Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
140
A trial fibrillation (AF) is the mostcommon, sustained arrhythmia diag-nosed in clinical practice. Given
that it is associated with significant mor-bidity and mortality, it is concerning thatthere is a steadily rising prevalence of AFworldwide (1,2). As a result, a greater under-
standing of modifiable, predisposing risk factors iswarranted in an attempt to slow the rising populationand economic burden of AF (3).
Obesity is a risk factor with increasingly broadimplications for health in both developed and devel-oping countries undergoing epidemiologic transition(4,5). Our evolving understanding regarding therelationship between AF and measures of obesity,body size, and weight change are, therefore, partic-ularly significant given the rising prevalence of bothAF and obesity (6). Although analyses have studiedthe association between obesity and AF in the past,these have been limited by the heterogeneous mea-sures of obesity reported in individual studies (7–9).In addition, there has since been increasing recogni-tion that obesity may influence the risk of AF in otherclinical scenarios, such as after cardiac surgery orcatheter ablation procedures (6,10). Given that anaccurate and reliable characterization of AF riskassociated with obesity would be immensely infor-mative to clinical practice, we sought to describethe association between obesity and AF in differentsettings, with standardization of obesity measuresallowing for a more comprehensive inclusion of
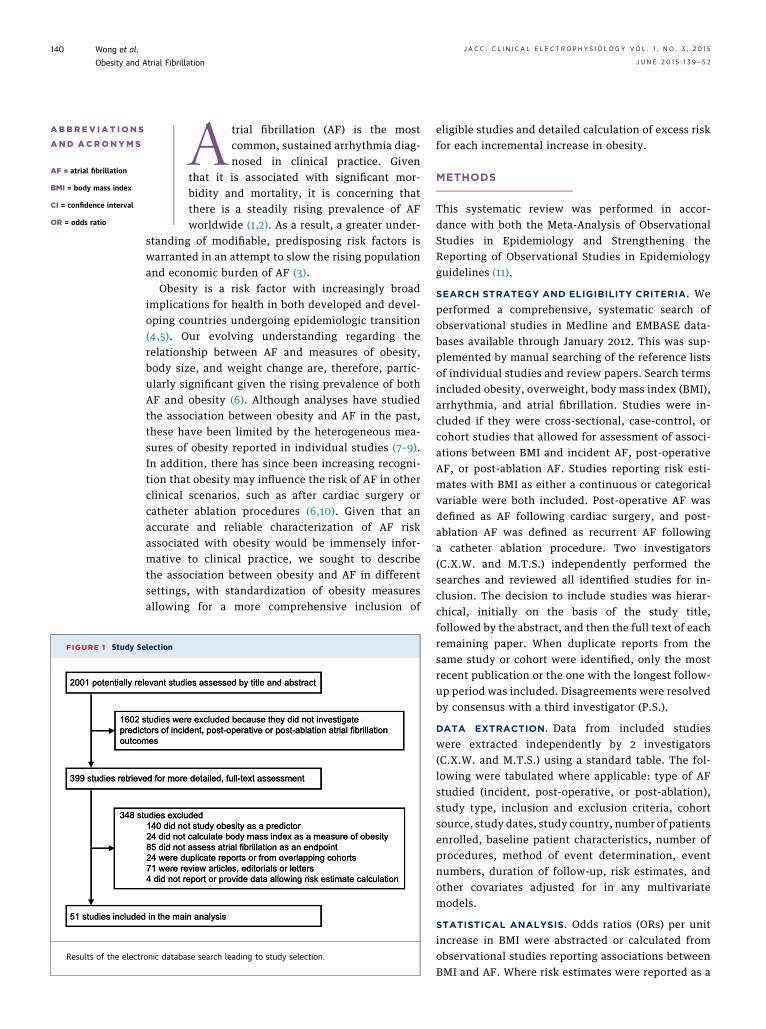
se search leading to study selection.
eligible studies and detailed calculation of excess riskfor each incremental increase in obesity.
METHODS
This systematic review was performed in accor-dance with both the Meta-Analysis of ObservationalStudies in Epidemiology and Strengthening theReporting of Observational Studies in Epidemiologyguidelines (11).
SEARCH STRATEGY AND ELIGIBILITY CRITERIA. Weperformed a comprehensive, systematic search ofobservational studies in Medline and EMBASE data-bases available through January 2012. This was sup-plemented by manual searching of the reference listsof individual studies and review papers. Search termsincluded obesity, overweight, body mass index (BMI),arrhythmia, and atrial fibrillation. Studies were in-cluded if they were cross-sectional, case-control, orcohort studies that allowed for assessment of associ-ations between BMI and incident AF, post-operativeAF, or post-ablation AF. Studies reporting risk esti-mates with BMI as either a continuous or categoricalvariable were both included. Post-operative AF wasdefined as AF following cardiac surgery, and post-ablation AF was defined as recurrent AF followinga catheter ablation procedure. Two investigators(C.X.W. and M.T.S.) independently performed thesearches and reviewed all identified studies for in-clusion. The decision to include studies was hierar-chical, initially on the basis of the study title,followed by the abstract, and then the full text of eachremaining paper. When duplicate reports from thesame study or cohort were identified, only the mostrecent publication or the one with the longest follow-up period was included. Disagreements were resolvedby consensus with a third investigator (P.S.).
DATA EXTRACTION. Data from included studieswere extracted independently by 2 investigators(C.X.W. and M.T.S.) using a standard table. The fol-lowing were tabulated where applicable: type of AFstudied (incident, post-operative, or post-ablation),study type, inclusion and exclusion criteria, cohortsource, study dates, study country, number of patientsenrolled, baseline patient characteristics, number ofprocedures, method of event determination, eventnumbers, duration of follow-up, risk estimates, andother covariates adjusted for in any multivariatemodels.
