56
Not Too Quick; Not Quick Enough: Getting Cesarean Safety Right Larry Veltman, MD, FACOG, CPHRM Northern and Central California Hospital Association June 24, 2015

Not Too Quick; Not Quick Enough:
Getting Cesarean Safety Right
Larry Veltman, MD, FACOG, CPHRM Northern and Central California Hospital
Association June 24, 2015

“They did a section…
• …after a whiff of pit.” • …because it was 5 o’clock.” • …after one decel.” • …because she pushed for an hour and was
exhausted.” • …because she didn’t want any pain.” • …because they get more.” • …because no one ever sues for doing a section,
only for delaying one.”
On The Other Hand,
“They should have done the section…
• …faster but all the ORs were busy.” • …because she was having decels for hours.” • …because the uterus had ruptured.” • …because the cord was prolapsed.” • …because they should have known the baby
was distressed.”

Cesarean Safety: Two Issues
Are There Too Many Cesareans? “Too Many Sections?
Statistics, Safety, Strategies” June 2014
When Needed, Is the Timing Appropriate?

The Path of Least Resistance
Delivery
Vaginal Birth Latent phase 3-12 hr Active Phase 3-6 hr 2nd stage 2-3 hr
Cesarean MD time 1-2 hr
Zhang, et.al, Obstetrics and Gynecology, 2010

VBAC Rate
Primary Cesarean Rate
Cesarean Rate

We’re Not The Only Ones

Are Too Many Cesareans A Safety Issue?

CDC, May 2015

02468
10
0 1 2 3 4+# of Cesarean Sections
% With Previa
Chance of Previa Relative to Number of Prior Cesarean Sections
Clark SL, et al. Placenta previa/accreta and prior cesarean section Obstet Gynecol 1985;66:89–92.
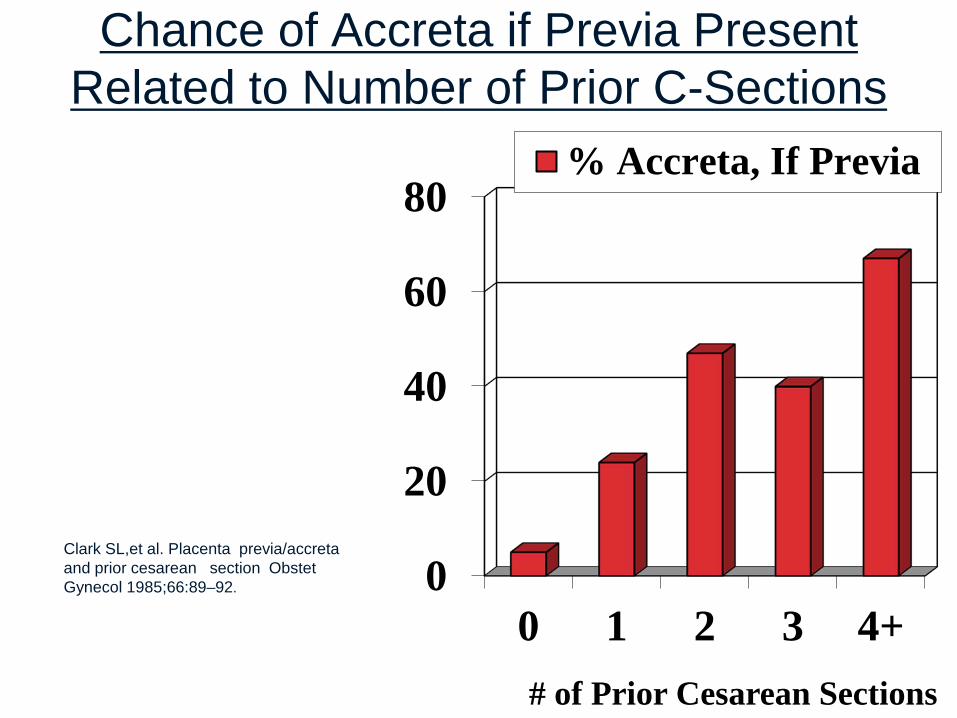
0
20
40
60
80
0 1 2 3 4+# of Prior Cesarean Sections
% Accreta, If Previa
Chance of Accreta if Previa Present Related to Number of Prior C-Sections
Clark SL,et al. Placenta previa/accreta and prior cesarean section Obstet Gynecol 1985;66:89–92.
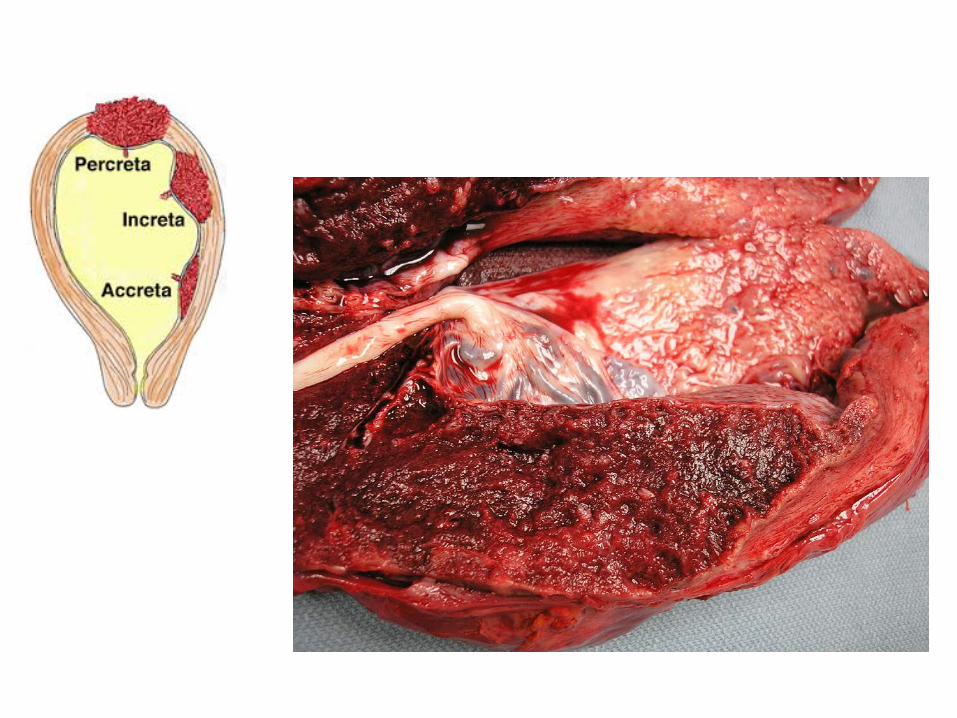

