87
Operative Session : Hair Transplantation Presented By : Dr. Shamendra Anand Sahu Burn, Plastic & Maxillofacial surgery VMMC & SAFDARJUNG HOSPITAL NEW DELHI
| Date post: | 11-Apr-2017 |
| Category: |
Education |
| Upload: | shamendra-sahu |
| View: | 508 times |
| Download: | 2 times |
Operative Session : Hair Transplantation Presented By : Dr. Shamendra Anand Sahu
Burn, Plastic & Maxillofacial surgeryVMMC & SAFDARJUNG HOSPITAL
NEW DELHI

HAIR RESTORATION TECHNIQUES
• There are three broad categories of surgical restoration procedures:
• 1. scalp flaps (advancement flaps, rotation flaps and free flaps)
• 2. surgical excision (alopecia reduction)• 3. free auto grafts of hairy scalp from the well haired to
the bald area.

Hair Transplantation
• Hair transplantation involves relocation or transfer of hairs from the occipital area to the bald area.
• The discussion of transplantation refers to micrografts or minigrafts or, more specifically in current nomenclature, follicular grafts.

Hair Transplantation
• Micrograft : one to two hairs• Minigraft : three to six hair . • Single FU : one to two / three to four hair • Multi FU : two to three unit/two to six hair grafts

The anatomy of the normal hairline
• Critical anatomic landmark in the mature male hairline is the frontal-temporal recession.

landmark is formed by the emergence of two convex lines making up the frontal and the temporal hairlines
Appearance of a patient who had undergone hair transplantation in the frontal area in which the acute frontal-temporal angles were maintained, resulting in a normal-appearing recession
The normal hairline
• Young males usually do not have this recession.• Both women and children tend to have a continuous line
between the frontal and temporal areas without this recession .
• Design of the frontal-temporal recession is critical to a natural result.

The normal hairline

The normal hairline
• 2. Natural hairlines are not straight and regular.
• 3. Other important factors are that the hair follicle sits about 3–3.5 mm below the surface of the scalp and that scalp thickness varies between 5.5 and 6.5 mm
PATTERNS OF BALDNESS
• Most common type of hair loss in both men and women is referred to as androgenic alopecia.
• The mechanism of androgenic alopecia is inherent in each individual hair follicle as it responds to external stimuli, essentially androgens.
• The progressive loss of hair is predetermined by genetic characteristics associated with these responsive scalp follicles.
• The mode of action of androgens on the target cells occurs at the bulbar region of the follicle.

PATTERNS OF BALDNESS• In most men with hair loss, the hair follicles in the frontal
and crown regions of the scalp appear most likely to be affected .
• Hair loss in women is frequently of a diffuse nature.• The pattern of hair loss, because of its diffuseness, often
results in a lack of appropriate donor hair.• However, there is a subgroup of women who demonstrate
hair loss similar to the male pattern.

PATTERNS OF BALDNESS• The family history in these women is also compatible with a male
pattern type of hair loss.
• The history these women give is fairly typical and is one of slow but progressive hair loss, and it is most evident on the superior scalp with good density on both the sides and posteriorly.
• These are appropriate candidates for hair transplantation because the posterior scalp area has adequate donor hair.

Other Important Causes Of Alopecia
• Secondary to numerous factors, such as surgery, metabolic disorders, chemotherapy, stress, and autoimmune disease.
• This type of hair loss is often of an acute nature most.
• Most of these patients are not candidates for transplantation.

Post chemotherapy Alopecia
In the patient who has had hair loss after chemotherapy, if enough time has transpired to allow recovery and there still has been no regrowth, transplantation may be appropriate. However, the take of the grafts has not been ideal in these patients.

Traumatic alopecia 1. Secondary to ischemia of the hair bulbs.2. Secondary to direct tissue loss as in post burn alopecia.
Prolonged pressure on the scalp in a single area –3. Patient who lies in a comatose position for hours at a time.4. Patients undergoing prolonged surgical procedures under general
anesthesia. 5. Aesthetic surgery of the face and scalp area.

Traumatic alopecia
• Significant ischemia, which reduces blood flow to the follicles, can explain the temporary loss of hair in hair transplantation.
• With severe ischemia, death of the bulb can lead to permanent alopecia

Hair cycle






FPHL

Follicular Units
• Follicular units - scalp hairs grow naturally in small compartments containing clusters of one to four follicles surrounded by concentric layers of collagen fibers.
• Peripheral areas such as the hairline have one and two-hair follicular units (FU), whereas the more dense central regions have more three and four-hair FU (and coarser hair shafts).


