Pan African Medical Journal – ISSN: 1937- 8688 (www.panafrican-med-journal.com) Published in partnership with the African Field Epidemiology Network (AFENET). (www.afenet.net)
Research
Open Access
Page number not for citation purposes 2
Introduction The lymph nodes are an integral part of the immune system, a complex system whose job is to adequately deal with foreign substances [1]. Mature lymphocytes are distributed throughout the body, where they are arranged in aggregations that exhibit various degrees of structural organisation. Individual lymphocytes are found in most loose supporting tissues and amongst epithelial cells, particularly the epithelium of the gastrointestinal and respiratory tracts. In addition, large non-encapsulated aggregations of lymphocytes are found in the walls of these tracts including the palatine tonsils and the Peyer patches of the small intestine [2]. Many lymphocytes are, however, located in encapsulated, highly organised structures called lymph nodes, which are interposed along the larger regional vessels of the lymph vascular system. Lymph nodes tend to occur in groups, particularly in areas where the lymphatics converge to form larger trunks as in the neck, axilla, groin, lung hilum and paraaortic regions [2]. Lymph nodes provide the perfect location for lymphocytes to be exposed to a wide variety of antigens and to undergo stimulation [2]. As lymph nodes deal with antigens, their histology reflects the reactivity of the immune system; the nature of the antigen determines whether a reaction will be mounted against it but also determines what effector cells will be employed. This will be reflected in the morphology of the lymph nodes [2]. Peripheral lymph node enlargement in adults signifies an underlying disease and has continued to pose a diagnostic dilemma to the physician. Several reports from the tropics document tuberculosis and other infectious aetiologies to be major causes of lymph node enlargement [3-6]. In contrast, malignancies are reported as the predominant causes of lymph node enlargement in the developed countries with rarity of infections [7]. However, an upsurge in the incidence of tuberculosis attributed to the advent and preponderance of HIV infection has been documented worldwide [7]. Malignancy is reported to be the most common cause of superficial lymphadenopathy in Lagos metropolis while tuberculosis is the most common in Ibadan and northern parts of Nigeria. and the age, sex and site prevalence agree with reports from some other parts of Nigeria and Africa with minimal variations in these studies [3-6]. Considering the plethora of diseases that may cause lymphadenopathy, it is essential to define the pattern of disorders presenting as lymph node enlargement in a particular environment [3]. This study aims at providing an update on the histopathological causes of peripheral lymphadenopathy and the pattern of lymph node distribution in patients seen in the University College Hospital, Ibadan, Nigeria. It is believed that information derived from this study will be of immense value to the clinician in managing patients presenting with lymphadenopathy in contemporary times.
Methods All lymph node biopsies received at the Department of Pathology, University College Hospital, Ibadan, Nigeria between January 1st 2003 and December 31 st 2012 were reviewed. The age, sex, clinical diagnosis and anatomical location of the site of biopsy were obtained from the request cards. The relevant slides were retrieved from the archives of the Department of Pathology. Where necessary, new slides were made from formalin fixed, paraffin embedded blocks and stained with haematoxylin and eosin stain. Special stains including Ziehl-Neelsen to demonstrate acid-fast bacilli; and periodic acid Schiff and Gomori methenamine silver stains to demonstrate fungal organisms were used where indicated. Immunohistochemistry was also performed. Inclusion criteria: all
the lymph node biopsies processed with satisfactory and adequate tissue section within the period of review.Exclusion criteria: all the cases with incomplete data in their request cards and poorly processed biopsies were excluded from this review.
