Page 1
Novel Agents in Relapsed
or Refractory Multiple Myeloma
Meletios A. Dimopoulos, MD
Department of Clinical Therapeutics,
University of Athens School of Medicine
Athens, Greece
Annual Hematology Conference
Taipei, Taiwan, 14 Apr 2013
Page 2
Natural History of Multiple Myeloma
MGUS or
smoldering
myeloma
Asymptomatic Symptomatic
ACTIVE
MYELOMA
M P
rote
in (
g/L
)
20
50
100
1. RELAPSE
2. RELAPSE
REFRACTORY
RELAPSE
First-line therapy
(the majority receives novel
agent-based therapies)
Plateau
remission
Second-line
therapy
Third-line
therapy
Page 3
When to Start Treatment in RR Myeloma?
1. Development of new soft tissue plasmacytomas or bone lesions
on skeletal survey, CT or MRI
2. Definite increase (ie at least 50% increase and at least 1 cm) of
existing plasmacytomas or bone lesions
3. Hypercalcemia (11.5 mg/dl)
4. Decrease in hemoglobin of >2g/dl or to less than 10 gm/dL
5. Rise in serum creatinine by 2 mg/dl or more
6. Hyperviscosity
Consider treatment if a significant monoclonal protein relapse,
defined as doubling in two consecutive measurements separated
by ≤ 2 months Anderson et al. Leukemia 2008;22:231
Page 4
Considerations in Patients With
Relapsed/Refractory Myeloma
• Previous therapy
• Response to previous therapy
• Patient characteristics and other prognostic factors
– Older than 65 yrs of age
– Increased β2-M, decreased serum albumin, low platelet count
– Cytogenetic abnormalities: del(13q), t(4;14)
– Renal dysfunction
• Up to 50% of patients with MM have renal dysfunction
• Between 20% and 30% of patients have concomitant renal failure
– Extensive bone disease; extramedullary MM
Kyle RA, et al. Mayo Clin Proc. 2003;78:21-33. Kumar SK, et al. Mayo Clin Proc. 2004;79:867-874. Facon T, et al. Blood.
2001;97:1566-1571. Barlogie B, et al. Blood. 2004;103:20-32. Fonseca R, et al. Cancer Res. 2004;64:1546-1558. Kyle RA. Stem
Cells. 1995;13(suppl 2):56-63. Bladé J, et al. Arch Intern Med. 1998;158:1889-1893.
Page 5
APEX Efficacy: VD vs. high-dose Dex
ORR with bortezomib improved from 38% to 43%
<1% nCR 25% PR
16% PR 7% nCR
6% CR
Bortezomib Dex
Resp
on
se %
38%
18%
P<0.0001
0
10
20
30
40
50
60
9% CR
7% nCR
27% PR
43%
Bortezomib
Primary analysis Updated analysis
<1% CR
Richardson et al. Blood 2007;110:3557-60
Page 6
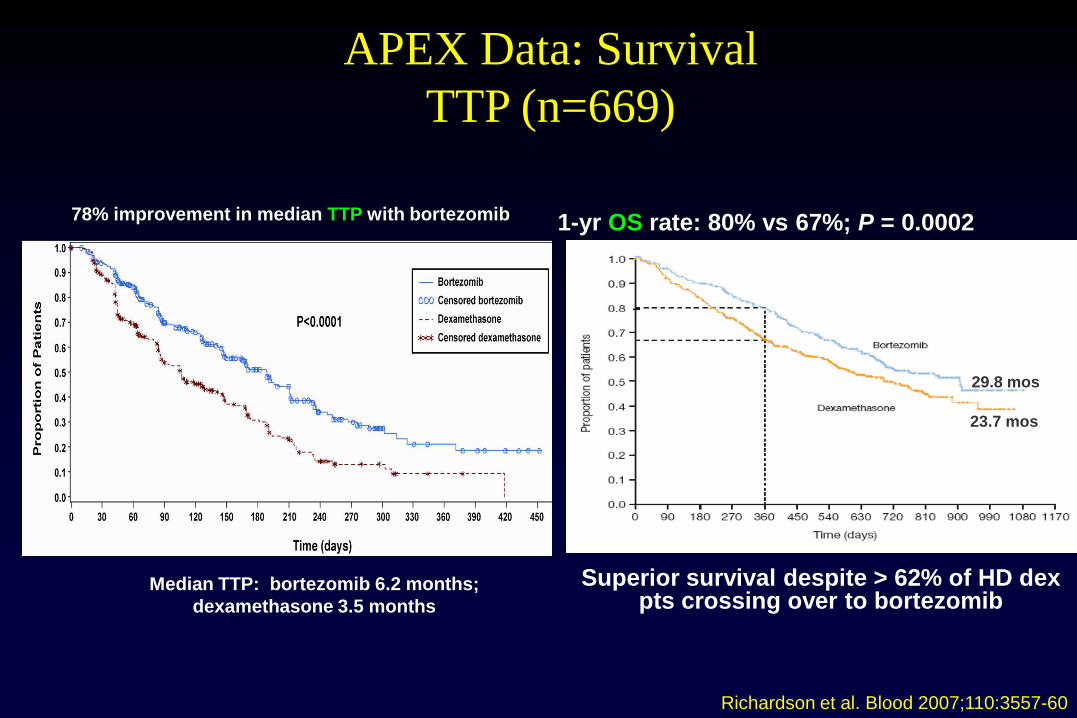
APEX Data: Survival
TTP (n=669)
Median TTP: bortezomib 6.2 months;
dexamethasone 3.5 months
78% improvement in median TTP with bortezomib
Richardson et al. Blood 2007;110:3557-60
Overall and 1-Year
P=.0272
29.8 mos
23.7 mos
1-yr OS rate: 80% vs 67%; P = 0.0002
Superior survival despite > 62% of HD dex pts crossing over to bortezomib
Page 7
MM-010 (Dimopoulos) MM-009 (Weber)
CR
PR + nCR (> 50%)
Re
sp
on
se
ra
te (
%)
*p < 0.001
0
20
40
60 60.2*
24.0* 44.3
15.9
20.6
3.4
80
Len + Dex
(n = 176)
Dex
(n = 175)
Re
sp
on
se
ra
te (
%)
*p < 0.001
0
20
40
60 61.0*
Len + Dex (n
= 177)
19.9*
46.9
14.1 19.3
0.6
80
Dex
(n = 176)
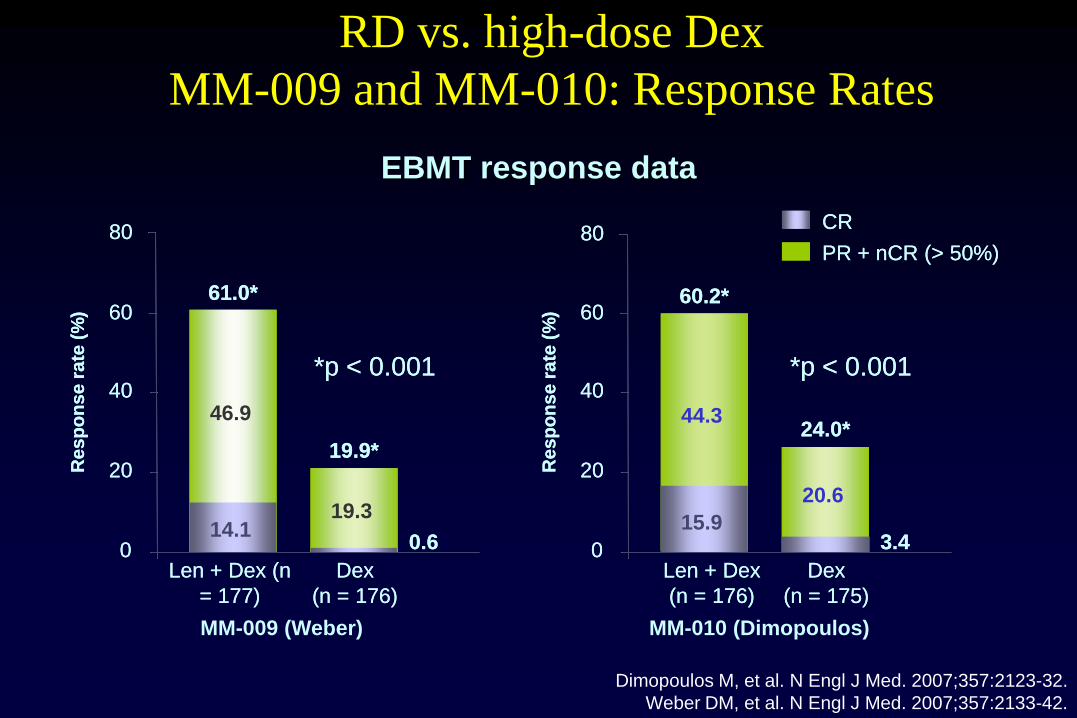
RD vs. high-dose Dex
MM-009 and MM-010: Response Rates
EBMT response data
Dimopoulos M, et al. N Engl J Med. 2007;357:2123-32.
Weber DM, et al. N Engl J Med. 2007;357:2133-42.
CR
PR + nCR (> 50%)
Re
sp
on
se
ra
te (
%)
*p < 0.001
0
20
40
60 60.2*
24.0* 44.3
15.9
20.6
3.4
80
Len + Dex
(n = 176)
Dex
(n = 175)
Re
sp
on
se
ra
te (
%)
*p < 0.001
0
20
40
60 61.0*
Len + Dex (n
= 177)
19.9*
46.9
14.1 19.3
0.6
80
Dex
(n = 176)
Page 8
0
25
50
75
100
p = 0.045
Longer TTP and OS with Len + Dex vs
Dex alone in relapsed/refractory patients
Pati
en
ts (
%)
Survival duration (months)
0 20 40 60 80
Median 38.0 months Median
31.6 months
Overall survival
p < 0.001
Pati
en
ts (
%)
Median 13.4 months Median
4.6 months
0 5 10 15 20 25 30 0
25
50
75
100
Dimopoulos MA, et al. Leukemia. 2009;23:2147-52.
