51
October 11, 2011 Texas Health Law Conference Ken Davis, MD Chief Medical Officer San Antonio Methodist Healthcare System Quality and Reimbursement: The New Payment World
| Date post: | 26-Dec-2015 |
| Category: |
Documents |
| Upload: | winifred-gilbert |
| View: | 213 times |
| Download: | 0 times |

October 11, 2011Texas Health Law Conference
Ken Davis, MDChief Medical Officer
San Antonio Methodist Healthcare System
Quality and Reimbursement: The New Payment World

The Truth
The public and payers demand care that is:– Accessible– Coordinated – Affordable– Evidenced-based– Free of avoidable complications– Transparent in clinical outcomes
This will require new systems of care delivery,
reimbursement and oversight
Who better than physicians to lead this change?

“If the rate of change on the outside exceeds the rate of change on the
inside, the end is near.”
Jack WelchFormer Chairman and CEO
General Electric Corp.
How Important Is The Rate Of Change?

2018 2019
Hospital Value-Based Purchasing (1-2%; Phased in over 4 Years)1.00% 1.25% 1.50% 1.75%
2016
2.00%
2011 2012 2013 2014 2015 2017
Hospital Acquired Conditions (1%)1.00%
Hospital Readmissions (1-3%; Phased in over 3 Years)1.00% 2.00% 3.00%
Total 2% 3.25% 5.5% 5.75% 6% ->
CMS Value-Based Purchasing:Linking Federal Reimbursement to Clinical Performance

Transformational Change
• Structure
• Measurement
• Leadership
• Structure– Organization– Care Process– EHR
• Measurement
• Leadership
Transformational Change

Methodist Healthcare, San Antonio Market
MHS Hospital Santa RosaMHS Surgery Center TexSanBaptist UniversitySTRIC Imaging Nix & SWG
Legend
343
43
4
43 43
5
43
6
$
Timberwood Park
Fair Oaks Ranch
Scenic Oaks
Cross Mountain
Helotes
China Grove
Live Oak
Windcrest
Kirby
Elmendorf
Somerset
Converse
Lackland AFB
Grey Forest
Lytle
Selma
Schertz
St. Hedwig
Cibolo
10
10
35
35 37
37
410
151
16
281
16
90
281
87
181
1604
1604
MethodistBoerneMedicalCenter
NortheastMethodistHospital
MethodistAmbulatory
SurgeryHospital
MetropolitanMethodistHospital
Methodist HospitalMethodist Heart Hospital
Methodist Children’s HospitalMethodist Specialty &
Transplant Hospital
MethodistStone OakHospital(2008)
MASC - MC
MASC - NC
STRIC
STRIC (2 Loc)
STRIC (8 Loc)
STRIC (2 Loc)
STRIC
STRIC
STRIC
STRIC
- 8 Hospitals- 2000 beds- HCA/Meth Min- 2700 physicians

MSOH MH MSTH MCH MMH MNE MTHMASH
Medical Board
Community Board
MHS Governing Board: MHM/HCA
Quality ImprovementPhysician ResourcePt Care Exp and SafetyMedical recordsTransfusionBioethicsCancer
MECs
CredentialsInfection ControlPharmacy & TherapeuticsPeripheral Vasc InterventionSpecial Care Utilization Review
BoardBoard
MHS Medical Staff Structure

Cardiovascular (Cardiology, CV Surgery, Heart Transplant, PV) Surgery (General, Trauma, Bariatrics, Renal/Liver Transplant) Hematology/Oncology (Adult and Pediatric BMT) Medicine (FP, IM, Hospitalists, Intensivists) Neurosciences (Neurology/ Neurosurgery) Orthopedics/Spine Surgery Pediatrics Women’s Services Psychiatry Post-Acute Care – Home Health, Rehab, SNF, Pharmacy Ambulatory Clinic Care
Emergency Svcs. Anesthesia Radiology Pathology
System Service Lines
Supporting Services – may have representatives on multiple Service Lines