Results A total of 429 lymph nodes biopsies seen in the Department of Pathology, University College Hospital, Ibadan between 2003 and 2012, were reviewed, constituting 1.15% of the total biopsies reviewed in the department during the study period. The year with the highest number of lymph node biopsies was 2011 with 52 cases (12.4%) Of the 429 lymph node biopsies reviewed, 251 cases (58.5%) were in females, while 178 cases (41.5%) were in males, with a male to female ratio of 1:1.4 The age range of the patients was 2 months to 105 years, with peak age incidence in the sixth decade For females the peak incidence was in the sixth decade of life while for males, it was in the second decade of life (χ2 = 39.4, df = 10, p = 0.000). The mean age of the 429 patients was 38.6 (+21.4) years. The mean age of the females (41.4-18.8 years) was significantly greater than that of males (34.5-24.1 years), (t = 3.3, df = 427, p = 0.001) Of the 429 lymph biopsies, 288 (67.1%) had the regional site indicated. The commonest site of lymph node biopsies was axillary group of lymph nodes with 135 cases (31.5%), followed by cervical group of lymph nodes with 103 cases (24.0%) and intra-abdominal group of lymph nodes with 36 cases (8.4 %) Table 1. The biopsies were mostly taken from the cervical region in males in 62 cases (34.8%), followed by axillary in 23 cases (12.9%); while the axillary group was the commonest in females with 112 cases (44.6%) followed by cervical group of lymph nodes having 41 cases (16.3%). Variation in site distribution between males and females was statistically significant (χ2 = 61.6, df =13, p = 0.000) The commonest lymph node disease was metastatic cancer with 153 cases (35.7%) followed by reactive hyperplasia with 109 cases (25.4%) and then granulomatous diseases with 61 cases (14.2%). In males the commonest diagnosed disease was Non-specific hyperplasia with 61 cases (34.3%) followed by Non-Hodgkin lymphoma with 42 cases (23.6%) and metastasis with 39 cases (21.9%). In females the commonest diagnosis was metastasis with 114 cases (45.4%) followed by non-specific hyperplasia with 48 cases (19.1%) and granulomatous inflammation in 39 cases (15.5%). This distribution is shown in Table 2. The variation in histological diagnosis with gender was statistically significant (χ2 = 9.3, df = 5, p = 0.000) Metastatic cancer had the highest mean age of occurrence of 46.5 followed by malignant lymphomas and non- specific hyperplasia with mean ages of occurrence of 38.4 and 34.7 years respectively.. The axillary group of lymph nodes had the highest number of cases of metastatic diseases with 75 cases (49%), followed by cervical group of lymph nodes with 22 cases (14.4%) and intra-abdominal group with 13 cases (8.5%) (Table 3). Non - specific hyperplasia was most common in the cervical group of nodes with 29 cases (26.6%), followed by the axillary group of lymph nodes which had 22 cases (20.1%) and the intra-abdominal group with 15 cases (13.8%). The granulomatous diseases were commonest in the cervical group of lymph nodes with 17 cases (27.9%) followed by the axillary nodes with 11 cases (18%). The non- Hodgkin lymphomas were most commonly diagnosed in the axillary region with 21 cases (27.6%) followed by cervical region with 18 cases (23.7%). Hodgkin lymphoma was most commonly diagnosed in the cervical region with 11 cases (46%) followed by the axillary region with 4 cases (16.7%). Table 3. 109 (25.4%) histologically confirmed cases of reactive hyperplasia was seen. Sixty-one (55.9%) occurred in males and 48 (44.1%) in females, with a male to female ratio of 1.4:1. There are 56 cases of
Page number not for citation purposes 3
follicular hyperplasia, 32 cases of sinus histiocytosis, 10 cases of parafollicular hyperplasia and 4 cases of dermatopathic lymphadenopathy. Fifty-six cases of Follicular Hyperplasia were seen constituting the highest proportion of non-specific hyperplasia (51.4%). They were diagnosed in all age groups with a peak in the 21-40 years age group and the highest number was seen in the neck group of lymph nodes. There were 32 cases of Sinus histiocytosis with 18 cases (56.3%) occurring in male and 14 cases (43.7%) in females. The commonest site of occurrence was the axillary group of lymph nodes. Parafollicular hyperplasia was diagnosed in 10 cases with seven cases (70%) in males and three cases (30%) in females. Peak age of occurrence was in ages 0-10 years with six cases (60%). The commonest group of lymph node affected was cervical. There were four cases of dermatopathic lymphadenopathy. Three of the cases are in male and one in female with two cases each in ages 11-20 years and 31-40 years. Three of the cases are in the cervical region. There were 61 cases of granulomatous lymphadenitis of which 39 cases (64%) were seen in females and 22 cases (36%) were seen in males giving a male to female ratio of 1:1.7.Thirty-nine cases (63.9%) occurred in ages 11-30 years. The highest incidence was in the cervical group of lymph nodes with 14 cases (23%) and the axillary group with 11 cases (18%). Figure 1 shows a representative photomicrograph of a case of chronic granulomatous inflammation due to tuberculous lymphadenitis. There were 100 cases of lymphoma, accounting for 23.3% of all lymph node biopsies. Seventy-six (76%) cases were