THE PREOPERATIVE PERIOD
• Patient care coordinator :
• Discontinue medications and diet supplements that can cause bleeding : aspirin, anticoagulants, ibuprofen-type anti-inflammatories, vitamin E, garlic pills, fish oil capsules, and herbal supplements, starting 2 weeks prior to surgery.

THE PREOPERATIVE PERIOD• Twice-daily application of topical Minoxidil 2% to 5% to
the recipient area beginning 1 week prior to surgery.• Patients are instructed to massage their scalp during the
final 4 weeks prior to surgery in order to increase scalp laxity within the donor area, thus enabling a wider strip harvest and a greater FU yield.

THE PREOPERATIVE PERIOD• Written consent for the procedure, anesthesia, and
photography must be obtained from the patient on the morning of the surgery.
Patient Evaluation • It is critical in the early phases of a patient's evaluation to design a hair
pattern that will be appropriate not only as the patient ages but also on the basis of progressive hair loss .
• Patients who demand an inappropriate hairline should be rejected for surgery because they are unrealistic and will be dissatisfied later like :
Example : a young patient in his late teens or early 20s who has significant hair loss to wish to redesign the hairline to a juvenile appearance.• Patient must be counselled that they are going to undergo extensive
further surgery
Planning of the hairline• Single hair grafts are used to create a natural hairline.• To locate the ideal hairline in a bald patient, it is necessary to divide
the face into three equal segments.• In the midline, the hairline starts 7-10 cm from the glabella. • A curve sweeps around to the lateral side of the forehead from the
center. At this point, the sides of the hairline should be oriented parallel to the curve when the subject is looking straight ahead.
• The lateral hairlines are usually 9.5–11.5 cm above the lateral canthus of the eyes.



• The temporal angles : form relatively sharp right angles or acute angles in most men
• but these angles should be more rounded in women.
The micrografts in the hairline should be placed in an irregular saw-toothed• pattern to give a natural appearance.

It is useful to draw a specific pattern on the scalp to demonstrate as the patient is looking in a mirror where the most appropriate hairline pattern should be
Widow's peak."
Throughout the hairline. the transition zone should contain both microirregularities(intermittent density clusters more noticeable under close examination than from a distance) and macroirregularities (protrusion along the path of the hairline that cause it to appear less linear when viewed from a distance).

• Usually 250–300 single hair (micro)grafts will be necessary to create a new hairline in any individual.
• Behind the hairline, two hair FUGs are used to provide new hair.
• Three or four hair FUGs are used just further behind.

• In most patients, the anterior level of the hairline in the midline should be at least 8 to 10 cm above the glabella. In addition, the anterior hairline appears more natural if it runs parallel to the ground when viewed from a lateral view.

• The colour, quality, and density of the donor hair, as well as the contrast between the hair and the skin colours, are important factors that affect the result. The lesser the contrast between the donor hair and the skin, the better is the result.
• It is also noted that frizzy, curly, or wavy hair are advantageous characteristics in transplanted hair

• Hair diameter is the other major factor in determining the coverage achievable with a transplant.
• Hair volume (hv) is defined in the following formula:• hv = π(r)2 (h) (d) (a)• It is key to note that a doubling of the radius results in a
quadrupling of hair volume, making hair diameter the most important single variable in the coverage achievable in a transplant.
• It is also the variable that is most beyond control.