Customer Sub-segmentation Requirements Data Source
Patients/Families In-patientOut-PatientEmergencyClinics
*Care Measures: Process Outcomes Efficiency Safety Experience
MHS Monthly Quality Reports
Staff VolunteersEmployedStudents
Opportunity to advance/learnCommitment to qualityConfidence in senior leadersTreated with respect
Employee Survey Results
Physicians AdmittingNon-admittingContractedEmployedPHONon-affiliatedIn Training
Care Measures: Process Outcomes Efficiency Safety ExperienceWorkflow EfficiencyInput into strategic planning and day-to-day operationsCommunicationCompetent Staff
MHS Quality Reports
Premier Efficiency ScoresSWOT analysis by SL
Phys Engagement SurveyMHS Competency Data
Customer Segmentation
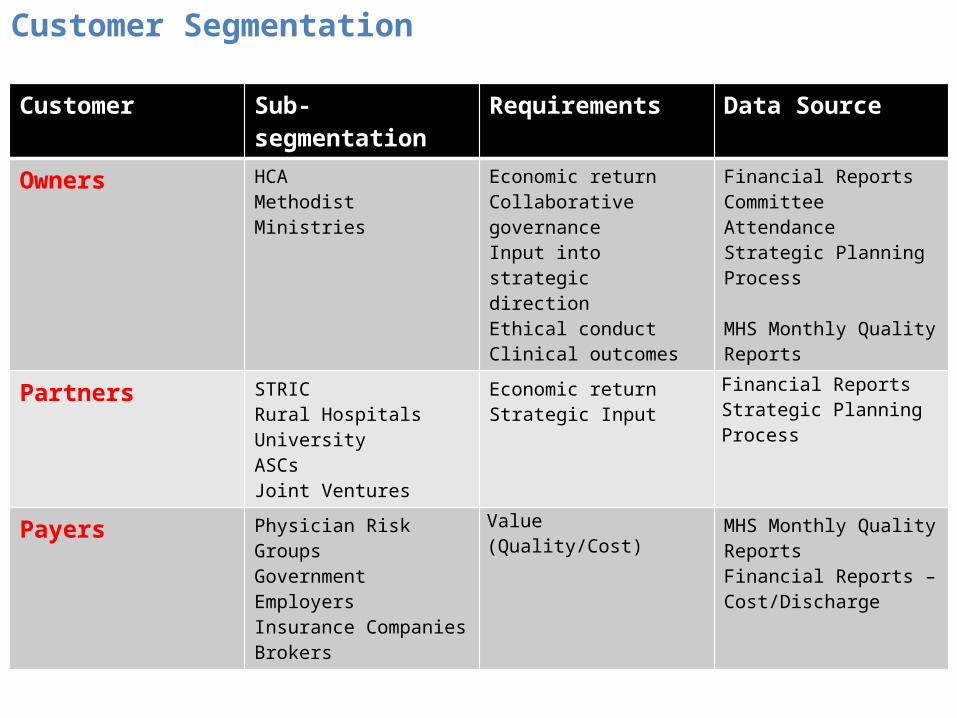
Customer Sub-segmentation Requirements Data Source
Owners HCAMethodist Ministries
Economic returnCollaborative governanceInput into strategic directionEthical conductClinical outcomes
Financial ReportsCommittee AttendanceStrategic Planning Process MHS Monthly Quality Reports
Partners STRICRural HospitalsUniversityASCsJoint Ventures
Economic returnStrategic Input
Financial ReportsStrategic Planning Process
Payers Physician Risk GroupsGovernmentEmployersInsurance CompaniesBrokers
Value (Quality/Cost) MHS Monthly Quality ReportsFinancial Reports – Cost/Discharge
Customer Segmentation
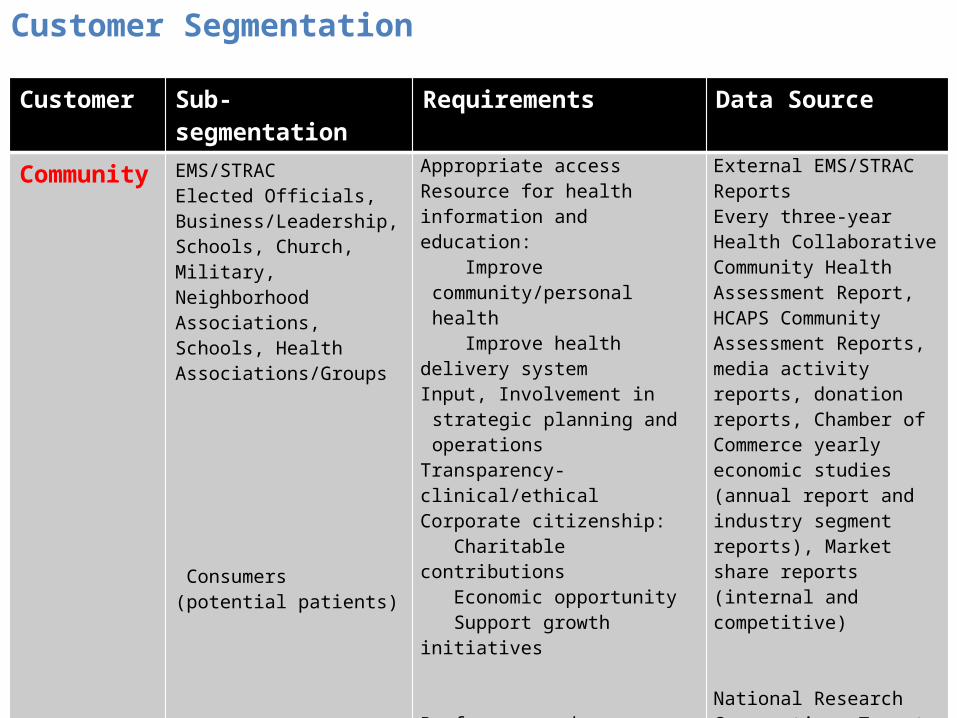
Customer Sub-segmentation Requirements Data Source
Community EMS/STRACElected Officials, Business/Leadership, Schools, Church, Military, Neighborhood Associations, Schools, Health Associations/Groups Consumers (potential patients) Media (awareness and perception)
Appropriate accessResource for health information and education: Improve community/personal
health Improve health delivery systemInput, Involvement in strategic
planning and operationsTransparency- clinical/ethicalCorporate citizenship: Charitable contributions Economic opportunity Support growth initiatives
Preference and perception for/and of Methodist services, access to services (e.g., physician referral, health information)
High regard for services, first stop for health information
External EMS/STRAC ReportsEvery three-year Health Collaborative Community Health Assessment Report, HCAPS Community Assessment Reports, media activity reports, donation reports, Chamber of Commerce yearly economic studies (annual report and industry segment reports), Market share reports (internal and competitive)
National Research Corporation, Target SA – preference and perception reports, Contact Center internal reports
Monthly Media Valuation report and internal competitive analysis
Customer Segmentation

