82
“Oh, I just work in Sterile Processing “ Wava Truscott, PhD Director, Medical Sciences and Clinical Education Halyard Health Care

“Oh, I just work in Sterile Processing “
Wava Truscott, PhD
Director, Medical Sciences and Clinical Education
Halyard Health Care

“OH, I JUST WORK IN STERILE
PROCESSING”
Objectives
• Describe what makes your career critical to optimal patient outcomes
• Identify consequences of doing an inadequate job
• Explain why a mindset of continual learning and improvement is essential
in your profession
• Determine how you can be a mentor in teaching, example and attitude

So, What Do You Do?

Oh, I just put my time at Sterile Processing…
I decontaminate, wash, assemble, pack, process, store---
Day in; Day out, same old thing

I wonder where I’m going.
I Feel I’m just coasting; Watching life go by.
I Never filled the shoes I thought I would.

…And Poop
I’m always in the dog house or
shoved in the corner

SOMETIMES I JUST FEEL I’M TRAPPED IN THIS JOB; WHO CARES

If I hear one more lecture beginning with:
“You’re not cleaning up well enough”
or, “You need to do an extra process now…”
or, “I want you to work closer with the OR and Cath Labs”

Holy Cow!! I’m just about to be wheeled into surgery.
How I survive (if I survive) may depend on that pack you prepared yesterday
I want you to think hard about the next few slides
Now The Patient’s Perspective

OH, I JUST WORK IN A CAR FACTORY
I Just…. Connect parts on engines
Install brake assemblies
Weld the same frame joints
Check hydraulic assembly pressures
Align and tighten wheel mounts
Connect the same freakin’ electrical leads
Install safety belts
Order parts from vendors
Do you think these car-assembly workers are an
important part of protecting you and preventing potentially
disastrous life-long complications for you and your family?

YOU CAN BET YOUR LIFE ON IT!EVERY DAY!!

All I do is check
elevator sensors
Hey man, all I do
is put air in tires

Genesis Solar Sampler 3yr journey
crashes. Sensors to deploy
parachutes mounted backwards
Woman dies as
shoot fails
Genesis Solar Sampler
OH, I JUST PACK PARACHUTES

In Seconds, Poorly Performed Tasks
Can Alter Lives and Families Forever

You bet your next surgical patient’s quality of life it is
As is their very life and the future of his/her family
So does the successful outcomes for invasive procedures in the
ICU, ED, Trauma, Ophthalmics, Anesthesiology, Respiratory
therapy, Research, Diagnostics, Interventional Radiology, Cath
Labs and the OR.
SO, YA’ THINK YOUR JOB IS NOT MISSION CRITICAL?

YOU & YOUR SP STAFF ARE ESSENTIAL MEMBERS OF THE MEDICAL TEAM
YOU ARE—AND MUST ALWAYS BE ---PROFESSIONALS

• A professional is a person working in an occupation
which requires extensive knowledge, skills and expertise
• A profession is limited to individuals with formal education in a
specialized body of knowledge
• Members of a profession are governed by a universal code of
ethics
Define a Professional
“First, Do No Harm”
….Know deep within, at your very core’ that what you do
has the power to save, improve, injure, ruin or take
lives….and with that comes serious responsibility
Both for you personally and as a part of
your Hospital or Ambulatory Surgery Center SP team

Started Not All That Long Ago
A Profession That

1774 Swedish chemist Scheele
discovered chlorine
1825 Frenchman Labarraque
used calcium hypochlorite
(chlorine compound) to remove
the smell of:
• morgues
• sewers
• privies (toilets)
• horse stables
• hospital wards
• ships
• prisons
French surgeons in late
1800s first used to reduce
odor of gangrene then to
treat:
• gangrene
• ulcers
• burns
• carbuncles
Germicides

Vienna 1840s: 1 of 5 mothers died giving birth
Semmelweiss thought connection with hands: Docs
did not wash between autopsy and examining mother in labor
He began to required surgeons wash hands with dilute bleach
Death rate dropped from 18.7% to 1.7% for an entire year!!
Staff did not like angry Semmelweiss, refused to believe data
Went back to contaminated hands and lab coats
High mortality rate returned
Semmelweiss committed to insane asylum; beaten by guards
because of his insulting obnoxious personality
Child-Birth Fever
Ignaz Semmelweiss
Managers: How you deliver a requirement makes a difference
Staff: If you ignore the evidence because you don’t like
messenger, patients could die

Florence Nightingale
Crimean War 1853 - 1856
Florence Nightingale visited wounded soldiers
10 times the soldiers died from infections they
acquired in the hospital than directly from their
battle wounds!

