49
Ophelia Templates and Additional Resources Templates and resources to support application of the Ophelia Manual

Ophelia Templates and Additional Resources
Templates and resources to support application of the Ophelia Manual

This research was supported under Australian Research Council’s Linkage Projects funding scheme (project LP120200111). The Victorian Department of Health contributed funds and in-kind support to the project. The views expressed herein are those of the authors and are not necessarily those of the Australian Research Council or the Victorian Department of Health.
AuthorsEditors: Dr Alison Beauchamp, Dr Sarity Dodson, Mr Roy Batterham and Professor Richard OsborneContributors: Ms Silvana Cavalli, Ms Christina Cheng, Ms Melanie Hawkins, Ms Kirsten Phillips, and Ms Jayne Power.
Cover and inside design, and layout: RoscherCreative
Funders: Australian Research Council, Victorian Government, Deakin University, Monash University
Suggested citationBeauchamp A, Dodson S, Batterham RW and Osborne RH. Ophelia Templates and Additional Resources – Templates and resources to support application of the Ophelia Manual 2017. Retrieved from www.ophelia.net.au.
© Deakin University 2017
Keywords1. Health literacy2. Health service access3. Consumer health information4. Health management and planning5. Health inequity6. Health promotion
Ophelia Templates and Additional Resources
Templates and resources to support application of the Ophelia Manual

Ophelia.net.au Templates and Additional Resources Copyright© 2017 Deakin University
ContentsPhase 1 / Step 1 – Set up 1
Activity 1.1 Identify a project focus, scope and overall aim for the project 1
Activity 1.2 Establish a project team and identify roles and responsibilities 2
Activity 1.3 Identify existing sources of data and gaps in available data 3
Activity 1.4 Establish project timelines and budget 4
Phase 1 / Step 2 – Data collection and/ or extraction 5
Activity 2.1 Establish a data collection plan 5
Activity 2.2 Obtain ethical and other approvals required 6
Activity 2.3 Collect and or extract data 7
Activity 2.4 Prepare materials for the consultation activities 8
Phase 1 / Step 3 – Response ideas consultation workshops 9
Activity 3.1 Establish a consultation plan 9
Activity 3.2 Make arrangements for the consultation workshops 9
Activity 3.3 Undertake the consultation workshops 10
Activity 3.4 Prepare a summary of the results of the consultation workshops 12
Phase 2 / Step 4 – Intervention Design 13
Activity 4.1 Confirm project focus, scope and overall aim, and specify objectives for the intervention 13
Activity 4.2 Conduct a rapid literature review and search for existing interventions 14
Activity 4.3 Identify which intervention ideas from the workshops match your intervention objectives 15
Activity 4.4 Select an intervention (or intervention package) 15
Activity 4.5 Work through the logic of your intervention, specifying how it will achieve its objective 16
Phase 2 / Step 5 – Intervention Planning 17
Activity 5.1 Identify members of your project team, and confirm project timelines and budget 17
Activity 5.2 Identify a set of project milestones, and associated activities 18
Activity 5.3 Develop an evaluation plan 19
Phase 2 / Step 6 – Intervention development and refinement 20
Activity 6.1 20

Ophelia.net.au Templates and Additional Resources Copyright© 2017 Deakin University
Activity 6.2 Undertake Quality Improvement cycles to test materials, training, manuals and processes 20
Activity 6.3 Refine materials and processes based on findings of QI cycles 21
Phase 3 / Step 7 – Implementation and evaluation 22
Activity 7.1 Refine implementation and evaluation plan 22
Activity 7.2 Implement the intervention(s) 22
Activity 7.3 Undertake evaluation activities 23
Phase 3 / Step 8 – Development of an ongoing Quality Improvement strategy 25
Activity 8.1 Identify intervention components to be embedded into usual practice 25
Activity 8.2 Develop a continuous Quality Improvement plan 25
Additional resources
Activity 1.1 Additional examples of project focus, scope and aims 27
Activity 2.1 How many people should we collect data from? Examples of sample size considerations 27
Activity 2.2 Obtain ethical and other approvals required – example of invitation letter for clients 28
Activity 2.2 Example of wording for participant information sheet 28
Activity 2.3 Sample script for recruiting clients or community members to the project 29
Activity 2.4 How to score the HLQ and present the results 30
Activity 2.4 Using cluster analysis to identify fine-grained health literacy profiles 31
Activity 2.4 Steps in undertaking cluster analysis in SPSS 32
Activity 2.4 Creating ‘vignettes’ using HLQ data 33
Activity 2.4 Template for interview to support vignette writing 34
Activity 3.2 Make arrangements for consultation workshops – Example invitation for community members 36
Activity 3.4 Examples of linking intervention ideas and intervention objectives 37
Activity 4.4 Example of combining locally generated intervention ideas with ideas from the literature 40
Activity 4.4 Selecting an intervention – what are mechanisms? 41
Activity 4.5 Example of a program logic model 42
Activity 5.3 Example of Ophelia Implementation and Evaluation Plan 43

Ophelia.net.au PAGE 1Templates and Additional Resources Copyright© 2017 Deakin University
Phase 1 / Step 1 Set up Activity 1.1 Identify a project focus, scope and overall aim for the project
What is the focus of your project (what is your project about / what issue do you want to address)?
What is the scope of your project (who will be included/ who is your target group)?
What is the aim of your project (what do you want to achieve and by when)?
Overall statement of project focus, scope and aims (e.g. our project focuses on participation in pap screening among Aboriginal and Torres Strait Islander women in our local government area. We aim to increase pap screening rates for Aboriginal and Torres Strait Islander women to the national average within 2 years).
Ophelia.net.au PAGE 2Templates and Additional Resources Copyright© 2017 Deakin University
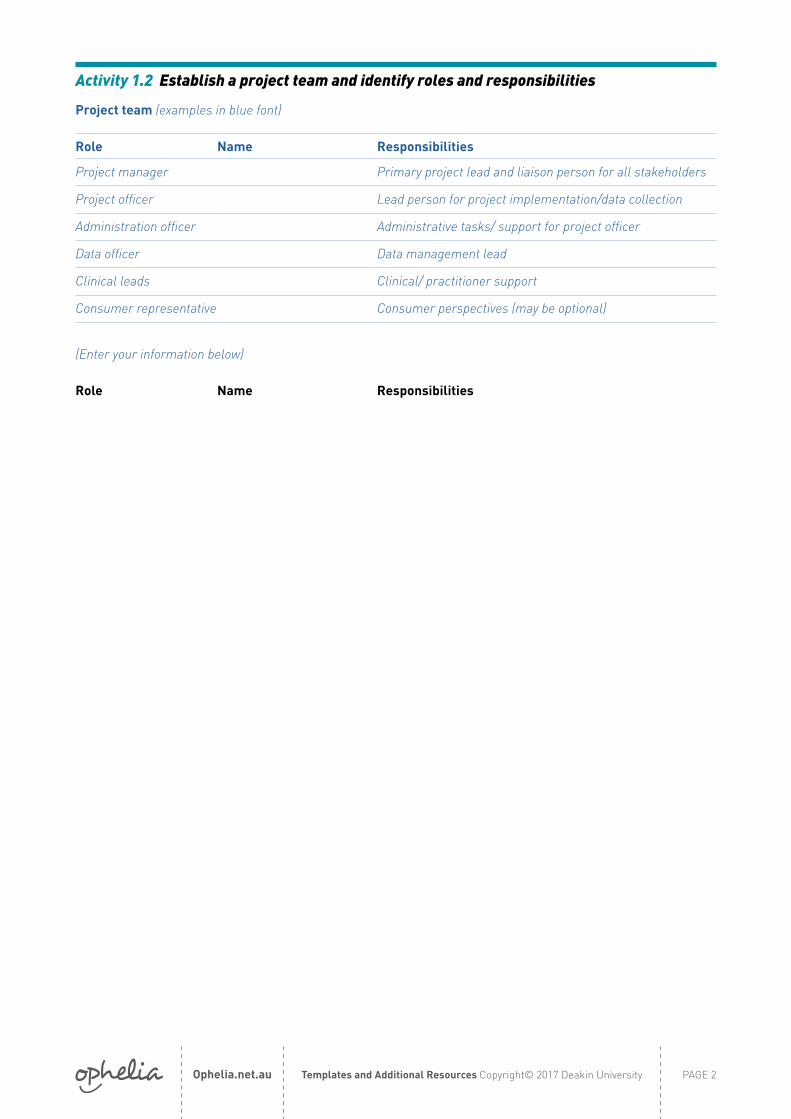
Activity 1.2 Establish a project team and identify roles and responsibilities
Project team (examples in blue font)
Role Name Responsibilities
Project manager Primary project lead and liaison person for all stakeholders
Project officer Lead person for project implementation/data collection
Administration officer Administrative tasks/ support for project officer
Data officer Data management lead
Clinical leads Clinical/ practitioner support
Consumer representative Consumer perspectives (may be optional)
(Enter your information below)
Role Name Responsibilities

Ophelia.net.au PAGE 3Templates and Additional Resources Copyright© 2017 Deakin University
Activity 1.3 Identify existing sources of data and gaps in available data
What sort of data do we need to tell us more about our target group?
Data type (Enter your information below examples in blue font)
Data type: Health status or outcomes data
What data could we collect? Data source How could we access this data?
e.g. Number of people in our service with diabetes and leg wounds; number of children under 5 with minor, self-limiting illness who present to Emergency; rates of smoking in our region
e.g. self-report; administrative data; local government data
e.g. conduct client survey; generate report from administrative datasets; access local government websites
Data type: Health/healthcare use
What data could we collect? Data source How could we access this data?
e.g. rates of Emergency Department presentations; numbers of people who fail to attend appointments
e.g. administrative data; self-report e.g. generate report from administrative datasets; conduct client survey
Data type: Health literacy strengths and limitations
What data could we collect? Data source How could we access this data?
e.g. capacity to access, understand and use information and services in relation to the project focus
e.g. interview clients; questionnaires e.g. administer the HLQ; conduct client interviews
Data type: Barriers and facilitators to engagement with health behaviours and services
What data could we collect? Data source How could we access this data?
e.g. consumer attitudes; clients’ previous experiences with service providers; referral processes; number of services available;
transport costs; social support;
e.g. survey; service-audits; administrative data; interview clients
e.g. conduct client survey or interviews, generate report from administrative datasets, audit of referral processes.

Ophelia.net.au PAGE 4Templates and Additional Resources Copyright© 2017 Deakin University
Activity 1.4 Establish project timelines and budget
Anticipated timelines
Step Time in months (example only)
1 2 3 4 5 6 7 8 9 10 11 12
1 Set up
2 Data collection and/ or extraction
3 Response ideas workshop
4 Intervention selection/ design
5 Intervention planning
6 Quality Improvement cycles to refine intervention
7 Intervention implementation and evaluation
8 Develop continuous Quality Improvement strategy
Preliminary budget template (Enter your information below examples in blue font)
Items Considerations / How much do we have available / how much will it cost?
Staffing
Printing surveys for data collection
Catering for workshops
Venue hire for workshops
Items Considerations / How much do we have available / how much will it cost?