non-Hodgkin lymphomas, while 24 (24%) were Hodgkin lymphomas. Forty-two cases of non-Hodgkins lymphomas occurred in males (55.3%) and 34 cases (44.7%) in females with a male to female ratio of 1.2:1. The commonest biopsy site was from the axillary group of lymph nodes with 21 cases (27.6%) followed by cervical group with 18 cases (23.7%). The mean age was 38.4 years with age range of 3-105 years. The blocks of cases were retrieved and subjected to immunohistochemistry and all the cases were B cell lymphomas using the following panels: CD 5, CD 10, CD 20, CD 23, Ki 67 and Bcl 2. The commonest type of non-Hodgkin lymphoma in both sexes was diffuse large B cell lymphoma with 34 cases (8.1%) followed by lymphoblastic lymphoma with 24 cases (5.7%) and small lymphocytic lymphoma with 18 cases (4.3%).Figure 2 show photomicrographs of representative case of non-Hodgkin lymphoma. The age range of patients with diffuse large B cell lymphoma was 10 months -76 years, that of lymphoblastic lymphoma was 5 -60 years while small lymphocytic lymphoma was seen in all age groups. All the sub types were seen in equal ratio in both sexes Three cases of Burkitt lymphoma were seen and they occurred in patients aged 8-13 years with two in the axillary group of lymph nodes and one in the inguinal group. There were 24 cases of Hodgkin lymphoma accounting for 5.6% of all lymph node biopsies with 12 cases in both male and female each giving a male to female ratio of 1:1. It occurred in all age groups. The commonest histological subtype in both males and females was the nodular sclerosis variant, accounting for 18 cases (4.3%). The commonest group of lymph nodes affected was cervical with a mean age of 36.3 and range of 5-80 years. Figure 3 shows photomicrographs of representative case of Hodgkin lymphoma. Metastatic diseases of lymph node accounted for 153 cases (35.7%) of all lymph node biopsies reviewed with 114 cases (74.5%) in females and 39 cases (25.5%) in males with a male to female ratio of 1:2.9 The group of lymph node most commonly involved was the axillary, with 79 cases (51.6%). The commonest primary site of malignancy metastasizing to the axillary lymph nodes was the breast, with 56 cases. Adenocarcinoma of unspecified primary site accounted for a total of 20 cases. There were 3 cases of metastatic sarcoma (two cases of leiomysarcoma and a case of fibrosarcoma) to the axillary lymph nodes. Metastasis to the cervical group is mostly of adenocarcinoma
(66.7%) and squamous cell carcinoma (33.3%). There was a case of malignant melanoma in the inguinal lymph node. Figure 4, Figure 5, Figure 6 show photomicrographs of representative cases of metastasis to lymph nodes. There were six miscellaneous lymph node diagnoses in the present study. Four of lymph node biopsies were categorized as normal lymph nodes. One case of Rosai-Dorfman disease was recorded in the cervical group of lymph nodes of an 11year old male. There was also a lymphoepithelial cyst involving the cervical lymph node of a 35 year old male.
Discussion Lymphadenopathy is one of the most common problems in clinical practice and offers an important diagnostic clue to the aetiology of the underlying condition [4]. The cause of lymphadenopathy often cannot be ascertained on clinical grounds alone and lymph node biopsy is commonly utilized to resolve this problem. Lymph node biopsies accounted for 1.15% of all surgical specimens received in the Department of Pathology University College Hospital Ibadan during the period of this study. This is lower than the figure of 2.1% cited by Anunobi et al from Lagos, Nigeria, and a frequency of 4% cited by Rahman et al from Bangladesh [4, 8]. This may be attributable to the rising use of cytology to make diagnosis in our centre thereby reducing the need for surgical biopsies of lymph node lesions, the ratio of cytology to histology of lymph node specimens in our centre increased from 1.4 : 1 in 2003 to 6 : 1 in 2012. The most common lymph node disease in the present study was metastases. This is similar to the findings of Anunobi et al from Lagos [4]. In an earlier study from Ibadan by Thomas et al (1995) [5] and in studies from Kano [6], Ilorin [12] and Benin [4] in Nigeria, as well as other studies from Bangladesh Rahman et al [8], India Kamal et al [9] and Ageep from Sudan [10], granulomatous lymphadenitis was the most common lymph node disease [9,11]. In some other studies from India- Vacchani et al, [11] and Ilorin, Nigeria -Oluwole et al, 1985 [12], non- specific hyperplasia was the most common lymph node disease. By contrast, Nadira et al [13] in a study from Bangladesh found that Malignant lymphomas were the most common causes of lymphadenopathy. In a study by Lee et al from U.S.A. [14] non specific hyperplasia was the most common lymph node disease. The observed frequency of 35.7% for metastatic lesions is relatively higher than that reported from previous studies in Nigeria,[4,5,12,15] which ranges between 19.3% and 33.6%. This finding may reflect the increasing burden of cancer in developing countries this is supported by the data from Ibadan Cancer Registry, which shows an increasing trend from 2001-2005 of all malignant tumours [16]. The WHO has projected that African countries will account for over a million new cancer cases a year and that by 2020, 