Annals of the Rheumatic Diseases 1985, 44, 610-613 Oesophageal dysfunction in patients with primary Sjogren' s syndrome E B TSIANOS, C D CHIRAS, A A DROSOS, AND H M MOUTSOPOULOS From the Department of Medicine, University of loannina, Medical School, loannina, Greece SUMMARY Oesophageal motility was studied in 22 patients with primary Sjogren's syndrome and 20 normal volunteers. Oesophageal dysfunction was detected in eight of the 22 patients (36-4%) with primary Sjogren's syndrome. No abnormalities were detected in the normal subjects. Individual analysis of the oesophageal motility studies showed different patterns of oesophageal dysfunction: aperistalsis (three patients), triphasic tertiary contractions (two patients), frequent non-peristaltic contractions (two patients), and low contractions (one patient). These oesophageal abnormalities did not correlate with the parotid flow rate, the degree of inflammatory infiltrate of the minor salivary glands, the extraglandular manifestations, or the presence of autoantibodies. Key words: Raynaud's phenomenon, dysphagia. Dysphagia is a common complaint of patients with primary Sjogren's syndrome. Despite that, studies of the oesophageal function in these patients are limited. In 1964 Stevens et al. studying oesophageal function in connective tissue disorders had included three patients with Sjogren's syndrome. In their work, however, it is not clear whether or not the patients with Sjogren's syndrome had any dysfunc- tion in the oesophageal motility.2 In 1976 Ramirez- Mata et al. observed that nine out of 10 patients with primary Sjogren's syndrome had a characteristic pattern of abnormal oesophageal motility.3 In the present study we have found that the oesophageal motility is affected in one third of patients with primary Sjogren's syndrome. The oesophageal dysfunction does not follow any charac- teristic pattern and does not correlate with clinical, histological, or serological parameters. Patients and methods Twenty-two female patients with primary Sjogren's syndrome were studied. Their ages ranged from 33 to 81 years (average 52-7±12-2 (SD) years). The diagnosis of Sjogren's syndrome was based on xerostomia (decreased parotid flow rate) and kera- Accepted for publication 5 March 1985. Correspondence to Dr E B Tsianos, Department of Medicine, Medical School, University of Ioannina, 453 32 loannina Greece. toconjunctivitis sicca (punctate corneal ulcers on slit-lamp examination and abnormal Schirmer's test).4 In all patients the diagnosis was confirmed by lip biopsy.5 None of these patients had other associated autoimmune disease. Eight of the 22 patients with Sjogren's syndrome had extraglandu- lar manifestations (Raynaud's phenomenon, lym- phadenopathy, splenomegaly, interstitial pneumoni- tis, vasculitis). The sera of all these patients were tested for rheumatoid factor (RF) titre and anti- bodies to Ro(SSA) and La(SSB) cellular antigens as previously described.6 Twenty normal volunteers had an oesophageal manometric study. Their ages ranged from 22 to 74 years (average 43-7±15-2 (SD) years). In all patients and normal volunteers the oesophageal manometric study was done after an overnight fast by the step pull-through method,7 which has been modified by us. MANOMETRIC PROCEDURE A solid state catheter with built-in three double pressure sensors was passed into the stomach through the nose. The three pressure sensors were spaced at 5 cm intervals and were oriented radially at angles of 600 to each other. The pressure sensing catheter generates voltages which were transmitted directly to a Beckman R 511 A multichannel ink recorder. Respiration and deglutition were moni- 610 copyright. on March 12, 2020 by guest. Protected by http://ard.bmj.com/ Ann Rheum Dis: first published as 10.1136/ard.44.9.610 on 1 September 1985. Downloaded from
Transcript
Annals of the Rheumatic Diseases 1985, 44, 610-613
Oesophageal dysfunction in patients with primarySjogren' s syndromeE B TSIANOS, C D CHIRAS, A A DROSOS, AND H M MOUTSOPOULOS
From the Department of Medicine, University of loannina, Medical School, loannina, Greece
SUMMARY Oesophageal motility was studied in 22 patients with primary Sjogren's syndrome and20 normal volunteers. Oesophageal dysfunction was detected in eight of the 22 patients (36-4%)with primary Sjogren's syndrome. No abnormalities were detected in the normal subjects.Individual analysis of the oesophageal motility studies showed different patterns of oesophagealdysfunction: aperistalsis (three patients), triphasic tertiary contractions (two patients), frequentnon-peristaltic contractions (two patients), and low contractions (one patient). Theseoesophageal abnormalities did not correlate with the parotid flow rate, the degree ofinflammatory infiltrate of the minor salivary glands, the extraglandular manifestations, or thepresence of autoantibodies.
