28
Nutrition & Diet Therapy, 7th edition Energy- & Protein-Modified Diets for Cancer & HIV Infection Chapter 25
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | claud-payne |
| View: | 223 times |
| Download: | 5 times |

Nutrition & Diet Therapy, 7th edition
Energy- & Protein-Modified Diets for Cancer & HIV Infection
Chapter 25

Nutrition & Diet Therapy, 7th edition
I. Cancer
• Growth of malignant tissue• Many different kinds of malignant
growth– Differ in characteristics– Occur in different locations in the body– Take different courses– Require different treatments
• Advanced cancers, especially those of GI tract, can seriously impair nutrition status
Malignant: cancerous cell or tumor which can injure healthy tissue & spread
cancer to other parts of the body

Nutrition & Diet Therapy, 7th edition
Cancer
• Cancer development (carcinogenesis)– Arises from mutations in genes that control cell
division– Abnormal mass of cells (tumor) develops own
blood supply to deliver oxygen & nutrients, & otherwise support tumor growth
– Tumor causes disruption of functioning of surrounding tissues
– May spread to another region of body (metastasis)
– Reasons for development varied, including exposure to cancer-causing agents (carcinogens) in environment

Nutrition & Diet Therapy, 7th edition

Nutrition & Diet Therapy, 7th edition
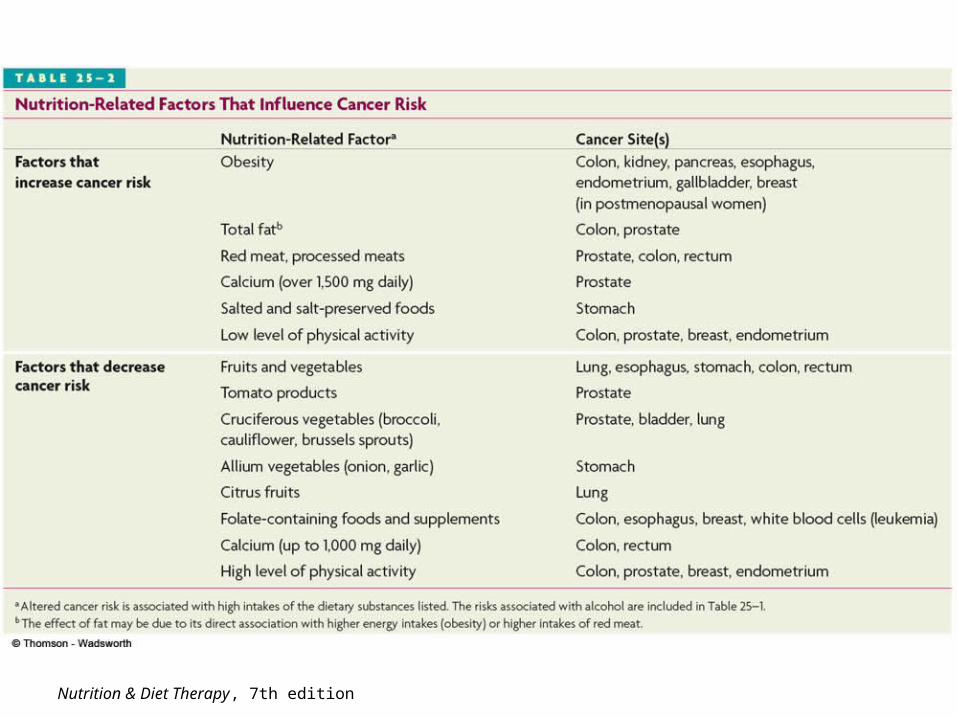
Cancer
• Nutrition & cancer risk– Diet, lifestyle, and environmental factors
have strong influence on cancer risk• Damage to DNA• Alteration of metabolism of carcinogens• Inhibition of formation of carcinogens

Nutrition & Diet Therapy, 7th edition
Nutrition & Diet Therapy, 7th edition

Nutrition & Diet Therapy, 7th edition
Cancer
• Consequences of cancer– Depends on location of
tumor, severity & treatment
– Complications often due to tumor’s effect on surrounding tissues
– Effectiveness of treatment is greatest with early detection & intervention
Frequent consequences – Cancer cachexia: wasting
syndrome characterized by anorexia, muscle wasting, weight loss & fatigue
– Metabolic changes– Anorexia & reduced food
intake related to…• Chronic nausea & early
satiety• Fatigue• Pain• Mental stress• Effects of cancer tx-
meds, chemo, etc.• Obstructions

Nutrition & Diet Therapy, 7th edition
Cancer• Treatments for cancer
– Main goals of treatment are to remove cancer cells, prevent further tumor growth & alleviate symptoms
– Primary treatment involves surgery, chemotherapy, radiation therapy, or combination of the three
– Surgery• Purpose
– Tumor removal– Determination of extent of involvement– Discern involvement of surrounding tissues
• Acute metabolic stress caused by surgery increases energy & protein needs; may increase muscle wasting
• Other effects can reduce food intake, contributing to nutrient losses & malnutrition