Methodist Healthcare Strategic and Business Planning Process• Serving Humanity to Honor God• Supporting the health status of
the community• Constantly improving quality
Mission
• A commitment to greatness• Creating healing experiences• Never-ending improvement• Preference for MHS by all served
Vision
Values
Review of Organization’s Critical Issues
Market Environment
Scan
Understanding Customer Demands
SWOT Analysis Board, Senior Leaders,
Physicians, Staff, Patients/Families,
Community, Payers, Owners, Partners,
Suppliers
How To:Maximize Strengths
Minimize Weaknesses Seize Opportunities Eliminate Threats
Breakthrough Strategies
People Service Quality Growth Finance Community
Development of System Yearly Business Plan
People Service Quality Growth Finance Community
Validation and EducationAcross the Enterprise
Budgeting Process
Finalize and
Deploy Yearly
Business Plan
Continuous Performance
Review
Validation and EducationAcross the Enterprise
Validation and EducationAcross the Enterprise
Evaluate and Improve
Strategic and Business Plan Process, and Deployment
Development of Facility
Yearly Business Plans
• Creating an appropriate work environment
• How we treat each other• How we treat our customers
1st Q
4th Q
3rd Q
2nd Q
2nd Q
90 day Action Plans
Plan Analysis Plan Development Plan Deployment

