UMC Health System Patient Label Here OB/GYN INTRAPARTUM PLAN PHYSICIAN ORDERS Weight ____________________________________________ Allergies ________________________________________________________ Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable. ORDER ORDER DETAILS Admit/Discharge/Transfer Patient Status Pt Status: Inpatient (LOS > 2 midnights) Pt Status: Observation (LOS < 2 midnights) Patient Care Vital Signs Per Unit Standards Per Unit Standards, BP every 15 minutes in left lateral position. Per Unit Standards, Check BP in left lateral, right lateral, sitting , standing, and supine positions. Patient Activity Up Ad Lib/Activity as Tolerated Bedrest, Instruct patient on importance of lateral position and to change position at least every 2 hours. Bedrest | Up to Bedside Commode Only Bedrest | Bathroom Privileges Ambulate Patient after 20 min reactive NST. Insert Peripheral Line Insert Urinary Catheter Foley, To: Dependent Drainage Bag Strict Intake and Output Per Unit Standards POC Urinalysis Dipstick w/o Microscopy After each void. On Admission Monitoring Fetal Monitoring Continuous External Fetal Monitor External Fetal Monitor as needed. Internal Scalp Monitor Notify Provider (Misc) Reason: Non-reassuring fetal heart pattern or hyperstimulation noted. Communication Notify Nurse (DO NOT USE FOR MEDS) Limit pelvic exams once rupture of membranes occurs. Notify Provider (Misc) Reason: Before performing pelvic exams on ALL TTUHSC patients. Notify Provider of VS Parameters Temp Greater Than 100.4, SBP Greater Than 140, DBP Greater Than 90 Dietary TO Read Back Scanned Powerchart Scanned PharmScan Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________ Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________ Page: 1 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15 1201 Diagnosis__________________________________ Page 1 of 10
Vital Signs Per Unit Standards Per Unit Standards, BP every 15 minutes in left lateral position. Per Unit Standards, Check BP in left lateral, right lateral, sitting , standing, and supine positions.
Patient Activity Up Ad Lib/Activity as Tolerated Bedrest, Instruct patient on importance of lateral position and to change position at least every 2 hours. Bedrest | Up to Bedside Commode Only Bedrest | Bathroom Privileges
Ambulate Patient after 20 min reactive NST.
Insert Peripheral Line
Insert Urinary Catheter Foley, To: Dependent Drainage Bag
Strict Intake and Output Per Unit Standards
POC Urinalysis Dipstick w/o Microscopy After each void. On Admission
Notify Nurse (DO NOT USE FOR MEDS) Limit pelvic exams once rupture of membranes occurs.
Notify Provider (Misc) Reason: Before performing pelvic exams on ALL TTUHSC patients.
Notify Provider of VS Parameters Temp Greater Than 100.4, SBP Greater Than 140, DBP Greater Than 90
Dietary
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 1 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Diagnosis__________________________________
Page 1 of 10
