Nudging the U.S. Defense Health Agency toward a facility infrastructure designed for change KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015 Stephen Kendall, PhD, RA Infill Systems US LLC Philadelphia, PA, 19119 www.infillsystemsus.com
Transcript
Nudging the U.S. Defense Health Agency toward a facility
infrastructure designed for change
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Stephen Kendall, PhD, RA Infill Systems US LLC
Philadelphia, PA, 19119 www.infillsystemsus.com
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Learning Objec>ve 1 Understand fundamental premises of healthcare facility design for flexibility Learning Objec>ve 2 Review several best prac<ce cases of healthcare facili<es designed for flexibility Learning Objec>ve 3 Hear recommenda<ons made to the DHA to adopt a new decision making model for acquiring flexible facili<es Learning Objec>ve 4 Discuss the implica<ons of adop<ng these recommenda<ons also in the private sector
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
FACT ONE: Hospitals, like cities, are never finished
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
FACT TWO: Detailed “architectural programs” are widely accepted as the necessary first step in healthcare facility planning • to document everything • to know the total cost • to avoid surprises
But ordinary “programs” are not useful when change is expected…
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
• Office buildings and shopping centers are designed to “churn”
• Clients ask architects to design empty base buildings with capacity for change, as a matter of course, with no controversy
• Other architects or interior architects design spaces for use, which are quite varied and inevitably change
• Specialized contractors and suppliers are responsible for each level
What “programs” make sense for office buildings and shopping centers?
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Change is an inescapable historical reality…but also permanence:
• The city structure is permanent relative to urban design • Urban design is permanent relative to the buildings • Buildings are permanent relative to their fit-out (functions) • Fit-out is permanent to the equipment and furnishings
Recognizing this hierarchical structure helps us manage change and uncertainty
THE KEY CONCEPT TO MANAGE CHANGE IS CAPACITY
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Courtesy Canton Bern OPB
Example: A Flexible Combat Infrastructure
• Capacity for change & development is possible at each level • Criteria and production for each level are separated but recognize other levels
• Interfaces are key design and management issues KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Courtesy Canton Bern OPB
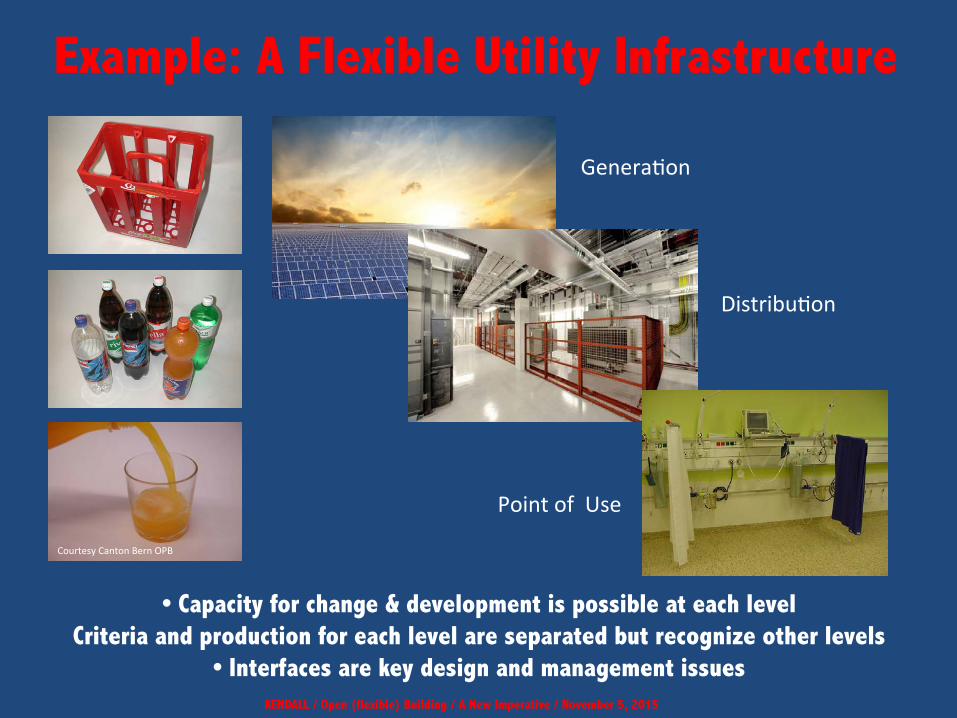
Example: A Flexible Utility Infrastructure
• Capacity for change & development is possible at each level Criteria and production for each level are separated but recognize other levels
• Interfaces are key design and management issues KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Courtesy Canton Bern OPB
Genera<on
Distribu<on
Point of Use
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
The Gonda Building at the Mayo Clinic Ellerbe Becket, Architects
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Conceptual Model- Separation of Circulation
• HVAC layout to allow for a variety of functional layouts
• Imaging • Clinic • Office • Labs
• Capacity for any use • Physician Office
• Future capacity
GONDA BUILDING @ MAYO CLINIC
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
infrastructure space fields
Banner Estrella Hospital in Phoenix architects: NBBJ
space fields
Circulation infrastructure
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Kortrijk Hospital in Belgium Baumschlater Eberle, Architects
Insel Hospital Campus, Bern, Switzerland
Another Example: INO hospital in Bern Primary System: Peter Kamm Secondary System: Itten &