70% of all new cases of cancer will be in developing countries where governments are least prepared to address the growing cancer burden and where survival rates are often less than half those of more developed countries. It is advocated that the only way to effectively prevent, detect and treat the rising number of cancers in the developing world is to develop broad and effective partnership of research institutions, international organisations, NGOs, national governments in developed and developing countries and pharmaceutical industries [17]. It was also noted in this study that 114(45.4%) of all the metastatic lesions occurred in females and that 75(65.8%) were in the axillary lymph nodes, both of which are mainly attributable to the high incidence of primary breast carcinoma in females in this environment [18]. Our findings are similar to those of Adeniji et al from Ilorin, Nigeria, who reported that breast carcinoma constituted about 50% of all metastasis to the axillary lymph node [15]. In this study, non-specific hyperplasia in the lymph nodes was next in frequency to metastatic lesions with 109(25.4%) cases and they included,
Page number not for citation purposes 4
follicular hyperplasia, sinus histiocytosis, parafollicular hyperplasia and dermatopathic lymphadenopathy. The high frequency seen in this study is in agreement with previous studies in Nigeria [4-6, 12, 15, 18-20] that recorded figures ranging from 10.5% to 31.4%. Kamal in India also noted it to constitute 30.7% and Rahman et al in Bangladesh reported that non-specific hyperplasia constituted 30.9% of cases of lymph node biopsies [9, 8]. Cervical and axillary regions were found to have the highest frequency of non-specific hyperplasia in this study. This is consistent with the findings of Rahman from Bangladesh [8] and Lee from the U.S.A [14]. This high frequency may in part be due to the increased frequency of reactive hyperplasia in lymph nodes draining malignant sites particularly ipsilateral carcinoma of the breast, which is of high incidence in these environments. However, Anunobi et al from Lagos, Nigeria [4] and Ageep from Sudan [10] reported that the inguinal lymph nodes constituted the highest group of nodes involved with reactive hyperplasia. The high frequency of inguinal non-specific lymphadenitis is probably attributable to repeated infections and trauma involving the feet due to tendency of walking barefooted among Africans [21]. Malignant lymphoma was the third commonest cause of lymphadenopathy constituting 100(23.3%) of all biopsies in the present study. Non-Hodgkin lymphoma accounted for 76% and Hodgkin lymphoma for 24% of cases. This is similar to the findings from other parts of Nigeria [4-6,12, 15, 19] and also in Caucasians [14]. In a previous 15-year review of lymphomas diagnosed both on the basis of biopsy and cytology, Oluwasola et al, also from Ibadan, noted that 558 (87.5%) of the 638 cases of lymphomas were non-Hodgkin lymphomas [22]. In agreement with the findings in the present study, Olu-Eddo et al reported that lymphomas comprised 26.2% of lymph node biopsies in Benin, Nigeria, with 66.4% being non-Hodgkin lymphomas [22]. Anunobi et al. from Lagos reported a lower frequency of 14.2% of all lymph node biopsies, with 61% of cases of lymphoma being non-Hodgkin lymphomas [4]. Ageep from Sudan reported that lymphomas accounted for 16.6% of all lymph node biopsies, with non-Hodgkin lymphoma accounting for 86.7% of all lymphomas [10]. Rahman et al from Bangladesh also noted that non-Hodgkin lymphoma constituted 66.7% and Hodgkin lymphoma 33.3% of all malignant lymphoma seen [8]. Lee et al. from U.S.A. also reported that non- Hodgkin lymphoma constituted 65% and Hodgkin lymphoma 35% of all malignant lymphomas [14]. This study also noted that non-Hodgkin lymphomas was more common in males, with a male to female ratio of 1.2:1. This ratio is similar to the findings of Mondal et al from India that also reported a male to female ratio of 1.2:118. It is however lower than the figures of 1.5:1 reported in the previous study of Oluwasola et al from Ibadan [22] and 3.3:1 was reported by Olu-Eddo et al. from Benin [3]. In the present study, the mean age of patients with non-Hodgkin lymphoma was 38.4 years, which is higher than that of 29.8 years previously reported by Oluwasola et al from Ibadan [22], this may be attributable to the inclusion of cytologically diagnosed cases in the study by Oluwasola et al because lymph node swellings in lower age groups are subjected to cytological evaluation more often compared to those in adults. However it is comparable to that of 39.4 years reported by Mondal et al from India [23]. Immunohistochemistry done on all the cases and all came out to be B-cell lymphomas. In a previous study from Ibadan, Thomas et al reported that 86.2% of non-Hodgkin lymphomas were B cell lymphomas [6]. The failure to retrieve all the blocks of lymphoma cases in our studies probably introduced a significant bias in our results. Mondal et al from India [22] and Almasri et al [24] from Jordan reported that B cell lymphomas accounted for 74.1% and 86% of all lymphomas, respectively. In this study, the common histological variants of non-Hodgkin lymphoma were diffuse large B cell lymphoma (44.8%), lymphoblastic lymphoma (31.5%) and small lymphocytic lymphoma
