38
Nutrition Aspects in Elderly Pranithi Hongsprabhas Division of Clinical Nutrition, Department of Medicine, Faculty of Medicine, KKU
| Date post: | 25-Dec-2015 |
| Category: |
Documents |
| Upload: | laurence-knight |
| View: | 215 times |
| Download: | 0 times |
Nutrition Aspects in Elderly
Pranithi HongsprabhasDivision of Clinical Nutrition, Department of Medicine,
Faculty of Medicine, KKU
Outline
Nutritional disorders Over nutrition Under nutrition
Etiology of malnutrition Nutrition related problems

Introduction
Changes in aging nutritional risk
Organ system reserve Weaken homeostasis control heterogenicity of response
Genetic Environment

Geriatric failure to thrive (FTT)
FTT: state of decline Decline in vitality… The causes of deterioration: not
identifiable or irreversible..
Undergo a process of functional decline, progressive apathy and loss of willingness
to eat and drink that culminate in death

4 Syndromes of FTT
Impaired physical function Malnutrition Depression Cognitive impairment

Manifestation Weight loss > 5% of baseline Appetite Poor nutrition Inactivity Accompanied by
Dehydration Depressive symptoms Impaired immune function Low cholesterol

Undernutrition syndrome in elderly More common
home 2-32% Long term care 25-60% Institution 1-83% Hospital 30-65%
Greater impact: less able to adapt to underfeeding Less frequent hunger Not regain total # of weight
Consequences
Functional disabilities Nosocomial infection Perioperative complication Morbidity, mortality Longer LOS Increased health care expenditure
Etiology of under nutrition
Inadequate intake (starvation)
Altered absorption Nutrient loss
Nutrient metabolism

Weight loss in elderly
Inadequate intake Inflammatroy effect of illness
(cachexia) Muscle atrophy (sarcopenia of elderly)

Nutrient intake in elderly
Anorexia Physical illness: organ dysfuction, cancer,
infection Mental illness Medication
Poor oral/dental health Dysphagia Visual impairment
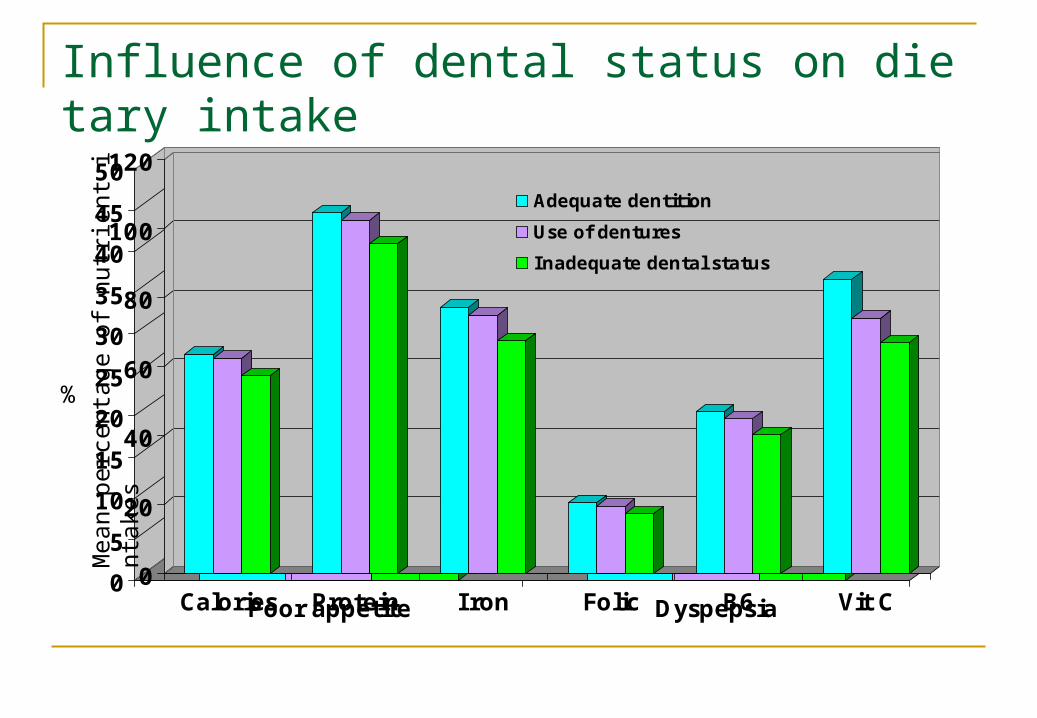
Influence of dental status on dietary intake
21.6 22.7
35
28.632.8
47.9
0
5
10
15
20
25
30
35
40
45
50
Poor appetite Dyspepsia
Adequate dentition
Use of dentures
inadequate dental status
P<0.01 P<0.001
%
0
20
40
60
80
100
120
Calories Protein Iron Folic B6 Vit C
Adequate dentition
Use of dentures
Inadequate dental status
Mea
n pe
rcen
tage
of
nutr
ient
inta
kes