Brechbuehl One of more than 20 projects using a Cantonal policy called SYSTEM SEPARATION
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Open (flexible) Building / A New Imperative / October 21, 2015
• Life cycle: 50-100 years • Long-term investment BASE BUILDING or PRIMARY SYSTEM • Life cycle: 5-20 years • Medium-term investment FIT-OUT or SECONDARY SYSTEM • Life cycle: 2-5 years • Short-term investment IO&T, FF&E or TERTIARY SYSTEM
Decoupled life-cycle decision levels
Courtesy Canton Bern OPB
Architecture on the Time Axis
Insel Hospital Campus, Bern, Switzerland
A variety of functional layouts on one typical floor Each is a proposal from one of the firms competing for the Secondary System design of the INO hospital in Bern The firm selected for the Secondary System had to accept the Primary System as its “site”.
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Primary system
Insel Hospital Campus, Bern, Switzerland
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Floor D -‐ opera<on clusters Floor E -‐ laboratories / intensive care
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
An example of managing the interface between permanent and changeable parts
The OLD ATTITUDE: it is more economical and it eases optimization when the “whole” with all its dependencies is programmed, designed and built accordingly.
That reasoning doesn’t see that a functionally complex project like a hospital can never be completely understood in advance because:
The need for changes is inevitable.
The whole is a development on the time axis.
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
THE NEW “Flexibility” CHALLENGE:
The analysis and determination of interfaces between levels requires an exploration of new management and technical solutions.
This is probably the most important aspect of OPEN (flexible) BUILDING
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
• Good infrastructure design offers decision flexibility through CAPACITY • Flexibility offers long-term ROI
• Criteria for long-lasting parts must be distinguished from criteria for shorter-term parts
• Independent groups can make criteria for (and design) each level, but each must understand the time horizons and drivers of the others
• An understanding of infrastructure interfaces is critical
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
SUMMARY
Courtesy Canton Bern OPB
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
FLEX I, II and III Three studies for the
Defense Health Agency
undertaken between 2012 and 2015 by a National Institute of Building Sciences research team
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
The question underlying the three studies
How should DHA (as an owner and portfolio manager) improve its business processes to assure that its healthcare facilities infrastructure is sustainable; i.e. prepared for change?
FLEX I & II
Consul>ng Team
• Thom D. Kurmel, DDES, AIA, President TDK Consul<ng, LLC
• Stephen H. Kendall, PhD, RA
Infill Systems US LLC
• Karel Dekker KD/Consultants BV, Strategic Research for
Building & Construc<on Voorburg, The Netherlands
Prepared by the Na>onal Ins>tute of Building Sciences 1090 Vermont Avenue, N.W., Suite 700, Washington, DC 20005
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Executive Summary
1. Decouple decisions • Separate decisions according to life-cycle principles (short-term decisions should not drive long term decisions);
2. Implement sequential decision-making • Implement sequential decision-making from the get-go; it’s how decision-making happens anyway into the future;
3. Design submittal documents need to demonstrate flexibility • Facility flexibility needs to be clear in design submittal documents and must be monitored by DHA;
4. A culture shift in DHA • DHA must adjust to “a continuum of facility care” to embed flexibility as a normal part of doing business.
