30
Oncology Treatment Guidelines : The Rules and Rationale Assoc. Prof. Dato’ Dr. Fuad Ismail & Dr. Paul Cornes
| Date post: | 14-Jul-2015 |
| Category: |
Health & Medicine |
| Upload: | pharmacyikn |
| View: | 194 times |
| Download: | 2 times |

Oncology Treatment Guidelines :
The Rules and Rationale
Assoc. Prof. Dato’ Dr. Fuad Ismail
&
Dr. Paul Cornes

What are Clinical Practice Guidelines?
Treatment of patients in the clinical setting requires complex inputs
• Disease factors – tumour type, stage, organs involved ..
• Patient factors - age, sex, PS, …
• Treatment factors - efficacy, toxicity, cost …
Clinician cannot keep abreast with evidence now
• Published randomized controlled trials grew from 5,000 per year in
1978–1985 to 25,000 per year in 1994–2001.
IOM (Institute of Medicine). 2011. Clinical Practice Guidelines We Can Trust. Washington, DC: The National Academies Press.
ISBN 978-0-309-16422-1.

What are Clinical Practice Guidelines?
Clinical practice guidelines are statements that include
recommendations intended to optimize patient care that are informed
by a systematic review of evidence and an assessment of the benefits
and harms of alternative care options.
Clinical Practice Guidelines (CPGs) are intended to provide a
systematic aid to making such complex medical decisions
• Help decision making
• Improve healthcare outcomes

Clinical guidelines
Act to reduce variation in
practice
• Permitting effective audit of
outcomes
Improve outcomes
• By steering physicians and
patients to chose the most
clinically effective treatments
Expose areas where evidence is
poor by
• Describing the evidence used
to make a recommendation
• Using grades and strengths of
evidence
Most OECD countries could save money by improving clinical guidelines and negotiating better drug prices, BMJ 2010;341:c5552
Many Malaysian oncologists
have relied on guidelines
from the USA and EU
Historically have not formally
included value judgements

Clinical guidelines
Some guidelines
explicitly make
decisions based on
cost effectiveness
• Example UK
N.I.C.E
Most OECD countries could save money by improving clinical guidelines and negotiating better drug prices, BMJ 2010;341:c5552
Erlotinib is recommended as an option
for the first-line treatment of people
with locally advanced or metastatic
non-small-cell lung cancer (NSCLC) if:
• they test positive for the epidermal growth
factor receptor tyrosine kinase (EGFRTK)
mutation
• the manufacturer provides erlotinib at the
discounted price agreed under the patient
access scheme (as revised in 2012).

Clinical guidelines
Most evidence
based guidelines
promote clinically
effective care –
which is generally
cost-effective too
Most OECD countries could save money by improving clinical guidelines and negotiating better drug prices, BMJ 2010;341:c5552

Clinical guidelines save money
Kosimbei et al. Health Research Policy and Systems 2011, 9:24 http://www.health-policy-systems.com/content/9/1/24
91% of guidelines
save money

What makes a Trustworthy Guideline :
To be trustworthy, guidelines should
• be based on a systematic review of the existing evidence;
• be developed by a knowledgeable, multidisciplinary panel of
experts and representatives from key affected groups;
• consider important patient subgroups and patient preferences;
• be based on an explicit and transparent process that minimizes
distortions, biases, and conflicts of interest;
• provide a clear explanation of the logical relationships between
alternative care options and health outcomes, and
• provide ratings of both the quality of evidence and the strength of
the recommendations; and
• be reconsidered and revised as appropriate when important new
evidence warrants modifications of recommendations.

What standards are there for guidelines?
Just as we have “CONSORT” standards to report clinical trials
Guidelines have standards from the “GRADE” Working Group
– Brozek JL, Akl EA, Alonso-
Coello P, Lang D, Jaeschke R, Williams JW. et al. GRADE Working
Group, Grading quality of evidence and strength of recommendations in clinical
practice guidelines. Part 1 of 3. An overview of the GRADE approach and
grading quality of evidence about interventions.. Allergy. 2009;64669-77
– Guyatt GH, Oxman AD, Kunz R, Jaeschke R, Helfand M, Liberati A. et
al. GRADE Working Group, Incorporating considerations of resources use into
grading recommendations.. BMJ. 2008;3361170-3
“
IOM (Institute of Medicine). 2011. Clinical Practice Guidelines We Can Trust. Washington, DC: The National Academies Press.
ISBN 978-0-309-16422-1.

