55
| Date post: | 28-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | khalid-ramadan |
| View: | 100 times |
| Download: | 1 times |


Khalid ShawkeyInternistICU Unit
Internal Medicine departmentZagazig University


Body weight
• Maintained at a set point by balance between energy intake and total energy expenditure
• Weight gain- Increase in energy intake- Decrease in energy expenditure (hypothyroidism) - Fluid retention (heart failure or ascites)
• Weight loss- Decrease energy intake due to loss of appetite ( cancer and
chronic diseases)- Increase in energy requirement (sepsis and severe trauma)

Why are so many hospital patients malnourished?
1 Increased nutritional requirements (eg sepsis, burns, surgery)2 Increased nutritional losses (eg malabsorption, output from stoma)3 Decreased intake (eg dysphagia, nausea, sedation, coma)4 Eff ect of treatment (eg nausea, diarrhoea)5 Enforced starvation (eg prolonged periods nil by mouth)6 Missing meals through being whisked off , eg for investigations7 Difficulty with feeding (eg lost dentures; no one available to assist)8 Unappetizing food

Screening of nutritional status
• To all patients on admission to hospital and during their hospital stay
History: - Recent weight loss - recent reduced intake- diet change - nausea, vomiting, pain , diarrhoea which
might have led to reduced intake.

Examination:- State of hydration : dehydration can go hand-in-hand with
malnutrition, and overhydration can mask malnutrition.- Evidence of malnutrition: skin hanging off muscles (eg
over biceps); no fat between fold of skin; hair rough and wiry; pressure sores; sores at corner of mouth.
- Calculate body mass index :BMI <20kg/m2 suggests malnour ishment.
- Anthropomorphic indices, eg mid arm circumference, skin fold measures and grip strength are also used.

Investigations:• plasma proteins: albumin, pre-albumin (shorter half life than albumin), transferrin(decrease may indicate decreased �nutritional status or disease state)• thyroid-binding globulin, retinol-binding protein (may be too sensitive)

Who need nutritional supportPatient malnourished or at risk of malnutrition
• Malnutrition- BMI<18.5 kg/m2- Unintentional weight loss >1% within the last
3-6 months- BMI<20 kg /m2 and unintentional weight loss
>5%within the last 3-6 months

• At risk of malnutrition- Eaten little or nothing for >5 days or likely to
eat little or nothing for the next 5 days or longer
- Poor absorptive capacity or high nutrient losses (malabsorption , fistula , short bowel syndrome ) or increased nutritional needs ( burn , trauma and sepsis)


Benefits of Nutritional Support
• Preservation of nutritional status
• Prevention of complications of protein malnutrition
• Post-operative complications

Entral nutrition
• Cheaper• More physiological (nutrients in the intestinal
lumen prevent atrophy of the gut and pancreas)• prevents gallstones by stimulating gallbladder
motility• Fewer complications• Should be used if the gastrointestinal tract is
functioning normally

Relative Contraindications
• non-functioning gut (e.g. intestinal obstruction, enteroenteral or enterocutaneous fistulae)• uncontrolled diarrhea• GI bleeding

Enteral versus Parenteral Nutrition for AcutePancreatitis
• Cochrane DB of Syst Rev 2010;1:CD002837• Purpose: Compare EN versus TPN on mortality, morbidity and
hospital stay in patients with pancreatitis.• Study Selection: RCTs of TPN versus EN in pancreatitis.• Results: Eight trials (n=348) were included.Enteral nutrition
decreases RR of death (0.50), multiple organ failure (0.55), infection (0.39) and other local complications (0.70). It also decreased hospital stay by 2.37 d.
• Conclusion: EN reduces mortality, organ failure, infections and length of hospital stay in patients with pancreatitis.