Key words: Raynaud's phenomenon, dysphagia.
Dysphagia is a common complaint of patients withprimary Sjogren's syndrome. Despite that, studiesof the oesophageal function in these patients arelimited. In 1964 Stevens et al. studying oesophagealfunction in connective tissue disorders had includedthree patients with Sjogren's syndrome. In theirwork, however, it is not clear whether or not thepatients with Sjogren's syndrome had any dysfunc-tion in the oesophageal motility.2 In 1976 Ramirez-Mata et al. observed that nine out of 10 patients withprimary Sjogren's syndrome had a characteristicpattern of abnormal oesophageal motility.3
In the present study we have found that theoesophageal motility is affected in one third ofpatients with primary Sjogren's syndrome. Theoesophageal dysfunction does not follow any charac-teristic pattern and does not correlate with clinical,histological, or serological parameters.
Patients and methods
Twenty-two female patients with primary Sjogren'ssyndrome were studied. Their ages ranged from 33to 81 years (average 52-7±12-2 (SD) years). Thediagnosis of Sjogren's syndrome was based onxerostomia (decreased parotid flow rate) and kera-
Accepted for publication 5 March 1985.Correspondence to Dr E B Tsianos, Department of Medicine,Medical School, University of Ioannina, 453 32 loannina Greece.
toconjunctivitis sicca (punctate corneal ulcers onslit-lamp examination and abnormal Schirmer'stest).4 In all patients the diagnosis was confirmed bylip biopsy.5 None of these patients had otherassociated autoimmune disease. Eight of the 22patients with Sjogren's syndrome had extraglandu-lar manifestations (Raynaud's phenomenon, lym-phadenopathy, splenomegaly, interstitial pneumoni-tis, vasculitis). The sera of all these patients weretested for rheumatoid factor (RF) titre and anti-bodies to Ro(SSA) and La(SSB) cellular antigens aspreviously described.6Twenty normal volunteers had an oesophageal
manometric study. Their ages ranged from 22 to 74years (average 43-7±15-2 (SD) years).
In all patients and normal volunteers theoesophageal manometric study was done after anovernight fast by the step pull-through method,7which has been modified by us.
MANOMETRIC PROCEDUREA solid state catheter with built-in three doublepressure sensors was passed into the stomachthrough the nose. The three pressure sensors werespaced at 5 cm intervals and were oriented radiallyat angles of 600 to each other. The pressure sensingcatheter generates voltages which were transmitteddirectly to a Beckman R 511 A multichannel inkrecorder. Respiration and deglutition were moni-
610
copyright. on M
arch 12, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.44.9.610 on 1 S
Oesophageal dysfunction in patients with primary Sjogren's syndrome 611
tored in one half of the subjects, who asked toswallow only when necessary. Oesophageal peristal-sis was elicited by both wet and dry swallows. Wetswallows consisted of 5 ml water at room tempera-ture. With the patient supine the catheter waswithdrawn slowly until first the proximal doublepressure sensor and next the other two were placedon the lower oesophageal sphincter (LOS). At eachstation the pressure of LOS was read as the meanamplitude recorded after three wet and three dryswallows (one mean for wet and another for dryswallows). The catheter was next positioned withthe distal double pressure sensor 1, 2, and 4 cmabove the LOS. The same technique as for LOSpressure was used to study the upper oesophagealsphincter (UOS) pressure. The catheter was nextpositioned with the proximal double pressure sensor2 cm above and 2 and 4 cm below the UOS.The manometric study and the reading of the
tracings were carried out by the first author who wasunaware of the patient's diagnosis.The statistical differences between the groups
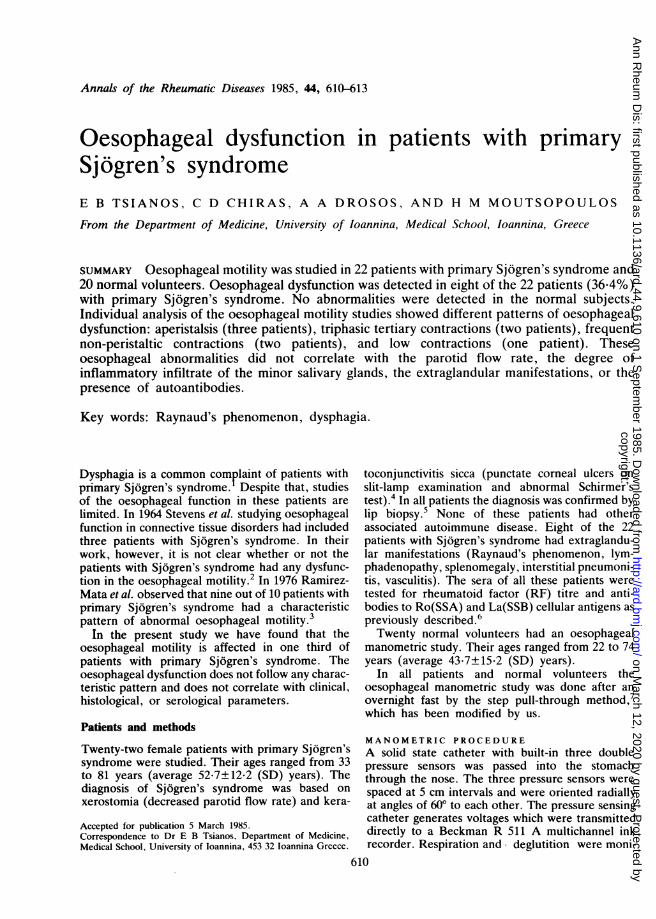
Fig. 2 Normal peristalsis in the same patient during wetswallows.