Nutrition & Diet Therapy, 7th edition
Cancer• Treatments for cancer (con’t)
– Chemotherapy• Relies on use of drugs to inhibit tumor growth• Most drugs are toxic to healthy cells as well as cancerous ones• Associated with variety of nutrition-related side effects
– Radiation therapy• Treatment of cancer cells by damaging DNA (& causing cell death)
with x-rays, gamma rays, other atomic particles• Focused directly on tumors with minimal damage to surrounding
tissues• See p. 679, T 25-5, for specific nutr. effects of chemo & radiation
– Bone marrow transplant• Replacement of bone marrow that has been destroyed by
chemotherapy or radiation therapy• Used as one of primary treatments for leukemia• Immunosuppressant drugs necessary when separate donor used• Major impact on food intake & nutrition status

Nutrition & Diet Therapy, 7th edition
Cancer
• Nutrition therapy for cancer– Goals of nutrition therapy
• Minimize loss of weight & muscle tissue• Correct nutrient deficiencies• Provide diet that can be tolerated & enjoyed despite
complications of disease
– Nutrition needs among cancer patients vary widely
– Appropriate nutrition helps patients preserve strength & improve recovery
– Initial screening & follow-up assessment for malnutrition is necessary during treatment & recovery periods-p.690

Nutrition & Diet Therapy, 7th edition
Cancer
• Nutrition therapy for cancer (con’t)– Protein & energy intake recommendations
• Recommended ranges vary depending on patient condition
• Energy needs may be 25-35 kcalories/kg, depending on patient’s current weight, activity level, degree of metabolic stress, energy needs for tissue repair & weight regain
• Protein requirements depend on level of metabolic stress, treatment stage & cachexia-p.680
• Regular monitoring of weight changes, nutrition status & adjustments of diet necessary
• Supplementation may be necessary or How To-p.681

Nutrition & Diet Therapy, 7th edition
Cancer
• Nutrition therapy for cancer (con’t)– Managing symptoms & complications
• Thorough nutritional assessment• Patient’s response to strategies varies
considerably
– Enteral & parenteral nutrition support• Necessary for patients with long-term or
permanent GI impairment or severe complications interfering with food intake
• Enteral nutrition preferred unless contraindicated

Nutrition & Diet Therapy, 7th edition
II. HIV Infection• Human immunodeficiency (HIV) virus
attacks immune system, disabling defenses against infection & some cancers
• Often leads to acquired immune deficiency syndrome (AIDS)
• Diagnosis devastating to patient– Can expect ever-worsening course of illness,
possibly death– Recent treatment options have expanded,
offering benefits to patients & improvements in quality of life

Nutrition & Diet Therapy, 7th edition
HIV Infection• World-wide epidemic
– Although no cure, progress in treatment has been made
– Best course of treatment is prevention
– Death rate in U.S. begin to decline during 1990s
– Progression from HIV to AIDS has also slowed
• Transmission– Sexual transmission– Direct contact with
contaminated body fluids, including blood, semen, vaginal secretions, breast milk
• Risk factors– Many individuals remain
asymptomatic during early stages—unknowingly passing infection to others
– Individuals at risk should be tested (T. 25-8)
– Testing can detect HIV antibodies within several months after exposure, sometimes sooner (1-2 wks.)
– Estimated 25% of infected individuals in U.S. are unaware of infection

Nutrition & Diet Therapy, 7th edition

Nutrition & Diet Therapy, 7th edition
HIV Infection
• Consequences of HIV Infection– Destruction of immune cells—
most affected are helper T cells– Nonspecific early symptoms
• Fever, sore throat, malaise, skin rashes, nausea, muscle & joint pain, diarrhea
• After initial symptoms, may remain asymptomatic for 5-10 years or more
• Untreated, depletion of T cells eventually increases susceptibility to opportunistic infections
Opportunistic Infection
Infection that results from microorganisms that do
not cause disease in healthy individuals, but are damaging to those
with compromised immune system (exs.
Thrush, pnuemonia, TB)

Nutrition & Diet Therapy, 7th edition
HIV Infection• Consequences of HIV Infection (con’t)
– AIDS-defining illnesses• Diseases and complications associated with later stages of HIV
infection, including…– Severe infections– Certain cancers– Wasting of lean tissue
• Disease progression monitored by measuring concentrations of helper T cells, circulating virus & monitoring clinical symptoms
– HIV-lipodystrophy syndrome• Collection of abnormalities in fat & glucose metabolism resulting
from HIV drug treatment• Includes body fat redistribution, abnormal blood lipid levels &
insulin resistance, breast enlargement (in men & women), fat accumulation at base of neck, lipomas
• Often develop hypertriglyceridemia, low HDL cholesterol levels, glucose intolerance & hyperinsulinemia

