55
NURSING CARE ELECTRICAL BURN INJURY IN ICU BANJARMASIN ULIN HOSPITAL 2 ND Group : Esmy Maulidya M. Nurmajid Nurlailatul Khairiyyah H. M. Syafi’i Nor Amali Hidayatni Khairunisa
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | rizal-ahmad |
| View: | 87 times |
| Download: | 5 times |

NURSING CARE
ELECTRICAL BURN INJURY IN ICU
BANJARMASIN ULIN HOSPITAL
2ND Group :
Esmy Maulidya
M. Nurmajid
Nurlailatul Khairiyyah
H. M. Syafi’i
Nor Amali Hidayatni
Khairunisa
Banjarmasin Muhammadiyah Health College
International Class Of Nursing Diploma Program
Academic Year 2013 / 2014

Objectives
After accomplished this case, the student will be
- Select the appropriate nursing theory and apply its principles in
rendering nursing care to a patient with suffering second degree
burn wound prior.
- Discuss the anatomy and physiology of the integumentary system
that are directly affected in a second degree burn and relate the
concept to the actual situation to the patient
- Explain the pathophysiology of a burn wound infection
- Determine the nursing priorities and nursing management requisite
and executable in a second degree burn case, and incorporate these
data with nursing care plan.
- Distinguish the different pharmacologic actions of the drugs
involved in treatment of a second degree.
- Formulate elevant health teachings and outpatient care for a patient
with a second degree after being discharge
Nursing Care Of Nursing Clinical Practice
International Class Of Nursing Diploma Program
Banjarmasin Muhammadiyah Health College
A. SHORT HISTORY OF CLENT
In the assessment on December 24th, 2013 at 11.00 a.m. Client’s name is Mr. A. He is 30 years old. He is a moslem. He is a dayakese. His job is an electrical repairer. He lives on Basarang, Kapuas, Kalimantan Tengah. Client was hospitalized with the medical diagnosis Electrical burn injury (combustio) grade III (Full Thickness) ± 29,25% with inhalation trauma.
Health history of client, on December 23th, 2013 at 02.00 p.m. the client repaired the trafo in Batulicin that was mispredicted as light off but actually not, because that is client duty as a electrical repairer in central-south kalimantan so he did his job, when client repaired the trafo and cut the cable, suddenly client got electrical shock and it burned half of his face and chest, his left wrist and left leg. After that client was admitted to the nearest hospital by people around there . During the way to the hospital client was fainting and was hospitalized on emergency room for about 5 hours and because client had a bad condition the doctor decided to move the client to the banjarmasin ulin general hospital and stayed on emergency room for debridement in surgical room and immeadietly moved to the ICU room on December 24th, 2013.
The data that were found on the client during assessment are client concioussness level is Composmentis , GCS : E4V5M6 , client’s blood pressure is 110/70 mmHg, pulse is 90x/minutes , RR is 31x/minutes and temperature is 36,8C, heart sound is I and II , chest auscultation sounds wheezing, abdomen is palpable flat, soft , liver/lymph within normal limit , peristaltic sound is 10x/m , neurological status : pupil is isocor , pupil’s diameter 3/3 , pupil reflex is positive , motor : muscle strength on upper extremities are 4444/3333 and on lower extremities is 4444/4444 , there is catheter installation on December 24th 2013, client wear oxygen mask 8 lpm, finger saturation is 65% , based on rule of nine form found : 29.25%

on the half of face (2.25%) the front of the chest (9%), the majority of the left hand (9%), and the right hand (9%).
Diagnostic examination; CT-Scan (-), thorax photo is normal, laboratorium examination result on December 24th 2013; Hb: 14,8, leucosit 17,9, eritrosit 4,95, trombosit 256, MCV 86,7, MCH 29,8, MCHC 34,4, ureum 20, kreatinin 0,9, GDS 145, kalium 3,9, chlorida 105, natrium 141,4, blood gas analysis; pH: 7,4, PACO2: 46,8, PAO2: 78,0, O2 saturation: 80,3, BE: 1,1, HCO3: 26,5, lactate Dehydrogenises 450, CKMB 23 .
Client said that never know of this disease before. And client said
that he has never been treated in hospital. The client doesn’t have a
history of hypertension or diabetes mellitus.
Client said that was no client family who have suffered the same
disease that client suffering now. And families who have no other
serious illnes.

B. ANATOMY OF INTEGUMENTARY SYSTEM
The integumentary system is an organ system consisting of the skin,
hair, nails, and exocrine glands. The skin is only a few millimeters thick yet
is by far the largest organ in the body. The average person’s skin weighs
10 pounds and has a surface area of almost 20 square feet. Skin forms the
body’s outer covering and forms a barrier to protect the body from
chemicals, disease, UV light, and physical damage. Hair and nails extend
from the skin to reinforce the skin and protect it from environmental
damage. The exocrine glands of the integumentary system produce sweat,
oil, and wax to cool, protect, and moisturize the skin’s surface.
Epidermis

The epidermis is the most superficial layer of the skin that covers
almost the entire body surface. The epidermis rests upon and
protects the deeper and thicker dermis layer of the skin.
Structurally, the epidermis is only about a tenth of a millimeter thick
but is made of 40 to 50 rows of stacked squamous epithelial cells.
The epidermis is an avascular region of the body, meaning that it
does not contain any blood or blood vessels. The cells of the
epidermis receive all of their nutrients via diffusion of fluids from the
dermis.
The epidermis is made of several specialized types of cells.
Almost 90% of the epidermis is made of cells known as
keratinocytes. Keratinocytes develop from stem cells at the base of
the epidermis and begin to produce and store the protein keratin.
Keratin makes the keratinocytes very tough, scaly and water-
resistant. At about 8% of epidermal cells, melanocytes form the
second most numerous cell type in the epidermis. Melanocytes
produce the pigment melanin to protect the skin from ultraviolet
radiation and sunburn. Langerhans cells are the third most common
cells in the epidermis and make up just over 1% of all epidermal
cells. Langerhans cells’ role is to detect and fight pathogens that
attempt to enter the body through the skin. Finally, Merkel cells
make up less than 1% of all epidermal cells but have the important
function of sensing touch. Merkel cells form a disk along the deepest
edge of the epidermis where they connect to nerve endings in the
dermis to sense light touch.
The epidermis in most of the body is arranged into 4 distinct
layers. In the palmar surface of the hands and plantar surface of the
feet, the skin is thicker than in the rest of the body and there is a
fifth layer of epidermis. The deepest region of the epidermis is the
stratum basale, which contains the stem cells that reproduce to
form all of the other cells of the epidermis. The cells of the stratum
basale include cuboidal keratinocytes, melanocytes, and Merkel

cells. Superficial to stratum basale is the stratum spinosum layer
where Langerhans cells are found along with many rows of spiny
keratinocytes. The spines found here are cellular projections called
desmosomes that form between keratinocytes to hold them
together and resist friction. Just superficial to the stratum spinosum
is the stratum granulosum, where keratinocytes begin to produce
waxy lamellar granules to waterproof the skin. The keratinocytes in
the stratum granulosum are so far removed from the dermis that
they begin to die from lack of nutrients. In the thick skin of the
hands and feet, there is a layer of skin superficial to the stratum
granulosum known as the stratum lucidum. The stratum lucidum is
made of several rows of clear, dead keratinocytes that protect the
underlying layers. The outermost layer of skin is the stratum
corneum. The stratum corneum is made of many rows of flattened,
dead keratinocytes that protect the underlying layers. Dead
keratinocytes are constantly being shed from the surface of the
stratum corneum and being replaced by cells arriving from the
deeper layers.
Dermis
The dermis is the deep layer of the skin found under the
epidermis. The dermis is mostly made of dense irregular connective
tissue along with nervous tissue, blood, and blood vessels. The
dermis is much thicker than the epidermis and gives the skin its
strength and elasticity. Within the dermis there are two distinct
regions: the papillary layer and the reticular layer.
The papillary layer is the superficial layer of the dermis that
borders on the epidermis. The papillary layer contains many finger-
like extensions called dermal papillae that protrude superficially

towards the epidermis. The dermal papillae increase the surface
area of the dermis and contain many nerves and blood vessels that
are projected toward the surface of the skin. Blood flowing through
the dermal papillae provide nutrients and oxygen for the cells of the
epidermis. The nerves of the dermal papillae are used to feel touch,
pain, and temperature through the cells of the epidermis.
The deeper layer of the dermis, the reticular layer, is the
thicker and tougher part of the dermis. The reticular layer is made
of dense irregular connective tissue that contains many tough
collagen and stretchy elastin fibers running in all directions to
provide strength and elasticity to the skin. The reticular layer also
contains blood vessels to support the skin cells and nerve tissue to
sense pressure and pain in the skin.
Hypodermis
Deep to the dermis is a layer of loose connective tissues
known as the hypodermis, subcutis, or subcutaneous tissue. The
hypodermis serves as the flexible connection between the skin and
the underlying muscles and bones as well as a fat storage area.
Areolar connective tissue in the hypodermis contains elastin and
collagen fibers loosely arranged to allow the skin to stretch and
move independently of its underlying structures. Fatty adipose
tissue in the hypodermis stores energy in the form of triglycerides.
Adipose also helps to insulate the body by trapping body heat
produced by the underlying muscles.
PHYSIOLOGY OF THE INTEGUMENTARY SYSTEM
Keratinization