were evaluated by Student's t test and x2 test whereindicated.
Results
32"~~~~~~~~~~~~~~-
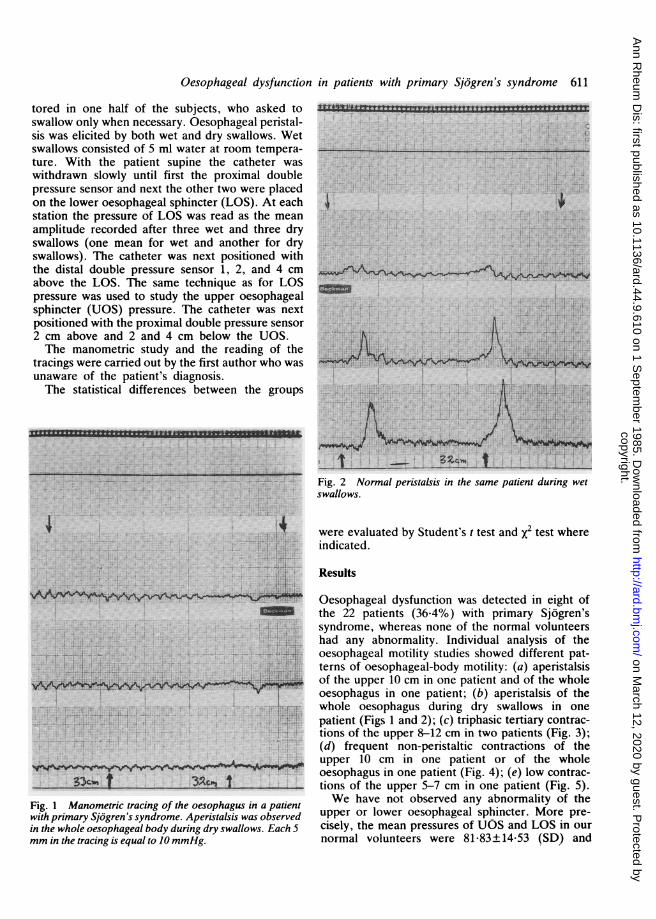
Fig. 1 Manometric tracing of the oesophagus in a patientwith primary Sjo5gren 's syndrome. Aperistalsis was observedin the whole oesophageal body during dry swallows. Each 5mm in the tracing is equal to JO mmHg.