(23.8%). In the study by Oluwasola et al [22], (which did not include immunohistochemistry) large cell lymphomas is the most common type of non-Hodgkin lymphomas. In agreement with the present study, Mondal et al from India [23] and Almasri et al from Jordan [24] reported that large B cell lymphomas were the most common sub type of non-Hodgkin lymphomas, accounting for 35.2% and 53.2% of all non-Hodgkin lymphomas, respectively. In this study, patients with Hodgkin lymphoma had a mean age of 36.3 years, which is similar to the findings of Mondal et al from India [23], which reported a mean age of 31.3 years. The most frequent lymph node group involved by Hodgkin lymphoma was cervical, closely followed by axillary and this is similar to reports from previous studies in Nigeria [12,18,20] and India [23]. Nodular sclerosis variant of Hodgkin lymphoma was commonest in this study, followed by the mixed cellularity variant. This is in agreement with the findings of a previous study of lymphoma from Ibadan by Oluwasola et al [22], which also reported nodular sclerosis, Hodgkin lymphoma as the commonest variant, followed by mixed cellularity Hodgkin lymphoma. In contrast to our findings Mondal et al [23] found mixed cellularity variant to be commoner than nodular sclerosis variant among Indian patients with Hodgkin's lymphoma. The reason for this geographical difference is not precisely apparent. Granulomatous lesions of the lymph nodes also constituted a significant cause of lymph node lesions in this study accounting for 14.2% of all cases. This figure is however lower than the findings of studies [4-6,12,15,19,20] from other parts of Nigeria with a range of 14.9% to 31.4 % and differs from findings in other developing countries like India (Karnataka) with 58.2% [9]. The latter figure is supported by the report of a rising incidence of tuberculosis in India [25]. Lee et al. reported a relatively lower figure from U.S.A. where it constitutes 11.2% [14]. The lower figure in the latter study may be attributable to the relatively lower incidence of tuberculosis in developed countries like U.S.A. In the present study, granulomatous lesions affected mainly the cervical lymph nodes, with a female preponderance and with a peak in 11-30 years age category, and with only 10 cases above the age of 41 years. All the cases of granulomatous diseases were subjected to special stains: ZN, PAS and GMS and all the cases came out to be of tuberculous origin. These findings are in agreement with what was reported in other similar studies from Nigeria [4, 15]. Anunobi et. al. cited cervical lymph node to be the commonest involved region and that 16-25 years age group recorded the highest cases constituting 29% out of a total of the 125 cases4. Also Olu-Eddo et al [19] from Benin, Eastern Nigeria reported that 85 out of the 114 cases were in the cervical nodes and that 92.8% of cases occurred before the age of 45 with most cases being between ages 15-24 years [19]. Lee et al [14] from U.S.A. also reported that 81% of cases occurred in the cervical and supraclavicular regions with 53 out of 73 cases (72,6%) occurring before the age of 40 years [14]. The commonest cause of granulomatous lymphadenitis in all these studies in this age range is tuberculosis and it has been attributed to low immunity, low socioeconomic class and malnutrition in African children. These findings also suggest that tuberculous lymphadenitis has a predilection for cervical lymph node group. This is supported by the work of Maharjan et al. in Nepal, South Asia [26]. Surprisingly in this study, granulomatous lymphadenitis and reactive hyperplasia accounted for a lower percentage, which may be due to the increasing use of cytology for diagnosing these conditions, followed by use of antibiotics, which usually resolves tuberculous or bacterial infections, thereby reducing their number in surgical biopsy samples.
Page number not for citation purposes 5
Conclusion The study has shown that the commonest causes of lymphadenopathy in this environment are metastatic cancer, reactive hyperplasia and granulomatous diseases. Metastatic cancer is predominantly found in female whereas reactive hyperplasia is relatively more common in males. In both male and female children reactive hyperplasia was the most common cause of lymphadenopathy. The relatively lower frequency of granulomatous diseases in this study compared to earlier studies can be partly explained by increasing use of cytology for diagnosis. It was also noted that commonest sites of involvement are axillary followed by the neck and intra-abdominal lymph nodes. Histochemical stains and immunohistochemistry were useful in resolving diagnosis in selected cases. What is known about this topic
• That tuberculosis use to be the commonest cause of peripheral lymph node enlargement in this environment.
• The second most common cause of peripheral lymphadenopathy is lymphoma and it's the commonest cause of malignant lymph node lesions. .
• Metastatic and reactive hyperplasia as cause of lymph node is of lower frequency.
What this study adds
• That the commonest cause of peripheral lymphadenopathy in this environment now is metastatic cancer.
• The second most common cause of peripheral lymphadenopathy in this environment now is reactive hyperplasia.