Criteria for rejection of a patient
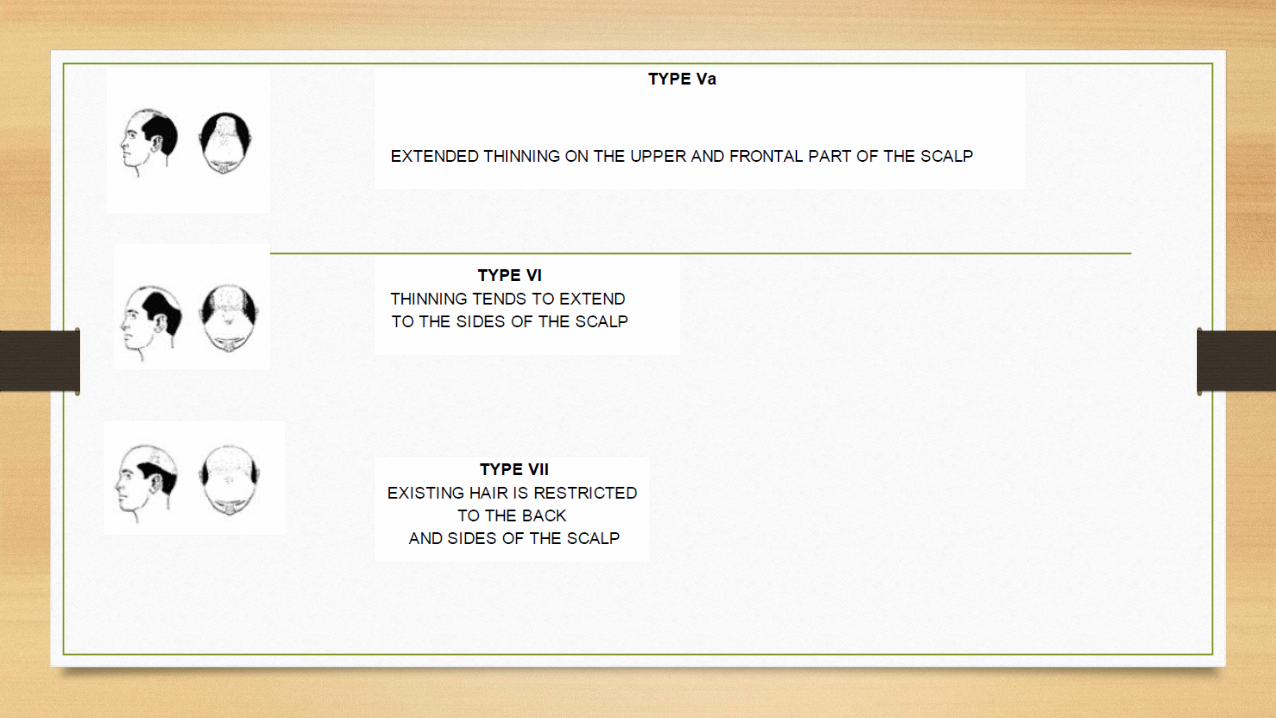
• Inadequate donor hair and too low a density, especially in patients with class VI or VII Norwood patterns.
• Patients who may have little available usable donor hair because of too much scarring from previous grafting that was healed by secondary intention.
• The patient who has unrealistic expectations.• There are also patients with medical problems that can
interfere with grafting, such as hypertension.

• Some authors avoid using adrenaline in the recipient area :
• because it increases telogen effluvium in the immediate postoperative period, and it also may diminish the uptake of the grafts.
• Adrenaline must definitely be avoided in the recipient area in women because severe effluvium has been reported after its use.

THE DONOR SITE• Objective of donor area evaluation : determine the area
from which hair is most likely to be permanent and thus will persist in the recipient area long after transplantation.
• Theses has been determined by various studies and called as “Safe Donor Area”



THE DONOR SITE• The ideal donor site is the region containing hair follicles that are not
subject to the gradual miniaturization process that causes baldness (invisible hair)
• Hair density is greatest at the midline and diminishes laterally above the ears and again below the inferior border approaching the nape of the neck.
• 50% of hair can be harvested before the donor site becomes noticeably depleted.

THE DONOR SITE• SDA fall short of helping practitioners determine the
quantity of "permanent" FU that may be transplanted over a patient's lifetime.
• Respondents suggested that the aforementioned patient presenting with an average density donor area could yield a lifetime harvest of 6,404 or 5,393 FU when destined to develop MPB types V or VI, respectively.
NUMBER OF PROCEDURES
• Patients will be pleased after only one procedure with limited hair loss• But usually with one procedure, the frontal hairline lacks adequate
density. It is appropriate to prepare most patients for at least two sessions to give a refined result.
• With current techniques of 1000 to 1500 grafts, many patients with limited hair loss require only on two procedures.
• The patient with more extensive hair loss, however, may require as many as three or four procedures.

Preoperative preparation
• The patient is asked to shampoo his head with Betadine surgical scrub on the day before, and on the morning of the surgery.

Preparation of the donor area• The hair in the donor area (occipital region) is trimmed to a length of 2–4
mm.• The local anaesthetic solution is injected just below the donor area.
The donor strip can be harvested with a single bladed knife or a multiple bladed knife containing three to seven blades.
• It is very important that while harvesting the donor area, the blades remain parallel to the direction of the hair so that the hair roots are not damaged.

Strip Excision
• Most important tenets for strip harvesting includes: 1. minimizing the amount of hair follicle transection2. extracting donor strip widths with caution in order to
minimize closing tension .3. producing only a single scar regardless of the number of
session.