What standards are there for guidelines?
Standards include
• Transparency
• Conflicts of interest
• Multidisciplinary and balanced, ideally with
patient representatives
• Should use systematic reviews
• A clear description of potential benefits and
harms.
• A summary of :
– relevant available evidence (and evidentiary
gaps),
– description of the quality (including applicability),
– quantity (including completeness), and
– consistency of the aggregate available evidence
IOM (Institute of Medicine). 2011. Clinical Practice Guidelines We Can Trust. Washington, DC: The National Academies Press.
ISBN 978-0-309-16422-1. PDF is available from The National Academies Press at
http://www.nap.edu/catalog.php?record_id=13058

What standards are there for guidelines?
An explanation of the part played by values,
opinion, theory, and clinical experience in
deriving the recommendation.
A rating of the level of confidence in (certainty
regarding) the evidence underpinning the
recommendation.
A rating of the strength of the
recommendation in light of the preceding
bullets.
A description and explanation of any
differences of opinion regarding the
recommendation.
IOM (Institute of Medicine). 2011. Clinical Practice Guidelines We Can Trust. Washington, DC: The National Academies Press.
ISBN 978-0-309-16422-1. PDF is available from The National Academies Press at
http://www.nap.edu/catalog.php?record_id=13058

Proposed CPG Standards
1. Establish transparency
2. Management of Conflict on Interest
• disclosure, divestment, exclusion
3. CPG Group Composition
• Multi-displinary, patients and patient groups
4. CPG – Systemic Review Intersection
5. Evidence based rating and strength of recommendations
6. Write-up on recommendations
• Explain recommendations, summarise evidence, input values
and judgement
7. External review
8. Updating

So why not just have one world guideline?
Treatment decisions must be relevant to the patient population in
Malaysia
• Including its relative wealth
• Access to medical resources (ranked 80th in the world 2010-11)
• And reflect Malaysian Societal Values
Country Spend as
a % of
GDP
(2010-11)
Annual
Spend in US
Dollar
equivalent
Malaysia 4.4 645
USA 17.7 8,508
UK 9.4 3,405
Korea Rep 7.4 2,198
Japan 9.6 3,213
Ref: Data – world Bank. Accessed URL: http://data.worldbank.org/indicator/SH.XPD.TOTL.ZS
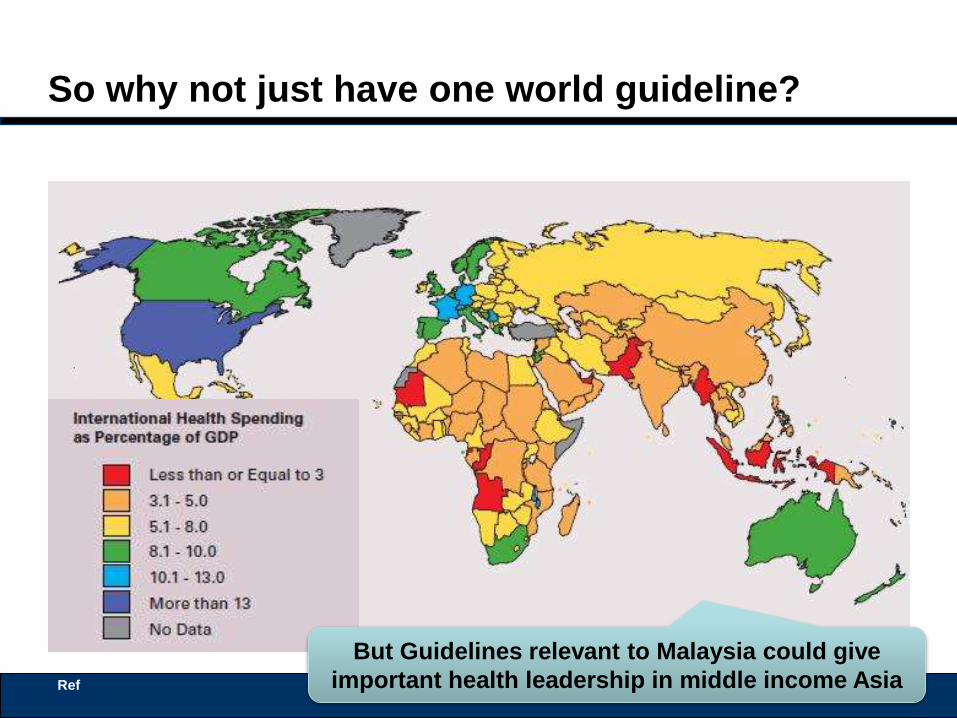
So why not just have one world guideline?
Ref
But Guidelines relevant to Malaysia could give
important health leadership in middle income Asia