GI problems in elderly and their relations to Nutritional disorders Dysphagia
Oropharygeal Esophageal
Atrophic gastritis Delayed GET Dyspepsia Diverticulum Colonic cancer

Atrophic gastritis Type A: pernicious
anemia (autoimmune)
Type B Chronic inflammation Associated with HP
Secretion of Acid Pepsin Intrinsic factor
0
5
10
15
20
25
30
35
40
60-69 70-79 80+
% Atrophic gastritis
Krasinski SD J Am Geriatr Soc. 1986 Nov;34(11):800-6.
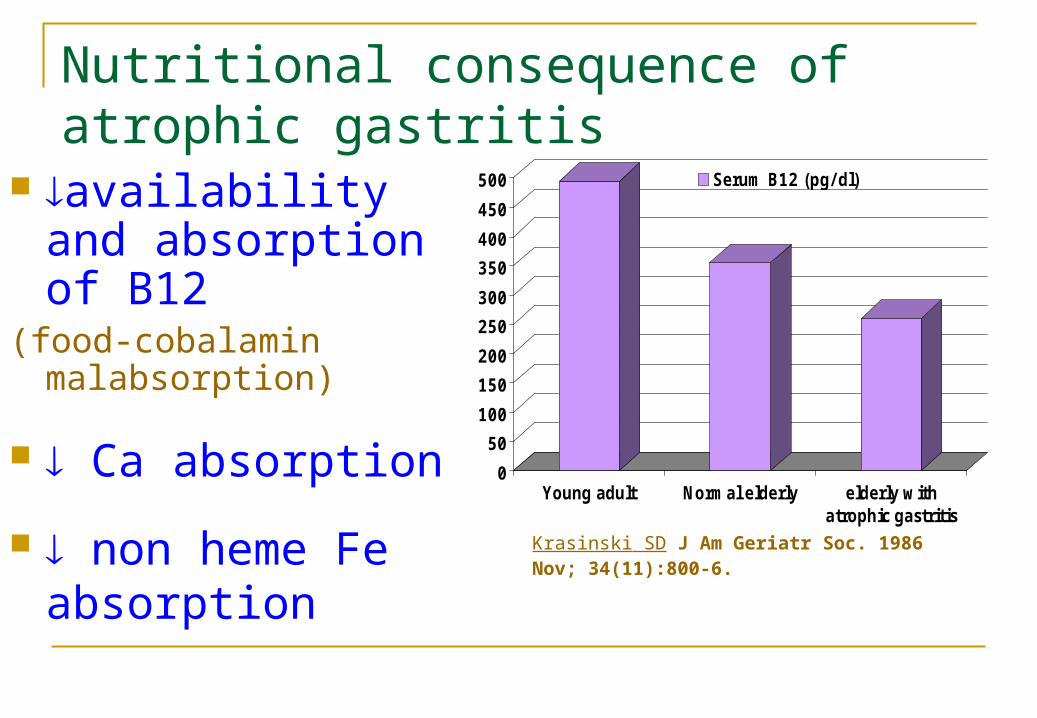
Nutritional consequence of atrophic gastritis
availability and absorption of B12
(food-cobalamin malabsorption)
Ca absorption
non heme Fe absorption
0
50
100
150
200
250
300
350
400
450
500
Young adult Normal elderly elderly withatrophic gastritis
Serum B12 (pg/ dl)
Krasinski SD J Am Geriatr Soc. 1986 Nov; 34(11):800-6.