Strip Excision
• To minimize the transection of hair follicles during strip harvesting :
1. Use magnification2. Use tumescent solution at the dermal level3. Skin hook technique


A long section of scalp that varies in width from 0.5 to 1.5 cm, and in length from 10 to 25 cm.
The multibladed knife harvests numerous (two to six) parallel strips of varying width (depending on the spacer used), which may be 1.5, 2, or 2.5 mm.Incision should be angled
so that the blade passes parallel to the follicles

The donor area is closed by a running/interlocking suture of 3-0 nylon suture .uture removal to be done after 14 days .

The "slivering" of thedonor strip
• The harvested donor strips are immediately immersed in chilled normal saline.
• A typical strip is 1× 20-cm (20 cm2) and contains 2,000 units.• Donor strip should be fixed to a cutting board with steady
tension applied to sustain inter-follicular spacing and ease the "slivering" process.
• A size 15 bladed scalpel is used to slice sections of tissue 1 or 2 FU.
The "slivering" of thedonor strip
• Harvested donor strip obtained using the single-blade excision method is cut into tiny slices that vary from 1 to 3 mm in width.
• The subcutaneous fatty tissue below the hair roots or bulbs is stripped leaving up to 2 mm of fat below the hair bulb.

A “sliver” produced by sectioning of the donor stripobtained with the single-blade technique showing how the follicular bulbs extend into the subcutaneous fat.