Methodist Healthcare Ministries of South Texas
Serve low income and uninsured families in South Texas
72 county service area Clinics:
– Primary care medical and dental– School-based– Church-based– Counseling, case management
social services 1998 – 2010
– $ 340 million– 3.24 million client encounters
2010 – $ 52 million– 516,000 client encounters
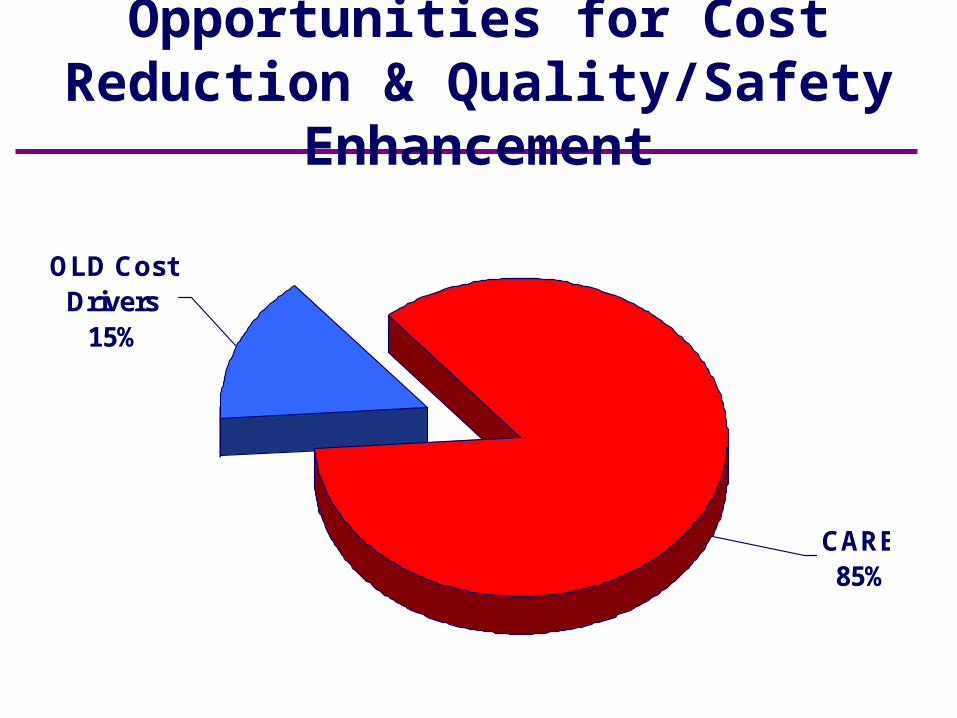
Opportunities for Cost Reduction & Quality/Safety Enhancement
CARE85%
OLD Cost Drivers
15%
Creating a Process Driven Organization
Everything we do is:
Defined - by customer need
Measured - by repeatable data
Improved - in a structured methodology–DMAIC
Aligned - across the organization
Improving customers’ Value (Quality/Cost)
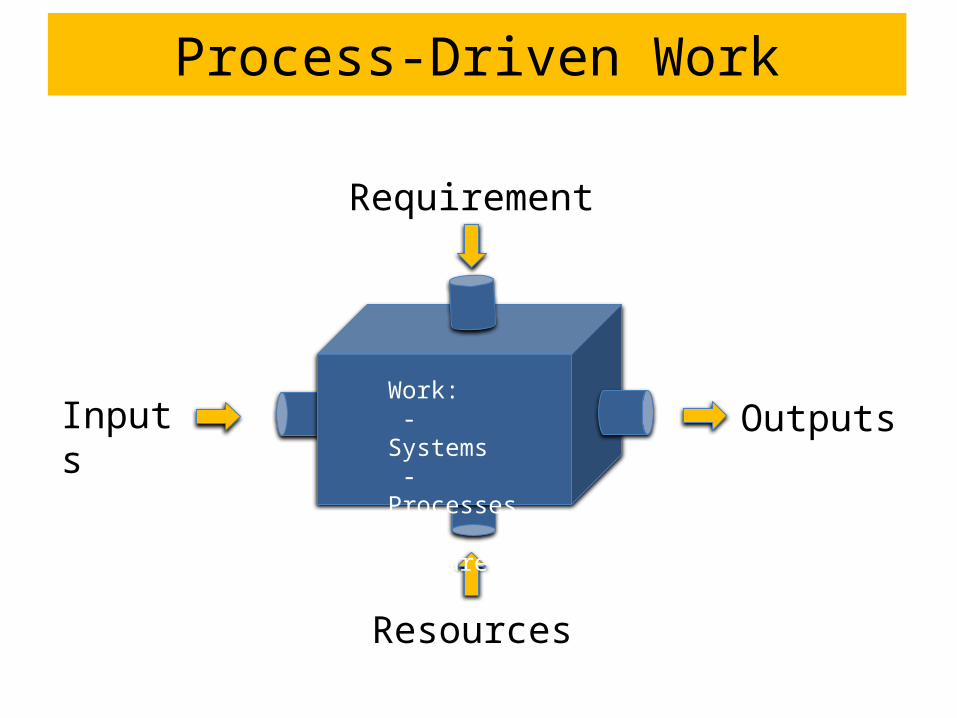
Process-Driven Work
Inputs
Resources
Requirements
OutputsWork: - Systems - Processes - Measures
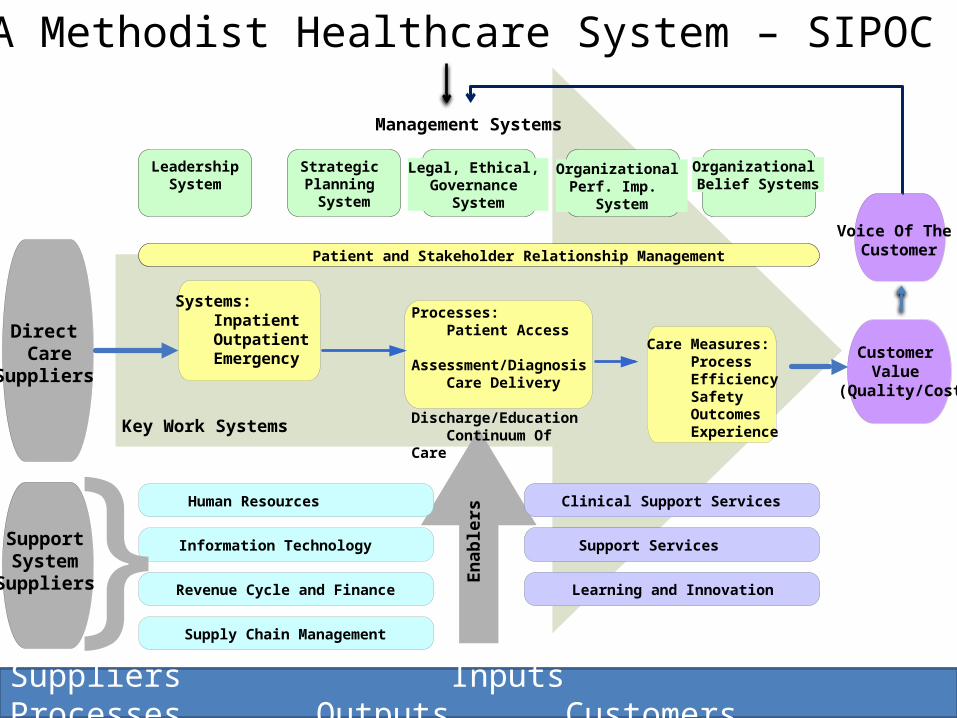
SA Methodist Healthcare System – SIPOC
Customer Value
(Quality/Cost
Key Work Systems
Enab
lers
Human Resources
Information Technology
Revenue Cycle and Finance
Supply Chain Management
Facilities and Infrastructure
Information Technology
Public Safety
SupportSystem
Suppliers
Management Systems
LeadershipSystem
Organizational Belief Systems
Strategic Planning System
Organizational Perf. Imp.
System
Clinical Support Services
Support Services
Learning and Innovation
Direct Care
Suppliers
Patient and Stakeholder Relationship Management
Processes: Patient Access Assessment/Diagnosis Care Delivery Discharge/Education Continuum Of Care
Care Measures: Process Efficiency Safety Outcomes Experience
Systems: Inpatient Outpatient Emergency
}
Voice Of The Customer
Legal, Ethical, Governance
System
Suppliers Inputs Processes Outputs Customers