Keratinization, also known as cornification, is the process of
keratin accumulating within keratinocytes. Keratinocytes begin their
life as offspring of the stem cells of the stratum basale. Young
keratinocytes have a cuboidal shape and contain almost no keratin
protein at all. As the stem cells multiply, they push older
keratinocytes towards the surface of the skin and into the superficial
layers of the epidermis. By the time keratinocytes reach the stratum
spinosum, they have begun to accumulate a significant amount of
keratin and have become harder, flatter, and more water resistant.
As the keratinocytes reach the stratum granulosum, they have
become much flatter and are almost completely filled with keratin.
At this point the cells are so far removed from the nutrients that
diffuse from the blood vessels in the dermis that the cells go
through the process of apoptosis. Apoptosis is programmed cell
death where the cell digests its own nucleus and organelles, leaving
only a tough, keratin-filled shell behind. Dead keratinocytes moving
into the stratum lucidum and stratum corneum are very flat, hard,
and tightly packed so as to form a keratin barrier to protect the
underlying tissues.
Temperature Homeostasis
Being the body’s outermost organ, the skin is able to regulate
the body’s temperature by controlling how the body interacts with
its environment. In the case of the body entering a state of
hyperthermia, the skin is able to reduce body temperature through
sweating and vasodilation. Sweat produced by sudoriferous glands
delivers water to the surface of the body where it begins to
evaporate. The evaporation of sweat absorbs heat and cools the
body’s surface. Vasodilation is the process through which smooth
muscle lining the blood vessels in the dermis relax and allow more
blood to enter the skin. Blood transports heat through the body,

pulling heat away from the body’s core and depositing it in the skin
where it can radiate out of the body and into the external
environment.
In the case of the body entering a state of hypothermia, the
skin is able to raise body temperature through the contraction of
arrector pili muscles and through vasoconstriction. The follicles of
hairs have small bundles of smooth muscle attached to their base
called arrector pili muscles. The arrector pili form goose bumps by
contracting to move the hair follicle and lifting the hair shaft upright
from the surface of the skin. This movement results in more air
being trapped under the hairs to insulate the surface of the body.
Vasoconstriction is the process of smooth muscles in the walls of
blood vessels in the dermis contracting to reduce the flood of blood
to the skin. Vasoconstriction permits the skin to cool while blood
stays in the body’s core to maintain heat and circulation in the vital
organs.
Vitamin D Synthesis
Vitamin D, an essential vitamin necessary for the absorption
of calcium from food, is produced by ultraviolet (UV) light striking
the skin. The stratum basale and stratum spinosum layers of the
epidermis contain a sterol molecule known as 7-dehydrocholesterol.
When UV light present in sunlight or tanning bed lights strikes the
skin, it penetrates through the outer layers of the epidermis and
strikes some of the molecules of 7-dehydrocholesterol, converting it
into vitamin D3. Vitamin D3 is converted in the kidneys into
calcitriol, the active form of vitamin D.
Protection

The skin provides protection to its underlying tissues from
pathogens, mechanical damage, and UV light. Pathogens, such as
viruses and bacteria, are unable to enter the body through unbroken
skin due to the outermost layers of epidermis containing an
unending supply of tough, dead keratinocytes. This protection
explains the necessity of cleaning and covering cuts and scrapes
with bandages to prevent infection. Minor mechanical damage from
rough or sharp objects is mostly absorbed by the skin before it can
damage the underlying tissues. Epidermal cells reproduce
constantly to quickly repair any damage to the skin. Melanocytes in
the epidermis produce the pigment melanin, which absorbs UV light
before it can pass through the skin. UV light can cause cells to
become cancerous if not blocked from entering the body.
Skin Color
Human skin color is controlled by the interaction of 3
pigments: melanin, carotene, and hemoglobin. Melanin is a brown or
black pigment produced by melanocytes to protect the skin from UV
radiation. Melanin gives skin its tan or brown coloration and
provides the color of brown or black hair. Melanin production
increases as the skin is exposed to higher levels of UV light resulting
in tanning of the skin. Carotene is another pigment present in the
skin that produces a yellow or orange cast to the skin and is most
noticeable in people with low levels of melanin. Hemoglobin is
another pigment most noticeable in people with little melanin.
Hemoglobin is the red pigment found in red blood cells, but can be
seen through the layers of the skin as a light red or pink color.
Hemoglobin is most noticeable in skin coloration during times of
vasodilation when the capillaries of the dermis are open to carry
more blood to the skin’s surface.

Cutaneous Sensation
The skin allows the body to sense its external environment by
picking up signals for touch, pressure, vibration, temperature, and
pain. Merkel disks in the epidermis connect to nerve cells in the
dermis to detect shapes and textures of objects contacting the skin.
Corpuscles of touch are structures found in the dermal papillae of
the dermis that also detect touch by objects contacting the skin.
Lamellar corpuscles found deep in the dermis sense pressure and
vibration of the skin. Throughout the dermis there are many free
nerve endings that are simply neurons with their dendrites spread
throughout the dermis. Free nerve endings may be sensitive to pain,
warmth, or cold. The density of these sensory receptors in the skin
varies throughout the body, resulting in some regions of the body
being more sensitive to touch, temperature, or pain than other
regions.
Excretion
In addition to secreting sweat to cool the body, eccrine
sudoriferous glands of the skin also excrete waste products out of
the body. Sweat produced by eccrine sudoriferous glands normally
contains mostly water with many electrolytes and a few other trace
chemicals. The most common electrolytes found in sweat are
sodium and chloride, but potassium, calcium, and magnesium ions
may be excreted as well. When these electrolytes reach high levels
in the blood, their presence in sweat also increases, helping to
reduce their presence within the body. In addition to electrolytes,
sweat contains and helps to excrete small amounts of metabolic
waste products such as lactic acid, urea, uric acid, and ammonia.
Finally, eccrine sudoriferous glands can help to excrete alcohol from

the body of someone who has been drinking alcoholic beverages.
Alcohol causes vasodilation in the dermis, leading to increased
perspiration as more blood reaches sweat glands. The alcohol in the
blood is absorbed by the cells of the sweat glands, causing it to be
excreted along with the other components of sweat.
C. PATHOPHYSIOLOGY
The pathophysiology of the burn wound is characterized by an
inflammatory reaction leading to rapid oedema formation, due to
increased microvascular permeability, vasodilation and increased
extravascular osmotic activity. These reactions are due to the direct
heat effect on the microvasculature and to chemical mediators of
inflammation. The earliest stage of vasodilatation and increased
venous permeability is commonly due to histamine release. Damage
to the cell membranes partly caused by oxygen-free radicals released
from polymorphonuclear leucocytes would activate the enzymes
catalyzing the hydrolysis of prostaglandin precursor (arachidonic
acid) with rapid formation of prostaglandin as the result.
Prostaglandins inhibit the release of norepinephrine and may thus be
of importance in modulating the adrenergic nervous system which is
activated in response to thermal injury. The morphological
interpretations of the changes in the functional ultrastructure of the

bloodlymph barrier following thermal injury seem to be an increase in
the numbers of vacuoles and many open endothelial intercellular
junctions. Furthermore changes of the interstitial tissue after burn
trauma are of great importance. The continuous loss of fluid from the
blood circulation within the thermally damaged tissue causes
increased haematocrit levels and a rapid fall in plasma volume, with
decreased cardiac output and hypoperfusion on the cellular level. If
the fluids are not adequately restored burn shock develops.
Furthermore, the burn wound provides a vast area of entry of surface
infection with a high risk of septic shock. Four main principles are of
utmost importance in the current management of patients with
severe thermal injury, namely early wound closure, prevention of
septic complications, adequate nutrition and control of the external
environment. (Ann Chir Gynaecol. 1980)
Degree of Combustio:
1. First degree of combustio
Skin still infarction, redness, not found bullae, and pain
2. Second degree of combustio
- Damage includes epidermis and dermis, a reaction accompanied by
inflammatory exudation process.
- Encountered of bulae.
- Pain due to irritation of nerve endings.
- The wound is red or pale, often located higher above the normal
skin