• Leading cause of emergency cesarean hysterectomy • Placenta accreta often leads to massive obstetric
hemorrhage – Average 3000-5000 cc (90% tranfused) • 62 Accretas (Miller, et. al.)
– Estimated Blood Loss • 41 cases had 2,000-5,000 cc (66%) • 9 cases > 5,000-10,000 cc (15%) • 4 cases > 10,000-2,0000 cc (6.5%) • 2 cases > 20,000 cc (3%)
Clinical Significance Placenta Accreta
24.5% had greater than 5 liter blood loss Kastner ES, Figueroa R, Garry D, Maulik D. Emergency peripartum hysterectomy: experience at a community teaching hospital. Obstet Gynecol 2002;99:971–5.

Associated highly significant complications: – Disseminated intravascular coagulopathy – Ureteral injury – Cystotomy (incidental or intentional) – Enterotomy – Other visceral injury – Adult respiratory distress syndrome – ventilator use,
ICU admission – Renal failure – Uterine rupture (prior to surgery)/hemoperitoneum – Fetal/Neonatal/Maternal Morbidity or Death
Clinical Significance

What About the Baby?
Obstet Gynecol 2006;108:885–90.

Routine Vacuum With Cesarean

The Elephants Are Still In The Room
• The need for change • The threat of liability • The use of time

The Overarching Strategy
AVOID THE FIRST CESAREAN

Avoid The First Section
– Elective inductions with an unfavorable cervix
– Adequate trial of labor – latent phase sections
– Is it really “fetal distress”? (Managing Category II tracings)
– Adopt newer approaches to the second stage
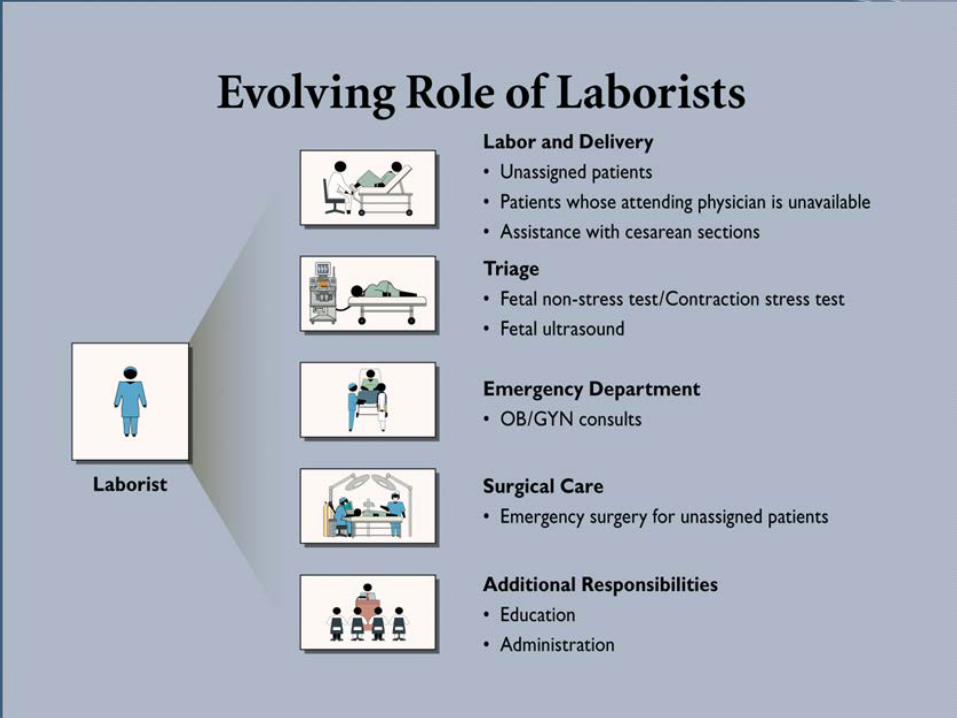
– OB Hospitalists
– Present balanced risks and benefits for elective primary sections
– Management of breeches – versions
– Management of multiples
– 1:1 support in labor (partner, experienced doula, CNM)
– VBAC approaches

Clark, AJOG, Feb, 2009
No Elective Inductions With An Unfavorable Cervix

CONCLUSION: “The active phase of labor may not start until 5 cm of cervical dilation in multiparas and even later in nulliparas. A 2-hour threshold for diagnosing labor arrest may be too short before 6 cm of dilation, whereas a 4-hour limit may be too long after 6 cm.” (Zhang, et al., Obstet Gynecol 2010;115:705–10).
Adequate Trial Of Labor: Six IS the New Four?

Is It Really Fetal Distress?
• What is the likelihood of the fetus developing significant acidemia prior to delivery?
• Moderate variability or accelerations = absent fetal acidemia at the point of observation
• 16 footnotes – must be read – E.g., Treat minimal to absent variability as one
entity.
Educate and Credential!

Other Issues That Effect Cesarean Rates
• Management of the second stage • Use of oxytocin checklist • Twins, breeches & versions • OB Hospitalists • Labor Support • Volume of deliveries • Day of the week, hour of the day

Second Stage Issues
• Length of the second stage: it is not just 2 hours any more
• To push or not to push: laboring down • How long is too long?
– Team huddle at 2 and 4 hours: – Fetal Well being, progress, situational awareness