B12 deficiency
Megaloblastic anemia Neurological damage
SCDS Dementia
Atherosclerosis (hyperhomocysteinemia)
Nutrition metabolism related to body composition changes Body composition
Fat free mass Fat mass
Energy expenditure Decreased: with aging and lean body mass Increased:
Parkinsonism Cancer Infection Chronic cardiac failure Chronic pulmonary diseases

Nutrition metabolism related to body composition changes Protein requirement: increased
catabolism in diseases synthesis
Cachexia Cancer Cardiac Pulmonary Chronic infection energy requirment ~10-15 % protein requirement Hormonal control: cortisol,
catecholamine Cytokines: TNF, IL-1, IL-6
Sarcopenia: ~poverty of flesh
lean body mass Concomitant fat
mass
Multifactorial disorders
sex hormone: testosterone/DHEA GH and IGF-1 cytokine production Neuromuscular changes Physical inactivity Malnutrition

G H secretion
f at m ass
I nactiv ity
D isabilityM orbidityM ortality
S arcopenia E strogen/A ndrogen
W eakness m etabolicreserve
M uscle m ass
M uscle quality
P roinfl am m atorycytok ines
C N S input ( loss of m otor neurones,changed m otor unit activation)
Consequence of Sarcopenia
energy expenditure insulin sensitivity muscle strength risk of disability risk of fall risk of mortality

Distinguishing sarcopenia from cachexia
Sarcopenia Cachexia
Appetite Not affected Suppress in earlyFood intake Not affected BW May FFM Alb N Cholesterol May Cortisol May Inflammatory disease
Not present Present
Response to refeeding
Resistant Resistant
Pathway Not lead to cachexia
May lead to sarcopenia
Clin Nutr 2006;26:389-99

Exercise Training and Nutritional Supplementation for Physical Frailty in Very Elderly People
Mean Changes in Muscle Strength after
Fiatarone MA et al. NEJM 1994; 330:1769-1775
Mean (±SE) Changes in Energy Intake in the Four Study Groups
Nutritional screening
Mininutritional assessment (MNA)Screening Food intake (3mo) Wt change (3mo) Mobility Psychological or acute disease Neuropsychological preoblems BMI
Markers Screening tools
MNA Hx
Wt loss Dietary Hx Medical Hx
Anthropometry Lab
CBC Alb Chol

Nutritional Rx:
Rx causes of poor intake Nutritinal intake
Diet Oral nutritional supplement (ONS) Enteral tube feeding (ETF)
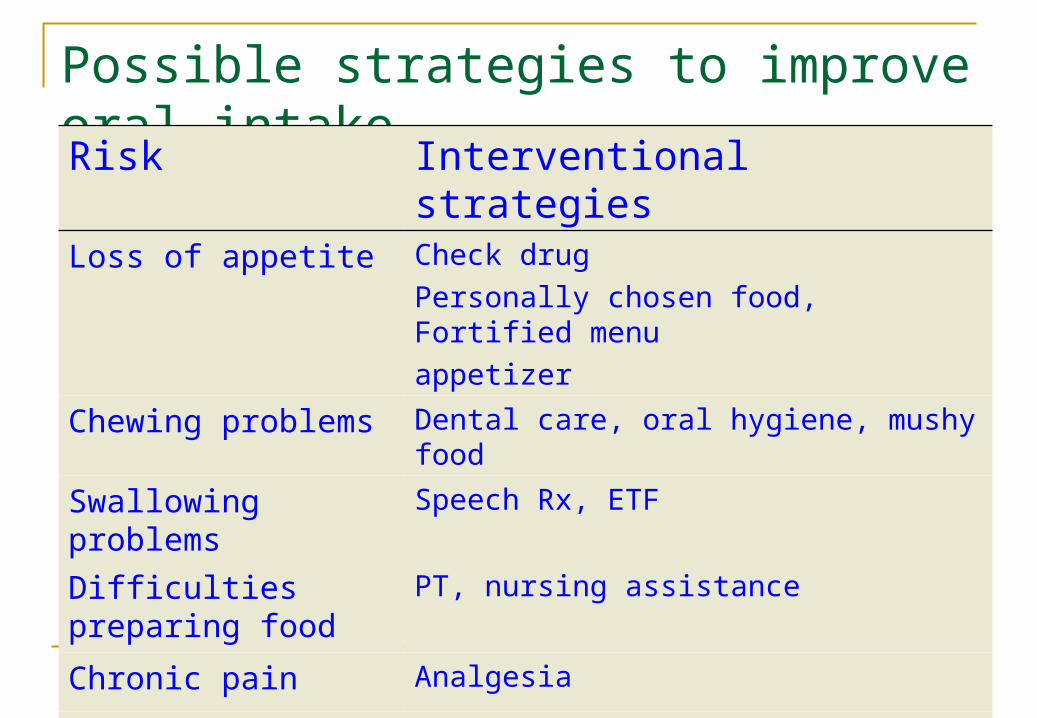
Possible strategies to improve oral intakeRisk Interventional strategiesLoss of appetite Check drug
Personally chosen food, Fortified menuappetizer
Chewing problems Dental care, oral hygiene, mushy food
Swallowing problems
Speech Rx, ETF
Difficulties preparing food
PT, nursing assistance
Chronic pain Analgesia Depression Check medication, medical Rx
Social isolation Social service, meals on wheels