- Second degree of combustio
Looks bullae, basic wound redness (degrees IIA), basic pale whitish
(degrees IIB), severe pain primarily on the degree of IIA
Second degree combustio are divided into 2 (two), they are:
1. Grade II shallow (superficial)
- Damage to the superficial part of the dermis.
- Organs of the skin such as hair follicles, sweat glands, sebaceous
glands are still intact.
- Healing occurs spontaneously within 10-14 days.
2. Grade II (deep)
- Damage on almost all parts of the dermis.
- Organs of the skin such as hair follicles, sweat glands, sebaceous
glands remains largely intact.
- Healing occurs over time, depending on the remaining
epithelium. Healing usually occurs over a month.
Third degree of combustio
- Damage includes all layers of the dermis and deeper layers.
- Organs of the skin such as hair follicles, sweat glands, sebaceous
glands were damaged.
- Not found bulae.
- The skin is combustio gray and pale. Because dry skin than the
lower lying around.
- Occurs coagulation proteins in the epidermis and dermis are
known as escar.
- There were no pain and loss of sensation, because the sensory
nerve endings damage / death.
- Healing occurred long as there is a process of spontaneous
epithellization of the wound.
Third degree of combustio
There bullae, skin necrosis appeared, basic black injuries, less
severe pain, sometimes visible tissue under the skin
(Muscle, bone, etc.)
Based on the seriousness of injuries
American Combustio Association classifies combustio into three
categories, they are:
• Major Combustio

- With extensive combustio over 25% in adults and more than 20% in
children.
- Full thickness combustio over 20%.
- There were combustio on the hands, face, eyes, ears, feet, and
perineum.
- There inhalation trauma and multiple injury regardless of the degree
and extent of injuries.
- There are high-voltage electrical combustio.
• moderate combustio
- With extensive combustio 15-25% in adults and 10-20% in children.
- Full thickness combustio less than 10%.
- There are no combustio on the hands, face, eyes, ears, feet, and
perineum.
• Minor Combustio
- Minor combustio as defined by Trofino (1991) and Griglak (1992)
are: extensive combustio with less than 15% in adults and less than
10% in children.
- Fullthickness combustio less than 2%.
- There are no combustio on the face, hands, and feet.
- Wounds not sirkumfer.
- There is no inhalation injury, electrical, fracture.
(Hudak & Gallo, 1996, 542)
The size of the combustio area
In determining the size of the combustio area we can use several
methods:
• Rule of Nine
- Head and neck: 9%
- Chest front and rear: 18%
- Abdomen front and rear: 18%
- The right hand and the left: 18%
- The right thigh and left: 18%
- The right leg and left: 18%
- Genital: 1%
Symptoms
Symptoms depend on many things, including:
Type and strength of voltage How long you were in contact with the electricity How the electricity moved through your body Your overall health
Symptoms may include:
Changes in alertness (consciousness) Broken bones Heart attack (chest, arm, neck, jaw, or back pain) Headache Problems with swallowing, vision, or hearing Irregular heartbeat Muscle spasms and pain Numbness or tingling Breathing problems or lung failure Seizures Skin burns
THE INDICATION OF CLIENT WITH COMBUSTION IN INTENSIVE CARE UNIT
According to Wirman 2007 , he stated that the criteria of client with combustion in intensive care unit, they are :
- The combustion with II-III degree and up to 25%- The client of combustion with injury of inhalation which has up to 80 %
possibility of low oxygen supply in blood bring it up to the death of tissue all over the body
- Client of combustion which needs the debridement treatment through the treatment results high possibility to infection.
- The rehydration needs to be fulfilled for client with combustion within special formula and need the intensive monitoring for its effectiveness
- Client with combustion has the imunosupression caused by lost of skin function for the body protection and it needs special action of keep the best aseptic antiseptic technic which is easier to be done in intensive care unit
- Client of combustion needs intensive care to keep it away from secondary or complication for the prevention into worse condition in intensive care unit (the consciousness level and all of the physical examination).
D. ASSESSMENT
1. Rational Assessment
a. Client’s Identity

Assessment of the patient's identity is important to improve the
accuracy of the information and coordination. (Barkaukass, et.al,
1994). In these cases, the patients were male, aged 30 years old, a
Muslim, worked as an electrical repair, is married and has two
children, lived in Basarang, Kapuas, Central Kalimantan.
b. Hospital Entrance Data
This is important because of the data obtained in this section
can be a major problem or the main reason patients come to the
health services (Smeltzer, 2005). This data will also be directed
some nursing interventions to address priority problems or major
complaints of patients. (Barkaukass et.al, 1994).
Assessment is the initial stage of the nursing process and is a
systematic process of collecting data from multiple data sources to
evaluate and identify the client's health status (Nursalam, 2000).
Assessment is the first step of the nursing process which aims to
collect data both subjective and objective data the data. Subjective
data was obtained based on the results of interviews with clients or
others, while the objective data acquired by observation and
physical examination. The initial step is to conduct an assessment
of the client's biographical data includes name, age, gender,
occupation, race, and others. Upon further review of biographical
data, among others, on the assessment conducted extensive
combustio. To determine the extent of combustio can use one of
the existing methods, the method of "rule of nine" or method "Lund
and Browder". And the depth of combustio can be classified into
four types, they are degree combustio I, stage II, stage III and
IV. Combustio about certain places require special attention,
therefore consequently can cause a variety of problems. Like, if the
combustio on the face, neck and chest can interfere with the
airway and chest expansion caused by edema of the
larynx. Whereas if the limb, it can cause a decrease in circulation
to the extremities due to the formation of edema and scar
tissue. Therefore, assessment of the airway (airway) and
respiratory (breathing) and circulation (circulation) is
indispensable. Combustio of the eye can cause corneal laceration,
retinal damage and decreased visual acuity. Location of combustio
can also sensitize staff on the possibility of inhalation injury. The

nurse should assess the following findings: Fur nose combustio,
combustio oral or pharyngeal mucous membranes, combustio
perioral area, or throat, cough or hoarse voice changes, a history of
combustioing in a confined area. And to assess pain / comfort,
examples of first degree combustio are eksteren sensitive to touch;
pressed; air movement and temperature changes; thickness
combustio were second degree is very painful; smentara response
on second-degree combustio thickness depends on the integrity of
nerve endings; wound third-degree combustio are not
painful. (Brunner & Suddarth, 1996)
The combustio is an injury caused by heat, electrical current,
chemicals and lightning of the skin, mucosa and deeper
tissues. Combustio skin and tissue will become necrotic tissue
(Maluegha, 2007). Electric combustio (electrical) caused by heat is
moved from the delivered electrical energy through the
body. Severity of injury is influenced by the length of exposure, and
high voltage electrical waves that way until about the body.
(Huddak and Gallo, 2010).
As described in the brief history of the patient Mr. A when the
client repaired the trafo in batu licin that mispredicted as light off
but was actually not. Client got electrical shock and it combustio
half of his face and chest, his left wrist and left leg. When viewed
from the history then we can conclude that Mr. A suffered electrical
combustio injury.
c. History of Previous and Family Disease
Past medical history is needed to identify the health problems of
patients who have passed. Analysis is intended to look at is there a
match between the health problems in the past with the present
health problems or not. While family health history is to identify
various genetic diseases, heredity, and natural environment that
affect patients' health problems at this time (Barkaukass, et.al,
1994). Past medical history of patients, the data to be obtained are
several factors that make complications or the patient's condition
becomes more severe condition. Complications of the disease can
be considered earlier. (Www.unca.com, 2006).
Clients say never experienced a disease that now affects,
and because the lien did not experience other serious