Use of Oxytocin Checklist
18.8% 15.8%
Clark, AJOG, 2014

Hospitalists May Make a Difference

Labor Support: Yes
2012. 15,288 women met inclusion criteria and provided usable outcome data. Women allocated to continuous support were: • More likely to have a spontaneous vaginal birth • Less likely to have intrapartum analgesia • Less likely to report dissatisfaction • More likely to have shorter labors • Less likely to have a caesarean • Less likely to have instrumental vaginal birth • Less likely to have regional analgesia • Less likely to have a baby with a low five-minute Apgar score •No apparent impact on other intrapartum interventions, maternal or neonatal complications, or breastfeeding.
Do You Have A Peanut Ball?
- 13%

Does Volume Matter?
“Patients delivered by obstetricians with the lowest delivery volumes (fewer than…60 deliveries per year) had a twofold increased rate of cesarean delivery as compared with patients delivered by higher-volume obstetricians…”
(Obstet Gynecol 2014;124:697–703)

Day of the Week
31
Weekday primary cesarean rate = 33.6% Weekend primary cesarean rate = 24.7%

Time of Primary Cesareans Do We Have an Convenience Issue?
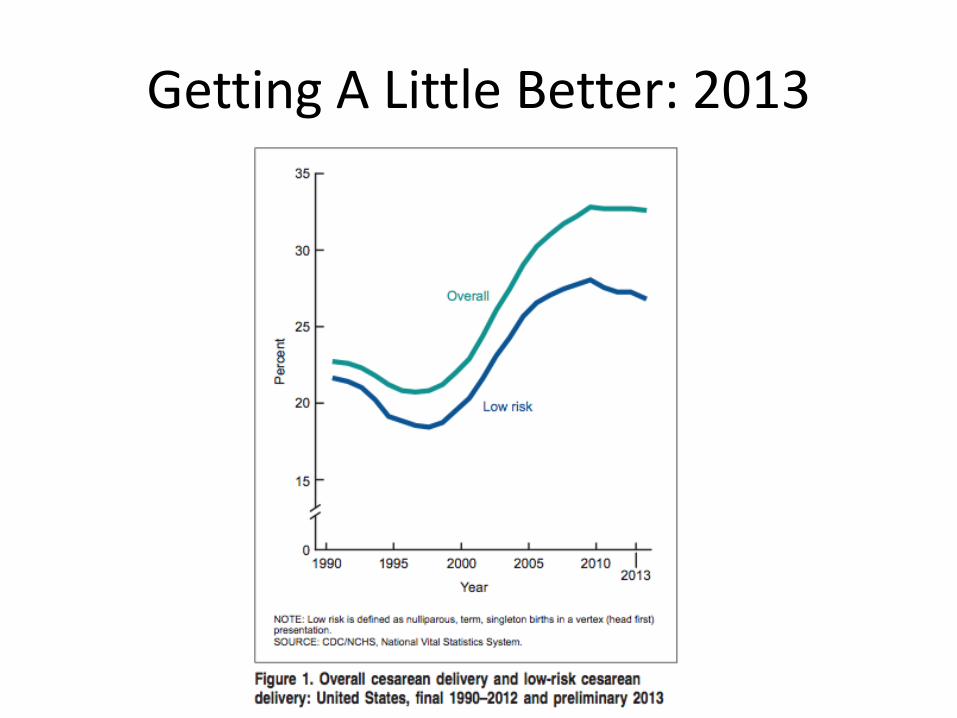
Getting A Little Better: 2013

International Efforts
• Portugal – 36.6% to 33.1% (2009-2014) – “a concerted action based on transmission of information and
training of healthcare professionals together with inclusion of cesarean rates as a criterion for hospital funding…”(AOGS, 2015)
• Canada (QUARISMA) – 22.5% to 21.8% (2008-2011); low risk 8.5% to 7.6% – “Audits, feedback to practitioners, implementation of
best practices…” (NEJM, April 20, 2015)
California Efforts
• Marin Hospital – 32.2% to 27.7% after adding CNM staffing for
private patients • Hoag Hospital
– 38% to 33% • Published physicians’ names with data • Payment adjustments with insurers • Tighter scheduling • Nurse bonuses • Public education

The Other Side Of The Coin
Emergency Cesarean Delivery: Can You Do It Quick Enough?
36