Ophelia.net.au PAGE 5Templates and Additional Resources Copyright© 2017 Deakin University
Phase 1 / Step 2 Data collection and/or extraction Activity 2.1 Establish a data collection plan
(Enter your information below examples in blue font)
Example Example Example
What data? Health literacy and demographic data Data related to clients’ experience engaging with health care services
Patterns of service use in target group
Source of data Sample will be 80-100 new clients with chronic disease attending a community health service
Sample will be 15 clients who have previously completed the HLQ and provided their consent to interview
Routine administrative data collected by local health service
How will the data be collected?
Paper-based HLQ with additional demographic questions
Telephone interviews using semi-structured interview guide
Extracted from administrative database
Timeframe 2 months 2 weeks 2 weeks
Staff involved Project officer, staff at health service Project officer Medical records staff
Steps – specific data collection activities
Train staff in HLQ administration. Invite all new clients at intake to complete the HLQ
Telephone clients directly and conduct semi-structured interview (15-20 minutes)
Discuss data needs with appropriate staff and seek permission to access data.

Ophelia.net.au PAGE 6Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.2 Obtain ethical and other approvals required
(Enter your information below examples in blue font)
Do we need ethics approval?
e.g. Our project aims to collect health literacy and use it in a Quality Improvement activity. We will discuss with the ethics officer for our healthcare service to see if clients need to provide written, informed consent
What strategies will we use to ensure people do not feel pressured to participate?
e.g. train staff in non-coercive methods of recruitment; ask staff who are not direct care providers to recruit clients; allow clients the option of discussing with family or other staff first
How will we help people feel safe if they decide to withdraw from the study?
e.g. if providing written consent, give people a ‘withdrawal from study’ form to keep in case they change their mind; ensure people recruiting reinforce that withdrawal or refusal is permissible
How can we provide enough information to potential participants to allow them to give informed consent?
e.g. provide a clear ‘plain language statement’ if written consent is required; use teach-back to ensure that client understands; have simplified wording and read aloud for all clients.
What measures do we need to put into place for clients who want to participate but do not want to sign a consent form
e.g. If written consent is required, check with ethics if a verbal consent (with witness signature) is an option

Ophelia.net.au PAGE 7Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.3 Collect and or extract data
Suggested considerations Examples
Training of data collectors
Who will deliver the training? Two project team members
Who will we train? 4 volunteers, 3 clinicians and 2 reception staff
When and where will we deliver training? Date, venue and time
What additional resources are needed for delivery of training? PowerPoint, handouts
Where can we obtain resources for training? The Ophelia website
Quality control strategies Develop a step by step guide that all data collectors must use
Have a central contact person that collectors can call if there are any issues or queries
One person to review all data collected after 2 weeks to ensure consistency
Monitoring data collection Set up a meeting with all data collectors after 2 weeks of commencing data collection to discuss any issues. Have regular fortnightly meetings thereafter
Data collection methods
What strategies will we use All new clients to the service will be invited by their clinicians and reception staff to answer paper-based surveys. Volunteers will be available to assist clients with the survey.
How will we know if these are working? Meeting with data collectors every 2 weeks. Review demographic data every 2 weeks to ensure data is collected from a range of clients
Do we need to make changes to data collection methods? Discuss at fortnightly meetings
Do we need to notify our ethics committee of any changes? Yes
Recording the data
Where will data be recorded when, and by whom Use Excel spreadsheet available from Ophelia website, entered weekly by xx
How will paper-based surveys be returned for data collection? This process to be discussed during initial training meeting to establish the most appropriate method

Ophelia.net.au PAGE 8Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.4 Prepare materials for the consultation activities
Example of how to present findings for a workshop
Vignette 1: Fairly confident in own abilities but feels they have little support from other including health professionals
Mrs Smith is a 50 year old woman living on the outskirts of Melbourne. She was divorced 10 years ago and had to move to the outer suburbs to be able to afford to buy a home. She qualified as a primary school teacher but since the birth of her first child 25 years ago she has only done sessional work. All her children live and work away from the area.
She tries to keep healthy; she walks three times a week, and would like to do more but finds it difficult to fit it in. She sees a male GP but sometimes feels that he is a bit impatient when she talks to him about her menopausal symptoms. She hears lots of things about how to manage hot flushes and mood swings, and sometimes goes on the internet to find out more, but isn’t really sure what is relevant for her, and whether it is trustworthy information.
Health literacy profile for Vignette 1
Possible score range 1-4 Possible score range 1-5
1 2 3 4 5 6 7 8 9Cluster number
% of sample in each cluster
Feeling understood and supported by health-care providers
Having sufficient information to manage health
Actively managing my health
Social support for health
Appraisal of health information
Ability to actively engage with healthcare providers
Navigating the healthcare system
Ability to find good health information
Understand health information well enough to know what to do
1 24% 3.10 3.01 2.98 2.91 2.76 4.10 4.00 3.83 4.00
Overview Number of people in this cluster = 25 Average age = 48.8 % female = 80% % attended tertiary education = 40% Average number of health conditions = 0.9 % people with musculoskeletal conditions = 53% Average BMI = overweight
Repeat this for each vignette. You may also like to present a summary of the demographic and health literacy findings for the overall sample.
Ophelia.net.au PAGE 9Templates and Additional Resources Copyright© 2017 Deakin University
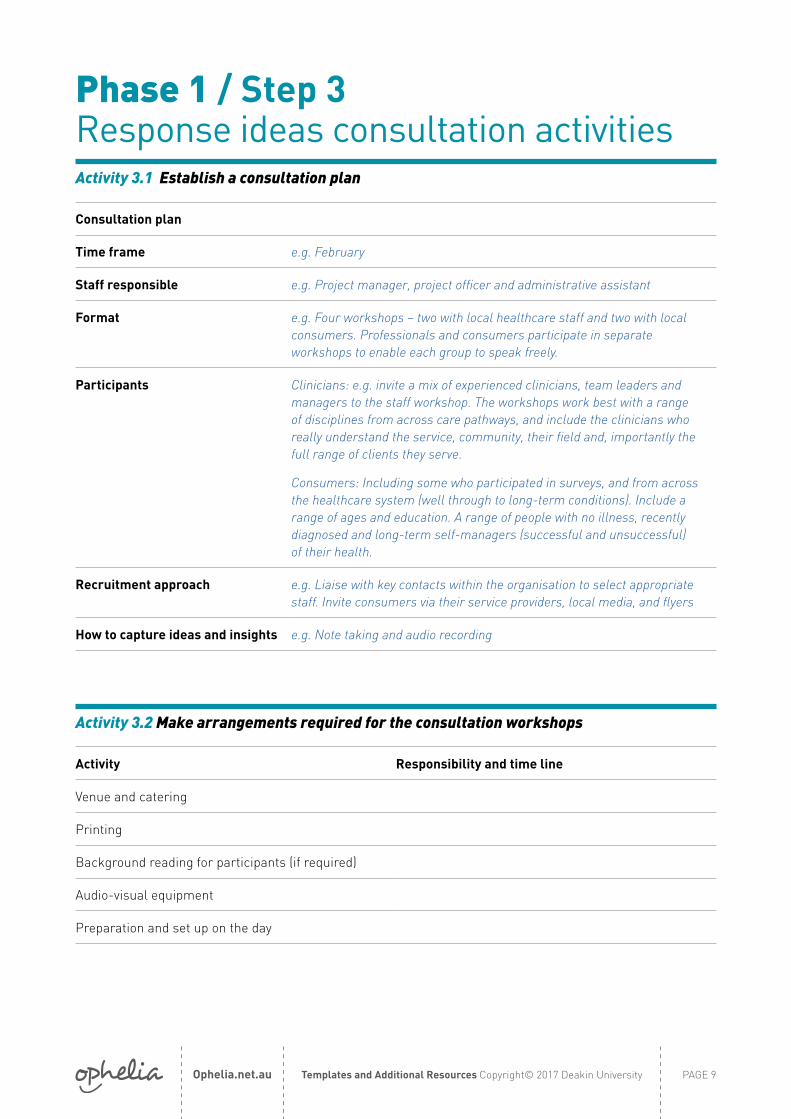
Phase 1 / Step 3 Response ideas consultation activitiesActivity 3.1 Establish a consultation plan
Consultation plan
Time frame e.g. February
Staff responsible e.g. Project manager, project officer and administrative assistant
Format e.g. Four workshops – two with local healthcare staff and two with local consumers. Professionals and consumers participate in separate workshops to enable each group to speak freely.
Participants Clinicians: e.g. invite a mix of experienced clinicians, team leaders and managers to the staff workshop. The workshops work best with a range of disciplines from across care pathways, and include the clinicians who really understand the service, community, their field and, importantly the full range of clients they serve.
Consumers: Including some who participated in surveys, and from across the healthcare system (well through to long-term conditions). Include a range of ages and education. A range of people with no illness, recently diagnosed and long-term self-managers (successful and unsuccessful) of their health.
Recruitment approach e.g. Liaise with key contacts within the organisation to select appropriate staff. Invite consumers via their service providers, local media, and flyers
How to capture ideas and insights e.g. Note taking and audio recording
Activity 3.2 Make arrangements required for the consultation workshops
Activity Responsibility and time line
Venue and catering
Printing
Background reading for participants (if required)
Audio-visual equipment
Preparation and set up on the day

Ophelia.net.au PAGE 10Templates and Additional Resources Copyright© 2017 Deakin University
Ophelia consultation workshops – what is involved?
The consultation workshops are brainstorming sessions where participants ‘respond to’ the HLQ vignettes. This is the step that is at the heart of the Ophelia process. The workshops need to have as good number of experienced frontline practitioners as possible. It is this group who see the many clients with the health literacy challenges we seek to support. The workshops allow the tacit knowledge of the best frontline clinicians and managers to emerge through a dynamic workshop environment. Given this, one of the most important attributes of the workshop facilitator is the ability to listen.
For each of the vignettes, ask the participants:
1. Do you see clients like this/ do you know people like this?
2. What sort of issues is this person facing?
3. What strategies could you use for an individual like this?
4. (for practitioners and managers) What could you do if you had many clients like this in your organisation?
Ideas are recorded by the note-taker and if desired, main themes/ ideas can also be noted on a whiteboard or flip char. Aim for at least 2 to 3 intervention ideas for each vignette.
In addition to discussing each of the vignettes, present the ‘interpretation of HLQ scales’ sheet (see the Ophelia Toolkit), and ask participants to brainstorm about what strategies they could use for people with lower scores on particular scales at both an individual and organisational level. It is not necessary to go through each of the scales, but target those scales which had lower mean scores in the overall sample from whom HLQ data was collected.
What do we mean by health literacy interventions?
In the workshops, participants are asked not to necessarily identify brand new strategies, but just to come up with response ideas. The ideas that are generated might be similar to normal practice, or may be something new. The interventions do not have to be about directly improving a client’s health literacy, but more about using health literacy as a means to achieving better health outcomes or improved access to services. Often, the interventions ideas are very broad strategies only, and the facilitator may need to gather more detail.
Key considerations for health literacy interventions are:• A focus on improving health and wellbeing
outcomes. This applies equally to efforts to optimise individuals’ health literacy and the health literacy responsiveness of the health system.
• A focus on increasing equity in health outcomes and access to services for people with varying health literacy needs
• Prioritise local wisdom, culture and systems• Focus on improvements at, and across, all levels
of the health system
If time permits and the participants are still engaged, summarise and prioritise the intervention ideas, considering their feasibility and relevance for the local context. Factors to consider in prioritising intervention ideas are:• Resources and timelines• The likelihood of achieving the goals and
objectives set out in Step 1• Are the intervention ideas likely to be equitable
and sustainable?• What is the general level of enthusiasm?• Are there major risks?• Do you want the intervention to focus on one
health literacy profile or on the broader target group?
Often, intervention ideas will overlap between different HLQ vignettes. Sometimes it is possible to combine these ideas to form a wider-reaching intervention.
Activity 3.3 Undertake the consultation workshops