illnesses. Clients who have never experienced pain to be
hospitalized.
Clients say does not exist between family members who
suffer from the same disease as the client and no family members
who suffer from infectious diseases and hereditary diseases such
as tuberculosis, hepatitis, diabetes, etc.
d. Neuromuscular System
It is well known that electrical injury can cause damage to the
central nervous system, affecting both the brain and spinal
cord. Both acute and delayed neurological syndromes have been
reported in Victims of electrical injury involving a variety of
symptoms, Including loss of consciousness, seizures, aphasia,
visual disturbances, headaches, tinnitus, paresis, and memory
disturbance. Neurologic sequel can occur Whether or not the head
is a point of direct contact with the electrical current.
Central nervous system damage results from direct thermal and
mechanical effects of electrical shock, and histopathological
changes in the central nervous system such as coagulation
necrosis (death of tissue due to clotting of blood vessels), reactive
gliosis (increase of in nonneural support cells within the central
nervous system as a response to injury), demyelinization
(destruction of the protein covering to many nerves), vacuolization
(small holes within the brain tissue), and perivascular hemorrhage
(small areas of bleeding) have been documented. Centra l nervous
system damage may also occur from anoxia due to
cardiorespiratory arrest or ischemic damage resulting from
thrombosis. Cause of death in fatal cases is Generally ascribed to
ventricular fibrillation with subsequent cardiorespiratory arrest.
Other neurologic status is the level of awareness of both
qualitative and quantity, studied as a reference in a more intensive
handling of patients, because these factors may be a clue the
damage (Vincent, 2005).
When damage to the frontal lobe damage in studying the
possibility of something, a memory or a higher intellectual
functions. Cognitive impairment is the limited level of patient
attention to something, it is difficult to understand something,
quickly forgotten, and lack of motivation. While psychological
problems characterized by emotional lability, frustration and lack of
co-operative attitude.
Both laboratory investigations, ECG and other vital because to
determine the extent of organ functions impaired. (Tjokronegoro &
Henderson, 2002) and (Black & Hawk, 2005).
At Mr. A said that he felt numbness on both hands, Client’s pupil
is isokor, the pupil diameter of 3 mm / 3 mm, the pupillary light
reflex direct + / +, pupillary reflexes to light indirectly + / +,
Babinski + / +, GCS score: E4M6V5, level of consciousness
composmentis. Communication skills and well-sensory perception,
can do a full assessment because the patient is awake the superior
extremity muscle strength 4444/3333 and lower extremities
4444/4444.
Description of muscle strength :
Muscle contracts against full resistance Strength reduced, but contraction can still move joint against resistance
4
Strength further reduced such that joint can be moved only against gravity with examiner's resistance completely removed.
3
Muscle can onlly move if resistance of gravity is removed. 2Only a trace or flicker of movement is seen or felt, or fasciculations are observed,
1
No movement 0
e. Urinary System
Assessment of urinary system do nurses need to obtain the
data if there are any changes in the structure and function of the
urinary system. Subjective assessment primarily focused on three
things: the pain, changes in the pattern of urination, and urinary
tract complaints. While physical examination by inspection,
palpation, and percussion to look over the suitability of the
patient's complaints. If there is a complaint and the complaint
finding that reinforces the data on this system show that there has
been a change in this system, at least in the urinary system
function. (Smeltzer & Bare, 2005).
In combustio patients do not experience urinary problems
except the combustio area until the genital area or have combustio
on up muscles and nerves in the urinary system.
In this case, the patient is catheterized. Urine out with clear
yellow color, there is no sediment or blood. The position of the
catheter was not bent / no obstacles. Oral fluid intake of 1200 cc /
24 hour, RL IV fluid line 2500cc / 24 hours, the output of fluid
through foley cathether the output 1600cc / 24 hours installed on
December 24th 2013. Laboratory tests on 24 december 2013:
sediment; 1 + epithelial cells, 3-5/lpb leukocytes, erythrocytes lot,
cylindrical (-), crystal (-), bacteria (-), BJ 1.015, pH 7.0, protein (-),
negative ketones, blood (-), bilirubin negative, uroblingen 0.2 mmol
/ L, negative nitrite, leukocyte esterase (-). Blood chemistry;. urea:
20 mg / l, creatinine: 0.9, acetone: -, Potassium: 3.90 mmol / l,
Sodium: 141.1 mmol / L, chloride: 105 mmol / l, analysis results of
urinary system is good.
Rehydration :
Baxter : 15 cc x Kg of BW x percent of combustion
: 15 x 71 x 29,25 %
: 15 x 71 x 29,25100
= 3641 cc /24 hours
IWL : 15 cc x Kg of BW
: 15 cc x 71 Kg = 1065 cc /24 hours
f. Breathing
Examination of the respiratory system organ and needs to be
done to assess the structure of the respiratory system as well as
the overall system function. In general, the assessment is directed
at the signs and symptoms of respiratory disorders such
as dyspnoea (difficulty breathing), cough, sputum production, chest
pain, the presence of wheezing and Ronchi, and cyanosis. Nurses
are reviewing this section should relate to the examination of the
heart and blood vessels so there is a connection because both of
them. The presence of clinical manifestations indicate that there
are changes in the structure and function of the respiratory
system. (Barkaukass, et.al, 1994). A history of smoking is
important we examine as a risk factor. An inability cough / airway

barrier, or the onset of irregular breathing. In Mr.A respiratory
assessment is important because of the combustio on the neck and
chest.
In physical examination of Mr.A patient said that he had
shortness of breath with respiration rate: 31 bpm, the nose mucus
is burn and redness , the nose hair is burnt up, the use of
accessory respiratory muscles, resonant percussion, auscultation is
wheezing. The results of examination of the piston 24 december
2013 were CRT 65%. Test results of blood gas analysis was pH: 7.4,
PACO2: 46.8, PAO2: 78.0, HCO3: 26.5., O2 Saturation: 80.3%., BE:
1.1., Blood Gas Sodium: 137., Potassium Gas Blood: 3.9., Chlorida
Blood Gas: 100.4.
g. Cardiovascular
Physical examination of the heart needs to be done because it
aims
to obtain data on the effectiveness of the heart pumps, the volume
and
filling pressure, cardiac output, and cardiac compensatory
mechanisms and
blood vessels. (Smeltzer & Bare, 2005).
Immediately after a combustio injury, released vasoactive
substances (catecholamine, histamine, serotonin, leukotrienes, and
prostaglandins) from tissue injury experience. These substances
cause increased capillary permeability so that plasma seeps into
the surrounding tissue. Heart rate increased in response to the
release catecholamin and the relative hypovolemia, which began
fall of cardiac output. Increase hematocrit levels of expenditure
that shows hemoconcentration intravascular fluid. Besides
spending evaporation of liquids through injuries occur 4-20 times
greater than normal. While the normal discharge in adults with
normal body Temperature per day is 350 ml. This can lead to a
decrease in organ perfusion. If not filled the intravascular space
back to the intravenous fluids hypovolemic shock and threat of
death for patients with extensive combustio may occur.
In electrical combustio, Passage of high voltage electricity
through the network led to its conversion into heat energy, he
raises not only combustio the skin and sub-cutis tissue, but also all
the networks on the electrical flow path. Electrical combustio are
usually caused by contact with a high voltage power source. Limb
is contact with hands and arms are more frequently injured than
the legs and feet. Contacts often lead to heart problems and or
respiratory and cardiopulmonary resuscitation is often required at
the time the accident occurred. Injuries to the local influx of electric
current is usually combustio and looked haggard.
In this case there are no signs and symptoms related to the
cardiovascular system change. In physical examination there was
no heart enlargement, heart sounds S1 and S2 regular, gallops (-),
nuts (-), percussion dullness. Blood pressure 110/90 mmHg, pulse:
60 x / min regular, Temperature: 36.30 C. CRT >3
seconds. hematology laboratory results 24th december
2013 were; Hb: 12.8 g / l, Ht: 42.9%, erythrocyte: 4.95 million / ul,
leukocytes: 11.200/ul, platelets 256.000/ul, MCV: 86.7 g / dl, MCH:
29.8 g / dl, MCHC : 34.4 g / dl. PT: 11.3 sec, PT control: 11.4 sec,
APTT: 29.3 sec, APTT control: 26.1 seconds, fibrinogen level 512
mg / dl, LDH: 450 U / l, CKMB: 23 u / l.
h. Digestion
In this case the patient is not using the NGT for feeding, Liquid
diet Nitrisol 200cc/4hours via oral. High protein high calorie 2700
kcal. RL infusion installed 20 dpm. There is no difficulty when the
food sucked. Abdominal palpation no palpable faecal
mass. Patients wear a diaper. On examination dated 24-12-2013
AST: 415, ALT: 85, GDS: 145 Client’s BW is 71 kg and client’s BH is
165 cm.
Antropometric Data:
BW : 71 Kg
BH : 165 cm
IBW : (165 – 100 ) ± (165 – 100 ) . 10%
: 65 – 6,5 ± 65 + 6,5
: 58,5 kg – 71,5 kg
i. Integument

Nurses need to assess the integument system to obtain data
related to dermatological disorders. Subjective assessment of
complaints directed at the primary, cause, duration of complaints,
location, pain, etc..Physical examination by inspection and
palpation directed at the general appearance, skin disorders such
as redness, itching, cyanosis, change in color; lesions on skin,
vascularization and hydration, nails and hair.(Smeltzer & Bare,
2005: Black & Hawk, 2005). In combustio patients will be damaged
the integrity of the skin, damage that occurs in people not only on
the skin only, tissue custody order starting from the low of nerves,
blood vessels, muscles, skin, tendons and bones. On a network that
prisoners would be much higher current through it, then the heat
will be raised higher. Because epidermis thicker, palms and feet
have a higher electrical resistance that combustio occurred also
heavier when the area is exposed to an electric current.
At the time of assessment Mr.A found a second-degree
combustion as much as 29.25% on the half of face (2.25%) the
front of the chest (9%), the majority of the left hand (9%), and the
right hand (9%). good skin turgor , Moisture skin: dry, smooth skin
texture , the wound had black colored, edema on upper extremities
, the peripheral area is cold .
Anatomy of combustion :
j. Daily activities at home.