Enteral nutrition Oral nutritional supplement
1081
957
45.9 38.3
0
200
400
600
800
1000
1200
Energy intake (kcal) Protein intake(g)
ONSControl
Bourdel-Marchasson I, et al Nutrition. 2000 Jan;16(1):1-5.
536 173 899. ( . to . )
Potter J, et al ใ BMJ199831;-7495501;
Meta-analysis of protein energy supplement (ONS)

ETF
Bourdel-Marchasson I, et al Nutrition. 2000 Jan;16(1):1-5 4.04 (3.15 4.94)to
Meta-analysis of protein energy supplement (ETF)
Potter J, et al ใ BMJ199831;-7495501;

Obesity in elderly

Diseases associated with obesity Cardiovascular, stroke HTN DM/Metabolic syndrome Dyslipidemia Cancer
Breast Endometrial Colorectal
GERD Cholelithiasis NASH OSA/OHS Asthma OA Gout Infertility PCOS incontinence
Am
eric
an J
ourn
al o
f Epi
dem
iolo
gy20
06;1
63:9
38
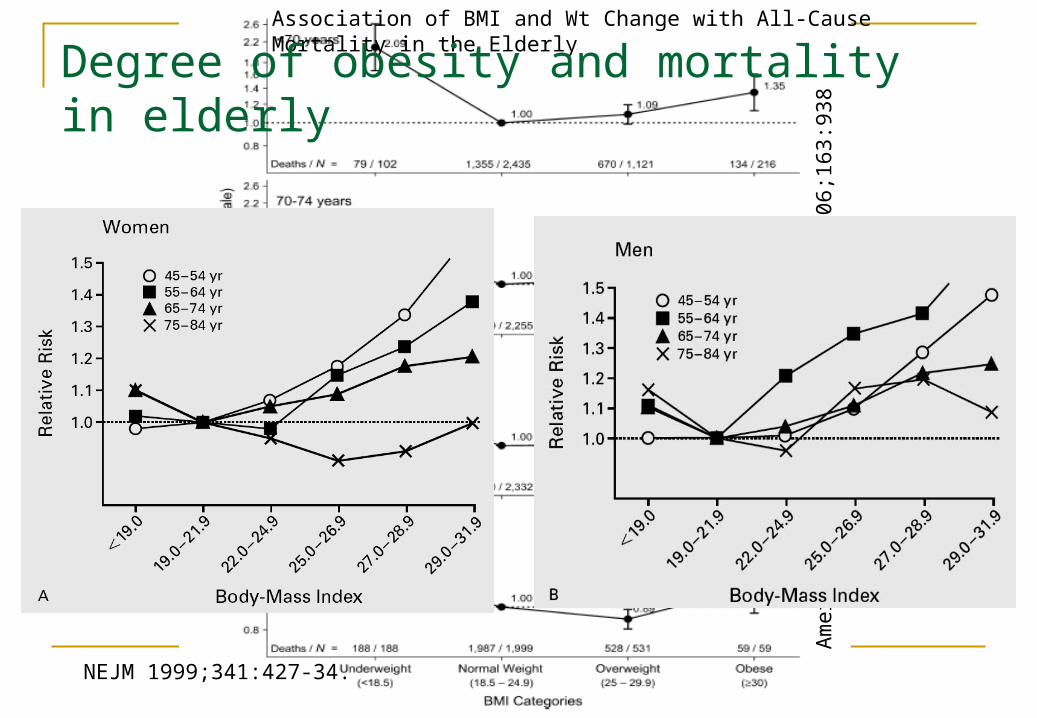
Association of BMI and Wt Change with All-Cause Mortality in the Elderly
Degree of obesity and mortality in elderly
NEJM 1999;341:427-34.

Relation between in Wt and RR of Type 2 DM, HTN, CHD, and Cholelithiasis.
FU 10 yr, age 40-65 yr FU 18 yr, age 30-55 yr
NEJM 1999;341:427-34.

Voluntary Wt Reduction in Older Men Hip Bone Loss: The Osteoporotic Fractures in Men Study

Andres, R. et. al. Ann Intern Med 1993;119:737-743
Association of Mild to Moderate Weight Loss with All-Cause Mortality*
Treatment strategies
Preventing weight gain and overweight healthy weights and
avoiding further weight gain among those already overweight
are important public health goals. Weight reduction in pts with mobility
problem Therapeutic lifestyle control

