Ophelia.net.au PAGE 11Templates and Additional Resources Copyright© 2017 Deakin University
Example agenda for workshop
Time Activity Resources/ comments
10.00 -10.15 Introductions
10.15 -10.30Background to the project: aims and focus, description of client group from whom HLQ data collected.
PowerPoint
10.30 -10.45 Discuss first vignette (see above questions) Brainstorming session. Could use a flip chart, whiteboard. Take notes10.45 -11.00 Discuss second vignette
11.00-11.15 Break
11.15 -11.30 Discuss third vignette Flip chart, whiteboard.
11.30 -11.45Discuss responses to lower scores for each scale
Interpretation of HLQ scores document.
11.45 -12.00 Discuss fourth vignetteFlip chart, whiteboard.
12.00 -12.15 If time permits, discuss fifth vignette
12.15 -12.45Summing up and discussion of main themes/ common intervention ideas.

Ophelia.net.au PAGE 12Templates and Additional Resources Copyright© 2017 Deakin University
Activity 3.4 Prepare a brief summary of the results of the workshops
General reflections and insights – example from a project aiming to improve clients’ management of acute exacerbation of heart failure
Vignette 1 Vignette 2 Vignette 3 Vignette 4
General insights about key issues
“This person would be someone who has a pile of information brochures from the hospital that just sit on their dining room table and never get read”
“This is a person that learns by listening to other people’s stories, like short videos or something. They also like to be shown how to do things”
This is a person who struggles to operationalise their care plan. When you ask them what they will do first, they can’t tell you”
This person has managed their health condition quite well until now, but now it is worsening. They need to know what else they must do to keep condition stable”
Intervention ideas
Make sure that we match all our patient education to how each person learns, and what they want to know
Train staff in use of teach-back and other sensitive teaching methods
Source client education materials in a variety of learning formats
Find out about local peer support groups
Train all staff in use of teach-back methods
Clients need help putting things into action – use teach-back in every interaction
Talk to other providers and family members about ways of helping clients to use care plan
Don’t try to reinvent the wheel, build upon what the client already knows or what they already use that is effective

Ophelia.net.au PAGE 13Templates and Additional Resources Copyright© 2017 Deakin University
Phase 2 / Step 4 Intervention designActivity 4.1 Confirm the project focus, scope and overall aim for the project,
and specify the intervention objectives
Statement of project focus, scope and aims and intervention objectives
e.g. Our project focuses on supporting patients with heart failure to better manage their condition and avoid preventable exacerbations. We aim to reduce the proportion of patients who present to the Emergency Department with potentially preventable exacerbations by 10% in 6 months. To achieve this, our intervention will support clients to better understand what steps are required to manage an exacerbation, to provide them with appropriate resources and to increase their use of heart failure action plans.
Ophelia.net.au PAGE 14Templates and Additional Resources Copyright© 2017 Deakin University
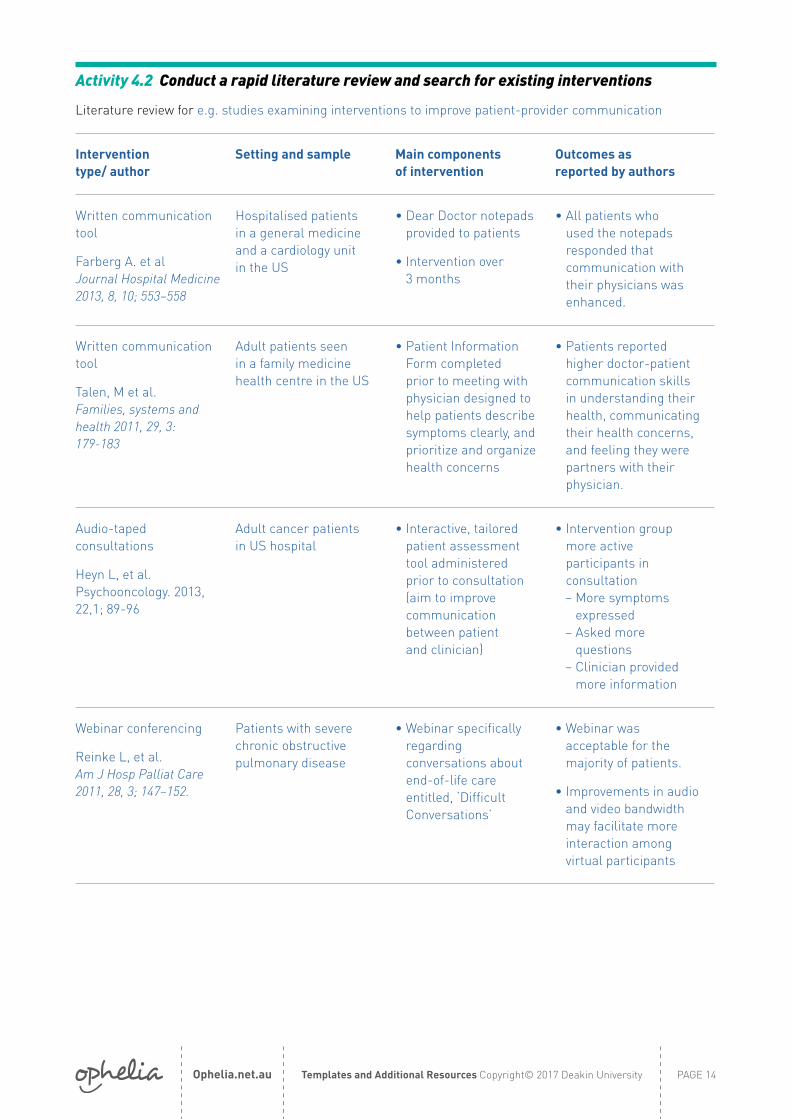
Activity 4.2 Conduct a rapid literature review and search for existing interventions
Literature review for e.g. studies examining interventions to improve patient-provider communication
Intervention type/ author
Setting and sample Main components of intervention
Outcomes as reported by authors
Written communication tool
Farberg A. et al Journal Hospital Medicine 2013, 8, 10; 553–558
Hospitalised patients in a general medicine and a cardiology unit in the US
• Dear Doctor notepads provided to patients
• Intervention over 3 months
• All patients who used the notepads responded that communication with their physicians was enhanced.
Written communication tool
Talen, M et al. Families, systems and health 2011, 29, 3: 179-183
Adult patients seen in a family medicine health centre in the US
• Patient Information Form completed prior to meeting with physician designed to help patients describe symptoms clearly, and prioritize and organize health concerns
• Patients reported higher doctor-patient communication skills in understanding their health, communicating their health concerns, and feeling they were partners with their physician.
Audio-taped consultations
Heyn L, et al. Psychooncology. 2013, 22,1; 89-96
Adult cancer patients in US hospital
• Interactive, tailored patient assessment tool administered prior to consultation (aim to improve communication between patient and clinician)
• Intervention group more active participants in consultation
– More symptoms expressed
– Asked more questions
– Clinician provided more information
Webinar conferencing
Reinke L, et al. Am J Hosp Palliat Care 2011, 28, 3; 147–152.
Patients with severe chronic obstructive pulmonary disease
• Webinar specifically regarding conversations about end-of-life care entitled, ‘Difficult Conversations’
• Webinar was acceptable for the majority of patients.
• Improvements in audio and video bandwidth may facilitate more interaction among virtual participants

Ophelia.net.au PAGE 15Templates and Additional Resources Copyright© 2017 Deakin University
Activity 4.3 Identify which intervention ideas from the workshops match your newly established intervention objectives
Intervention objectives Intervention ideas
• Increase clients’ use of heart failure exacerbation plans from 30% to 50% in 6 months
• Clients with heart failure can describe the steps required to manage exacerbation of their condition.
• Supports and resources to enable clients to understand how to manage heart failure exacerbations
• Find out each client’s preferred learning style and use this as a basis for a discussion about their individual educational needs
• Provide material in formats that patients demonstrate they understand
• Use teach-back in every interaction
• Build upon what the client already knows and what they already use that is effective
Activity 4.4 Select an intervention (or intervention package)
Agreement between stakeholders about selected intervention – and brief description of reason for choice

Ophelia.net.au PAGE 16Templates and Additional Resources Copyright© 2017 Deakin University
Activity 4.5 Work through the logic of your intervention, specifying how it will achieve its objective
Program Logic Template
Longer-term Outcomes e.g. reduce unplanned admissions to hospital for heart failure
↑Medium-term Outcomes e.g. clients use their heart failure action plans more effectively
↑Short-term Outcomes e.g. clients have increased knowledge and confidence to put their heart
failure plans into action
↑Outputs e.g. clinicians use teach-back with clients to help them understand how
to use their heart failure action plan
↑Activities e.g. train clinicians in use of teach-back and provide supporting resources
↑Inputs e.g. The Ophelia learning styles assessment tool, develop understandable information
for clients, develop teach-back training program and resources for clinicians
Definitions
Resources/ inputs – What is needed for the activities to occur. These can include human, organisational or community resources in any combination.
Activities – The specific actions that make up the program. Activities are synonomous with interventions
Outputs – What the specific activities will produce or create. Outputs can include descriptions of audiences or targets delivered by the program.
Outcomes – Changes as a result of the program. These are often divided into short, medium and long-term outcomes
Figure 2 – Program logic template
Long term outcomes
Start with outcomes
Medium term
outcomes
Short term outcomes
OutputsActivitiesResources/
inputs

Ophelia.net.au PAGE 17Templates and Additional Resources Copyright© 2017 Deakin University
Phase 2 / Step 5 Intervention planningActivity 5.1 Identify members of your project team, identify roles and responsibilities,
and confirm your project time frame and budget
Project team
Role Name Responsibilities
Project manager Primary project lead and liaison with stakeholders
Project officer Lead person for intervention implementation/ evaluation
Administration officer Administrative tasks/ support for project officer
Training lead Trains staff in delivery of intervention
Clinical leads Clinical/ practitioner support
Working groups
Working group activities Staff
Develop implementation and evaluation plan
Develop training program and materials for staff
Develop resources for intervention delivery
Pilot testing
Evaluation of intervention and final report
Budget
Items How much will it cost?
Staff training in delivery of the intervention
Staff time for delivering the intervention
Venue for staff training
Printing of resources used in training
Printing of resources used in delivery of the intervention
Timelines
Task Time
Finalise implementation and evaluation plan 2 weeks
Preparation of resources for training and intervention
4 weeks
Pilot testing of resources and processes 1 month
Delivery of training to all staff 2 weeks
Delivery of intervention 3 months
Evaluation of intervention 1 month