These data further elucidate the behavior of the patient's health
in meeting daily needs at home. This data is needed to be adjusted
later in the preparation of strategic planning in hospital
nursing. (Smeltzer & Bare, 2005). This section also describes the
activity patterns and exercises that patients can do at home. This
needs to be studied because of the pattern of activity in the home
can affect and can assist nurses in determining the activity or
activities in accordance with the habits of the patient. (Barkaukass
et.al, 1994).
In this case, the patient's family said that the activity or
activities of the day - the day before the home done by the
patient's pain, elimination patterns BAK good no complaints, either
defecation pattern and no complaints, own shower 2 times a day,
wash hair 3 days, brushing teeth 2 times a day, a good appetite,
eating 3 meals a day, regular diet, drink 6 glasses of water a day,
never exercise, sleep about 6-8 hours a day. Currently in meeting
all the needs of activities of daily living (ADL) assisted by nurses
and family because there is a combustio patient's leg and bandage
elastice.
Daily activities in the hospital
Client is swab once a day by nurse within the oral hygiene
and genitalia hygiene, urinate facilitate by foley cathether the
output 1600cc / 24 hours installed on December 24th 2013,
defecation facilitate by diapers, diet is Nutrisol 200cc/ 4 hours
sucked with straw, sleep for about 8-9 hours in a day. The activities
are need help and monitoring by others with the scale of 2.
Activity scale :
1 : Independent
2 : Need help and monitoring by others
3 : Need the simple help and monitoring by others
4 : Need help, monitoring by others, and the aid stuff
5 : Totally dependent
(Robert Priharjo,2001 :159, Pengkajian Fisik Keperawatan. Jakarta : EGC)
Supporting Examination
HematologyHemoglobin 12.8 14.00 – 18.00 g/dl MethodLeukocyte 11.2 4.0 – 10.5 k/ul Impedance

Erytrocytes 4.95 4.50 – 6.00 Million/ul ImpedanceHematocryte 42.9 42.00 – 52.00 Vol% Analyzer
CalculatesThrombocyte 256 150 – 450 k/ul ImpedanceRDW-CV 11.5 11.5 – 14.7 % Analyzer
CalculatesMCV 86.7 80.0 – 97.0 Fl Analyzer
calculatesMCH 29.8 27.0 – 32.0 Pg Analyzer
CalculatesMCHC 34.4 32.0 – 38.0 % Analyzer
CalculatesGran% 83.8 50.0 – 70.0 % ImpedanceLymphocytes% 11.5 25.0 – 40.0 % ImpedanceMID% 4.7 4.0 – 11.0 % ImpedanceGran# 15.00 2.50 – 7.00 k/ul ImpedanceLymphocytes# 2.1 1.25 – 4.0 k/ul ImpedanceMID# 0.8 k/ul Impedance
PROTHROMBIN TIMEPT result 11.3 9.9-13.5 second NephelometryINR 0.99 NephelometryNormal Control of PT
11.4 Nephelometry
APTT result 29.3 22.2-37.0 second NephelometryNormal Control of APTT
26.1 Nephelometry
CHEMISTRYUreum 20 10-50 Mg/dl Modif-berchelotCreatinine 0.9 0.7-1.4 Mg/dl JaffeELECTROLYTENatrium 141.4 135-146 Mmol/l ISEKalium 3.9 3.4-5.4 Mmol/l ISEChlorida 105.0 95-100 Mmol/l ISE
CHEMISTRY
FAT AND HEART FAALLDH 450 225 – 450 U/L Optimised ( C )
CKMB 23 0 – 24 U/L Optimised ( C )
Arterial Blood Gases ExaminationExamination Result Normal Range UnitChemistryBlood Gas AnalysisTemperature 37,0 36,5 – 37,5 CelciusPH 7,4 7,350 – 7,450PACO2 46,8 35,0 – 45,0 mmHgPAO2 78,0 80,0 – 100,0 mmHg

HCO3 26,5 22,0 – 26,0 Mmol/lSPAO2 80,3 75,00 – 99,00 %BE 1,1 -3,00 – 3,00 Mmol/lNatrium Blood Gases
137,0 135,0 – 148,0 Mmol/l
Kalium blood Gases
3,9 3,50 – 4,50 Mmol/l
Chloride Blood Gases
100,4 98,0 – 107,0 Mmol/l
k. Pharmacological Therapy
Therapeutic dated December 24, 2013 as follows;
· IUVD RL 2500 / 24hours
. Oral intake 1200/24hours (Nutrisol)
· Oxygen 8 lpm
· Inj. Ceftriaxone 2x1 gr
· Cetorolac 3x30 mg
· 2x50 mg Ranitidine
· Debridement
Information about drug:
Ceftriaxone ( Cephalosporin )
Indication:
Infections caused by pathogens that is sensitive to Ceftriaxone, such as
respiratory tract infection, ENT infection, urinary tract infection, sepsis,
meningitis, bone infection, joint and soft tissue, intra-abdominal infection,
genital infection (including gonorrhea), perioperative prophylaxis , and
infection in patients with the disorder the body's defenses.
Contra indication:
Hypersensitivity to cephalosporin and penicillin (as a cross allergic reaction).
Cetorolac ( Non-steroidal anti-inflammatory drug )
Indication:
Cetorolac is indicated for the short-term management of acute moderate to
severe pain after surgical procedures. Cetorolac total duration should not be
more than five days. Parenterally administered cetorolac is recommended
immediately after surgery. Should be changed to alternative analgesics as
soon as possible, as long as cetorolac therapy should not exceed 5 days.

Cetorolac is not recommended to be used as an obstetrical preoperative
medication or for obstetric analgesia because adequate studies have not been
conducted on this subject, and because it is known to have the effect of
inhibiting the biosynthesis of prostaglandins or uterine contractions and fetal
circulation.
Contra Indication:
- Patients that have had a previous allergic to this drug, because there is the
possibility of cross-sensitivity.
- Patients that demonstrate a serious allergic manifestation due
administration of aspirin or nonsteroidal anti-inflammatory drugs other.
- Patients hat suffering from active peptic ulcer.
- Cerebrovascular disease that suspected and that it is definitely.
- Hemorrhagic diathesis including coagulation disorder.
- Syndrome complete or partial nasal polyps, angioedema or bronchospasm.
- Concomitant therapy with ASA and other NSAID.
- Hypovolemia due to dehydration or other causes.
- Moderate renal impairment to severe (serum creatinine> 160 mmol / L).
- History of asthma.
- The postoperative patient with a high risk of bleeding or incomplete
hemostasis, patient with anticoagulant including low dose heparin (2500-
5000 units every 12 hours).
- Concomitant therapy with Ospentyfilline, Probenecid or lithium salts.
- During pregnancy, labor, delivery or lactation.
- Children <16 years.
- patient that have a history of Steven-Johnson syndrome or rash
- vesikulobulosa.
- Giving neuraxial (epidural or intrathecal).
- Prophylaxis prior to major surgery or intra-operative hemostasis if
absolutely necessary because of the high risk of bleeding.
Ranitidine (antacid, anti-reflux drug and anti-ulceration)
Indication:
- Short-term treatment of intestinal ulcers that Twelve fingers is active,
active stomach ulcers, reduce the symptoms of reflux esophagitis.
- Maintenance therapy after healing intestinal ulcers of twelve fingers,
peptic ulcers.
- Treatment of pathological hypersecretory state (eg: Zollinger Ellison
syndrome and systemic mastocytosis).
- Ranitidine injection is indicated for inpatients in a state hospital with
pathological hypersecretion or twelve fingers ulcers that are difficult to
overcome, or as an alternative treatment of short-term oral administration
to patients who can not take oral Ranitidine.
Contra Indication:
- Patients who are hypersensitive to Ranitidine.
Debridement
Debridement is the removal of unhealthy tissue from a wound to promote healing
it can be done by surgical, chemical, mechanical or autolytic (using your body’s
own processes) the removal tissue.
Purpose of debridement
Debridement is used to clean dead and contaminated material from your wound
to aid in healing. The procedure is most often the following reasons :
To remove tissue contaminated area, foreign tissue, dead cells, or
crusting)
To create a neat wound edge to decrease scarring
To aid in the healing of vey severe burns or pressure sores (decubitus
sores)
To get a sample of tissue for testing and diagnosis
Possible Complications Pain Bleeding Infection Delayed healing Removal of healthy tissue with mechanical debridement
PROBLEM PRIORITY OF NURSING DIAGNOSIS
1. Ineffective airway clearance related to Injury of inhalation2. Impaired Gas Exchange related to change of capillary-alveolar membrane3. Ineffective Peripheral Tissue Perfusion related to low Oxygen supply
secondary to edema4. Acute pain related to Injury agent secondary to the wound
5. Impaired Physical Ability related to contracture6. Impaired Skin Integrity related to Injury in the Skin Secondary Intention.7. Risk for Imbalance Fluid Volume8. Risk for Infection

