OpenNotes: Breaking barriers, changing culture, engaging patients Patient Experience Conference 2018 Liz Salmi OpenNotes Amy Cohen, PhD, BCBA, PMP The University of Vermont Medical Center Steve O’Neill, LICSW, BCD, JD OpenNotes and Beth Israel Deaconess Medical Center #OpenNotes
What is OpenNotes?• National movement dedicated to making
healthcare more open and transparent
• Initiative to give patients access to their medical providers’ notes via secure patient portals
• Not a vendor product or software
OpenNotes is supported by a combined grant from the following organizations:
Clinical notesü Document medical historyü Interpret patient needs and communicationü Outline next stepsü Serve as a reminder for future visitsü Act as “bread crumbs” for other healthcare
providers
#OpenNotes
What the patient seesWhat the doctor writesaka notes
The Note vs. the After Visit Summary
vs.
Salmi, L. Medical record. (6 Feb. 2017)#OpenNotes
Original study: 2010• Research and demonstration project• 105 PCPs and 20,000 patients in Boston
(BIDMC), rural Pennsylvania (Geisinger), and Seattle safety net hospital (Harborview)
• Now replicated at VA, Kaiser, Cedars-Sinai, and many other sites
Delbanco, Walker, et al, Annals of Internal Medicine#OpenNotes
Initial study findings3 out of 4 patients reported:• Taking better care of themselves• Understanding health and medical conditions
better• Feeling more in control of their health• Being better prepared for visits• Doing better taking medications as
prescribed
Delbanco, Walker, et al, Annals of Internal Medicine#OpenNotes
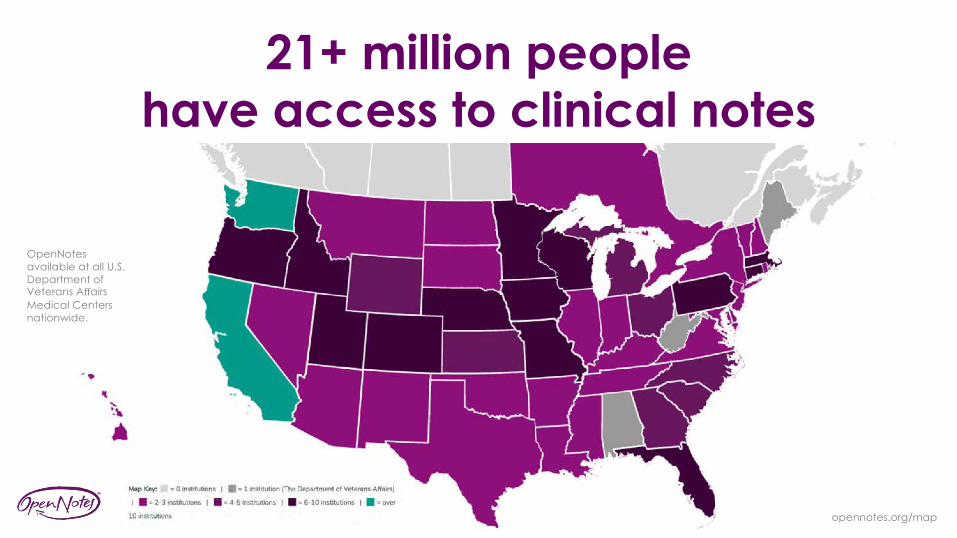
OpenNotes available at all U.S. Department of Veterans Affairs Medical Centers nationwide.
