34
OBSTETRICS OSCE REVIEWER egpt2010
| Date post: | 14-Dec-2015 |
| Category: |
Documents |
| Upload: | arlene-mclaughlin |
| View: | 273 times |
| Download: | 0 times |

OBSTETRICS OSCE REVIEWER
egpt2010
Internal Examination
DilatationEffacement

Clinical Pelvimetry
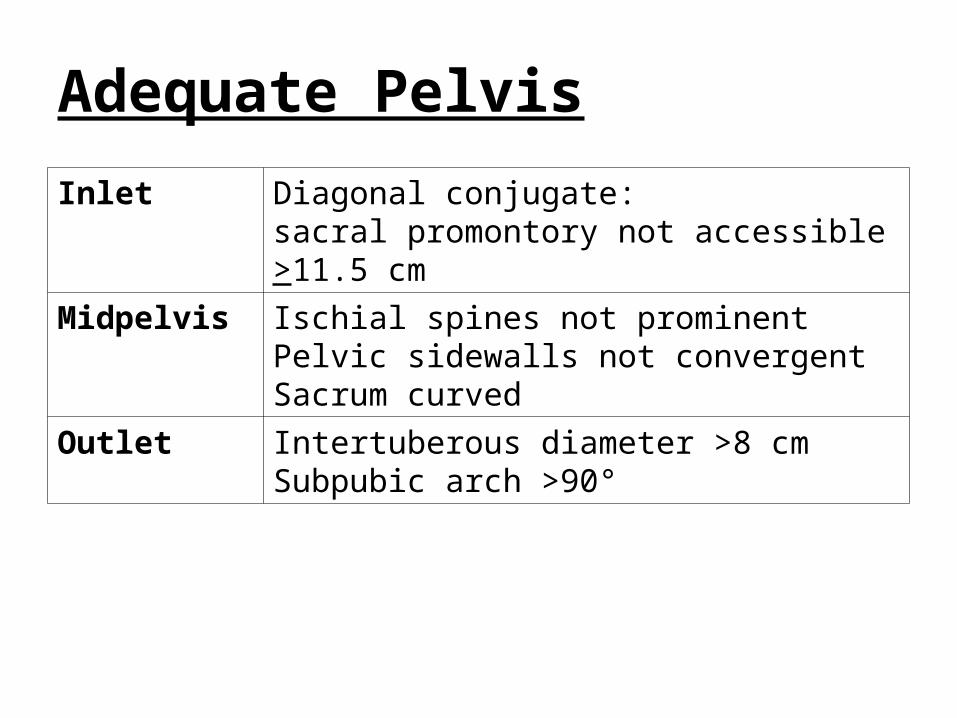
Inlet Diagonal conjugate:sacral promontory not accessible >11.5 cm
Midpelvis Ischial spines not prominentPelvic sidewalls not convergentSacrum curved
Outlet Intertuberous diameter >8 cmSubpubic arch >90°
Adequate Pelvis

