Page 1
1 of 22 6/7/17, 12:08 PM
Number: 0384
Policy
*Please see amendment for Pennsylvania Medicaid at the end
of this CPB.
Aetna considers magnetic resonance cholangiopancreatography
(MRCP) medically necessary when any of the following is met:
1. Based on the initial work‐up, the member only requires
diagnosis of suspected pancreaticobiliary pathology without
the need for therapeutic intervention; or
2. Member has a documented allergy to iodine‐based contrast
materials, or has a general history of atopy; or
3. Member has altered biliary tract anatomy that precludes
endoscopic retrograde cholangiopancreatography (ERCP) (e.g.,
post‐surgical biliary tract alterations, prior gastrectomy,
choledochojejunostomy, etc.); or
4. Member has undergone unsuccessful ERCP and requires
further evaluation; or
5. Member is an infant or young child, or is an adult who is
debilitated or uncooperative in such a manner that ERCP is
unsafe or cannot be performed; or
6. Member requires definition of pancreaticobiliary anatomy
proximal to a biliary tract system obstruction that cannot be
opened by ERCP; or
Last Review 04/13/2017
Effective: 02/01/2000
Next Review: 04/12/2018
Review History
Definitions
Clinical Policy Bulletin Notes
Page 2
2 of 22 6/7/17, 12:08 PM
7. Member requires evaluation for a suspected congenital
anomaly of the pancreaticobiliary tract (e.g., aberrant ducts,
choledochal cysts, pancreas divisum, etc.); or
8. Diagnosing biliary obstruction in orthoptic liver transplant
recipients.
Aetna considers MRCP experimental and investigational for all
other indications (e.g., diagnosing autoimmune pancreatitis, and
monitoring of persons with primary sclerosing cholangitis)
because its effectiveness for indications other than the ones listed
above has not been established.
Aetna considers MRCP without IV contrast experimental and
investigational in the staging of pancreatic cancer, except in cases
of renal failure or other contraindications to administration of
gadolinium intravenous contrast.
Background
Ultrasonography (US) and computed tomography (CT) scanning
have been the standard non‐invasive techniques for showing
biliary calculi and pancreatic diseases, although magnetic
resonance imaging (MRI) and more recently endoscopic
ultrasound have shown excellent results. Magnetic resonance
cholangiopancreatography (MRCP) is a new non‐invasive modality
that shows fluid in the biliary and pancreatic ducts in an axial or
three‐dimensional image format, somewhat comparable in
appearance and diagnostic accuracy to radiographic techniques
seen with direct contrast endoscopic retrograde
cholangiopancreatography (ERCP). The major advantages of
MRCP include: (i) does not require administration of exogenous
contrast materials; and (ii) the potential avoidance of a purely
diagnostic ERCP with its attendant complications of cholangitis
and post‐ERCP pancreatitis. The major disadvantages of MRCP
include: (i) the lack of therapeutic capability; (ii) MRCP images are
not satisfactorily comparable to those provided by ERCP; (iii)
inability to provide information with regard to resectability of
pancreatic cancer; and (iv) MRCP equipment is not available at
every institution.
Endoscopic retrograde cholangiopancreatography remains the
gold standard in the diagnostic work‐up of the pancreaticobiliary
Page 3
3 of 22 6/7/17, 12:08 PM
system. The real benefits of ERCP, as well as transhepatic
cholangiography, include: (i) ability to offer therapeutic
intervention at the time of the diagnostic procedure; (ii)
manometry can be performed; (iii) the ampulla of Vater can be
directly visualized; and (iv) the radiographic images obtained with
ERCP have a higher spatial resolution.
In current clinical practice, the majority of patients evaluated for
biliary tract disease have a high pre‐test likelihood of having a
problem requiring therapy (sphincterotomy, stone removal,
stenting, etc.), and should be directed toward ERCP for this
reason.
Magnetic resonance cholangiopancreatography may have a role
in those situations where initial evaluation suggests a benign
cause of biliary pathology requiring further cholangiographic
confirmation but not necessarily intervention. It may also be
useful in cases of failed ERCP before transhepatic
cholangiography, especially in cases where minimal intrahepatic
dilatation is suggested by ultrasound or CT, making percutaneous
transhepatic cholangiography more difficult. With complex
problems of the biliary tree, MRCP may allow a definitive
diagnosis, which may help plan a directed intervention
(endoscopic or transhepatic) that would have an increased
likelihood of success, with decreased risk. The utility of MRCP to
assess bile duct injuries, primary sclerosing cholangitis, sphincter
of Oddi dysfunction, and acute pancreatitis is unknown.
Fernandez‐Esparrach and colleagues (2007) compared the
diagnostic value of endoscopic ultrasonography (EUS) and MRCP
in: (i) patients with a dilated biliary tree unexplained by US (group
1), and (ii) the diagnosis of choledocholithiasis in patients with
non‐dilated biliary tree (group 2). Patients were prospectively
evaluated with EUS and MRCP. The gold standard used was
surgery or EUS‐FNA and ERCP, intra‐operative cholangiography, or
follow‐up when EUS and/or MRCP disclosed or precluded
malignancy, respectively. Likelihood ratios (LR) and pre‐test and
post‐test probabilities for the diagnosis of malignancy and
choledocholithiasis were calculated. A total of 159 patients met
one of the inclusion criteria but 24 of them were excluded for
Page 4
4 of 22 6/7/17, 12:08 PM
different reasons. Therefore, 135 patients constituted the study
population. The most frequent diagnosis was choledocholithiasis
(49 % in group 1 and 42 % in group 2, p = 0.380) and malignancy
was more frequent in group 1 (35 % versus 7 %, respectively, p <
0.001). When EUS and MRCP diagnosed malignancy, its
prevalence in this series (35 %) increased up to 98 % and 96 %,
respectively, whereas it decreased to 0 % and 2.6 % when EUS
and MRCP precluded this diagnosis. In patients in group 2, when
EUS and MRCP made a positive diagnosis of choledocholithiasis,
its prevalence (42 %) increased up to 78 % and 92 %, respectively,
whereas it decreased to 6 % and 9 % when any pathological
finding was ruled out. The authors concluded that EUS and MRCP
are extremely useful in diagnosing or excluding malignancy and
choledocholithiasis in patients with dilated and non‐dilated biliary
tree. Thus, they are critical in the approach to the management
of these patients.