Len + Dex
Dex
TTP (months)
Time to progression
MM-009 and MM-010: pooled analysis
despite 47.6% cross-over of patients who
were randomized to dexamethasone-placebo
Page 9
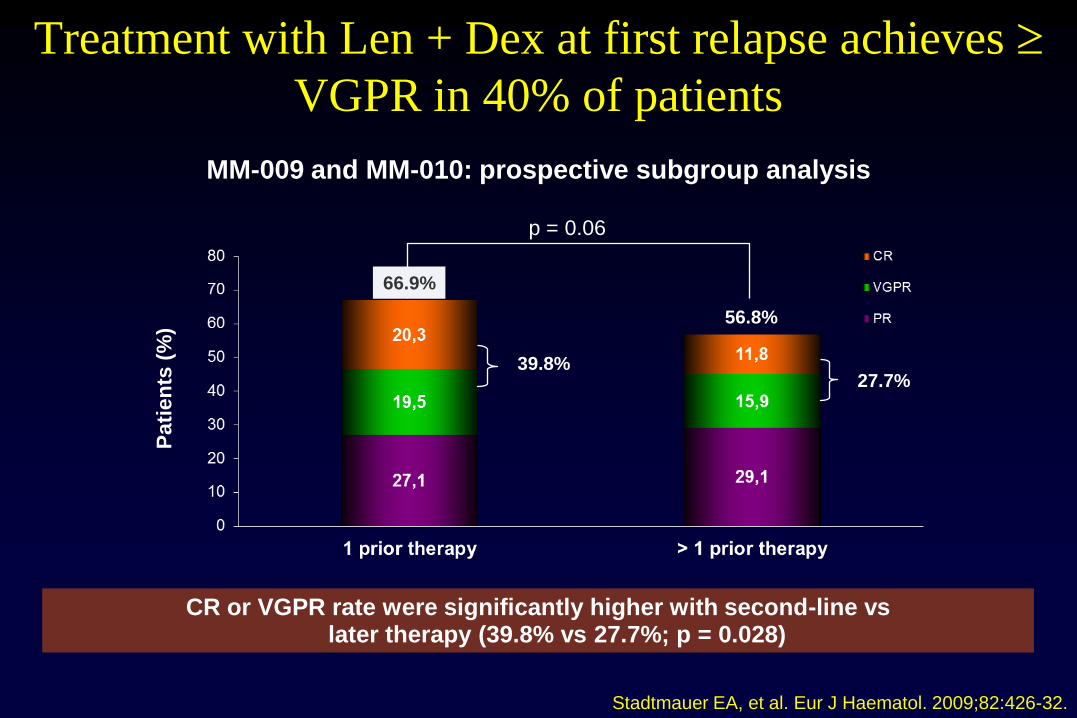
Treatment with Len + Dex at first relapse achieves
VGPR in 40% of patients
Pati
en
ts (
%)
66.9%
39.8%
56.8%
27.7%
p = 0.06
MM-009 and MM-010: prospective subgroup analysis
Stadtmauer EA, et al. Eur J Haematol. 2009;82:426-32.
CR or VGPR rate were significantly higher with second-line vs later therapy (39.8% vs 27.7%; p = 0.028)
Page 10
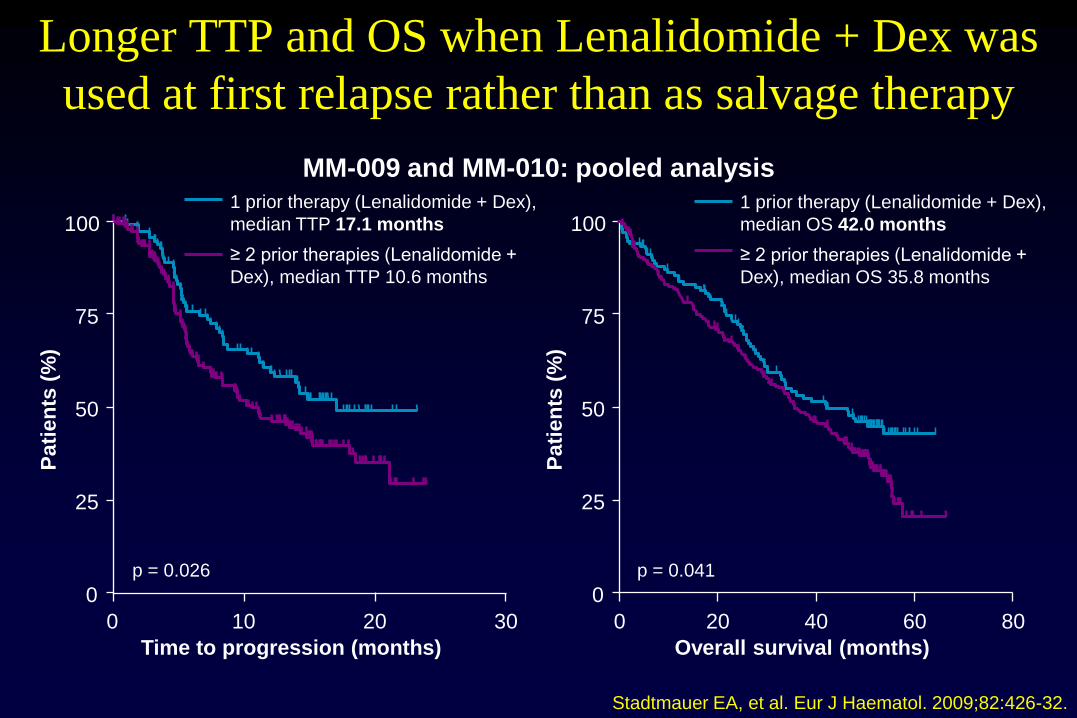
Stadtmauer EA, et al. Eur J Haematol. 2009;82:426-32.
Longer TTP and OS when Lenalidomide + Dex was
used at first relapse rather than as salvage therapy
1 prior therapy (Lenalidomide + Dex),
median TTP 17.1 months
≥ 2 prior therapies (Lenalidomide +
Dex), median TTP 10.6 months
p = 0.026 p = 0.041
0
25
50
75
100
Pati
en
ts (
%)
Time to progression (months)
0 10 20 30
1 prior therapy (Lenalidomide + Dex),
median OS 42.0 months
≥ 2 prior therapies (Lenalidomide +
Dex), median OS 35.8 months
0
25
50
75
100
Pati
en
ts (
%)
Overall survival (months)
0 20 40 80 60
MM-009 and MM-010: pooled analysis
Page 11
Pati
en
ts w
ith
CR
or
VG
PR
(%
)
Treatment cycle
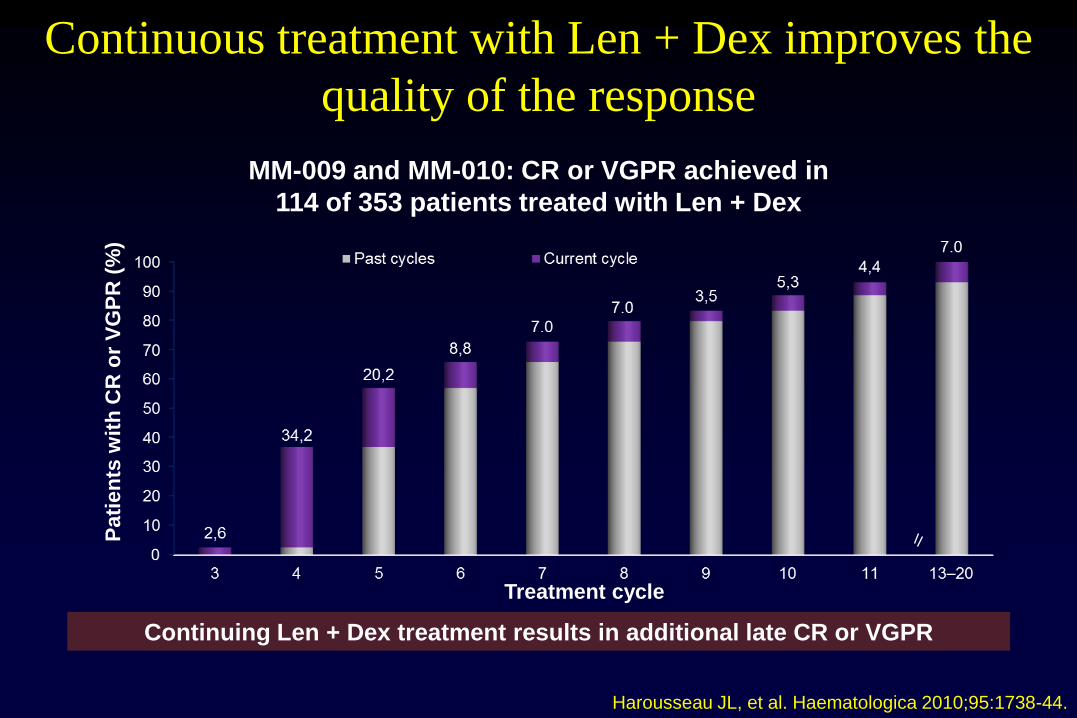
Continuous treatment with Len + Dex improves the
quality of the response
MM-009 and MM-010: CR or VGPR achieved in
114 of 353 patients treated with Len + Dex
Continuing Len + Dex treatment results in additional late CR or VGPR
Harousseau JL, et al. Haematologica 2010;95:1738-44.
Page 12
Patients having a VGPR or better with
Len + Dex treatment have longer TTP
Pooled analysis of MM-009 and MM-010 (N = 114)
27.7 months
vs
12.0 months
0
20
40
60
100
80
Pati
en
ts (
%)
TTP (months)
p < 0.001
0 20 40 60 80
Median follow-up
48 months
CR or VGPR
PR
Harousseau JL, et al. Haematologica 2010;95:1738-44.
Page 13
Dimopoulos et al. ASH 2011; poster 2929
0
10
20
30
40
50
60
70
80
90
100
CR
Near CR/VGPR
PR
50
17
33
16
7
37
PFS ≥ 2 years
(n = 64)
All patients
(N = 353)
Pa
tie
nts
(%
)
≥ PR, 100%
≥ PR, 60%
18% of Patients Have a PFS ≥2 years with RD (pooled
MM-009 and MM-010 Data)
Page 14
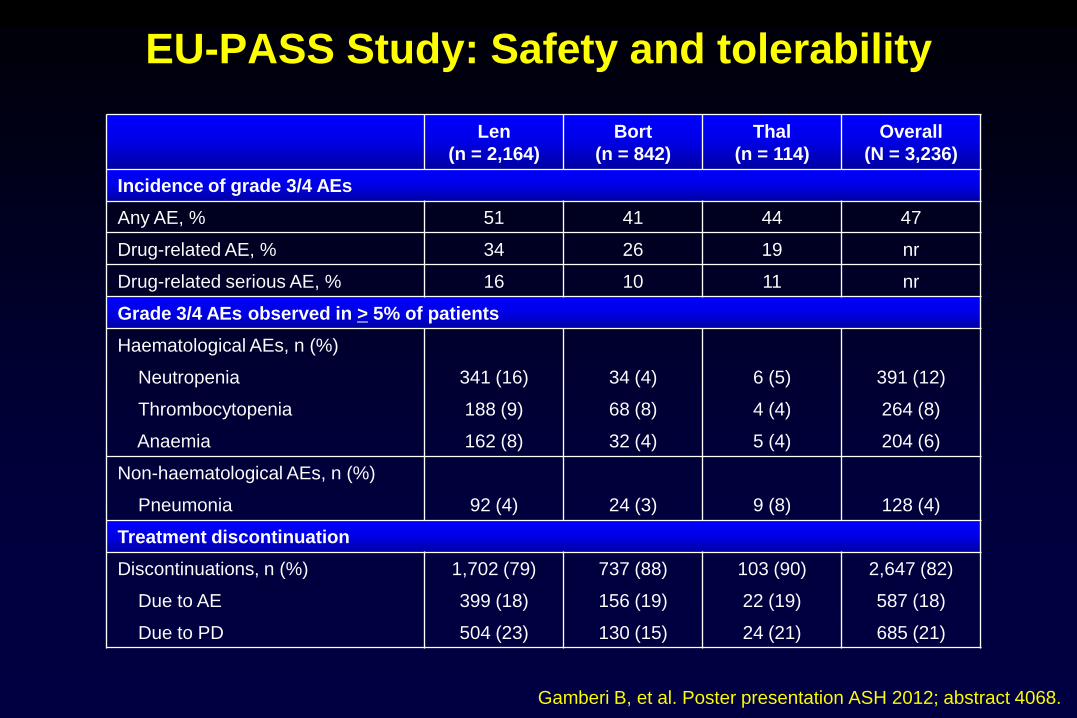
Gamberi B, et al. Poster presentation ASH 2012; abstract 4068.
