46
OBSCURE GI BLEED Talat Bessissow, MC CM, FRCPC Assistant Professor, Department of Medicine Division of Gastroenterology McGill University Health Center
| Date post: | 15-Dec-2015 |
| Category: |
Documents |
| Upload: | randall-dence |
| View: | 221 times |
| Download: | 2 times |

OBSCURE GI BLEEDTalat Bessissow, MC CM, FRCPCAssistant Professor, Department of MedicineDivision of GastroenterologyMcGill University Health Center

Definition• Definition = GI bleeding of uncertain etiology after EGD, C-scope, and
small bowel radiography
• Overt OGIB = hematochezia, melena, hematemesis or CG emesis
• Occult OGIB = FOB + in abscence of visible blood, Iron deficiency Anemia

Fecal occult blood testing
• Guaiac-based tests: The pseudoperoxidase activity of hemoglobin turns the guaiac compound blue in the presence of hydrogen peroxide


Epidemiology 300,000 pts hospitalized/yr in US ... 5% of these will have
normal EGD and C-scopes
Median time for diagnosis is 2 years
Average cost $33,630 per patient
Average 7.3 tests per patient
Paradigm shift since introduction of VCE and DBE

Etiology of Obscure GI Bleeding 5% of patients presenting with GI hemorrhage have no source found by
upper endoscopy and colonoscopy.
Of these, 75% are 2ndry to small bowel lesions
Of these, 30-60% angiectasias
Am J Surg 1992;163:90–92Br Med J (Clin Res Ed)1984;288:1663–1665.

Etiology of Obscure GI BleedingUpper and lower GI
bleedingoverlooked
Mid GI bleeding
Cameron’s erosions Tumors
Fundic varices Meckel’s diverticulum
Peptic ulcer Dieulafoy’s lesion
Angiectasia Crohn’s disease
Dieulafoy’s lesion Celiac disease
GAVE Angiectasia
Neoplasms NSAID enteropathy
Erosive gastritis Hemobilia
Ischemic colitis/UC Aortoenteric fistula
Large polyps Vasculitis

Etiology
• 40% of OGIB - due to angiectasias (AVMs) Angiectasias : ectatic blood vessels made of thin wall with or
without endothelial liningo Natural history of angiectasias is not well known
o Only 10% of all patients with angioectasia will eventually bleed
o Once a lesion has bled up to 50% will not rebleed --- predictors of rebleeding: multiple bleeding episodes, transfusion requirement
o Bleeding angiectasias are associated with abnormal von Willebrand’s factor (vWF)

AVM• Conditions/diseases associated with angiodysplastic lesions:
• Elderly
• CRF
• Aortic valve disease (Heyde’s syndrome)
• Cirrhosis
• Collagen vascular disease

AVM

What is Heyde’s syndrome ?
Heyde’s syndrome: Bleeding from angiectasias in patients with AS.
o Increased consumption of high-molecular-weight multimers of VWF due to shear stress of the abnormal valve which corrects after aortic valve replacement with decreased severity of bleeding
Transfus Med Rev 2003;17:272–286.; Abdom Imaging (2009) 34:311–319

Small Bowel Bleeding• Etiology depends on the age of the patient
• Young: small intestinal tumors, Meckel’s diverticulum, Dieulafoy lesion, Crohn’s disease
• Older: (>40) vascular lesions, NSAID-induced SB disease
• Uncommon: hemobilia, hemosuccus pancreaticus, aortoenteric fistula

History and Physical Examination The nature of the exact presenting symptom is important in deciding a
practical, efficient, and cost-effective evaluation plan Hematemesis indicate upper GI bleed Melena can be anywhere from the nose to the right colon Hematochezia can be a lower GI bleed or a fast upper GI bleed
History of medications (mainly OTC)
Family history
Skin signs

Hereditary hemorrhagic telangiectasia

Blue rubber bleb nevus syndrome

Dermatitis herpetiformis

Plummer–Vinson syndrome

Tylosis

Investigation options
I. Repeat G & C
II. CTE
III. Capsule endoscopy
IV. Enteroscopy - push or SBE/DBE
V. Angiography
VI. Tagged RBC scan