STATISTICAL ANALYSIS. Odds ratios (ORs) per unitincrease in BMI were abstracted or calculated fromobservational studies reporting associations betweenBMI and AF. Where risk estimates were reported as a
TABLE 1 Obesity and AF: Cohort Studies
First Author(Ref. #), Year Cohort Source
Dates ofEnrollment Country
Subjects(% Women)
Mean Age(yrs)
Body MassIndex (kg/m2)
Body Mass IndexData Reported
Follow-Up(yrs)
Cases of AF(%) AF Diagnosis Other Covariates in Model
Mean 20.0 175 (1.1%) National hospitalizationand death registries
Age, sex, systolic blood pressure,diabetes, cholesterol, forcedexpiratory volume, smoking,social class
Gami et al.(29), 2007
Mayo Clinic 1987–2003 UnitedStates
3,542 (34%) 49 Mean 33 Continuous Mean 4.7 133 (3.8%) ECG Age, sex, smoking, hypertension,diabetes, ischemic heart disease,heart failure
Rosengren et al.(14), 2009
Swedish PrimaryPreventionStudy
1970–1973 Sweden 6,903 (0%) 52 Mean 22.4 Continuous andcategorical
Maximum34.3
1,253 (18.2%) National hospitalizationregistry
Age, systolic blood pressure,antihypertensive therapy,diabetes, smoking, alcohol,social class
Tedrow et al.(13), 2010
Women’s HealthStudy
1993–2004 UnitedStates
34,309 (100%) 55 16,765 (49%)overweightor obese
Continuous andcategorical
Mean 12.9 834 (2.4%) ECG or medical record Age, ethnicity, hypertension,hypercholesterolemia, diabetes,alcohol consumption, smoking,physical activity, inflammatorymarkers
Smith et al.(30), 2009
Malmo Diet andCancer Study
1991–1996 Sweden 30,447 (60%) 58 Mean 25.8 Continuous andcategorical
Mean 11.2 1,430 (4.7%) National hospitalizationand death registries
AF ¼ atrial fibrillation; ECG ¼ electrocardiogram.
JACC:CLIN
ICAL
ELECTROPHYSIO
LOGY
VOL.1,
NO.3,2015
Wong
etal.
JUNE
2015:1
39–52
Obesity
andAtrial
Fibrillation
141
FIGURE 2 Obesity and AF in Cohort Studies
Relation between 5-U increases in body mass index and atrial fibrillation (AF) from cohort studies. The point estimate (center of each gray
square), statistical size (proportional area of square) and 95% confidence interval (CI) (horizontal line) for estimate of each study are shown.
The overall summary estimate is also shown (blue diamond). AGES ¼ Age, Gene/Environment Susceptibility-Reykjavik Study; CHS ¼ Cardio-
vascular Health Study; OR ¼ odds ratio.
Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
142
series of dose-specific risk estimates compared with areference BMI category, these were transformed intorisk estimates per unit of BMI (12). Authors werecontacted for additional data allowing transformation(e.g., patient and event numbers within BMI cate-gories) where it was not reported in the publication.To assess the validity of this transformation, weplotted the natural logarithm of the AF risk estimatesfor studies that assessed at least 3 different BMIgroups against the assigned BMI dose for this cate-gory, after subtracting a factor b1 � (XAref � 22.5),where XAref is the assigned dose in the referencecategory, as previously described (12). There wassome evidence of deviation, but overall evidence wasof linearity consistent with that described in indi-vidual studies (Online Figure 1) (13,14). If both dose-specific risk estimates compared with a referenceBMI category and risk estimates per unit of BMI werereported, the latter were preferentially used. Asan additional test, we also transformed categoricalBMI risk estimates using the previously mentionedmethod in these studies, and transformed risk esti-mates per unit of BMI were comparable to those re-ported by the investigators. Risk estimates for every
5-U increase in BMI were subsequently calculatedand pooled using random effects meta-analysis (15).Where risk estimates were reported separately by sexor other subgroups only, these were pooled sepa-rately. Risk estimates from multivariate modelsadjusting for potential confounders were used whereavailable. Heterogeneity across studies was assessedusing I2 statistics and, where present, the potentialrole of study characteristics (age, sex, year, geo-graphic region, study numbers, AF diagnosticmethod, follow-up duration, and AF type) exploredvia subgroup analyses and meta-regression tech-niques (16). The presence of publication bias wasassessed using funnel plots of effect size againststandard error. A 2-tailed value of p < 0.05 wasconsidered statistically significant, and all analyseswere performed using SAS version 9.3 (SAS InstituteInc., Cary, North Carolina) and Stata version 12.0(Stata Corp., College Station, Texas).
