39
Myosites du sujet âgé Olivier Benveniste Département de Médecine Interne Centre de Référence Maladies Neuro-Musculaires Equipe Muscle Inflammatoire U974 Groupe Hospitalier Pitié-Salpêtrière

Myosites du sujet âgé
Olivier Benveniste
Département de Médecine Interne
Centre de Référence Maladies Neuro-Musculaires Equipe Muscle Inflammatoire U974
Groupe Hospitalier Pitié-Salpêtrière

Myositis classification
Most of the literature is based on this paper:

Peter and Bohan criteria for PM or DM
1. Symmetrical proximal muscle weakness;
2. Muscle biopsy abnormalities : 1. Muscle fiber destruction;
2. Muscle fiber regeneration;
3. Perivascular and interstitial inflammatory infiltrates with muscle fiber destruction.
3. Elevation of CPK, Transaminases, LDH or aldolase activity;
4. Electromyography changes: 1. Fibrillation potentials (on needle insertion at rest);
2. Complex repetitive discharges (on needle insertion at rest);
3. Positive sharp waves (on needle insertion at rest);
4. Short duration, low amplitude complex (polyphasic) potentials on contraction.
5. Typical skin rash.
• DEFINITE: any 4 of the criteria
• PROBABLE: any 3 of the criteria

Example, 84 years old patient
– 75 y, proximal deficit, difficulties to climb stairs
– 79 y, proximal and distal muscle weakness (anterior
tibialis, quadriceps, finger and wrist flexors, ankle
dorsiflexors)
– 82 y, use a stick
– Swallowing tbs

Old patient 2
• CK: 450 U/l
• EMG: myogenic syndrome
• Muscular biopsy
• Diagnosis : polymyositis.
(definite with Peter and Bohan criteria)
• Treatment : 2 years
1) Corticosteroids
2) IVIg
• No success → 2nd biopsy →

sIBM features

Many proteins related to neurodegenerative diseases:
• b-amyloid and bAPP
• phosphorylated tau
• a1ACT
• a-synuclein
• prion protein
• ApoE
• ab-crystallin
• Parkin
• copper zinc superoxide dismutase
• manganese superoxide dismutase
• apoptotic regulators (Bcl-2, Bcl-x and BAX)
• Lipoprotein receptors
• Ubiquitins
Content of protein inclusions
Amyloid deposits
IBM AD
Werner Stenzel

Unanswered question
Dalakas M, Nat Clin Pract Neurol. 2006
Is IBM a degenerative or an inflammatory myopathy?
ICOS
Treg
IFN-g
CD28-
Plasma
cells
?

sIBM clinical features


Evaluation
Visit 1 Visit 2
9 months
Visit 3
4 years

Baseline visit: strength measurements
left
right
0 10 20 30 40 50 60 70 80 90 100
Grip
Wrist flexion
Wrist extension
Elbow flexion
Elbow extension
Ankle flexion
Ankle extension
Knee flexion
Knee extension
% predicted
*
*
*
*
*
*
Upper limb
Lower limb

Relation between knee extension strength and
6MWD
0
10
20
30
40
50
60
70
80
90
100
0 20 40 60 80 100
Knee extension strength (% predicted normal)
6M
WD
(%
pre
dic
ted
no
rmal
)

Neurology 2014
• Finger flexor or quadriceps weakness, and
• Endomysial inflammation, and
• Invasion of nonnecrotic muscle fibres or rimmed vacuoles
→ 90% sensitivity and 96% specificity