• Its discovered in the study now that tuberculosis as a cause of peripheral lymphadenopathy in this environment is now of a lower frequency.
Competing interests The author declare no competing interests.
Authors’ contributions All authors read and agreed to the final version of this manuscript and equally contributed to its content and to the management of the case.
Acknowledgments This is to all secretariat staff, laboratory staff and the consultants in the Department of Pathology, University College Hospital Ibadan for making this work a reality.
Tables and figures Table 1: Sex and region distribution of lymph node enlargement in 429 patients Table 2: Sex distribution of patients in relation to histological diagnosis of nodal diseases.
Table 3: Anatomical distribution of different histological categories of lymph node diseases Figure 1: Photomicrograph showing a case of chronic granulomatous lymphadenitis in the cervical lymph node of a 14-year-old female Figure 2: Photomicrographs showing a case of small lymphocytic lymphoma in the cervical lymph node of a 60-year-old female Figure 3: Photomicrographs showing a case of a mixed cellularity hodgkin lymphoma in the cervical lymph node of a 25-year-old female Figure 4: Photomicrographs showing a case of metastatic mucinous adenocarcinoma in the axillary lymph node of a 65-year-old male Figure 5: Photomicrographs showing a case of metastatic leiomyosarcoma in the axillary lymph node of a 35-year-old female Figure 6: Photomicrographs showing a case of metastatic malignant melanoma in the inguinal lymph node of a 42-year-old male
References 1. Van der Valk P, Meijer CJLM. Lymph nodes In: Histology for
Pathologists. Lippincott Williams & Wilkins, New York. 2007: 764-778. PubMed | Google Scholar
2. Young B, Lowe JS, Stevens A, Heath JW, Deakin PJ. Lymph
nodes In: wheater's Functional Histology. Elsevier, Edinburgh. 2006:218-22. Google Scholar
3. Olu-Eddo AN, Egbagbe EE. Peripheral lymphadenopathy in
EK. Review of the histopathologic pattern of superficial lymph node diseases in Lagos. Niger Postgrad Med J. 2008; 15(4), 243-6. PubMed | Google Scholar
5. Thomas JO, Ladipo JK, Yawe T. Histopathology of
lymphadenopathy in a tropical country. East Afr Med J. 1995; 72(11): 703-5. PubMed | Google Scholar
6. Ochicha O, Edino ST, Mohammed AZ, Umar AB, Atanda AT.
Pathology of peripheral lymph node biopsies in Kane, Northern Nigeria. Ann. 2007; 6(3): 104-8. PubMed | Google Scholar
7. Ioachim HL, Medeiros L J. Ioachim's lymph node pathology, ed.
4. Philadelphia, Lippincott Williams & Wilkins, 2008. Google Scholar
8. Rahman A, Biswas MA, Siddika ST, Sikder AM.
Histopathological evaluation of lymph node biopsies: A hospital based study. J Enam Med Col. 2012; 2(1):8-14. PubMed | Google Scholar
9. Kamal GC. A ten year histopathological study of generalised
lymphadenopathy in India. S Afr Fam Pract. 2011; 53(3):267-270. PubMed | Google Scholar
10. Ageep AK. Assessment of adult peripheral lymphadenopathy in
Red Sea State Sudan. Int Journal of Tropical Diseases and Health. 2012; 2 (1): 24-32. PubMed | Google Scholar
11. Vacchani A, Bhuva K, Jasani J, Patel D, Savjiani N, Patel K et al
.Histopathological study of lymph node biopsy. IJBAR. 2013; 04 (11). PubMed | Google Scholar
