Chief Editor: Ahmad Husari Ethics Editor and Publisher: Ms Lesley Pocock medi+WORLD International Email: [email protected]Editorial enquiries: [email protected]Advertising enquiries: [email protected]While all efforts have been made to ensure the accuracy of the information in this journal, opinions expressed are those of the authors and do not necessarily reflect the views of The Publishers, Editor or the Editorial Board. The publishers, Editor and Editorial Board cannot be held responsible for errors or any consequences arising from the use of information contained in this journal; or the views and opinions expressed.Publication of any advertisements does not constitute any endorsement by the Publishers and Editors of the product advertised. The contents of this journal are copyright. Apart from any fair dealing for purposes of private study, research, criticism or review, as permitted under the Australian Copyright Act, no part of this program may be reproduced without the permission of the publisher. 2 Editorial Ahmad Husari Original Contribution / Clinical Investigation 3 Effectiveness of an Interventional Program for the Management of Hy- pertension through Strengthening of the Health Care Delivery System: a Pilot Study Waris Qidwai, Khawar Kazmi, Kashmira Nanji, Sana Anees 12 Acute chest syndrome does not have a chronic inflammatory background in sickle cell diseases Mehmet Rami Helvaci, Mustafa Sahan, Nesrin Atci, Orhan Ayyildiz, Orhan Ekrem Muftuoglu, Lesley Pocock 19 Splenomegaly in Patients with Sideropenic Anemias: Clinical and Hematologic Significance Safaa A. A. Khaled, �ehan S. Seifeldein �ehan S. Seifeldein Review Article 31 Update on the Use of Vitamin B12 in Management of pain Abdulrazak Abyad ISSN 1837 9052 August 2016 - Volume 9, Issue 2 nternal edicine Middle East Journal of Internal Medicine
Transcript
�
Chief Editor:Ahmad Husari
Ethics Editor and Publisher:Ms Lesley Pocockmedi+WORLD InternationalEmail: [email protected]
While all efforts have been made to ensure the accuracy of the information in this journal, opinions expressed are those of the authors and do not necessarily reflect the views of The Publishers, Editor or the Editorial Board. The publishers, Editor and Editorial Board cannot be held responsible for errors or any consequences arising from the use of information contained in this journal; or the views and opinions expressed.Publication of any advertisements does not constitute any endorsement by the Publishers and Editors of the product advertised.
The contents of this journal arecopyright. Apart from any fair dealing for purposes of private study, research, criticism or review, as permitted under the Australian Copyright Act, no part of this program may be reproduced without the permission of the publisher.
2 Editorial Ahmad Husari
Original Contribution / Clinical Investigation
3 Effectiveness of an Interventional Program for the Management of Hy-pertension through Strengthening of the Health Care Delivery System: a Pilot Study
Waris Qidwai, Khawar Kazmi, Kashmira Nanji, Sana Anees
12 Acute chest syndrome does not have a chronic inflammatory background in sickle cell diseases Mehmet Rami Helvaci, Mustafa Sahan, Nesrin Atci, Orhan Ayyildiz,
Orhan Ekrem Muftuoglu, Lesley Pocock
19 Splenomegaly in Patients with Sideropenic Anemias: Clinical and Hematologic Significance Safaa A. A. Khaled, �ehan S. Seifeldein�ehan S. Seifeldein
Review Article
31 Update on the Use of Vitamin B12 in Management of pain Abdulrazak Abyad
ISSN 1837 9052 August 2016 - Volume 9, Issue 2
nternal edicine
Middle East Journal of Internal Medicine
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 32
In this issue of the journal a number of issues are discussed including hypertension, sickle cell anemia, use of vitamin B12 and splenomegaly.
A paper from Pakistan attempts to assess the effectiveness of an interventional program to improve hypertension manage-ment through strengthening of the health care delivery system. A pilot study was conducted from February to December 2014 in two off-site Family Medicine clinics of the Aga Khan Hos-pital Karachi, Pakistan. Patients aged > 40 years, with known hypertension were included. At the intervention site, Family Physicians were trained; individual and group education ses-sions were conducted for catchment population, while usual care was provided at the control site. Referral system between primary, secondary and tertiary levels of care was strength-ened. Data was entered and analyzed in SPSS version 19. T-test for independent sample was used for comparison between in-tervention and control groups. 118 patients were recruited but 90 patients (44 intervention, 46 control group) were included in the final analysis. Mean age of patients in the intervention group was 50.5+ 8.7 years in comparison to 52.0 +8.3 years in the control group. A statistically significant mean difference was observed in systolic BP control in the intervention group (140.2 + 14.6 mm Hg) after a follow-up of six months. There was a significant difference in the mean scores of satisfaction levels between intervention (3.9 + 0.2) and control groups (3.7 + 0.2, P=0.003). Post intervention, 55% of patients in the inter-vention group and 39% in the control group were taking anti-hypertensive medications regularly. The authors concluded that intervention at primary care level along with strengthening of the health care delivery system should be undertaken to better manage hypertension.
A paper from Turkey looked at whether in sickle cell diseases Acute chest syndrome has a chronic inflammatory background. All patients with the SCDs were taken into the study. The study included 411 patients (199 females). As one of the significant endpoints of SCDs, patients with chronic obstructive pul-monary disease (COPD) and without were collected into two groups. There were 60 patients (14.5%) with COPD. Mean age (33.0 versus 29.5 years, P=0.005) and male ratio (80.0% ver-sus 46.7%, P<0.001) were higher in the COPD group. Smoking (36.6% versus 9.9%, P<0.001) and alcohol (3.3% versus 0.8%, P<0.05) were also higher among the COPD cases. Transfused red blood cell units in their lives (69.1 versus 32.9, P=0.001), priapism (10.0% versus 1.9%, P<0.001), leg ulcers (26.6% versus 11.6%, P<0.001), digital clubbing (25.0% versus 7.1%, P<0.001), coronary heart disease (26.6% versus 13.1%, P<0.01), chronic renal disease (16.6% versus 7.1%, P<0.01), and stroke (20.0% versus 7.9%, P<0.001) were all higher among the COPD cases, too. Interestingly, against the higher rates of above prob-lems in the COPD group, incidence of ACS was even lower among them, nonsignificantly (1.6% versus 3.9%, P>0.05). The authors concluded that SCDs cause severe chronic endothelial damage particularly at the capillary level, and terminate with accelerated atherosclerosis induced end-organ failures in early years of life. Probably ACS is a sudden onset event without any chronic inflammatory background in the SCDs.
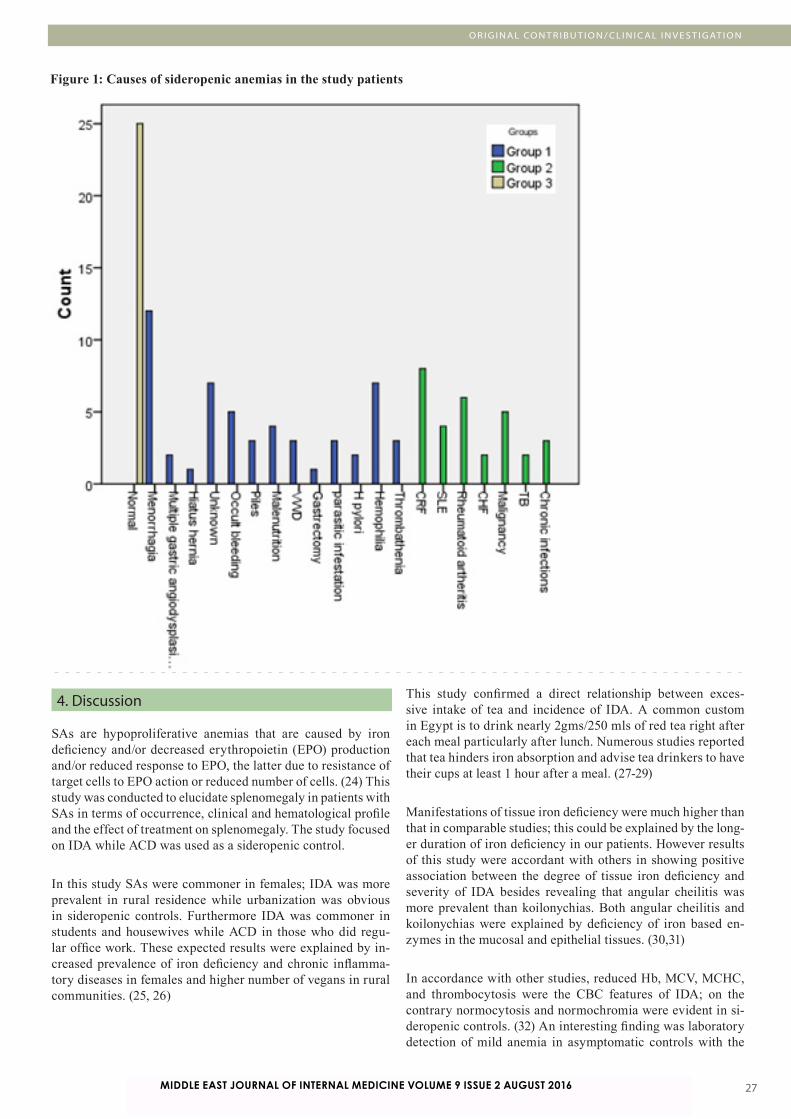
A paper from Egypt looked at clinical and hematologic signifi-cance of Splenomegaly in Patients with Sideropenic Anemias. A prospective study was conducted on 83 patients with SAs and 25 normal sex and age matched healthy controls. Patients’ demographic, clinical and hematologic data were collected through thorough history and clinical examination. Splenom-egaly was assessed with clinical examination of the study subjects and was graded with Hackett’s clinical grading, then confirmed with ultrasonographic examination. Patients were treated as per the published guidelines for treatment of SAs. Those with splenomegaly were subjected to a strict follow up plan. Analysis of the collected data showed that splenomegaly is of robust clinical and hematologic significance in patients with SAs.
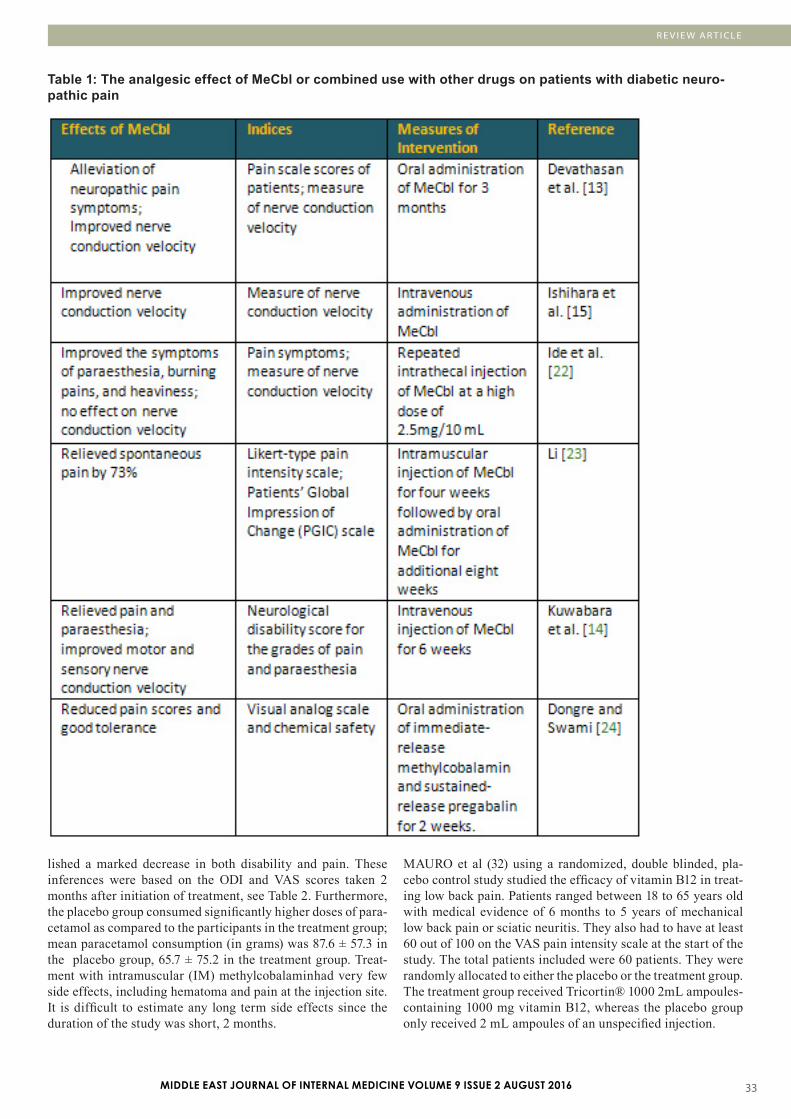
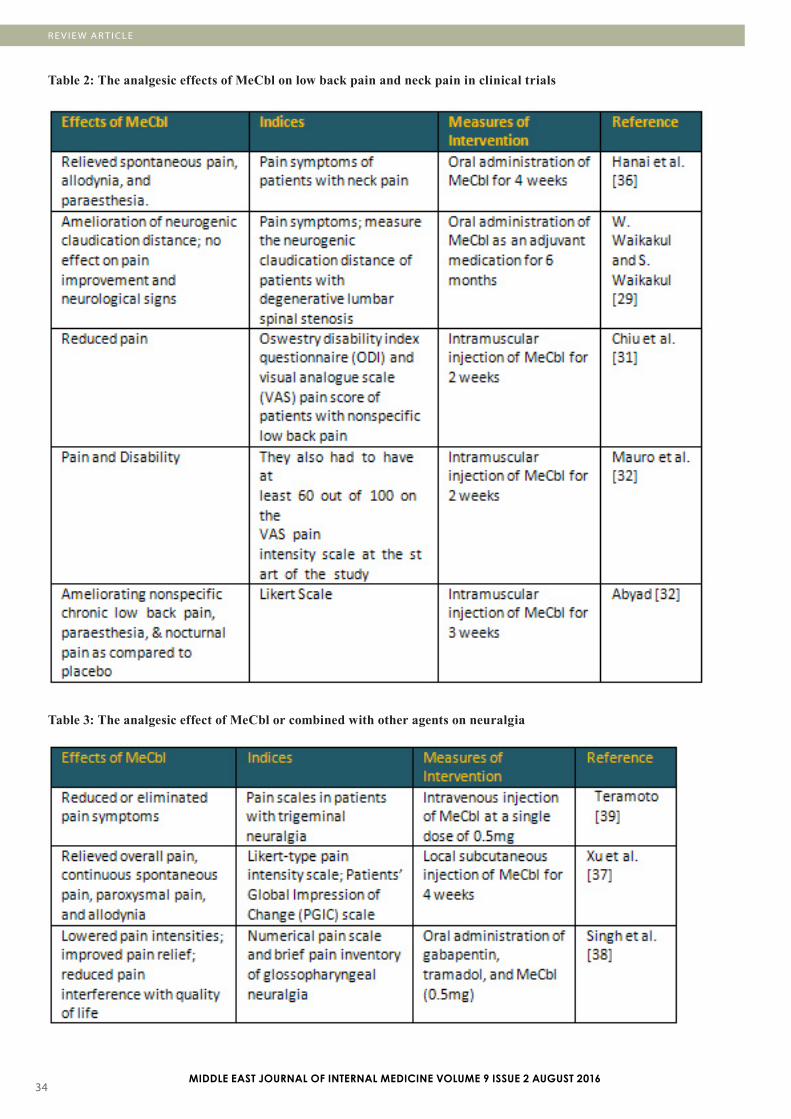
A paper from Lebanon looked at the use of Use of Vitamin B12 in Management of pain. Methylcobalamin (MeCbl), the activated form of vitamin B12, has been used to manage some nutritional diseases and other diseases in the clinic, including Alzheimer’s disease and rheumatoid arthritis. As an adjuvant, it effects neuronal protection by fostering regeneration of in-jured nerves and alienating glutamate-induced neurotoxicity. Recently several studies revealed that MeCbl may have con-ceivable analgesic effects in experimental and clinical studies. It can reduce pain behaviors in diabetic neuropathy, low back pain and neuralgia. MeCbl ameliorates nerve conduction, stim-ulates the regeneration of injured nerves, and inhibits ectopic spontaneous discharges of injured primary sensory neurons.
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 3MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Effectiveness of an Interventional Program for the Management of Hypertension through Strengthening of the Health Care Delivery System: a Pilot Study
(1) Dr. Waris Qidwai,Professor and ChairmanDepartment of Family Medicine, The Aga Khan University, Karachi(2) Dr. Khawar Kazmi, Professor of Cardiology Department of Medicine, Aga Khan University, Karachi(3) Kashmira Nanji, Senior Instructor (Research)Department of Family Medicine, Aga Khan University, Karachi(4) Sana Anees, Research Associate Department of Family Medicine, Aga Khan University, Karachi
Correspondence:Dr. Waris QidwaiThe Tajuddin Chatoor, Professor and ChairmanDepartment of Family Medicine, Aga Khan University, KarachiStadium Road, PO Box: 3500, Karachi-74800, PakistanTel: 92-21-3486-4842 (Office) 92-3332317836 (Cell)Email: [email protected]
ABSTRACT Background: The aim of the study was to assess the effectiveness of an interventional program to improve hy-pertension management through strengthening of the health care delivery system.
Methods: A pilot study was conducted from February to December 2014 in two off-site Family Medicine clinics of the Aga Khan Hospital Karachi, Pakistan. Patients aged > 40 years, with known hypertension were included. At the intervention site, Family Physicians were trained; individual and group education sessions were con-ducted for catchment population, while usual care was provided at the control site. Referral system between primary, secondary and tertiary levels of care was strengthened. Data was entered and analyzed in SPSS version 19. T-test for independent sample was used for comparison between intervention and control groups.
Results: 118 patients were recruited but 90 patients (44 intervention, 46 control group) were included in the final analysis. Mean age of patients in intervention group was 50.5+ 8.7 years in comparison to 52.0 +8.3 years in the control group. A statistically significant mean difference was observed in systolic BP control in the interven-tion group (140.2 + 14.6 mm Hg) after a follow-up of six months. There was a significant difference in the mean scores of satisfaction levels between intervention (3.9 + 0.2) and control groups (3.7 + 0.2, P=0.003). Post inter-vention, 55% of patients in the intervention group and 39% in the control group were taking antihypertensive medications regularly.