EU-PASS Study: Safety and tolerability
Len
(n = 2,164)
Bort
(n = 842)
Thal
(n = 114)
Overall
(N = 3,236)
Incidence of grade 3/4 AEs
Any AE, % 51 41 44 47
Drug-related AE, % 34 26 19 nr
Drug-related serious AE, % 16 10 11 nr
Grade 3/4 AEs observed in > 5% of patients
Haematological AEs, n (%)
Neutropenia 341 (16) 34 (4) 6 (5) 391 (12)
Thrombocytopenia 188 (9) 68 (8) 4 (4) 264 (8)
Anaemia 162 (8) 32 (4) 5 (4) 204 (6)
Non-haematological AEs, n (%)
Pneumonia 92 (4) 24 (3) 9 (8) 128 (4)
Treatment discontinuation
Discontinuations, n (%) 1,702 (79) 737 (88) 103 (90) 2,647 (82)
Due to AE 399 (18) 156 (19) 22 (19) 587 (18)
Due to PD 504 (23) 130 (15) 24 (21) 685 (21)
Page 15
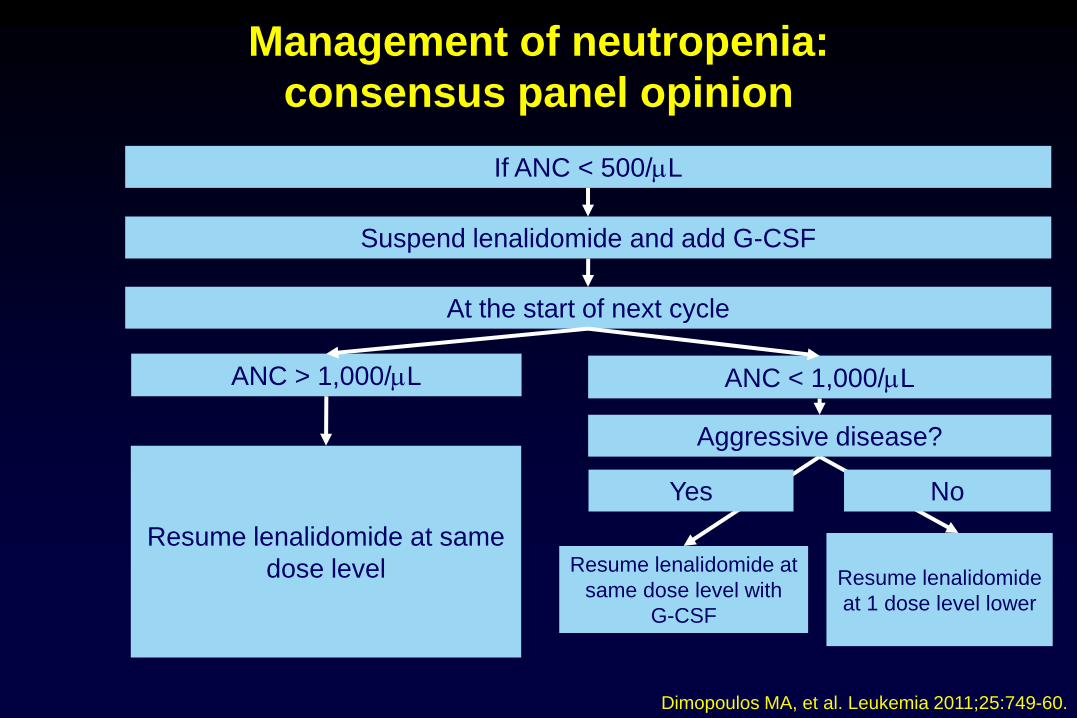
Management of neutropenia:
consensus panel opinion
If ANC < 500/L
Suspend lenalidomide and add G-CSF
At the start of next cycle
ANC > 1,000/L ANC < 1,000/L
Resume lenalidomide at same
dose level
Aggressive disease?
Yes No
Resume lenalidomide at
same dose level with
G-CSF
Resume lenalidomide
at 1 dose level lower
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Page 16
• When platelet level first falls to < 30 × 109/L
– interrupt lenalidomide treatment
• When platelet level returns to ≥ 30 × 109/L
– resume lenalidomide at dose level 1
• For each subsequent drop to < 30 × 109/L
– interrupt lenalidomide treatment
• Upon return to ≥ 30 × 109/L
– resume lenalidomide at next lower dose level
• Do not dose below 5 mg once daily
Starting dose 25 mg
Dose level 1 15 mg
Dose level 2 10 mg
Dose level 3 5 mg
Management of thrombocytopenia
Revlimid® SmPC. Celgene Europe Limited (Windsor, UK). Last updated 31/01/2011.
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Page 17
• When platelet level first falls to < 30 × 109/L
– interrupt lenalidomide treatment
• When platelet level returns to ≥ 30 × 109/L
– resume lenalidomide at dose level 1
• For each subsequent drop to < 30 × 109/L
– interrupt lenalidomide treatment
• Upon return to ≥ 30 × 109/L
– resume lenalidomide at next lower dose level
• Do not dose below 5 mg once daily
Starting dose 25 mg
Dose level 1 15 mg
Dose level 2 10 mg
Dose level 3 5 mg
Management of thrombocytopenia
Revlimid® SmPC. Celgene Europe Limited (Windsor, UK). Last updated 31/01/2011.
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Page 18
Adjustment of lenalidomide dose according to renal
function, neutropenia or thrombocytopenia
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Renal function
Baseline ANC2
> 1,000 l and
platelets > 50,000 l
Baseline ANC2
< 1,000 l or platelets
< 50,000 l
Creatinine clearance
Normal
CLCr 50ml/min
Moderate RI
30ml/min CLCr <
50ml/min
Severe RI
CLCr < 30ml/min
End-stage renal
disease
CLCr < 30ml/min
(requiring dialysis)
Lenalidomide starting dose
25 mg
once daily
10 mg
once daily
15 mg
every other day
5 mg
once daily
15 mg once daily
(GF support / platelet
transfusion as
needed; monitor
frequently)
15 mg every other
day (GF support /
platelet transfusion as
needed; monitor
frequently)
5 mg once daily
(GF support / platelet
transfusion as
needed; monitor
frequently)
5 mg every other
day (GF support /
platelet transfusion
as needed; monitor
frequently)
Adjust the dose at each cycle if changes in CLCr
or blood cell count occurs
Page 19
Management and prevention of peripheral
neuropathy
• Lenalidomide can be given to patients with existing neuropathy or a
history of peripheral neuropathy (PN)1
• Lenalidomide rarely exacerbates pre-existing PN1,2
• For agents that are associated with PN, assessment before every
dose is recommended3
• If PN occurs, prompt intervention is crucial to enable the
improvement /reversal of symptoms3
• In patients with pre-existing PN, the use of drugs without neurotoxic
potential such as Lenalidomide is preferred3
1. Dimopoulos MA, et al. Leukemia 2011;25:749-60. 2. Delforge M, et al.
Poster presented at ASH. Blood. 2009;114:[abstract 3873]. 3. Ludwig H, et al. The Oncologist. 2011;16:388-403.
Page 20
Management and prevention of VTE:
consensus panel opinion
• Thromboprophylaxis should be considered for patients treated with
Lenalidomide + Dex and should continue for the entire duration of
treatment*
• Lenalidomide + Dex should be resumed in patients considered
stable on anticoagulation therapy
• Aspirin prophylaxis is appropriate for patients with standard VTE
risk; LMWH is recommended for patients with higher risk of VTE*
• LMWH prophylaxis should continue for at least the first 4 cycles of
therapy; thereafter, patients may be switched to aspirin
prophylaxis*
* Not in line with SmPC; opinion of consensus panel.
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Page 21
Management and prevention of other AEs during
Lenalidomide + Dex: consensus panel opinion
• Limited, localized rash
– antihistamines and topical steroids
• Diffuse, desquamating, exfoliative, bullous rash
– discontinue lenalidomide
• Infection
– routine antibiotic prophylaxis for first 3 cycles of therapy
• Muscle cramps
– magnesium supplementation
• Dex-related symptoms (myopathy, non-neutropenic infection,
psychological changes, hyperglycaemia)
– consider reduction in Dex dose
Dimopoulos MA, et al. Leukemia 2011;25:749-60.
Page 22
A Multicenter, Open-Label Phase 2 Study of
Lenalidomide Plus Low-Dose Dexamethasone in
Chinese Patients With Relapsed/Refractory
Multiple Myeloma: The MM-021 Trial
Page 23
Investigators
Jian Hou1, Xin Du2, Jie Jin3, Zhen Cai3, Fangping Chen4, Dao-bin Zhou5, Li
Yu6, Xiaoyan Ke7, Xiao Li8, Depei Wu9, Fanyi Meng10, Huisheng Ai11, Jianmin
Wang12, Jingshan Zhang13, Honeylet Wortman-Vayn13, Nianhang Chen13, Jay
Mei13
• 1Shanghai Changzheng Hospital, Shanghai, China; 2Guangdong General Hospital, Guangzhou, China; 3The 1st
Hospital, Zhejiang University, Hangzhou, China; 4Xiangya Hospital of Central South University, Changsha,
China; 5Peking Union Medical College Hospital, Beijing, China; 6The 301 Military Hospital, Beijing, China; 7Peking University Third Hospital, Beijing, China; 8Shanghai 6th Hospital, Shanghai, China; 9The 1st Affiliated
Hospital of Soochow University, Suzhou, China; 10Nanfang Hospital, Southern Medical University, Guangzhou,
Guangzhou, China; 11The 307 PLA Hospital, Beijing, China; 12Changhai Hospital, Shanghai, China; 13Celgene
Corporation, Summit, NJ, USA
Page 24
Study Design • Phase 2, multicenter, single-arm, open-label
• Patients with RRMM received:
– LEN (25 mg/day on days 1–21)
– and LoDEX (40 mg on days 1, 8, 15, and 22)
– in 28-day treatment cycles until disease progression
– Starting dose of DEX adjusted according to patient age:
– 40 mg/day ( ≤ 75 years)
– 20 mg/day ( > 75 years)
