42


GENERAL INFORMATION
This Benefits Handbook is provided to employees as a comprehensive resource for the City’s benefits. This Handbook is not intended to be a contract (expressed or implied), nor is it intended to otherwise create any legally enforceable obligations on the part of the City, its agents, or its employees. The purpose of this Handbook is to summarize the City’s employee benefits and the policies and procedures regarding these benefits. For the most detailed and up-to-date information, please refer to the appropriate plan document, evidence of coverage booklet, insurance policy or contract, as well as applicable rules, regulations, resolutions, ordinances and Memoranda of Understanding/Memoranda of Agreements. These documents can be obtained by from the Stop W: Drive in the HR Resources folder.
1
TABLE OF CONTENTS
Open Enrollment News ............................................................................. 2 Dates & Action Items ................................................................................... 3 Plan Rates & Changes ............................................................................. 4-5
Life Events ................................................................................................. 6
Medical Insurance .................................................................................. 7-8 Medical Plan Contact Information and Websites .................................... 9-10
Dental Insurance ..................................................................................... 11 Dental Insurance Comparison ................................................................... 12
Vision Insurance ..................................................................................... 13
Basic Life Insurance & AD&D ................................................................ 14 Voluntary Additional Life Insurance ........................................................... 14
Optional Benefits .................................................................................... 15 Employee Assistance Program (EAP) ....................................................... 15 Flexible Spending Account (FSA) ............................................................. 16 Healthcare Reimbursement Account Worksheet ....................................... 17 Healthcare Reimbursement Account Eligible/Ineligible Expenses ........... 18 Dependent Care Reimbursement Account Worksheet ............................. 19
Deferred Compensation Plans – 401(k) and 457 ............................. 20-21
Employee Benefit Notices ................................................................. 21-39 Medicare Part D Notice of Creditable Coverage .................................. 22-23 Consolidated Omnibus Budget Reconciliation Act (COBRA) ............... 24-27 Womens’ Health and Cancer Rights Act ................................................... 28 Newborns’ and Mothers’ Health Protection Act ......................................... 28 Notice of Privacy Practices ................................................................... 29-35 Domestic Partner Information ............................................................... 36-37
New Health Insurance Marketplace Coverage Options and Your Health Coverage .................................................................................. 38-39
2
IMPORTANT OPEN ENROLLMENT NEWS
2019 PLAN YEAR
Open Enrollment will begin on Monday, September 10, 2018, and end at 5:00 p.m. on Friday, October 5, 2018. Please review the information contained in this handbook before making benefit decisions. Health insurance forms and information are also available on the Stop W: Drive in the HR Resources folder, and at www.calpers.ca.gov (medical insurance information).
During the open enrollment period, employees may:
• Enroll, change, or opt out of health plans. Plan changes are effective: January 1, 2019. Employees who do not make plan changes on or before October 5, 2018, must wait until the 2020 Open Enrollment period (approx. September 2019) unless there is a qualifying life event (see Life Events section on page 7).
• Add or delete eligible dependents to medical, dental, and/or vision care. If you wish to add a new dependent to your medical insurance, you will be required to provide a copy of your marriage certificate (adding a spouse), or birth/adoption certificate (adding a child) to Human Resources before Open Enrollment ends.
• Purchase additional life insurance for you and/or your spouse/domestic partner.
• Enroll in the medical or dependent care flexible spending account (FSA) reimbursement programs. If you wish to contribute to a medical and/or dependent care reimbursement account for the 2019 plan year, you MUST enroll or re-enroll during the Open Enrollment period, or within 30 days of a qualifying life event. Enrollment does not automatically continue from year to year. Online enrollment instructions are available in the Stop W: Drive HR Resources folder.
Purchase or change Aflac optional insurances, such as accident, critical care, hospital, short-term disability, and cancer insurance. Contact Jeff Boykins at (818) 468-6216 or [email protected] to schedule an appointment.

3
2019 OPEN ENROLLMENT – DATES & ACTION ITEMS
Monday, September 10
Open Enrollment Begins
Wednesday, September 26
PSC Sanitation East Lunch Room, starting at 8 a.m.
City Hall Lunch Room, starting at 1 p.m.
Flu Shots – By Appointment Only. More information to follow.
Thursday, September 13
Open Enrollment Meetings
9:00 a.m. - City Hall Council Chambers
Representatives from some of the medical plans, dental, vision, EAP, Standard (life insurance), and Aflac plans will be in attendance to
provide information and answer questions.
Wednesday, September 19
8:00 a.m. - PSC/Sanitation Training Room
This meeting will include representatives from the dental, vision, EAP, Standard (life insurance), and Aflac plans only. Medical plan
representatives will only be available during the 9/13/18 meeting.
September 20
@ PSC
September 18 and 25
@ City Hall
Individual meetings with Aflac Representative
Contact Jeff Boykin, Alfac Representative at (818) 468-6216 or
[email protected] to schedule an appointment.
October 5
OPEN ENROLLMENT ENDS!
LAST DAY TO MAKE ENROLLMENT CHANGES FOR THE 2019 PLAN YEAR
4
2019 OPEN ENROLLMENT – PLAN RATES & CHANGES
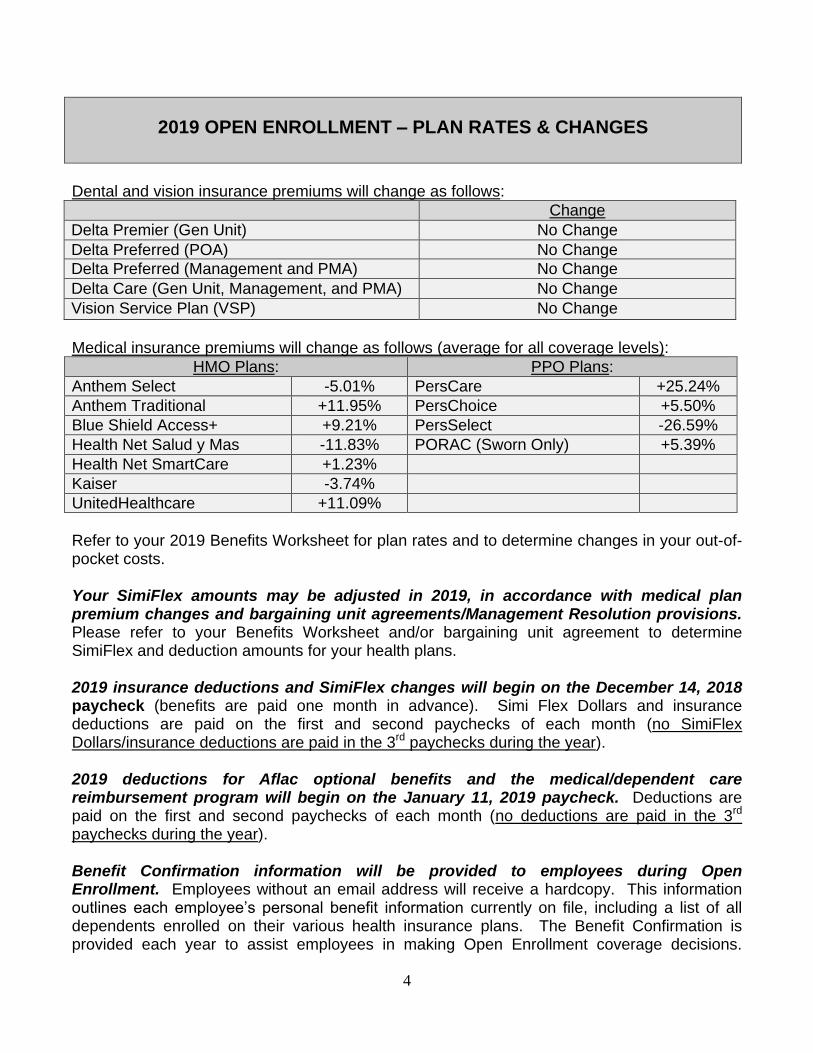
Dental and vision insurance premiums will change as follows:
Change
Delta Premier (Gen Unit) No Change
Delta Preferred (POA) No Change
Delta Preferred (Management and PMA) No Change
Delta Care (Gen Unit, Management, and PMA) No Change
Vision Service Plan (VSP) No Change
Medical insurance premiums will change as follows (average for all coverage levels):
HMO Plans: PPO Plans:
Anthem Select -5.01% PersCare +25.24%
Anthem Traditional +11.95% PersChoice +5.50%
Blue Shield Access+ +9.21% PersSelect -26.59%
Health Net Salud y Mas -11.83% PORAC (Sworn Only) +5.39%
Health Net SmartCare +1.23%
Kaiser -3.74%
UnitedHealthcare +11.09%
Refer to your 2019 Benefits Worksheet for plan rates and to determine changes in your out-of-pocket costs. Your SimiFlex amounts may be adjusted in 2019, in accordance with medical plan premium changes and bargaining unit agreements/Management Resolution provisions. Please refer to your Benefits Worksheet and/or bargaining unit agreement to determine SimiFlex and deduction amounts for your health plans. 2019 insurance deductions and SimiFlex changes will begin on the December 14, 2018 paycheck (benefits are paid one month in advance). Simi Flex Dollars and insurance deductions are paid on the first and second paychecks of each month (no SimiFlex Dollars/insurance deductions are paid in the 3rd paychecks during the year). 2019 deductions for Aflac optional benefits and the medical/dependent care reimbursement program will begin on the January 11, 2019 paycheck. Deductions are paid on the first and second paychecks of each month (no deductions are paid in the 3rd paychecks during the year). Benefit Confirmation information will be provided to employees during Open Enrollment. Employees without an email address will receive a hardcopy. This information outlines each employee’s personal benefit information currently on file, including a list of all dependents enrolled on their various health insurance plans. The Benefit Confirmation is provided each year to assist employees in making Open Enrollment coverage decisions.