Dissection of individual FU from the "slivers."
• The grafts may be cut on wooden tongue depressors or on a clear vinyl dissecting surface with a backlighting system.
• Loupe magnification of 2X or 3X power is useful in creating FUGs.
• Graft preparation with a dissecting stereo microscope makes the dissection a little slower, but it is much more accurate.
Dissection of individual FU from the "slivers."
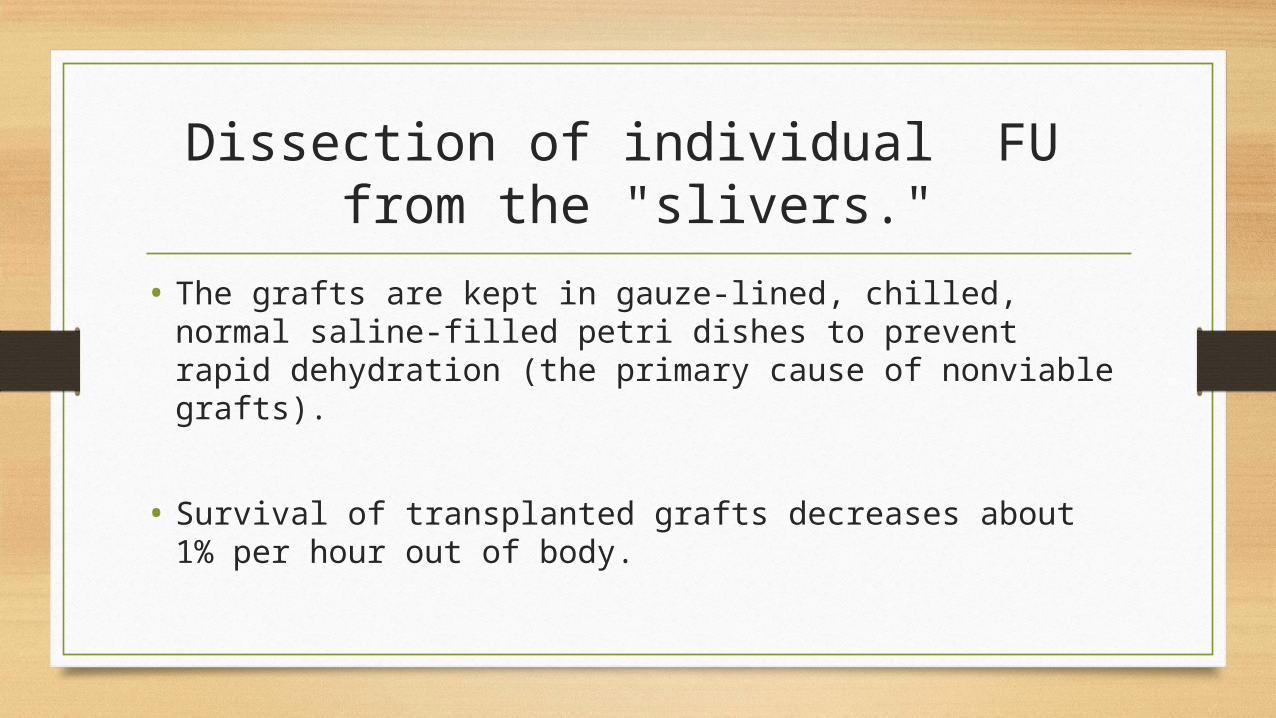
• The grafts are kept in gauze-lined, chilled, normal saline-filled petri dishes to prevent rapid dehydration (the primary cause of nonviable grafts).
• Survival of transplanted grafts decreases about 1% per hour out of body.
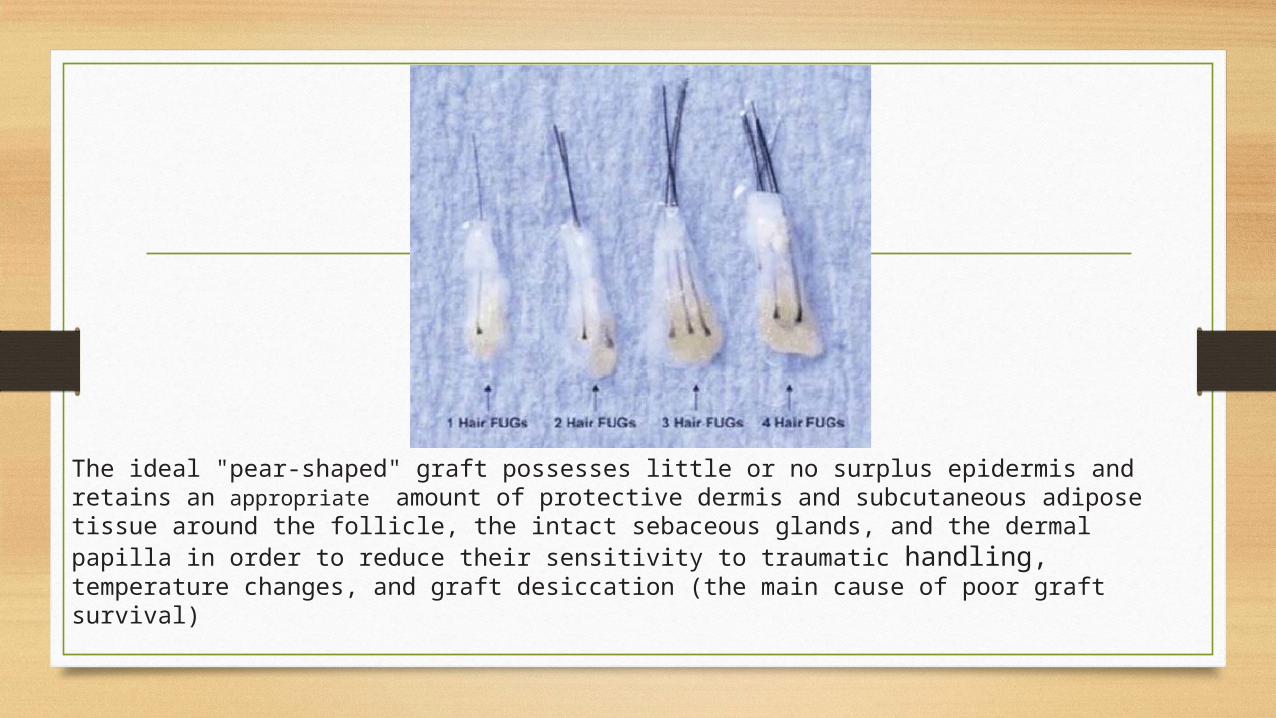
The ideal "pear-shaped" graft possesses little or no surplus epidermis and retains an appropriate amount of protective dermis and subcutaneous adipose tissue around the follicle, the intact sebaceous glands, and the dermal papilla in order to reduce their sensitivity to traumatic handling, temperature changes, and graft desiccation (the main cause of poor graft survival)