• Thromboembolic prophylaxis
Page 25
• High percentage of pts with advanced disease and high
number of prior therapies – 86% with Durie-Salmon Stage III disease
– 57% had received 4 prior therapies
– 69% with prior THAL, 64% with prior BORT, and 46% had received
both
• Unusually high proportion (5%) with IgD subtype Associated with more
severe disease and lower response rates than other types of MM1
1. Maisnar v, et al. Bone Marrow Transplant. 2008;41:51-54.
Summary of
Baseline Characteristics
Page 26
Parameter
Median (range)
Caucasian
N = 34 (MM-001 and MM-002)
Japanese
N = 12 (MM-017)
Chinese
N = 9 (MM-021)
Age (yrs) 59 (40–69) 63 (43–66) 55 (44–68)
Body weight (kg) 82 (50–118) 59 (48–75) 65 (54–84)
CrCl (mL/min) 101 91 95
AUC∞ (ng•h/mL) 2,124 2,305 2,202
Cmax (ng/mL) 487 572 596
Tmax (h) 1.0 1.0 0.93
t½ (h) 3.18 2.70 3.18
Similar Pharmacokinetics
in Chinese MM patients
Despite lower body weight
Page 27
Results Response Rates and Comparison
7.5 15.0 2.0
46.0
45.6
19.9
0%
20%
40%
60%
80%
100%
Len-d (n=187) Len-D (n=353) Pla-D (n=351)
PR-VGPR
CR
p < 0.001
MM-021
MM-009
MM-010
Data from Dimopoulos M, et al. Leukemia., 2009]
53.5% 60.1%
21.9%
Page 28
14.0 5.0
50.0
45.0
0%
20%
40%
60%
80%
100%
1-2 prior (n=50) > 2 prior (n=137)
PR-VGPR
CR
50.0 %
Responses
by Prior Therapy
64.0 %
Page 29
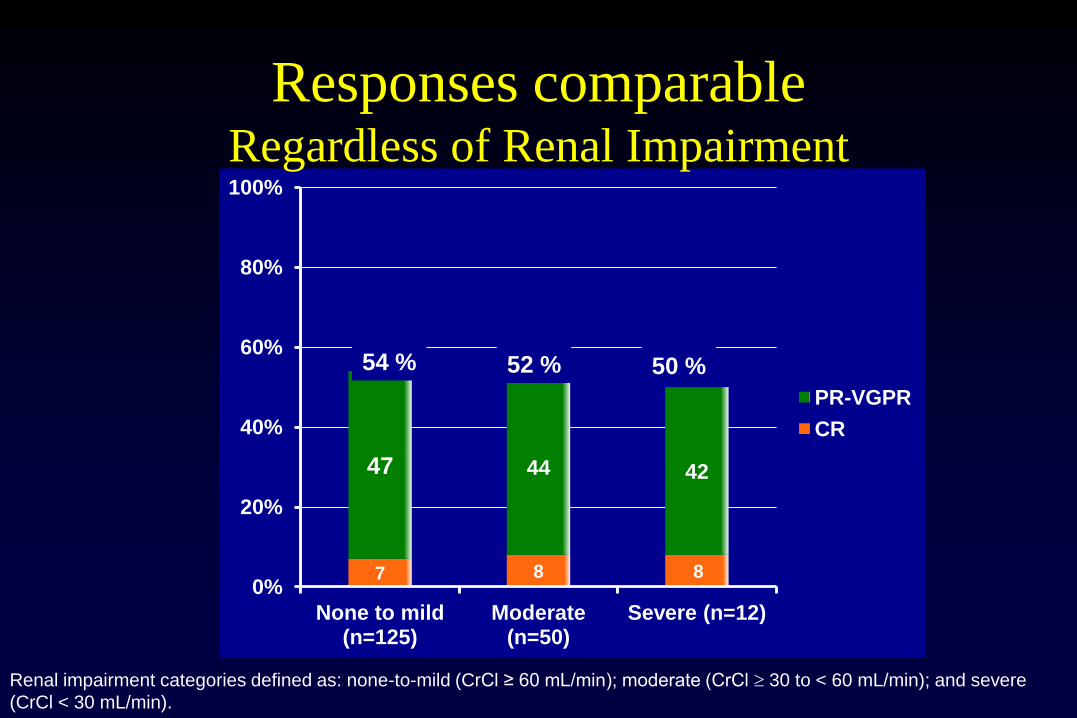
7 8 8
47 44 42
0%
20%
40%
60%
80%
100%
None to mild (n=125)
Moderate (n=50)
Severe (n=12)
PR-VGPR
CR
54 % 52 % 50 %
Responses comparable Regardless of Renal Impairment
Renal impairment categories defined as: none-to-mild (CrCl ≥ 60 mL/min); moderate (CrCl 30 to < 60 mL/min); and severe
(CrCl < 30 mL/min).
Page 30
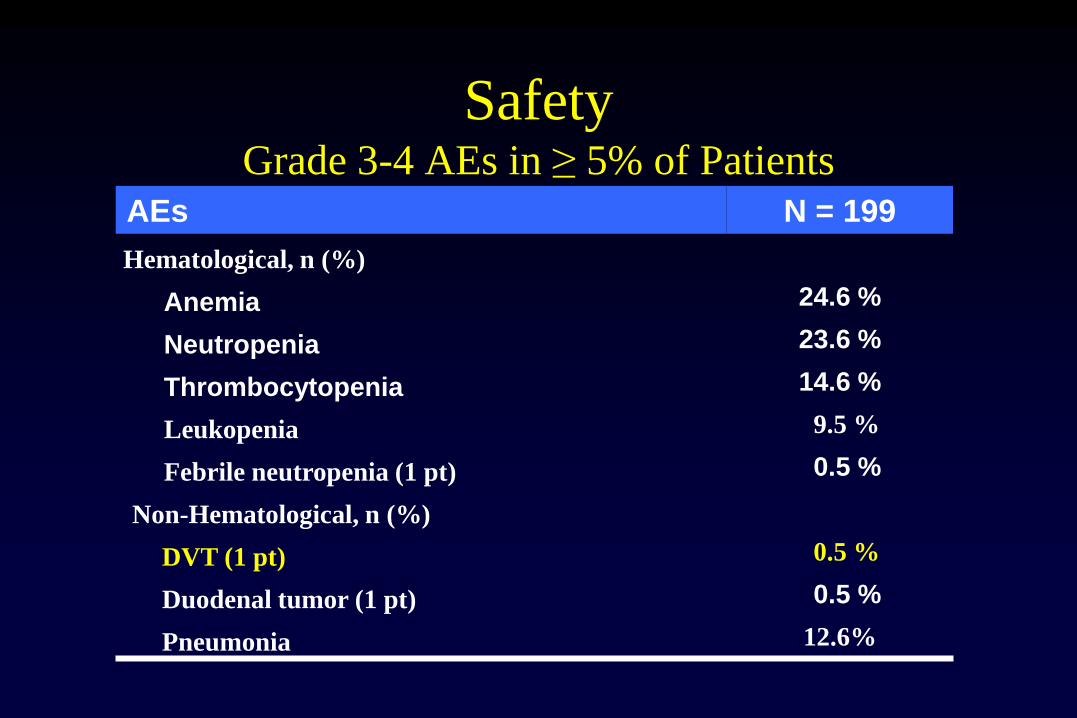
AEs N = 199
Hematological, n (%)
Anemia 24.6 %
Neutropenia 23.6 %
Thrombocytopenia 14.6 %
Leukopenia 9.5 %
Febrile neutropenia (1 pt) 0.5 %
Non-Hematological, n (%)
DVT (1 pt) 0.5 %
Duodenal tumor (1 pt) 0.5 %
Pneumonia 12.6%
Safety Grade 3-4 AEs in ≥ 5% of Patients
Page 31
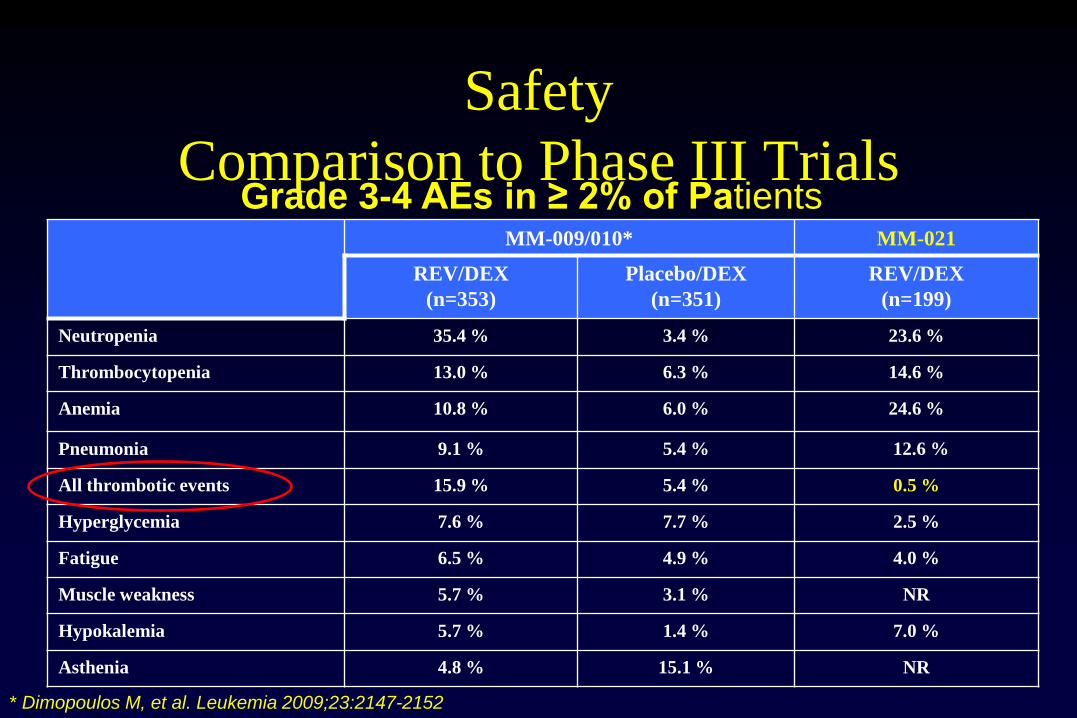
Safety
Comparison to Phase III Trials MM-009/010* MM-021
REV/DEX
(n=353)
Placebo/DEX
(n=351)
REV/DEX
(n=199)
Neutropenia 35.4 % 3.4 % 23.6 %
Thrombocytopenia 13.0 % 6.3 % 14.6 %
Anemia 10.8 % 6.0 % 24.6 %
Pneumonia 9.1 % 5.4 % 12.6 %
All thrombotic events 15.9 % 5.4 % 0.5 %
Hyperglycemia 7.6 % 7.7 % 2.5 %
Fatigue 6.5 % 4.9 % 4.0 %
Muscle weakness 5.7 % 3.1 % NR
Hypokalemia 5.7 % 1.4 % 7.0 %
Asthenia 4.8 % 15.1 % NR
* Dimopoulos M, et al. Leukemia 2009;23:2147-2152
Grade 3-4 AEs in ≥ 2% of Patients
Page 32
Dose Level Used
According to Time
Cycle
% of Treated Patients on Each Lenalidomide Dose
25 mg
10 mg
15 mg 20 mg
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 9 10 11 12
Page 33
MM-021 Trial
Conclusions
• Largest registration trial for RR MM Chinese patients
• Overall response rates
– 54% in predominantly heavily pre-treated pts
– 64% in pts treated earlier (i.e. 1-2 prior therapies)
– Consistent with those observed in pivotal phase III trials in caucasians
– Regardless of the severity of disease
– Consistent across subgroups including patients with renal impairment
Page 34
MM-021 Trial
Conclusions (cont.)