Advances in Earliest
Ambulatory Surgery Centers
She and recruited volunteers
cleaned & disinfected everything
Result: 6 months of disinfection dramatically
reduced infections & deaths of wounded soldiers
Wounded died of infection:42% before disinfection started
2% after disinfection procedures in place
Nightingale

Joseph Lister 1827-1912
Mid 1800s post-surgical infections accounted for
death of almost 50% of all patients undergoing major surgery
Common medical report:
“Operation successful, but the patient died”
Lister used carbolic acid to clean the skin, mist over surgical site,
soak wounds and disinfect the instruments
No systemic infections or infection-related deaths for 9 months!
Father of surgical antisepsis

During the Franco-Prussian war: of the 13,200
men who had limbs amputated 10,000 died of
infection (gangrene)
Koch was appalled. He entered the war served
as a physician: learned of the work of Lister and
the germ theory proposed by Pasteur,
so used hypochlorite (bleach) with success
Father of Steam Sterilization
Then, in 1878 steam sterilized instruments
and dressings with similar results to the
hypochlorite - starting the era of steam
sterilization
Robert Koch 1843-1910

25
WHAT A WONDERFUL TIME TO BE IN HEALTHCARE!
Public Reporting
of Errors,
Infections
Pay for
Performance &
Penalties for Poor
Performance
26
JOY OF NEW LIFE Joy of New Lives

27
JOY OF EXPERIENCED LIFE
1 in 10,000 individuals in the US reaches age 100
Now 60,000 in US >100; up to 70 are beyond age 110!
Charles Yogi age 85

28
THERE’S NEVER BEEN A BETTER TIME TO HAVE CANCER

29
OR TO NEED A HEART TRANSPLANT

30
OR REQUIRE HEART SURGERY
Open on pump
Open off pump beating heart

31
OR TO FIND HOPE & A NEW LIFE

32
PENG SHUILIN
• 1995, 37 yr old Peng was hit by freight truck severed his body in half
• 2 years in the hospital with series of surgeries to reroute nearly every major organ or system
• Kept exercising, taking care of hygiene, positive attitude
• Fitted in socketed bucket with prosthesis

33
DALLAS WIENS
• 26yr Dallas face touched live electrical wire while repairing church window
• Burned face & half of scalp completely off
• Doctors series of surgeries 2.5yrs then skin from his back onto face
• Could not smell, breathe through nose or see
• Assumed this would be the rest of his life
• May 2011 received first US full face transplant
• Feels his lips and nose - can smell
• It is believed that in a few years, technology will be able to restore sight in his one eye
Daddy, you’re so handsome

34
FACES OF YOUR SUCCESSFUL PATIENTS!!

YOU ARE A PROFESSIONALA Member of The Healthcare Profession
That should give you and your family great pride
You should find personal joy and fulfillment in those successes
….and must embrace this very serious responsibility

36
SURVIVORS OFTEN INCREASED VULNERABILITY
“HOSPITAL OF CRITICAL PATIENTS”
Cancer treatment
Burns-extent and severity
Diabetes
Hemodialysis
HBV, HCV
HIV/AIDS
Implants: knees, hips, etc
Leukemia
Obesity
Organ transplants-human
• Extreme life saving procedures
Organ transplants-animal
Premature neonate survival
Poor nutritional status
Premature births
Smokers
Trauma severe
Tubes used in body
Very old and aging
New heart for baby
Along With Advances in Medicine and Progress in
“Enjoying the Good Life” comes increased vulnerability

37
WHEN THINGS GO WRONG
And What If It Was Your Fault
100,000 die of a
Hospital acquired
Infection - yearly
240 will die today

38
DON’T LET SOMEONE ELSE MAKE THAT MISTAKE
• Mistakes should not recur
• But an even more egregious mistake is failing to make certain sure no one else repeats it
• Golden opportunity is the “it almost happened”

39
• Remember the joy of learning
• …the joy of sharing knowledge of how to do things with children?
• …and the child’s thrill at accomplishing something new?
KNOWLEDGE AND EXPERIENCE: SHARE IT!!