Pelvic Inlet
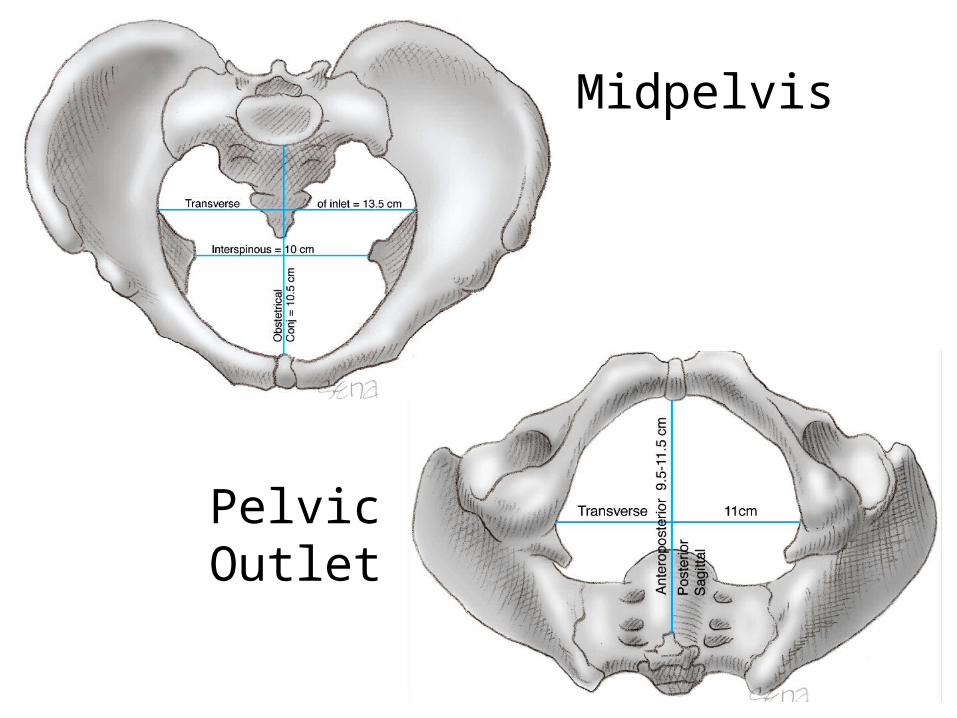
Midpelvis
Pelvic Outlet

Partograph
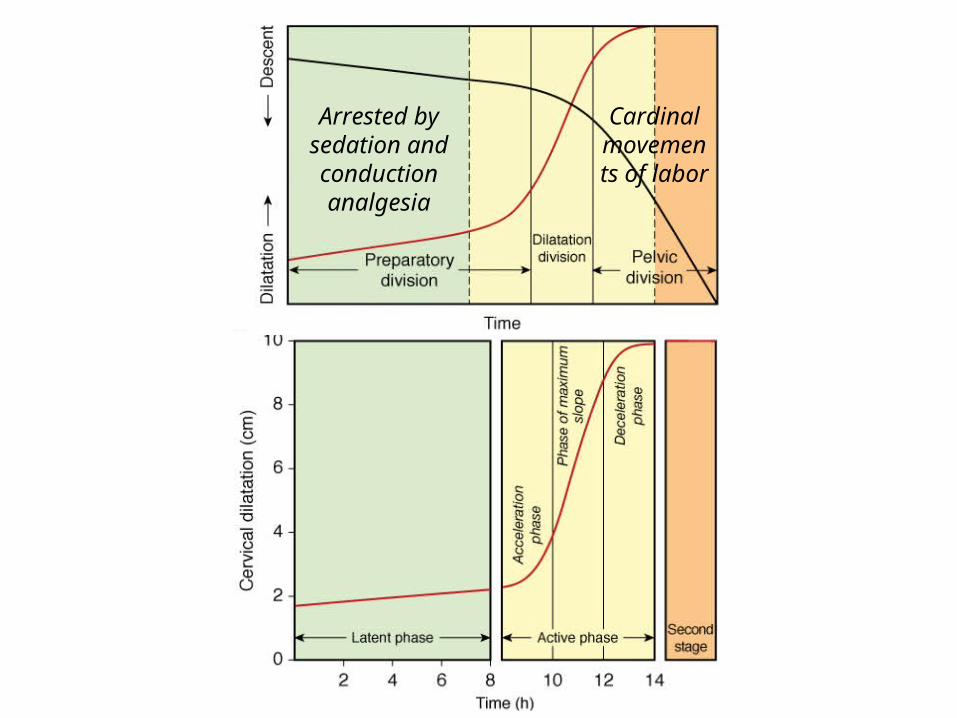
Arrested by sedation and conduction analgesia
Cardinal movements of labor
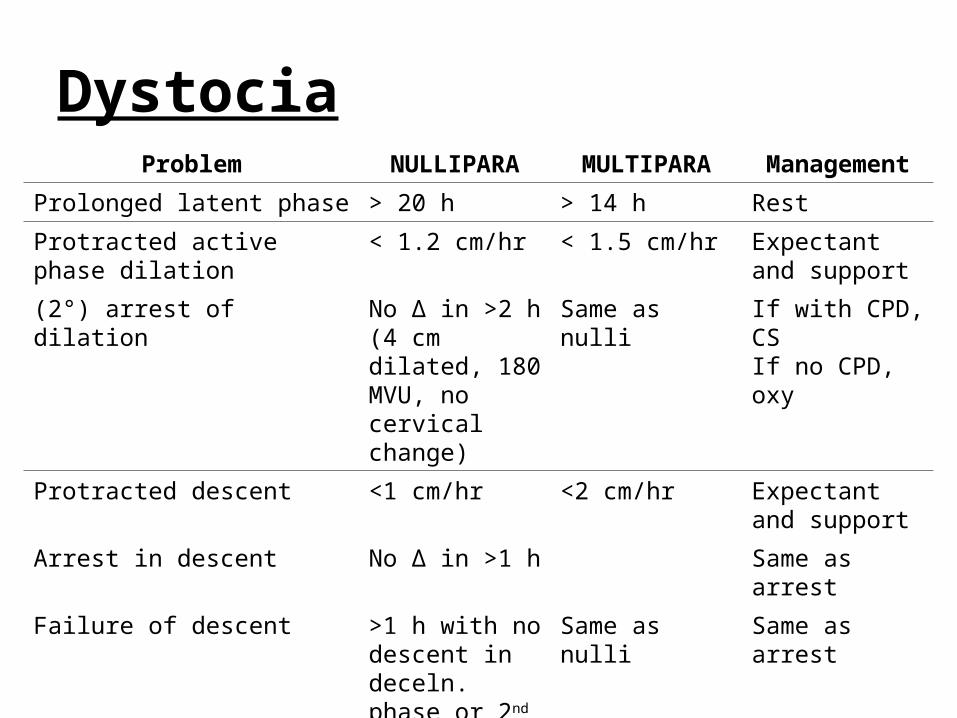
DystociaProblem NULLIPARA MULTIPARA Management
Prolonged latent phase > 20 h > 14 h Rest
Protracted active phase dilation < 1.2 cm/hr < 1.5 cm/hr Expectant and support
(2°) arrest of dilation No Δ in >2 h (4 cm dilated, 180 MVU, no cervical change)
Same as nulli If with CPD, CSIf no CPD, oxy
Protracted descent <1 cm/hr <2 cm/hr Expectant and support
Arrest in descent No Δ in >1 h Same as arrest
Failure of descent >1 h with no descent in deceln. phase or 2nd stage
Same as nulli Same as arrest
Prolonged deceleration phase >3 h >1 h Same as arrest