• PK profile similar to that seen in prior studies of Caucasian and Japanese patients
• Len + low dose dex is tolerable – No DVT challenge in Chinese patients
– No Peripheral Neuropathy Challenge
– No special dose-adaptation required in Chinese patients
Rd regimen will address the unmet clinical need for effective
treatment of Chinese patients with RRMM
Page 35
Is retreatment with novel agents
feasible?
Page 36
2nd-line combinations after bortezomib-based
therapies: data from VISTA trial
Mateos MV, et al. J Clin Oncol 2010;28:2259-2266
Bortezomib mono or
combination
(n = 107)
Thalidomide
combination
(n = 155)
Lenalidomide
combination
(n = 36)
MPV (n = 129) MP (n = 194)
Overa
ll r
esp
on
se*
rate
(%
)
* Responses PR.
Page 37
Studies of bortezomib retreatment: results of a meta-
analysis presented at ASH 2012
ORR,
%
TTP,
mos
OS,
mos
All patients 39 7.5 16.6
BTZ-refractory:
0% (relapsed only)* 57 8.5 19.7
<50% 28 – –
≥50% 19 5.9 20.4
100% (refractory
only)
23 – 11.2
Unknown 49 6.0 –
Prior therapies:
≤4 43 8.2 13.3
>4 29 7.1 20.0
Unknown 45 5.6 –
ORR,
%
TTP,
mos
OS,
mos
Time since last BTZ:
<9 months 49 9.5 19.7
≥9 months 43 7.3 –
Unknown 30 5.9 15.4
Therapy:
BTZ ± dex 51 7.9 19.2
Combination 36 7.1 16.1
Knopf et al. ASH 2012 (Abstract 1863), poster presentation
Page 38
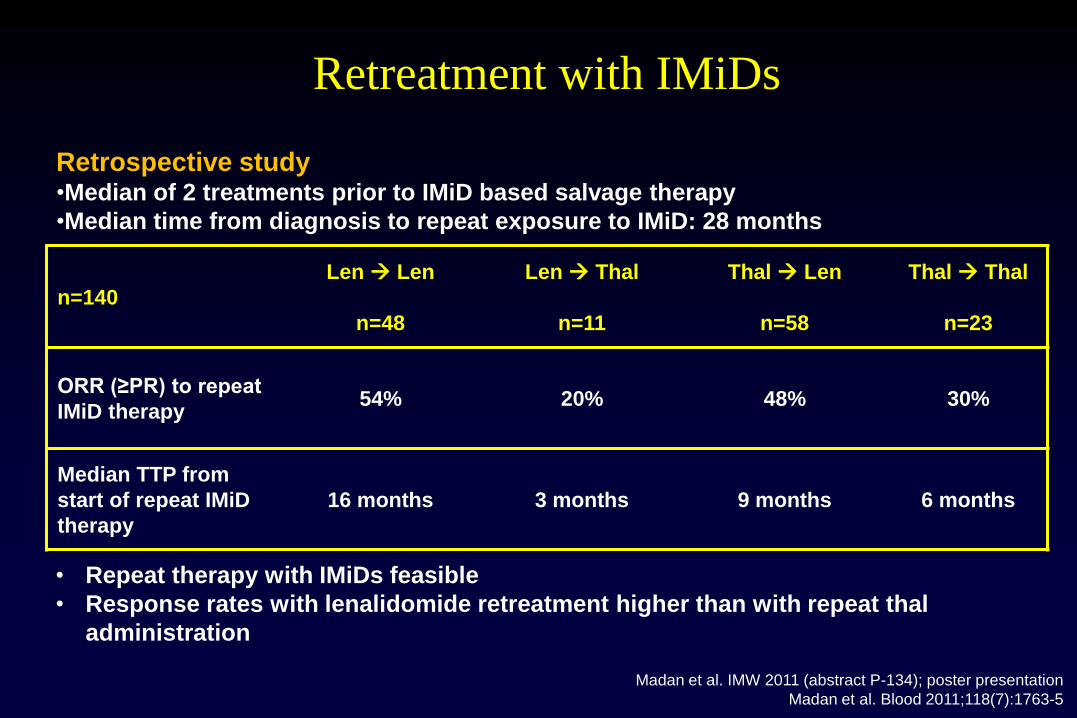
Retreatment with IMiDs
n=140
Len Len
n=48
Len Thal
n=11
Thal Len
n=58
Thal Thal
n=23
ORR (≥PR) to repeat
IMiD therapy 54% 20% 48% 30%
Median TTP from
start of repeat IMiD
therapy
16 months 3 months 9 months 6 months
• Repeat therapy with IMiDs feasible
• Response rates with lenalidomide retreatment higher than with repeat thal
administration
Madan et al. IMW 2011 (abstract P-134); poster presentation
Madan et al. Blood 2011;118(7):1763-5
Retrospective study •Median of 2 treatments prior to IMiD based salvage therapy
•Median time from diagnosis to repeat exposure to IMiD: 28 months
Page 39
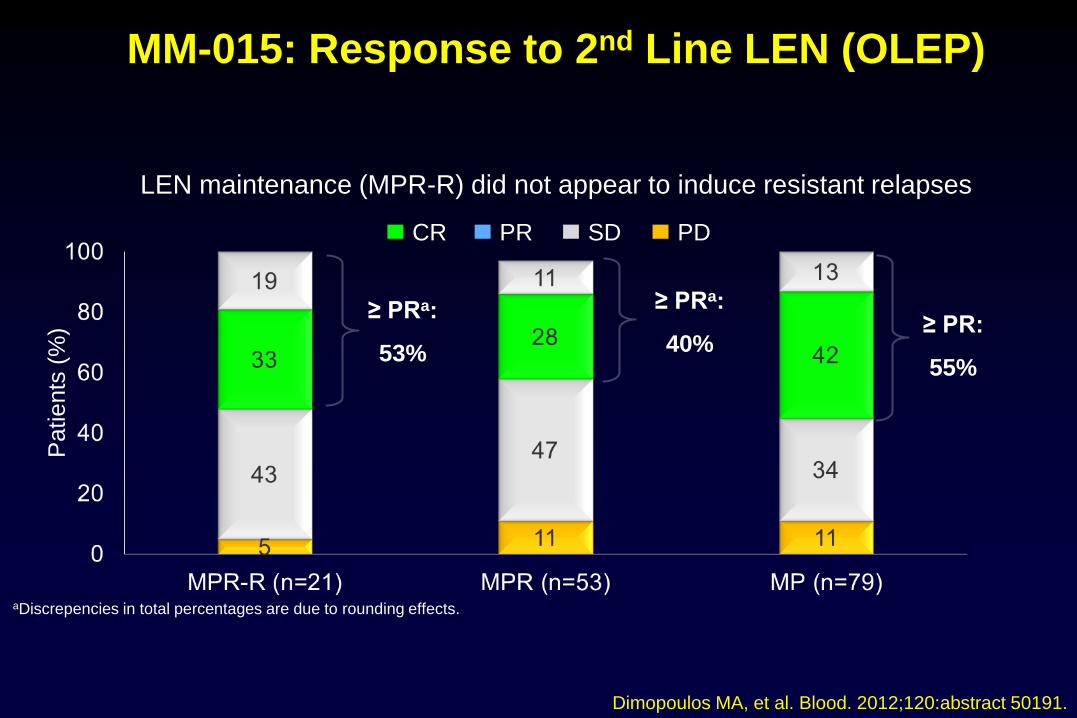
Dimopoulos MA, et al. Blood. 2012;120:abstract 50191.
MM-015: Response to 2nd Line LEN (OLEP)
≥ PRa:
53%
≥ PRa:
40% ≥ PR:
55%
aDiscrepencies in total percentages are due to rounding effects.
Patients
(%
)
CR PR SD PD
LEN maintenance (MPR-R) did not appear to induce resistant relapses
Page 40
Unmet Clinical Needs for RR MM
Multiple myeloma refractory to both
lenalidomide- and bortezomib- based regimens
Plasmacytoma relapses
High risk features, i.e. del17p
Important for treatments to target tumour growth
and concomitant immunosuppression while being
easy to administer and well tolerated for long-
term use
Page 41
Novel Drugs for
Relapsed/Refractory Myeloma
Page 42
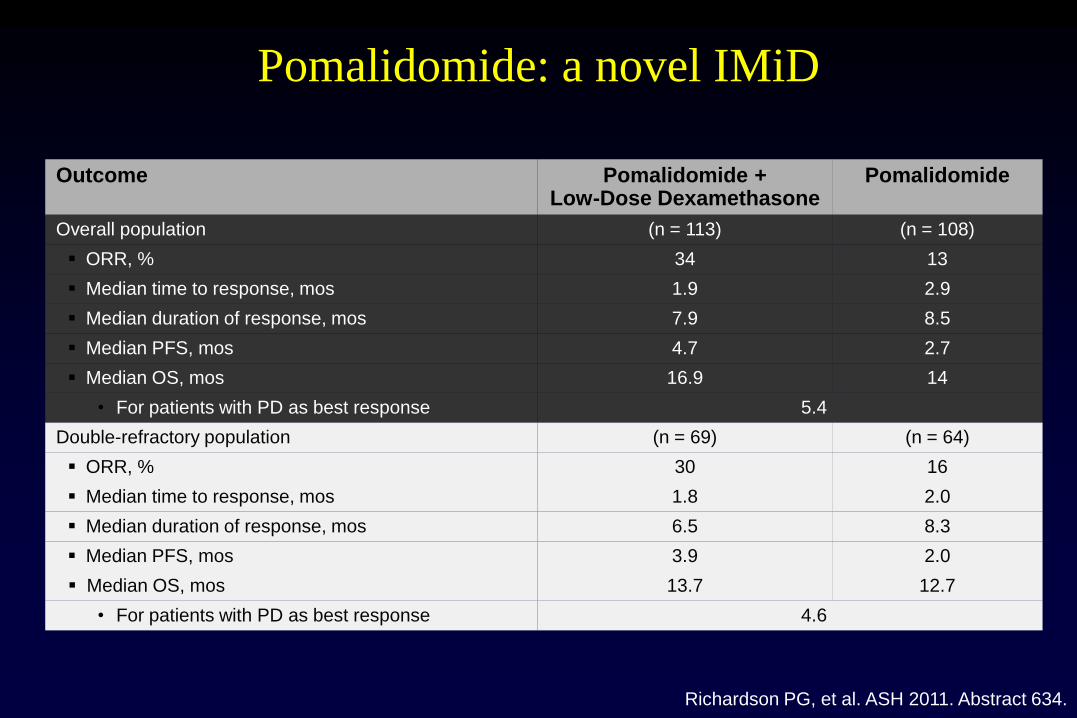
Pomalidomide: a novel IMiD
Richardson PG, et al. ASH 2011. Abstract 634.