Individual Patient Care
Standard Care by Protocol
Direct Physician Intervention

MHS Order Sets and Protocols
Additional Review
by EBCT and Specialty
Group
Implement Measure*
CreateRevisePilot
Medical Record Committee
Medical
Board
*evaluate adoption, periodic review, revision based on clinician feedback
yes
no
Evidence Based Care Team
Multidisciplinary System-wide
Approval

• Lab, Pathology, Microbiology• Radiology, Cardiology, General
Transcription• Filter Preferences
– Result, Patient Type, Physician Role– No Duplicates
• Private, Secure, Audited Exchange
• Browser View• Filter / Sort• Batch Print
HL7
EMR
Hospital Assistant
Fir
ewal
l
Practice – No EMR
EMR
• Discrete Data• Directly Into
Chart or Worklist
• Alerts & Flowsheet
• Image Data• Manual
Indexing• Filename
Based on Patient Data
Office Assistant
Practice – EMR, No HL7
Practice – EMR / HL7
Firew
all
Data ExchangeServer
MHS: Hospital-Clinic Data Exchange Server

HITECH Timeline
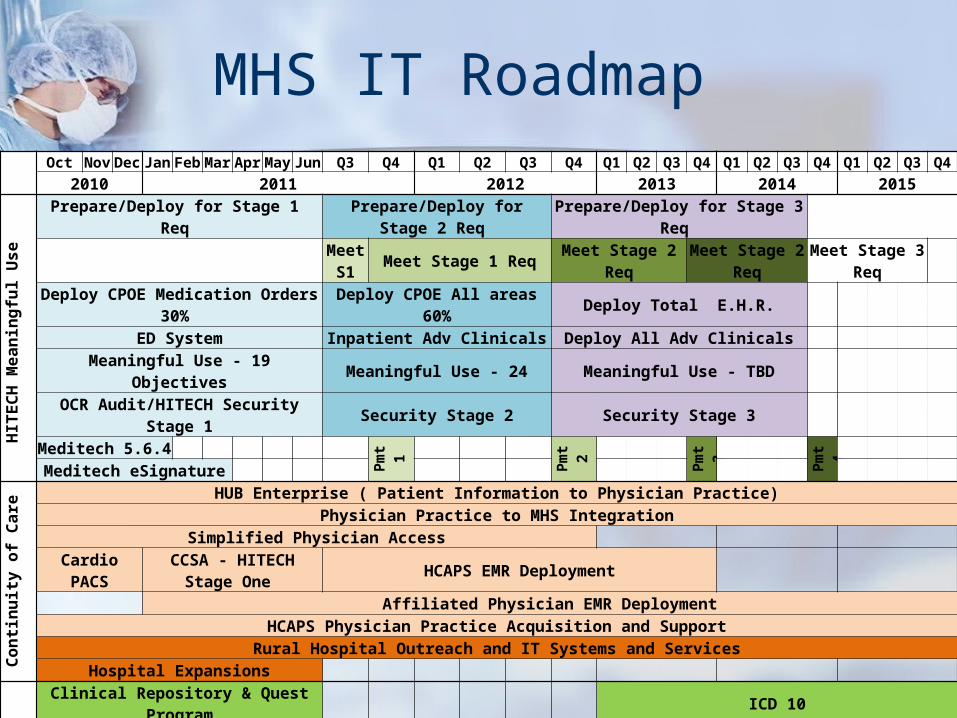
MHS IT Roadmap Oct Nov Dec Jan Feb Mar Apr May Jun Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
2010 2011 2012 2013 2014 2015
HITECH
Meaningf
ul Use
Prepare/Deploy for Stage 1 Req Prepare/Deploy for Stage 2 Req Prepare/Deploy for Stage 3 Req
Meet S1 Meet Stage 1 Req Meet Stage 2 Req Meet Stage 2 Req Meet Stage 3 Req
Deploy CPOE Medication Orders 30% Deploy CPOE All areas 60% Deploy Total E.H.R. ED System Inpatient Adv Clinicals Deploy All Adv Clinicals
Meaningful Use - 19 Objectives Meaningful Use - 24 Meaningful Use - TBD OCR Audit/HITECH Security Stage 1 Security Stage 2 Security Stage 3
Meditech 5.6.4 Pmt 1
Pmt 2 Pmt
3 Pmt
4
Meditech eSignature
Continuity
of Care
HUB Enterprise ( Patient Information to Physician Practice)Physician Practice to MHS Integration
Simplified Physician Access Cardio PACS CCSA - HITECH Stage One HCAPS EMR Deployment
Affiliated Physician EMR DeploymentHCAPS Physician Practice Acquisition and Support
Rural Hospital Outreach and IT Systems and ServicesHospital Expansions
Core &
Support Clinical
Systems
Clinical Repository & Quest Program ICD 10Real-time Location - Assets Real-time Location System - Patients
Automate and Streamline Workflow to Improve Clinician EfficiencyCSG Clinical Transformation
Bar Coded Transfusion Clinical Monitoring Integration Staff Scheduling
Medical Staff (Cactus) Case Management (Midas)
Facility Construction Projects

