24
OBJECTIVE ASSESSMENT: HYPOTHESIS TESTING. Msc Manual Therapy The Knee
| Date post: | 24-Dec-2015 |
| Category: |
Documents |
| Upload: | augustus-clark |
| View: | 215 times |
| Download: | 0 times |
OBJECTIVE ASSESSMENT:HYPOTHESIS TESTING.
Msc Manual TherapyThe Knee
Observation
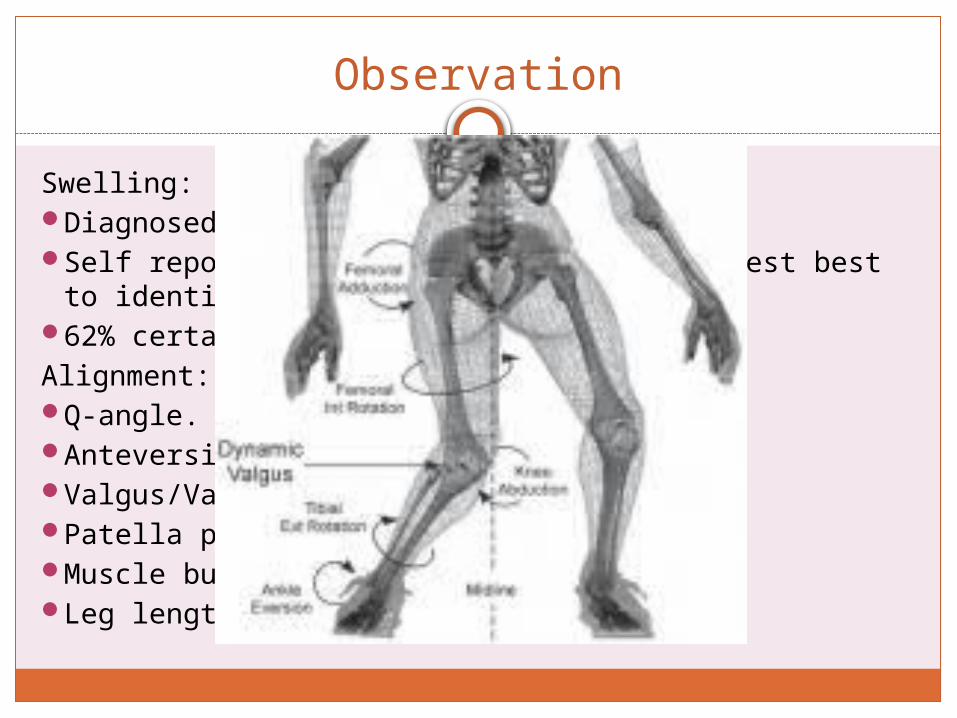
Swelling:Diagnosed by MRI.Self reported swelling and Ballottment test best to
identify effusion (Kasteline, 2009).62% certainty if negative.Alignment:Q-angle.Anteversion/retroversion.Valgus/Varus.Patella position.Muscle bulk/tone.Leg length.

Functional test
GaitSquatSingle leg dipStep upStep downKneelHopFunctional activity relevant to agg and ease.Differential tests
Active Movements
FlexionExtensionMedial rotation
through rangeLateral rotation
through range
RepeatSustainCombine movementsSpeed alterationDifferentiate
arthrogenic, myogenic, neurogenic.

Passive Movements
FlexionExtensionMedial rotationLateral rotationF/Ab and F|Ad quadrantE/Ab and E/Ad quadrantOverpressureSustained

Muscle function
IsometricIsotonicThrough range strengthPNFFlexibilityCore stability

Meniscal Tests
Joint effusion, McMurrays and JLT combined may result in superior diagnostic accuracy (Scholten et al 2001)
Good history and several clinical tests may provide greater diagnostic accuracy than a specific physical test. Don't seem to apply to acutely injured knees, or those with degenerative menisci (Callaghan, Best Bet, 2008).