Outcome Pomalidomide + Low-Dose Dexamethasone
Pomalidomide
Overall population (n = 113) (n = 108)
ORR, % 34 13
Median time to response, mos 1.9 2.9
Median duration of response, mos 7.9 8.5
Median PFS, mos 4.7 2.7
Median OS, mos 16.9 14
• For patients with PD as best response 5.4
Double-refractory population (n = 69) (n = 64)
ORR, % 30 16
Median time to response, mos 1.8 2.0
Median duration of response, mos 6.5 8.3
Median PFS, mos 3.9 2.0
Median OS, mos 13.7 12.7
• For patients with PD as best response 4.6
Page 43
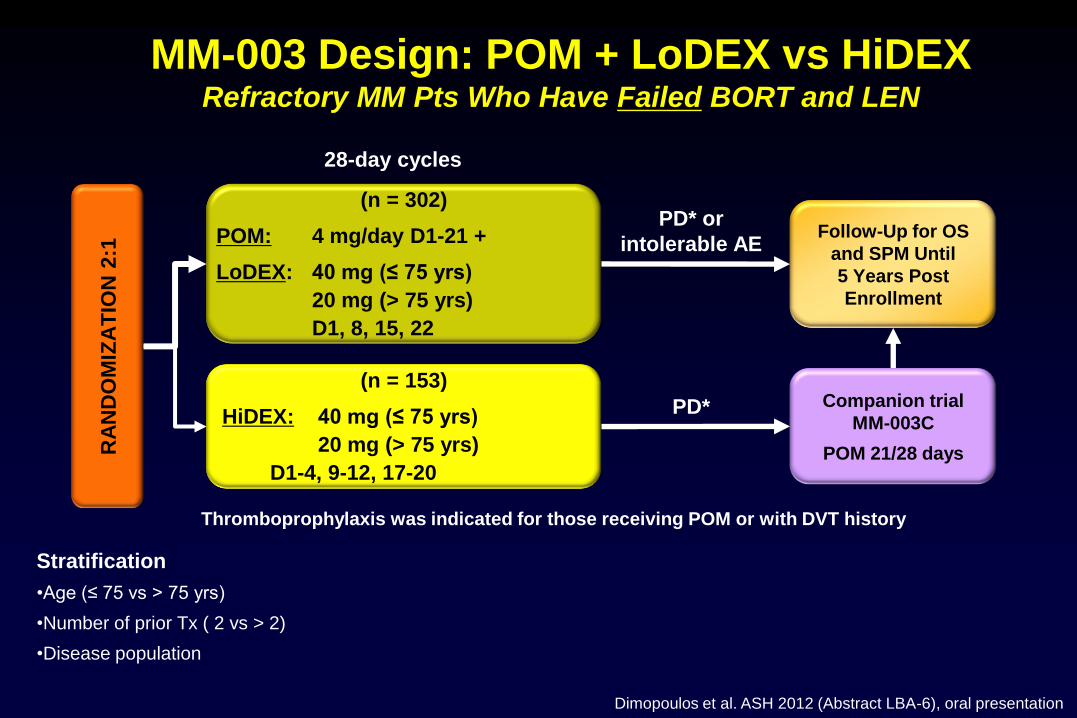
MM-003 Design: POM + LoDEX vs HiDEX Refractory MM Pts Who Have Failed BORT and LEN
(n = 302)
POM: 4 mg/day D1-21 +
LoDEX: 40 mg (≤ 75 yrs)
20 mg (> 75 yrs)
D1, 8, 15, 22
RA
ND
OM
IZA
TIO
N 2
:1 Follow-Up for OS
and SPM Until
5 Years Post
Enrollment
(n = 153)
HiDEX: 40 mg (≤ 75 yrs)
20 mg (> 75 yrs)
D1-4, 9-12, 17-20
28-day cycles
PD* or
intolerable AE
PD* Companion trial
MM-003C
POM 21/28 days
Stratification
•Age (≤ 75 vs > 75 yrs)
•Number of prior Tx ( 2 vs > 2)
•Disease population
Thromboprophylaxis was indicated for those receiving POM or with DVT history
Dimopoulos et al. ASH 2012 (Abstract LBA-6), oral presentation
Page 44
MM-003: Results
Figure 3: Ongoing Evaluation of Response by IRAC
POM + LoDEX
(n = 302)
HiDEX
(n = 153)
Resp
on
se (
%)
≥ PR = 21%
≥ MR = 37%
≥ PR = 3%
≥ MR = 8%
3
1
2
IRAC IRAC Randomized ≥ 6 Months
POM + LoDEX
(n = 204)
HiDEX
(n = 99)
≥ PR = 24%
≥ MR = 38%
3
Dimopoulos et al. IMW 2013 (Abstract 311)
Page 45
MM-003: Progression-Free Survival
0 4 8 12 16 0.0
0.2
0.4
0.6
0.8
1.0
Progression-Free Survival (months)
Pro
po
rtio
n o
f P
ati
ents
Median PFS
POM + LoDEX (n = 302) 3.6 months
HiDEX (n = 153) 1.8 months
HR = 0.45 P < .001
Dimopoulos et al. ASH 2012 (Abstract LBA-6), oral presentation
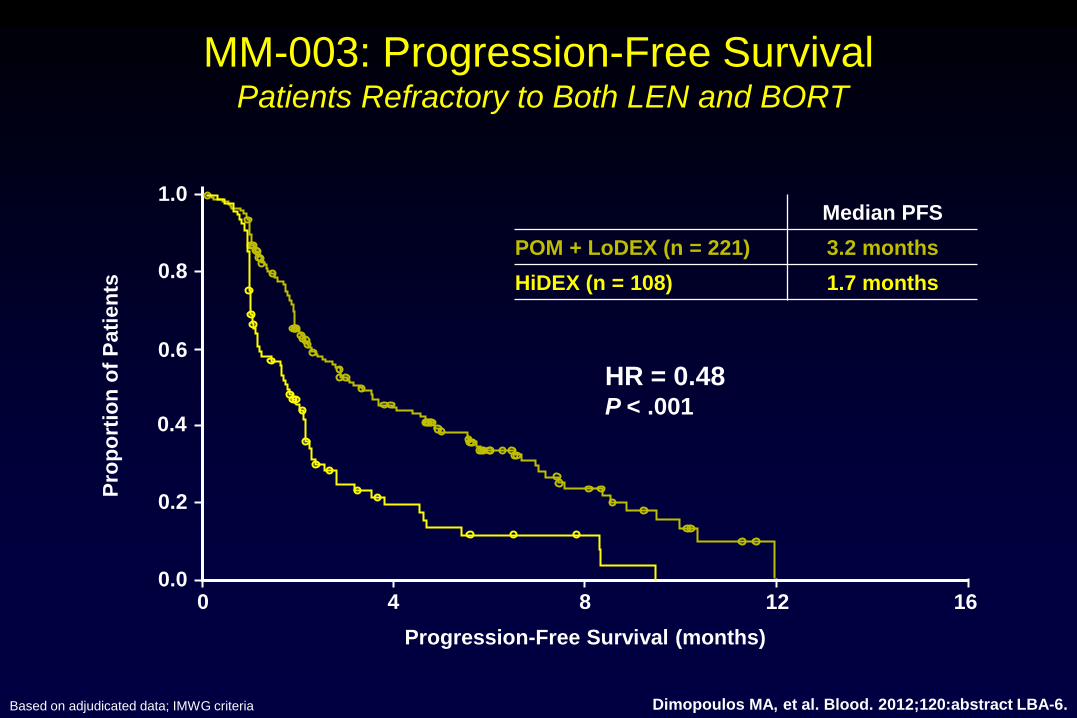
Page 46
MM-003: Progression-Free Survival Patients Refractory to Both LEN and BORT
Based on adjudicated data; IMWG criteria
Pro
po
rtio
n o
f P
ati
en
ts
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16
HR = 0.48 P < .001
Progression-Free Survival (months)
Median PFS
POM + LoDEX (n = 221) 3.2 months
HiDEX (n = 108) 1.7 months
Dimopoulos MA, et al. Blood. 2012;120:abstract LBA-6.
Page 47
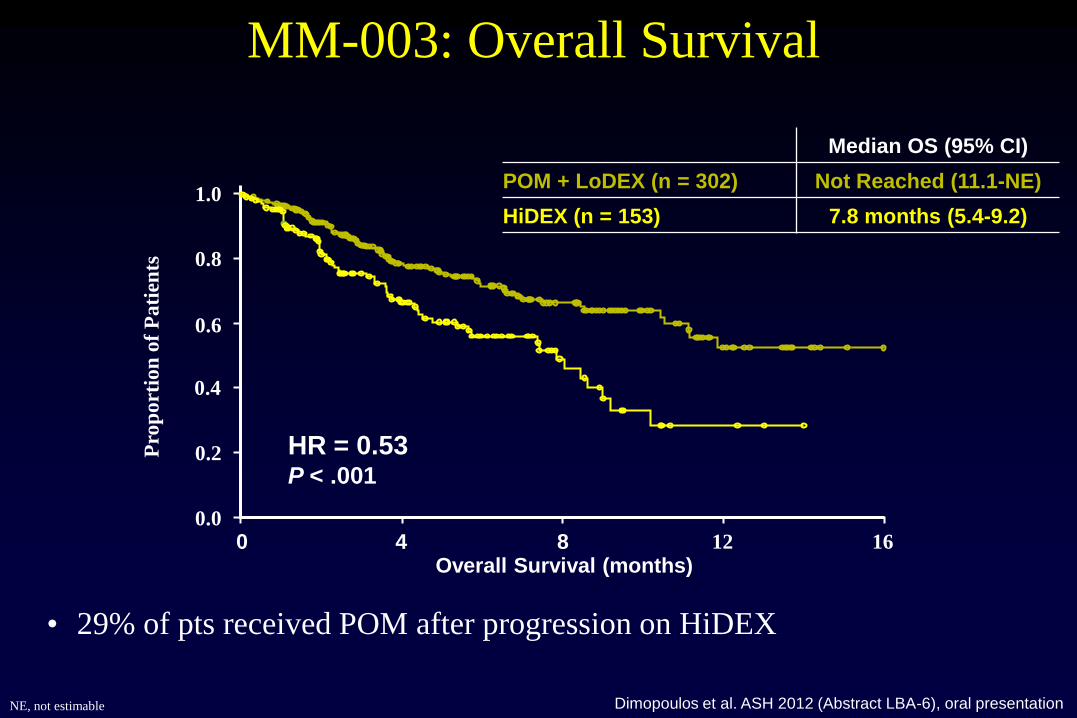
MM-003: Overall Survival
NE, not estimable
Overall Survival (months)
0.0
0.2
0.4
0.6
0.8
1.0
0 4 8 12 16
Pro
po
rtio
n o
f P
ati
ents
Median OS (95% CI)
POM + LoDEX (n = 302) Not Reached (11.1-NE)
HiDEX (n = 153) 7.8 months (5.4-9.2)
HR = 0.53 P < .001
• 29% of pts received POM after progression on HiDEX
Dimopoulos et al. ASH 2012 (Abstract LBA-6), oral presentation
Page 48
MM-003: Overall Survival Patients Refractory to Both LEN and BORT
0.0
0.2
0.4
0.6
0.8
1.0
Overall Survival (months) 0 4 8 12 16
Pro
po
rtio
n o
f P
ati
en
ts
HR = 0.56 P = .003
• 29% of pts received POM after progression on HiDEX
Median OS (95% CI)
POM + LoDEX (n = 221) Not Reached (8.5-NE)
HiDEX (n = 108) 7.4 months (4.3-9.2)
Dimopoulos MA, et al. Blood. 2012;120:abstract LBA-6.