UMC Health System Patient Label Here
OB/GYN INTRAPARTUM PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
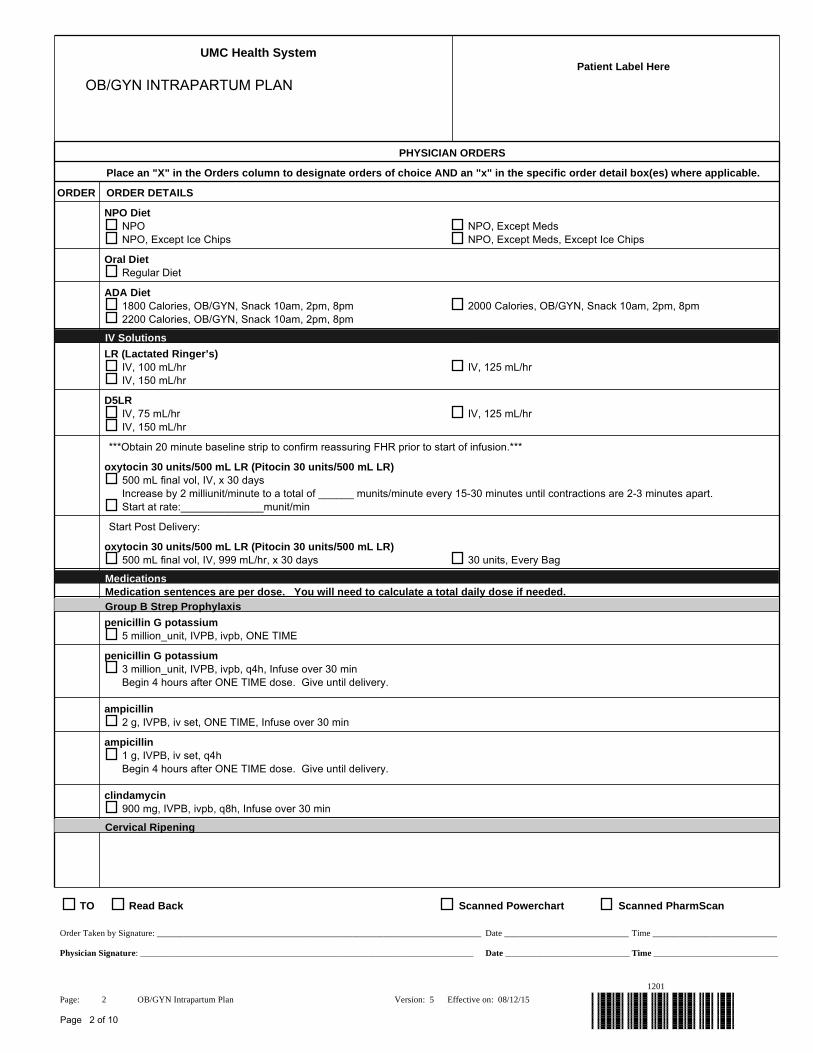
LR (Lactated Ringer’s) IV, 100 mL/hr IV, 125 mL/hr IV, 150 mL/hr
D5LR IV, 75 mL/hr IV, 125 mL/hr IV, 150 mL/hr
***Obtain 20 minute baseline strip to confirm reassuring FHR prior to start of infusion.***
oxytocin 30 units/500 mL LR (Pitocin 30 units/500 mL LR) 500 mL final vol, IV, x 30 days Increase by 2 milliunit/minute to a total of ______ munits/minute every 15-30 minutes until contractions are 2-3 minutes apart. Start at rate:______________munit/min
Start Post Delivery:
oxytocin 30 units/500 mL LR (Pitocin 30 units/500 mL LR) 500 mL final vol, IV, 999 mL/hr, x 30 days 30 units, Every Bag
MedicationsMedication sentences are per dose. You will need to calculate a total daily dose if needed.
Group B Strep Prophylaxis
penicillin G potassium 5 million_unit, IVPB, ivpb, ONE TIME
penicillin G potassium 3 million_unit, IVPB, ivpb, q4h, Infuse over 30 min Begin 4 hours after ONE TIME dose. Give until delivery.
ampicillin 2 g, IVPB, iv set, ONE TIME, Infuse over 30 min
ampicillin 1 g, IVPB, iv set, q4h Begin 4 hours after ONE TIME dose. Give until delivery.
clindamycin 900 mg, IVPB, ivpb, q8h, Infuse over 30 min
Cervical Ripening
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 2 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 2 of 10
UMC Health System Patient Label Here
OB/GYN INTRAPARTUM PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
dinoprostone topical (dinoprostone 10 mg vaginal insert) 10 mg, intra-vaginal, insert, ONE TIME
misoprostol 25 mcg, intra-vaginal, tab, q3h Notify physician once the Bishop score is greater or equal to 6. 25 mcg, intra-vaginal, tab, q4h Notify physician once the Bishop score is greater or equal to 6.
Pain Management
butorphanol 1 mg, IVPush, inj, q1h, PRN pain
meperidine 50 mg, IVPush, inj, q6h, PRN pain Meperidine is only approved for pain in OB/GYN patients. It may be used for drug rigors throughout the hospital. The physician must be contacted if it is being prescribed outside of these approved uses. 25 mg, IVPush, inj, q6h, PRN pain Meperidine is only approved for pain in OB/GYN patients. It may be used for drug rigors throughout the hospital. The physician must be contacted if it is being prescribed outside of these approved uses. 50 mg, IVPush, inj, q2h, PRN pain Meperidine is only approved for pain in OB/GYN patients. It may be used for drug rigors throughout the hospital. The physician must be contacted if it is being prescribed outside of these approved uses. 25 mg, IVPush, inj, q2h, PRN pain Meperidine is only approved for pain in OB/GYN patients. It may be used for drug rigors throughout the hospital. The physician must be contacted if it is being prescribed outside of these approved uses.
promethazine 12.5 mg, Slow IVPush, inj, q6h, PRN nausea/vomiting ***VESICANT*** Dilute with 10 ml NS & IVP over 5 min through a running IV line with large-bore access.