Knowledge and Experience: Share It!!
40
• Learn best by example
• Learn why something must be a certain way
• Get deep into the problems; tackle them one bite at a time
• Seek support when needed rather than guessing

41
BE MENTOR!Be A Student!

42
DON’T BE A LUKEWARM ONLOOKER
• Be active; Be vital
• Be helpful, Be positive
• It’s OK to adjust the way you have been to be more
• Don’t live your life looking at a rearview mirror
• Everyday: learn, grow, teach, appreciate

43
Though sometimes difficult and unwelcome, change is absolutely necessary for Progress to proceed: Be a part of it!
Change
“A year from now you will wish you had started today.” -Karen Lamb
“It doesn’t matter where you are, you are nowhere compared to
where you can go.” -Bob Proctor
“Never too old, never too bad, never too late, never too sick to
start from scratch once again.” -Bikram Choudhury
“Nobody can go back and start a new beginning, but anyone
can start today and make a new ending.”-M Robinson
“Today is the first day of the rest of your life.”

44
Two Categories:
1. Corrective Change. Required to correct compliance errors committed against:
• established guidelines
• manufacturers’ instructions
• best practices
• facility policies
2. Progressive Change. Required to implement new technologies and discoveries:
– new devices
– new cleaning agents, disinfectants, sterilization units
– new ways to work with OR
– new knowledge, learning opportunities
– new government policies (healthcare plan, CMS, OSHA)
Change Required

45
Corrective Change

PATIENTS SUSCEPTIBLE TO OUR ERRORS
• 2008 Las Vegas: 50,000 former patients notified
‒ Hepatitis B
‒ Hepatitis C
‒ HIV
• 2010 Vancouver: 500 former patients notified
‒ Hepatitis B
‒ Hepatitis C
‒ HIV
Hepatitis C
Liver

MORE POSSIBLEHIV, HBV, HCV AND E. COLI
• 2011 Ottawa: 6,800 patients notified they may have been exposed to infectious agents as proper cleaning protocols not always followed
• 2009 Miami: thousands of patients notified of possible infection: endoscope irrigation tubing rinsed, but not disinfected
• 2009 Tennessee: thousands notified of possible infection: misassembled endoscope replaced one way valve with two-way valve
• 2006 Los Angeles: Endoscope infected 19 heart surgery patients with E. coli within 2 week period. Leak identified, intended for repair, but not quarantined, so went back into use – poorly processed and not observed for damage

48
CDC: CLUSTER INFECTIONS 1996 AND 1998
• 2006: Several infants.Bacterial infections contracted in Los Angeles
NICU due to inconsistent and improper cleaning practices
• 2003: 42 surprise inspections found fewer than half had adequate
sterilization standards
• 1996 and 1998 28 clusters reported by CDC: bronchoscopy
– Klebsiella
– Pseudomonas aeruginosa
– Mycobacterium tuberculosis
– Mycobacterium intracellulare
– Mycobacterium avium

49
DRYING ENDOSCOPES: SO IMPORTANT• Dry prior to disinfection/sterilization to prevent:
– over dilution of high level disinfectants– cycle cancellation in some sterilizers– colonization of waterborne pathogens
• 70% alcohol and forced air after every reprocessing (that is between patients and before storage)
• Dry and store safely
• Trapped residual moisture encourages biofilm formation
• 70% alcohol wipe-down outside surface before each use
Pseudomonas

50
Progressive Change

PROGRESSIVE CHANGE
• Colored television
• Slide projectors
• Star Trek
• Computers: binary punch cards
• Man on the moon
• Desk top computers
• PowerPoint
• Star Trek Next Generation
• Internet
• Laptop computers
• Cell phones
• Star Trek Voyager
• Smart phones
• Social media
• Tablet computing

52
Better vaccines
Non-woven fabrics
Small-pox eradication
Polio almost eradicated in the US
Phenomenal life-saving procedures
Implants
Viral treatment drugs (e.g. HIV)
Minimally invasive procedures with endoscopes
Automated endoscope reprocessors
Ambulatory Surgery Centers (>65% all elec. surgeries)
RF technology
Plasma sterilization
Role of particles complications
Biofilm studies
Progressive Change