Page 49
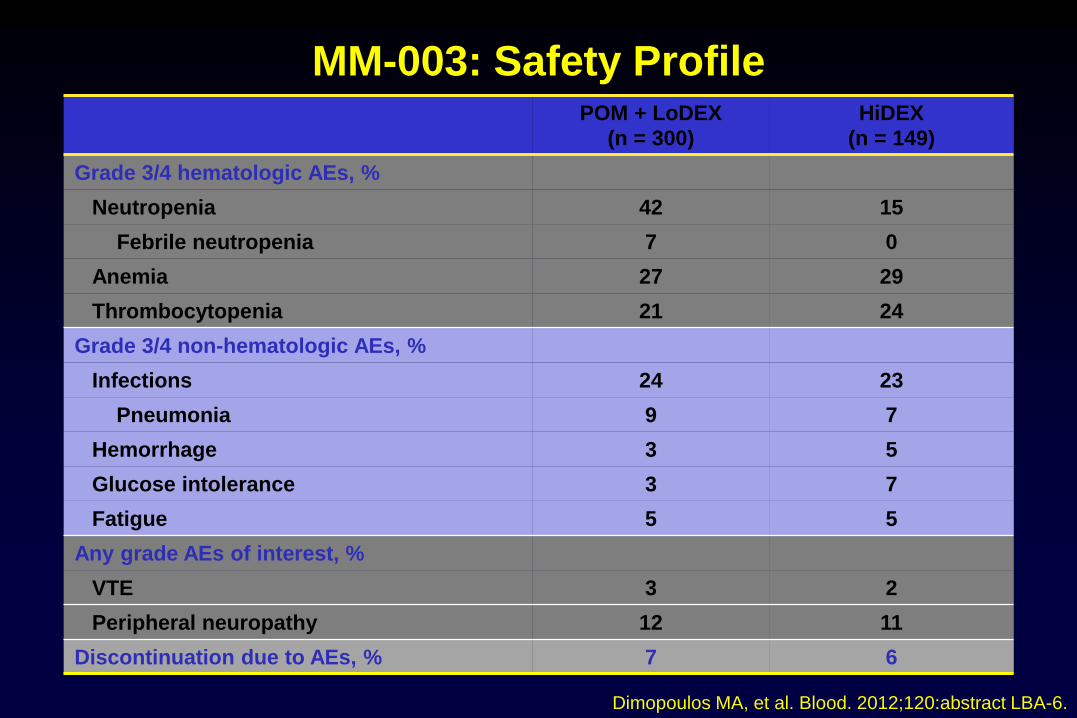
MM-003: Safety Profile POM + LoDEX
(n = 300)
HiDEX
(n = 149)
Grade 3/4 hematologic AEs, %
Neutropenia 42 15
Febrile neutropenia 7 0
Anemia 27 29
Thrombocytopenia 21 24
Grade 3/4 non-hematologic AEs, %
Infections 24 23
Pneumonia 9 7
Hemorrhage 3 5
Glucose intolerance 3 7
Fatigue 5 5
Any grade AEs of interest, %
VTE 3 2
Peripheral neuropathy 12 11
Discontinuation due to AEs, % 7 6
Dimopoulos MA, et al. Blood. 2012;120:abstract LBA-6.
Page 50
Carfilzomib
Trial N* Population Previous
Lines, n
ORR, % MR/SD% Median TTP,
Mos
003-A0[1]
39 Relapsed/
refractory
> 2 18 8/41 6.2
003-A1[2]
257 Relapsed/
refractory
≥ 2 24 12/-- --
004 (Bz exposed)[3] 35 Relapsed/
refractory
1-3 21 12/35 8.1
004 (Bz naive)[4] 20 mg/m2
20/27 mg/m2
59
67
Relapsed/
refractory
1-3 42
52
17/22
12/15
8.3
NR
006 (combo with len/dex)[5] 50 Relapsed/
refractory
1-3 78 2/8 --
Neuropathy from phase II experience
9.6% grades 1/2 and 1.4% grade 3
1. Jagannath S, et al. ASCO 2009. Abstract 8504. 2. Siegel DSD, et al. ASCO 2011. Abstract 8027. 3. Vij R, et al. ASCO 2010. Abstract
8000. 4. Vij R, et al. ASH 2011. Abstract 813. 5. Wang M, et al. ASCO 2011. Abstract 8025.
*Evaluable for response.
Page 51
PX-171-006: Phase II Trial of Carfilzomib
Plus Len/Dex in Relapsed/Refractory MM
Response (N = 51) n (%)
CR/nCR
VGPR
PR
MR
SD
ORR
12 (24)
9 (18)
19 (37)
1 (2)
3 (6)
40 (78)
Wang M, et al. ASCO 2011. Abstract 8025.
Week 1 Week 2 Week 3 Week 4: rest
Carfilzomib
20/27 mg/m2 IV*
Dexamethasone
40 mg/d PO
Lenalidomide D1-D21
25 mg/d PO
D1/D2 D8/D9 D15/D16
D1 D8 D15 D22
*20 mg/m2 cycle 1 days 1 and 2 only,
27 mg/m2 thereafter
Page 52
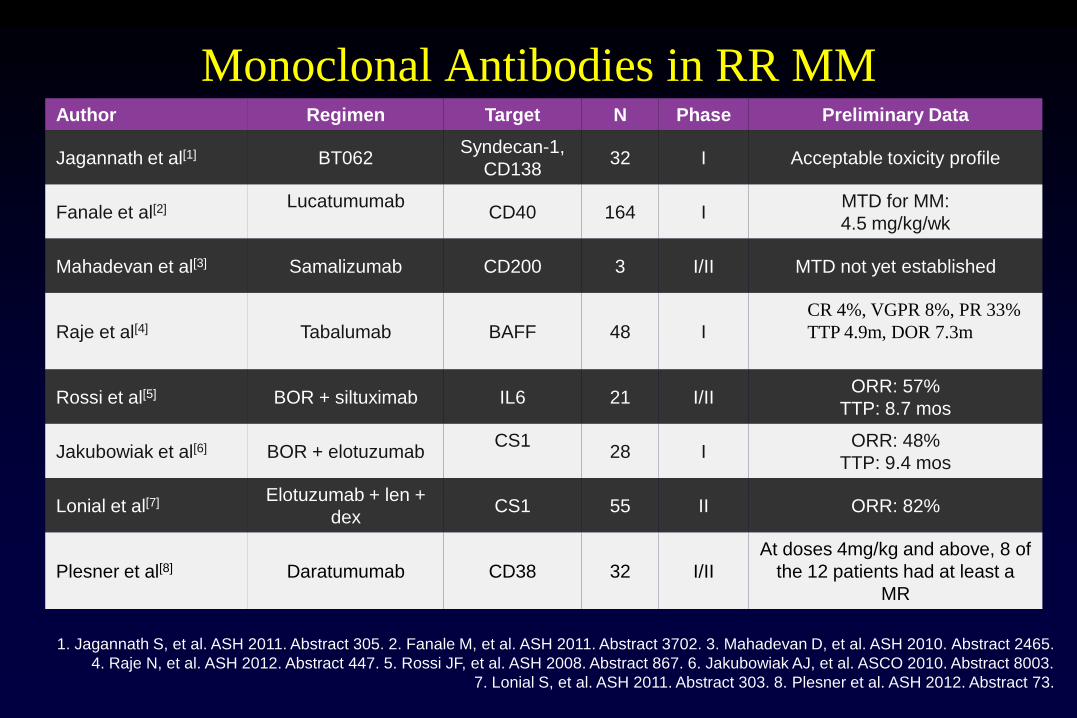
Monoclonal Antibodies in RR MM Author Regimen Target N Phase Preliminary Data
Jagannath et al[1] BT062 Syndecan-1,
CD138 32 I Acceptable toxicity profile
Fanale et al[2] Lucatumumab
CD40 164 I
MTD for MM:
4.5 mg/kg/wk
Mahadevan et al[3] Samalizumab CD200 3 I/II MTD not yet established
Raje et al[4] Tabalumab BAFF 48 I
CR 4%, VGPR 8%, PR 33%
TTP 4.9m, DOR 7.3m
Rossi et al[5] BOR + siltuximab IL6 21 I/II ORR: 57%
TTP: 8.7 mos
Jakubowiak et al[6] BOR + elotuzumab CS1
28 I
ORR: 48%
TTP: 9.4 mos
Lonial et al[7] Elotuzumab + len +
dex CS1 55 II ORR: 82%
Plesner et al[8] Daratumumab CD38 32 I/II
At doses 4mg/kg and above, 8 of
the 12 patients had at least a
MR
1. Jagannath S, et al. ASH 2011. Abstract 305. 2. Fanale M, et al. ASH 2011. Abstract 3702. 3. Mahadevan D, et al. ASH 2010. Abstract 2465.
4. Raje N, et al. ASH 2012. Abstract 447. 5. Rossi JF, et al. ASH 2008. Abstract 867. 6. Jakubowiak AJ, et al. ASCO 2010. Abstract 8003.
7. Lonial S, et al. ASH 2011. Abstract 303. 8. Plesner et al. ASH 2012. Abstract 73.
Page 53
Patient 3
0
5
10
15
20
25
Med
co
n
Con I
gG
SG
N-4
0
Len
alid
om
ide
S +
L
Tia YT, et al. Cancer Res. 2005;65:11712-11720.