Limitations of CPG
Variable quality of individual scientific studies;
Limitations in systematic reviews (SRs)
Lack of transparency of development groups’ methodologies
Failure to multi-stakeholder, multi-disciplinary guideline development
groups
Unmanaged conflicts of interest (COI)
Failure to use rigorous methodologies in CPG development.
Lack of evidence in subpopulations eg comorbidities, low socio-
economic groups, rare conditions.
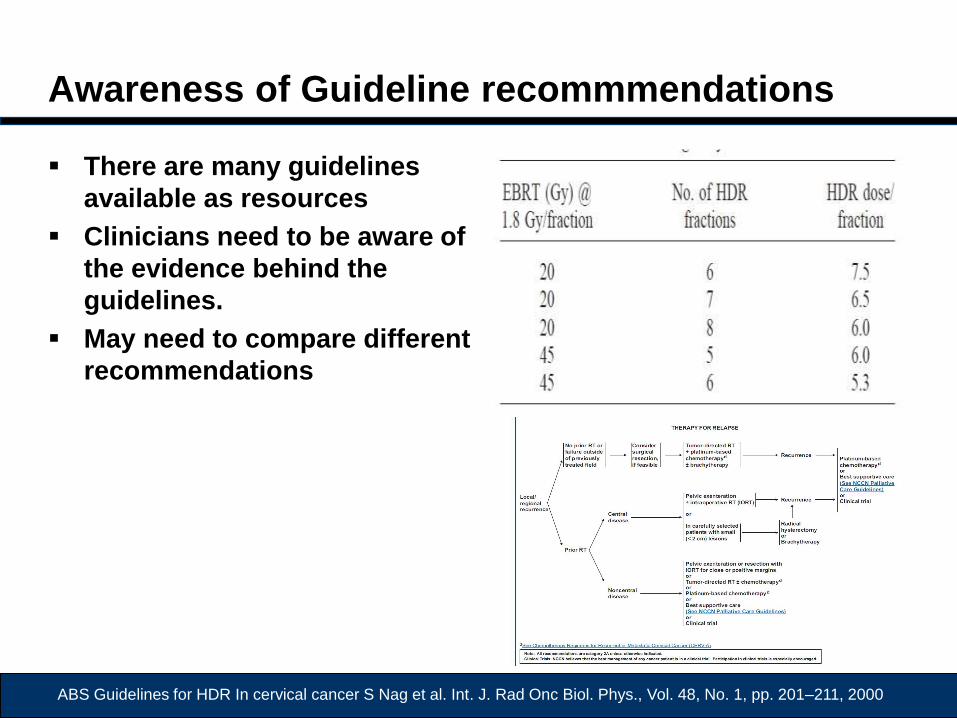
Awareness of Guideline recommmendations
There are many guidelines
available as resources
Clinicians need to be aware of
the evidence behind the
guidelines.
May need to compare different
recommendations
ABS Guidelines for HDR In cervical cancer S Nag et al. Int. J. Rad Onc Biol. Phys., Vol. 48, No. 1, pp. 201–211, 2000

Guidelines vs Guidelines : Which do we use?
http://www.uspreventiveservicestaskforce.org/uspstf/uspscolo.htm Accessed 23 Nov 2014

NCCN Guideline on Cervical Cancer 2010
All recommendations are
category 2A unless stated
otherwise

Relevance of trail results versus real world
clinical practice
O’Shaughnessy J et al J Clin Oncol 20:2812-2823
Although overall survival was demonstrated, regime was
not widely used due to toxicity