• If a multibladed knife has been used, it is possible to perform graft preparation using a device called the Mangubat graft cutter. This is a rectangular-shaped, stainless steel base containing a series of parallel, closely spaced (1- to 2-mm) blades. The strip is stretched and placed over these blades so that the hair follicles are parallel to the cutting edges. Next, a wooden tongue blade (“force spreader”) is laid on top of the strip and a rubber mallet is employed to strike (“impulsive force”) the wood surface with several rapid strokes. The entire strip is cut into grafts instantly. This saves a great deal of time for microdissection, but carries an increased risk of splitting follicular units and transecting follicles.
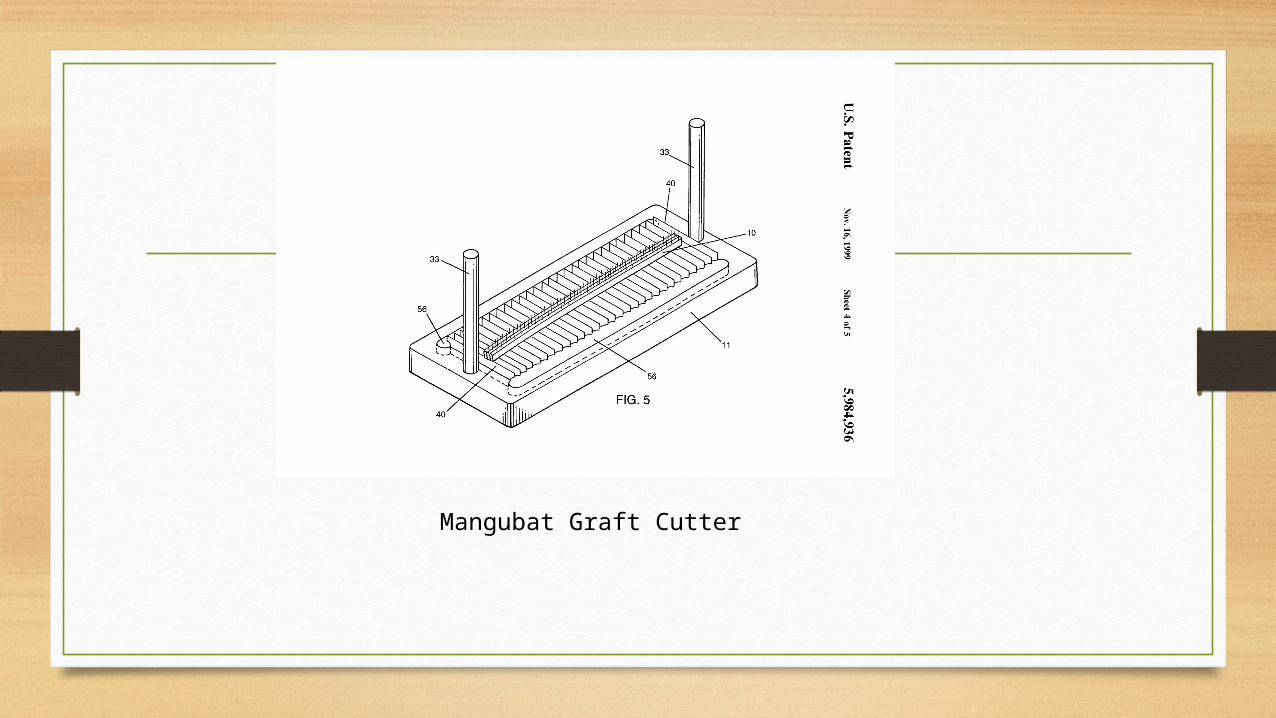
Mangubat Graft Cutter

Preparation of the recipient area
• Anesthesia : The recipient site is anesthetized using a local ring block with 1%Xylocaine with 1:100,000 epinephrine followed by infiltration of the recipient site with normal saline with 1:100,000 to 1:150,000 epinephrine.
• Regional nerve blocks of the supraorbital and supratrochlear nerves in their respective foramina located above the eyebrow can also reduce discomfort at the recipient site.

• The best long-term results are obtained by transplanting from front to back rather than back to front.
• While making slits or holes in the recipient area, it is very important to follow the direction of the existing hair in that region.

Transplanting the Midscalp region
improves density from a lateral and overhead view but also provides a thickened backdrop to a thinning frontal area as well as providing indirect coverage of a crown as transplanted midscalp hairs cascade posteriorly over it .

Transplanting The Vertex region
• Patients should also be advised that coverage may not have the same cosmetic impact in this region as elsewhere. (shingling effect).
• Decision to transplant a progressively thinning and expanding vertex carries an increased risk that an unnatural distribution of hair will result in the future in which an isolated island of transplanted hair may be surrounded by an alopecic scalp.
• May require one or more additional sessions to the "whorl" of the vertex.
Transplanting The Vertex region
• For the majority of patients, the front and midscalp have first priority and most of the donor hairs should be reserved for those regions.
• The best candidates for vertex transplantation are patients past the age of 40 years with ample donor reserve and a minimal hair-to-scalp color contrast.

Halo head” hair pattern produced by transplanting the vertex area followed by loss of hair in the peripheral regions.