Conclusion: Intervention at primary care level along with strengthening of the health care delivery system should be undertaken to better manage hypertension.
Key words: Hypertension, Primary Care, Family Physician, Health Care System
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�
Introduction Hypertension is an emerging public health challenge globally; with an increasing prevalence in developing countries.(1) Adverse impact of huge disease burden, arising from hypertensive patients in developing countries, is made worse because of weak health care delivery and lack of resources. Despite such adverse condition awareness, treatment and control of blood pressure among hypertensive patients is improving in these countries.(2, 3)
Pakistan is a developing country and 33% of the adult population suffers from hypertension.(4) This huge disease burden puts immense pressure on limited resources. A recent study has reported blood pressure control in accordance to guidelines, among 30.8% of hypertensive patients in Pakistan.(5) An earlier study has reported younger age and poor awareness about hypertension as factors that adversely affect adherence to antihypertensive medication and blood pressure control among hypertensive patients in Pakistan.(6)
Primary care is the frontline of a health care delivery system where patients are screened and managed for hypertension. It has been shown that strengthening of primary care can result in better blood pressure control among hypertensive patients.(7) It has been reported that training of General Practitioners in management of hypertensive patients results in better blood pressure control among patients in their clinical care.(8)
Limited evidence is available from Pakistan on effectiveness of intervention aimed at strengthening the primary care and health care system to effectively control hypertension. Based on this identified need, we conducted a trial on effectiveness of strengthening the primary care and health care delivery system to effectively control hypertension.
Methods Study Settings:A quasi-experimental study was conducted in two off-site “Integrated Medical Services” Family Medicine clinics, Aga Khan University Hospital Karachi, Pakistan, from February 2014 to December 2014. Integrated Medical Services (IMS) are community based health care facilities that offer Family Medicine services in addition to diagnostic support.
Patients:Individuals aged 40 years or more, visiting the selected IMS centers with known hypertension or with consistently elevated BP on two separate visits (mean of last two of three measurements of systolic pressure > 140 mm Hg or mean diastolic pressure > 90 mm Hg) or already receiving treatment, were recruited in the study.
Those patients who require intensive care unit or coronary care unit admissions, or were diagnosed to have cognitive impairment, were agitated due to severe pain, non-resident of Karachi, or having language barrier were excluded from the study.
InterventionIntervention arm:Multiple interventions were used including training of family physicians, patient health education sessions and development of a referral system with secondary and tertiary levels of health care.
Training of Family Physician: Consultant Family Physicians conducted training sessions for Family Physicians regarding hypertension and they were given updated information for its management.
Patient Education Sessions: Patients in the intervention arm were provided with individual counseling during which the participants were given detailed information regarding their disease process, optimum blood pressure levels, lifestyle modification (exercise and diet) and importance of adherence to treatment. Participants were also given written brochures/pamphlets about hypertension management. The education session was conducted by a Research Medical Officer (RMO) who was trained for this task by a Consultant Physician. The Family Physician also provided customized education to patients according to their needs.
Initiating a Referral system (primary-secondary-tertiary) for hypertension management:Primary care: Patients with uncomplicated hypertension were managed by the Family Physician at the IMS clinics. Those with complicated hypertension such as with target organ damage, CVD, CKD or needing more than 3 drugs were referred for secondary care.
Secondary care: Community Health Center, Aga Khan University Hospital served as the secondary care service provider. Patients with CVD, CKD or needing more than 3 drugs, not responding to treatment, or patients with secondary hypertension were referred to tertiary care level.
Tertiary care: Cardiologist at AKU managed secondary, resistant and difficult to treat hypertension. The patients were then referred back to the Family Physician at primary care level.
Control Arm: Standard Care: Patients coming to the control clinic of IMS were given usual hypertension care received at the IMS centers.
Outcome Ascertainment:The primary outcome was to observe a difference of at least 20 points in the blood pressure levels among the intervention and control groups within 06 months of follow-up. The other secondary outcomes of this study were: adherence to life style modification (exercise, and medication) by the patients. Cost of hypertension treatment, this included: cost of medication (self-report by patient), cost of physician visit (clinic data), and cost of laboratory work. Patient Satisfaction to the care was inquired through PSQ-18. (9) It is a short form of the PSQ III which has
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 �
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
80 questions and includes seven dimensions of satisfaction that is general satisfaction, technical quality, interpersonal man-ner, communication, financial aspects, time spent with doctor, and accessibility and convenience.
Baseline Assessment: Baseline assessment included detailed history, physical examination, laboratory investigations and a care plan.
Follow up visits:At 3 and 6 months: Patients in both arms were reassessed at 03 and 06 months intervals and outcome assessment was car-ried out. The study covered anthropometric measurements, blood pressure assessment and lab investigations. Adherence to medications and life style modification (diet, exercise) were evaluated through self-report and counting of empty medica-tion blisters.
Questionnaire Development: The questionnaire was initially developed in English language and was then translated into local language and back translated in English. The consistency in the back translated questionnaire was checked by the princi-pal investigator/co-investigators, and any discrepancies found were removed.
Ethical Consideration: The study was reviewed and approved by the Ethical Review Committee of Aga Khan University. The trial was also registered at clinical trial.gov (NCT02186067).
Written Informed Consent was obtained from all participants after explaining to them about the study protocol. All study personnel were trained in procedures for maintaining patient confidentiality. No personal identifiers were used in any report or publication arising from this study.
Statistical Analysis: Sample Size: The study was designed to enroll 90 patients (45 patients in each group). This number of patients would provide the study with the ability to detect a 20 percent dif-ference among groups (treatment and control) in six months with a power of 80%. The proportion in the treatment group is assumed to be 0.60. The sample size was calculated using NCSS PASS.
Analysis: Data was entered and analyzed in SPSS version 19. For continuous variables (e.g. SBP, DBP) means with stand-ard deviations (SDs) were reported. For dichotomous data, we calculated proportions. Independent t-test was used to identify the difference in mean BP level among intervention and con-trol groups. Chi-square test was applied to observe effect of in-tervention on exercise habits and medication adherence. Items within each scale of PSQ 18 are averaged after scoring. These scale scores represent the average for all items in the scale that were answered. High scores on PSQ 18 reflect satisfaction with medical care. Intention to treat analysis was carried out for all participants.
Results
A total of 126 (intervention: 62, control: 64) patients were recruited at baseline, out of which 90 patients (44 interven-tion group, 46 control group) completed the study protocol and were included in the final analysis. The overall attrition rate was 29% in the control group and 19% in the intervention group (Figure 1 - next page).
The mean age of the participants in the intervention group was 50.5+ 8.7 years and 52.0 +8.3 years in the control group. The socio demographic characteristics of study participants are given in Table 1 (page 7). Both the study groups had prepon-derance of female participants (intervention: 61.4% v/s control: 69.6%). About 11% of the participants in the intervention group and 8.7% in the control group were unable to read or write. Over 80% of the participants in both the groups had family history of hypertension. Both the study groups were similar in terms of the demographic characteristics such as age, gender, educational status etc.
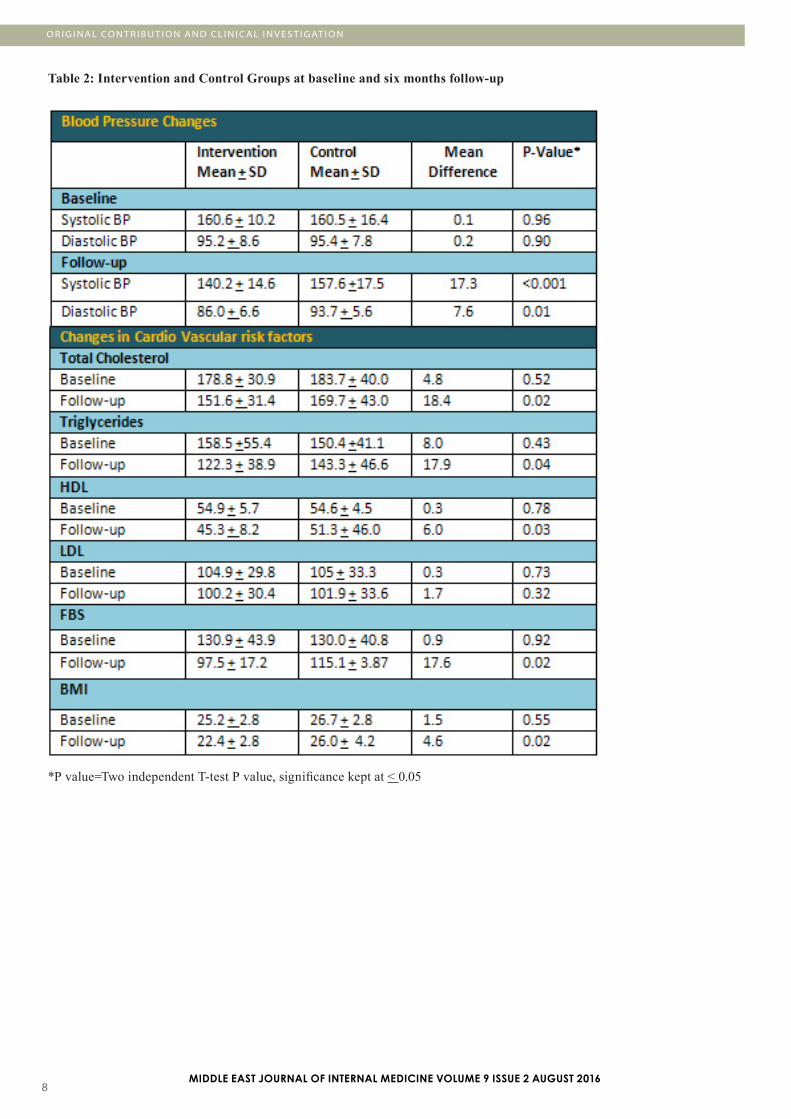
A statistically significant mean difference of 17.35 mm Hg was observed in systolic BP of intervention (140.2 + 14.6 mm Hg) and control group (157.6 + 17.5) after a follow-up of 06 months (Table 2 - page 8). Likewise a 7 point difference was observed in diastolic BP (intervention: 86.0 + 6.6). Changes in blood markers of blood pressure control at six months follow-up are presented in Table 2.
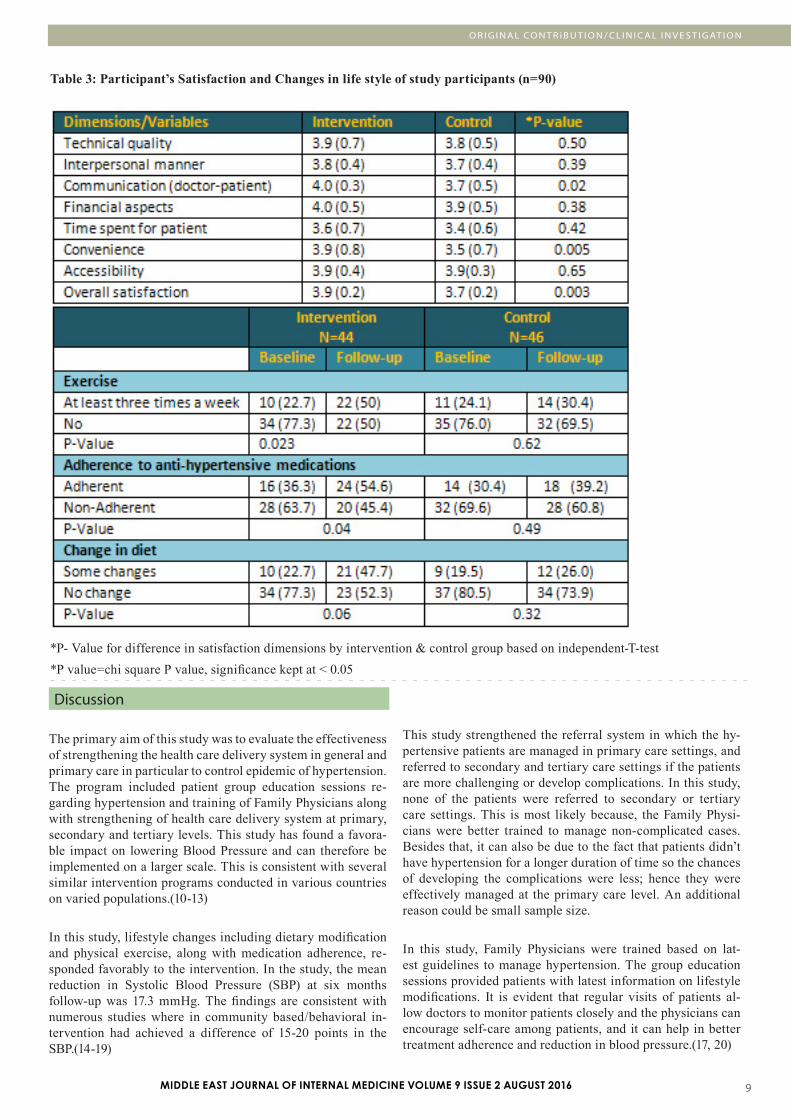
Satisfaction with services was assessed through PSQ-18 scale which has seven dimensions. There was a significant differ-ence in the mean scores of satisfaction levels between inter-vention (3.9 + 0.2) and control groups (3.7 + 0.2) with a P-value of 0.003 (Table 3) .
The average monthly cost of hypertension treatment was PKR.653 + 376 among the intervention and PKR.753 + 817 in the control group. This difference however, was not statisti-cally significant (P=0.45).
The majority (54.6%) of the patients in the intervention group were taking antihypertensive medications regularly, in com-parison to 39.2% of the patients in the control group (P=0.001). About 50% of the participants in the intervention group started some level of exercise (at least thrice a week for 30 minutes) after the intervention (Table 3 - page 9).
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
Figure 1: Flow of Study participants
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 �
O R I G I N A L CO N T R i B U T I O N / CL I N I C A L I N V E S T I G AT I O N
Table 1 : Descriptive Characteristics of Intervention and Control Groups
*P value=chi square P value, significance kept at < 0.05
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
Table 2: Intervention and Control Groups at baseline and six months follow-up
*P value=Two independent T-test P value, significance kept at < 0.05
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 �
O R I G I N A L CO N T R i B U T I O N / CL I N I C A L I N V E S T I G AT I O N
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Table 3: Participant’s Satisfaction and Changes in life style of study participants (n=90)
*P- Value for difference in satisfaction dimensions by intervention & control group based on independent-T-test*P value=chi square P value, significance kept at < 0.05
Discussion
The primary aim of this study was to evaluate the effectiveness of strengthening the health care delivery system in general and primary care in particular to control epidemic of hypertension. The program included patient group education sessions re-garding hypertension and training of Family Physicians along with strengthening of health care delivery system at primary, secondary and tertiary levels. This study has found a favora-ble impact on lowering Blood Pressure and can therefore be implemented on a larger scale. This is consistent with several similar intervention programs conducted in various countries on varied populations.(10-13)
In this study, lifestyle changes including dietary modification and physical exercise, along with medication adherence, re-sponded favorably to the intervention. In the study, the mean reduction in Systolic Blood Pressure (SBP) at six months follow-up was 17.3 mmHg. The findings are consistent with numerous studies where in community based/behavioral in-tervention had achieved a difference of 15-20 points in the SBP.(14-19)
This study strengthened the referral system in which the hy-pertensive patients are managed in primary care settings, and referred to secondary and tertiary care settings if the patients are more challenging or develop complications. In this study, none of the patients were referred to secondary or tertiary care settings. This is most likely because, the Family Physi-cians were better trained to manage non-complicated cases. Besides that, it can also be due to the fact that patients didn’t have hypertension for a longer duration of time so the chances of developing the complications were less; hence they were effectively managed at the primary care level. An additional reason could be small sample size.
In this study, Family Physicians were trained based on lat-est guidelines to manage hypertension. The group education sessions provided patients with latest information on lifestyle modifications. It is evident that regular visits of patients al-low doctors to monitor patients closely and the physicians can encourage self-care among patients, and it can help in better treatment adherence and reduction in blood pressure.(17, 20)
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�0
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
Repeated reminder calls for medication adherence and life style modifications have yielded the desired results observed at six months interval. Regular contact with physicians increases patients comfort level with doctors. This is consistent with our study wherein patients in the intervention group had higher satisfaction scores than control.
It is reported that weight loss leads to blood pressure reduc-tion on a long term basis.(21) In the current study; there was a significant improvement in Body Mass Index (BMI) levels post intervention. This adds to the favorable impact of weight management in the current study on blood pressure control.
Lack of adherence to medications is the common cause for un-controlled hypertension. Prevalence of non-adherence to hy-pertensive medication is demonstrated to be a significant for lack of control of blood pressure. (22) This study demonstrates positive impact of intervention that improves adherence to treatment with resultant favorable outcome on blood pressure control.
Significant results were observed in this study, however, the findings of this study should be interpreted cautiously as it was conducted in two study clinics located at a reasonable distance to one another and with less attrition rates observed as com-pared to other community based intervention trials. Moreover, the lack of blinding of patients and assessor could have resulted in more impact of intervention; as the patients in the interven-tion arm have received the best possible treatment. Moreover, the follow-up period of this study was only six months so we were unable to determine the long-term sustainability of BP and effect of the interventions on cardiovascular outcomes. Despite these limitations, there is evidence emerging from this pilot study that intervention at primary care level along with strengthening of the health care system results in better blood pressure control among patients with hypertension.
Conclusion
Hypertension can be effectively managed in the primary care setting through interventions even in developing countries with weak primary health care structure. Such intervention at primary care level along with strengthening of the health care system should be undertaken to better manage hypertension.
Acknowledgement:We are grateful to The Aga Khan University Research Council, for providing a grant to conduct this study. We are also grateful to the administration of two study clinics for their cooperation during the implementation of the study. We would also like to thank all the patients for giving their time to this project.