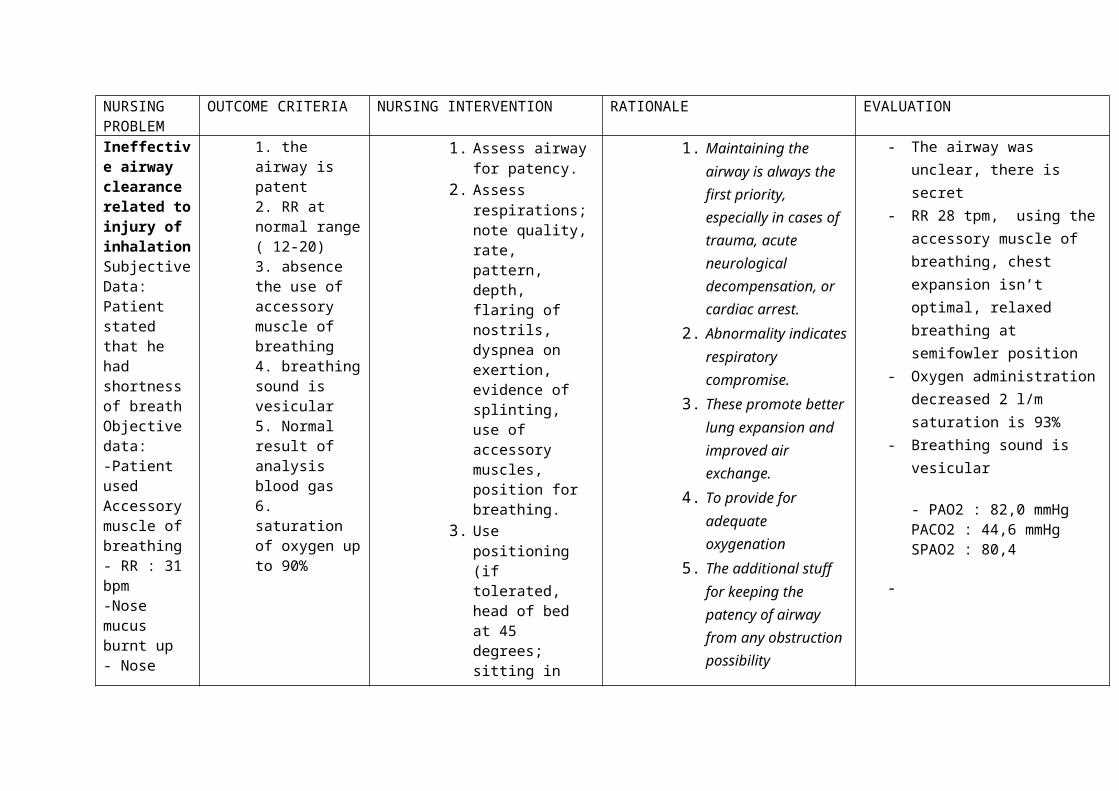
NURSING PROBLEM
OUTCOME CRITERIA NURSING INTERVENTION RATIONALE EVALUATION
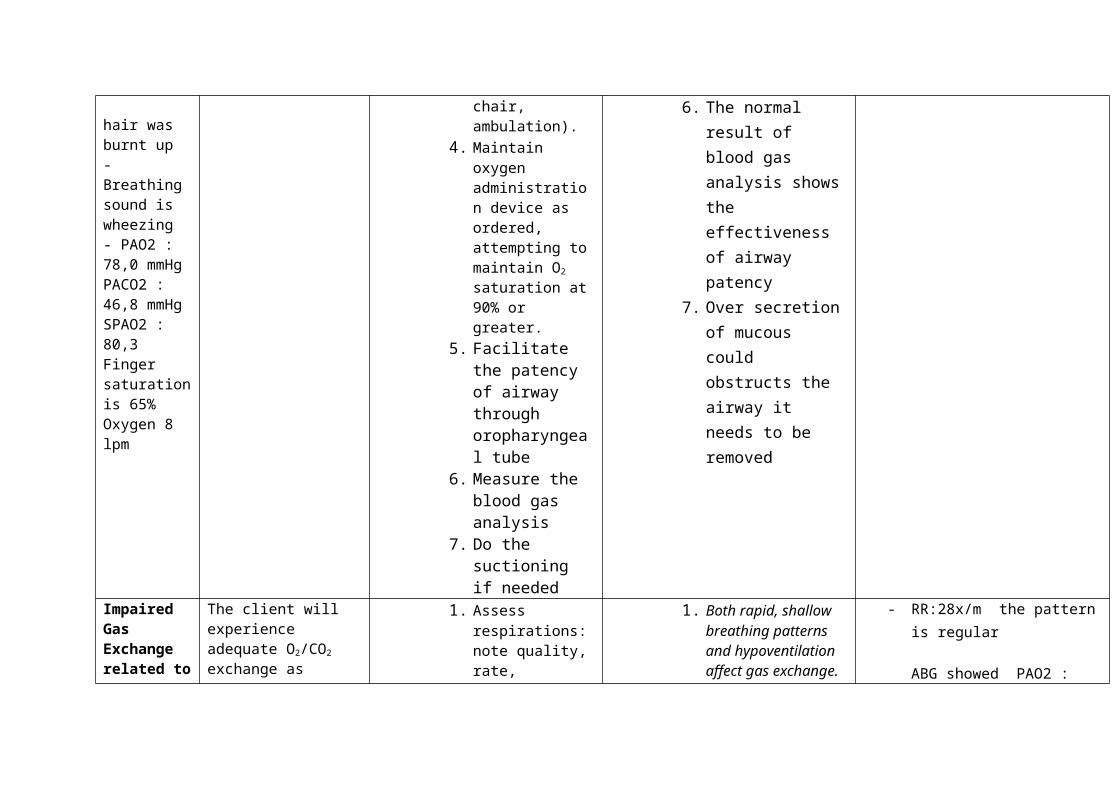
Ineffective airway clearance related to injury of inhalationSubjective Data:Patient stated that he had shortness of breathObjective data:-Patient used Accessory muscle of breathing- RR : 31 bpm-Nose mucus burnt up- Nose hair was burnt up- Breathing sound is wheezing- PAO2 : 78,0 mmHg
1. the airway is patent2. RR at normal range ( 12-20)3. absence the use of accessory muscle of breathing4. breathing sound is vesicular5. Normal result of analysis blood gas6. saturation of oxygen up to 90%
1. Assess airway for patency.
2. Assess respirations; note quality, rate, pattern, depth, flaring of nostrils, dyspnea on exertion, evidence of splinting, use of accessory muscles, position for breathing.
3. Use positioning (if tolerated, head of bed at 45 degrees; sitting in chair, ambulation).
4. Maintain oxygen administration device as ordered, attempting to maintain O2 saturation at 90% or greater.
5. Facilitate the patency of
1. Maintaining the airway is always the first priority, especially in cases of trauma, acute neurological decompensation, or cardiac arrest.
2. Abnormality indicates respiratory compromise.
3. These promote better lung expansion and improved air exchange.
4. To provide for adequate oxygenation
5. The additional stuff for keeping the patency of airway from any obstruction possibility
6. The normal result of blood gas
- The airway was unclear, there is secret
- RR 28 tpm, using the accessory muscle of breathing, chest expansion isn’t optimal, relaxed breathing at semifowler position
- Oxygen administration decreased 2 l/m saturation is 93%
- Breathing sound is vesicular
- PAO2 : 82,0 mmHgPACO2 : 44,6 mmHgSPAO2 : 80,4
-