RESULTS
SEARCH RESULTS. The systematic search of elec-tronic databases identified 2,001 papers, from which
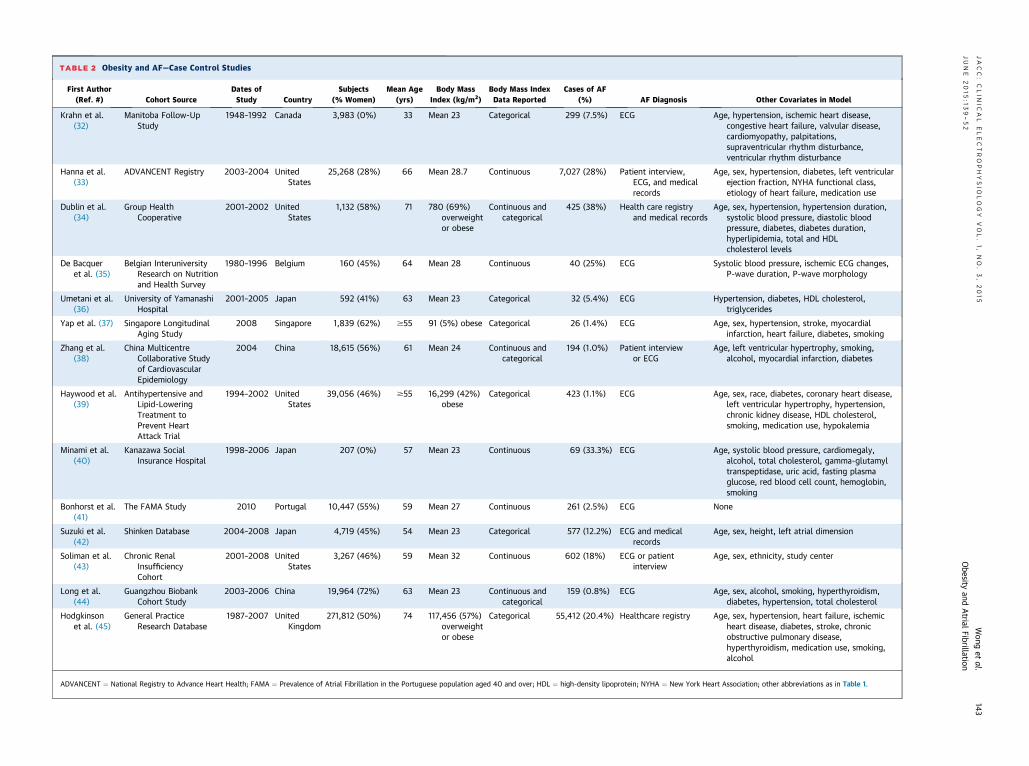
TABLE 2 Obesity and AF—Case Control Studies
First Author(Ref. #) Cohort Source
Dates ofStudy Country
Subjects(% Women)
Mean Age(yrs)
Body MassIndex (kg/m2)
Body Mass IndexData Reported
Cases of AF(%) AF Diagnosis Other Covariates in Model
ADVANCENT ¼ National Registry to Advance Heart Health; FAMA ¼ Prevalence of Atrial Fibrillation in the Portuguese population aged 40 and over; HDL ¼ high-density lipoprotein; NYHA ¼ New York Heart Association; other abbreviations as in Table 1.
JACC:CLIN
ICAL
ELECTROPHYSIO
LOGY
VOL.1,
NO.3,2015
Wong
etal.
JUNE
2015:1
39–52
Obesity
andAtrial
Fibrillation
143
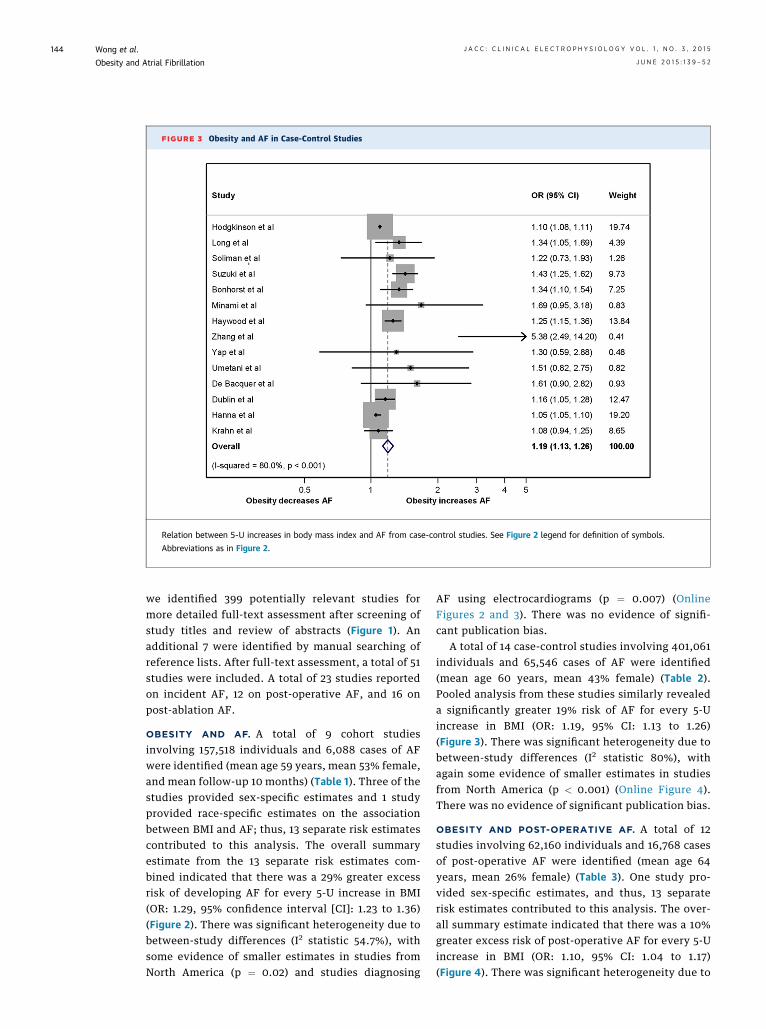
FIGURE 3 Obesity and AF in Case-Control Studies
Relation between 5-U increases in body mass index and AF from case-control studies. See Figure 2 legend for definition of symbols.
Abbreviations as in Figure 2.
Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
144
we identified 399 potentially relevant studies formore detailed full-text assessment after screening ofstudy titles and review of abstracts (Figure 1). Anadditional 7 were identified by manual searching ofreference lists. After full-text assessment, a total of 51studies were included. A total of 23 studies reportedon incident AF, 12 on post-operative AF, and 16 onpost-ablation AF.
OBESITY AND AF. A total of 9 cohort studiesinvolving 157,518 individuals and 6,088 cases of AFwere identified (mean age 59 years, mean 53% female,and mean follow-up 10 months) (Table 1). Three of thestudies provided sex-specific estimates and 1 studyprovided race-specific estimates on the associationbetween BMI and AF; thus, 13 separate risk estimatescontributed to this analysis. The overall summaryestimate from the 13 separate risk estimates com-bined indicated that there was a 29% greater excessrisk of developing AF for every 5-U increase in BMI(OR: 1.29, 95% confidence interval [CI]: 1.23 to 1.36)(Figure 2). There was significant heterogeneity due tobetween-study differences (I2 statistic 54.7%), withsome evidence of smaller estimates in studies fromNorth America (p ¼ 0.02) and studies diagnosing
AF using electrocardiograms (p ¼ 0.007) (OnlineFigures 2 and 3). There was no evidence of signifi-cant publication bias.