Summary of sensitivity and specificity
Test Sensitivity Specificity
McMurray’s 16-70% 59-98%
JLT 55-95% 15-97%
Bounce Home 36-47% 67-86%
Apley’s 13-41% 80-93%
Thessaly’s 65-92% 80-97%
Ege’s 64-67% 81-90%
Composite 11-100% 77-99%
Meniscus evaluation should include McMurrays and JLT. Thessaly’s test has shown promise but future research is required to define it’s diagnostic accuracy (Chivers, 2009).
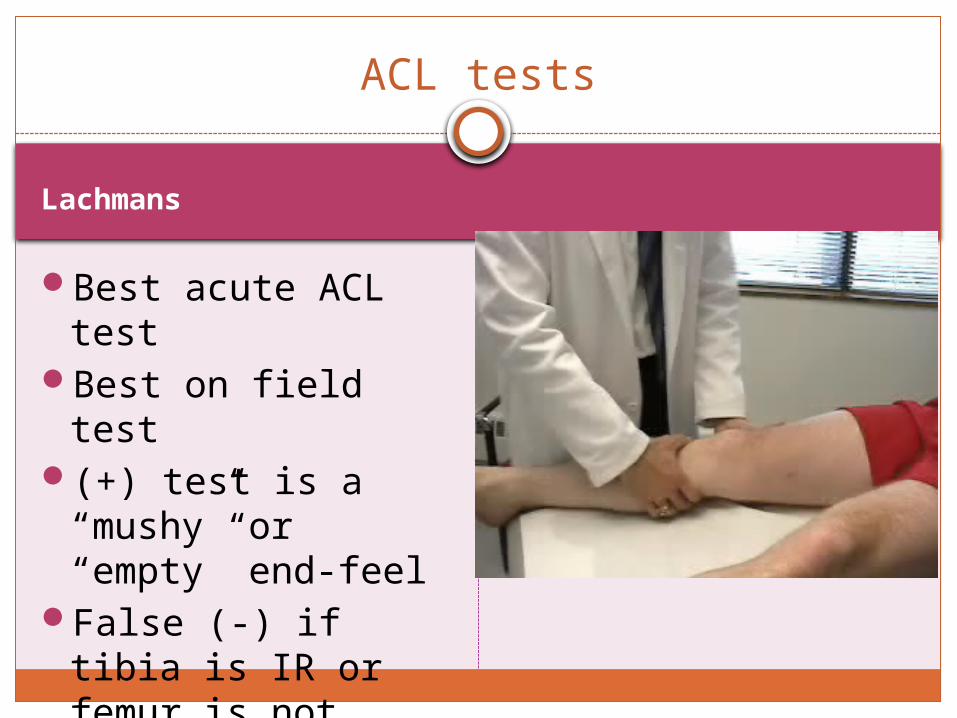
Lachmans
ACL tests
Best acute ACL test
Best on field test(+) test is a
“mushy” or “empty” end-feel
False (-) if tibia is IR or femur is not properly stabilized

(+) Test is increased anterior tibial translation over 6 mm
(+) test indicates: ACL (anteromedial bundle) posterior lateral capsule posterior medial capsule MCL (deep fibers) ITB Arcuate complex
False (-) if only ACL is torn False (-) if there is swelling
or hamstring spasm False (+) if there is a
posterior sag sign present
Anterior Drawer Test