References
1. Temilolu Olayinka Aje, Michael Miller. Cardiovascular dis-ease: A global problem extending into the developing world. World J Cardiol. 2009 Dec 31; 1(1): 3-10.2. Ibrahim MM, Damasceno A. Hypertension in developing countries. The Lancet. 2013; 380(9841):611-9.3. Pereira M, Lunet N, Azevedo A, Barros H. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. Journal of hy-pertension. 2009; 27(5):963-75.4. Safdar NF, Bertone-Johnson ER, Cordeiro L, Jafar TH4, Co-hen NL. Dietary patterns and their association with hyperten-sion among Pakistani urban adults. Asia Pac J Clin Nutr. 2015; 24(4):710-95. Ragot S, Beneteau M, Guillou-Bonnici F, Herpin D. Preva-lence and management of hypertensive patients in clinical practice: Cross-sectional registry in five countries outside the European Union. Blood Pressure. 2016 Apr; 25(2):104-16.6. Hashmi SK, Afridi MB, Abbas K, Sajwani RA, Saleheen D, Frossard PM, et al. Factors associated with adherence to anti-hypertensive treatment in Pakistan. PLoS One. 2007; 2(3):e280.7. Feng YJ, Wang HC, Li YC, Zhao WH. Hypertension Screen-ing and Follow-up Management by Primary Health Care Sys-tem among Chinese Population Aged 35 Years and above. Bi-omed Environ Sci. 2015 May; 28(5):330-40.8. Jafar TH. Combined patient and GP training best for BP control in Pakistan. PharmacoEconomics & Outcomes News. 2011; 640:29.9. Stallard P. Validity and reliability of the Parent Satisfac-tion Questionnaire. British journal of clinical psychology. 1996;35(2):311-8.10. Rakotz MK, Ewigman BG, Sarav M, Ross RE, Robicsek A, Konchak CW, et al. A technology-based quality innovation to identify undiagnosed hypertension among active primary care patients. The Annals of Family Medicine. 2014; 12(4):352-8.11. Look ARG. Long term effects of a lifestyle intervention on weight and cardiovascular risk factors in individuals with type 2 diabetes: four year results of the Look AHEAD trial. Archives of internal medicine. 2010; 170(17):1566.12. Ogedegbe GO, Boutin-Foster C, Wells MT, Allegrante JP, Isen AM, Jobe JB, et al. A randomized controlled trial of posi-tive-affect intervention and medication adherence in hyperten-sive African Americans. Archives of internal medicine. 2012; 172(4):322-6.13. Stevens VJ, Corrigan SA, Obarzanek E, Bernauer E, Cook NR, Hebert P, et al. Weight loss intervention in phase 1 of the Trials of Hypertension Prevention. Archives of internal medi-cine. 1993; 153(7):849-58.14. Anchala R, Kaptoge S, Pant H, Di Angelantonio E, Franco OH, Prabhakaran D. Evaluation of Effectiveness and Cost-Ef-fectiveness of a Clinical Decision Support System in Managing Hypertension in Resource Constrained Primary Health Care Settings: Results From a Cluster Randomized Trial. Journal of the American Heart Association. 2015; 4(1):e001213.
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 ��
15. Appel LJ, Champagne CM, Harsha DW, Cooper LS, Obar-zanek E, Elmer PJ, et al. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA: Journal of the American Med-ical Association. JAMA. 2003; 289(16):2083-93 2003.16. Bosworth HB, Olsen MK, Neary A, Orr M, Grubber J, Svetkey L, et al. Take Control of Your Blood Pressure (TCYB) study: a multifactorial tailored behavioral and educational in-tervention for achieving blood pressure control. Patient educa-tion and counseling. 2008; 70(3):338-47.17. Aziz KU. Evolution of systemic hypertension in Pakistani population. Journal of the College of Physicians and Surgeons--Pakistan: JCPSP. 2015; 25(4):286-91.18. Hasandokht T, Farajzadegan Z, Siadat ZD, Paknahad Z, Rajati F. Lifestyle interventions for hypertension treatment among Iranian women in primary health-care settings: Results of a randomized controlled trial. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences. 2015; 20(1):54.19. Margolis KL, Asche SE, Bergdall AR, Dehmer SP, Maci-osek MV, Nyboer RA, et al. A Successful Multifaceted Trial to Improve Hypertension Control in Primary Care: Why Did it Work? Journal of general internal medicine. 2015:1-8.20. Gwadry-Sridhar FH, Manias E, Lal L, Salas M, Hughes DA, Ratzki-Leewing A, et al. Impact of interventions on medi-cation adherence and blood pressure control in patients with essential hypertension: a systematic review by the ISPOR med-ication adherence and persistence special interest group. Value in Health. 2013;16(5):863-71.21. Stevens VJ, Obarzanek E, Cook NR, Lee IM, Appel LJ, West DS, et al. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention phase II. Annals of internal medicine. 2001; 134(1):1-11.22. Raebel MA, Ellis JL, Carroll NM, Bayliss EA, McGinnis B, Schroeder EB, et al. Characteristics of patients with primary non-adherence to medications for hypertension, diabetes, and lipid disorders. Journal of general internal medicine. 2012; 27(1):57-64.
O R I G I N A L CO N T R i B U T I O N / CL I N I C A L I N V E S T I G AT I O N
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�2
Acute chest syndrome does not have a chronic inflammatory background in sickle cell diseases
Mehmet Rami Helvaci (1)Mustafa Sahan (2)Nesrin Atci (3)Orhan Ayyildiz (4)Orhan Ekrem Muftuoglu (4)Lesley Pocock (5)
(1) Medical Faculty of the Mustafa Kemal University, Antakya, Professor of Internal Medicine, M.D.(2) Medical Faculty of the Mustafa Kemal University, Antakya, Assistant Professor of Radiology, M.D.(3) Medical Faculty of the Dicle University, Diyarbakir, Professor of Internal Medicine, M.D.(4) medi+WORLD International, Australia
Correspondence:Mehmet Rami Helvaci, M.D.Medical Faculty of the Mustafa Kemal University,31100, Serinyol, Antakya, Hatay, TURKEYPhone: 00-90-326-2291000 (Internal 3399) Fax: 00-90-326-2455654 Email: [email protected]
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
ABSTRACT Background: Sickle cell diseases (SCDs) are chronic catastrophic processes on vascular endothelium initiating at birth all over the body. We tried to understand whether or not there is a chronic inflammatory background of acute chest syndrome (ACS) in the SCDs.
Methods: All patients with the SCDs were taken into the study.
Results: The study included 411 patients (199 females). As one of the significant endpoints of SCDs, patients with chronic obstructive pulmonary disease (COPD) and without were collected into two groups. There were 60 patients (14.5%) with COPD. Mean age (33.0 versus 29.5 years, P=0.005) and male ratio (80.0% versus 46.7%, P<0.001) were higher in the COPD group. Smoking (36.6% versus 9.9%, P<0.001) and alcohol (3.3% versus 0.8%, P<0.05) were also higher among the COPD cases. Transfused red blood cell units in their lives (69.1 versus 32.9, P=0.001), priapism (10.0% versus 1.9%, P<0.001), leg ulcers (26.6% versus 11.6%, P<0.001), digital clubbing (25.0% versus 7.1%, P<0.001), coronary heart disease (26.6% versus 13.1%, P<0.01), chronic renal disease (16.6% versus 7.1%, P<0.01), and stroke (20.0% versus 7.9%, P<0.001) were all higher among the COPD cases, too. Interestingly, against the higher rates of the above problems in the COPD group, inci-dence of ACS was even lower among them, nonsignificantly (1.6% versus 3.9%, P>0.05).
Conclusion: SCDs cause severe chronic endothelial damage particularly at the capillary level, and terminate with accelerated atherosclerosis induced end-organ failures in early years of life. Probably ACS is a sudden onset event without any chronic inflammatory background in the SCDs.
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 �3
Introduction Chronic endothelial damage may be the major cause of aging by causing disseminated tissue ischemia all over the body. For instance, cardiac cirrhosis develops due to the prolonged hepatic hypoxia in individuals with pulmonary and/or cardiac diseases. Probably whole afferent vasculature including capillaries are mainly involved in the process. Some of the well-known accelerators of the inflammatory process are physical inactivity, weight gain, smoking, and alcohol for the development of irreversible endpoints including obesity, hypertension (HT), diabetes mellitus (DM), cirrhosis, peripheric artery disease (PAD), chronic obstructive pulmonary disease (COPD), chronic renal disease (CRD), coronary heart disease (CHD), mesenteric ischemia, osteoporosis, and stroke, all of which terminate with early aging and death. They were researched under the title of metabolic syndrome in the literature, extensively (1, 2). Similarly, sickle cell diseases (SCDs) are the causes of severe chronic endothelial damage particularly at the capillary level. Hemoglobin S (HbS) causes loss of elastic and biconcave disc shaped structures of red blood cells (RBCs). Probably loss of elasticity instead of shape is the major problem since sickling is very rare in peripheric blood samples of patients with associated thalassemia minors, and human survival is not so affected in hereditary spherocytosis or elliptocytosis. Loss of elasticity is present in whole lifespan, but exaggerated with stresses induced increased metabolic rate of the body. The hard cells induce prolonged endothelial inflammation, edema, and fibrosis mainly at the capillary level and terminate with disseminated cellular hypoxia all over the body (3, 4). On the other hand, obvious vascular occlusions may not develop in greater vasculature due to their transport instead of distribution function for the hard cells. We tried to understand whether or not there is a chronic inflammatory background of acute chest syndrome (ACS) in the SCDs.
Material and Methods
The study was performed in the Medical Faculty of the Mustafa Kemal University between March 2007 and July 2015. All patients with SCDs were studied. The SCDs are diagnosed with hemoglobin electrophoresis performed via high performance liquid chromatography (HPLC). Medical histories including smoking habit, regular alcohol consumption, painful crises per year, transfused RBC units in their lives, surgical operations, priapism, leg ulcers, and stroke were learnt. Patients with a history of one pack-year were accepted as smokers, and one drink-year were accepted as drinkers. Cases with acute painful crisis or another inflammatory event were treated at first, and the laboratory tests and clinical measurements were performed on the silent phase. A check up procedure including serum iron, iron binding capacity, ferritin, creatinine, liver function tests, markers of hepatitis viruses A, B, and C and human immunodeficiency virus, a posterior-anterior chest x-ray film, an electrocardiogram, a Doppler echocardiogram both to evaluate cardiac walls and valves and to measure the systolic blood pressure (BP) of pulmonary artery, an abdominal ultrasonography, a computed tomography of brain, and a magnetic resonance imaging (MRI) of hips was performed. Other bones for avascular necrosis were scanned according to the patients’ complaints. Associated thalassemia minors were detected with serum iron, iron binding
capacity, ferritin, and hemoglobin electrophoresis performed via HPLC. The criterion for diagnosis of COPD is post-bronchodilator forced expiratory volume in one second/forced vital capacity of less than 70% (5). ACS is diagnosed clinically with the presence of new infiltrates on chest x-ray film, fever, cough, sputum production, dyspnea, or hypoxia (6). An x-ray film of abdomen in upright position was taken just in patients with abdominal distention or discomfort, vomiting, obstipation, or lack of bowel movement, and ileus was diagnosed with gaseous distention of isolated segments of bowel, vomiting, obstipation, cramps, and with the absence of peristaltic activity on the abdomen. Systolic BP of the pulmonary artery of 40 mmHg or higher is accepted as pulmonary hypertension (7). CRD is diagnosed with a persistent serum creatinine level of 1.3 mg/dL in males and 1.2 mg/dL in females. Cirrhosis is diagnosed with physical examination, hepatic function tests, ultrasonographic results, and tissue sample in case of indication. Digital clubbing is diagnosed with the ratio of distal phalangeal diameter to interphalangeal diameter which is greater than 1.0, and with the presence of Schamroth’s sign (8, 9). An exercise electrocardiogram is just performed in cases with an abnormal electrocardiogram and/or angina pectoris. Coronary angiography is taken just for the exercise electrocardiogram positive cases. So CHD was diagnosed either angiographically or with the Doppler echocardiographic findings as the movement disorders in the cardiac walls. Rheumatic heart disease is diagnosed with the echocardiographic findings, too. Avascular necrosis of bones is diagnosed by means of MRI (10). Stroke is diagnosed by the computed tomography of brain. Ophthalmologic examination was performed according to the patients’ complaints. Eventually as one of the significant endpoints of the SCDs, cases with COPD and without were collected into the two groups, and they were compared in between. Mann-Whitney U test, Independent-Samples t test, and comparison of proportions were used as the methods of statistical analyses.
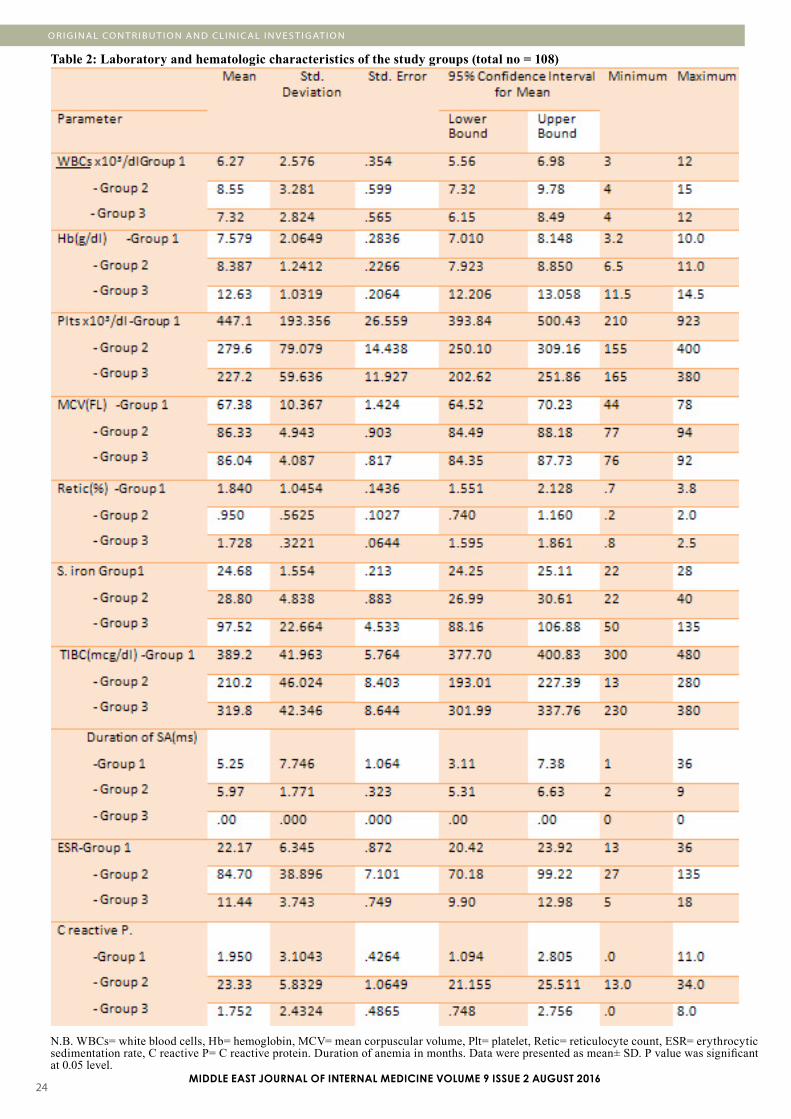
Results The study included 411 patients with SCDs (199 females and 212 males). There were 60 patients (14.5%) with COPD. Mean age (33.0 versus 29.5 years, P=0.005) and male ratio (80.0% versus 46.7%, P<0.001) were higher in the COPD group. Smoking (36.6% versus 9.9%, P<0.001) and alcohol (3.3% versus 0.8%, P<0.05) were also higher among the COPD cases. Prevalence of associated thalassemia minors were similar in both groups (71.6% versus 66.6% in the COPD group and other, respectively, P>0.05) (Table 1). Beside these, transfused RBC units in their lives (69.1 versus 32.9, P=0.001), priapism (10.0% versus 1.9%, P<0.001), leg ulcers (26.6% versus 11.6%, P<0.001), digital clubbing (25.0% versus 7.1%, P<0.001), CHD (26.6% versus 13.1%, P<0.01), CRD (16.6% versus 7.1%, P<0.01), and stroke (20.0% versus 7.9%, P<0.001) were all higher among the COPD cases. Interestingly, against the higher rates of above problems in the COPD group, incidence of ACS was even lower among them, nonsignificantly (1.6% versus 3.9%, P>0.05) (Table 2). The differences according to the mean white blood cell (WBC) count, hematocrit (Hct) value, and platelet (PLT) count of peripheric blood were nonsignificant between the two groups (Table 3). There were 27 mortalities (14 males) during the nine-year follow up period, and only two of them in the group without COPD were due to the ACS. The mean ages of mortality were
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3��
33.6 ± 9.5 years (range 19-47) in females and 30.8 ± 8.9 years (range 19-50) in males (P>0.05). On the other hand, there were three patients with sickle cell retinopathy; all of them were found in cases without COPD. Additionally, there were four patients with HBsAg positivity (0.9%) but HBV DNA was positive in none of them by polymerase chain reaction (PCR). Although antiHCV was positive in 6.0% (25) of the study cases, HCV RNA was detected as positive just in four (0.9%) by PCR.
Table 1: Characteristic features of the study cases
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 ��
Discussion
Chronic endothelial damage may be the most common type of vasculitis, and the leading cause of aging in human beings. Physical inactivity, weight gain, smoking, alcohol, prolonged infections, and chronic inflammatory processes such as SCDs, rheumatologic disorders, and cancers accelerate the process. Probably whole afferent vasculature including capillaries are mainly involved in the process. Much higher BP of the afferent vasculature may be the major underlying cause, and efferent endothelium are probably protected due to the much lower BP in them. Secondary to the chronic endothelial damage, inflam-mation, and fibrosis, vascular walls become thickened, their lumens are narrowed, and they lose their elastic natures that reduce the blood flow and increase BP further. Although early withdrawal of the causative factors may prevent terminal con-sequences, after development of cirrhosis, COPD, CRD, CHD, PAD, or stroke, the endothelial changes may not be reversed completely due to the fibrotic natures of them (11).