Lenalidomide Can Enhance the efficacy
of Monoclonal Antibodies in Myeloma %
Spec
ific
Lysi
s
Medium
Control IgG
SGN-40
Lenalidomide
SGN-40 +
lenalidomide
Target: 12BM
E/T Ratio
% S
pe
cif
ic L
ys
is Target: 28BM
E/T Ratio
% S
pec
ific
Lys
is
0
15
30
45
60
2 5 10 40
0
15
30
45
60
2 5 10 40
A
B Patient 1
0 10 20 30 40 50 60
Med
con
Con I
gG
SG
N-4
0
Len
alid
om
ide
S +
L
Patient 2
0
10
20
30
40
50
* M
ed c
on
Con I
gG
SG
N-4
0
Len
alid
om
ide
S +
L
Page 54
Elotuzumab 10 mg/kg
Elotuzumab 20 mg/kg Total
Patients, n 36 37 73
ORR (≥PR), n (%) 33 (92) 28 (76) 61 (84)
CR/stringent CR, n (%) 5 (14) 4 (11) 9 (12)
VGPR, n (%) 17 (47)
14 (38) 31 (43)
PR, n (%) 11 (31) 10 (27) 21 (29)
<PR, n (%) 3 (8) 9 (24) 12 (16)
Efficacy: Best Response
Phase II (Study 1703)
1. Moreau P et al. J Clin Oncol 2012;Abstract 8020
• Overall median time to response: 1 mo (range, 0.7-19.2); 1 deepening response was observed in the 20mg/kg
arm since the previous data cut (April 27, 2012)1
• Overall median time to best response: 2.5 mo (range, 0.7-24.7)
• Median duration of objective response: 17.8 mo (range, 1.0-30.4)
Page 55
Progression Free Survival
Phase II (Study 1703)
At a median follow-up of 20.8 mo, median PFS has not been reached in the 10 mg/kg arm
– In the abstract, a preliminary median PFS of 26.9 mo was reported; however, no disease progression/death has been reported
since then; continued maturation of the results has increased the number of patients at risk post the preliminary median PFS (in
the denominator). Therefore, in this updated dataset the median has not been crossed
Median Time to Progression/Death:
10 mg/kg (n=36): not yet reached
20 mg/kg (n=37): 18.6 mo (95% CI 12.9-29.7)
0
10
20
30
40
50
60
70
80
90
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33
Months
Pro
po
rtio
n o
f
Pro
gre
ss
ion
Fre
e P
ati
en
ts (
%)
36 32 30 29 23 20 18 18 13 9 3 0
Number at Risk:
37 29 26 23 21 17 15 13 13 10 3 0
10 mg/kg
20 mg/kg
Page 56
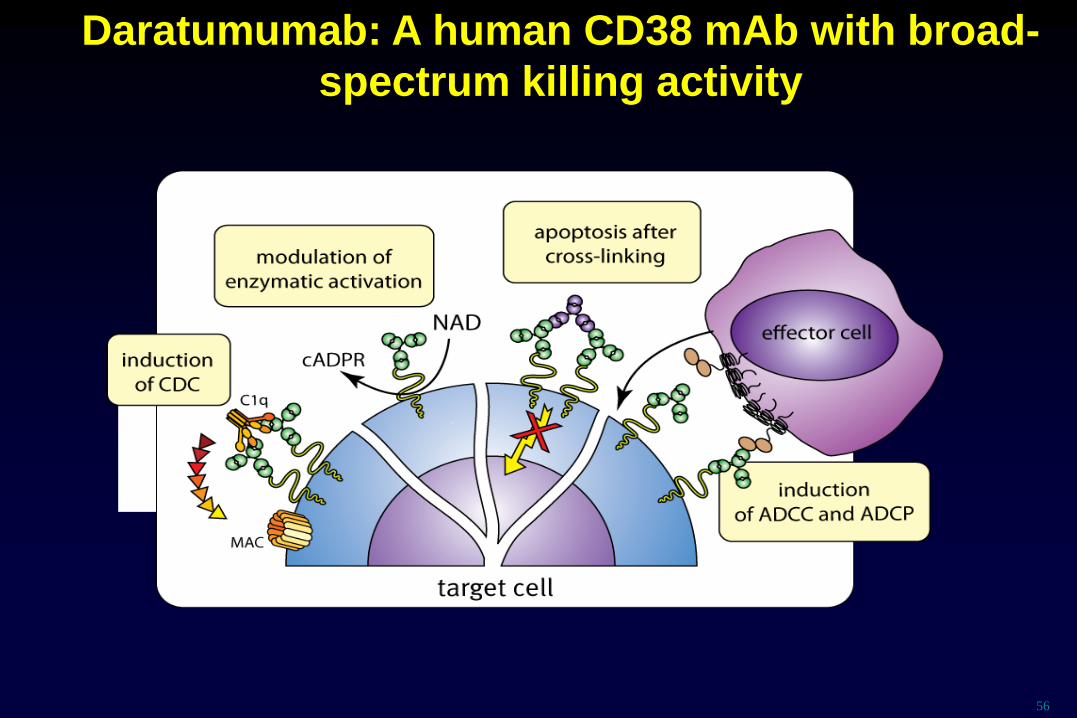
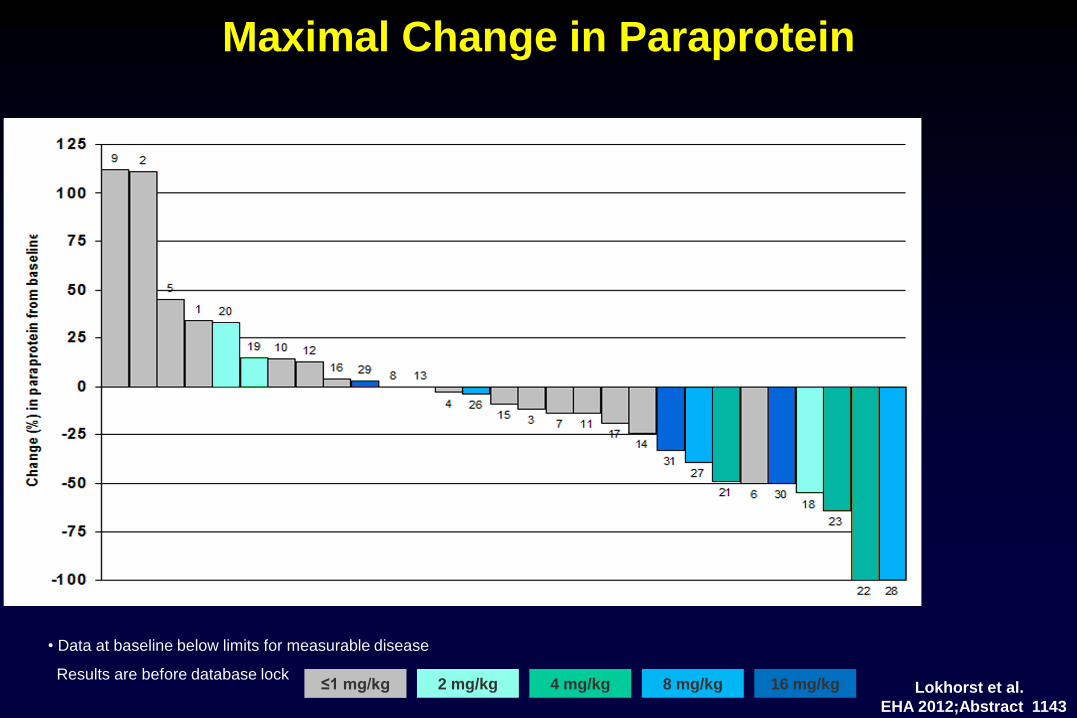
Daratumumab: A human CD38 mAb with broad-
spectrum killing activity
56
Page 57
Maximal Change in Paraprotein
≤1 mg/kg 2 mg/kg 4 mg/kg 8 mg/kg 16 mg/kg
• Data at baseline below limits for measurable disease
Results are before database lock
C* C A A A A A A A A
A A A A A A A A A B B B B C* C*
C
A A
C
Lokhorst et al.
EHA 2012;Abstract 1143
Page 58
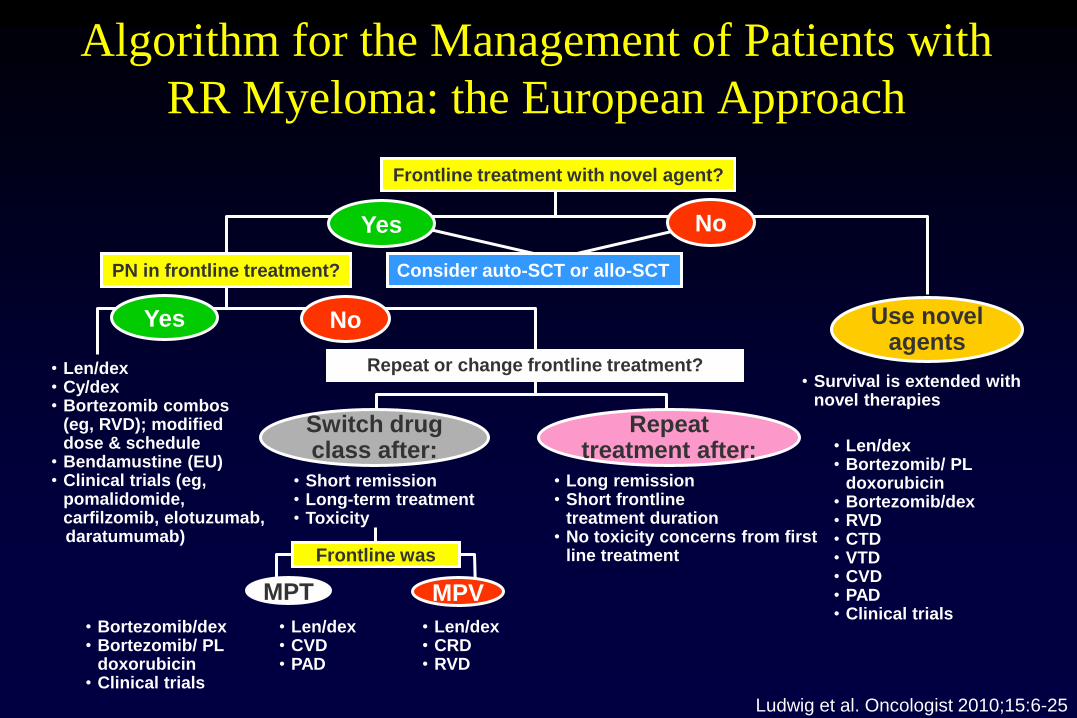
Algorithm for the Management of Patients with
RR Myeloma: the European Approach
Frontline treatment with novel agent?
PN in frontline treatment?
• Len/dex • Cy/dex • Bortezomib combos
(eg, RVD); modified dose & schedule
• Bendamustine (EU) • Clinical trials (eg,
pomalidomide, carfilzomib, elotuzumab,
daratumumab)
Repeat or change frontline treatment?
• Long remission • Short frontline
treatment duration • No toxicity concerns from first
line treatment
• Short remission • Long-term treatment • Toxicity
• Survival is extended with novel therapies
• Bortezomib/dex • Bortezomib/ PL
doxorubicin • Clinical trials
• Len/dex • CRD • RVD
Yes No
Yes No
Switch drug class after:
Repeat treatment after:
Use novel agents
MPT MPV
• Len/dex • Bortezomib/ PL
doxorubicin • Bortezomib/dex • RVD • CTD • VTD • CVD • PAD • Clinical trials
• Len/dex • CVD • PAD
Frontline was
Consider auto-SCT or allo-SCT
Ludwig et al. Oncologist 2010;15:6-25
Page 59
Conclusions
• The combination of lenalidomide and dexamethasone is associated with the
highest response and the longest TTP reported so far from large randomized
trials
• When lenalidomide and dexamethasone is administered as second-line
therapy, response rates are even higher and TTP is even longer
• Pomalidomide and carfilzomib may be effective in both bortezomib and
lenalidomide refractory patients.
• Novel monoclonal antibodies (daratumumab, elotuzumab) in combination
with PIs, IMiDs or conventional chemotherapy show promise for the
management of RR myeloma patients.