• Incisional instruments : needles, miniblades, and micropunches.• For one to two hair grafts, the most commonly used instruments are
probably an 18-gauge hypodermic needle for coarse hairs and a 19-gauge hypodermic needle for finer hairs.
• Nokor needles (16/18 gauge) / 1.5-mm tribevel (Rossati Starr) punches : large (three- to four-hair) single-unit and small (three- to five-hair) double-unit grafts.
• 2-mm tribevel (Rossati Starr) punches : larger (two- to three-unit/four- to seven-hair) grafts
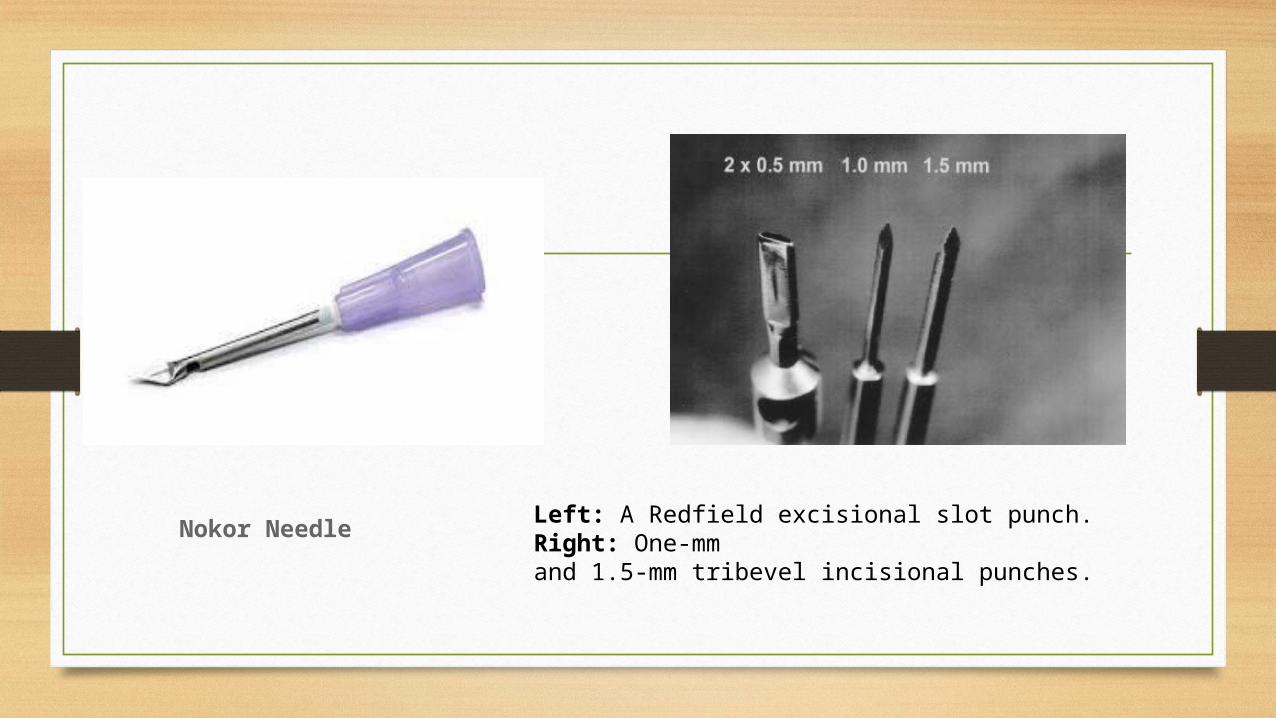
Nokor Needle Left: A Redfield excisional slot punch. Right: One-mmand 1.5-mm tribevel incisional punches.

Excisional devices : Punch
• Excisional devices : Redfield and Butterfield punches• Round and elliptical/slot• The grafts must be “cut to fit” the site, which may necessitate breaking
up follicular units.• If the grafts are of smaller diameter than the site, there will be a gap
between the sides of the graft and the walls of the recipient well. Healing will then occur by secondary intention, which may reduce graft survival.
• It may also result in “pitting” or even epidermoid cyst formation if the graft “sinks” below the surface and gets “buried alive.”
Excisional devices : Punch
• USE : employ these instruments in very fibrotic/inelastic scalps, where it is necessary to remove some tissue in order to place grafts with more than one to two hairs.
• lower-density donor sites and finer hair texture : larger grafts may be needed to achieve optimal density with fewer sessions.
• Recipient site incisions are made 0.5 to 2.0 mm apart, depending on the size and location of the grafts.