McMahon (2008) evaluated the relative roles of MRCP and EUS in
the investigation of common bile duct (CD) calculi using
"evidence‐based practice" methods. A focused clinical question
was constructed. A structured search of primary and secondary
evidence was performed. Retrieved studies were appraised for
validity, strength and level of evidence (Oxford/CEBM scale: 1 to
5). Retrieved literature was divided into group A: MRCP slice
thickness greater than or equal to 5 mm, group B: MRCP slice
thickness = 3 mm or 3D‐MRCP sequences. Six studies were
eligible for inclusion (3 = level 1b, 3 = level 3b). Group A:
sensitivity and specificity of MRCP and EUS were (40 %, 96 %) and
(80 %, 95 %), respectively. Group B: sensitivity and specificity of
MRCP and EUS were (87 %, 95 %) and (90 %, 99 %), respectively.
The authors concluded that MRCP should be the first‐line
investigation for CD calculi and EUS should be performed when
MRCP is negative in patients with moderate or high pre‐test
probability.
Autoimmune pancreatitis (AIP) represents a special type of
chronic pancreatitis. It occurs most commonly in elderly males
with painless jaundice or mild abdominal pain. It is a relatively
newly recognized type of pancreatitis that is characterized by
diffuse or focal swelling of the pancreas due to lympho‐
Page 5
5 of 22 6/7/17, 12:08 PM
plasmacytic infiltration and fibrosis of the pancreatic
parenchyma. It is also known as ducto‐centric AIP, lobulo‐
centric AIP, idiopathic duct‐destructive pancreatitis, and lympho‐
plasmacytic sclerosing pancreatitis. The differential diagnosis of
AIP versus pancreatic cancer is important because AIP has been
found to respond to steroid treatment.
Fukumori and colleagues (20050 stated that MRCP visualizes only
the main pancreatic duct (MPD) in the pancreas head region.
Furthermore, while MRCP imaging of the MPD may be helpful in
the diagnosis of AIP, a negative result does not preclude such
diagnosis.
Carbognin et al (2009) retrospectively determined MRI, MRCP,
and secretin‐MRCP findings in patients with AIP. A total of 28
patients with histopathologically proven AIP were reviewed. In
14 cases, secretin‐enhanced MRCP was performed. The
observers evaluated pancreatic parenchymal enlargement, signal
intensity abnormalities, enhancement, vascular involvement,
bile‐duct diameter and MPD narrowing (diffuse/focal
/segmental). After secretin administration, the presence of the
"duct‐penetrating" sign was evaluated. Magnetic
resonance imaging showed diffuse pancreatic enlargement in
8/28 (29 %) cases, focal pancreatic enlargement in 16/28 (57 %)
cases and no enlargement in 4/28 (14 %) cases. The alteration of
pancreatic signal intensity was diffuse in 8/28 (29 %) cases (8
diffuse AIP) and focal in 20/28 (71 %) cases (20 focal AIP).
Delayed pancreatic enhancement was present in all AIP, with
peripheral rim of enhancement in 8/28 (29 %) AIP (1/8 diffuse,
7/20 focal); vascular encasement was present in 7/28 (25 %) AIP
(1/8 diffuse, 6/20 focal); distal common bile duct narrowing was
present in 12/28(43 %) AIP (5/8 diffuse, 7/20 focal). Magnetic
resonance cholangiopancreatography showed MPD narrowing in
17/28 (61 %) AIP (4/8 diffuse, 15/20 focal), MPD dilation in 8/28
(29 %) AIP (3/8 diffuse, 5/20 focal) and normal MPD in 1/8 diffuse
AIP. Secretin‐MRCP showed the duct‐penetrating sign in 6/14 (43
%) AIP (1 diffuse AIP with MPD segmental narrowing, 5 focal AIP
with MPD focal narrowing), demonstrating integrity of the MPD.
The authors concluded that delayed enhancement and MPD
stenosis are suggestive for AIP on MR and MRCP imaging.
Page 6
6 of 22 6/7/17, 12:08 PM
Kamisawa et al (2009) stated that it is important to differentiate
AIP from pancreatic cancer. Irregular narrowing of the MPD is a
characteristic finding in AIP; it is useful for differentiating AIP from
pancreatic cancer stenosis. These investigators evaluated the
usefulness of MRCP for the diagnosis of AIP and assessed if MRCP
could replace ERCP for diagnosing AIP. The MRCP and ERCP
findings of 20 AIP patients were compared. On MRCP, the
narrowed portion of the MPD was not visible, while the non‐
involved segments of the pancreatic duct were visible. The
degree of upstream dilatation of the proximal MPD was milder in
AIP than in pancreatic cancer patients. In the skipped type, only
skipped narrowed lesions were not visible. After steroid therapy
for AIP, the non‐visualized MPD became visible. The authors
concluded that MRCP can not replace ERCP for the diagnosis of
AIP, since narrowing of the MPD in AIP was not visible on MRCP.
Moreover, MRCP findings of segmental or skipped non‐visible
MPD accompanied by a less dilated upstream MPD
may suggest the presence of AIP.
In a review on AIP, Detlefsen and Drewes (2009) stated that
pathologically, AIP shows narrowing of the pancreatic ducts and
the intra‐pancreatic portion of the common bile duct.
Obstructive jaundice is a common symptom at presentation, and
pancreatic cancer represents an important clinical differential
diagnosis. In late stages of the disease, the normal pancreatic
parenchyma is often replaced by large amounts of fibrosis.
Histologically, there seem to be 2 subtypes of the disease: (i) one
showing infiltration with IgG4‐positive plasma cells but lacking
granulocytic epithelial lesions (GELs), and (ii) the other showing
GELs but lacking strong IgG4 positivity. On the basis of
conventional pancreatic imaging (e.g., contrast‐enhanced CT, EUS,
dynamic T2‐weighted MRI, and trans‐abdominal US), together
with serological measurement of IgG4 and evaluation of other
organ involvement, many AIP patients can be identified. The
remaining patients require further diagnostic work‐up. In these
patients, pancreatic core needle biopsy and a trial with steroids
(since AIP responds to steroid treatment) can help to differentiate
AIP from pancreatic cancer.
Greenberger (2009) noted that the diagnostic criteria of AIP
Page 7
7 of 22 6/7/17, 12:08 PM
proposed by the Mayo Clinic (the "HISORT" criteria) are most
commonly used in the United States and include the presence of
one or more of the following:
Diagnostic histology (based on resection specimen or
pancreatic core needle biopsy)
Response to steroid therapy of pancreatic (only in those
patients in whom a trial with steroid is indicated)/extra‐
pancreatic manifestations
Typical imaging (CT and pancreatography) plus any of the
following:
Compatible histology (i.e., at least supportive of AIP); or
Elevated serum IgG4 levels; or
Other organ involvement.