5
Please take a moment to review your Benefit Confirmation for accuracy. Should you find a discrepancy, please contact Human Resources.
WHAT DO YOU NEED TO DO?
If you have no benefit changes, sign the front page of your Benefits Worksheet indicating you have no changes, and return it to Human Resources by Friday, October 5, 2018; or,
If you would like to make changes to your benefits, indicate the changes on your Benefits Worksheet and return it (along with any required enrollment/change forms and applicable supporting documentation) to Human Resources by Friday, October 5, 2018. Contact Human Resources for assistance in determining required forms and documentation.
If you are currently enrolled in the ASIFlex medical or dependent care flexible spending account (FSA) reimbursement program, please remember your enrollment does not automatically continue for next year. You must re-enroll every year. Online enrollment instructions are available in the W: Stop/HR Resources folder, or contact Human Resources to request instructions.
Be sure to carefully review your pay stubs on December 14, 2018, and January 11, 2019, to ensure deductions for health premiums were taken appropriately.
QUESTIONS?
We highly recommend attending one of our Open Enrollment meetings listed on Page 4 of this booklet to discuss your questions with a plan representative. In addition, the following Human Resources staff are available to help you:
Extension Tamara Cusano [email protected] 6740 Jill Kramer [email protected] 6742 Jamie Cross [email protected] 6337

6
LIFE EVENTS THAT MAY AFFECT HEALTH PLAN COVERAGE
Certain events in your life, such as marriage, divorce, or a death in the family, can affect your health and insurance coverage with the City. These events can also affect who you name as your designated beneficiary(ies). Employees are responsible for ensuring that their (and their family member’s) health enrollment and beneficiary information is accurate, and for reporting any changes in a timely manner. As such, please notify Human Resources of life events affecting benefits in a timely manner so that the necessary forms may be completed. Please refer to the information below for instructions regarding common life events and related forms/timelines.
Life Event Required Documents Required Forms Timeline Change in Address N/A Employee Information Form ASAP
Marriage Copy of Certified Marriage Certificate
Employee Information Form Health Insurance Change Forms Life Insurance Beneficiary Change Form
Within 30 Days of Event
Registration of Domestic Partner
State of California Certificate of Domestic Partnership
Employee Information Form Health Insurance Change Forms Life Insurance Beneficiary Change Form
Within 30 Days of Event
Divorce or Termination of Domestic Partnership
Divorce Decree or Termination of Domestic Partnership
Employee Information Form Health Insurance Change Forms Life Insurance Beneficiary Change Form
Within 30 Days of Event
Name Change Court Document Ordering Name Change
Employee Information Form Health Insurance Change Forms Life Insurance Beneficiary Change Form
Within 30 Days of Event
Birth or Adoption of Child Copy of Birth Certificate or Adoption Certificate
Health Insurance Change Forms Life Insurance Beneficiary Change Form
Within 30 Days of Event
Dependent Reaches 26th Birthday/No Longer Eligible for Insurance
N/A Health Insurance Change Forms Within 30 Days of Event
Loss of Other Insurance Coverage
Notice from prior insurance provider or employer verifying loss of coverage
Health Insurance Enrollment Forms
Within 30 Days of Event
Please also remember to update your beneficiaries with CalPERS Retirement, Aflac, and deferred compensation (401k and 457) providers, if applicable. You may change your beneficiaries at any time.

7
MEDICAL INSURANCE
The City participates in the CalPERS Health Benefits Program, under the Public Employees’ Medical and Hospital Care Act (PEMHCA). CalPERS Health offers a variety of HMO and PPO plans to choose from. Employees may access detailed medical plan information on the CalPERS website at www.calpers.ca.gov, or on the City’s Stop W: Drive in the HR Resources folder. Employees may also request a hardcopy of plan information from Human Resources. In addition, the Summary of Benefits and Coverage for all CalPERS Health plans may be obtained from the respective plan’s website (included on the following page). Enrolling in Two CalPERS Health Plans is NOT ALLOWED – Dual CalPERS coverage occurs when you are enrolled in a CalPERS health plan as both a member and a dependent, or as a dependent on two enrollments. Per PEMHCA, this duplication of coverage is against the law. When dual CalPERS coverage is discovered, the enrollment that caused the dual coverage will be retroactively canceled. Employees may be responsible for all costs incurred from the date the dual coverage began. However, employees may enroll in both a CalPERS health plan and a health plan provided through another non-CalPERS Health employer. Split Enrollment of Dependents is NOT ALLOWED – When two active or retired members are married to each other or in a domestic partnership, each member can enroll separately. However, when these individuals enroll in a CalPERS Health plan in their own right, PEMHCA requires that one parent must carry all dependents on one health plan. Parents cannot split enrollment of dependents. CalPERS will retroactively cancel split enrollments. Employees may be responsible for all costs incurred from the date the split enrollment began. Plan Comparison Information – Please refer to the current CalPERS Health Summary of Benefit and Coverage at www.calpers.ca.gov to review a summary of the coverage available under each of the plans offered by CalPERS. For more detailed plan information, please refer to the plan’s Evidence of Coverage document by visiting the respective plan provider’s website (included at the end of this section). Please note that the following CalPERS Health plans are available in Ventura and Los Angeles Counties: HMOs: Anthem Traditional, Anthem Select, Blue Shield Access+, Health Net Salud y Mas (not available in Ventura County), Health Net SmartCare (limited availability), Unitedhealthcare, Kaiser Permanente PPOs: PERS Choice, Basic PERS Care, PERS Select, PORAC (POA employees only) Limited Network Plans – The Anthem Select HMO and PERS Select PPO plans offer a reduced monthly premium in exchange for a more limited doctor and hospital network. If you are considering one of these plans, please carefully research doctor and hospital availability before enrolling.

8
Need help choosing a medical plan? – CalPERS Health offers many medical plan choices. Not sure which plan is the best for you? Log in to https://my.calpers.ca.gov to use the Find a Medical Plan tool to research the health plan and benefits most important to your family. CalPERS Compare - CalPERS Compare online service is available for employees currently enrolled in the Basic PERS Care, PERS Choice, and PERS Select PPO plans. This online tool is available at no additional cost and helps you:
Compare quality information and prices in order to make informed decisions.
Shop for convenient, quality health care services’ prescriptions; and doctors in your network.
Track all of your medical spending.
View estimated costs of future services. Visit www.calperscompare.com get started. HMO or PPO? Which Plan is Right for Me? Under HMO plans, most services and medicines are covered with a small, pre-determined copayment. You select a Primary Care Physician (PCP) to coordinate your care. You may not seek care from physicians/specialists that are outside of your designated medical group. Under PPO plans, participants have a choice of going directly to a physician/specialist without a referral. There is an annual deductible to meet before benefits apply. Employees are also responsible for paying 10-20% of the charges, after the deductible is satisfied (see the respective plan’s website for copay, coinsurance, and deductible information).
Why Would I Choose a PPO Plan? Why Would I Choose an HMO Plan?
You want the flexibility to see specialists and other providers without having to first get a referral.
You want the freedom to see providers who are not in the HMO network.
You are confident that you can manage your own care.
You have the ability to pay higher coinsurance amounts that are not pre-determined.
You don’t want the extra responsibility of managing your own care.
You do not want to pay the higher costs of a PPO.
Your doctor accepts HMO plans, and you don’t mind getting referrals to see specialists within the HMO network.
You do not want to get bills from providers, and prefer to pay pre-established copays rather than percentage-based coinsurance.
Insurance premiums for medical, dental, and vision are pre-tax. Any payroll deduction you have for insurance premiums is deducted from your income before taxes are applied, which decreases the amount of taxes you pay and increases your take home pay. If you do not want your premiums deducted pre-tax, contact Human Resources.

9
MEDICAL PLAN CONTACT INFORMATION & WEBSITES
To assist you in selecting a plan that meets your needs, employees are encouraged to visit the websites below to search for their respective doctors, hospitals, medical groups, and prescription information before choosing a CalPERS health plan. Changes are not permitted until the following open enrollment period. ANTHEM BLUE CROSS (PPO) PERSCare, PERS Choice, and PERS Select plans (855) 839-4524 www.anthem.com/ca/calpers ANTHEM BLUE CROSS (HMO) Anthem Traditional and Anthem Select plans (855) 839-4524 www.anthem.com/ca/calpershmo BLUE SHIELD OF CALIFORNIA (HMO) Blue Shield Access+ plan (800) 334-5847 www.blueshieldca.com/calpers KAISER PERMANENTE (HMO) (800) 464-4000 www.kp.org/calpers POLICE OFFICERS RESEARCH ASSOCIATION OF CALIFORNIA – PORAC (PPO) PPO plan available to POA employees only (800) 288-6928 http://ibtofporac.org/ HEALTH NET OF CALIFORNIA (HMO)* (888) 926-4921 Health Net Salud y Mas and Health Net SmartCare plans www.healthnet.com/calpers UNITEDHEALTHCARE (HMO) (877) 359-3714 http://www.uhc.com/calpers *Health Net provides limited to no coverage in Ventura County. Please carefully research plans before selecting.

10
OPTUMRX PHARMACY – Pharmacy Administrator for Anthem, Unitedhealthcare, and Health Net plans (Blue Shield and Kaiser pharmacy benefits are available on their respective websites). (855) 505-8106 www.optumrx.com/calpers CalPERS Website - Medical plan information and updates. www.calpers.ca.gov LiveHealth Online – Only for PERS Care, PERS Choice, and PERS Select PPO plans and Anthem Traditional and Anthem Select HMO plans Consult with a doctor face-to-face online regarding health issues without leaving home. Obtain prescriptions for routine issues without visiting a doctor’s office. Ideal for ear infections, colds, flu, rashes, eye infections, and other routine health issues. www.livehealthonline.com

11
DENTAL INSURANCE
The City provides group dental benefits through Delta Dental for employees and their spouse, domestic partner, and eligible dependents up to their 26th birthday (regardless of student or marital status). Benefits vary, depending on the employee’s bargaining unit/employee group. General Unit, Non-Sworn Management, and Police Management may choose either a Delta PPO plan or a Delta HMO plan. Police Officers’ Association employees may enroll in a Delta PPO plan. Dental PPO (Preferred Provider Organization) plans offer a network feature and usually offer a balance between lower costs and dentist choice. PPO dentists participate in the network thereby agreeing to accept contracted fees as payment in full rather than their usual fee for patients with the PPO. When you visit a PPO dentist, you typically pay a certain percentage of the reduced rate (called coinsurance) and the plan pays the rest. The percentage usually varies by the type of coverage such as diagnostic and preventive, major services, etc. For example, preventive services are covered at 100%, while crowns and bridges may be covered closer to 50%. PPOs usually require you to meet a deductible and have an annual maximum amount of coverage. While you typically have the lowest out-of-pocket costs if you visit a PPO dentist, the plan allows you to visit the dentist of your choice, even if she is not in the network. Dental Health Maintenance Organization (DHMO) plans, also referred to as pre-paid plans, require you to choose one dentist or dental facility to coordinate all of your oral health needs. If you need to see a specialist, your primary care dentist will refer you; specialty care may require preauthorization. A typical DHMO-type plan doesn't have any deductibles or maximums. Instead, when you receive a dental service, you pay a fixed dollar amount for the treatment (a "copayment"). Often, diagnostic and preventive services have no copayment, so you pay nothing for these services. However, generally if you visit a dentist outside of the network, you may be responsible for the entire bill. These plans can be a very affordable option for individuals and families. Please refer to the dental comparison sheet on the following page for a summary of benefit for the various dental options available. The summary is intended as an overview only and each policy should be consulted for detailed coverage information, limitations, and exclusions. Policies and detailed plan information are available on the Stop W: Drive/HR Resources folder. Employees may search for dentists by visiting the Delta Dental website at www.deltadentalins.com. To help you in your search, the network names for the available plans is listed on the following page.