Characteristics of 136 patients
Variable Result
Gender : male (n=136) 78 (57.3%)
Age at first symptoms, years (n=136) 61 [55-69]
First symptoms (n=136)
Muscle weakness only
Swallowing troubles only
Muscle weakness and swallowing troubles
119 (87.5%)
6 (4.4%)
11 (8.1%)
Previous diagnosis (n=136)
None
Polymyositis
Amyotrophic Lateral Sclerosis
Dystrophy
Other
94 (69.1%)
23 (16.9%)
3 (2.2%)
4 (2.9%)
12 (8.8%)
Delay between first symptoms and diagnosis, months
(n=136)
59 [29-95]
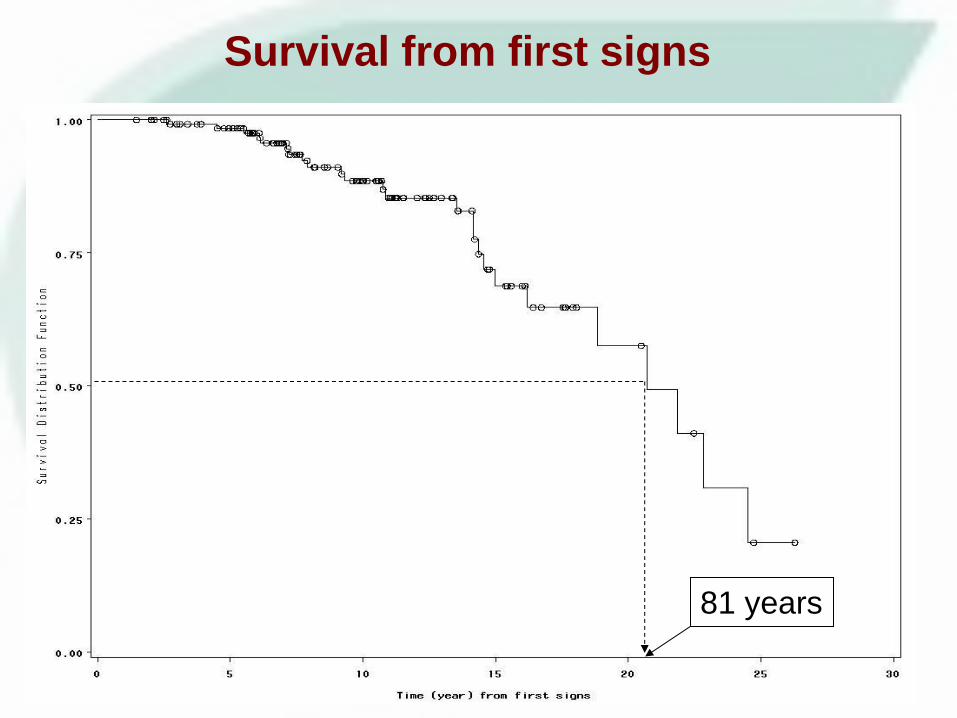
Survival from first signs
81 years

Description of received treatments
by 71 (52%) sIBM patients
Molecules and duration Results
Corticosteroids (prednisone, 1 mg/kg/day) 65 (92%)
(n=63)
Intravenous Immunoglobulins 40 (56%)
(n=39)
Azathioprine 19 (27%)
(n=17)
Methotrexate 23 (32%)
(n=21)
Combination of treatment
Corticosteroids only
Corticosteroids and other drugs
Other drugs only
19 (27%)
46 (65%)
6 (8%)
Duration of treatment, months [n=69]
41 [13.0-89.2] ~ 3.5 years

Status at the last visit Untreated
(n=65)
Treated
(n=71)
p
CK, u/ml (n=87) 367 [219 -649] 209 [117-559] 0.11
Grip test (n=76) 13.4 [11.0-17.2] 13.5 [9.0-18.0] 0.84
Walton (n=113) 4 [3-6] 6 [3-6] 0.007
RMI (n=88) 11 [9-13] 10 [4-11] 0.004
IWCI (n=71) 50 [30-65] 40 [25-50] 0.04
Current handicap for walking (n=136)
None
1 or 2 canes
Wheelchair
20 (31%)
26 (40%)
19 (29%)
13 (18%)
26 (37%)
32 (45%)
0.10
Comparison of treated and untreated
sIBM patients

Estimates of covariate effect on each
transition in the multi-state model
Transition HR (95%CI) p
Age at first symptoms
(> 60 yrs vs <60 yrs)
No handicap – walking with aid
No handicap – wheelchair
Walking with aid – wheelchair
Alive - Death
1.98 (1.27-3.08)
0.62 (0.19-2.07)
1.35 (0.68-2.71)
3.65 (1.22-10.92)
0.003
0.44
0.39
0.02
Treatment
(Yes vs No)
No handicap – walking with aid
No handicap – wheelchair
Walking with aid – wheelchair
Alive - Death
2.05 (1.30-3.25)
2.09 (0.70-6.24)
1.74 (0.92-3.30)
1.47 (0.67-3.22)
0.002
0.18
0.09
0.34

Discussion / conclusions
Onset
Diagnosis
=
Walk support
Wheelchair Death
5 y. 9 y.
61 y. 66 y. 75 y. 80 y.
• IS treatments don’t seem to ameliorate the handicap
- Are treated patients more severely affected?
- Are treatments deleterious?
• IS treatments don’t seem to delay the dates of wheelchair
or death

IBM: 6 controlled prospective studies
Authors N Intervention Efficacy
Dalakas, 1997
Walter, 2000
Dalakas, 2001
Muscle study Group, 2001
and 2004
Rutkove, 2002
Badsrising, 2002
19
22
34
57
19
44
IVIg or placebo
IVIg or placebo
CS + IVIg or placebo
Beta IFN or placebo
Oxandrolone or placebo
MTX or placebo
No, 3 mo
No, 6 mo
No, 3 mo
No, 6 mo
No, 3 mo
No, 12 mo