PACO2 : 46,8 mmHgSPAO2 : 80,3Finger saturation is 65%Oxygen 8 lpm
airway through oropharyngeal tube
6. Measure the blood gas analysis
7. Do the suctioning if needed
analysis shows the effectiveness of airway patency
7. Over secretion of mucous could obstructs the airway it needs to be removed
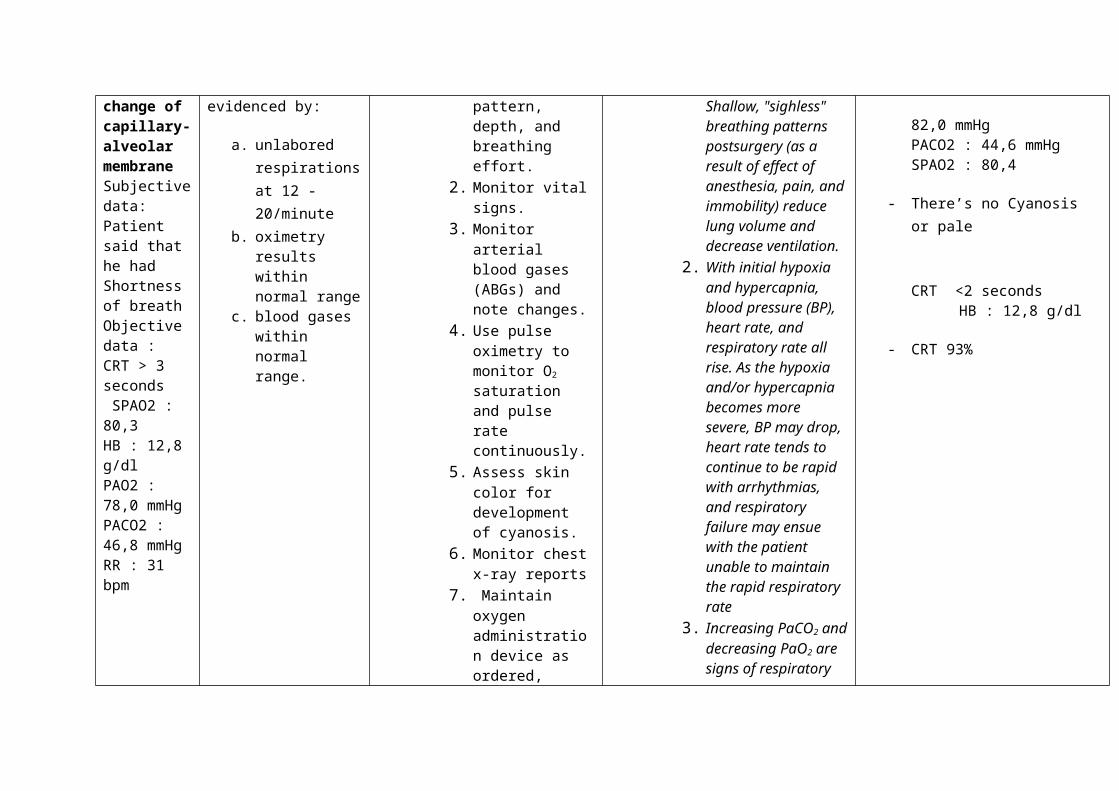
Impaired Gas Exchange related to change of capillary-alveolar membraneSubjective data:Patient said that he had Shortness of breathObjective data :CRT > 3 seconds SPAO2 : 80,3 HB : 12,8 g/dlPAO2 : 78,0
The client will experience adequate O2/CO2 exchange as evidenced by:
a. unlabored respirations at 12 - 20/minute
b. oximetry results within normal range
c. blood gases within normal range.
1. Assess respirations: note quality, rate, pattern, depth, and breathing effort.
2. Monitor vital signs.
3. Monitor arterial blood gases (ABGs) and note changes.
4. Use pulse oximetry to monitor O2 saturation and pulse rate continuously.
5. Assess skin color for development of cyanosis.
1. Both rapid, shallow breathing patterns and hypoventilation affect gas exchange. Shallow, "sighless" breathing patterns postsurgery (as a result of effect of anesthesia, pain, and immobility) reduce lung volume and decrease ventilation.
2. With initial hypoxia and hypercapnia, blood pressure (BP), heart rate, and respiratory rate all rise. As the
- RR:28x/m the pattern is regular
ABG showed PAO2 : 82,0 mmHgPACO2 : 44,6 mmHgSPAO2 : 80,4
- There’s no Cyanosis or pale
CRT <2 secondsHB : 12,8 g/dl
- CRT 93%

mmHgPACO2 : 46,8 mmHgRR : 31 bpm
6. Monitor chest x-ray reports
7. Maintain oxygen administration device as ordered, attempting to maintain O2 saturation at 90% or greater.
8. Administer medications as prescribed.
hypoxia and/or hypercapnia becomes more severe, BP may drop, heart rate tends to continue to be rapid with arrhythmias, and respiratory failure may ensue with the patient unable to maintain the rapid respiratory rate
3. Increasing PaCO2 and decreasing PaO2 are signs of respiratory failure. As the patient begins to fail, the respiratory rate will decrease and PaCO2 will begin to rise. Some patients, such as those with COPD, have a significant decrease in pulmonary reserves, and any physiological stress may result in acute respiratory failure.

4. Pulse oximetry is a useful tool to detect changes in oxygenation. O2 saturation should be maintained at 90% or greater.
5. Chest x-rays may guide the etiologic factors of the impaired gas exchange. Keep in mind that radiographic studies of lung water lag behind clinical presentation by 24 hours.
6. To provide for adequate oxygenation
7. The type depends on the etiologic factors of the problem (e.g., antibiotics for pneumonia, bronchodilators for COPD, anticoagulants/thrombolytics for pulmonary embolus,

analgesics for thoracic pain).
Ineffective Peripheral Tissue Perfusion related to low oxygen supply secondary to edemaSubjective DataPatient felt numbness on both of handsObjective DataEdema on the handsCRT > 3Cold on peripheral areaWeak pulse : 58 bpmOxygen saturation is 65%
Patient maintains optimal tissue perfusion tovital organs, as evidenced by strongperipheral pulses, normal ABGs, alert LOC,and absence of chest pain
a. Assess color, sensation, movement, peripheral pulses, and capillary refill on extremities with circumferential burns. Compare with findings of unaffected limb.
b. discourage positions that compromise blood flow in lower extremities
c. Administer humidified oxygen via appropriate mode, e.g., face mask.
1. Edema formation can readily compress blood vessels, thereby impeding circulation and increasing venous stasis/edema. Comparisons with unaffected limbs aid in differentiating localized versus systemic problems (e.g., hypovolemia/decreased cardiac output).
2. in order to allow time for autoregulatory mechanisms to adjust to the change in the distribution of blood associated with an upright position
- The skin color wasn’t pale, the numbness is lessen
- CRT is fine <2 seconds- At semifowler position,
the extremities put low in line with heart
- pulse 84 times a minute
- Oxygen saturation 93%- Oxygen 2 lpm

Oxygen 8 lpm
3. oxygen supplies will fulfill the optimal tissue perfussion
Acute pain related to post of debridement action
Subjective data :Patient said that he felt painP: the wound on the skinQ : stabbingR : wound areaS : 2 ( 1-5)T : 15 minutes
Objective data :- Patient
looked winced in pain
Report pain reduced/controlled.
Display relaxed facial expressions/body posture.
1. Assess reports of pain, nothing location/character and intensity (0–5 scale).
2. Teach the deep breathing technique
3. Change position frequently.
4. Administer analgesics ( Ketorolac)
1. Pain is nearly always present to some degree because of varying severity of tissue involvement/destruction but is usually most severe during dressing changes and debridement. Changes in location, character, intensity of pain may indicate developing complications (e.g., limb ischemia) or herald improvement/return of nerve function/sensation.
2. To reduce the pain3. Movement and
exercise reduce joint stiffness and muscle fatigue, but type of exercise depends on location
- Patient reported the pain is a bit relived.
- The scale is 1 (mild) P: the wound on the skin Q : stabbing R : wound area S : 1 ( 1-5)
T : 15 minutes- Patient showed relax
facial expression and distracted from the onset pain
- The pain was bearable after changing the position
- After administering via IV ketorolac 3x30 mg, the pain was relieved . as pprevention for side effect of ketorolac, given injection Ranitidine 2x50mg