12
DENTAL INSURANCE COMPARISON
EE GROUP PROVIDER DEDUCTIBLE COVERAGE ANNUAL LIMIT CLAIMS
Gene
ral U
nit
Non
-Sw
orn
Man
agem
ent
Polic
e M
ana
ge
rs’ A
ssocia
tion
Delta Care USA
HMO type of plan.
Select a dentist from the DeltaCare USA Network.
$0 Preventive Care: No charge.
Basic Treatment: Co-payment set by published schedule.
Major Treatment: Co-payment set by published schedule.
Orthodontia:
Co-payment set by published schedule
for adults and children.
None. No claim forms needed.
Gene
ral U
nit
Delta Dental Premier
PPO type of plan. Select any dentist.
If you would like to
choose an in-network dentist, select a Delta Dental Premier Dentist
$100 per person, $300 per family
Waived for preventive care.
Preventive Care: 100% of Delta rate.
Basic Treatment: 80% of Delta rate.
Major Treatment: 50% of Delta rate; Pre-determination
suggested.
Orthodontia: 50% of services for dependent children to a lifetime max of $1,000 per patient.
$2,000 per calendar year.
None required for participating
dentists.
Member completes form and dentist submits if non-participating
dentist.
Non
-Sw
orn
Man
agem
ent
Polic
e M
ana
ge
rs’ A
ssocia
tion
Polic
e O
ffic
ers
’ A
ssocia
tion
Delta Dental Preferred
PPO type of plan. Select any dentist.
If you would like to
choose an in-network dentist, select a Delta Dental PPO Dentist
$25 per person, $75 per family
Waived for
preventive care.
Preventive Care: 100% of Delta rate.
Basic Treatment: 90% for PPO participating
dentists; 80% for Premier and non-
participating dentists.
Major Treatment: 50% of Delta rate; Pre-determination
suggested.
Orthodontia: 50% of services for dependent children.
$2,500 per calendar year.
$750 orthodontia.
None required for participating
dentists.
Member completes form and dentist submits if non-participating
dentist.

13
VISION INSURANCE
The City provides group vision benefits through Vision Service Plan (VSP) for employees and their spouse, domestic partner, and eligible dependents up to their 26th birthday (regardless of student or marital status). See the summary of benefits (below) for more information. Policies and detailed plan information are available on the Stop W: Drive/HR Resources folder. Employees may search for VSP providers by visiting their website at www.vsp.com.
ALL EMPLOYEE GROUPS
The information listed above is intended as an overview only and the policy should be consulted for detailed coverage information, limitations and exclusions.
COPAY
PROVIDER
COVERAGE
CLAIMS
Participating Doctor Non-Participating Doctor
$0 Copay Vision Service Plan (VSP)
Listing of participating doctors available at:
www.vsp.com
Examinations: One exam every 12 months
(100%).
Spectacle Lenses: One standard pair of lenses every 12 months, if required
(100%).
Frames: One standard frame every 24
months up to $150 allowance.
Contact Lenses:
Every 12 months up to $130 for elective contact lenses in lieu of spectacle lenses and frame. Visually necessary lenses (100%). Up to $60 member copay for contact lens fitting & evaluation. Discounted laser surgery through VSP approved
centers.
Examinations: One exam every 12 months
up to $50.
Spectacle Lenses: $50-$125 allowance
depending upon type of lenses.
Frames:
Up to $70.
Contact Lenses: Every 12 months up to $105 for elective contact lenses in lieu of spectacle lenses and frame. Visually necessary
lenses up to $210.
No claim forms needed.

14
BASIC LIFE INSURANCE & AD&D
Basic Life Insurance pays your beneficiary a lump sum if you die. Accidental Death and Dismember (AD&D) provides another layer of benefits to either you or your beneficiary if you suffer from loss of a limb, speech, sight, or hearing, or if you die in an accident. Premiums are paid by the City for full-time employees and are pro-rated for part-time employees. Please refer to your bargaining unit agreement or the Management Resolution to determine your benefit coverage amount. Coverage is provided by The Standard. Beneficiary Reminder: Make sure that you have named a beneficiary for your life insurance benefit. Please contact Human Resources at any time to update your beneficiary. Taxes: Due to IRS regulations, a life insurance benefit of $50,000 or more is considered a taxable benefit. You will see the value of the benefit included in your taxable income on your paycheck and W-2.
NEW VOLUNTARY ADDITIONAL LIFE AND AD&D PLAN
While you have a Basic Life insurance benefit, you may choose to enroll in Additional Life insurance for you and your dependents, subject to providing evidence of insurability. The City has a new Voluntary Life plan which will take the place of the previous Voluntary Life plan with many enhancements. The New coverage amounts available to employees will be in increments of $10,000 up to the lesser of $750,000 or (5) five times annual earnings. For Spouses in increments of $5,000 up to $500,000. The New guarantee issue amounts (no evidence of insurability requirements) for employees will be the lessor of $300,000 or three (3) times annual earnings and for spouses $50,000. In addition, for most age categories, the monthly rates are lower. There will also be new Voluntary AD&D plan that will match the amount of your Voluntary Life coverage. If you would like to purchase the Voluntary Life and AD&D insurance or obtain additional information, please go to the Stop W: Drive/HR Resources folder. To be eligible for Additional Life Insurance: You must be insured for Basic Life You must be one of the following: An active Full-time employee of the City of Simi
Valley, regularly working at least 30 hours each week; regularly working at least 20 hours each week; or an active City Council Member of the City of Simi Valley.
The plan excludes temporary or seasonal employees, full-time member of the armed forces, leased employees and independent contractors.
For Spouse/Domestic Partner coverage, your Spouse/Domestic Partner must not be a full-time member of the armed forces of any country.
15
OPTIONAL BENEFITS
Optional insurances, such as hospital, accident, cancer, and other insurances may be purchased through Aflac on a pre-tax or post-tax basis under the City’s Section 125 Plan. To purchase Aflac products, please call Jeff Boykins, Aflac Representative at (818) 468-6216 or e-mail [email protected] to schedule an appointment... All Aflac changes/enrollments must be submitted during the Open Enrollment Period or within 30 days of hire. Requests after this date will not be processed. Once Open Enrollment ends, the Aflac Representative will not be available until January for individual appointments.
EMPLOYEE ASSISTANCE PROGRAM (EAP)
Managed Health Network (MHN) provides confidential assistance with work, home, personal, and family issues. An MHN intake specialist or counselor provides your initial assessment. Depending on your needs, you may be referred to a network psychologist, social worker, marriage and family counselor, financial advisor, lawyer, childcare or eldercare provider, or other trusted professional. MHN abides by state and federal mandates governing confidentiality, and your identity is protected by law. Services are available to you and your family household members 24 hours a day, 7 days a week, 365 days a year. One toll-free call to (800) 977-7593 can provide you with information and assistance on a wide range of topics/issues including, but not limited to:
Marriage, family, and relationship issues
Stress and anxiety
Personal and work-related problems
Depression
Grief and loss
Anger management
Daily living services
Domestic violence
Legal and financial issues
Addiction and recovery
Parenting and child care
Elder care services
Identity theft recovery
Up to eight (8) face-to-face or telephone sessions are available free of charge per incident, per calendar year, per member. Web Video Consultations are unlimited.

16
FLEXIBLE SPENDING ACOUNT (FSA)
The City offers you the opportunity to participate in a Healthcare and/or Dependent Care Flexible Spending Account (FSA). Employees can set aside a fixed amount of money from each paycheck for anticipated covered expenses. The money is deducted from your check prior to taxes (federal, state, and Medicare) being withheld, so you are paying for dependent care and/or medical expenses AND lowering your taxable income! These programs are administered by ASIFlex. You may participate in one or both plans. Healthcare FSA Account This plan allows you to pay for eligible out-of-pocket healthcare expenses with pre-tax dollars. Eligible expenses include medical, dental, or vision costs such as plan deductibles, copays, coinsurance amounts, and other non-covered healthcare costs for you and your tax dependents. For 2019, you can set aside up to $2,600 for the year. Dependent Care FSA Account This plan allows you to pay for eligible out-of-pocket dependent care expenses with pre-tax dollars. Eligible expenses may include daycare centers, in-home child care, and before or after school care for your dependent children under age 13. Other individuals may qualify if they are considered your tax dependent and are incapable of self-care. It is important to note that you can access money only after it is placed into your dependent care FSA account. All caregivers must have a tax ID or Social Security number. This information must be included on your federal tax return. If you use the dependent care reimbursement account, the IRS will not allow you to claim a dependent care credit for reimbursed expenses. Consult your tax advisor to determine whether you should enroll in this plan. For 2019, you can set aside up to $5,000 per household ($2,500 if you are married, filing separate tax returns) for eligible dependent care expenses. Important Considerations:
You must use all of your FSA funds by March 31, 2020 or else you will lose them. The FSA plans have an added feature (Grace Period) that allows you to continue to incur new claims up until 3/15/2020, with any remaining funds from your 2019 elected amount. So, you should be careful when calculating the amount you wish to contribute. Use the Reimbursement Account Worksheets on the next few pages to carefully predict your qualifying expenses for the year.
Elections cannot be changed during the plan year, unless you have a qualified change in family status.
FSA funds can be used for you, your spouse, and your tax dependents only.
Once you have incurred a covered expense, simply submit receipts to ASIFlex for reimbursement from the money that you set aside. To obtain a reimbursement, simply submit a claim online at www.asiflex.com or via the ASIFlex mobile app. Claims will be paid via direct deposit or a check sent to the employee’s home, within approximately three business days after claim filing.