A total of 14 case-control studies involving 401,061individuals and 65,546 cases of AF were identified(mean age 60 years, mean 43% female) (Table 2).Pooled analysis from these studies similarly revealeda significantly greater 19% risk of AF for every 5-Uincrease in BMI (OR: 1.19, 95% CI: 1.13 to 1.26)(Figure 3). There was significant heterogeneity due tobetween-study differences (I2 statistic 80%), withagain some evidence of smaller estimates in studiesfrom North America (p < 0.001) (Online Figure 4).There was no evidence of significant publication bias.
OBESITY AND POST-OPERATIVE AF. A total of 12studies involving 62,160 individuals and 16,768 casesof post-operative AF were identified (mean age 64years, mean 26% female) (Table 3). One study pro-vided sex-specific estimates, and thus, 13 separaterisk estimates contributed to this analysis. The over-all summary estimate indicated that there was a 10%greater excess risk of post-operative AF for every 5-Uincrease in BMI (OR: 1.10, 95% CI: 1.04 to 1.17)(Figure 4). There was significant heterogeneity due to
TABLE 3 Obesity and Post-Operative AF
First Author(Ref. #) Dates of Study Country
Subjects(% Women)
Mean Age(yrs)
Body MassIndex (kg/m2)
Body Mass IndexData Reported
Post-OperativeCases of AF (%) AF Diagnosis Other Covariates in Model
Age, sex, ethnicity, obstructive sleep apnea, hypertension, diabetes,family history of coronary artery disease, myocardial infarction,heart failure, ejection fraction, stroke, chronic kidney disease,operation urgency, smoking, hypercholesterolemia, medications,graft number
Tadic et al.(56)
2006–2008 Serbia 322 (28%) 60 Mean 26.2 Categorical 72 (22.4%) Continuousmonitoringor ECG
Age, sex, hypertension, diabetes, hypercholesterolemia, smoking,medications, left atrial diameter, left ventricular kineticdisturbances, triple vessel disease, leukocytosis
CCS ¼ Canadian Cardiovascular Society; N/A ¼ not available; other abbreviations as in Tables 1 and 2.
JACC:CLIN
ICAL
ELECTROPHYSIO
LOGY
VOL.1,
NO.3,2015
Wong
etal.
JUNE
2015:1
39–52
Obesity
andAtrial
Fibrillation
145
FIGURE 4 Obesity and Post-Operative AF
Relation between 5-U increases in body mass index and post-operative AF. See Figure 2 legend for definition of symbols. Abbreviations as in
Figure 2.
Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
146
between-study differences (I2 statistic 82.9%), withsome evidence of larger estimates in studies fromAsia (p ¼ 0.003) and in studies diagnosing AF withcontinuous monitoring or electrocardiograms (p ¼0.045) (Online Figures 5 and 6). There was no evi-dence of significant publication bias.
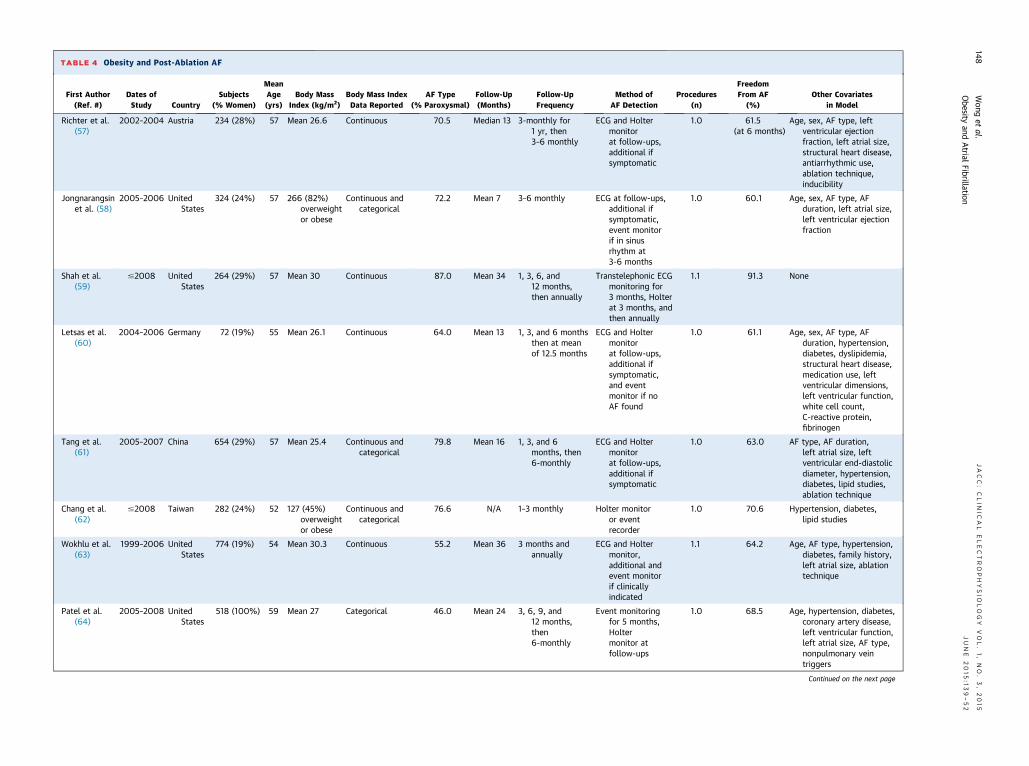
OBESITY AND POST-ABLATION AF. A total of 16studies involving 5,864 individuals were included(mean age 56 years, mean 30% female, mean follow-up 20 months) (Table 4). The overall summary esti-mate indicated that there was a 13% greater excessrisk of recurrent AF post-ablation for every 5-Uincrease in BMI (OR: 1.13, 95% CI: 1.06 to 1.22)(Figure 5). There was significant heterogeneity due todifferences between studies (I2 statistic 78.6%),although exploratory analyses could not identifyany significant contributing factors. There was noevidence of significant publication bias.