Ophelia.net.au PAGE 18Templates and Additional Resources Copyright© 2017 Deakin University
Activity 5.2 Identify a set of project milestones, and associated activities – for intervention development, implementation and evaluation
Milestone Example milestones Example activities
Milestone 1: Finalisation of the project implementation and evaluation plan
Produce a project implementation and evaluation plan that includes:a) an overview of the project focus, aims
and intervention objectives;b) the intervention logic model;c) a table specifying the evaluation plan,d) a summary of the project staffing, timelines
and budget, and;e) a table specifying the materials, staff training, tools and
equipment required for implementation and evaluation of the intervention, their availability and their cost.
Milestone 2: Finalisation of intervention materials and process guidelines
Purchase (or develop) the materials, training, manuals, etc. detailed in the implementation and evaluation plan
Test and refine the processes, materials, training, manuals, tools and equipment
Milestone 3: Ethics approval (if required) Submit ethics application/s and refine processes as required to obtain ethical approval
Milestone 4: Intervention commencement
Undertake intervention and evaluation activities as detailed in the implementation and evaluation plan
Milestone 5: Intervention completion
Milestone 6: Evaluation completion
Ophelia.net.au PAGE 19Templates and Additional Resources Copyright© 2017 Deakin University
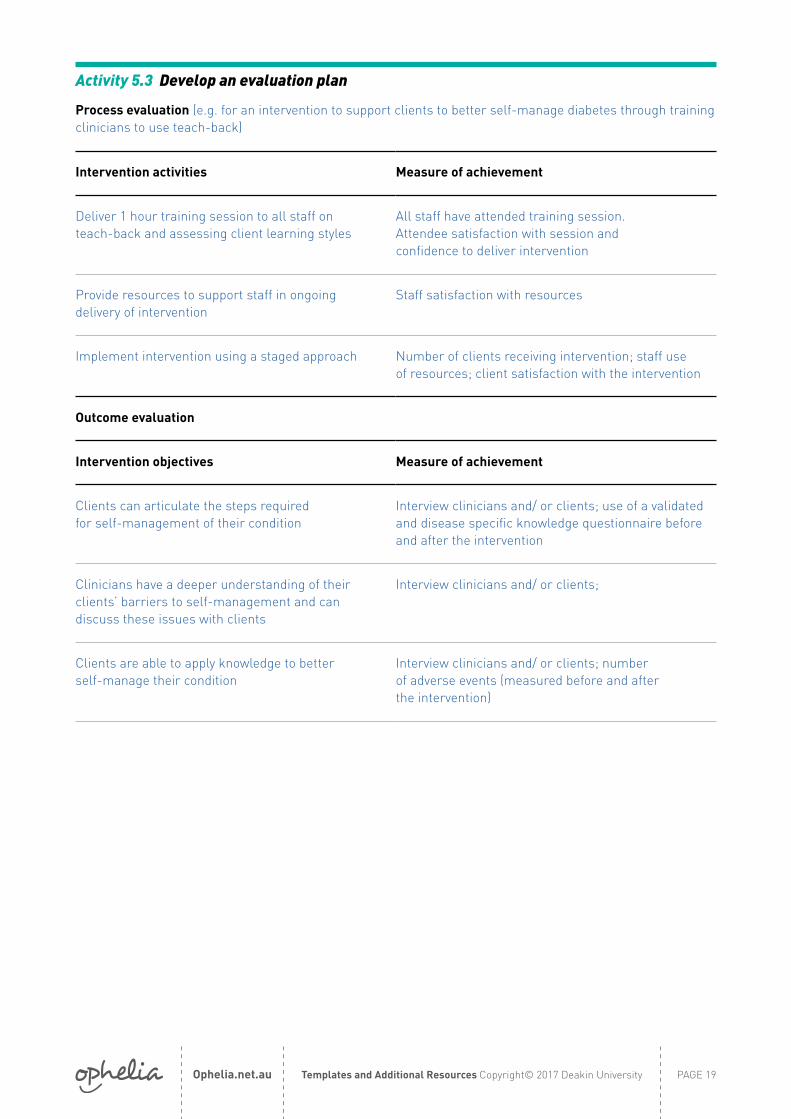
Activity 5.3 Develop an evaluation plan
Process evaluation (e.g. for an intervention to support clients to better self-manage diabetes through training clinicians to use teach-back)
Intervention activities Measure of achievement
Deliver 1 hour training session to all staff on teach-back and assessing client learning styles
All staff have attended training session. Attendee satisfaction with session and confidence to deliver intervention
Provide resources to support staff in ongoing delivery of intervention
Staff satisfaction with resources
Implement intervention using a staged approach Number of clients receiving intervention; staff use of resources; client satisfaction with the intervention
Outcome evaluation
Intervention objectives Measure of achievement
Clients can articulate the steps required for self-management of their condition
Interview clinicians and/ or clients; use of a validated and disease specific knowledge questionnaire before and after the intervention
Clinicians have a deeper understanding of their clients’ barriers to self-management and can discuss these issues with clients
Interview clinicians and/ or clients;
Clients are able to apply knowledge to better self-manage their condition
Interview clinicians and/ or clients; number of adverse events (measured before and after the intervention)

Ophelia.net.au PAGE 20Templates and Additional Resources Copyright© 2017 Deakin University
Phase 2 / Step 6 Intervention development and refinementActivity 6.1 Purchase or develop the materials, training, and processes
detailed in the implementation and evaluation plan
Materials/ trainings/ processes Staff responsible Planned Completion Date
Activity 6.2 Undertake Quality Improvement (QI) cycles to test materials, training, manuals and processes
Quality Improvement cycle e.g. for project aiming to improve referral processes between co-located dental service and primary health service
Plan Preparatory activities include the following:• Establish electronic referral process between dental services to primary health
services. • Develop marketing material for dental team and for primary health care team• Orientate ‘pilot’ dentist(s) and primary health central intake staff to intervention
Planned completion date =
Do • One dentist engaged to action 1-2 referrals to primary health following agreed process. Referral actioned by central intake staff. Modify process and repeat if necessary.
• Provide marketing material to up to 5 clients of each service.• Modify intervention and repeat if necessary.
Planned completion date =
Study Undertake the following evaluation activities, review results and make decisions about required modifications to the interventions or evaluation strategies.• Participants referred between dental service and primary health services, and
participants viewing marketing material take part in evaluation activities (Semi structured phone interviews focused upon satisfaction with referral, marketing material, and utility of service provided in their daily lives.) Modify questions if required and repeat.
• All referrers, referees and intake staff take part in evaluation activities (Semi structured phone interviews focused upon satisfaction with process). Modify questions if required and repeat.
• Documentation of referrals made, rates of attendance of participants to primary health services
Planned completion date =
Act • Modify evaluation activities and repeat if necessary.• Modify interventions and repeat if necessary
Planned completion date =

Ophelia.net.au PAGE 21Templates and Additional Resources Copyright© 2017 Deakin University
Activity 6.3 Refine materials and processes based on findings of QI cycles
Materials / trainings / processes
Changes required Staff responsible Planned Completion Date