17
Account Requirements
As you consider establishing a Section 125 Health Care Reimbursement Account, keep in mind that all of the following guidelines must be met:
1. Eligible Expenses must be incurred for services rendered during the Plan Year, January 1 through December 31, or during the Grace Period (January 1 through March 15 of the following year);
2. Services must have been "incurred" prior to reimbursement;
3. Expenses must be for diagnosis, treatment or prevention of disease, or for treatment affecting any part or function of the body;
4. Expenses cannot be reimbursed from any other source or used as a deduction on personal income taxes. You have until March 31 after the Plan Year to submit expenses for reimbursement from your account. Unused account balances will be forfeited. Consult IRS Publication 502 for additional information. Coverage of registered domestic partners and/or their children may be subject to federal tax for this benefit.
Worksheet
The following worksheet will help you estimate your health care expenses for the upcoming Plan Year. Many health care expenses are covered by your insurance, while you pay only deductibles and co-payments. Other insurance benefits, such as orthodontia, are subject to a cap on the maximum insurance coverage. Your payment of these deductibles, co-payments, and amounts above the maximum benefit are expenses which are eligible for reimbursement up to a maximum of $2,650 per year. Refer to the next page for an extensive list of eligible/ineligible expenses.
Estimated Annual Expenses
Last Year's Expenses Projected Expenses 1. Health Care Expenses (not covered by insurance)
Insurance Deductibles $_______________ $______________
Medical co-payments +_______________ +______________
Dental co-payments +_______________ +______________
Immunizations, injections, and vaccinations +_______________ +______________
Routine exams and physicals (above the maximum) +_______________ +______________
Orthodontic expenses (above the maximum) +_______________ +______________
Eyeglasses and contact lenses (above the maximum) +_______________ +______________
Hearing Aids (above the maximum) +_______________ +______________
Prescription co-payments + ______________ +______________
Other Expenses +_______________ +______________ 2. Sub-Total (Uninsured expenses for the Plan Year) $_______________ $______________ 3. Divide by 24 pay periods. 24 24 4. This is the amount that will be deducted from your paycheck. $_______________ $______________ This is a worksheet only. If you would like to enroll in the Section 125 Health Care Reimbursement Program, on-line instructions can be found at W:\HR Resources\Benefits & Health Insurance.
CITY OF SIMI VALLEY
HEALTH CARE REIMBURSEMENT ACCOUNT WORKSHEET
18
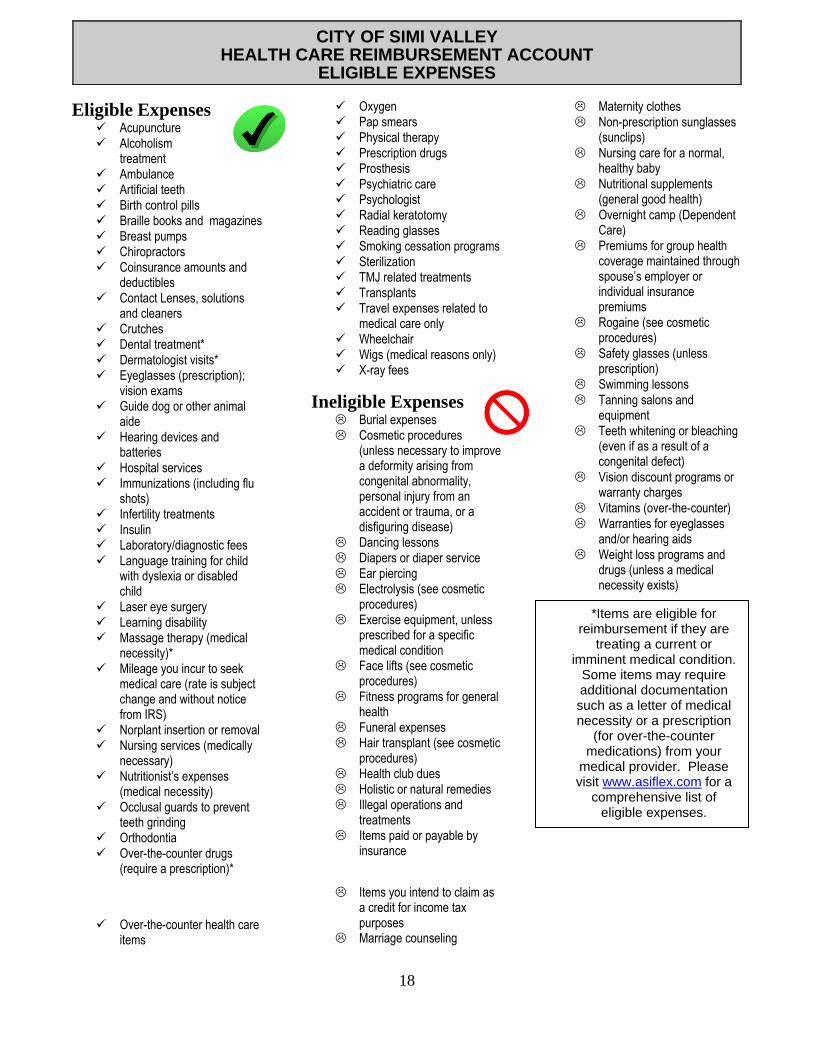
Eligible Expenses Acupuncture Alcoholism
treatment Ambulance Artificial teeth Birth control pills Braille books and magazines Breast pumps Chiropractors Coinsurance amounts and
deductibles Contact Lenses, solutions
and cleaners Crutches Dental treatment* Dermatologist visits* Eyeglasses (prescription);
vision exams Guide dog or other animal
aide Hearing devices and
batteries Hospital services Immunizations (including flu
shots) Infertility treatments Insulin Laboratory/diagnostic fees Language training for child
with dyslexia or disabled child
Laser eye surgery Learning disability Massage therapy (medical
necessity)* Mileage you incur to seek
medical care (rate is subject change and without notice from IRS)
Norplant insertion or removal Nursing services (medically
necessary) Nutritionist’s expenses
(medical necessity) Occlusal guards to prevent
teeth grinding Orthodontia Over-the-counter drugs
(require a prescription)*
Over-the-counter health care items
Oxygen Pap smears Physical therapy Prescription drugs Prosthesis Psychiatric care Psychologist Radial keratotomy Reading glasses Smoking cessation programs Sterilization TMJ related treatments Transplants Travel expenses related to
medical care only Wheelchair Wigs (medical reasons only) X-ray fees
Ineligible Expenses Burial expenses Cosmetic procedures
(unless necessary to improve a deformity arising from congenital abnormality, personal injury from an accident or trauma, or a disfiguring disease)
Dancing lessons Diapers or diaper service Ear piercing Electrolysis (see cosmetic
procedures) Exercise equipment, unless
prescribed for a specific medical condition
Face lifts (see cosmetic procedures)
Fitness programs for general health
Funeral expenses Hair transplant (see cosmetic
procedures) Health club dues Holistic or natural remedies Illegal operations and
treatments Items paid or payable by
insurance
Items you intend to claim as a credit for income tax purposes
Marriage counseling
Maternity clothes
Non-prescription sunglasses (sunclips)
Nursing care for a normal, healthy baby
Nutritional supplements (general good health)
Overnight camp (Dependent Care)
Premiums for group health coverage maintained through spouse’s employer or individual insurance premiums
Rogaine (see cosmetic procedures)
Safety glasses (unless prescription)
Swimming lessons
Tanning salons and equipment
Teeth whitening or bleaching (even if as a result of a congenital defect)
Vision discount programs or warranty charges
Vitamins (over-the-counter)
Warranties for eyeglasses and/or hearing aids
Weight loss programs and drugs (unless a medical necessity exists)
CITY OF SIMI VALLEY
HEALTH CARE REIMBURSEMENT ACCOUNT ELIGIBLE EXPENSES
*Items are eligible for reimbursement if they are
treating a current or imminent medical condition.
Some items may require additional documentation such as a letter of medical necessity or a prescription
(for over-the-counter medications) from your
medical provider. Please visit www.asiflex.com for a
comprehensive list of eligible expenses.

19
Account Requirements
As you consider establishing a Dependent Care Reimbursement Account, keep in mind that all of the following guidelines must be met: 1. The expenses to be reimbursed must be for services rendered during the Plan Year, January 1 through December 31, or during
the Grace Period (January 1 through March 15 of the following year);
2. The dependent care cost must be incurred to enable both you and your spouse or registered domestic partner to be employed;
3. If service is provided by a facility outside your home which cares for more than six children, that facility must be a qualified day care center meeting all state and local regulations;
4. Eligible services include the care of dependents under age 13, or the care of a dependent, spouse, or registered domestic partner who is physically or mentally incapable of caring for himself or herself;
5. You must reside with the qualifying person(s);
6. For Dependent Care expenses outside your household, the eligible dependent must spend at least eight hours a day in your home. Charges for overnight stays are not eligible;
7. The service must be provided by someone whom you do not claim as a dependent, and if the service was provided by your child, he or she must have been age 19 or greater by the end of the year;
8. Your total reimbursements for the Plan Year may not exceed the lowest of the following:
a. $5,000 ($2,500 if you are married, filing separate tax returns) b. Your taxable compensation (after your salary reduction under the plan) c. If you are married, your spouse's or registered domestic partner’s actual or deemed earned income;
9. Expenses related to overnight camps/activities and program registration fees are not considered to be eligible for reimbursement under the plan; and,
10. You must include the taxpayer identification number for each dependent care service provider on your federal tax return.
You have until March 31 after the Plan Year to submit expenses for reimbursement from your account. Unused account balances will be forfeited. Consult IRS Publication 503 for more information. Coverage of registered domestic partners and/or their children may be subject to federal tax for this benefit.
Worksheet
The following worksheet is designed to help you estimate your dependent care expenses for the upcoming Plan Year.
1. Multiply your weekly day care expenses by the number of weeks you expect to pay for each type of care during the Plan Year.
Babysitter $ Day Care Center + Pre-School + Before and After School Care + Custodial Care + Other Dependent Care +
2. Sub-total (Up to $5,000 or $2,500 if you are married, filing separate tax returns). $
3. Divide by 24 pay periods. 24
4. This is the amount that will be deducted from your paycheck. $
This is a worksheet only. If you would like to enroll in the Section 125 Health Care Reimbursement Program, on-line instructions can be found at W:\HR Resources\Benefits & Health Insurance.
CITY OF SIMI VALLEY
DEPENDENT CARE REIMBURSEMENT ACCOUNT WORKSHEET

