54
Observation Workshop EDDA 2 2019 Michael A. Granovsky, MD CPC FACEP President LogixHealth
Observation WorkshopEDDA 2 2019
Michael A. Granovsky, MD CPC FACEP
President LogixHealth

▪ CMS Recovery Audit Contractors (RACs) focusing on inpatient DRG payments vs. Observation status
▪ Hospitals under pressure to cut costs– Global contracts/ACOs/directly insuring
communities▪ ED groups ideally suited to run efficient units
with short lengths of stay– The masters of the throughput mindset!
Why Is Obs Important Now?

▪ Medicare pays a fixed amount for inpatient care▪ Typically a large amount
– Much more than the observation payment▪ Recent study calculated use of Obs instead of
inpatient reduce CMS cost dramatically▪ Average cost savings per patient = $1,572▪ Annual savings calculated: $3.1 Billion
DRG Economics

▪ Hospitals were paid for a total of 1,074,267 short inpatient stays. In our review 39% were potentially inappropriate for payment because the claims did not meet CMS’s criteria for an appropriate short inpatient stay.
OIG Report and Analysis: Compliance with the 2 Midnight Rule

Current RAC Contracts

Region States Websites Email Phone Number
Region 1Performant Recovery, Inc.
CT, IN, KY, MA, ME, MI, NH, NY, OH, RI, and VT
https://performantrac.com/PROVIDERPORTAL.aspx [email protected] 1-866-201-0580
Region 2Cotiviti, LLC
AR, CO, IA, IL, KS, LA, MO, MN, MS, NE, NM, OK, TX, and WI
https://Cotiviti.com/RAC [email protected] 1-866-360-2507
Region 3Cotiviti LLC
AL, FL, GA, NC, SC, TN, VA, WV, Puerto Rico and U.S. Virgin Islands
https://www.Cotiviti.com/RAC [email protected] 1-866-360-2507
Region 4HMS Federal Solutions
AK, AZ, CA, DC, DE, HI, ID, MD, MT, ND, NJ, NV, OR, PA, SD, UT, WA, WY, Guam, American Samoa and Northern Marianas
https://racinfo.hms.com/home.aspx [email protected]
Part A:1-877-350-7992
Part B:1-877-350-7993
Region 5DME/HHE/Performant Recovery, Inc.
Nationwide for DMEPOS/HHA/Hospice
https://performantrac.com/PROVIDERPORTAL.aspx [email protected] 1-866-201-0580
RAC Contact Information
Recovery Audit Contractors

▪ Complex Medicare Report▪ Supplies hospital data related to
potentially improper DRG payments– Number of discharges per DRG– Payments per DRG– Length of stay per DRG
• Highlights hospital LOS < 1 calendar day– RAC focus for DRG take backs
Your Hospital’s DRG ProfileThe Pepper Report

▪ Hospitals pressured to avoid short-stay inpatient admissions
▪ Increased use of “observation status”▪ Initially, a billing change…
now a delivery model change▪ Now have opportunities for cost efficiency▪ Accelerated throughput yields cost savings▪ Requires throughput focused providers:
Doctors, Nurses, Mid Levels, Support Staff!
RAC Impact and Hospital Response
▪ Maximize RVUs/patient– Physician documentation– Coding methodology
▪ Optimize RVUs/day– Appropriate patient selection
▪ Refine the profit margin– Census and staffing
▪ Facility revenue considerations
Optimizing Observation Revenue

Observation care is a well-defined set of specific, clinically appropriate services, that are furnished while a decision is being made regarding whether patients will require further treatment as hospital inpatients.
CMS Transmittal 1745, 290.1 - Obs Services Overview
Such services are covered only when provided by order of a physician…
“The following codes are used to report encounters by the supervising physician…and performance of periodic reassessments” CPT 2019 page 13
2019 Obs CPT & CMS

▪ Timed/dated order toplace in observation status
▪ A short treatment plan regarding the goals of observation
▪ Clinically appropriate progress notes– Asthma different than chest pain
▪ A discharge summary reviewing the course in observation, findings, and plan
General Documentation Requirements