Electronic Fetal Monitoring
BFHRVariability
AccelerationsDecelerations

Electronic Fetal Monitoring
• Normal BFHR = 110-160
• Variability– Minimal: fluctuations of 5 bpm– Moderate: 6-25 bpm– Marked/Saltatory: > 25bpm
• Accelerations (2 or more)– At least 15 bpm x 15 sec-2 min in term (20 min strip)– At least 10 bpm x 10 sec in preterm (20-30 min strip)

Electronic Fetal Monitoring
• Decelerations (decrease 15 bpm, > 30 sec)– Early: head compression– Variable: cord compression (abrupt decrease)– Late: uteroplacental insufficiency– Prolonged: >2 but <10 min

3 cm/min.
1 minute
1cm/min.

Montevideo units are calculated by subtracting the baseline uterine pressure from the peak contraction pressure for each contraction in a 10-minute window and adding the pressures generated by each contraction. In the example shown, there were five contractions, producing pressure changes of 52, 50, 47, 44, and 49 mm Hg, respectively. The sum of these five contractions is 242 Montevideo units.
Montevideo Units

Cardinal Movements of Labor

• Engagement– biparietal diameter passes through the pelvic inlet
• Descent
• Flexion– results from descending head meeting resistance
(cervix, walls of pelvis, pelvic floor)– chin is brought closer to the fetal thorax– shorter suboccipitobregmatic diameter is substituted
for the longer occipitofrontal diameter
Cardinal Movements of Labor

• Internal rotation– occiput gradually moves anteriorly toward the symphysis
pubis (or less commonly, posteriorly toward the hollow of the sacrum)
• Extension– base of the occiput in direct contact with inferior margin of
the symphysis pubis– progressive distension of the perineum and vaginal
opening increasingly larger portion of the occiput gradually appears
– head is born as the occiput, bregma, forehead, nose, mouth, and finally the chin pass successively over the anterior margin of the perineum
Cardinal Movements of Labor

• External rotation– delivered head undergoes restitution
• if the occiput was originally directed toward the left, it rotates toward the left ischial tuberosity; if it was originally directed toward the right, the occiput rotates to the right
– followed by completion of external rotation to the transverse position– rotation of the fetal body – one shoulder is anterior behind the symphysis and the other is
posterior
• Expulsion– anterior shoulder appears under the symphysis pubis, and the
perineum soon becomes distended by the posterior shoulder– after delivery of the shoulders, the rest of the body quickly passes
Cardinal Movements of Labor