Other Medications
mineral oil 30 mL, topical, liq, as needed, PRN to assist with delivery
sodium biphosphate-sodium phosphate (Fleet Enema) 132 mL, rectally, enema, as needed, PRN to assist with delivery
Soap Suds Enema prior to delivery
Laboratory
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 3 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 3 of 10
UMC Health System Patient Label Here
OB/GYN INTRAPARTUM PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
CBC Routine STAT Next Day in AM,
CBC with Differential Routine STAT Next Day in AM
Prothrombin Time with INR Routine STAT Next Day in AM
PTT Routine STAT Next Day in AM
Comprehensive Metabolic Panel Routine STAT Next Day in AM
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 4 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 4 of 10
UMC Health System Patient Label Here
TYPE AND SCREEN PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
Laboratory
BB Blood Type (ABO/Rh)
BB Antibody Screen
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 5 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 5 of 10
UMC Health System Patient Label Here
TYPE AND CROSS 2 UNITS PRBC FOR PRE-OP
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
Laboratory
BB Blood Type (ABO/Rh)
BB Antibody Screen
BB Clot to Hold
BB PRBCs for Pre-Op Priority: On Hold, Quantity: 2
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 6 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 6 of 10
UMC Health System Patient Label Here
DISCOMFORT MED PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
Patient Care
Perform Bladder Scan Scan PRN, If more than 250, Then: Call MD, Perform as needed for patients complaining of urinary discomfort and/or bladder distention present OR 6 hrs post Foley removal and patient has not voided.
MedicationsMedication sentences are per dose. You will need to calculate a total daily dose if needed.
phenol-menthol topical (phenol-menthol 2.9%-0.12% (Cepastat) lozenge) 1 lozenge, PO, lozenge, q4h, PRN sore throat Do not exceed 6 lozenges in 24 hours
acetaminophen 500 mg, PO, tab, q6h, PRN pain-mild (scale 1-3) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen ineffective/contraindicated, USE ibuprofen if ordered:***** 1,000 mg, PO, tab, q4h, PRN pain-mild (scale 1-3) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen ineffective/contraindicated, USE ibuprofen if ordered:*****
acetaminophen 650 mg, rectally, supp, q4h, PRN pain-mild (scale 1-3) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****If acetaminophen ineffective/contraindicated, USE ibuprofen if ordered:*****
ibuprofen 400 mg, PO, tab, q6h, PRN pain-mild (scale 1-3) ***Do not exceed 3,200 mg of ibuprofen from all sources in 24 hours*** Give with food. Use if acetaminophen ineffective or contraindicated.
HYDROcodone-acetaminophen (HYDROcodone-acetaminophen 5 mg-325 mg oral tablet) 1 tab, PO, tab, q4h, PRN pain-moderate (scale 4-7) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF HYDROcodone-acetaminophen ineffective/contraindicated or NPO, USE ketorolac if ordered***** 2 tab, PO, tab, q4h, PRN pain-moderate (scale 4-7) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF HYDROcodone-acetaminophen ineffective/contraindicated or NPO, USE ketorolac if ordered*****
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 7 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 7 of 10
UMC Health System Patient Label Here
DISCOMFORT MED PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
acetaminophen-codeine (acetaminophen-codeine #3) 1 tab, PO, q4h, PRN pain-moderate (scale 4-7) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen-codeine #3 ineffective/contraindicated or NPO, USE ketorolac if ordered***** 2 tab, PO, q4h, PRN pain-moderate (scale 4-7) ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen-codeine #3 ineffective/contraindicated or NPO, USE ketorolac if ordered*****
ketorolac 15 mg, IVPush, inj, q6h, PRN pain-moderate (scale 4-7), x 48 hr ***May give IM if no IV access*** Use if HYDROcodone-acetaminophen ineffective or contraindicated. 30 mg, IVPush, inj, q6h, PRN pain-moderate (scale 4-7), x 48 hr ***May give IM if no IV access*** Use if HYDROcodone-acetaminophen ineffective or contraindicated.
morphine 2 mg, IVPush, inj, q4h, PRN pain-severe (scale 8-10) ***Slow IV Push*** *****IF morphine is ineffective/contraindicated, USE HYDROmorphone if ordered***** 4 mg, IVPush, inj, q4h, PRN pain-severe (scale 8-10) ***Slow IV Push*** *****IF morphine is ineffective/contraindicated, USE HYDROmorphone if ordered*****
HYDROmorphone 1 mg, IVPush, inj, q4h, PRN pain-severe (scale 8-10) ***Slow IV Push*** Use if morphine ineffective or contraindicated.