Moreover, Greenberger (2009) stated that ERCP or MRCP may
reveal a narrowed MPD and dorsal pancreatic duct; diffuse,
irregular narrowing of the pancreatic duct (beaded appearance),
or a focal stricture of the pancreatic duct, proximal or distal
common bile duct; or irregular narrowing of the intra‐hepatic
ducts. A stricture in the common bile duct or the finding of a
lesion in the head of the pancreas often prompts consideration of
malignancy. Thus, it may not be possible to distinguish AIP from
pancreatic cancer based upon the results of these imaging tests
alone.
Primary sclerosing cholangitis (PSC) is an immune‐
mediated, chronic cholestatic liver disease characterized by
progressive inflammation and fibrosis of the bile ducts, resulting
in biliary cirrhosis and is associated with a high‐risk of
cholangiocarcinoma (CCA), which develops in 10 to 30 % of PSC
patients. Early detection of CCA in PSC is achieved by using
serum tumor markers (carbohydrate antigen 19‐9 [CA 19‐9] and
carcinoembryonic antigen [CEA]), endoscopic ultrasonography
[EUS], as well as fluorescent in situ hybridization
[FISH] techniques to enhance the accuracy of biliary cytology
(Abbas and Lindor, 2009). Weismüller and colleagues (2008)
stated that the diagnosis of PSC is primarily based on endoscopic
cholangiography although MRI is increasingly used; biochemistry
Page 8
8 of 22 6/7/17, 12:08 PM
and immuno‐serology as well as histology play only a minor role.
Due to the high‐risk of developing CCA and also other tumours of
the GI tract, surveillance strategies are essential, however they
have yet to be established and evaluated. Karnam and associates
(2009) stated that ERCP remains preferred in patients with PSC.
Moreover, the role of MRCP in the diagnosis and management of
bile duct malignancy is not yet defined.
Weber and associates (2008) stated that MRCP is a less‐invasive
alternative to ERCP for the diagnosis of PSC. These investigators
evaluated the diagnostic accuracy of MRCP in PSC compared with
ERCP, and assessed the diagnostic accuracy of different T2w
sequences. A total of 95 patients (69 PSC, 26 controls) were
evaluated using both ERCP and MRCP. Exclusion criteria included
secondary sclerosing cholangitis and contraindications to MRCP.
The diagnosis of PSC was confirmed in 69 patients based on ERCP
as the reference gold standard. Magnetic resonance
cholangiopancreatography was performed using a 1.5 Tesla MR
unit, using breath hold, coronal and transverse half‐Fourier
acquisition single‐shot turbo spin‐echo (HASTE), coronal‐oblique,
fat‐suppressed half‐Fourier rapid acquisition with relaxation
enhancement (RARE), and coronal‐oblique, fat‐suppressed, multi‐
section, thin‐section HASTE (TS‐HASTE) sequences. The MRCP
morphological criteria of PSC were evaluated and compared with
ERCP. The sensitivity, specificity, and diagnostic accuracy were 86
%, 77 %, and 83 %, respectively, using the MRCP‐RARE sequence,
and increased further to 93 %, 77 %, and 88 %, respectively, by
the inclusion of follow‐up MRCP in 52 patients, performed at 6‐
and 12‐month intervals. HASTE and TS‐HASTE sequences showed
significantly lower diagnostic accuracy but provided additional
morphologic information. The authors concluded that MRCP can
diagnose PSC but has difficulties in early PSC and in cirrhosis, and
in the differentiation of cholangiocarcinoma, Caroli's disease, and
secondary sclerosing cholangitis. A positive MRCP would negate
some diagnostic ERCP studies; but a negative MRCP would not
obviate the need for ERCP.
In a meta‐analysis, Dave et al (2010) determined the diagnostic
accuracy of MRCP for detection of PSC in patients with
biochemical cholestasis. Two reviewers searched MEDLINE,
Page 9
9 of 22 6/7/17, 12:08 PM
EMBASE, and other electronic databases to identify prospective
studies in which MRCP was evaluated and compared with ERCP,
clinical examination, and/or histologic analysis for diagnosis of
PSC in cholestasis and control cases. Main study inclusion criteria
were (i) use of ERCP or percutaneous transhepatic
cholangiography (PTC) as part of the reference standard for the
diagnosis of PSC, (ii) inclusion of patients with hepatobiliary
disease other than PSC (i.e., non‐healthy control subjects), (iii)
blinding of MRCP image readers to reference‐standard results, (iv)
prospective study with ERCP or MRCP performed after subject
recruitment into the study, and (v) inclusion of raw data (for true‐
positive, false‐positive, true‐negative, and false‐negative results)
that could be found or calculated from the original study data.
Major exclusion criteria were duplicate article (on a primary
study) that contained all or some of the original study data and
inclusion of fewer than 10 patients with PSC. Methodologic
quality was assessed by using the Quality Assessment of
Diagnostic Accuracy Studies tool. Bi‐variate random‐effects meta‐
analytic methods were used to estimate summary, sensitivity,
specificity, and receiver operating characteristic (ROC) curves. A
total of 6 manuscripts with 456 subjects (with 623 independent
readings) ‐‐ 185 with PSC ‐‐ met the study inclusion criteria. The
summary area under the ROC curve was 0.91. High heterogeneity
(inconsistency index, 78 %) was found but became moderate
(inconsistency index, 36 %) with the exclusion of 1 study in which
the diagnostic threshold was set for high sensitivity. There was no
evidence of publication bias (p = 0.27, bias coefficient analysis).
Sensitivity and specificity of MRCP for PSC detection were 0.86
and 0.94, respectively. Positive and negative likelihood ratios with
MRCP were 15.3 and 0.15, respectively. In patients with high pre‐
test probabilities, MRCP enabled confirmation of PSC; in patients
with low pre‐test probabilities, MRCP enabled exclusion of PSC.
Worst‐ case‐scenario (pre‐test probability, 50 %) post‐test
probabilities were 94 % and 13 % for positive and negative MRCP
results, respectively. The authors concluded that MRCP has high
sensitivity and very high specificity for diagnosis of PSC. In many
cases of suspected PSC, MRCP is sufficient for diagnosis, and, thus,
the risks associated with ERCP can be avoided.
Page 10
10 of 22 6/7/17, 12:08 PM
In a prospective study, Nebiker and colleagues (2009) analyzed
the rate of clinically inapparent common bile duct (CBD) stones,
the predictive value of elevated liver enzymes for CBD stones, and
the influence of the radiological results on the peri‐operative
management. A total of 465 patients were cholecystectomized
within 18 months, mainly laparoscopically. Pre‐operative MRCP
was performed in 454 patients. With MRCP screening, clinically
silent CBD stones were found in 4 %. Elevated liver enzymes have
only a poor predictive value for the presence of CBD stones
(positive predictive value, 21 %; negative predictive value, 96 %).