• Structure
• Measurement– Care
• Process• Outcome• Efficiency• Safety• Experience
• Leadership
Transformational Change

Clinical Quality Measures
Care– 1. Process – 2. Outcomes– 3. Efficiency– 4. Safety– 5. Experience
Each measure segmented by hospital, clinical service, nursing unit and physician

Profiles: - System - Service Line - Hospital - Nursing Unit - Practitioner

2727
Composite Quality Measures
Care:–Process
–Outcomes
–Efficiency
–Safety
–Experience

1Q
07
2Q
07
3Q
07
4Q
07
1Q
08
2Q
08
3Q
08
4Q
08
1Q
09
2Q
09
3Q
09
4Q
09
1Q
10
2Q
10
3Q
10
4Q
10
1Q
11
2Q
11
P
3Q
11
P
80%
85%
90%
95%
100%
81.8%
84.3%
86.9% 87.4%
92.6% 92.5%
95.1% 95.5%96.3% 96.6% 97.1% 96.8%
97.5%96.6%
97.7% 98.0% 97.9% 97.8%98.9%
All CMS/HQA Measures in Each Facility Rolled intoOne Composite Score
Quarter
good

2929
Composite Quality Measures
Care:–Process
–Outcomes
–Efficiency
–Safety
–Experience

Acute Care Inpatient Mortality Rate

Methodist Hospital (5 in 1) ReadmissionsJune 1, 2007 – June 30, 2010
Rate per 100 AdmissionsHospitalcompare.gov
MH CMS Avg.
AMI(991 pts)
18.7 19.8
HF(2124 pts)
22.8* 24.8
PN(1444 pts)
17 18.4
* Statistically different