SCDs are life-threatening genetic disorders affecting around 100,000 individuals in the United States (12). As a difference from other causes of chronic endothelial damage, the SCDs may keep vascular endothelium particularly at the capillary level (13), since the capillary system is the main distributor of the hard RBCs to the tissues. The hard cells induced chronic endothelial damage, inflammation, edema, and fibrosis build up an advanced atherosclerosis in much younger ages of the patients. As a result, average lifespans of the patients were 48 years in females and 42 years in males in the literature (14), whereas they were 33.6 and 30.8 years in the present study, respectively. The great differences may be secondary to de-layed initiation of hydroxyurea therapy and inadequate RBC supports in severe crises in our country. On the other hand, longer lifespan of females with the SCDs (14) and longer over-all survival of females in the world (15) cannot be explained by the atherosclerotic effects of smoking and alcohol alone, instead it may be explained by more physical power requiring role of male sex in life that may terminate with an exaggerated sickling and/or atherosclerosis all over the body (16).
ACS is responsible for a considerable mortality in the SCDs (17). According to the literature, it occurs most often as a sin-gle episode, and a past history is associated with an early mor-tality. Similarly, all of 15 cases with ACS had only a single epi-sode, and two of them in the group without COPD were fatal in spite of rigorous RBC and ventilation support and antibiotic therapy in the present study. The remaining 13 patients are still alive without a recurrence at the end of the nine-year follow up period. ACS is most common between the ages of 2 to 4 years, and its incidence decreases with aging (18). Parallel to the knowledge, its incidence was only 3.6% among the patients with an average age of 30.0 ± 10.1 years (range 5-59) in the present study. The decreased incidence with aging may be due to a high mortality during the first episode and an acquired im-munity against various antigens with aging. On the other hand, ACS may also show inborn severity of the SCDs. For example, its incidence is higher in severe cases such as cases with sickle cell anemia (HbSS) and a higher WBC count (17, 18). Probably, ACS is a complex event, and the terminology of ‘ACS’ does not indicate a definite diagnosis but reflects clinical difficulty of defining a distinct etiology in the majority of such episodes. One of the major clinical problems lies in distinguishing be-tween infection and infarction, and in establishing clinical sig-nificance of fat embolism. For example, ACS did not show an infectious etiology in 66% of episodes in the above studies (17, 18). Similarly, 12 of 27 episodes of ACS had evidence of fat embolism as the cause in another study (19). But according to our nine-year experiences, the increased metabolic rate during infections may terminate with ACS. In other words, ACS may be a complex sequel characterized by disseminated endothelial damage and fat embolism at the capillary level, not in the pul-monary vasculature alone, instead all over the body. A prelimi-nary result from the Multi-Institutional Study of Hydroxyurea in the SCDs indicating a significant reduction of ACS episodes with hydroxyurea suggests that a substantial number of epi-sodes are secondary to capillary inflammation and edema (20). Similarly, we strongly recommend hydroxyurea therapy for all patients and that may also be a cause of the low incidence of ACS among our follow up cases. Additionally, some authors showed that antibiotics do not shorten the clinical course (21, 22), and RBC support must be given whenever there is evi-dence of clinical deterioration. RBC support has the obvious benefits of decreasing sickle cell concentration directly, and
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Table 3: Peripheric blood values of the study cases
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3��
suppressing bone marrow for production of the abnormal cells. So they prevent further sickling induced damage to the lungs and other organs. RBC support should be given early in the course since it has prophylactic benefit. According to our experiences, simple RBC transfusions are superior to exchange. First of all, preparation of one or two units of RBC suspensions each time, rather than preparation of six units or higher gives time to prepare more units by preventing sudden death of such cases. Secondly, transfusions of one or two units of RBC suspensions each time will decrease the severity of pain, and relax anxiety of the patients and their relatives in a short period of time. Thirdly, transfusion of RBC suspensions in secondary health centers may prevent some deaths that have developed during transport to tertiary centers for exchange.
COPD is the third leading cause of death with various underlying causes, worldwide (23). It is an inflammatory disease mainly affecting the pulmonary vasculature, and smoking, excess weight, and aging may be the major causes. As also seen in the present study, regular alcohol consumption may also take place in the inflammatory process. Similarly, COPD was one of the most frequent diagnoses in patients with alcohol dependence in another study (24). Additionally, 30-day readmission rate was higher in COPD patients with alcoholism (25). Probably the accelerated atherosclerotic process is the main structural background of functional changes characteristic of the disease. The endothelial process is enhanced by release of various chemicals by inflammatory cells, and terminates with atherosclerosis, fibrosis, and pulmonary losses. Although COPD may mainly be an accelerated atherosclerotic process of the pulmonary vasculature, there are several reports about coexistence of an associated endothelial inflammation all over the body (26, 27). For instance, it was shown in a previous study that there may be close relationships between COPD, CHD, PAD, and stroke (28). Similarly, two-thirds of mortality were caused by cardiovascular diseases and lung cancers, and CHD was the most common one among them in a multi-center study performed on 5,887 smokers (29). When the hospitalizations were researched, the most common causes were the cardiovascular diseases again (29). In another study, 27% of all mortality were due to the cardiovascular causes in the moderate and severe COPD patients (30). As also observed before (31), COPD may be one of the terminal endpoints of the SCDs due to the higher prevalence of priapism, leg ulcers, digital clubbing, CHD, CRD, and stroke in the SCDs cases with COPD.
Smoking may have a major role in systemic atherosclerotic processes such as COPD, digital clubbing, cirrhosis, CRD, PAD, CHD, stroke, and cancers (11, 32). Its atherosclerotic effects are the most obvious in Buerger’s disease and COPD. Buerger’s disease is an inflammatory process terminating with obliterative changes in small and medium-sized vessels, and it has never been reported in the absence of smoking. Smoking induced endothelial damage probably affects pulmonary vasculature much more than other organs due to the higher concentration of its products in the respiratory system. But it may even cause cirrhosis, CRD, PAD, CHD, stroke, and cancers with the transport of its products in the blood. COPD may also be accepted as a localized Buerger’s disease of the lungs. Beside the strong atherosclerotic effects, smoking in human beings and nicotine administration in animals may be associated with some
weight loss (33). There may be an increased energy expenditure during smoking (34), and nicotine may decrease caloric intake in a dose-related manner (35). Nicotine may lengthen intermeal time, and decrease amount of meal eaten (36). Body mass index (BMI) seems to be the highest in former, the lowest in current, and medium in never smokers (37). Similarly, smoking may also show the weakness of volition to control eating, and prevalences of HT, DM, and smoking were the highest in the highest triglyceride having group as a significant parameter of the metabolic syndrome (38). Additionally, although CHD was detected with similar prevalences in both sexes, smoking and COPD were higher in males against the higher prevalences of BMI and its consequences including dyslipidemia, HT, and DM in females (32). Probably tobacco smoke induced acute inflammation on vascular endothelium all over the body is the major cause of loss of appetite, since the body doesn’t want to eat during fighting. On the other hand, when we thought some antidepressant properties of smoking and alcohol, the higher prevalences of them in males may also indicate some additional stresses on male sex and shortened survival of them.
Digital changes may help to identify some systemic disorders in the body. For instance, digital clubbing is characterized by loss of normal <165° angle between the nailbed and fold, increased convexity of the nail fold, and thickening of the whole distal finger (39). Some authors found clubbing in 0.9% of all patients admitted to the department of internal medicine (8), whereas the prevalence was 4.2% in the same department in our university (11). The exact cause and significance is not known but chronic tissue hypoxia induced vasodilation and secretion of growth factors have been proposed (40-43). In the above study, only 40% of clubbing cases turned out to have significant underlying diseases while 60% remained well over the subsequent years (8). But according to our experiences, digital clubbing is frequently associated with smoking and pulmonary, cardiac, or hepatic disorders that are featuring with chronic tissue hypoxia. Lungs, heart, and liver are closely related organs that affect their functions in a short period of time. Similarly, digital clubbing may be an indicator of disseminated atherosclerosis particularly at the capillary level in the SCDs, and we observed clubbing in 9.7% of patients with the SCDs in the present study. In addition to the SCDs, the higher prevalences of smoking (P<0.001) and clubbing (P<0.001) in the COPD group may also indicate some additional roles of smoking and COPD on digital clubbing.
Leg ulcers are seen in 10 to 20% of patients with the SCDs (44), and the ratio was 13.8% in the present study. The incidence increases with age, and they are also common in HbSS cases and in males (44). Similarly, leg ulcers were found as 19.3% in males versus 8.0% in females (P<0.001) in the present study. Beside that, mean ages of the patients with leg ulcers were higher than the patients without (34.8 versus 29.2 years, P<0.000). The leg ulcers have an intractable nature, and around 97% of healed ulcers relapse in a period of one year (45). As a proof of their atherosclerotic natures, the leg ulcers occur in distal areas with less collateral blood flow in the body (45). The hard RBCs induced chronic endothelial damage particularly at the capillary level may be the major cause in the SCDs (44). Prolonged exposure to the hard cells due to blood pooling in the lower extremities may also explain the leg but not arm ulcers in the SCDs. As also detected in venous ulcers of the legs, venous
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 ��MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
insufficiency may also accelerate the process by causing pool-ing of causative hard cells in the legs. Probably pooling of blood in the lower extremities may also have effects in the diabetic ulcers, Buerger’s disease, digital clubbing, and onychomyco-sis. Beside the hard cells, smoking and alcohol may also have some additional effects for the leg ulcers since both of them are much more common in males, and their atherosclerotic effects are more obvious in COPD, Buerger’s disease, and cirrhosis (44). According to our experiences, prolonged resolution of leg ulcers with hydroxyurea may also suggest that they may be secondary to increased WBC and PLT counts induced dissemi-nated endothelial inflammation and edema particularly at the capillary level.
Stroke is also a common complication of the SCDs (46). Simi-lar to the ACS and leg ulcers, it is more common in the HbSS cases and in cases with a higher WBC count (47, 48). Sickling induced disseminated endothelial damage and activations of WBC and PLTs may terminate with chronic endothelial in-flammation, edema, and fibrosis in the brain (49). Stroke of the SCDs may not have a macrovascular origin instead dissemi-nated endothelial inflammation and edema may be much more prominent at the capillary level. Infections, inflammations, and various stresses may precipitate stroke since increased metabolic rate during such events may precipitate sickling and endothelial edema. Similar to the ACS and leg ulcers, a sig-nificant reduction of stroke with hydroxyurea may also suggest that a significant proportion of stroke is secondary to increased WBC and PLT counts induced disseminated endothelial edema in the diseases (13, 20).
As a conclusion, SCDs cause severe chronic endothelial damage particularly at the capillary level, and terminate with accelerated atherosclerosis induced end-organ failures in early years of life. Probably ACS is a sudden onset event without any chronic inflammatory background in the SCDs.
References
1. Eckel RH, Grundy SM, Zimmet PZ. The metabolic syn-drome. Lancet 2005; 365: 1415-1428.2. Helvaci MR, Kaya H, Seyhanli M, Yalcin A. White coat hypertension in definition of metabolic syndrome. Int Heart J 2008; 49: 449-457.3. Helvaci MR, Aydogan A, Akkucuk S, Oruc C, Ugur M. Sickle cell diseases and ileus. Int J Clin Exp Med 2014; 7: 2871-2876.4. Helvaci MR, Acipayam C, Aydogan A, Akkucuk S, Oruc C, Gokce C. Acute chest syndrome in severity of sickle cell diseases. Int J Clin Exp Med 2014; 7: 5790-5795.5. Global strategy for the diagnosis, management and preven-tion of chronic obstructive pulmonary disease 2010. Global ini-tiative for chronic obstructive lung disease (GOLD).6. Castro O, Brambilla DJ, Thorington B, Reindorf CA, Scott RB, Gillette P, et al. The acute chest syndrome in sickle cell disease: incidence and risk factors. The Cooperative Study of Sickle Cell Disease. Blood 1994; 84: 643-649.7. Fisher MR, Forfia PR, Chamera E, Housten-Harris T, Cham-
pion HC, Girgis RE, et al. Accuracy of Doppler echocardiogra-phy in the hemodynamic assessment of pulmonary hyperten-sion. Am J Respir Crit Care Med 2009; 179: 615-621.8. Vandemergel X, Renneboog B. Prevalence, aetiologies and significance of clubbing in a department of general internal medicine. Eur J Intern Med 2008; 19: 325-329.9. Schamroth L. Personal experience. S Afr Med J 1976; 50: 297-300.10. Mankad VN, Williams JP, Harpen MD, Manci E, Longenecker G, Moore RB, et al. Magnetic resonance imaging of bone marrow in sickle cell disease: clinical, hematologic, and pathologic correlations. Blood 1990; 75: 274-283.11. Helvaci MR, Aydin LY, Aydin Y. Digital clubbing may be an indicator of systemic atherosclerosis even at microvascular level. HealthMED 2012; 6: 3977-3981.12. Yawn BP, Buchanan GR, Afenyi-Annan AN, Ballas SK, Hassell KL, James AH, et al. Management of sickle cell dis-ease: summary of the 2014 evidence-based report by expert panel members. JAMA 2014; 312: 1033-1048.13. Helvaci MR, Aydin Y, Ayyildiz O. Hydroxyurea may pro-long survival of sickle cell patients by decreasing frequency of painful crises. HealthMED 2013; 7: 2327-2332.14. Platt OS, Brambilla DJ, Rosse WF, Milner PF, Castro O, Steinberg MH, et al. Mortality in sickle cell disease. Life ex-pectancy and risk factors for early death. N Engl J Med 1994; 330: 1639-1644.15. Mathers CD, Sadana R, Salomon JA, Murray CJ, Lopez AD. Healthy life expectancy in 191 countries, 1999. Lancet 2001; 357: 1685-1691.16. Helvaci MR, Ayyildiz O, Gundogdu M. Gender differences in severity of sickle cell diseases in non-smokers. Pak J Med Sci 2013; 29: 1050-1054.17. Poncz M, Kane E, Gill FM. Acute chest syndrome in sickle cell disease: etiology and clinical correlates. J Pediatr 1985; 107: 861-866.18. Sprinkle RH, Cole T, Smith S, Buchanan GR. Acute chest syndrome in children with sickle cell disease. A retrospective analysis of 100 hospitalized cases. Am J Pediatr Hematol On-col 1986; 8: 105-110.19. Vichinsky E, Williams R, Das M, Earles AN, Lewis N, Adler A, et al. Pulmonary fat embolism: a distinct cause of severe acute chest syndrome in sickle cell anemia. Blood 1994; 83: 3107-3112.20. Charache S, Terrin ML, Moore RD, Dover GJ, Barton FB, Eckert SV, et al. Effect of hydroxyurea on the frequency of painful crises in sickle cell anemia. Investigators of the Multi-center Study of Hydroxyurea in Sickle Cell Anemia. N Engl J Med 1995; 332: 1317-1322.21. Charache S, Scott JC, Charache P. ‘’Acute chest syndrome’’ in adults with sickle cell anemia. Microbiology, treatment, and prevention. Arch Intern Med 1979; 139: 67-69.22. Davies SC, Luce PJ, Win AA, Riordan JF, Brozovic M. Acute chest syndrome in sickle-cell disease. Lancet 1984; 1: 36-38.23. Rennard SI, Drummond MB. Early chronic obstructive pulmonary disease: definition, assessment, and prevention.
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3��
Lancet 2015; 385: 1778-1788.24. Schoepf D, Heun R. Alcohol dependence and physical comorbidity: Increased prevalence but reduced relevance of individual comorbidities for hospital-based mortality during a 12.5-year observation period in general hospital admissions in urban North-West England. Eur Psychiatry 2015; 30: 459-468.25. Singh G, Zhang W, Kuo YF, Sharma G. Association of Psychological Disorders With 30-Day Readmission Rates in Patients With COPD. Chest 2016; 149: 905-915.26. Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA 1998; 279: 1477-1482.27. Mannino DM, Watt G, Hole D, Gillis C, Hart C, McConnachie A, et al. The natural history of chronic obstructive pulmonary disease. Eur Respir J 2006; 27: 627-643.28. Mapel DW, Hurley JS, Frost FJ, Petersen HV, Picchi MA, Coultas DB. Health care utilization in chronic obstructive pulmonary disease. A case-control study in a health maintenance organization. Arch Intern Med 2000; 160: 2653-2658.29. Anthonisen NR, Connett JE, Enright PL, Manfreda J; Lung Health Study Research Group. Hospitalizations and mortality in the Lung Health Study. Am J Respir Crit Care Med 2002; 166: 333-339.30. McGarvey LP, John M, Anderson JA, Zvarich M, Wise RA; TORCH Clinical Endpoint Committee. Ascertainment of cause-specific mortality in COPD: operations of the TORCH Clinical Endpoint Committee. Thorax 2007; 62: 411-415.31. Helvaci MR, Erden ES, Aydin LY. Atherosclerotic background of chronic obstructive pulmonary disease in sickle cell patients. HealthMED 2013; 7: 484-488.32. Helvaci MR, Aydin Y, Gundogdu M. Smoking induced atherosclerosis in cancers. HealthMED 2012; 6: 3744-3749.33. Grunberg NE, Greenwood MR, Collins F, Epstein LH, Hatsukami D, Niaura R, et al. National working conference on smoking and body weight. Task Force 1: Mechanisms relevant to the relations between cigarette smoking and body weight. Health Psychol 1992; 11: 4-9.34. Walker JF, Collins LC, Rowell PP, Goldsmith LJ, Moffatt RJ, Stamford BA. The effect of smoking on energy expenditure and plasma catecholamine and nicotine levels during light physical activity. Nicotine Tob Res 1999; 1: 365-370.35. Hughes JR, Hatsukami DK. Effects of three doses of transdermal nicotine on post-cessation eating, hunger and weight. J Subst Abuse 1997; 9: 151-159.36. Miyata G, Meguid MM, Varma M, Fetissov SO, Kim HJ. Nicotine alters the usual reciprocity between meal size and meal number in female rat. Physiol Behav 2001; 74: 169-176.37. Laaksonen M, Rahkonen O, Prattala R. Smoking status and relative weight by educational level in Finland, 1978-1995. Prev Med 1998; 27: 431-437.38. Helvaci MR, Kaya H, Gundogdu M. Association of increased triglyceride levels in metabolic syndrome with coronary artery disease. Pak J Med Sci 2010; 26: 667-672.39. Myers KA, Farquhar DR. The rational clinical examination. Does this patient have clubbing? JAMA 2001; 286: 341-347.40. Uppal S, Diggle CP, Carr IM, Fishwick CW, Ahmed M, Ibrahim GH, et al. Mutations in 15-hydroxyprostaglandin dehydrogenase cause primary hypertrophic osteoarthropathy. Nat Genet 2008; 40: 789-793.