DISCUSSION
MAJOR FINDINGS. The present meta-analysis pooleddata from 51 studies and more than 600,000 in-dividuals in a range of clinical settings. For every 5-U
increase in BMI, there were 10% to 29% greater excessrisks of incident, post-operative, and post-ablationAF. These findings provide a comprehensive quanti-fication of the relationship between incremental in-creases in obesity and the risk of AF in these differentclinical settings.
THE EPIDEMIC OF AF. AF is increasingly recognizedas a major public health burden. The worldwideprevalence of AF is already estimated at 33 million,and this is possibly a significant underestimate of thetrue figure given the likelihood of study methodo-logical limitations and under-diagnosis (17,18). Theannual incremental cost of AF is estimated at $26billion in the United States alone, and hospitaliza-tions, the major driver of cost, appear to be increasingmore rapidly than other cardiovascular conditions(2,17). Given that the risk of AF increases rapidly withgreater age, an already rising prevalence is expectedto further accelerate given aging population struc-tures. Studies suggest, however, that the age-specificincidence of AF is increasing in addition to anyeffect from population aging (19). It is likely that theepidemiologic transition in both developed anddeveloping countries toward increased longevity and
FIGURE 5 Obesity and Post-Ablation AF
Relation between 5-U increases in body mass index and post-ablation atrial fibrillation. See Figure 2 legend for definition of symbols.
Abbreviations as in Figure 2.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5 Wong et al.J U N E 2 0 1 5 : 1 3 9 – 5 2 Obesity and Atrial Fibrillation
147
unhealthy lifestyles is resulting in an increasingprevalence and multiplicative effect of AF risk factors(4). A greater focus on and effort to reduce these riskfactors is thus required to prevent the initial devel-opment and the subsequent burden of AF (20).OBESITY AND AF. Obesity is an important contrib-utor to the burden of AF, explaining one-fifth of all AFcases (21). It has also been estimated that obesity mayaccount for approximately 60% of the rising age- andsex-adjusted incidence of AF (1). From a public healthperspective, obesity is, therefore, a modifiable riskfactor that could be profitably targeted. Moreover,dietary and lifestyle improvements addressingobesity would also favorably affect other AF riskfactors, such as hypertension and diabetes, reducingthe burden of AF greater than that attributable toobesity alone. We and other investigators have pre-viously shown that obesity is associated with dele-terious electrical, structural, and hemodynamicabnormalities in the left atria, predisposing to AF(22,23). More recently, we described how a weightand risk factor management program can improve
such cardiac remodeling and subsequent arrhythmiaburden in people with AF (24,25).
Although previous analyses have studied theobesity-related risk of AF in different clinical set-tings individually, the present report provides themost comprehensive summary estimates to date(7–9). Key differences compared with prior studiesinclude the greater power of our meta-analysis(51 studies, n ¼ 626,603), the inclusion of studiesreporting risk estimates with either BMI as a cate-gorical or continuous variable, and the comparisonof obesity-related risk across different clinical set-tings (7–9). Our results suggest that there is a 10% to29% excess risk of AF associated with every 5-U in-crease in BMI in the general population, after cardiacsurgery, and after catheter ablation procedures. Theconsistency of obesity-related risk across thesedifferent settings lends further weight to the reli-ability of obesity as an AF risk factor. Thus, evenmoderate reductions in population body mass in-dexes are likely to have a significant effect on thepublic health burden of AF.
TABLE 4 Obesity and Post-Ablation AF
First Author(Ref. #)
Dates ofStudy Country
Subjects(% Women)
MeanAge(yrs)
Body MassIndex (kg/m2)
Body Mass IndexData Reported
AF Type(% Paroxysmal)
Follow-Up(Months)
Follow-UpFrequency
Method ofAF Detection
Procedures(n)
FreedomFrom AF
(%)Other Covariates
in Model
Richter et al.(57)
2002–2004 Austria 234 (28%) 57 Mean 26.6 Continuous 70.5 Median 13 3-monthly for1 yr, then3–6 monthly
ECG and Holtermonitorat follow-ups,additional ifsymptomatic
1.0 61.5(at 6 months)
Age, sex, AF type, leftventricular ejectionfraction, left atrial size,structural heart disease,antiarrhythmic use,ablation technique,inducibility
Jongnarangsinet al. (58)
2005–2006 UnitedStates
324 (24%) 57 266 (82%)overweightor obese
Continuous andcategorical
72.2 Mean 7 3–6 monthly ECG at follow-ups,additional ifsymptomatic,event monitorif in sinusrhythm at3-6 months
1.0 60.1 Age, sex, AF type, AFduration, left atrial size,left ventricular ejectionfraction
Shah et al.(59)
#2008 UnitedStates
264 (29%) 57 Mean 30 Continuous 87.0 Mean 34 1, 3, 6, and12 months,then annually
94 (20%) 59 Mean 25.0 Categorical 0.0 Mean 20 1, 3, 6, and12 months
ECG and Holtermonitor
1.0 66.0 Age, sex, AF type, AFduration, hypertension,diabetes, left atrialdiameter, leftventricular ejectionfraction
Letsas et al.(70)
#2011 Germany 226 (19%) 56 Mean 26.6 Continuous 59.3 Mean 14 3 and 6 months,then at meanof 14 months
Holter monitor 1.0 58.0 None
Ejima et al.(71)
#2011 Japan 80 (19%) 58 Mean 24 Continuous 81.3 Median 17 1, 2, 3, 6, 9, and12 months, then6-monthly
ECG and Holtermonitor
1.1 90.0 None
Abbreviations as in Table 1.
JACC:CLIN
ICAL
ELECTROPHYSIO
LOGY
VOL.1,
NO.3,2015
Wong
etal.
JUNE
2015:1
39–52
Obesity
andAtrial
Fibrillation
149
PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE:
Incremental increases in obesity are associated with
incident, post-operative, and post-ablation AF. For
every 5-U increase in BMI, there is a 10% to 29%
greater risk of AF in these clinical settings.