Compared to the recent literature, the post‐operative morbidity in
this study was low (0 % bile duct injury, 0.4 % residual
gallstones). The authors concluded that although MRCP is
diagnostically useful in the peri‐operative management in some
cases, its routine use in the diagnosis related group (DRG)‐era may
not be justified due to the costs.
Jorgensen et al (2011) stated that biliary complications are the
second leading cause of morbidity and mortality in orthotopic
liver transplant (OLT) recipients. Endoscopic retrograde
cholangiography is considered the diagnostic criterion standard
for post‐orthotopic liver transplantation biliary obstruction, but
incurs significant risks. These researchers ascertained the
diagnostic accuracy of MRCP for biliary obstruction in OLT
patients. A systematic literature search identified studies
primarily examining the utility of MRCP in detecting post‐
orthotopic liver transplantation biliary obstruction. A meta‐
analysis was then performed according to the Quality of
Reporting Meta‐Analyses statement. A meta‐analysis of 9 studies
originally performed at major transplantation centers was carried
out. A total of 382 OLT patients with clinical suspicion of biliary
obstruction were included in this analysis. major outcome
measures were sensitivity and specificity of MRCP for diagnosis of
biliary obstruction. The composite sensitivity and specificity were
0.96 (95 % confidence interval [CI]: 0.92 to 0.98) and 0.94 (95 %
CI: 0.90 to 0.97), respectively. The positive and negative
likelihood ratios were 17 (95 % CI: 9.4 to 29.6) and 0.04 (95 % CI:
0.02 to 0.08), respectively. All but 1 included study had
significant design flaws that may have falsely increased the
reported diagnostic accuracy. The authors concluded that high
Page 11
11 of 22 6/7/17, 12:08 PM
sensitivity and specificity demonstrated in this meta‐analysis
suggested that MRCP is a promising test for diagnosing biliary
obstruction in patients who have undergone liver
transplantation. However, given the significant design flaws in
most of the component studies, additional high‐quality data are
necessary before unequivocally recommending MRCP in this
setting.
Giljaca et al (2015) stated that EUS and MRCP are tests used in
the diagnosis of common bile duct stones in patients suspected of
having common bile duct stones prior to undergoing invasive
treatment. There has been no systematic review of the accuracy
of EUS and MRCP in the diagnosis of common bile duct stones
using appropriate reference standards. These researchers
determined and compared the accuracy of EUS and MRCP for the
diagnosis of common bile duct stones. They searched MEDLINE,
EMBASE, Science Citation Index Expanded, BIOSIS, and
Clinicaltrials.gov until September 2012. In addition, they searched
the references of included studies to identify further
studies and of systematic reviews identified from various
databases (Database of Abstracts of Reviews of Effects (DARE),
Health Technology Assessment (HTA), Medion, and ARIF
(Aggressive Research Intelligence Facility)). They did not restrict
studies based on language or publication status, or whether data
were collected prospectively or retrospectively. These
investigators included studies that provided the number of true
positives, false positives, false negatives, and true negatives for
EUS or MRCP. They only accepted studies that confirmed the
presence of common bile duct stones by extraction of the stones
(irrespective of whether this was done by surgical or endoscopic
methods) for a positive test, and absence of common bile duct
stones by surgical or endoscopic negative exploration of the
common bile duct or symptom free follow‐up for at least 6
months for a negative test, as the reference standard in people
suspected of having common bile duct stones. They included
participants with or without prior diagnosis of cholelithiasis; with
or without symptoms and complications of common bile duct
stones, with or without prior treatment for common bile duct
stones; and before or after cholecystectomy. At least 2 authors
independently screened abstracts and selected studies for
Page 12
12 of 22 6/7/17, 12:08 PM
inclusion. Two authors independently collected the data from
each study. They used the bi‐variate model to obtain pooled
estimates of sensitivity and specificity. The authors included a
total of 18 studies involving 2,366 participants (976 participants
with common bile duct stones and 1,390 participants without
common bile duct stones); 11 studies evaluated EUS alone, and 5
studies evaluated MRCP alone; 2 studies evaluated both tests.
Most studies included patients who were suspected of having
common bile duct stones based on abnormal liver function tests;
abnormal trans‐abdominal ultrasound; symptoms such as
obstructive jaundice, cholangitis, or pancreatitis; or a
combination of the above. The proportion of participants who
had undergone cholecystectomy varied across studies. Not one
of the studies was of high methodological quality. For EUS, the
sensitivities ranged between 0.75 and 1.00 and the specificities
ranged between 0.85 and 1.00. The summary sensitivity (95 % CI)
and specificity (95 % CI) of the 13 studies that evaluated EUS
(1,537 participants; 686 cases and 851 participants without
common bile duct stones) were 0.95 (95 % CI: 0.91 to 0.97) and
1.97 (95 % CI: 0.94 to 0.99). For MRCP, the sensitivities ranged
between 0.77 and 1.00 and the specificities ranged between 0.73
and 0.99. The summary sensitivity and specificity of the 7 studies
that evaluated MRCP (996 participants; 361 cases and 635
participants without common bile duct stones) were 0.93 (95 %
CI: 0.87 to 0.96) and 0.96 (95 % CI: 0.90 to 0.98). There was no
evidence of a difference in sensitivity or specificity between EUS
and MRCP (p value = 0.5). From the included studies, at the
median pre‐test probability of common bile duct stones of 41 %
the post‐test probabilities (with 95 % CI) associated with positive
and negative EUS test results were 0.96 (95 % CI: 0.92 to 0.98)
and 0.03 (95 % CI: 0.02 to 0.06). At the same pre‐test probability,
the post‐test probabilities associated with positive and negative
MRCP test results were 0.94 (95 % CI: 0.87 to 0.97) and 0.05 (95
% CI: 0.03 to 0.09). The authors concluded that both EUS and
MRCP have high diagnostic accuracy for detection of common bile
duct stones. People with positive EUS or MRCP should undergo
endoscopic or surgical extraction of common bile duct stones and
those with negative EUS or MRCP do not need further invasive
tests. However, if the symptoms persist, further investigations
will be indicated. The 2 tests are similar in terms of diagnostic
Page 13
13 of 22 6/7/17, 12:08 PM
accuracy and the choice of which test to use will be informed by
availability and contra‐indications to each test.
An UpToDate review on “Magnetic resonance
cholangiopancreatography” (Karnam et al, 2015) states that
“Common bile duct stones ‐‐ The choice of procedure varies with
the clinical setting and local availability. In patients with
cholangitis, for example, ERCP is preferred because it permits
therapeutic drainage of the obstruction. However, MRCP may be
performed if cholangitis is not severe and the risks of ERCP are
high. MRCP may also be useful after unsuccessful or incomplete
ERCP and in imaging the CBD in patients undergoing laparoscopic
cholecystectomy. Endoscopic ultrasound may also be an option in
individuals considered at increased risk for ERCP”.