Nutrition & Diet Therapy, 7th edition
HIV Infection• Consequences of HIV Infection
(con’t)– Weight loss & wasting (AIDS-
related wasting syndrome)• 10% weight loss within 6
months• Diarrhea or fever for more than
30 days with no known cause• Linked to disease progression,
reduced strength & fatigue• Severe in later stages; increases
risk of death• Causes
– Anorexia & reduced food intake
– Altered metabolism & malabsorption
– Chronic diarrhea– Diet-drug interactions
Anorexia & reduced food intake
• Key factor in development of wasting
• Results from many associated problems– Emotional distress, pain
& fatigue– Oral infections– Respiratory disorders– Cancer– Medications
Nutrition & Diet Therapy, 7th edition
HIV Infection
• Consequences of HIV Infection (con’t)– GI tract complications
• May result from opportunistic infections, medications or HIV infection itself
• High risk of malnutrition related to…– Infections in stomach & intestines (villi short & flat)– Nausea, vomiting & diarrhea from medications– Bacterial overgrowth resulting from antiviral, antibiotic
& antifungal medications
• Treatment– No cure, but treatment can slow progression,
reduce complications & alleviate pain

Nutrition & Diet Therapy, 7th edition
HIV Infection
• Treatment– Highly active antiretroviral therapy (HAART)
• Combination of 3 or more antiretroviral agents• Improved lifespan & quality of life for many patients• Multiple adverse effects from drugs
– GI effects; diet-drug interactions– Skin rashes– Headache– Anemia– Tingling & numbness– Hepatitis– Pancreatitis– Kidney stones
Nutrition & Diet Therapy, 7th edition
HIV Infection• Treatment (con’t)
– Control of anorexia & wasting
• Appetite stimulants• Physical activity • Anabolic hormones (HGH)
– Control of lipodystrophy• Under investigation• Aerobic activity &
resistance training help reduce abdominal fat
• Alternative antiretroviral drugs to alleviate symptoms
• Medication treatment for abnormal blood lipids & insulin resistance
– Alternative therapies• May be unconventional• Many harmless, but
can be expensive• Monitoring use of
dietary supplements is essential to reduce risk of nutrient-drug & herb-drug interactions

Nutrition & Diet Therapy, 7th edition
HIV Infection
• Medical nutrition therapy– Initial nutrition assessment to provide baseline– Weight maintenance
• Primary objective: maintain weight & muscle tissue• Determine dietary & lifestyle factors that may
interfere with food intake, appetite & physical activity• Provide suggestions to prevent future weight
problems• Small, frequent feedings may be better tolerated
than large meals• Addition of nutrient-dense food and snacks, protein or
energy bars, oral supplements may help

Nutrition & Diet Therapy, 7th edition
HIV Infection
• Medical nutrition therapy (con’t)– Vitamins & minerals
• Needs are variable• Multivitamin-mineral supplements often recommended to
reduce risk of deficiencies associated with reduced food intake, malabsorption, diet-drug interactions & nutrient losses
– Metabolic complications• Dietary adjustments for treatment of insulin resistance &
elevated triglyceride & LDL levels should be tried before medication treatment
– Achieve & maintain desirable weight– Replace saturated fats with monounsaturated & polyunsaturated
fats– Limit intake of trans fats & cholesterol– Replace sugar intake with complex carbohydrates
• Maintain regular physical activity

Nutrition & Diet Therapy, 7th edition
HIV Infection
• Medical nutrition therapy (con’t)– Symptom management– Food safety-use safe handling and food
preparation (HIV risk of infections)– Enteral & parenteral nutrition support
• Patients may need aggressive nutrition support during later stages
• Tube feeding preferred if GI tract is functional
• Parenteral nutrition reserved for patients who cannot tolerate enteral nutrition

Nutrition & Diet Therapy, 7th edition
Nutrition in Practice—Ethical Issues in Nutrition Care
• New technologies, including availability of specialized nutrition support, results in difficult ethical dilemmas
• When medical treatments prolong life by delaying death, reduced quality of life may result
• Decisions to withhold or withdraw nutrition support require careful consideration of ethical principles

Nutrition & Diet Therapy, 7th edition
Nutrition in Practice—Ethical Issues in Nutrition Care
• Life-sustaining procedures– Nutrition support & hydration– CPR– Defibrillation– Mechanical ventilation– Dialysis
• Patient’s rights to treatment– Difficult to determine best course of action for terminally
ill or patients who are unlikely to regain consciousness– When patients (or caregivers) demand treatment (when
health practioners consider it to be futile), legal resolution may follow

Nutrition & Diet Therapy, 7th edition
Nutrition in Practice—Ethical Issues in Nutrition Care
• Advance directive– Living will or medical directive: include detailed
instructions regarding life-sustaining procedures individual wants or does not want
– Take effect when it is determined that the patient lacks ability to understand & make treatment decisions
• Durable power of attorney (or health care proxy)– Another person, or health care agent, is appointed to act
as decision-maker in event of patient incapacitation– Agent is given comprehensive power to supervise care,
make decisions about medical staff, facility & procedures

