53
LINT & PARTICLES IMPACT ON POST-SURGICAL RECOVERY
Breast implant capsular contracture is a hard scar tissue capsule that form around the implant
Now understood that this is often caused by a tissue reaction to a subclinical infection (e.g. Staphylococcus epidermidis) micro-biofilm on implant surface
Lint, powder, debris increase likelihood of biofilm formation and resulting inflammation initiating capsule to prevent spread
Dobke MK 1995 // Pajkos AB 2003// Netscher D 2004// Mladick RA 2005// Netscher DT 2005

54
FRUSTRATED WHITE CELLS “SPIT” DESTRUCTION
• Activated white blood cells (WBC) recognize bacterial biofilm threat on implant
• WBCs spit out biocidal oxygen radicals and enzymes trying to kill biofilm bacteria

55
ACTIVATED NEUTROPHIL SPITS KILLER RADICALS & ENZYMES TRYING TO STOP INVADER PARTICLES

56
FRUSTRATED WHITE CELLS “SPIT” DESTRUCTION
• Activated white blood cells (WBC) recognize bacterial biofilm threat on implant
• WBCs spit out biocidal oxygen radicals and enzymes trying to kill biofilm bacteria
• Injure the tissues that were trying to accept the implant
• Result: inflammation, delayed poor quality healing, capsule formation, potential spread of biofilm infection

57
Convinced particles + few bacteria responsible, Surgeon performed all breast implant surgeries:
– Lint-free materials sterile drapes, wrap, gowns, etc.
– Powder-free gloves
– No implant placement on drapes
– No touch of patient skin (even though thorough skin prep)
Mladick RA. Plast Reconstr Surg 2005; 1426-27
Eight years without a single capsular contraction!
Little things like lint, powder, other particles matter!
Principle applies to all implants!!
BREAST IMPLANTS

58
FRUSTRATED WHITE CELLS “SPIT” DESTRUCTION
15 to 20% breast implants still result in
capsule formation and contracture
• Activated white blood cells (WBC) recognize bacterial biofilm threat on implant
• WBCs spit out biocidal oxygen radicals and enzymes trying to kill biofilm bacteria
• Injure the tissues that were trying to accept the implant
• Result: inflammation, delayed poor quality healing, capsule formation, potential spread of biofilm infection

59
Distraction
CRIME OF DISTRACTION
• Things that strongly attract the attention of the immune system – become the center of attention so microorganisms are ignored and can multiply
germ

60
Bacteria(Pseudomonas)
Bacteria(Pseudomonas)
ParticulatesOr dead biofilm chunks
Macrophage Protecting Against Invasion
of Particles and Bacteria

61
BACTERIA MULTIPLY UNCHECKED: BIOFILM HALO
Particulates
White Blood CellMacrophage
Pseudomonas
Biofilm initiated by and now surrounding
particle

62
ALTERED THRESHOLD FOR INFECTION
Jaffray:• Wound: no particles + 1,000 Staph: 1/10 infected
• Wound: 2mg sterile particles + 1,000 Staph: 9/10 infected
Staphylococcus aureus
Elek:
• Wound: no particles = 10,000,000 to cause infection
• Wound: with particles = 100 to cause infection