41. Toovey OT, Eisenhauer HJ. A new hypothesis on the mechanism of digital clubbing secondary to pulmonary pathologies. Med Hypotheses 2010; 75: 511-513.42. Alam MT, Sheikh SS, Aziz S, Masroor M. An unusual side effect of interferon alfa 2A: digital clubbing. J Ayub Med Coll Abbottabad 2008; 20: 165-166.43. Fomin VV, Popova EN, Burnevich EZ, Kuznetsova AV. Hippocratic fingers: clinical importance and differential diagnosis. Klin Med (Mosk) 2007; 85: 64-68.44. Minniti CP, Eckman J, Sebastiani P, Steinberg MH, Ballas SK. Leg ulcers in sickle cell disease. Am J Hematol 2010; 85: 831-833.45. Trent JT, Kirsner RS. Leg ulcers in sickle cell disease. Adv Skin Wound Care 2004: 17; 410-416.46. Gueguen A, Mahevas M, Nzouakou R, Hosseini H, Habibi A, Bachir D, et al. Sickle-cell disease stroke throughout life: a retrospective study in an adult referral center. Am J Hematol 2014; 89: 267-272.47. Majumdar S, Miller M, Khan M, Gordon C, Forsythe A, Smith MG, et al. Outcome of overt stroke in sickle cell anaemia, a single institution’s experience. Br J Haematol 2014; 165: 707-713.48. Helvaci MR, Aydogan F, Sevinc A, Camci C, Dilek I. Platelet and white blood cell counts in severity of sickle cell diseases. Pren Med Argent 2014; 100: 49-56.49. Kossorotoff M, Grevent D, de Montalembert M. Cerebral vasculopathy in pediatric sickle-cell anemia. Arch Pediatr 2014; 21: 404-414.
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 ��MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Splenomegaly in Patients with Sideropenic Anemias: Clinical and Hematologic Significance
Safaa A. A. Khaled (1)Gehan S. Seifeldein (2)
(1) MD, Department of Internal Medicine, Hematology & BMT unit, Assiut University Hospital, Faculty of Medicine, Assiut University, Assiut, Egypt.(2) MD, Department of Diagnostic Radiology, Assiut University Hospital, Faculty of Medicine, Assiut University, Assiut, Egypt.
Correspondence:Dr. Safaa A.A. KhaledDepartment of Internal Medicine, Hematology & BMT unit.Assiut University Hospital, Assiut, Egypt. Tel: 002 0882 413940.Email: [email protected]; [email protected]
ABSTRACT Background, Objectives: Sideropenic anemias (SAs) are a group of hypoproliferative anemias characterized by hyposideremia. Although they run an insidiously started slowly progressive course, they are a pointer for an underlying serious disease. Fortunately, in most cases, management of SAs is available, effective and rela-tively inexpensive. Splenomegaly was reported in patients with SAs with variation in Hackett’s grading and hematological profile. Etiopathogenesis of splenomegaly in SAs was mainly explained as related to the un-derlying pathologic process of anemia or as a component of the rarely occurring Paterson-Kelly syndrome. Apart from the etiopathogenesis of splenomegaly of SAs it is still a fruitful point for current research. The aim of the present study was to assess splenomegaly in patients with SAs in terms of frequency, clinical and hematological profile of splenomegaly in SAs. Another aim was to assess prognostic significance and to as-sume etiopathogenesis of splenomegaly in SAs.
Methods: A prospective study was conducted on 83 patients with SAs and 25 normal sex and age matched healthy controls. Patients’ demographics, clinical and hematologic data were collected through thorough history and clinical examination. Splenomegaly was assessed with clinical examination of the study subjects and was graded with Hackett’s clinical grading, then confirmed with ultrasonographic examination. Patients were treated as per the published guidelines for treatment of SAs. Those with splenomegaly were subjected to a strict follow up plan.
Results and Conclusion: Analysis of the collected data showed that splenomegaly is of robust clinical and hematologic significance in patients with SAs.
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 320MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
�. Introduction
Sideropenic anemia is a hematologic term referred to anemias with reduced serum iron levels; the term includes iron deficien-cy anemia (IDA), and anemia of chronic disease (ACD), or a di-morphic anemia of IDA and ACD. SAs are the most prevalent types of anemias worldwide, firstly IDA and secondly ACD. (1-3)
In vitro and in vivo studies demonstrated reduced serum iron in patients with chronic inflammatory conditions, infections and malignancies. Inflammatory cytokines such as interleukin-1, interleukin-6, and tumor necrosis factor-alpha are the main trigger for hypoferemia; other bone morphogenetic proteins 2, 4, 6, & 9 produce the same effect in patients with malignancy. These effects were mediated through hepcidin. (4-6)
The differentiation between IDA and ACD is quiet difficult, nevertheless in ACD there is confounding evidence of chronic infectious, inflammatory, or malignant disease causing the ane-mia. Furthermore in ACD the RBCs indices are usually nor-mal (MCV from 80- 100fl, MCHC from 32-36 gm/dl and RDW 12.0-14.6%), while in IDA all RBCs indices are below normal except the RDW which is commonly raised. Total iron bind-ing capacity (TIBC) was found raised in IDA and reduced in ACD, however serum hepcidin levels were considered the most important difference between IDA and ACD. Unfortunately, laboratory assay of serum hepcidin is difficult, expensive and not widely available. Soluble transferrin receptor (sTfR) was found to be a good differential test between IDA and ACD; it was found raised in patients with IDA however standardization of the test was difficult. (7-9)
Hepcidin is a hepatic protein that is found to be raised in pa-tients with ACD and reduced in IDA. Inflammatory cytokines are the most important triggers for hepcidin production. Hep-cidin affects iron homeostasis by inhibition of a divalent iron transporter protein-1, that in turn hinders enteral iron absorp-tion; and blocking a ferroprotin that inhibits release of iron from iron stores. Both cause sideropenia and raised iron levels in the reticulo-endothelial tissues. (9,10)
Splenomegaly was reported in patients with SAs; in IDA splenomegaly was described with Paterson-Kelly syndrome, and hypopituitarism whereas in ACD it is a diagnostic feature of the underlying disease. The classic triad of Paterson-Kelly syndrome is retropharyngeal dysphagia, eosophageal web, and iron deficiency anemia. (11-14)
This study was conducted to evaluate the frequency, and clini-cal significance (diagnostic/prognostic) of splenomegaly in patients with SAs, also to assess the association between dif-ferent grades of splenomegaly and both clinical and hemato-logical profiles of patients.
2. Materials and Methods
2.1. Study design and subjectsA prospective longitudinal study was conducted at the Depart-ment of Internal Medicine, Assiut University Hospital over a period of 6 months. Three groups of patients were enrolled in the study, patients with IDA patients with ACD, and another group of gender and age matched healthy volunteers was in-cluded as controls. Patients were recruited among those who were admitted or attending the outpatient clinics of Internal Medicine Department, while controls were among students, staff and co-workers. Consent of patients and controls were ob-tained before enrollment in the study. However, as mentioned before, splenomegaly in ACD is related to the underlying eti-ology, accordingly the study focused on patients with IDA. Hence the study participants were grouped into three groups 1: patients with IDA, group 2: sideropenic control (patients with ACD), and group 3: normal controls.
2.2. Methods2.2.1. Data collectionDemographic and clinical data of the study groups were ob-tained through detailed medical history and clinical examina-tion, with particular stress on dietary habits and nutritional his-tory, also detailed menstrual history was obtained in females. Hematological profiles were obtained from results of labora-tory investigations. Patients with splenomegaly were asked for regular follow up at the outpatient clinic every 2-weeks, in each follow up visit patients’ splenic sizes were reassessed clinically together with laboratory assessment of anemia.
2.2.2. Diagnosis of SAs in the study groupsDiagnosis of SAs was accomplished by presence of general symptoms and signs suggestive of anemia. Specific signs such as smooth tongue, flattened nails, angular cheilitis, and koilo-nychias were suggestive of IDA. (15) Presence of chronic in-fection, inflammation, or malignancy was suggestive of ACD. Diagnosis of SAs was ascertained by laboratory detection of blood hemoglobin level < 11.8 gm/dl in females and < 13.8 gm/dl in males.
Hematologically, presence of microcytosis (MCV< 80 fl0, hy-pochromia (MCHC< 32 gm/dl), sideropenia (serum iron < 50 mcg/dl) and impaired reticulocytic response to anemia were diagnostic of SAs in the study subjects. Normocytic, normo-chromic anemia and reduced TIBC were diagnostic of ACD, while raised TIBC were present in IDA. Blood film with target cells or pencil shaped poikilocytes was highly suggestive of IDA. Patients with dimorphic blood film were excluded from the study.
In patients with microcytic hypochromic anemia and splenom-egaly hemoglobin electrophoresis was performed to exclude thalassemia minor or trait. Bone marrow aspirate was per-formed in selected cases to exclude hypersplenism and differ-entiate IDA from ACD. In presence of reticulocytosis direct antiglobulin test was done.
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 2�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
2.2.3. Diagnosis of the etiology of SAs in the study patientsVarious laboratory, radiological and histopathological inves-tigations were performed in a trial to verify the underlying etiology of SAs in the study groups. These included thorough nutritional history, stool and urine analyses, ESR, C-reactive protein, KFT and LFT. Abdominal or pelvic ultrasound, upper or lower endoscope were also performed as indicated.
2.2.4. Assessment of splenomegaly in patients with si-deropenic anemias Splenomegaly was assessed in the study groups by thorough clinical history and examination. On detailed clinical examina-tion splenomegaly was considered by detection of dull Traube’s area or palpable spleen either in supine or Rt. Lateral positions. In our practice clinical examination of patients attending the outpatient clinics or admitted in the ward usually takes place early in the morning before patients have their breakfast, how-ever some of the patients had their breakfast before examina-tion. All patients were examined by the hematology resident in charge, before the researcher. Grading of splenomegaly was mainly based on the WHO proven Hackett’s clinical grading as following. (16)
Class 0: Impalpable spleen, Class 1: Just palpable spleen only with deep inspiration.Class 2: Palpable spleen but not below a horizontal line pass-ing half way between the costal margin and umbilicus.Class 3: Palpable spleen but not below a horizontal linepassing through the umbilicus.Class 4: Palpable spleen but not below a horizontal line between the umbilicus and pubic symphysis.Class 5: Palpable spleen beyond class (4).
Splenomegaly was diagnosed mild, moderate or massive if it is Hackett’s class 1&2, 3, 4&5, respectively.
Confirmation of presence or absence of splenomegaly was done with the least hazardous radiographic assessment tool, abdominal U/S.
Abdominal US was performed using an Ultrasound Sys-tem (GE, LOGIQ 3 Color Doppler) for all patients using 3.5-5.0MHz convex transducer. The splenic size was measured (in cm) with the probe in the left upper quadrant. The larg-est superior- inferior dimension of the spleen was identified and measured. US scoring system was by evaluating the edge, surface and parenchymal texture of the spleen. Score 0 means normal and score 2 means Splenomegaly, that was defined as an anteroposterior dimension >13 cm, without any abnormal-ity of the structure. (17)
2.2.5. Treatment of the study groups Treatment of SAs included treatment of the underlying etiol-ogy of SA; those with IDA received ferrous fumarate tablets 200 mg Tds immediately after meals together with vitamin C supplementation and were advised regarding consuming iron rich diets. In ACD erythropoietin and iron supplementation were provided. Intravenous iron and packed RBCs transfu-sions were used to treat those with severe anemia and those intolerant to oral iron supplements. (18-22) Anemia was con-sidered mild if Hb>10g/dl, moderate if Hb7-10g/dl and severe if Hb<7g/dl.
2.2.6. Follow up for the study groupsPatients with evident splenomegaly were asked for regular fol-low up at the Hematology outpatient clinic firstly after 10-days and then every two weeks until hemoglobin reached near nor-mal values within 2-3 months. In the first visit assessment of response to treatment was evaluated by the rising reticulocyte count. In each visit patients were re-assessed clinically, and with laboratory investigations. Abdominal U/S was repeated in the last follow up visit. Data were recorded in a hand written follow up file available at the clinic for each patient. Patients with IDA were advised to continue treatment for 6 months after hemoglobin reached normal values to replenish iron stores.
2.2.7. Ethical considerationsThe study aims and methodology were discussed with patients and controls; furthermore they were consistent with the World Medical Association (WMA) declaration of Helsinki for ethics in medical research. (23) Consent for participation in the study was obtained from both patients and controls. Patients were asked to feel free to withdraw from the study at any time.
2.2.8. Statistical analysis Data were collected then introduced into a personal computer substituting patients’ names with code numbers. The collected data were analyzed with Graphpad Prism V5, Italy and SPSS V. 17 software (SPSS Inc. Chicago, TL, USA). Quantitative variables were expressed as mean ±SD, median, and range while qualitative variables were expressed as percentages from the total number. The one-way ANOVA and Tukey’s multiple comparison tests were used to compare means while the chi-square test was used to analyze differences among qualitative variables among the study groups.
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 322
3. Results
3.1. Characteristics of the study population 3.1.1. Demographic and clinical characteristics of the study groupsA total of 108 participants were included in the study. Among these 53 were with IDA (group 1), 30 sideropenic controls (group 2) and 25 healthy controls (group 3), the means of their ages were 30.89±13.39, 31.21± 15.15 and 31.01± 14.01 respec-tively, P=0.912. Gender analysis showed female predominance in the study patients with male to female ratio 1:1.1 in IDA and 1: 1.5 in sideropenic controls. The vast majority of the study participants were from Assiut governorate, 56.5%. Due to perfect matching there were no significant differences in age, gender and residential distribution among the study groups. SAs were commoner in rural residents compared with urban residents (59.3% vs 39.8 %). 47.2% of patients with IDA were singles while 83.3% of sideropenic controls were parents. IDA was commoner in students and housewives, 28.3% and 26.4% respectively.
The most common presenting complaints were dizziness in those with IDA (98.2%), while non hematological manifesta-tions were commoner in sideropenic controls (60%). One pa-tient with IDA (1.8%) presented with delayed puberty. More than two thirds (69.8%) of group 1 patients were excessive drinkers of tea vs 50% and 36% in groups 2&3, respectively. Malnutrition was documented in 22.6% and 20% of groups 1&2 patients respectively. Specific features of IDA as angular stomatitis and koilonychia were present in 45.3% and 32.1%, of group 1, respectively. 3.8 % of patients of groups 1 or 2 had hepatomegaly. Table 1 shows demographic and clinical charac-teristics of the study groups.
3.1.2. Hematologic and disease characteristics of the study groupsExpectedly, hypochromia, microcytosis, thrombocytosis and raised TIBC were present in group 1 patients. On the contrary normocytic normochromic anemia with decreased TIBC and raised ESR and C-reactive protein were the most common fea-tures of group 2. Sideropenia was the unique feature of all the study patients. There was no significant difference in WBCs count among the study groups. There were significant differ-ences in Hb, Plts, MCV S .iron and TIBC between group 1 patients and the controls. Group 2 differences were significant in Hb, retic., S.iron, TIBC, ESR and C-reactive protein as de-picted in tables 2 & 3. 47.2%, 52.8% and 0 % of group 1 pa-tients had severe, moderate and mild anemia, vs 13.3%, 80%, and 6.7% in group 2 respectively. Interestingly mild anemia was detected in 20% of the healthy controls with a minimum hemoglobin level of 11.5g/dl as in Table 4.
3.2. Underlying etiology of sideropenic anemia in the study patientsThe most prevalent causes of IDA were menorrhagia, hemo-philia, unknown etiology and occult bleeding while those for ACD were CRF, rheumatoid arthritis, malignancy and systemic lupus erythematosus in descending order. Benzidine test was positive in 9.4 % of patients with IDA denoting occult blood in stools as in figure 1.
3.3. Splenomegaly in patients with IDA compared with the sideropenic and healthy control subjectsSplenomegaly was present in 11.3%, 40 % and 0 % of groups 1, 2 & 3, respectively. In IDA half most of the patients had Hackett’s G1 (9.4%) and only 1.9% had G2, also in ACD G1 comprised 33.3% followed by grade 0 (16.7%) and lastly grade 2 (6.7%). However splenomegaly was sonographically proven only in 5-patients of group 1 (9.4%), and 10 patients in group 2 (33.3%). Table 1 shows distribution of splenomegaly in the study groups, and Table 5 shows diagnostic performance of US variables in predicting splenomegaly among groups 1 & 2.
Splenomegaly in patients with IDA was commoner in males 4(80%) and rare in those from urban community (20%). Their medical history denoted insufficient dietary intake of iron, and they had pica and malnutrition. They were excessive drinkers of tea (100%) with angular stomatitis (80%), and koilonychias (100%). Hepatomegaly was associated with splenomegaly in 0 % & 90% of patients of IDA and sideropenic controls, respec-tively.
When we correlated hematological parameters with grading of splenomegaly in patients with IDA they were negatively as-sociated with HB, MCV, and reticulocytes, and all patients had severe anemia (Hb ranged from 3.2-6 g/dl). Table 6 showed factors associated with splenomegaly in patients with IDA.
The stool analyses showed Giardia lamblia cysts in 2-patients with IDA and splenomegaly, hookworm ova in 1 patient and occult bleeding in 1 patient. The possible etiology of IDA in the other patient was unknown, however the defective dietary intake of iron was marked in all patients and was continuous for many years.