National Comprehensive Cancer Network’s clinical practice
guideline on “Pancreatic adenocarcinoma” (Version 1.2017) states
that “MR cholangiopancreatography (MRCP) without IV contrast
should not be utilized in the staging of pancreatic cancer, except
in cases of renal failure or other contraindications to
administration of gadolinium intravenous contrast”.
CPT Codes / HCPCS Codes / ICD‐10 Codes
Information in the [brackets] below has been added for clarification
purposes. Codes requiring a 7th character are represented by "+":
Other CPT codes related to the CPB:
43260 Endoscopic retrograde cholangiopancreatography
(ERCP); diagnostic, including collection of specimen(s)
by brushing or washing, when performed (separate
procedure)
74181 ‐
74183
Magnetic resonance (e.g., proton) imaging, abdomen
HCPCS codes covered if selection criteria are met:
S8037 Magnetic resonance cholangiopancreatography
(MRCP)
ICD‐10 codes covered if selection criteria are met:
B25.2 Cytomegaloviral pancreatitis
Page 14
14 of 22 6/7/17, 12:08 PM
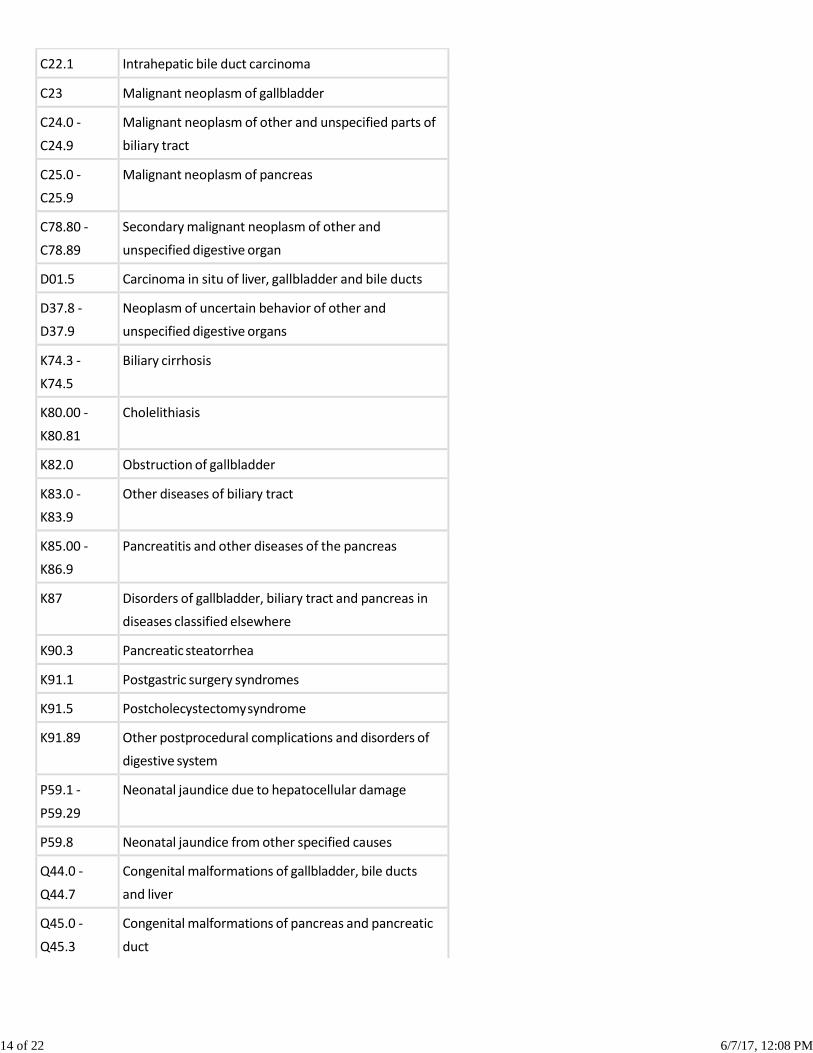
C22.1 Intrahepatic bile duct carcinoma
C23 Malignant neoplasm of gallbladder
C24.0 ‐
C24.9
Malignant neoplasm of other and unspecified parts of
biliary tract
C25.0 ‐
C25.9
Malignant neoplasm of pancreas
C78.80 ‐
C78.89
Secondary malignant neoplasm of other and
unspecified digestive organ
D01.5 Carcinoma in situ of liver, gallbladder and bile ducts
D37.8 ‐
D37.9
Neoplasm of uncertain behavior of other and
unspecified digestive organs
K74.3 ‐
K74.5
Biliary cirrhosis
K80.00 ‐
K80.81
Cholelithiasis
K82.0 Obstruction of gallbladder
K83.0 ‐
K83.9
Other diseases of biliary tract
K85.00 ‐
K86.9
Pancreatitis and other diseases of the pancreas
K87 Disorders of gallbladder, biliary tract and pancreas in
diseases classified elsewhere
K90.3 Pancreatic steatorrhea
K91.1 Postgastric surgery syndromes
K91.5 Postcholecystectomy syndrome
K91.89 Other postprocedural complications and disorders of
digestive system
P59.1 ‐
P59.29
Neonatal jaundice due to hepatocellular damage
P59.8 Neonatal jaundice from other specified causes
Q44.0 ‐
Q44.7
Congenital malformations of gallbladder, bile ducts
and liver
Q45.0 ‐
Q45.3
Congenital malformations of pancreas and pancreatic
duct
Page 15
15 of 22 6/7/17, 12:08 PM
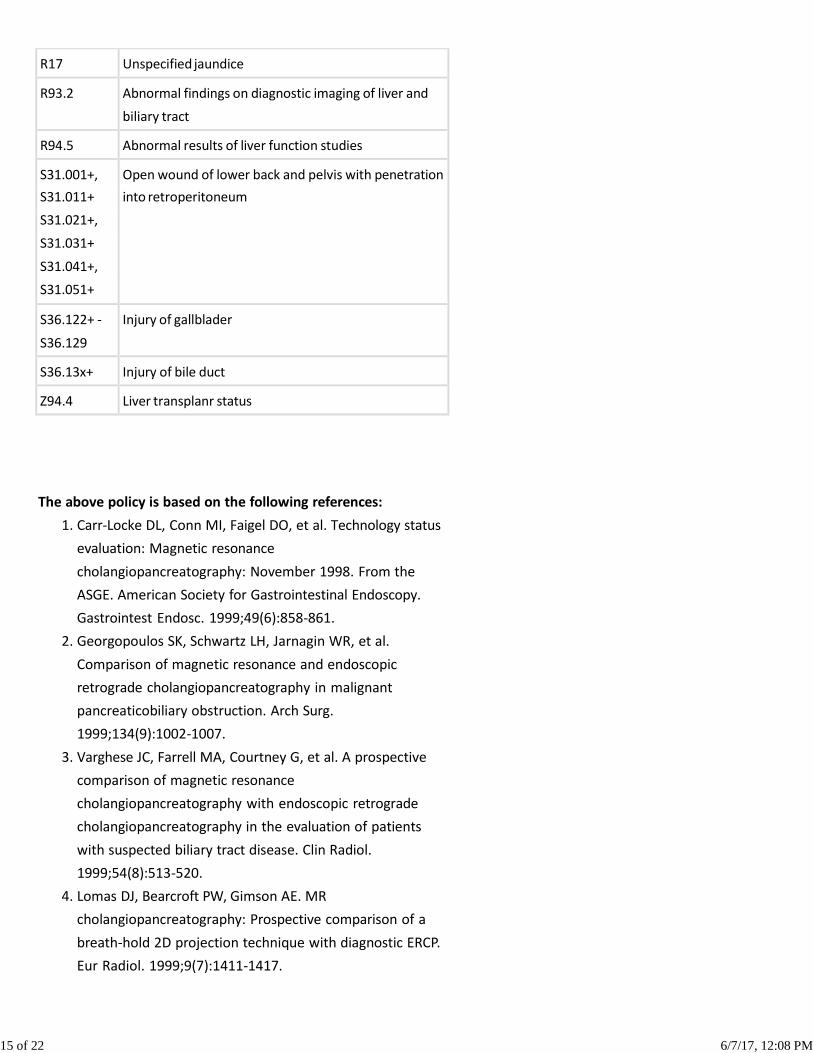
R17 Unspecified jaundice
R93.2 Abnormal findings on diagnostic imaging of liver and
biliary tract
R94.5 Abnormal results of liver function studies
S31.001+, Open wound of lower back and pelvis with penetration
S31.011+ into retroperitoneum
S31.021+,
S31.031+
S31.041+,
S31.051+
S36.122+ ‐
S36.129
Injury of gallblader
S36.13x+ Injury of bile duct
Z94.4 Liver transplanr status
The above policy is based on the following references:
1. Carr‐Locke DL, Conn MI, Faigel DO, et al. Technology status
evaluation: Magnetic resonance
cholangiopancreatography: November 1998. From the
ASGE. American Society for Gastrointestinal Endoscopy.
Gastrointest Endosc. 1999;49(6):858‐861.