3232
Composite Quality Measures
Care:–Process
–Outcomes
–Efficiency
–Safety
–Experience
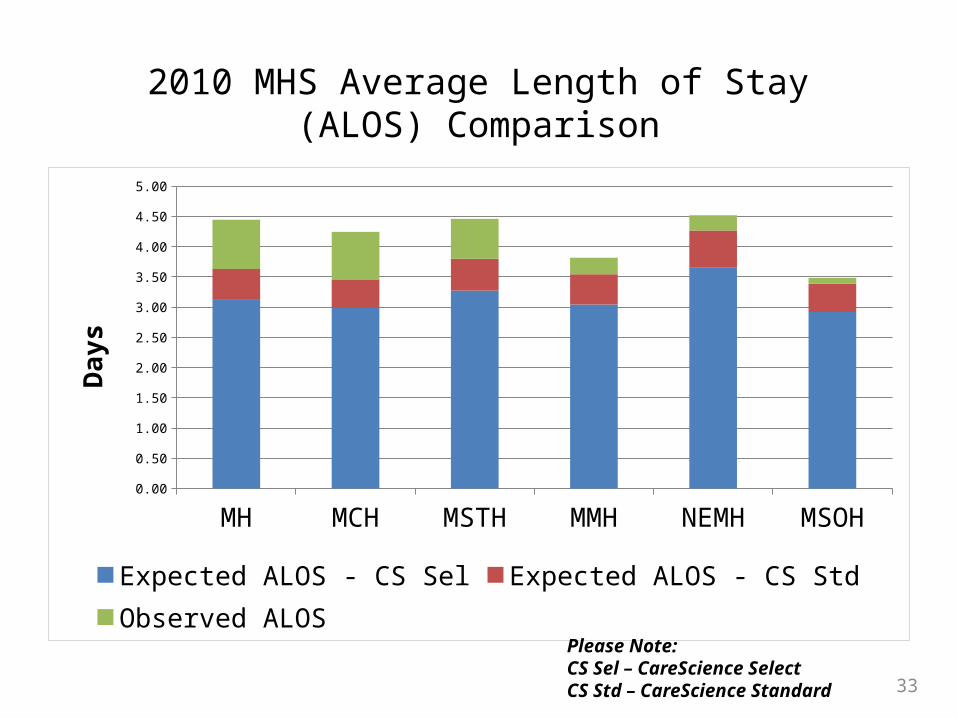
2010 MHS Average Length of Stay (ALOS) Comparison
MH MCH MSTH MMH NEMH MSOH0.00
0.50
1.00
1.50
2.00
2.50
3.00
3.50
4.00
4.50
5.00
Expected ALOS - CS Sel Expected ALOS - CS StdObserved ALOS
Day
s
Please Note:CS Sel – CareScience SelectCS Std – CareScience Standard 33
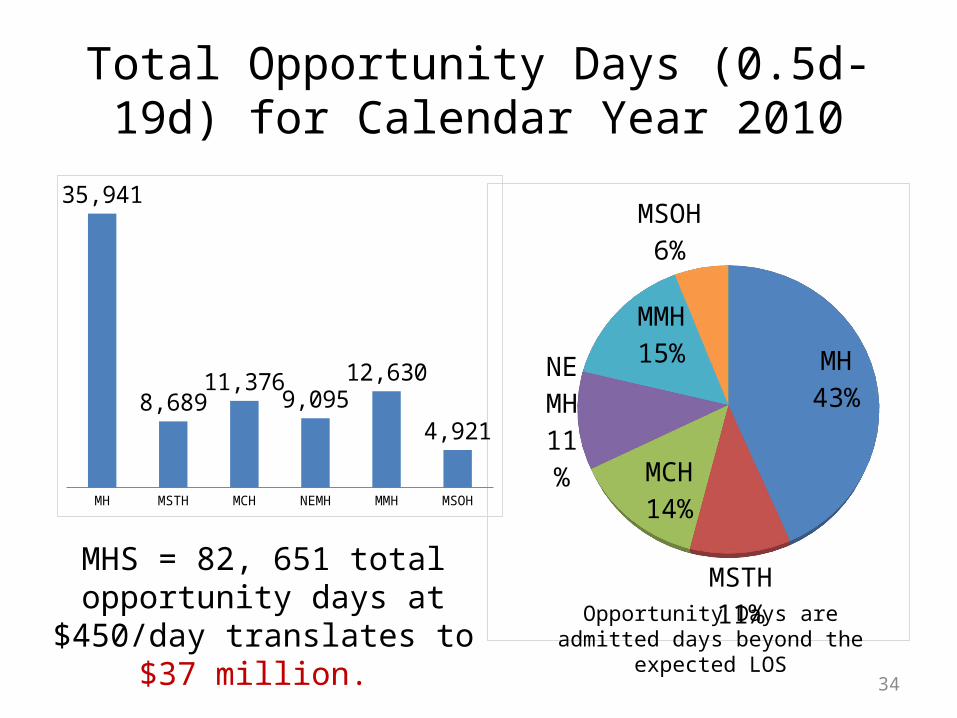
Total Opportunity Days (0.5d-19d) for Calendar Year 2010
• ALOS Observed vs. ALOS Expected (CS Std)
MH43%
MSTH11%
MCH14%
NEMH11%
MMH15%
MSOH6%
MH MSTH MCH NEMH MMH MSOH
35,941
8,689 11,376
9,095 12,630
4,921
MHS = 82, 651 total opportunity days at $450/day translates to
$37 million. Opportunity Days are admitted days
beyond the expected LOS
34