Same day admit and discharge CPT Codes:▪ 99234 – Low severity
– Low-complexity MDM▪ 99235 – Moderate severity
– Moderate-complexity MDM▪ 99236 – High severity
– High-complexity MDM
Professional Observation CPT Codes
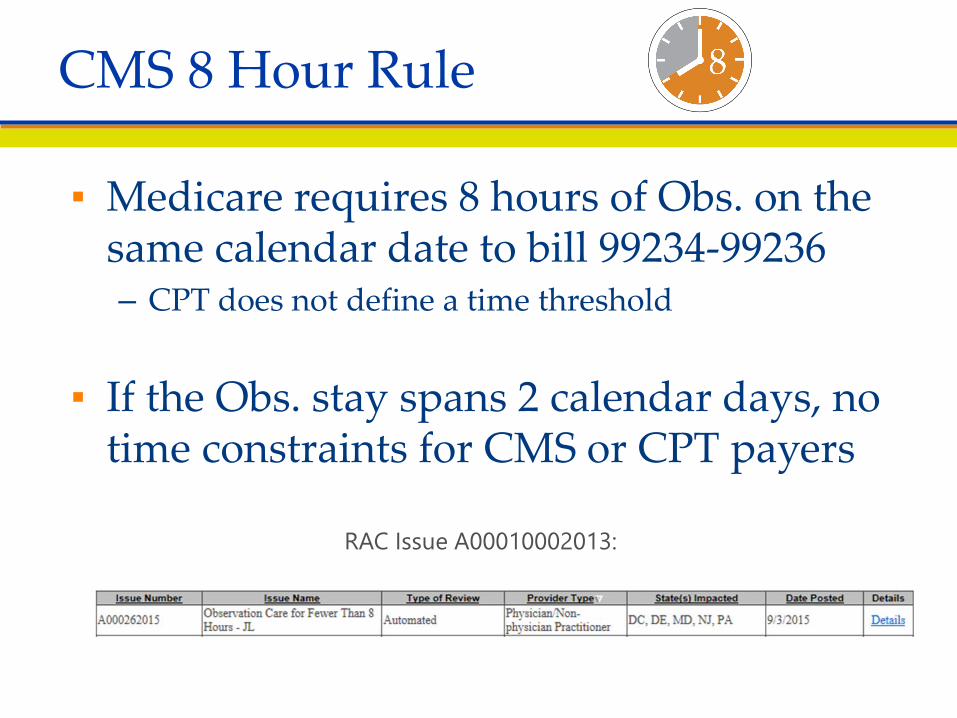
▪ Medicare requires 8 hours of Obs. on the same calendar date to bill 99234-99236– CPT does not define a time threshold
▪ If the Obs. stay spans 2 calendar days, no time constraints for CMS or CPT payers
CMS 8 Hour Rule
RAC Issue A00010002013:

▪ Admit and discharge more than one calendar day:
▪ Initial Day CPT codes:– 99218 – Low severity
• Low-complexity MDM– 99219 – Moderate severity
• Moderate-complexity MDM– 99220 – High severity
• High-complexity MDM
Professional Observation CPT Codes

Discharge day CPT Code:▪ 99217- Discharge Day▪ Includes final exam, discussion of
observation stay, follow-up instructions, and documentation
▪ Used with codes from the initial observation day codes series (99218/99219/99220)
Professional Observation CPT Codes

Observation Level of Care
Care All on the Same Day
Care Covers Two Calendar Days
1 99234 99218 + 99217
2 99235 99219 + 99217
3 99236 99220 + 99217
Coding Scenarios Observation Services

▪ A high complexity patient is placed in Observation Status at 9 am and discharged home later that day at 8 PM.
▪ What physician code(s) would be assigned– 99285– 99220– 99236– 99291– **99236
Audience QA

▪ A high complexity patient is placed in Observation Status at 9 pm and discharged home the next day at 8 AM.
▪ What physician code(s) would be assigned– 99285– 99220 + 99217– 99236– 99291– **99220 + 99217
Audience QA

▪ All but the lowest level Obs require very significant Hx and PE documentation
▪ Comprehensive Hx and PE:99219/99220 & 99235/99236– HPI: 4 elements– PFSHx: 3 areas (Requires Family Hx)– ROS: 10 systems– PE: 8 organ systems
Obs services typically require a family history
▪ Beware overuse of macros for ROS and PE
Physician Documentation

▪ CMS requires that comprehensive observation histories have 3 of 3 PFSH elements rather than the 2 of 3 requirement for ED E/M codes
Medicare 1995 DGs page 6
– May utilize the nurse’s notes but beware• Rarely document a Family Hx
“A review of all three history areas is required for services that by their nature include a comprehensive assessment
or reassessment of the patient.”
CMS PFSHx Observation Requirement

Level HPI ROS PFSHx PE99234 4 2 1 5
99235 4 10 3 8
99236 4 10 3 8
Summary Documentation Requirements
Complete and Appropriate DocumentationBeware Macro Over use

▪ A chest pain Obs patient coded 99236 requires which of the following?– 4 HPI– 10 Review of Systems– Past Medical and Social History– Family History– **All of the above
Audience QA