2. Georgopoulos SK, Schwartz LH, Jarnagin WR, et al.
Comparison of magnetic resonance and endoscopic
retrograde cholangiopancreatography in malignant
pancreaticobiliary obstruction. Arch Surg.
1999;134(9):1002‐1007.
3. Varghese JC, Farrell MA, Courtney G, et al. A prospective
comparison of magnetic resonance
cholangiopancreatography with endoscopic retrograde
cholangiopancreatography in the evaluation of patients
with suspected biliary tract disease. Clin Radiol.
1999;54(8):513‐520.
4. Lomas DJ, Bearcroft PW, Gimson AE. MR
cholangiopancreatography: Prospective comparison of a
breath‐hold 2D projection technique with diagnostic ERCP.
Eur Radiol. 1999;9(7):1411‐1417.
Page 16
16 of 22 6/7/17, 12:08 PM
5. Hochwalk SN, Dobryansky M BA, Rofsky NM, et al.
Magnetic resonance cholangiopancreatography accurately
predicts the presence or absence of choledocholithiasis. J
Gastrointest Surg. 1998;2(6):573‐579.
6. Ferrucci JT. MRI and MRCP in pancreaticobiliary malignancy.
Ann Oncol. 1999;10 Suppl 4:18‐19.
7. Barish MA, Yucel EK, Ferrucci JT. Magnetic resonance
cholangiopancreatography. N Engl J Med.
1999;341(4):258‐264.
8. Halme L, Doepel M, von Numers H, et al. Complications of
diagnostic and therapeutic ERCP. Ann Chir Gynaecol.
1999;88(2):127‐131.
9. Deviere J, Matos C, Cremer M. The impact of magnetic
resonance cholangiopancreatography on ERCP. Gastrointest
Endosc. 1999;50(1):136‐140; discussion 140‐143.
10. Larena JA, Astigarraga E, Saralegui I, et al. Magnetic
resonance cholangiopancreatography in the evaluation of
pancreatic duct pathology. Br J Radiol.
1998;71(850):1100‐1104.
11. Sica GT, Braver J, Cooney MJ, et al. Comparison of
endoscopic retrograde cholangiopancreatography with MR
cholangiopancreatography in patients with pancreatitis.
Radiology. 1999;210(3):605‐610.
12. Owens GR, Shutz SM. Value of magnetic‐resonance
cholangiopancreatography (MRCP) after unsuccessful
endoscopic‐retrograde cholangiopancreatography (ERCP).
Gastrointest Endosc. 1999;49(2):265‐266.
13. Shimizu S, Kutsumi H, Fujimoto S, et al. Diagnostic
endoscopic retrograde cholangiopancreatography.
Endoscopy. 1999;31(1):74‐79.
14. Coakley FV, Schwartz LH. Magnetic resonance
cholangiopancreatography. J Magn Reson Imaging.
1999;9(2):157‐162.
15. Neuhaus H. The future of endoscopic retrograde
cholangiopancreatography: What is necessary and what
should be improved? Endoscopy. 1998;30(9):A207‐A211.
16. Fulcher AS, Turner MA, Capps GW. MR cholangiography:
Technical advances and clinical applications. Radiographics.
1999;19(1):25‐41; discussion 41‐44.
17. Barish MA, Soto JA, Yucel EK. Magnetic resonance
Page 17
17 of 22 6/7/17, 12:08 PM
cholangiopancreatography of the biliary ducts: Techniques,
clinical applications, and limitations. Top Magn Reson
Imaging. 1996;8:302‐311.
18. Bret PM, Reinhold C. Magnetic resonance
cholangiopancreatography. Endoscopy. 1997;29:472‐486.
19. Miyazaki T, Yamashita Y, Tang Y, et al. Single‐shot MR
cholangiopancreatography of neonates, infants, and young
children. Am J Radiol. 1998;170:33‐37.