Common lesions that are overlooked• EGD: Cameron’s erosions, fundic varices, PUD, angioectasias,
Dieulafoy lesion, GAVE
• C-scope: angioectasias, neoplasms

Investigation Repeat standard endoscopy, especially if anemia and overt GI
bleeding:o Overlooked lesions: fundus
o high lesser curvature antrum C loop of duodenum, posterior wall of
duodenal bulb Random SB Bx can be + for celiac disease in up to 12%
The yield of repeat colonoscopy is 6%, yield of repeat EGD is 29% (ASGE)
Am J Gastroenterol 1996;91:2099–2102

Investigation Consider side-viewing scope if pancreatobiliary
pathology is suspected Small bowel series/SBFT:
o When compared with capsule endoscopy• diagnostic yield 8% vs 67%• clinically significant finding 6% vs 42%
(NNT 3)
o Used if SB obstruction is suspected
Gastroenterology 2002;123:999–1005

Investigation CT Enterography:
o Thin sections and large volumes of enteric contrast material to better display the small bowel lumen and wall.
o Neutral enteric contrast + IV contrast
o 1.5 – 2 L of milk, PEG electrolytes or low-concentration barium

Investigation
CT Enterography:
o Advantages: displays entire wall thickness examination of deep ileal loops mesentery & perienteric fat no need for NGT

CTE

Investigation
Technetium-99m–labeled RBC scan: Limited value Blood loss of 0.1-0.4 ml/min (2U PRBCs /d) Poor localization of SB bleeding - not enough to direct operative therapy
Angiography: Useful in massive bleeding (>0.5ml/min) Diagnostic & therapeutic
Nucl Med Commun 2002;23:591–594

Investigation Endoscopic imaging:
o Intraoperative enteroscopy; Terminal ileum can be reached in 90% of cases
• diagnostic yield 58-88%• mortality up to 17%

Investigations
Push enteroscopy: Length 220-250 cm usually limited to 150 cm diagnostic yield up to 70% angioectasias in up to 60% some suggest push enteroscopy over repeat EGD as
second look

Capsule endoscopy
oSize 11x26 mmoObtains images and transmits the data via radiofrequency to a recording deviceoThe capsule is disposableoExamination takes at least 8 hours (57,600 images)oReading 60 – 120 minutes oSB obstruction is a contraindication

Capsule endoscopy Capsule endoscopy: yield 63% vs 23% for push enteroscopy Sensitivity 89 - 95% Specificity 75 – 95% +ve predictive value 97% -ve predictive value 86%
•
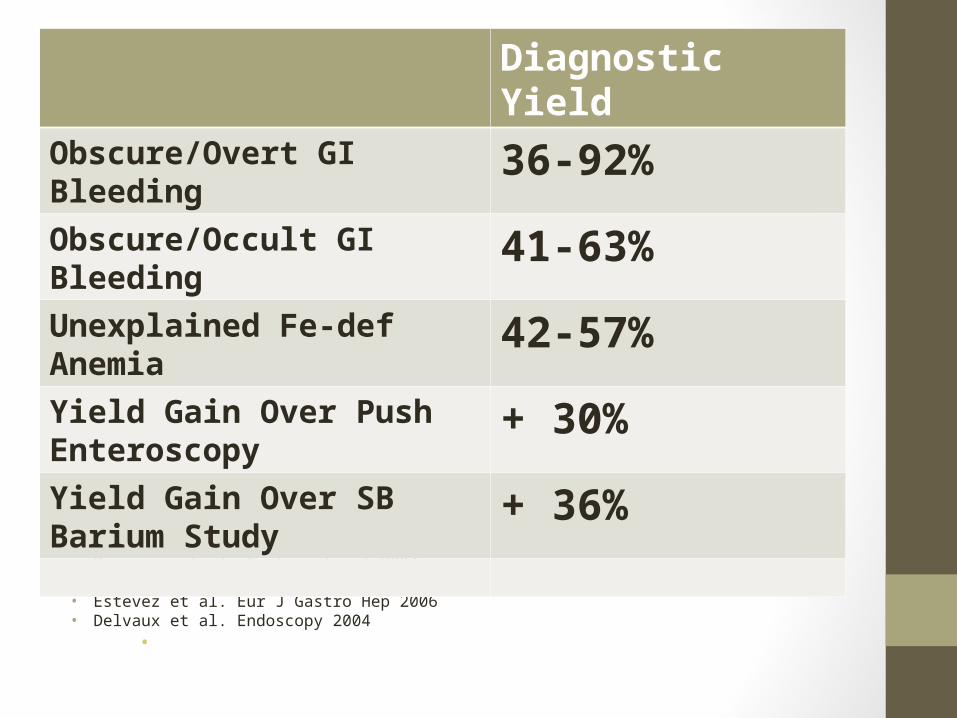
• Lin, GIE 2008• Rastogi et al. GIE 2004• Pennazio et al. Gastroenterol 2004• Apostolopoulos et al. Endoscopy 2006• Estevez et al. Eur J Gastro Hep 2006• Delvaux et al. Endoscopy 2004
•
Diagnostic YieldObscure/Overt GI Bleeding 36-92%Obscure/Occult GI Bleeding 41-63%Unexplained Fe-def Anemia 42-57%Yield Gain Over Push Enteroscopy
+ 30%
Yield Gain Over SB Barium Study + 36%