▪ 53 y.o. male with CP placed in Observation at 9 am and discharged at 7pm.
▪ What code set would we consider?– 99234-99236
▪ Documentation includes 4 HPI, 10 ROS, Past/Family/Social Hx/ 8 PE organ systems
▪ Assuming high complexity what code would be applied?– 99236
▪ What if the Family Hx is omitted?– 99234
Audience Coding Vignette

Same Day Obs Total RVU
Over Midnight
Obs Total RVU ED E/M
Service Total RVU
99234 3.75 99217 2.06 99284 3.3299235 4.77 99218 2.81 99285 4.8999236 6.13 99219 3.83
99220 5.23
2019 RVUs Observation Services
99217 + 99220 = 7.29 RVUs Total
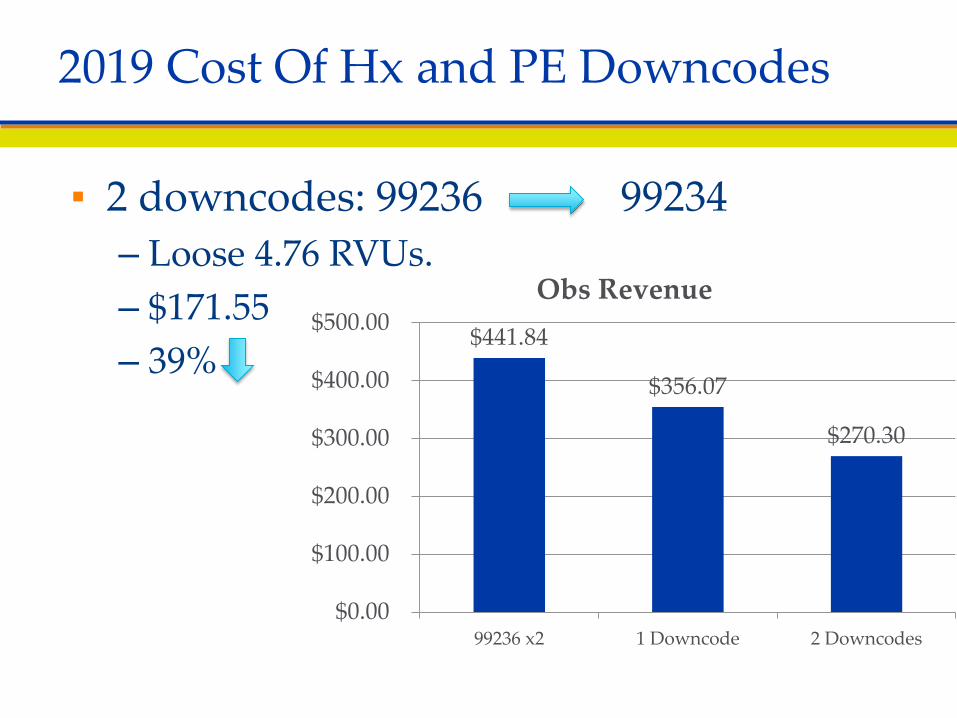
▪ 2 downcodes: 99236 99234– Loose 4.76 RVUs.– $171.55– 39%
2019 Cost Of Hx and PE Downcodes
$441.84
$356.07
$270.30
$0.00
$100.00
$200.00
$300.00
$400.00
$500.00
99236 x2 1 Downcode 2 Downcodes
Obs Revenue

List the below codes in order of lowest to highest RVUs– 99285– 99220 + 99217– 99236– 99284
▪ RVUs lowest highest– 99284– 99285– 99236– 99220 + 99217– **2.40 RVUs > 99285
Audience QA

▪ Most ED run Observation units see higher acuity patients
▪ Chest pain or clinically equivalent complexity is very common
▪ ED Observation E/M distribution influenced by pre-selected complexity
Obs Coding Methodology

Clinical Benchmarks of Patient Complexity
▪ No AMA CPT Appendix C Obs code vignettesCMS RUC data base vignettes
▪ 99234: 19 y.o. pregnant patient (9 weeks gestation) presents to the ED with vomiting X 2 days. The patient is admitted for observation and discharged later on the same day.
▪ 99235: 48-year-old presents with an asthma exacerbation in moderate distress.
▪ 99236: 52-year-old patient comes to the ED because of chest pain.