Treatment of IBM, in practice :
• Physiotherapy +++
• If « young » patient, rapid evolution, many inflammatory
infiltrates on biopsy…
• Prednisone (1 mg/kg/d)
• MTX
• For a limited duration (3 to 6 months)
• If swallowing troubles
• IVIg
• Cricoid myotomy


sIBM: Th1 Signature and Treg deficiency
FoxP3
CD4
Dapi
Y Allenbach, PLoS One 2014
% o
f p
os
itiv
e
ce
lls
sIBM Controls
sIBM

Effect of Rapamycin in our mouse model
PBS 1mg 3mg PBS 1mg 3mg
2.5E7
B c
ell
s
T c
ell
s
CD
4+
CD
8+
PBS
Rapa 3mg
Ce
ll c
ou
nt
1.5E7
0.5E7
% o
f T
reg
s
PBS Rapa 3mg
N Prevel: PLoS One 2014

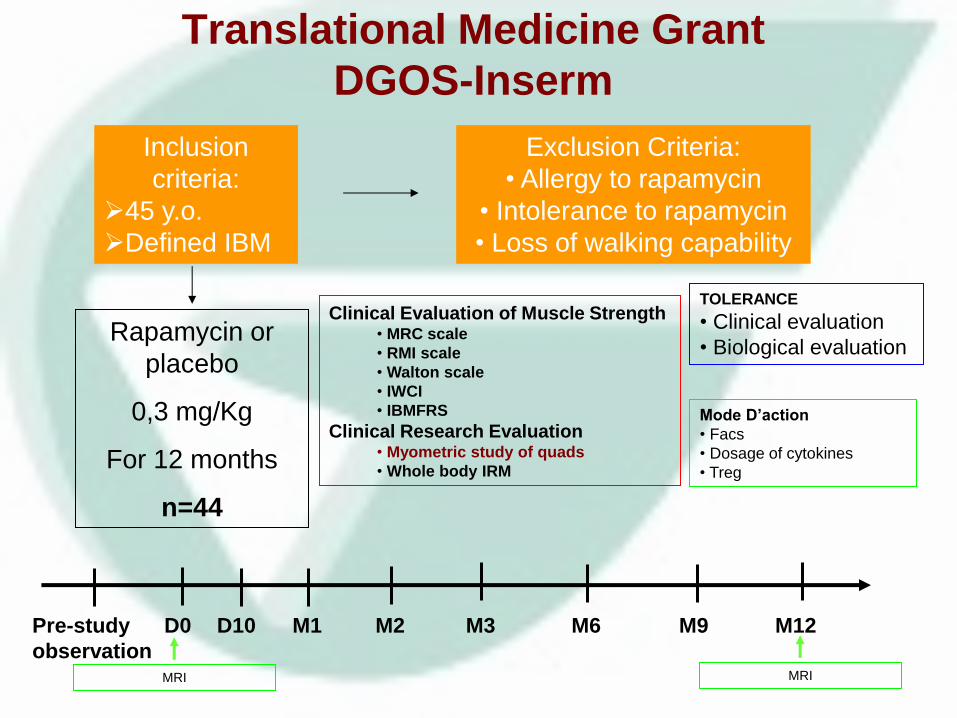
Inclusion
criteria:
45 y.o.
Defined IBM
Exclusion Criteria:
• Allergy to rapamycin
• Intolerance to rapamycin
• Loss of walking capability
Rapamycin or
placebo
0,3 mg/Kg
For 12 months
n=44
Pre-study
observation
D0 D10 M1 M2 M3 M6 M12 M9
Clinical Evaluation of Muscle Strength • MRC scale
• RMI scale
• Walton scale
• IWCI
• IBMFRS
Clinical Research Evaluation • Myometric study of quads
• Whole body IRM
TOLERANCE
• Clinical evaluation
• Biological evaluation
Mode D’action
• Facs
• Dosage of cytokines
• Treg
MRI
Translational Medicine Grant
DGOS-Inserm
MRI

Efficacy and Safety of Bimagrumab/BYM338 at 52
Weeks on Physical Function, Muscle Strength, Mobility
in sIBM Patients (RESILIENT)
Phase 2, 3: 240 patients
Sponsor: Novartis Pharmaceuticals
ClinicalTrials.gov Identifier: NCT01925209
ClinicalTrials.gov