Routes of entral nutrition
• Per mouth• Naso gastric tube for short term enteral
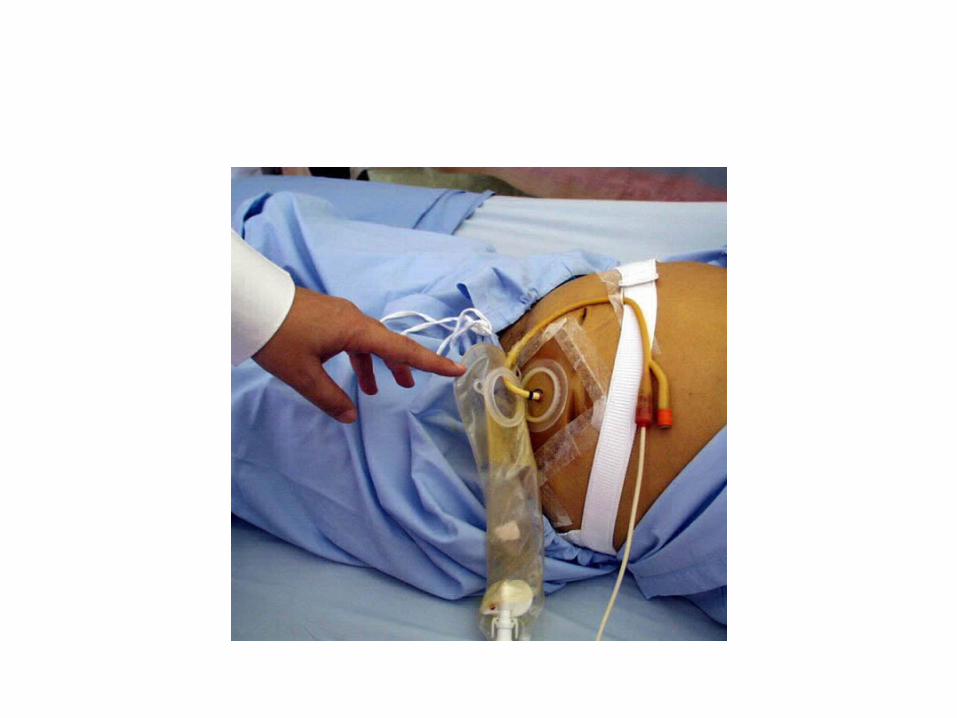
nutrition• nasojejunal (NJ) tube• Percutanous endoscopic gastrostomy(PEG) for
patients who need feeding for longer than 2 weeks
• Percutanous jejunostomy





ENTERAL NUTRITION FORMULAS
• Polymeric feeds consist of whole protein, carbohydrate, fat as a liquid, with or without fibre (eg Osmolite, Isocal, Ensure, Jevity ). Normally contain ~1kCal/mL and 4–6g protein per 100mL. Most people’s requirements are met with 2L/24h.
• Elemental feeds consist of protein as amino acids, carbohydrate as simple sugars, fat content low (therefore high osmolarity) (e.g. Vivonex)
• Also disease-specifi c feeds, eg in liver cirrhosis with hepatic encephalopathy branched-chain amino acid-enriched formulae, High energy low electrolyte diet for dialysis patients and low carbohydrate high fat solutions for ventilated patients.


standard enteral formula
• Tolerated by the majority of patients. • Composition: polymeric/whole protein,
maltodextrins, vegetable fat, electrolytes and micronutrients.
• Nutrison: 1 kcal/ml & 4g protein/100ml. • Energy: 1.5 kcal/ml & 6g protein/100ml. • Protein Plus: 1.25 kcal/ml & 6.3g protein/100ml
Guidelines for success
• Use fine-bore (9 Fr) nasogastric feeding tube when possible.• Elevation of the head of the bed • Check position of nasogastric tube (pH testing) or nasoduodenal tube (X-ray) before starting feeding.• continuous gastric infusion is initiated using a half-strength diet at a rate of 25-50 mL/h. This can be advanced to full strength as tolerated to meet the energy target. • Weigh weekly, check blood glucose and plasma electrolytes (including phosphate, zinc, and magnesium, if previously malnourished).• Treat underlying conditions vigorously, eg sepsis may impede +ve nitrogen balance.• Close liaison with a dietician is essential.

Complications of entral feeding
Gastrointestinal• Distension
• Nausea and vomiting
• Diarrhoea
• Constipation
• Intestinal ischaemia
Infectious
• Aspiration pneumonia
• Bacterial contamination
Mechanical• Malposition of feeding tube• Sinusitis• Ulcerations / erosions• Blockage of tubes

Parenteral nutrition
the practice of feeding a person intravenously, by passing the usual process of eating and
digestion

Indications• short term (<1 mo)- whenever GI tract not functioning�- only situations where PN has been well shown to �increase survival are after bone marrow transplant and in short bowel syndrome, some evidence for benefit in gastric cancer, but often used in ICU, perioperatively and difficult to control sepsis- preoperative: only useful in severely malnourished (e.g. loss of >15% of pre-morbid weight, serum albumin <28 g/L or <2.8 g/dL), and only if given for ≥2 wk