Oesophageal dysfunction was detected in eight ofthe 22 patients (36.4%) with primary Sjogren'ssyndrome, whereas none of the normal volunteershad any abnormality. Individual analysis of theoesophageal motility studies showed different pat-terns of oesophageal-body motility: (a) aperistalsisof the upper 10 cm in one patient and of the wholeoesophagus in one patient; (b) aperistalsis of thewhole oesophagus during dry swallows in one
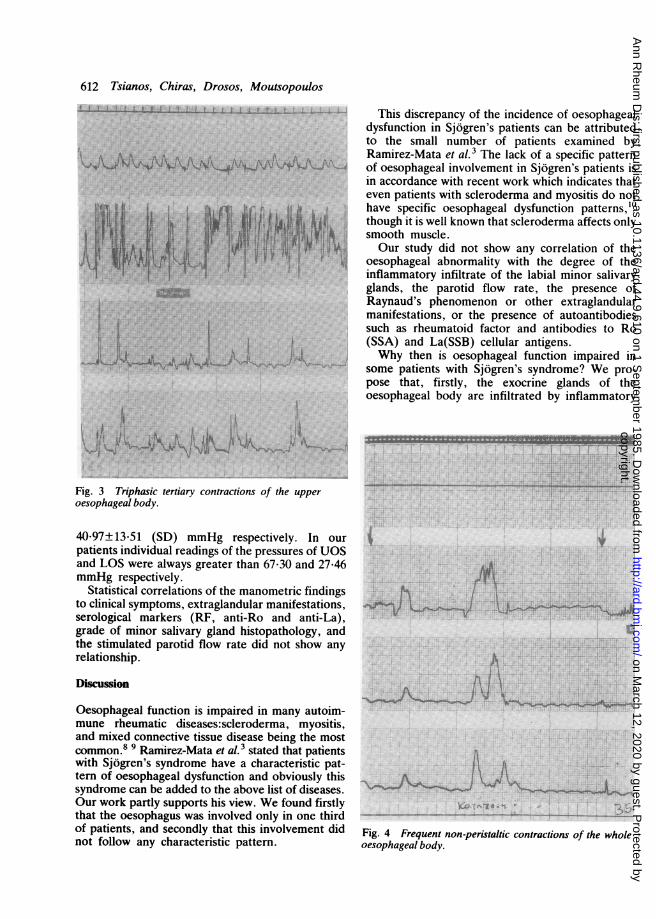
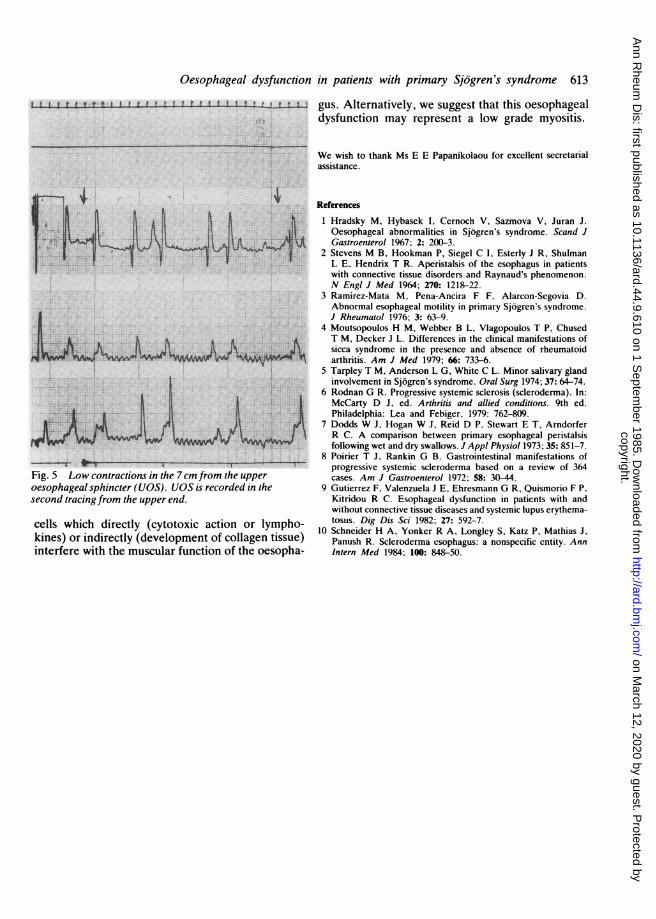
patient (Figs 1 and 2); (c) triphasic tertiary contrac-tions of the upper 8-12 cm in two patients (Fig. 3);(d) frequent non-peristaltic contractions of theupper 10 cm in one patient or of the wholeoesophagus in one patient (Fig. 4); (e) low contrac-tions of the upper 5-7 cm in one patient (Fig. 5).We have not observed any abnormality of the
upper or lower oesophageal sphincter. More pre-cisely, the mean pressures of UOS and LOS in our
normal volunteers were 81 83±14-53 (SD) and
=. .
... .....
YTTYrr3rlryyymxx-.. . . v IEW-K-KAU
c4,:
D
iji +,+.
3Z4-.. t
copyright. on M
arch 12, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.44.9.610 on 1 S
-.'Sw -I-II L ftL 1. I-L1-- -t-fIIfI Li--4.I -- This discrepancy of the incidence of oesophagealdysfunction in Sjdgren's patients can be attributedto the small number of patients examined byRamirez-Mata et al.3 The lack of a specific patternof oesophageal involvement in Sjdgren's patients isin accordance with recent work which indicates thateven patients with scleroderma and myositis do nothave specific oesophageal dysfunction patterns,'0though it is well known that scleroderma affects onlysmooth muscle.Our study did not show any correlation of the
oesophageal abnormality with the degree of theinflammatory infiltrate of the labial minor salivaryglands, the parotid flow rate, the presence ofRaynaud's phenomenon or other extraglandularmanifestations, or the presence of autoantibodiessuch as rheumatoid factor and antibodies to Ro(SSA) and La(SSB) cellular antigens.Why then is oesophageal function impaired in
some patients with Sj6gren's syndrome? We pro-pose that, firstly, the exocrine glands of theoesophageal body are infiltrated by inflammatory
1~ ~~ 1id
1k ,k
Fig. 3 Triphasic tertiary contractions of the upperoesophageal body.