New classification of myositides
• Dermatomyositis, 30% paraneoplastic
• Inclusion body myositis
• Polymyositis
• Overlap myositis (Troyanov) – Myositis associated to a connective tissue disease
– Myositis with associated Abs (PmScl, Ku …)
– Myositis with specific Abs (anti-synthetases, anti-SRP…)
• Immune mediated necrotizing myopathies (Hoogendijk) with anti-SRP+, anti-HMGCoA Reductase+ (post-statines), or paraneoplastic

MDA-5
TIF-1g Cancer
Jo-1
PL-7
PL-12
EJ
OJ
Ku
PM-Scl
U1-RNP
SAE
HMGCR
SRP
Mi-2 NXP2
Ove
rlap
Myo
siti
s D
erm
atom
yositis
Po
lym
yosi
tis
Imm
un
e M
ed
iated
N
ecro
tizing M
yop
athy
Inclusion Body Myopathy
5’-Nucleotidase
KS
Zo
YRS
ASA
ILD Cancer

Arthritis, Sept 2010
• 225 patients
• 38 necrotizing myopathies
- 4 anti-synthetase
- 6 anti-SRP
- 16 anti-p200/100


• En ELISA HMGCoAR : 100% + patients anti-p200/100
• Specificity :
Immunoprecipitation
W blot
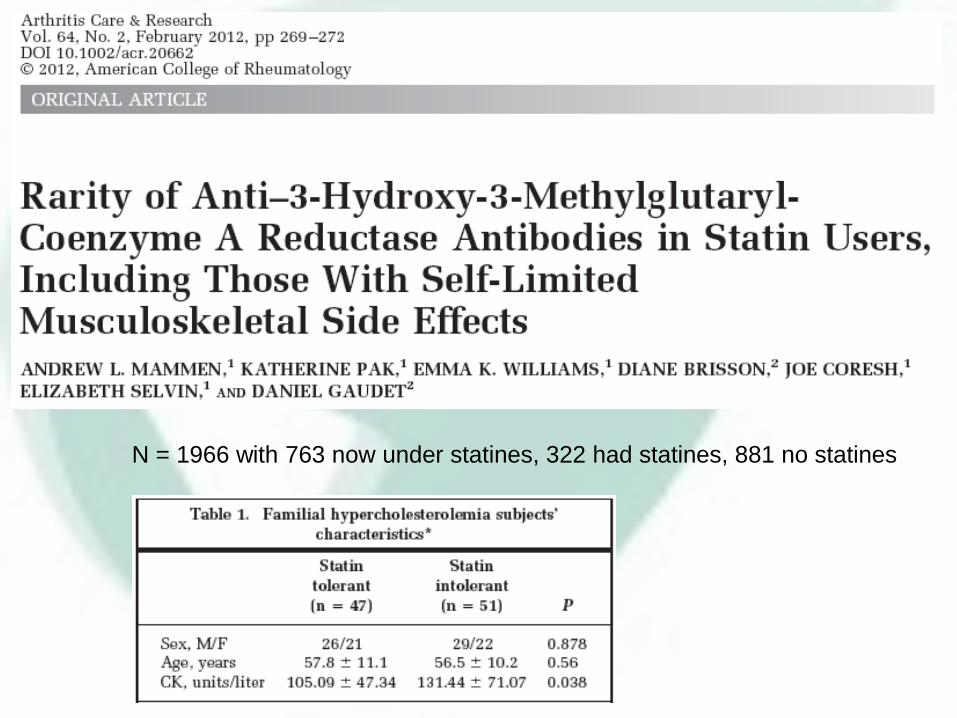
N = 1966 with 763 now under statines, 322 had statines, 881 no statines

Medicine 2014

Characteristics of the patients
Paris
n=45
Baltimore
n=50
Age (year) 44 ± 19 52 ± 16
Patients < 16 5 2
Women 81% 62%
Statines + 44% 72.7%
First signs:
- Muscle weakness: 87%
- Isolated increase of CK: 13% (n=5)

• Myalgia: 75%
• Muscle weakness: 87% (Paris) vs 95% (Baltimore) – Bilateral, proximal, severe ≤3/5: 72%
– Rapidly progressive in < 6 mo: 47%
– Axial: 61%
– Bedridden: 10%
– No facial weakness
– Dysphagia: 41%
• Amyotrophia: 15% – Scapula wings: 1 patient
Muscle involvement

Acknowledgements
• Werner Stenzel, Berlin, D
• David Hilton-Jones, Oxford, UK
• Baziel GM van Engelen, Nijmegen, NL
• Olivier Boyer, Rouen, F
and my colleagues from:
• Bruno Eymard
• Pascal Laforêt
• Baptiste Hervier
• Yves Allenbach


