- � renal failure: PN shown to increase rate of recovery; no increase in survival- liver disease: branched chain amino acids may shorten duration �of encephalopathy; no increase in survival- IBD: PN closes fistulae and heals acute exacerbations of mucosal inflammation, but effect is transient (EN is equally effective)- some evidence for efficacy, but convincing data not available for: .radiation/chemotherapy-induced enteritis� .AIDS with wasting diarrhea� .severe acute pancreatitis�

• long term (>1 mo): can be given at home- severe untreatable small bowel disease (e.g. radiation enteritis, extensive CD, high output fistulae)- following surgical resection of >70% of bowel (e.g. bowel infarction)- severe motility diseases (e.g. scleroderma affecting bowel)

Relative Contraindications
• functional GI tract for enteral nutrition• active infection; at least until appropriate antibiotic coverage• inadequate venous access; triple-lumen central venous lines usually prevent this problem• unreliable patient or clinical setting

Two primary types of PN
• Central parenteral nutrition (CPN) and • Peripheral parenteral nutrition (PPN).

Central parenteral nutrition or total parenteral nutrition (TPN)
• provides nutrients through a large-diameter vein, usually the superior vena cava by access of the subclavian or internal jugular vein.
• With CPN a hyperosmolar formula (1300 to 1800 mOsm/L) can be provided consisting of glucose (15% to 25% final concentration), amino acids, and electrolytes to fully meet the nutrient needs of the patient.
• Central parenteral nutrition can be maintained for prolonged periods and can be adjusted to meet nutrient and volume needs for patients who may require a fluid restriction (1). When venous access for the delivery of nutrients is required for greater than 2 weeks, CPN is indicated (2).1. Mirtallo JM. Introduction to parenteral nutrition. In: Gottschlich MM, ed. The Science and Practice of Nutrition
Support: A Case-Based Core Curriculum. Dubuque, Ia: Kendall/Hunt Publishing Co; 2001.2. ASPEN Board of Directors and The Clinical Guidelines Task Force. Guidelines for the use of parenteral and enteral
nutrition in adult and pediatric patients. JPEN. 2002;26 (suppl)(1):1SA-138SA.


Peripheral parenteral nutrition• uses the peripheral vein as venous access. This form of parenteral nutrition is similar to
CPN except lower formula concentrations have to be provided due to use of the peripheral vein that can only tolerate solutions providing less than 900 mOsm/L.
• Compared with CPN formulas, PPN formulas have a lower dextrose concentration (5% to 10% final) and amino acid (3% final) concentrations.
• Because of the inability to infuse higher concentrations via the peripheral vein, larger fluid volumes often have to be administered in PPN to provide comparable energy and protein doses seen with CPN. This poses a challenge for patients requiring fluid restriction.
• The maximum volume of PPN usually tolerated is 3 L/day (125 mL/hour). Repletion of nutrient stores is not a goal of PPN, and it is not intended to be used in severely malnourished patients (1).
• PPNis indicated only for mildly to moderately malnourished patients when they are unable to ingest adequate energy orally or enterally, or when CPN is not feasible. Typically, PPN is used for short periods (up to 2 weeks) because of limited tolerance and vulnerability of peripheral veins (eg, risk of peripheral venous thrombophlebitis) (1).
1. ASPEN Board of Directors and The Clinical Guidelines Task Force. Guidelines for the use of parenteral and enteral nutrition in adult and pediatric patients. JPEN. 2002;26 (suppl)(1):1SA-138SA.

Requirements
• The components of parenteral nutrition include adequate fluid (30 mL/kg body weight/24 h for adults, plus any abnormal loss);
• energy from glucose, amino acids, and lipid solutions;
• nutrients essential in severely ill pts, such as glutamine, nucleotides, and products of methionine metabolism; and electrolytes, vitamins, and minerals.