20. Lee M‐G, Lee H‐J, Kim MH, et al. Extrahepatic biliary
diseases: 3D MR cholangiopancreatography compared with
endoscopic retrograde cholangiopancreatography.
Radiology. 1997;202:663‐669.
21. Soto JA, Barish MA, Yucel EK, et al. Magnetic resonance
cholangiography: Comparison with endoscopic retrograde
cholangiopancreatography. Gastroenterology.
1996;110:589‐597.
22. Hintze RE, Adler A, Veltske W, et al. Clinical significance of
magnetic resonance cholangiopancreatography (MRCP)
compared to endoscopic retrograde
cholangiopancreatography (ERCP). Endoscopy.
1997;29:182‐187.
23. Reinhold C, Bret PM, Guibaud L, et al. MR
cholangiopancreatography: Potential clinical applications.
Radiographics. 1996;16:309‐320.
24. Adamek HE, Albert J, Breer H, et al. Pancreatic cancer
detection with magnetic resonance
cholangiopancreatography and endoscopic retrograde
cholangiopancreatography: A prospective controlled
study. Lancet. 2000;356(9225):190‐193.
25. Eisen GM, Dominitz JA, Faigel DO, et al. An annotated
algorithmic approach to malignant biliary obstruction.
Gastrointest Endosc. 2001;53(7):849‐852.
26. Prasad SR, Sahani D, Saini S. Clinical applications of
magnetic resonance cholangiopancreatography. J Clin
Gastroenterol. 2001;33(5):362‐366.
27. Albert JG, Riemann JF. ERCP and MRCP ‐‐ when and
why. Best Pract Res Clin Gastroenterol. 2002;16(3):399‐419.
28. Kalra M, Sahani D, Ahmad A, et al. The role of magnetic
resonance cholangiopancreatography in patients with
suspected biliary obstruction. Curr Gastroenterol
Page 18
18 of 22 6/7/17, 12:08 PM
Rep. 2002;4(2):160‐166.
29. Aronson N, Flamm CR, Mark D, et al. Endoscopic retrograde
cholangiopancreatography. Summary, Evidence
Report/Technology Assessment: Number 50. AHRQ
Publication No. 02‐E008. Rockville, MD: Agency for
Healthcare Research and Quality (AHRQ); January
2002. Available at: http://www.ahrq.gov/clinic/epcsums
/ercpsum.htm. Accessed October 30, 2002.
30. Balfe DM, Ralls PW, Bree RL, et al. Imaging strategies in the
evaluation of the jaundiced patient. American College of
Radiology. ACR Appropriateness Criteria. Radiology.
2000;215(Suppl):125‐133.
31. American College of Radiology (ACR). ACR Appropriateness
Criteria™ for acute pancreatitis. Reston, VA: ACR; 2001.
32. Motohara T, Semelka RC, Bader TR. MR
cholangiopancreatography. Radiol Clin North
Am. 2003;41(1):89‐96.
33. Fayad LM, Kowalski T, Mitchell DG. MR
cholangiopancreatography: Evaluation of common
pancreatic diseases. Radiol Clin North
Am. 2003;41(1):97‐114.
34. Kaltenthaler E, Vergel YB, Chilcott J, et al. A systematic
review and economic evaluation of magnetic resonance
cholangiopancreatography compared with diagnostic
endoscopic retrograde cholangiopancreatography. Health
Technol Assess. 2004;8(10):iii, 1‐89.
35. Dalal PU, Howlett DC, Sallomi DF, et al. Does intravenous
glucagon improve common bile duct visualisation during
magnetic resonance cholangiopancreatography? Results in
42 patients. Eur J Radiol. 2004;49(3):258‐261.
36. Metreweli C, So NM, Chu WC, Lam WW. Magnetic
resonance cholangiography in children. Br J Radiol.
2004;77(924):1059‐1064.
37. Andersson M, Kostic S, Johansson M, et al. MRI combined
with MR cholangiopancreatography versus helical CT in the
evaluation of patients with suspected periampullary
tumors: A prospective comparative study. Acta Radiol.
2005;46(1):16‐27.
38. Hallal AH, Amortegui JD, Jeroukhimov IM, et al. Magnetic
resonance cholangiopancreatography accurately detects
Page 19
19 of 22 6/7/17, 12:08 PM
common bile duct stones in resolving gallstone pancreatitis.
J Am Coll Surg. 2005;200(6):869‐875.
39. Shanmugam V, Beattie GC, Yule SR, et al. Is magnetic
resonance cholangiopancreatography the new gold
standard in biliary imaging? Br J Radiol.
2005;78(934):888‐893.
40. Romagnuolo J, Bardou M, Rahme E, et al. Magnetic
resonance cholandiopancreatography: A metaanalysis of
test performance in suspected biliary disease. Ann Intern
Med. 2003;139(7):547‐557.
41. Medical Services Advisory Committee (MSAC). Magnetic
resonance cholangiopancreatography. MSAC Reference 25.
Canberra, ACT: MSAC; 2005.
42. Verma D, Kapadia A, Eisen GM, Adler DG. EUS vs MRCP for
detection of choledocholithiasis. Gastrointest Endosc.
2006;64(2):248‐254.
43. Hoeffel C, Azizi L, Lewin M, et al. Normal and pathologic
features of the postoperative biliary tract at 3D MR
cholangiopancreatography and MR imaging. Radiographics.
2006;26(6):1603‐1620.
44. Halefoglu AM. Magnetic resonance
cholangiopancreatography: A useful tool in the evaluation
of pancreatic and biliary disorders. World J Gastroenterol.
2007;13(18):2529‐2534.
45. Tipnis NA, Werlin SL. The use of magnetic resonance
cholangiopancreatography in children. Curr Gastroenterol
Rep. 2007;9(3):225‐229.
46. Fernández‐Esparrach G, Ginès A, Sánchez M, et al.
Comparison of endoscopic ultrasonography and magnetic
resonance cholangiopancreatography in the diagnosis of
pancreatobiliary diseases: A prospective study. Am J
Gastroenterol. 2007;102(8):1632‐1639.
47. McMahon CJ. The relative roles of magnetic resonance
cholangiopancreatography (MRCP) and endoscopic
ultrasound in diagnosis of common bile duct calculi: A
critically appraised topic. Abdom Imaging. 2008;33(1):6‐9.
48. Jain M, Agarwal A. MRCP findings in recurrent pyogenic
cholangitis. Eur J Radiol. 2008;66(1):79‐83.
49. McMahon CJ. The relative roles of magnetic resonance
cholangiopancreatography (MRCP) and endoscopic
Page 20
20 of 22 6/7/17, 12:08 PM
ultrasound in diagnosis of common bile duct calculi: A
critically appraised topic. Abdom Imaging. 2008;33(1):6‐9.