and extent of injury4. The burned patient
may require around-the-clock medication and dose titration. IV method is often used initially to maximize drug effect. Concerns of patient addiction or doubts regarding degree of pain experienced are not valid during emergent/acute phase of care, but narcotics should be decreased as soon as feasible and alternative methods for pain relief initiated
Impaired Physical Mobility related to contracturSubjective Data :Patient said that he couldn’t move his right hand
Maintain position of function as evidenced by absence of contractures.
Maintain or increase strength and function of
1. Maintain proper body alignment with supports or splints, especially for burns over joints.
2. Note circulation, motion, and sensation of digits frequently.
3. Assess the muscle strenght
4. Perform ROM exercises
1. Promotes functional positioning of extremities and prevents contractures, which are more likely over joints.
2. Edema may compromise circulation to extremities, potentiating tissue necrosis/development of contractures.
- Bandage on contracture hand
- The circulation, motion and sensation are good
- Muscle strength is low on the right hand
- Patient was doing ROM cooperatively as procedure. With passive ways then active
Objective Data:Contractor on right handMuscle strength
4444
3333
4444
4444
Activity scale is 2 (need help and monitoring by others)
affected and/or compensatory body part.
Verbalize and demonstrate willingness to participate in activities.
Demonstrate techniques/behaviors that enable resumption of activities.
consistently, initially passive, then active.
5. Encourage family/SO support and assistance with ROM exercises.
6. Encourage patient participation in all activities as individually able.
3. To analyze the strength of each extremity
4. Prevents progressively tightening scar tissue and contractures; enhances maintenance of muscle/joint functioning and reduces loss of calcium from the bone.
5. Enables family/SO to be active in patient care and provides more constant/consistent therapy.
6. Promotes independence, enhances self-esteem, and facilitates recovery process.
- Patient was motivated to do the ROM exercise, ADL and being optimistic for recovery
Muscle strength
4444
3333
4444444
4Activity scale is 2 (need help and
monitoring by others)
-
Impaired Skin Integrity related to Injury in the Skin Secondary Intention.
Subjective data :The client said
Wound Healing: Secondary Intention (NOC)
Demonstrate tissue regeneration.
Achieve timely healing of
1. Assess/document size, color, depth of wound, noting necrotic tissue and condition of surrounding skin
2. Change burn dressing using the topicals and dressing materials
1. Provides baseline information about need for skin grafting and possible clues about circulation in area to support graft.
2. Some topicals perform better if they are change once a day or twice a day, etc. It is important to follow the prescribed order and the company's recommendation
- Patient is having 3 degree of burn injury, the color is pink and the surface area of wound is 29,25% skin surrounds wounds are redness
- The burn injury was cleaned and poured with NaCl and covered with sterile gauze, once a day
That he felt pain on the wound area of skinObjective data :There was an electrical burnt on chest ( 9%) left hand (9%) right hand (9%) half of face ( 2,25%) total (29,25%)
The depth of wound was 3 Degree (full thickness)
The wound area had black colored
burned areas ordered, at the prescribed frequency.
3. maintain sterile technique.
4. observe the burn area for evidence of healing (i.e. sloughing of burn eschar, bleeding, “budding” evidence of new skin cell regeneration and wound closure). While dressing
regarding the topical ordered.
3. good sterile technique during dressing changes assists in preventing burn wound infections.
4. As the burn heals the practitioner may need to change the burn topical or skin care regimen. Evidence of poor wound healing may indicate the burn is becoming infected or the patient’s nutritional status needs to be improved
- Nurses kept the hygiene and used the aseptic technique before and after the nursing action.
- Patient wasn’t having bleeding, the wound became dried showed the regeneration of tissue
Risk for Imbalance Fluid
Demonstrate improved fluid balance as evidenced
1. Monitor vital signs, central venous pressure (CVP). Note capillary refill and
1. Serves as a guide to fluid replacement needs and assesses cardiovascular
- Vital signs was normal BP : 110/80 mmhgRR : 20 bpmHR : 78 bpm
VolumeObjectiveIntake : Oral : 1200 cc/ 24 hours Parenteral :2500 cc /24 hours- Output :IWL = 1.065 cc/24 hoursUrine : 1600 cc / 24 hours
-client has combustion all over the skin of 29.25%SPAO2 : 80,3 PAO2 : 78,0 mmHgPACO2 : 46,8 mmHg
by individually adequate urinary output with normal specific gravity, stable vital signs, moist mucous membranes.
Balance of Electrolyte and PH
strength of peripheral pulses.
2. Monitor intake and urinary output. Observe urine color and Hematest as indicated.
3. Insert/maintain indwelling urinary catheter.
4. Administer calculated IV replacement of fluids
5. Monitor laboratory studies (e.g., Hb/Hct, electrolytes, random urine sodium and blood PH).
response. Note: Invasive monitoring is indicated for patients with major burns, smoke inhalation, or preexisting cardiac disease, although there is an associated increased risk of infection, necessitating careful monitoring and care of insertion site.
2. Generally, fluid replacement should be titrated to ensure average urinary output of 30–50 mL/hr (in the adult). Urine can appear red to black (with massive muscle destruction) because of presence of blood and release of myoglobin. If gross myoglobinuria is present, minimum urinary output should be 75–100 mL/hr to reduce risk of tubular damage and renal failure
3. Allows for close observation of renal
T : 36,5 C- CRT refilling time is < 2
seconds- The color of urine isn’t
pure yellow as clear- Installed cathether since
December 24th 2013- Installed the IV line since
24th 2013- Intake :
Oral : 1200 cc/ 24 hoursParenteral :2500 cc /24 hours- Output :IWL = 1.065 cc/24 hoursUrine : 1600 cc / 24 hours
-client has combustion all over the skin of 29.25%
PAO2 : 82,0 mmHgPACO2 : 44,6 mmHgSPAO2 : 80,4

function and prevents urinary retention. Retention of urine with its by-products of tissue-cell destruction can lead to renal dysfunction and infection.
4. Fluid resuscitation replaces lost fluids/electrolytes and helps psrevent complications, e.g., shock, acute tubular necrosis (ATN).
5. Identifies blood loss/RBC destruction and fluid and electrolyte replacement needs. Urine sodium less than 10 mEq/L suggests inadequate fluid resuscitation. Note: During first 24 hr after burn, hemoconcentration is common because of fluid shifts into the interstitial space.

Risk for Infection
Objective data :WBC : 11,2 k/ul
Hb : 12,8 g/dl
There was electrical burn wound (29.25%)Client would get the invasive procedure
Patient will achieve timely wound healing free of purulent exudate and be afebrile
1. Observe the sign and symptom of infection
2. Proper hand washing technique (6 ways )
3. Use aseptic technique when do the procedure
4. Check lab result of leucocytes
5. Give antibiotic as indication
1. To detect the early sign of infection
2. Prevent bacterial transmitted
3. To maintain the hygiene and prevent infection
4. The increase of leucocytes as indicate of infection
5. To reduce infection.
- administering the antibiotics injection of ceftriaxone 2x1 gr
- Through there is no sign of infection or exudates
- Nurses keep the aseptic and antiseptic technic
- Nurse clean the wound once a day
- There is no sign of inflammation ; rubor, kalor, dollor, tumor, or function laysia.

THE LAST CONDITION OF CLIENT BEFORE MOVE INTO THE WARD
The airway was unclear, there is secret, RR 28 tpm, using the accessory
muscle of breathing, chest expansion isn’t optimal, relaxed breathing at
semifowler position, Oxygen administration decreased 2 l/m saturation is 93% ,
Breathing sound is vesicular, PAO2 : 82,0 mmHg, PACO2 : 44,6 mmHg, SPAO2 :
80,4, The skin color wasn’t pale, the numbness is lessen, CRT is fine <2
seconds, pulse 84 times a minute, Patient reported the pain is a bit
relived, The scale is 1 (mild), P: the wound on the skin, Q : stabbing, R : wound
area, S : 1 ( 1-5), T : 15 minutes, Patient showed relax facial expression and
distracted from the onset pain, The pain was bearable after changing the
position, After administering via IV ketorolac 3x30 mg, the pain was relieved . as
pprevention for side effect of ketorolac, given injection Ranitidine 2x50mg,
Bandage on contracture hand, The circulation, motion and sensation are good,
Muscle strength is low on the right hand, Patient was doing ROM cooperatively as
procedure. With passive ways then active, Patient was motivated to do the ROM
exercise, ADL and being optimistic for recovery.
Muscle strength
4
44
4
3
333
4
44
4
4
444
Activity scale is 2 (need help and monitoring by others),
Patient is having 3 degree of burn injury, the color is pink and the
surface area of wound is 29,25% skin surrounds wounds are
redness, The burn injury was cleaned and poured with NaCl and
covered with sterile gauze, once a day, Nurses kept the hygiene and
used the aseptic technique before and after the nursing action,
Patient wasn’t having bleeding, the wound became dried showed
the regeneration of tissue, Vital signs was normal : “BP : 110/80

mmhg, RR : 20 bpm, HR : 78 bpm, T : 36,5 C”. The color of urine
isn’t pure yellow as clear, Installed cathether since December 24th
2013, Installed the IV line since 24th 2013, Intake : “Oral : 1200 cc/
24 hours, Parenteral :2500 cc /24 hours” Output : “IWL = 1.065
cc/24 hours, Urine : 1600 cc / 24 hours”. administering the
antibiotics injection of ceftriaxone 2x1 gr, Through there is no sign
of infection or exudates, Nurses keep the aseptic and antiseptic
technic, There is no sign of inflammation ; rubor, kalor, dollor,
tumor, or function laysia.

