Lateral Pivot Shift Maneuver
Tests for ACL and posterolateral rotary instability Posterolateral capsule Arcuate complex
(+) test is the tibia reduces on the femur at 30 to 40 degrees of flexion, subluxation of the tibia on extension
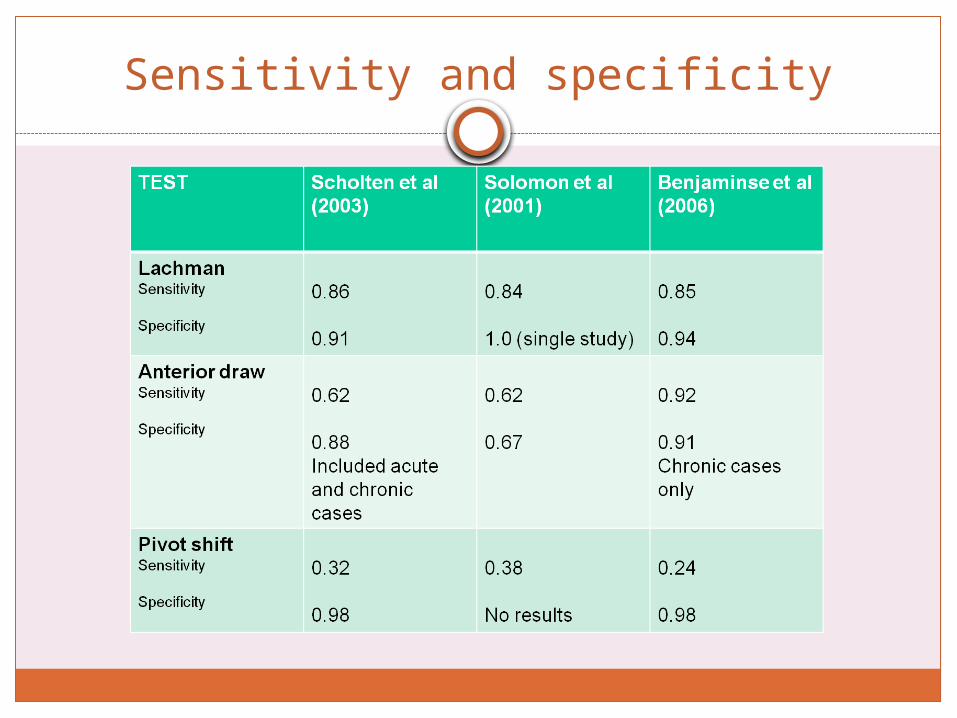
Sensitivity and specificity
PCL tests
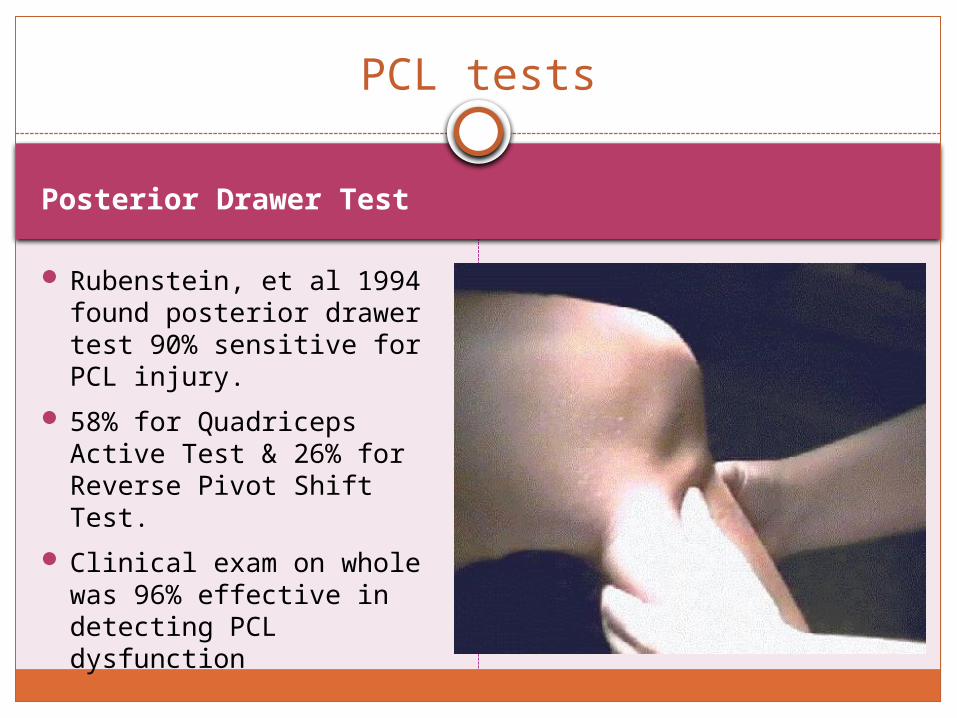
Posterior Drawer Test
Rubenstein, et al 1994 found posterior drawer test 90% sensitive for PCL injury.
58% for Quadriceps Active Test & 26% for Reverse Pivot Shift Test.
Clinical exam on whole was 96% effective in detecting PCL dysfunction
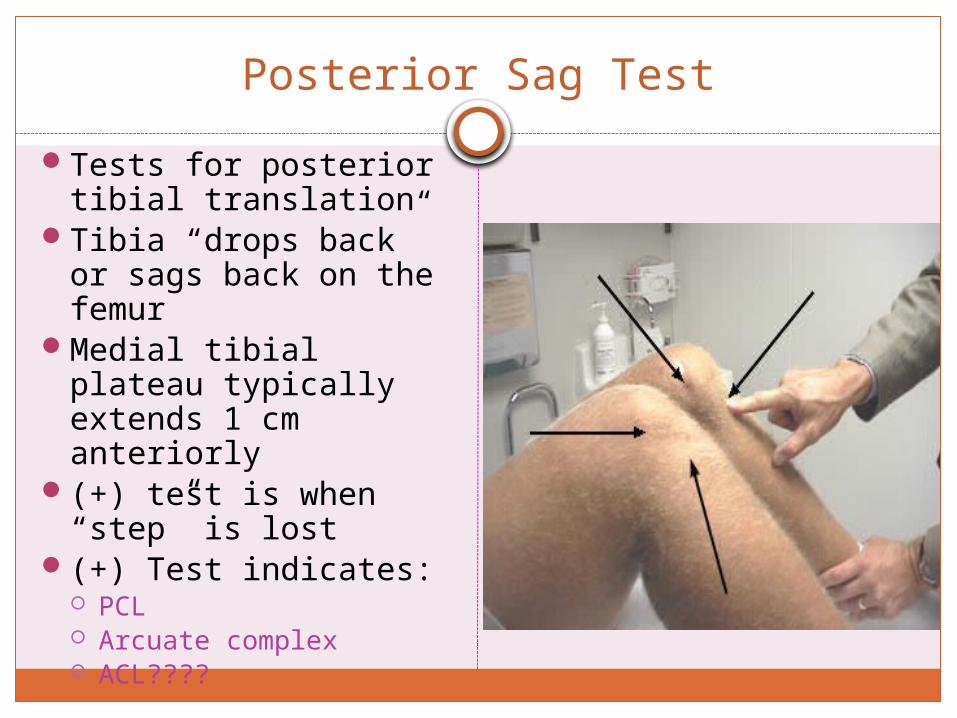
Posterior Sag Test
Tests for posterior tibial translation
Tibia “drops back” or sags back on the femur
Medial tibial plateau typically extends 1 cm anteriorly
(+) test is when “step” is lost
(+) Test indicates: PCL Arcuate complex ACL????
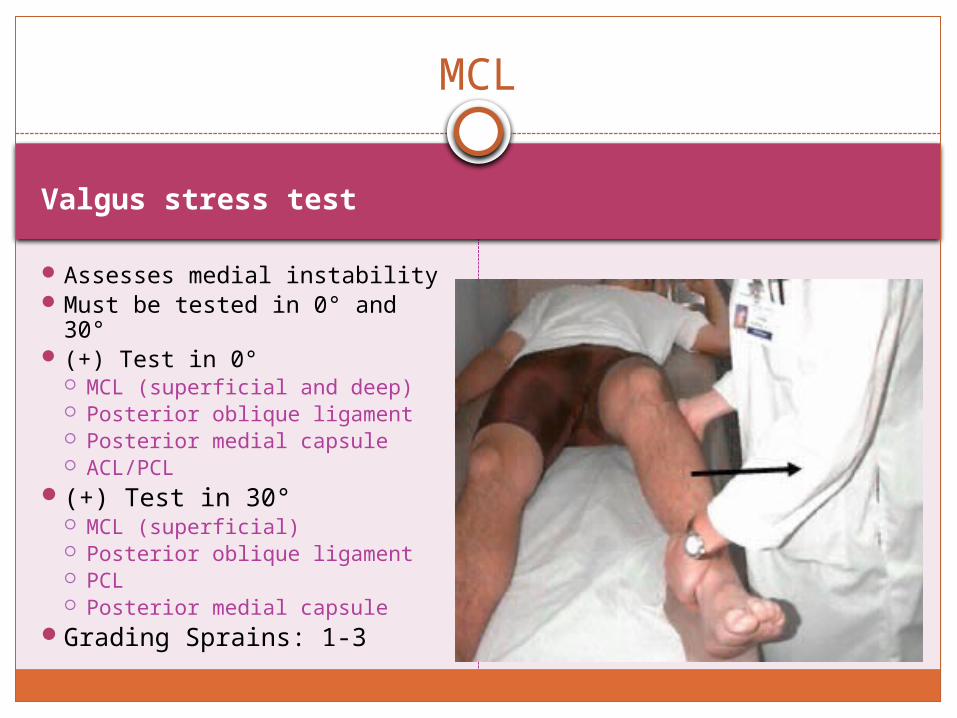
Valgus stress test