Asynclitism
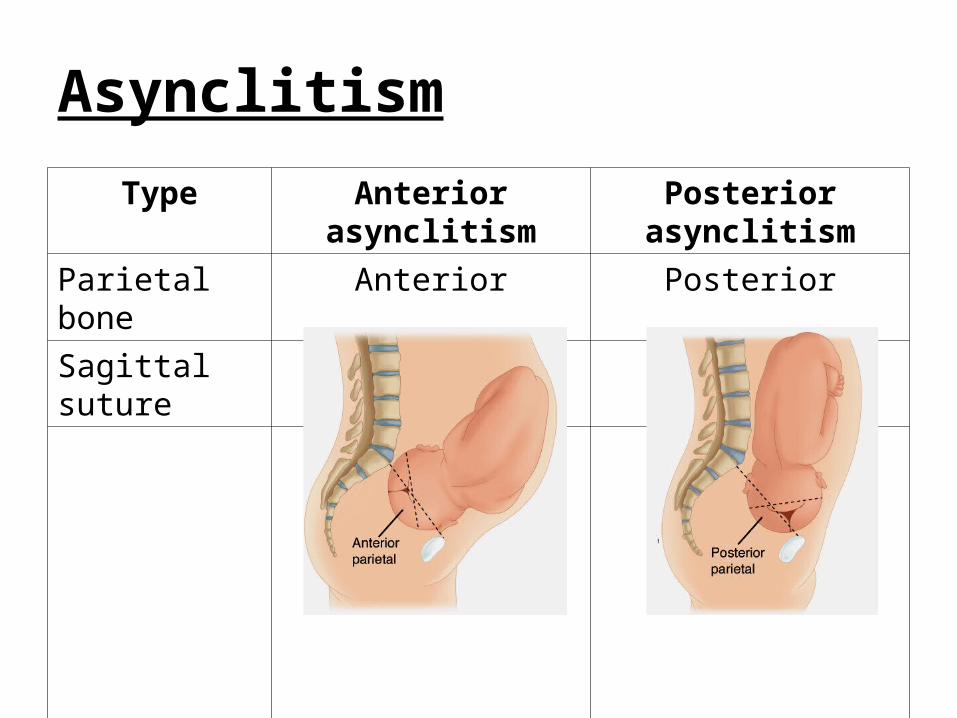
Type Anterior asynclitism Posterior asynclitismParietal bone Anterior PosteriorSagittal suture Posterior Anterior
Asynclitism

Active Management of the Third Stage of Labor

AMTSL
1. As soon as baby is out and you are sure there is no second baby, infuse oxytocin.
2. Apply controlled cord traction and suprapubic countertraction.
3. When placenta is at introitus, slowly rotate 360°.
4. Inspect placenta and membranes.5. Massage the uterus.

Instrument Identification

Rampley dressing forceps Foerster sponge holding forceps

Grave vaginal speculum Pederson vaginal speculum

Halsted Mosquito Micro ForcepsStraight / Curved
Kelly ForcepsStraight / Curved
Crile ForcepsStraight / Curved

Simpson Obstetrical Forceps Kielland Obstetrical Forceps
Piper Obstetrical Forceps

Pestalozza Obstetrical Curette
Backhaus towel forceps

Pudendal Nerve Block

• sensory innervation to the perineum, anus, and the more medial and inferior parts of the vulva and clitoris
• derived from ventral branches S2-S4• passes beneath the posterior surface of the
sacrospinous ligament just as the ligament attaches to the ischial spine– courses between the piriformis and coccygeus muscles – exits through the greater sciatic foramen in a location
posteromedial to the ischial spine– courses along obturator internus muscle within the
pudendal canal (Alcock canal), which is formed by splitting of the obturator fascia
Pudendal Nerve

• three terminal branches in the perineum:– dorsal nerve of the clitoris supplies the skin of the
clitoris– perineal nerve serves the muscles of the anterior
triangle and labial skin– inferior rectal branch supplies the external anal
sphincter, the mucous membrane of the anal canal, and the perianal skin
Pudendal Nerve

Knot Tying
Two-handOne-hand
Instrument

