Ophelia.net.au PAGE 22Templates and Additional Resources Copyright© 2017 Deakin University
Phase 3 / Step 7 Implementation and evaluationActivity 7.1 Refine implementation and evaluation plan
What changes are needed?
Who is responsible for making these changes
By when Are additional resources required?
Activity 7.2 Implement the intervention(s)
Example of record keeping for an intervention to increase clients’ use of heart failure action plans
Monthly reports on:
Number of eligible clients
Number of clients seen
% that chose each of the learning styles
% who had their learning styles needs met
% clinicians who reported applying teach back
Reason for using teach-back
Average number of times teach-back used for each client
Any challenges noted by clinicians or clients
Any adverse events or other issues
Any changes made to the intervention as a result of the adverse event
Ophelia.net.au PAGE 23Templates and Additional Resources Copyright© 2017 Deakin University
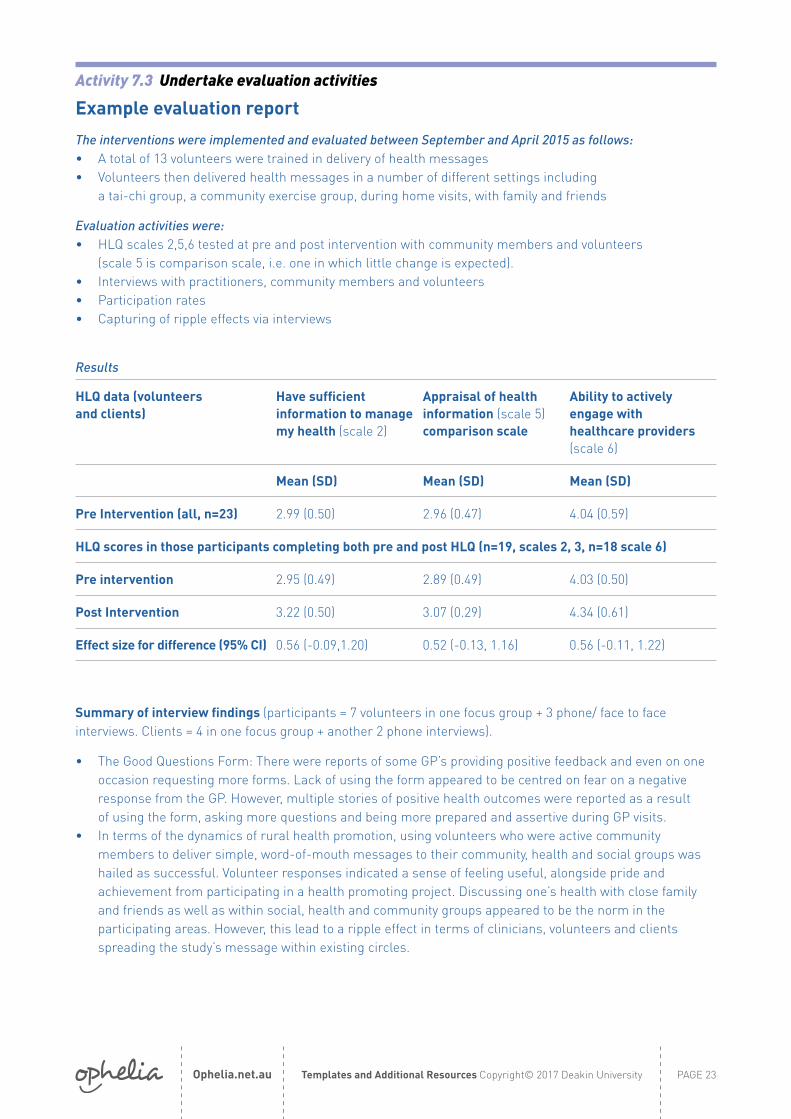
Activity 7.3 Undertake evaluation activities
Example evaluation report
The interventions were implemented and evaluated between September and April 2015 as follows: • A total of 13 volunteers were trained in delivery of health messages • Volunteers then delivered health messages in a number of different settings including
a tai-chi group, a community exercise group, during home visits, with family and friends
Evaluation activities were:• HLQ scales 2,5,6 tested at pre and post intervention with community members and volunteers
(scale 5 is comparison scale, i.e. one in which little change is expected). • Interviews with practitioners, community members and volunteers• Participation rates• Capturing of ripple effects via interviews
Results
HLQ data (volunteers and clients)
Have sufficient information to manage my health (scale 2)
Appraisal of health information (scale 5) comparison scale
Ability to actively engage with healthcare providers (scale 6)
Mean (SD) Mean (SD) Mean (SD)
Pre Intervention (all, n=23) 2.99 (0.50) 2.96 (0.47) 4.04 (0.59)
HLQ scores in those participants completing both pre and post HLQ (n=19, scales 2, 3, n=18 scale 6)
Pre intervention 2.95 (0.49) 2.89 (0.49) 4.03 (0.50)
Post Intervention 3.22 (0.50) 3.07 (0.29) 4.34 (0.61)
Effect size for difference (95% CI) 0.56 (-0.09,1.20) 0.52 (-0.13, 1.16) 0.56 (-0.11, 1.22)
Summary of interview findings (participants = 7 volunteers in one focus group + 3 phone/ face to face interviews. Clients = 4 in one focus group + another 2 phone interviews).
• The Good Questions Form: There were reports of some GP’s providing positive feedback and even on one occasion requesting more forms. Lack of using the form appeared to be centred on fear on a negative response from the GP. However, multiple stories of positive health outcomes were reported as a result of using the form, asking more questions and being more prepared and assertive during GP visits.
• In terms of the dynamics of rural health promotion, using volunteers who were active community members to deliver simple, word-of-mouth messages to their community, health and social groups was hailed as successful. Volunteer responses indicated a sense of feeling useful, alongside pride and achievement from participating in a health promoting project. Discussing one’s health with close family and friends as well as within social, health and community groups appeared to be the norm in the participating areas. However, this lead to a ripple effect in terms of clinicians, volunteers and clients spreading the study’s message within existing circles.
Ophelia.net.au PAGE 24Templates and Additional Resources Copyright© 2017 Deakin University
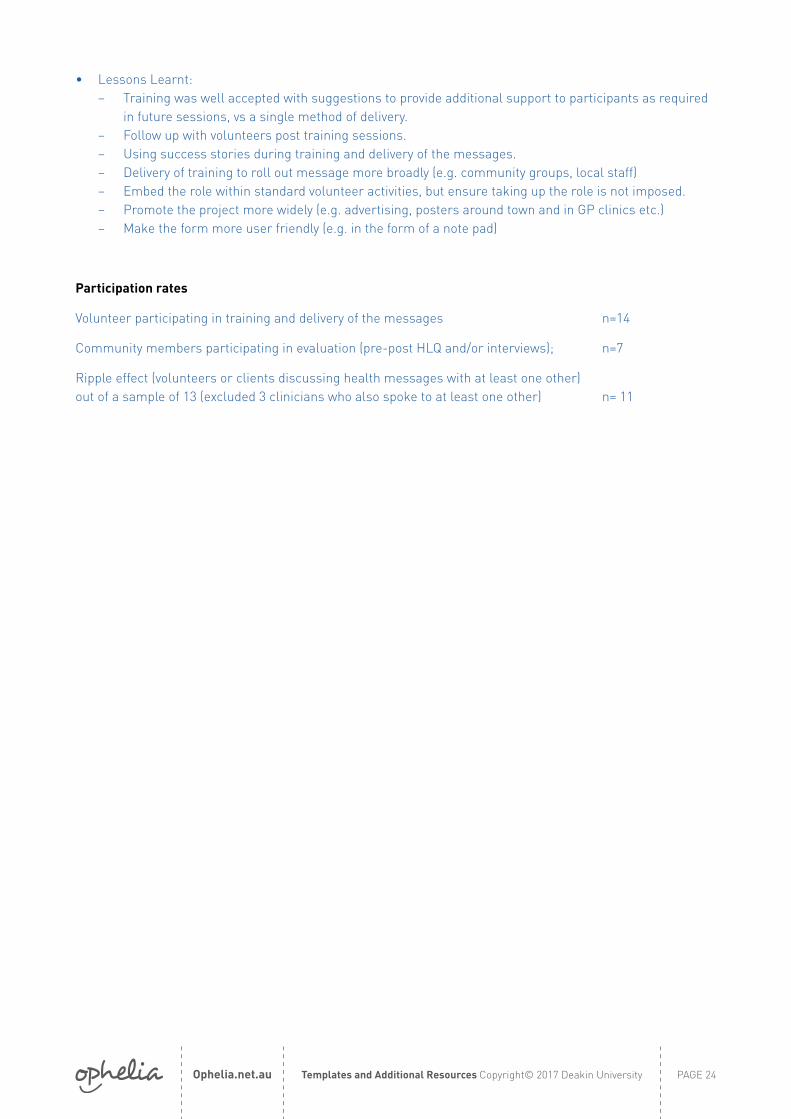
• Lessons Learnt: – Training was well accepted with suggestions to provide additional support to participants as required
in future sessions, vs a single method of delivery. – Follow up with volunteers post training sessions. – Using success stories during training and delivery of the messages. – Delivery of training to roll out message more broadly (e.g. community groups, local staff) – Embed the role within standard volunteer activities, but ensure taking up the role is not imposed. – Promote the project more widely (e.g. advertising, posters around town and in GP clinics etc.) – Make the form more user friendly (e.g. in the form of a note pad)
Participation rates
Volunteer participating in training and delivery of the messages n=14
Community members participating in evaluation (pre-post HLQ and/or interviews); n=7
Ripple effect (volunteers or clients discussing health messages with at least one other) out of a sample of 13 (excluded 3 clinicians who also spoke to at least one other) n= 11

Ophelia.net.au PAGE 25Templates and Additional Resources Copyright© 2017 Deakin University
Phase 3 / Step 8 Development of an ongoing Quality Improvement strategyActivity 8.1 Identify intervention components to be embedded into usual practice
Does the organisation plan to continue to provide all or some of the interventions?
Do you envisage any problems or barriers to continuing to offer all or some of the interventions?
Do you see any benefits associated with continuing to offer all or some of the interventions?
Do you plan to make any changes to the materials or processes and why?
Activity 8.2 Develop a continuous Quality Improvement plan
Outline your strategy for continuing to develop the intervention:
What are the next steps?
Who will be responsible for developing this?
What will you do to overcome potential risks/problems?
What approach will you take to monitoring and reviewing progress and success?
What resources and supports do you / would you need to continue to offer the intervention and ensure it grows/develops/succeeds?
How, when and to whom will the QI activities be reported?
How will you ensure the intervention continues to be implemented?
Ophelia Manual – Additional Resources

Ophelia.net.au PAGE 27Templates and Additional Resources Copyright© 2017 Deakin University
Phase 1 Additional resourcesActivity 1.1 Establish a focus, scope and aim – additional examples of project focus, scope
and aims
Project focus: High numbers of falls among elderly people in the community
Project scope: Older people in the community who are frail and socially isolated
Project aim: To decrease the rate of falls in older community members within 2 years
Project focus: Access to diabetes educational materials for people who are vision impaired
Project scope: Nationwide, people with diabetes who are vision impaired
Project aim: To develop educational materials that are appropriate for visually impaired people with diabetes
Project focus: Building emergency first aid providers’ capacity to deliver health education in the community
Project scope: All emergency first providers in 3 shanty towns in South Africa
Project aim: For 60% of emergency first aid providers to routinely deliver health education in the community within 12 months
Project focus: Inappropriate use of General Practitioners’ (GP) services for minor illness in children under 5 years
Project scope: Parents and carers of children under 5 years in a GP catchment area
Project aim: To reduce the inappropriate use of GP services by 20% in 2 years
Activity 2.1 Establish a data collection plan.
How many people should we collect data from? Examples of sample size considerations
A multicultural service wanted to explore health service use in migrants. They aimed to collect data from 150 people in total. Their sample included 50 people born in Australia, 50 people who were ‘new’ migrants, and 50 people who had emigrated to Australia more than 5 years previously.
A small service wanted to increase adolescent client’s use of action plans for exacerbation of asthma. Because they were a small service, they invited all eligible clients to participate in a survey. Data was collected from 73 of the 170 clients who were eligible to participate.
A university health service wanted to understand students’ health behaviours, particularly for international students. They aimed to collect data from 300 students in total. This included students across 3 courses, half of whom were international students, and half domestic. This allowed for comparison of health behaviours between domestic and international students, and between students from the 3 different courses.
Ophelia.net.au PAGE 28Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.2 Obtain ethical and other approvals required – example of invitation letter for clients
(minimum size 12 font)
You are invited to take part in a study about health information. We would like to find out if the health information you are given by XXX is useful to you.
You do not have to help but if you would like to know more about this study, then please read the participant information form below.
After you have read the participant information form, if you decide you would like to be in this study, please fill out the consent form and give it back to the person who discussed it with you.
The ethics committee of XXX has approved this research.
Activity 2.2 Obtain ethical and other approvals required – example of wording for participant information sheet
For ethics application for data collection using the HLQ
As a client of [service, program], you are invited to take part in a study about health information.
What the study is aboutThe main reason for this study is to help your health service understand whether the information they give you is useful. This will help them to improve the services they provide.
What does being in the study involve?Being in the study involves filling in a survey. For most people it takes 10 to 20 minutes to complete the survey.
There are three ways that you can fill in the survey: 1. Someone at the health service can help you. This could be someone you know, or – if you prefer –
someone who is not involved in your care.2. OR you can complete it yourself (a family member or friend can help), 3. OR a researcher from xx can telephone you and ask you the survey questions over the phone.
If you decide to be in the study we would also like your permission for [service provider] to give us some information about which programs and services they are providing to you.
Risks and potential benefits to participantsWe do not expect that there will be any risk to you from being in this study.
There are no direct benefits to you if you take part in this study; however, your involvement will help [service provider] better understand what their clients need.
How your privacy and confidentiality will be protectedYour privacy and confidentiality will be fully protected. Your name or any identifying details will not be included in any reports or articles about the study. All data will be stored on password protected computers or in locked filing cabinets. Ethical approval for this study has been granted by XXX Human Research Ethics Committee.
Ophelia.net.au PAGE 29Templates and Additional Resources Copyright© 2017 Deakin University
How the study’s findings will be publishedA summary of the results will be given to [service provider] and you will be able to get a copy. Conference papers and scientific journal articles will submitted for publication. You will not be identified in any of these reports or publications.
Withdrawing from the studyYou have the right to withdraw from this study at any time, without giving a reason.
If you choose not to be in this study or if you choose to withdraw it will not affect your relationship with [service provider] in any way.
Researcher’s contact detailsIf you have any further questions about this study, please contact the study’s principal investigator (provide contact details)
ComplaintsIf you have any complaints about this study, the way it is being conducted, or any questions about your rights as a study participant, then you may contact: (provide contact details)
Activity 2.3 Collect and/ or extract data – Sample script for recruiting clients or community members to the project
This is a sample script that staff may wish to use when asking clients if they would like to participate in data collection.
I’d like to ask you about being in a project that [name of organisation/ service] is involved in. The project wants to find out about how well our clients understand the information we give them, and the ways in which they use health services.
Would you like to contribute to this project? If so, you will need to complete a survey about health and health information. It takes about 20 minutes.
You can fill the survey in yourself or we can help you with it. It doesn’t need to be done all at once.
Your answers are confidential. Only staff involved in the project will have access to your answers on the survey. If you don’t want to do the survey, that’s fine. It won’t affect or change anything about your care.
Please have a think about this, or talk to your family about helping with this project and let me know. [If signed consent to participate is required] If you do want to do the survey you will need to sign a form from the ethics committee at [xxx] to say you agree to be in the project.