Follow up of patients with SAs and splenomegaly after treat-ment revealed gradual progressive reduction of splenic size with increase in hemoglobin. After 3-months follow up spleen was nearly impalpable in those with grade 1 Hackett’s how-ever dullness at Traube’s area was still detected in patients with grade 2. Splenomegaly was still sonographically detected in 2 patients. These findings were noted in patients with IDA (group 1). On the contrary splenic size remained stable in the sideropenic control patients (group 2).
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 23
Table 1. Demographic and clinical characteristics of the study groups (total n = 108).
Data were presented as mean± SD, or as percentage from the total number.
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 32�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Table 2: Laboratory and hematologic characteristics of the study groups (total no = 108)
N.B. WBCs= white blood cells, Hb= hemoglobin, MCV= mean corpuscular volume, Plt= platelet, Retic= reticulocyte count, ESR= erythrocytic sedimentation rate, C reactive P= C reactive protein. Duration of anemia in months. Data were presented as mean± SD. P value was significant at 0.05 level.
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 2�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
Table 3: Tukey multiple comparison test of quantitative variables of patients with SAs compared with the controls (total no=108)
N.B. WBCs= white blood cells x103, Hb= hemoglobin g/dl , MCV= mean corpuscular volume FL, Plts= platelets x103, Retic= reticulocyte count%, ESR= erythrocytic sedimentation rate mm/hr, C reactive P= C reactive protein mg/dl , TIBC= total iron binding capacity mcg/dl, S. iron= serum iron.
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 32�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Table 4: Degree and treatment modalities of SAs in the study patients (total n = 83)
Table 5: Diagnostic performance of US variables in predicting splenomegaly among groups 1&2
*P value <0.05 , ** No splenomegaly found in group 3.
Table 6: Factors associated with splenomegaly in patients with IDA (total no = 53)
N.B. P value was significant at 0.05 level.
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 2�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
Figure 1: Causes of sideropenic anemias in the study patients
�. Discussion
SAs are hypoproliferative anemias that are caused by iron deficiency and/or decreased erythropoietin (EPO) production and/or reduced response to EPO, the latter due to resistance of target cells to EPO action or reduced number of cells. (24) This study was conducted to elucidate splenomegaly in patients with SAs in terms of occurrence, clinical and hematological profile and the effect of treatment on splenomegaly. The study focused on IDA while ACD was used as a sideropenic control.
In this study SAs were commoner in females; IDA was more prevalent in rural residence while urbanization was obvious in sideropenic controls. Furthermore IDA was commoner in students and housewives while ACD in those who did regu-lar office work. These expected results were explained by in-creased prevalence of iron deficiency and chronic inflamma-tory diseases in females and higher number of vegans in rural communities. (25, 26)
This study confirmed a direct relationship between exces-sive intake of tea and incidence of IDA. A common custom in Egypt is to drink nearly 2gms/250 mls of red tea right after each meal particularly after lunch. Numerous studies reported that tea hinders iron absorption and advise tea drinkers to have their cups at least 1 hour after a meal. (27-29)
Manifestations of tissue iron deficiency were much higher than that in comparable studies; this could be explained by the long-er duration of iron deficiency in our patients. However results of this study were accordant with others in showing positive association between the degree of tissue iron deficiency and severity of IDA besides revealing that angular cheilitis was more prevalent than koilonychias. Both angular cheilitis and koilonychias were explained by deficiency of iron based en-zymes in the mucosal and epithelial tissues. (30,31)
In accordance with other studies, reduced Hb, MCV, MCHC, and thrombocytosis were the CBC features of IDA; on the contrary normocytosis and normochromia were evident in si-deropenic controls. (32) An interesting finding was laboratory detection of mild anemia in asymptomatic controls with the
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 32�
minimum hemoglobin 11.5g/dl in females. This finding denoted that the lower cut of value of hemoglobin should be tailored for each population specifically.
In this study the most common etiology of IDA was menor-rhagia while chronic renal failure was the commonest cause of ACD. This study confirmed the findings of others that IDA could retard growth and development in children and also reaf-firmed that gastrointestinal tract blood loss and H-pylori infec-tions are common causes of IDA. As reported by others, hiatus hernia was the underlying etiology of IDA in one of our pa-tients. (33-36) Although the recommended daily requirements of iron are very small, IDA due to ineffective dietary intake was noted in our patients. This could be explained by most of them being from a rural community. Accordingly the main elements of their diets were, milk and milk products, fruits and vegeta-bles; both are poor sources of iron.
Splenomegaly was detected in approximately one tenth of pa-tients with IDA; this was albeit consistent and inconsistent with other studies. Unlike other studies there was no detectable splenomegaly in the control group. (37-39)
When considering the sideropenic control group splenomegaly was detected in more than half of the patients and was close-ly related to the underlying etiology of anemia, furthermore hepatosplenomegaly was evident in a considerable proportion of patients. However there was no association between the de-gree of anemia and Hackett’s grading of splenomegaly in the sideropenic control group. As reported by others, treatment of the underlying etiology of anemia improved hematological pro-file of the patient, (18,40,41) however it did not affect splenic size. This denoted that the etiopathogenesis of splenomegaly in the sideropenic controls is not related to the anemia itself.
In this study patients with IDA and splenomegaly were mostly from a rural community and the vast majority of them were males in their late teens or early twenties. Their nutritional his-tory denoted ineffective dietary supply of iron and pica. Para-sitic infestation was detected in 3 of the patients. They were suffering from IDA for years, with periods of interrupted iron supplementation. Concomitant with other studies splenomegaly was impalpable or mild to moderate (Hackett’s grades 1 & 2) in most of the patients. Furthermore the degree of splenomegaly was positively correlated with the severity of anemia. This was consistent with Hussain et al and inconsistent with Dabadghao and his coworkers. (14, 42,43) Notably this study showed re-duction in splenic size with correction of hemoglobin. Another important finding was the strong association between splenom-egaly and kioilonychia in patients with IDA; kioilonychia is a sign of severe long standing IDA.(30) Expectedly the degree of splenomegaly will be directly correlated with both the sever-ity and duration of IDA; this assumption was proved with the results of the current study.
The etiopathogenesis of splenomegaly in patients with IDA is still unclear. However the most acceptable explanation is that IDA is a hypoproliferative anemia with poikilocytosis and ani-socytosis both leading to splenic hyperplasia. Another explana-
tion is extramedullary hematopoiesis. This could in turn ex-plains the rare association of hepatomegaly and splenomegaly in patients with IDA. The latter assumption could explain the association of splenomegaly with duration and severity of IDA, furthermore it explained resolution of splenomegaly with cor-rection of ID. Although malnutrition was detected in our pa-tients it could not explain the occurrence of splenomegaly in IDA as it was a micronutrient malnutrition rather than a protein energy malnutrition.( 44) However the presence of giardiasis in 2 of our patients could be a contributing factor for development of splenomegaly in them. (25)
�. Conclusion
In conclusion the current study demonstrated that splenom-egaly had considerable clinicohematologic significance in pa-tients with SAs. Hackett’s grade 1, or 2 splenomegaly was a common finding in patients with severe, chronic IDA that was mainly caused by malnutrition. Furthermore iron supplementa-tion and replenishment of iron stores led to gradual resolution of splenomegaly. This denoted that splenomegaly, in patients with IDA, is a very simple clinically based diagnostic/prognos-tic index. However every effort has to be made to exclude tha-lassemia in patients with microcytic hypochromic anemia and splenomegaly before prescribing iron supplementation. This was not the case in patients with ACD where splenomegaly was found to be related to the underlying etiology of anemia rather than the anemia itself.
Based on the findings of this study we recommended reduc-ing tea drinking particularly in children and females who are already in a state of negative iron balance due to increased de-mands. Furthermore we advise people to avoid drinking tea af-ter the main meal where a great proportion of iron requirements are supplied.
AcknowledgementsThe authors wish to express deep thanks and gratitude to the entire control group who volunteered participation in the study for the seeking of robust medical knowledge. Also great thanks to hematology residents and paramedical staff at Assiut Uni-versity Hospital, Assiut, Egypt for their help during data col-lection.
References
[1]- Cavill I., Auerbach M., Bailie G.R., Barrett-Lee P., Beguin Y., Kaltwasser P., et al. Iron and the anaemia of chronic disease: a review and strategic recommendations. Current Medical Re-search and Opinion 2006; 22: 731-737.[2]- Dallman PR, Yi PR, Johnson C. Prevalence and causes of anemia in the United States, 1976 to1980. Am J Clin Nutr 1984; 39:437-45.[3]- WHO Global Database on Anemia.. Worldwide Prevalence of anemia 1993-2005. Geneva, Switzerland: World Health Or-ganization, 2008.
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 2�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
O R I G I N A L CO N T R I B U T I O N / CL I N I C A L I N V E S T I G AT I O N
[4]- Alvarez-Herna´ndez, X., Lice aga, J., McKay, I.C. & Brock, J.H. Induction of hypoferremia and modulation of macrophage iron metabolism by tumor necrosis factor. Laboratory Investi-gation 1989 ; 61: 319-322.[5]- Cazzola M., Ponchio L., de Benedetti F., Ravelli A., Rosti V., Beguin, Y., et al. Defective iron supply for erythropoiesis and adequate endogenous erythropoietin production in the ane-mia associated with systemic-onset juvenile chronic arthritis. Blood 1996; 87: 4824-4830.[6]- Ferrucci L., Semba R.D., Guralnik J.M., Ershler W.B., Bandinelli, S., Patel K.V., et al. Proinflammatory state, hepci-din, and anemia in older persons. Blood 2010; 115: 3810-3816.[7]- Ganz T, Nemeth E. Hepcidin and disorders of iron metabo-lism. Annu Rev Med. 2011; 62:347-360.[8]- Busbridge M., Griffiths C., Ashby D., Gale D., Jayantha, A., Sanwaiya A. et al. Development of a novel immunoassay for the iron regulatory peptide hepcidin. British Journal of Bio-medical Science 2009; 66: 150-157.[9]- Skikne BS, Punnonen K, Caldron PH, Bennett MT , Rehu M, Gasior GH, et al. Improved differential diagnosis of anemia of chronic disease and iron deficiency anemia: a prospective multicenter evaluation of soluble transferring receptor and the sTfR/log ferritin index. Am J Hematol. 2011; 86(11):923-927. [10]- Brasse-Lagnel C., Karim Z., Letteron P., Bekri S., ado A. & Beaumont C. Intestinal DMT1 cotransporter is down-regu-lated by hepcidin via proteasome-internalization and degrada-tion. Gastroenterology 2011; 140: 1261-1271.[11]- Hoffman RM, Jaffe PE. Plummer-Vinson syndrome. A case report and literature review. Arch Intern Med. 1995; 155(8):2008-11.[12]- Prasad AS, Halsted JA, Nadimi M. Syndrome of iron defi-ciency anemia, hepatosplenomegaly, hypogonadism, dwarfism and geophagia. Am J Med 1961; 31:532-46.[13]-King R, Mizban N, Rajeswaran C. Iron deficiency anae-mia due to hypopituitarism. Endocrine Abstr 2009; 19:278.[14]- Safaa A. A. Khaled. Aggravation of Iron Deficiency Ane-mia after Hormone Replacement Therapy in a Patient with Hy-popituitarism and Hepatosplenomegaly . Int. J. Adv. Res. Biol. Sci. 2015; 2(12):324-329.[15]- Shah A. Iron deficiency anemia Part II (Etiopathogenesis and diagnosis). Indian J Med Sci 2004? 58:134-7.[16]- Ogilvie C. Evans CC: Splenomegaly. In: Wratt G. Symp-toms and signs in Tropical Disease. Chamberlaine’s symptoms and signs in Clinical medicine: 12th edition. Butterworth- Heineman, 1997, ( 315-324).[17]- Benter T, Klühs L, Teichgräber U. Sonography of the spleen. J Ultrasound Med. 2011; 30(9):1281-93.[18]- Doyle M.K., Rahman M.U., Han C., Han J., Giles J., Bing-ham C.O. et al. Treatment with infliximab plus methotrexate improves anemia in patients with rheumatoid arthritis inde-pendent of improvement in other clinical outcome measures-a pooled analysis from three large, multicenter, double-blind, randomized clinical trials. Seminars in Arthritis and Rheuma-tism 2009; 39:123-131.[19]- Liu K, Kaffes AJ. Iron deficiency anemia : a review of diagnosis, investigation and management. Eur J Gastroenterol
Hepatol. 2012; 24(2):109-116. [20]- Goddard AF, James MW, Mclntyre AS, Scott BB. British Society of Gastroenterology Guidelines for the management of iron deficiency anemia. Gut. 2011; 60 (10): 1309-1316.[21]- Auerbach M., Ballard H., Trout J.R., McIlwain M., Acker-man A., Bahrain H., et al. Intravenous iron optimizes the re-sponse to recombinant human erythropoietin in cancer patients with chemotherapy-related anemia: a multi-center, open-label, randomized trial. Journal of Clinical Oncology 2004; 22:1301-1307.[22]- Auerbach, M. & Ballard, H. Clinical use of intravenous iron: administration, efficacy, and safety. Hematology. Ameri-can Society of Hematology. Education Program, 2010; 338-347.[23]- World Medical Association. World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects. Clinical Review & Education 2013; 310(20): 2191-94. [24]- Faquin W.C., Schneider T.J. & Goldberg M.A. Effect of inflammatory cytokines on hypoxia- induced erythropoietin production. Blood 1992; 79: 1987-1994.[25]- Kim JY, Shin S, Han K, Lee KC, Kim JH, Choi YS, et al. Relationship between socioeconomic status and anemia preva-lence in adolescent girls based on the fourth and fifth Korea National Health and Nutrition Examination Surveys. Eur J Clin Nutr. 2014 ; 68(2):253-8.[26]- Betsy Lozoff, M.D, Elias Jimenez, and Julia B. Smith, Double burden of iron deficiency in infancy and low socio-eco-nomic status: a longitudinal analysis of cognitive test scores to 19 years. Arch Pediatr Adolesc Med. 2006 ; 160(11): 1108-1113.[27]-Nelson M. , Poulter J. Impact of tea drinking on iron status in the UK: a review. J Hum Nutr Dietet 2004; 17: 43-54.[28]-Disler PB, Lynch SR, Charlton RW, Torrance J D, Both-well T H, Walker R B, et al. The effect of tea on iron absorp-tion. Gut 1975; 16:193-200.[29]- J P Kaltwassera, ,E Wernerb,, K Schalka, C Hansenb, R Gottschalka, C Seidl. Clinical trial on the effect of regular tea drinking on iron accumulation in genetic haemochromatosis. Gut 1998; 43:699-704 doi:10.1136/gut.43.5.699.[30]- Kumar G, Vaidyanathan L, Stead LG. Images in emer-gency medicine. Koilonychia, or spoon-shaped nails, is gener-ally associated with iron-deficiency anemia. Ann Emerg Med. 2007; 49(2):243, 250.[31]- Uchida T, Matsuno M, Ide M, Kawachi Y. The frequency and development of tissue iron deficiency in 6 iron deficiency anemia patients with Plummer-Vinson syndrome. Rinsho Ket-sueki. 1998 39(11):1099-102. Japanese[32]- Yates JM, Logan EC, Stewart RM. Iron deficiency anemia in general practice: clinical outcomes over three years and fac-tors influencing diagnostic investigations. Postgraduate Medi-cal Journal. 2004; 80(945): 405-410.[33]- Bandhu R, Shankar N, Tandon OP. Effect of iron on growth in iron deficient anemic school going children. Indian J Physiol Pharmacol. 2003; 47:59-66.
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 330 MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 8 ISSUE 2 MAY 2015MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
[34]- Soliman AT, Al Dabbagh MM, Habboub AH, Adel A, Humaidy NA, Abushahin A. Linear growth in children with iron deficiency anemia before and after treatment. J Trop Pedi-atr. 2009; 55:324-7.[35]- Rockey DC, Cello JP. Evaluation of the gastrointestinal tract in patients with iron deficiency anemia. New England Journal of Medicine 1993; 329: 1691-5.[36]- Windsor CW, Collis JL. Anaemia and hiatus hernia: ex-perience in 450 patients. Thorax 1967; 22(1): 73-8.[37]- Nadeem A., Ali N., Hussain T. Anwar M. Frequency and etiology of splenomegaly in adults seeking medical in Com-bined Military Hospital, Attock. J Ayub Med Coll 2004; 16(4): 44-47.[38]-Sundaresan JB, Dutta TK, Badrinath S , Jagdish S, Basu D. A Hospital based Study of Splenomegaly with special refer-ence to the Group of Indeterminate Origin. J Indian Med As-soc 2008; 106(3):150- 152.[39]-McIntyre OR, Ebaugh FG. Palpable spleen in college freshmen. Ann Intern Med 1967? 66: 30-33.[40]-Ali N, Anwar M, Ayyub A, Nadeem M, Ejaz A, Qureshi AH, et al. Hematological evaluation of splenomegaly. J Coll Physicians Surg Pakistan 2004; 14(7):404-406.[41]- Papadaki, H.A., Kritikos, H.D., Balatas, V., Boumpas, D.T. & Eliopoulos, G.D. Anemia of chronic disease in rheumatoid arthritis is associated with increased apoptosis of bone mar-row erythroid cells: improvement following antitumor necrosis factor-alpha antibody therapy. Blood, 2002; 100: 474-482.[42]-Hussain I, Ahmed I, Mohsin A. Causes of splenomegaly in adult local population presenting at tertiary care centre in Lahore. Pakistan J Gastroenterol 2002; 16(1):12-16.[43]- Dabadghao VS, Diwan AG, Raska AM. A Clinicohae-matological Profile of Splenomegaly. Bombay Hospital Journal 2012; 54:10-17.[44]- Anwar, I. and J.A. Awan. Nutritional status comparison of rural with urban school children in Faisalabad, Pakistan. J. Rural Remote Health, , 2003 1-7.[45]-Charalabopoulos K, Charalabopoulos A, Papadopoulou CH, Papalimneou V. Giardia lamblia intestinalis: a new patho-gen with possible link to Kikuchi-Fujimoto disease. An ad-ditional element in the disease jigsaw. Int J Clin Pract. 2004 Dec;58(12):1180-3.