10.9%
27.3%
61.8%
0%
10%
20%
30%
40%
50%
60%
70%
99234 99235 99236
Medicare E Med Obs Codes Reported
CMS Obs E/M Distribution

– Chest pain• High complexity
– Moderate Asthma• Mod. complexity
– TIA• High complexity
– Syncope• High complexity
– Mild dehydration healthy
• Low complexity
Audience Exercise Re Complexity
30
Benchmark your distribution based on complexity of clinical protocols:
Determine if High/Moderate/Low

▪ Cost reduction $1,500 - $2,000 per case– Brigham Health Affairs data $1,572 / case– Emory TIA $2,062 / case– Indirect Cost reduction:
• Risk reduction – re-admissions, medical legal (i.e. missed MI)
▪ Smart top line revenue growth– “back filled admissions”– Baugh “options modeling” data presented
MCEP - $2,908 / case
Macro Economic Considerations

▪ Varies by department acuity and your Obs protocols– How wide you cast the net
▪ Basic benchmarks– Typically 5% - 10% for many groups– 1 out of 3 admissions– Chest pain most common…typically a third
▪ Most groups have a 10% - 20% failure rate– Converted to inpatient
How Many Patients?

▪ 40K ED with a 22% admission rate▪ How many patients daily potentially qualify
for Obs?– 40,000 per year /365 days = – 110 patients per day– 110 X .22 =
▪ 24 daily admissions– 30% qualified for Obs– Average of 7 Obs patients per day
• Chest pain, syncope, cellulitis, pyelo, allergic reaction, Asthma, dehydration,
Audience Case Study Community Hospital

▪ What were the cost savings?▪ 10 bed unit …. occupied 28 days a month▪ With overnight stays 2,555 patients treated▪ Prior LOS for cohort 25 hours▪ Obs mean LOS 15 hours
– Staffing bed hours saved?– 2,555 X (25-15) – 25,555 bed hours!– Days of LOS eliminated?– 25,555/24 hours per day = 1,064 day decrease in LOS
Audience Case Study Community Hospital

▪ 50,000 visit ED▪ 22% admit rate▪ How many potential Obs cases▪ First how many daily “admissions”?
– 50,000 / 365=– 137 patients per day– 137 X 22%=– 30 “admissions”– How many Obs patients?– 30 “admissions” X .3 = 10 Obs patient per day
Audience Case Study

Selecting correct patients is key to the operational success of an observation unit▪ Select patients with diagnoses that have that
have associated clinical protocols▪ Expedite throughput▪ Achieve decreased length of stay▪ Reach a successful clinical endpoint▪ Prolonged stays drag down RVU efficiency
Patient Selection for Observation Services

▪ Chest pain▪ Abdominal pain▪ Headache▪ Cellulitis▪ Pyelonephritis▪ Asthma▪ Dehydration▪ Renal colic▪ Hypoglycemia▪ Allergic reaction▪ Pharyngitis
▪ Closed head injury▪ Vertigo▪ Hematuria▪ Pancreatitis▪ SOB▪ CHF/COPD▪ Back pain*
– non ambulatory▪ Extremes of age*▪ Mental Health*
– Substance abuse
The Spectrum of Complexity
Easier Harder

▪ Place in order the desirability for Obs– 81 y.o. dizzy– 52 y.o. pancreatitis– 27 y.o. moderate
asthma– Chest pain
– Chest pain– 27 y.o. moderate
asthma– 52 y.o. pancreatitis– 81 y.o. dizzy non
ambulatory
Audience Exercise

ACEP Observation Medicine Sectionwww.Acep.org– Clinical & Practice Management » Resources
» Observation Medicine– http://www.acep.org/observationsection/– Brigham, Duke, Hospital of Central CT, Houston
Northwest, William Beaumont– http://www.bidmc.org/Centers-and-
Departments/Departments/Emergency-Medicine/Services/Observation-Medicine.aspx#D
– http://www.obsprotocols.org
Observation Protocol Resources

▪ Efficient quality care with decreased length of stay
▪ Create hospital bed capacity▪ Obs service line that adds value to the
HospitalShort LOS with great care is the paradigm
Summary Goals

Patient Selection: Smart Bed Use
A Driver of Financial Success
▪ CHF 3 day stay– Htn, Creat. 2.3 & BS 385
▪ Monday placed in CDU▪ Tuesday slow diuresis
– BS, K+ abnormal, BP▪ Home late Wednesday
▪ Alternative bed use▪ Day 1- Chest pain patient
– 15 hour LOS▪ Day 2 – pyelonephritis
– Stays overnight– Dc’d in the AM
▪ Day 3 Chest pain– 15 hour LOS
RVU Modelling: LOS and Bed Use

CHF 3 day stay Mon- Wed▪ Monday high complexity
first Obs day– 99220 5.27 RVUs
▪ Tuesday – 99225 2.07 RVUs
▪ Wed discharge– 99217 2.07 RVUs
Alternate Use Monday Chest Pain 99236 6.18 RVUs
Tuesday Morning Pyelo 99220 5.27 RVUs
Wednesday Morning Pyelo DC 99217 2.07 RVUs
▪ Wednesday Chest pain– 99236 6.18 RVUs
Audience Code & RVU Exercise