4O-97±13*51 (SD) mmHg respectively. In ourpatients individual readings of the pressures of UOSand LOS were always greater than 67-30 and 27-46mmHg respectively.
Statistical correlations of the manometric findingsto clinical symptoms, extraglandular manifestations,serological markers (RF, anti-Ro and anti-La),grade of minor salivary gland histopathology, andthe stimulated parotid flow rate did not show anyrelationship.
Discussion
Oesophageal function is impaired in many autoim-mune rheumatic diseases:scleroderma, myositis,and mixed connective tissue disease being the mostcommon.8 9 Ramirez-Mata et al.3 stated that patientswith Sjbgren's syndrome have a characteristic pat-tern of oesophageal dysfunction and obviously thissyndrome can be added to the above list of diseases.Our work partly supports his view. We found firstlythat the oesophagus was involved only in one thirdof patients, and secondly that this involvement didnot follow any characteristic pattern.
4
j~~~~~
A
-, a1 10 1rk4L
Fig. 4 Frequent non-peristaltic contractions of the wholeoesophageal body.
copyright. on M
arch 12, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.44.9.610 on 1 S
Oesophageal dysfunction in patients with primary Sjogren's syndrome 613
I j I t t t I I tt I I I t 1 I I I I t I L t t 1 gus. Alternatively, we suggest that this oesophagealdysfunction may represent a low grade myositis.
We wish to thank Ms E E Papanikolaou for excellent secretarialassistance.
*-I-~-01 I -T
Fig. 5 Low contractions in the 7cm from the upperoesophageal sphincter (UOS). UOS is recorded in thesecond tracing from the upper end.
cells which directly (cytotoxic action or lympho-kines) or indirectly (development of collagen tissue)interfere with the muscular function of the oesopha-
References
1 Hradsky M, Hybasek I, Cernoch V, Sazmova V, Juran J.Oesophageal abnormalities in Sjogren's syndrome. Scand JGastroenterol 1967; 2: 200-3.
2 Stevens M B, Hookman P, Siegel C I, Esterly J R, ShulmanL E, Hendrix T R. Aperistalsis of the esophagus in patientswith connective tissue disorders and Raynaud's phenomenon.N Engl J Med 1964; 270: 1218-22.
3 Ramirez-Mata M, Pena-Ancira F F. Alarcon-Segovia D.Abnormal esophageal motility in primary Sjogren's syndrome.J Rheumatol 1976; 3: 63-9.
4 Moutsopoulos H M, Webber B L, Vlagopoulos T P, ChusedT M, Decker J L. Differences in the clinical manifestations ofsicca syndrome in the presence and absence of rheumatoidarthritis. Am J Med 1979; 66: 733-6.
5 Tarpley T M, Anderson L G, White C L. Minor salivary glandinvolvement in Sjogren's syndrome. Oral Surg 1974; 37: 64-74.
6 Rodnan G R. Progressive systemic sclerosis (scleroderma). In:McCarty D J, ed. Arthritis and allied conditions. 9th ed.Philadelphia: Lea and Febiger. 1979: 762-809.
7 Dodds W J, Hogan W J, Reid D P, Stewart E T, ArndorferR C. A comparison between primary esophageal peristalsisfollowing wet and dry swallows. J Appl Physiol 1973; 35: 851-7.
8 Poirier T J, Rankin G B. Gastrointestinal manifestations ofprogressive systemic scleroderma based on a review of 364cases. Am J Gastroenterol 1972; 58: 30-44.
9 Gutierrez F, Valenzuela J E, Ehresmann G R, Quismorio F P,Kitridou R C. Esophageal dysfunction in patients with andwithout connective tissue diseases and systemic lupus erythema-tosus. Dig Dis Sci 1982; 27: 592-7.
10 Schneider H A, Yonker R A, Longley S, Katz P, Mathias J,Panush R. Scleroderma esophagus: a nonspecific entity. AnnIntern Med 1984; 100: 848-50.
copyright. on M
arch 12, 2020 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.44.9.610 on 1 S