Why do Malaysian guidelines advocate MDT
decisions?
Because we believe it improves outcomes and reduces
variability in treatment and improves cost-effectiveness
Evidence from UK NHS case control study
Definition of MDT
• A specialist breast surgeon operating
• on > 50 breast cancers per year.
• Plus a pathologist, oncologist, radiologist, specialist nurse.
• Evidence based guidelines.
• Formal weekly MDT meeting.
• Audit of clinical activity.
Ref: Eileen Kesson. The influence of MDT care on survival from Breast Cancer. NCIN & UKACR London, June 2011. URL:
www.ncin.org.uk/view?rid=712. Accessed Nov 20, 2014
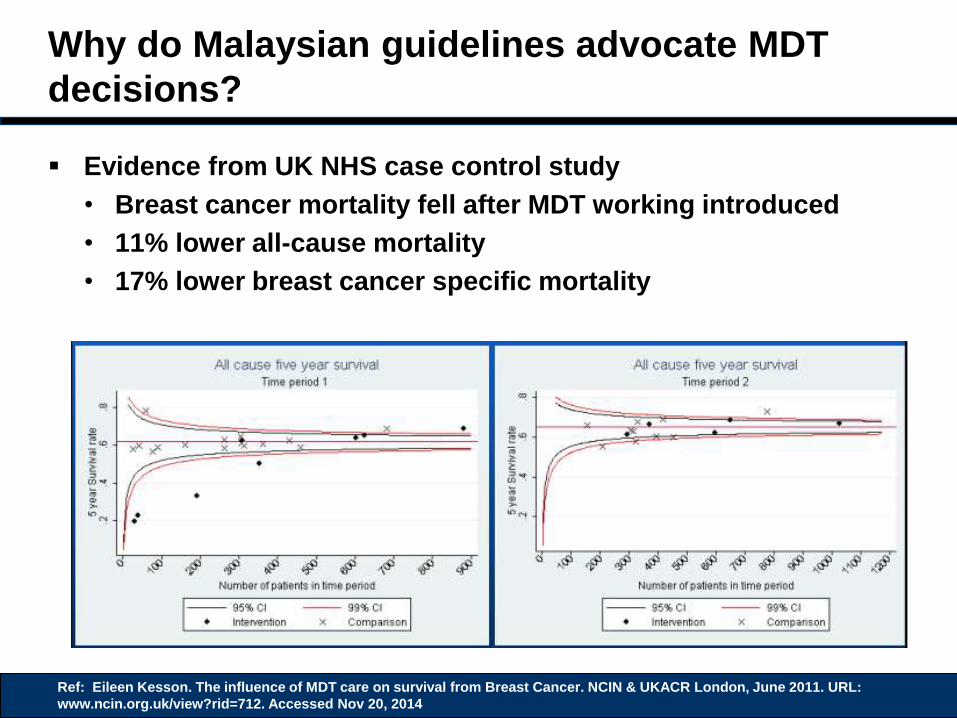
Why do Malaysian guidelines advocate MDT
decisions?
Evidence from UK NHS case control study
• Breast cancer mortality fell after MDT working introduced
• 11% lower all-cause mortality
• 17% lower breast cancer specific mortality
Ref: Eileen Kesson. The influence of MDT care on survival from Breast Cancer. NCIN & UKACR London, June 2011. URL:
www.ncin.org.uk/view?rid=712. Accessed Nov 20, 2014

Why do Malaysian guidelines advocate MDT
decisions?
Evidence from UK NHS case control study
• Breast cancer mortality fell after MDT working introduced
• 11% lower all-cause mortality
• 17% lower breast cancer specific mortality
Ref: Eileen Kesson. The influence of MDT care on survival from Breast Cancer. NCIN & UKACR London, June 2011. URL:
www.ncin.org.uk/view?rid=712. Accessed Nov 20, 2014

Why do Malaysian guidelines advocate palliative
care expertise be available?
Palliative care process enhances patient satisfaction, quality of
care, and outcomes while reducing costs.
– Verret D, Rohloff RM. The value of palliative care.. Healthc Financ Manage.
2013 Mar;67(3):50-4.
“There are no examples of chemotherapy that save money
compared to best supportive care”
– Payne SK et al. The Health Economics of Palliative Care.
http://www.cancernetwork.com/review-article/health-economics-palliative-care-1
Payne SK et al. The Health Economics of Palliative Care. http://www.cancernetwork.com/review-article/health-economics-palliative-
care-1