21+ million people have access to clinical notes
opennotes.org/map
21 MILLION = less than 6% of U.S. population
#OpenNotes
Rights under HIPAA• See a copy of your medical record• Get a copy of your medical record• Change incorrect information• Find out who has seen your health
information
#OpenNotes
My notes
Salmi, L. Medical record. (2010)
Printed record = $725.40
Digital record = $45 for 3 DVDs
Salmi, L. Office visit. Kaiser Medical Secretaries. (23 Feb 2017)
Salmi, L. Medical record. (16 Dec 2017)
Of the 40,000 Google searches made
every second, 2,000 are health-related
Wilbanks, J.T. & Topol, E.J. Stop the privatization of health data. Nature 535, 345–348 (21 July 2016) doi:10.1038/535345a
#OpenNotes
People who read notes…• Have a better understanding of their
health and medical conditions• Better recall and follow their care plan• Feel more in control of their health
Delbanco et al, Ann Intern Med 2012#OpenNotes
People who read notes…• Take better care of themselves• Do a better job taking medications as
prescribed• Can identify inaccuracies in the record
and play a role in the safety of care
Delbanco et al, Ann Intern Med 2012#OpenNotes
People who read notes…• Feel comfortable sharing notes with
care partners and others involved in their care
• Can communicate more clearly, helping to strengthen the partnership between themselves and their health care team
Delbanco et al, Ann Intern Med 2012#OpenNotes
99% of people are likely to feel the same
or better about their doctor after reading just one note
Bell SK, Gerard M, Fossa A, et al A patient feedback reporting tool for OpenNotes: implications for patient-clinician safety and quality
partnerships. BMJ Qual Saf Published Online First: 13 December 2016. doi: 10.1136/bmjqs-2016-006020
#OpenNotes
Older, non-Caucasian patients, with poorer health, and lower
formal education… more likely to feel better about their doctor
when reading notes
#OpenNotesBell SK, Gerard M, Fossa A, et al A patient feedback reporting tool for OpenNotes: implications for patient-clinician safety and quality
partnerships. BMJ Qual Saf Published Online First: 13 December 2016. doi: 10.1136/bmjqs-2016-006020
Caregivers benefit as much as patients• 88% of patients and 86% of caregivers had better formulated
questions for the doctor
• 86% of patients and 82% of caregivers had more productive discussions about the patient’s care
• 94% of patients and their caregivers said they had a better understanding of patient health conditions, better remembered the patient’s care plan, and felt more in control of care
• 71% of both patient and caregivers reported patients taking medications as prescribed more often
• Collaboration through intentionally engaging patients and families– Recruitment and deployment of patient/family advisors– Patient & Family Advisory Councils– Engaging advisors in key leader hiring processes
Strategic Movement Towards Patient- and Family-Centered Care Guided by Principles
37
• Goal to identify a strategic change that:• addressed patient/family priorities and need for improved transparency• demonstrated we were prepared to “walk the walk”
• OpenNotes established as a year 3 PFCC goal to improve information sharing and increase reciprocal engagement between patients and providers• CMO & CMIO introduction
• Representation from each health care service/department
• Intentional engagement of skeptics
• Inclusion of patients and families
Engaging Stakeholders
42
Patients and Families as Partners in OpenNotes
43
• Patient/Family advisor participation on the PFCC Executive Steering Committee
• Initial introduction and ongoing updates at Patient and Family Advisory Council
• Recruitment, selection and support of advisors for OpenNotes workgroup– Making the right selection– “Do we really need 3?”– Provider vs. patient priorities
• Advisor review of education/communication materials
• Workgroup– Patients and Families– Skeptics
• Purpose– Diverse needs/issues– Buy-in
• Scope• Sequence• Education Plan
– Built-in educators/champions
Tactics
44
Tactics
45
• Adequate resources must be available to providers and staff for education and roll out
• Contingency plan for unexpected volumes of messages
• Education for patients regarding standards of note content and structure
• Avoid incomplete or inadequate (e.g. “dictation completed”) note distribution
Tactics
46
Workgroup Recommendations
• Included all ambulatory care appointments, including the ED
• All providers included- opting out is not an option
• Any note can be excluded at discretion of the provider
• Only exception- behavioral health providers; Opt-in per note
• Adolescents- shared with adolescent, not with proxy
• Ability to disable patient portal access
• Plan for patient questions/requests for changes: provider practice, followed by Patient and Family Advocacy, if needed
presentations by champions focused heavily on data
• Patients and Families:• Clinic flyers/posters• Rack cards• Patient portal email at launch• Notes available alert
• Soft opening- May 31, 2017– Troubleshooting, not evaluating for feasibility
• “Big Bang” – June 14, 2017
Deploy
49
Evaluate
50
Evaluate
51
“It’s a non-event from the provider perspective.”- UVM Medical Group Leadership
“This is a giant step forward. I have recently been a patient at UVM in primary care, specialist, surgery, inpatient, ED, all within the last 2 weeks. The notes were particularly helpful with aftercare instructions and reminded me of follow up expectations. Having these noted will support my recollections of those often introspective moments.”