15. Adeniji KA, Anjorin AS. Peripheral lymphadenopathy in Nigeria.
Afr J Med Med Sci. 2000; 29(3-4): 233-7.PubMed | Google Scholar
16. Abdulkareem FB. Neoplasia 1- Cancer epidemiology and
carcinogenesis: National Postgraduate Medical College of Nigeria. Update and Revision Course. February 2013. Google Scholar
17. London Declaration on Cancer Control in Africa: 2007; London
U.K. Google Scholar 18. Akarolo SN, Ogundiran TO, Adebamowo CA. Emerging breast
cancer epidemic: evidence from Africa. Breast cancer research. 2010; 12 (suppl 4): S8. PubMed | Google Scholar
19. Olu-Eddo AN, Ohanaka CE. Peripheral lymphadenopathy in
Nigeria adults. J Pak Med Assoc. 2006;56(9); 405-8. PubMed | Google Scholar
20. Obafunwa JO, Olomu LN, Onyia NJ. Primary peripheral lymphadenopathy in Jos, Nigeria. West Afr J Med. 1992; 11(1): 25-8. PubMed | Google Scholar
21. Aster JC. Diseases of White blood cells, Lymph Nodes, Spleen
and Thymus; In: Robbins and Cotran Pathologic Basis of Disease: Saunders. Elsevier, Philadelphia. 2010: pages 598-638. Google Scholar
22. Oluwasola AO, Olaniyi JA, Otegbayo JA, Ogun GO, Akingbola
TS, Ukah CO et al. A fifteen- year review of lymphomas in a Nigerian tertiary healthcare centre. J Health Popul Nutr .2011; 29(4): 310-316. PubMed |Google Scholar
Roy S. Malignant lymphoma in Eastern India: A retrospective analysis of 455 cases according to World Health Organisation classification. Indian J Med Paediatric Oncol. 2013:34 (4): 242-246. PubMed | Google Scholar
lymphoma in Jordan: Types and patterns of 111 cases classified according to the WHO classification of haematological malignancies. Saudi Med J. 2004; 25 (5): 609-614. PubMed | Google Scholar
25. Chakraborty AK. Epidemiology of tuberculosis current status in
India. Indian J Med Res. 2004; 120(4): 248-276. PubMed | Google Scholar
26. Maharjan M, Hirachan S, Kafle PK, Bista M, Sherstha S, Toran
KC et al.Incidence of tuberculosis in enlarged neck nodes, our experience. Kathmandu Univ Med J (KUMJ). 2009; 7(25) 54-8. PubMed | Google Scholar