TRANSLATIONAL OUTLOOK: Given the associa-
tion between obesity and AF, further studies are
warranted to characterize the effect that weight
reduction may have not only in preventing incident
AF, but also in managing patients with established AF.
Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
150
STUDY LIMITATIONS. The overall summary esti-mates obtained in these analyses may be over-estimates due to coexistent confounding factors.Although most studies are adjusted for other co-morbid AF risk factors, it is not possible to fully takeinto account the possible effect on the observed as-sociations. However, overall summary estimates mayalso be underestimates due to the underdiagnosis ofAF in some included studies, the magnitude of whichhas only recently become apparent with increasinglysensitive diagnostic modalities. Significant hetero-geneity was also observed in the present analysesdue to between-study differences. Subgroup analysesand meta-regression techniques suggested that thismay in part be due to differing study populationcharacteristics (such as geographic region) and diag-nostic methods of ascertaining AF. Despite this het-erogeneity, however, our findings appeared to beconsistent across a broad range of clinical settings,and thus they provide the most comprehensiveanalysis so far with regard to the obesity-relatedrisk of AF.
CONCLUSIONS
Incremental increases in BMI are associated witha significant excess risk of AF in different clinicalsettings. For every 5-U increase in BMI, there were10% to 29% greater excess risks of incident, post-
operative, and post-ablation AF. Given that bur-geoning rates of obesity are likely to have anincreasing effect on an already rising burden of AF,these data suggest that achieving even moderatereductions in body mass indexes is likely to havesignificant clinical and public health impact.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Prashanthan Sanders, Centre for Heart Rhythm Dis-orders, Department of Cardiology, Royal AdelaideHospital, Adelaide SA 5000, Australia. E-mail: [email protected].
RE F E RENCE S
1. Miyasaka Y, Barnes ME, Gersh BJ, et al. Seculartrends in incidence of atrial fibrillation in OlmstedCounty, Minnesota, 1980 to 2000, and implica-tions on the projections for future prevalence.Circulation 2006;114:119–25.
2. Wong CX, Brooks AG, Leong DP, Roberts-Thomson KC, Sanders P. The increasing burden ofatrial fibrillation compared to heart failure andmyocardial infarction: a 15-year study of all hos-pitalizations in Australia. Arch Intern Med 2012;172:739–41.
3. Wong CX, Lau DH, Sanders P. Atrial fibrillationepidemic and hospitalizations: how to turn therising tide? Circulation 2014;129:2361–3.
4. Gaziano JM. Fifth phase of the epidemiologictransition: the age of obesity and inactivity. JAMA2010;303:275–6.
5. Balkau B, Deanfield JE, Despres JP, et al.International Day for the Evaluation of AbdominalObesity (IDEA): a study of waist circumference,cardiovascular disease, and diabetes mellitus in168,000 primary care patients in 63 countries.Circulation 2007;116:1942–51.
6. Wong CX, Abed HS, Molaee P, et al. Pericardialfat is associated with atrial fibrillation severity andablation outcome. J Am Coll Cardiol 2011;57:1745–51.
7. Wanahita N, Messerli FH, Bangalore S, Gami AS,Somers VK, Steinberg JS. Atrial fibrillation andobesity—results of a meta-analysis. Am Heart J2008;155:310–5.
8. Guijian L, Jinchuan Y, Rongzeng D, Jun Q,Jun W, Wenqing Z. Impact of body mass index onatrial fibrillation recurrence: a meta-analysis ofobservational studies. Pacing Clin Electrophysiol2013;36:748–56.
9. Zhuang J, Lu Y, Tang K, Peng W, Xu Y. Influenceof body mass index on recurrence and quality oflife in atrial fibrillation patients after catheterablation: a meta-analysis and systematic review.Clin Cardiol 2013;36:269–75.
10. Reeves BC, Ascione R, Chamberlain MH,Angelini GD. Effect of body mass index on earlyoutcomes in patients undergoing coronary arterybypass surgery. J Am Coll Cardiol 2003;42:668–76.
11. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis Of Observational Studies in Epidemiology(MOOSE) Group. Meta-analysis of observationalstudies in epidemiology: a proposal for reporting.JAMA 2000;283:2008–12.
12. Hartemink N, Boshuizen HC, Nagelkerke NJ,Jacobs MA, van Houwelingen HC. Combiningrisk estimates from observational studies with
different exposure cutpoints: a meta-analysis onbody mass index and diabetes type 2. Am J Epi-demiol 2006;163:1042–52.
13. Tedrow UB, Conen D, Ridker PM, et al. Thelong- and short-term impact of elevated bodymass index on the risk of new atrial fibrillation theWHS (Women’s Health Study). J Am Coll Cardiol2010;55:2319–27.
14. Rosengren A, Hauptman PJ, Lappas G,Olsson L, Wilhelmsen L, Swedberg K. Big men andatrial fibrillation: effects of body size and weightgain on risk of atrial fibrillation in men. Eur Heart J2009;30:1113–20.
15. DerSimonian R, Laird N. Meta-analysis inclinical trials. Control Clin Trials 1986;7:177–88.
16. Higgins JP, Thompson SG. Quantifying het-erogeneity in a meta-analysis. Stat Med 2002;21:1539–58.
17. Rahman F, Kwan GF, Benjamin EJ. Globalepidemiology of atrial fibrillation. Nat Rev Cardiol2014;11:639–54.
18. Fitzmaurice DA, Hobbs FD, Jowett S, et al.Screening versus routine practice in detection ofatrial fibrillation in patients aged 65 or over:cluster randomised controlled trial. BMJ 2007;335:383.
J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5 Wong et al.J U N E 2 0 1 5 : 1 3 9 – 5 2 Obesity and Atrial Fibrillation
151
19. Wong CX, Brooks AG, Lau DH, et al. Factorsassociated with the epidemic of hospitalizationsdue to atrial fibrillation. Am J Cardiol 2012;110:1496–9.