1. Ability to diagnose the need for emergency cesarean 2. Availability of an operating room where an emergency cesarean can be
performed 3. Ability to assemble the team – OB, Anesthesia, OR support 4. Ability to move the patient to the operating room; open instruments; prep
patient 5. Ability to administer appropriate anesthesia for an emergency cesarean section 6. Ability to begin and deliver the infant with an emergency cesarean section 7. Ability to provide the technical and nursing support for the performance of an
emergency cesarean section 8. Ability to provide for resuscitation of a newborn
Components of An Emergency Cesarean
37
Responding To An Emergency
• Any hospital providing an obstetric service should have the capability of responding to an obstetric emergency.
• The required personnel, including nurses, anesthesia personnel, neonatal resuscitation team members, and obstetric attendants, should be in the hospital or readily available.
Guidelines for Perinatal Care, 7th Edition, 2012

Assuring A Rapid Response
• Establish a system of anesthesia, obstetrical and neonatal coverage, surgical assistant availability, and OR team readiness for performance of rapid cesarean.
• Consider a model of in-house physicians as a safety net for obstetrical emergencies.
• Conduct drills/simulation training in performance of emergency cesarean deliveries, including neonatal resuscitation.

Is Everyone Connected? Available?
41

Are You Ready?

“Effective drills may lead to improved standardization of response, health care provider satisfaction, and
patient outcomes.” ACOG CO 487, April 2011, Preparing for Clinical Emergencies in Obstetrics and Gynecology
Emergency Cesarean: The 30-Minute “Rule”
Guidelines for Perinatal Care, 2012
17 Minutes (Am J Obstet Gynecol 1993;169:945-50)
18 Minutes (Obstet Gynecol 2012;119:725–31)
30 Minutes: Not Always!

30 Minutes: Not Always!
46
“The best survival rate for infant…occurs when the delivery of the infant occurs no more than 5 minutes after the mother’s heart stops beating. This typically requires that the provider begin the hysterotomy about 4 minutes after cardiac arrest.”

Green Routine Yellow Priority Orange Urgent Red Emergent
911
Sample Cesarean Priority Schemes

What Can You Skip? • Level 1 – emergent – immediate threat to maternal or fetal well-being
Immediate – no preoperative documentation required, no CHG wipes, no timeout, anticipate general anesthesia or rapid extension of a functioning epidural anesthesia, and modified/expedited abdominal prep.
• Level 2 – urgent – deteriorating maternal or fetal conditions, delay in delivery may result in maternal or fetal morbidity
Within 30minutes from decision to incision – preoperative documentation including time out should be completed, CHG wipes should be used quickly (at least on abdomen), choice of anesthesia and prep made by obstetrician and anesthesiologist.
• Level 3 – unscheduled/priority/non-emergent – no evidence of threat to mother or fetus but cesarean section is indicated, takes precedence over scheduled cases.
Within 2 hours from decision to incision – all preoperative measures should be completed
• Level 4 – routine/scheduled
Within 8 hours – all preoperative measures should be completed

What Can Your Nurses Do?
• Alert the entire team (initiate the process) • Move the patient to the OR • Open the sterile packs • Check fetal heart and prep
– “… in women requiring unscheduled cesarean delivery, fetal surveillance should continue until abdominal sterile preparation has begun.” (Guidelines for Perinatal Care, 2012)
• Scrub / circulate / assist

Can You
• Perform cesarean under local anesthesia? • Perform cesarean hysterectomy?
– Instruments in OR – Obstetrician/surgeon availability – Obstetrician back up/assistant – Nursing OR skills
• Implement a massive fluid transfusion policy?

Don’t Forget The Baby!
“At every delivery, there should be at least one individual whose primary responsibility is the newborn and who is capable of initiating resuscitation….Either this individual or someone else who is immediately available should have the skills required to perform a complete resuscitation, including endotracheal intubation, establishment of vascular access, and the use of medications.”
(Guidelines for Perinatal Care, 2012)
52
Don’t Forget The Baby II
N Engl J Med 371;2 July 10, 2014
The 6 “A”s for Rapid Cesarean Delivery
1. Assess 2. Alert 3. Align 4. Assemble 5. Act 6. Analyze
What’s A MAC
Maternal Assisted Cesarean