- Patient Feedback
Six Month Check-in
52
• Sharing inpatient discharge summaries with patients
Opening Our (Therapy and Medical) Notes to Our Patients
Steve O’Neill, LICSW, BCD, JDSocial Work Manager for Psychiatry, Primary Care, ID, Pain, and Opioid Services
Associate Director for Ethics ProgramsBehavioral Health Specialist for OpenNotes
Beth Israel Deaconess Medical Center
Faculty, Center for BioethicsDepartment of Social Medicine
Harvard Medical School
Beryl InstituteApril, 2018
No Conflicts
� …………..to report
� Funding sources: Cambia Health Foundation, Gordon and Betty Moore Foundation, Peterson Center on Healthcare, Robert Wood Johnson Foundation
56
Goals § Share early impressions from several years of national experience with fully open medical records, especially mental health
§ Notes as (narrative) therapy for behavioral health and mental illness
§ OpenNotes as a movement……….. ……….transparency, trust and partnership!
57
Relevant BIDMC History� 1972 Patient Bill of Rights
� 1976 “Orders Not to Resuscitate”: NEJM
� 1986 First Electronic Health Records (Warner Slack, MD and Howard
Bleich, MD)
� 2008 Preventable Harm Initiative
� 2010 OpenNotes starts in Primary Care
� 2013 All Medical/Surgical/Specialty notes opened up
� 2014 Preventable Harm to Respect/Dignity Initiative
� 2014 OpenNotes for Behavioral Health starts
58
Relevant BIDMC History
�Culture of Transparency
�Culture of Respect
59
About the OpenNotes movement§ Began in 2010 with 105 volunteer primary care doctors and
19,000 of their patients in Boston, rural Pennsylvania, and the Seattle inner city in Washington state.
§ The doctors invited the patients to read their notes via electronic portals
§ Now, more than 20 million patients in the USA, thousands of doctors, nurses, therapists, trainees, physician assistants, case managers, and other clinicians are sharing notes
What’s going on?
Funded primarily by the Robert Wood Johnson Foundation60
21+ Million Patients Have Access to Notes
Three Principal Questions
§Would OpenNotes help patients become more engaged in their care?
§Would OpenNotes be the straw that breaks the therapist’s back?
§After 1 year, would patients and therapists want to continue?
62
Always start with……..What is Best for the Patient??!!
63
Staff
� 15 Psychiatrists/Therapists In Psychiatry Department
� 28 Social Work Staff agreed to pilot; 4 declined; pediatric therapists and fellows excluded; staff turn over; or no eligible patients = 24 started
� 440 patients at start; Currently better than 3000 participating in open therapy notes
64
BIDMC Social Work Staff Fears1. Increased Work Burden—”feeling a sense of pressure to get notes entered in a timely manner so that they can be useful to the patient”
2. Misunderstanding: “I’m concerned about patients misunderstanding information in the notes……On the other hand, I am hopeful that the open notes may actually enhance the therapy process and promote greater communication/understanding on both sides.”
65
BIDMC Social Work Staff Fears3. Re-languaging Notes and Processing of Notes-
“….will they be angry about certain content?!”
4. Patients with severe mental illness, especially psychosis and paranoia will flee
5. “It’s one thing to tell them in session we think they are having paranoid thoughts and another for them to read it at home alone”
66
Additional Issues:� Domestic Violence and Safety Exclusions
� Who is ‘note’ intended for? Would OpenNotes adversely effect teaming communications?
� Obsessive patients (“I’ve spent my whole life learning not to double think.”; “When I go to my mechanic, I don’t want to look under the hood. Same here!”)
� Paranoid patients (“I’d be petrified to look. I’m not gonna do it.”)
� Patients “in denial” and ‘premature’ info
67
Social Work Therapist Work Group:� FAQ’s and scripts/info sheets developed
� Anticipating reactions or feedback from patients and colleagues and staff
� Thesaurus approach for altering language
68
Additional Issues
� “Ruining Psychotherapy” (NYTimes, Washington Post, etc public comments after articles)
� Destroying the privacy expectations and the fiduciary relationship whereby patients entrust us with their ‘secrets’, especially if already agreed to under informed consent (ie- monitoring)
� “Helpful only for high functioning, well educated patients”� “Will need to hide our diagnostic impressions”
69
§ Better than 90% of patients agreed that opening up therapy notes is a good idea!