• Superior yield to other diagnostic modalities in both active and inactive obscure GI bleeds
Study Sens (%) Spec (%) PPV (%) NPV (%)
Pennazio 2004, Gastroenterol 88.9 95 97 82.6
Hartmann 2005, GIE 95 75 95 86
* Marmo, APT 2005, Triester, AJG 2005, Saperas AJG 2007




Double Balloon Enteroscopy
Double Balloon Enteroscopy (DBE)
o 1st described in 2001
o 200-cm enteroscope
o 140-cm overtube



Double Balloon Enteroscopy (DBE)
o Antegrade approach:
mean distance 240 +/- 100 cmmean time 72.5 +/- 23 min
• Retrograde approach:
mean distance 140 +/- 90 cm mean time 75 +/- 28 min

How Effective is DBE?
Study Diagnostic Yield (%)
Kaffes 2004, Clin Gastro Hep 76
Mehdizadeh 2006, GIE 51
Yamamoto 2006, Am J Gastro 76
Jacobs 2007, GIE 75
Tanaka 2008, GIE 54
Yadav 2010, abstract DDW 52%

How Effective is DBE?
Study Patients (n) Yield
Matsumoto 2005, Endo 13 Equivalent
May 2005, GIE 52 DBE better
Hadithi 2006, Am J Gastro 35 CE better
Mehdizadeh 2006, GIE 115 Equivalent
Ohmiya 2007, GIE 74 Equivalent
Kameda 2008, J Gastroenterol 32 Equivalent
Teshima 2010, DDW (Meta-) 1293 CE favoured although
nearly equivalent

Complications
- Perforation – 0.3-1.1%
- Bleeding (post-polypectomy) – 1.4-1.9%
- Pancreatitis – 0.2-0.3%
Melsink Endoscopy 2007, Gerson ACG 2008

Single Balloon Enteroscopy- Much more recent- Simpler to set up, works with existing Olympus
equipment- Same specifications as DBE without the second balloon
on the endoscope
Hartmann, Endoscopy 2007

Single Balloon Enteroscopy
Kawamura GIE 2008

SBE versus DBE
• Efthymiou, abstract 2010• RCT involving 79 patients recruited for mainly
OvGIB/ObGIB• About half had SBE• Depth of insertion retrograde was identical (100 cm)• Depth of insertion orally favoured DBE (250 versus 205
cm but not significant)• Therapeutic yield was 54% DBE, 37% SBE (not
significant)• Targetted biopsies or application of cautery or argon plasma

Pennazio et al. Endoscopy 2005 & AGA Technical Insitute. Gastroenterol 2007

















