CASE REPORT Ocular coherence tomography findings in a case of choroideremia Savleen Kaur • Nishant Sachdev Received: 7 December 2012 / Accepted: 18 March 2013 / Published online: 29 March 2013 Ó Springer Science+Business Media Dordrecht 2013 Introduction Choroideremia is an X-linked progressive chorioret- inal dystrophy [1]. It usually affects males who develop early-onset night blindness, restriction of the peripheral visual field, and a decrease in central visual acuity, leading to blindness in the advanced stages of the disease. Fundus examination shows a progressive atrophy of the choroid and retinal pigment epithelium. Spectral-domain optical coherence tomography (SD-OCT) is the latest modality for the morphological analysis of the retinal layers. Due to the paucity of data on the OCT analysis of choroideremia (method of search: pubmed) we decided to carry out a similar study in our patient. Case report A 22-year-old old male presented to our out-patient department with a history of nyctalopia and decreased central vision. Visual fields demonstrated variable peripheral field restriction, and due to the character- istic fundus findings (including choroidal and retinal pigment epithelium degenerative changes throughout the posterior pole and mid-peripheral retina) a diag- nosis of choroideremia was made (Fig. 1, 2). SD-OCT revealed increased retinal thickening (mean retinal thickness 420 lm) and cystic spaces in the retina in both eyes (Fig. 3). The cystic spaces ranged from small cysts in the outer plexiform layer to huge cysts confirming cystoid macular edema (CME). Clinical examination failed to detect cystic spaces. Discussion Earlier reports of choroideremia revealed a positive correlation between retinal thickness and choriocap- illaris preservation and advanced stages being marked by chorioretinal atrophy [2]. Another study revealed subtle retinal pigment epithelium irregularities with attenuation more pronounced outside the macular region on OCT [3]. The presence of cystic macular changes of variable degrees on SD-OCT with an overall prevalence of 62.5 % in at least one eye and 50 % in both eyes was first reported in 2011 [4]. Cystic changes ranging from microcysts to diffuse macular edema along with rosette-like structures were found in some patients. The authors were unable to find any previous reports of choroideremia (Fig. 3). S. Kaur Á N. Sachdev PGIMER, Chandigarh, Punjab, India S. Kaur (&) 47 Shakti Nagar, Jalandhar 144001, Punjab, India e-mail: [email protected]123 Int Ophthalmol (2014) 34:297–299 DOI 10.1007/s10792-013-9767-x
Transcript
CASE REPORT
Ocular coherence tomography findings in a caseof choroideremia
Savleen Kaur • Nishant Sachdev
Received: 7 December 2012 / Accepted: 18 March 2013 / Published online: 29 March 2013
� Springer Science+Business Media Dordrecht 2013
Introduction
Choroideremia is an X-linked progressive chorioret-
inal dystrophy [1]. It usually affects males who
develop early-onset night blindness, restriction of the
peripheral visual field, and a decrease in central visual
acuity, leading to blindness in the advanced stages of
the disease. Fundus examination shows a progressive
atrophy of the choroid and retinal pigment epithelium.
Spectral-domain optical coherence tomography
(SD-OCT) is the latest modality for the morphological
analysis of the retinal layers. Due to the paucity of data
on the OCT analysis of choroideremia (method of
search: pubmed) we decided to carry out a similar
study in our patient.
Case report
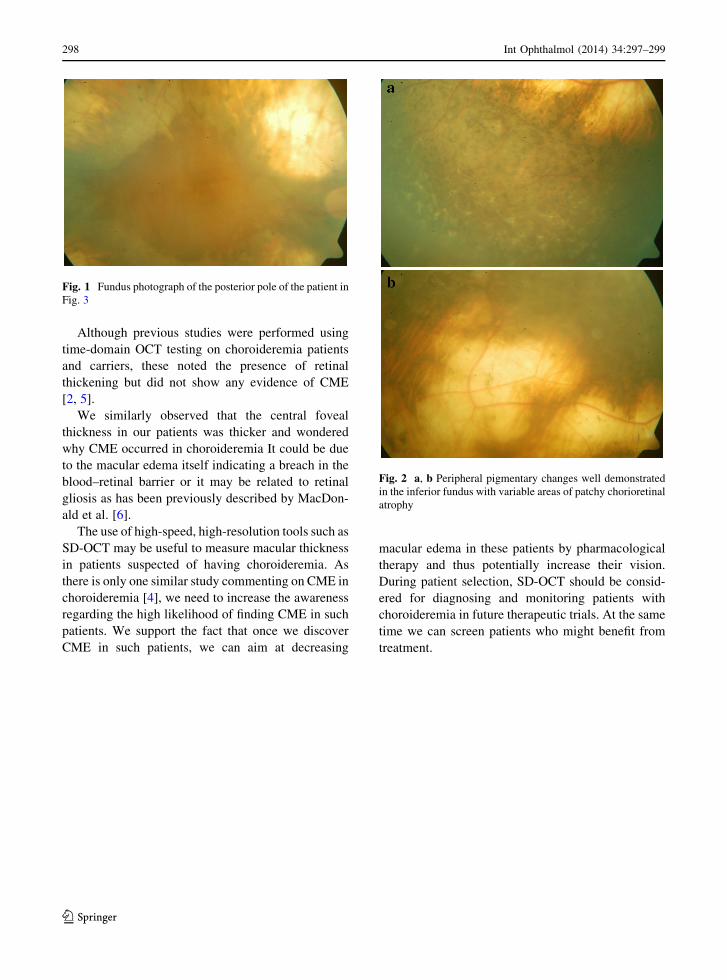
A 22-year-old old male presented to our out-patient
department with a history of nyctalopia and decreased
central vision. Visual fields demonstrated variable
peripheral field restriction, and due to the character-
istic fundus findings (including choroidal and retinal
pigment epithelium degenerative changes throughout
the posterior pole and mid-peripheral retina) a diag-
nosis of choroideremia was made (Fig. 1, 2).
SD-OCT revealed increased retinal thickening
(mean retinal thickness 420 lm) and cystic spaces in
the retina in both eyes (Fig. 3). The cystic spaces
ranged from small cysts in the outer plexiform layer to