital-fk-uwks-2012-c-viewtumor-traktus-urogenital.jpg)