Ophelia.net.au PAGE 30Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.4 Prepare materials for the consultation activities – How to score the HLQ and present the results
The HLQ is a multi-dimensional tool comprised of 9 separate scales. The HLQ is not designed to provide a single summative score; rather it provides a comprehensive picture of a person’s health literacy needs and strengths.
The HLQ has nine individual scales
HLQ scales Scores
1. Feeling understood and supported by healthcare providers High
2. Having sufficient information to manage my health Mod
3. Actively managing my health Low
4. Social support for health Very high
5. Appraisal of health information Very low
6. Ability to actively engage with healthcare providers High
7. Navigating the healthcare system Low
8. Ability to find good health information Very low
9. Understand health information well enough to know what to do Very high
This person scores more highly on their ability to understand health information and to engage with healthcare providers. They have at least one trusted healthcare provider, and strong social support for health. They have lower scores in their ability to find and appraise health information to navigate the healthcare system. They also score relatively low on actively managing their health.
Each scale contains between 4 to 6 questions. Scales are scored by summing the responses to each question and dividing by the number of questions in that scale. This provides a mean score for each scale. The first 5 scales have a mean score range of 1-4, while the last 4 scales have a mean score range of 1-5.
HLQ data can be presented in several ways:
Presenting the mean scores for each scale for the overall sample:
The mean scores for each of the nine scales can be presented for an overall group of clients.
Or HLQ scores can be compared between two different demographic groups to show where differences in health literacy profiles occur.
You can also enter HLQ data into the Ophelia website (www.ophelia.net.au). The website will calculate the scores for you and provide you with a table of the results. To do this, you will need to be a registered user of the website. See Ophelia.net.au for more details.
1
1.5
2
2.5
3
3.5
4
4.5
5
1
1.5
2
2.5
3
3.5
4
4.5
5
1.Healthcareprovidersupport
2.Sufficientinformation
3.Activitymanagehealth
4.Socialsupporthealth
5.Appraisalinformation
6.Engage withproviders
7.Navigatehealth system
8.Find healthinformation
9.Understandhealth
information
1.Healthcareprovidersupport
2.Sufficientinformation
3.Activitymanagehealth
4.Socialsupporthealth
5.Appraisalinformation
6.Engage withproviders
7.Navigatehealth system
8.Find healthinformation
9.Understandhealth
information
HLQ scale scores (mean, SD) Differences by language (mean, SD)

Ophelia.net.au PAGE 31Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.4 Using cluster analysis to identify fine-grained health literacy profiles
Within any group of clients/ community members, there will be variation in their health literacy profiles. Presenting just the overall mean scores for the group will hide this variation. Cluster analysis is a technique for grouping people with similar health literacy profiles together. The analogy we use is supermarket trolleys – the healthy eaters have more fresh, low fat items in their trolley and just a few high sugar items, while the less healthy eaters have more high sugar, high fat products, and fewer fresh items.
Cluster analysis can be undertaken in several common statistical packages including SPSS. The pivot table function in Excel is then used to format the data for presentation.
Example of health literacy profiles of a group of clients (using cluster analysis)
Possible score range 1-4 Possible score range 1-5
Cluster number
% of sample in each cluster
1 Feeling understood and supported by health-care providers
2 Having sufficient information to manage health
3 Actively managing my health
4 Social support for health
5 Appraisal of health information
6 Ability to actively engage with healthcare providers
7 Navigating the healthcare system
8 Ability to find good health information
9 Understand health information well enough to know what to do
1 22% 3.68 3.45 3.40 3.50 3.16 4.55 4.40 4.26 4.46
2 24% 3.17 3.01 2.93 2.98 2.76 4.10 4.00 3.83 4.00
3 20% 3.35 2.91 3.08 3.12 2.84 3.74 3.47 2.96 2.83
4 20% 2.72 2.49 2.74 2.54 2.43 3.44 3.32 3.31 3.71
5 14% 2.83 2.39 2.70 2.68 2.23 2.38 2.19 1.94 2.24
A traffic light system of colour coding is used, so that green cells represent higher scores and red cells represent lower scores for this sample. In this example, 22% of the sample have overall ‘higher’ health literacy scores (cluster number 1), 34% of the sample have ‘lower’ health literacy scores (cluster numbers 4 and 5), and 44% have a mix of scores (cluster numbers 2 and 3).
Importantly, the health literacy profiles of each cluster are distinctly different from each other.

Ophelia.net.au PAGE 32Templates and Additional Resources Copyright© 2017 Deakin University
Activity 2.4 Steps in undertaking cluster analysis in SPSS
Data preparation
Ensure any demographic or other variables that you want to include in your final vignettes are either continuous (such as age) or binary (yes/no). Categorical data will need to be converted to binary.
Run cluster analysis in SPSS (more detail in SPSS handbook)
1. Click ‘ hierarchical cluster analysis’ from ‘analyse’ menu (located within ‘classify’ option)2. Select the appropriate variables (in this case the nine scale scores)3. Label cases by ‘caseid’4. Cluster by ‘cases’5. Click ‘statistics’ button. Select ‘range of solutions’ option and enter 3 to 16 (you may decide
on more or less). Click ‘continue’6. Click ‘method’ button. Select ‘Ward’s method’ option from ‘cluster method’ drop down menu. 7. In the ‘method’ box, select ‘Standardize’. Select the z-scores option. 8. Click ‘save’ button. Save the same range of solutions entered in step 5.9. Click ‘OK’. 10. Click ‘save as’ option from ‘file’ menu. Save as ‘excel 2007 through to 2010’ file to appropriate location.
Finalise excel data file
1. Give worksheet an appropriate name.2. Create StDev columns. One for the items in part 1 of the questionnaire and one for part 2.
Calculate stdev using stdev s (sample) option.3. Create ‘overall average score’ column. Calculate ‘overall average score’ for all HLQ items.4. Ensure binary (yes/no) variables are coded as 0 = no and 1 = yes (e.g. for gender, create a variable
called female, with females = 1 and males = 0)5. Find and replace ‘#NULL!’ with nothing.
Create pivot table
1. Select ‘pivot table’ from the ‘data’ menu. Select ‘new sheet’ option.
2. To ‘values’ field add:
– Caseid
– Each scale score (change to average)
– Overall score (change to average)
– Std_dev for parts 1 and 2 (change to average)
– Each scale score (change to Std_dev)
– And any demographic variables that will help you describe the people in each cluster. Examples of these are:
• Age (change to average)
• Sex (change to sum)
• Number of conditions (change to average)
– If demographic/ clinical variables are continuous data such as age, then change to average, if binary, then change to sum.
Examine cluster solutions
1. Add a worksheet and label it ‘clusters’2. Set up column headings and ‘freeze’ top row3. Return to the pivot table, add ‘cluster 1’ to ‘row labels’ field4. Copy and paste results from pivot table into ‘cluster’ worksheet. Check data corresponds

Ophelia.net.au PAGE 33Templates and Additional Resources Copyright© 2017 Deakin University
to heading labels.5. Examine available cluster solutions and select the most meaningful and usable solution.
Generally, this will be somewhere between 4 and 8 clusters. a) Consider standard deviation (SD). If > 0.6, this indicates there is still considerable variation within
a cluster. If the number of people in that cluster is very small, SD is likely to be naturally high, so is not a reliable indicator in this case.
b) Consider whether the pattern of health literacy scores in one cluster appear different to others. Examine demographic and clinical data associated with that cluster to determine if there are obvious differences between clusters.
c) The agglomeration schedule can also be used to help determine the optimal cluster solution (see SPSS handbook for more detail).
Preparing materials for presentation
1. Produce cluster summary document by copying relevant components of table outlining selected cluster solution.
2. Develop vignettes to present alongside each selected cluster (see Activity 2.4, below). – You will probably not have enough time to present a large number of clusters and vignettes
during the workshop. – Select a range of clusters that show the diversity in your sample.
Activity 2.4 Creating ‘vignettes’ using HLQ data
In cluster analysis, HLQ data can be combined with demographic data to provide a clear picture of what a typical person in each cluster might look like. This is done using pivot tables in Excel.
Example of health literacy profiles of a group of clients (using cluster analysis)
Possible score range 1-4 Possible score range 1-5
Cluster number
% of sample in each cluster
1 Feeling understood and supported by health-care providers
2 Having sufficient information to manage health
3 Actively managing my health
4 Social support for health
5 Appraisal of health information
6 Ability to actively engage with healthcare providers
7 Navigating the healthcare system
8 Ability to find good health information
9 Understand health information well enough to know what to do
4 20% 2.72 2.49 2.74 2.54 2.43 3.44 3.32 3.31 3.71
Average age of people in cluster
% in cluster who are female
% in cluster who live alone
% in cluster with low education
% in cluster with private health insurance
% in cluster born overseas
% in cluster who speak other primary language
Average number of chronic conditions in people in cluster
% in cluster who report feeling depressed
76.3 years
73% 84% 69% 30% 81% 69% 3 77%