O R I G I N A L CO N T R I B U T I O N A N D CL I N I C A L I N V E S T I G AT I O N
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 3�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 8 ISSUE 2 MAY 2015MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
Update on the Use of Vitamin B12 in Management of pain
A. Abyad
Correspondence:A. Abyad, MD, MPH, MBA, AGSF , AFCHSECEO, Abyad Medical CenterChairman, Middle-East Academy for Medicine of Aging President, Middle East Association on Age & Alzheimer’s Coordinator, Middle-East Primary Care Research Network Coordinator, Middle-East Network on AgingEmail: [email protected]
ABSTRACT Methylcobalamin (MeCbl), the activated form of vitamin B12, has been used to manage some nu-tritional diseases and other diseases in the clinic, including Alzheimer’s disease and rheumatoid ar-thritis. As an adjuvant, it effects neuronal protec-tion by fostering regeneration of injured nerves and alienating glutamate-induced neurotoxicity. Recently several studies revealed that MeCbl may have conceivable analgesic effects in experimental and clinical studies. It can reduce, pain behaviors in diabetic neuropathy, low back pain and neural-gia. MeCbl ameliorate nerve conduction, stimu-lated the regeneration of injured nerves, and in-hibited ectopic spontaneous discharges of injured primary sensory neurons.
Low back pain is an everyday problem worldwide. It can lead to a great financial burden to society due to absenteeism or having work limitations. Back pain is one of the most common symptoms for seeing primary care physicians and one of the top 5 causes of surgery.
Recent studies have shown a correlation between vitamin B12 injection and a decrease in Low back pain. This review aims to synopsize the analgesic effect and mechanisms of MeCbl at the present with particular stress on chronic low back pain. Intramuscular vitamin B12 injections appear to be of benefit in the reduction of chronic low back pain and also improve associated disability. However, further research is necessary to study the possible long term adverse reactions of these intramuscu-lar injections.
Key words: Vitamin B12, methylcobalamin, low back pain
�. Introduction
Vitamin B12 is essential for the health of our nervous system and blood cells, and vitamin B12 replacement is known for its role in the treatment of peripheral neuropathy and megaloblas-tic anemia (1).
Vitamin B12 is one of the body’s main building blocks, assist-ing it to make DNA and keep nerves and blood tissue vigor-ous. Vitamin B12 is present in animal products, including beef, seafood, milk, and cheese. Therefore, vegetarians run the risk of having vitamin B12 deficiencies. Vitamin B12 is essential for prime health. Even in the absence of deficiency, shots of the vitamin have been considered recently as an alternative therapy for chronic conditions, including back pain.
Traditionally vitamin B12 had been used to treat anemic eld-erly patients and as an adjuvant in sport nutrition. It was con-sidered as a painkiller since 1950 in some countries. Lately studies have shown that vitamin B12 played a major part in the normal functioning of the brain and nervous system and the formation of blood. Vitamin B12 is generally implicated in sev-eral metabolisms such as DNA synthesis and regulation, fatty acid synthesis, and energy production. Vitamin B12 has some analogs including cyanocobalamin (CNCbl), methylcobalamin (MeCbl), hydroxocobalamin (OHCbl), and adenosylcobalamin (AdoCbl). In mammalian cells, CNCbl and OHCbl are inac-tive forms and AdoCbl acts as a coenzyme of methylmalonyl Co-A mutase in mitochondria. However, vitamin B12 was not used directly in the human body, and it should be translated into activating forms such as MeCbl or AdoCbl. MeCbl differs from vitamin B12 in that the cyanide is replaced by a methyl group (2). It is a coenzyme of methionine synthase, which is needed for the formation of methionine from homocysteine in the methylation cycle which includes methylation of DNA or proteins (3-6). Compared with other analogs, MeCbl is the most effective one in being uptaken by subcellular organelles of neurons. Therefore, MeCbl can provide better treatments for nervous disorders through effective systemic or local delivery.
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 332
As a supporting agent, MeCbl has been forever used to manage several diseases, such as B12 deficiency and Alzheimer’s disease syndromes (7, 8). L-methylfolate, MeCbl, and N-acetylcysteine ameliorate memory, emo-tional functions, and communication with other people among Alzheimer’s patients (8,9). MeCbl also has neuro-nal protection embracing promoting injured nerve and ax-onal regeneration (10, 11) and antagonizing glutamate-in-duced neurotoxicity (10, 12). In addition, MeCbl amended nerve conduction in either patients of diabetic neuropathy (13-15) or streptozotocin-diabetic rats (16) and experi-mental acrylamide neuropathy (17). MeCbl also enhanced visual function (18), rheumatoid arthritis (19), Bell’s palsy, and sleep-wake rhythm disorder (20, 21). Lately, MeCbl has been revealed to have possible analgesic effects on neuropathic pain in experimental and clinical studies.
2. The analgesic effect of MeCbl
MeCbl is one active form of vitamin B12 which can directly participate in homocysteine metabolism. Accumulating evi-dence is showing the beneficial effects of MeCbl on clinical and experimental peripheral neuropathy.
2.1. Diabetic Peripheral Neuropathic PainParaesthesia, burning pains, and spontaneous pain in legs, were ameliorated by MeCbl (22,23) (Table 1). The effects of single use of MeCbl or combined use with other drugs were exam-ined in diabetic neuropathy pain (13, 24) (Table 1 - next page). Clinical evidence showed that MeCbl had the ability to inhibit the neuropathic pain accompanying diabetic neuropathy.
The severity of the pain is variable and may be explained as a hot, burning, cold, aching, or itching sensation with, at times, increased skin sensitivity. It is a challenge in clinical practice to treat diabetic neuropathic pain. Several medications have been tried including Carbamazepine, and dolantin with no suc-cess. Similarly, therapeutic effects of aldose reductase inhibi-tors and nimodipine were not promising in clinic as much as basic studies showed. Fortunately, MeCbl may convey a spar-kle of hope to treat diabetic neuropathic pain.
2.2. Low Back PainBack pain is one of the most frequent health complaints. It is a common complaint affecting 70-85% of people worldwide at some point during their life (25). The differential is extensive including, cancer, infection, inflammatory disorders, structural disorders of the spine itself, and disk herniation, are somewhat more common, and together account for back pain.
According to the WHO (World Health Organization), low back pain leads to a high economic burden due to the effects this often chronic problem has on work productivity (26). It is one of the most frequent causes behind visiting a primary care pro-vider, and in the top five of the most common reasons for hav-ing surgery(27).
Initially, low back pain is usually managed with anti-inflamma-tories including non-steroidal, muscle relaxants, and narcotics. Persistent back pain is further treated with physical therapy, TENS units, massage, epidural steroid injections, and surgery. Treatment varies depending on the patient. The majority of pa-tients recover within 12 weeks, while 10 to 20% endure low back pain past this time period, even with treatment (27,28). It emerges that vitamin B12 might be one of those additional treatment options.
The advantage of using B12 shots included decreasing the amount of non-steroidal anti-inflammatory drugs (NSAID), such as aspirin and ibuprofen. Vitamin B12 has no known side effects, according to the National Institutes of Health Office of Dietary Supplements, rivaled to long-term NSAID use, which may harm the gastrointestinal system and probably lead to heart attacks and strokes. Researchers aren’t sure how vita-min B12 shots help patients decrease back pain. However, they anticipate that the vitamin helps nerves repair and regenerate in the back. Additional benefits to treating back pain with B12 shots include the vitamin’s low cost, minimal side effects, and ability to get patients back to work and enjoying their lives.
Furthermore neurogenic claudication distance was ameliorated markedly after the application of MeCbl [29] (Table 2). How-ever Waikakul’s research showed that MeCbl was not good for pain on lumbar spinal stenosis [29]. In a trial, the analgesic effect of MeCbl has been examined in nonspecific low back pain patients with intramuscular injection [30] (Table 2 - page 35). The varying effect of MeCbl may be secondary to differ-ent causes of lumbar spinal stenosis and nonspecific low back pain. Additional studies are required to establish the effect of MeCbl on low back pain.
Three studiesStudies have shown that vitamin B12 shots can successfully decrease back pain.
One study conducted in 2000 by Italian researchers at the Uni-versity of Palermo found that vitamin B12 helped to alleviate lower back pain. The study evaluated 60 patients aged between 18 and 65 with proven back pain lasting anywhere from six months to five years.
Study participants were divided into two groups and received either a B12 shot or a placebo. Results showed injections allevi-ated back pain in patients even if they entered the study with adequate blood levels of vitamin B12.
CHIU et al (31) conducted a randomized, double-blinded, pla-cebo control study (5) to evaluate both the efficacy and safety of intramuscular methylcobalamin injections for treatment of chronic low back pain. Certain eligibility criteria were used for selection of the patient population. Included were patients who were between 20 and 65 years old and who had a history of low back pain, which had to be nonspecific in nature, and for greater than 6 months in duration. At the study’s conclusion neither disability nor pain was meaningfully reduced in the placebo group. However, in the treatment group they estab-
MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 33MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
Table 1: The analgesic effect of MeCbl or combined use with other drugs on patients with diabetic neuro-pathic pain
lished a marked decrease in both disability and pain. These inferences were based on the ODI and VAS scores taken 2 months after initiation of treatment, see Table 2. Furthermore, the placebo group consumed significantly higher doses of para-cetamol as compared to the participants in the treatment group; mean paracetamol consumption (in grams) was 87.6 ± 57.3 in the placebo group, 65.7 ± 75.2 in the treatment group. Treat-ment with intramuscular (IM) methylcobalaminhad very few side effects, including hematoma and pain at the injection site. It is difficult to estimate any long term side effects since the duration of the study was short, 2 months.
MAURO et al (32) using a randomized, double blinded, pla-cebo control study studied the efficacy of vitamin B12 in treat-ing low back pain. Patients ranged between 18 to 65 years old with medical evidence of 6 months to 5 years of mechanical low back pain or sciatic neuritis. They also had to have at least 60 out of 100 on the VAS pain intensity scale at the start of the study. The total patients included were 60 patients. They were randomly allocated to either the placebo or the treatment group. The treatment group received Tricortin® 1000 2mL ampoules-containing 1000 mg vitamin B12, whereas the placebo group only received 2 mL ampoules of an unspecified injection.
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 33�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Table 2: The analgesic effects of MeCbl on low back pain and neck pain in clinical trials
Table 3: The analgesic effect of MeCbl or combined with other agents on neuralgia
R E V I E W A R T I CL E
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 3�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
Pain was evaluated with the VAS, a test in which the partici-pants scored their pain on a scale of 0-100, where 0 meant no pain at all, and 100 was the worse pain one can have. In addi-tion the use of paracetamol was used to assess pain. Disability was assessed by using the DQ, a test that is made up of 24 ques-tions and is then scored on a 0-24 scale. In both the placebo and treatment group Pain and disability improved. In the placebo group the VAS score declined from 70.63 ± 7.9 to 36.83 ± 27.4, whereas in thetreatment group it declined from 75.53 ± 8.9 to 9.53 ± 16.5. The DQ score decreased from 11.53 ± 2.2 to 5.80 ± 3.3 in the placebo group and it decreased from 13.27 ± 2.7 to 2.43 ± 2.6 in the treatment group.
Nevertheless, there was a more statistically significant im-provement in the treatment group. Paracetamol was used less in the treatment group. There were no reported adverse effects. Therefore IM injection of vitamin B12 is safe in the short term. However, long term effects of IM injections of vitamin B12 were not examined nor discussed in this study.
A study from Lebanon (33) examined the usefulness of cobolamin injection in lumbosacral disc disease in patients with mechanical or irritative lumbago. Over 4 years a hundred and twenty patients with Lumbosacra l disease were enrolled in the study. Patients’ ages ranged between 18 to 65 years. The pa-tients were divided randomly into treatment and control group. Both groups received relative bed rest, NSAID’s and daily in-jection of vitamin B12 for the treatment group and sterile water for the control group. The duration of treatment lasted for three weeks, and the concentration of vitamin B12 was 1000 mg/ml. Patients were seen initially and at the end of treatment. Both treatment groups experienced a sharp decrease in pain and dis-ability. However, comparison between groups at the end of the treatment period showed a statistically significant difference in favour of the active treatment both for pain, paraesthesia, and nocturnal pain. Consumption of paracetamol proved signifi-cantly higher in the placebo group than in the active treatment (p < 0.0001). The author concluded that Intramuscular vitamin B12 injections seem to be effective at ameliorating nonspecific chronic low back pain as compared to placebo. Vitamin B12 in-jections also have exhibited only minimal side effects. There is a need for a larger study with longer duration that spans several years to assess the long term side effects, especially as long term effects can possibly be serious.
2.3. Neck PainChronic neck pain is becoming a common problem in the adult population, with the prevalence of 30%-50% in 12 months [34, 35]. It was shown that spontaneous pain, allodynia, and paraes-thesia of patients with neck pain were improved significantly in the MeCbl group, and with the increase of treatment time of MeCbl, the analgesic effect was more obvious [36] (Table 2).
2.4. Neuralgia2.4.1. Subacute Herpetic NeuralgiaThe use of MeCbl markedly decrease unremitting pain, parox-ysmal pain, and allodynia in the subacute herpetic neuralgia (SHN) patients (37) (Table 3). Therefore, Vitamin B12 can be used as an adjuvant treatment for SHN.
2.4.2. �lossopharyngeal NeuralgiaIn pain clinics Glossopharyngeal neuralgia (GPN) is common. It was stated that the numerical pain scales were reduced mark-edly with the treatment of MeCbl combined with gabapentin and tramadol in GPN patients (38) (Table 3). In addition the quality of life improved markedly (38).
2.4.3. Trigeminal NeuralgiaThe pain of trigeminal neuralgia (TN) can be portrayed as ex-cruciating, paroxysmal and lancinating which may be activat-ed by minor deeds such as chewing, speaking, and swallowing. A recent study showed that the pain of TN patients was eased significantly in the MeCbl group, and no recurrence of TN in 64% of the cases(39) (Table 3).
3. Analgesic Properties
Since many decades, the B12 group of vitamins had been used to treat pain. In some countries, vitamin B12 was labeled as an analgesic drug. It was implied that vitamin B12 may aug-ment the availability and effectiveness of noradrenaline and 5-hydroxytryptamine in the descending inhibitory nociceptive system (40). MeCbl has therapeutic effects on neuropathic pain in diabetics, conceivably through its neurosynthesis and neuro-protective actions (14, 41). However the analgesic mechanisms of MeCbl continue to be obscure. There are three sets of specu-lation on that matter below.
3.1. Improving Nerve Conduction VelocitySeveral authors revealed that high doses of MeCbl amended nerve conduction in either patients with diabetic neuropathy (13-15), streptozotocin-diabetic rats (16), or experimental acrylamide neuropathy (17). Morphological and histological evidence established that a long-term administration of MeCbl stimulated the synthesis and regeneration of myelin (42). These morphological and histological recoveries of myelin can lead to ameliorating nerve conduction velocity and neuronal func-tion in peripheral neuropathy.
3.2. Promoting the Regeneration of Injured NervesIn vivo MeCbl advanced the incorporation of radioactive leucine into the protein fraction of the crushed sciatic nerve. Therefore, this led to the recovery of the injured nerve activ-ity (43). In this study, most terminals were degenerated in the mutant mouse, but the sprouts were more often observed in the MeCbl treatment group (44). MeCbl had the power to support the injured nerves’ regeneration. In the experimental acryla-mide neuropathy and sciatic nerve injury models, the number of regenerations of motor fibers showed significant increase with high-dose methylcobalamin (17). In addition, the combined use of L-methylfolate, MeCbl, and pyridoxal 5?-phosphate amelio-rate the calf muscle surface neural density (45).
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 33� MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
3.3. Inhibiting Ectopic Spontaneous DischargeEctopic spontaneous discharges are possible to start spontaneous pain, hyperalgesia, and allodynia (46-49). It was reported that MeCbl suppressed the ectopic firing triggered by chemical materials in the dog dorsal root (50).
�. Discussion
Chronic pain is a usual complaint, leading the sufferer to be up to five times more likely to pursue medical attention as compared to those people without chronic pain (8). Lumbago, is a main cause of chronic pain. Within a year period one third of patients with this pain will experience lumbago (28). It has also been projected that around 80% of people will have low back pain at some point during their life (27). The bulk of low back pain (90%) without related neurological symptoms improves within 3 months (51). The remaining 10% are a challenge to many healthcare providers, not only because chronic low back pain is challenging to manage, it is also normally linked to anxiety, depression, job dissatisfaction, poor body image and somatization (28)
The therapeutic options for low back pain include NSAIDs, tramadol acetaminophen combinations, non-SSRI antidepressants, and glucocorticoids or local anesthetic to = the spine (52). These medications may lead to serious side effects, particularly when used for long periods of time. NSAIDS, for example can lead to kidney dysfunction, acetaminophen can cause liver dysfunction and glucocorticoids can cause weight gain, insomnia, and Cushing syndrome. Studies revealed that out of the available treatments only NSAIDs seem to ameliorate function (52). Recent studies (31,32,33) have shown that injectable cobalamin might also be a promising treatment option for lumbago.
Several studies (53-59), have suggested that large doses of vitamin B12 in combination with NSAIDs may lead to heightening effect on the analgesic properties of NSAIDs, therefore possibly decreasing NSAID dosing.
Vitamin B12 is mostly used for treatment of deficiency, which is often due to malabsorption, insufficient dietary intake, pernicious anemia, gastric surgery, GI disease, and particular medications (60). If longterm effects of vitamin B12 injection show to be safe, vitamin B12 might be a precious treatment alternative for low back pain. This will be particularly important for the elderly, for patients prone to liver or kidney disease or people interested in natural substance. The three randomized clinical trials (31-33) revealed that vitamin B12 compared to placebo, decreases low back pain and improves function significantly. However these studies have limitations, including small size that leads to large confidence intervals that the possibility that treatment effect was not precise. In addition none of the studies investigated the longterm effects of injectable vitamin B12.