20. Benjamin EJ, Chen PS, Bild DE, et al. Preven-tion of atrial fibrillation: report from a NationalHeart, Lung, and Blood Institute workshop. Cir-culation 2009;119:606–18.
21. Huxley RR, Lopez FL, Folsom AR, et al. Abso-lute and attributable risks of atrial fibrillation inrelation to optimal and borderline risk factors: theAtherosclerosis Risk in Communities (ARIC) study.Circulation 2011;123:1501–8.
22. Abed HS, Samuel CS, Lau DH, et al. Obesityresults in progressive atrial structural and elec-trical remodeling: implications for atrial fibrilla-tion. Heart Rhythm 2013;10:90–100.
23. Munger TM, Dong YX, Masaki M, et al. Elec-trophysiological and hemodynamic characteristicsassociated with obesity in patients with atrialfibrillation. J Am Coll Cardiol 2012;60:851–60.
24. Abed HS, Wittert GA, Leong DP, et al. Effect ofweight reduction and cardiometabolic risk factormanagement on symptom burden and severity inpatients with atrial fibrillation: a randomizedclinical trial. JAMA 2013;310:2050–60.
25. Pathak RK, Middeldorp ME, Lau DH, et al.Aggressive risk factor reduction study for atrialfibrillation and implications for the outcome ofablation: the ARREST-AF cohort study. J Am CollCardiol 2014;64:2222–31.
26. Wang TJ, Parise H, Levy D, et al. Obesity andthe risk of new-onset atrial fibrillation. JAMA2004;292:2471–7.
27. Frost L, Hune LJ, Vestergaard P. Overweightand obesity as risk factors for atrial fibrillation orflutter: the Danish Diet, Cancer, and Health Study.Am J Med 2005;118:489–95.
28. Murphy NF, MacIntyre K, Stewart S, Hart CL,Hole D, McMurray JJ. Long-term cardiovascularconsequences of obesity: 20-year follow-up ofmore than 15 000 middle-aged men and women(the Renfrew-Paisley study). Eur Heart J 2006;27:96–106.
29. Gami AS, Hodge DO, Herges RM, et al.Obstructive sleep apnea, obesity, and the risk ofincident atrial fibrillation. J Am Coll Cardiol 2007;49:565–71.
30. Smith JG, Platonov PG, Hedblad B,Engstrom G, Melander O. Atrial fibrillation in theMalmo Diet and Cancer study: a study of occur-rence, risk factors and diagnostic validity. Euro-pean journal of epidemiology 2010;25:95–102.
31. Schnabel RB, Aspelund T, Li G, et al. Validationof an atrial fibrillation risk algorithm in whites andAfrican Americans. Arch Intern Med 2010;170:1909–17.
32. Krahn AD, Manfreda J, Tate RB, Mathewson FA,Cuddy TE. The natural history of atrial fibrillation:incidence, risk factors, and prognosis in theManitoba Follow-Up Study. Am J Med 1995;98:476–84.
33. Hanna IR, Heeke B, Bush H, et al. The rela-tionship between stature and the prevalence ofatrial fibrillation in patients with left ventriculardysfunction. J Am Coll Cardiol 2006;47:1683–8.
34. Dublin S, French B, Glazer NL, et al. Risk ofnew-onset atrial fibrillation in relation to bodymass index. Arch Intern Med 2006;166:2322–8.
35. De Bacquer D, Willekens J, De Backer G. Long-term prognostic value of p-wave characteristicsfor the development of atrial fibrillation in sub-jects aged 55 to 74 years at baseline. Am J Cardiol2007;100:850–4.
36. Umetani K, Kodama Y, Nakamura T, et al. Highprevalence of paroxysmal atrial fibrillation and/oratrial flutter in metabolic syndrome. Circ J 2007;71:252–5.
37. Yap KB, Ng TP, Ong HY. Low prevalence ofatrial fibrillation in community-dwelling Chineseaged 55 years or older in Singapore: a population-based study. J Electrocardiol 2008;41:94–8.
38. Zhang X, Zhang S, Li Y, et al. Association ofobesity and atrial fibrillation among middle-agedand elderly Chinese. Int J Obes (Lond) 2009;33:1318–25.
39. Haywood LJ, Ford CE, Crow RS, et al. Atrialfibrillation at baseline and during follow-up inALLHAT (Antihypertensive and Lipid-LoweringTreatment to Prevent Heart Attack Trial). J AmColl Cardiol 2009;54:2023–31.
40. Minami M, Kobayashi Y, Toyokawa S, Inoue K,Takeshita Y. Risk factors for new-onset atrialfibrillation during routine medical checkups ofJapanese male workers. Int Heart J 2009;50:457–64.
41. Bonhorst D, Mendes M, Adragao P, et al.Prevalence of atrial fibrillation in the Portuguesepopulation aged 40 and over: the FAMA study.Rev Port Cardiol 2010;29:331–50.
42. Suzuki S, Yamashita T, Ohtsuka T, et al. Bodysize and atrial fibrillation in Japanese outpatients.Circ J 2010;74:66–70.
43. Soliman EZ, Prineas RJ, Go AS, et al. Chronickidney disease and prevalent atrial fibrillation: theChronic Renal Insufficiency Cohort (CRIC). AmHeart J 2010;159:1102–7.
44. Long MJ, Jiang CQ, Lam TH, et al. Atrialfibrillation and obesity among older Chinese: theGuangzhou Biobank Cohort Study. Int J Cardiol2011;148:48–52.
45. Hodgkinson JA, Taylor CJ, Hobbs FD. Pre-dictors of incident atrial fibrillation and influenceof medications: a retrospective case-control study.Br J Gen Pract 2011;61:e353–61.
46. Moulton MJ, Creswell LL, Mackey ME, Cox JL,Rosenbloom M. Obesity is not a risk factor forsignificant adverse outcomes after cardiac surgery.Circulation 1996;94:II87–92.