Graft insertion• It is important to employ an atraumatic technique for graft
placement.
• The grafts are placed into the recipient slits / holes using fine angled forceps.
• To avoid damage, the FUGs are grasped by the 2 mm of subcutaneous tissue left below the hair bulbs to position them into the recipient sites and not by the follicle
Graft insertion• Steady pressure is applied to ensure that the grafts are flush with
the surrounding skin .• Burying the grafts beneath the level of the skin avoided 1. because it can give a pitted appearance2. lead to the formation of epidermal cysts
If the grafts are too elevated from the surface : cobblestone appearance
Postoperative care• The patient is discharged the same day, usually without any bandage. • Traditional dressing is a bilayered protective and absorptive affair
with the first layer made from several nonstick Telfa pads covered with a thin layer of an antibiotic.
• Some swelling is obvious after a hair transplantation surgery and the patient should be informed of this prior to the procedure. Headband worn immediately after the operation is useful in preventing the swelling from coming down on to the face and creating a puffy appearance.

Postoperative care• The patient is instructed to wash his hair with a mild shampoo on
the 2 or 3 postoperative day. • While combing the hair in the transplanted area for three weeks,
the tooth of the comb should not strike against the transplanted grafts.
• Wearing clothes like T shirts or pullovers which have to be taken off over the head should also be avoided for three weeks.
• Hair oils or other stronger shampoos as well as helmets are also to be avoided for the same period.

Postoperation Adjunctive Therapy
Topical minoxidil application (2-5 %) : 1. not only for its vasodilatory effects that may enhance wound healing but
also because data suggest that minoxidil decreases postoperative effluvium .
2. Continued minoxidil use is encouraged for to 5 - 12 weeks postoperatively.
To slow or prevent further hair loss : 1 mg of finasteride to slow or prevent further hair loss and thus prevent or delay the need to “chase baldness” with multiple procedures.

Post operation Complications
1. The common complication is the occurrence of variable numbers of lesions (pustules, papules, nodules, and cysts) due to transplanted tissue becoming trapped beneath the surface in the recipient region. They appear 8 to 12 weeks after the surgery.
2. It is also fairly common to have a small number of grafts extruded in first 24 hours after surgery, with some associated localized bleeding in the recipient site.

Donor-site complications
• (a) Infection (0.1%)• (b) keloid/hypertrophic• (c) Hematoma formation • (d) Wound dehiscence/necrosis • (e) Persistent neuralgia/neuroma formation

Recipient Site Complications a) Change in hair texture usually characterized as being coarser or “frizzy,”(b) Poor graft survival ( related to tissue handling that cause follicular bulb transection)(c) Elevated (“cobblestoning”) or depressed (“pitting”) grafts that occur when grafts do not fit well into excisional recipient sites or are placed below the surface during implantation. (d) Chronic folliculitis caused by bacterial infection or foreign-body type reaction to “spicules” of transected hair shafts left in grafts
Recipient Site Complications
e) Postfrontal tissue/graft necrosis caused by inadequate blood supply to the postfrontal region where “dense packing” of grafts is commonly performed to achieve maximum density.(f) Hyperfibrotic frontal ridging caused by an overreaction to larger grafts or, perhaps, spicules of transected hairs associated with these grafts. This reaction has not been reported with single (one- to two-hair) FU grafting in the frontal line.

Postoperation Follow-up Visits
1. 1 day after the operation : for dressing change2. 14 days : Sutures are removed 3. 8 weeks : wound-healing check4. 16 weeks early regrowth check5. 6 to 12 months : final visit for photography

Outcome
• In healthy individuals with unscarred recipient sites, it is reasonable to expect 90% to 95% of the grafts to grow successfully.

Follicular Unit Extraction• This is technique that involves the removal of the intact follicular unit
directly from the donor area using a 1 mm punch.
• The yield by this harvesting technique can decrease due to transection and avulsion injury to the follicular unit.
• Although marketed as a technique that leaves no scar in the donor area, it leaves multiple ‘dotscars’ in the donor area, which are larger than those left by the strip method.

Sequel• The epidermis and dermis along with the shaft of the transplanted hair outside the
skin fall off as scabs in the two to three weeks after the surgery, but the follicles remain and go into a resting phase.
• New hairs start growing about three- six months after the procedure.
• It usually takes six to nine months to appreciate the result of a hair transplant.
• If a second procedure has been planned, it must be at least three to six months after the first sitting

Hair transplants in special sites• the direction of the eyebrow hairs while creating a new line.• Around 150 micrografts are usually required for an eyebrow of one side.• The donor site for eyebrow transplantation : should be of finer hair
preferably from• the nape of the neck or the temporal region.• Recipient holes are made with : No. 20 or 21gauge needle or a 0.7 mm
micro blade• The immediate postoperative period : Cyanoacrylate glue may be used
over the grafted areas to keep the grafts in place

