20
DEFERRED COMPENSATION PLANS – 401(K) & 457
PLEASE NOTE: The 2019 deferral limits have not yet been released by the Internal Revenue Service (IRS). A separate memorandum will be distributed to all employees if deferral limits are adjusted from the limits listed below.
The City’s Deferred Compensation Plans are a great way to save for your retirement. Plan availability varies by bargaining/employee group as follows:
457 All groups
401(k) Management, Executive Management, Police Managers’ Association, Police Officers’ Association, Eligible City Council Members
401(k) Roth Management, Executive Management, Police Managers’ Association, Police Officers’ Association, Eligible City Council Members
The Federal Economic Growth and Tax Reconciliation Act of 2001 (EGTRRA), sets tax deferrals and limits on deferred compensation plans. There are three deferral options to consider: they are the “base limit” provision, the “age 50 and over” provision, and the “457 catch-up” provision.
“Base Limit” Provision - The “base limit” is reviewed by the Internal Revenue Service (IRS) in October each year to determine if a cost of living increase is justified. The “base limit” for the 401(k) and 457 plans for 2018 is $18,500. The “base limit” provision is subject to an annual cost of living adjustment, and may change from year to year.
“Age 50 and Over” Provision - In addition to the base limit of $18,500, 457 and 401(k) participants age 50 and over may contribute an additional $6,000 during the 2018 calendar year for a total of $24,000 in each plan. The “age 50 and over” provision is subject to an annual cost of living adjustment, and may change from year to year. The “457 Catch-Up” Provision – Allows 457 plan participants during the three years prior to retirement age (age 50 +) to defer twice the base deferral limit (current max is $37,000). Participants may not participate in the “age 50 and over” and “457 catch-up” provisions at the same time. Employees who are interested in the “457 catch-up” provision need to meet with the 457 representative to ensure eligibility. Please note that you may not do the “457 catch-up” provision the year that you actually retire. How to Enroll or Change Deferral - Employees may enroll or change their deferred compensation deferrals at any time. Enrollment and change forms are available on the Stop W: Drive/HR Resources, or may be requested from Human Resources.
Changes to the 457 deferral amount must be received by Human Resources by the end of the month prior to the effective date of the change.

21
401(k) change requests will be processed the pay period following receipt of the change by Human Resources.
Employees who want to enroll in or change their deferred compensation for the first paycheck in January must submit forms to Human Resources by:
December 27, 2018 for the 457 plan
If you are not contributing the maximum, you may increase your deductions at any time.
Please note, deferrals are deducted over 26 pay periods; therefore, employees contributing the maximum base limit of $18,500 in either the 457 or the 401(k) plan will indicate a bi-weekly deferral of $711.53. Employees who also utilize the “age 50 and over” provision (max of $24,500), the bi-weekly deferral is $942.30.
EMPLOYEE BENEFIT NOTICES
State and federal laws regulate and protect various aspects of employee benefit coverage. To ensure that employees have the necessary information to make informed benefit selection decisions, and in compliance with regulations, the City provides its employees with the notices listed below on an annual basis. Whenever there is new law establishing new regulations or benefits, or if there are changes to any existing regulations or benefits, updated information is provided to all employees. The following notices are provided: • Medicare Part D Notice of Creditable Coverage (for employees over 65 or with spouses over
65) • Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) • Womens’ Health and Cancer Rights Act • Newborns and Mothers’ Health Protection Act • Medical Privacy Practices • Domestic Partner Information • New Health Insurance Marketplace Coverage Options and Your Health Coverage

22
FEDERALLY REQUIRED IMPORTANT NOTICE ABOUT YOUR PRESCRIPTION DRUG COVERAGE AND MEDICARE
(For employees and their spouses over 65 years of age)
September 10, 2018 Please read this notice carefully and keep it with your other important insurance documents. This notice has information about your current prescription drug coverage with the City of Simi Valley and prescription drug coverage available for employees/spouses with Medicare. It also explains the options you have under Medicare prescription drug coverage and can help you decide whether or not you want to enroll. At the end of this notice there is information about where you can get help to make decisions about your prescription drug coverage. Medicare prescription drug coverage became available in 2006 to everyone with Medicare through Medicare prescription drug plans and Medicare Advantage Plans that offer prescription drug coverage. All Medicare prescription drug plans provide at least a standard level of coverage set by Medicare. Some plans may also offer more coverage for a higher monthly premium. The City of Simi Valley has determined that the prescription drug coverage offered by the City’s plans are, on average for all plan participants, expected to pay out as much as the standard Medicare prescription drug coverage will pay and is considered Credible Coverage. Because your existing coverage is, on average, at least as good as standard Medicare prescription drug coverage, you can keep your City coverage and not pay extra if you later decide to enroll in Medicare prescription drug coverage. Individuals can enroll in a Medicare prescription drug plan when they first become eligible for Medicare and each year from October 15th through December 7th. If you wait to join later, you may pay a higher premium (a penalty). If it is determined that you have to pay a penalty, you will have to pay that penalty as long as you have Medicare prescription drug coverage. However, if you lose credible prescription drug coverage, through no fault of your own, you will be eligible to join a Part D plan for a sixty (60) day Special Enrollment Period (SEP) without paying a penalty (as long as you do not go 63 or more days without credible coverage). In addition, if you or your beneficiary lose coverage or decide to drop the City’s coverage, you will be eligible to join a Part D plan at that time using an Employer Group Special Enrollment Period without paying a penalty (as long as you do not go 63 or more days without credible coverage). However, should you decide to enroll in a Medicare prescription drug plan and drop your City of Simi Valley prescription drug coverage, be aware that you and your dependents may not be able to get this coverage back. Please note that if you drop or lose your coverage with the City and don’t enroll in Medicare prescription drug coverage within 63 continuous days after your current coverage ends, you may pay a penalty to enroll in Medicare prescription drug coverage later. There is a one percent per month penalty for every month that you do not have prescription drug coverage that is at least as good as Medicare’s prescription drug coverage. For example, if you are without coverage for nineteen months, your premium will always be at least 19% higher than what others may pay. You will have to pay this higher premium as long as you have Medicare prescription drug coverage. In addition, you may have to wait until the following October to enroll. It is recommended that you compare your current coverage, including which drugs are covered, with the coverage and cost of the plans offering Medicare prescription drug coverage in your area. As part of the City’s prescription drug benefit program, your prescription coverage includes coverage for
23
generic and brand name prescriptions. There is also the option for mail order prescriptions. Please see your benefit summary for more information. For more information about your options under Medicare prescription drug coverage, detailed information is in the “Medicare & You” handbook. You will get a copy of the handbook in the mail every year from Medicare. You may also be contacted directly by Medicare prescription drug plans. For more information about Medicare prescription drug plans:
Visit www.medicare.gov
Call your State Health Insurance Assistance Program (see your copy of the Medicare & You handbook for their telephone number) for personalized help
Call 1-800-MEDICARE (1-800-633-4227). TTY users should call 1-877-486-2048. If you have limited income and resources, extra help paying for Medicare prescription drug coverage is available from the Social Security Administration (SSA) online at www.socialsecurity.gov, or you may call them at 1-800-772-1213 (TTY 1-800-325-0778). For more information about this notice or your current prescription drug coverage, contact Jill Kramer in Human Resources at 805-583-6742. NOTE: You will receive this notice annually before the next enrollment period for Medicare prescription drug coverage or if coverage through the City changes. You also may request a copy of this notice at any time.
Remember: KEEP THIS NOTICE. If you enroll in one of the plans approved by Medicare drug plans (not a City sponsored plan) you may be required to provide a copy of this notice when you enroll to show that you are not required to pay a higher premium amount.

24
CONSOLIDATED OMNIBUS BUDGET RECONCILIATION ACT OF 1985 (COBRA) The City of Simi Valley allows continued medical, dental, and vision benefits for you and your covered dependents, under certain circumstances because of a federal law -- the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA). It is important that you are aware of this plan provision, since you will be required to take specific actions to exercise your rights to continued coverage. Please review the following information carefully and save it for future reference. There may be other coverage options for you and your family through the Health Insurance Marketplace. In the Marketplace, you could be eligible for a new kind of tax credit that lowers your monthly premiums right away, and you can see what your premium, deductibles, and out-of-pocket costs will be before you make a decision to enroll. Being eligible for COBRA does not limit your eligibility for coverage for a tax credit through the Marketplace. Additionally, you may qualify for a special enrollment opportunity for another group health plan for which you are eligible (such as a spouse’s plan), even if the plan generally does not accept late enrollees, if you request enrollment within 30 days. What is continuation coverage? Federal law requires that most group health plans (including this Plan) give employees and their families the opportunity to continue their health care coverage when there is a “qualifying event” that would result in a loss of coverage under an employer’s plan. Depending on the type of qualifying event, “qualified beneficiaries” can include the employee (or retired employee) covered under the group health plan, the covered employee’s spouse, and the dependent children of the covered employee. Continuation coverage is the same coverage that the Plan gives to other participants or beneficiaries under the Plan who are not receiving continuation coverage. Each qualified beneficiary who elects continuation coverage will have the same rights under the Plan as other participants or beneficiaries covered under the Plan, including open enrollment and special enrollment rights. How long will continuation coverage last? In the case of a loss of coverage due to end of employment or reduction in hours of employment, coverage generally may be continued for up to a total of 18 months. In the case of losses of coverage due to an employee’s death, divorce or legal separation, the employee’s becoming entitled to Medicare benefits or a dependent child ceasing to be a dependent under the terms of the plan, coverage may be continued for up to a total of 36 months. When the qualifying event is the end of employment or reduction of the employee's hours of employment, and the employee became entitled to Medicare benefits less than 18 months before the qualifying event, COBRA continuation coverage for qualified beneficiaries other than the employee lasts until 36 months after the date of Medicare entitlement. This notice shows the maximum period of continuation coverage available to the qualified beneficiaries. Continuation coverage will be terminated before the end of the maximum period if:
any required premium is not paid in full on time,
a qualified beneficiary becomes covered, after electing continuation coverage, under another group health plan that does not impose any pre-existing condition exclusion for a pre-existing condition of the qualified beneficiary (note: there are limitations on plans’ imposing a preexisting condition exclusion and such exclusions will become prohibited beginning in 2014 under the Affordable Care Act),
25
a qualified beneficiary becomes entitled to Medicare benefits (under Part A, Part B, or both) after electing continuation coverage, or
the employer ceases to provide any group health plan for its employees.
Continuation coverage may also be terminated for any reason the Plan would terminate coverage of a participant or beneficiary not receiving continuation coverage (such as fraud). How can you extend the length of COBRA continuation coverage?
COBRA continuation coverage is a temporary continuation of coverage that generally lasts for 18 months due to employment termination or reduction of hours of work. Certain qualifying events, or a second qualifying event during the initial period of coverage, may permit a beneficiary to receive a maximum of 36 months of coverage. You must notify Human Resources of a disability or a second qualifying event in order to extend the period of continuation coverage. Failure to provide notice of a disability or second qualifying event may affect the right to extend the period of continuation coverage. There are also ways in which this 18-month period of COBRA continuation coverage can be extended: Disability An 11-month extension of coverage may be available if any of the qualified beneficiaries is determined by the Social Security Administration (SSA) to be disabled. The disability has to have started at some time before the 60th day of COBRA continuation coverage and must last at least until the end of the 18-month period of continuation coverage. Each qualified beneficiary who has elected continuation coverage will be entitled to the 11-month disability extension if one of them qualifies. If the qualified beneficiary is determined by SSA to no longer be disabled, you must notify the Plan of that fact within 30 days after SSA’s determination. Second Qualifying Event An 18-month extension of coverage will be available to spouses and dependent children who elect continuation coverage if a second qualifying event occurs during the first 18 months of continuation coverage. The maximum amount of continuation coverage available when a second qualifying event occurs is 36 months. Such second qualifying events may include the death of a covered employee, divorce or separation from the covered employee, the covered employee’s becoming entitled to Medicare benefits (under Part A, Part B, or both), or a dependent child’s ceasing to be eligible for coverage as a dependent under the Plan. These events can be a second qualifying event only if they would have caused the qualified beneficiary to lose coverage under the Plan if the first qualifying event had not occurred. You must notify the Plan within 60 days after a second qualifying event occurs if you want to extend your continuation coverage. How can you elect COBRA continuation coverage? To elect continuation coverage, you must complete the Election Form and furnish it according to the directions on the form. Each qualified beneficiary has a separate right to elect continuation coverage. For example, the employee’s spouse may elect continuation coverage even if the employee does not. Continuation coverage may be elected for only one, several, or for all dependent children who are qualified beneficiaries. A parent may elect to continue coverage on behalf of any dependent children. The employee or the employee's spouse can elect continuation coverage on behalf of all of the qualified beneficiaries.