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
New opportunity for just-in-time planning and cost estimating
Our basic recommendation:
Move from unified to sequential decision- making
Recommended Flex Requirements (for inclusion in the World Class Check-list)
1. Site Capacity 2. BUILDING EXPANSION FLEXIBILITY 3. GEOMETRY OF THE STRUCTURAL SYSTEM 4. NATURAL LIGHT 5. Floor-to-Floor Height Requirement 6. Loading Capacity of Floors 7. Minimal Internal Structural Walls 8. Flexible Facades 9. Separated Systems based on expected life expectancy 10. Layout and MEP flexibility for the Fit-Out 11. Opportunity for Vertical Mechanical Equipment in the Future 12. MULTIFUNCTIONAL USE OF ROOMS 13. Capacity for Variable Inpatient Bedroom Sizes (2, 3, 4, 12 are in the current check-list – we have made recommendations to augment them)
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Recommendations Recommendation 1:
FLEXIBILITY must be included as a tenet in the Medical Uniform Facilities Criteria (UFC) linking technical and project planning principles.
Recommendation 2:
Incorporate specific performance requirements to be followed in the acquisition and long-term exploitation (management, adaptation and conversion) of facilities.
Recommendation 3: Explicitly link requirements for flexible facilities with requirements for
sustainable-high performance buildings.
Recommendation 4:
Develop and implement systematic tracking of facility behavior over time.
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2015
Recommendations (continued) Recommendation 5: Implement, monitor and assess the suggested SEQUENTIAL planning and
acquisition process. Recommendation 6: Audit and revise (de-conflict) existing criteria Recommendation 7: Develop criteria for achieving flexibility of existing facilities Recommendation 8: Initiate a periodic shared learning forum
KENDALL / Open (flexible) Building / A New Imperative / November 5, 2016
FLEX III
Consulting Team
• Thom D. Kurmel, DDES, AIA, DBIA President , TDK Consulting, LLC
• Stephen H. Kendall, PhD, RA
Infill Systems US LLC
• Bart Harmon, MD, MPH, Clinical Informatics Experts, Inc.
• Ray Doyle, PE, WB Engineers+Consultants
• Randy Kray, AIA, HOK Architects
• Wendy Weitzner, FACHE, The Innova Group
• Nanne Davis Eliot, AIA, Esq., ADBIA, PMP National Institute of Building Sciences
5
Prepared by the Na>onal Ins>tute of Building Sciences 1090 Vermont Avenue, N.W., Suite 700, Washington, DC 20005
Open (flexible) Building / A New Imperative / October 21, 2015
Executive Summary 1. COORDINATED CRITERIA DEVELOPMENT
• The MHS should apply system-level resources in a routine process of coordinated criteria and standards development.
2. LONG-LASTING INFRASTRUCTURE
• The focus should be on acquisition of long-lasting infrastructure that is flexible by design - that is, evaluated on its capacity to accommodate changing missions, practices, and technologies.
3. HFEC and HFIC SHOULD BE USED
• Two existing organizational units - the Health Facilities Executive Committee (HFEC) and the Health Facilities Integration Council (HFIC) - should be used to implement the recommendations offered in this report.
Open (flexible) Building / A New Imperative / October 21, 2015
Key Findings 1. Medical technology (e.g. EHR, telemedicine, robotics, diagnostics, etc.) and
building technology (e.g. environmental controls, energy monitoring, etc.) are designed, installed and managed by different providers, and as such place sometimes conflicting demands on the MHS system;
2. HIT in the MHS – and especially the current EHR implementation project – is
now the major technology demand signal. 3. An effort focused on organizational alignment of Clinical Operations, HIT, CIO
and Facilities/Logistics is needed, with CLINOPS as the chief client and all other shared service entities providing support.
4. Development of MHS criteria for building technology needs renewed attention; 5. CIO and Facilities criteria in the MHS should complement each other; 6. The organization and hierarchical structure of current MHS facilities criteria are
confusing.
Open (flexible) Building / A New Imperative / October 21, 2015
Key Findings (continued) 7. The Facilities shared services team is under-resourced for the comprehensive
effort needed to sort out and streamline its outputs and processes.
8. The difficulties faced in facilities procurement with regard to facility flexibility (e.g. conflicts during IO&T IT installation with work done prior to equipment specification) need to be remedied.
9. The teams providing asset acquisition, maintenance and provisioning (facilities,
logistics, IT, maintenance) are not operating with the same vision or assumptions regarding their portfolio boundaries, resources, interface protocols, acquisition strategies and timing.
10. Current acquisitions (ROB and Bethesda) should be used to investigate new ways
of coordinating HIT, CIO, LOG and FAC efforts.
11. The FLEX III Survey was designed to help the MHS focus on areas that the field identified as needing additional coordination work. Criteria development efforts should focus on those areas first.