§ Better than 85% of patients want to continue having notes available
§ Few patients said reading notes made them feel§ Judged (Less than 15%)§ Worried (Less than 10%)§ Offended (Less than 5%)
70(Delbanco, Walker, et al, Ann Intern Med, 2012)
Patients were pleased…
� Patients with ‘adverse effects’ tended to clarify these concerns as underlying concerns such as privacy or already existing issues; or misinterpreted questions when asked
� Biggest issue, as in medicine, seems to be whether there is concordance between what the therapist says in session and what they write in the note
71(Delbanco, Walker, et al, Ann Intern Med, 2012)
Patients were pleased…
Note Reading� The vast majority of patients never mentioned to their therapist about
having read their notes
� Note Reading drops off due to redundancy…………………..
72
Privacy vs. Confidentiality
18% shared notes with others (20-42% in medicine), mostly family 73
The NIGHTMARE Patient!!Recurrent staff concerns about the “nightmare patient” reported at BIDMC, as well as other practices…….
74
Is this really an index for ‘contagious’ staff angst???
These are labor intensive patients irrespective of the therapeutic interventions………….!
75
The NIGHTMARE Patient!!
Therapy Patient Examples
1. Self-deprecatory Patient
2. Paranoid/Severely Depressed Patient
3. Delusional Patient
4. The Patient with a Documentation Error
Patients reportedimportant clinical benefits
� Better than 50% felt more in control of their care
� Better than 50% reported feeling better at self-care
� Better than 40% reported better remembering what working on in therapy
� Better than 40% felt more engaged in their therapy
� Better than 50% felt better able to trust their therapist
77
� Better than 80% of patients wanted to continue to be able to see their visit notes online.
� Better than 60% of patients said availability of open notes would affect their future choice of a therapist.
� Not one therapist or patient asked to stop, and almost all have since joined.
� And now…………………………..
78
The Bottom Line
Lessons Learned�70/30 Rule�Stigma, especially in mental health!
Mainstream!!�Professionals Fears: looking foolish or
incompetent
�Active vs. Passive Utilizers!
79
Importance of Notifications
0
10
20
30
40
50
60
70
80
90
100
Jun-10
Jul-10
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Jan-12
Feb-12
Mar-12
Apr-12
May-12
Jun-12
Not
es v
iew
ed w
ithin
30
days
of
avai
labi
lity
(%)
BIDMCGHS
Notifications to view notes stop at
GHS and continue at
BIDMC
Reading rates dropped when GHS stopped sending patients messages to let them know a new note was available
…and the best possible outcomes
Communication
EngagementTrust
81
(Culture of Respect/Transparency)
OurNotes
� Collaborative Electronic Health Record!
� What happens when providers and patients and families collaborate on the record???
83
OurNotes
� 1. Participants anticipated patients and families would greatly benefit from contributing to medical notes.
� 2. The interventions most endorsed were asking patients before visits to write history and goals for visit
� 3. Patients' contributions to records must not increase clinician workload. � 4. OurNotes could impose unaccustomed and unwelcome accountabilities on
some patients. � 5. Participants had many specific ideas about how OurNotes might work � Mafi, Walker, Delbanco, et al. Ann Intern Med. Published online November 14, 2017. doi:10.7326/M17-0583

























































































![CaseReport Habit Breaking Appliance for Multiple Corrections · Habit Breaking Appliance for Multiple Corrections ... removable habit breaking appliances [15, 16]. Hence, habit breaking](https://static.documents.pub/doc/80x56/5f15893424a8522d646af1b7/casereport-habit-breaking-appliance-for-multiple-corrections-habit-breaking-appliance.jpg)