Caloric Requirements
Schofield Equation
25 to 30 kcal/kg/dayHow Much CHO & Fats?
4-7 mg/kg/min/24h (Espen 2009) of glucoseContain 4 kcal /gCHO usually form 60-70 % of calories
0.7-1.5 g / kg Lipid(Espen 2006)Contain 9 kcal/gFats usually form 30 to 40% of calories

How Much Protein to Give?
Non-stress patients 0.8 g / kg / day
Mild stress 1.0 to 1.2 g / kg / day
Moderate stress 1.3 to 1.75 g / kg / day
Severe stress 2 to 2.5 g / kg / day
Contain 4 kcal/g
15-20% of total calories

Electrolyte Requirements
Cater for maintenance + replacement needsNa+ 1 to 2 mmol/kg/d (or 60-120 meq/d)K+ 0.5 to 1 mmol/kg/d (or 30 - 60 meq/d)
Mg++ 0.35 to 0.45 meq/kg/d (or 10 to 20 meq /d)
Ca++ 0.2 to 0.3 meq/kg/d (or 10 to 15 meq/d)
PO42- 20 to 30 mmol/d

Trace Elements
Zn 2-4 mg/day
Cr 10-15 ug/day
Cu 0.3 to 0.5 mg/day
Mn 0.4 to 0.8 mg/day

DISEASE SPECIFIC FORMULATIONS
• Renal failureeg. kidmin
- High energy feeds is used (2kcal/ml) to reduce volume
- In TPN essential amino acids may stimulate protein synthisis and reduce urea by recycling nitrogen into non essential amino acids
- Low sodium and potassium feeds with supplemental vitamins may be required

COPD
- Malnutrition is common- Ventilatiun in respiratory failure has high
energy expenditure- Over feeding with carbohydrate causes high
co2 production- Feed should contain less carbohydrate and
high fat- Fat oxidation produce 30% less co2

Hepatic failure
eg. AMINOLEBAN- Impaired fat metabolism and carbohydrate
intolerance are common- Use of branched chain ( instead of aromatic )
amino acids may improve mental status in hepatic encephalopathy
- TPN must contain less sodium and volume because of aldosterone induced water retention

Complications of TPN
• Catheter related-sepsis-Thrombosis-embolism-pneumothorax• Metabolic-hyperglycemia-hypercalcemia• Electrolyte disturbances• Liver dysfunction and gall stones• Fluid overload
Stopping TPN
• Stop TPN when enteral feeding can restart • Wean slowly to avoid hypoglycaemia• wean TPN while introducing enteral feeding and stop
when enteral intake meets TEE

Monitoring of artificial nutrition
• Fluid balance (weight, intake vs. output)• Glucose, electrolytes, BUN (daily until stable, then 2x per week)• Serum creatinine, albumin, phosphorus, calcium, magnesium, Hb/Hct,• WBC (baseline, then 2x per week)• INR (baseline, then weekly)• Micronutrient tests as indicated
Nutritional Balance
Nutritional Balance = Ninput - Noutput
1 g N = 6.25 g proteinNinput = (protein in g x 6.25) Noutput = 24h urinary urea nitrogen + non-
urinary N losses(estimated normal non-urinary Nitrogen
losses about 3-4g/d)

Refeeding syndrome
• Occurs within few days of refeeding• Underrecognized and can be fatal• The shift from the use of fat as energy source
during starvation to use of carbohydrate during refeeding
• Carbohydrate lead to augmentation of insulin release with rapid intracellular passage of phosphate , magnisium and potassium that lead to hypophosphatemia , hypomagnesemia and hypokalemia

• Hypophosphatemia lead to multiple organ dysfunction ( muscle weakness, rhabdomyolysis, cardic failure , immune suppression, hemolytic anemia ,thrombocytopenia ,hallucinations and fits)

NICE 2006 criteria for who at risk for refeeding syndrome
• 2 of the following- BMI < 18.5 KG/M2- Unintentional wt loss >10% in the last 3-6 months- History of alcohol abuse or drug including insulin , diuritics
, chemotheraby and antacids• One of the following - BMI < 16 kg/m2- Unintentional wt loss > 15% in the last 3-6 months- Little or no nutritional intake for more than 10 days- Low level of K ,Ph , Mg prior to feeding
• Begin feeding at 25-50% of estimated calorie requirement
• Increasing by 100 calories per day• Restore circulatory volume and monitor fluid
balance and overall clinical status closely• Serum phosphate ,mg, ca , k , urea and creatinine
should be checked daily for the first week• parenteral phosphate administration (eg
18mmol/d) in addition to oral supplementation

Immunonutrition
• Use compounds that may improve metabolic and immune response in critically ill patients
• Glutamine, an amino acid and primary energy source for enterocytes , preserve intestinal integrity
• Arginine stimulate immune function and nitrogen balance
• Omega 3 unsaturated fatty acids from fish oil are anti inflammatory agent and immunomodulators


