63
OPHTHALMIC SURGERY
• Tissue, mineral particles, biofilm left after reprocessing
• One practice: 2.5 yrs: over 100 cases of endophthalmitis– Lint in air & on devices
attracted to eye
– Realized too late-lost practice
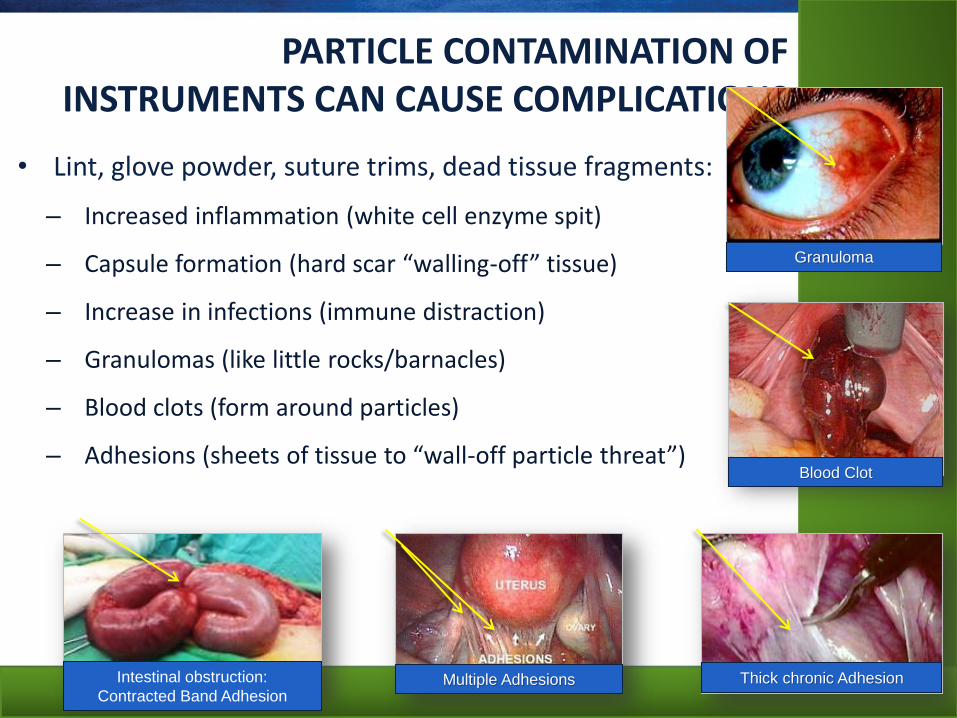
• Lint, glove powder, suture trims, dead tissue fragments:
– Increased inflammation (white cell enzyme spit)
– Capsule formation (hard scar “walling-off” tissue)
– Increase in infections (immune distraction)
– Granulomas (like little rocks/barnacles)
– Blood clots (form around particles)
– Adhesions (sheets of tissue to “wall-off particle threat”)
64
PARTICLE CONTAMINATION OF INSTRUMENTS CAN CAUSE COMPLICATIONS
Intestinal obstruction:
Contracted Band Adhesion
Granuloma
Blood Clot
Thick chronic AdhesionMultiple Adhesions

65
LINT & PARTICULATE SOURCES
Poorly cleaned devices: tissues, fat, blood
Linting sterilization wrap
Gasket seals oxidizing on containers or devices
Sweaters, fleece vests in SPD room
Devices dried with/on linting materials
Hair, lint, debris from staff and traffic
Corrugated cardboard, newspapers, tissues
Rigid containers not washed clear of debris
OR: gowns, hair, drapes, back table cover,
sterilization wrap, glove powder

66
ENDOSCOPE BIOFILM
Two different air/water channels
• (A) Multilayered biofilm – Held days before processing
• (B) Low-power view showing a confluent layer of soil and biofilm after processed, dried and sterilized
Pajkos K J Hosp Infec 2004;58:224-9
B
A

67
POST CLEANING AND DISINFECTION
• Electron micrographs of suction channel damaged inner surface: cracks, grooves pits, cuts
– (a) Cleaning brush caused damage
– (b) Residual soil and bacterial biofilm with its gooey coating
A
B
Pajkos K J Hosp Infec 2004;58:224-9.

68
BIOFILM DRIED ON; BLOCKED EFFECTIVE DISINFECTION
• Electroencephalogram electrodes not properly cleaned
• Biofilm left on preventing adequate sterilization
• Several patients acquired hepatitis B (HBV)
• $27.5 million legal settlement against neurologist & hospital
Mackay B CMAJ 2002; 166(7):943

69
FDA INSPECTIONHAWAII 2008
• “Dirty instruments in sterile trays, specifically orthopedic (bone) trays.” In one documented case, “three out of three trays in one day had instruments with bone or cement on them.”
• “Residue and debris on sterile instruments in sterile surgical containers.”
• “A dirty and grimy sink in the Sterile Processing Department work area.”
• “A number of outdated sterile devices and other outdated supplies”
• “Failed to ensure the integrity and cleanliness of surgical suites, procedure rooms and sterile processing department.”
• “Technician washed dirty surgical instruments with gloves on, then opened a door and answered the phone without removing the wet gloves”

70
SPD ERRORS REPEATED
• 2009: 17% of ambulatory surgery centers (ASC) who responded to a Sterile Processing News online poll reported outbreaks of toxic anterior segment syndrome (TASS) at their facilities.
– TASS is a post-operative, acute inflammation of the anterior segment of the eye that linked to ophthalmic devices
• Oct 2011: Poll of ASC “compliance challenges”:
20% stated sterile processing continues as a major compliance challenge