50. McMahon CJ. The relative roles of magnetic resonance
cholangiopancreatography (MRCP) and endoscopic
ultrasound in diagnosis of malignant common bile duct
calculi: A critically appraised topic. Abdom Imaging.
2008;33(1):10‐13.
51. Hekimoglu K, Ustundag Y, Dusak A, et al. MRCP vs. ERCP in
the evaluation of biliary pathologies: Review of current
literature. J Dig Dis. 2008;9(3):162‐169.
52. Fukumori K, Shakado S, Miyahara T, et al. Atypical
manifestations of pancreatitis with autoimmune
phenomenon in an adolescent female. Intern Med.
2005;44(8):886‐891.
53. Weismüller TJ, Wedemeyer J, Kubicka S, et al. The
challenges in primary sclerosing cholangitis ‐‐
aetiopathogenesis, autoimmunity, management and
malignancy. J Hepatol. 2008;48 Suppl 1:S38‐S57.
54. Carbognin G, Girardi V, Biasiutti C, et al. Autoimmune
pancreatitis: Imaging findings on contrast‐enhanced MR,
MRCP and dynamic secretin‐enhanced MRCP. Radiol Med.
2009;114(8):1214‐1231.
55. Kamisawa T, Tu Y, Egawa N, et al. Can MRCP replace ERCP
for the diagnosis of autoimmune pancreatitis? Abdom
Imaging. 2009;34(3):381‐384.
56. Detlefsen S, Drewes AM. Autoimmune pancreatitis. Scand J
Gastroenterol. 2009;44(12):1391‐1407.
57. Greenberger NJ. Autoimmune pancreatitis. UpToDate
[online serial]. Waltham, MA: UpToDate; reviewed
September 2009.
58. Abbas G, Lindor KD. Cholangiocarcinoma in primary
sclerosing cholangitis. J Gastrointest Cancer.
2009;40(1‐2):19‐25.
59. Karnam US, Kruskal JB, Reddy KR. Magnetic resonance
cholangiopancreatography. UpToDate [online serial].
Waltham, MA: UpToDate; reviewed September 2009.
60. Weber C, Kuhlencordt R, Grotelueschen R, et al. Magnetic
resonance cholangiopancreatography in the diagnosis of
primary sclerosing cholangitis. Endoscopy.
2008;40(9):739‐745.
Page 21
21 of 22 6/7/17, 12:08 PM
61. Nebiker CA, Baierlein SA, Beck S, et al. Is routine MR
cholangiopancreatography (MRCP) justified prior to
cholecystectomy? Langenbecks Arch Surg.
2009;394(6):1005‐1010.
62. Sugumar A, Chari ST. Diagnosis and treatment of
autoimmune pancreatitis. Curr Opin Gastroenterol.
2010;26(5):513‐518.
63. Dave M, Elmunzer BJ, Dwamena BA, Higgins PD. Primary
sclerosing cholangitis: Meta‐analysis of diagnostic
performance of MR cholangiopancreatography. Radiology.
2010;256(2):387‐396.
64. Jorgensen JE, Waljee AK, Volk ML, et al. Is MRCP equivalent
to ERCP for diagnosing biliary obstruction in orthotopic liver
transplant recipients? A meta‐analysis. Gastrointest Endosc.
2011;73(5):955‐962.
65. Xu YB1, Min ZG, Jiang HX, et al. Diagnostic value of
magnetic resonance cholangiopancreatography for biliary
complications in orthotopic liver transplantation: A meta‐
analysis. Transplant Proc. 2013;45(6):2341‐2346.
66. Rustagi T, Njei B. Magnetic resonance
cholangiopancreatography in the diagnosis of pancreas
divisum: A systematic review and meta‐analysis. Pancreas.
2014;43(6):823‐828.
67. Giljaca V, Gurusamy KS, Takwoingi Y, et al. Endoscopic
ultrasound versus magnetic resonance
cholangiopancreatography for common bile duct stones.
Cochrane Database Syst Rev. 2015;2:CD011549.
68. Karnam US, Kruskal JB, Reddy KR. Magnetic resonance
cholangiopancreatography. UpToDate [online serial].
Waltham, MA: UpToDate; reviewed February 2015.
69. Polistina FA, Frego M, Bisello M, et al. Accuracy of magnetic
resonance cholangiography compared to operative
endoscopy in detecting biliary stones, a single center
experience and review of literature. World J Radiol.
2015;7(4):70‐78.
70. Ward WH, Fluke LM, Hoagland BD, et al. The role of
magnetic resonance cholangiopancreatography in the
diagnosis of choledocholithiasis: Do benefits outweigh the
costs? Am Surg. 2015;81(7):720‐725.
71. Shen Z, Munker S, Zhou B, et al. The accuracies of
Page 22
22 of 22 6/7/17, 12:08 PM
diagnosing pancreas divisum by magnetic resonance
cholangiopancreatography and endoscopic ultrasound: A
systematic review and meta‐analysis. Sci Rep.
2016;6:35389.
72. De Castro VL, Moura EG, Chaves DM, et al. Endoscopic
ultrasound versus magnetic resonance
cholangiopancreatography in suspected
choledocholithiasis: A systematic review. Endosc
Ultrasound. 2016;5(2):118‐128.
73. Kang HJ, Lee JM, Joo I, et al. Assessment of malignant
potential in intraductal papillary mucinous neoplasms of
the pancreas: Comparison between multidetector CT and
MR imaging with MR cholangiopancreatography. Radiology.
2016;279(1):128‐139.
74. National Comprehensive Cancer Network
(NCCN). Pancreatic adenocarcinoma. NCCN Clinical Practice
Guidelines in Oncology, Ve rsion 1.2017. Fort Washington,
PA : NCCN; 2017.
Page 23
23 of 22 6/7/17, 12:08 PM
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in administering plan
benefits and constitute neither offers of coverage nor medical advice. This Clinical Policy Bulletin contains only a
partial, general description of plan or program benefits and does not constitute a contract. Aetna does not provide
health care services and, therefore, cannot guarantee any results or outcomes. Participating providers are
independent contractors in private practice and are neither employees nor agents of Aetna or its affiliates. Treating
providers are solely responsible for medical advice and treatment of members. This Clinical Policy Bulletin may be
updated and therefore is subject to change.
Copyright © 2001‐2017 Aetna Inc.
Page 24
AETNA BETTER HEALTH® OF PENNSYLVANIA
Amendment to Aetna Clinical Policy Bulletin Number:
0384 Magnetic Resonance Cholangiopancreatography
There are no amendments for Medicaid.
www.aetnabetterhealth.com/pennsylvania revised 06/09/2017