Open (flexible) Building / A New Imperative / October 21, 2015
Conclusions / Recommendations Recommendation #1:
Adopt recommendations and concepts of FLEX I and II Recommendation #2:
Build an interdisciplinary (coordinated) MHS System [Shared Service] criteria development capability
Recommendation #3:
DHA Facilities, HIT and Clinical Operations should join forces especially during the new EHR deployment
Recommendation #4:
Conduct and invest in an on-going criteria audit and updating process Recommendation #5:
DHA should develop building technology expertise Recommendation #6:
Create an interface resolution team Recommendation #7:
Invest in lessons learned
Open (flexible) Building / A New Imperative / October 21, 2015
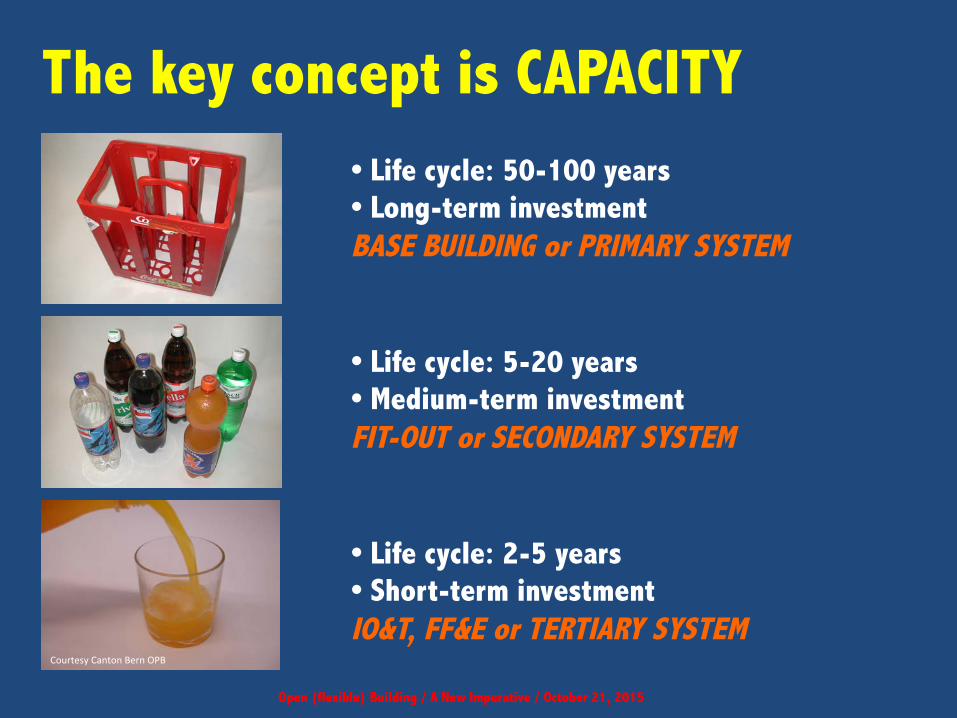
• Life cycle: 50-100 years • Long-term investment BASE BUILDING or PRIMARY SYSTEM • Life cycle: 5-20 years • Medium-term investment FIT-OUT or SECONDARY SYSTEM • Life cycle: 2-5 years • Short-term investment IO&T, FF&E or TERTIARY SYSTEM
The key concept is CAPACITY
Courtesy Canton Bern OPB
A NEEDED SHIFT IN PERSPECTIVE
FROM TO
• Assets understood as static • Assets understood as subject to transformation
• Decision making focused on the • Decision making over time (assets will
initial acquisition of an asset be transformed over time)
• Flexibility focused on technology • Flexibility focused on sequenced decision- making over time
• Flexibility separate from sustainability • Flexibility ENABLING sustainability • Flexibility as an option • Flexibility as a requirement
Open (flexible) Building / A New Imperative / October 21, 2015
Adopting Open (flexible) Building is imperative, but it is not inevitable…
…yet there are precedents…
Open (flexible) Building / A New Imperative / October 21, 2015
It’s time for OPEN (flexible) BUILDING to become ordinary
– an imperative just as important as
fire resistance and sustainability
THIS IS WHAT WE RECOMMENDED TO THE DHA
Open (flexible) Building / A New Imperative / October 21, 2015










































![Ethical Guidelines for Nudging in Information Security ... · practice. Nudging has been applied in a variety of contexts (e.g. health [2], smoking [3] and obesity [4]). Digital nudging](https://static.documents.pub/doc/80x56/5f8b61e51157ad021841dfeb/ethical-guidelines-for-nudging-in-information-security-practice-nudging-has.jpg)