3535
Composite Quality Measures
Care:–Process
–Outcomes
–Efficiency
–Safety
–Experience
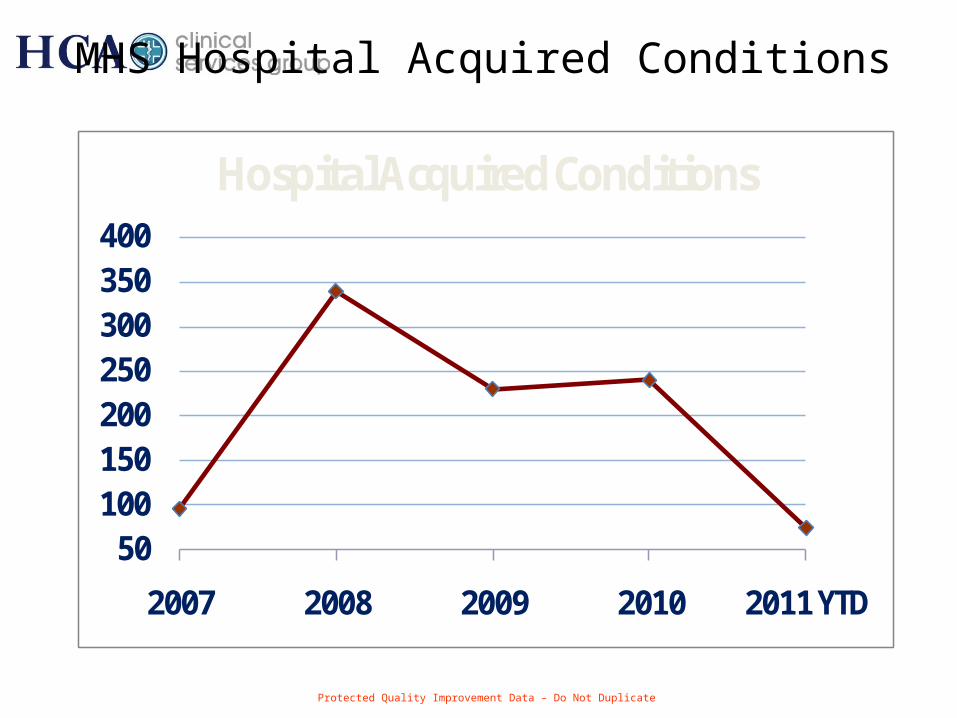
50100150200250300350400
2007 2008 2009 2010 2011 YTD
Hospital Acquired Conditions
MHS Hospital Acquired Conditions

3737
Composite Quality Measures
Care:–Process
–Outcomes
–Efficiency
–Safety
–Experience

Service – HCAHPS Composite

• Structure
• Measurement
• Leadership–Culture–Training–Measurement
Transformational Change
Definition: Leadership Culture
How leaders influence others to get the work done
Organizational culture where:– leaders use their skills of influencing people – to enthusiastically work towards goals
identified as being for the common good –with character that inspires confidence
James C. Hunter

Definition: Leadership Culture

Transformational Change
Greatest Health System Leadership Cultural Change:
Engaging Clinicians
Empowering Clinicians


MHS Leadership:Alignment/Deployment
GOALS System Hospital Department or Svc. Line
Unit Individual
People
Service
Quality
Finance
Growth
Community
One System goal per Pillar Goals tied to System Pillar goals LEM goals

Leadership - Skills Training
Management Leadership Training
Physician Leadership Training
Nursing Outcomes College
Board Education and Planning Retreats
Clinical Outcome Manager Training – (Clinical Nurse Leader)

Physician Leadership Development:“Training Physicians for Empowered Leadership Positions”
Elected Physician leaders and those delegated by MECs
Two year leadership training program Topics:
– Comparative Clinical Outcome Measures– Servant Leadership– Crucial Conversations– Scripted Patient Communication “AIDET”– High Performing Teams– Integrated Delivery Systems– Creating a Safety Culture– Strategic Planning– Hospital Finance– Health Law– Value Based Purchasing– Others…

Leadership Model:Servant Leadership
Character Development
Listening
Accountability
Results
– Not only What you achieve , but How you achieve it

Leadership Skills:Crucial Conversations
Patterson, Kerry. Grenny, Joseph. McMillan, Ron. Switzler, Al. Crucial Conversations, Tools for Talking When Stakes are High. McGraw Hill 2002.
Dialogue (free flow of information)
Group decision
Shared pool of information
Commitment to act

Leadership 360 Feedback
Honest- Is someone people can trust - Is a leader people feel confident following
Respectful- Treats people with respect - Does not engage in backstabbing, (talking behind backs, “managing down”)- Does not embarrass or punish staff in front of others
Committed- Makes clear to staff what is expected - Holds staff accountable for care standards - Works with staff in a team approach - Holds others accountable for care standards
Humble- Is a good listener - Is not overly controlling or domineering
Adapted from James C. Hunter “The Worlds Most Powerful Leadership Principle”

Leadership 360 Feedback
Patient- Shows patience and self-control with others - Has a consistent manner and stays calm
Kind- Shows appreciation to others - Gives encouragement to others - Gives credit to those who deserve it
Selfless- Meets legitimate needs (as opposed to wants) of others - Is sensitive to implications of their decisions on others
Forgiving- Is able to forgive mistakes and not hold grudges - Spends time on the problem, not assigning blame
What are the greatest leadership strengths/skills this physician possesses?
What leadership skills does this physician need to work on and improve?
Adapted from James C. Hunter “The Worlds Most Powerful Leadership Principle”
Ask yourself everyday:
“Are you trying to do something or be somebody?”
Leadership Culture and Accountability

