5.23
2.06 2.06
9.35
6.137.29
6.13
19.55
0
5
10
15
20
25
Day 1 Day 2 Day 3 Total
CHF 3 Day RVUs$337.45CPx2, Pyelo RVUs$704.56
Chest Pain
Chest Pain
Pyelo
2019 Controlling Bed Flow to Maximize RVUs
RVU Comparison Over 3 Days

▪ 10 bed unit…turned 1.3 times daily– Blend of moderate and high ….5.7 RVUs per case– 74 RVUs….$36/RVU….$2,700 daily = $112/hr– Cost: salary, benefits, overhead…?tough to cover costs
Innovative Profit Solutions▪ MD coverage in the morning and evening
– New admits and discharges– 10hrs X $150 = $1500
▪ PA/NP interim coverage – 12hrs X $70 = $840– Protocol driven at night
▪ Creep up volume to be profitable– Expand beyond chest pain to include protocol driven complaints
such as Dehydration, Pyelonephritis, Asthma, Cellulitis
Observation Unit Staffing for Profit

▪ Facility observation is a composite APC ▪ Requires a qualifying visit and 8 hours of facility time
– 2015 limited ED visit types qualified – Type A 99284/99285/99291– Level 5 Type B ED visit (G0384)– An outpatient clinic visit (G0463)
▪ 2019 Observation many types of visits potentially qualify – 99281-99285 (Type A ) or G0381- G0385 (Type B)– 99291– G0463 (hospital outpatient clinic visit)– G0379-(direct referral for observation)
2019 Observation Coding Construct

Qualifying Visit 9928x, 99291, outpatient clinic G0463 8 hours reported as units of G0378 (in the
units field) There must be a physician order for
observation No T status procedure
2019 Observation Requirements

▪ CMS has continued to expand the concept of outpatient packaging– Comprehensive APCs
A C-APC is defined as a classification for the provision of a primary service and all adjunctive services provided to support the delivery of the primary service. We established C-APCs as a category broadly for OPPS payment and implemented 25 C-APCs beginning in CY 2015
-2016 OPPS 124/1221▪ Observation APC 8009 retired in 2016▪ New observation C- APC 8011 continues for 2019
2019 Observation as a Comprehensive APC

▪ Everything! (Most: Labs, CT, US, procedures, IVF, Meds)▪ Except (S.I. F, G, H, L and U)
• Some Brachytherapy services (status indicator U)• Pass-through drugs, biologicals and devices (status
indicators G or H)• Corneal tissue, CRNA services, and hepatitis B
vaccinations (status indicator F)• Influenza and pneumococcal pneumonia vaccine
services (status indicator L)• Ambulance services• Mammography
What’s Included in the Observation Comprehensive APC?

Year CMSPayment
2012 $720.64
2013 $798.47
2014 $1,199.00
2015 $1,234.22
2016 $2,174.14
2017 $2,221.70
2018 $2,349.66
2019 $2,386.80
2019 Observation Facility Payment
$720.64
$798.47
$1,199.00
$1,234.22
$2,174.14 $2,21.70$2,349.66
$2,386.80
$0.00
$500.00
$1,000.00
$1,500.00
$2,000.00
$2,500.00
$3,000.00
2012 2013 2014 2015 2016 2017 2018 2019

▪ Observation is a Comprehensive APC- mini DRG
▪ Bundling: Most Labs, ancillaries, radiology, procedures, hydration/injection/infusion
Observation Increased Payments in 2018What's the Catch?

▪ Risks: overuse of observation– Financial- lower payment to hospital vs. inpatient
• $5,142 vs. $1,741 (looking at top 10 diags.)– Loss of 3 day qualifying stay for SNF coverage– Potential higher out-of-pocket expense for patients
▪ Risks: underuse of observation– Inappropriate inpatient admissions - RAC target– Short inpatient stays:
• Decrease CMI• Hospital payment denials
The Obs Pendulum: Facility Financial Risk/Reward

▪ Observation services will be an expanding determinant of our financial success
▪ Documentation and correct coding methodology drive the revenue per patient
▪ Focused patient selection, throughput and protocols optimize RVUs/day
▪ Packaging of services will lead to resource use pressure and efficiency pressure!
▪ The ED throughput culture is ideally suited to maximize Observation financial success
Conclusions

Contact Information
Michael A. Granovsky, MD CPC FACEP
President LogixHealth
www.logixhealth.com

