26
In considering whether to elect continuation coverage, you should take into account that you have special enrollment rights under federal law. You have the right to request special enrollment in another group health plan for which you are otherwise eligible (such as a plan sponsored by your spouse’s employer) within 30 days after your group health coverage ends because of the qualifying event listed above. You will also have the same special enrollment right at the end of continuation coverage if you get continuation coverage for the maximum time available to you. How much does COBRA continuation coverage cost? Generally, each qualified beneficiary may be required to pay the entire cost of continuation coverage. The amount a qualified beneficiary may be required to pay may not exceed 102 percent (or, in the case of an extension of continuation coverage due to a disability, 150 percent) of the cost to the group health plan (including both employer and employee contributions) for coverage of a similarly situated plan participant or beneficiary who is not receiving continuation coverage. When and how must payment for COBRA continuation coverage be made? First payment for continuation coverage If you elect continuation coverage, you do not have to send any payment with the Election Form. However, you must make your first payment for continuation coverage not later than 45 days after the date of your election. (This is the date the Election Notice is post-marked, if mailed.) If you do not make your first payment for continuation coverage in full not later than 45 days after the date of your election, you will lose all continuation coverage rights under the Plan. You are responsible for making sure that the amount of your first payment is correct. You may contact Human Resources to confirm the correct amount of your first payment. Periodic payments for continuation coverage After you make your first payment for continuation coverage, you will be required to make periodic payments for each subsequent coverage period. The periodic payments can be made on a monthly basis. Under the Plan, each of these periodic payments for continuation coverage is due on the 1st of the month for that coverage period. If you make a periodic payment on or before the first day of the coverage period to which it applies, your coverage under the Plan will continue for that coverage period without any break. The Plan will send periodic notices of payments due for these coverage periods. Grace periods for periodic payments Although periodic payments are due on the 1st of each month, you will be given a grace period of 30 days after the first day of the coverage period to make each periodic payment. Your continuation coverage will be provided for each coverage period as long as payment for that coverage period is made before the end of the grace period for that payment. However, if you pay a periodic payment later than the first day of the coverage period to which it applies, but before the end of the grace period for the coverage period, your coverage under the Plan will be suspended as of the first day of the coverage period and then retroactively reinstated (going back to the first day of the coverage period) when the periodic payment is received. This means that any claim you submit for benefits while your coverage is suspended may be denied and may have to be resubmitted once your coverage is reinstated.
27
If you fail to make a periodic payment before the end of the grace period for that coverage period, you will lose all rights to continuation coverage under the Plan. Your first payment and all periodic payments for continuation coverage should be sent to: City of Simi Valley, Human Resources 2929 Tapo Canyon Road Simi Valley, CA 93063 For more information This notice does not fully describe continuation coverage or other rights under the Plan. More information about continuation coverage and your rights under the Plan is available in your summary plan description or from the Plan Administrator. If you have any questions concerning the information in this notice, your rights to coverage, or if you want a copy of your summary plan description, you should contact Jill Kramer, Senior Human Resources Analyst, at (805) 583-6742. For more information about your rights under ERISA, including COBRA, the Health Insurance Portability and Accountability Act (HIPAA), and other laws affecting group health plans, visit the U.S. Department of Labor’s Employee Benefits Security Administration (EBSA) website at www.dol.gov/ebsa or call their toll-free number at 1-866-444-3272. For more information about health insurance options available through a Health Insurance Marketplace, visit www.healthcare.gov. Keep Your Plan Informed of Address Changes In order to protect your and your family’s rights, you should keep the Plan Administrator informed of any changes in your address and the addresses of family members. You should also keep a copy, for your records, of any notices you send to the Plan Administrator. Paperwork Reduction Act Statement According to the Paperwork Reduction Act of 1995 (Pub. L. 104-13) (PRA), no persons are required to respond to a collection of information unless such collection displays a valid Office of Management and Budget (OMB) control number. The Department notes that a Federal agency cannot conduct or sponsor a collection of information unless it is approved by OMB under the PRA, and displays a currently valid OMB control number, and the public is not required to respond to a collection of information unless it displays a currently valid OMB control number. See 44 U.S.C. 3507. Also, notwithstanding any other provisions of law, no person shall be subject to penalty for failing to comply with a collection of information if the collection of information does not display a currently valid OMB control number. See 44 U.S.C. 3512. The public reporting burden for this collection of information is estimated to average approximately four minutes per respondent. Interested parties are encouraged to send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, to the U.S. Department of Labor, Office of the Chief Information Officer, Attention: Departmental Clearance Officer, 200 Constitution Avenue, N.W., Room N-1301, Washington, DC 20210 or email [email protected] and reference the OMB Control Number 1210-0123.

28
WOMEN’S HEALTH AND CANCER RIGHTS ACT On October 21, 1998, the Women’s Health and Cancer Rights Act became effective. This law requires group health plans that provide coverage for mastectomies to also cover reconstructive surgery and prostheses following mastectomies. The Act requires that the City inform you of the law’s provisions annually. The law mandates that a member receiving benefits for a medically necessary mastectomy will also receive coverage for:
reconstruction of the breast on which the mastectomy has been performed
surgery and reconstruction of the other breast to produce a symmetrical appearance
prostheses
treatment of physical complications of all stages of mastectomy, including lymphedemas This coverage will be provided in consultation with the attending physician and the patient, and will be subject to the same annual deductible and coinsurance provisions that apply for the mastectomy.
NEWBORNS’AND MOTHERS’ HEALTH PROTECTION ACT
The Newborns’ and Mothers’ Health Protection Act of 1996 (the Newborns’ Act) was signed into law on September 26, 1996, and requires plans that offer maternity hospital benefits for mothers and newborns to pay for a least a 48-hour hospital stay for the mother and newborn following childbirth (or in the case of a cesarean section, a 96-hour hospital stay) unless the attending provider, in consultation with the mother, decides to discharge earlier. This law became effective for group health plans for plan years beginning on or after January 1, 1998. In any case, plans and issuers may not, under Federal law, require that a provider obtain authorization from the plan or the insurance issuer for prescribing a length of stay not in excess of 48 hours (or 96 hours).
29
NOTICE OF PRIVACY PRACTICES
THIS NOTICE OF PRIVACY PRACTICES DESCRIBES HOW MEDICAL INFORMATION ABOUT YOU MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION. PLEASE REVIEW IT CAREFULLY. This Notice of Privacy Practices (the "Notice") describes the legal obligations of health carriers listed below and your legal rights regarding your protected health information held by the Plan under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the Health Information Technology for Economic and Clinical Health Act (HITECH Act). Among other things, this Notice describes how your protected health information may be used or disclosed to carry out treatment, payment, or health care operations, or for any other purposes that are permitted or required by law. We are required to provide this Notice of Privacy Practices to you pursuant to HIPAA. The HIPAA Privacy Rule protects only certain medical information known as "protected health information." Generally, protected health information is health information, including demographic information, collected from you or created or received by a health care provider, a health care clearinghouse, a health plan, or your employer on behalf of a group health plan, from which it is possible to individually identify you and that relates to:
(1) your past, present, or future physical or mental health or condition; (2) the provision of health care to you; or (3) the past, present, or future payment for the provision of health care to you.
If you have any questions about this Notice or about our privacy practices, please contact Jill Kramer, Senior Human Resources Analyst, at (805) 583-6742. This notice applies to the privacy practices of the group health plans and health insurers or health care providers listed below:
CARRIER TYPE OF COVERAGE
CalPERS Health Plans MEDICAL
DELTA DENTAL DENTAL
VSP VISION
MHN EMPLOYEE ASSISTANCE PROGRAM
ASIFlex SECTION 125 PLAN/HEALTH CARE REIMBURSEMENT
Our Responsibilities We are required by law to:
• maintain the privacy of your protected health information; • provide you with certain rights with respect to your protected health information; • provide you with a copy of this Notice of our legal duties and privacy practices with respect to
your protected health information; and • follow the terms of the Notice that is currently in effect.