It is known that high serum levels of vitamin B12 are linked to cancer, liver, renal, and inflammatory diseases (61). In one study vitamin B12 serum levels of >1275 pg/mL were associated with hematologic malignancies (62). Therefore, it is important to consider the possible side effects associated with long term risk. Studies that evaluate longterm effects of high serum cobalamin levels had their limitations. In one study the age of the patient was important in determining the level of vitamin B12 where the older patients had a higher level (63).
It is known that elderly have multiple comorbidities. Hence it was challenging to attribute the results of the study to the vitamin B12 levels versus the participants age (64). One more limitation is the fact that vitamin B12 was the only lab value looked at for its possible relation to cancer development (65). Other electrolyte abnormality or vitamin deficiency may be implicated for the cause for an increased risk of cancer.
In addition we are not sure that the cobalamin doses used in the treatment of low back pain were high enough to lead to high serum vitamin B12 levels discussed (63,64).
Although vitamin B12 seems to have significant benefit in the treatment of chronic low back pain, further research, with elimination of some of these limiting factors, is needed to study whether the intramuscular vitamin B12 injection doses are indeed harmful in the long run.
�. Conclusions
Intramuscular vitamin B12 injections seem to be effective at ameliorating nonspecific chronic low back pain as compared to placebo. Vitamin B12 injections also have exhibited only minimal side effects, which include hematoma and pain at the injection site.
There is a need for larger study with longer duration that spans several years to assess the longterm side effects. Especially that longterm effects can be possibly serious. Meanwhile, physicians may use vitamin B12 treatments in addition to established treatment to prudently selected patients.
MeCbl or its joint use with other agents has the conceivable analgesic effect in specific patients and animal models, for example, nonspecific low back pain; neck pain; diabetic neuropathic pain, subacute herpetic neuralgia, glossopharyngeal neuralgia, and trigeminal neuralgia. However, the mechanisms underlying the analgesic effect were badly comprehended. On the basis of recent work, the likely mechanisms can be considered as follows. (1) MeCbl improved nerve conduction velocity; (2) MeCbl promoted injured nerve regeneration, recovering the neuromuscular functions in peripheral hyperalgesia and allodynia; and (3) MeCbl inhibited the ectopic spontaneous discharges from peripheral primary sensory neurons in neuropathic pain states. Therefore, MeCbl can be used for treating peripheral neuropathy with good safety.
R E V I E W A R T I CL E
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 3�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
References
1. Patel MS, Rasul Z, Sell P. Dual pathology as a result of spinal stenosis and vitaminB12 deficiency. Eur Spine J. 2011;20: 2247-2251.2. L. R. McDowell, Vitamins in Animal and Human Nutrition, John Wiley & Sons, 2008.3. R. Banerjee and S. W. Ragsdale, “The many faces of vitamin B12: catalysis by cobalamin-dependent enzymes,” Annual Review of Biochemistry, vol. 72, pp. 209-247, 2003. 4. S. K. Ghosh, N. Rawal, S. K. Syed, W. K. Paik, and S. D. Kim, “Enzymic methylation of myelin basic protein in myelin,” Biochemical Journal, vol. 275, part 2, pp. 381-387, 1991. 5. A. Pfohl-Leszkowicz, G. Keith, and G. Dirheimer, “Effect of cobalamin derivatives on in vitro enzymatic DNA methylation: methylcobalamin can act as a methyl donor,” Biochemistry, vol. 30, no. 32, pp. 8045-8051, 1991. 6. J. I. Toohey, “Vitamin B12 and methionine synthesis: a critical review. Is nature’s most beautiful cofactor misunderstood?” BioFactors, vol. 26, no. 1, pp. 45-57, 2006. 7. Y. Takahashi, S. Usui, and Y. Honda, “Effect of vitamin B12 (mecobalamin) on the circadian rhythm of rat behavior,” Clinical Neuropharmacology, vol. 15, supplement 1, part A, pp. 46A-47A, 1992. 8. A. McCaddon and P. R. Hudson, “L-methylfolate, methylcobalamin, and N-acetylcysteine in the treatment of Alzheimer’s disease-related cognitive decline,” CNS Spectrums, vol. 15, supplement 1, no. 1, pp. 2-6, 2010. 9. T. Ikeda, K. Yamamoto, K. Takahashi et al., “Treatment of Alzheimer-type dementia with intravenous mecobalamin,” Clinical Therapeutics, vol. 14, no. 3, pp. 426-437, 1992. 10. M. Kikuchi, S. Kashii, Y. Honda, Y. Tamura, K. Kaneda, and A. Akaike, “Protective effects of methylcobalamin, a vitamin B12 analog, against glutamate-induced neurotoxicity in retinal cell culture,” Investigative Ophthalmology and Visual Science, vol. 38, no. 5, pp. 848-854, 1997. 11. X. Kong, X. Sun, and J. Zhang, “The protective role of Mecobalamin following optic nerve crush in adult rats,” Yan Ke Xue Bao, vol. 20, no. 3, pp. 171-177, 2004. 12. A. Akaike, Y. Tamura, Y. Sato, and T. Yokota, “Protective effects of a vitamin B12 analog, methylcobalamin, against glutamate cytotoxicity in cultured cortical neurons,” European Journal of Pharmacology, vol. 241, no. 1, pp. 1-6, 1993. 13. G. Devathasan, W. L. Teo, and A. Mylvaganam, “Methylcobalamin in chronic diabetic neuropathy. A double-blind clinical and electrophysiological study,” Clinical Trials Journal, vol. 23, no. 2, pp. 130-140, 1986. 14. S. Kuwabara, R. Nakazawa, N. Azuma et al., “Intravenous methylcobalamin treatment for uremic and diabetic neuropathy in chronic hemodialysis patients,” Internal Medicine, vol. 38, no. 6, pp. 472-475, 1999. 15. H. Ishihara, M. Yoneda, W. Yamamoto, et al., “Efficacy of intravenous administration of methycobalamin for diabetic peripheral neuropathy,” Med Consult N Remedies, vol. 29, no. 1, pp. 1720-1725, 1992.
16. M. Sonobe, H. Yasuda, I. Hatanaka et al., “Methylcobalamin improves nerve conduction in streptozotocin-diabetic rats without affecting sorbitol and myo-inositol contents of sciatic nerve,” Hormone and Metabolic Research, vol. 20, no. 11, pp. 717-718, 1988.17. T. Watanabe, R. Kaji, N. Oka, W. Bara, and J. Kimura, “Ultra-high dose methylcobalamin promotes nerve regeneration in experimental acrylamide neuropathy,” Journal of the Neurological Sciences, vol. 122, no. 2, pp. 140-143, 1994.18. T. Iwasaki and S. Kurimoto, “Effect of methylcobalamin in accommodative dysfunction of eye by visual load,” Journal of UOEH, vol. 9, no. 2, pp. 127-132, 1987. 19. M. Yamashiki, A. Nishimura, and Y. Kosaka, “Effects of methylcobalamin (vitamin B12) on in vitro cytokine production of peripheral blood mononuclear cells,” Journal of Clinical and Laboratory Immunology, vol. 37, no. 4, pp. 173-182, 1992. 20. M. Ikeda, M. Asai, T. Moriya, M. Sagara, S. Inoué, and S. Shibata, “Methylcobalamin amplifies melatonin-induced circadian phase shifts by facilitation of melatonin synthesis in the rat pineal gland,” Brain Research, vol. 795, no. 1-2, pp. 98-104, 1998. 21. K. Takahashi, M. Okawa, M. Matsumoto et al., “Double-blind test on the efficacy of methylcobalamin on sleep-wake rhythm disorders,” Psychiatry and Clinical Neurosciences, vol. 53, no. 2, pp. 211-213, 1999. 22. H. Ide, S. Fujiya, Y. Asanuma, M. Tsuji, H. Sakai, and Y. Agishi, “Clinical usefulness of intrathecal injection of methylcobalamin in patients with diabetic neuropathy,” Clinical Therapeutics, vol. 9, no. 2, pp. 183-192, 1987. 23. G. Li, “Effect of mecobalamin on diabetic neuropathies. Beijing Methycobal Clinical Trial Collaborative Group,” Zhonghua Nei Ke Za Zhi, vol. 38, no. 1, pp. 14-17, 1999. 24. Y. U. Dongre and O. C. Swami, “Sustained-release pregabalin with methylcobalamin in neuropathic pain: an Indian real-life experience,” International Journal of General Medicine, vol. 6, pp. 413-417, 2013. 25. J. W. Frymoyer, “Back pain and sciatica,” The New England Journal of Medicine, vol. 318, no. 5, pp. 291-300, 1988. 26. Andersson GBJ. Epidemiological features of chronic low back pain. Lancet. 1999;354:581-85.27. World Health Organization. Low Back Pain. http://www.who.int/medicines/areas/priority_medicines/BP6_24LBP.pdf?ua=1. Updated March 2013. Accessed March 19, 2014.28. Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Practice & Research Clinical Rheumatology. 2010;24:769-781.29. W. Waikakul and S. Waikakul, “Methylcobalamin as an adjuvant medication in conservative treatment of lumbar spinal stenosis,” Journal of the Medical Association of Thailand, vol. 83, no. 8, pp. 825-831, 2000. 30. C. K. Chiu, T. H. Low, Y. S. Tey, V. A. Singh, and H. K. Shong, “The efficacy and safety of intramuscular injections of methylcobalamin in patients with chronic nonspecific low back pain: a randomised controlled trial,” Singapore Medical Journal, vol. 52, no. 12, pp. 868-873, 2011.31. Chiu CK, Low TH, Tey YS, Singh VA, Shong HK
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 33� MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
The efficacy and safety of intramuscular injections of methylcobalamin in patients with chronic nonspecific low back pain: a randomized controlled trial. Singapore Med J. 2011;52(12):868-873.32. Mauro GL, Martorana U, Cataldo P, Brancato G, Letizia G. Vitamin B12 in low back pain: a randomized, double-blind, placebo-controlled study. European Review for Medical and Pharmacological Sciences. 2000;4:53-58.33. Abyad, A. (2016). Cobalamin Injection: Is it Useful in Lumbosacral Diseases.? Middle East Journal of Family Medicine. 14(3): 26-3034. L. Manchikanti, E. E. Dunbar, B. W. Wargo, R. V. Shah, R. Derby, and S. P. Cohen, “Systematic review of cervical discography as a diagnostic test for chronic spinal pain,” Pain Physician, vol. 12, no. 2, pp. 305-321, 2009. 35. L. Manchikanti, S. Abdi, S. Atluri, et al., “American Society of Interventional Pain Physicians (ASIPP) guidelines for responsible opioid prescribing in chronic non-cancer pain: part I-evidence assessment,” Pain Physician, vol. 15, no. 3, pp. S1-S65, 2012. 36. I. Y. Hanai, M. K’Yatsume, et al., “Clinical study of methylcobalamin on cervicales,” Drug Therapy, vol. 13, no. 4, p. 29, 1980. 37. G. Xu, Z. W. Lv, Y. Feng, W. Z. Tang, and G. X. Xu, “A single-center randomized controlled trial of local methylcobalamin injection for subacute herpetic neuralgia,” Pain Medicine, vol. 14, no. 6, pp. 884-894, 2013. 38. P. M. Singh, M. Dehran, V. K. Mohan, A. Trikha, and M. Kaur, “Analgesic efficacy and safety of medical therapy alone vs combined medical therapy and extraoral glossopharyngeal nerve block in glossopharyngeal neuralgia,” Pain Medicine, vol. 14, pp. 93-102, 2013. 39. J. Teramoto, “Effects of Methylcobalamin on neuralgia,” Neurological Therapeutics, vol. 1, no. 2, p. 315, 1984. 40. I. Jurna, “Analgesic and analgesia-potentiating action of B vitamins,” Schmerz, vol. 12, no. 2, pp. 136-141, 1998. 41. Y. Sun, M. S. Lai, and C. J. Lu, “Effectiveness of vitamin B12 on diabetic neuropathy: systematic review of clinical controlled trials,” Acta Neurologica Taiwanica, vol. 14, no. 2, pp. 48-54, 2005. 42. K. Okada, H. Tanaka, K. Temporin et al., “Methylcobalamin increases Erk1/2 and Akt activities through the methylation cycle and promotes nerve regeneration in a rat sciatic nerve injury model,” Experimental Neurology, vol. 222, no. 2, pp. 191-203, 2010. 43. K. Yamatsu, Y. Yamanishi, T. Kaneko, and I. Ohkawa, “Pharmacological studies on degeneration and regeneration of peripheral nerves. (II). Effects of methylcobalamin on mitosis of Schwann cells and incorporation of radio active leucine into protein fraction of crushed sciatic nerve in rats,” Folia Pharmacologica Japonica, vol. 72, no. 2, pp. 269-278, 1976 (Japanese). 44. K. Yamazaki, K. Oda, C. Endo, T. Kikuchi, and T. Wakabayashi, “Methylcobalamin (methyl-B12) promotes regeneration of motor nerve terminals degenerating in anterior gracile muscle of gracile axonal dystrophy (GAD) mutant mouse,” Neuroscience Letters, vol. 170, no. 1, pp. 195-197,
1994. 45. A. M. Jacobs and D. Cheng, “Management of diabetic small-fiber neuropathy with combination L-methylfolate, methylcobalamin, and pyridoxal 5?-phosphate,” Reviews in Neurological Diseases, vol. 8, no. 1-2, pp. 39-47, 2011. 46. W.-H. Xiao and G. J. Bennett, “Synthetic ?-conopeptides applied to the site of nerve injury suppress neuropathic pains in rats,” Journal of Pharmacology and Experimental Therapeutics, vol. 274, no. 2, pp. 666-672, 1995. 47. Y. W. Yoon, H. S. Na, and J. M. Chung, “Contributions of injured and intact afferents to neuropathic pain in an experimental rat model,” Pain, vol. 64, no. 1, pp. 27-36, 1996. 48. Y. S. Lyu, S. K. Park, K. Chung, and J. M. Chung, “Low dose of tetrodotoxin reduces neuropathic pain behaviors in an animal model,” Brain Research, vol. 871, no. 1, pp. 98-103, 2000. 49. J. Lai, M. S. Gold, C. S. Kim et al., “Inhibition of neuropathic pain by decreased expression of the tetrodotoxin-resistant sodium channel, NaV1.8,” Pain, vol. 95, no. 1-2, pp. 143-152, 2002. 50. S. R. Chaplan, H.-Q. Guo, D. H. Lee et al., “Neuronal hyperpolarization-activated pacemaker channels drive neuropathic pain,” The Journal of Neuroscience, vol. 23, no. 4, pp. 1169-1178, 2003.51. Wheeler SG, Wipf JE, Staiger TO, Deyo RA. Approach to the diagnosis and evaluation of low back pain in adults. In: UpToDate, Atlas SJ (Ed), UpToDate, Waltham, MA, 2014.52. Bannwarth B, Kostine M, Shipley E. Nonspecific low back pain: Assessment of availablemedications. Joint Bone Spine. 2012;79:134-136.53. Rocha-Gonzales HI, Teran-Rosales F, Reyes-Garcia G, Medina-Santillan R, Granados-SotoV. B vitamins increase the analgesic effect of diclofenac in the rat. Proc West Pharmacol Soc. 2004;47:84-7.54. Reyes-Garcia G, Medina-Santillan R, Teran-Rosales F, et al. B vitamins increase the antihyperalgesic effect of diclofenac in the rat. Proc West Pharmacol Soc. 2002;45:147-9.55. Reyes-Garcia G, Medina-Santillan R, Teran-Rosales F, Mateos-Garcia E, Castillo-Henkel C.56. Characterization of the potentiation of the antinociceptive effect of diclofenac by vitamin B complex in the rat. J Pharmacol Toxicol Methods. 1999;42:73-7.57. Bartoszyk GD, Wild A. B-vitamins potentiate the antinociceptive effect of dicloenacin carrageenan-induced hyperalgesia. 58. Bruggemann G, Koehler CO, Koch EM. Results of a double-blind study of diclofenac +vitamin B1, B6, B12 versus diclofenac in patients with acute pain of the lumbar vertebrae. A multicenter study. Klin Wochenschr. 1990;68:116-20. 59. Kuhlwein A, Meyer HJ, Koehler CO. Reduced diclofenac administration by B vitamins: results of a randomized double blind study with reduced daily doses of diclofenac (75 mg diclofenac versus 75 mg diclofenac plus B vitamins) in acute lumbar vertebral syndrome. Klin Wochenschr. 1990;68:107-15.
R E V I E W A R T I CL E
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3 3�MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME9 ISSUE 2 AUGUST 2016
R E V I E W A R T I CL E
60. Vetter G, Bruggemann G, Lettko M, et al. Shortnening di-clofenac therapy by B vitamins. Results of a randomized double blind study, diclofenac 50 mg versus diclofenac 50 mg plus B vitamins, in painful spinal diseases with degenerative changes. Z Rheumatol. 1988;47:351-62. 61. Leishear K, Boudreau RM, Studenski SA, et al. Relation-ship between vitamin B12 and sensory and motor peripheral nerve function in older adults. The American Geriatrics Soci-ety. 2012;60:1057-1063.62. Schrier SL. Physiology of vitamin B12 and folate deficiency. In: UpToDate, Motil KJ (Ed), UpToDate, Waltham, MA, 2014.63. Chiche L, Jean R, Romain F, et al. Clinical implications of high cobalamin blood levels for internal medicine. Rev Med Interne. 2008;29:187.64. Arendt JFB, Nexo E. Cobalamin related parameters and disease patterns in patients with increased serum cobalamin levels. PLOS ONE. 2012;7:1-8.65. Arendt JFB, Pederson L, Nexo E, Sørensen HT. Elevated plasma vitamin b12 levels as a marker for cancer: a population-based cohort study. Journal of the National Cancer Institute. 2013;105(23):1799-1805.
M I D D L E E A S T J O U R N A L O F I N T ER N A L M ED I CI N E • VO LU M E 2 , I SSU E 3�0 MIDDLE EAST JOURNAL OF INTERNAL MEDICINE VOLUME 9 ISSUE 2 AUGUST 2016
Middle East Journal of Internal Medicine medi+WORLD International 2016
R E V I E W A R T I CL E
Middle East Journal of Internal Medicine medi+WORLD International 2016