47. Engelman DT, Adams DH, Byrne JG, et al.Impact of body mass index and albumin onmorbidity and mortality after cardiac surgery.J Thorac Cardiovasc Surg 1999;118:866–73.
48. Brandt M, Harder K, Walluscheck KP, et al.Severe obesity does not adversely affect periop-erative mortality and morbidity in coronary arterybypass surgery. Eur J Cardiothorac Surg 2001;19:662–6.
49. Zacharias A, Schwann TA, Riordan CJ,Durham SJ, Shah AS, Habib RH. Obesity and risk ofnew-onset atrial fibrillation after cardiac surgery.Circulation 2005;112:3247–55.
50. Yap CH, Zimmet A, Mohajeri M, Yii M. Effect ofobesity on early morbidity and mortality followingcardiac surgery. Heart Lung Circ 2007;16:31–6.
51. Girerd N, Pibarot P, Fournier D, et al. Middle-aged men with increased waist circumference andelevated C-reactive protein level are at higher riskfor postoperative atrial fibrillation following cor-onary artery bypass grafting surgery. Eur Heart J2009;30:1270–8.
52. Alam M, Siddiqui S, Lee VV, et al. Isolated cor-onary artery bypass grafting in obese individuals: apropensity matched analysis of outcomes. Circ J2011;75:1378–85.
53. Bramer S, van Straten AH, Soliman Hamad MA,Berreklouw E, van den Broek KC, Maessen JG.Body mass index predicts new-onset atrial fibril-lation after cardiac surgery. Eur J CardiothoracSurg 2011;40:1185–90.
54. Melduni RM, Suri RM, Seward JB, et al. Dia-stolic dysfunction in patients undergoing cardiacsurgery: a pathophysiological mechanism under-lying the initiation of new-onset post-operativeatrial fibrillation. J Am Coll Cardiol 2011;58:953–61.
55. Sun X, Boyce SW, Hill PC, et al. Association ofbody mass index with new-onset atrial fibrillationafter coronary artery bypass grafting operations.Ann Thorac Surg 2011;91:1852–8.
56. Tadic M, Ivanovic B, Zivkovic N. Predictors ofatrial fibrillation following coronary artery bypasssurgery. Med Sci Monit 2011;17:CR48–55.
57. Richter B, Gwechenberger M, Filzmoser P,Marx M, Lercher P, Gossinger HD. Is inducibility ofatrial fibrillation after radio frequency ablationreally a relevant prognostic factor? Eur Heart J2006;27:2553–9.
58. Jongnarangsin K, Chugh A, Good E, et al. Bodymass index, obstructive sleep apnea, and out-comes of catheter ablation of atrial fibrillation.J Cardiovasc Electrophysiol 2008;19:668–72.
59. Shah AN, Mittal S, Sichrovsky TC, et al. Long-term outcome following successful pulmonaryvein isolation: pattern and prediction of very laterecurrence. J Cardiovasc Electrophysiol 2008;19:661–7.
60. Letsas KP, Weber R, Burkle G, et al. Pre-ablative predictors of atrial fibrillation recurrencefollowing pulmonary vein isolation: the potentialrole of inflammation. Europace 2009;11:158–63.
61. Tang RB, Dong JZ, Liu XP, et al. Metabolicsyndrome and risk of recurrence of atrial fibrilla-tion after catheter ablation. Circ J 2009;73:438–43.
62. Chang SL, Tuan TC, Tai CT, et al. Comparisonof outcome in catheter ablation of atrial fibrillationin patients with versus without the metabolicsyndrome. Am J Cardiol 2009;103:67–72.
63. Wokhlu A, Hodge DO, Monahan KH, et al.Long-term outcome of atrial fibrillation ablation:impact and predictors of very late recurrence.J Cardiovasc Electrophysiol 2010;21:1071–8.
64. Patel D, Mohanty P, Di Biase L, et al. Out-comes and complications of catheter ablation foratrial fibrillation in females. Heart Rhythm 2010;7:167–72.
Wong et al. J A C C : C L I N I C A L E L E C T R O P H Y S I O L O G Y V O L . 1 , N O . 3 , 2 0 1 5
Obesity and Atrial Fibrillation J U N E 2 0 1 5 : 1 3 9 – 5 2
152
65. Jin Hwang H, Myung Lee J, Joung B, et al.Atrial electroanatomical remodeling as a determi-nant of different outcomes between two currentablation strategies: circumferential pulmonaryvein isolation vs pulmonary vein isolation. ClinCardiol 2010;33:E69–74.
66. Winkle RA, Mead RH, Engel G, Patrawala RA.Relation of early termination of persistent atrialfibrillation by cardioversion or drugs to ablationoutcomes. Am J Cardiol 2011;108:374–9.
67. Chao TF, Lin YJ, Chang SL, et al. Associationsbetween renal function, atrial substrate propertiesand outcome of catheter ablation in patients withparoxysmalatrialfibrillation.Circ J2011;75:2326–32.
68. Mohanty S, Mohanty P, Di Biase L, et al.Impact of metabolic syndrome on proceduraloutcomes in patients with atrial fibrillation un-dergoing catheter ablation. J Am Coll Cardiol2012;59:1295–301.
69. Kang JH, Lee DI, Kim S, et al. Prediction oflong-term outcomes of catheter ablation ofpersistent atrial fibrillation by parameters of pre-ablation DC cardioversion. J Cardiovasc Electro-physiol 2012;23:1165–70.
70. Letsas KP, Siklody CH, Korantzopoulos P, et al.The impact of body mass index on the efficacy andsafety of catheter ablation of atrial fibrillation. IntJ Cardiol 2013;164:94–8.
71. Ejima K, Shoda M, Arai K, et al. Impact of dia-stolic dysfunction on the outcome of catheterablation in patients with atrial fibrillation. Int JCardiol 2013;164:88–93.
KEY WORDS atrial fibrillation, body massindex, cardiac surgery, catheter ablation,obesity, substrate, weight reduction
APPENDIX For supplemental figures, pleasesee the online version of this article.