30
We reserve the right to change the terms of this Notice and to make new provisions regarding your protected health information that we maintain, as allowed or required by law. If we make any material change to this Notice, we will provide you with a copy of our revised Notice of Privacy Practices by mail, electronically, or by another method permitted under the law. How We May Use and Disclose Your Protected Health Information Under the law, we may use or disclose your protected health information under certain circumstances without your permission. The following categories describe the different ways that we may use and disclose your protected health information. For each category of uses or disclosures we will explain what we mean and present some examples. Not every use or disclosure in a category will be listed. However, all of the ways we are permitted to use and disclose information will fall within one of the categories. For Treatment. We may use or disclose your protected health information to facilitate medical treatment or services by providers. We may disclose medical information about you to providers, including doctors, nurses, technicians, medical students, or other hospital personnel who are involved in taking care of you. For example, we might disclose information about your prior prescriptions to a pharmacist to determine if prior prescriptions contraindicate a pending prescription. For Payment. We may use or disclose your protected health information to determine your eligibility for Plan benefits, to facilitate payment for the treatment and services you receive from health care providers, to determine benefit responsibility under the Plan, or to coordinate Plan coverage. For example, we may tell your health care provider about your medical history to determine whether a particular treatment is experimental, investigational, or medically necessary, or to determine whether the Plan will cover the treatment. We may also share your protected health information with a utilization review or precertification service provider. Likewise, we may share your protected health information with another entity to assist with the adjudication or subrogation of health claims or to another health plan to coordinate benefit payments. For Health Care Operations. We may use and disclose your protected health information for other Plan operations. These uses and disclosures are necessary to run the Plan. For example, we may use medical information in connection with conducting quality assessment and improvement activities; underwriting, premium rating, and other activities relating to Plan coverage; submitting claims for stop-loss (or excess-loss) coverage; conducting or arranging for medical review, legal services, audit services, and fraud and abuse detection programs; business planning and development such as cost management; and business management and general Plan administrative activities. However, we will not use your genetic information for underwriting purposes. Treatment Alternatives or Health-Related Benefits and Services. We may use and disclose your protected health information to send you information about treatment alternatives or other health-related benefits and services that might be of interest to you. To Business Associates. We may contract with individuals or entities known as Business Associates to perform various functions on our behalf or to provide certain types of services. In order to perform these functions or to provide these services, Business Associates will receive, create, maintain, transmit, use, and/or disclose your protected health information, but only after they agree in writing with us to implement appropriate safeguards regarding your protected health information. For example, we may disclose your protected health information to a Business Associate to process your claims for Plan benefits or to provide support services, such as utilization management, pharmacy benefit

31
management, or subrogation, but only after the Business Associate enters into a Business Associate contract with us. As Required by Law. We will disclose your protected health information when required to do so by federal, state, or local law. For example, we may disclose your protected health information when required by national security laws or public health disclosure laws. To Avert a Serious Threat to Health or Safety. We may use and disclose your protected health information when necessary to prevent a serious threat to your health and safety, or the health and safety of the public or another person. Any disclosure, however, would only be to someone able to help prevent the threat. For example, we may disclose your protected health information in a proceeding regarding the licensure of a physician. To Plan Sponsors. For the purpose of administering the plan, we may disclose to certain employees of the Employer protected health information. However, those employees will only use or disclose that information as necessary to perform plan administration functions or as otherwise required by HIPAA, unless you have authorized further disclosures. Your protected health information cannot be used for employment purposes without your specific authorization. Special Situations. In addition to the above, the following categories describe other possible ways that we may use and disclose your protected health information without your specific authorization. For each category of uses or disclosures, we will explain what we mean and present some examples. Not every use or disclosure in a category will be listed. However, all of the ways we are permitted to use and disclose information will fall within one of the categories. Organ and Tissue Donation. If you are an organ donor, we may release your protected health information after your death to organizations that handle organ procurement or organ, eye, or tissue transplantation or to an organ donation bank, as necessary to facilitate organ or tissue donation and transplantation. Military. If you are a member of the armed forces, we may release your protected health information as required by military command authorities. We may also release protected health information about foreign military personnel to the appropriate foreign military authority. Workers' Compensation. We may release your protected health information for workers' compensation or similar programs, but only as authorized by, and to the extent necessary to comply with, laws relating to workers' compensation and similar programs that provide benefits for work-related injuries or illness. Public Health Risks. We may disclose your protected health information for public health activities. These activities generally include the following:
• to prevent or control disease, injury, or disability; • to report births and deaths; • to report child abuse or neglect; • to report reactions to medications or problems with products; • to notify people of recalls of products they may be using; • to notify a person who may have been exposed to a disease or may be at risk for contracting or
spreading a disease or condition;

32
• to notify the appropriate government authority if we believe that a patient has been the victim of abuse, neglect, or domestic violence. We will only make this disclosure if you agree, or when required or authorized by law.
Health Oversight Activities. We may disclose your protected health information to a health oversight agency for activities authorized by law. These oversight activities include, for example, audits, investigations, inspections, and licensure. These activities are necessary for the government to monitor the health care system, government programs, and compliance with civil rights laws. Lawsuits and Disputes. If you are involved in a lawsuit or a dispute, we may disclose your protected health information in response to a court or administrative order. We may also disclose your protected health information in response to a subpoena, discovery request, or other lawful process by someone involved in a legal dispute, but only if efforts have been made to tell you about the request or to obtain a court or administrative order protecting the information requested. Law Enforcement. We may disclose your protected health information if asked to do so by a law-enforcement official;
• in response to a court order, subpoena, warrant, summons, or similar process; • to identify or locate a suspect, fugitive, material witness, or missing person; • about the victim of a crime if, under certain limited circumstances, we are unable to obtain the
victim's agreement; • about a death that we believe may be the result of criminal conduct; and • about criminal conduct.
Coroners, Medical Examiners, and Funeral Directors. We may release protected health information to a coroner or medical examiner. This may be necessary, for example, to identify a deceased person or determine the cause of death. We may also release medical information about patients to funeral directors, as necessary to carry out their duties. National Security and Intelligence Activities. We may release your protected health information to authorized federal officials for intelligence, counterintelligence, and other national security activities authorized by law. Inmates. If you are an inmate of a correctional institution or are in the custody of a law-enforcement official, we may disclose your protected health information to the correctional institution or law-enforcement official if necessary (1) for the institution to provide you with health care; (2) to protect your health and safety or the health and safety of others; or (3) for the safety and security of the correctional institution. Research. We may disclose your protected health information to researchers when:
• the individual identifiers have been removed; or • when an institutional review board or privacy board has reviewed the research proposal and
established protocols to ensure the privacy of the requested information, and approves the research.
Required Disclosures The following is a description of disclosures of your protected health information we are required to make.

33
Government Audits. We are required to disclose your protected health information to the Secretary of the United States Department of Health and Human Services when the Secretary is investigating or determining our compliance with the HIPAA privacy rule. Disclosures to You. When you request, we are required to disclose to you the portion of your protected health information that contains medical records, billing records, and any other records used to make decisions regarding your health care benefits. We are also required, when requested, to provide you with an accounting of most disclosures of your protected health information if the disclosure was for reasons other than for payment, treatment, or health care operations, and if the protected health information was not disclosed pursuant to your individual authorization. Other Disclosures Personal Representatives. We will disclose your protected health information to individuals authorized by you, or to an individual designated as your personal representative, attorney-in-fact, etc., so long as you provide us with a written notice/authorization and any supporting documents (i.e., power of attorney). Note: Under the HIPAA privacy rule, we do not have to disclose information to a personal representative if we have a reasonable belief that:
• you have been, or may be, subjected to domestic violence, abuse, or neglect by such person; or • treating such person as your personal representative could endanger you; and • in the exercise of professional judgment, it is not in your best interest to treat the person as your
personal representative.
Spouses and Other Family Members. With only limited exceptions, we will send all mail to the employee. This includes mail relating to the employee's spouse and other family members who are covered under the Plan, and includes mail with information on the use of Plan benefits by the employee's spouse and other family members and information on the denial of any Plan benefits to the employee's spouse and other family members. If a person covered under the Plan has requested Restrictions or Confidential Communications (see below under "Your Rights"), and if we have agreed to the request, we will send mail as provided by the request for Restrictions or Confidential Communications. Authorizations. Other uses or disclosures of your protected health information not described above will only be made with your written authorization. For example, in general and subject to specific conditions, we will not use or disclose your psychiatric notes; we will not use or disclose your protected health information for marketing; and we will not sell your protected health information, unless you give us a written authorization. You may revoke written authorizations at any time, so long as the revocation is in writing. Once we receive your written revocation, it will only be effective for future uses and disclosures. It will not be effective for any information that may have been used or disclosed in reliance upon the written authorization and prior to receiving your written revocation. Your Rights You have the following rights with respect to your protected health information: Right to Inspect and Copy. You have the right to inspect and copy certain protected health information that may be used to make decisions about your Plan benefits. If the information you request is maintained electronically, and you request an electronic copy, we will provide a copy in the electronic form and format you request, if the information can be readily produced in that form and format; if the information cannot be readily produced in that form and format, we will work with you to come to an agreement on form and format. If we cannot agree on an electronic form and format, we will provide you with a paper copy.
34
To inspect and copy your protected health information, you must submit your request in writing to Jill Kramer, Senior Human Resources Analyst. If you request a copy of the information, we may charge a reasonable fee for the costs of copying, mailing, or other supplies associated with your request. We may deny your request to inspect and copy in certain very limited circumstances. If you are denied access to your medical information, you may request that the denial be reviewed by submitting a written request to Jill Kramer, Senior Human Resources Analyst. Right to Amend. If you feel that the protected health information we have about you is incorrect or incomplete, you may ask us to amend the information. You have the right to request an amendment for as long as the information is kept by or for the Plan. To request an amendment, your request must be made in writing and submitted to Jill Kramer, Senior Human Resources Analyst, at Extension 6742. In addition, you must provide a reason that supports your request. We may deny your request for an amendment if it is not in writing or does not include a reason to support the request. In addition, we may deny your request if you ask us to amend information that:
• is not part of the medical information kept by or for the Plan; • was not created by us, unless the person or entity that created the information is no longer
available to make the amendment; • is not part of the information that you would be permitted to inspect and copy; or • is already accurate and complete.
If we deny your request, you have the right to file a statement of disagreement with us and any future disclosures of the disputed information will include your statement. Right to an Accounting of Disclosures. You have the right to request an "accounting" of certain disclosures of your protected health information. The accounting will not include (1) disclosures for purposes of treatment, payment, or health care operations; (2) disclosures made to you; (3) disclosures made pursuant to your authorization; (4) disclosures made to friends or family in your presence or because of an emergency; (5) disclosures for national security purposes; and (6) disclosures incidental to otherwise permissible disclosures. To request this list or accounting of disclosures, you must submit your request in writing to Jill Kramer, Senior Human Resources Analyst. Your request must state the time period you want the accounting to cover, which may not be longer than six years before the date of the request. Your request should indicate in what form you want the list (for example, paper or electronic). The first list you request within a 12-month period will be provided free of charge. For additional lists, we may charge you for the costs of providing the list. We will notify you of the cost involved and you may choose to withdraw or modify your request at that time before any costs are incurred. Right to Request Restrictions. You have the right to request a restriction or limitation on your protected health information that we use or disclose for treatment, payment, or health care operations. You also have the right to request a limit on your protected health information that we disclose to someone who is involved in your care or the payment for your care, such as a family member or friend. For example, you could ask that we not use or disclose information about a surgery that you had.