Antiemetics
promethazine 25 mg, PO, tab, q4h, PRN nausea/vomiting *****IF promethazine is ineffective/contraindicated or patient is NPO, USE ondansetron if ordered*****
ondansetron 4 mg, IVPush, soln, q8h, PRN nausea/vomiting Use if promethazine ineffective or contraindicated.
Gastrointestinal Agents
docusate 100 mg, PO, cap, Nightly, PRN constipation *****IF docusate is contraindicated or ineffective after 12 hours, USE bisacodyl if ordered*****
bisacodyl 10 mg, rectally, supp, Daily, PRN constipation *****IF bisacodyl is contraindicated or ineffective after 6 hours, USE Fleet Enema if ordered*****
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 8 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 8 of 10
UMC Health System Patient Label Here
DISCOMFORT MED PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
loperamide 4 mg, PO, cap, ONE TIME, PRN diarrhea Initial dose after first loose stool 4 mg, PO, liq, ONE TIME, PRN diarrhea Initial dose after first loose stool
loperamide 2 mg, PO, cap, as needed, PRN diarrhea 2 mg after each loose stool, up to 16 mg per day 2 mg, PO, liq, as needed, PRN diarrhea 2 mg after each loose stool, up to 16 mg per day
Antacids
Al hydroxide-Mg hydroxide-simethicone (aluminum hydroxide-magnesium hydroxide-simethicone 200 mg-200 mg-20 mg/5 mL oral suspension) 30 mL, PO, susp, q4h, PRN indigestion Administer 1 hour before meals and nightly.
simethicone 80 mg, PO, tab chew, q4h, PRN gas 160 mg, PO, tab chew, q4h, PRN gas
Sedatives
ALPRAZolam 0.25 mg, PO, tab, TID, PRN anxiety *****IF ALPRAZolam is ineffective/contraindicated or patient is NPO, USE LORazepam if ordered*****
zolpidem 5 mg, PO, tab, Nightly, PRN insomnia may repeat x1 in one hour if ineffective
Antihistamines
diphenhydrAMINE 25 mg, PO, cap, q4h, PRN itching *****IF diphenhydrAMINE PO is ineffective or patient is NPO, USE diphenhydrAMINE inj if ordered*****
diphenhydrAMINE 25 mg, IVPush, inj, q4h, PRN itching Use if oral dose is ineffective or patient is NPO
Anti-pyretics
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 9 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15
1201
Page 9 of 10
UMC Health System Patient Label Here
DISCOMFORT MED PLAN
PHYSICIAN ORDERS
Place an "X" in the Orders column to designate orders of choice AND an "x" in the specific order detail box(es) where applicable.
ORDER ORDER DETAILS
acetaminophen 500 mg, PO, tab, q4h, PRN fever ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen is ineffective/contraindicated, USE ibuprofen if ordered***** 1,000 mg, PO, tab, q4h, PRN fever ***Do not exceed 4,000 mg of acetaminophen from all sources in 24 hours*** *****IF acetaminophen is ineffective/contraindicated, USE ibuprofen if ordered*****
ibuprofen 200 mg, PO, tab, q4h, PRN fever Do not exceed 3,200 mg in 24 hours. Give with food. Use if acetaminophen is ineffective or contraindicated. 400 mg, PO, tab, q4h, PRN fever Do not exceed 3,200 mg in 24 hours. Give with food. Use if acetaminophen is ineffective or contraindicated.
Anorectal Preparations
witch hazel-glycerin topical (witch hazel-glycerin 50% topical pad) 1 app, topical, pad, as needed, PRN hemorrhoid care Wipe affected area *****IF witch hazel-glycerin or phenylephrine ointment ineffective/contraindicated, USE hydrocortisone-pramoxine foam if ordered*****
phenylephrine topical (phenylephrine 0.25%-3% rectal ointment) 1 app, rectally, oint, q6h, PRN hemorrhoid care Apply to affected area *****IF witch hazel-glycerin or phenylephrine ointment ineffective/contraindicated, USE hydrocortisone-pramoxine foam if ordered*****
hydrocortisone-pramoxine topical (hydrocortisone-pramoxine 1%-1% rectal foam) 1 app, rectally, foam, q8h, PRN hemorrhoid care apply to affected area
TO Read Back Scanned Powerchart Scanned PharmScan
Order Taken by Signature: _________________________________________________________________________ Date ____________________________ Time ____________________________
Physician Signature: ___________________________________________________________________________ Date ____________________________ Time ____________________________
Page: 10 OB/GYN Intrapartum Plan Version: 5 Effective on: 08/12/15