Table 1: sex and region distribution of Lymph Node Enlargement in 429 patients
Region Female Male Total
Percentage (%)
Cervical 41 62 103 24.0
Intra-abdominal 15 21 36 8.4
Axillary 112 23 135 31.5
Inguinal 7 7 14 6.3
Unknown 76 65 141 32.9
Total 251 178 429 100
Table 2: sex distribution of patients in relation to histological diagnosis of nodal diseases
Diseases Female (%)
Male (%)
Total (%)
Non-Hodgkin lymphoma
34(13.5) 42(23.6) 76(17.7)
Hodgkin lymphoma 12(4.5) 12(6.7) 24(5.6)
Metastatic cancer 114(45.4) 39(21.9) 153(35.7)
Non-specific hyperplasia
48(19.1) 61(34.3) 109(25.4)
Granulomatous 39(15.5) 22(12.4) 61(14.2)
Others 4(1.6) 2(1.1) 6(1.4)
Total 251(100) 178(100) 429(100)
Page number not for citation purposes 7
Table 3: anatomical distribution of different histological categories of lymph node diseases
Site Non Hodgkin Lymphoma
Hodgkin Lymphoma
Metastasis Reactive hyperplasia
Granulomatous Others Total
Cervical 18 11 22 29 17 4 103
Intra Abdominal
3 2 13 15 4 0 36
Axillary 21 4 75 22 11 1 135
Inguinal 5 0 2 5 2 0 14
Unknown 29 7 41 32 27 1 141
Total 76 24 153 109 61 6 429
Figure 1: Photomicrograph showing a case of chronic granulomatous lymphadenitis in the cervical lymph node of a 14-year-old female
Figure 2: Photomicrographs showing a case of small lymphocytic lymphoma in the cervical lymph node of a 60-year-old female
Page number not for citation purposes 8
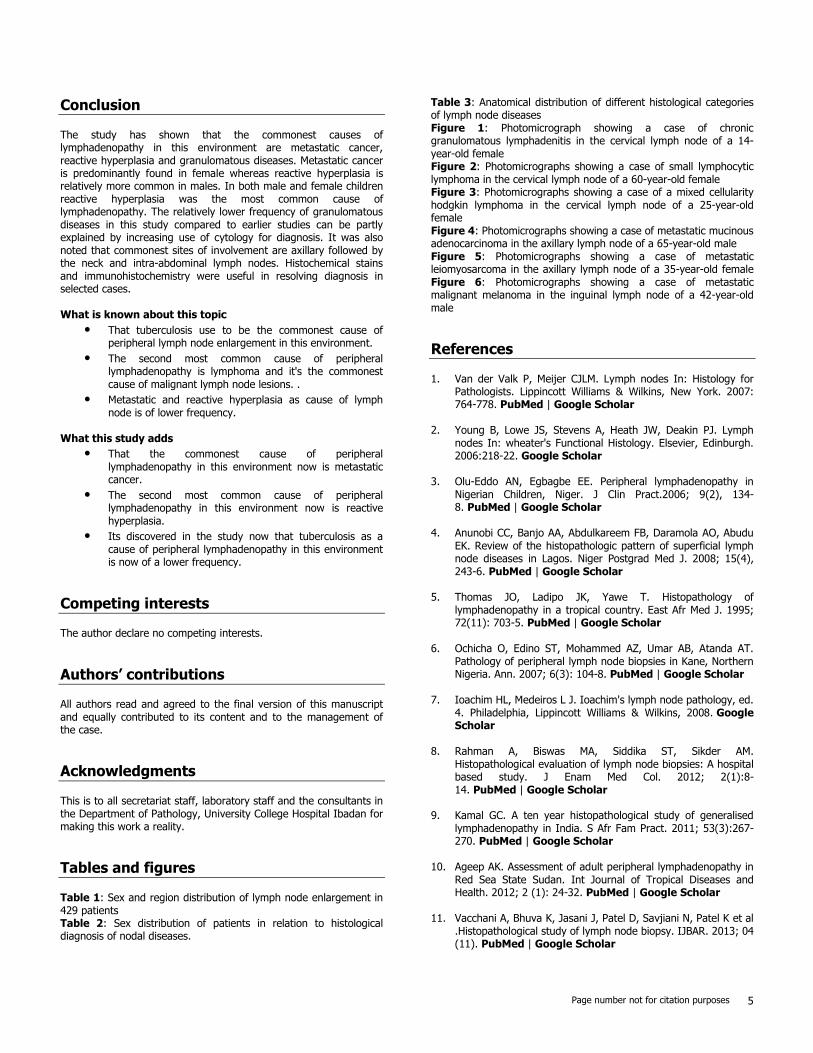
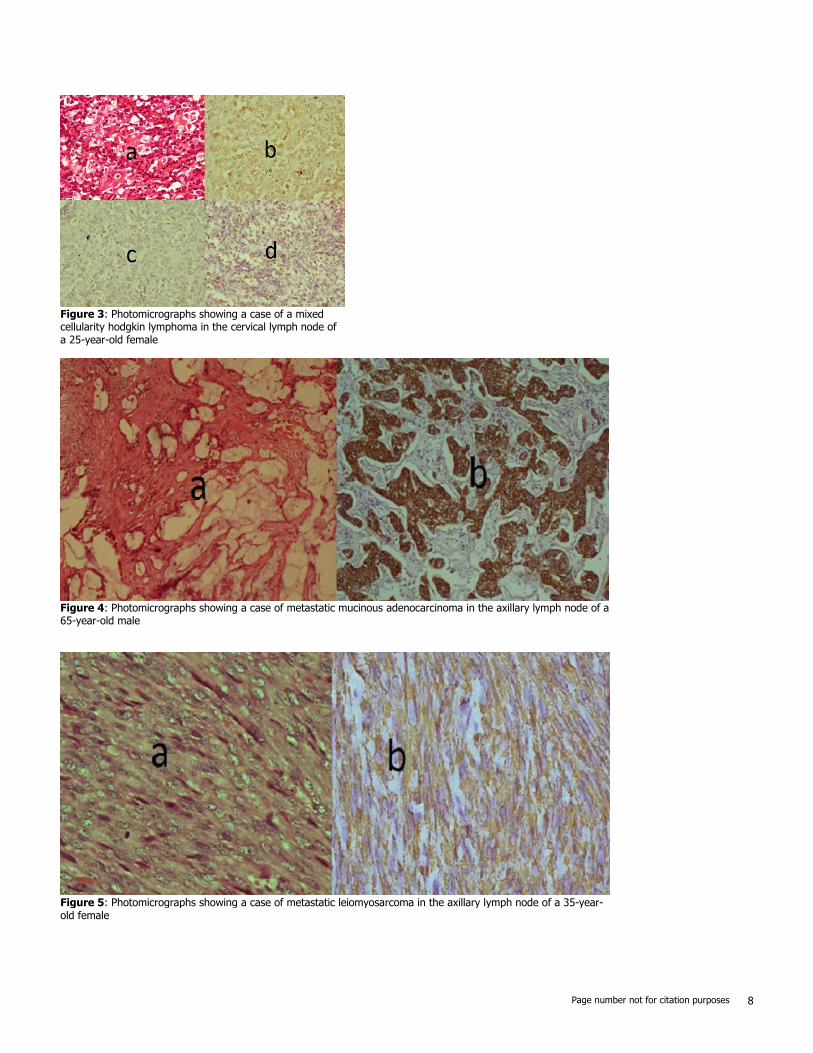
Figure 3: Photomicrographs showing a case of a mixed cellularity hodgkin lymphoma in the cervical lymph node of a 25-year-old female
Figure 4: Photomicrographs showing a case of metastatic mucinous adenocarcinoma in the axillary lymph node of a 65-year-old male
Figure 5: Photomicrographs showing a case of metastatic leiomyosarcoma in the axillary lymph node of a 35-year-old female
Page number not for citation purposes 9
Figure 6: Photomicrographs showing a case of metastatic malignant melanoma in the inguinal lymph node of a 42-year-old male