Ophelia.net.au PAGE 34Templates and Additional Resources Copyright© 2017 Deakin University
Demographic data for people in cluster number 4 shows that a typical person is female, older, and is likely to live alone. They are also likely to have lower education (i.e. not completed secondary school), and to not have private health insurance, suggesting they may have lower socioeconomic status. They are likely to be born overseas and to not speak the local language. The average number of chronic health conditions for people in this cluster is 4, and nearly 80% of this cluster report feeling depressed.
We can then combine the health literacy profile of people in this cluster with their demographic data to build a vignette or ‘story’ about the challenges that person might experience in trying to look after their own health. An example of a scenario for a typical person from cluster 4, above, might be:
Lucinda is a 76 year old lady who lives alone. She was born in Poland, and left there 35 years ago. She speaks limited English. Her husband died some years ago, and Lucinda has an adult daughter who lives the other side of town. Lucinda doesn’t like to ask her daughter for help to get to medical appointments as she knows she is busy with her own family (HLQ scale 4). Lucinda has Type 2 diabetes, arthritis and back pain, and most of the time feels quite low in her mood. She sees lots of different health professionals, but struggles to find one she can really talk to and trust (scale 1). Recently her doctor told her that her blood pressure was too high and that she needed to start a low salt diet. She was too afraid to ask him questions about this (scale 6) as he always seems in too much of a hurry, and now she is not sure where she can go to for more help (scales 2 & 7) or information (scale 8). She thinks maybe she should ask her elderly neighbour for advice (scale 5). She is not sure that she can be bothered anyway to change her diet – it all seems too hard, and she has plenty of other things to worry about (scale 3).
Interviews can also be conducted with a sample of people who answered the HLQ to understand more about the answers they gave. This information can be used to provide further evidence for the vignettes (see below for interview template). These vignettes can then be used in consultation activities with expert front-line practitioners, managers and/ or community members in order to generate practical and needs-based interventions to improve health outcomes.
Activity 2.4 Template for interview to support vignette writing
Purpose: the main purpose of these interviews is to explore the stories behind why participants have answered questions from the HLQ in the way that they have. This information will be used to provide context for vignette development.
Interview preparation: This stage is undertaken after HLQ data is collected and analysed. There are two ways of identifying which clients to interview. You can either examine the HLQ results and randomly identify clients who appear to have overall patterns of lower, medium and higher scores, or you can undertake cluster analysis and then interview 2 or 3 clients from within 3-5 key clusters. You will need the client’s HLQ scores to determine in which domains they have lower scores and in which they have higher scores. Choose the most significant HLQ domains only, there is no need to talk about them all.
Information for the participant: “The information you give will contribute to the work we are doing in understanding healthcare. It will take us about 15 – 30 minutes to answer the questions. The questions are about the answers you gave on the questionnaire. There are no right or wrong answers, so please answer the questions based on your own experience. If you need to stop at any time, just let me know. I will be recording the interview for accuracy and writing up.”
Ophelia.net.au PAGE 35Templates and Additional Resources Copyright© 2017 Deakin University
Examples of interview questions as indicated by HLQ (lower /higher) scores
Scale 1. Feeling understood and supported by healthcare providers
Higher scores: Your answers for this scale suggest you have good relationships with your healthcare providers – is this how you see it? Why is this? OR
Lower scores: Your answer for this scale suggest that you’ve found it difficult to establish good relationships with healthcare providers. Has it always been this way? What would help you to improve these relationships?
Scale 2. Having sufficient information to manage my health
Higher scores: What helps you to feel you have enough information to manage your health and make decisions? OR
Lower scores: What would help you to feel confident that you have enough information about your health?
Scale 3. Actively managing my health
Higher scores: How did you learn to manage your health? What do you do to manage your health? OR Lower scores: What do you need to help you manage your health differently?
Scale 4. Social support for health
Higher scores: What has helped you to build a strong system of support from family and friends? ORLower scores: What would help you to build relationships with family or friends?
Scale 5. Appraisal of health information
Higher scores: What helps you to understand health information? How do you work out what is best for you? OR
Lower scores: What would help you to understand health information and work out what is best for you?
Scale 6. Ability to actively engage with healthcare providers
Higher scores: How comfortable do you feel about talking about your health with healthcare providers? What has helped you with this? OR
Lower scores: How comfortable do you feel about talking with healthcare providers? What would help you to feel more comfortable to talk with them about your health?
Scale 7. Navigating the healthcare system
Higher scores: How do you find out about the health and support services that you need? OR Lower scores: What would help you to find out about health support services that you need?
Scale 8. Ability to find good health information
Higher scores: What has helped you to find information about your health? OR Lower scores: What would help you to find information about your health?
Scale 9. Understanding health information well enough to know what to do
Higher scores: What has helped you to understand written health information? OR Lower scores: What would help you to understand written information about your health?
Ophelia.net.au PAGE 36Templates and Additional Resources Copyright© 2017 Deakin University
Activity 3.2 Make arrangements for consultation workshops – Example invitation for community members
(minimum size 12 font)
Community workshop on health literacy
We invite you to attend a group workshop at (venue) on (date) from (start time and end time)
What is the workshop about?
The group workshop is to find out about how easy or difficult it is for you and people you know to: • talk with health care workers such as your family doctor • find good health information • look after your own health and that of your family • get the health services that you need
People from the community – like you – already know what they need to be able to do these things. This is what we will ask you about in the workshop
What will happen in the workshop?
We will first show you some short ‘stories’ about the way in which people manage to look after their own health.
The people in these stories are made up, even though they may sound like someone you know.
We will then ask you, and other people in the group workshop some questions. These questions will be about: • what you think that person might need, or • what their local health or community services might do you help them look after their health more easily.
We will ask you these questions as a group. Please feel free to answer the question honestly and put forward any ideas you have.
The workshop will be run by (name of person running workshop)
What will happen to the answers I give?
The answers that the group provides will be recorded so that we can write them down and discuss them with local community organisations and health services.
You will not be identified in anything that we write about this workshop. Your name will be removed from any notes that we take, and if you prefer, you can use a false name.
If you are interested in being part of this workshop, please contact xxxxx
Ophelia.net.au PAGE 37Templates and Additional Resources Copyright© 2017 Deakin University
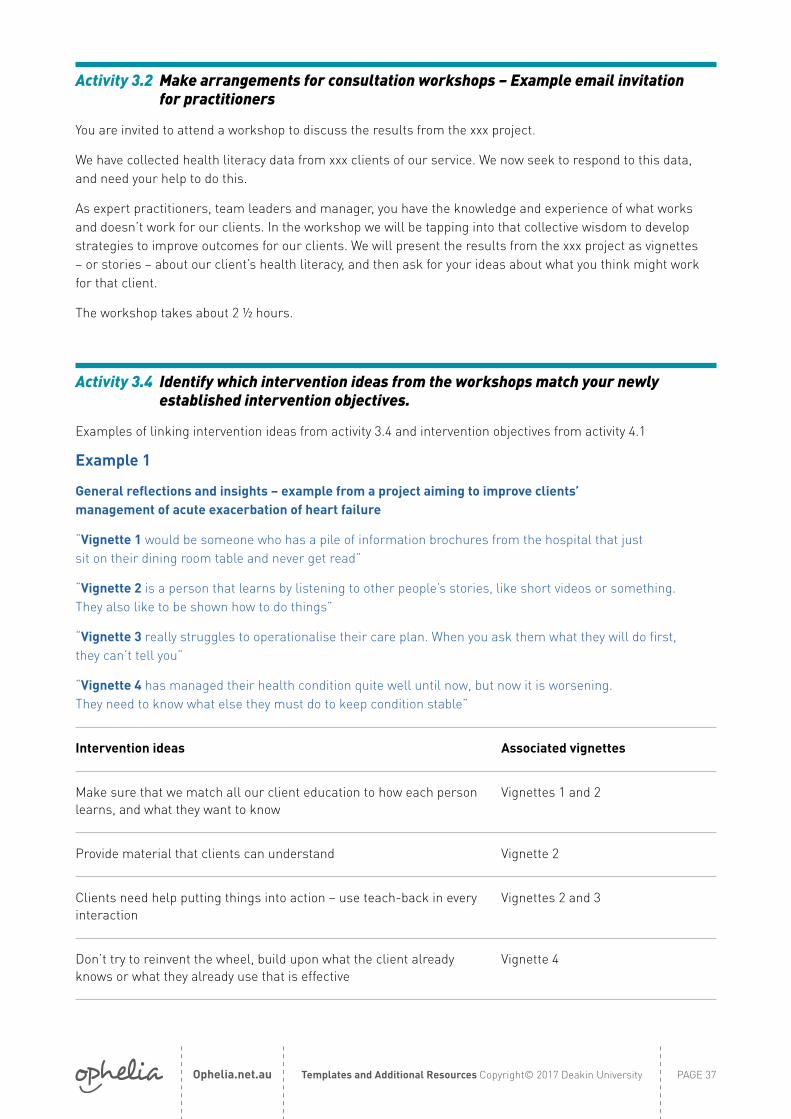
Activity 3.2 Make arrangements for consultation workshops – Example email invitation for practitioners
You are invited to attend a workshop to discuss the results from the xxx project.
We have collected health literacy data from xxx clients of our service. We now seek to respond to this data, and need your help to do this.
As expert practitioners, team leaders and manager, you have the knowledge and experience of what works and doesn’t work for our clients. In the workshop we will be tapping into that collective wisdom to develop strategies to improve outcomes for our clients. We will present the results from the xxx project as vignettes – or stories – about our client’s health literacy, and then ask for your ideas about what you think might work for that client.
The workshop takes about 2 ½ hours.
Activity 3.4 Identify which intervention ideas from the workshops match your newly established intervention objectives.
Examples of linking intervention ideas from activity 3.4 and intervention objectives from activity 4.1
Example 1
General reflections and insights – example from a project aiming to improve clients’ management of acute exacerbation of heart failure
“Vignette 1 would be someone who has a pile of information brochures from the hospital that just sit on their dining room table and never get read”
“Vignette 2 is a person that learns by listening to other people’s stories, like short videos or something. They also like to be shown how to do things”
“Vignette 3 really struggles to operationalise their care plan. When you ask them what they will do first, they can’t tell you”
“Vignette 4 has managed their health condition quite well until now, but now it is worsening. They need to know what else they must do to keep condition stable”
Intervention ideas Associated vignettes
Make sure that we match all our client education to how each person learns, and what they want to know
Vignettes 1 and 2
Provide material that clients can understand Vignette 2
Clients need help putting things into action – use teach-back in every interaction
Vignettes 2 and 3
Don’t try to reinvent the wheel, build upon what the client already knows or what they already use that is effective
Vignette 4

Ophelia.net.au PAGE 38Templates and Additional Resources Copyright© 2017 Deakin University
Intervention objectives
Consumer health behaviours• Increase clients’ use of heart failure exacerbation plans from 30% to 50% in 6 months
Consumer skills, knowledge and attitudes• Clients with heart failure can describe the steps required to manage exacerbation of their condition.
Supports and resources for consumers• Supports and resources to enable clients to understand how to manage heart failure exacerbations
Linking intervention objectives with intervention ideas
Intervention objectives Intervention ideas
• Increase clients’ use of heart failure exacerbation plans from 30% to 50% in 6 months
• Clients with heart failure can describe the steps required to manage exacerbation of their condition.
• Supports and resources to enable clients to understand how to manage heart failure exacerbations
• Find out each client’s preferred learning style and use this as a basis for a discussion about their individual educational needs
• Provide material that clients can understand• Use teach-back in every interaction • Build upon what the client already knows
and what they already use that is effective
Example 2
General reflections and insights- example from a project aiming to improve breast cancer survivors activity levels
“Vignette 1 would be someone who would likely exercise if she had someone to do it with”
“Vignette 2 is a person that gets inspired by listening to how other people have succeeded with something”
“Vignette 3 just doesn’t feel confident about exercising
Intervention ideas Associated vignettes
Use existing volunteers as health mentor ‘buddies’ for socially isolated or less motivated clients
Vignettes 1 & 3
Link clients to groups that already exist in the community Vignette 1
Share ‘success stories’ about how women have managed to increase their activity
Vignette 2