MCL
Assesses medial instability Must be tested in 0° and 30° (+) Test in 0°
MCL (superficial and deep) Posterior oblique ligament Posterior medial capsule ACL/PCL
(+) Test in 30° MCL (superficial) Posterior oblique ligament PCL Posterior medial capsule
Grading Sprains: 1-3
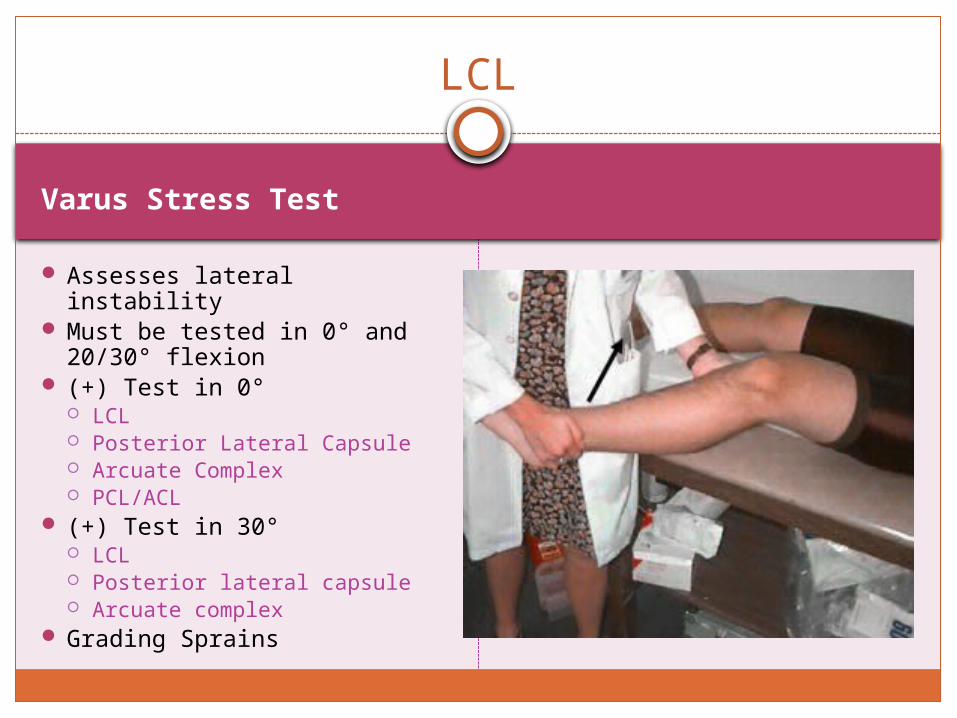
Varus Stress Test
LCL
Assesses lateral instability Must be tested in 0° and
20/30° flexion (+) Test in 0°
LCL Posterior Lateral Capsule Arcuate Complex PCL/ACL
(+) Test in 30° LCL Posterior lateral capsule Arcuate complex
Grading Sprains
Reverse Lachmans Dial Test
Prone, femur fixed.Ant drawer to end
point.+ve tib tuberosity
and fib head move lat.
Prone, knees flexed to 90˚.
Externally rotate feet.
+ve if effected foot moves ?15˚ more.
PLC

Valgus Stress Test Hyperextension
Full extension.20˚ flex.If increase in
movement think PLC.
In standing/walking will have ext/lat thrust.
Prone heels over bed: +ve if heel dropped.

Clarke’s (grind) test
No evidence.Many false
positives.+ve if reproduces
pain or unable to hold contraction.
Patellofemoral Tests
Compression test Apprehension test
Force patella into trochlea.
Monitor pain response.
Flex knee to 20-30˚.Laterally displace
patella.
Tibio femoral Tibio fibular
Tibia:
Femur:
Fibular head:
Accessrory Movements: neutral/through range

Patellofemoral
Round the clockRotation
Other joints/structures
LumbarThoracicSIJHipFoot and ankleNeural: PKB +/- slump, SLR +/- peroneal
nerve bias
Conclusion
Have you confirmed/negated your hypothesis/es?Have you indentified subjective and objective
markers for retesting ?What is your clinical impression?What is your prognosis for recovery?Formulate a treatment plan incorporating
comparable findings, functional difficulties, patient specific goals and best available evidence.
How will you progress treatment to ensure maximum recovery?

