71
TASS WITHOUT INFECTION(TOXIC ANTERIOR SEGMENT SYNDROME)
• Abnormal pH or osmolarity,
• Impurities of autoclave steam
• Residual biofilm, tissues (sterile, but present)
• Irritants on surfaces of surgical instruments
• Corroded or chemically altered devices
• Improperly rinsed devices
• Heat stable endotoxins
• Anesthetic agents and preservatives
• Topical ophthalmic ointments
• Instruments & Intraocular lenses – chemical leach out
Van Philips L.A.M, 2011

INCOMPATIBILITY ERRORS: DAMAGE
• Inappropriate sterilization modes or disinfectants can be incompatible with instruments and surfaces
• Example: Plasma sterilization for ophthalmic instruments
– degraded brass into copper & zinc that deposited into patient’s eyes during surgery
– corneal decompensation, loss of visual acuity, irreversible injuries
– several cases of blindness
• Microorganisms can be protected from sterilization in corroded crevasses
Duffy RE, 2000

73
May we:
Accept change as probable progress, we are part of the future
Embrace that changes may need new procedures, new techniques
Recognize changes may help us to do things that will:
• improve ease of compliance
• be more efficient or effective
• be more cost effective by reducing time, effort, do-overs
• be safer for staff to perform
• better for the patient
However, as experts we must still determine if:
• anticipated benefit is real
• puts the patient at increased risk
• does not cause ancillary incompatibilities or problems
May we instigate improvement changes wherever needed
Progressive Change

74
American Civil War 642,000 soldiers died
2/3 from infection
Barton vowed to address healthcare conditions
Founded American Red Cross
CLARA BARTON – THE PASSION
“I have an almost complete disregard of precedent and a faith in
the possibility of something better. It irritates me to be told howthings always have been done .... I defy the tyranny of precedent.I cannot afford the luxury of a closed mind. I go for anything newthat might improve the past.” Clara Barton

75
BE CHALLENGED NOT DISCOURAGED

76
BE CHALLENGED NOT DISCOURAGED

77
ATTITUDE IS A DECISION AND IT INFLUENCES OTHERS POSITIVELY OR NEGATIVELY
• Decide right now what your Attitude will be the first day back to work
• How will you influence your colleagues?
• How Will You Impact Patient care?

78
CHANGE IS NECESSARY FOR PROGRESS HELP MAKE IT POSITIVE!
I am only one, but I am one. I cannot do everything, but I can do something. And I will not let what I cannot do interfere with what I can do. ~Edward Everett Hale
I've learned that you shouldn't go through life with a catchers mitt on both hands. You need to be able to throw something back. ~Maya Angelou
The destroyer of weeds, thistles and thorns is a benefactor, whether he soweth grain or not.
~Robert Ingersoll, inscription to Volume I, Collected Works
If you have time to whine and complain about something then you have the time to do something about it. ~Anthony J. D'Angelo,
If you have no will to change it, you have no right to criticize it. ~Author Unknown

79
IS THIS CAREER FOR YOU? FOR YOUR STAFF?
• Everyone of us can make changes where needed
• A very few will choose not to
• This profession is too critical to patient safety for:
– “This is sooo stupid”
– “No body’s going to tell me what to do!”
– “I hate what I am doing”
– “blah, blah, blah”
• If this is how you really feel:
– SPD may not be the right place for you
– You may be happier in a different career
• Patients will be safer and SPD teams more efficient when all are dedicated to the same purpose
• Managers: addressing “poor fit” personnel issues is never easy, but is a very important responsibility
Because:

80
Patients Entrust Their Quality Of Life And Life Itself Into Our Care

81
So that’s what you do!
Wow, that’s really a lot of Responsibility!
But, Man it’s really Cool!
Yah Dude, I’m Impressed!!
Thank You!!I Wanna become the Best SPD Professional I can Be
I don’t understand a lot of stuff, but I’ll learn!!
I wanna be certified!!
I’ll help you Bro! Cause……..

“I’m A Sterile Processing Professional”
Wava Truscott, PhD
Director, Medical Sciences and Clinical Education
Halyard Health Care











![[ CERTIFIED IN STERILE PROCESSING MANAGEMENT - CSPM ... · [ CERTIFIED STERILE PROCESSING AND DISTRIBUTION TECHNICIANS - CSPDT ] Total Sat for Exam = 1,220 Total Passed = 784 (64%)](https://static.documents.pub/doc/80x56/5e9f1daa192fcb713d18fada/-certified-in-sterile-processing-management-cspm-certified-sterile-processing.jpg)