Ophelia.net.au PAGE 39Templates and Additional Resources Copyright© 2017 Deakin University
Intervention objectives
Consumer health behaviours• Increase average physical activity rates among our service’s breast cancer survivors
from 30 minutes to 120 minutes per week over the next five years
Consumer skills, knowledge and attitudes• Breast cancer survivors have increased confidence and motivation to exercise
Supports and resources for consumers• Supports and resources to enable clients to feel more confident and motivated to exercise
Linking intervention objectives with intervention ideas
Intervention objectives Intervention ideas
• Increase average physical activity rates among our service’s breast cancer survivors from 30 minutes per week to 120 minutes per week over the next five years
• Breast cancer survivors have increased confidence and motivation to exercise
• Supports and resources to enable clients to feel more confident and motivated to exercise
• Use existing volunteers as health mentor ‘buddies’ for socially isolated or less motivated clients
• Link clients to groups that already exist in the community
• Share ‘success stories’ about how women have managed to increase their activity
Ophelia.net.au PAGE 40Templates and Additional Resources Copyright© 2017 Deakin University
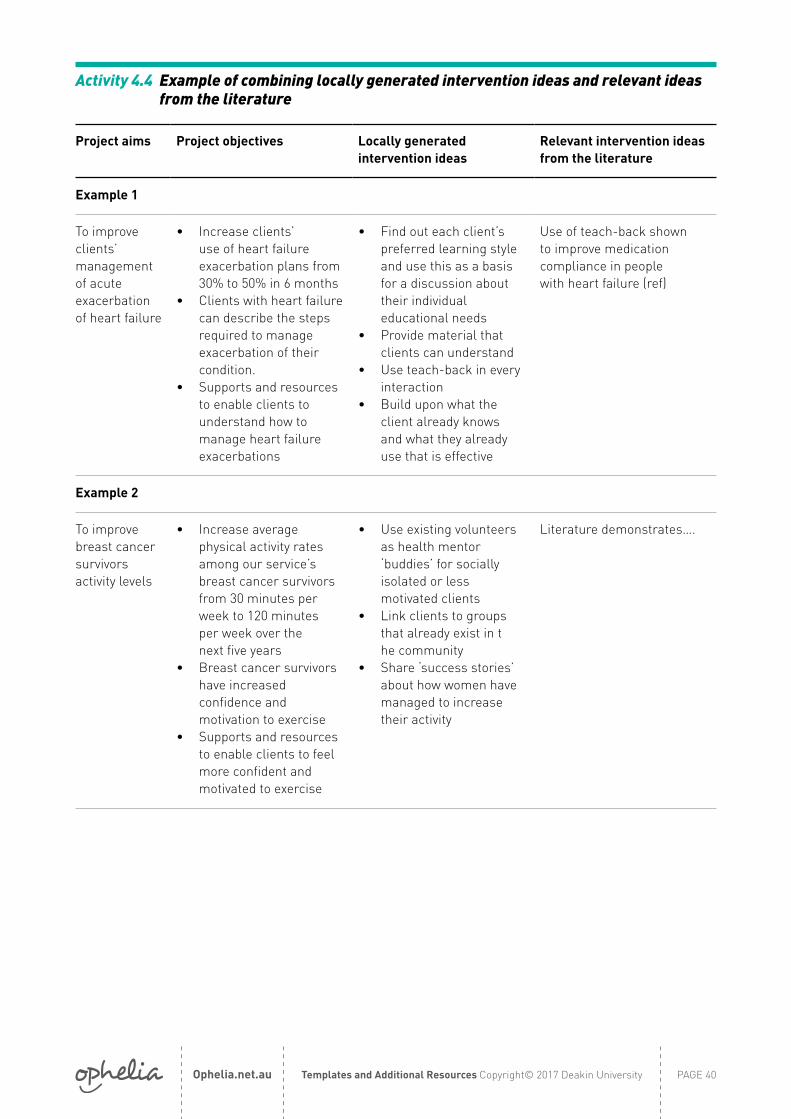
Activity 4.4 Example of combining locally generated intervention ideas and relevant ideas from the literature
Project aims Project objectives Locally generated intervention ideas
Relevant intervention ideas from the literature
Example 1
To improve clients’ management of acute exacerbation of heart failure
• Increase clients’ use of heart failure exacerbation plans from 30% to 50% in 6 months
• Clients with heart failure can describe the steps required to manage exacerbation of their condition.
• Supports and resources to enable clients to understand how to manage heart failure exacerbations
• Find out each client’s preferred learning style and use this as a basis for a discussion about their individual educational needs
• Provide material that clients can understand
• Use teach-back in every interaction
• Build upon what the client already knows and what they already use that is effective
Use of teach-back shown to improve medication compliance in people with heart failure (ref)
Example 2
To improve breast cancer survivors activity levels
• Increase average physical activity rates among our service’s breast cancer survivors from 30 minutes per week to 120 minutes per week over the next five years
• Breast cancer survivors have increased confidence and motivation to exercise
• Supports and resources to enable clients to feel more confident and motivated to exercise
• Use existing volunteers as health mentor ‘buddies’ for socially isolated or less motivated clients
• Link clients to groups that already exist in t he community
• Share ‘success stories’ about how women have managed to increase their activity
Literature demonstrates….

Ophelia.net.au PAGE 41Templates and Additional Resources Copyright© 2017 Deakin University
Activity 4.4 Select an intervention – what are mechanisms?
What are ‘mechanisms’?
Mechanisms are the hypothesised or actual means by which an intervention produces a benefit. Mechanisms always involve some change in client experiences (either a specific intervention or a change in the way services are delivered or exposure to new influences (people or information)) and nearly always this change is expected to produce some change in internal factors in the client (knowledge, beliefs, balancing of priorities, ability to link advice to action etc.) which, in turn, will lead to some change in actions. If the client experiences nothing new or different then nothing will change.
While other mechanism operate at different levels of an intervention (e.g. staff and organisational levels), these all support the activation of the core mechanism at the patient level:
Changes in what clients experience → changes in internal factors that enable changed health actions and outcomes
Three examples related to health literacy are:
1. Patients who contact the service for the first time feel that they are being listened to and that their concerns are the primary interest of the staff rather than the completion of a set of bureaucratic activities is hypothesised to lead to patients have greater trust in the organisation and greater belief in its relevance and the likelihood that it will help them
2. Following a consultation with the doctor patients are given support to plan exactly how they will put the doctor’s advice into action is hypothesised to lead to increased ability to understand medical advice and translate it into a set of daily actions.
3. Patients have the opportunity to discuss practical issues related to caring for their health with other people who they consider to be ‘like them’ is hypothesised to lead to people have a greater belief that looking after their health well is possible and have a pool of practical ideas and access to problem solving support.
Different interventions can be used to activate the same mechanism depending on client needs, the local context and the way in which the service is organised.
• For example, in example 2 above, the support for action planning could be provided in many different ways: by the doctor, by a follow-up nurse consultation, by phone-follow-up, by community health volunteers etc. The most appropriate strategy may depend on workforce and scheduling issues, proximity to the community, availability of phones, community health infrastructure and so forth.
• Similarly a single intervention may activate many beneficial mechanisms.
Focusing on the link between client experiences and internal processes (mechanisms) helps us to draw ideas and evidence from a broad body of literature
• For example, we may be led to examine questions such as ‘What experiences build trust between patients and doctors’? ‘What experiences help people translate advice into an action plan?’ ‘What experiences make people feel confident that they know which advice to trust?’ These are mechanism oriented questions that will lead to a set of principles that still allow organizations in different contexts, cultures, heath systems etc. to develop their own approaches to providing their client group with the requisite experiences.

PAGE 42Templates and Additional Resources Copyright© 2015 Deakin UniversityOphelia.net.au
Activity 4.5 Example of a program logic model
Example of a program logic for an intervention to train Country Women’s Association (CWA) members to act as mentors for frail elderly community members, to support them with gentle exercise and to deliver health messages.
Resources/ inputs → Activities → Outputs → Short term outcomes → Medium term outcomes → Long term outcomes
Resources and training content for educating CWA members is developed
→
Training for CWA members in delivery of health messages & supporting clients within gentle exercise group programs →
CWA mentors are able to support elderly people with gentle exercise and to deliver simple health messages. →
CWA mentors engage with elderly community members during the group exercise programs
→
Elderly clients feel cared about, and gain practical support and information.
CWA mentors improve their communication skills.
Both grups have increased social connectedness.
→
Improved knowledge of falls prevention and simple health activities among elderly community members at risk of falls
Source existing gentle exercise program
→Train facilitator to deliver the exercise program in a group setting
→Appropriate gentle exercise program is delivered, supported by CWA mentors
↑

PAGE 43Templates and Additional Resources Copyright© 2015 Deakin UniversityOphelia.net.au
Activity 5.3 Example of Ophelia Implementation and Evaluation Plan
Overall focus/ goal: The overall focus for the activities is for clients with chronic conditions to better self-manage their health
TO MAKE THE INTERVENTION WORK WE NEED: THE INTERVENTION IS: THE OUTPUTS ARE: WHAT WE WANT TO ACHIEVE
Inputs (what is needed for activities to occur)
Activities (specific activities that make
up the intervention)
Outputs (what the specific activities
will produce)Short term outcomes Medium term outcomes Longer term outcomes
• Develop practitioner training materials and content.
• Develop materials for ongoing support
• Develop strategy for engaging staff in the intervention
• Deliver 1 hour training session to staff on teach-back and assessing client learning styles
• Implement intervention using a staged approach
• Provide resources to support staff in ongoing delivery of intervention
• Practitioners are skilled and confident to engage with clients in appropriate education activities
• Mode of intervention delivery is matched to clients’ individual health literacy needs
• Clients and practitioners have increased rapport
• Improved health literacy in clients in relation to self- management.
• Clients have established and effective health management routines that they can maintain independently
• Impact = increased appropriate demand for early intervention and self-management services.
HOW THESE ACTIVITIES AND OUTCOMES COULD BE EVALUATED
• Staffing time and costs for training
• Staffing time and costs for ongoing delivery of the intervention
• Costs related to printing of resources
• Response and continued participation rates (clients and practitioners)
• Practitioners’ confidence and skill evaluated via focus groups after 2 months
• Satisfaction with delivery evaluated using semi-structured interviews with a sample of clients
• Shorter term outcomes measured by interview with clients and practitioners
• Medium term outcomes measured using relevant domains of the HLQ pre and post intervention
• Longer term outcomes measured by client and practitioner interview or self-management questionnaires
• Increased use of services measured by changes in the number and types of services engaged.
What materials, staff training, manuals, tools and equipment are required for implementation and evaluation of the intervention?Materials Available Need to purchase? Time to develop Training content for clinician training No No 4 weeks Resources to support staff in assessing learning stylesStaff training
Tools and equipment

The Ophelia team would like to make this resource as useful as possible.
Please send your feedback to:

