35
Except as provided in the next paragraph, we are not required to agree to your request. However, if we do agree to the request, we will honor the restriction until you revoke it or we notify you. We will comply with any restriction request if (1) except as otherwise required by law, the disclosure is to a health plan for purposes of carrying out payment or health care operations (and is not for purposes of carrying out treatment); and (2) the protected health information pertains solely to a health care item or service for which the health care provider involved has been paid in full by you or another person. To request restrictions, you must make your request in writing to Jill Kramer, Senior Human Resources Analyst, at Extension 6742. In your request, you must tell us (1) what information you want to limit; (2) whether you want to limit our use, disclosure, or both; and (3) to whom you want the limits to apply-for example, disclosures to your spouse. Right to Request Confidential Communications. You have the right to request that we communicate with you about medical matters in a certain way or at a certain location. For example, you can ask that we only contact you at work or by mail. To request confidential communications, you must make your request in writing to Jill Kramer, Senior Human Resources Analyst, at Extension 6742. We will not ask you the reason for your request. Your request must specify how or where you wish to be contacted. We will accommodate all reasonable requests. Right to Be Notified of a Breach. You have the right to be notified in the event that we (or a Business Associate) discover a breach of unsecured protected health information. Right to a Paper Copy of This Notice. You have the right to a paper copy of this notice. You may ask us to give you a copy of this notice at any time. Even if you have agreed to receive this notice electronically, you are still entitled to a paper copy of this notice. To obtain a paper copy of this notice, contact Jill Kramer, Senior Human Resources Analyst, at Ext 6742.
Complaints
If you believe that your privacy rights have been violated, you may file a complaint with the Plan or with the Office for Civil Rights of the United States Department of Health and Human Services. To file a complaint with the Plan, contact Jill Kramer, Senior Human Resources Analyst, at Extension 6742. All complaints must be submitted in writing.
Carrier/TPA REQUEST FOR ACCOUNTING
RECORD OF DISCLOSURES
FILING A COMPLAINT
QUESTIONS
CalPERS Health Plans
1-888-CalPERS
Delta Dental 1-888-335-8227
VSP 1-800-877-7195
MHN 1-800-977-7593
ASIFlex 1-800-659-3035
You will not be penalized, or in any other way retaliated against, for filing a complaint with the Office for Civil Rights or with the City.

36
DOMESTIC PARTNER INFORMATION
In order for a domestic partner to be eligible for health (medical, dental, and vision) and life insurance benefits, the employee must provide a copy of the Certification of Domestic Partnership to Human Resources in accordance with standard enrollment deadlines and requirements. To terminate a domestic partnership, the employee must provide Human Resources with a copy of the Termination of Domestic Partnership paperwork in a timely manner. Note: The City withholds taxes based on the value of this benefit unless the employee claims the domestic partner as a dependent on his or her income taxes (or in the case of State taxes, if they are registered with the State as domestic partners). Requirements for a Domestic Partnership - Sections 297 and 297.5 of the California Family Code outline the requirements for a domestic partnership. A domestic partnership shall be established in California when both persons file a Declaration of Domestic Partnership with the Secretary of State. In addition, at the time of filing, all of the following requirements must be met: 1. Both persons are at least 18 years of age, except as provided in California Family Code Section
297.1;
2. Both persons are capable of consenting to the domestic partnership;
3. Neither person is married to someone else or is a member of another domestic partnership with someone else that has not been terminated, dissolved, or adjudged a nullity;
4. The two persons are not related by blood in a way that would prevent them from being married
to each other in this State; and, 5. Both persons are members of the same sex or one or both of the persons are over 62 years of
age and meet the eligibility criteria under Title II of the Social Security Act as defined in Section 402 (a) of Title 42 of the United States Code or Title XVI of the Social Security Act as defined in Section 1381 of Title 42 of the United States Code for aged individuals.
Tax Treatment of Health Benefits - The federal government does not recognize domestic partnerships for tax purposes. Employer contributions to health premiums for an employee’s domestic partner and children of a domestic partner are taxable (imputed) income. Employee premium contributions are paid on a post-tax basis. By comparison, if an employee is married to a member of the same (eff. 9/16/13) or opposite sex, no taxable imputed income results from employer contributions to the spouse’s health premium costs and employee premium contributions for the spouse are paid pre-tax. IRS Exemption for Enrolled Health Plan Dependents Who Meet Certain Requirements The Internal Revenue Service (IRS) offers a tax break for health-related expenses incurred by a “qualifying relative.” Under IRS code section 152, a domestic partner (of either gender), and children of a domestic partner qualify for favorable tax treatment if the: 1. Domestic partner or the domestic partner’s child receives more than half of his or her financial
support from the employee;

37
2. Domestic partner or the domestic partner’s child lived with the employee as a member of his or her household for the entire calendar year (January I-December 31), with the exception of temporary absences due to vacation, education, or military service; and,
3. Domestic partner or the domestic partner’s child is a citizen of the United States, or a resident of
the United States, Canada, or Mexico. If an enrolled dependent meets all of these requirements, the employee may submit an annual declaration to the City, and there will be no imputed income for the employer contribution to dependent health premiums, and employee premium contributions will be paid pretax. To take advantage of this favorable tax treatment, you must file a declaration annually with Human Resources by the required deadlines. Consult with Your Tax Advisor - This is an overview regarding the tax treatment of health benefits for domestic partners and their children. Please consult with a professional tax advisor before taking any action. If you have any questions or need further information, please contact Jill Kramer at Extension 6742.

38
NEW HEALTH INSURANCE MARKETPLACE COVERAGE OPTIONS AND YOUR HEALTH COVERAGE
PART A: General Information When key parts of the health care law take effect in 2014, there will be a new way to buy health insurance: the Health Insurance Marketplace. To assist you as you evaluate options for you and your family, this notice provides some basic information about the new Marketplace. What is the Health Insurance Marketplace? The Marketplace is designed to help you find health insurance that meets your needs and fits your budget. The Marketplace offers "one-stop shopping" to find and compare private health insurance options. You may also be eligible for a new kind of tax credit that lowers your monthly premium right away. Open enrollment for health insurance coverage through the Marketplace begins in October 2013 for coverage starting as early as January 1, 2014. Can I Save Money on my Health Insurance Premiums in the Marketplace? You may qualify to save money and lower your monthly premium, but only if your employer does not offer coverage, or offers coverage that doesn't meet certain standards. The savings on your premium that you're eligible for depends on your household income. Does Employer Health Coverage Affect Eligibility for Premium Savings through the Marketplace? Yes. If you have an offer of health coverage from your employer that meets certain standards, you will not be eligible for a tax credit through the Marketplace and may wish to enroll in your employer's health plan. However, you may be eligible for a tax credit that lowers your monthly premium, or a reduction in certain cost-sharing if your employer does not offer coverage to you at all or does not offer coverage that meets certain standards. If the cost of a plan from your employer that would cover you (and not any other members of your family) is more than 9.5% of your household income for the year, or if the coverage your employer provides does not meet the "minimum value" standard set by the Affordable
Care Act, you may be eligible for a tax credit.1
Note: If you purchase a health plan through the Marketplace instead of accepting health coverage offered by your employer, then you may lose the employer contribution (if any) to the employer-offered coverage. Also, this employer contribution - as well as your employee contribution to employer-offered coverage - is often excluded from income for Federal and State income tax purposes. Your payments for coverage through the Marketplace are made on an aftertax basis. How Can I Get More Information? For more information about your coverage offered by your employer, please check your summary plan description or contact Jill Kramer, Senior Human Resources Analyst, at Extension 6742. The Marketplace can help you evaluate your coverage options, including your eligibility for coverage through the Marketplace and its cost. Please visit www.HealthCare.gov for more information, including an online application for health insurance coverage and contact information for a Health Insurance Marketplace in your area. 1 An employer-sponsored health plan meets the "minimum value standard" if the plan's share of the total allowed benefit costs covered by the plan is no less than 60 percent of such costs.

39
PART B: Information About Health Coverage Offered by Your Employer
This section contains information about any health coverage offered by your employer. If you decide to complete an application for coverage in the Marketplace, you will be asked to provide this information. This information is numbered to correspond to the Marketplace application.
3. Employer name: City of Simi Valley
4. Employer Identification Number (EIN): 95-2626170
5. Employer address: 2929 Tapo Canyon Road
6. Employer phone number: (805) 583-6700
7. City: Simi Valley
8. State: California
9. Zip Code: 93063
10. Who can we contact about employee health coverage at this job? Jill Kramer, Senior Human Resources Analyst
11. (805) 583-6742
Here is some basic information about health coverage offered by this employer: As your employer, we offer a health plan to: Some employees, eligible employees are: Regular Status employees working at least 20 hours per week. With respect to dependents: We do offer coverage, eligible dependents are: Spouse; domestic partner; eligible dependent children up to their 26th birthday; dependents over the age of 26 with a qualifying medical condition. Coverage provided to you meets the minimum value standard, and the cost of coverage to you is intended to be affordable, based on employee wages. Even if your employer intends your coverage to be affordable, you may still be eligible for a premium discount through the Marketplace. The Marketplace will use your household income, along with other factors, to determine whether you may be eligible for a premium discount. If, for example, your wages vary from week to week (perhaps you are an hourly employee or you work on a commission basis), if you are newly employed mid-year, or if you have other income losses, you may still qualify for a premium discount. If you decide to shop for coverage in the Marketplace, HealthCare.gov will guide you through the process. Enter the information above when you visit HealthCare.gov to find out if you can get a tax credit to lower your monthly premiums.
OMB No. 1210-0149 (expires 5-31-2020)


