Why do Malaysian guidelines advocate palliative
care expertise be available?
• OS better with novel
therapy
• QOL better
• hazard ratio for death in
the standard care
group, 1.70; 95% CI,
1.14 to 2.54; P = 0.01
Temel JS. N Engl J Med 2010;363:733-42.
Early
supportive
care
Care when
symptoms
progress
“targeted treatment”
was supportive care

How can we improve Malaysian Guidelines?
By being explicit about the clinical effectiveness of the
interventions
• In terms of clinically relevant end points – not surrogate end
points
• Overall Survival – Not DFS, PFS = Added Life Years (ALYs)
• Quality of life – Not Toxicity scores = Q
• The metric for our key endpoints; Q x ALY = QALY
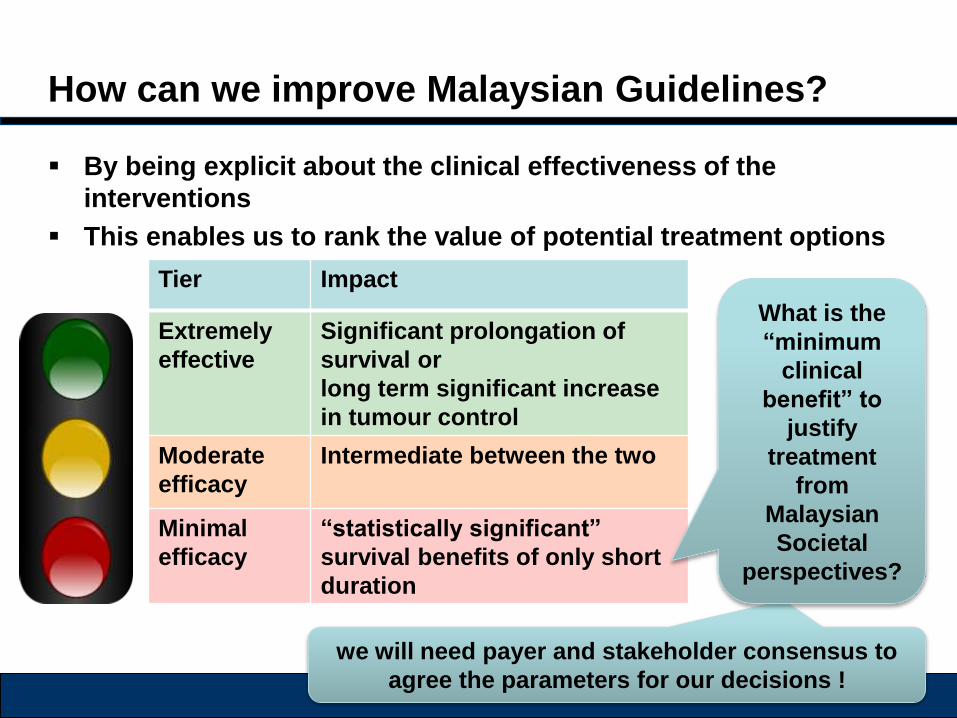
How can we improve Malaysian Guidelines?
By being explicit about the clinical effectiveness of the
interventions
This enables us to rank the value of potential treatment options
Tier Impact
Extremely
effective
Significant prolongation of
survival or
long term significant increase
in tumour control
Moderate
efficacy
Intermediate between the two
Minimal
efficacy
“statistically significant”
survival benefits of only short
duration
we will need payer and stakeholder consensus to
agree the parameters for our decisions !
What is the
“minimum
clinical
benefit” to
justify
treatment
from
Malaysian
Societal
perspectives?

How can we improve Malaysian Guidelines?
Resource issues:
International Guidelines from the EU and USA
are freely available
• But may not be relevant from a Malaysian
perspective
Writing guidelines relevant to Malaysia takes
time and resource
• Access to medical libraries
• MDT input implies staff time will be needed
away from clinical duties
• The ability to involve stakeholders from
payers and the patient advocacy groups
Initial guidelines will require the most resource,
subsequent revisions should prove easier

How to improve Malaysian Guidelines :
Language issues
The language used in guidelines show be easily understood
Use of technical English may need to be controlled

Standards for Malaysian Guidelines
Good clinical guidelines should be:

Questions & Discussion
“Knowing is not enough; we must apply.
Willing is not enough; we must do.”
—Goethe

















